Wardlaw’s
PERSPECTIVES IN
NutritionUpdated with 2015–2020 Dietary Guidelines for Americans
Final PDF to printer
Final PDF to printer
Wardlaw’s Perspectives in
CAROL BYRD-BREDBENNERRutgers, The State University of New Jersey GAILE MOESeattle Pacific University JACQUELINE BERNING University of Colorado at Colorado Springs DANITA KELLEYWestern Kentucky University
Updated with 2015–2020 Dietary Guidelines for Americans
Final PDF to printer
WARDLAW’S PERSPECTIVES IN NUTRITION Updated with 2015-2020 Dietary Guidelines for Americans,
TENTH EDITION
Published by McGraw-Hill Education, 2 Penn Plaza, New York, NY 10121. Copyright © 2016 by
McGraw-Hill Education. All rights reserved. Printed in the United States of America. Previous editions
© 2013, 2009, and 2007. No part of this publication may be reproduced or distributed in any form or by any
means, or stored in a database or retrieval system, without the prior written consent of McGraw-Hill Education,
including, but not limited to, in any network or other electronic storage or transmission, or broadcast for
distance learning.
Some ancillaries, including electronic and print components, may not be available to customers outside the
United States.
This book is printed on acid-free paper.
1 2 3 4 5 6 7 8 9 DOW 21 20 19 18 17 16
ISBN 978-1-259-91837-7
MHID 1-259-91837-8
Senior Vice President, Products & Markets: Kurt L. Strand
Vice President, General Manager, Products & Markets: Marty Lange
Vice President, Content Design & Delivery: Kimberly Meriwether David
Managing Director: Michael Hackett
Brand Managers: Amy Reed/Marija Magner
Director, Product Development: Rose Koos
Director of Digital Content: Michael G. Koot, PhD
Product Developer: Darlene M. Schueller
Marketing Manager: Kristine Rellihan
Digital Product Analyst: Christine Carlson
Director, Content Design & Delivery: Linda Avenarius
Program Manager: Angela R. FitzPatrick
Content Project Managers: MaryJane Lampe/Brent dela Cruz
Buyer: Jennifer Pickel
Design: Matt Backhaus
Content Licensing Specialists: Lori Hancock/Lorraine Buczek
Cover Image: © Adrianna Williams/Corbis
Compositor: SPi Global
Printer: R. R. Donnelley
All credits appearing on page or at the end of the book are considered to be an extension of the copyright page.
Library of Congress Cataloging-in-Publication Data
Names: Wardlaw, Gordon M. | Byrd-Bredbenner, Carol. | Moe, Gaile. | Berning,
Jacqueline R. | Kelley, Danita S.
Title: Wardlaw’s perspectives in nutrition.
Other titles: Perspectives in nutrition
Description: Tenth edition, updated with 2015-2020 dietary guidelines for
Americans / Carol Byrd-Bredbenner, Rutgers, The State University of New
Jersey, Gaile Moe, Seattle Pacific University, Jacqueline Berning,
University of Colorado at Colorado Springs, Danita Kelley, Western
Kentucky University. | New York, NY: McGraw-Hill Education, [2016] |
Includes bibliographical references and index.
Identifiers: LCCN 2016009387 | ISBN 9781259918377 (alk. paper)
Subjects: LCSH: Nutrition.
Classification: LCC QP141 .W38 2016b | DDC 612.3—dc23 LC record available at http://lccn.loc.gov/2016009387
The Internet addresses listed in the text were accurate at the time of publication. The inclusion of a website
does not indicate an endorsement by the authors or McGraw-Hill Education, and McGraw-Hill Education does
not guarantee the accuracy of the information presented at these sites.
www.mhhe.com
Final PDF to printer
v
PART 1 NUTRITION BASICS
1 The Science of Nutrition 22 Tools of a Healthy Diet 383 The Food Supply 724 Human Digestion and Absorption 116
PART 2 ENERGY-YIELDING NUTRIENTS AND ALCOHOL
5 Carbohydrates 1546 Lipids 1907 Proteins 2268 Alcohol 260
PART 3 METABOLISM AND ENERGY BALANCE
9 Energy Metabolism 28410 Energy Balance, Weight Control,
and Eating Disorders 31811 Nutrition, Exercise, and Sports 364
PART 4 VITAMINS AND MINERALS
12 The Fat-Soluble Vitamins 40213 The Water-Soluble Vitamins 43814 Water and Major Minerals 48815 Trace Minerals 540
PART 5 NUTRITION APPLICATIONS IN THE LIFE CYCLE
16 Nutritional Aspects of Pregnancy and Breastfeeding 57617 Nutrition during the Growing Years 61618 Nutrition during the Adult Years 656
Brief Contents
Final PDF to printer
vi
Meet the Author TeamCaro l Byrd-Bredbenner, Ph .D. , R .D. , FAND, received her doctorate from Pennsylvania State University. Currently, she is Professor in the Nutritional Sciences Department at Rutgers, The State University of New Jersey. She teaches a wide range of undergraduate and graduate nutrition courses. Her research interests focus on investigating environmental factors that affect dietary choices and health outcomes. Dr. Byrd-Bredbenner has authored numerous nutrition texts, journal articles, and computer software packages. She has received teaching awards from the American Dietetic Association (now called the Academy of Nutrition and Dietetics), Society for Nutrition Education, and U.S. Department of Agriculture. She was the recipient of the American Dietetic Association’s Anita Owen Award for Innovative Nutrition Education Programs. She also was a Fellow of the United Nations, World Health Organization at the WHO Collaborating Center for Nutrition
Education, University of Athens, Greece. She enjoys exploring food and culinary customs, traveling, diving, and gardening.
G a i l e L . M o e , P h . D . , R . D . , earned a doctorate in nutritional sciences at the University of Washington. She is a registered dietitian who has worked in clinical nutrition, research, and management, as well as education. She is currently Professor and Director of the Didactic Program in Dietetics at Seattle Pacific University. She has published in peer-reviewed journals in the areas of nutrition and cancer and media reporting of nutrition research. Gaile enjoys swimming, cycling, walking, and hiking, along with learning about culinary traditions, food, and food policy.
J a c q u e l i n e R . B e r n i n g , P h . D . , R . D . , C S S D , earned her doctorate in nutrition from Colorado State University in Fort Collins, Colorado. She is currently Professor and Chair of the Health Science Department at the University of Colorado at Colorado Springs
(UCCS), where she has won numerous teaching awards. Dr. Berning is published in the area of sports dietetics and was the sport dietitian for the Denver Broncos for over 25 years, Cleveland Indians for 18 years, and Colorado Rockies for 10 years. Currently she is the sport dietitian for UCCS athletics and US Lacrosse. She is active in the Academy of Nutrition and Dietetics, where she served as the chair of the Program Planning Committee for FNCE and is currently Chair of the Appeals Committee. In 2014, Dr. Berning was awarded the Mary Abbot Hess Award for Culinary Events for teaching the University of Colorado football team how to grocery shop and cook. Additionally, she served 6 years as an ADA spokesperson and is a former chair of the Sports, Cardiovascular, and Wellness Nutritionists dietetics practice group. She enjoys walking, hiking, and gardening.
D a n i t a S a x o n Ke l l e y, P h . D . , R . D . , earned her doctorate in nutritional sciences from the University of Kentucky. She serves as Associate Dean of the College of Health and Human Services and is a Professor in the Family and Consumer Sciences Department at Western Kentucky University. Previously, Dr. Kelley was Director of the Didactic Program in Dietetics at Western Kentucky University. She is a Past President of the Board of Directors for the Kentucky Academy of Nutrition and Dietetics. Her scholarly work has focused on healthy eating of adolescents, communication skills of dietetic students, histaminergic activity and regulation of food intake, and dietary restriction effects on the antioxidant defense system. She has received awards for teaching from the Kentucky Academy of Nutrition and Dietetics and the Dietetic Educators of Practitioners of the Academy of Nutrition and Dietetics. She enjoys singing, walking her dog, cheering for her family in water-ski competitions, and watching her children participate in athletic and musical endeavors.
Final PDF to printer

vii
Preface
Welcome to the Tenth Edition of
Wardlaw’s Perspectives in Nutrition Updated with
2015–2020 Dietary Guidelines for Americans
Wardlaw’s Perspectives in Nutrition has the richly deserved reputation of providing an accurate,
current, in-depth, and thoughtful introduction to the dynamic field of nutrition. We have endeavored
to build upon this tradition of excellence by enriching this edition for both students and instructors.
Our passion for nutrition, our genuine desire to promote student learning, and our commitment to
scientific accuracy, coupled with constructive comments from instructors and students, guided us
in this effort. Our primary goal has been to maintain the strengths and philosophy that have been
the hallmark of this book yet continue to enhance the accessibility of the science content and the
application of materials for today’s students.
Nutrition profoundly affects all of our lives every day. For the authors, as well as many other
educators, researchers, and clinicians, this is the compelling reason for devoting our careers to this
dynamic field. The rapid pace of nutrition research and provocative (and sometimes controversial)
findings challenge us all to stay abreast of the latest research and understand its implications for
health. We invite you to share with us topics that you believe deserve greater or less attention in
the next edition.
To your health!
Carol Byrd-Bredbenner
Gaile Moe
Jacqueline Berning
Danita Kelley
Final PDF to printer
viii
McGraw-Hill LearnSmart® is one of the most effective and successful adaptive learning resources available on the market today. More than 2 million students have answered more than 1.3 billion questions in LearnSmart since 2009, making it the most widely used and intelligent adaptive study tool that’s proven to strengthen memory recall, keep students in class, and boost grades. Students using LearnSmart are 13% more likely to pass their classes and 35% less likely to drop out.
LearnSmart continuously adapts to each student’s needs by building an individual learning path so students study smarter and retain more knowledge. Turnkey reports provide valuable insight to instructors, so precious class time can be spent on higher-level concepts and discussion.
Personalized, Adaptive Learning
Fueled by LearnSmart—the most widely used and intelligent adaptive learning resource—SmartBook® is the first and only adaptive reading experience available today.
Distinguishing what students know from what they don’t, and honing in on concepts they are most likely to forget, SmartBook personalizes content for each student in a continuously adapting reading experience. Reading is no longer a passive and linear experience but an engaging and dynamic one where students are more likely to master and retain important concepts, coming to class better prepared. Valuable reports provide instructors insight into how students are progressing through textbook content and are useful for shaping in-class time or assessment.
As a result of the adaptive reading experience found in SmartBook, students are more likely to retain knowledge, stay in class, and get better grades.
“LearnSmart has helped me to understand exactly what concepts I do not yet understand. I feel like after I complete a module I have a deeper understanding of the material and a stronger base to then build on to apply the material to more challenging concepts.”
Student
Final PDF to printer
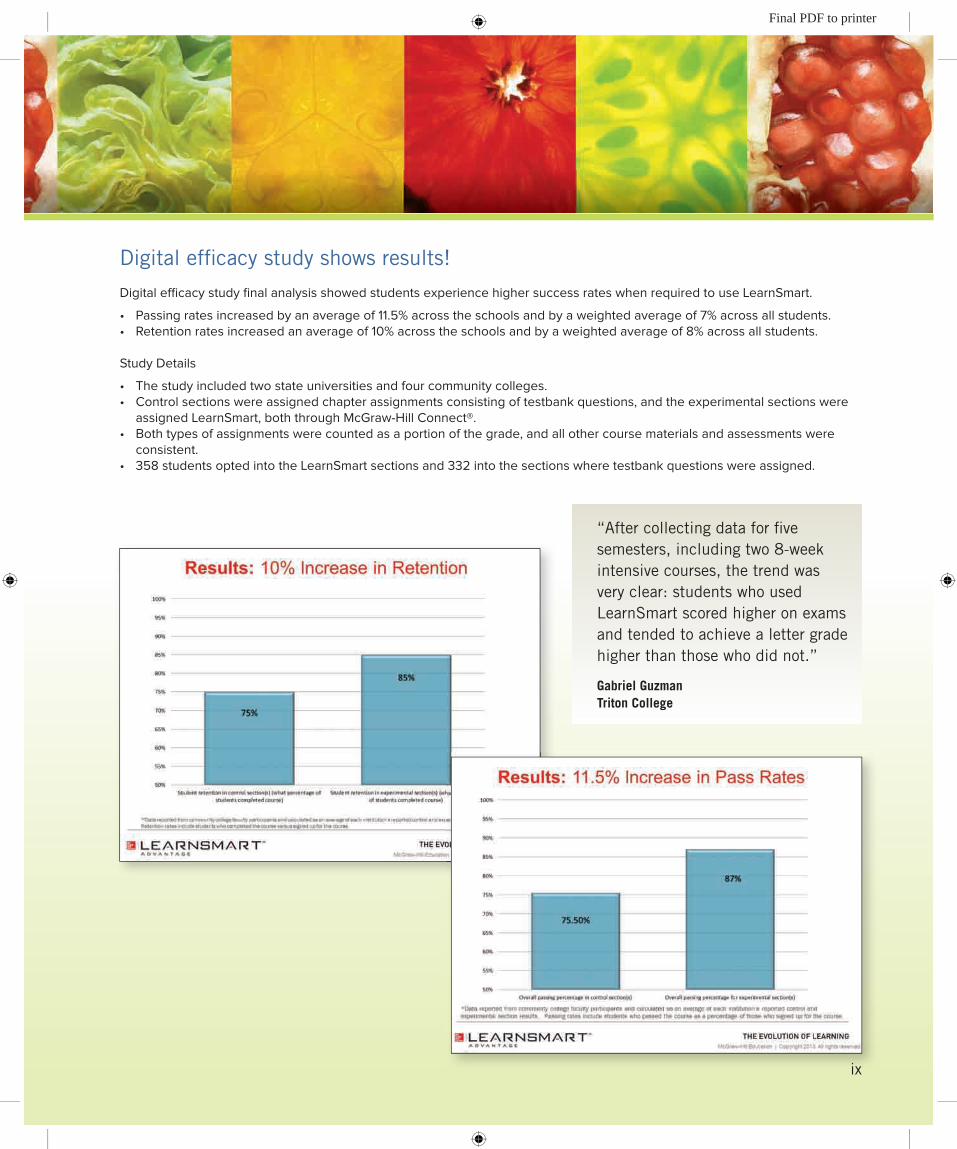
Digital efficacy study shows results!
Digital efficacy study final analysis showed students experience higher success rates when required to use LearnSmart.
• Passingratesincreasedbyanaverageof11.5%acrosstheschoolsandbyaweightedaverageof7%acrossallstudents.• Retentionratesincreasedanaverageof10%acrosstheschoolsandbyaweightedaverageof8%acrossallstudents.
Study Details
• Thestudyincludedtwostateuniversitiesandfourcommunitycolleges.• Controlsectionswereassignedchapterassignmentsconsistingoftestbankquestions, andtheexperimentalsectionswere
assigned LearnSmart, both through McGraw-Hill Connect®.• Bothtypesofassignmentswerecountedasaportionofthegrade,andallothercoursematerialsandassessmentswere
consistent.• 358studentsoptedintotheLearnSmartsectionsand332intothesectionswheretestbankquestionswereassigned.
“After collecting data for five semesters, including two 8-week intensive courses, the trend was very clear: students who used LearnSmart scored higher on exams and tended to achieve a letter grade higher than those who did not.”
Gabriel GuzmanTriton College
ix
Final PDF to printer
x
Connecting Instructors to StudentsSaves students and instructors time while improving performance
McGraw-Hill Connect® Nutrition is a digital teaching and learning environment that saves students and instructors time while improving performance over a variety of critical outcomes.
• Auto-grade assessments and tutorials Instructors can easily create customized assessments that will be automati-
cally graded. All Connect content is created by nutrition instructors, so it is pedagogical, instructional, and at the appropriate level. Interactive ques-tions using high-quality art from the textbook and animations and videos from a variety of sources take students way beyond multiple choice.
• Gather assessment information All Connect questions are tagged to a learning outcome, specific section
and topic, and Bloom’s level for easy tracking of assessment data.
• Access content anywhere, anytime The media-rich eBook allows students to do full text searches, add notes
and highlights, and access their instructor’s shared notes and highlights.
• Streamline lecture creation Presentation tools, such as PowerPoint® lecture outlines, including art,
photos, tables, and animations, allow instructors to customize their lectures.
McGraw-Hill Connect® Insight is a powerful data analytics tool that allows instructors to leverage aggregated information about their courses and students to provide a more personalized teaching and learning experience.
Final PDF to printer
xi
Dietary Analysis Tool
NutritionCalc Plus is a suite of powerful dietary self-assessment tools that help students track their food intake and activity and analyze their diet and health goals. Students and instructors can trust the reliability of the ESHA database while interacting with a robust selection of reports.
LearnSmart Prep® is designed to get students ready for a forthcoming course by quickly and effectively addressing prerequisite knowledge gaps that may cause problems down the road.
McGraw-Hill Campus® integrates all of your digital products from McGraw-Hill Education with your school’s Learning Manage-ment System for quick and easy access to best-in-class content and learning tools.
and Students to Core Concepts
Presentation Tools allow you to customize your lectures
Enhanced Lecture Presentations contain lecture outlines, art, photos, tables, and animations. Fully customizable, complete, and ready to use—these presentations will streamline your work and let you spend less time preparing for lecture!
Editable Art Fully editable (labels and leaders) line art from the text.
Animations Over 50 animations bring key concepts to life, available for instructors and students.
Animation PPTs Animations are truly embedded in PowerPoint for ultimate ease of use! Just copy and paste into your custom slideshow and you’re done!
Digital Lecture CaptureTegrity® is a fully automated lecture capture solution used in traditional, hybrid, “flipped classes” and online courses to record lessons, lectures, and skills.
Final PDF to printer
xii
Our Intended Audience
This textbook was developed for students pursuing nutrition and health science careers as well as those wanting a better understanding of how nutrition affects their lives. Because this course often attracts students from a broad range of majors, we have been careful to include examples and explanations that are relevant to them and to include sufficient sci-entific background to make the science accessible to them. The appendices help students who wish to learn more or need assistance with the science involved in human physiology, chemistry, and metabolism.
To better bridge the span of differing science backgrounds and to enhance student interest and achievement of course objectives, we organized the presentation of the mate-
rial within chapters to flow seamlessly from concrete to abstract learning. In chapters focusing on nutrients, for example, con-crete concepts, such as food sources of the nutrients and recommended intakes, are introduced early in the chapter to create a framework for more abstract concepts, such as functions, digestion, and absorption.
Accurate, Current Science That Engages Students
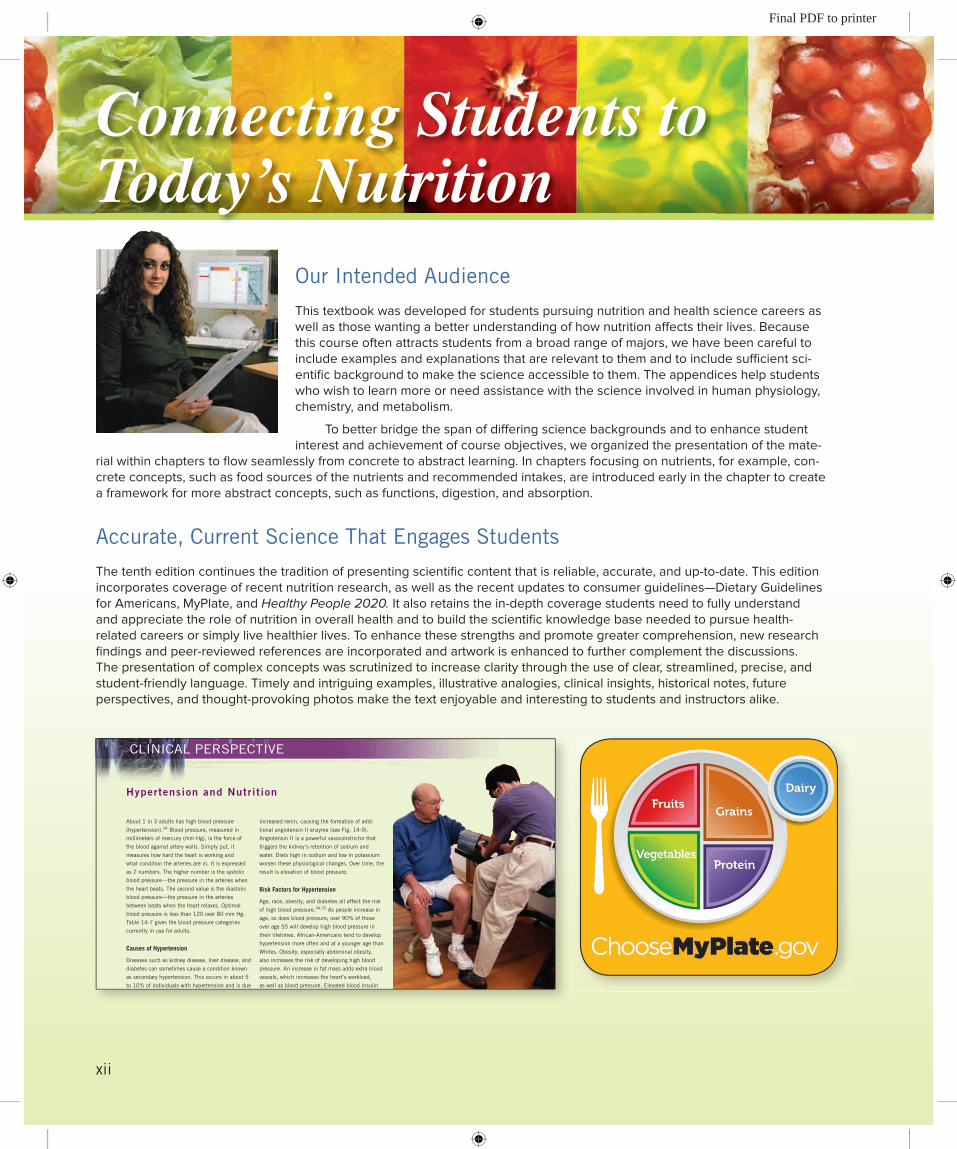
The tenth edition continues the tradition of presenting scientific content that is reliable, accurate, and up-to-date. This edition incorporates coverage of recent nutrition research, as well as the recent updates to consumer guidelines—Dietary Guidelines for Americans, MyPlate, and Healthy People 2020. It also retains the in-depth coverage students need to fully understand and appreciate the role of nutrition in overall health and to build the scientific knowledge base needed to pursue health-related careers or simply live healthier lives. To enhance these strengths and promote greater comprehension, new research findings and peer-reviewed references are incorporated and artwork is enhanced to further complement the discussions. The presentation of complex concepts was scrutinized to increase clarity through the use of clear, streamlined, precise, and student-friendly language. Timely and intriguing examples, illustrative analogies, clinical insights, historical notes, future perspectives, and thought-provoking photos make the text enjoyable and interesting to students and instructors alike.
First Pages
CLINICAL PERSPECTIVE
Hypertension and Nutrit ion
513
increased renin, causing the formation of addi-
tional angiotensin II enzyme (see Fig. 14-9).
Angiotensin II is a powerful vasoconstrictor that
triggers the kidney’s retention of sodium and
water. Diets high in sodium and low in potassium
worsen these physiological changes. Over time, the
result is elevation of blood pressure.
Risk Factors for Hypertension
Age, race, obesity, and diabetes all affect the risk
of high blood pressure.34,35 As people increase in
age, so does blood pressure; over 90% of those
over age 55 will develop high blood pressure in
their lifetimes. African-Americans tend to develop
hypertension more often and at a younger age than
Whites. Obesity, especially abdominal obesity,
also increases the risk of developing high blood
pressure. An increase in fat mass adds extra blood
vessels, which increases the heart’s workload,
as well as blood pressure. Elevated blood insulin
concentration associated with insulin-resistant adi-
pose cells is another reason for this link to obesity.
Insulin increases sodium retention in the body and
accelerates atherosclerosis. An estimated 65% of
people with diabetes also have hypertension.
Hypertension is a serious chronic disease
and health hazard. Recall from Chapter 6 that the
high pressure in the arteries damages the arteries
over time. Eventually, this high pressure damages
the “target organs” of hypertension—the heart,
brain, kidney, and eyes—increasing the risk of
heart attack, stroke, dementia, kidney disease,
and vision loss (approximately 51% of all strokes
and 45% of coronary heart disease events are
caused by high blood pressure).36 Recall from
About 1 in 3 adults has high blood pressure
(hypertension).34 Blood pressure, measured in
millimeters of mercury (mm Hg), is the force of
the blood against artery walls. Simply put, it
measures how hard the heart is working and
what condition the arteries are in. It is expressed
as 2 numbers. The higher number is the systolic
blood pressure—the pressure in the arteries when
the heart beats. The second value is the diastolic
blood pressure—the pressure in the arteries
between beats when the heart relaxes. Optimal
blood pressure is less than 120 over 80 mm Hg.
Table 14-7 gives the blood pressure categories
currently in use for adults.
Causes of Hypertension
Diseases such as kidney disease, liver disease, and
diabetes can sometimes cause a condition known
as secondary hypertension. This occurs in about 5
to 10% of individuals with hypertension and is due
to the underlying disease. Most individuals with
hypertension, however, are classifi ed as having
primary (essential) hypertension. Primary hyper-
tension develops over a period of years in response
to changes in the arteries, kidneys, and sodium/
potassium balance.29,30,35 As we age, our arteries
tend to narrow and become more rigid through
a process called arteriosclerosis. Additionally,
endothelial cells that line the arteries often release
vasoconstrictors, substances that cause the arter-
ies to constrict, in response to arterial damage,
poor blood fl ow, stress, and other factors. Although
these events alone can result in increased blood
pressure, their additive effects on kidney function
increase arterial pressure. The kidney releases
Category SBP (mm Hg) DBP (mm Hg)
Normal ,120 and ,80
Prehypertension 120–139 or 80–89
Hypertension, stage 1 140–159 or 90–99
Hypertension, stage 2 $160 or $100*SBP 5 systolic blood pressure; DBP 5 diastolic blood pressure.Source: Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC 7), NIH Publication Number 03-5231, May 2003.
Category SBP (mm Hg) DBP (mm Hg)
Table 14-7 Classifi cation of Blood Pressure*
The risk of hypertension increases with age.
Pregnancy-induced hypertension (PIH) is
a type of hypertension that can occur during
pregnancy. It can be very dangerous for the
mother and growing fetus. (See Chapter 16.)
The link between blood lead concentrations
and hypertension risk appears to be mediated by
biological factors, including race, ethnicity, and
the form of the protein that carries lead in the
blood. Lead, an environmental toxin, may damage
the kidneys, cause arterial stiffness, or disrupt
vascular function, eventually increasing blood
pressure. Fortunately, lead exposure and blood
levels are decreasing in the U.S.44
Chapter 1 that cardiovascular disease, stroke, and
kidney failure are leading causes of death. Unfor-
tunately, hypertension is often a silent disease,
with no warning signs or symptoms. This is why it
is important to get your blood pressure checked
regularly. If hypertension is detected in its early
stages, treatment is often more effective.
byr21413_ch14_488-539.indd 513 04/09/14 5:00 pm
Connecting Students to Today’s Nutrition
Final PDF to printer
xiii
Applying Nutrition on a Personal Level
A key objective in nearly all introductory courses is for students to apply their new knowledge of nutrition to their own lives. Practical applications clearly linked to nutritional science concepts are woven throughout each chapter to help students apply their knowledge to improving and maintaining their own health and that of others for whom they are responsible, such as future patients or offspring.
• Take Action features in each chapter allow students to examine their own diets and health issues.
• Updatedcase studies showcase realistic scenarios and thought-provoking questions.
• NewdiscussionoftheNutritionalCareProcess(Ch.1)outlines for students the benefits of working with a nutrition professional to improve their health and diet.
Connecting with a Personal Focus
Confirming Pages
171CHAPTER 5 Carbohydrates
5.4 Functions of Carbohydrates in the BodyThe digestible and indigestible carbohydrates in our diets have vital functions in our bodies.3,8
These diverse functions are critical to normal metabolism and overall health.
Digestible Carbohydrates
Most of the digestible carbohydrates in our diets are broken down to glucose. As glucose, they provide a primary source of energy, spare protein from use as an energy source, and prevent ketosis.
Providing Energy
The main function of glucose is to act as a source of energy for body cells. In fact, red blood cells and cells of the central nervous system derive almost all their energy from glucose. Glucose also fuels muscle cells and other body cells, although many of these cells rely on fatty acids to meet energy needs, especially during rest and light activity. Recall that glucose provides 4 kcal of energy per gram.
Estimate Your Fiber Intake
ake ActionTo roughly estimate your daily fi ber consumption, determine the number of servings that you ate yesterday
from each food category listed here. Multiply the serving amount by the value listed and then add up the
total amount of fi ber. How does your total fi ber intake for yesterday compare with the general recommenda-
tion of 25 to 38 g of fi ber per day for women and men, respectively? If you are not meeting your needs, how
could you do so?
Food Servings Grams
Vegetables(Serving size: 1 cup raw leafy greens or ½ cup other vegetables) ______ × 2 ______
Fruits(Serving size: 1 whole fruit; ½ grapefruit; ½ cup berries or cubed fruit; ¼ cup dried fruit) ______ × 2.5 ______
Beans, lentils, split peas(Serving size: ½ cup cooked) ______ × 7 ______
Nuts, seeds(Serving size: ¼ cup; 2 tbsp peanut butter) ______ × 2.5 ______
Whole grains(Serving size: 1 slice whole-wheat bread, ½ cup whole-wheat pasta, brown rice, or other whole grain; ½ bran or whole-grain muffi n) ______ × 2.5 ______
Refi ned grains(Serving size: 1 slice bread; ½ cup pasta, rice, or other processed grain; ½ refi ned bagel or muffi n) ______ × 1 ______
Breakfast cereals(Serving size: check package for serving size and grams of fi ber per serving) ______ × fi ber per ______
serving Total grams of fi ber = ______
Copyright 1999. Consumers Union of U.S., Inc. Yonkers, NY 10703-1057, a nonprofi t organization. Adapted from “Fiber: Strands of Protection” with permission from the August 1999 issue of Consumer Reports on Health® for educational purposes only. www.ConsumerReports.org/health.
byr21413_ch05_154-189.indd 171 04/09/14 5:10 pm
(Serving size: 1 cup raw leafy greens or ½ cup other vegetables) ______ × 2 ______
Fruits(Serving size: 1 whole fruit; ½ grapefruit; ½ cup berries or cubed fruit; ¼ cup dried fruit) ______ × 2.5 ______
Beans, lentils, split peas(Serving size: ½ cup cooked) ______ × 7 ______
Nuts, seeds(Serving size: ¼ cup; 2 tbsp peanut butter) ______ × 2.5 ______
Confirming Pages
Bottled water is a convenient but relatively expensive source of water. In most cases, tap water is just as healthy a choice to meet water needs.
Food recalls occur when food products are
found to be contaminated. Examples include
• Sliced apples, avocado pulp, and sliced turkey for Listeria
• Bagged spinach and ground beef for E. coli
• Spices, pot pies, peanut butter, and hazelnuts for Salmonella
Recent food recall notifi cations are listed at
www.foodsafety.gov.
Raw milk has not undergone pasteurization,
the heat-treatment process that kills pathogenic
bacteria and makes milk safe to drink.
Pasteurization does not alter milk’s nutrient
content or make milk less healthy or allergenic.
According to the FDA and the CDC, raw milk
can harbor dangerous bacteria and should
not be consumed. Many states prohibit the
sale of raw milk to consumers, and interstate
commerce is prohibited. From 1998 to 2010,
raw milk products caused 148 outbreaks with
2384 illnesses and 2 deaths. Learn more at
www.cdc.gov/foodsafety/raw-milk-index.html.
99CHAPTER 3 The Food Supply
(e.g., lead and arsenic) and submit test results to the EPA.62 Water treatments vary, depend-ing on the water source, but all water is disinfected, usually with a chlorine-based chemical. Private water supplies, such as wells, are not regulated by the EPA but still should be tested for chemical and microbial contaminants. Local health departments can give advice on test-ing and keeping well water safe.
Bottled Water
Bottled water is a popular source of water. Many consumers are attracted to its convenience, perceived health value, or taste. All bottled waters must list the source of the water on the label. Sources include wells, spas, springs, geysers, and quite often the public water supply. Some bottled water contains minerals, such as calcium, magnesium, and potassium, that either occur naturally or are added by the bottling company to improve the water’s taste. The water is carbonated when carbon dioxide gas naturally occurs in the water source (called naturally sparkling water) or is added. Additives such as fl avors and vitamins also are com-mon. Bottled waters are regulated by the FDA, which sets high standards for their purity. It periodically collects and analyzes samples, but not to the extent that municipal water sup-plies are monitored. Water that is bottled in a sanitary manner and kept sealed will not spoil, although off-fl avors may develop over time.
Threats to Safe Water
The U.S. enjoys one of the cleanest water supplies in the world, but there are numerous threats to the safety of our water—agricultural runoff (animal waste, pesticides, fertilizer), inappro-priate disposal of chemicals, municipal solid waste (containing bacteria, viruses, nitrates, synthetic detergents, household chemicals) leaking into waterways, inadequate treatment of human wastes, and pollution from boats and ships (contains solvents, gas, detergents, raw sewage), to name just a few. This makes regular testing of the water supply critical.
The EPA requires that the public be notifi ed if water contamination is a danger to public health. For instance, nitrate contamination from fertilizer runoff is particularly dan-gerous to infants because it prevents oxygen from circulating in the body. As related earlier, Cryptosporidium can contaminate water supplies (it is not affected by normal chlorination procedures). Boiling tap water for a minimum of 1 minute is the best way to kill Cryptospo-ridium. Alternatively, individuals can purchase a water fi lter that screens out this parasite.
Even though the U.S. has one of the cleanest water supplies in the world, ill nesses from contaminated drinking water do occur. The CDC monitors water-related outbreaks, which average about 30 per year.63 Water safety experts note that these data likely underes-timate the true number of illnesses caused by contaminated water.
Preventing Foodborne and Waterborne Illnesses
Safe food and water supplies require a “farm-to-fork” approach. All those who grow our food, along with processors, distributors, and consumers, are responsible for food and water
CASE STUDYAaron and his wife attended an international
potluck on a warm July afternoon. Their
contribution was Argentine beef, a stewlike dish.
They followed the recipe and the cooking time
carefully, removed the dish from the oven at 1 P.M.,
and kept it warm by wrapping the pan in a towel.
They drove to the party and set the dish out on
the buffet table at 3 P.M. Dinner was to be served at 4 P.M., but the guests
were enjoying themselves so much that no one began to eat until 6 P.M.
Aaron made sure he sampled the Argentine beef they had prepared, but his
wife did not. He also had some salads, garlic bread, and a sweet coconut
dessert. The couple returned home at 11 P.M. and went to bed. At 2 A.M.,
Aaron knew something was wrong. He had severe abdominal pain and had
to make a mad dash to the toilet. He spent most of the next 3 hours in the
bathroom with diarrhea. By dawn, the diarrhea had subsided and he was
feeling better. He ate a light breakfast and felt fi ne by noon. It’s very likely
that Aaron contracted foodborne illness from the Argentine beef. What
precautions for avoiding foodborne illness were ignored by Aaron and the
rest of the people at the party? How might this case study be rewritten to
substantially reduce the risk of foodborne illness?
byr21413_ch03_072-115_new.indd 99 04/09/14 5:10 pm
Applying Nutrition to Career and More• Expert Perspectives from the Field features examine cutting-edge topics and demonstrate how
emerging, and sometimes controversial, research results affect nutrition knowledge and practice.
• Clinical Perspectives highlight the role of nutrition in the prevention and treatment of disease. These topics will be especially interesting to students planning careers in dietetics or health-related fields.
• Global Perspectives discuss concepts related to critical health and nutrition issues around the world. These timely features also aim to engage students with thought-provoking challenges.
• Historical Perspectives heighten awareness of critical discoveries and events that have affected our understanding of nutritional science.
• Perspective on the Futures address emerging trends affecting nutrition science and practice.
• Eachmajorheadinginthe chaptersisnumberedandcross-referencedtotheend-of-chaptersummary and study questions to make it easy to locate and prioritize important concepts.
Confirming Pages
341CHAPTER 10 Energy Balance, Weight Control, and Eating Disorders
you like to eat or the concerns you have about your diet in the left column and consider the descriptions/characteristics of the diet program in the center column. Finally, take a look at the diet resources listed in the last column to help you achieve the diet changes that are important to you.
According to Dr. Judith Rodriguez,* fi nding a weight loss diet that suits your lifestyle is the key to controlling weight and eating a healthy diet. In her book The Diet Selector, Dr. Rodriguez groups diets based on common principles to help consumers match their lifestyles with popular diets. Find what
xpert Perspective from the Field
Tailoring a Healthy Eating Plan to Fit Your Lifestyle
Eating Pattern/Lifestyle Characteristics/Descriptions Resources
Enjoy eating a variety of foods from different food groups in a reasonable balance
These diets develop and manage healthy eating patterns.
• The New Sonoma Diet by Connie Guttersen, PhD, RD• Cinch by Cynthia Sass, MPH, RD• Intuitive Eating by Evelyn Tribole, RD• Change One by John Hastings, Peter Jaret, Mindy Hermann, RD
Would like to manage lifestyle diseases through diet
These diets have specifi c eating patterns and foods to consume based on certain diseases or risk of disease.
• Healthy Eating for Lower Blood Pressure by Paul Gayler• Prevent a Second Heart Attack by Janet Bond Brill, PhD, RD, LD• The Cancer Fighting Kitchen by Rebecca Katz• DASH Diet for Hypertension by Thomas J. Moore, Mark Jenkins• Better Digestion by The American Dietetic
Association, Leslie Bonci, RD
Would like to manage weight and healthy food choices in college
These diets teach students how to make better food choices for health and weight management.
• The College Student’s Guide to Eating Well on Campus by Ann Litt, MS, RD
Enjoy eating ethnic foods and making them a part of a normal diet
These plans and diets help focus on international foods and eating patterns.
• Mediterranean Diet & Pyramid• Latino Diet & Pyramid• African Diet & Pyramid• Asian Diet & PyramidAll at www.oldwayspt.org/
Enjoy eating more vegetables and whole grains compared to animal products
These diets encourage consumers to consume more fruits, vegetables, and whole grains to help with weight loss and prevention of lifestyle disease.
• Volumetrics Weight-Control Plan by Barbara Rolls, PhD, RD
• The Whole Grain Diet Miracle by Lisa Hark, PhD, RD• The Flexitarian Diet by Dawn Jackson Blatner, RD• Food Matters: A Guide to Conscious Eating by Mark Bittman
Enjoy eating more animal products instead of cereals, breads, and pasta
These diets focus on a low carbohydrate and higher protein diet that include lean meats and healthy fats.
• South Beach Diet by Arthur Agatston, MD• The New Atkins for a New You by Eric C. Westman,
Stephen D. Phinney, Jeff S. Volek
Enjoy preparing quick meals and want nutrition tips for busy families with kids
These resources provide tips for teaching children healthy eating and making family food fun.
• Quick Meals for Healthy Kids and Busy Parents: Wholesome Family Recipes in 30 Minutes or Less from Three Leading Child Nutrition Experts by Sandra Nissenberg RD, Margaret L. Bogle, Audrey C. Wright.
• www.kidseatright.org website
*Judith Rodriguez, PhD, RD FADA, LDN is Chairperson and Professor of Nutrition in the Brooks College of Health, Department of Nutrition & Dietetics, at the University of North Florida. She is author of The Diet Selector: From Atkins to The Zone, More Than 50 Ways to Help You Find the Best Diet for You, and Contemporary Nutrition for Latinos: Latino Lifestyle Guide to Nutrition and Health. Dr. Rodriguez has served as President of the American Dietetic Association, has received the Distinguished Dietitian Award from Florida Dietetic Association, and was named an Outstanding Dietetics Educator by the American Dietetic Association (now called The Academy of Nutrition and Dietetics).
byr21413_ch10_318-363.indd 341 04/09/14 5:12 pm
According to Dr. Judith Rodriguez,* fi nding a weight loss diet that suits your lifestyle is the key to controlling weight
The Diet Selector,Dr. Rodriguez groups diets based on common principles to help consumers match their lifestyles with popular diets. Find what
Confirming Pages
Poultry 29%
Eggs 18%
Pork 12%
Vine vegetables, fruits,and nuts 13%
Beef 8%
Other (sprouts, leafy greens, roots,fish, grains, beans, shellfish, oil, sugar,and dairy) 20%
Percentage of Salmonella infections associated with food types.Source: Centers for Disease Control and Prevention. Making Food Safer to Eat, Reducing contamination from the farm to the table. 2011; www.cdc.gov/VitalSigns/FoodSafety.
104
CLINICAL PERSPECTIVE
• Listeriosis. Listeria monocytogenes bacteria
cause listeriosis, a rare, but serious, disease.
Listeriosis begins with muscle aches, fever, and
nausea. It can spread to the nervous system,
causing severe headache, stiff neck, loss of
balance, and confusion. Pregnant women and
their fetuses are particularly vulnerable—
listeriosis can cause miscarriage, premature
delivery, infection in the fetus, and fetal death.
During pregnancy, women are 20 times more
likely to develop the disease. The elderly also
are susceptible. A 2008 outbreak in Canada
from contaminated deli meats resulted in
29 deaths; almost all of them were elderly
individuals. About 1 in 5 persons with listeriosis
will die from the infection.
• Guillain-Barré syndrome (GBS). Campylobacter jejuni is one cause of this rare nervous system
disorder. In GBS, peripheral nerves (those
that connect the spinal cord and brain to the
rest of the body) are damaged by the body’s
own immune system. Early symptoms of GBS
include tingling and pain in the legs, followed
by severe muscular weakness. Paralysis
can occur, and some individuals need help
Foodborne illness often means a few hours or
even a few days of discomfort and then the ill-
ness resolves on its own. In some cases, though,
foodborne illness causes more serious medical
problems, which can have lifelong effects. High-
risk populations—infants and young children, the
elderly, pregnant women and their fetuses, and
those with impaired immune systems—have the
greatest risk of serious complications like these:
• Hemolytic uremic syndrome (HUS). Most cases
of HUS are caused by the toxin produced by
Escherichia coli 0157:H7. The toxin attacks red
blood cells, causing them to break apart (called
hemolysis), and the kidneys, causing waste
products to build up (called uremia). Early
symptoms of HUS include bloody diarrhea,
vomiting, sleepiness, and low urine output. In
the worst cases, the toxin damages multiple
organs, causing seizures, permanent kidney
failure, stroke, heart damage, liver failure,
and even death. Fortunately, most individuals
recover completely, although usually after weeks
of intensive medical care. HUS affl icts children
more often than adults, but adults experience
the most severe infections.
breathing with a ventilator. Recovery can take
weeks to months, and about 30% of those with
GBS do not fully recover, experiencing lifelong
pain, weakness, and/or paralysis.
• Reactive arthritis. Foodborne illness caused by
Salmonella, Shigella, Campylobacter, and others
can cause reactive arthritis. This condition
usually develops 2 to 6 weeks after the initial
infection and causes infl ammation throughout
the body, but especially in the joints and eyes.
Pain and swelling of the knees, ankles, and
feet are common. Infl ammation of the urinary
tract and blistering of the palms of the hands
and soles of the feet also are common. Genetic
factors play an important role in determining
who develops the disease. Most people with
reactive arthritis require medical treatment and
will recover after 2 to 6 months, but about 20%
experience mild arthritis for a much longer time.
These diseases highlight the need for a safe food
supply and safe food handling all along the food
chain.
Foodborne I l lness Can Be Deadly
byr21413_ch03_072-115_new.indd 104 04/09/14 5:15 pm
xiii
Listeria monocytogenes bacteria Listeria monocytogenes bacteria Listeria monocytogenescause listeriosis, a rare, but serious, disease.
Listeriosis begins with muscle aches, fever, and
nausea. It can spread to the nervous system,
breathing with a ventilator. Recovery can take
weeks to months, and about 30% of those with
GBS do not fully recover, experiencing lifelong
pain, weakness, and/or paralysis.
Confirming Pages
Growing evidence indicates that what we eat may affect not only our personal health but also that of the environment. Many scientists believe that meat rich
diets and the agricultural practices that support the production of food for these diets negatively affect the environment. For instance, producing food for
nonvegetarian diets (especially beef-based diets) uses more water, fossil fuel energy, fertilizer, pesticides, and acres of farmland than vegetarian diets.29
Meat rich diets also cause greater emissions of greenhouse gases, such as carbon dioxide, methane, and nitrous oxide, which are associated with global
warming.30 Scientists are concerned that continued global warming may, in turn, decrease agricultural productivity, reduce farmers’ incomes, and increase
global food insecurity.31
Not all scientists agree with these fi ndings and concerns, however. Some believe that consuming a small amount of dairy and/or meat may actually increase land
use effi ciency, thereby protecting environmental resources and promoting food security.32 They point out that high quality farmland is required to grow fruits,
vegetables, and grains, whereas meat and dairy products can be produced on the more widely available, lower quality land. Even though diets containing meat use
more land, they can feed more people because of the greater availability of lower quality farmland. It appears that diets have different “agricultural land footprints,”
depending on the amount of plant-based and animal-based food they contain. Supporters of mixed animal/vegetable–based diets point out that vegetarian diets
often include tofu and other meat substitutes produced from soy, chickpeas, and lentils. Many meat substitutes are highly processed and require energy-intensive
production methods. Thus, including small amounts of meat may offer both environmental and nutritional benefi ts.
GL BAL PERSPECTIVE
How big is your foot pr int?t p
251
an allergic reaction in a person do not come
in contact with the food to be served to that
individual. Even trace amounts of an allergen
can cause a reaction. To prevent cross-contact,
anything that will be used to prepare an allergen-
free meal (e.g., hands, workspace, pans, utensils,
plates) should be washed thoroughly before
preparing the allergen-free meal. Unlike foodborne
illness pathogens, such as bacteria and viruses,
cooking an allergenic food often does not render
its allergens harmless.16
The prevalence of food allergies has
increased in the last 20 years.15 Although diffi cult
to estimate, it appears that approximately 6 to
7% of children and 1 to 2% of adults have food
allergies.15 It is unclear why some people develop
allergies and what steps might help decrease the
risk of developing food allergies. Although some
studies have shown that women can help prevent
or delay the onset of food allergies in their child
by avoiding peanuts and tree nuts during their
pregnancy and lactation, currently it appears
that maternal dietary restrictions do not play a
signifi cant role in preventing food allergies in their
children.15,17 After the child is born, the following
steps may help prevent food allergies.9 These
guidelines are especially important for families
with a history of any type of allergy.
• Feed babies only breast milk or infant formula
until they are at least 6 months old.
• Delay feeding cow milk and milk products until
infants are at least 1 year of age.
• Serve egg whites only after children reach age
2 years.
• Keep diets free of peanuts, tree nuts, fi sh, and
shellfi sh until children are at least 3 years old.
Many young children with food allergies
outgrow them.15,18 Thus, parents should not
assume that the allergy will be long-lasting.
Allergies to certain foods (e.g., milk, egg, soy,
wheat) are more likely to be outgrown than are
allergies to other foods (e.g., peanuts, tree nuts,
fi sh, and shellfi sh).15 Those with allergies may
be tested by physicians periodically to determine
whether they have outgrown the allergy. If so,
the food(s) can be reintroduced into the diet and
eaten safely.
Food allergies and food intolerances are not the
same. Food allergies cause an immune response
as a result of exposure to certain food components,
typically proteins. In contrast, food intolerances
(see Chapter 4) are caused by an individual’s
inability to digest certain food components,
usually due to low amounts of specifi c enzymes.
Generally, larger amounts of an offending food
are required to produce the symptoms of food
intolerance than to trigger allergic symptoms. Food
allergies tend to be far more life threatening than
food intolerances.
The American Academy of Allergy and
Immunology has a 24-hour toll-free hot line (800-
822-2762) to answer questions about food allergies
and help direct people to specialists who treat
allergy problems. Free information
on food allergies is available by contacting
The Food Allergy & Anaphylaxis Network
at www.foodallergy.org.
1. What are the symptoms of food allergies?2. Which foods cause most food allergies?3. What steps can parents take to help prevent food allergies in their children?
Knowledge Check
byr21413_ch07_226-259.indd 251 04/09/14 5:15 pm
Confirming Pages
177CHAPTER 5 Carbohydrates
5.6 Health Concerns Related to Carbohydrate Intake
As a part of a nutritious diet, adequate carbohydrate intake is important for maintaining health and decreasing the risk of chronic disease. However, as with many nutrients, excessive intakes of different forms of carbohydrate can be harmful to overall health. The following dis-cussions will help you understand the risks of high intakes of different types of carbohydrates.
Very-High-Fiber Diets
Adequate fi ber intake provides many health benefi ts. However, very high intakes of fi ber (i.e., above 50 to 60 g/day) can cause health risks. For example, high fi ber consumption combined with low fl uid intake can result in hard, dry stools that are painful to eliminate. Over time, this may cause hemorrhoids, as well as rectal bleeding, from increased exertion and pressure. In severe cases, the combination of excess fi ber and insuffi cient fl uid may con-tribute to blockages in the intestine, requiring surgery.
Very-high-fi ber diets also may decrease the absorption of certain minerals and increase the risk of defi ciencies. This occurs because some minerals can bind to fi ber, which prevents them from being absorbed. In countries where fi ber intake is often greater than 60 g/day, defi ciencies of zinc and iron have been reported.
High fi ber diets can be of concern in young children, elderly persons, and malnour-ished individuals, all of whom may not eat adequate amounts of foods and nutrients. For these individuals, high fi ber intakes may cause a sense of fullness and reduce their overall intake of foods, energy, and nutrients.
High Sugar Diets
For many Americans, sugars constitute a large part of their diets. In fact, on average, 13% of the calories consumed by U.S. adults are from added sugars. Daily intake is about 335 kcal for men and 239 kcal for women.17 Teens consume about 360 kcal of added sugars per day.18 Recall that most of the sugar we eat comes from foods and beverages to which sugar has been added during processing and/or manufacturing. Major sources of added sugar are soft drinks, cakes, cookies, fruit punch, and dairy desserts, such as ice cream. Although sugars supply calories, they usually provide little else and often replace the intake of more nutritious foods. Children and adolescents are typically at greatest risk of overconsuming sugar and empty calories. Dietary surveys indicate that many children and adolescents are drinking an excess of sugar-sweetened beverages and too little milk. Milk contains calcium and vitamin D, both of which are essential for bone health. Thus, substi-tuting sugared drinks for milk can compromise bone development and health.
High intakes of sugars also can increase the risk of weight gain and obesity. (However, it is important to note that, although obesity is a risk factor for type 2 diabetes, high sugar diets do not directly cause diabetes.) The “supersizing” trend noted in food and beverage promotions is contributing to this concern. For example, in the 1950s, a typical soft drink serving was a 6.5-ounce bottle. Today, a 20-ounce bottle is a typical serving. This change alone contributes 170 extra calories of sugar to the diet. Drinking 1 bottle per day for a year amounts to 62,050 extra calories and a 17- to 18-pound (7.75 to 8.25 kg) weight gain.
The sugar in cakes, cookies, and ice cream also supplies extra energy, which pro-motes weight gain. Although dieters may be choosing more low fat and fat-free snack products, these usually are made with substantial amounts of added sugar in order to pro-duce a dessert with an acceptable taste and texture. The resulting product often is a high calorie food that equals or even exceeds the energy content of the original high fat food product it was designed to replace.
High intakes of energy and sugar (especially fructose) have been associated with con-ditions that increase the risk of cardiovascular disease—namely, increased blood levels of triglycerides and LDL-cholesterol and decreased levels of HDL-cholesterol. Studies also have suggested a potential link between the increased consumption of sugar-sweetened bev-erages and energy with an increased risk of type 2 diabetes and Metabolic Syndrome.25
HISTORICALPERSPECTIVE
Photographing AtomsDiscovering the molecular layout of biologically important molecules is critical to understanding their function and treating disease. The biochemist and crystallographer Dorothy Crowfoot Hodgkin developed new x-ray techniques that permitted her to determine the structure of over 100 molecules, including insulin, vitamin B-12, vitamin D, and penicillin. Her work with insulin improved treatment of diabetes. Knowing the structure of vitamin B-12 advanced our knowledge of its role in blood health. Learn more about this Nobel Prize winner at www.nobelprize.org/nobel_prizes/chemistry/laureates/1964/hodgkin-bio.html.
High carbohydrate beverages can contribute to tooth decay.
byr21413_ch05_154-189.indd 177 04/09/14 5:11 pm
Confirming Pages
338 PART 3 Metabolism and Energy Balance
Save 140 kcal by choosing 3 oz lean beef instead of 3 oz well-marbled beef
Save 175 kcal by choosing ½ broiled chicken instead of ½ batter-fried chicken
Save 210 kcal by choosing 3 oz lean roast beef instead of ½ cup beef stroganoff
Save 65 kcal by choosing ½ cup boiled potatoes instead of ½ cup fried potatoes
Save 140 kcal by choosing 1 cup raw vegetables instead of ½ cup potato salad
Save 150 kcal by choosing 2 tbsp low kcal salad dressing
instead of 2 tbsp regular salad dressing
Save 310 kcal by choosing 1 apple instead of 1 slice apple pie
Save 150 kcal by choosing 1 English muffi n instead of 1 Danish pastry
Save 60 kcal by choosing 1 cup cornfl akes instead of 1 cup sugar-coated cornfl akes
Save 45 kcal by choosing 1 cup 1% milk instead of 1 cup whole milk
Save 150 kcal by choosing 6 oz wine cooler made with sparkling water
instead of 6 oz gin and tonic
Save 150 kcal by choosing 1 cup plain popcorn instead of 1 oz potato chips
Save 185 kcal by choosing 1 slice angel food cake instead of 1 slice white iced cake
Save 150 kcal by choosing 12 oz sugar free soft drink
instead of 12 oz regular soft drink
Save 140 kcal by choosing 12 oz light beer instead of 12 oz regular beer
Save 140 kcal by choosing 3 oz lean beef instead of 3 oz well-marbled beef
Table 10-4 Saving Calories: Ideas for Getting Started
Spot-reducing by using diet and physical
activity is not possible. “Problem” local fat
deposits can be reduced in size, however,
using lipectomy (surgical removal of fat).
This procedure carries some risks and is
designed to help a person lose about 4 to
8 lb per treatment.
A pedometer is a low-cost device that
monitors the number of steps taken. An often-
stated goal for activity is to take 10,000 steps/
day—typically, we take half that many or less.
Table 10-5 Approximate Energy Costs of Various Activities
kcal/kg kcal/kg kcal/kgActivity per Hour Activity per Hour Activity per Hour
Aerobics—heavy 8.0 Dressing/showering 1.6 Running or jogging (10 mph) 13.2
Aerobics—medium 5.0 Driving 1.7 Downhill skiing (10 mph) 8.8
Aerobics—light 3.0 Eating (sitting) 1.4 Sleeping 1.2
Backpacking 9.0 Food shopping 3.6 Swimming (.25 mph) 4.4
Basketball—vigorous 10.0 Football—touch 7.0 Tennis 6.1
Cycling (5.5 mph) 3.0 Golf 3.6 Volleyball 5.1
Bowling 3.9 Horseback riding 5.1 Walking (2.5 mph) 3.0
Calisthenics—heavy 8.0 Jogging—medium 9.0 Walking (3.75 mph) 4.4
Calisthenics—light 4.0 Jogging—slow 7.0 Water skiing 7.0
Canoeing (2.5 mph) 3.3 Ice skating (10 mph) 5.8 Weight lifting—heavy 9.0
Cleaning 3.6 Lying down 1.3 Weight lifting—light 4.0
Cooking 2.8 Racquetball—social 8.0 Window cleaning 3.5
Cycling (13 mph) 9.7 Roller skating 5.1 Writing (sitting) 1.7
The values refer to total energy expenditure, including that needed to perform the physical activity plus that needed for basal metabolism, the thermic effect of food, and thermogenesis.Example: For a 150 lb person who played tennis for 1.5 hours, 150 lb/2.2 5 68 kg 68 kg 3 6.1 kcal/hr 3 1.5 hr 5 622 kcal expenditure
performance, rather than intensity, are the keys to success with this weight loss approach. Another key is fi nding activities that are enjoyable and can be continued throughout life. There is no single activity that is better than another—for example, walking vigorously 3 miles daily can be as helpful as aerobic dancing or jogging. Activities of lighter intensity
on the FutureThe common wisdom that eating 3500 kcal less than you need will result in the loss of 1 pound has come under great scrutiny. Weight-loss research models based on thermodynamics, mathematics, physics, and chemistry indicate many more than 3500 calories may be stored in a pound of body fat. Researchers are working to build and validate more accurate weight-loss prediction models.57 Learn more at www.pbrc.edu/research-and-faculty/calculators/weight-loss-predictor.
byr21413_ch10_318-363.indd 338 04/09/14 5:13 pm
Final PDF to printer
xiv
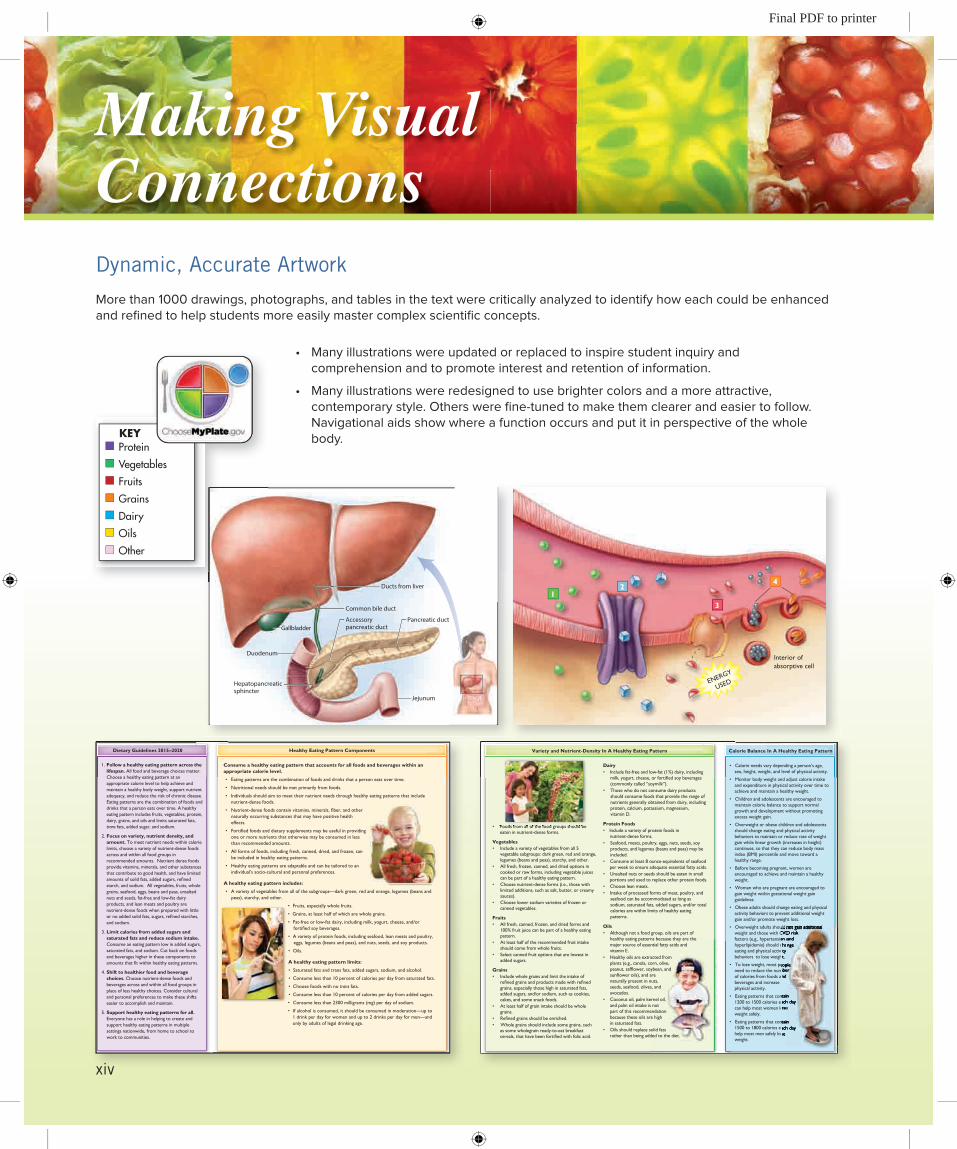
Making Visual ConnectionsDynamic, Accurate Artwork
More than 1000 drawings, photographs, and tables in the text were critically analyzed to identify how each could be enhanced and refined to help students more easily master complex scientific concepts.
• Manyillustrationswereupdatedorreplacedtoinspirestudentinquiry andcomprehension and to promote interest and retention of information.
• Manyillustrationswereredesignedtousebrightercolorsandamoreattractive,contemporary style. Others were fine-tuned to make them clearer and easier to follow. Navigational aids show where a function occurs and put it in perspective of the whole body.
Adult women RDA = 700 μgRDA
adultwomen
RDAadultmen
Adult men RDA = 900 μgDaily Value = 1000 μg*
Margarine, 2 tbsp
Beef liver, 3 oz
Cheddar cheese, 3 oz
Fat-free milk, 1 cup
Sweet potato, 1⁄2 cup
Carrots, 1⁄2 cup
Kale, 1⁄2 cup
Broccoli, 1⁄2 cup
Spinach, 1⁄2 cup
Romaine lettuce, 1⁄2 cup
Acorn squash, 1⁄2 cup
Apricot, 1⁄2 cup
Mango, 1⁄2 cup
Peach, 1⁄2 cup
% Daily Value
*Calculated from International Units.
50%(500 μg)
0% 100%(1000 μg)
150%(1500 μg)
200%(2000 μg)
540%
205%
Protein
Vegetables
Fruits
Grains
Dairy
Oils
Other
KEY
1 Retinol Activity Equivalent (RAE) 1 IU Vitamin A Activity5 1 μg retinol 5 0.3 μg retinol5 12 μg beta-carotene 5 3.6 μg beta-carotene5 24 μg alpha-carotene and beta-cryptoxanthin 5 7.2 μg alpha-carotene and
beta-cryptoxanthin
408 PART 4 Vitamins and Minerals
Another term, retinol equivalent (RE), is an older unit of measurement for vitamin A activity. The RE was based on the assumption that carotenoids made a greater contribution to vitamin A needs than is now known to be the case. Nutrient databases may contain this older RE standard because it will take some time to update these resources.
To compare the older RE or IU standards with current RAE recommendations, assume that, for any preformed vitamin A in a food or added to food, 1 RE (3.3 IU) 5 1 RAE. There is no easy way to convert RE or IU units to RAE units for foods that naturally contain provitamin A carotenoids. A general rule of thumb is to divide the older values for foods containing carotenoids by 2, and then do the conversion from RE to IU to RAE, as shown in Table 12-1. There also is no easy way to do this calculation for food containing a mixture of preformed vitamin A and carotenoids. Generally speaking, these foods contain less vitamin A than the RE or IU values suggest.
Vitamin A Needs
The RDA for vitamin A is 900 μg Retinol Activity Equivalents (RAE) per day for adult men and 700 μg RAE per day for adult women.2 At this intake, adequate body stores of vitamin A are maintained in healthy adults. The Daily Value used on food packages and supplements is 5000 IU, or about 1000 μg. At present, there is no DRI for beta-carotene or any of the other provitamin A carotenoids.1 The average intakes of adult men and women in North America currently meet DRI guidelines for vitamin A.
Figure 12-3 Food sources of vitamin A. In addition to MyPlate food groups, yellow is used for oils and pink is used for substances that do not fit easily into food groups (e.g., candy, salty snacks).
Table 12-1 Conversion Values for Retinol Activity Equivalents
Ducts from liver
Common bile duct
GallbladderPancreatic duct
Jejunum
Accessorypancreatic duct
Duodenum
Hepatopancreaticsphincter
Elise is a 20-year-old college sophomore. Over the last few months, she has
been experiencing regular bouts of esophageal burning, pain, and a sour taste
in the back of her mouth. This usually happens after a large lunch or dinner.
Elise often takes an over-the-counter antacid to relieve these unpleasant
symptoms. However, the symptoms have worsened and Elise has decided to
visit the university health center.
The nurse practitioner at the center tells Elise it is good she came in for a checkup because she
suspects Elise is experiencing heartburn and acid indigestion, but she might also be experiencing
gastroesophageal reflux disease (GERD). What types of lifestyle and dietary changes may help
reduce or prevent heartburn and GERD? What types of medications are especially helpful in treating
this problem?
CASE STUDY
132 PART 1 Nutrition Basics
feces—this is how cholesterol, one of the components of bile, is removed from the body. The pancreas produces about 5 to 6 cups (1.5 liters) of pancreatic juice per day. This juice is an alkaline (basic) mixture of sodium bicarbonate (NaHCO3) and
enzymes. The sodium bicarbonate neutralizes the acidic chyme arriving from the stomach, thereby protecting the small intes-tine from damage by acid. Digestive enzymes from the pan-
creas include pancreatic amylase (to digest starch), pancreatic lipase (to digest fat), and several proteases (to digest pro-tein). Pancreatic enzymes break large macronutrient mol-ecules into smaller subunits.
Gastrointestinal Hormones: A Key to Orchestrating Digestion
The remarkable work of the digestive system requires the careful regulation and coordination of several processes, including the production and release of hormones throughout the length of the GI tract. Five hormones, part of the endocrine system, play
key roles in this regulation: gastrin, secretin, cholecystokinin (CCK), somatostatin and glucose-dependent insulinotropic peptide (Table 4-4). To illustrate their functions, let’s follow a turkey sandwich through the digestive system:
1. As you eat a turkey sandwich (or even just think about it), gastrin is produced by cells in the stomach. Gastrin signals other stomach cells to release HCl and pepsinogen (for protein digestion). After thorough mixing, the turkey sandwich, now chyme, is released in small amounts into the small intestine.
2. As chyme is gradually released from the stomach into the small intestine, gastrin pro-duction slows and the small intestine secretes secretin and CCK. Both hormones trig-ger the release of enzyme- and bicarbonate- containing pancreatic juices that digest carbohydrate, fat, and protein and reduce the acidity of the intestinal contents. Fat in the small intestine (from the mayonnaise and the turkey) further stimulates the
enterohepatic circulation Continual recycling of compounds between the small intestine and the liver. Bile is an example of a recycled compound.
Figure 4-15 The common bile duct from the liver and gallbladder and the pancreatic duct join together at the hepatopancreatic sphincter to deliver bile, pancreatic enzymes, and bicarbonate to the duodenum.
In cystic fibrosis, the most common lethal
inherited genetic disease in White populations,
thick, sticky mucus builds up in organs,
especially the lungs and pancreas. This buildup
prevents pancreatic enzymes from reaching the
small intestine. If the condition is not treated,
malabsorption of nutrients, weight loss, and
malnutrition occur. Most individuals with cystic
fibrosis are prescribed pancreatic enzyme
replacements, which are taken right before
eating. An enteric coating protects the enzymes
from destruction by stomach acid. Maintaining
good nutritional status helps prevent the
respiratory infections common in those with
cystic fibrosis.
Largeintestine
Stomach
Gallbladder
Liver
Anus
Pancreas
Smallintestine
Stomach
Small intestine
Large intestine
Alcohol (20% of total)Water (minor amount)
Calcium, magnesium, iron, and other mineralsGlucoseAmino acidsFatsVitaminsWater (70 to 90% of total)Alcohol (80% of total)Bile acids
SodiumPotassiumSome fatty acidsVitamin K and biotin (synthesized by microorganisms in the large intestine)GasesWater (10 to 30% of total)
1
2
31
23
Organ Primary Nutrients Absorbed
ENERGY
USED
Interior ofabsorptive cell
12
3
4
134 PART 1 Nutrition Basics
Figure 4-16 Major sites of absorption along the GI tract. Note that some synthesis and absorption of vitamin K and biotin takes place in the large intestine.
The medical history of a young girl who is greatly underweight shows that she had three-quarters of her small intestine removed after she was injured in a car accident. Explain how this accounts for her underweight condition, even though her medical chart shows that she eats well.
Critical Thinking
Figure 4-17 Nutrient absorption relies on 4 major absorptive processes. 1 Passive diffusion (in green) is diffusion of nutrients across the absorptive cell membranes. 2 Facilitated diffusion (in blue) uses a carrier protein to move nutrients down a concentration gradient. 3 Active absorption (in red) involves a carrier protein as well as energy to move nutrients (against a concentration gradient) into absorptive cells. 4 Phagocytosis and pinocytosis (in gray and orange) are forms of active transport in which the absorptive cell membrane forms an invagination that engulfs a nutrient to bring it into the cell.
Confirming Pages
byr18378_ch02_038-071.indd 56 03/29/16 07:36 PM
Dietary Guidelines 2015–2020 Healthy Eating Pattern Components Variety and Nutrient-Density In A Healthy Eating Pattern Calorie Balance In A Healthy Eating Pattern
Consume a healthy eating pattern that accounts for all foods and beverages within an appropriate calorie level.
• Eating patterns are the combination of foods and drinks that a person eats over time.
• Nutritional needs should be met primarily from foods.
• Individuals should aim to meet their nutrient needs through healthy eating patterns that include nutrient-dense foods.
• Nutrient-dense foods contain vitamins, minerals, fiber, and other naturally occurring substances that may have positive health effects.
• Fortified foods and dietary supplements may be useful in providing one or more nutrients that otherwise may be consumed in less than recommended amounts.
• All forms of foods, including fresh, canned, dried, and frozen, can be included in healthy eating patterns.
• Healthy eating patterns are adaptable and can be tailored to an individual’s socio-cultural and personal preferences.
A healthy eating pattern includes:
• A variety of vegetables from all of the subgroups—dark green, red and orange, legumes (beans and peas), starchy, and other.
• Fruits, especially whole fruits.
• Grains, at least half of which are whole grains.
• Fat-free or low-fat dairy, including milk, yogurt, cheese, and/or fortified soy beverages.
• A variety of protein foods, including seafood, lean meats and poultry, eggs, legumes (beans and peas), and nuts, seeds, and soy products.
• Oils.
A healthy eating pattern limits:
• Saturated fats and trans fats, added sugars, sodium, and alcohol.
• Consume less than 10 percent of calories per day from saturated fats.
• Choose foods with no trans fats.
• Consume less than 10 percent of calories per day from added sugars.
• Consume less than 2300 milligrams (mg) per day of sodium.
• If alcohol is consumed, it should be consumed in moderation—up to 1 drink per day for women and up to 2 drinks per day for men—and only by adults of legal drinking age.
• Calorie needs vary depending a person’s age, sex, height, weight, and level of physical activity.
• Monitor body weight and adjust calorie intake and expenditure in physical activity over time to achieve and maintain a healthy weight.
• Children and adolescents are encouraged to maintain calorie balance to support normal growth and development without promoting excess weight gain.
• Overweight or obese children and adolescents should change eating and physical activity behaviors to maintain or reduce rate of weight gain while linear growth (increases in height) continues, so that they can reduce body mass index (BMI) percentile and move toward a healthy range.
• Before becoming pregnant, women are encouraged to achieve and maintain a healthy weight.
• Women who are pregnant are encouraged to gain weight within gestational weight gain guidelines.
• Obese adults should change eating and physical activity behaviors to prevent additional weight gain and/or promote weight loss.
• Overweight adults should not gain additional weight and those with CVD risk factors (e.g., hypertension and hyperlipidemia) should change eating and physical activity behaviors to lose weight.
• To lose weight, most people need to reduce the number of calories from foods and beverages and increase physical activity.
• Eating patterns that contain 1200 to 1500 calories each day can help most women lose weight safely.
• Eating patterns that contain 1500 to 1800 calories each day help most men safely lose weight.
• Foods from all of the food groups should be eaten in nutrient-dense forms.
Vegetables• Include a variety of vegetables from all 5
vegetable subgroups: dark green, red and orange, legumes (beans and peas), starchy, and other.
• All fresh, frozen, canned, and dried options in cooked or raw forms, including vegetable juices can be part of a healthy eating pattern.
• Choose nutrient-dense forms (i.e., those with limited additions, such as salt, butter, or creamy sauces).
• Choose lower sodium varieties of frozen or canned vegetables.
Fruits• All fresh, canned, frozen, and dried forms and
100% fruit juice can be part of a healthy eating pattern.
• At least half of the recommended fruit intake should come from whole fruits.
• Select canned fruit options that are lowest in added sugars.
Grains• Include whole grains and limit the intake of
refined grains and products made with refined grains, especially those high in saturated fats, added sugars, and/or sodium, such as cookies, cakes, and some snack foods.
• At least half of grain intake should be whole grains.
• Refined grains should be enriched.• Whole grains should include some grains, such
as some wholegrain ready-to-eat breakfast cereals, that have been fortified with folic acid.
Dairy• Include fat-free and low-fat (1%) dairy, including
milk, yogurt, cheese, or fortified soy beverages (commonly called “soymilk”).
• Those who do not consume dairy products should consume foods that provide the range of nutrients generally obtained from dairy, including protein, calcium, potassium, magnesium, vitamin D.
Protein Foods• Include a variety of protein foods in
nutrient-dense forms.• Seafood, meats, poultry, eggs, nuts, seeds, soy
products, and legumes (beans and peas) may be included.
• Consume at least 8 ounce-equivalents of seafood per week to ensure adequate essential fatty acids.
• Unsalted nuts or seeds should be eaten in small portions and used to replace other protein foods.
• Choose lean meats.• Intake of processed forms of meat, poultry, and
seafood can be accommodated as long as sodium, saturated fats, added sugars, and/or total calories are within limits of healthy eating patterns.
Oils• Although not a food group, oils are part of
healthy eating patterns because they are the major source of essential fatty acids and vitamin E.
• Healthy oils are extracted from plants (e.g., canola, corn, olive, peanut, safflower, soybean, and sunflower oils), and are naturally present in nuts, seeds, seafood, olives, and avocados.
• Coconut oil, palm kernel oil, and palm oil intake is not part of this recommendation because these oils are high in saturated fats.
• Oils should replace solid fats rather than being added to the diet.
1. Follow a healthy eating pattern across the lifespan. All food and beverage choices matter. Choose a healthy eating pattern at an appropriate calorie level to help achieve and maintain a healthy body weight, support nutrient adequacy, and reduce the risk of chronic disease. Eating patterns are the combination of foods and drinks that a person eats over time. A healthy eating pattern includes fruits, vegetables, protein, dairy, grains, and oils and limits saturated fats, trans fats, added sugar, and sodium.
2. Focus on variety, nutrient density, and amount. To meet nutrient needs within calorie limits, choose a variety of nutrient-dense foods across and within all food groups in recommended amounts. Nutrient dense foods provide vitamins, minerals, and other substances that contribute to good health, and have limited amounts of solid fats, added sugars, refined starch, and sodium. All vegetables, fruits, whole grains, seafood, eggs, beans and peas, unsalted nuts and seeds, fat-free and low-fat dairy products, and lean meats and poultry are nutrient-dense foods when prepared with little or no added solid fats, sugars, refined starches, and sodium.
3. Limit calories from added sugars and saturated fats and reduce sodium intake. Consume an eating pattern low in added sugars, saturated fats, and sodium. Cut back on foods and beverages higher in these components to amounts that fit within healthy eating patterns.
4. Shift to healthier food and beverage choices. Choose nutrient-dense foods and beverages across and within all food groups in place of less healthy choices. Consider cultural and personal preferences to make these shifts easier to accomplish and maintain.
5. Support healthy eating patterns for all. Everyone has a role in helping to create and support healthy eating patterns in multiple settings nationwide, from home to school to work to communities.
56 PART 1 Nutrition Basics
2.4 Dietary Guidelines for Americans
The diets of many people in the U.S. and Canada are too high in calories, fat, saturated fat, trans fat, cholesterol, sugar, salt, and alcohol.16 Many consume insufficient amounts of whole grains, fruits, and vegetables. These dietary patterns put many of us at risk of major chronic “killer” diseases, such as cardiovascular disease and cancer. In response to concerns about the prevalence of these killer disease patterns, every 5 years since 1980, the U.S. Department of Agriculture (USDA) and U.S. Department of Health and Human Services (DHHS) have published the Dietary Guidelines for Americans (Dietary Guidelines, for short).
The Dietary Guidelines are the foundation of the U.S. government’s nutrition policy and education. They reflect what scientific experts believe is the most accurate and up-to-date scientific knowledge about nutritious diets, physical activity, and related healthy lifestyle choices. The Dietary Guidelines are designed to meet nutrient needs while reduc-ing the risk of obesity, hypertension, cardiovascular disease, type 2 diabetes, osteoporosis,
Figure 2-6 Key recommendations from the latest Dietary Guidelines for Americans.
Confirming Pages
byr18378_ch02_038-071.indd 57 03/29/16 07:36 PM
Dietary Guidelines 2015–2020 Healthy Eating Pattern Components Variety and Nutrient-Density In A Healthy Eating Pattern Calorie Balance In A Healthy Eating Pattern
Consume a healthy eating pattern that accounts for all foods and beverages within an appropriate calorie level.
• Eating patterns are the combination of foods and drinks that a person eats over time.
• Nutritional needs should be met primarily from foods.
• Individuals should aim to meet their nutrient needs through healthy eating patterns that include nutrient-dense foods.
• Nutrient-dense foods contain vitamins, minerals, fiber, and other naturally occurring substances that may have positive health effects.
• Fortified foods and dietary supplements may be useful in providing one or more nutrients that otherwise may be consumed in less than recommended amounts.
• All forms of foods, including fresh, canned, dried, and frozen, can be included in healthy eating patterns.
• Healthy eating patterns are adaptable and can be tailored to an individual’s socio-cultural and personal preferences.
A healthy eating pattern includes:
• A variety of vegetables from all of the subgroups—dark green, red and orange, legumes (beans and peas), starchy, and other.
• Fruits, especially whole fruits.
• Grains, at least half of which are whole grains.
• Fat-free or low-fat dairy, including milk, yogurt, cheese, and/or fortified soy beverages.
• A variety of protein foods, including seafood, lean meats and poultry, eggs, legumes (beans and peas), and nuts, seeds, and soy products.
• Oils.
A healthy eating pattern limits:
• Saturated fats and trans fats, added sugars, sodium, and alcohol.
• Consume less than 10 percent of calories per day from saturated fats.
• Choose foods with no trans fats.
• Consume less than 10 percent of calories per day from added sugars.
• Consume less than 2300 milligrams (mg) per day of sodium.
• If alcohol is consumed, it should be consumed in moderation—up to 1 drink per day for women and up to 2 drinks per day for men—and only by adults of legal drinking age.
• Calorie needs vary depending a person’s age, sex, height, weight, and level of physical activity.
• Monitor body weight and adjust calorie intake and expenditure in physical activity over time to achieve and maintain a healthy weight.
• Children and adolescents are encouraged to maintain calorie balance to support normal growth and development without promoting excess weight gain.
• Overweight or obese children and adolescents should change eating and physical activity behaviors to maintain or reduce rate of weight gain while linear growth (increases in height) continues, so that they can reduce body mass index (BMI) percentile and move toward a healthy range.
• Before becoming pregnant, women are encouraged to achieve and maintain a healthy weight.
• Women who are pregnant are encouraged to gain weight within gestational weight gain guidelines.
• Obese adults should change eating and physical activity behaviors to prevent additional weight gain and/or promote weight loss.
• Overweight adults should not gain additional weight and those with CVD risk factors (e.g., hypertension and hyperlipidemia) should change eating and physical activity behaviors to lose weight.
• To lose weight, most people need to reduce the number of calories from foods and beverages and increase physical activity.
• Eating patterns that contain 1200 to 1500 calories each day can help most women lose weight safely.
• Eating patterns that contain 1500 to 1800 calories each day help most men safely lose weight.
• Foods from all of the food groups should be eaten in nutrient-dense forms.
Vegetables• Include a variety of vegetables from all 5
vegetable subgroups: dark green, red and orange, legumes (beans and peas), starchy, and other.
• All fresh, frozen, canned, and dried options in cooked or raw forms, including vegetable juices can be part of a healthy eating pattern.
• Choose nutrient-dense forms (i.e., those with limited additions, such as salt, butter, or creamy sauces).
• Choose lower sodium varieties of frozen or canned vegetables.
Fruits• All fresh, canned, frozen, and dried forms and
100% fruit juice can be part of a healthy eating pattern.
• At least half of the recommended fruit intake should come from whole fruits.
• Select canned fruit options that are lowest in added sugars.
Grains• Include whole grains and limit the intake of
refined grains and products made with refined grains, especially those high in saturated fats, added sugars, and/or sodium, such as cookies, cakes, and some snack foods.
• At least half of grain intake should be whole grains.
• Refined grains should be enriched.• Whole grains should include some grains, such
as some wholegrain ready-to-eat breakfast cereals, that have been fortified with folic acid.
Dairy• Include fat-free and low-fat (1%) dairy, including
milk, yogurt, cheese, or fortified soy beverages (commonly called “soymilk”).
• Those who do not consume dairy products should consume foods that provide the range of nutrients generally obtained from dairy, including protein, calcium, potassium, magnesium, vitamin D.
Protein Foods• Include a variety of protein foods in
nutrient-dense forms.• Seafood, meats, poultry, eggs, nuts, seeds, soy
products, and legumes (beans and peas) may be included.
• Consume at least 8 ounce-equivalents of seafood per week to ensure adequate essential fatty acids.
• Unsalted nuts or seeds should be eaten in small portions and used to replace other protein foods.
• Choose lean meats.• Intake of processed forms of meat, poultry, and
seafood can be accommodated as long as sodium, saturated fats, added sugars, and/or total calories are within limits of healthy eating patterns.
Oils• Although not a food group, oils are part of
healthy eating patterns because they are the major source of essential fatty acids and vitamin E.
• Healthy oils are extracted from plants (e.g., canola, corn, olive, peanut, safflower, soybean, and sunflower oils), and are naturally present in nuts, seeds, seafood, olives, and avocados.
• Coconut oil, palm kernel oil, and palm oil intake is not part of this recommendation because these oils are high in saturated fats.
• Oils should replace solid fats rather than being added to the diet.
1. Follow a healthy eating pattern across the lifespan. All food and beverage choices matter. Choose a healthy eating pattern at an appropriate calorie level to help achieve and maintain a healthy body weight, support nutrient adequacy, and reduce the risk of chronic disease. Eating patterns are the combination of foods and drinks that a person eats over time. A healthy eating pattern includes fruits, vegetables, protein, dairy, grains, and oils and limits saturated fats, trans fats, added sugar, and sodium.
2. Focus on variety, nutrient density, and amount. To meet nutrient needs within calorie limits, choose a variety of nutrient-dense foods across and within all food groups in recommended amounts. Nutrient dense foods provide vitamins, minerals, and other substances that contribute to good health, and have limited amounts of solid fats, added sugars, refined starch, and sodium. All vegetables, fruits, whole grains, seafood, eggs, beans and peas, unsalted nuts and seeds, fat-free and low-fat dairy products, and lean meats and poultry are nutrient-dense foods when prepared with little or no added solid fats, sugars, refined starches, and sodium.
3. Limit calories from added sugars and saturated fats and reduce sodium intake. Consume an eating pattern low in added sugars, saturated fats, and sodium. Cut back on foods and beverages higher in these components to amounts that fit within healthy eating patterns.
4. Shift to healthier food and beverage choices. Choose nutrient-dense foods and beverages across and within all food groups in place of less healthy choices. Consider cultural and personal preferences to make these shifts easier to accomplish and maintain.
5. Support healthy eating patterns for all. Everyone has a role in helping to create and support healthy eating patterns in multiple settings nationwide, from home to school to work to communities.
• Foods from all of the food groups should be
• Overweight adults should not gain additional • Overweight adults should not gain additional weight and those with CVD risk factors (e.g., hypertension and hyperlipidemia) should change eating and physical activity
to lose weight.
• To lose weight, most people need to reduce the number of calories from foods and
• Eating patterns that contain 1200 to 1500 calories each day can help most women lose
• Eating patterns that contain 1500 to 1800 calories each day help most men safely lose
• Overweight adults should not gain additional weight and those with CVD risk factors (e.g., hypertension and hyperlipidemia) should change
• To lose weight, most people need to reduce the number
• Eating patterns that contain 1200 to 1500 calories each day can help most women lose
• Eating patterns that contain 1500 to 1800 calories each day
57CHAPTER 2 Tools of a Healthy Diet
alcoholism, and foodborne illness. The Dietary Guidelines also guide government nutri-tion programs, research, food labeling, and nutrition education and promotion. For exam-ple, the Dietary Guidelines provide the scientific basis for the design of federal nutrition assistance programs, such as the USDA’s school breakfast and lunch programs, SNAP (Supplemental Nutrition Assistance Program), and the WIC Program (Special Supplemen-tal Nutrition Program for Women, Infants, and Children). In addition, MyPlate is based on the recommendations of the Dietary Guidelines (see the next section in this chapter).
A basic premise of the Dietary Guidelines is that nutrient needs should be met primar-ily by consuming foods.17 Foods provide an array of nutrients and other compounds that may have beneficial effects on health. In certain cases, fortified foods and dietary supple-ments may be useful sources of one or more nutrients that otherwise might be consumed in less than recommended amounts. These practices are especially important for people whose typical food choices lead to a diet that cannot meet nutrient recommendations, such as for calcium. However, dietary supplements are not a substitute for a healthful diet.
Final PDF to printer
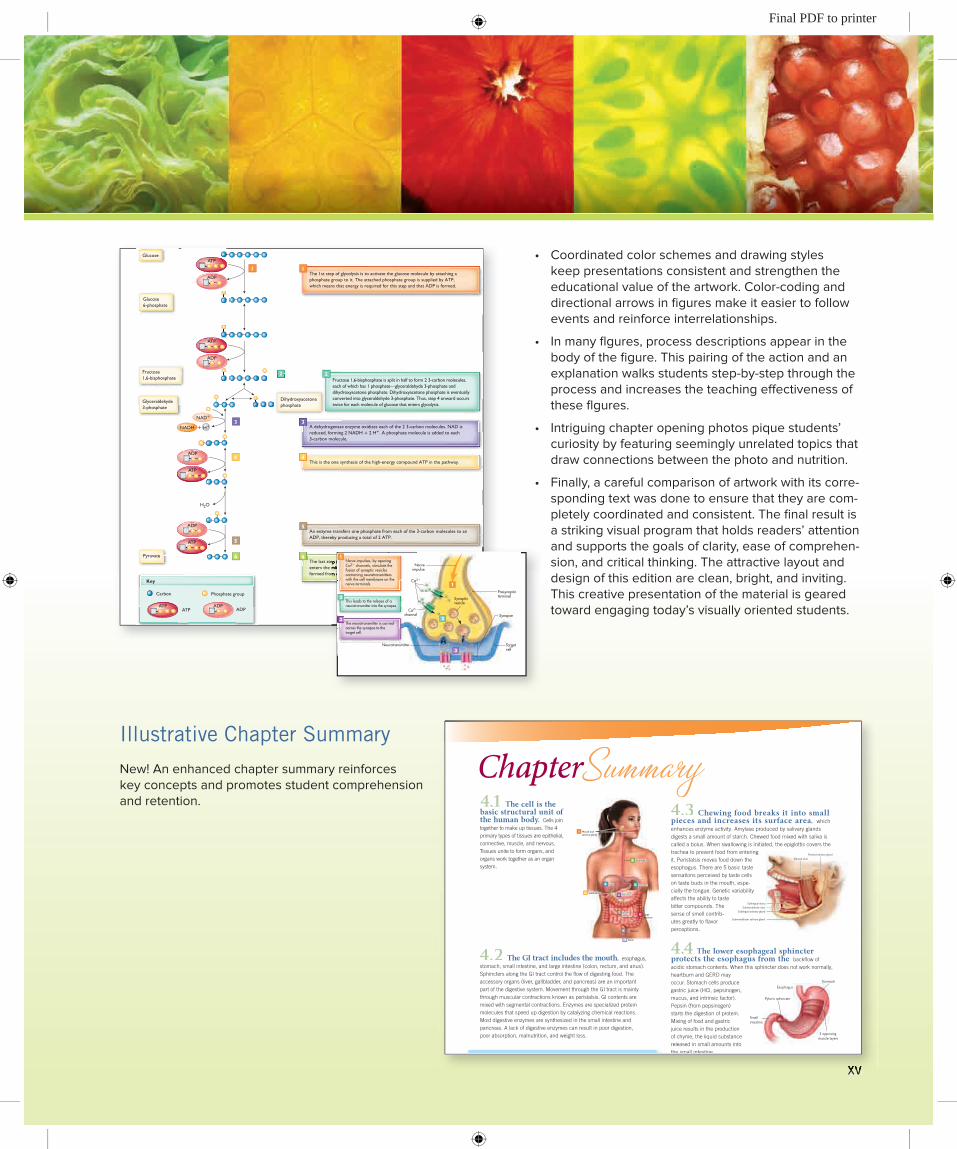
xv
• Coordinatedcolorschemesanddrawingstyleskeep presentations consistent and strengthen the educational value of the artwork. Color-coding and directional arrows in figures make it easier to follow events and reinforce interrelationships.
• Inmanyflgures,processdescriptionsappearinthebody of the figure. This pairing of the action and an explanation walks students step-by-step through the process and increases the teaching effectiveness of these flgures.
• Intriguingchapteropeningphotospiquestudents’curiosity by featuring seemingly unrelated topics that draw connections between the photo and nutrition.
• Finally,acarefulcomparisonofartworkwithitscorre-sponding text was done to ensure that they are com-pletely coordinated and consistent. The final result is a striking visual program that holds readers’ attention and supports the goals of clarity, ease of comprehen-sion, and critical thinking. The attractive layout and design of this edition are clean, bright, and inviting. This creative presentation of the material is geared toward engaging today’s visually oriented students.
~ ~
~
~~~~~~~~~ ~~~~~~~~~~~
~~~~~~~~
~ ~
~
~~~~~~~~~ ~~~~~~~~~~
~~~~~~~~
~ ~
~
~~~~~~~~~~ ~~~~~~~~~~
~~~~~~~~
~ ~~~~~~~~~~~ ~~~~~~~~~~ ~~~~~~~~~
~ ~
~
~~~~~~~~~~~ ~~~~~~~~~~~
~~~~~~~~
2
Key
Carbon Phosphate group
ATP ADP
Glucose
Glucose 6-phosphate
Fructose 1,6-bisphosphate
Glyceraldehyde 3-phosphate
Pyruvate
H2O
~
~
ATP
ADP
ATP
ADP
ATP
ADP
ATP ADP
The 1st step of glycolysis is to activate the glucose molecule by attaching aphosphate group to it. The attached phosphate group is supplied by ATP,which means that energy is required for this step and that ADP is formed.
1
The last step in glycolysis is the formation of pyruvate. Generally, pyruvateenters the mitochondria for further metabolism. A total of 2 pyruvates areformed from each glucose that enters glycolysis.
66
This is the one synthesis of the high-energy compound ATP in the pathway.44
An enzyme transfers one phosphate from each of the 3-carbon molecules to anADP, thereby producing a total of 2 ATP.
5
5
A dehydrogenase enzyme oxidizes each of the 2 3-carbon molecules. NAD isreduced, forming 2 NADH + 2 H+. A phosphate molecule is added to each3-carbon molecule.
33
2
1
+ H+NADH
NAD+
Dihydroxyacetone phosphate
ATP
ADP
Fructose 1,6-bisphosphate is split in half to form 2 3-carbon molecules,each of which has 1 phosphate—glyceraldehyde 3-phosphate anddihydroxyacetone phosphate. Dihydroxyacetone phosphate is eventuallyconverted into glyceraldehyde 3-phosphate. Thus, step 4 onward occurstwice for each molecule of glucose that enters glycolysis.
291CHAPTER 9 Energy Metabolism
Figure 9-7 Glycolysis takes place in the cytosol portion of the cell. This process breaks glucose (a 6-carbon compound) into 2 units of a 3-carbon compound called pyruvate. More details can be found in Appendix C.
The last step in glycolysis is the formation of pyruvate. Generally, pyruvateenters the mitochondria for further metabolism. A total of 2 pyruvates areenters the mitochondria for further metabolism. A total of 2 pyruvates areformed from each glucose that enters glycolysis.
Nerve impulses, by openingCa2+ channels, stimulate thefusion of synaptic vesiclescontaining neurotransmitterswith the cell membrane on thenerve terminals.
1
The neurotransmitter is carriedacross the synapse to thetarget cell.
3
This leads to the release of aneurotransmitter into the synapse.
2
1
3
2
Ca2+
Nerveimpulse
Synapticvesicle
Neurotransmitter Targetcell
Presynapticterminal
SynapseCa2+
channel
522 PART 4 Vitamins and Minerals
During times of growth, total osteoblast activity exceeds osteoclast activity, so we make more bone than we break down. This also can occur when bone is put under high stress—a right-handed tennis player, for example, builds more bone in that arm than in the left arm. Most bone is built from infancy through the late adolescent years. Calcium recom-mendations are set high during these times to support this bone-building activity. Small increases in bone mass continue between 20 and 30 years of age. Genetic background con-trols up to 80% of the variation in the peak bone mass ultimately built.56
Throughout adulthood, bone remodeling is ongoing. In fact, most of the adult skeleton is replaced about every 10 years.57 However, beginning in middle age, osteoclast activity generally becomes more dominant in both men and women. This can result in a total loss of about 25% of bone, depending on how long the person lives.57 Women experience even greater bone loss when estrogen levels fall in menopause because estrogen inhibits bone breakdown by decreasing osteoclast activity. Women can experience an additional 20% loss of bone in the first 5 to 7 years following menopause.56,57 Absent or irregular menses in younger women, which can occur because of very low body weight, eating disorders, or the female athlete triad (see Chapter 11), signal low estrogen levels and a likelihood of substan-tial bone loss before middle age. When the rate of bone loss exceeds the rate at which bone is rebuilt, bone mass and bone strength decline and the risk of fracture rises greatly. Significant bone mass loss, known as osteoporosis, is discussed in Clinical Perspective: Osteoporosis.
Blood Clotting
Calcium ions participate in several reactions in the cascade that leads to the formation of fibrin, the main protein component of a blood clot. (See Fig. 12-21 in Chapter 12 for more details on blood clotting.)
Transmission of Nerve Impulses to Target Cells
When a nerve impulse reaches its target site—such as a muscle, other nerve cells, or a gland—the impulse is transmitted across the synapse, the junction between the nerve and its target cells. In many nerves, the arrival of the impulse at the target site causes calcium ions from the extracellular medium to flow into the nerve. The rise in calcium ions in the nerve triggers synaptic vesicles to release their store of neurotransmitters. The released neu-rotransmitter then carries the impulse across the synapse to the target cells (Fig. 14-20).
Figure 14-20 The release of neurotransmitters from nerve cells requires an influx of calcium through specialized calcium channels. This physiological function of calcium is vital for normal functioning of the nervous system.
Milk provides good amounts of many of the
nutrients needed for building bone. Drinking milk
during childhood (the bone-building years) is
associated with a lower risk of fracture later in life.
The tooth consists of a hard, yellowish tissue
called dentin, which is covered with enamel in
the crown and cementum in the root. Enamel, the
hardest substance in the body, is almost entirely
hydroxyapatite crystals. Produced before the tooth
erupts, enamel is not a living tissue and, unlike
bone, does not undergo remodeling. Enamel can
be easily damaged by acids produced by bacteria
in the mouth from the metabolism of sugars and
carbohydrates. This damage is known as dental
caries, or cavities. Repairing dental caries requires
the skills of a dentist. The number of dental caries
in the U.S. population has declined because of
the addition of fluoride to some municipal water
supplies, bottled water, and oral care products.
Fluoride helps strengthen the enamel and makes it
more resistant to acids. It also helps remineralize
enamel in the earliest stages of damage.
bone resorption Process in which osteoclasts break down bone and release minerals, result-ing in a transfer of calcium from bone to blood.
tetany Continuous, forceful muscle contraction without relaxation.
xv
149
4.1 The cell is the basic structural unit of the human body. Cells join together to make up tissues. The 4 primary types of tissues are epithelial, connective, muscle, and nervous. Tissues unite to form organs, and organs work together as an organ system.
Chewing food breaks it into small pieces and increases its surface area, which enhances enzyme activity. Amylase produced by salivary glands digests a small amount of starch. Chewed food mixed with saliva is called a bolus. When swallowing is initiated, the epiglottis covers the trachea to prevent food from entering it. Peristalsis moves food down the esophagus. There are 5 basic taste sensations perceived by taste cells on taste buds in the mouth, espe-cially the tongue. Genetic variability affects the ability to taste bitter compounds. The sense of smell contrib-utes greatly to flavor perceptions.
The lower esophageal sphincter protects the esophagus from the backflow of acidic stomach contents. When this sphincter does not work normally, heartburn and GERD may occur. Stomach cells produce gastric juice (HCl, pepsinogen, mucus, and intrinsic factor). Pepsin (from pepsinogen) starts the digestion of protein. Mixing of food and gastric juice results in the production of chyme, the liquid substance released in small amounts into the small intestine.
The small intestine has 3 sections: duodenum, jejunum, and ileum. Most digestion occurs in the small intestine. Secretions from the liver, gallbladder, and pancreas are released into the small intestine. These secretions contain enzymes, bile, and sodium bicarbonate. Villi in the small intestine greatly increase its surface area, which enhances absorption. Villi are lined by enterocytes that release enzymes. Enterocytes
Organs Digestive Functions
Mouth and salivary glands
Prepare food for swallowing: chewing, moistening with salivaDetect taste moleculesStart digestion of starch with amylase enzyme
Esophagus Moves food to stomach by peristaltic waves initiated by swallowing
Stomach Secretes gastric juice containing acid and enzymesMixes food with gastric juice, converting it to liquid chymeStarts digestion of protein with pepsin enzymeKills microorganisms with acidSecretes intrinsic factor, a protein required for vitamin B-12 absorption Slowly releases chyme to the small intestine
Liver Produces bile to aid fat digestion and absorption
Gallbladder Stores and concentrates bile and releases it to the small intestine
Pancreas Secretes pancreatic juice containing digestive enzymes and bicarbonate into the small intestine
Small intestine Mixes chyme with bile and pancreatic juice to complete digestionAbsorbs nutrients and other compounds in foods Transports remaining residue to large intestine
Large intestine (colon)
Absorbs water and electrolytes (sodium and potassium)Forms and stores fecesHouses most of the gut microbiota
Rectum Holds and expels feces via the anus
Table 4-2 Overview of Digestion and Absorption GI Tract Functions
SummaryChapter
4.2
4.3
4.4
Smallintestine Large
intestine
Stomach
Esophagus
Liver
Mouth andsalivary glands
Stomach
Rectum
Anus
Esophagus
1
Gallbladder6Pancreas4
2
3
8
9
7
5
10
The GI tract includes the mouth, esophagus, stomach, small intestine, and large intestine (colon, rectum, and anus). Sphincters along the GI tract control the flow of digesting food. The accessory organs (liver, gallbladder, and pancreas) are an important part of the digestive system. Movement through the GI tract is mainly through muscular contractions known as peristalsis. GI contents are mixed with segmental contractions. Enzymes are specialized protein molecules that speed up digestion by catalyzing chemical reactions. Most digestive enzymes are synthesized in the small intestine and pancreas. A lack of digestive enzymes can result in poor digestion, poor absorption, malnutrition, and weight loss.
Parotid duct
Parotid salivary gland
Sublingual ducts
Sublingual salivary gland
Submandibular salivary gland
Submandibular duct
Small intestine
Stomach
3 opposing muscle layers
Esophagus
Pyloric sphincter
Stomach
Ducts from liver
Common bile duct
GallbladderPancreatic duct
Jejunum
Accessorypancreatic duct
Duodenum
Hepatopancreatic sphincter
Illustrative Chapter Summary
New! An enhanced chapter summary reinforces key concepts and promotes student comprehension and retention.
Final PDF to printer
xvi
Global Updates and Changes
• CompleteDietaryGuidelinesupdatetoinclude2015–2020recommendations.
• Theentiretentheditionhasbeenupdated,refined,andstreamlined to enhance learning.
• NewfeaturesthroughoutthetentheditionincludeHistorical Perspectives, Perspectives on the Future, and illustrative end-of-chapter summaries.
Chapter 1, The Science of Nutrition
• NewPerspective on the Future, “Nutritional Genomics,” added.• “ThePriceofFood,”anewGlobal Perspective created.• GeneticsandnutritionisnowaClinical Perspective.• NewHistorical Perspective, “War on Pellegra,” included.• Updatedstatisticsonleadingcausesofdeath.• Fresh,newphotosforvisualengagement.• Sectionintroducingsystematicreviews,includingtheAcademy
of Nutrition and Dietetics’ Evidence Analysis Libraries and Cochrane Collaboration, included.
Chapter 2, Tools of a Healthy Diet
• CompleteDietaryGuidelinesupdatetoinclude2015–2020recommendations.
• Extensivelyrevisedthefigure(figure2.6)summarizingtheDietary Guidelines to reflect the five overarching concepts of the2015–2020DietaryGuidelines.
• AddedanewfiguretographicallyillustratetheproportionofAmericans currently meeting dietary intake goals.
• UpdatedcoverimageoftheDietaryGuidelinesreport.• Perspective on the Future, “Updating the Nutrition Facts
Panel,” added.• Portionsizeestimatephotosenrichedandexpanded.• Enhancedpresentationontheoriginandevolutionoffood
enrichment.• Expert Perspective revised to showcase the menu labeling policies.
Chapter 3, The Food Supply
• Updateddomesticandinternationalfoodinsecuritystatisticshighlighting the worldwide burden of malnutrition and hunger.
• Sectiononorganicfoodsandgeneticallymodifiedfoodsupdated.• Expandeddiscussionoffoodadditives,drawingattentionto
inadequate safety testing of some food additives.• Historical Perspective on features the early use of food
preservation compounds, such as sodium nitrate and sodium nitrite.
• Emergingtrendsrelatedtonorovirusinfectionsoncruiseshipsincluded.
• Additionofthepharmaceuticalcompoundbotox,derivedfromthe foodborne illness bacterium Clostridum botulinum, linking text concepts to novel applications.
Connecting with the Latest Updates
• LatestCDCfoodborneillnessstatisticsincluded.• NewTake Action personalizing food safety practices and risks.
Chapter 4, Human Digestion and Absorption
• NewPerspective on the Future featuring potential relationships between gut microbiota and health conditions, such as type 2 diabetes and obesity.
• Tableaddedtosummarizethefunctionsoftheorgansofthegastrointestinal system.
• Innovativenewfigureadded,clearlyillustratingtheprocessesof mixing, segmentation, and peristalsis.
• Conditionofdrymouth,relatedtodecreasedsalivaproduction, added.
• EngagingHistorical Perspective featuring Dr. William Castle’s novel research method leading to the discovery of a substance in gastric secretions required for absorption of vitamin B-12.
• New,enhancedphotoclearlyillustratingthestructureofthesmall intestine.
• Global Perspective on diarrhea in infants and children updated with latest statistics.
• Discussionofrelationshipsamonggutmicrobiotaandhealthand disease expanded.
• BristolStoolScale,atoolfordescribingcharacteristicsofstools, added.
• NewTake Action, which helps students investigate gluten content of grains.
• NewTake Action teaches students how dietary patterns may contribute to digestive health.
• Expert Perspective from the Field updated to include new terminology and statistics for gluten-related disorders.
Chapter 5, Carbohydrates
• Updatedinformationonnon-nutritivesweetenershighlightingthe sweetness level of alternatives compared to sucrose.
• Expandedfigureonthestructureofpolysaccharides,increasing the clarity of similarities and differences in carbohydrate chemistry.
• Statisticsoncarbohydrateandsugarconsumptionrevised.• UpdatedExpert Perspective “Taxing Sugar-Sweetened
Beverages”.• NewfigurecomparingaddedsugarsourcesoftheU.S.
population.• Fiberconsumptionpresentationenhancedwithafigure
comparing fiber intake by nation.• Revisedfigureclarifyingtheabsorptionofglucoseinthesmall
intestine.• Clinical Perspective “Diabetes Mellitus” enhanced with lab
values for diagnosis and medical nutrition therapy.• Historical Perspective featuring the development of
techniques to better determine the molecular structure of
Final PDF to printer

xvii
vitamin B-12, vitamin D, and insulin by Dorothy Crowfoot Hodgkin.
• Critical Thinking feature added to address city-mandated limit on sweetened beverage consumption.
Chapter 6, Lipids
• Enhanceddiscussionofcholesterolsources.• Restructuredpresentationoflipidtransport.• NewCritical Thinking feature on fat and weight loss.• NewCase Study focusing on the links between eating
practices as a young adult and chronic disease risk in later adulthood.
• Updatedtableonfatintakerecommendations.• NewgraphillustratingbloodcholesteroltrendsintheU.S.• StreamlinedExpert Perspective “Omega-6 Fatty Acids: Harmful
or Healthful?” and new illustrative table.• Revisedimageillustratingincorporationoftriglycerides
into fat cells.
Chapter 7, Proteins
• Perspective on the Future “Timing Protein Intake” added.• Streamlinedfiguredepictingtransaminationanddeamination.• Clarifiedfigureshowingproteinsynthesis.• FoodproteinallergiesformattedasaClinical Perspective.• Latestresearchonmeatintakeandhealthincorporated.
Chapter 8, Alcohol
• Alcoholusestatisticsupdated.• Newfigureclearlyillustratingthesizeofastandarddrink.• Newfiguredemonstratingtherelationshipamongblood
alcohol content, behaviors, feelings, and impairments.• NewfigureilllustratingtheJ-shapedrelationbetweenalcohol
intake and health risks.• Statisticsonfetalalcoholspectrumdisordersupdated.• NewTake Action, helping students evaluate myths about
alcohol intake.
Chapter 9, Energy Metabolism
• Newfigurecontrastinganabolicandcatabolicreactions.• Clarifiedfiguredemonstratingniacin’sandriboflavin’srolesin
energy metabolism.• Improvedfigureshowingaerobiccarbohydratemetabolism.• AdditionofdiscussionandfigureontheCoricycle.• NewsectiononATPrecycling.• EnhanceddiscussionofATPproduction.• Streamlinedglycolysisfigure.• Newanerobicglycolysisfigureandupdatedbeta-oxidation
figure.• Figuresrestyledtoenhancestudentunderstanding.• NewStudyQuestionsaddedtopromotelearning.
Chapter 10, Energy Balance, Weight Control, and Eating Disorders
• LatestmapofobesityratesintheU.S.• Perspective on the Future “Rethinking the Calories in a Pound
of Fat” added.• Enhanceddiscussionofbrownadiposetissue.• Clarifiedpresentationonshort-termsatietycontrol.• Newheadingsaddedtoguidestudyofeatingbehaviorregulation.• Additionalheadingsinsertedtoimproveunderstandingof
types of fad diets.• Eatingdisorderssectionoverhauledandstreamlinedtoreflect
latest diagnostic criteria (DSM-5).
Chapter 11, Nutrition, Exercise, and Sports
• Expandedsectiononwarm-upandcool-downphysicalexercise activities.
• Clarifiedfigureillustratingenergysourcesformuscularactivity.• EnhancedfigureillustratingATPformationfromthe
macronutrients.• Historical Perspective feature on oral rehydration added.• Proteinrecommendationsupdatedtoreflectcurrent
evidence-based literature.
Chapter 12, The Fat-Soluble Vitamins
• LatestdataonantioxidantsupplementsfromtheAge-RelatedEye Disease (ARED) Study 2 Group incorporated.
• Updateddietarysupplementssection.• Critical Thinking on vitamin A food sources added.• Critical Thinking on carotenoid foods updated.• Global Perspective on vitamin A deficiency revised with new
statistics added.• Casestudyonsupplementintakeupdated.• Historical Perspective highlighting the work of Elmer
McCollum, the discovery of B vitamins and vitamin D added.
Chapter 13, The Water-Soluble Vitamins
• Water-solublevitaminintakes,prominentfoodsources,andthe prevalence of inadequate intake statistics updated.
• Newcasestudyonvitamindeficiencyincorporated.• Historical Perspective about the work of Christjaan Eijkman to
discover the cure for beriberi added.• Updatedinformationonthepharmacologicaluseofvitamin B-6.• Ready-to-eatbreakfastcerealsproviding100%oftheDaily
Value for folic acid included.• NewtablesummarizingcausesofvitaminB-12deficiency.• Historical Perspective describing the work of Albert Szent-Gyorgyi
in identifying the oxidation and reduction functions of vitamin C added.
• Carnitineandtaurinediscussionupdated.
Final PDF to printer

xviii
Chapter 14, Water and Major Minerals
• Enhancedinformationontheconsumptionofwaterandsweetened beverages.
• Expandeddiscussionofdehydrationanditscauses.• Newtablesummarizingthefactorsinfluencingmineral
bioavailability.• Lateststatisticsonmajormineralintakes,prominentfood
sources, and the prevalence of inadequate intake included.• Newtablesummarizingrecommendationsfordietarysodium
intake.• NewfiguredisplayingsourcesofdietarysodiumintheU.S.diet.• Updatedtablesummarizingtheeffectoflifestylemodification
on blood pressure lowering.• New,detailedclinicalcase,helpingstudentsdescribethe
effects of diet and physical activity on blood pressure and make recommendations for improvement.
• NewrecommendationsfromtheU.S.PreventiveServicesforthe routine use of calcium supplements included.
• Newfigureillustratingtheregulationofserumcalciumincluded.
Chapter 15, Trace Minerals
• NewGlobal Perspective on the e-Library of Evidence for Nutrition Actions identifing a credible source for accessing evidenced-based information related to nutrition interventions across the globe.
• Newfiguretoillustratefoodsourcesofironandoverallironabsorption incorporated.
• Casestudyoniron-deficiencyanemiaaddedtohelpenhancestudent integration of knowledge about food sources of iron intake, clinical symptoms, and related biochemical data.
• Statisticsaboutthefluoridationofthewatersupplysystemsupdated.
• Clinical Perspective “Nutrients, Diet, and Cancer” updated to reflect latest data.
• Statisticsforirondeficiencyrevised.• Informationoniodinedeficiencyandaccesstoiodizedsalt
worldwide updated.
Chapter 16, Nutritional Aspects of Pregnancy and Breastfeeding
• Perspective on the Future “Fetal Origins of Disease” added.• Historical Perspective “The First 10 Minutes of Life”
incorporated.• Fresh,newphotos,enhancingvisualengagement.• Effectsofadvancesinreproductivetechnologyonmultiple
births and nutrient needs introduced.• Definitionof“term”deliveriesincorporated.• Criticalroleofmaternalweightonpregnancyoutcomenow
featured in its own section.• Newheadings,highlightingkeyaspectsofthematernalfood
supply on pregnancy outcome.
Chapter 17, Nutrition during the Growing Years
• SeparateClinical Perspectives focusing on potential nutrition-related problems during infancy, childhood, and adolescence created.
• Enhancedtabledescribingthephysicalandeatingskillsofyoung children.
• Imagesaddedtotabledescribingfood-relatedskillsofpreschoolers to enhance understanding of child development.
• NewHealthyEatingDailyPlanforPreschoolersfigureincluded.
• Global Perspective “Autism” expanded to include latest nutrition-related findings.
• FDAbanonbisphenolAinbabybottlesandsippycupsaddressed.
• Parentresponsibilitiesforchildandteennutritiontablerestyled to promote better comprehension.
Chapter 18, Nutrition during the Adult Years
• Updatedandenhancedtablesummarizingpopularherbalremedies, nutrient supplements, and hormones.
• Expandeduseofphotostoreinforcekeyconcepts.• Enhanceddiscussionofthecompressionofmorbidityfigure.• Exerciserecommendationsforolderadultsupdatedand
expanded.• WarningsignsofAlzheimerdiseaseupdatedtolatestcriteria.
Final PDF to printer
Connections That Suit Your Needs
xix
Logical Organization, Flexible Sequencing
This new edition addresses the curricular realities of today’s college coursework by organizing and consolidating the content into 5 main parts and 18 chapters. This organization presents the core content in a thorough yet manageable fashion. To give instructors even greater flexibility in tailoring reading assignments to course requirements and cross-referencing lectures to the book, each major section in the chapters is numbered. If, for example, an instructor plans to address only part of a chapter on a certain day, he or she can direct students to focus on just those sections.
Assessment and Evaluation of Learning
One of our primary goals as nutrition educators is to ensure that students leave our courses with a meaningful understanding of the nutrition principles and concepts they need to advance their education and improve their diets and health. Determining how well we have met this goal requires assessment, on both the student and the instructor levels. To this end, we have built in assessment tools that allow both students and instructors to measure their success:
• StudentLearningObjectivesatthebeginningofeachchapter• OnlinetestbankquestionscorrelatedtoindividualStudentLearningObjectives• KnowledgeCheckquestionsaftereachmajorsection• StudyQuestionsattheendofeachchapter• CriticalThinkingquestionsinthemargins
Customize your course materials to your learning outcomes!
Create what you’ve only imagined.
Introducing McGraw-Hill Create™—a self-service website that allows you to create custom course materials—print and eBooks—by drawing upon McGraw-Hill Education’s comprehensive, cross-disciplinary content. Add your own content quickly and easily. Tap into other rights-secured third-party sources as well. Then, arrange the content in a way that makes the most sense for your course.
Even personalize your book with your course name and informa-tion! Choose the best format for your course: color print, black-and-white print, or eBook. The eBook is now even viewable on an iPad®! And when you are done, you will receive a free PDF review copy in just minutes!
Finally, a way to quickly and easily create the course materials you’ve always wanted.
Imagine that!Visit McGraw-Hill Create—www.mcgrawhillcreate.com—today and begin building your perfect book.
Final PDF to printer
xx
AcknowledgmentsWe offer a hearty and profound thank you to the many individuals who have supported and guided us along the way.
To our loved ones: Without your patience, understanding, assistance, and encouragement, this work would not have been possible.
To our wonderful students—past, present, and future: The lessons you have taught us over the years have enlightened us and sustained our desire to provide newer, better opportunities to help you successfully launch your careers and promote healthful lifelong living.
To our amazing team at McGraw-Hill Education. Brand Managers, Marija Magner and Amy Reed and Product Developer Darlene Schueller—we thank you most of all for your confidence in us! We deeply appreciate your endless encouragement and patience as you expertly shepherded us along the way. A special thanks to Vice President, General Manager, Products & Markets Marty Lange, Managing Director Michael Hackett, and Marketing Manager Kristine Rellihan and the entire marketing team. Sincere thanks to Content Project Manager MaryJane Lampe for keeping production on track, Designer Matt Backhaus, and Copy Editor Debra DeBord for her meticulous attention to detail. We also thank Content Licensing Specialists Lorraine Buczek and Lori Hancock, Photo Researcher Mary Reeg, and the many talented illustrators and photographers for their expert assistance.
To Your Health!
Carol Byrd-Bredbenner Gaile Moe Jacqueline BerningDanita Kelley
Thank You, Reviewers and Symposium ParticipantsTo our conscientious, dedicated expert reviewers and instructors: Thank you for sharing your insightful and constructive comments with us. We truly appreciate the time you committed to reviewing this book and discussing your thoughts and goals for this course. We especially appreciate the assistance provided by Angie Tagtow, Cynthia Kupper, Stephanie Atkinson, Maureen Story, Penny Kris-Etherton, Wahida Karmally, Robert P. Heaney, Judith Rodriguez, Clare Hasler-Lewis, Kelly Brownell, Margo Wootan, and Judi Adams, those who shared their expertise in compiling the Expert Perspective from the Field features. Your suggestions and contributions clearly reflect dedication to excel-lence in teaching and student learning and are invaluable to this edition.
List of ReviewersSheila Barrett Northern Illinois University
Renee Barrile UMass Lowell
Cynthia Blanton Idaho State University
Angelina Boyce Hillsborough Community College
Kurt Campbell Northern Oklahoma College
Gale Carey University of New Hampshire
Caryn Coffman Cuesta College
Mary Dean Coleman-Kelly The Pennsylvania State University
Ilko G. Iliev Southern University at Shreveport
Karen Israel Anne Arundel Community College
Mark Knauss Georgia Highlands College
Allen Knehans University of Oklahoma Health Sciences Center
Final PDF to printer
xxi
Robert Lee Central Michigan University
Makuba Lihono University of Arkansas at Pine Bluff
Mary Katherine Lockwood University of New Hampshire
Doug Mashek University of Minnesota
Debra Mason Mt. Hood Community College
Mary P. Miles Montana State University
Judith Myhand Louisiana State University
Lisa Nicholson California Polytechnic State University–San Luis Obispo
Ryan Paruch Tulsa Community College
Eleanor B. Pella Harrisburg Area Community College Mount St. Mary’s University
Christian Roberts UCLA
Daniel H. Rowlson Oakland Community College
Amy Schmidt Edinboro University of Pennsylvania
Karla Shelnutt University of Florida
Melissa M. Shock University of Central Arkansas
Bernice G. Spurlock Hinds Community College
Chris Wendtland Monroe Community College
Najat Yahia Central Michigan University
Symposium ParticipantsLaurie Allen University of North Carolina at Greensboro
Hawley C. Almstedt Loyola Marymount University
Alex Kojo Anderson University of Georgia
Catherine M. Berry University of Wisconsin–Eau Claire
Jackie Buell Ohio State University
Melanie Tracy Burns Eastern Illinois University
Thomas W. Castonguay University of Maryland
Prithiva Chanmugam, Emeritus Louisiana State University
Mary Dean Coleman-Kelly The Pennsylvania State University
Janet Colson Middle Tennessee State University
Maggi Dorsett Butte College
Sara Bachman Ducey Montgomery College
Julia Erbacher Salt Lake Community College
Eugene J. Fenster Metropolitan Community College–Longview
Katie Ferraro University of California, San Francisco
William A. Forsythe East Carolina University
Lisa Gurule Central New Mexico Community College
Donna Handley University of Rhode Island
Final PDF to printer
xxii
Stacy Hastey Connors State College
Beverly W. Henry Northern Illinois University
Clarie B. Hollenbeck San Jose State University
Donna Huisenga Illinois Central College
Jasminka Ilich-Ernst Florida State University
Jean Jackson Bluegrass Community and Technical College
Thunder Jalili University of Utah
Janine Jensen Tulsa Community College
Demaree L. Johnson Dixie State University
Rachel Jones University of Utah
Shanil Juma Texas Woman’s University
Colleen Kvaska Fullerton College
Linda Johnston Lolkus Indiana University–Purdue University Fort Wayne
Anne B. Marietta Southeast Missouri State University
Suresh T. Mathews Auburn University
Molly M. Michelman University of Nevada, Las Vegas
Allison Miner Prince George’s Community College
Mithia Mukutmoni Sierra College
Kimberly B. Myers East Carolina University
Millicent Owens College of the Sequoias
Gloria Payne Middle Tennessee State University
Robin Polokoff Cal State University East Bay Diablo Valley College Las Positas College
Joan E. Quinn Northern Illinois University
Wanda Ragland Macomb Community College
Maureen Reidenauer Camden County College
Ruth A. Reilly University of New Hampshire
B. Burgin Ross University of North Carolina–Greensboro
Lisa A. Sheldon Greenfield Community College
Dana Sherman Ozarks Technical Community College
Ilse Silva-Krott Upper Iowa University
Carole Sloan Henry Ford Community College
Marsha Spence The University of Tennessee
Priya Venkatesan Pasadena City College
Ann Volk Antelope Valley College
Heidi Wengreen Utah State University
Najat Yahia Central Michigan University
Final PDF to printer

xxiii
Contents
Meet the Author Team viPreface vii
Part 1 Nutrition Basics
1 THE SCIENCE OF NUTRITION 2
1.1 Nutrition Overview 4Nutrients 4Phytochemicals and Zoochemicals 8
Expert Perspective from the Field: Functional Foods 9 1.2 Energy Sources and uses 10 1.3 The North American diet 12
What Influences Our Food Choices? 13Take Action: Why You Eat What You Do 14Global Perspective: The Price of Food 15
1.4 Nutritional Health Status 16Health Objectives for the U.S. for the Year
2020 16Assessing Nutritional Status 17Limitations of Nutritional Assessment 18Importance of Being Concerned about
Nutritional Status 19Getting Nutrition-Related Advice:
The Nutrition Care Process 19Clinical Perspective: Genetics and Nutrition 21Take Action: Create Your Family Tree for
Health-Related Concerns 24 1.5 Using Scientific Research to Determine
Nutrient Needs 24Making Observations and
Generating Hypotheses 25Laboratory Animal
Experiments 27Human Experiments 27
1.6 Evaluating Nutrition Claims and Products 31Buying Nutrition-Related
Products 31
Chapter Summary 33Study Questions 35References 37
2 TOOLS OF A HEALTHY DIET 38
2.1 Dietary Reference Intakes (DRIs) 40Estimated Average Requirements (EARs) 40Recommended Dietary Allowances (RDAs) 41Adequate Intakes (AIs) 42Tolerable Upper Intake Levels (Upper
Levels, or ULs) 42Estimated Energy Requirements (EERs) 42Acceptable Macronutrient Distribution
Ranges (AMDRs) 43Appropriate Uses of the DRIs 43Putting the DRIs into Action to Determine
the Nutrient Density of Foods 44 2.2 Daily Values (DVs) 45
Reference Daily Intakes (RDIs) 45Daily Reference Values (DRVs) 45Putting the Daily Values into Action on
Nutrition Facts Panels 47Take Action: Applying the Nutrition Facts Label to
Your Daily Food Choices 52Global Perspective: Front-of-Package Nutrition
Labeling 53 2.3 Nutrient Composition of Foods 53
Putting Nutrient Databases into Action to Determine Energy Density and Dietary Intake 54
Expert Perspective from the Field: Menu Labeling: How Many Calories Are in That? 55
2.4 Dietary Guidelines for Americans 56Putting the Dietary Guidelines into Action 58
Take Action: Are You Putting the Dietary Guidelines into Practice? 60
2.5 MyPlate 60Putting MyPlate into Action 61Rating Your Current Diet 66
Take Action: Does Your Diet Meet MyPlate Recommendations? 67
Chapter Summary 68Study Questions 70References 71
Final PDF to printer
xxiv
3 THE FOOD SUPPLY 72
3.1 Food Availability and Access 74Health Consequences of Malnutrition and
Food Insecurity 74Food Insecurity in the U.S. 75Programs to Increase Food Security in the
U.S. 76Food Insecurity and Malnutrition in the
Developing World 78 3.2 Food Production 79
Organic Foods 79Biotechnology—Genetically Modified Foods 80
3.3 Food Preservation and Processing 83Food Irradiation 84Food Additives 84
3.4 Food and Water Safety 87Foodborne Illness Overview 87
Take Action: A Closer Look at Food Additives 88Microbial Pathogens 89Water Safety 98Preventing Foodborne and Waterborne
Illnesses 99 3.5 Enviromental Contaminants in Foods 100
Lead 100Take Action: Check Your Food Safety Skills 102
Dioxins 103Clinical Perspective: Foodborne Illness Can Be
Deadly 104Mercury 105Polychlorinated Biphenyls (PCBs) 105Pesticides and Antibiotics 105
Global Perspective: Traveler’s Diarrhea 106Expert Perspective from the Field: Organic Foods
and Local Food Systems 109Chapter Summary 110Study Questions 112References 114
4 HUMAN DIGESTION AND ABSORPTION 116
4.1 Organization of the Human Body 118 4.2 Digestive System Overview 122
Anatomy of the GI Tract 123 GI Motility: Mixing and Propulsion 124Digestive Enzymes and other Secretions 124
4.3 Moving through the GI Tract: Mouth and Esophagus 126Taste and Smell 126Swallowing 127
4.4 Moving through the GI Tract: Stomach 128 4.5 Moving through the GI Tract: Small Intestine
and Accessory Organs 130Liver, Gallbladder, and Pancreas 131Gastrointestinal Hormones: A Key to
Orchestrating Digestion 132Absorption in the Small Intestine 133
Global Perspective: Diarrhea in Infants and Children 135
4.6 Moving Nutrients around the Body: Circulatory Systems 136Cardiovascular System 137Lymphatic System 137
4.7 Moving through the GI Tract: Large Intestine 137Gut Microbiota 138Absorption of Water and Electrolytes 139Elimination of Feces 139
4.8 When Digestive Processes Go Awry 140Heartburn and Gastroesophageal Reflux
Disease 140Ulcers 140Gallstones 142Food Intolerances 142Intestinal Gas 142Constipation 143
Take Action: Investigate Flours and Grains for Gluten Content 144
Expert Perspective from the Field: Gluten-related Disorders: Celiac Disease and Non-celiac Gluten Sensitivity 145
Diarrhea 146Irritable Bowel Syndrome 146Inflammatory Bowel Disease 147Hemorrhoids 147
Take Action: Are You Eating for a Healthy Digestive System? 148
Chapter Summary 149Study Questions 151References 152
Final PDF to printer
xxv
Part 2 Energy-Yielding Nutrients and Alcohol
5 CARBOHYDRATES 154 5.1 Structures of Carbohydrates 156
Monosaccharides: Glucose, Fructose, Galactose, Sugar Alcohols, and Pentoses 156
Disaccharides: Maltose, Sucrose, and Lactose 158
Oligosaccharides: Raffinose and Stachyose 159
Polysaccharides: Starch, Glycogen, and Fiber 159
5.2 Carbohydrates in Foods 162Starch 163Fiber 163Nutritive Sweeteners 163Non-Nutritive (Alternative) Sweeteners 165
Take Action: Choose the Sandwich with the Most Fiber 167
5.3 Recommended Intake of Carbohydrates 167Our Carbohydrate Intake 168
Take Action: Estimate Your Fiber Intake 171 5.4 Functions of Carbohydrates in the Body 171
Digestible Carbohydrates 171Indigestible Carbohydrates 172
5.5 Carbohydrate Digestion and Absorption 174Digestion 174Absorption 175
Expert Perspective from the Field: Taxing Sugar-Sweetened Beverages 176
5.6 Health Concerns Related to Carbohydrate Intake 177Very-High-Fiber Diets 177High Sugar Diets 177Lactose Intolerance 178Glucose Intolerance 178
Clinical Perspective: Diabetes Mellitus 179Glycemic Index and Glycemic Load 184
Chapter Summary 186Study Questions 188References 189
6 LIPIDS 190
6.1 Triglycerides 192Structure 192Naming Fatty Acids 194Essential Fatty Acids 195
6.2 Food Sources of Triglycerides 196Hidden Fats 198Fat Replacements 198
Take Action: Is Your Diet High in Saturated and Trans Fat? 199
6.3 Functions of Triglycerides 200Provide Energy 200Provide Compact Energy Storage 200Insulate and Protect the Body 200Aid Fat-Soluble Vitamin Absorption and
Transport 201Essential Fatty Acid Functions 201
6.4 Phospholipids 202Phospholipid Functions 202Sources of Phospholipids 203
6.5 Sterols 204Sterol Functions 204Sources of Sterols 204
6.6 Recommended Fat Intakes 205Mediterranean Diet 206Essential Fatty Acid Needs 206Our Fat Intake 206
6.7 Fat Digestion and Absorption 207Digestion 207Absorption 208
6.8 Transporting Lipids in the Blood 210Transporting Dietary Lipids Utilizes
Chylomicrons 210Transporting Lipids Mostly Made by
the Body Utilizes Very-Low-Density Lipoproteins 212
LDL Removal from the Blood 213HDL’s Role in Removing Blood LDL 213
Final PDF to printer
xxvi
6.9 Health Concerns Related to Fat Intake 214High Polyunsaturated Fat Intake 214Excessive Omega-3 Fatty Acid Intake 214Imbalances in Omega-3 and Omega-6 Fatty
Acids 214Intake of Rancid Fats 214
Expert Perspective from the Field: Omega-6 Fatty Acids: Harmful or Healthful? 215
Clinical Perspective: Cardiovascular Disease (CVD) 216
Diets High in Trans Fat 218Diets High in Total Fat 219
Take Action: What Is Your 10-Year Risk of Cardiovascular Disease? 220
Chapter Summary 222Study Questions 224References 225
7 PROTEINS 226
7.1 Structure of Proteins 228Amino Acids 228Synthesis of Non-
essential Amino Acids 229
Amino Acid Composition:Complete and Incomplete Proteins 230
7.2 Synthesis of Proteins 231Transcription and Translation of Genetic
Information 231Protein Organization 233Denaturation of Proteins 234Adaptation of Protein Synthesis to Changing
Conditions 234 7.3 Sources of Protein 234
Evaluation of Food Protein Quality 235 7.4 Nitrogen Balance 238
Recommended Intakes of Protein 238Take Action: Meeting Protein Needs When Dieting
to Lose Weight 240 7.5 Protein Digestion and Absorption 240 7.6 Functions of Proteins 242
Producing Vital Body Structures 243Maintaining Fluid Balance 243Contributing to Acid-Base Balance 244Forming Hormones, Enzymes, and
Neurotransmitters 245Contributing to Immune Function 245
Transporting Nutrients 245Forming Glucose 245
Expert Perspective from the Field: Nutrition and Immunity 246
Providing Energy 247 7.7 Health Concerns Related to
Protein Intake 247Protein-Energy Malnutrition 247High-Protein Diets 249
Clinical Perspective: Food Protien Allergies 250Global Perspective: How Big Is your Foodprint? 251
7.8 Vegetarian Diets 252 Take Action: Protein and the Vegan 254
Special Concerns for Infants and Children 255Chapter Summary 256
Study Questions 258References 259
8 ALCOHOL 260
8.1 Sources of Alcohol 262Production of Alcoholic Beverages 262
8.2 Alcohol Absorption and Metabolism 264Alcohol Metabolism: 3 pathways 264
8.3 Alcohol Consumption 267Take Action: Alcohol and Driving 269
8.4 Health Effects of Alcohol 269Guidance for Using Alcohol Safely 269Potential Benefits of Alcohol Intake 270Risks of Excessive Alcohol Intake 270Effects of Alcohol Abuse on Nutritional
Status 272Alcohol Consumption during Pregnancy and
Breastfeeding 274Global Perspective: Alcohol Intake around the
World 275 8.5 Alcohol Use Disorders: Alcohol Abuse and
Alcoholism 275Genetic Influences 276Effect of Gender 276Age of Onset of Drinking 276Ethnicity and Alcohol Abuse 277Mental Health and Alcohol Abuse 277
Clinical Perspective: Diagnosis and Treatment of Alcoholism 278
Take Action: Do You Know Why These are Alcohol Myths? 279
Chapter Summary 280Study Questions 282References 283
Final PDF to printer
xxvii
Part 3 Metabolism and Energy Balance
9 ENERGY METABOLISM 284
9.1 Metabolism: Chemical Reactions in the Body 286Converting Food into Energy 286Oxidation-Reduction Reactions: Key
Processes in Energy Metabolism 288 9.2 ATP Production from Carbohydrates 289
Glycolysis 290Transition Reaction: Synthesis of
Acetyl-CoA 290Citric Acid Cycle 292Electron Transport Chain 292The Importance of Oxygen 293 Anaerobic Metabolism 294
9.3 ATP Production from Fats 296ATP Production from Fatty Acids 296Carbohydrate Aids Fat Metabolism 298Ketones: By-products of Fat
Catabolism 298Ketosis in Diabetes 298Ketosis in Semistarvation or Fasting 298
9.4 Protein Metabolism 300Gluconeogenesis: Producing Glucose
from Glucogenic Amino Acids and Other Compounds 301
Gluconeogenesis from Typical Fatty Acids Is Not Possible 301
Disposal of Excess Amino Groups from Amino Acid Metabolism 301
Global Perspective: Cancer Cell Metabolism 302
9.5 Alcohol Metabolism 303 9.6 Regulation of Energy Metabolism 304
The Liver 306ATP Concentrations 306Enzymes, Hormones, Vitamins, and
Minerals 306 9.7 Fasting and Feasting 307
Fasting 307Feasting 308
Take Action: Weight Loss and Metabolism 310Clinical Perspective: Inborn Errors of
Metabolism 311Take Action: Newborn Screening in Your
State 312
Chapter Summary 313Study Questions 315References 316
10 ENERGY BALANCE, WEIGHT CONTROL, AND EATING DISORDERS 318
10.1 Energy Balance 320Energy Intake 321Energy Expenditure 322
10.2 Measuring Energy Expenditure 324 10.3 Eating Behavior Regulation 326 10.4 Estimating Body Weight and Composition 328
Body Mass Index 328Measuring Body Fat Content 328Assessing Body Fat Distribution 330
10.5 Factors Affecting Body Weight and Composition 332Role of Genetics 332Role of Environment 333Genetic and Environmental Synergy 334Diseases and Disorders 334
10.6 Treatment of Overweight and Obesity 335Control of Energy Intake 337Regular Physical Activity 337Control of Problem Behaviors 339
Expert Perspective from the Field: Tailoring a Healthy Eating Plan to Fit Your Lifestyle 341
Weight-Loss Maintenance 34210.7 Fad Diets 342
Clinical Perspective: Professional Help for Weight Control 346Take Action: Changing for the Better 348 10.8 Eating Disorders 350Prevalence and Susceptibility 350Anorexia Nervosa 351Bulimia Nervosa 354Binge-Purge Cycle 355Binge Eating Disorder 357Eating Disorders Not Otherwise Specified
(EDNOS) 358Other Related Conditions 358Prevention of Eating Disorders 358
Take Action: Assessing Risk of Developing an Eating Disorder 359
Chapter Summary 360Study Questions 362References 363
Final PDF to printer
xxviii
11 NUTRITION, EXERCISE, AND SPORTS 364
11.1 Benefits of Fitness 366 11.2 Characteristics of a Good Fitness Program 367
Mode 367Duration 367Frequency 367Intensity 367Progression 369Consistency 369Variety 369Achievement and Maintenance of
Fitness 369 11.3 Energy Sources for Muscle Use 371
ATP: Immediately Usable Energy 371Phosphocreatine: Initial Resupply of
Muscle ATP 371Take Action: How Physically Fit Are You? 372
Carbohydrate: Major Fuel for Short-Term, High-Intensity, and Medium-Term Exercise 375
Fat: Main Fuel for Prolonged, Low Intensity Exercise 378
Protein: A Minor Fuel Source during Exercise 379
Fuel Use and VO2max 380 11.4 The Body’s Response to Physical Activity 381
Specialized Functions of Skeletal Muscle Fiber Types 381
Adaptation of Muscles and Body Physiology to Exercise 381
11.5 Power Food: Dietary Advice for Athletes 382Energy Needs 382Carbohydrate Needs 383Fat Needs 386Protein Needs 386
Take Action: Meeting the Protein Needs of an Athlete: A Case Study 387
Vitamin and Mineral Needs 388
11.6 Fluid Needs for Active Individuals 389Fluid Intake and Replacement Strategies 391Water Intoxication 391Sports Drinks 392
11.7 Food and Fluid Intake before, during, and after Exercise 392Pre-Exercise Meal 392Fueling during Exercise 393Recovery Meals 394
Global Perspective: Gene Doping and the Wide World of Sports 395
11.8 Ergogenic Aids to Enhance Athletic Performance 395
Chapter Summary 398Study Questions 400References 401
Part 4 Vitamins and Minerals
12 THE FAT-SOLUBLE VITAMINS 402
12.1 Vitamins: Essential Dietary Components 404Absorption of Vitamins 404Malabsorption of Vitamins 404Transport of Vitamins 405Storage of Vitamins in the Body 405Vitamin Toxicity 406
12.2 Vitamin A 406Vitamin A in Foods 407Vitamin A Needs 408Absorption, Transport, Storage, and
Excretion of Vitamin A 409Functions of Vitamin A (Retinoids) 410Carotenoid Functions 411Vitamin A Deficiency Diseases 412Vitamin A Toxicity 413
Global Perspective: Vitamin A Deficiency 415 12.3 Vitamin D 416
Vitamin D2 in Foods 416Vitamin D3 Formation in the Skin 416Vitamin D Needs 417Absorption, Transport, Storage, and
Excretion of Vitamin D 417Functions of Vitamin D 419Vitamin D Deficiency Diseases 420Vitamin D Toxicity 421
Final PDF to printer
xxix
12.4 Vitamin E 422Vitamin E in Foods 422Vitamin E Needs 422Absorption, Transport, Storage, and
Excretion of Vitamin E 423Functions of Vitamin E 423Vitamin E Deficiency 425Vitamin E Toxicity 425
12.5 Vitamin K 425Vitamin K Sources 426Vitamin K Needs 426Absorption, Transport, Storage, and
Excretion of Vitamin K 426Functions of Vitamin K 426Vitamin K Deficiency 427
Take Action: Does Your Fat-Soluble Vitamin Intake Add Up? 428
Vitamin K Toxicity 428 12.6 Dietary Supplements: Healthful or Harmful? 430
Take Action: A Closer Look at Supplements 432Chapter Summary 433Study Questions 435References 436
13 THE WATER-SOLUBLE VITAMINS 438
13.1 Water-Soluble Vitamin Overview 440Coenzymes: A Common Role of
B-Vitamins 441Enrichment and Fortifi cation of Grains 442
13.2 Thiamin 443Thiamin in Foods 444Thiamin Needs and Upper Level 444Absorption, Transport, Storage, and
Excretion of Thiamin 445Functions of Thiamin 445Thiamin Deficiency 446
13.3 Riboflavin 447Riboflavin in Foods 447Riboflavin Needs and Upper Level 447Absorption, Transport, Storage, and
Excretion of Riboflavin 448Functions of Riboflavin 448Riboflavin Deficiency 449
13.4 Niacin 449Niacin in Foods 450Niacin Needs and Upper Level 451Absorption, Transport, Storage, and
Excretion of Niacin 451Functions of Niacin 451
Niacin Deficiency 452Pharmacological Use of Niacin 453
13.5 Pantothenic Acid 454Pantothenic Acid in Foods 454Pantothenic Acid Needs and Upper
Level 454Absorption, Transport, Storage, and
Excretion of Pantothenic Acid 454Functions of Pantothenic Acid 455Pantothenic Acid Deficiency 455
13.6 Biotin 456Sources of Biotin: Food and Microbial
Synthesis 456Biotin Needs and Upper Level 456Absorption, Transport, Storage, and
Excretion of Biotin 457Functions of Biotin 457Biotin Deficiency 457
13.7 Vitamin B-6 458Vitamin B-6 in Foods 458Vitamin B-6 Needs and Upper Level 458Absorption, Transport, Storage, and
Excretion of Vitamin B-6 459Functions of Vitamin B-6 459Vitamin B-6 Deficiency 460Pharmacological Use of Vitamin B-6 460
13.8 Folate 461Folate in Foods 461Dietary Folate Equivalents 462Folate Needs 462Upper Level for Folate 462Absorption, Transport, Storage, and
Excretion of Folate 462Functions of Folate 463Folate Deficiency 464
Clinical Perspective: Neural Tube Defects 466 13.9 Vitamin B-12 467
Vitamin B-12 in Foods 467Vitamin B-12 Needs and Upper Level 468Absorption, Transport, Storage, and
Excretion of Vitamin B-12 468Functions of Vitamin B-12 469Vitamin B-12 Deficiency 469
13.10 Choline 471Choline in Foods 471Choline Needs and Upper Level 471Absorption, Transport, Storage, and
Excretion of Choline 472Functions of Choline 472
Take Action: B-vitamin Supplements 473Choline Deficiency 473
Final PDF to printer
xxx
13.11 Vitamin C 474Vitamin C in Foods 474Vitamin C Needs 475Upper Level for Vitamin C 475Absorption, Transport, Storage, and
Excretion of Vitamin C 475Functions of Vitamin C 475Vitamin C Deficiency 477Vitamin C Intake above the RDA 479
13.12 Vitamin-like compounds 480Carnitine 480Taurine 480
Take Action: Spotting Fraudulent Claims for Vitamins and Vitamin-like Substances 481
Chapter Summary 482Study Questions 484References 486
14 WATER AND MAJOR MINERALS 488 14.1 Water 490
Water in the Body: Intracellular and Extracellular Fluids 490
Functions of Water 493Water in Beverages and Foods 494Water Needs 496Regulation of Water Balance 497
Global Perspective: Water for Everyone 501 14.2 Overview of Minerals 501
Food Sources of Minerals 502Absorption and Bioavailability of
Minerals 502Transport and Storage of Minerals 504Excretion of Minerals 504Functions of Minerals 504Mineral Deficiencies 504Mineral Toxicity 504
14.3 Sodium (Na) 505Sodium in Foods 505Sodium Needs 506Absorption, Transport, Storage, and
Excretion of Sodium 507Functions of Sodium 507Sodium Deficiency 507Excess Sodium and Upper Level 508
14.4 Potassium (K) 509Potassium in Foods 509Potassium Needs 510Absorption, Transport, Storage, and
Excretion of Potassium 510Functions of Potassium 510
Potassium Deficiency 510Excess Potassium and Upper Level 511
14.5 Chloride (CI) 511Chloride in Foods 511Chloride Needs 511Absorption, Transport, Storage, and
Excretion of Chloride 512Functions of Chloride 512Chloride Deficiency 512Upper Level for Chloride 512
Clinical Perspective: Hypertension and Nutrition 513
14.6 Calcium (Ca) 516Calcium in Foods 516Calcium Needs 517Calcium Supplements 518Calcium Absorption, Transport, Storage,
Regulation, and Excretion 519Functions of Calcium 519
Take Action: Estimate Your Calcium Intake 523Clinical Perspective: Osteoporosis 524Take Action: Bone Health 527
Potential Health Benefits of Calcium 527Upper Level for Calcium 527
14.7 Phosphorus (P) 528Phosphorus in Foods 528Phosphorus Needs 528Absorption, Transport, Storage, and
Excretion of Phosphorus 528Functions of Phosphorus 529Phosphorus Deficiency 529Toxicity and Upper Level for
Phosphorus 529 14.8 Magnesium (Mg) 529
Magnesium in Foods 529Magnesium Needs 530Absorption, Transport, Storage, and
Excretion of Magnesium 530Functions of Magnesium 531Magnesium Deficiency 531Upper Level for Magnesium 532
14.9 Sulfur (S) 532Chapter Summary 534Study Questions 536References 538
Final PDF to printer
xxxi
15 TRACE MINERALS 540
15.1 Iron (Fe) 542Iron in Foods 542Iron Needs 542Absorption, Transport, Storage, and
Excretion of Iron 543Functions of Iron 545Iron Deficiency 547Iron Overload and Toxicity 548
15.2 Zinc (Zn) 549Zinc in Foods 549Dietary Needs for Zinc 550Absorption, Transport, Storage, and
Excretion of Zinc 550Functions of Zinc 551Zinc Deficiency 551Zinc Toxicity 551
Take Action: Iron and Zinc Intake in a Sample Vegan Diet 552
15.3 Copper (Cu) 552Copper in Foods 552Dietary Needs for Copper 552Absorption, Transport, Storage, and
Excretion of Copper 553Functions of Copper 553Copper Deficiency 554Copper Toxicity 554
15.4 Manganese (Mn) 554Manganese in Foods 554Dietary Needs for Manganese 555Absorption, Transport, Storage, and
Excretion of Manganese 555Functions of Manganese 555Manganese Deficiency and Toxicity 555
15.5 Iodine (I) 556Iodine in Foods 556Dietary Needs for Iodine 557Absorption, Transport, Storage, and
Excretion of Iodine 557Functions of Iodine 557Iodine Deficiency Disorders (IDD) 557Iodine Toxicity 558
15.6 Selenium (Se) 560Selenium in Foods 560Dietary Needs for Selenium 561Absorption, Transport, Storage, and
Excretion of Selenium 561Functions of Selenium 561Selenium Deficiency 562Selenium Toxicity 562
15.7 Chromium (Cr) 563Chromium in Foods 563Dietary Needs for Chromium 563Absorption, Transport, Storage, and
Excretion of Chromium 563Functions of Chromium 563Chromium Deficiency and Toxicity 563
15.8 Fluoride (F) 564Fluoride in Foods 564Dietary Needs for Fluoride 564Absorption, Transport, Storage, and
Excretion of Fluoride 564Functions of Fluoride 564Fluoride Deficiency and Toxicity 565
Take Action: Is Your Local Water Supply Fluoridated? 567
15.9 Molybdenum (Mo) and Ultratrace Minerals 567Global Perspective: The e-Library of Evidence for
Nutrition Actions 568Clinical Perspective: Nutrients, Diet, and
Cancer 569Chapter Summary 572Study Questions 574References 575
Part 5 Nutrition Applications in the Life Cycle
16 NUTRITIONAL ASPECTS OF PREGNANCY AND BREASTFEEDING 576
16.1 Pregnancy 578Prenatal Developmental Stages: Conception,
Zygotic, Embryonic, and Fetal 579Nourishing the Zygote, Embryo, and
Fetus 583 16.2 Nutritient Needs of Pregnant Women 584
Energy Needs 585Nutrients Needed for Building New
Cells 585Nutrients Needed for Bone and Tooth
Development 587Expert Perspective from the Field: Grains and Folic
Acid Fortification 588Pregnant Women Do Not Have an Instinctive
Drive to Consume More Nutrients 588
Final PDF to printer
xxxii
16.3 Diet and Exercise Plan for Pregnancy 589Prenatal Vitamin and Mineral
Supplements 591Physical Activity during Pregnancy 591
Global Perspective: Pregnancy and Malnutrition 592
16.4 Maternal Weight and Pregnancy Outcome 593Maternal Prepregnancy Weight 593Maternal Weight Gain 593Pattern of Maternal Weight Gain 594
16.5 Nutrition-Related Factors Affecting Pregnancy Outcome 595Young Maternal Age 596Maternal Eating Patterns 596Maternal Health 596Maternal Sociocultural Factors 598Maternal Food Supply 598Maternal Lifestyle 600
Take Action: Healthy Diets for Pregnant Women 601
Clinical Perspective: Nutrition-Related Physiological Changes of Concern during Pregnancy 602
16.6 Lactation 604Milk Production 604
16.7 Nutrient Needs of Breastfeeding Women 606Maternal Nutritional Status 606Food Choices during Lactation 607
16.8 Factors Affecting Lactation 608Maternal Weight 608Maternal Age 608Maternal Eating Patterns 608Maternal and Infant Health 608Sociocultural Factors 609Maternal Food Supply 610Maternal Lifestyle Choices 610
Take Action: Investigating Breastfeeding 611Chapter Summary 612Study Questions 614References 615
17 NUTRITION DURING THE GROWING YEARS 616
17.1 Growing Up 618Height and Weight 618Body Composition 619Body Organs and Systems 619
17.2 Physical Growth 620Tracking Growth 620Using Growth Chart Information 622
17.3 Nutrient Needs 623Global Perspective: Autism 624Energy 624Protein 624Fat 625Carbohydrate 625Water 625Vitamins and Minerals 626 17.4 Feeding Babies: Human Milk and
Formula 628Nutritional Qualities of Human Milk 628Nutritional Qualities of Infant Formula 629Comparing Human Milk and Infant
Formula 630Feeding Technique 631Preparing Bottles 632
17.5 Feeding Babies: Adding Solid Foods 634Deciding When to Introduce Solid
Foods 634Rate for Introducing Solid Foods 636Sequence for Introducing Solid Foods 636Weaning from the Breast or Bottle 638Learning to Self-Feed 638
Clinical Perspective: Potential Nutrition-Related Problems of Infancy 639
17.6 Children as Eaters 640Appetites 641When, What, and How Much to Serve 642Food Preferences 643Mealtime Challenges 644
Take Action: Getting Young Bill to Eat 645Clinical Perspective: Potential Nutrition-Related
Problems of Childhood 646 17.7 Teenage Eating Patterns 648
Factors Affecting Teens’ Food Choices 648Helping Teens Eat More Nutritious
Foods 649Take Action: Evaluating a Teen Lunch 650Clinical Perspective: Potential Nutrition-Related
Problems of the Adolescence 651Chapter Summary 652Study Questions 654References 655
Final PDF to printer
xxxiii
18 NUTRITION DURING THE ADULT YEARS 656
18.1 Physical and Physiological Changes during Adulthood 658Usual and Successful Aging 660Factors Affecting the Rate of Aging 660
Take Action: Stop the Clock! Are You Aging Healthfully? 662
18.2 Nutrient Needs during Adulthood 663Defining Nutrient Needs 664
18.3 Factors Influencing Food Intake and Nutrient Needs 668Physical and Physiological Factors 668Psychosocial Factors 676Economic Factors 677
18.4 Nutrition Assistance Programs 678 18.5 Nutrition-Related Health Issues of the Adult
Years 679Alcohol Use 680Slowed Restoration of Homeostasis 680Alzheimer Disease 680Arthritis 681
Take Action: Helping Older Adults Eat Better 682Clinical Perspective: Complementary Health
Approaches 683Chapter Summary 687Study Questions 689References 690
AppendicesA Human Physiology: A Tool for Understanding
Nutrition A-1B Chemistry: A Tool for Understanding
Nutrition A-25C Detailed Depictions of Glycolysis, Citric
Acid Cycle, Electron Transport Chain, Classes of Eicosanoids, and Homocysteine Metabolism A-48
D Dietary Advice for Canadians A-54E The Food Lists for Diabetes: A Helpful Menu
Planning Tool A-66F Fatty Acids, Including Omega-3 Fatty Acids,
in Foods A-80G Metropolitan Life Insurance Company Height-
Weight Table and Determination of Frame Size A-82
H English-Metric Conversions and Nutrition Calculations A-85
I Caffeine Content of Beverages, Foods, and Over-the-Counter Drugs A-90
J Estimated Average Requirements (EARs) for Nutrients A-92
K CDC Growth Charts A-94L Sources of Nutrition Information A-103M Dietary Intake and Energy Expenditure
Assessment A-106N Food Composition Table A-115 Glossary Terms G-1 Photo Credits C-1 Index I-1
Final PDF to printer







