dr. john has gone: assessing health professionals’ contribution to remote rural community...
TRANSCRIPT
Social Science & Medicine 57 (2003) 673–686
Dr. John has gone: assessing health professionals’ contributionto remote rural community sustainability in the UK
Jane Farmera,*, William Lauderb, Helen Richardsc, Siobhan Sharkeyd
aDepartment of Management, University of Aberdeen, Edward Wright Building, Dunbar Street, Aberdeen AB24 3QY, UKbFaculty of Arts Health & Sciences, School of Nursing & Health Studies, Central Queensland University, Rockhampton,
Queensland 4702, Australiac Highlands & Islands Health Research Institute, University of Aberdeen, The Green House, Beechwood Business Park North,
Inverness IV2 3ED, UKd Department of Nursing and Midwifery, University of Stirling, Highland Campus, Old Perth Road, Inverness IV2 3FG, UK
Abstract
Due mainly to increasing difficulties in recruiting and retaining health professionals to work in remote and peripheral
areas of Scotland, there is discussion of the need to implement new models of primary health care provision. However,
innovative service models may imply a reduction in the number of health professionals who live and work in remote
communities. Currently decisions about remodelling service provision are being taken by National Health Service
stakeholders, apparently with little consideration of the wider social and economic impacts of change. This paper aims
to argue that health professionals contribute to the fabric of rural life in a number of ways and that decisions about
health service redesign need to take this into account. As well as fulfilling a wide health and social care role for patients,
the authors seek to show that health professionals are important to the social sustainability of rural communities as, due
to their unique position, they are often at the heart of networks within and between communities. The wider economic
contribution of health services in remote communities is important, but often underplayed. The authors propose that
theories of capital, principally the concept of social capital, could help in investigating the wider contribution of health
professionals to their local communities. Ultimately, it is proposed that health services, as embodied in nurses, doctors
and others, could be highly important to the ongoing livelihood and social infrastructure of fragile remote communities.
Since this area is poorly understood, there is a need for prospective primary research and evaluation of service redesign
initiatives.
r 2003 Elsevier Science Ltd. All rights reserved.
Keywords: Rural healthcare; Service redesign; Professional roles; Community sustainability; Social capital; Scotland, UK
y the task of achieving sustainability—economic,
environmental and social—is a complex one, de-
manding direct attention to retaining and weaving in
the strands that make up the fabric of social lifey
(Reed, 1999)
Introduction
Rural areas are suddenly on the UK policy agenda
(Department of Environment, Transport & the Regions,
2000). The agricultural industry has been in decline for
years and tourism is a fragile replacement. Many rural
areas have been experiencing the curious joint effects of
out-migration of young people and in-migration of older
retired people which has led to an ageing population
(Philips, 1999). Accessible rural areas have been
colonised by commuters and the decline of local
services—the village shop, post office, bank—are
ARTICLE IN PRESS
*Corresponding author. Tel.: +44-1224-273237; fax: +44-
1224-273843.
E-mail address: [email protected] (J. Farmer).
0277-9536/03/$ - see front matter r 2003 Elsevier Science Ltd. All rights reserved.
PII: S 0 2 7 7 - 9 5 3 6 ( 0 2 ) 0 0 4 1 0 - 0

hastened. In 2001, the effects of UK rural decline also
hit urbanites as, for some considerable time, the
countryside (their idyllic green and leafy heritage park
(Pahl, 1970)) closed to public access due to foot and
mouth disease.
In Scotland, the effects of these economic and
demographic changes have prompted policymakers to
make:
y a commitment to economic, social and environ-
mental development of y rural communities—even
the most remote (Scottish Executive Rural Affairs
Department, 2000).
A parallel interest in remote and rural health care has
emerged, with policymakers’ attention tracing back to a
key Scottish health services review in 1998 (The Scottish
Office Department of Health, 1998). This confirmed the
views of academics that there was a dearth of remote
and rural health care research in the UK (Higgs, 1999).
Remote and rural health care research is now develop-
ing, particularly in relation to health service concerns
about a crisis in recruitment and retention of health
professionals to more remote places (Cox, 1997; Remote
and Rural Areas Resources Initiative (RARARI) Solu-
tions Group, 2002).1
Due mainly to the manpower crisis, though partly to
the availability of new technologies and desire to
rationalise costs, new models of providing primary
health care services are being considered, some targeted
specifically at remote rural areas. These include: branch
surgeries; mobile clinics; peripatetic teams working from
a central hub; family health nurses (Proctor, 2000) and
nurse practitioners (who would take on some of the roles
of general practitioners (GPs)); enhancing the role of
paramedics; training local people for a first responder
role; NHS24 telephone advice line; telemedicine and
telehealth; and health ‘booths’ providing information
and an advice link to external health professionals
(Scottish National Rural Partnership, 2000; Deaville,
2001; RARARI, 2002).
These ‘solutions’ will sometimes mean radical change
in the provision of primary health care services to
remote or peripheral communities. They may imply
some loss of locally resident health professionals.
Further, given the interconnected nature of life in such
places, the ripples of decisions about service redesign
may have wider and unpredictable effects on social
stability. Evidence points to the importance of secure
infrastructure in resilient communities (Reimer, 2000).
Health care provision is often included among a list of
services noted as being fundamental to community life
(Cloke, Milbourne, & Thomas, 1994; Hope, Anderson,
& Sawyer, 2000), although there is still a lack of evidence
regarding what people in different areas consider to be
an ‘acceptable level’ of local service provision. Acces-
sible health services are certainly seen as crucial by many
local people as highlighted by recent action of commu-
nities in the Scottish Highlands mobilised by loss of GP
and consultant surgeon services (see, for example:
Helmsdale & District GP Action Group, 2001). Rural
areas have traditionally been seen as bastions of
‘holistic’, patient-oriented continuing care and studies
have shown the adverse effects on utilisation of services
(Haynes & Bentham, 1982; Jones et al., 1998), screening
uptake (Bentham, Hinton, Haynes, Lovett, & Bestwick,
1995), health outcomes (Launoy, Coutour, Gignoux,
Pottier, & Dugleux, 1992; Jones & Bentham, 1995, 1997;
Jones, Bentham, & Horwell, 1999; Campbell et al., 2000)
and rural patients’ health and quality of life (Baird,
Donnelly, Miscampbell, & Wemyss, 2000) of having to
travel some distance to access health services. However,
perhaps rural patients also sense that more than
accessible health services would be lost to their commu-
nity should some of the new models of service provision
be implemented. The presence of many professionals
(clergy, police, teachers, local government) living and
working in remote communities has already been eroded
(Boyle & Halfacree, 1998). The further potential loss of
health professionals, leads one to ask—can service
infrastructure continue to decline without heavy costs
to community wellbeing?
Of course, change is not necessarily wrong. Commu-
nities and service provision should not be in stasis, but
there are important issues at stake. Evidence to inform
decision-making about rural health service redesign is
essential. This paper highlights the need to know more
about the contribution of health professionals to the
sustainability of remote rural communities. We propose
that health services, embodied in GPs, nurses and allied
health staff, are part of the important underpinning for
community and not simply because of their direct
(curative, preventive and palliative care) contributions
to patient health. Due to their role and status in rural
communities, health professionals are often deeply
embedded in the social networks that make up the
‘fabric’ of rural life. The existence of dense social
networks is said to build social capital, a concept
currently popular among policymakers and social
scientists in helping to explain communities’ ability to
adapt to change (Putnam, 1993a). We briefly consider
how theories of capital might provide a useful frame-
work for examining the contribution of health
professional to remote communities. This paper brings
together evidence from existing literature and seeks to
ARTICLE IN PRESS
1The crisis has arisen for different and complex reasons,
including: general lack of medical and nursing staff, increased
specialisation of clinical workforce, feminisation of medical
model of working, comparison with perceived urban ‘9 to 5’,
poor mobility for career moves out of remote/rural work.
J. Farmer et al. / Social Science & Medicine 57 (2003) 673–686674

make a case for research on the wider role of
health professionals in remote communities. There is
little evaluation of the social impacts of different
models of health service provision. We argue there is a
need to generate knowledge before personnel are lost or
replaced by alternatives and before change is wrought
that might affect the viability of some remote commu-
nities.
Remote and peripheral communities
The diversity and fluidity of rural areas is widely
accepted (Halfacree, 1993). While a multitude of
definitions and typologies of rurality exist (Hoggart,
Buller, & Black, 1995), it is probably impossible to
identify a definition that encompasses the many facets
relevant to primary care across the UK (Farmer,
Iversen, & Baird, 2001) and, indeed, researchers have
been advised to use a definition that best suits their area
of enquiry (Rousseau, 1995). Therefore, this paper does
not tie itself to a quantitative or factorial characterisa-
tion, but instead broadly characterises the types of
remote or peripheral locations envisaged.
Research on migration in several countries has shown
that accessible and attractive rural areas have actually
experienced a renaissance in population growth in recent
years (Boyle & Halfacree, 1998). This has been variously
attributed to greater car ownership, willingness to travel
over longer distances to work and failure to develop
attractive inner city living environments (Hugo &
Smailes, 1985; University of Aberdeen & University of
Cardiff, 2001). Many rural areas adjacent to towns and
cities have thus experienced ‘rurbanisation’ effects
(European Society for Rural Sociology, 2001) which
have changed the nature of communities. Change tends
to be characterised by mutually reinforcing effects;
chiefly, travel over longer distances to access products
and services and decline in local amenities (Joseph &
Chalmers, 1995). Service decline impacts most on
indigenous, poorer and elderly people as it is experi-
enced as a loss (White, Guy, & Higgs, 1997). The result,
reported by long-standing rural residents, is deteriorat-
ing community cohesion and identity.
While sharing these wider rural problems of local
service decline, the types of areas envisaged in this paper
are yet more challenged as they are characterised by
relatively greater inaccessibility to urban centres and
sparser infrastructure. These are the more remote areas
of Scotland, including the Highlands and Islands,
Argyll, Dumfriesshire and Galloway which contain
areas of high peripherality, lack transport and commu-
nications infrastructure and do not readily attract
medical or nursing staff. They generally have few
economic opportunities and are highly dependent on
service industry employment. These are areas:
y at the edge of a communication systemyaway
from the core or controlling centre of the economyy
(Goodall, 1987).
A study considering health care for UK island
communities noted that remote islands, in particular,
experience a ‘penalty’ in service provision (Gould &
Moon, 2000). This occurs through multiple effects:
having to provide a certain standard of service to meet
statutory and professional requirements although popu-
lation numbers may be low; the need to cater for
fluctuating population of temporary residents; high
proportions of elderly patients; costs of transporting
goods; and the need to pay incentives to recruit and
retain health professionals.
The Scottish Highlands and Islands area extends over
39; 050 km2 and is described as one of the last unspoilt
areas of Europe, a fifth of the land being classed as
National Scenic Area and almost all of it as Less-
Favoured Area for agriculture (Highlands & Islands
Enterprise, 2001).
The area is one of most sparsely populated in the
European Union (EU), with a population density of 9.5
people per square kilometre compared with Scottish
average of 65.5 and EU average of 116 people per square
kilometre in 1998. This places the region on a par with
northern parts of Finland and Sweden. Thirty per cent
of the population live on more than 90 inhabited islands
including those forming the Orkney and Shetlands
Islands to the north and the Inner and Outer Hebrides
(Western Isles) to the west (Highlands & Islands
Enterprise, 2001).
While more accessible areas within the Highlands are
flourishing, the population of island and remote areas is
declining and ageing. The population of the Western
Isles has fallen by five per cent since 1991 (Highlands &
Islands Enterprise, 2001).
Average gross weekly earnings for males and females
in 1999 were lower in the Highlands and Islands
compared with a Scottish average (male: d377:40
(Highlands and Islands) d406:00 (Scotland); female:
d276:50 (Highlands and Islands) d297:70 (Scotland)).
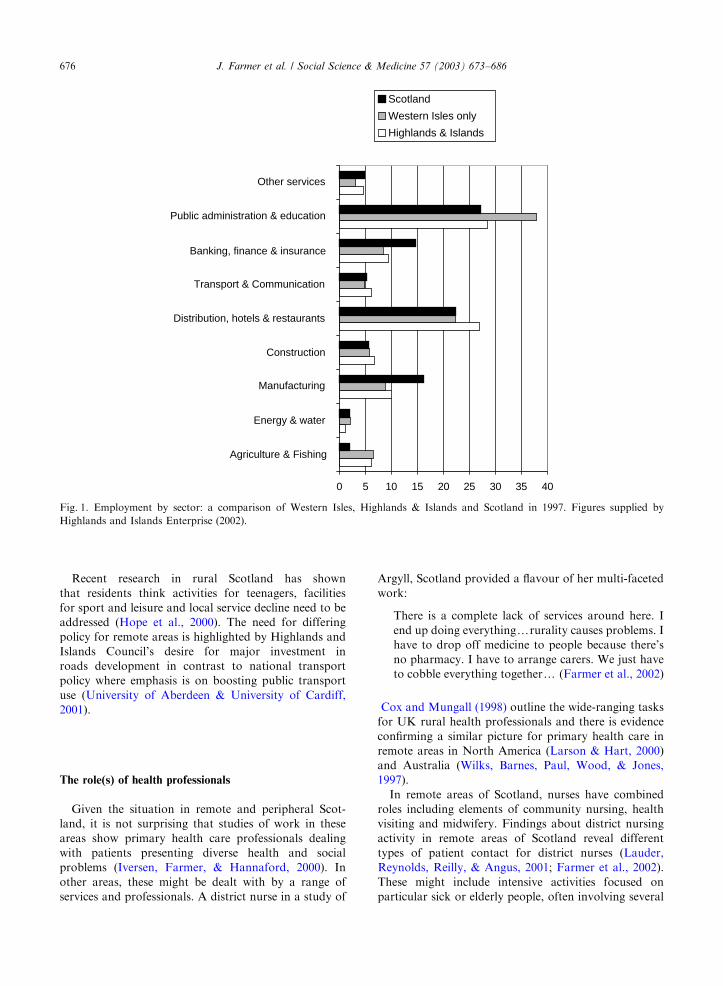
Highest employment is within service sector jobs (as
shown in Fig. 1). Employment in public administration,
education and health accounted for 39% of jobs on the
Western Isles in 1997. Women occupied 74.9% of these
jobs, many working part-time. There are high rates of
long-term unemployment in island and remote areas,
particularly among older age groups. The cost of living
is higher than in more accessible parts of Scotland, with
average prices for a range of goods being 9.8% higher,
in winter 2000/01, than in the North-East Scotland city
of Aberdeen. At that time, the price of petrol on the
island of Islay, Argyll was 18.4% higher than in
Aberdeen (Highlands & Islands Enterprise, 2001).
ARTICLE IN PRESSJ. Farmer et al. / Social Science & Medicine 57 (2003) 673–686 675
Recent research in rural Scotland has shown
that residents think activities for teenagers, facilities
for sport and leisure and local service decline need to be
addressed (Hope et al., 2000). The need for differing
policy for remote areas is highlighted by Highlands and
Islands Council’s desire for major investment in
roads development in contrast to national transport
policy where emphasis is on boosting public transport
use (University of Aberdeen & University of Cardiff,
2001).
The role(s) of health professionals
Given the situation in remote and peripheral Scot-
land, it is not surprising that studies of work in these
areas show primary health care professionals dealing
with patients presenting diverse health and social
problems (Iversen, Farmer, & Hannaford, 2000). In
other areas, these might be dealt with by a range of
services and professionals. A district nurse in a study of
Argyll, Scotland provided a flavour of her multi-faceted
work:
There is a complete lack of services around here. I
end up doing everythingyrurality causes problems. I
have to drop off medicine to people because there’s
no pharmacy. I have to arrange carers. We just have
to cobble everything togethery (Farmer et al., 2002)
Cox and Mungall (1998) outline the wide-ranging tasks
for UK rural health professionals and there is evidence
confirming a similar picture for primary health care in
remote areas in North America (Larson & Hart, 2000)
and Australia (Wilks, Barnes, Paul, Wood, & Jones,
1997).
In remote areas of Scotland, nurses have combined
roles including elements of community nursing, health
visiting and midwifery. Findings about district nursing
activity in remote areas of Scotland reveal different
types of patient contact for district nurses (Lauder,
Reynolds, Reilly, & Angus, 2001; Farmer et al., 2002).
These might include intensive activities focused on
particular sick or elderly people, often involving several
ARTICLE IN PRESS
0 5 10 15 20 25 30 35 40
Agriculture & Fishing
Energy & water
Manufacturing
Construction
Distribution, hotels & restaurants
Transport & Communication
Banking, finance & insurance
Public administration & education
Other services
Scotland
Western Isles only
Highlands & Islands
Fig. 1. Employment by sector: a comparison of Western Isles, Highlands & Islands and Scotland in 1997. Figures supplied by
Highlands and Islands Enterprise (2002).
J. Farmer et al. / Social Science & Medicine 57 (2003) 673–686676
visits each day to provide health and social care and
support to patients and relatives. One Hebridean nurse
reflected her emphasis on keeping sick or elderly people
‘on the island’:
I’m a great believer in keeping patients in their own
homes here because if you send them away from here
you’re taking them away from what they’re used to.
(Farmer et al., 2002)
While there is increasing evidence of the multiple facets
of nursing in remote areas, coupled with findings about
gaps in social (Harrop, 2000) and voluntary care
provision (Craig & Manthorpe, 2000; Milligan, 2000),
there is still a lack of explicit acknowledgement by senior
health service management that social and wider ‘caring’
responsibilities are a valid part of the nurse’s job. This
implies that a range of ‘social care’ tasks currently
undertaken, may be undervalued (Audit Commission,
1992; Lauder et al., 2001). Because the wider role is
difficult to record and undertaken implicitly, nurses may
be left in a vulnerable position when their workload and
productivity are audited.
General practice, regardless of where it is conducted,
should take into account patients’ social and cultural
contexts. In remote rural areas, where there may be no
choice of GP, and poorer access to secondary care,
social services and other support networks, the holistic
nature of primary care is particularly important. In
urban settings, continuity of care, a core value of UK
general practice, is being eroded (Guthrie & Wyke,
2000). This relates to organisational changes, such as the
move towards larger practices and the establishment of
out-of-hours co-operatives. In remote rural areas, which
often have small practices and little scope for sharing
on-call, continuity remains (Cox, 1997). These organisa-
tional differences mean that rural general practitioners
are likely to be more intensively involved with the health
and social needs of their patients compared with their
urban counterparts.
In addition to a responsive role in health and social
care, it has been suggested that health professionals in
remote areas can use their rich knowledge of community
and patients proactively to protect and sustain health. A
Scottish study found that rural district nurses became
aware of a wide range of family and individual health
problems at an early stage and from sources other than
formal channels (Lauder et al., 2001). The researchers
identified the concept of ‘community embeddedness’ as a
central feature of the work of district nurses in rural
areas. Embeddedness refers to nurses’ degree of integra-
tion with place and people in the community in which
they practice. The research concluded:
The theme of community embeddedness suggests that
rural nurses have a unique position within their
community. This enables them to gain early insights
into evolving human problems in the context of
family systems and the dysfunctional person’s posi-
tion within that community. This community-family
perspective has both a practical and a symbolic
elementy[rural nurses]y are seen as central to a
healthy and vigorous sense of community, in a very
similar way to the local primary school. (Lauder
et al., 2001)
As this last point suggests, the presence of health
professionals may bring yet another category of benefits
to communities. Indeed, we are proposing that health
professionals may have a key role within the social
structure of fragile remote and peripheral places. This
role emerges from their situation and status in the
community which legitimates them to be richly inte-
grated in formal and informal social, as well as
organisational, networks.
There is some evidence supporting this proposition,
although none emerging from direct empirical study of
health professionals’ contribution to social aspects of
community. Cutchin (Cutchin et al., 1994; Cutchin,
1997a,b) studied the relationship between physician
retention and ‘place integration’ in rural America.
Intriguingly, he found that rural doctors who made a
commitment to staying in a location, actively sought out
roles in community associations and networks. Over
time, rural doctors’ integration in the local social fabric,
made quitting their job a less likely or attractive option.
As the researcher concluded:
yby interacting through time with the emergent and
ongoing problems posed by place, physicians become
woven into the fabric of place. (Cutchin, 1997b)
Those who were not integrated tended to leave rural
places. The overall theme emerging from Cutchin’s
studies was that, if communities desired to retain doctors
and nurses, they should make efforts to include them in
local activities. These findings infer that health profes-
sionals who stay in rural areas over a number of years
are likely to be well integrated socially.
Further evidence of health professionals’ roles in
social structure is provided by Scottish research. An
investigation of life in the Highlands and Islands
described local district nurses and teachers acting as
‘mediators’ for their communities in negotiations with
external bureaucrats (Shucksmith, Chapman, & Clark,
1996). These ‘boundary spanners’ (Anderson, 2000) were
seen to be legitimised by the community to make such
‘vertical linkages’, while also enjoying ‘horizontal
linkages’ through wide social contact with local people
(O’Brien, Raedeke, & Hassinger, 1998). A study in rural
Grampian, Scotland revealed that GPs were sometimes
called upon to help in organising local events and
arbitrate in disputes among neighbours; findings that
ARTICLE IN PRESSJ. Farmer et al. / Social Science & Medicine 57 (2003) 673–686 677

infer a role in community ‘leadership’ (Iversen et al.,
2000).
While this evidence exists, we do not wish to suggest
that health professionals hold a unique position regard-
ing social integration and community leadership. In-
deed, other service professionals, ‘entrepreneurial
incomers’ (Anderson, 2000) and others may be similarly
placed. However, it seems their position as respected
cosmopolitan members of the local community must
locate health professionals as key points of (apparently)
‘neutral’ advice and participation.
Empirical evidence about primary health care in
remote areas of Scotland is only beginning to emerge,
but data so far suggest the importance of carefully
examining existing models of service provision before
changes are considered (Farmer et al., 2002). Current
provision may already represent efficient and effective
models of supplying seamless health and social care for
communities, simultaneously bridging gaps in access,
and sparing demand on secondary care and centralised
social services. Also, and of perhaps key importance to
the ongoing life of fragile remote communities, they may
be providing a crucial contribution to social infrastruc-
ture. It is interesting to note that in countries such as
Australia where the problems of recruitment and
retention of rural health professionals have been
recognised for many years, there is still a policy of
employing doctors and nurses locally, where possible
(National Rural Health Policy Forum, 1999). Attention
to the value of rural health professionals is evident at a
number of levels including the establishment of several
Australian university departments of rural health, a
rural medical school, a range of incentives to rural
working and support for health professionals’ families.
It seems the presence of rural nurses and GPs is
perceived as being intrinsically valuable as a sign of
confident and sustainable rural communities (Bryant &
Strasser, 1999). On a political level this is a sign of the
value of the Australian rural vote.
To summarise, this initial consideration of health
professionals’ roles suggests there is evidence of social
contributions to community that extend beyond desig-
nated health service responsibilities. In considering
health service redesign, it is important to appreciate
and understand the full value of health professionals to
community sustainability.
Life for health professionals working in remote areas
Studies of health professionals who continue to live
and work in remote rural areas indicate that they and
their families appreciate aspects such as ‘clean air’,
beautiful scenery and a secure environment for bringing
up children. Professional aspects such as variety of work
and the chance to practise continuing holistic care are
also reported to be important (Hamilton, Gillies, Ross,
& Sullivan, 1997).
However, professional life in remote areas can be less
than idyllic. A common view expressed is ‘it’s like living
in a goldfish bowl’. It can be difficult to attain family
privacy and appropriate employment for health profes-
sionals’ spouses (Hays, 1999). More than this, isolated
populations can tend to engender feelings that the local
doctor or nurse is ‘owned’ by the community (Rosenthal
& Campbell-Heider, 2001). As Scottish researchers
found:
Many district nurses took the view that locals
regarded them as their own property and not
someone doing a job for 37.75 hours a week. (Lauder
et al., 2001)
In turn, health professionals may feel they are ‘obliged’
to help out at all times:
District nurses embedded in the community reported
feeling a commitment towards their community,
which went beyond their professional remit. (Lauder
et al., 2001)
Far from being a source of job satisfaction, health
professionals’ status can act as a barrier to ‘normal’ life
as it is perhaps difficult to integrate as an ‘ordinary
person’.
Since there are undoubted pressures inherent in
working as a health professional in remote and
peripheral areas, it is perhaps worth asking why some
health professionals do actually stay? Do some profes-
sionals obtain more benefit from life in these commu-
nities than others? While Cutchin’s work, previously
discussed, reveals how health professionals become
‘entangled’ in community networks, it is also likely to
be true that some are more inclined to life and work in
rural communities due to a variety of personal and
professional traits and preferences.
Accomplishing community
In seeking to understand health professionals’ pro-
posed social contribution, it is first necessary to review
some findings about what is meant by ‘community’ and
how people accomplish it (Scott, Park, & Cocklin, 2000).
Shortall (1994) defines community in terms of people
‘‘y living in the same geographical area and frequently
feeling a sense of ‘community spirit’ ’’. It has been
suggested, when considering health policy, that the term
‘locale’ is most useful as it describes the ‘space used as a
setting for routinised interaction’ (Moon, 1990). Having
examined many definitions of ‘community’, Hillery
(1955) defined a typology based on:
ARTICLE IN PRESSJ. Farmer et al. / Social Science & Medicine 57 (2003) 673–686678
* Geographical location: a human settlement with a
fixed and bounded territory.* Social system: the inter-relationships between and
among people living in the same area.* Sense of identity: community resides in a group of
people who share a particular set of values.
In this paper we are interested in health professional’s
contribution to each of these aspects of community.
Although the myth of the rural idyll has been firmly
dispelled (Cloke & Thrift, 1994), rural communities are
still often portrayed as the last strongholds of ‘tradi-
tional society’, characterised by ecological friendliness,
self-sufficiency, spirituality of life and exchange based on
trust and kinship (Pawar, 2001). Exemplified by strong
family or neighbourhood ties, as in Tonnies’ (1887)
notion of ‘gemeinschaft’, they are held to be imbued with
qualities of solidarity and reciprocity, where something
of high value is obtainable: ‘‘y a sense of belonging to a
face-to-face group’’ (Crichton, 1964). In Sack’s (1997)
terms they are communities where life is ‘thick’, enriched
by closely bound networks interacting in relative
isolation (Rousseau, 1995).
Discussions of rural community see their identity
emerging from a combination of historical, relationship
and spatial elements (Jones, 1995). ‘Institutions’ (includ-
ing public services and the churches) have effects on
shaping identity and sense of place, laying down
‘‘sediments’’ of action that serve to shape the norms of
life (Philo & Parr, 2000). Cloke and Jones (2001) discuss
the ‘‘taskscapes’’ that meld together jobs, people and
place like the elements of a landscape. These elements
combine to build the social structures with which local
people identify to give them a sense of belonging to a
place. Place and people are actively involved in this
process of identity building (Entrikin, 1999) which has
significant emotional effects (Cloke & Jones, 2001).
Indeed, Casey (1993) highlights the power of place to:
ydirect and stabilize us, to memorialize and identify
us, to tell us who and what we are in terms of where
we arey .
Findings from ethnographic studies of rural locations
are salutary in warning that beneath the apparent
interconnectedness of ‘communities of place’, there lies
a diversity of ‘communities of interest’ (Bell & Newby,
1971). Philo (1992) has highlighted the importance of
considering the often-excluded ‘‘others’’ of rural com-
munities (that is, non-middle-class, white, male perspec-
tives (Murdoch & Pratt, 1997)). A study of the
Mangakahia valley in New Zealand revealed three key
social groupings (affluent incomers, traditional farming
families and poorer Maoris returning from cities), each
with a different perspective on societal change (Scott
et al., 2000). In the Orkney islands of Scotland, Forsythe
(1980) revealed a number of communities of interest
affected differently by migration effects: former out-
migrant returners, service professionals, ‘urban refugees’
and ‘natives’. Research in rural Grampian, Scotland
revealed health professionals’ perceptions of a number
of different patient groups, with differing service needs
and demands: commuters, women at home with
children, older people, families with socio-economic
difficulties, incomers and rural people who had been
born and brought up in the area (Iversen et al., 2000).
The Cattell (2001) description of ‘membership groups’ in
London communities highlights that such groups can
appear distinct, but are generally inter-linked through
patterns of membership.
These ideas about community suggest factors that
could be important in examining health professionals’
contribution to social structure. They raise questions of:
whether health services as ‘institutions’ might represent
part of a geographical focus for ‘community of place’?;
whether health professionals are a vital part of the
network of social interactions that bind together
disparate ‘communities of interest’?; or whether the
presence of health professionals is important in main-
taining community identity and values? The local
presence of health professionals might have varying
importance and relevance for different ‘communities of
interest’.
According to a study by Shucksmith et al. (1996),
there are three essentials of community: school, church,
and a medical practice. (At the time of that study, only
56% of the Scottish Highland population had access to
a GP within five miles). Later research revealed that the
‘‘core services’’ for a community were thought to be:
shop, primary school, GP and community hall (Hope
et al., 2000). These statements about essential or core
elements require serious consideration. Are they really
saying that, without these institutions, community is
threatened?; or is a spatial concept of ‘community of
place’ focused on central infrastructure being implied? If
so, it is important to develop understanding of how key
services affect the social and cultural fabric such that
they bind together communities, enhancing quality of
life and nurturing a sense of identity. If, in the future,
fewer services are provided in situ, lost through societal
change, service redesign or inability to recruit staff,
might make a community lose its sustainability or begin
to disintegrate?
This is clearly a bleak scenario whose existence can
currently only be sustained through amalgamating hints
of evidence. A New Zealand study revealed that the
combined problems of ageing population and service
depletion make life ‘tough’ for older people who choose
to remain living in rural communities (Joseph &
Chalmers, 1995). Younger people tended to move out
to areas where services were accessible. Bryant and
Strasser (1999) suggest that people need to feel ‘secure’
that they will be able to access the necessary level of
ARTICLE IN PRESSJ. Farmer et al. / Social Science & Medicine 57 (2003) 673–686 679

health care, should a serious situation arise. People will
not move to, or remain in, a community where they
cannot receive health care in an emergency. It is perhaps
mostly from these feelings of insecurity that anger about
local health services decline arise, even although some
studies (for example of rural hospital closures in Canada
(Liu, Hader, Brossart, White, & Lewis, 2001)) have
shown little impact on actual health. Clearly, there is a
need for further information about how deteriorating
access to local primary health care services might affect
longer-term community viability.
Discussion has so far focused on ‘communities of
place’. There are, as noted earlier, other constructions of
community. Massey (1994), for example, argues that
place is not static or authentic, but resides in social
interaction. Thus, predicting the decline of remote
communities through service depletion is both unrealis-
tically romantic, regarding place; and an over-reaction,
regarding community decline. Massey (1994) describes
community as residing where social interactions knit
together. These ‘hubs’ may, indeed should, change over
time. Further, due to the existence of different ‘commu-
nities of interest’, everyone has a different sense of place
and community.
Following this line of argument, there would be little
point in worrying about the effects of service decline on
existing remote communities because societal change
and adaptation are inevitable. Alternative constructions
of community and identity will emerge around places
and social systems. There are other societal forces, such
as access to information and communications technol-
ogies, which are reconstructing the concept of commu-
nity. Counter-migration back into remote and rural
areas by entrepreneurial incomers and those seeking
improved quality of life are engendering economic and
social revival in some places (Anderson, 2000). Given
the distances over which affluent people will commute or
consume, it could be that a sense of community will be
formed over wider geographical areas. Within such
scenarios, although traditional community infrastruc-
ture changes and new patterns of health service
provision emerge, the concept of community is still
sustainable.
Community sustainability
Within a considerable literature on sustainability,
Bryden (1994) highlights the need for rural communities
to have:
ythe capacity to regenerate socially and economic-
allyythe capacity to reproduceyand evolve eco-
nomically, socially, culturally and ecologically.
Sustainability is a concept notoriously difficult to
define, but Bryden’s description seems to encapsulate the
notion envisaged in this paper. That is, we are interested
in health professionals’ contribution to a community’s
capacity to evolve and be a vibrant place to live, in the
face of societal change.
Traditionally, discussion of community sustainability
has emphasised the economic dimension, and it is only
fairly recently that environmental, social and cultural
aspects have become recognised as important (Rivlin,
1993). The Brundtland Commission on Environment
and Development has urged work on measures of
sustainability that emphasise the relationship between
economic, environmental and social conditions (World
Commission on Environment and Development, 1987).
As yet, though, the relationship between factors and
how they work to engender community sustainability is
still poorly understood (Reed, 1999).
There is a developing discussion about the importance
of social aspects in sustainability (Smailes, 1995). Social
sustainability is said to depend on elements of ‘‘liveli-
hood, social participation, justice, equity’’ (Scott et al.,
2000) and sense of place (Stedman, 1999). Research
involving Canadian forestry communities (Nadeau,
Shindler, & Kakoyannis, 1999) has identified a set of
concepts that are important in enriching understanding
of social sustainability, as follows:
* Community stability: is proposed as a measure of the
prosperity, adaptability and cohesiveness of people in
an area and their positive reaction to change (Society
of American Foresters, 1989).* Community capacity: is the characterisation of a
community’s ability to face changing economic,
social and political circumstances.* Community wellbeing: focuses on the degree of match
between local community resources and the social,
cultural and psychological needs of people living
locally.* Community resiliency: is concerned with the capacity
of people and institutions to adapt to change over a
long period of time.
These concepts are all underpinned by notions that
infrastructural and social resources are required for
communities to adapt successfully to change. We argue
that local primary health care provision simultaneously
contributes service infrastructure and ‘social capital’
(discussed later). The concepts listed above present a
useful framework for analysing these inputs and
considering the mechanisms by which they help com-
munities to function and cope with change
Health professionals and community sustainability
We need to begin to understand the role of
health professionals in sustaining remote and rural
ARTICLE IN PRESSJ. Farmer et al. / Social Science & Medicine 57 (2003) 673–686680

communities, particularly in light of what has already
been lost to social structure through increasing centra-
lisation. Research has revealed the significance of
services that have already declined: the social role of
resident clergy (Francis & Lankshear, 1992); the
problems (real or perceived) with rural crime due to
lack of police presence (Morris, 2001); the role of post
offices, banks and village shops as ‘social hubs’ (The
Countryside Agency, 2001): rural schools’ relevance in
helping in-migrant parents to integrate and as a meeting
place for parents from all social groups (Joint Unit for
Research on the Urban Environment and the Depart-
ment of Educational Enquiry, 1981; Witten, McCrea-
nor, Kearns, & Ramasubramanian, 2001).
The current focus on access to health services in
remote areas has revealed a surprising lack of under-
standing of the value of health services to communities.
Some studies have noted the physical importance of the
GP surgery as a meeting place (Farmer & Kennedy,
2001), but there has been little research into the nature
of health professionals’ contribution to wider social
wellbeing. The significance of health professionals to
specific ‘communities of interest’ within localities is also
poorly understood, for example, the importance of visits
from the district nurse for the social inclusion of people
with mobility problems.
The economic contribution of health service employ-
ment to remote communities has also been underplayed.
Roberts (2002) described the increasingly important part
played by the state funding of public sector activity in
remote communities as the traditional economic base
(fishing and textiles in the case of the Western Isles)
declines. The key contribution of the public sector in
local people’s employment has already been shown (see
Fig. 1). Around 17,000 jobs are directly provided by the
health care sector in the Scottish Highlands and Islands
compared with around 8,000 in education and 12,000 in
local government.2 A recent US study highlighted that
15–20% of local employment was generated by direct
health care posts and jobs created in servicing the health
care community (Doeksen & Schott, 2002). A glance at
the local directory on the Hebridean island of Tiree
demonstrates little industrial activity and surprisingly
little tourism-related development. Yet the island sup-
ports a population of around 750 people, many of whom
obtain full or part-time employment from services such
as transport, education and health care. It could be that
service sector employment is making a key contribution
to some younger families’ decisions to remain living and
working in the community. With such a complex inter-
dependent network of jobs and people, decline in the
health service sector would have impacts on both direct
health service employment and on associated posts.
Further, both US and Scottish studies have highlighted
the important economic effect of local public service
infrastructure in attracting tourists and retirees to locate
in rural areas (Roberts, 2002; Doeksen & Schott, 2002).
These are important groups in terms of their propensity
to consume within local communities.
We argue that assessing the social and economic
contribution of health professionals to community
sustainability is worthwhile and timely. Examination
of different types of remote communities (i.e. those that
have traditionally had poor health service infrastructure,
those that have recently lost services and those where
service provision is still vigorous) could assist in
detecting the contribution of health professionals. This
strategy could prove useful in developing knowledge of
who fulfils the proposed extended social role of health
professionals, as well as their professional role, when
they are gone. Such studies could reveal whether
communities with and without accessible working health
professionals exhibit different patterns of social inter-
connections. And, if infrastructural changes occur in
communities, whether, and at what pace, society adapts.
Health professionals and capital
A growing body of work by sociologists, political
scientists and others could provide a potential theore-
tical framework for understanding and analysing the
resources necessary for community sustainability. This
envisages the generation and spending of ‘capital’
(resources) within a number of key areas, including:
material, cultural, symbolic and social. Consideration of
health professionals’ role in relation to capital could be
important in understanding their contribution to com-
munity. The possible relevance of theories of capital is
discussed briefly here.
Social capital
The concept of social capital is currently prevalent in
policy and academic circles (Baron, Field, & Schuller,
2000; Cote & Healy, 2001; Atterton, 2001) and it is
therefore particularly relevant in examining issues
pertinent to public services design. It is additionally
apposite in the examination of remote communities
which are thought to be more ‘traditional’ and therefore
might be assumed to have greater potential to generate
social capital. Like sustainability, social capital is an ill-
defined concept. Although it is generally agreed that
high levels of formal and informal social interaction
benefit society, it is unclear whether this amounts to
‘social capital’. A lack of empirical evidence means that
mechanisms, indicators and tools for measurement of
social capital, are poorly developed (Baron et al., 2000).
ARTICLE IN PRESS
2Figures supplied by Highlands and Islands Enterprise
(2002).
J. Farmer et al. / Social Science & Medicine 57 (2003) 673–686 681

Social capital is said to form out of repeated social
interaction between individuals and groups which
develops trust, reciprocity and norms of behaviour
(Coleman, 1994). The amount of capital built depends
on the quality and quantity of interactions (Falk &
Kilpatrick, 2000). A recent study of social capital within
a rural community described resources as emerging
through exchange of ‘knowledge resources’ and ‘identity
resources’; that is, frequent allusions to shared knowl-
edge, history and vision for the future served to enhance
and embed social relations (Falk & Kilpatrick, 2000).
Since it is proposed that health professionals in remote
communities have a high level of interaction within their
local community (horizontal linkages) and externally
(vertical linkages), they are likely to be important
contributors to building social capital.
There is some debate as to whether social capital can
only reside with groups (Lochner, Kawachi, & Kennedy,
1999), having developed out of interaction; or whether
individuals can hold ‘slices’ of social capital that are
dependent on their place and status in social groups
(Bourdieu, 1986). Adherence depends on different
interpretations of the concept of social capital (Siisiai-
nen, 2000). Use of the word ‘capital’ would imply that
the idea of social capital is premised on rational
economic ‘exchange theory’. Bourdieu’s (1986) inter-
pretation certainly holds that no accumulation of capital
is disinterested and thus social capital would be built as
a source of personal power. However, in viewing social
capital as a by-product of social activities, other
interpretations imply that it could have developed out
of altruistic actions (Putnam, 1993b).
A disturbing element of social capital is its potential
use to maintain status in the social hierarchy (Hawe &
Shiell, 2000). Shucksmith (2000) notes the discord
inherent within the concept of social capital which:
ycan be a source of cohesion, but also of conflict as
those who are excluded from the group in which the
capital resides will not benefity .
He provides an illustrative example from his own work,
which found that European Union LEADER pro-
gramme funds tended to be granted to those well-
networked local ‘notables’ who already dominated rural
development rather than to less experienced applicants.
Massey (1991) confirms this notion of ‘power geometry’,
conspicuous in rural areas. It might be argued that
health professionals, simply through their position in the
social hierarchy, exclude others from meaningful social
roles; although again, there is no evidence on this issue.
Social capital is argued by some to be a key element in
community viability and whether or not it develops to
become a coherent and enduring concept, there is wide
support for the relevance of strong social infrastructure
to community wellbeing. Evidence indicates that health
professionals are well placed to contribute to social
infrastructure and, therefore, the relevance of social
capital to an underlying theory for health care provision
in remote communities should be considered. It is
important also to reflect on those who stand to gain
and lose from health professionals’ role in producing
social capital when assessing the effects of their loss to
communities. Again, it might be that different ‘commu-
nities of interest’ might be affected in varying ways.
Symbolic and cultural capital
Since we are hypothesising that health professionals
play a role in community sustainability and that they are
important contributors to social capital, it is now
pertinent to ask—to what extent does this role reside
with the job or with the individual? One school of
thought argues that it is charismatic individuals who
energise community or group achievement (Wilkinson,
1991). A study of the Scottish Highlands and Islands
noted that:
y in the scattered communities, the doctors were
revered for their commitment to the community and
their accessibilityypersonal involvement with the
community, integrity and conscientious visiting
habitsy[They were]yviewed as key local personal-
ities. (Shucksmith et al., 1996)
Only two of the features present in that statement,
‘visiting’ and ‘accessibility’, might be construed as
related to doctors’ health care role. Indeed the emphasis
is on their value as individual personalities.
Contrary to this position, theories of capital would see
power residing in the cultural and symbolic resources
inherent in the professional role (Bhaskar, 1979).
Bourdieu’s writing on social theory implies that health
professionals are seen as respected ‘leaders’ by their
communities both because of the cultural capital they
hold (derived from educational and professional quali-
fications) and their symbolic capital or power (Swartz,
1997). Symbolic capital is that which is accrued through
exercising their professional status. Health professionals
and their patients might be viewed as being involved in a
cyclical process of developing this capital. Put simply,
because it is perceived by the community as important to
have a local doctor, the person in that role can gain
symbolic power within the community. Bourdieu’s
philosophy suggests that such arrangements would be
typical within traditional societies, where:
yindividuals and groups draw on a variety of
cultural, social and symbolic resources in order to
maintain and enhance the social order (Swartz,
1997).
ARTICLE IN PRESSJ. Farmer et al. / Social Science & Medicine 57 (2003) 673–686682

While the relevance of this theory within the context of
contemporary (i.e. non-traditional) Western societies
might be considered doubtful, there is some evidence
from research in remote rural Scotland suggesting its
validity. The Ennew (1980) ethnographic study of life on
a Hebridean island and previously mentioned work by
Shucksmith et al. (1996) noted that service professionals
such as doctors, nurses and teachers were ‘expected’ to
undertake tasks such as negotiating with those external
to the community. Forsythe’s (1980) study of an Orkney
island showed that cosmopolitan incomers tended to
become community leaders and were ‘expected’ to provide
employment, while the attitudinal norms of indigenous
people forced them to be more reticent and passive.
This choice between charismatic personality or symbolic
role being most important in ascribing health profes-
sionals’ identity in the community implies a dichotomy.
Inevitably, the situation is probably more complex than
this. Indeed, it seems likely that aspects of personality and
role are inter-twined. It may even be that only certain types
of personality respond to the social responsibilities
attendant with working in remote communities.
Conclusions
This paper has attempted to develop the argument
that health professionals, working and residing locally,
make a valuable contribution to the social structure of
remote communities, in addition to health care, social
care and economic contributions. It seeks to stimulate
consideration of the extent to which primary health care
services are necessary to the infrastructure required to
sustain communities into the future. It suggests that
consideration of theories of capital, and particularly the
concept of social capital, might be pertinent in under-
standing the extended role of health professionals in
remote places. At the same time, it acknowledges that
society thrives on change and communities might form
around different models. New ‘communities of place’
and ‘communities of interest’ might have different
patterns of leadership and perspectives on social activity
and identity. New models of health care provision, with
fewer local health professionals, might actually empower
those traditionally excluded from participation in social
infrastructure by prevailing hegemonies.
At root, we are urging for greater understanding of
the roles of health care professionals in remote commu-
nities before new models of primary health care
provision are introduced which might have unforeseen
effects on social and economic structure. Currently, it
seems, decisions about service redesign are being
considered solely by health service stakeholders. Yet
health service decisions regarding fragile communities
may affect their sustainability and are relevant to all in
society. A holistic approach to service redesign needs to
be taken, informed by evidence about the potential
impacts of change. At the very least, any new health care
models implemented should be evaluated by assessing
social and economic, as well as health care, effects.
Moreover, decisions about health service remodelling
should ideally be seen as part of a wider debate about
the future sustainability of remote communities. As a
society, do we value these communities? Do we want to
keep them? Are they important to our cultural and
historical heritage? What do they contribute to the
future we envisage for our country? If they are valued,
we need to invest in supporting them. This is a debate
relevant to all in society, rural and urban dwellers alike.
Government policies may need to reorient so that they
are not simply addressing economic issues such as
compensation for agricultural decline and small business
start-ups. (Only so many pottery shops are needed in the
Hebrides!) A substantial proportion of current full and
part-time employment in remote communities is based
around service and utility jobs. If society decided it
wanted to invest in retaining remote communities, then
steps to maintain service infrastructure could be taken.
Careful reflection on policies and their outcomes in
countries with a record of considering the rural agenda
(for example, Canada, Sweden, Norway and Australia)
would be instructive in highlighting the relationship
between government support for services and rural
community vibrancy. This paper does not seek to
romanticise the role of health professionals in rural areas
nor does it advocate an anti-change ‘museum strategy’ to
service provision. It merely proposes that we need to
explore health professionals’ roles in remote rural areas so
evidence can be generated to inform strategic investment
decisions about future health care provision.
Acknowledgements
The authors would like to thank: Dr Craig Veitch,
Associate Professor of Rural Health, James Cook
University, Townsville, Australia; Dr Gordon Baird,
general practitioner, Sandhead, Dumfries & Galloway;
Dr Andrea Nightingale, Research Fellow, University of
Aberdeen Arkleton Centre for Rural Development
Research; and Mrs Lisa Iversen, Chief Scientist Office
Health Services Research Fellow, University of Aberd-
een Department of General Practice & Primary Care
and anonymous reviewers of this paper for their time in
considering earlier versions and for their helpful
comments and suggestions.
References
Anderson, A. R. (2000). Paradox in the periphery: An
entrepreneurial reconstruction? Entrepreneurship & Regional
Development, 12, 91–109.
ARTICLE IN PRESSJ. Farmer et al. / Social Science & Medicine 57 (2003) 673–686 683
Atterton, J. (2001). The role of civil society and the business
community in rural restructuring. Edinburgh: Scottish
Executive Central Research Unit.
Audit Commission (1992). Caring systems: Effective implemen-
tation of ward nursing management systems. London: Her
Majesty’s Stationery Office.
Baird, A. G., Donnelly, C. M., Miscampbell, N. T., & Wemyss,
H. D. (2000). Centralisation of cancer services in rural areas
has disadvantages. British Medical Journal, 320(7236),
717.
Baron, S., Field, J., & Schuller, T. (Eds.). (2000). Social
capital—critical perspectives. Oxford: Oxford University
Press.
Bell, C., & Newby, H. (1971). Community studies. London:
Allen & Unwin.
Bentham, G., Hinton, J., Haynes, R., Lovett, A., & Bestwick,
C. (1995). Factors affecting non-response to cervical
cytology screening in Norfolk, England. Social Science &
Medicine, 40(1), 131–135.
Bhaskar, R. (1979). The possibility of naturalism. Brighton:
Harvester.
Bourdieu, P. (1986). The forms of capital. In J. E. Richardson
(Ed.), Handbook of theory of research for the sociology of
education (pp. 241–258). London: Greenwood Press.
Boyle, P., & Halfacree, K. (1998). Migration into rural areas:
Theories and issues. Chichester: Wiley.
Bryant, L., & Strasser, R. (1999). The delivery of sustainable
rural and remote health services (Regional Australia Summit
papers 27–29 October 1999). Canberra: Regional Australia
Summit Unit [wwwdbtrs.gov.au/regional/summit]. Accessed
10/12/01.
Bryden, J. (1994). Some preliminary perspectives on sustainable
rural communities. In J. Bryden (Ed.), Towards sustainable
rural communities: The Guelph seminar series (pp. 40–50).
Guelph: Canada: School of Rural Planning & Development.
Campbell, N. C., Elliott, A. M., Sharp, L., Ritchie, L. D.,
Cassidy, J., & Little, J. (2000). Rural factors and survival
from cancer: Analysis of Scottish cancer registrations.
British Journal of Cancer, 82(11), 1863–1866.
Casey, E. (1993). Getting back into place: Toward a renewed
understanding of the place-world. Bloomington: Indiana
University Press.
Cattell, V. (2001). Poor people, poor places, and poor health:
The mediating role of social networks and social capital.
Social Science & Medicine, 52(10), 1501–1516.
Cloke, P., Milbourne, P., & Thomas, C. (1994). Lifestyles in
rural England. A research report to the Department of the
Environment and the Economic and Social Research
Council and the Rural Development Commission.
Cloke, P., & Thrift, N. (1994). Refiguring the rural. In P. Cloke,
M. Doel, D. Matless, M. Phillips, & N. Thrift (Eds.) Writing
the rural: Five cultural geographies (pp. 1–5). London: Paul
Chapman.
Cloke, P., & Jones, O. (2001). Dwelling, place and landscape:
An orchard in Somerset. Environment & Planning A, 33,
649–666.
Coleman, J. S. (1994). Foundations of social theory. Cambridge,
MA: The Belknap Press of Harvard University Press.
Cote, S., & Healy, T. (2001). The well-being of nations. The role
of human and social capital. Paris: Organisation for
Economic Co-operation & Development.
Cox, J. (1997). Rural general practice: A personal view of
current issues. Health Bulletin, 55(5), 309–315.
Cox, J., & Mungall, I. (Eds.). (1998). Rural healthcare. Oxford:
Radcliffe Medical Press.
Craig, G., & Manthorpe, J. (2000). Fresh fields: Rural social
care: Research, policy and practice agendas. York: Joseph
Rowntree Foundation.
Crichton, R. (1964). Commuters’ village; a study of community
and commuting in a Berkshire village. Dawlish: David &
Charles.
Cutchin, M. P. (1997a). Community and self: Concepts for
rural physician integration and retention. Social Science &
Medicine, 44(11), 1661–1674.
Cutchin, M. P. (1997b). Physician retention in rural commu-
nities: The perspective of experiential place integration.
Health & Place, 3(1), 25–41.
Cutchin, M. P., Norton, J. C., Quan, M. M., Bolt, D., Hughes,
S., & Lindeman, B. (1994). To stay or not to stay: Issues in
rural primary care physician retention in Eastern Kentucky.
The Journal of Rural Health, 10(4), 273–278.
Deaville, J. A. (2001). The nature of rural general practice in the
UK: Preliminary research. Newtown, Wales: Institute of
Rural Health.
Department of Environment, Transport & the Regions (2000).
Our countryside: The future: A fair deal for rural England.
Cm 4909. London: The Stationery Office.
Doeksen, G. A., & Schott, V. (2002). The economic importance
of the health care sector on a rural economy. Paper
presented at the Fifth Wonca World Conference on Rural
Health, Melbourne, Australia, April 30–May 3, 2002.
Ennew, J. (1980). The Western Isles today. Cambridge: Cam-
bridge University Press.
Entrikin, J. N. (1999). Political community, identity and
cosmopolitan place. International Sociology, 14(3), 269–282.
European Society for Rural Sociology (2001). The term is used
in the call for papers for the XIXth Congress of the
European Society for Rural Sociology. ‘‘Society, Nature,
Technology: The Contribution of Rural Sociology’’. Dijon,
France 3–7th September 2001 [http://cc.joensuu.fi/~alma/
esrs/arc/19calpa.htm] Accessed on 24th October 2001.
Falk, I., & Kilpatrick, S. (2000). What is social capital? A study
of interaction in a rural community. Sociologica Ruralis,
40(1), 87–110.
Farmer, J., Iversen, L., & Baird, G. (2001). Rural deprivation:
Reflecting reality. British Journal of General Practice, 51,
486–491.
Farmer, J., & Kennedy, L. (2001). Citizen’s Advice Bureau
outreach services evaluation. Aberdeen: University of
Aberdeen.
Farmer, J., West, C., Whyte, B., Black, F., Mulvenna, G.,
Morton, D. (2002). Rural–urban morbidity recording project:
Interim evaluation report of the early stages. Aberdeen:
University of Aberdeen.
Forsythe, D. E. (1980). Urban incomers and rural change. The
impact of migrants from the city on life in an Orkney
community. Sociologica Ruralis, 20, 287–307.
Francis, L. J., & Lankshear, D. W. (1992). The rural rectory:
The impact of a resident priest on local church life. Journal
of Rural Studies, 8(1), 97–103.
Goodall, B. (1987). The dictionary of human geography.
London: Penguin.
ARTICLE IN PRESSJ. Farmer et al. / Social Science & Medicine 57 (2003) 673–686684
Gould, M. I., & Moon, G. (2000). Problems of providing health
care in British island communities. Social Science &
Medicine, 50, 1081–1090.
Guthrie, B., & Wyke, S. (2000). Does continuity in general
practice really matter? British Medical Journal, 321(7263),
734–736.
Halfacree, K. H. (1993). Locality and social representation—
space, discourse and alternative definitions of the rural.
Journal of Rural Studies, 9, 23–27.
Hamilton, I. J., Gillies, J., Ross, S., & Sullivan, F. (1997).
Attitudes of general practitioners who practice in remote
communities. Health Bulletin, 55(2), 103–108.
Harrop, A. (Ed.). (2000). Changing views of rural Britain: Why
services matter. London: New Policy Institute.
Hawe, P., & Shiell, A. (2000). Social capital and health
promotion: A review. Social Science & Medicine, 51,
871–885.
Haynes, R. M., & Bentham, C. G. (1982). The effects of
accessibility on general practitioner consultations, out-
patient attendances and in-patient admissions in Norfolk,
England. Social Science & Medicine, 16(5), 561–569.
Hays, R. B. (1999). Common international themes in rural
medicine. Australian Journal of Rural Health, 7(3),
191–194.
Helmsdale & District GP Action Group (2001). Helmsdale &
District GP Action Group. Our Position in Brief.
[www.helmsdale.org/News/news.html]. Accessed 18/12/01.
Higgs, G. (1999). Investigating trends in rural health outcomes:
A research agenda. Geoforum, 30(3), 203–221.
Highlands & Islands Enterprise. (2001). Highlands & Islands
Enterprise Economic Information. [http://www.hie.co.uk/
welcome.asp.locID-hieecoint.htm]. Accessed 10/12/01.
Hillery, G. A. (1955). Definitions of community: Areas of
agreement. Rural Sociology, 20(2), 111–123.
Hoggart, K., Buller, H., & Black, R. (1995). Rural Europe:
Identity and change. London: Arnold.
Hope, S., Anderson, S., & Sawyer, B. (2000). The quality of
services in rural Scotland. Edinburgh: Scottish Executive
Central Research Unit.
Hugo, G., & Smailes, P. (1985). Urban–rural migration in
Australia: A process view of the turnaround. Journal of
Rural Studies, 1, 11–30.
Iversen, L., Farmer, J., & Hannaford, P. (2000). Perceptions of
work and workload pressures in rural and urban general
practice: A pilot study. Final report. Aberdeen: University of
Aberdeen Department of General Practice & primary Care.
Joint Unit for Research on the Urban Environment and the
Department of Educational Enquiry (1981). The social
effects of rural primary school reorganization in England: A
study on behalf of the Department of the Environment and the
Department of Education and Science. Final report.
Birmingham: University of Aston.
Jones, O. (1995). Lay discourses of the rural: Developments and
implications for rural studies. Journal of Rural Studies, 11,
35–49.
Jones, A. P., & Bentham, G. (1995). Emergency medical service
accessibility and outcome from road traffic accidents. Public
Health, 109, 169–177.
Jones, A. P., & Bentham, G. (1997). Health service accessibility
and deaths from asthma in 401 local authority districts in
England and Wales 1988–1992. Thorax, 52(3), 218–222.
Jones, A. P., Bentham, G., Harrison, B. D. W., Jarvis, D.,
Badminton, R. M., & Wareham, N. J. (1998). Accessibility
and health service utilization for asthma in Norfolk,
England. Journal of Public Health Medicine, 20(3),
312–317.
Jones, A. P., Bentham, G., & Horwell, C. (1999). Health service
accessibility and deaths from asthma. International Journal
of Epidemiology, 28(1), 101–105.
Joseph, A. E., & Chalmers, A. I. (1995). Growing old in place:
A view from rural New Zealand. Health & Place, 1(2),
79–90.
Larson, E. H., & Hart, L. G. (2000). The rural physician. In J.
P. Geyman, T. E. Norris, & L. G. Hart (Eds.), Textbook of
rural medicine. New York: McGraw-Hill.
Lauder, W., Reynolds, W., Reilly, A., & Angus, N. (2001). The
role of district nurses in caring for people with mental health
problems in rural settings. Journal of Clinical Nursing,
Special Edition: Primary Care, 10(3), 337–344.
Launoy, G., Coutour, X., Gignoux, M., Pottier, D., & Dugleux,
G. (1992). Influence of rural environment on diagnosis,
treatment and prognosis of rectal cancer. Journal of
Epidemiology and Community Health, 46, 365–367.
Liu, L., Hader, J., Brossart, B., White, R., & Lewis, S. (2001).
Impact of rural hospital closures in Saskatchewan, Canada.
Social Science & Medicine, 52, 1793–1804.
Lochner, K., Kawachi, I., & Kennedy, B. P. (1999). Social
capital: A guide to its measurement. Health & Place, 5(4),
259–270.
Massey, D. (1991). A global sense of place. Marxism Today,
June (pp. 24–29).
Massey, D. (1994). Space, place and gender. Oxford: Polity
Press.
Milligan, C. (2000). ‘Breaking out of the asylum’: Develop-
ments in the geography of mental ill-health—the influence
of the informal sector. Health & Place, 6(3), 189–200.
Moon, G. (1990). Conceptions of space and community in
British health policy. Social Science & Medicine, 30(1),
165–171.
Morris, S. (2001). Rural policing is no better, say villagers. The
Guardian Wed Oct 31, 2001. [wysiwyg://162/http://
www.guardian.co.uk/martin/article/0,2763,583837,00.html].
Accessed on 18/12/01.
Murdoch, J., & Pratt, A. C. (1997). From the power of
topography to the topography of power: A discourse on
strange ruralities. In P. Cloke, & J. Little (Eds.), Contested
countryside cultures: Otherness, marginalisation and rurality
(pp. 51–69). London: Routledge.
Nadeau, S., Shindler, B., & Kakoyannis, C. (1999). Forest
communities: New frameworks for assessing sustainability.
The Forestry Chronicle, 75(5), 747–754.
National Rural Health Policy Forum (1999). Health horizons:
1999–2003: A framework for improving the health of rural,
regional and remote Australians. Adelaide: NRHPF.
O’Brien, D. J., Raedeke, A., & Hassinger, E. W. (1998). The
social networks of leaders in more or less viable commu-
nities six years later: A research note. Rural Sociology, 63(1),
109–127.
Pahl, R. (1970). Patterns of urban life. London: Longman.
Pawar, M. (2001). Resurrection of traditional communities in
postmodern societies. Accessed Dec 10th, 2001 [http://
www.csu.edu.au].
ARTICLE IN PRESSJ. Farmer et al. / Social Science & Medicine 57 (2003) 673–686 685
Philips, M. (1999). Migration and social change. In The Rural
Group of Labour MPs, Rural audit: A health check on rural
Britain (pp. 26–29). Cheltenham: The Rural Group of
Labour MPs.
Philo, C. (1992). Neglected rural geographies: A review. Journal
of Rural Studies, 8, 193–207.
Philo, C., & Parr, H. (2000). Institutional geographies:
Introductory remarks. Geoforum, 31(4), 513–521.
Proctor, M. (2000). The future of community nursing. In
Scottish Council for Postgraduate Medical and Dental
Education, Seeking solutions: Education and training for
remote and rural health professionals. Report of a multi-
disciplinary conference 30–31 March 2000.
Putnam, R. (1993a). Making democracy work: Civic traditions in
modern Italy. Princeton: Princeton University Press.
Putnam, R. D. (1993b). The prosperous community. The
American Prospect, 4(13), 35–42.
Reed, M. G. (1999). ‘‘Jobs Talk’’: Retreating from the social
sustainability of forestry communities. The Forestry Chroni-
cle, 75(5), 755–763.
Reimer, B. (2000). Leading and lagging sites in rural Canada.
Conference paper presented at ‘European Rural policy at the
crossroads’. Aberdeen: University of Aberdeen Arkleton
Centre for Rural Development.
Remote and Rural Areas Resources Initiative (RARARI)
Recruitment and Retention Working Group. (2002)
[www.rararibids.org.uk/rarari/index.asp?TopicID ¼ 107].
Accessed 29th Jan 2002.
Remote and Rural Areas Resources Initiative (RARARI)
Solutions Group. (2002). Solutions for the provision of
health care in the remote and rural areas of Scotland in the
21st century. Fort William, Scotland: RARARI.
Rivlin, A. M. (1993). Values, institutions and sustainable
forestry. In G. H. Aplet, N. Johnson, J. T. Olson, & V. A.
Sample (Eds.), Defining sustainable forestry (pp. 255–259).
Washington, DC: Island Press.
Roberts, D. (2002). The changing economic base of rural areas:
A SAM-based analysis of the Western Isles. A report for
Western Isles Enterprise. Aberdeen: University of Aberd-
een.
Rosenthal, T. C., & Campbell-Heider, N. (2001). The rural
health care team. In J. P. Geyman, T. E. Norris, & L. G.
Hart (Eds.), Textbook of rural medicine (pp. 41–55). New
York: McGraw-Hill.
Rousseau, N. (1995). What is rurality? In J. Cox (Ed.), Rural
general practice in the UK (pp. 1–4). Occasional paper 71.
London: Royal College of General Practitioners.
Sack, R. (1997). Homo geographicus. Baltimore, MD: John
Hopkins University Press.
Scott, K., Park, J., & Cocklin, C. (2000). From ‘sustainable
rural communities’ to ‘social sustainability’: Giving voice to
diversity in Mangakahia Valley, New Zealand. Journal of
Rural Studies, 16(4), 433–446.
Scottish Executive Rural Affairs Department. (2000). Rural
Scotland: A new approach. Edinburgh: Scottish Executive.
Scottish National Rural Partnership. (2000). Services in rural
Scotland. Edinburgh: Scottish Executive.
Shortall, S. (1994). The Irish rural development paradigm: An
exploratory analysis. Economic & Social Review, 25,
233–260.
Shucksmith, M. (2000). Endogenous development, social
capital and social inclusion: Perspectives from LEADER
in the UK. Sociologica Ruralis, 40(2), 208–218.
Shucksmith, M., Chapman, P., & Clark, G. M. (1996). Rural
Scotland today: The best of both worlds?. Avebury: Alder-
shot.
Siisiainen, M. (2000). Two concepts of social capital: Bourdieu
vs. Putnam. Paper presented at International Society for
Third-Sector Research (ISTR) Fourth International Confer-
ence ‘‘The Third Sector: For what and for whom?’’ Trinity
College, Dublin, July 5–8 2000.
Smailes, P. J. (1995). The enigma of social sustainability in rural
Australia. Australian Geographer, 26(2), 140–150.
Society of American Foresters. (1989). Report of the Society of
American Foresters (SAF) National Task Force on Commu-
nity Stability. SAF Resource Policy Series. Bethesda, MD:
SAF.
Stedman, R. C. (1999). Sense of place as an indicator of
community sustainability. The Forestry Chronicle, 75(5),
765–770.
Swartz, D. (1997). Culture and power: The sociology of Pierre
Bourdieu. Chicago: University of Chicago Press.
The Countryside Agency (2001). Rural services in 2000.
London: The Countryside Agency.
The Scottish Office Department of Health. (1998). Acute
services review report. Edinburgh: The Stationery Office.
Tonnies, F. (1887). Community and society: Gemeinschaft and
gesellschaft. (C. P. Loomis Trans. and Ed.). New York:
Harper and Row, 1957, Preprint.
University of Aberdeen & University of Cardiff. (2001).
Transport policies for rural Scotland: The assessment of
policies in relation to rural development and sustainability
objectives. Edinburgh: Scottish Executive Central Research
Unit.
White, S. D., Guy, C. M., & Higgs, G. (1997). Changes in
service provision in rural areas: Part 2: Changes in post
office provision in Mid Wales: A GIS-based evaluation.
Journal of Rural Studies, 13(4), 451–465.
Wilkinson, K. P. (1991). The community in rural America. New
York: Greenwood Press.
Wilks, J., Barnes, J., Paul, K., Wood, M., & Jones, D. (1997).
Managing patient records and documenting service delivery:
The results of a ‘best practice’ remote area nursing program.
Australian Journal of Rural Health, 5(3), 153–157.
Witten, K., McCreanor, T., Kearns, R., & Ramasubramanian,
L. (2001). The impacts of a school closure on neighbour-
hood social cohesion: Narratives from Invercargill, New
Zealand. Health & Place, 7, 307–317.
World Commission on Environment and Development. (1987).
A common future. Oxford: Oxford University Press.
ARTICLE IN PRESSJ. Farmer et al. / Social Science & Medicine 57 (2003) 673–686686