economic costs of osteoporosis
TRANSCRIPT
O steoporosis—a bone disor-der associated with in-creased susceptibility to
fracture of the hip, spine, wrist,shoulder, and ribs—afflicts an esti-mated 25 million people in theUnited States. Osteoporosis accountsfor approximately 1.5 million newfractures each year, with associatedmedical charges (including rehabili-tation and extended treatment facili-ties) costing an estimated $10 billion,according to the National Osteo-porosis Foundation. Because osteo-porosis affects primarily the elderly,the National Osteoporosis Founda-tion estimates that these costs willincrease to $60 billion by the year2000 and to $200 billion by the year2040, as the number of Americansover the age of 65 years grows.
But medical charges are not theonly costs to consider. Lost produc-tivity (from missing work due todisability and premature death)from osteoporosis-related fracturespose additional costs. This article isbased on research funded by USDA’sEconomic Research Service (ERS) toestimate economic costs of osteo-porosis-related hip fractures. Eco-nomic costs include medical charges
and costs associated with lost pro-ductivity.
Hip fractures are the most seriousconsequence of osteoporosis. About20 percent result in death, and thosewho survive often have disabilityand loss of independence. Osteo-porosis-related hip fractures resultin estimated costs of $12.8 billion to$17.8 billion per year for medicalcare, extended treatment facilities,and the value of lost productivity.Rehabilitation and institutionaliza-tion costs, at about $5.1 billion to$7.1 billion, account for 40 percent ofthe estimated total economic cost ofosteoporosis-related hip fractures.The value of lost productivity due tomissed work is less than 1 percent oftotal economic costs, while value ofpremature death accounts for 35.3percent. Initial medical costs for hos-pitalization and outpatient care, atabout $3.1 billion to $4.3 billion, ac-count for 24.4 percent of the totaleconomic cost of osteoporosis-re-lated hip fractures.
Bone Is Constantly Being Renewed
Many people think of bone as ahard, permanent substance that doesnot change after childhood. How-ever, bone is alive and dynamic,constantly renewed through aprocess of removal or reabsorptionof old bone and formation or layingdown of new bone. Through this re-modeling process, about one-fifth of
the skeleton is replaced each year inadults.
Bone grows in length at first, thenduring adolescence there is a dra-matic increase in bone mass or den-sity. Peak bone mass is the maxi-mum skeletal mineral contentachieved by a person. During thefirst three decades of life more boneis formed than lost, and peak bonemass is achieved. After that time thebody removes old bone faster thannew bone forms, leading to a loss ofbone mass. If bone loss is excessive,bones become fragile and more sus-ceptible to fracture.
Half of All Women OverAge 50 Are Affected
Bone loss is a natural part of theaging process. Two factors makewomen more susceptible to osteo-porosis than men. First, women aresusceptible to greater bone lossesthan men. Starting around thefourth or fifth decade of life, bothmen and women lose bone mass at arate of 0.3 to 0.5 percent per year.After the onset of menopause, therate of bone loss in women can in-crease as much as 10-fold due to thereduced production of estrogen, afemale hormone that plays an im-portant role in maintaining bonemass. Women can lose up to 20 per-cent of their total bone mass in the
Moving Toward Healthier Diets
January-April 1996
31
Osteoporosis-Related HipFractures Cost $13 Billion
to $18 Billion YearlyEric Barefield
(404) 880-6289
The author is a research specialist at ClarkAtlanta University. This research was conductedunder a cooperative agreement with the Food andConsumer Economics Division, Economic ResearchService, USDA.

first 5 to 7 years following meno-pause. By age 70 or 80, women havetypically lost about 30 to 50 percentof their bone mass, compared with aloss of only 20 to 30 percent amongmen.
Second, women achieve peakbone mass earlier than men. Conse-quently, men have more years tobuild up bone mass and fewer yearsto lose bone mass. A related factor isthat men also tend to have largerbones than women.
The National Osteoporosis Foun-dation estimates that half of allwomen over the age of 50 are af-fected by osteoporosis, comparedwith one in every five men. By age75, 90 percent of women will experi-ence an osteoporosis-related frac-ture, as opposed to only 33 percentof men.
Higher Intake of CalciumMay Prevent/Delay HipFractures...
Genetics is a major determinant ofosteoporosis. Women account for 80percent of the 25 million Americansaffected by osteoporosis. Nationalincidence rates of hip fractures inthe United States are highest forWhite women, about 2 to 2.4 timesthe rates for White men and Blacks.Blacks have about 10 percent morebone mass than Whites.
There is interest in learning moreabout the factors within an individ-ual’s control, such as exercise anddiet, that might reduce the risk ofsuffering an osteoporosis-relatedfracture. Research suggests thatamong the dietary factors, calciummay play an important role in pre-venting or delaying the onset of os-teoporosis and that higher intakes ofcalcium could prevent 40 to 60 per-cent of osteoporosis-related hip frac-tures.
Calcium is the most abundantmineral in the body, accounting forabout 2 percent of total bodyweight. The bones and teeth containabout 99 percent of the calcium inthe human body, with the remaining1 percent circulating in the blood.Without calcium, the body cannotmaintain strong, healthy bones.
Calcium requirements are greatestduring the periods of rapid growthduring childhood and adolescence,during pregnancy and lactation, andin later adult years to compensatefor age-related bone loss. Increasedcalcium intake during the first threedecades of life may allow for attain-ment of genetic peak bone mass. In-creasing the level of bone mass fromwhich loss occurs reduces a person’srisk of hip fracture.
...But Women Often DoNot Consume EnoughCalcium
The Recommended Dietary Al-lowance (RDA) for calcium is 800milligrams per day for children age10 years and under and for mostadults age 25 years and over (not including pregnant and lactatingwomen) and is 1,200 milligrams perday for those ages 11-24 years. How-ever, experts at the National Insti-tute of Health’s 1994 Consensus De-velopment Conference on OptimalCalcium Intake recommended in-creasing these levels to between1,000 and 1,500 milligrams and be-tween 1,200 and 1,500 milligrams,respectively, per day.
Dairy products are good sourcesof calcium, with 1 cup of lowfatmilk and plain yogurt providing 37and 52 percent, respectively, of theRDA for most adults 25 years of ageand older. Leafy green vegetables,canned sardines and salmon, andfortified fruit juices are other easilyaccessible sources. Collard greensprovide 22 percent of the calciumRDA in each half-cup serving, while
a half cup of broccoli contains 6 per-cent of the RDA. Canned sardinesand salmon provide 41 and 23 per-cent, respectively, of the calciumRDA per 3-ounce serving.
Dairy products are the majorsource of calcium in the U.S. foodsupply, contributing 75 percent in1990. Fluid milk provided 37 percentof the calcium in 1990, while cheeseprovided 23 percent and other dairyproducts provided 15 percent. Meat,eggs, and legumes together pro-vided 9 percent of the calcium in1990, and vegetables provided 6 per-cent.
Most American men get the rec-ommended calcium intake, but mostwomen do not consume enough cal-cium. USDA consumption surveysindicate that men’s calcium intakefrom dietary sources increases withage, peaks during late adolescenceat 1,145 milligrams, and then de-clines. The pattern is similar forwomen, although the peak occurs atage 11 with 916 milligrams per day.Average calcium intake among boysages 12 to 19 is 95 percent of theRDA, but only 66 percent for girls inthe same age group—making it un-likely that many of them will fullyreach their genetic potential for peakbone mass. In fact, after age 11, mostAmerican girls never get their cal-cium consumption up to recom-mended levels.
Men 20 years and older consumean average of 101 percent of theRDA for calcium, while women ofthe same age consume an average ofonly 75 percent of the RDA for cal-cium. Calcium intake for womenages 20 and over is typically 632milligrams per day, 25 percent lowerthan among men 20 and over. Cal-cium intake for women generally in-creases during pregnancy and lacta-tion.
FoodReview
32
Moving Toward Healthier Diets
Hip Fractures Are theMost SeriousConsequence ofOsteoporosis
Although hip fractures are not asnumerous as fractures of the wristor spine, they are by far the most se-rious consequence of osteoporosis.Often times, spinal fractures will gountreated. However, osteoporosis-related hip fractures typically re-quire surgery, hospitalization, andan extended period of rehabilitation.Hip fractures also lead to prematuredeath, with an estimated 20 percentof people who fracture their hipdying within 1 year.
The Older Women’s League esti-mates that hip fractures account for18 percent of the annual 1.5 millionosteoporosis-related fractures, whilethe National Osteoporosis Founda-tion estimates that hip fractures ac-count for 25 percent. This range of270,000 to 375,000 osteoporosis-related hip fractures each year isused as the basis for the medical andlost productivity cost estimates inthis article.
The annual costs of osteoporosis-related hip fractures were estimatedby using the traditional cost-of-ill-ness method. This method catego-rizes disease cases by the level ofseverity, then calculates the costs ofmedical treatment and lost produc-tivity for each severity category, andsums up the categories for an esti-mate of the total economic cost.
Hospitalization andOutpatient Care Cost $3.1 Billion to $4.3 Billiona Year
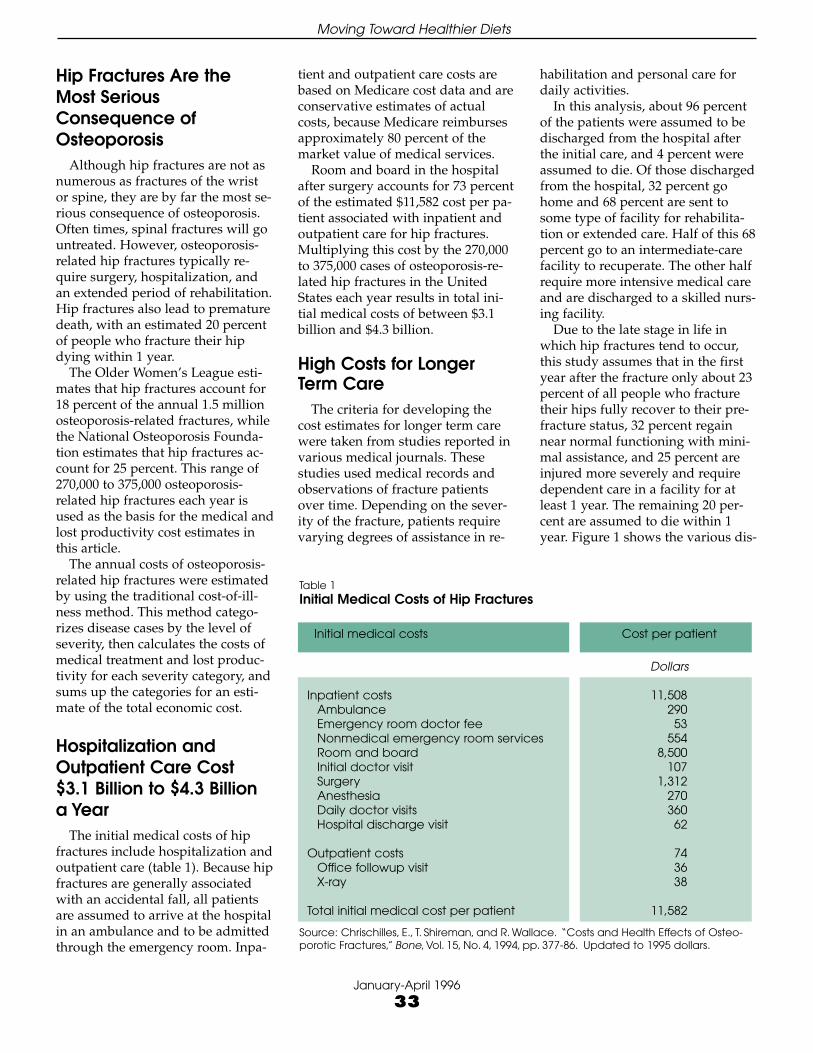
The initial medical costs of hipfractures include hospitalization andoutpatient care (table 1). Because hipfractures are generally associatedwith an accidental fall, all patientsare assumed to arrive at the hospitalin an ambulance and to be admittedthrough the emergency room. Inpa-
tient and outpatient care costs arebased on Medicare cost data and areconservative estimates of actualcosts, because Medicare reimbursesapproximately 80 percent of themarket value of medical services.
Room and board in the hospitalafter surgery accounts for 73 percentof the estimated $11,582 cost per pa-tient associated with inpatient andoutpatient care for hip fractures.Multiplying this cost by the 270,000to 375,000 cases of osteoporosis-re-lated hip fractures in the UnitedStates each year results in total ini-tial medical costs of between $3.1billion and $4.3 billion.
High Costs for LongerTerm Care
The criteria for developing thecost estimates for longer term carewere taken from studies reported invarious medical journals. Thesestudies used medical records andobservations of fracture patientsover time. Depending on the sever-ity of the fracture, patients requirevarying degrees of assistance in re-
habilitation and personal care fordaily activities.
In this analysis, about 96 percentof the patients were assumed to bedischarged from the hospital afterthe initial care, and 4 percent wereassumed to die. Of those dischargedfrom the hospital, 32 percent gohome and 68 percent are sent tosome type of facility for rehabilita-tion or extended care. Half of this 68percent go to an intermediate-carefacility to recuperate. The other halfrequire more intensive medical careand are discharged to a skilled nurs-ing facility.
Due to the late stage in life inwhich hip fractures tend to occur,this study assumes that in the firstyear after the fracture only about 23percent of all people who fracturetheir hips fully recover to their pre-fracture status, 32 percent regainnear normal functioning with mini-mal assistance, and 25 percent areinjured more severely and requiredependent care in a facility for atleast 1 year. The remaining 20 per-cent are assumed to die within 1year. Figure 1 shows the various dis-
Moving Toward Healthier Diets
January-April 1996
33
Table 1Initial Medical Costs of Hip Fractures
Initial medical costs Cost per patient
Dollars
Inpatient costs 11,508Ambulance 290Emergency room doctor fee 53Nonmedical emergency room services 554Room and board 8,500Initial doctor visit 107Surgery 1,312Anesthesia 270Daily doctor visits 360Hospital discharge visit 62
Outpatient costs 74Office followup visit 36X-ray 38
Total initial medical cost per patient 11,582
Source: Chrischilles, E., T. Shireman, and R. Wallace. “Costs and Health Effects of Osteo-porotic Fractures,” Bone, Vol. 15, No. 4, 1994, pp. 377-86. Updated to 1995 dollars.

charge destinations and health out-comes within 1 year of the fracture.
Table 2 shows the estimated perpatient cost associated with the vari-ous levels of rehabilitation and long-term care. The patients dischargedto their homes are assumed to re-quire a minimum amount of careafter being discharged from the hos-pital. This study conservatively as-sumes that these patients require aminimum of 6 weeks of rehabilita-tion, regardless of whether theyfully recover to their prefracture sta-tus or to a near normal level. Three-fourths of the patients discharged toan intermediate-care facility are as-sumed to recover to a near normallevel of functioning and returnhome after spending an average of90 days in the facility.
The remaining patients dis-charged to an intermediate-care fa-cility are assumed to remain se-
verely handicapped and to requirecare for at least 1 year. Among thepatients discharged to a skillednursing facility, 51 percent are as-sumed to require institutional carefor at least 1 year, 10 percent are as-sumed to die within 6 months, and39 percent are assumed to die within6 to 12 months. Total costs associ-ated with rehabilitation and institu-tional care are estimated at $5.1 bil-lion to $7.1 billion each year.
Lost ProductivityIncreases the AnnualCost of Hip Fractures
The estimate of lost productivitydue to osteoporosis-related hip frac-tures uses average weekly earningsto value lost wages for those whomiss work and, for those who diewithin a year, the Landefeld-Seskin
value of a statistical life. This valueprovides a conservative estimate ofthe value of a statistical life, becauseit does not account for the value oflost leisure time of patients or fortheir pain and suffering. This studyassumes that the average patientsuffers an osteoporosis-related hipfracture at age 75, about 20 percentof whom die within the year. Basedon $83,632 as the value of a statisti-cal life at age 76 and the two earlierestimates of annual cases, osteo-porosis-related hip fractures resultin losses from premature death of$4.5 billion to $6.3 billion.
The study assumes that individu-als in the laborforce miss work forthe duration of their rehabilitationfollowing osteoporosis-related hipfractures. The laborforce participa-tion rate is the percentage of thetotal population (or a subgroup ofthe population) that is in the labor-
FoodReview
34
Moving Toward Healthier Diets
Figure 1
Discharge destination Outcome after 1 year Final outcome
32% of total recover to near normal
25% of total remain severely handicapped
23% of totalfully recover
96% live and are discharged
32% go home
75% fully recover
49% die
74% recover to near normal
26% remain severely handicapped
51% remain severely handicapped
Patient status at end of hospital stay
20% of total die within 1 year
50% go to a skilled nursing facility
25% recover to near normal
50% go to an intermediate-care facility
4% die in hospital
Almost Half of Those Hospitalized With Osteoporosis-Related Hip Fractures Never Fully Recover
Total entering hospital with osteoporosis-related hip fractures
68% go to an extended-care facility

force. For the 80 percent of patientswho survive, osteoporosis-relatedhip fractures result in $75 million to$104 million in lost productivity dueto missed work (using a 4.6-percentlaborforce participation rate for peo-ple 75 years and older and an aver-age daily wage rate of $48.14 forthose working at the time of the hipfracture) (table 3).
This study estimates that the totaleconomic cost of osteoporosis-re-lated hip fractures is $12.8 billion to$17.8 billion each year. The costs ofhospitalization and outpatient careare $3.1 billion to $4.3 billion peryear. Further, because hip fracturestend to occur among the elderly, thevalue of lost productivity due tomissed work is a smaller componentof the total cost than is the value ofpremature death or the costs of re-habilitation and institutionalization.Rehabilitation and institutionaliza-tion costs of $5.1 billion to $7.1 bil-lion account for 40 percent of the es-
Moving Toward Healthier Diets
January-April 1996
35
Table 2Although the Majority of Patients Recover From Osteoporosis-Related Hip Fractures,Two-Thirds Require Institutional Care
Discharge Outcome Share of Days Daily Total costdestination after patients in care rate Low High
discharge facility1 range2 range3
Percent Number Dollars Million dollars
Home Fully recover 23.0 42 8 20.87 28.98Home Near normal 7.7 42 8 6.99 9.70Intermediate care facility Near normal 24.1 90 73 427.50 593.76Intermediate care facility Severely handicapped 8.5 360 73 603.12 837.68Skilled nursing facility Severely handicapped 16.6 360 135 2,178.25 3,025.35Skilled nursing facility Die within 3 months 1.3 90 135 42.64 59.23Skilled nursing facility Die within 3-6 months 2.0 180 135 131.22 182.25 Skilled nursing facility Die within 6-12 months 12.7 360 135 1,666.49 2,314.57
Total N/A 95.94 N/A N/A 5,077.08 7,051.52
Notes: Costs are in 1995 dollars. N/A = Not applicable. 1Assumes that patients discharged to the home still require an average of 6weeks of rehabilitation regardless of their final outcome. Patients discharged to an intermediate care facility and who recover stay anaverage of 3 months in the facility; others stay 1 year. Patients discharged to a skilled nursing facility stay at least 1 year, unless they die.2Based on the Older Women’s League estimate that 18 percent of the 1.5 million fractures each year are osteoporosis-related hip frac-tures (270,000 hip fractures per year). 3Based on the National Osteoporosis Foundation estimate that 25 percent of the 1.5 million frac-tures each year are osteoporosis-related hip fractures (375,000 hip fractures per year). 4The remaining 4 percent of patients die in thehospital before being discharged.
Table 3Largest Cost of Osteoporosis-Related Hip Fractures Due to Rehabilita-tion and Extended Care
Item CostLow range1 High range2
Million dollars
Initial medical costs 3,127.14 4,343.25Rehabilitation and institutional costs 5,077.08 7,051.52Value of missed work 74.72 103.79Value of premature death 4,516.13 6,272.4
Total cost 12,795.07 17,770.96Costs attributed to diet3 5,118.03 10,662.58
Notes: Costs are in 1995 dollars. 1The low range is based on the Older Women’sLeague estimate that 18 percent of the 1.5 million fractures each year are osteoporo-sis-related hip fractures (270,000 hip fractures per year). 2The high range is based onthe National Osteoporosis Foundation estimate that 25 percent of the 1.5 million frac-tures each year are osteoporosis-related hip fractures (375,000 hip fractures per year).3Studies suggest that 40 to 60 percent of osteoporosis-related hip fractures could beprevented by increasing calcium intake.

timated total economic cost of osteo-porosis-related hip fractures.
Since there is no known cure forosteoporosis, preventive measuresare important. Increasing evidenceindicates that inadequate calcium in-take is at least partly responsible forthe risk of osteoporosis-related hipfractures. Medical research suggeststhat increased consumption of cal-cium could prevent 40 to 60 percentof osteoporosis-related hip fractures.This study estimates that these diet-related fractures result in costs of$5.1 billion to $10.7 billion per yearfor medical care, extended-treatmentfacilities, and the value of lost pro-ductivity. Since bone loss begins inthe mid-thirties, it is best not to wait
until the process begins to start pre-ventive action. Consuming adequatedietary calcium should be a lifelongprocess, especially for women be-cause of their increased risk.
ReferencesBowen, Otis. “Osteoporosis: Pre-
vention and the Quality of Life forOlder Americans,” Public Health Re-ports, U.S. Department of Healthand Human Services, Sept.-Oct. 1989(suppl.) pp. 11-13.
Chapuy, Marie, Monique Arlot,and Francois Duboeuf. “Vitamin D3and Calcium to Prevent Hip Frac-tures in Elderly Women,” The NewEngland Journal of Medicine, Vol. 327,No. 23, Dec. 3, 1992, pp. 1637-42.
Chrischilles, E., T. Shireman, andR. Wallace. “Costs and Health Ef-fects of Osteoporotic Fractures,”Bone, Vol. 15, No. 4, 1994, pp. 377-86.
Holbrook, Troy, Elizabeth Barrett-Connor, and Deborah Wingard. “Di-etary Calcium Intake and Risk ofHip Fracture: 14 Year ProspectivePopulation Study,” The Lancet, Nov.5, 1988, pp. 1046-48.
Landefeld, Steven J., and EugeneSeskin. “The Economic Value of Life:Linking Theory to Practice,” Ameri-can Journal of Public Health, Vol. 72,No. 6, pp. 555-66.
McBean, Lois D., Tab Forgac, andSusan Calvert Finn. “Osteoporosis:Visions for Care and Prevention—AConference Report,” Journal of theAmerican Dietetic Association, Vol. 94,No. 6, June 1994, pp. 668-71. ■
FoodReview
36
Moving Toward Healthier Diets