ebstein’s anomaly with paradoxical embolism … v 64 2 ebstein’s anomaly with paradoxical...
TRANSCRIPT
82 Journal of The Association of Physicians of India ■ Vol. 64 ■ December 2016
Ebstein’s Anomaly with Paradoxical Embolism to Lower LimbGouranga Santra1, Shinjan Patra2
Introduction
Eb s t e i n ’ s a n o m a l y ( E A) i s a malformation of tricuspid valve
characterised by apical displacement of the septal and posterior leaflefts from the atrioventricular ring. There is atrialisation of right ventricle (RV). In India, it represents just over 1% of all congenital heart diseases (CHD).1 Paradoxical embolism (PDE) to brain or extremities may occur in EA due to associated atrial septal defect (ASD).2,3
Case Report
A n 1 8 y e a r o l d m a l e p a t i e n t presented with swelling of left leg with severe pain for five days. He had shortness of breath on exertion for last two years. No family history of CHD was present. His mother had no history of antenatal intake of benzodiazepine or lithium carbonate. He had clubbing of second degree, polycythemia, mild cyanosis and bilateral pedal oedema. His blood pressure was 112/72 mm
AbstractEbstein’s anomaly (EA) is a rare congenital heart disease. Paradoxical embolism (PDE) may occur in EA due to associated atrial septal defect (ASD). An 18 year old male with EA presented with left lower limb ischemia due to PDE to the limb. No features of cerebral embolism was present. PDE is a potential complication of EA. High level of awareness is needed for early diagnosis of PDE in EA to save a limb in case of embolism to the extremity.
1Associate Professor; 2Post-graduate trainee, Dept. of Medicine, Midnapore Medical College, Midnapore, West BengalReceived: 07.12.2015; Accepted: 25.05.2016
both sides were normally palpable. Laboratory investigations revealed
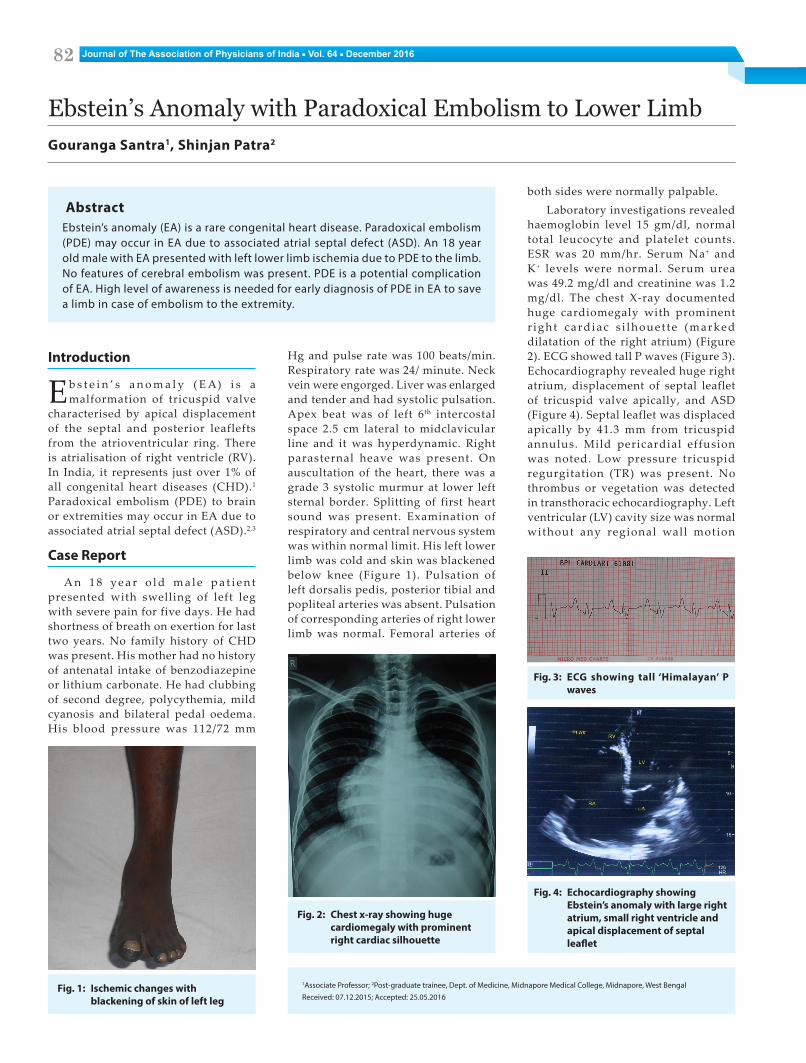
haemoglobin level 15 gm/dl, normal total leucocyte and platelet counts. ESR was 20 mm/hr. Serum Na+ and K+ levels were normal. Serum urea was 49.2 mg/dl and creatinine was 1.2 mg/dl. The chest X-ray documented huge cardiomegaly with prominent r ight cardiac s i lhouet te (marked dilatation of the right atrium) (Figure 2). ECG showed tall P waves (Figure 3). Echocardiography revealed huge right atrium, displacement of septal leaflet of tricuspid valve apically, and ASD (Figure 4). Septal leaflet was displaced apically by 41.3 mm from tricuspid annulus. Mild pericardial effusion was noted. Low pressure tricuspid regurgitation (TR) was present. No thrombus or vegetation was detected in transthoracic echocardiography. Left ventricular (LV) cavity size was normal without any regional wall motion
Hg and pulse rate was 100 beats/min. Respiratory rate was 24/ minute. Neck vein were engorged. Liver was enlarged and tender and had systolic pulsation. Apex beat was of left 6th intercostal space 2.5 cm lateral to midclavicular line and it was hyperdynamic. Right parasternal heave was present. On auscultation of the heart, there was a grade 3 systolic murmur at lower left sternal border. Splitting of first heart sound was present. Examination of respiratory and central nervous system was within normal limit. His left lower limb was cold and skin was blackened below knee (Figure 1). Pulsation of left dorsalis pedis, posterior tibial and popliteal arteries was absent. Pulsation of corresponding arteries of right lower limb was normal. Femoral arteries of
Fig. 1: Ischemic changes with blackening of skin of left leg
Fig. 4: Echocardiography showing Ebstein’s anomaly with large right atrium, small right ventricle and apical displacement of septal leaflet
Fig. 2: Chest x-ray showing huge cardiomegaly with prominent right cardiac silhouette
Fig. 3: ECG showing tall ‘Himalayan’ P waves

83Journal of The Association of Physicians of India ■ Vol. 64 ■ December 2016
abnormality but LV systolic function was moderatly compromised. LV ejection fraction was 36 %. Administration of intravenous agitated saline revealed a right-to-left shunt. Transesophageal echocardiography was not possible. Duplex ultrasound of arterial system revealed a thrombus at left popliteal artery, other arteries being normal. No other cause of thrombophilia was found. Coagulation study was normal. The case was finally diagnosed as EA with PDE to left lower limb.
Discussion
EA is associated with atrialisation of RV. RV may also be dysplastic. Other associated cardiac malformations are ASD (80%), left ventricular fibrosis and ventricular non-compaction. EA represents only ~1 % of all CHD, but it is disproportionately represented in the adult CHD population because of its favourable natural history. Congenital giant right atrium may sometimes be mistaken as EA.4
EA has variable clinical course. Long-term prognosis depends on the severity of TR and the right to left shunt. Patients may have progressive cyanosis, congestive cardiac failure (CCF) and atrial fibrillation (AF).5 Paroxysmal atrial tachyarrythmias with or without Wol f -Park inson-Whi te syndrome (atroventricular bypass tract) may occur. ASD predisposes EA patients to PDE.2,3 Infective endocarditis, brain abscess and sudden death may also occur. Our patient was symptomatic for two years with shortness of breath due to CCF. He had tall ‘Himalayan’ P waves due to huge right atrial enlagement suggestive of EA.6 History suggestive of supraventricular tachycardia was
absent. Brain infarct was absent but PDE to left lower extremity was present due to associated ASD.
A patent foramen ovale or ASD is commonly seen in PDE. Emboli arising in systemic veins may pass directly to systemic circulation because of right to left intracardiac shunt which allows venous blood to bypass the normal filtering action of the lungs. The shunt may be a consequence of CHD but can also occur across a patent foramen ovale if pressure in the right atrium exceeds that in the left. Such a pressure reversal is a transient occurrence during normal cardiac cycle but it may also occur when right atrial pressure is raised physiological ly during Valsalva’s manoeuvre, or pathologically in right heart fa i lure or acute pulmonary embolus. Paradoxical emboli lodge with almost equal frequency in cerebral and limb circulations, but they may occasionally reach the coronary, renal or splenic arteries.
In presence of ASD, increased right atrial pressure induced by the haemodynamic and functional changes of EA causes reversed shunting (right-to-left), which can cause PDE leading to stroke or limb ischemia.2,3 PDE may be from right heart, venous system or embolism of unknown origin. Deep vein thrombosis (DVT) may be occult upon physical examination and doppler study. PDE may be associated with a hypercoagulable state, neoplasms (e.g., of the pancreas), protein C or S deficiency, factor V Leiden mutation and prothrombin mutations.
PDE is a diagnosis of exclusion. It is easily mimicked by other diseases causing cerebral and peripheral arterial
embol ism. The major di f ferent ia l diagnoses are thrombus, vegetations and tumour embolisms from left side of heart and atheroembolic diseases. In our case of EA, echochocardiography and duplex u l t rasound exc luded the source of embolism from lef t side of circulation. Enlarged right atrium was the possible source of thromboembolism. However, occult DVT might be there.
I n E A , P D E n e e d s s p e c i a l consideration. Anticoagulant with warfarin is recommended for patients with PDE and AF. Amputation may be required for ischemia and gangrene of limbs. High level of awareness is needed for early diagnosis of PDE in EA to save a limb in case of embolism to the extremity.
Conclusion
PDE is a potential complication of EA. High level of awareness is needed for early diagnosis of PDE in EA to save a limb in case of embolism to the extremity.
References1. Saxena A. Congenital heart disease in India: a status report.
Indian J Pediatr 2005; 72:595-8.
2. Uyan C, Yazici M, Uyan AP, Dokumaci B. Paradoxical embolism in Ebstein’s anomaly. Exp Clin Cardiol 2001; 6:173.
3. Melao F, Correia AS, Maciel MJ. Paradoxical embolism associated with Ebstein’s anomaly in an adult: Case report. Rev Port Cardiol 2013; 32:1023-5.
4. Santra G, Paul R, Das S, Datta A, Pradhan S. Sarkar RN. Congenital giant right atrium in an elderly woman. J Assoc Physicians India 2014; 62:634-6.
5. Roby A, Amrithlal. Ebstein anomaly with congestive cardiac failure. J Assoc Physicians India 2004; 52:486.
6. Kaushik ML, Sharma M, Kashyap R. ‘Himalayan’ p wave. J Assoc Physicians India 2007; 55:856.