dr viviana elliott consultant physician acute medicine pulmonary embolism
TRANSCRIPT

Dr Viviana Elliott
Consultant Physician
Acute Medicine
Pulmonary Embolism

Aim
• Provide a practical approach for the diagnosis and management of pulmonary embolism
Objectives
• To be able to understand pathophysiology
• To be able to understand importance of early diagnosis
• To be able to recognise signs and symptoms
• To be able to request investigations appropriately
• To be able to treat pulmonary embolism
• To be able to investigate and treat PE in special situations ( Massive PE, pregnancy and cancer)

Pathophysiology
Venous thrombi originatepredominantly in venous valve pockets and at other sites of
presumed venous stasis
Virchow’s Triad

Why is it so important to think PE?

Case 1
• Female 40 years old
• Chest tightness and shortness of breath for two days
• Past Medical History: Crohn’s disease
• Presents to ED RR 35x’, BP 80/40 mmHg, Sat: 80%
• Transferred to resus with suspected PE
• Thrombolised
• Arrested and died within 20’ of arrival
• Post mortem: massive PE

PE is an acute medical emergency!

Incidence of Pulmonary embolism• 60-70 cases/100.000
• 50% develop PE while in hospital or in long term care
• 25% idiopathic cases
• 25% have recognised risk factors

Most VTE affect acutely ill patients

Risk factors for VTE
• Acquired
• Hereditary

Reduced mobility
• Hospitals stay !!!!!!• Fractures (Hip-Knee- Ankle)• Major surgery • Trauma • Spinal cord injury• Immobilizer or cast

Acute medical conditions
Hospital admission for acute illnessPregnancy Postpartum periodPolycythemia veraOral contraceptives Hormone-replacement Cancer Chemotherapy Advanced age Obesity Central venous catheterization

Hereditary Clue in the history!!!
Factor V LeidenAntithrombin deficiencyProtein C deficiencyProtein S deficiencyActivated protein C resistance without factor V LeidenProthrombin gene mutationDysfibrinogenemiaPlasminogen deficiency

Which are the most common symptoms?

PIOPED- symptoms and signs
Symptoms Dyspnoea (SOB) 73%
Pleuritic pain 66%
Cough 37%
Haemoptisis 13%
Signs Tachypnoea70%
Crackles 51%
Tachycardia 30%
Syndromes Pain & haemoptisis 65%
CVS collapse 8%


Which are the most common radiological signs?

CXR findings in PE• Normal
• Laminar atelectasia
• Wedge infarct
• Pleural effusion
• Infiltrates
• Prominent pulmonary arteries (Fleishner sign)
• Oligemia ( Westermark’s sign)
• Pleural based opacity (Hampton’s hump sign)





Case• Female 82
• Admitted to ED
• Carers rung the ambulance as patient was short of breath and collapsed at home
• Ambulance crew
HR: 115 x’ RR: 32 x’ Sat: 82% on air
• PMH:
Discharged from hospital the week before admission with haemorrhagic cystitis
Recurrent UTIs :E. Coli ESBL (Extended Spectrum Beta Lactamase )




USS BOTH LEGS AND ABDOMEN• Right leg:
occlusive DVT is seen in right femoral vein extending to adductor canal region. The right popliteal vein was patent. Left leg: Short segment of non-occlusive DVT in the common femoral vein. The rest of the SFV and popliteal vein remain patent. US Pelvis (Transabdominal) : Urinary bladder empty with catheter in situ. No pelvic free fluid. uterus and ovaries not seen. No pelvic masses.

How many patients with PE have a DVT?
How many patients with DVT will have a PE?

More informatio:
• 79% of patients presenting with PE have DVT in their legs!!!
• 50% of patients with DVT will have a PE

Symptoms and signs are nonspecific the clue is in the history!!!!!

What test would you request initially?

Preliminary Testing• Blood tests:
Mildly raised WBC and CRP
• ECG:
tachycardia
atrial fibrilation
manifestations of acute cor pulmonale
S1, Q3, T3 pattern,
right bundle-branch block
P-wave pulmonale
right axis deviation

Patient to ED with suspected PE
History + Risk factors + CxR and ECG
Potential PE identified &Well’s Score
Low probability(Well’s Score <4) High probability
abnormal X ray pre-existing cardio respiratory disease
High probabilityNormal chest X ray
D Dimer
If –ve, discharge
CTPA undertakenwithin 24 hours
UHCW:Q/VQ scan (weekdays)
CTPA (weekends)
Management plan

How would you treat a suspected PE?

Anticoagulation cascade
Enoxaparine

Treatment• LMWH 1.5 mg/kg
• Warfarin until INR between 2-3
• When INR 2-3 continue LMWH 5 more days– INR is often deceptive in the first days
factor VII has a half-life of 6 to 8 hours, the initial increase in
INR following the start of warfarin therapy reflects factor
VII depletion rather than attainment of true systemic anticoagulation.
- Factor II and X depletion takes 4 to 5 days
• Duration 6 months at UHCW
( 3 months same mortality less bleeding risk)

Special situations
• Massive PE
• Pregnancy and PE
• Cancer and PE

Massive PE• High suspicious
50% EMD (electromechanical dissociation)
Asystolic
very few survive whatever you do
• Diagnosis
ECHODiagnostic abnormal in 80%dilated RV & PAregional RV wall abnormalityintracardiac clot
CTPA (if stable)

Treatment for massive PE Thrombolysis
• What to give?
• 50 mg bolus of Alteplase
• If cardiac arrest CPR 60’
• Alternative to thrombolisis:
Embolectomy / right heart catheter clot fragmentation
can be considered if experience and facilities available

PE and pregnancy: How would you investigate?

Suspected PE in pregnancy
• History with risk factors
• D Dimer? : NO THANK YOU!!!
• ECG
• Further investigation: gold standard USS both legs
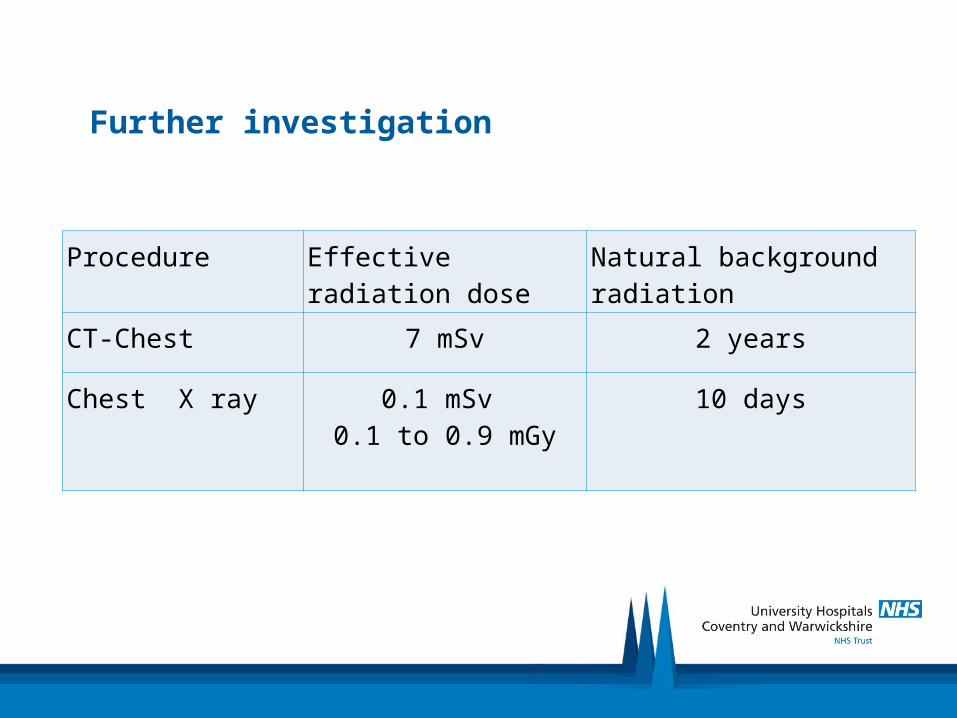
Further investigation
Procedure Effective radiation dose Natural background radiation
CT-Chest 7 mSv 2 years
Chest X ray 0.1 mSv 0.1 to 0.9 mGy
10 days

Pregnancy and PEFetal Radiation
V/Q 0.11-0.22 mGy (milligray)
CTPA 0.01-0.06 mGy
Incidence of malignancy 1:16,000 per mGy
IV iodinated contrast : neonatal hypotyroidism
Mother
CTPA 35 mGy per breast
½ perfusion V/Q 0.25 mGy per breast
Life time risk of breast cancer reported with one dose of 10 mGy

PE in pregnancy- imaging at UHCW
• CxR to exclude other causes
• Half dose perfusion V/Q
• CTPA only in cardio respiratory disease or abnormal CxR

PE and pregnancy: How would you treat?

Treatment of PE in pregnancy
• Treatment:
Enoxaparine 1 mg BD
Warfarine is teratogenic
UFH should be given as delivery approaches
? Stop 4-6 hs pre – delivery
Continue anticoagulation 6 weeks post delivery or 3 months post event

Cancer Screening in PE
• 7 -12 % of idiopatic VTE presents with cancer in next 6 – 12 months
• Should we hunt for it?
• Most will be picked up by:
clinical history examination CxR
• Further tests are not warranted
1 year survival of occult cancer is 12 %
Most have metastasis at the diagnosis
VTE in cancer patients is poor prognostic factor
• Treatment LMWH

Messages to take home• PE is a medical emergency
• High level of suspicion
• Think PE in all patients recently discharged from hospital
• Request D Dimer only in low probability PEs
• Remember to continue Enoxaparine 5 more days after the INR is in range (2-3)
• Thrombophylia screen after the treatment has been completed
• Best treatment: PREVENTION!!!
Has the patient been assessed?
Has prophylaxis been prescribed?


References• British Thoracic Society guidelines for the
management of suspected acute pulmonary embolism. Thorax 2003;58:470–484
• Victor F. Tapson, M.D Acute Pulmonary Embolism NEJM 358;10, 2008
• Why shouldn’t we use Warfarin alone to treat acute venous thrombosis? Cleveland Clinic Journal of medicine, volume 69, number 7 July 2002
• Investigating suspected pulmonary embolism in pregnancy. BMJ 2007:334:418-9