
ORIGINAL ARTICLE
White-to-white corneal diameter, pupil diameter, central cornealthickness and thinnest corneal thickness values of emmetropicsubjects
Juan A. Sanchis-Gimeno • Daniel Sanchez-Zuriaga •
Francisco Martinez-Soriano
Received: 29 November 2010 / Accepted: 11 October 2011 / Published online: 22 October 2011
� Springer-Verlag 2011
Abstract
Purpose This report assesses white-to-white corneal
diameter, pupil diameter, central corneal thickness and
thinnest corneal thickness values in a large sample of
emmetropic subjects.
Methods Three hundred and seventy-nine eyes of 379
young healthy emmetropic subjects were analyzed by means
of scanning-slit corneal topography. The age of the subjects
ranged from 18 to 53 years (mean ± SD = 29 ± 7). The
mean of five consecutive measurements of the central
corneal thickness, the thinnest corneal thickness, the white-
to-white corneal diameter, and the photopic pupil diameter
was recorded.
Results The central corneal thickness ranged from 528 to
588 lm; the thinnest corneal thickness ranged from 504 to
574 lm; the white-to-white corneal diameter ranged from
11.5 to 12.3 mm; and the pupil diameter ranged from 3.0 to
4.7 mm. The central and the thinnest corneal thickness
were positively correlated (r = 0.94, p \ 0.001), and the
pupil diameter was significantly higher in females
(p \ 0.001).
Conclusions This study shows that there are no differ-
ences in white-to-white corneal diameter, central corneal
thickness, and thinnest corneal thickness between emme-
tropic females and males. However, pupil diameters are
greater in emmetropic females.
Keywords Corneal thickness �White-to-white diameter �Pupil diameter � Scanning-slit corneal topography �Ocular surface
Introduction
An anatomist’s ‘‘definition of the normal eye’’ is different
from an ophthalmologist’s. From an ophthalmologist’s
point of view the normal eye is the non-pathological eye,
not the emmetropic eye as accepted by anatomists [21].
Assessment of ocular dimensions is essential for oph-
thalmic surgeons, because it must be measured before
scheduling excimer laser refractive surgery and cataract
surgery [8, 16]. Cataract is the world’s leading cause of
blindness [28], and excimer laser refractive surgery has
been reported to be performed on more than six million
people worldwide [10]. This is why studies of ocular
dimensions are usually carried out in these patients and not
in emmetropic subjects.
The analysis of distribution of refractive errors has
detected that emmetropia may be more prevalent than
myopia and hyperopia in European populations [14]
although different studies carried out in Asian populations
have found that hyperopia and myopia are more prevalent
than emmetropia [13, 27].
Previous studies analyzed the ocular axial length values
and corneal thickness values of the emmetropic and non-
emmetropic eye [19, 20, 22, 23], but based on a biblio-
graphic search using MEDLINE, we have found no study
dedicated exclusively to the white-to-white corneal diam-
eter and pupil diameter in healthy emmetropic eyes (i.e.,
those subjects with spherical equivalent refraction
of ±0.5 diopters). Thus, currently, there is a lack of
information on the quantitative ocular anatomy of
J. A. Sanchis-Gimeno (&) � D. Sanchez-Zuriaga �F. Martinez-Soriano
Department of Anatomy and Human Embryology,
Faculty of Medicine, University of Valencia,
Av. Blasco Ibanez, 15, Valencia 46010, Spain
e-mail: [email protected]
123
Surg Radiol Anat (2012) 34:167–170
DOI 10.1007/s00276-011-0889-4
emmetropic eyes, because ocular size studies are not usu-
ally performed on these eyes. Moreover, all these subjects
are candidates for developing cataracts in the future so it is
important to know the quantitative ocular anatomy of the
emmetropic eye.
In the light of the above, the present paper analyzes the
white-to-white corneal diameter, pupil diameter, central
corneal thickness, and thinnest corneal thickness values of
a large sample of healthy emmetropic subjects.
Methods
We carried out a prospective study involving 379 eyes of
379 healthy emmetropic subjects. Inclusion criteria were
healthy emmetropic subjects (volunteers with manifest
sphere and manifest cylinder of ±0.5 diopters) with best
corrected visual acuity C20/20.
Measurements of the white-to-white, pupil diameter,
central corneal thickness, and thinnest corneal thickness
were carried out by means of scanning-slit corneal topog-
raphy (SSCT), as described previously [4, 19, 22], with the
Orbscan topography system II (Orbscan, Inc., Salt Lake
City, UT). SSCT was used on all patients, with an acoustic
equivalent factor of 0.92 as recommended by the manu-
facturer. All the procedures were conducted in accordance
with the principles of the World Medical Association’s
Declaration of Helsinki. Detailed consent forms were
obtained from each of the patients.
Scanning-slit corneal topography makes it possible to
determine over 9,000 data points in 1.5 s, mapping the
entire corneal surface without touching it. With SSCT two
scanning slit-lamps project beams at 458 to the right or
left of the instrument axis. Forty images—20 with slit
beams projected from the left and 20 from the right—are
obtained at two intervals, each lasting 0.7 s. Surface data
points are measured on the x, y, and z axes. It creates true
3-D maps from the anterior segment of the eye using
measurements based on the Scheimpflug principle [17].
SSCT measures anterior and posterior corneal elevation
(relative to a best-fit sphere), surface curvature, pupil
diameter, white-to-white diameter, and corneal thickness
values using a scanning-slit mechanism. The corneal
thickness is calculated by measuring the distance in ele-
vation between the anterior and posterior surfaces of the
cornea [17]. During examination, the patient’s chin is
positioned on the chin rest and the forehead against the
forehead strap. The volunteers are asked to look at a
blinking red light coaxial to the imaging system while the
tracking system measures involuntary eye movements
during the examination. The images of the cornea are
taken using a placido disc, and are shown on the screen of
the instrument.
The mean of five consecutive SSCT measurements was
obtained for each parameter. All ocular measurements were
carried out from 10 a.m. to 1 p.m. During examination the
temperature ranged from 18 to 228C, and the relative
humidity ranged from 38 to 45%. All the measurements
were performed in a well-lit room, this is to say, under
photopic conditions.
Only one eye per subject was contemplated for the
statistical analysis. The eye analyzed was chosen at ran-
dom. The Kolmogorov–Smirnov test, Student’s t-test and
Pearson’s correlation coefficients were applied. P values
less than 0.05 were considered to be statistically
significant.
Results
The mean age of the subjects analyzed was 29 ± 7 (range
18–53 years). One hundred eighty-one subjects were
female (mean age 29 ± 7 years, range 18–49 years) and
198 male (mean age 30 ± 7 years, range 18–53 years).
There were no significant differences in the mean age
between females and males (p = 0.312; Student’s t-test).
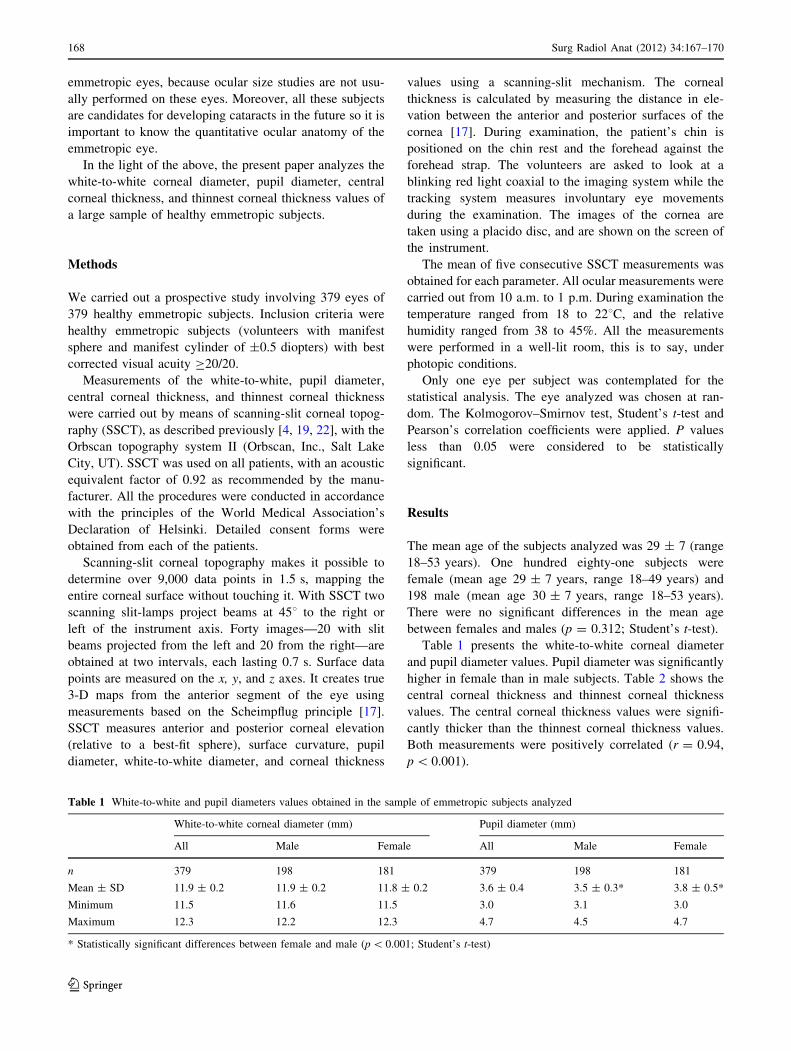
Table 1 presents the white-to-white corneal diameter
and pupil diameter values. Pupil diameter was significantly
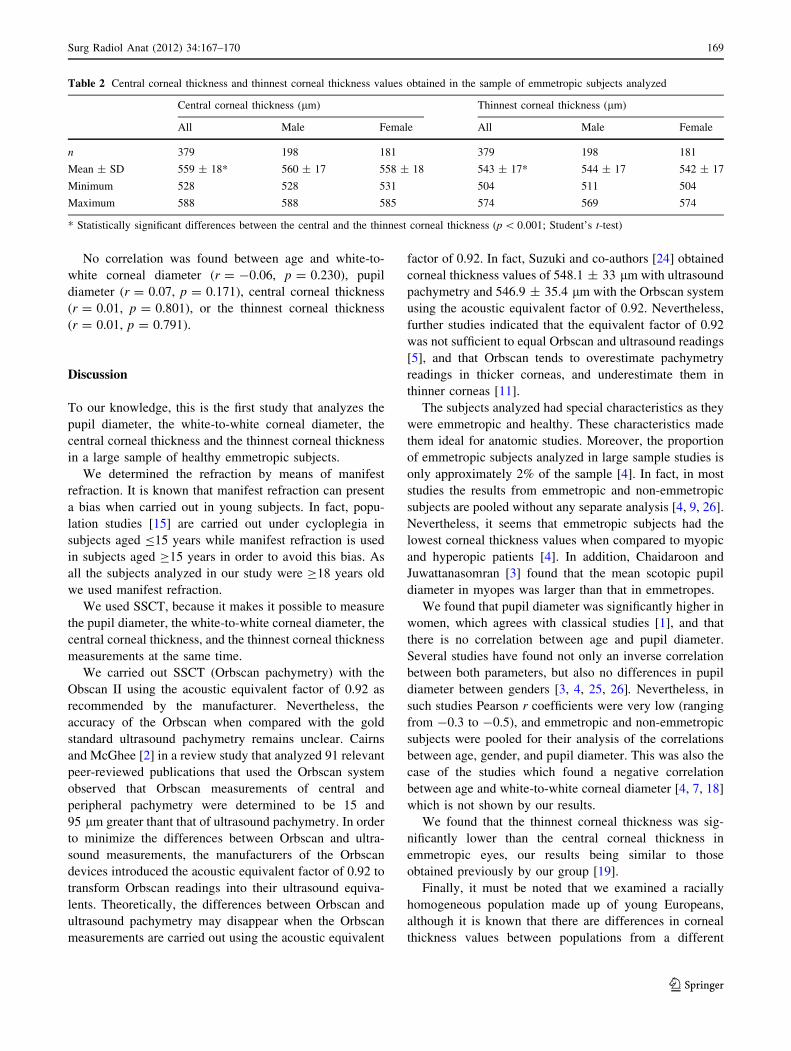
higher in female than in male subjects. Table 2 shows the
central corneal thickness and thinnest corneal thickness
values. The central corneal thickness values were signifi-
cantly thicker than the thinnest corneal thickness values.
Both measurements were positively correlated (r = 0.94,
p \ 0.001).
Table 1 White-to-white and pupil diameters values obtained in the sample of emmetropic subjects analyzed
White-to-white corneal diameter (mm) Pupil diameter (mm)
All Male Female All Male Female
n 379 198 181 379 198 181
Mean ± SD 11.9 ± 0.2 11.9 ± 0.2 11.8 ± 0.2 3.6 ± 0.4 3.5 ± 0.3* 3.8 ± 0.5*
Minimum 11.5 11.6 11.5 3.0 3.1 3.0
Maximum 12.3 12.2 12.3 4.7 4.5 4.7
* Statistically significant differences between female and male (p \ 0.001; Student’s t-test)
168 Surg Radiol Anat (2012) 34:167–170
123
No correlation was found between age and white-to-
white corneal diameter (r = -0.06, p = 0.230), pupil
diameter (r = 0.07, p = 0.171), central corneal thickness
(r = 0.01, p = 0.801), or the thinnest corneal thickness
(r = 0.01, p = 0.791).
Discussion
To our knowledge, this is the first study that analyzes the
pupil diameter, the white-to-white corneal diameter, the
central corneal thickness and the thinnest corneal thickness
in a large sample of healthy emmetropic subjects.
We determined the refraction by means of manifest
refraction. It is known that manifest refraction can present
a bias when carried out in young subjects. In fact, popu-
lation studies [15] are carried out under cycloplegia in
subjects aged B15 years while manifest refraction is used
in subjects aged C15 years in order to avoid this bias. As
all the subjects analyzed in our study were C18 years old
we used manifest refraction.
We used SSCT, because it makes it possible to measure
the pupil diameter, the white-to-white corneal diameter, the
central corneal thickness, and the thinnest corneal thickness
measurements at the same time.
We carried out SSCT (Orbscan pachymetry) with the
Obscan II using the acoustic equivalent factor of 0.92 as
recommended by the manufacturer. Nevertheless, the
accuracy of the Orbscan when compared with the gold
standard ultrasound pachymetry remains unclear. Cairns
and McGhee [2] in a review study that analyzed 91 relevant
peer-reviewed publications that used the Orbscan system
observed that Orbscan measurements of central and
peripheral pachymetry were determined to be 15 and
95 lm greater thant that of ultrasound pachymetry. In order
to minimize the differences between Orbscan and ultra-
sound measurements, the manufacturers of the Orbscan
devices introduced the acoustic equivalent factor of 0.92 to
transform Orbscan readings into their ultrasound equiva-
lents. Theoretically, the differences between Orbscan and
ultrasound pachymetry may disappear when the Orbscan
measurements are carried out using the acoustic equivalent
factor of 0.92. In fact, Suzuki and co-authors [24] obtained
corneal thickness values of 548.1 ± 33 lm with ultrasound
pachymetry and 546.9 ± 35.4 lm with the Orbscan system
using the acoustic equivalent factor of 0.92. Nevertheless,
further studies indicated that the equivalent factor of 0.92
was not sufficient to equal Orbscan and ultrasound readings
[5], and that Orbscan tends to overestimate pachymetry
readings in thicker corneas, and underestimate them in
thinner corneas [11].
The subjects analyzed had special characteristics as they
were emmetropic and healthy. These characteristics made
them ideal for anatomic studies. Moreover, the proportion
of emmetropic subjects analyzed in large sample studies is
only approximately 2% of the sample [4]. In fact, in most
studies the results from emmetropic and non-emmetropic
subjects are pooled without any separate analysis [4, 9, 26].
Nevertheless, it seems that emmetropic subjects had the
lowest corneal thickness values when compared to myopic
and hyperopic patients [4]. In addition, Chaidaroon and
Juwattanasomran [3] found that the mean scotopic pupil
diameter in myopes was larger than that in emmetropes.
We found that pupil diameter was significantly higher in
women, which agrees with classical studies [1], and that
there is no correlation between age and pupil diameter.
Several studies have found not only an inverse correlation
between both parameters, but also no differences in pupil
diameter between genders [3, 4, 25, 26]. Nevertheless, in
such studies Pearson r coefficients were very low (ranging
from -0.3 to -0.5), and emmetropic and non-emmetropic
subjects were pooled for their analysis of the correlations
between age, gender, and pupil diameter. This was also the
case of the studies which found a negative correlation
between age and white-to-white corneal diameter [4, 7, 18]
which is not shown by our results.
We found that the thinnest corneal thickness was sig-
nificantly lower than the central corneal thickness in
emmetropic eyes, our results being similar to those
obtained previously by our group [19].
Finally, it must be noted that we examined a racially
homogeneous population made up of young Europeans,
although it is known that there are differences in corneal
thickness values between populations from a different
Table 2 Central corneal thickness and thinnest corneal thickness values obtained in the sample of emmetropic subjects analyzed
Central corneal thickness (lm) Thinnest corneal thickness (lm)
All Male Female All Male Female
n 379 198 181 379 198 181
Mean ± SD 559 ± 18* 560 ± 17 558 ± 18 543 ± 17* 544 ± 17 542 ± 17
Minimum 528 528 531 504 511 504
Maximum 588 588 585 574 569 574
* Statistically significant differences between the central and the thinnest corneal thickness (p \ 0.001; Student’s t-test)
Surg Radiol Anat (2012) 34:167–170 169
123

ethnic origin [6, 12]. According to these studies, different
results would probably be obtained if another population of
emmetropic subjects was analyzed.
In conclusion, the present study has revealed the quan-
titative anatomy of the white-to-white corneal diameter,
pupil diameter, central corneal thickness, and thinnest
corneal thickness of healthy emmetropic subjects, which
shows that the photopic pupil diameter is greater in
emmetropic women. Nevertheless, further research is
necessary to detect if there are differences in such values
between emmetropic, myopic, and hyperopic subjects, and
between populations with different ethnic origins.
Acknowledgments This study was supported by a grant from the
University of Valencia (UV-3691).
Conflict of interest None.
References
1. Alexandridis E (1985) The Pupil. Springer-Verlag, New York,
p 117
2. Cairns G, McGhee CN (2005) Orbscan computerized topography:
attributes, applications, and limitations. J Cataract Refract Surg
31:205–220 (Review)
3. Chaidaroon W, Juwattanasomran W (2002) Colvard pupillometer
measurement of scotopic pupil diameter in emmetropes and
myopes. Jpn J Ophthalmol 46:640–644
4. Cosar BC, Sener BA (2003) Orbscan corneal topography system
in evaluating the anterior structures of the human eye. Cornea
22:118–121
5. Doughty MJ, Jonuscheit S (2010) The orbscan acoustic (correc-
tion) factor for central corneal thickness measures of normal
human corneas. Eye Contact Lens 36:106–115
6. Doughty MJ, Zaman ML (2000) Human corneal thickness and its
impact on intraocular pressure measures: a review and meta-
analysis approach. Surv Ophthalmol 44:367–408
7. Fea AM, Annetta F, Cirillo S, Campanella D, De Giuseppe M,
Regge D, Grignolo FM (2005) Magnetic resonance imaging and
Orbscan assessment of the anterior chamber. J Cataract Refract
Surg 31:1713–1718
8. Findl O (2005) Biometry and intraocular lens power calculation.
Curr Opin Ophthalmol 16:61–64 (Review)
9. Goldsmith JA, Li Y, Chalita MR, Westphal V, Patil CA, Rollins
AM, Izatt JA, Huang D (2005) Anterior chamber width mea-
surement by high-speed optical coherence tomography. Oph-
thalmology 112:238–244
10. Hammond MD, Madigan WP Jr, Bower KS (2005) Refractive
surgery in the United States Army, 2000–2003. Ophthalmology
112:184–190
11. Hashemi H, Roshani M, Mehravaran S, Parsafar H, Yazdani K
(2007) Effect of corneal thickness on the agreement between
ultrasound and Orbscan II pachymetry. J Cataract Refract Surg
33:1694–1700
12. La Rosa FA, Gross RL, Orengo-Nania S (2001) Central corneal
thickness of Caucasian and African Americans in glaucomatous
and nonglaucomatous populations. Arch Ophthalmol 119:23–27
13. Liang YB, Wong TY, Sun LP, Tao QS, Wang JJ, Yang XH,
Xiong Y, Wang NL, Friedman DS (2009) Refractive errors in a
rural Chinese adult population: the Handan eye study. Ophthal-
mology 116:2119–2127
14. Montes-Mico R, Ferrer-Blasco T (2000) Distribution of refractive
errors in Spain. Doc Ophthalmol 101:25–33
15. Ostadimoghaddam H, Fotouhi A, Hashemi H, Yekta A, Heravian
J, Rezvan F, Ghadimi H, Rezvan B, Khabazkhoob M (2011)
Prevalence of the refractive errors by age and gender in Mashhad,
Iran: the Mashhad eye study. Clin Exp Ophthalmol. doi:
10.1111/j.1442-9071.2011.02584.x
16. Price FW, Koller DL, Price MO (1999) Central corneal pachy-
metry in patients undergoing laser in situ keratomileusis. Oph-
thalmology 106:2216–2220
17. Rabsilber TM, Becker KA, Frisch IB, Auffarth GU (2003)
Anterior chamber depth in relation to refractive status measured
with the Orbscan II topography system. J Cataract Refract Surg
29:2115–2121
18. Rufer F, Schroder A, Erb C (2005) White-to-white corneal
diameter: normal values in healthy humans obtained with the
Orbscan II topography system. Cornea 24:259–261
19. Sanchis-Gimeno JA, Herrera M, Lleo-Perez A, Alonso L, Rahhal
MS (2006) Quantitative corneal anatomy in emmetropic subjects.
Eur J Ophthalmol 16:235–238
20. Sanchis-Gimeno JA, Herrera M, Sanchez-del-Campo F, Marti-
nez-Soriano F (2006) Differences in ocular dimensions between
normal and dry eyes. Surg Radiol Anat 28:267–270
21. Sanchis-Gimeno JA, Lleo-Perez A, Alonso L, Rahhal MS, Mar-
tinez-Soriano F (2005) Corneal endothelial cell density decreases
with age in emmetropic eyes. Histol Histopathol 20:423–427
22. Sanchis-Gimeno JA, Lleo-Perez A, Alonso L, Rahhal MS, Mar-
tinez-Soriano F (2004) Anatomic study of the corneal thickness
of young emmetropic subjects. Cornea 23:669–673
23. Selovic A, Juresa V, Ivankovic D, Malcic D, Bobonj GS (2005)
Relationship between axial length of the emmetropic eye and the
age, body height, and body weight of schoolchildren. Am J Hum
Biol 17:173–177
24. Suzuki S, Oshika T, Oki K, Sakabe I, Iwase A, Amano S, Araie
M (2003) Corneal thickness measurements: scanning-slit corneal
topography and noncontact specular microscopy versus ultrasonic
pachymetry. J Cataract Refract Surg 29:1313–1318
25. Twa MD, Bailey MD, Hayes J, Bullimore M (2004) Estimation
of pupil size by digital photography. J Cataract Refract Surg
30:381–389
26. Winn B, Whitaker D, Elliott DB, Phillips NJ (1994) Factors
affecting light-adapted pupil size in normal human subjects.
Invest Ophthalmol Vis Sci 35:1132–1137
27. Yekta AA, Fotouhi A, Khabazkhoob M, Hashemi H, Ostadi-
moghaddam H, Heravian J, Mehravaran S (2009) The prevalence
of refractive errors and its determinants in the elderly population
of Mashhad, Iran. Ophthalmic Epidemiol 16:198–203
28. Yorston D (2005) High-volume surgery in developing countries.
Eye 19:1083–1089
170 Surg Radiol Anat (2012) 34:167–170
123







