early pregnancy hemorrhage
TRANSCRIPT

Early Pregnancy Hemorrhage
Dr. Hem Nath SubediIIND Year ResidentOBGYN, COMSTH
Bharatpur

Contents
• Objectives • Incidence• Causes • Investigation• Diagnosis• Management• Controversies

ObjectivesAfter completing this chapter, participants will be able to:
• Describe different entity of the vaginal bleeding in pregnancy and its management.
• Describe the process, diagnosis and management of miscarriage.
• Describe the techniques of suction curettage for the treatment of incomplete miscarriage.
Early Pregnancy Hemorrhage
• Complications arise more frrequently during the first trimester than any other stage of pregnancy.
• Most present with bleeding , pain or both.
Incidence • Vaginal bleeding occurs in about 20% of clinically diagnosed
pregnancy.
• Approximately 15% to 20% of clinically recognized pregnancies miscarry.
• When bleeding occurs in 1st trimester 30% of pregnancies will miscarry.
• 10 % to 15% will be an ectopic pregnancy, 0.2% will be hydatidiform mole and 5% will have termination of pregnancy.
• The remaining 50% will continue beyond the 20weeks.

Causes
• The causes of bleeding in early pregnancy are broadly divided into two groups:
• Those related to the pregnancy : This group relates to – Spontaneous Abortion – Ectopic pregnancy– Gestational trophoblastic disease – Implantation bleeding.– Decidual bleeding
• Those associated with the pregnant state: The lesions are unrelated to pregnancy—either pre-existing or aggravated during pregnancy.– Cervical lesions such as vascular erosion, polyp, ruptured
varicose veins and malignancy.

Abortion
• The word abortion derives from the Latin aboriri—to miscarry.
• Abortion is defined as the spontaneous or induced termination of pregnancy before fetal viability.
• Popular use of abortion by laypersons implies a deliberate intact pregnancy termination, many prefer miscarriage for spontaneous fetal loss.
• Newer terms included early pregnancy loss, wastage, or failure.

Terms • Viability : gestational age of 22(154days) weeks period and weight of
500 gms. (WHO) in North America it is 20 weeks. Following features should noted for diagnosis of the pregnancy in Ultrasonography.– Gestational sac : TVS 4 to 5 weeks sac is 2 to 5 mm in diameter .– Yolk sac : Visible at 5.5 weeks and 2-5mm in diameter – Fetal cardiac activity: at 6 to 6.5 weeks with an embryonic length
of 1 to 5 mm and a mean sac diameter of 13 to 18 mm.– A 5-mm embryo without cardiac activity is likely dead.– Anembryonic gestation: when the mean gestational sac diameter
measures ≥ 20 mm and no embryo is seen.– Embryonic death: if an embryo measuring ≥ 10 mm has no
cardiac activity.


• Pregnancy of unknown location (PUL): discreminatory value of beta-hCG is there but no ultrasonic evidence of implantation.
• Uterine pregnancies that eventuate in a spontaneous abortion are also termed early pregnancy loss or early pregnancy failure.

classification of pregnancy loss

Terms that have been in clinical use for many decades are generally used to describe later pregnancy losses. These include:
1. Spontaneous abortion—this category includes threatened, inevitable, incomplete, complete, and missed abortion. Septic abortion is used to further classify any of these that are complicated further by infection.
2. Recurrent abortion—this term is variably defined, but it is meant to identify women with repetitive spontaneous abortions so that an underlying factor(s) can be treated to achieve a viable newborn.
3. Induced abortion—this term is used to describe surgical or medical termination of a live fetus that has not reached viability.


Spectrum of pregnancy

Spontaneous abortion
• Abortion is the expulsion or extraction from its mother of an embryo or fetus weighing 500 g or less when it is not capable of independent survival.
• 31 percent of pregnancies were lost after implantation.
• 12% of early pregnancies in which bleeding occurred went on to miscarry.

Causes
• Fetal Factors– Genetic Factors
• Maternal factors – Endocrine and metabolic – Anatomic – Infection– Immunological – Antifetal antibodies – Thrombophilias – Others

s

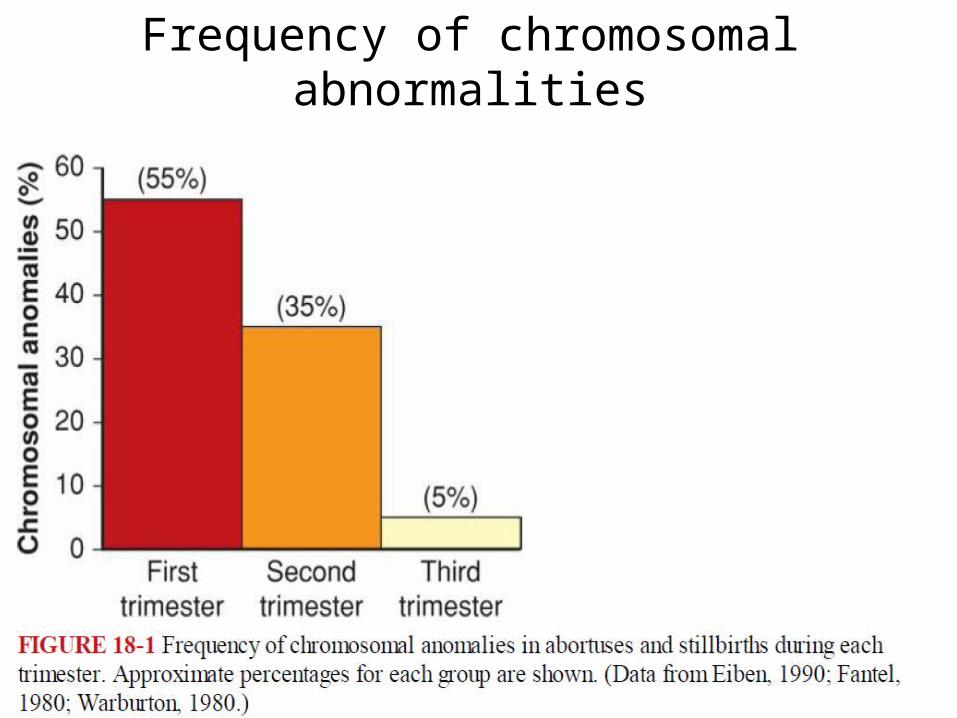
Frequency of chromosomal abnormalities

Types
• Threatened abortion • Inevitable abortion• Incomplete abortion• Complete abortion• Missed abortion • Septic abortion

Threatened abortion• Definition: It is a clinical entity where the process of miscarriage has
started but has not progressed to a state from which recovery is impossible.
• Clinical features:– Bleeding per vaginum – Pain lower abdomen – Speculum examination reveals—bleeding if any, escapes through
the external os. – Digital examination reveals the closed external os.– The uterine size corresponds to the period of amenorrhea. – The uterus and cervix feel soft. – Pelvic examination is avoided when ultrasonography is available.

Adverse Pregnancy outcomes after threatened abortion

Investigation
• Ultrasonography: for viability of fetus .
• Routine blood examination.
• Routine urine examination .
• If need serum b-hCG and serum progesterone level .

Threatened Abortion versus Ectopic Pregnancy.
• Diagnosis should focused on the differentiation of threatened abortion or ectopic pregnancy because if missed sometime leads to disaster .
• For this purpose following can be done – Serum hCG level monitoring – Serum Progesterone monitoring – Serial ultrasonography TVS as well as TAS.

Management
• Expectant management – Rest (pelvic rest: abstinence from intercourse, douching,
tampon use and strenuous physical activity)– Adequate diet – Save pads – Folic acid – Anti D-Immunoglobulin if mother is Rh negative
• No role of beta hcg , multivitamins, tocolytics.• Role of progesterone for threatened abortion is not evidence
based till now.
Inevitable Abortion
• Definition:– It is the clinical type of abortion where the changes
have progressed to a state from where continuation of pregnancy is impossible.
• Clinical Features:
The patient, having the features of threatened miscarriage, develops the following manifestations.
– Increased vaginal bleeding. – pain in the lower abdomen.– Dilated internal os of the cervix through which the products
of conception are felt.

• Management– to accelerate the process of expulsion– to maintain strict asepsis– General measures: • Intravenous fluid therapy • Blood transfusion if needed.
– Active treatment:• Before 12 weeks:–Dilatation and evacuation – Suction evacuation followed by curettage is done.
• After 12 weeks: – The uterine contraction is accelerated by oxytocin drip

(A) Threatened miscarriage; (B) Inevitable miscarriage; (C) Incomplete miscarriage

Incomplete Abortion• Definition: – When the entire products of conception are not expelled, instead a
part of it is left inside the uterine cavity, it is called incomplete miscarriage.
• Clinical features: – History of expulsion of a fleshy mass per vagina– Continuation of pain lower abdomen– Persistence of vaginal bleeding– Uterus smaller than the period of amenorrhea– Patulous cervical os often admitting tip of the finger– Varying amount of bleeding

• Management: • Resuscitation • Dilatation and evacuation• Suction curette• Medical management–Misoprostol – oxytocin

Complete Abortion• Definition: – When the products of conception are completely expelled ,it
is called complete miscarriage.
• Clinical features:– Expulsion of a fleshy mass per vagina – Subsidence of abdominal pain.– Vaginal bleeding becomes trace or absent – Uterus is smaller than the period of amenorrhea and a little firmer– Cervical os is closed– Bleeding is trace.
– Examination of the expelled fleshy mass is found to be complete.

• USG: women with heavy bleeding, an empty uterus with endometrial thickness < 15 mm is a diagnosis of completed miscarriage.
• Management:– Conservative – Blood transfusion if needed– Rest – Rh-negative women• Anti-D gammaglobulin

Missed Miscarriage
• Definition: – When the fetus is dead and retained inside the uterus for a
variable period, it is called missed miscarriage or early fetal demise.
• Clinical features: – Persistence of brownish vaginal discharge– Subsidence of pregnancy symptoms– Retrogression of breast changes – Cessation of uterine growth– Cervix feels firm and close – Test for pregnancy becomes negative


Management
• Uterus is less than 12 weeks:– Expectant management– Medical management: – Prostaglandin E1 (Misoprostol) 800 mg vaginally 3 hourly
for max 3 doses . – Suction evacuation or dilatation and evacuation

• Uterus more than 12 weeks:– Induction to be done– Prostaglandins are more effective than oxytocin in such
cases. – The methods used are:• Prostaglandin E1 analogue.• Oxytocin
– Dilatation and evacuation

• Some of the risks and benefits are summarized as follows:
1. Expectant management of spontaneous incomplete abortion has failure rates as high as 50 percent.
2. Medical therapy with prostaglandin E1 (PGE1) has varying failure rates of 5 to 40 percent.
3. Curettage usually results in a quick resolution that is 95- to 100-percent successful. It is invasive and not necessary for all women.



Technique for surgical management of spontaneous abortion
• Dilatation and curettage.• Dilatation and evacuation. • Dilatation and extraction.• Vacuum aspiration

Preparation for above mention procedures.• Dilatation of cervix by mechanical dilators,
hygroscopic dilators and prostaglandins. • Prophylactic antibiotics • Proper anesthesia and analgesia
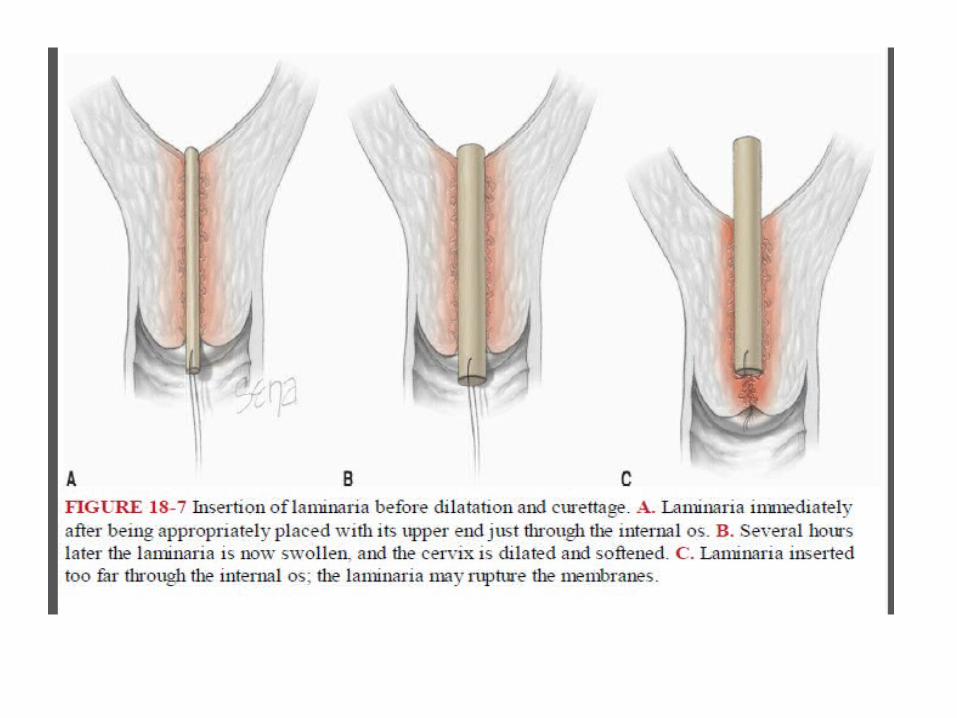

Different types of hygroscopic dilators






Septic abortion
Definition:• Any abortion associated with clinical evidences of infection
of the uterus and its contents, is called septic abortion.
Although clinical criteria vary, abortion is usually considered septic when there are:
• rise of temperature of at least 100.4°F (38°C) for 24 hours or more
• offensive or purulent vaginal discharge.• other evidences of pelvic infection such as lower abdominal
pain and tenderness.

Mode of infection:
The microorganisms involved in the sepsis are usually those normally present in the vagina (endogenous).
The microorganisms are:
(a) Anaerobic—• Bacteroides group (fragilis)• Anaerobic Streptococci• Cl. welchii• tetanus bacillus
(b) Aerobic—• Escherichia coli (E. coli)• Klebsiella• Staphylococcus• Pseudomonas • hemolytic Streptococcus
(usually exogenous).

Clinical features: – Depending upon the severity and the extent of infection, the
clinical picture varies widely. – History of illegal termination by an unauthorized person is
mostly concealed. – Pyrexia is an important clinical manifestation. – Pain abdomen of varying degrees is almost a constant feature.– A rising pulse rate of 100–120/min or more is a significant
finding than even pyrexia.– Variable systemic and abdominal findings depending upon the
spread of infection.– purulent vaginal discharge or a tender

Investigations:
Routine investigations include:
(1) Cervical or high vaginal swab is taken prior to internal examination.
(2) Blood for hemoglobin estimation, total and differential count of white cells, ABO and Rh grouping.
(3) Urine analysis including culture.

Special investigations—• Ultrasonography of pelvis and abdomen• Blood
(a) Culture—if associated with spell of chills and rigors
(b) Serum electrolytes—as an adjunct to the management protocol of endotoxic shock .
(c) Coagulation profile.• Plain X-ray
a) Abdomen—in suspected cases of bowel injury
b) Chest—for cases with pulmonary complications(atelectasis).
General management:Principles of management are:
(a) To control sepsis
(b) To remove the source of infection
(c) To give supportive therapy to bring back the normal homeostatic and cellular metabolism
(d) To assess the response of treatment.

Implantation Bleeding
• As the trophoblast erodes the endometrial endothelium and the blastocyst implants, a small vaginal loss may be apparent .
• Occurs at approximately 10-12 days post conception, around the same time as expected menses and may be mistaken for a woman’s period, although abnormal (usually bright red and lighter) .
• It is significant when calculating LMP for estimation of due date

Decidual Bleeding
• Occasionally there is bleeding from the decidua during the first 10 weeks, usually at around the time menses is expected.
• Caused by menstrual hormones.
• Especially common in the early stages of pregnancy, before the lining has completely attached to the placenta.
• Not thought to be a health threat to mother or fetus.
• May affect calculation of EDD

Controversies
• Regarding gestational age of viability and weight of viability.
• Role of progesterone in threatened abortion.
• Role of beta –hcg, tocolysis, multivitamins .
• With threatened abortion, immunoglobulin prophylaxis is controversial because of sparse evidence-based data.

References
• Early pregnancy hemorrhage in Williams obstetrics 24th edition, cunninghams, macgraw hill publication , 2014 newyork pp
• Early pregnancy hemorrage , In Dc dutta text book of Gynecology 6th edition, hiralal konor, pp.
• Early pregnancy complication in High Risk Pregnancy Management Option, 4th edition , D.K. James , macgraw Hill , pp
• American College of Obstetricians and Gynecologists, 2013c; Hannafin, 2006; Weiss, 2002).
• Early pregnancy complication: in Dewhurths text book of gynecology and obstetrics, 7th edition, 2011, newyork ,pp

• Thank you