economic consequences of diagnostic imaging for vocal...
TRANSCRIPT
Economic Consequences of Diagnostic Imaging for Vocal Cord Paralysis 1
Amon Y. Liu, MD, David M. Yousern, MD, Ara A. Chalian, MD, Curtis P. Langlotz, MD, PhD
Rationale and Objectives. The purpose of this retrospective study was to estimate the economic consequences of evaluat- ing suspected vocal cord paralysis with magnetic resonance (MR) imaging and computed tomography (CT).
Materials and Methods. Reports from MR imaging (n = 30) or CT (n = 19) studies of the neck in 49 patients were retrospectively reviewed for causes of vocal cord paralysis. The patients were divided into high-suspicion (n = 20) and low-suspicion (n = 29) groups, based on the presence or absence of a clinically detectable abnormality other than vocal cord immobility. Clinic and inpatient charts were examined to determine the work-up in all cases. The Medicare Re- source-based Relative Value Scale was u~ed to estimate the costs of most procedures.
Results. The high-clinical-suspicion group included nine true-positive, four false-positive, seven true-negative, and no false-negative cases. Further work-up was performed in seven true-positive, three false-positive, and one true-negative cases. The total cost of immediate diagnostic work-up in these 20 patients, including MR imaging and/or CT, was $20,737 ($2,304 per true-positive case). The low-suspicion group included two true-positive, nine false-positive, 18 true- negative, and no f~/lse-negative cases. Further work-up was performed in both true-positive, four false-positive, and two true-negative cases. The total cost of immediate diagnostic work-up in these 29 patients was $21,698, (mean, $748; $10,849 per true-positive case).
Conclusion. The average cost of finding space-occupying lesions in patients with vocal cord paralysis is more than 4.5 times higher in patients without suspicious antecedent clinical findings than in those with such a history. The benefits of obtaining negative findings and of detecting a small number of space-occupying lesions should be weighed against the costs of such examinations and of additional work-up for false-positive findings.
Key Words. Cost-effectiveness; economics, medical; neck, CT; neck, MR; vocal cords, neoplasms.
Vocal cord paralysis has numerous causes, including
trauma, neoplasms, infection, inflammation, and congeni-
tal or idiopathic conditions. Paralysis can be acute or
chronic and can be caused by a recurrent laryngeal nerve,
superior laryngeal nerve, or total vagal nerve deficit. Both
Acad Radiol 2001; 8:137-148
1 From the Department of Radiology, Virginia Commonwealth University, Richmond (A.Y.L.); the Department of Radiology, Division of Neuroradiol- ogy, The Johns Hopkins Hospital, 600 N Wolfe St, Houck B-112, Baltimore, MD 21287 (D.M.Y.); and the Departments of Otorhinolaryngology, Head and Neck Surgery (A.A.C.) and Biostatistics and Epidemiology (C.P.L.), Uni- versity of Pennsylvania Medical Center, Philadelphia. Received July 10, 2000; revision requested September 12; revision received Septerpber 25; accepted September 26. Address correspondence to D.M.Y.
© AUR, 2001
central and peripheral lesions may result in vocal cord
paralysis. Radiologic imaging is used in the evaluation of
vocal cord paralysis, primarily to detect an underlying
malignancy that may have vocal cord paralysis as its only
manifestation.
Although surgical trauma has long been recognized as
the most common cause of unilateral (and bilateral) vocal
cord paralysis (1,2), authors of other studies have con-
cluded that malignant neoplasms are a more common
cause, accounting for up to 40% of cases of unilateral
vocal cord paralysis (3,4).
A variety of imaging procedures have been advocated
in the work-up of vocal cord paralysis, including neck
ultrasonography, chest computed tomography (CT),
137
esophagography, and chest radiography (5-7). The opti- mal role for CT or magnetic resonance (MR) imaging of the neck, frequently requested in the work-up, is uncer- tain. In this study, we sought to estimate the economic consequences of using neck MR imaging o1" CT in the
evaluation of patients suspected of having vocal cord pa- ralysis.
Between January 1992 and October 1997, 96 patients were referred to the ear, nose, and throat (ENT) clinic of the University of Pennsylvania for evaluation of suspected vocal cord paralysis. These patients underwent cross-sec- tional imaging of the neck (MR imaging or CT) at this institution. The decision to perform neck CT or MR im-
aging was made after vocal cord immobility or hypomo- bility was detected, along with hoarseness at clinical ex- amination. The primary purpose of cross-sectional imag-
• ing was to exclude an underlying mass causing vocal cord paralysis rather than simply to find radiologic evidence of
vocal cord paralysis. The presence of vocal cord paralysis was confirmed by means of outpatient nasopharyngolaryn- goscopy (NPL).
Clinical records could be obtained for 49 of the 96 patients. The medical records of the remaining 47 patients could not be retrieved from the hospital film library, med- ical records, or ENT clinic. Many of these patients were referred by physicians outside the home institution. In
practice patterns analyzed by an otorhinolaryngologist (A.A.C.), however, there were no patient differences noted between outside and inside refen-als.
The 49 patients who form the basis of this study were examined with MR imaging (n = 30) or CT (n = 19) of the neck (from the skull base to the aortic arch) to deter- rnine the origin of the vocal cord paralysis. The cases of these patients were retrospectively divided into high-sus- picion (n = 20) and low-suspicion (n = 29) groups, based on the presence or absence of a clinically detected abnormality other than vocal cord immobility. These ab- normalities included a known history of head and neck cancer (including thyroid carcinoma) in 10 cases, other cancer in nine cases, and other space-occupying lesions (nodal enlargement) in one case.
All enhanced CT examinations were performed with either an HSA or a 9800 Quick scanner (GE Medical Systems, Milwaukee, Wis). The patient was placed in the supine position with the neck extended in a modified coronal head holder and was asked to breathe quietly and
resist swallowing during acquisitions. Axial images were
obtained with 3-5-mm-thick contiguous sections from the cavernous sinuses to the aortic arch. The field of view was 22 x 22 cm. The total scanning time was 1-1 V2 minutes (HSA scanner) or 5-10 minutes (9800 Quick
scanner), and the radiation dose was 280 mAs at 140 kV. Iothalamate meglumine (Conray; Mallinkrodt Medical, St Louis, Mo) was intravenously administered by an injector with an automated two-phase program: an initial 100-mL bolus injected at a rate of 2 rnL/sec fbllowed by 50 mL at
1 mL/sec, for a total dose of 150 mL. Scanning was initi- ated after a 50-second delay.
The MR images were obtained with a 1.5-T Signa im-
ager (GE Medical Systems) and included 5-toni-thick contiguous T I-weighted images (500-700/11-17 [repeti- tion time msec/echo time msec]; number of signals aver-
aged [NSA], 1-2), fat-suppressed fast-spin-echo T2- weighted images (3,000-5,000/80-102; NSA, 1-2), and fat-suppressed gadolinium-enhanced Tl-weighted images (either 600-750/11-30; NSA, 1; or spoiled gradient-echo sequences, 35/I.8-2.3: NSA, I, 30o-40 ° flip angle). Ga-
dopentetate dimeglumine (Magnevist: Berlex, Fairfield, NJ) was injected at standard doses and rates (0.1 mmol/kg over 20 seconds).
MR and CT imaging were performed from the skull base to the level of the aortic arch to cover the course of the vagus and recurrent laryngeal nerves bilaterally. When the upper mediastinum was not visualized on the initial images, the patient was asked to return for additional im- aging.
All of the MR and CT studies were interpreted by board-certified neuroradiologists, and the radiology re- ports were retrospectively reviewed in all cases for signs of vocal cord impairment, including adduction or medial
deviation of the vocal cord and aryepiglottic fold, rotation of the arytenoid cartilage, atrophy of the true vocal cord, or enlargement of the piriforna sinus, vallecula, or laryn- geal ventricle. Reports were further reviewed for the pres- ence of masses (medullary, skull base, carotid sheath, thyroid, esophageal, mediastinal, or laryngeal/tracheal) that may cause vocal cord paralysis. Clinic and inpatient charts were examined to deternfine the extent and nature of additional work-up after MR imaging o1" CT, as well as the clinical outcome (eg, results of direct laryngoscopy or biopsies).
The cases were classified into four categories for both the high- and low-suspicion groups: true-positive, false- positive, true-negative, and false-negative. The classifica- tion was based on the presence of radiologic abnornlali-
138
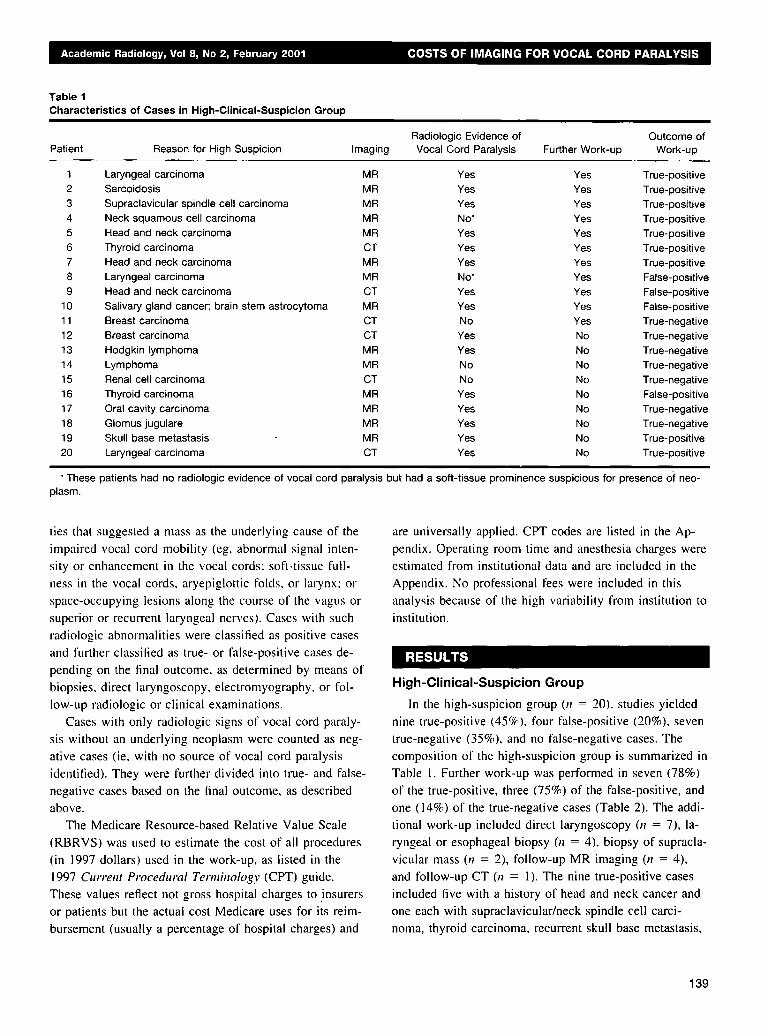
Table 1 Characteristics of Cases in High-Clinical-Suspicion Group
Radiologic Evidence of Outcome of Patient Reason for High Suspicion Imaging Vocal Cord Paralysis Further Work-up Work-up
1 Laryngeal carcinoma MR Yes Yes 2 Sarcoidosis MR Yes Yes 3 Supraclavicular spindle cell carcinoma MR Yes Yes 4 Neck squamous cell carcinoma MR No" Yes 5 Head and neck carcinoma MR Yes Yes 6 Thyroid carcinoma CT Yes Yes 7 Head and neck carcinoma MR Yes Yes 8 Laryngeal carcinoma MR No* Yes 9 Head and neck carcinoma CT Yes Yes
10 Salivary gland cancer; brain stem astrocytoma MR Yes Yes 11 Breast carcinoma CT No Yes 12 Breast carcinoma CT Yes No 13 Hodgkin lymphoma MR Yes No 14 Lymphoma MR No No 15 Renal cell carcinoma CT No No 16 Thyroid carcinoma MR Yes No 17 Oral cavity carcinoma MR Yes No 18 Glomus jugulare MR Yes No 19 Skull base metastasis MR Yes No 20 Laryngeal carcinoma CT Yes No
True- )ositive True- )ositive True- )ositive True- )ositive True- )ositive True- )ositive True- )ositive False- 3ositive False- 3ositive False- 3ositive True-negative True-negative True-negative True-negative True-negative False-positive True-negative True-negative True-positive True-positive
* These patients had no radiologic evidence of vocal cord paralysis but had a soft-tissue prominence suspicious for presence of neo- plasm.
ties that suggested a mass as the underlying cause of the
impaired vocal cord mobility (eg, abnormal signal inten-
sity or enhancement in the vocal cords: soft-tissue full-
ness in the vocal cords, aryepiglottic folds, or larynx: or
space-occupying lesions along the course of the vagus or
superior or recurrent laryngeal nerves). Cases with such
radiologic abnormalities were classified as positive cases
and further classified as true- or false-positive cases de-
pending on the final outcome, as determined by means of
biopsies, direct laryngoscopy, electromyography, or fol-
low-up radiologic or clinical examinations.
Cases with only radiologic signs of vocal cord paraly-
sis without an underlying neoplasm were counted as neg-
ative cases (ie, with no source of vocal cord paralysis
identified). They were further divided into true- and false-
negative cases based on the final outcome, as described
above.
The Medicare Resource-based Relative Value Scale (RBRVS) was used to estimate the cost of all procedures
(in 1997 dollars) used in the work-up, as listed in the
1997 Current Procedural Terminology (CPT) guide. These values reflect not gross hospital charges to insurers
or patients but the actual cost Medicare uses for its reim- bursement (usually a percentage of hospital charges) and
are universally applied. CPT codes are listed in the Ap-
pendix. Operating room time and anesthesia charges were
estimated from institutional data and are included in the
Appendix. No professional tees were included in this
analysis because of the high variability from institution to
institution.
RESULTS
High-Clinical-Suspicion Group
In the high-suspicion group (n = 20). studies yielded
nine true-posit ive (45%), four false-posit ive (20%), seven
true-negative (35%), and no false-negative cases. The
composi t ion of the high-suspicion group is summarized in
Table 1. Further work-up was performed in seven (78%)
of the true-positive, three (75%) of the false-positive, and
one (14%) of the true-negative cases (Table 2). The addi-
tional work-up included direct laryngoscopy 07 = 7), la-
ryngeal or esophageal biopsy (77 = 4), biopsy of supracla-
vicular mass 01 = 2), follow-up MR imaging (17 = 4),
and follow-up CT (n = 1). The nine true-positive cases
included five with a history of head and neck cancer and
one each with supraclavicular/neck spindle cell carci-
noma, thyroid carcinoma, recurrent skull base metastasis,
139
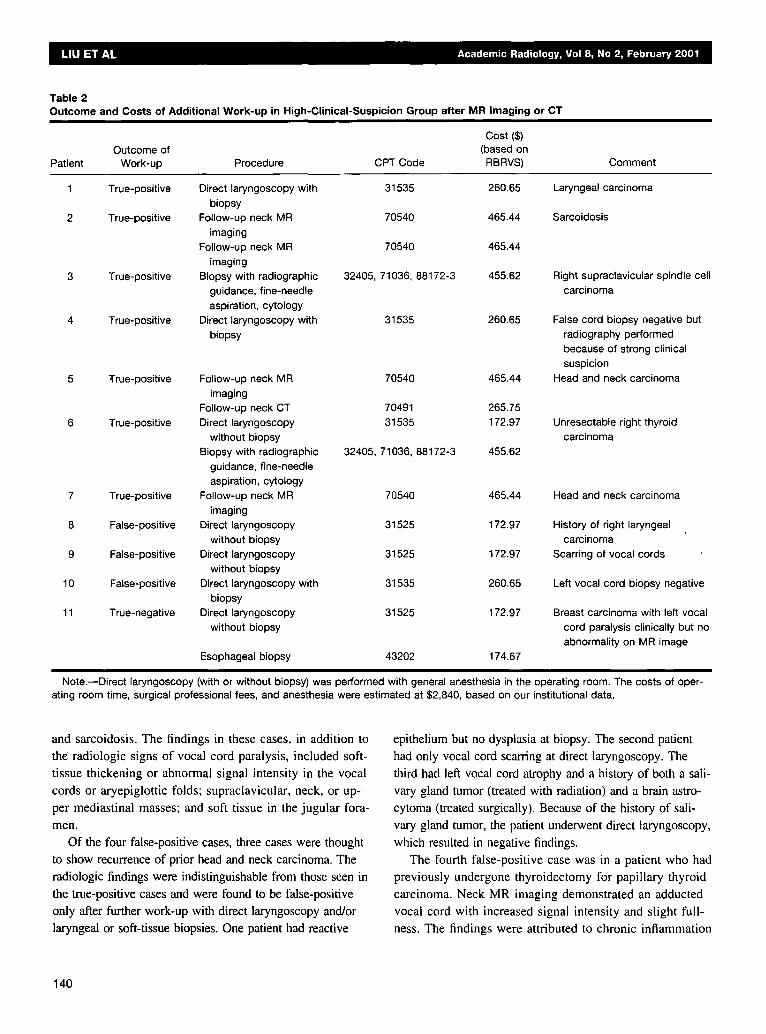
Table 2 Outcome and Costs of Additional Work-up in High-Clinical-Suspicion Group after MR Imaging or CT
Cost ($) Outcome of (based on
Patient Work-up Procedure CPT Code RBRVS) Comment
1 True-positive Direct laryngoscopy with 31535 260.65 biopsy
2 True-positive Follow-up neck MR 70540 465.44 imaging
Follow-up neck MR 70540 465.44 imaging
3 True-positive Biopsy with radiographic 32405, 71036, 88172-3 455.62 guidance, fine-needle aspiration, cytology
4 True-positive Direct laryngoscopy with 31535 260.65 biopsy
5 True-positive Follow-up neck MR 70540 465.44 imaging
Follow-up neck CT 70491 265.75 6 True-positive Direct laryngoscopy 31535 172.97
without biopsy Biopsy with radiographic 32405, 71036, 88172-3 455.62
guidance, fine-needle aspiration, cytology
7 True-positive Follow-up neck MR 70540 465.44 imaging
8 False-positive Direct laryngoscopy 31525 172.97 without biopsy
9 False-positive Direct laryngoscopy 31525 172.97 without biopsy
10 False-positive Direct laryngoscopy with 31535 260.65 biopsy
11 True-negative Direct laryngoscopy 31525 172.97 without biopsy
Esophageal biopsy 43202 174.67
Laryngeal carcinoma
Sarcoidosis
Right supraclavicular spindle cell carcinoma
False cord biopsy negative but radiography performed because of strong clinical suspicion
Head and neck carcinoma
Unresectable right thyroid carcinoma
Head and neck carcinoma
History of right laryngeal carcinoma
Scarring of vocal cords
Left vocal cord biopsy negative
Breast carcinoma with left vocal cord paralysis clinically but no abnormality on MR image
Note.--Direct laryngoscopy (with or without biopsy) was performed with general anesthesia in the operating room. The costs of oper- ating room time, surgical professional fees, and anesthesia were estimated at $2,840, based on our institutional data.
and sarcoidosis. The findings in these cases, in addition to the radiologic signs of vocal cord paralysis, included soft- tissue thickening or abnormal signal intensity in the vocal cords or aryepiglottic folds; supraclavicular, neck, or up- per mediastinal masses; and soft tissue in the jugular fora- men.
Of the four false-positive cases, three cases were thought to show recurrence of prior head and neck carcinoma. The radiologic findings were indistinguishable from those seen in
the true-positive cases and were found to be false-positive only after further work-up with direct laryngoscopy and/or laryngeal or soft-tissue biopsies. One patient had reactive
epithelium but no dysplasia at biopsy. The second patient had only vocal cord scarfing at direct laryngoscopy. The third had left vocal cord atrophy and a history of both a sali- vary gland tumor (treated with radiation) and a brain astro-
cytoma (treated surgically). Because of the history of sali- vary gland tumor, the patient underwent direct laryngoscopy, which resulted in negative findings.
The fourth false-positive case was in a patient who had previously undergone thyroidectomy for papillary thyroid
carcinoma. Neck MR imaging demonstrated an adducted vocal cord with increased signal intensity and slight full- ness. The findings were attributed to chronic inflammation
140

Table 3 Outcome and Costs of Additional Work-up Induced by False-Positive CT or MR Findings in High-Clinical-Suspicion Group
Patient CT/MR Finding Further Work-up Cost ($) Outcome of Work-up
Enhancing largyngeal soft-tissue fullness (mass vs radiation therapy change)
Asymmetric thickening of oropharynx, tonsils, valleculae
Direct laryngoscopy with biopsy 260.65
Operating room, anesthesia 2,840.00 Direct laryngoscopy 172.95
Operating room, anesthesia 2,840.00 10 Left vocal cord atrophy Direct laryngoscopy 172.95
Operating room, anesthesia 2,840.00 Total 9,126.55
False cord biopsy negative (reactive epithelium without dysplasia)
Scarring of vocal cords at direct laryngoscopy
Because of history of salivary gland tumor, direct laryngoscopy was performed (negative)
Note.--Direct laryngoscopy (with or without biopsy) was performed with general anesthesia in the operating room. The costs of oper- ating room time, surgical professional fees, and anesthesia were estimated at $2,840, based on our institutional data.
rather than neoplastic involvement, because they had been
stable for 14 months. MR imaging contributed additional information to the management of this case, however, by demonstrating an interval decrease in the size of multiple retropharyngeal and jugulodigastric lymph nodes after therapy for thyroid cancer. No further work-up was per- formed.
One true-negative case received further work-up. This
patient had a history of breast carcinoma with clinical symptoms of left vocal cord paralysis but no abnormali-
ties detected at MR imaging. Since there was still a strong clinical suspicion of occult malignancy (ie, meta- static nodal involvement) causing vocal cord paralysis, and because the patient also complained of dysphagia, direct laryngoscopy and an esophageal biopsy were per-
formed. Both of these tests had findings negative for ma- lignancy.
The total cost of immediate diagnostic work-up in these 20 patients, including the MR imaging or CT, was $20,737. The mean cost of work-up per patient was $1,037 ($20,737 for 20 high-suspicion cases). The cost per true-positive case was $2,304 ($20,737 for nine true-
positive cases). (The "immediate diagnostic work-up" costs included only the initial work-up and care of pa- tients suspected of having vocal cord paralysis. The costs of treatment and induced costs from false-positive work-
ups were not included in this initial analysis.) Further' work-up induced by false-positive CT or MR findings ("induced costs") included three direct laryngoscopies, one with a laryngeal biopsy and two without, at a total cost of $9,127 (Table 3). The induced cost per false-posi-
tive case was $2,282 ($9,127 divided by four false-posi- tive cases) or $3,042 ($9,127 divided by three) for the three false-positive cases that received further work-up. The mean induced cost for all patients imaged was $456 ($9,127 divided by a total of 20 high-suspicion patients).
L o w - C l i n i c a l - S u s p i c i o n G r o u p
In the low-suspicion cases (n = 29), studies yielded
two true-positive (7%), nine false-positive (31%), 18 true- negative (62%), and no false-negative cases. The compo- sition of the low-suspicion group is summarized in Table 4. Further work-up was obtained in both true-positive cases (100%), and in four (44%) of the nine false-positive and two (1 1%) of the 18 true-negative cases (Table 5).
Further work-up included direct laryngoscopy 01 = 3), laryngeal electromyography (n = 3), video stroboscopy (n = 1), false vocal cord biopsy (n = 1), thyroid biopsy 07 = 1), follow-up CT 01 = 1), and chest CT (n = 1). There were two true-positive cases, in which underlying
malignancy was unexpectedly found to explain the pa- tient's vocal cord paralysis. In one patient, a mediastinal mass and adenopathy were found. The other patient was thought to have idiopathic left vocal cord paralysis be- cause of an outside report. Neck CT was performed after the initial clinic visit, which demonstrated dilatation of the left piriform sinus and a 1.5-cm left thyroid mass. CT-guided needle aspiration of the lesion was subse- quently performed, which revealed a papillary thyroid
carcinoma. Four of nine false-positive cases (44%) received fur-
ther work-up (Table 6). None had an antecedent clinical
141
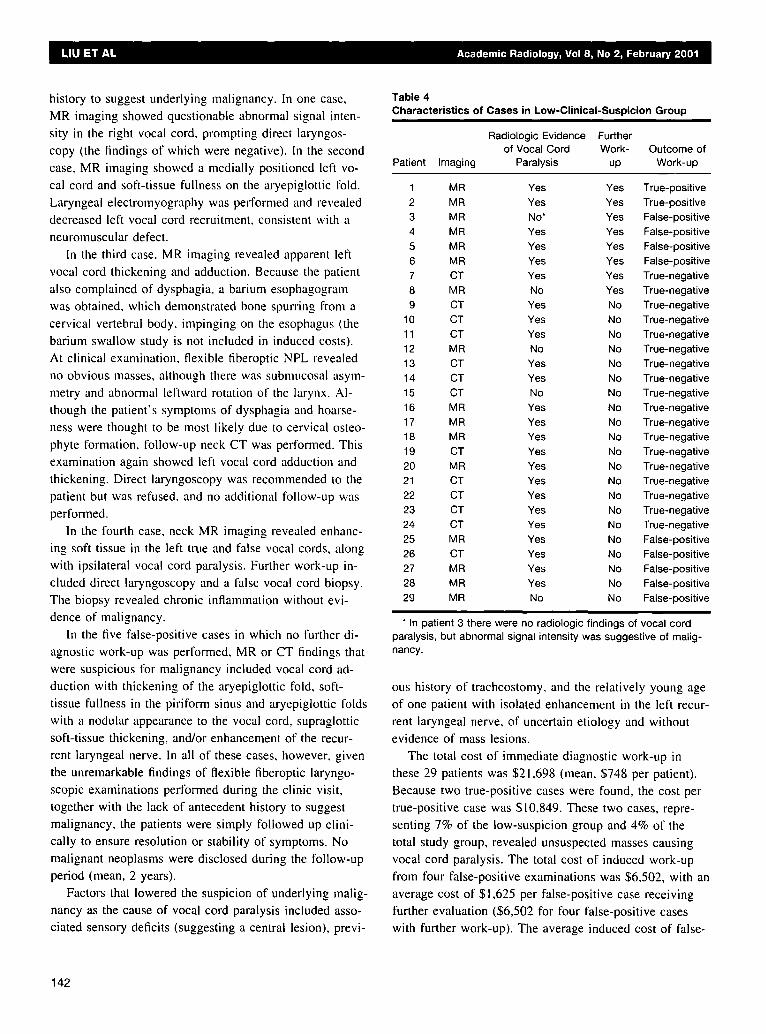
history to suggest underlying malignancy. In one case, MR imaging showed questionable abnormal signal inten- sity in the right vocal cord, prompting direct laryngos- copy (the findings of which were negative). In the second case, MR imaging showed a medially positioned left vo- cal cord and soft-tissue fullness on the aryepiglottic I'old.
Laryngeal electromyography was performed and revealed decreased left vocal cord recruitment, consistent with a neuromuscular defect.
In the third case, MR imaging revealed apparent let1
vocal cord thickening and adduction. Because the patient also complained of dysphagia, a barium esophagogram was obtained, which demonstrated bone spurting from a cervical vertebral body. impinging on the esophagus (the barium swallow study is not included in induced costs). At clinical examination, flexible fiberoptic NPL revealed
no obvious masses, although there was submucosal asym- metry and abnormal leftward rotation of the larynx. Al- though the patient's symptoms of dysphagia and hoarse- ness were thought to be most likely due to cervical osteo- phyte formation, follow-up neck CT was performed. This examination again showed left vocal cord adduction and thickening. Direct laryngoscopy was recommended to the
patient but was refused, and no additional follow-up was performed.
In the fourth case, neck MR imaging revealed enhanc- ing soft tissue in the left true and false vocal cords, along with ipsilateral vocal cord paralysis. Further work-up in- cluded direct laryngoscopy and a false vocal cord biopsy. ;l'he biopsy revealed chronic inflammation without evi- dence of malignancy.
In the five false-positive cases in which no further di- agnostic work-up was performed, MR or CT findings that were suspicious for malignancy included vocal cord ad-
duction with thickening of the aryepiglottic fold, soft- tissue fullness in the piriform sinus and aryepiglottic folds with a nodular appearance to the vocal cord, supraglottic soft-tissue thickening, and/or enhancement of the recur-
rent laryngeal nerve. In all of these cases, however, given the unremarkable findings of flexible fiberoptic laryngo-
scopic examinations performed during the clinic visit, together with the lack of antecedent history to suggest malignancy, the patients were simply followed up clini- cally to ensure resolution or stability of symptoms. No malignant neoplasms were disclosed during the follow-up period (mean, 2 years).
Factors that lowered the suspicion of underlying malig- nancy as the cause of vocal cord paralysis included asso- ciated sensory deficits (suggesting a central lesion), previ-
Table 4 Characteristics of Cases in Low-Clinical-Suspicion Group
Radiologic Evidence Further of Vocal Cord Work- Outcome of
Patient Imaging Paralysis up Work-up
1 MR Yes Yes True-positive 2 MR Yes Yes True-positive 3 MR No" Yes False-positive 4 MR Yes Yes False-positive 5 MR Yes Yes False-positive 6 MR Yes Yes False-positive 7 CT Yes Yes True-negative 8 MR No Yes True-negative 9 CT Yes No True-negative
10 CT Yes No True-negative 11 CT Yes No True-negative 12 M R No No True-negative 13 CT Yes No True-negative 14 CT Yes No True-negative 15 CT No No True-negative 16 M R Yes No True-negative 17 M R Yes No True-negative 18 MR Yes No True-negative 19 CT Yes No True-negative 20 MR Yes No True-negative 21 CT Yes No True-negative 22 CT Yes No True-negative 23 CT Yes No True-negative 24 CT Yes No True-negative 25 MR Yes No False-positive 26 CT Yes No False-positive 27 MR Yes No False-positive 28 MR Yes No False-positive 29 MR No No False-positive
° In patient 3 there were no radiologic findings of vocal cord paralysis, but abnormal signal intensity was suggestive of malig- nancy.
ous history of tracheostomy, and the relatively young age of one patient with isolated enhancement in the left recur- rent laryngeal nerve, of uncertain etiology and without evidence of mass lesions.
The total cost of immediate diagnostic work-up in these 29 patients was $21,698 (mean, $748 per patient). Because two true-positive cases were found, the cost per true-positive case was $10,849. These two cases, repre- senting 7% of the low-suspicion group and 4% of the total study group, revealed unsuspected masses causing vocal cord paralysis. The total cost of induced work-up from four false-positive examinations was $6,502, with an average cost of $1,625 per false-positive case receiving further evaluation ($6,502 for four false-positive cases with further work-up). The average induced cost of false-
142
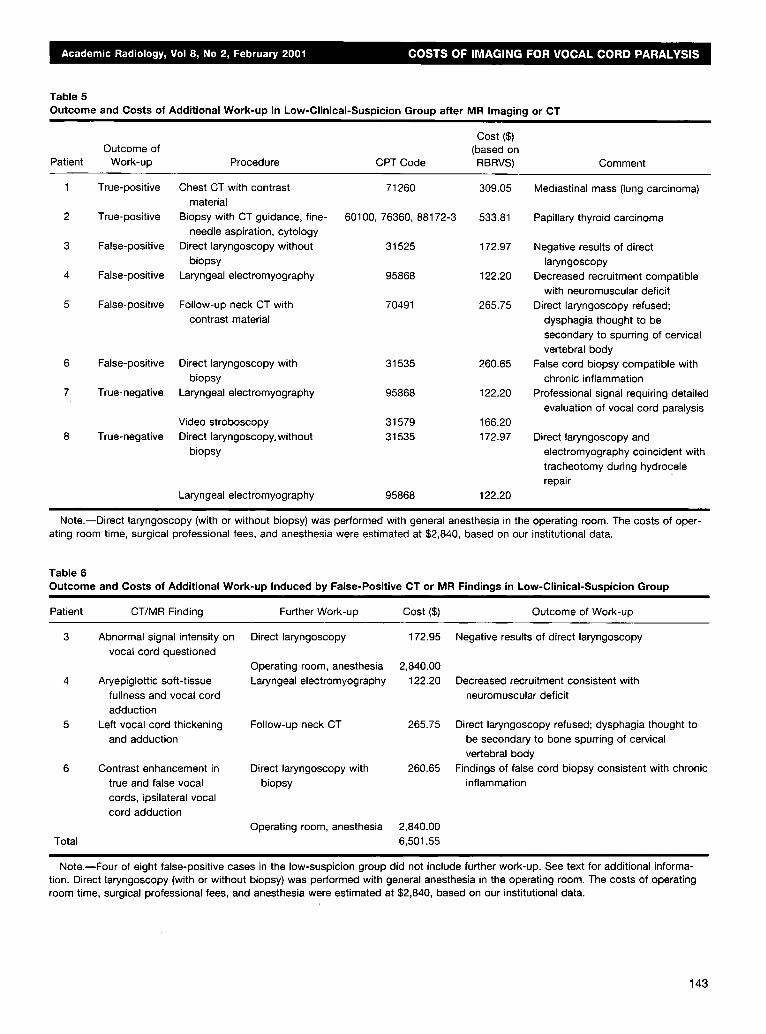
Table 5 Outcome and Costs of Additional Work-up in Low-Clinical-Suspicion Group after MR Imaging or CT
Cost ($) Outcome of (based on
Patient Work-up Procedure CPT Code RBRVS) Comment
1 True-positive Chest CT with contrast 71260 309.05 material
2 True-positive Biopsy with CT guidance, fine- 60100, 76360, 88172-3 533.81 needle aspiration, cytology
3 False-positive Direct laryngoscopy without 31525 172.97 biopsy
4 False-positive Laryngeal electromyography 95868 122.20
5 False-positive Follow-up neck CT with 70491 265.75 contrast material
6 False-positive Direct laryngoscopy with 31535 260.65 biopsy
7 True-negative Laryngeal electromyography 95868 122.20
Video stroboscopy 31579 166.20 8 True-negative Direct laryngoscopy.without 31535 172.97
biopsy
Laryngeal electromyography 95868 122.20
Mediastinal mass (lung carcinoma)
Papillary thyroid carcinoma
Negative results of direct laryngoscopy
Decreased recruitment compatible with neuromuscular deficit
Direct laryngoscopy refused; dysphagia thought to be secondary to spurring of cervical vertebral body
False cord biopsy compatible with chronic inflammation
Professional signal requiring detailed evaluation of vocal cord paralysis
Direct laryngoscopy and electromyography coincident with tracheotomy during hydrocele repair
Note.--Direct laryngoscopy (with or without biopsy) was performed with general anesthesia in the operating room. The costs of oper- ating room time, surgical professional fees, and anesthesia were estimated at $2,840, based on our institutional data.
Table 6 Outcome and Costs of Additional Work-up Induced by False-Positive CT or MR Findings in Low-Clinical-Suspicion Group
Patient CT/MR Finding Further Work-up Cost ($) Outcome of Work-up
3 Abnormal signal intensity on Direct laryngoscopy 172.95 Negative results of direct laryngoscopy vocal cord questioned
Operating room, anesthesia 2,840.00 4 Laryngeal electromyography 122.20 Aryepiglottic soft-tissue
fullness and vocal cord adduction
5 Left vocal cord thickening Follow-up neck CT 265.75 and adduction
6 Contrast enhancement in Direct laryngoscopy with 260.65 true and false vocal biopsy cords, ipsilateral vocal cord adduction
Total Operating room, anesthesia 2,840.00
6,501.55
Decreased recruitment consistent with neuromuscular deficit
Direct laryngoscopy refused; dysphagia thought to be secondary to bone spurring of cervical vertebral body
Findings of false cord biopsy consistent with chronic inflammation
Note.--Four of eight false-positive cases in the low-suspicion group did not include further work-up. See text for additional informa- tion. Direct laryngoscopy (with or without biopsy) was performed with general anesthesia in the operating room. The costs of operating room time, surgical professional fees, and anesthesia were estimated at $2,840, based on our institutional data.
143
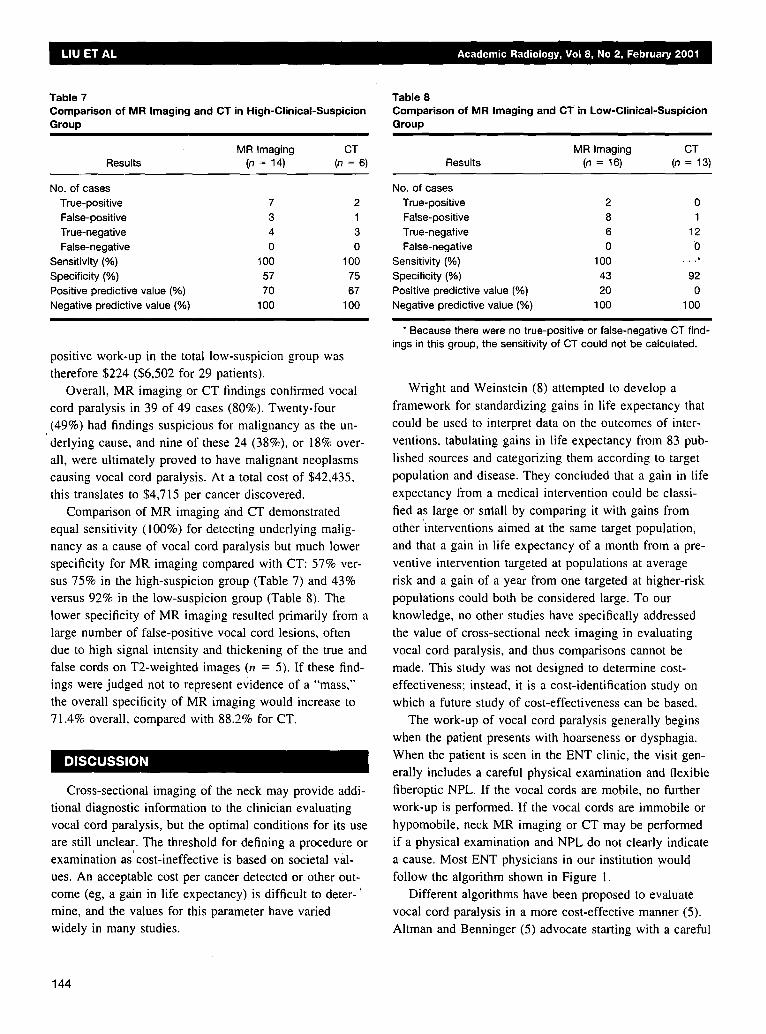
Table 7 Comparison of MR Imaging and CT in High-Clinical-Suspicion Group
MR Imaging CT Results (n = 14) (n = 6)
No. of cases True-positive 7 2 False-positive 3 1 True-negative 4 3 False-negative 0 0
Sensitivity (%) 100 100 Specificity (%) 57 75 Positive predictive value (%) 70 67 Negative predictive value (%) 100 100
positive work-up in the total low-suspicion group was therefore $224 ($6,502 for 29 patients).
Overall, MR imaging or CT findings confirmed vocal
cord paralysis in 39 of 49 cases (80%). Twenty-four (49%) had findings suspicious for malignancy as the un- derlying cause, and nine of these 24 (38%), or 18% over- all, were ultimately proved to have malignant neoplasms causing vocal cord paralysis. At a total cost of $42,435, this translates to $4,715 per cancer discovered.
Comparison of MR imaging and CT demonstrated equal sensitivity (100%) for detecting underlying malig- nancy as a cause of vocal cord paralysis but much lower specificity for MR imaging compared with CT: 57% ver- sus 75% in the high-suspicion group (Table 7) and 43% versus 92% in the low-suspicion group (Table 8). The lower specificity of MR imaging resulted primarily from a large number of false-positive vocal cord lesions, often due to high signal intensity and thickening of the true and
false cords on T2-weighted images (n = 5). If these find- ings were judged not to represent evidence of a "mass," the overall specificity of MR imaging would increase to 71.4% overall, compared with 88.2% for CT.
Cross-sectional imaging of the neck may provide addi- tional diagnostic information to the clinician evaluating vocal cord paralysis, but the optimal conditions for its use are still unclear. The threshold for defining a procedure or examination as' cost-ineffective is based on societal val- ues. An acceptable cost per cancer detected or other out- come (eg, a gain in life expectancy) is difficult to deter-' mine, and the values for this parameter have varied widely in many studies.
Table 8 Comparison of MR Imaging and CT in Low-Clinical-Suspicion Group
MR Imaging CT Results (n = 16) (n = 13)
No. of cases True-positive 2 0 False-positive 8 1 True-negative 6 12 False-negative 0 0
Sensitivity (%) 100 . . . * Specificity (%) 43 92 Positive predictive value (%) 20 0 Negative predictive value (%) 100 100
* Because there were no true-positive or false-negative CT find- ings in this group, the sensitivity of CT could not be calculated.
Wright and Weinstein (8) attempted to develop a
framework for standardizing gains in life expectancy that could be used to interpret data on the outcomes of inter-
ventions, tabulating gains in life expectancy from 83 pub-
lished sources and categorizing them according to target
population and disease. They concluded that a gain in life
expectancy from a medical intervention could be classi-
fied as large or small by comparing it with gains from other interventions aimed at the same target population,
and that a gain in life expectancy of a month from a pre-
ventive intervention targeted at populations at average
risk and a gain of a year from one targeted at higher-risk
populations could both be considered large. To our knowledge, no other studies have specifically addressed
the value of cross-sectional neck imaging in evaluating
vocal cord paralysis, and thus comparisons cannot be
made. This study was not designed to determine cost- effectiveness; instead, it is a cost-identification study on
which a future study of cost-effectiveness can be based. The work-up of vocal cord paralysis generally begins
when the patient presents with hoarseness or dysphagia.
When the patient is seen in the ENT clinic, the visit gen-
erally includes a careful physical examination and flexible fiberoptic NPL. If the vocal cords are mobile, no further
work-up is performed. If the vocal cords are immobile or hypomobile, neck MR imaging or CT may be performed
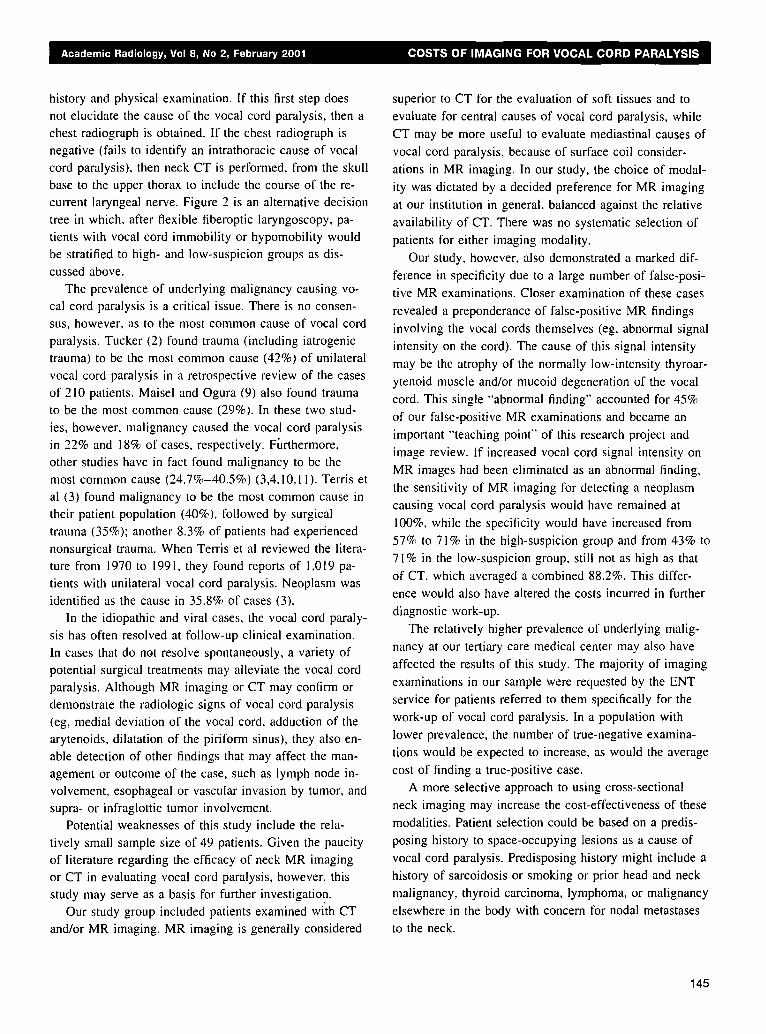
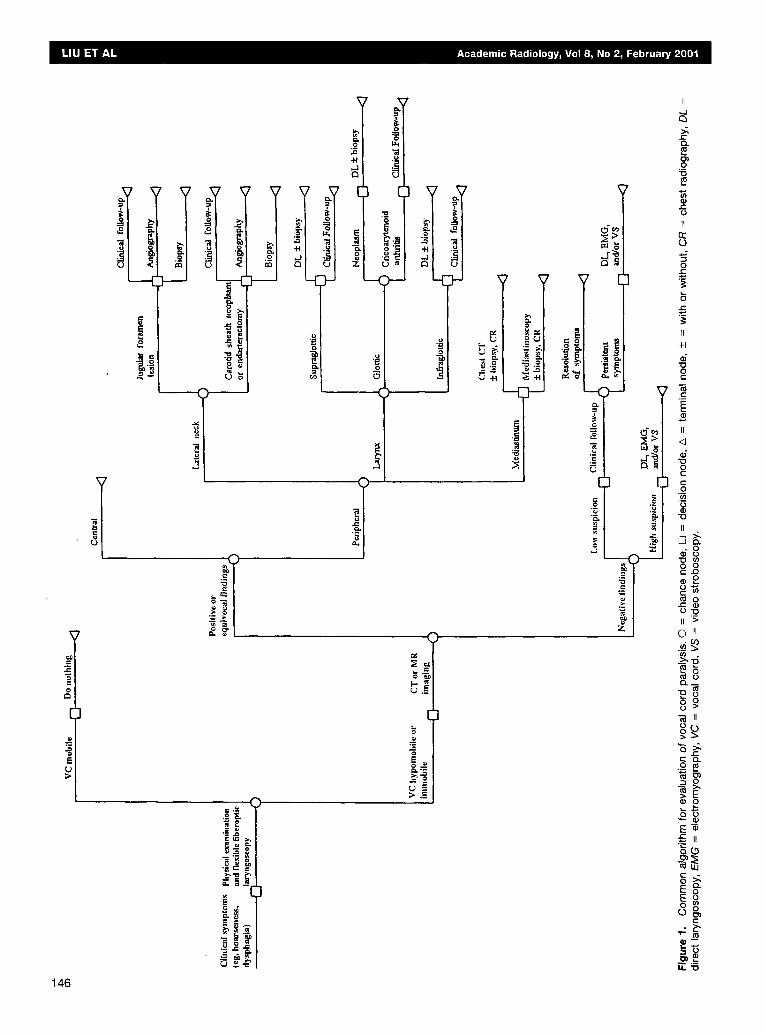
if a physical examination and NPL do not clearly indicate a cause. Most ENT physicians in our institution ,would
follow the algorithm shown in Figure 1. Different algorithms have been proposed to evaluate
vocal cord paralysis in a more cost-effective manner (5). Altman and Benninger (5) advocate starting with a careful
144
history and physical examination. If this first step does
not elucidate the cause of the vocal cord paralysis, then a chest radiograph is obtained. If the chest radiograph is negative (fails to identify an intrathoracic cause of vocal cord paralysis), then neck CT is perfornled, from the skull
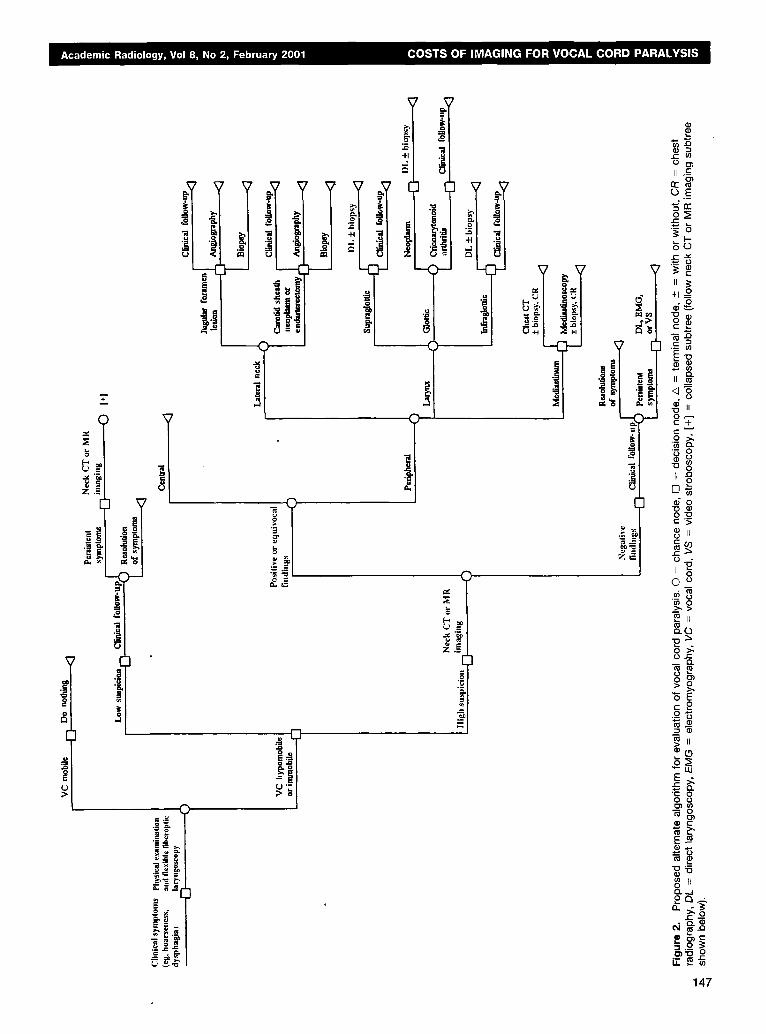
base to the upper thorax to include the course of the re- current laryngeal nerve. Figure 2 is an alternative decision
tree in which, after flexible fiberoptic laryngoscopy, pa- tients with vocal cord immobility or hypomobility would
be stratified to high- and low-suspicion groups as dis- cussed above.
The prevalence of underlying malignancy causing vo- cal cord paralysis is a critical issue. There is no consen-
sus, however, as to the most common cause of vocal cord paralysis. Tucker (2) found trauma (including iatrogenic trauma) to be the most common cause (42%) of unilateral vocal cord paralysis in a retrospective review of the cases
of 210 patients. Maisel and Ogura (9) also found trauma to be the most common cause (29%). In these two stud- ies, however, malignancy caused the vocal cord paralysis
in 22% and 18% of cases, respectively. Ffirthermore, other studies have in fact found malignancy to be the most common cause (24.7%-40.5%) (3,4,10,11). Terris et al (3) found malignancy to be the most common cause in
their patient population (40%), followed by surgical trauma (35%); another 8.3% of patients had experienced nonsurgical trauma. When Terris et al reviewed the litera- ture from 1970 to 1991, they found reports of 1,019 pa-
tients with unilateral vocal cord paralysis. Neoplasm was identified as the cause in 35.8% of cases (3).
In the idiopathic and viral cases, the vocal cord paraly- sis has often resolved at follow-up clinical examination. In cases that do not resolve spontaneously, a variety of
potential surgical treatments may alleviate the vocal cord paralysis. Although MR imaging or CT may confirm or demonstrate the radiologic signs of vocal cord paralysis (eg, medial deviation of the vocal cord, adduction of the arytenoids, dilatation of the piriform sinus), they also en-
able detection of other findings that may affect the man- agement or outcome of the case, such as lymph node in- volvement, esophageal or vascular invasion by tumor, and
supra- or infraglottic tumor involvement. Potential weaknesses of this study include the rela-
tively small sample size of 49 patients. Given the paucity of literature regarding the efficacy of neck MR imaging or CT in evaluating vocal cord paralysis, however, this study may serve as a basis for further investigation.
Our study group included patients examined with CT and/or MR imaging. MR imaging is generally considered
superior to CT for the evaluation of soft tissues and to
evaluate for central causes of vocal cord paralysis, while
CT may be more useful to evaluate mediastinal causes of
vocal cord paralysis, because of surface coil consider-
ations in MR imaging. In our study, the choice of modal-
ity was dictated by a decided preference for MR imaging
at our institution in general, balanced against the relative
availability of CT. There was no systematic selection of
patients for either imaging modality.
Our study, however, also demonstrated a marked dif-
ference in specificity due to a large number of false-posi-
tive MR examinations. Closer examination of these cases
revealed a preponderance of false-positive MR findings
involving the vocal cords themselves (eg, abnormal signal
intensity on the cord). The cause of this signal intensity
may be the atrophy of the normally low-intensity thyroar-
ytenoid muscle and/or mucoid degeneration of the vocal
cord. This single "abnormal finding" accounted for 45%
of our false-positive MR examinations and became an
important "teaching point" of this research project and
image review. If increased vocal cord signal intensity on
MR images had been eliminated as an abnormal finding,
the sensitivity of MR imaging for detecting a neoplasm
causing vocal cord paralysis would have remained at
100%, while the specificity would have increased from
57% to 71% in the high-suspicion group and from 43% to
71% in the low-suspicion group, still not as high as that
of CT, which averaged a combined 88.2%. This differ-
ence would also have altered the costs incurred in further
diagnostic work-up.
The relatively higher prevalence of underlying malig-
nancy at our tertiary care medical center may also have
affected the results of this study. The majority of imaging
examinations in our sample were requested by the ENT
service for patients referred to them specifically for the
work-up of vocal cord paralysis. In a population with
lower prevalence, the number of true-negative examina-
tions would be expected to increase, as would the average
cost of finding a true-positive case.
A more selective approach to using cross-sectional
neck imaging may increase the cost-effectiveness of these
modalities. Patient selection could be based on a predis-
posing history to space-occupying lesions as a cause of
vocal cord paralysis. Predisposing history might include a history of sarcoidosis or smoking or prior head and neck
malignancy, thyroid carcinoma, lymphoma, or malignancy
elsewhere in the body with concern for nodal metastases
to the neck.
145
146
t
l
t
U
)
~~
] 0 "
;~ ._=
5"
r. ,~,
-H
--[ t---
~7
-i
' 1
II
o
c ,
II
0 °
o
II
÷ l
~S " o o
E
IL
"t3 o E E o
o
" o
II D~
- 0 0
"p (n 0 0 c-.Q
® 2
m o e-. I~ o " O
II >
O II
CL__
" ~ II
21 O
• O
E-~
o g e-
. ~ -
._~ .~
÷
t
O 13~
II .{::
,f -~I' , °.° ' " ~ r r
.o ~. ~. ~ ,-°~,_
'5 - .= =
• . , .=
.~ ,,,= .=
i Z
=
z , - =
• ~ 0
~o r4 rT.~ ~ o 8 . 8 o ¢ iI
0 - l o
0 o ._~ "~ m o ~ >
o > , 0 e.-
~ E c ~ .9 ~
m~
"E Q o o 131(/) ~ g • E
E_~
e~ ,..1
o ~
L~ ~. ~
1 4 7
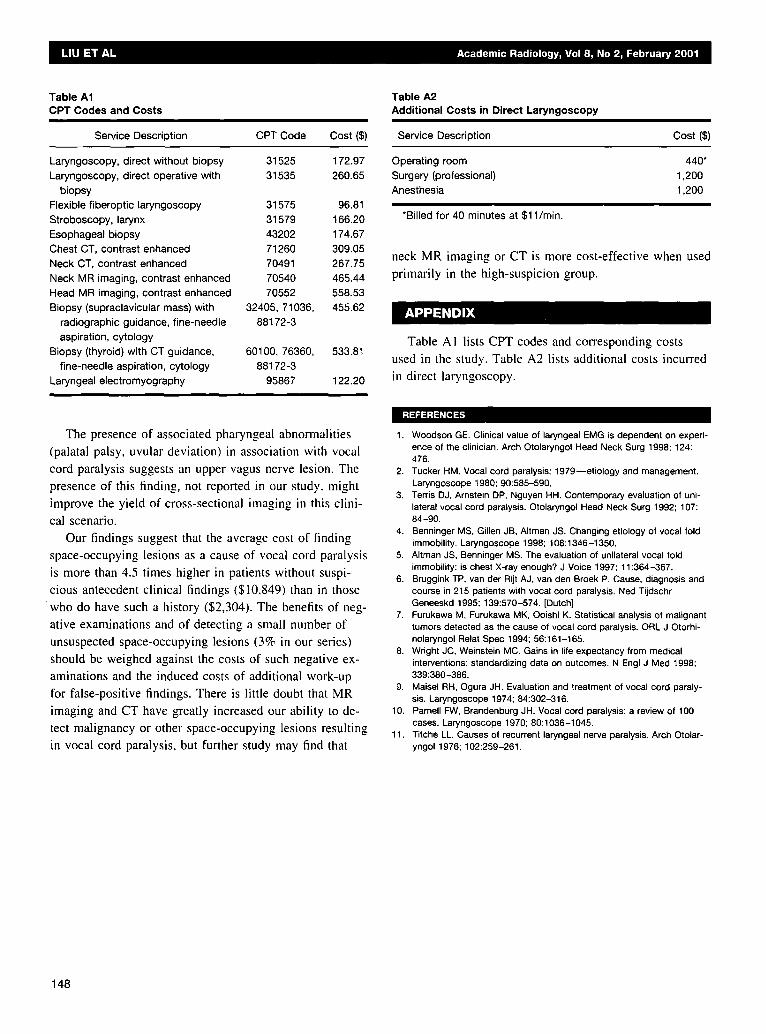
Table A1 OPT Codes and Costs
i
Service Description CPT Code Cost(S)
Laryngoscopy, direct without biopsy Laryngoscopy, direct operative with
biopsy Flexible fiberoptic laryngoscopy
Stroboscopy, larynx Esophageal biopsy Chest CT, contrast enhanced Neck CT, contrast enhanced Neck MR imaging, contrast enhanced Head MR imaging, contrast enhanced Biopsy (supraclavicular mass) with
radiographic guidance, fine-needle aspiration, cytology
Biopsy (thyroid) with CT guidance, fine-needle aspiration, cytology
Laryngeal electromyography
31525 172.97 31535 260.65
31575 96.81
31579 166.20 43202 174.67 71260 309.05 70491 267.75 70540 465.44 70552 558.53
32405, 71036, 455.62 88172-3
60100, 76360, 533.81 88172-3
95867 122.20
Table A2 Additional Costs in Direct Laryngoscopy
Service Description Cost ($)
Operating room 440* Surgery (professional) 1,200 Anesthesia 1,200
*Billed for 40 minutes at $11/min.
neck MR imaging or CT is more cost-effective when used primarily in the high-suspicion group.
Table AI lists CPT codes and corresponding costs
used in the study. Table A2 lists additional costs incun'ed in direct laryngoscopy.
:IEFERENCE -c
The presence of associated pharyngeal abnormalities (palatal palsy, uvular deviation) in association with vocal
cord paralysis suggests an upper vagus nerve lesion. The presence of this finding, not reported in our study, might improve the yield of cross-sectional imaging in this clini- cal scenario.
Our findings suggest that the average cost of finding space-occupying lesions as a cause of vocal cord paralysis is more than 4.5 times higher in patients without suspi- cious antecedent clinical findings ($10,849) than in those
w h o do have such a history ($2,304). The benefits of neg- ative examinations and of detecting a small number of unsuspected space-occupying lesions (3% in our series)
should be weighed against the costs of such negative ex- aminations and the induced costs of additional work-up for false-positive findings. There is little doubt that MR imaging and CT have greatly increased our ability to de- tect malignancy or other space-occupying lesions resulting in vocal cord paralysis, but further study may find that
1. Woodson GE. Clinical value of laryngeal EMG is dependent on experi- ence of the clinician. Arch Otolaryngol Head Neck Surg 1998; 124: 476.
2. Tucker HM. Vocal cord paralysis: 1979--etiology and management. Laryngoscope 1980; 90:585-590.
3. Terris D J, Arnstein DP, Nguyen HH. Contemporary evaluation of uni- lateral vocal cord paralysis. Otolaryngol Head Neck Surg 1992; 107: 84 -90.
4. Benninger MS, Gillen JB, Altman JS. Changing etiology of vocal fold immobility. Laryngoscope 1998; 108:1346-1350.
5. Altman JS, Benninger MS. The evaluation of unilateral vocal fold immobility: is chest X-ray enough? J Voice 1997; 11:364-367.
6. Bruggink TP, van der Rijt A J, van den Broek P. Cause, diagnosis and course in 215 patients with vocal cord paralysis. Ned Tijdschr Geneeskd 1995; 139:570-574. [Dutch]
7. Furukawa M, Furukawa MK, Ooishi K. Statistical analysis of malignant tumors detected as the cause of vocal cord paralysis. ORL J Otorhi- nolaryngol Relat Spec 1994; 56:161-165.
8. Wright JC, Weinstein MC. Gains in life expectancy from medical interventions: standardizing data on outcomes. N Engl J Med 1998; 339:380-386.
9. Maisel RH, Ogura JH. Evaluation and treatment of vocal cord paraly- sis. Laryngoscope 1974; 84:302-316.
10. Parnell FW, Brandenburg JH. Vocal cord paralysis: a review of 100 cases. Laryngoscope 1970; 80:1036-1045.
11. Titche LL. Causes of recurrent laryngeal nerve paralysis. Arch Otolar- yngo11976; 102:259-261.
148