ect response in delusional versus non-delusional depressed inpatients
TRANSCRIPT

Journal of Affective Disorders 74 (2003) 191–195www.elsevier.com/ locate/ jad
Brief report
ECT response in delusional versus non-delusional depressedinpatients
a , a b*¨Tom K. Birkenhager , Esther M. Pluijms , Stefan A.P. LuciusaDepartment of Biological Psychiatry, Parnassia Psychomedical Center, P.O. Box 53002, 2505AA The Hague, The Netherlands
bDepartment of Research, Parnassia Psychomedical Center, P.O. Box 53002, 2505AA The Hague, The Netherlands
Received 20 February 2001; accepted 30 November 2001
Abstract
Background: ECT is often considered more effective in delusional than in non-delusional depressives, although theliterature does not support this view.Methods: We reviewed the records of 55 consecutive inpatients with major depressionaccording to the DSM-III-R criteria and distinguished two subtypes: patients with delusions and those without. We examinedwhether the deluded patients showed a higher response rate.Results: using 50% reduction on the Hamilton Rating Scale forDepression (HRSD) as response criterion, the efficacy of ECT was higher in patients with delusional depression (92%response) than in the non-deluded patients (55% response). Considering a post-ECT HRSD score of# 7 as responsecriterion, patients with delusions again showed a higher response rate (57% versus 24%).Limitations: this study has aretrospective nature and a rather homogenous sample.Conclusion: ECT appears to be an effective treatment for severelydepressed inpatients, both with and without delusions. The efficacy of ECT was superior in patients with delusionaldepression, considering the number of patients achieving partial remission as well as full remission. 2002 Elsevier Science B.V. All rights reserved.
Keywords: Major depression; Delusional depression; Psychotic depression; Electroconvulsive therapy
1. Introduction considered an exceptional treatment, administered toseverely depressed patients only.
Electroconvulsive therapy (ECT) is considered to The presence of delusions has been considered abe the most effective treatment for major depression useful predictor of a favorable response to ECT, but(Abrams, 1997). In many countries, ECT is still the more recent literature is divided on this point.
Some studies report a superior response in delusionalthan in non-delusional depressives (Avery and Lub-rano, 1979; Buchan et al., 1992) and others fail to*Corresponding author. Tel.:131-70-391-6391; fax:131-70-find a difference (Rich et al., 1986; Solan et al.,391-6465.
¨E-mail address: [email protected] (T.K. Birkenhager). 1988; Kindler et al., 1991; O’Leary et al., 1995;
0165-0327/02/$ – see front matter 2002 Elsevier Science B.V. All rights reserved.doi:10.1016/S0165-0327(02)00005-8
¨192 T.K. Birkenhager et al. / Journal of Affective Disorders 74 (2003) 191–195
Sobin et al., 1996). Most studies show methodo- ECT, because of insufficient response after three tological flaws (see O’Leary et al., 1995), with the 11 treatments, and 17 patients received bilateral ECTstudies of Kindler et al. (1991) and Sobin et al. from the start, because of the severity of the illness(1996) being considered the most valuable. based on clinical observation (see Table 3). ECT was
The results of the above studies may not be administered with a brief-pulse, constant-currentapplicable to the population of depressed patients apparatus (Thymatron, Somatics, Lake Bluff, IL,receiving ECT in the Netherlands, where ECT is an USA) under thiopental anesthesia (1.0–2.5 mg/kg)exceptional treatment. The present study retrospec- and succinylcholine (1.0 mg/kg) for muscle relaxa-tively examines the relation between the presence or tion. Patients were oxygenated (100% oxygen, posi-absence of delusions and the efficacy of ECT in a tive pressure) until the resumption of spontaneouspopulation of severely depressed inpatients, most of respiration. Physiological monitoring included pulsethem being medication resistant. oximetry, electrocardiogram (ECG) and electroence-
phalogram (EEG). ECT was administered at aschedule of two treatments per week with moderate-
2. Methods to-high stimulus intensity (288–504 millicoulomb),without measuring seizure threshold by empirical
2.1. Patient selection stimulus titration. The number of ECT treatmentswas determined by clinical observation, and a mini-
We reviewed the records of 55 inpatients who met mum of 10 bilateral treatments was required beforethe DSM-III-R (American Psychiatric Association, evaluation as a non-responder. ECT was continued1987) criteria for major depression. Diagnoses were until patients were either asymptomatic or had notbased on clinical observation. A diagnosis of delu- shown further improvement over three consecutivesional depression was made only when the patient treatments. Patients were withdrawn from all psycho-had expressed, either spontaneously or on inquiry, tropic medication at least 1 week before ECT anddefinite mood-congruent delusions. When the case were maintained medication free during the course ofnotes of an individual patient left any room for doubt ECT in all but seven cases. Those patients received 5about the presence of delusions, the patient was mg droperidol prior to ECT for severe anxiety. Threeincluded in the non-psychotic group. of them also received haloperidol 1–3 mg daily to
All patients were treated consecutively with ECT control severe agitation.between December 1993 and December 2000 at theDepartment of Biological Psychiatry of ParnassiaPsychomedical Center, The Hague, The Netherlands.2.3. Evaluation of treatment outcomeThis department is almost exclusively reserved forpatients suffering from severe resistant depression. The presence of delusions and each patient’sPatients receiving ECT were either medication resis- strongest antidepressant medication trial prior totant or in a critical condition (mutistic, refusing ECT were evaluated independently and rated by afood). We restricted our sample to patients who were psychiatrist (T.K.B.) and a resident (E.M.P.) usingfree from neurologic or serious medical illness and the Antidepressant Treatment History Form (ATHF)who had never been treated with ECT previously. (Keller et al., 1986; Sackeim et al., 1990). Patients
If patients received more than one course of ECT scoring 3 or more on this 0–5 scale are classified asduring the study period, only the first course of ECT medication resistant. Scores on the 17-item Hamiltonwas reviewed. Rating Scale for Depression (HRSD) (Bech et al.,
1986) were routinely recorded in the patients’ case2.2. Electroconvulsive therapy notes prior to ECT, during ECT and following
treatment termination. These HRSD scores wereNineteen patients received right unilateral (d’ Elia) used in two different ways for classification of the
ECT only, another 19 patients initially received right response to ECT: a reduction in HRSD score of atunilateral ECT and were crossed over to bilateral least 50% post-treatment compared to pre-treatment
¨T.K. Birkenhager et al. / Journal of Affective Disorders 74 (2003) 191–195 193
and a post-treatment HRSD score of# 7 in patients Patients without delusions had a significantlyconsidered in full remission. longer mean duration of their current depressive
Chi-square tests were used to analyze the differ- episode than the deluded patients (29.4 versus 16.1ences in response rate between patients with delu- months;P 5 0.008), which may well have influencedsional depression and the non-deluded patients. the results to the disadvantage of the non-deludedStudent’s two-tailedt-tests were used to compare group. The mean number of ECT treatments forgroup means. Statistical analyses were performed patients achieving full remission for patients withusing SPSS for Windows (version 9.0). and without delusions was 10.4 (range 4–18) and
13.7 (range 7–25), respectively. The mean numberof ECTs for patients who failed to achieve full
3. Results remission was 16.7 (range 10–24) in the deludedsample and 16.9 (range 10–27) in patients without
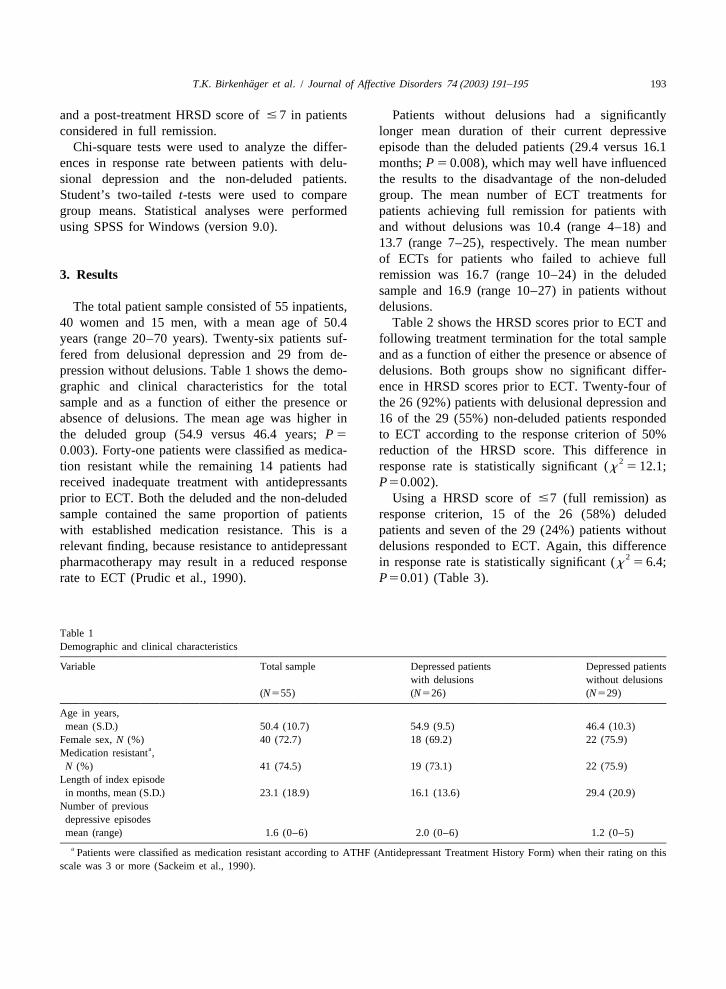
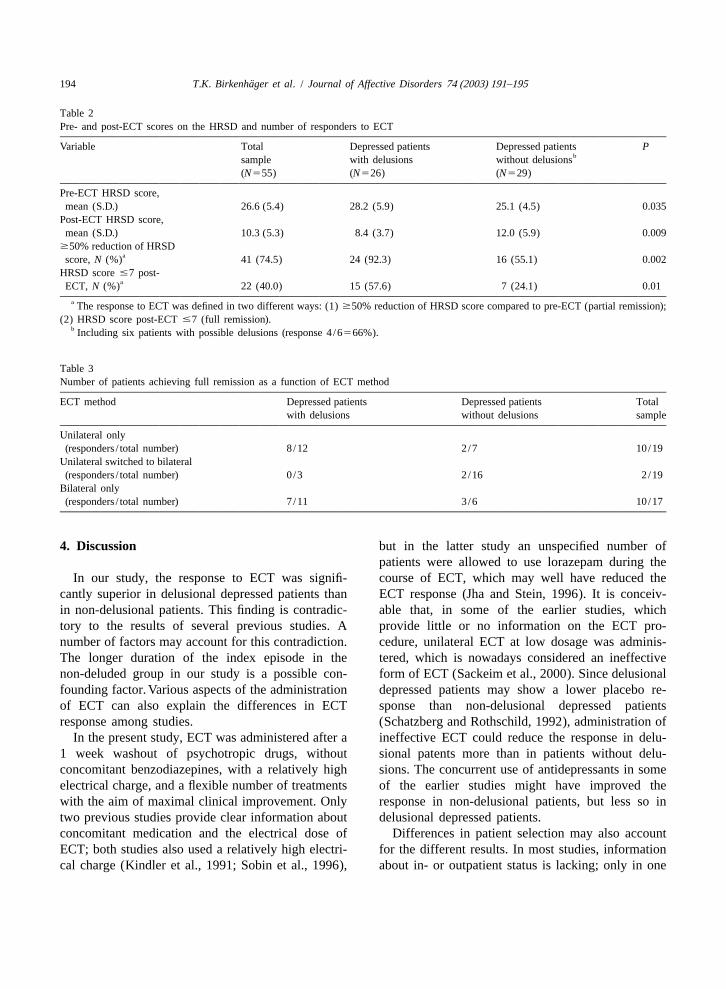
The total patient sample consisted of 55 inpatients, delusions.40 women and 15 men, with a mean age of 50.4 Table 2 shows the HRSD scores prior to ECT andyears (range 20–70 years). Twenty-six patients suf- following treatment termination for the total samplefered from delusional depression and 29 from de- and as a function of either the presence or absence ofpression without delusions. Table 1 shows the demo- delusions. Both groups show no significant differ-graphic and clinical characteristics for the total ence in HRSD scores prior to ECT. Twenty-four ofsample and as a function of either the presence or the 26 (92%) patients with delusional depression andabsence of delusions. The mean age was higher in 16 of the 29 (55%) non-deluded patients respondedthe deluded group (54.9 versus 46.4 years;P 5 to ECT according to the response criterion of 50%0.003). Forty-one patients were classified as medica- reduction of the HRSD score. This difference in
2tion resistant while the remaining 14 patients had response rate is statistically significant (x 5 12.1;received inadequate treatment with antidepressantsP50.002).prior to ECT. Both the deluded and the non-deluded Using a HRSD score of#7 (full remission) assample contained the same proportion of patients response criterion, 15 of the 26 (58%) deludedwith established medication resistance. This is a patients and seven of the 29 (24%) patients withoutrelevant finding, because resistance to antidepressant delusions responded to ECT. Again, this difference
2pharmacotherapy may result in a reduced response in response rate is statistically significant (x 5 6.4;rate to ECT (Prudic et al., 1990). P50.01) (Table 3).
Table 1Demographic and clinical characteristics
Variable Total sample Depressed patients Depressed patientswith delusions without delusions
(N555) (N526) (N529)
Age in years,mean (S.D.) 50.4 (10.7) 54.9 (9.5) 46.4 (10.3)
Female sex,N (%) 40 (72.7) 18 (69.2) 22 (75.9)aMedication resistant ,
N (%) 41 (74.5) 19 (73.1) 22 (75.9)Length of index episodein months, mean (S.D.) 23.1 (18.9) 16.1 (13.6) 29.4 (20.9)
Number of previousdepressive episodesmean (range) 1.6 (0–6) 2.0 (0–6) 1.2 (0–5)
a Patients were classified as medication resistant according to ATHF (Antidepressant Treatment History Form) when their rating on thisscale was 3 or more (Sackeim et al., 1990).
¨194 T.K. Birkenhager et al. / Journal of Affective Disorders 74 (2003) 191–195
Table 2Pre- and post-ECT scores on the HRSD and number of responders to ECT
Variable Total Depressed patients Depressed patients Pbsample with delusions without delusions
(N555) (N526) (N529)
Pre-ECT HRSD score,mean (S.D.) 26.6 (5.4) 28.2 (5.9) 25.1 (4.5) 0.035
Post-ECT HRSD score,mean (S.D.) 10.3 (5.3) 8.4 (3.7) 12.0 (5.9) 0.009$50% reduction of HRSD
ascore,N (%) 41 (74.5) 24 (92.3) 16 (55.1) 0.002HRSD score#7 post-
aECT, N (%) 22 (40.0) 15 (57.6) 7 (24.1) 0.01a The response to ECT was defined in two different ways: (1)$50% reduction of HRSD score compared to pre-ECT (partial remission);
(2) HRSD score post-ECT#7 (full remission).b Including six patients with possible delusions (response 4/6566%).
Table 3Number of patients achieving full remission as a function of ECT method
ECT method Depressed patients Depressed patients Totalwith delusions without delusions sample
Unilateral only(responders/ total number) 8/12 2/7 10/19
Unilateral switched to bilateral(responders/ total number) 0/3 2/16 2/19
Bilateral only(responders/ total number) 7/11 3/6 10/17
4. Discussion but in the latter study an unspecified number ofpatients were allowed to use lorazepam during the
In our study, the response to ECT was signifi- course of ECT, which may well have reduced thecantly superior in delusional depressed patients than ECT response (Jha and Stein, 1996). It is conceiv-in non-delusional patients. This finding is contradic- able that, in some of the earlier studies, whichtory to the results of several previous studies. A provide little or no information on the ECT pro-number of factors may account for this contradiction. cedure, unilateral ECT at low dosage was adminis-The longer duration of the index episode in the tered, which is nowadays considered an ineffectivenon-deluded group in our study is a possible con- form of ECT (Sackeim et al., 2000). Since delusionalfounding factor.Various aspects of the administration depressed patients may show a lower placebo re-of ECT can also explain the differences in ECT sponse than non-delusional depressed patientsresponse among studies. (Schatzberg and Rothschild, 1992), administration of
In the present study, ECT was administered after a ineffective ECT could reduce the response in delu-1 week washout of psychotropic drugs, without sional patents more than in patients without delu-concomitant benzodiazepines, with a relatively high sions. The concurrent use of antidepressants in someelectrical charge, and a flexible number of treatments of the earlier studies might have improved thewith the aim of maximal clinical improvement. Only response in non-delusional patients, but less so intwo previous studies provide clear information about delusional depressed patients.concomitant medication and the electrical dose of Differences in patient selection may also accountECT; both studies also used a relatively high electri- for the different results. In most studies, informationcal charge (Kindler et al., 1991; Sobin et al., 1996), about in- or outpatient status is lacking; only in one

¨T.K. Birkenhager et al. / Journal of Affective Disorders 74 (2003) 191–195 195
Keller, M.B., Lavori, P.W., Klerman, G.L., Andreasen, N.C.,previous paper is it clearly mentioned that the sampleEndicott, J., Coryell, W., Fawcett, J., Rice, J.P., Hirschfeld,consisted of inpatients (Kindler et al., 1991). In theR.M.A., 1986. Low levels and lack of predictors of
present study we included only delusional depressed somatotherapy and psychotherapy received by depressed pa-patients with mood-congruent delusions. Except for tients. Arch. Gen. Psychiatry 43, 458–466.one study (Sobin et al., 1996), the qualification of Kindler, S., Shapira, B., Hadjez, J., Abramowitz, M., Brom, D.,
Lerer, B., 1991. Factors influencing response to bilateralmood-congruence with regard to delusions is notelectroconvulsive therapy in major depression. Convulsivementioned.Ther. 7, 245–254.
In the present study, although ECT was shown to O’Leary, D., Gill, D., Gregory, S., Shawcross, C., 1995. Whichbe an effective treatment for depressed patients both depressed patients respond to ECT? The Nottingham results. J.with and without delusions, the response of patients Affect. Disord. 33, 245–250.
Prudic, J., Sackeim, H.A., Devanand, D.P., 1990. Medicationwith delusions was significantly superior.resistance and clinical response to electroconvulsive therapy.Psychiatry Res. 31, 287–296.
Rich, C.L., Spiker, D.G., Jewell, S.W., Neil, J.F., Phillipson, M.,References 1986. ECT response in psychotic versus nonpsychotic unipolar
depressives. J. Clin. Psychiatry 47, 123–125.Sackeim, H.A., Prudic, J., Devanand, D.P., Decina, P., Kerr, B.,Abrams, R., 1997. Prediction of response to electroconvulsive
Malitz, S., 1990. The impact of medication resistance andtherapy. In: Abrams, R. (Ed.), Electroconvulsive Therapy, 3rdcontinuation pharmacotherapy on relapse following response toEdition. Oxford University Press, New York, pp. 41–48.electroconvulsive therapy in major depression. J. Clin. Psycho-American Psychiatric Association, 1987. Diagnostic and Statisticalpharmacol. 10, 96–104.Manual of Mental Disorders, 3rd Edition revised. American
Sackeim, H.A., Prudic, J., Devanand, D.P., Nobler, M.S., Lisanby,Psychiatric Association, Washington, DC.S.H., Peyser, S., Fitzsimons, L., Moody, B.J., Clark, J., 2000.Avery, D., Lubrano, A., 1979. Depression treated with imipramineA prospective, randomized, double blind comparison of bilater-and ECT. The DeCarolis study reconsidered. Am. J. Psychiatryal and right unilateral electroconvulsive therapy at different136, 559–562.stimulus intensities. Arch. Gen. Psychiatry 57, 425–434.Bech, P., Kastrup, M., Rafaelsen, O.J., 1986. Mini-compendium of
Schatzberg, A.F., Rothschild, A.J., 1992. Psychotic (delusional)rating scales for states of anxiety, depression, mania andmajor depression: should it be included as a distinct syndromeschizophrenia with corresponding DSM-III syndromes. Actain DSM-IV? Am. J. Psychiatry 149, 733–745.Psychiatr. Scand. (Suppl.) 326, 23–28.
Sobin, C., Prudic, J., Devanand, D.P., Nobler, M.S., Sackeim,Buchan, H., Johnstone, E., McPherson, K., Palmer, R.L., Crow,H.A., 1996. Who responds to electroconvulsive therapy? AT.J., Brandon, S., 1992. Who benefits from electroconvulsivecomparison of effective and ineffective forms of treatment. Br.therapy? Combined results of the Leicester and Northwick ParkJ. Psychiatry 169, 322–328.trials. Br. J. Psychiatry 160, 355–359.
Solan, W.J., Khan, A., Avery, D.H., Cohen, S., 1988. PsychoticJha, A., Stein, G., 1996. Decreased efficacy of combined benzo-and nonpsychotic depression: comparison of response to ECT.diazepines and unilateral ECT in treatment of depression. ActaJ. Clin. Psychiatry 49, 97–99.Psychiatr. Scand. 94, 101–104.