effects of antihypertensive therapy on cardiac function
TRANSCRIPT

Effects of antihypertensive therapy on cardiac function
The failure of clinical trials in the treatment of hypertension to show protection against mortality from coronary heart disease has prompted a major reconsideration of the indications and modes of therapy. One area of concern is the lipid disturbances seen with diuretics and non-ISA (intrinsic sympathomimetic activity) beta blockers; another is the negative inotropic effect of beta blockers. The more widespread use of vasodilators-either alpha-blockers, angiotensin-converting enzyme (ACE) inhibitors, or calcium channel blockers-therefore seems appropriate. Among the calcium channel blockers, nicardipine appears to be a particularly attractive choice, in part because of its lack of negative inotropism. (AM HEART J lg88;118:280.)
Norman M. Kaplan, MD. Dallas, Texas
The heart may be involved in the pathogenesis of hypertension. Whether it is or not, the heart certain- ly is affected by the rise in systemic vascular resis- tance that is the hemodynamic hallmark of estab- lished hypertension. Increasing attention is being directed to the (presumably) secondary conse- quences of hypertension on the heart and the more clinically relevant effects of various antihyperten- sive therapies on cardiac function.
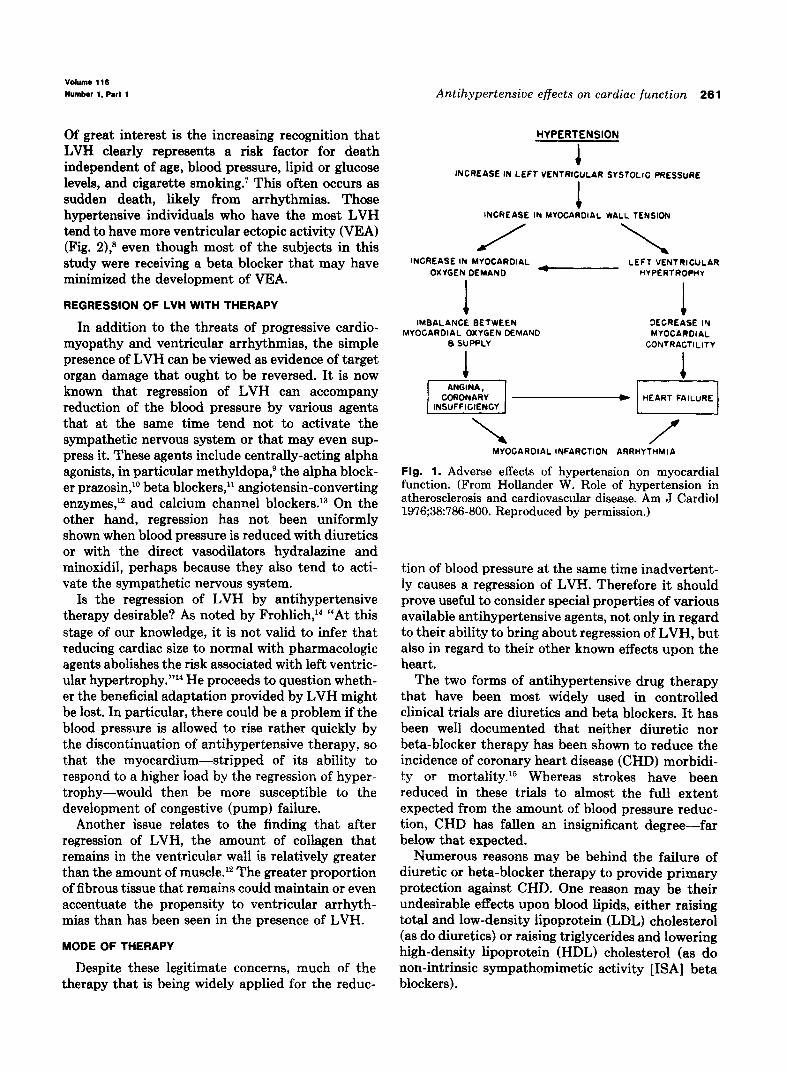
Notwithstanding the possible direct and primary role of an increased cardiac output in the causation of hypertension, the effects of increased blood pres- sure on the heart are more certain, largely because they are easier to study and to observe. Hollander’ outlined the adverse effects of hypertension on myocardial function sometime before it was com- mon practice to document left ventricular hypertro- phy (LVH) and to study the effects of antihyperten- sive therapy on LVH (Fig. 1).
THE RECOGNITION OF LVH
Much of the current interest in LVH reflects the greater ease of its recognition. Whereas fewer than 10% of hypertensive patients could be shown to have LVH by electrocardiography, more than 50% have increased ventricular wall dimensions when assessed by echocardiography. LVH determined by echocardiography may be seen even among adoles- cents with mild hypertension.3
LVH develops in response to long-term, persis-
From the Department of Internal Medicine, University of Texas South- western Medical School
Reprint requests: Norman M. Kaplan, MD, University of Texas South- western Medical School, Harry Hines Blvd., Dallas, TX 75235-9030.
tent elevations of systemic pressure. Therefore it comes as no surprise that the presence of LVH on echocardiography correlates more closely to 24-hour ambulatory blood pressure measurements-more to those taken during work than to those measured in physicians’ offices.4 Systolic pressure is most closely correlated to relative wall thickness, which is the best predictor of the degree of concentric LVH.S Left ventricular chamber size and wall thickness are independently related to body weight, intravascular volume, and age.
THE EFFECTS OF HYPERTENSION ON THE HEART
The positive inotropic response to the elevated systemic pressure that results in LVH can be looked upon as both beneficial (in fact, necessary) and detrimental. It is beneficial in that it allows the heart to adapt to the increased load placed upon the myocardium. As a result, the left ventricle increases its mass and wall thickness in direct proportion to the increase in pressure and vascular resistance.2 The heart can thereby handle the pressure load without the development of congestive failure that results when the load exceeds the heart’s capacity to pump.
DETRIMENTAL EFFECTS OF LVH
At the same time, LVH may be detrimental. In some patients, what probably starts out as a useful adaptation can progress to a cardiomyopathy with ii&& ;iiyuctidiJ co&r-aciiliiy and impaired coro- nary reserve.6 As shown by Hollander in Fig. 1, the increase in myocardial oxygen demand may tip the balance between supply and demand so that angina, coronary insufficiency, or infarction may supervene.
260
volume 116 Numbar 1. Part 1 Antihypertensive effects on cardiac function 261
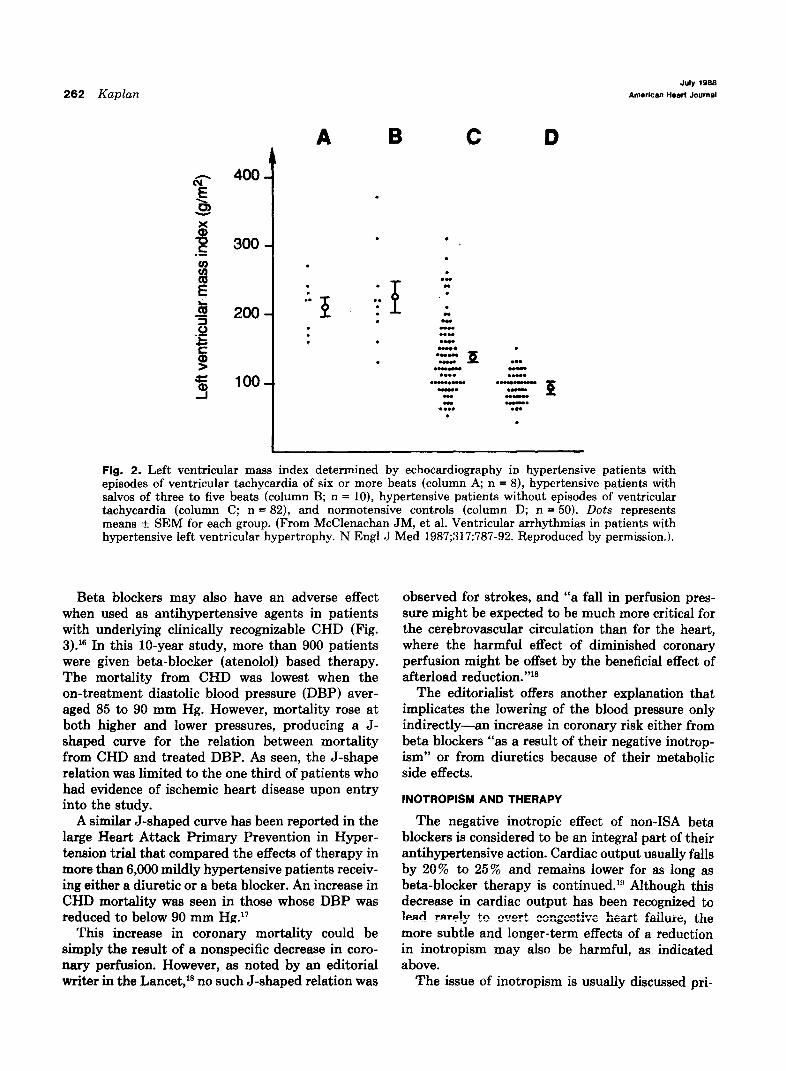
Of great interest is the increasing recognition that LVH clearly represents a risk factor for death independent of age, blood pressure, lipid or glucose levels, and cigarette smoking.’ This often occurs as sudden death, likely from arrhythmias. Those hypertensive individuals who have the most LVH tend to have more ventricular ectopic activity (VEA) (Fig. 2),8 even though most of the subjects in this
HYPERTENSION
1 INCREASE IN LEFT VENTRICULAR SYSTOLIC PRESSURE
L INCREASE IN MYOCPAOIAL WALL TENSION
study were receiving a beta blocker that may have INCREASE IN MYOCAROIAL LEFT VENTRICULAR
minimized the development of VEA. OXYGEN DEMAND HYPLRTROPHY
I I
REGRESSION OF LVH WITH THERAPY
In addition to the threats of progressive cardio- myopathy and ventricular arrhythmias, the simple presence of LVH can be viewed as evidence of target organ damage that ought to be reversed. It is now known that regression of LVH can accompany reduction of the blood pressure by various agents that at the same time tend not to activate the sympathetic nervous system or that may even sup- press it. These agents include centrally-acting alpha agonists, in particular methyldopa,s the alpha block- er prazosin,‘O beta blockers,” angiotensin-converting enzymes, l2 and calcium channel blockers.13 On the other hand, regression has not been uniformly shown when blood pressure is reduced with diuretics or with the direct vasodilators hydralazine and minoxidil, perhaps because they also tend to acti- vate the sympathetic nervous system.
IMBALANCE BETWEEN 4
DECREASE lh( MYOGAROIAL OXYGEN DEMAND
A
MYOCAROIAL a SUPPLY CONTRACTILITY
MYOCAROIAL INFARCTION ARRHYTHMIA
Fig. 1. Adverse effects of hypertension on myocardial function. (From Hollander W. Role of hypertension in atherosclerosis and cardiovascular disease. Am J Cardiol 1976;38:786-800. Reproduced by permission.)
tion of blood pressure at the same time inadvertent- ly causes a regression of LVH. Therefore it should prove useful to consider special properties of various available antihypertensive agents, not only in regard to their ability to bring about regression of LVH, but also in regard to their other known effects upon the heart.
Is the regression of LVH by antihypertensive therapy desirable? As noted by Frohlich,14 “At this stage of our knowledge, it is not valid to infer that reducing cardiac size to normal with pharmacologic agents abolishes the risk associated with left ventric- ular hypertrophy.“14 He proceeds to question wheth- er the beneficial adaptation provided by LVH might be lost. In particular, there could be a problem if the blood pressure is allowed to rise rather quickly by the discontinuation of antihypertensive therapy, so that the myocardium-stripped of its ability to respond to a higher load by the regression of hyper- trophy-would then be more susceptible to the development of congestive (pump) failure.
Another issue relates to the finding that after regression of LVH, the amount of collagen that remains in the ventricular wall is relatively greater than the amount of muscle.12 The greater proportion of fibrous tissue that remains could maintain or even accentuate the propensity to ventricular arrhyth- mias than has been seen in the presence of LVH.
MODE OF THERAPY
Despite these legitimate concerns, much of the therapy that is being widely applied for the reduc-
The two forms of antihypertensive drug therapy that have been most widely used in controlled clinical trials are diuretics and beta blockers. It has been well documented that neither diuretic nor beta-blocker therapy has been shown to reduce the incidence of coronary heart disease (CHD) morbidi- ty or mortality. l5 Whereas strokes have been reduced in these trials to almost the full extent expected from the amount of blood pressure reduc- tion, CHD has fallen an insignificant degree-far below that expected.
Numerous reasons may be behind the failure of diuretic or beta-blocker therapy to provide primary protection against CHD. One reason may be their undesirable effects upon blood lipids, either raising total and low-density lipoprotein (LDL) cholesterol (as do diuretics) or raising triglycerides and lowering high-density lipoprotein (HDL) cholesterol (as do non-intrinsic sympathomimetic activity [ISA] beta blockers).
262 Kaplan Jtiy 1988
American HearI Journal
I 400-
300-
200-
loo-
A B C D
.
. .
. . . .” . . ” . . . .
P . . . P . . . .”
:
. . . .
. . ”
. . . “ .
.-. .“..a . .“.a p. J.
.- “- . . . . ..W.
.-....- ..-n- -. .-
- z P
..Z . . . . .
Fig. 2. Left ventricular mass index determined by echocardiography in hypertensive patients with episodes of ventricular tachycardia of six or more beats (column A; n = 8), hypertensive patients with salvos of three to five beats (column B; n = lo), hypertensive patients without episodes of ventricular tachycardia (column C; n = 82), and normotensive controls (column D; n = 50). Dots represents means ~fr. SEM for each group. (From McClenachan JM, et al. Ventricular arrhythmias in patients with hypertensive left ventricular hypertrophy. N Engl J Med 1987;317:787-92. Reproduced by permission.).
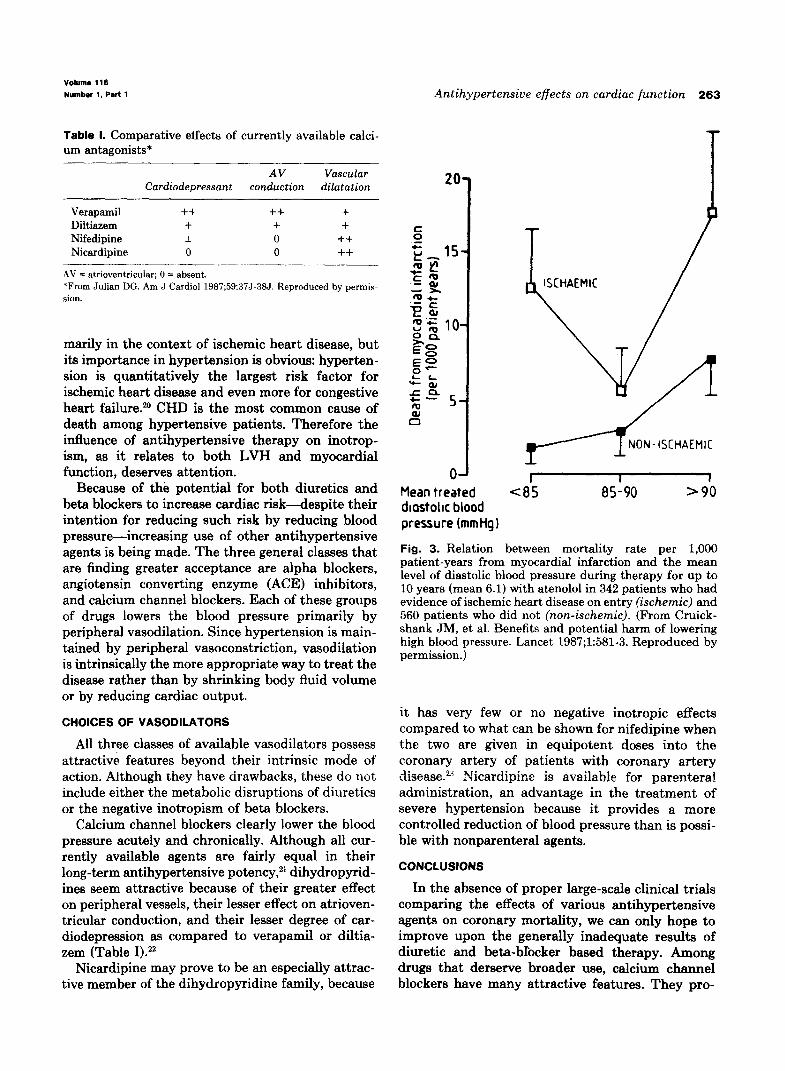
Beta blockers may also have an adverse effect when used as antihypertensive agents in patients with underlying clinically recognizable CHD (Fig. 3).16 In this lo-year study, more than 900 patients were given beta-blocker (atenolol) based therapy. The mortality from CHD was lowest when the on-treatment diastolic blood pressure (DBP) aver- aged 85 to 90 mm Hg. However, mortality rose at both higher and lower pressures, producing a J- shaped curve for the relation between mortality from CHD and treated DBP. As seen, the J-shape relation was limited to the one third of patients who had evidence of ischemic heart disease upon entry into the study.
A similar J-shaped curve has been reported in the large Heart Attack Primary Prevention in Hyper- tension trial that compared the effects of therapy in more than 6,000 mildly hypertensive patients receiv- ing either a diuretic or a beta blocker. An increase in CHD mortality was seen in those whose DBP was reduced to below 90 mm Hg.17
This increase in coronary mortality could be simply the result of a nonspecific decrease in coro- nary perfusion. However, as noted by an editorial writer in the Lancet,18 no such J-shaped relation was
observed for strokes, and “a fall in perfusion pres- sure might be expected to be much more critical for the cerebrovascular circulation than for the heart, where the harmful effect of diminished coronary perfusion might be offset by the beneficial effect of afterload reduction.“18
The editorialist offers another explanation that implicates the lowering of the blood pressure only indirectly-an increase in coronary risk either from beta blockers “as a result of their negative inotrop- ism” or from diuretics because of their metabolic side effects.
INOTROPlSM AND THERAPY
The negative inotropic effect of non-ISA beta blockers is considered to be an integral part of their antihypertensive action. Cardiac output usually falls by 20% to 25% and remains lower for as long as beta-blocker therapy is continued.lg Although this decrease in cardiac output has been recognized to lentj rmm!y tc n-r& n--~--+k- rULabwOwLvG heart faihure, the more subtle and longer-term effects of a reduction in inotropism may also be harmful, as indicated above.
The issue of inotropism is usually discussed pri-
Volume 116
Number 1, Part 1 Antihypertensive effects on cardiac function 263
Table 1. Comparative effects of currently available calci- um antagonists*
AV Vascular Cardiodepressant conduction dilatation
Verapamil ++ ++ + Diltiezem + + + Nifedipine * 0 ++ Nicardipine 0 0 ++
-“.__.-_l__--.~.. .___ AV = atrioventricular; 0 = absent. *From Julian DG. Am J Cardiol 1987;59:37J-387. Reproduced by permis- sion.
marily in the context of ischemic heart disease, but its importance in hypertension is obvious: hyperten- sion is quantitatively the largest risk factor for ischemic heart disease and even more for congestive heart failure.20 CHD is the most common cause of death among hypertensive patients. Therefore the influence of antihypertensive therapy on inotrop- ism, as it relates to both LVH and myocardial function, deserves attention.
Because of the potential for both diuretics and beta blockers to increase cardiac risk-despite their intention for reducing such risk by reducing blood pressure -increasing use of other antihypertensive agents is being made. The three general classes that are finding greater acceptance are alpha blockers, angiotensin converting enzyme (ACE) inhibitors, and calcium channel blockers. Each of these groups of drugs lowers the blood pressure primarily by peripheral vasodilation. Since hypertension is main- tained by peripheral vasoconstriction, vasodilation is intrinsically the more appropriate way to treat the disease rather than by shrinking body fluid volume or by reducing cardiac output.
CHOICES OF VASODILATORS
All three classes of available vasodilators possess attractive features beyond their intrinsic mode of action. Although they have drawbacks, these do not include either the metabolic disruptions of diuretics or the negative inotropism of beta blockers.
Calcium channel blockers clearly lower the blood pressure acutely and chronically. Although all cur- rently available agents are fairly equal in their long-term antihypertensive potency,2l dihydropyrid- ines seem attractive because of their greater effect on peripheral vessels, their lesser effect on atrioven- tricular conduction, and their lesser degree of car- diodepression as compared to verapamil or diltia- zem (Table I).22
Nicardipine may prove to be an especially attrac- tive member of the dihydropyridine family, because
OJ I I 1 Mean treated (85 85-90 >90 diastohc blood pressure (mmtig 1
Fig. 3. Relation between mortality rate per 1,000 patient-years from myocardial infarction and the mean level of diastolic blood pressure during therapy for up to 10 years (mean 6.1) with atenolol in 342 patients who had evidence of ischemic heart disease on entry (ischemic) and 560 patients who did not (non-ischemic). (From Cruick- shank JM, et al. Benefits and potential harm of lowering high blood pressure. Lancet 1987;1:581-3. Reproduced by permission.)
it has very few or no negative inotropic effects compared to what can be shown for nifedipine when the two are given in equipotent doses into the coronary artery of patients with coronary artery disease.23 Nicardipine is available for parenteral administration, an advantage in the treatment of severe hypertension because it provides a more controlled reduction of blood pressure than is possi- ble with nonparenteral agents.
CONCLUSIONS
In the absence of proper large-scale clinical trials comparing the effects of various antihypertensive agents on coronary mortality, we can only hope to improve upon the generally inadequate results of diuretic and beta-blocker based therapy. Among drugs that derserve broader use, calcium channel blockers have many attractive features. They pro-

264 Kaplan July 1988
American Haart Journal
vide both coronary and peripheral vasodilation, without the negative side effects of many other agents. Dihydropyridines may be the most effective of the calcium channel blockers as antihypertensive agents, and of those currently being studied, nicar- dipine offers the added benefit of having the least negative inotropic effect.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
Hollander W. Role of hypertension in atherosclerosis and cardiovascular disease. Am J Cardiol 1976;38:786-806. Dunn FG, Chandraratna P, decarvalho JGR, Basta LL, Frohlich ED. Pathophysiologic assessment of hypertensive heart disease with echocardiography. Am J Cardiol 1977; 39789-95. Baird WP, Fixler DE. Left ventricular hypertrophy in adoles- cents with elevated blood pressure: assessment by chest roentgenography, electrocardiography, and echocardiogra- phy. Pediatrics 1981;67:255-9. Devereaux RB, Pickering TG, Harshfield GA, et al. Left ventricular hypertrophy in patients with hypertension: importance of blood pressure response to regularly recurring stress. Circulation 1983;68:470-6. Messerli FH, Sundgaard-Riise K, Ventura HO, Dunn FG, Oigman W, Frohlich ED. Clinical and hemodynamic determi- nants of left ventricular dimensions. Arch Intern Med 1984;144:477-81. Tarazi RC, Fouad FM. Assessment of cardiac status in hypertensive patients. J Hypertens 1985;3(Suppl 2):S27- s31. Kannel WB, Abbott RD. A prognostic comparison of asymp- tomatic left ventricular hypertrophy and unrecognized myo- cardial infarction: the Framingham Study. AM HEART J 1986;111:391-7. McLenachan JM, Henderson E, Morris KI, Dargie HJ. Ventricular arrhythmias in patients with hypertensive left ventricular hypertrophy. N Engl J Med 1987;317:787-92. Weinstein M, Hilewitz H, Rogel S. The effect of single-dose
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
methyldopa and diuretic on BP and left ventricular mass. Arch Intern Med 1984;144:1629-32. Leenen FHH, Smith DL, Farkas RM, Reeves RA, Marquez- Julio A. Vasodilators and regression of left ventricular hvner- trophy: hydralezine versus prazosin in hypertensive humans. Am J Med 1987;82:969-78. Dunn FG, Ventura HO, Messerli FH, Kobrin I, Frohlich ED. Time course of regression of left ventricular hypertronhv in hypertensive patients treated with atenolol.- Circulation 1987:7&254-g. Nakashima Y, Fouad FM, Taraxi RC. Regression of left ventricular hypertrophy from systemic hypertension by enal- april. Am J Cardiol 1984:53:1044-9. S‘chmieder RE, Messerli FH, Garavaglia GE, Nunez BD. Cardiovascular effects of verapamil in patients with essential hypertension. Circulation 1987;75:1030-6. Frohlich ED. Cardiac hypertrophy in hypertension [Editori- al]. N Engl J Med 1987;317:831-3. MacMahon SW, Cutler JA, Furberg CD, Payne GH. The effects of drug treatment for hypertension on morbidity and mortality from cardiovascular disease: a review of randomiz- ed controlled trials. Prog Cardiovasc Dis 1986;29(Suppl1):99- 118. Cruickshank JM, Thorp JM, Zacharias FJ. Benefits and potential harm of lowering high blood pressure. Lancet 1987;1:581-3. Berglund C, Samuelsson 0. Lowered blood pressure and the J-shaped curve. Lancet 1987;1:1154-5. Anonymous. How far to lower blood pressure? [Editorial]. Lancet 1987;2:251-2. Lund-Johansen P. Hemodynamic consequences of long-term beat-blocker therapy: a 5-year follow-up study of atenolol. J Cardiovasc Pharmacol 1979;1:487-95. Kannel WB, Sytkowski PA. Atherosclerosis risk factors. Pharmacol Ther 1987;32:207-35. Kaplan NM. Treatment of hypertension: drug therapy In: Kaplan NM, ed. Clinical Hypertension. 4th ed. Baltimore: The Williams & Wilkins Co. 1986180-2’72. Julian DG. Concluding remarks. Am J Cardiol 1987;59:37J- 385. Visser CA, Koolen JJ, van Wezel H, Dunning AJ. Hemody- namics of nicardipine in coronary artery disease. Am J Cardiol 1987;59:9J-125.