dvt prophylaxis.ppt
TRANSCRIPT

Prophylaxis Pt. I
DVT Prophylaxis in the SICU
Gabriel Brat, MSIII
6/18/2007

Introduction
• Importance of DVTs
• Risk Factors
• Methods of Prophylaxis
• Recommendations
• Compliance

Bundles
• PE third most common cause of iatrogenic death.
• 2001 AHRQ report emphasized 1A evidence
• IHI 5 million lives campaign—VAP bundle
LE DUS for PE
• 90% PE’s originate in lower extremity• 1st symptomatic DVT
– Sensitivity 95%, specificity 96%– Increased sensitivity:
• serial US at 5-7 days• combining with clinical suspicion

Lower Extremity Veins
Iliac
(Superficial)Femoral
Deep (Common) Femoral
External Saphenous
Internal Saphenous
Popliteal
Hauer. UCSF 2005

Risk Factors for DVTSurgeryTrauma (major or lower extremity)ImmobilityParesisMalignancyCancer therapy (hormonal, chemotherapy, or radiotherapy)Previous VTEIncreasing agePregnancy and the postpartum periodEstrogen-containing oral contraception or hormone replacement therapySelective estrogen receptor modulatorsAcute medical illnessHeart or respiratory failureInflammatory bowel diseaseNephrotic syndromeMyeloproliferative disordersParoxysmal nocturnal hemoglobinuriaObesitySmokingVaricose veinsCentral venous catheterizationInherited or acquired thrombophilia

Risk of DVT
Patient GroupDVT Prevalence,
%
Medical patients 10–20
General surgery 15–40
Major gynecologic surgery 15–40
Major urologic surgery 15–40
Neurosurgery 15–40
Stroke 20–50
Hip or knee arthroplasty, hip fracture surgery 40–60
Major trauma 40–80
Spinal cord injury 60–80
Critical care patients 10–80
Geerts et al.Chest, 2004;126:338S

Inherited Hypercoagulability
Prevalence DVT
Population Prevalence
Factor V Leiden 12-21%** 6%
Prothrombin mut 6-8% 2%
Protein C, S def 2-4% < 1%
AT III def 1-2% <1%
All Thrombophilia 24-37% 10%
**OR 5.9 (CI 2-18) for breakthrough
Albrecht. Online 2007Baba Ahmed. Thromb Haemost 2007; 97: 171

Mechanical Prophylaxis

Overview
Mechanical Compression
• No convincing evidence of mortality value over placebo.
Plantar vs. Calf
• DVT in 21.0% plantar vs. 6.5% calf (p = 0.009).
Knee-length vs. Thigh-length
• Equivalent effect w improved compliance in KL group.
Mechanical vs. Chemical
• OR 0.46 (CI 0.16-1.29) for all heparin vs. mechanical
Gregory et al. J Trauma 1999; 47:1

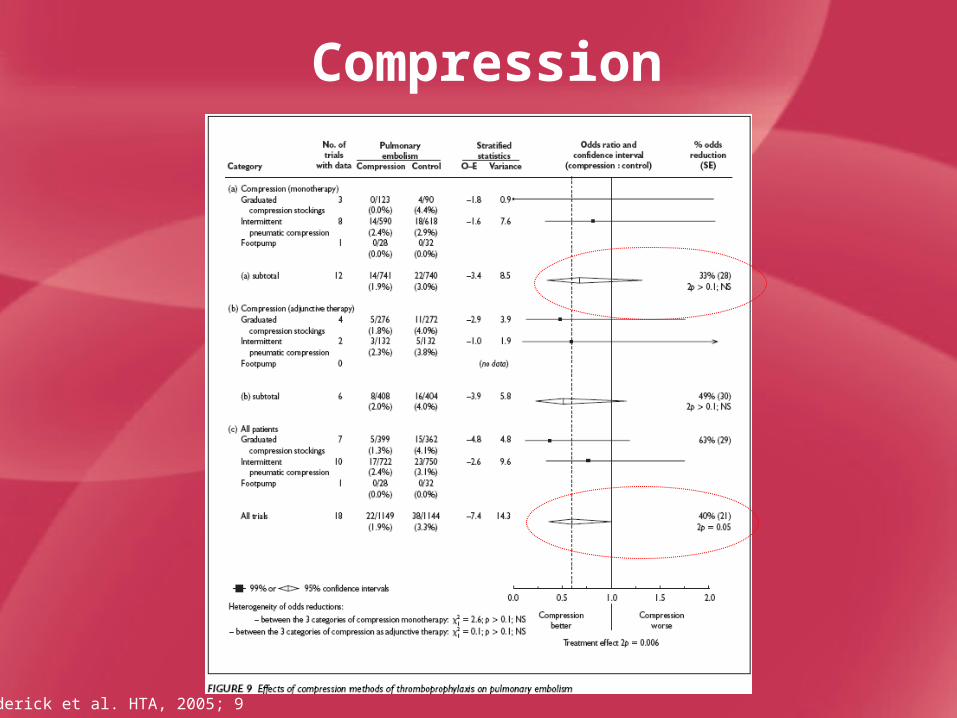
Compression
Roderick et al. HTA, 2005; 9
Compression
Roderick et al. HTA, 2005; 9

Chemical Prophylaxis

Overview
Aspirin
• Not recommended for DVT prophylaxis
• Aspirin vs. LMWH
• 63% RRR among 205 ortho pts LMWH vs. ASA.
• Among hip trauma pts, 44% vs. 28% ASA vs. LMWH
UFH and LMWH• UFH decreases incidence of DVT by 20% over placebo• LMWH decreases incidence of DVT by 30% over UFH.

Mechanism of Heparins
Weitz. NEJM, 1997; 337:688
Unfractionated heparin inactivates both Factor IIa and Xa
LMWH has increased affinity for Factor Xa
Fondiparinux is only a pentasaccharide sequence
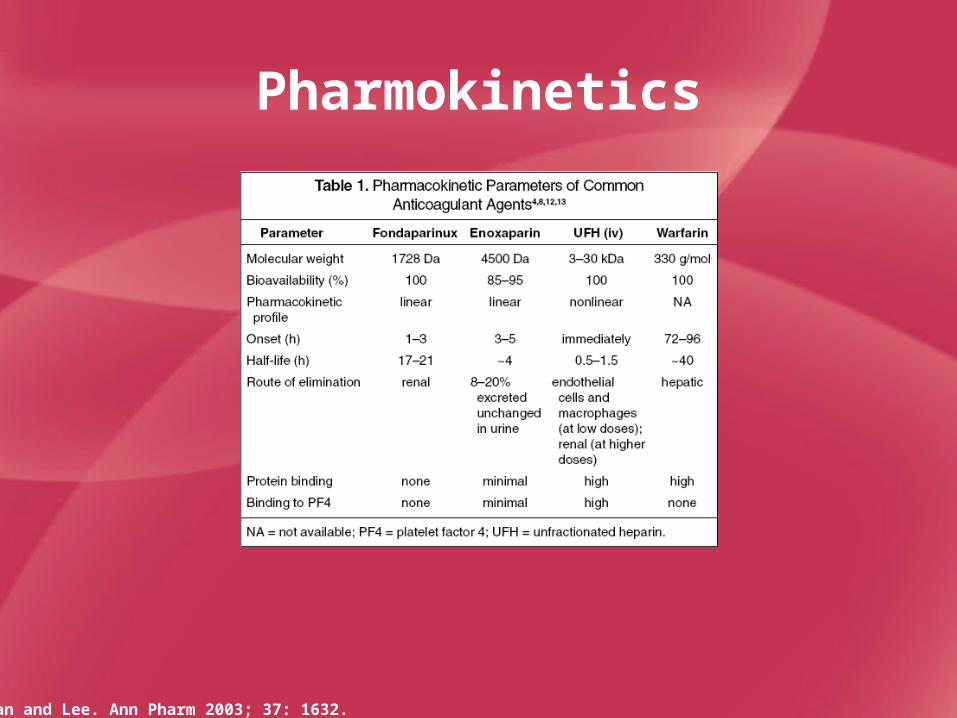
Pharmokinetics
Tran and Lee. Ann Pharm 2003; 37: 1632.

Dolovich, L. R. et al. Arch Intern Med 2000;160:181-188.
LMWH vs. UFH

Dolovich, L. R. et al. Arch Intern Med 2000;160:181-188.
LMWH vs. UFH 2

Dolovich, L. R. et al. Arch Intern Med 2000;160:181-188.
LMWH vs. UFH 3

Atia et al. Arch Intern Med 2001; 161: 10.
LMWH vs. UFH in Trauma

LMWH vs. UFH in Trauma
Geerts et al. NEJM 1996
• Double blind, RCT• 344 major trauma—no ICH• 1st dose within 36 hours of injury • No mechanical prophylaxis• 5000 U LDUH v. 30 mg enoxaparin BID• RRR DVT 30% for LMWH• Higher bleeding in LMWH, but not
significant

Leonardi, M. J. et al. Arch Surg 2006;141:790-799.
Complication Rates

LMWH
Advantages• Longer half life• Improved efficacy• Less heparin-induced
thrombocytopenia• Cost-effective for
trauma and gen surg
Disadvantages• Poor protamine
response (60%)• Variable effect w
renal failure, obesity• Concern for
bleeding

DVT Recommendations
Geerts et al. Chest, 2004; 126:338S
DVT, %
PE, %
Level of Risk
Calf Proximal Clinical Fatal Successful Prevention Strategies
Low risk 2 0.4 0.2 <0.01
Minor surgery in patients < 40 yr with no additional risk factors
No specific prophylaxis; early and "aggressive" mobilization
Moderate risk 10–20 2–4 1–2
0.1–0.4
Minor surgery in patients with risk factors LDUH (q12h), LMWH ( 3,400 U daily), GCS, or IPC
High risk 20–40 4–8 2–4
0.4–1.0
Surgery in patients > 60 yr LDUH (q8h), LMWH (> 3,400 U daily), or IPC
Highest risk 40–80 10–20 4–10 0.2–5
Surgery in patients with multiple risk factors, Trauma, Ortho
LMWH (> 3,400 U daily), fondaparinux, oral VKAs (INR, 2–3), or IPC/GCS + LDUH/LMWH

IVC Filters

IVCF Reasons for Use
• Clot with active cerebral bleeding
• Clot despite anticoagulation
• Massive PE with chronically compromised pulmonary vasculature

IVCF Effectiveness
Filter No filter p
PE at day 12 1% 5% 0.03
PE at 2 years 3% 6% NS
DVT at 2 years 21% 12%0.02
Death 22% 21% NS
Major bleed 9% 12% NS
DeCousus et al. NEJM 1998; 338:409

Recommendations

DVT Recommendations
Geerts et al. Chest, 2004; 126:338S
DVT, %
PE, %
Level of Risk
Calf Proximal Clinical Fatal Successful Prevention Strategies
Low risk 2 0.4 0.2 <0.01
Minor surgery in patients < 40 yr with no additional risk factors
No specific prophylaxis; early and "aggressive" mobilization
Moderate risk 10–20 2–4 1–2
0.1–0.4
Minor surgery in patients with risk factors LDUH (q12h), LMWH ( 3,400 U daily), GCS, or IPC
High risk 20–40 4–8 2–4
0.4–1.0
Surgery in patients > 60 yr LDUH (q8h), LMWH (> 3,400 U daily), or IPC
Highest risk 40–80 10–20 4–10 0.2–5
Surgery in patients with multiple risk factors, Trauma, Ortho
LMWH (> 3,400 U daily), fondaparinux, oral VKAs (INR, 2–3), or IPC/GCS + LDUH/LMWH

Trauma RecsTrauma patients with at least one risk factor for VTE receive thromboprophylaxis, if possible (Grade 1A).
In the absence of a major contraindication, LMWH prophylaxis starting as soon as it is considered safe to do so (Grade 1A).
Mechanical prophylaxis with IPC be used if LMWH prophylaxis is delayed or if it is currently contraindicated due to active bleeding or a high risk for hemorrhage (Grade 1B).
DUS screening in patients who are at high risk for VTE (eg, SCI, lower extremity or pelvic fracture, major head injury, or an indwelling femoral venous line, suboptimal prophylaxis) (Grade 1C).
No use of IVCFs as primary prophylaxis in trauma patients (Grade 1C).
Continuation of thromboprophylaxis until hospital discharge, including the period of inpatient rehabilitation (Grade 1C+).
Continuing prophylaxis after hospital discharge in patients with major impaired mobility (Grade 2C).

Compliance
Yu. Am J HP, 2007; 64: 69.

Causes for Poor Compliance
Nathens et al. J Trauma. 2007;62:557
Three fold increase in DVTs
after 4 days in TICU.

Summary• DUS
– Clinical suspicion + serial testing• Risk factors
– Trauma and thrombophilia• Treatment
– LMWH superior to UFH– Start early – Cost effective
• Plans – Uptake poor at hospitals

Summary

Thank you.
Thanks to pt. DW for worrying me about this issue every day for a week.

Clinical Probability of PE
Wells, Ann Intern Med 2001
Leg swelling, tenderness 3Pulse > 100 1.5Immobilization, surgery 1.5Prior DVT/PE 1.5Hemoptysis 1Cancer 1No other more likely Dx 3
< 2 = Low probability 2-6 = Moderate > 6 = High