1
Who Will Be Writing Your
Prescriptions in the Future?
Jared N. Schwartz, MD, PhD, FCAPDirector, Pathology & Lab Medicine
Presbyterian HealthcareCharlotte, NC
President, College of American Pathologists
In the beginning God created the heavens and the earth. Now the earth was formless and empty, darkness was over the surface
of the deep, and the Spirit of God was hovering over the waters.
And God said, “Let there be light,” …
2
…and the light microscope was born
More than 100 years later, it is still the primary tool
• Majority of tissue-based diagnostics is still based on the interpretation of the morphologic characteristics of fixed and stained cells and tissues as seen under the microscope
• An experienced surgical pathologist may confidently render an unequivocal diagnosis of a malignant neoplasm with as few as 10 cells from a biopsy that contains thousands

3
These observations render it painfully obvious that unraveling the molecular features of cancer will
take many years, probably decades, and that the crucial role microscopy will continue to play during
this period will provide irreplaceable data if properly integrated with newer techniques.
Any new technique must provide information of prognostic or
therapeutic significance beyond that provided by the current gold
standard
Juan Rosai, MDLaboratory Investigation (2007) 87, 403–408.
doi:10.1038/labinvest.3700551; published online 2 April 2007
Only if molecular markers are identified that robustly and specifically identify discrete cell populations will the need for histologic assessment disappear
Christopher A Moskaluk MD, PhDDepartment of Pathology, University of Virginia
Health System, Charlottesville, VA
4
I guess I was wrong…
“…This challenge is intended to lay the groundwork for changing the basis of tumor classification from morphological to molecular characteristics.”
1999 NIH Director Dr. Harold Varmus
5
Molecular profiling is a reality today• Single Biomarker Analysis
– IgH and T cell receptor gene rearrangements, together with analysis of specific translocations increasingly applied to the diagnosis oflymphoma
– Microsatellite instability, either for diagnosis of hereditary nonpolyposiscolorectal cancer or for prognostication, is readily used in many centers
– Fluorescence in situ hybridization is still the preferred mode of analysis of HER2-neu amplification status in breast cancer
– EGFR mutation analysis is commonly used for therapeutic decision-making in lung cancer as is detection of KIT (c-kit) mutations in gastrointestinal stromal tumors
– Presence of 1p/19q loss of heterozygosity has diagnostic and prognostic implications in brain neoplasms
– Human papillomavirus subtype analysis by molecular testing advocated to play an important part in cervical screening
– Translocation-related sarcomas accurately diagnosed by PCR translocation detection
– Molecular fingerprinting revolutionizing analysis of putative metastases
Molecular profiling is a reality today• Whole-genome approaches to molecular
diagnosis– DNA microarray analysis used to assay DNA
and RNA content– Single nucleotide polymorphisms (SNPs) that
can determine the presence of specific polymorphic sequences on chromosomes
– Mass spectrometry
6
What is driving the growth in molecular testing
• Many so-called blockbuster drugs show only limited efficacy in as many as 70% of treated patients
• Current roster of phenotypically derived drugs that often treat only the symptoms of diseases is no longer acceptable to the public
• High volume of adverse drug reactions caused by the failure to predict toxicity in individuals and toxic drug-drug interactions
The Integration of Molecular Diagnostics With Therapeutics, AJCP, Jeffrey S. Ross, MD, Geoffrey S. Ginsburg, MD, PhD
What is driving the growth in molecular testing
• As many as 20% to 40% of people receiving pharmaceutical agents may be receiving the wrong drug
• Discovery of the human genome and subsequent expansion of proteomics research combined with emerging technologies are producing unprecedented changes in today's health care
• An increasingly educated public demanding more information about their predisposition for serious diseases
The Integration of Molecular Diagnostics With Therapeutics, AJCP, Jeffrey S. Ross, MD, Geoffrey S. Ginsburg, MD, PhD

7
Molecular diagnostics integration with therapeutics represents a major new opportunity for pathology
to emerge as leaders of the new medicine• Detection of disease predisposition• Screening and early disease diagnosis• Prognosis assessment• Guiding the selection, dosage, route of administration,
and multi-drug combinations• Pharmacogenomic measurements of drug efficacy and
risk of toxic effects• Monitoring of the illness until the final disease outcome is
known
The future consequence of this trend is clear: conventional surgical pathology will not be less important…but molecular testing, rather than
morphological characterization, may provide the decisive information for diagnosis and
treatment.
A Case for Integrated Morphomolecular Diagnostic PathologistsManuel Salto-Tellez
Department of Pathology, National University Hospital, Yong Loo Lin Medical School and, Oncology Research Institute, National University of
Singapore, Singapore
8
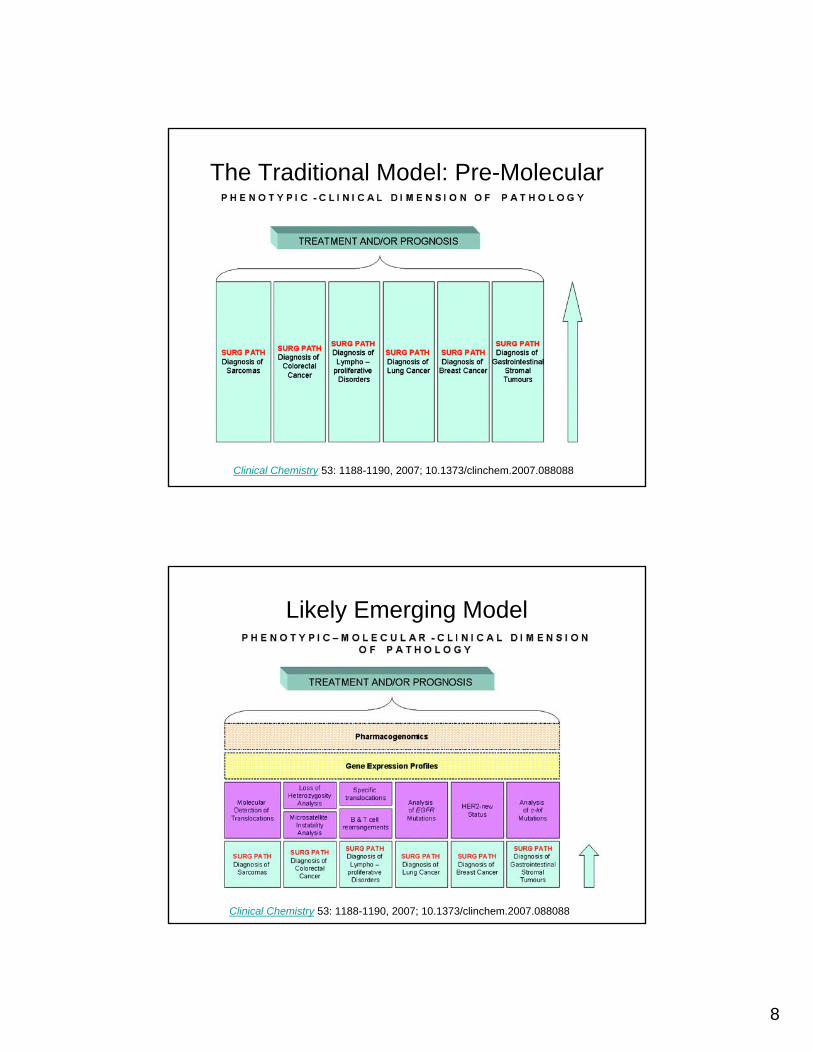
Clinical Chemistry 53: 1188-1190, 2007; 10.1373/clinchem.2007.088088
The Traditional Model: Pre-Molecular
Clinical Chemistry 53: 1188-1190, 2007; 10.1373/clinchem.2007.088088
Likely Emerging Model
9
Think about it…
Your diagnosis of invasive malignancy triggers a course oftherapy for a breast cancer patient that may include a dangerous and traumatic course of surgery, chemotherapy and radiation
Pathologists are clinicians guiding patient care
Pathology
10
This expanded responsibility comes with challenges and
expectations
Quality Control is largely assumed
Treating physician assumes test is done right; pathologist assumes specimen was handled appropriately
11
State of the art QC practices for molecular diagnostic tests are lagging
• New and rapidly evolving technologies• High expectations of accuracy for once-in-
a-lifetime genetic tests• Lack of quality control materials• Lack of quantitative test system outputs• The almost daily appearance of new
genetic test targets
Based on information from GeneTests, molecular genetic testing is presently performed for at least
1,000 diseases
Accuracy and reliability of molecular Dx tests can be influenced by many factors:– Diversity of testing methodology– Rate of technology evolution– Variety of applications– Regional differences in the tests
offered and the populations tested– Low-volume testing for many
conditions and genetic targets– Lack of standardization inherent in
in-house methods developed by individual laboratories
12
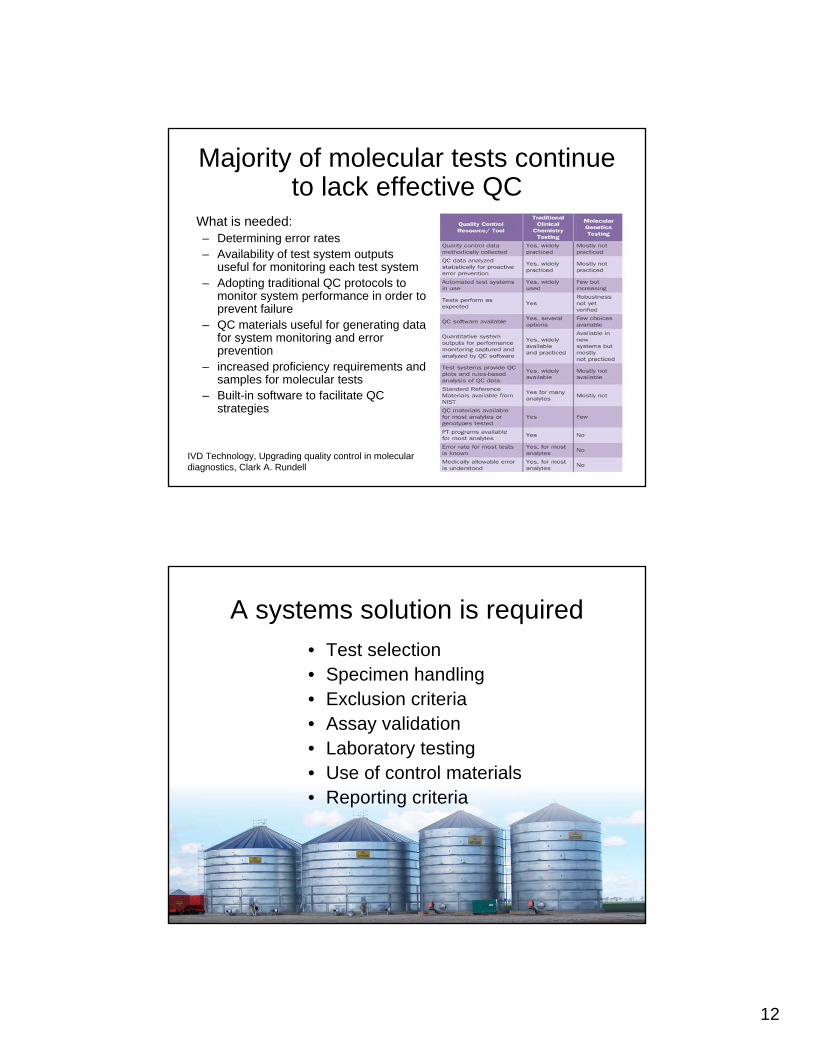
Majority of molecular tests continue to lack effective QC
What is needed:– Determining error rates– Availability of test system outputs
useful for monitoring each test system– Adopting traditional QC protocols to
monitor system performance in order to prevent failure
– QC materials useful for generating data for system monitoring and error prevention
– increased proficiency requirements and samples for molecular tests
– Built-in software to facilitate QC strategies
IVD Technology, Upgrading quality control in molecular diagnostics, Clark A. Rundell
A systems solution is required• Test selection• Specimen handling• Exclusion criteria• Assay validation• Laboratory testing• Use of control materials• Reporting criteria
13
Case in Point: HER2
• Results of clinical trials demonstrate significant benefit of HER2 targeted therapy for early stage breast cancer patients
• Results from the same trials show significant variation in HER2 testing
• Current quality assurance methods had not reduced testing variation
• HER2 testing: not simply a special stain; a single observation leads to a major difference in treatment– Testing critical to patient and clinician since trastuzumab is effective
only for patients whose HER2 test is positive– Test interpretation assumed by both clinician and patient to be accurate
• Quantitative HER2 testing is different from the ordinary IHC stains• QA systems and lab accreditation standards not specifically tailored
to ensure accuracy and precision of FISH and IHC HER2 testing– Only about 25% of labs perform technical validation before offering
HER2 testing– Only about 33% of labs offering HER2 testing participate in PT– ~50% of labs that use FDA-approved IHC kits vary from the approved method
Case: HER2 Testing
14
Impact on PatientsInappropriate Treatment
• Up to 18% of patients could receive HER2 targeted therapy unnecessarily
• Delays appropriate treatment• Unnecessary expense ($70,000 –$100,000 per
patient) • Up to 10% of patients may not receive
appropriate HER2 targeted therapy
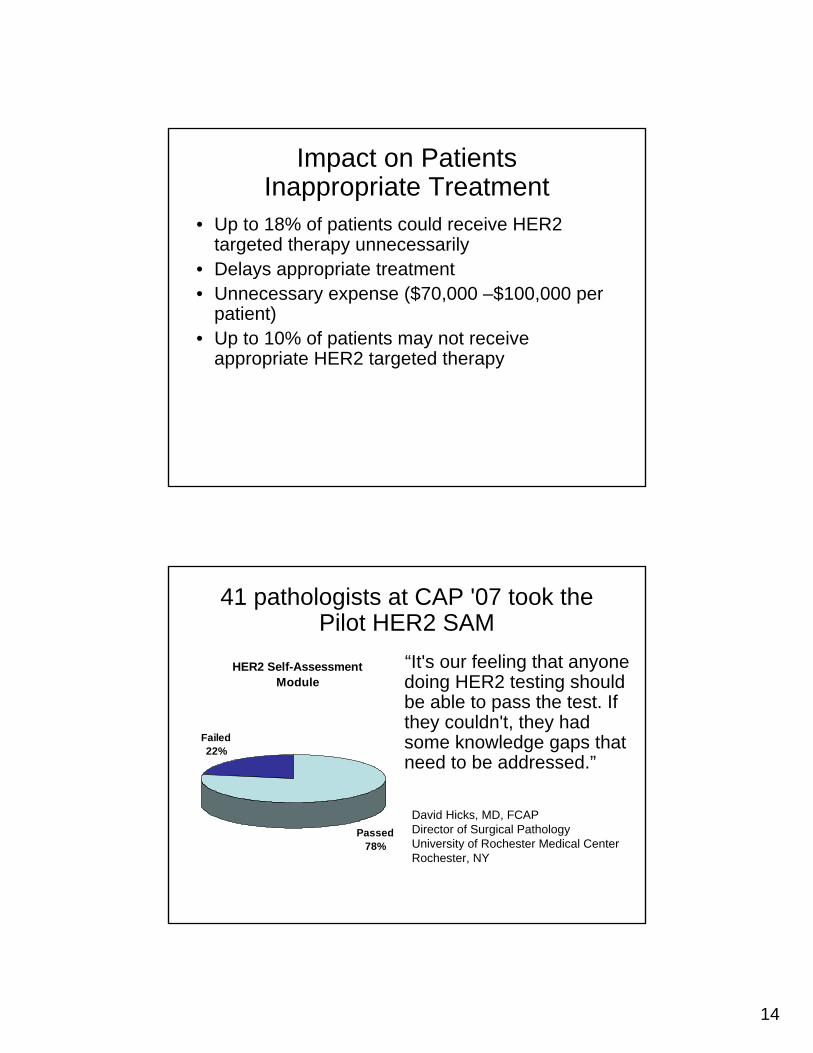
41 pathologists at CAP '07 took the Pilot HER2 SAM
HER2 Self-Assessment Module
Passed78%
Failed22%
“It's our feeling that anyone doing HER2 testing should be able to pass the test. If they couldn't, they had some knowledge gaps that need to be addressed.”
David Hicks, MD, FCAPDirector of Surgical PathologyUniversity of Rochester Medical CenterRochester, NY
15
Pathologists can’t do it alone
Cross specialty communication &
education is essential
CAP & ASCO collaborated on KRAS gene mutation testing
• KRAS normal– No mutation identified– Report will specify assay type and
controls used• KRAS abnormal
– Treatment with anti-EGFR monoclonal antibody therapy not recommended
– Mutation found in codon 12 or 13– Report will specify what mutation was
found, what assay was done, and what controls were used
“Based on systematic reviews of the relevant literature, all patients with metastaticcolorectal carcinoma who are candidates for anti-EGFR antibody therapy should have their tumor tested for KRAS mutations in a CLIA-accredited laboratory.”
CAP: www.cap.org/POETJCO: http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2009.21.9170
16
Opportunity knocks…
“If we are unable to find a way to implement molecular profiling into our practices, surgical pathologists will be
excluded from one of the most exciting and transformational
developments to come around in a long time. And that, in my opinion as
an academic and molecular pathologist, would be a real shame.”
Thomas J. Giordano, MD, PhDUniversity of Michigan
17
“Never forget that it is not a pneumonia, but a
pneumonic man who is your patient. Not a typhoid fever, but a typhoid man”
~William Withey Gull
Modern HealthcareA Crain Communication Publication
Hot Topic: The Questionable Future of the Microscope / Page 7
THE ONLY HEALTHCARE BUSINESS NEWS WEEKLY JANUARY 6, 2020
CAP leads caucus on standards development worldwide / Page 23
Pathologists take center stage in patient care
Pathologists take center stage in patient care
Disease diagnosis and treatment determination using molecular imaging from your local pathologist / Page 45
Modern HealthcareA Crain Communication Publication
Hot Topic: The Questionable Future of the Microscope / Page 7
THE ONLY HEALTHCARE BUSINESS NEWS WEEKLY JANUARY 6, 2020
CAP leads caucus on standards development worldwide / Page 23
Pathologists take center stage in patient care
Pathologists take center stage in patient care
Disease diagnosis and treatment determination using molecular imaging from your local pathologist / Page 45
Who will be writing your prescriptions
in the future?







