drugs acting on the kidney lectures 1 and 2
TRANSCRIPT
Learning Objectives
Following this lecture, students should be able to:
Recall the range of drugs that act upon the kidney
Identify the major sites of diuretic action in the nephron
Describe in detail the mechanism of action of the loop diuretics
List the clinical uses and main adverse effects of the loop diuretics
Describe in detail the mechanism of action of the thiazide diuretics
List the clinical uses and main adverse effects of the thiazide diuretics
Explain why loop and thiazide diuretics cause hypokalaemia
Describe the mechanisms of action of the potassium sparing diuretics
noting the distinct modes of action of aldosterone antagonists and
blockers of the epithelial sodium channel, ENaC
Describe the clinical uses of the potassium sparing diuretics and their
adverse effects
Recommended ReadingRang and Dale’s Pharmacology (7th. Ed.) Chapter 28
Drugs Acting on the Kidney
Drugs acting on the kidney include
Diuretics are the most commonly used agents that:
increase urine flow, normally by inhibiting the reabsorption of
electrolytes (mainly sodium salts) at various sites in the nephron
Diuretics
Vasopressin (antidiuretic hormone; ADH) receptor agonists and
antagonists
Uricosuric drugs (agents promoting excretion of uric acid into the
urine)
are used to enhance excretion of salt and water in conditions where
an increase in the volume of interstitial fluid (i.e. oedema) causes
tissue swelling
Inhibitors of sodium-glucose co-transporter 2 (SGLT2)
Those used in renal failure
Those that alter the pH of the urine
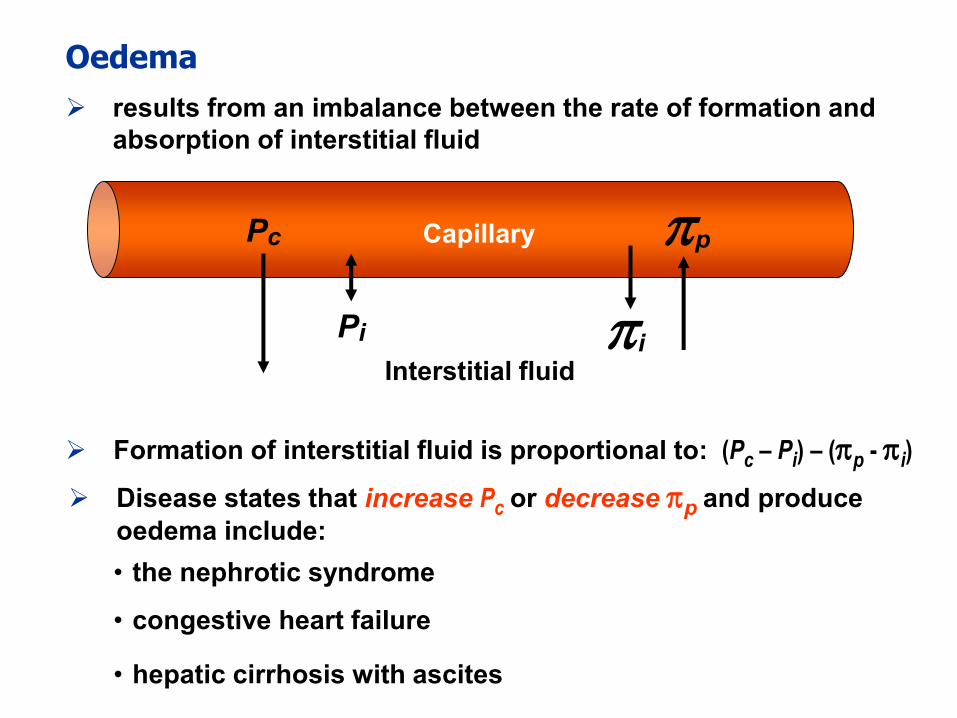
Formation of interstitial fluid is proportional to: (Pc – Pi) – (p - i)
Disease states that increase Pc or decrease p and produce
oedema include:
• the nephrotic syndrome
Oedema
results from an imbalance between the rate of formation and
absorption of interstitial fluid
Pc p
Pi i
Capillary
Interstitial fluid
• hepatic cirrhosis with ascites
• congestive heart failure
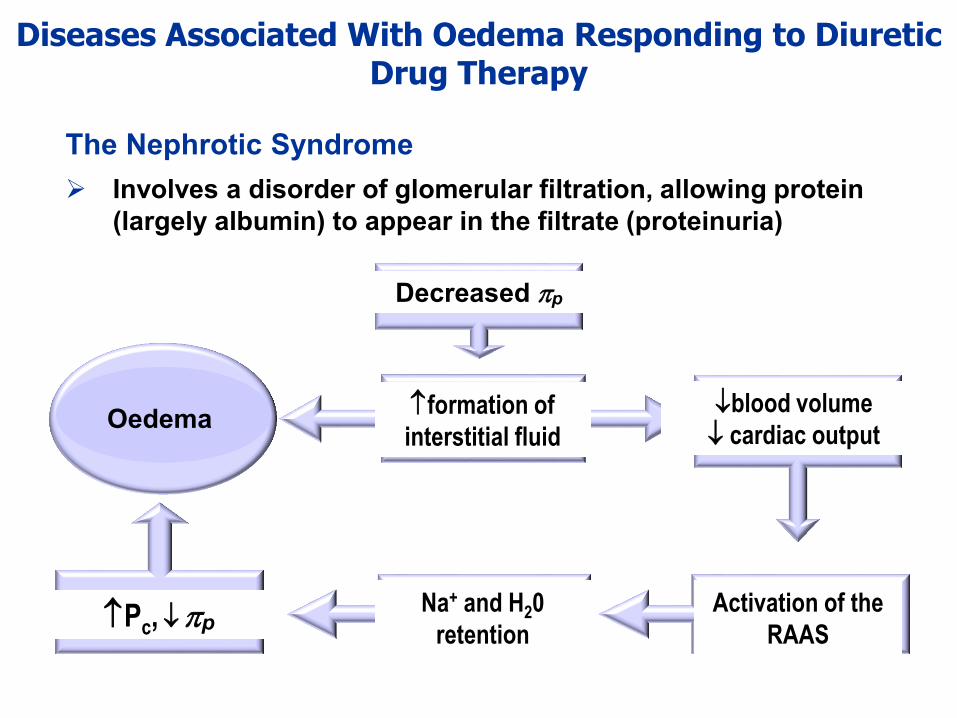
Diseases Associated With Oedema Responding to Diuretic Drug Therapy
The Nephrotic Syndrome
Involves a disorder of glomerular filtration, allowing protein
(largely albumin) to appear in the filtrate (proteinuria)
Decreased p
formation of
interstitial fluid
blood volume
cardiac outputOedema
Activation of the
RAAS
Na+ and H20
retentionPc,p
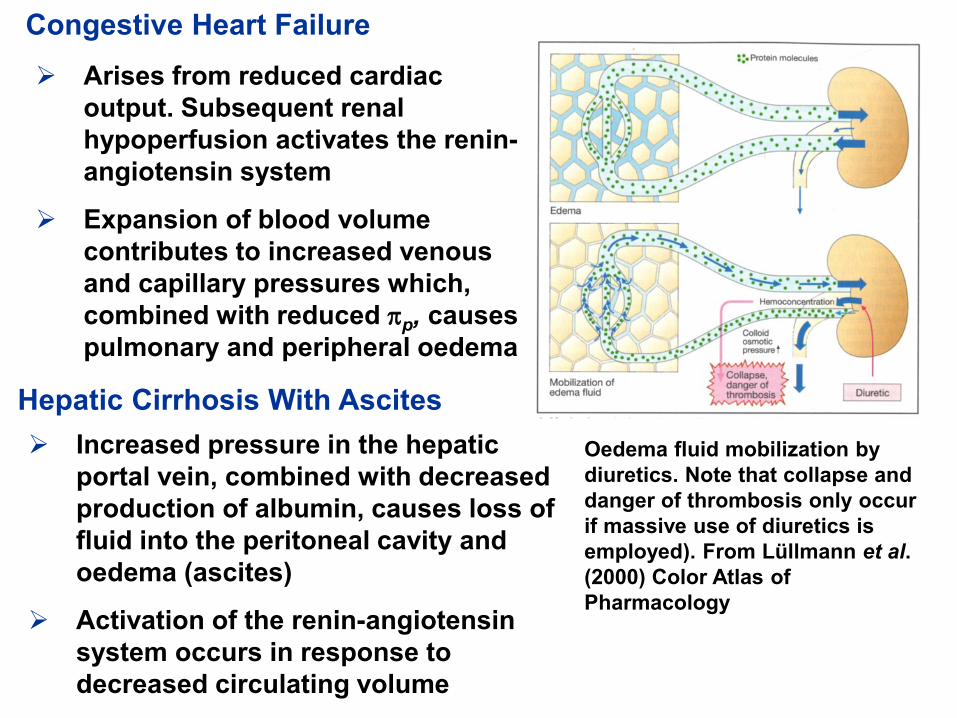
Congestive Heart Failure
Arises from reduced cardiac
output. Subsequent renal
hypoperfusion activates the renin-
angiotensin system
Expansion of blood volume
contributes to increased venous
and capillary pressures which,
combined with reduced p, causes
pulmonary and peripheral oedema
Hepatic Cirrhosis With Ascites
Increased pressure in the hepatic
portal vein, combined with decreased
production of albumin, causes loss of
fluid into the peritoneal cavity and
oedema (ascites)
Activation of the renin-angiotensin
system occurs in response to
decreased circulating volume
Oedema fluid mobilization by
diuretics. Note that collapse and
danger of thrombosis only occur
if massive use of diuretics is
employed). From Lüllmann et al.
(2000) Color Atlas of
Pharmacology
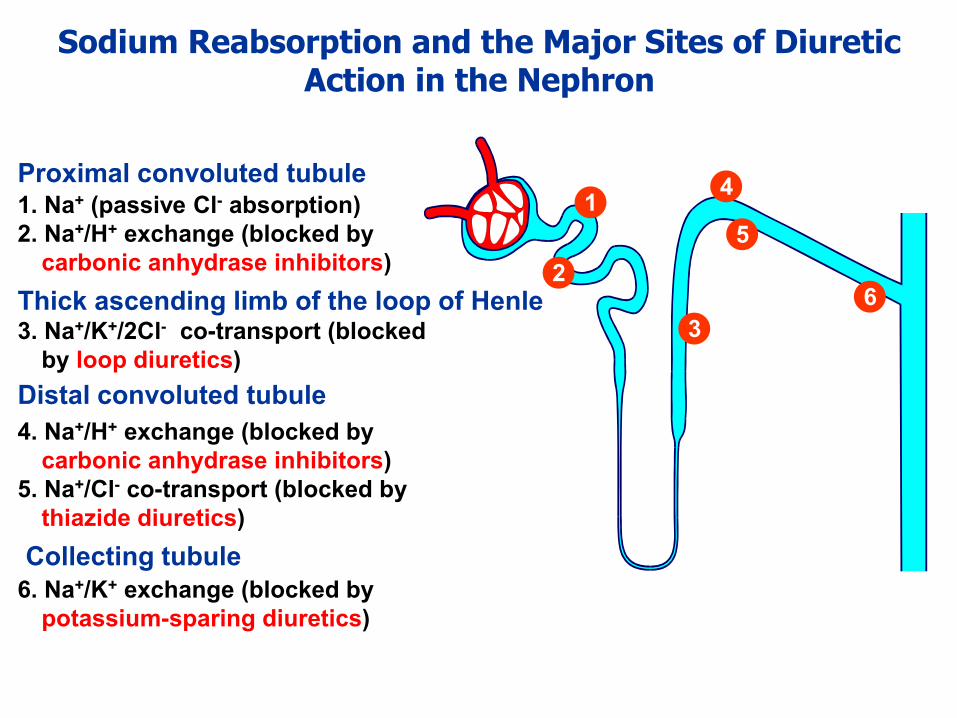
Sodium Reabsorption and the Major Sites of Diuretic Action in the Nephron
Proximal convoluted tubule1. Na+ (passive Cl- absorption)
2. Na+/H+ exchange (blocked by
carbonic anhydrase inhibitors)
Thick ascending limb of the loop of Henle3. Na+/K+/2Cl- co-transport (blocked
by loop diuretics)
Distal convoluted tubule
4. Na+/H+ exchange (blocked by
carbonic anhydrase inhibitors)
5. Na+/Cl- co-transport (blocked by
thiazide diuretics)
Collecting tubule
6. Na+/K+ exchange (blocked by
potassium-sparing diuretics)
1
2
3
4
5
6
Diuretics – General Aspects
A very large proportion of NaCl and H2O that passes into the filtrate
via the glomerulus is reabsorbed – hence even a small inhibition of
reuptake can cause a marked increase in Na+ excretion
The site of action of many diuretics (thiazides, loop agents, potassium
sparing) is the apical membrane of tubular cells hence, if hydrophilic,
they must enter the filtrate to access that site
Entry to the filtrate is by either:
glomerular filtration (for drug not bound to plasma protein)
secretion via transport process in the proximal tubule
two transport systems are important
The organic anion transporters (OATs) – transport acidic drugs (e.g.
thiazides and loop agents)
The organic cation transporters (OCTs) – transport basic drugs (e.g.
triamterene and amiloride)
Secretion results in the concentration of diuretic in the filtrate being higher
than that in blood, contributing to pharmacological selectivity
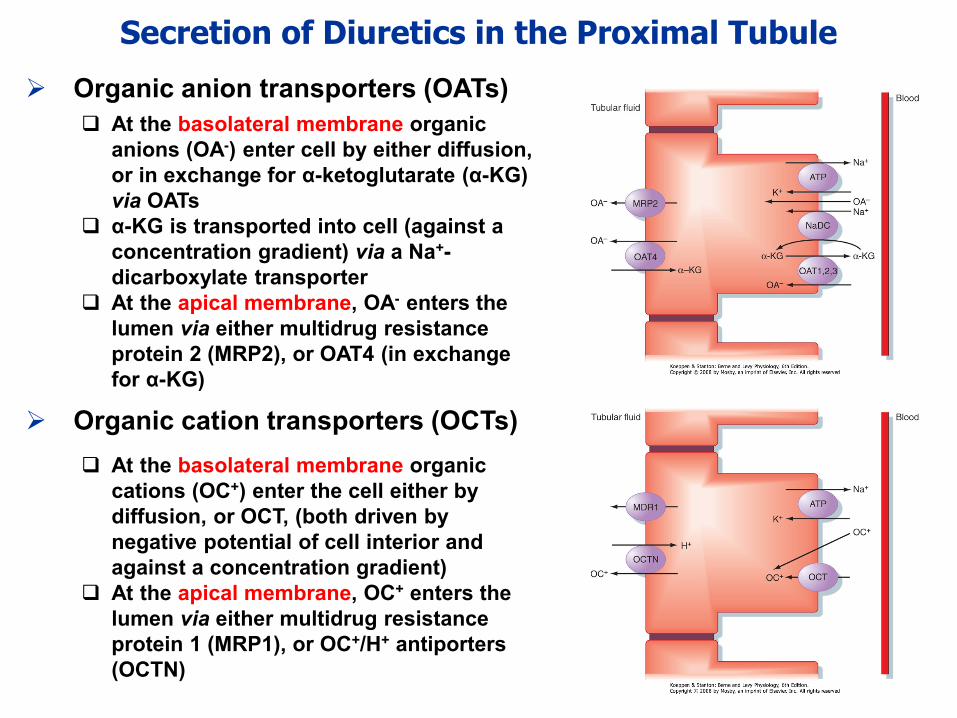
Secretion of Diuretics in the Proximal Tubule
Organic anion transporters (OATs)
At the basolateral membrane organic
anions (OA-) enter cell by either diffusion,
or in exchange for α-ketoglutarate (α-KG)
via OATs
α-KG is transported into cell (against a
concentration gradient) via a Na+-
dicarboxylate transporter
At the apical membrane, OA- enters the
lumen via either multidrug resistance
protein 2 (MRP2), or OAT4 (in exchange
for α-KG)
Organic cation transporters (OCTs)
At the basolateral membrane organic
cations (OC+) enter the cell either by
diffusion, or OCT, (both driven by
negative potential of cell interior and
against a concentration gradient)
At the apical membrane, OC+ enters the
lumen via either multidrug resistance
protein 1 (MRP1), or OC+/H+ antiporters
(OCTN)
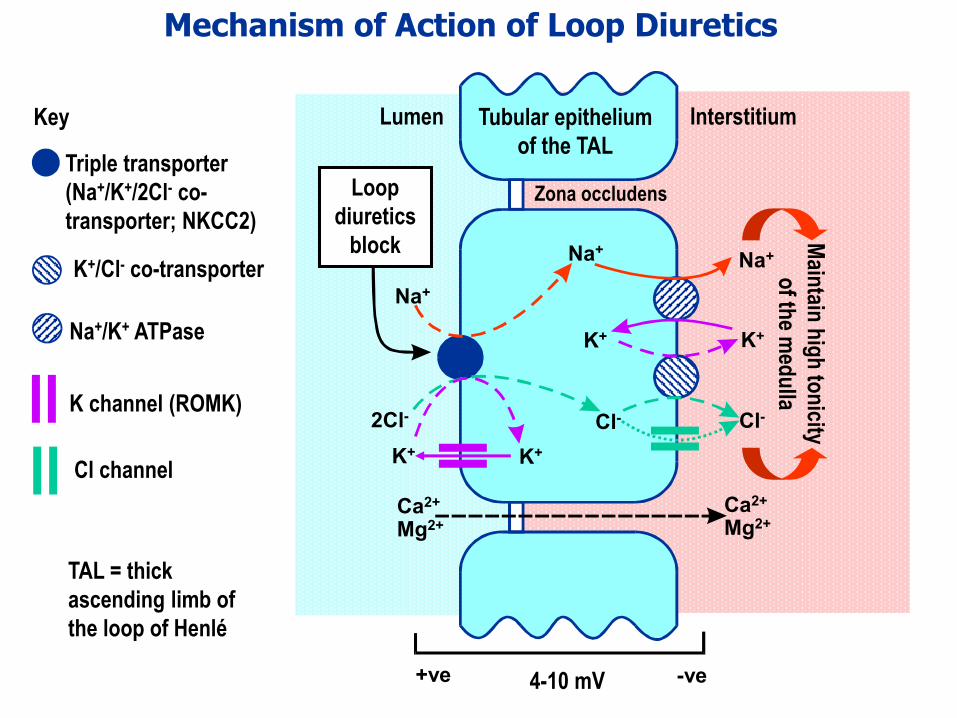
Mechanism of Action of Loop Diuretics
Na+
Na+
Na+
K+K+
K+ K+
Cl-2Cl- Cl-
Zona occludens
+ve -ve4-10 mV
Lumen Interstitium
Mg2+
Ca2+
Mg2+Ca2+
Loop
diuretics
block Main
tain h
igh
ton
icity
of th
e med
ulla
Tubular epithelium
of the TALTriple transporter
(Na+/K+/2Cl- co-
transporter; NKCC2)
K+/Cl- co-transporter
Na+/K+ ATPase
Key
K channel (ROMK)
Cl channel
TAL = thick
ascending limb of
the loop of Henlé
Pharmacodynamics
Inhibit the Na+/K+/2Cl- carrier by binding to the Cl- site and thus:
Loop Diuretics (1)
Principal drugs: Furosemide and Bumetanide
Possess an additional, indirect, venodilator action (before diuresis)
that is beneficial in pulmonary oedema caused by heart failure–possibly results from: 1) increased formation of vasodilating
prostaglandins; 2) decreased responsiveness to angiotensin II and
noradrenaline; 3) opening of K+ channels in resistance vessels
Increase the load of Na+ delivered to distal regions of the nephron
(causing K+ loss)
Decrease the tonicity of the interstitium of the medulla
Prevent dilution of the filtrate in the thick ascending limb
Increase excretion of Ca2+ and Mg2+
Are ‘high ceiling’ agents causing 15-25% of filtered load of Na+ to
be excreted – rapid onset following i.v. administration
Loop Diuretics (2)
To treat hypertension (in patients resistant to other diuretics or anti-
hypertensive drugs - usually in the presence of renal insufficiency)
To reduce acutely elevated calcium levels in the serum
(hypercalcaemia) - note paracellular pathway in the thick
ascending limb of the loop of Henle
To increase urine volume in acute kidney failure
Clinical indications
To reduce salt and water overload associated with:
Acute pulmonary oedema (i.v.) Chronic heart failure
Chronic kidney failure Nephrotic syndrome
Hepatic cirrhosis with ascites
Pharmacokinetics
Well absorbed from the G.I. tract
Strongly bound to plasma protein
Enter nephron by the organic anion transport mechanism
Loop Diuretics (3)
Potassium loss producing low serum potassium levels
(hypokalaemia) – corrected by the concomitant use of potassium
sparing diuretics or potassium supplements
(note increases toxicity of digoxin and Class III antidysrhythmic drugs)
Increased plasma uric acid (hyperuricaemia) – partially
explained by competition between uric acid and loop agents
for the organic acid secretory mechanism in the proximal
tubule
Depletion of calcium and magnesium (paracellular pathway)
Decreased volume of circulating fluid (hypovolaemia) and
hypotension (particularly in the elderly)
Shift in acid-base towards alkaline side (metabolic alkalosis) –
caused by increased H+ secretion from intercalated cells in
collecting tubule
Adverse effects
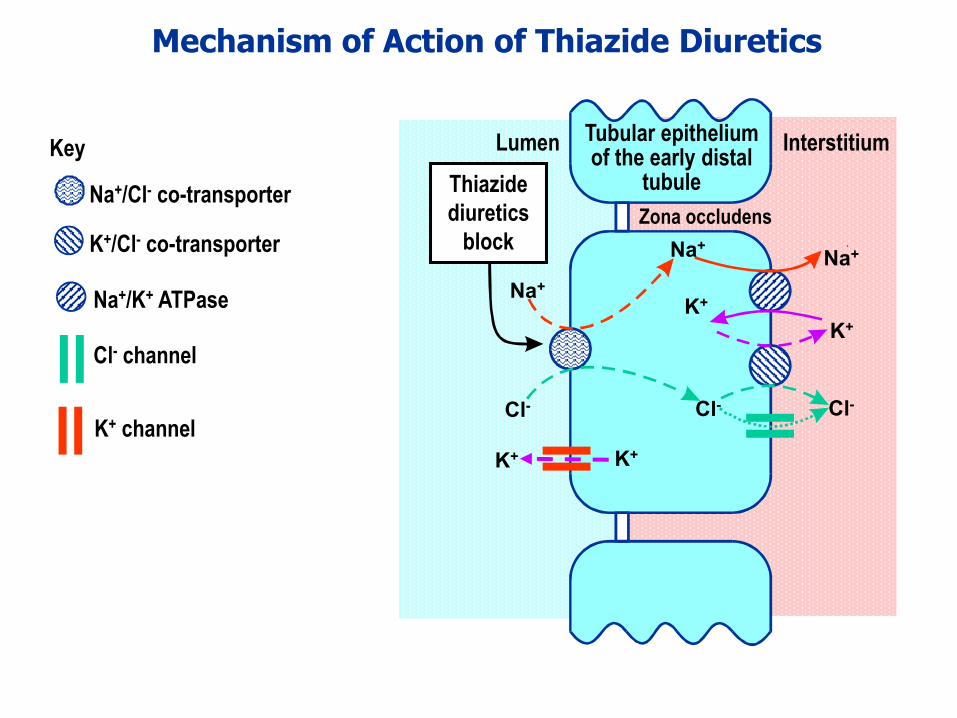
Mechanism of Action of Thiazide Diuretics
Na+
Na+
Na++
K+
K+
Cl-Cl- Cl-
Zona occludens
Lumen Interstitium
Thiazide
diuretics
block
Tubular epithelium of the early distal
tubuleNa+/Cl- co-transporter
K+/Cl- co-transporter
Na+/K+ ATPase
Key
Cl- channel
K+ channel
K+K+
Pharmacodynamics
Inhibit the Na+/Cl- carrier by binding to the Cl- site and thus:
Cause up to 5% of Na+ to be excreted, producing a modest
diuresis
Possess an additional, indirect, vasodilator action (mechanism
uncertain) that contributes to their effectiveness in the treatment
of hypertension (where they are used in combination with other
antihypertensive agents)
Thiazide Diuretics (1)
Principal drugs: Bendroflumethiazide (bendrofluazide) and
hydrochlorothiazide
Prevent the dilution of filtrate in the early distal tubule
Increase the load of Na+ delivered to the collecting tubule (causing K+
loss)
Increase reabsorption of Ca2+ (cf. loop agents) (mechanism debatable)
Thiazide Diuretics (2)
Nephrogenic diabetes insipidus (caused by diminished
vasopressin responsiveness of the collecting ducts (paradoxically,
thiazides decrease the volume of urine – mechanism poorly
understood)
Renal stone disease (nephrolithiasis). Reduced urinary excretion
of Ca2+ discourages Ca2+ stone formation (mainly aggregates of
particles of calcium oxalate)
Severe resistant oedema (with a loop agent)
…and additionally in:
Clinical indications
Widely used in:
Mild heart failure Hypertension
Pharmacokinetics
Well absorbed from the G.I. tract
Enter nephron by the organic anion transport mechanism
(proximal tubule)
Thiazide Diuretics (3)
Adverse effects
Male sexual dysfunction
Hyperuricaemia – mechanism as for loop agents – may
precipitate gout
Metabolic alkalosis
Depletion of magnesium (not calcium)
Hypovolaemia and hypotension (particularly in the elderly)
Hypokalaemia, particularly likely and corrected as for loop
diuretics
Impaired glucose tolerance
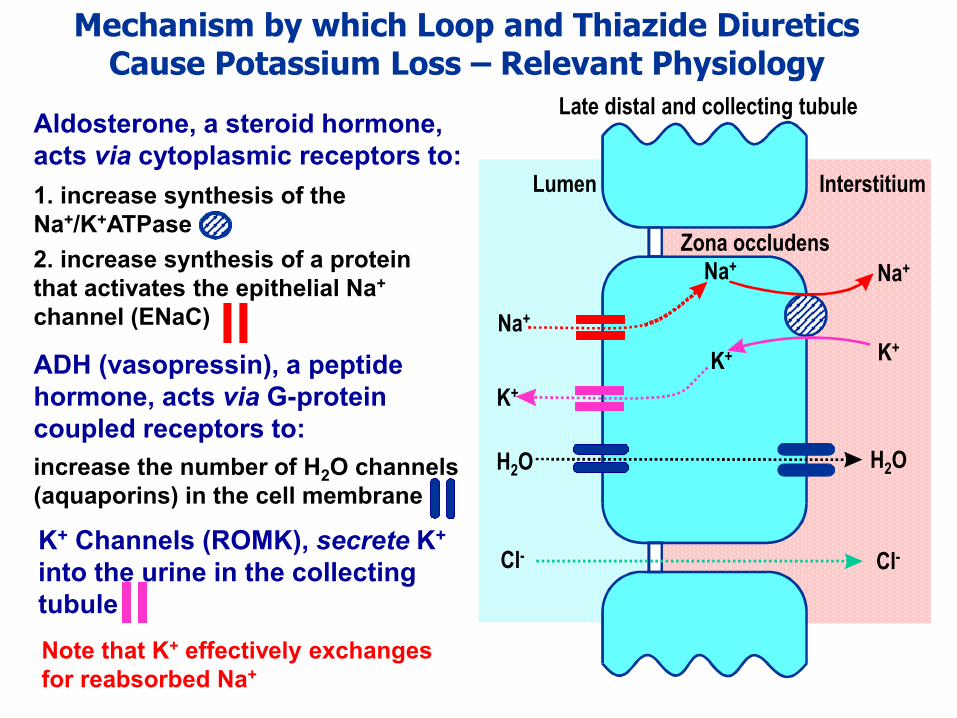
Mechanism by which Loop and Thiazide Diuretics Cause Potassium Loss – Relevant Physiology
Aldosterone, a steroid hormone,
acts via cytoplasmic receptors to:
1. increase synthesis of the
Na+/K+ATPase
2. increase synthesis of a protein
that activates the epithelial Na+
channel (ENaC)
increase the number of H2O channels
(aquaporins) in the cell membrane
ADH (vasopressin), a peptide
hormone, acts via G-protein
coupled receptors to:
Na+ Na+
K+K+
Zona occludens
Lumen Interstitium
Late distal and collecting tubule
H2O
Cl- Cl-
H2O
Na+
K+
K+ Channels (ROMK), secrete K+
into the urine in the collecting
tubule
Note that K+ effectively exchanges
for reabsorbed Na+
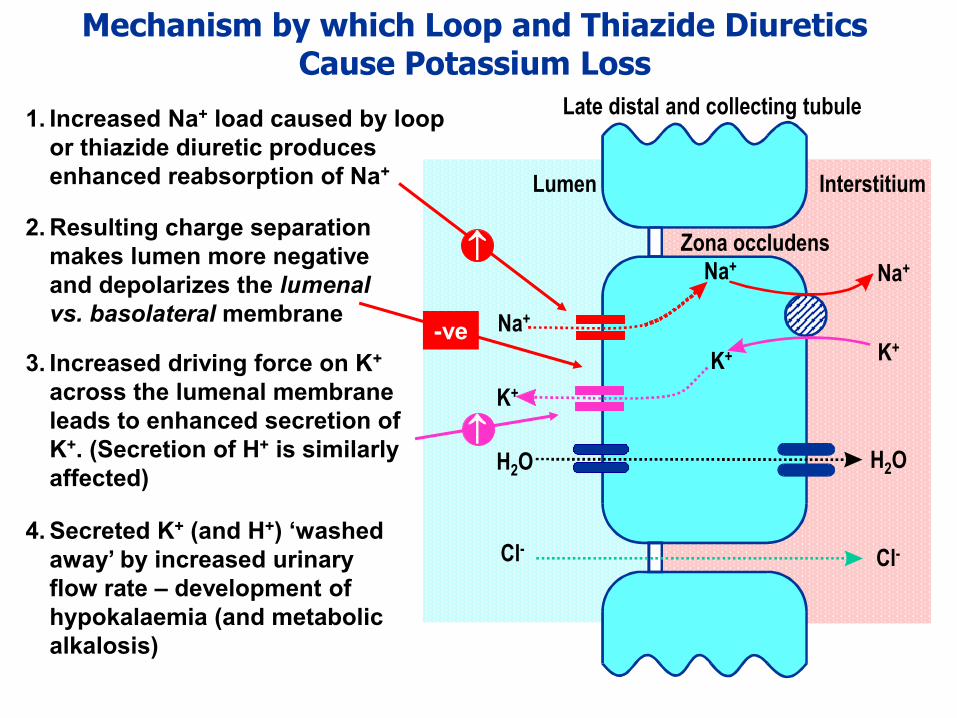
Mechanism by which Loop and Thiazide Diuretics Cause Potassium Loss
Na+ Na+
K+K+
Zona occludens
Lumen Interstitium
Late distal and collecting tubule
H2O
Cl- Cl-
H2O
Na+
K+
1. Increased Na+ load caused by loop
or thiazide diuretic produces
enhanced reabsorption of Na+
2. Resulting charge separation
makes lumen more negative
and depolarizes the lumenal
vs. basolateral membrane-ve
3. Increased driving force on K+
across the lumenal membrane
leads to enhanced secretion of
K+. (Secretion of H+ is similarly
affected)
4. Secreted K+ (and H+) ‘washed
away’ by increased urinary
flow rate – development of
hypokalaemia (and metabolic
alkalosis)
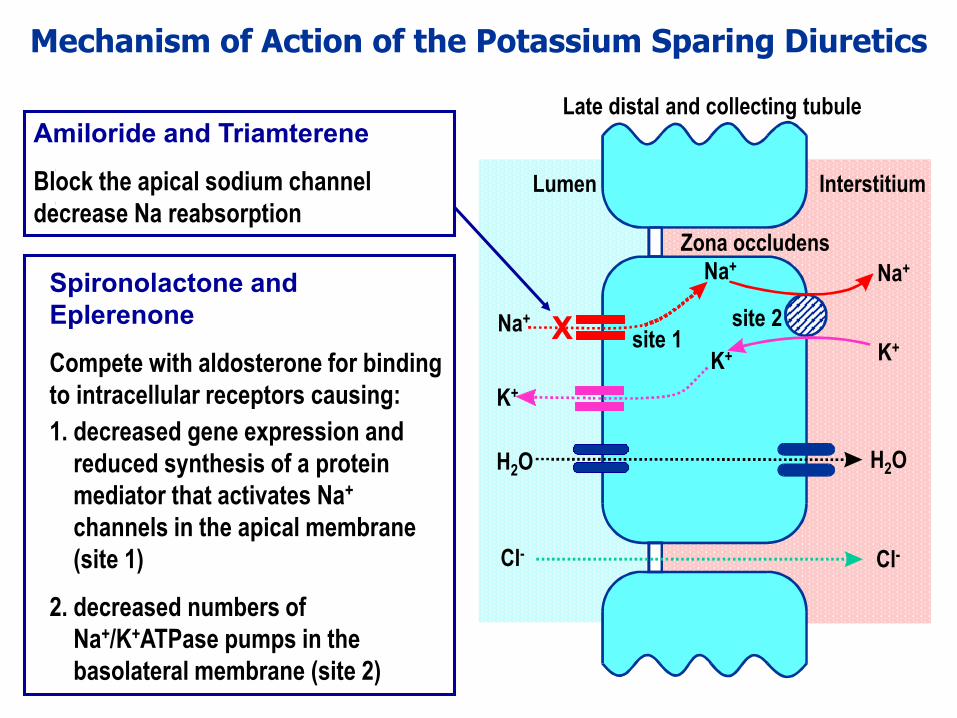
Mechanism of Action of the Potassium Sparing Diuretics
Spironolactone and
Eplerenone
Compete with aldosterone for binding
to intracellular receptors causing:
1. decreased gene expression and
reduced synthesis of a protein
mediator that activates Na+
channels in the apical membrane
(site 1)
2. decreased numbers of
Na+/K+ATPase pumps in the
basolateral membrane (site 2)
Amiloride and Triamterene
Block the apical sodium channel
decrease Na reabsorption
Na+ Na+
K+K+
Zona occludens
Lumen Interstitium
Late distal and collecting tubule
H2O
Cl- Cl-
H2O
Na+
K+
X site 1site 2
Potassium Sparing Diuretics
Spironolactone and Eplerenone
Have limited diuretic action (modulated by aldosterone levels)
Competitively antagonise the action of aldosterone at
cytoplasmic aldosterone receptors, gain access to cytoplasm via
the basolateral membrane
Increase and decrease the excretion of Na+ and K+ respectively
Are well absorbed from the G.I. tract and in the case of
spironolactone rapidly metabolised to canrenone (which
accounts for most of the action of the drug)
Amiloride and Triamterene
Block lumenal sodium channels in the collecting tubules. Effect
on ion fluxes are similar to those of spironolactone
Enter the nephron via the organic cation transport system in the
proximal tubule
Triamterene is well absorbed from the G.I tract, absorption of
amiloride is poor
Clinical indications
The major use of potassium sparing diuretics is in conjunction
with other agents that cause potassium loss. Given alone, they
cause hyperkalaemia
Aldosterone antagonists are used in the treatment of:
Heart failure
Primary hyperaldosteronism (Conn’s syndrome)
Resistant essential hypertension
Secondary hyperaldosteronism (due to hepatic cirrhosis with
ascites)
Thiazide and loop diuretics activate the renin-angiotensin-
aldosterone system (in response to reduced blood pressure)
Aldosterone antagonists potentiate the actions of thiazide and
loop agents by blocking the effect of aldosterone