Download - Utrasound Gall-bladder & biliary tract
USG BILIARY TREE &GB
DR MOHIT GOEL4/06/2013
GBGallstone Disease
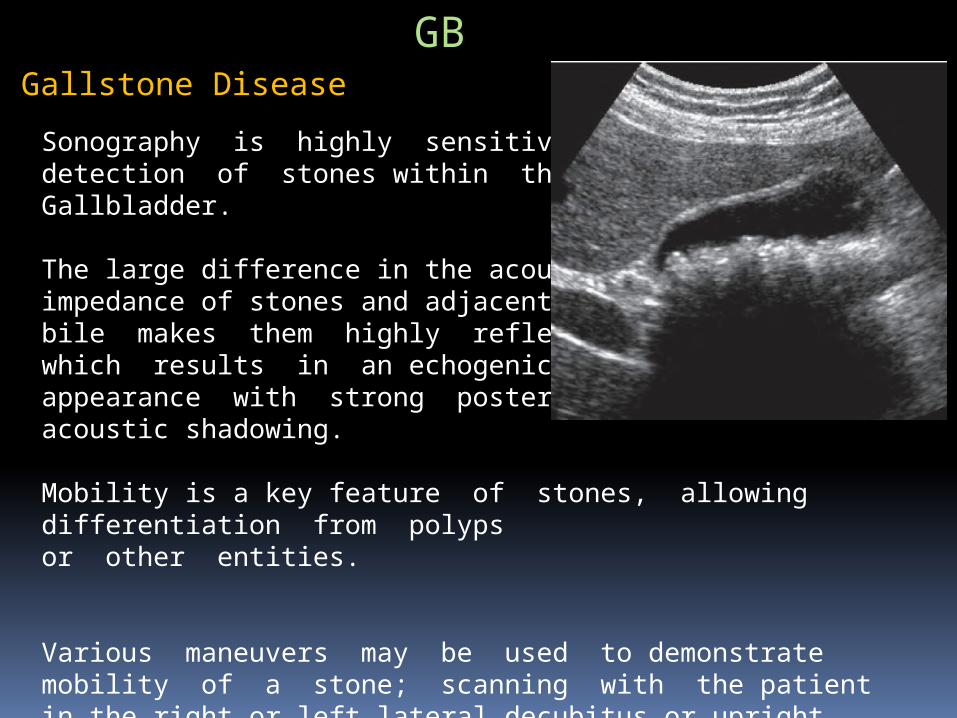
Sonography is highly sensitive in the detection of stones within the Gallbladder.
The large difference in the acoustic impedance of stones and adjacent bile makes them highly reflective, which results in an echogenic appearance with strong posterior acoustic shadowing.
Mobility is a key feature of stones, allowing differentiation from polyps or other entities.
Various maneuvers may be used to demonstrate mobility of a stone; scanning with the patient in the right or left lateral decubitus or upright standing position may allow the stone to roll within the gallbladder.
Biliary Sludge
Biliary sludge, also known as biliary sand or microlithiasis, is defined as a mixture of particulate matter and bile that occurs when solutes in bile precipitate.
The sonographic appearance of sludge is that of amorphous, low-level echoes within the gallbladder in a dependent position, with no acoustic shadowing.
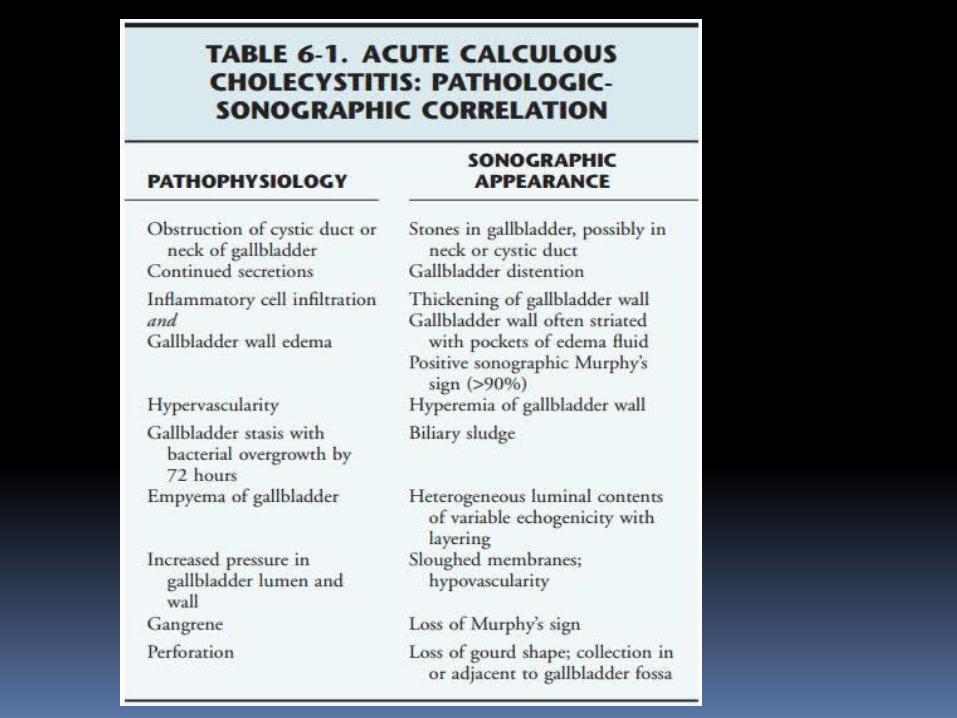
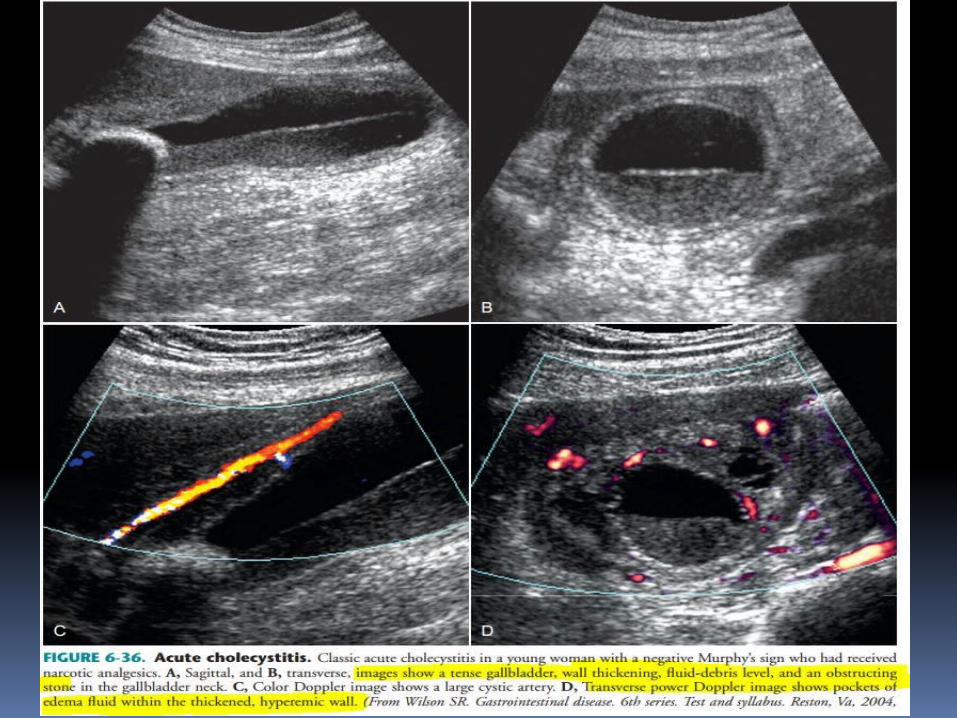
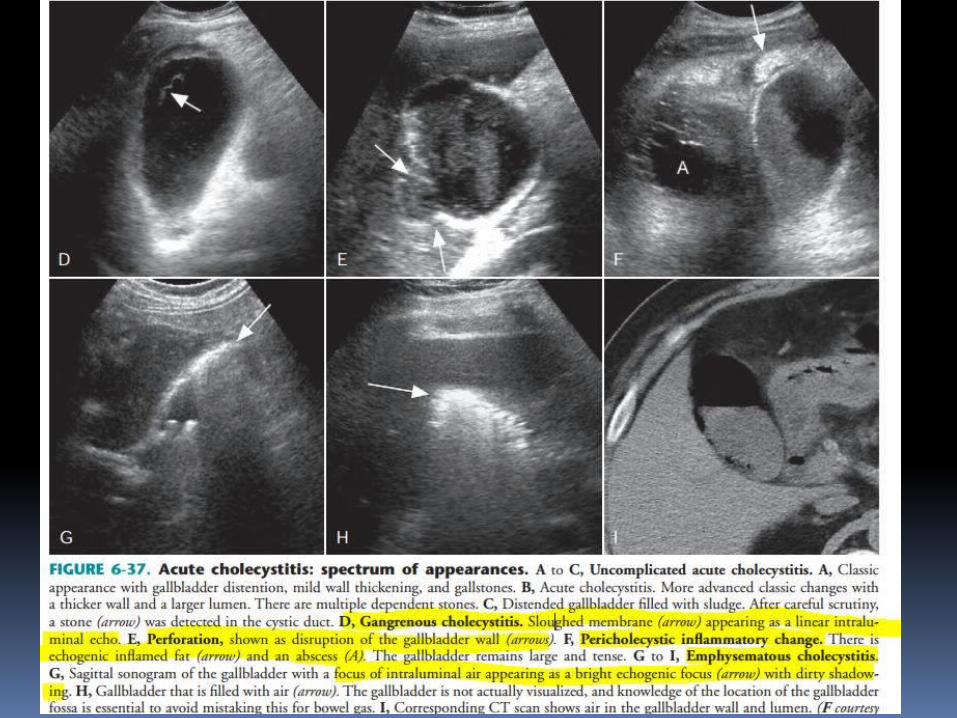
Acute Cholecystitis
It is caused by gallstones in more than 90% of patients.
Clinically, patients present with a prolonged, constant RUQ or epigastric pain associated with RUQ tenderness. Fever, leukocytosis, and increased serum ALP and bilirubin levels may be present.
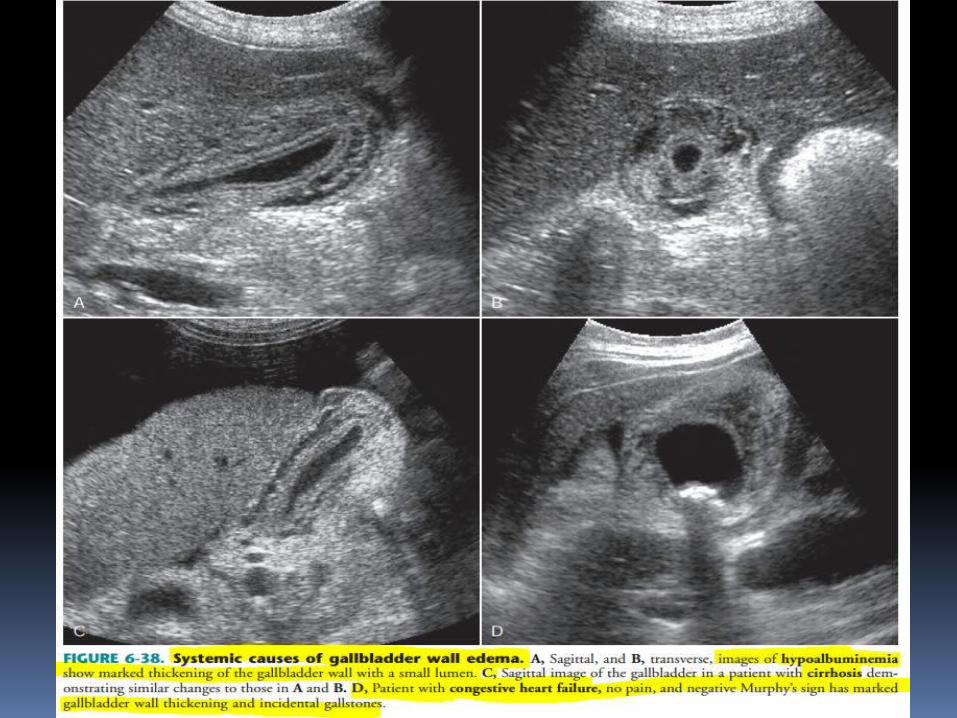
Porcelain Gallbladder
Calcification of the gallbladder wall is termed “porcelain” gallbladder.
The degree and pattern of calcification determines the sonographic appearance.
When the entire gallbladder wall is thickly calcified, a hyperechoic semilunar line with dense posterior acoustic shadowing is noted.
Mild calcification appears as an echogenic line with variable degrees of posterior acoustic shadowing.

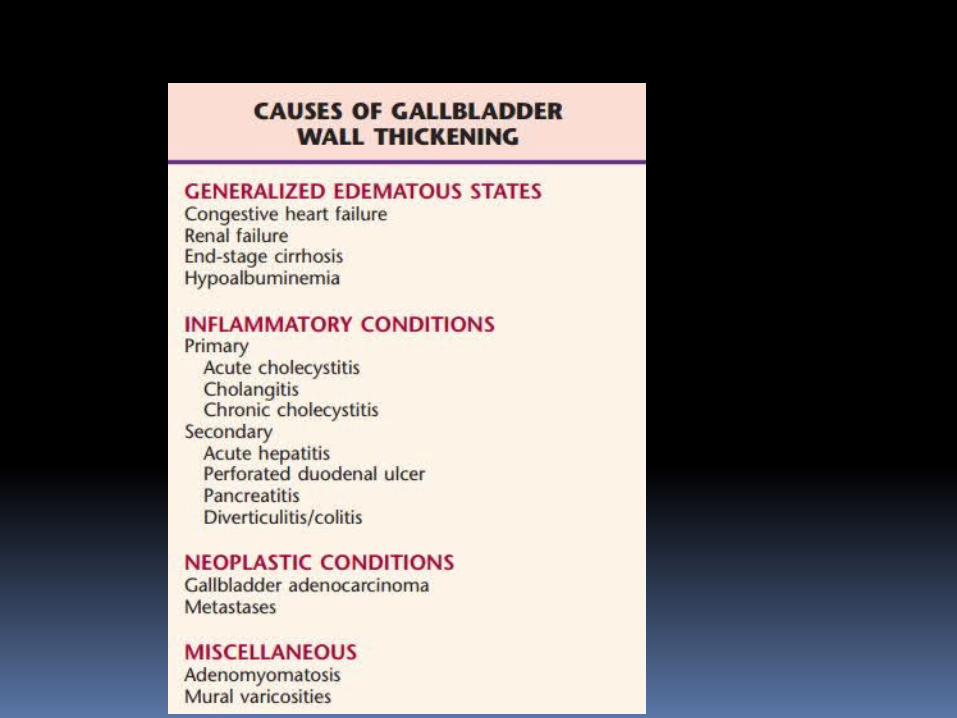
Chronic Cholecystitis
Chronic cholecystitis is associated with the mere presence of gallstones; therefore patients are usually asymptomatic and have mild disease. \
More advanced cases involve wall thickening and fibrosis, appearing on sonographic examination as a thickwalled gallbladder with gallstones.
Differentiation from acute cholecystitis is made by the absence of other signs, namely, gallbladder distention, Murphy’s sign, and hyperemia in the wall.
Bouts of acute cholecystitis may complicate chronic cholecystitis.

Adenomyomatosis (Adenomatous Hyperplasia)
Gallbladder adenomyomatosis is a benign condition caused by exaggeration of the normal invaginations of the luminal epithelium (Rokitansky-Aschoff sinuses) with associated smooth muscle proliferation.
The great majority of adenomyomatoses are asymptomatic.
Adenomyomatosis may be focal or diffuse.
The most common appearance on sonography is tiny, echogenic foci in the gallbladder wall that create comet-tail artifacts , presumably caused by either the cystic space itself or the internal debris.
Prominent mass like focal areas of adenomyomatosis, called adenomyomas,are the next most common manifestation. Echogenic foci with ringdown or “twinkling” artifact on Doppler examination are also typical.
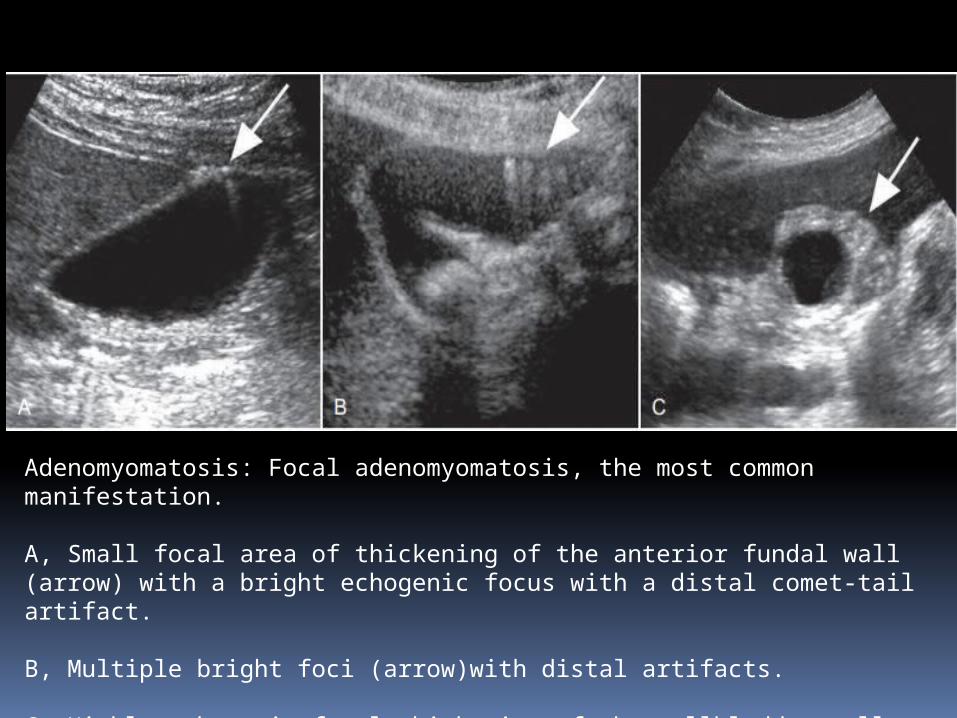
Adenomyomatosis: Focal adenomyomatosis, the most common manifestation.
A, Small focal area of thickening of the anterior fundal wall (arrow) with a bright echogenic focus with a distal comet-tail artifact.
B, Multiple bright foci (arrow)with distal artifacts.
C, Highly echogenic focal thickening of the gallbladder wall (arrow).Increased echogenicity is unusual for a malignant tumor that is more likely to appear hypoechoic.
Polypoid Masses of Gallbladder
Cholesterol Polyps
Approximately one half of all polypoid gallbladder lesions are cholesterol polyps. These represent the focal form of gallbladder cholesterolosis, a common nonneoplastic condition of unknown etiology.
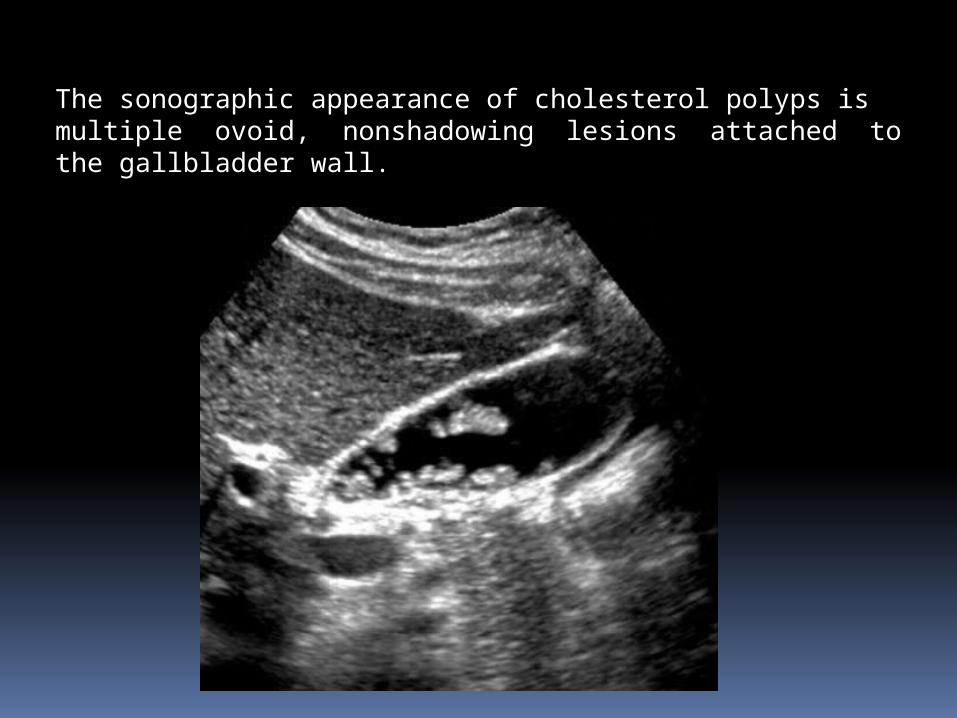
The sonographic appearance of cholesterol polyps is multiple ovoid, nonshadowing lesions attached to the gallbladder wall.
Gallbladder Carcinoma
The following three patterns of disease have been described:
1. Mass arising in the gallbladder fossa, obliterating the
gallbladder and invading the adjacent liver (most
common pattern)
2. Focal or diffuse, irregular wall thickening
3. Intraluminal polypoid mass
On Doppler interrogation the mass may demonstrate internal arterial and venous flow.
Diffuse, malignant thickening of the wall differs from other causes in that the wall is irregular with loss of the normal mural layers.
Polypoid intraluminal masses are differentiated from nonneoplastic abnormalities by immobility of the mass, larger size (>1 cm), and prominent internal vascularity.
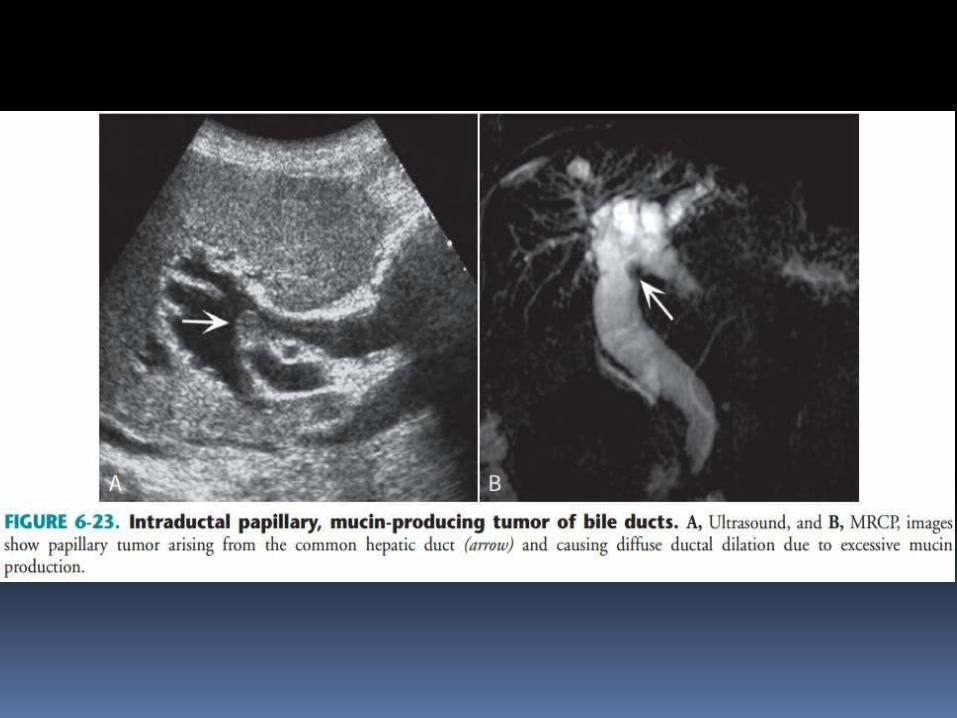
Gallbladder carcinomas may produce large quantities of mucin,which distends the gallbladder
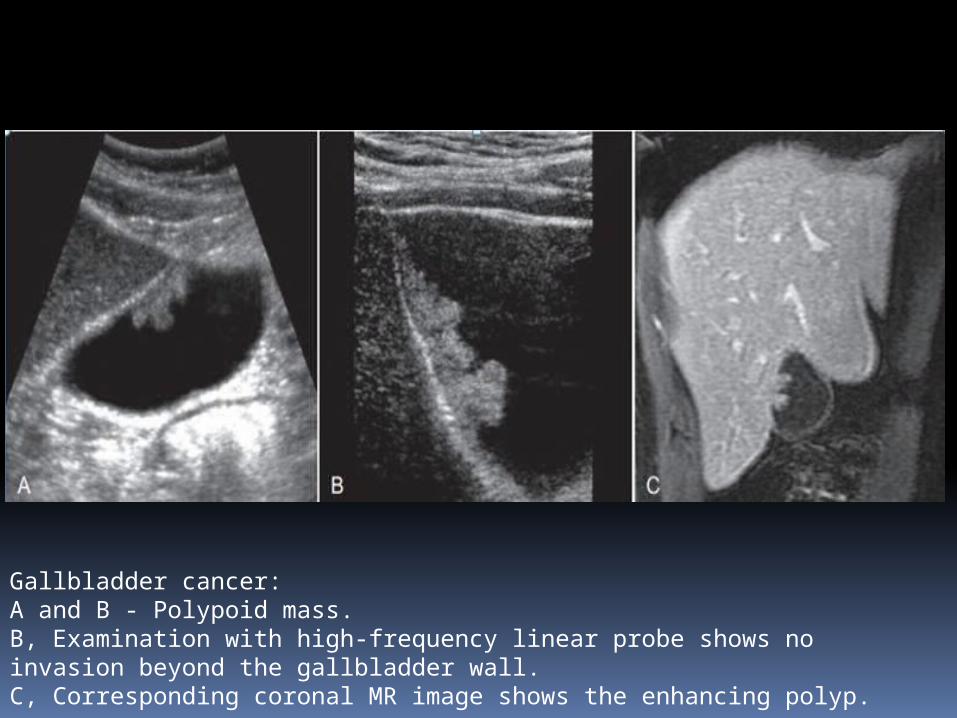
Gallbladder cancer: A and B - Polypoid mass.B, Examination with high-frequency linear probe shows no invasion beyond the gallbladder wall. C, Corresponding coronal MR image shows the enhancing polyp.
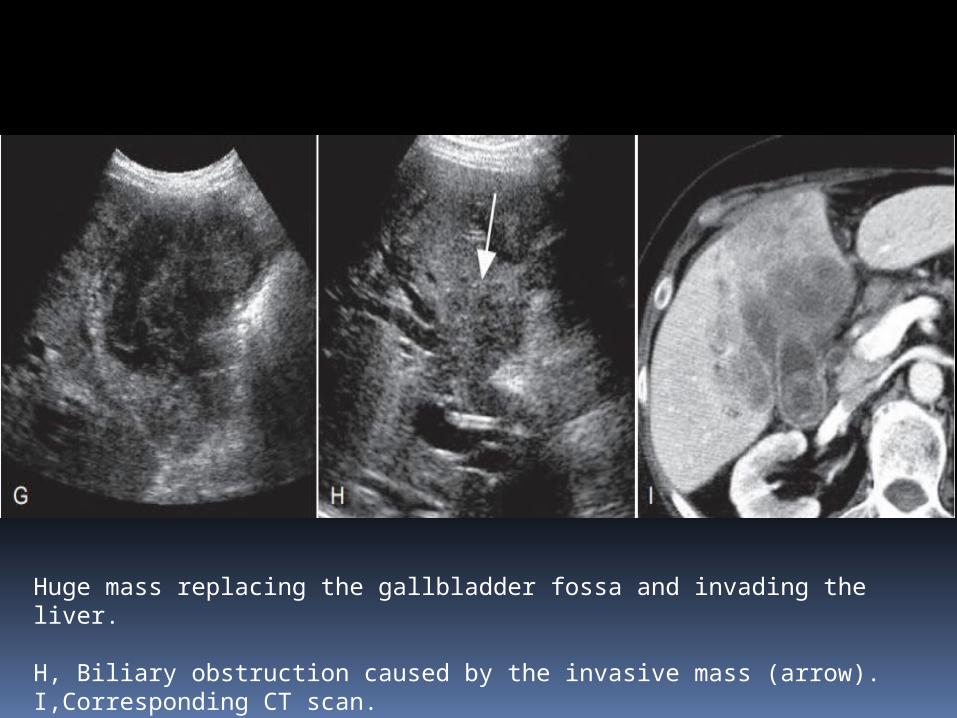
Huge mass replacing the gallbladder fossa and invading the liver.
H, Biliary obstruction caused by the invasive mass (arrow). I,Corresponding CT scan.
Biliary Tree
The normal caliber of the CHD/CBD in patients without history of biliary disease is up to 6 mm.
Although diameters of up to 10 mm have been recorded in an asymptomatic normal population, the great majority of the diameters are under 7 mm.
Therefore, a ductal diameter of 7 mm or greater should prompt further investigations, such as correlation with serum levels of cholestatic liver enzymes.
Choledochal Cysts
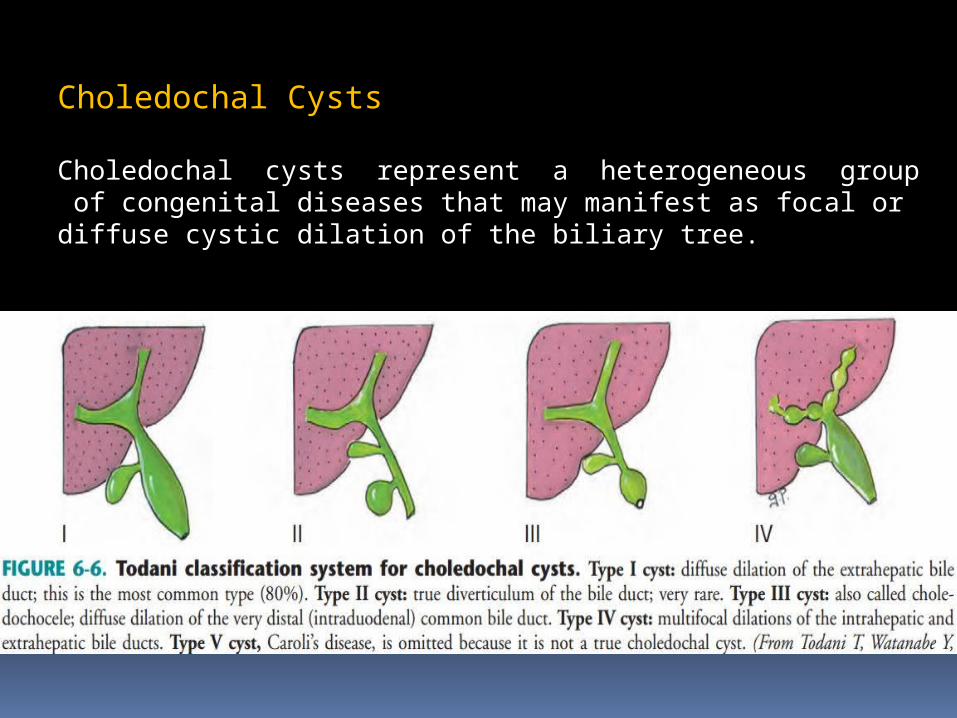
Choledochal cysts represent a heterogeneous group of congenital diseases that may manifest as focal or diffuse cystic dilation of the biliary tree.
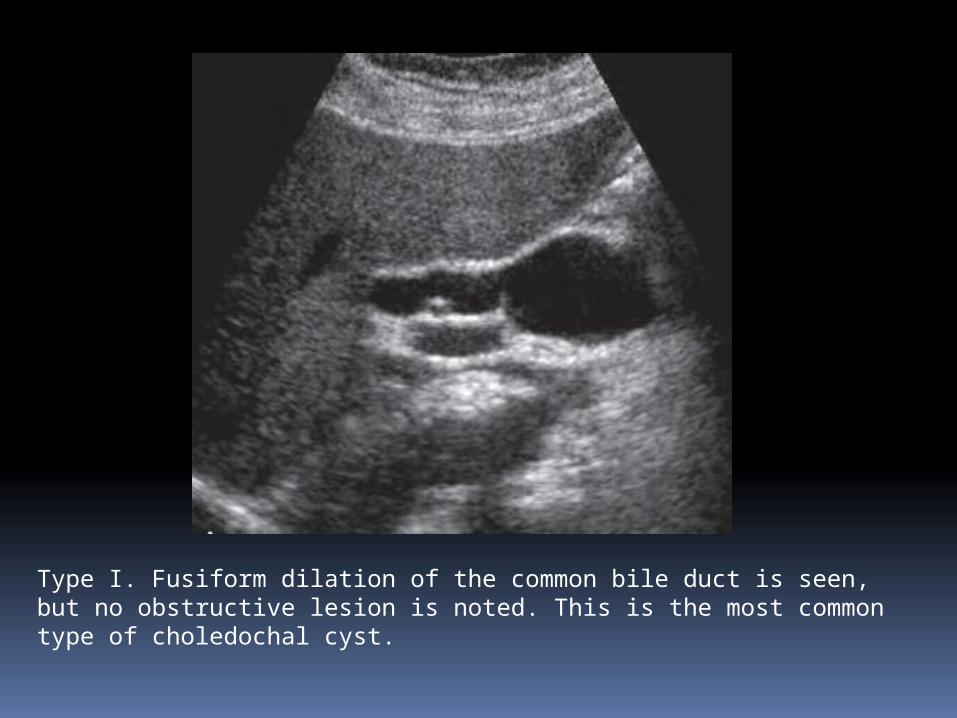
Type I. Fusiform dilation of the common bile duct is seen, but no obstructive lesion is noted. This is the most common type of choledochal cyst.
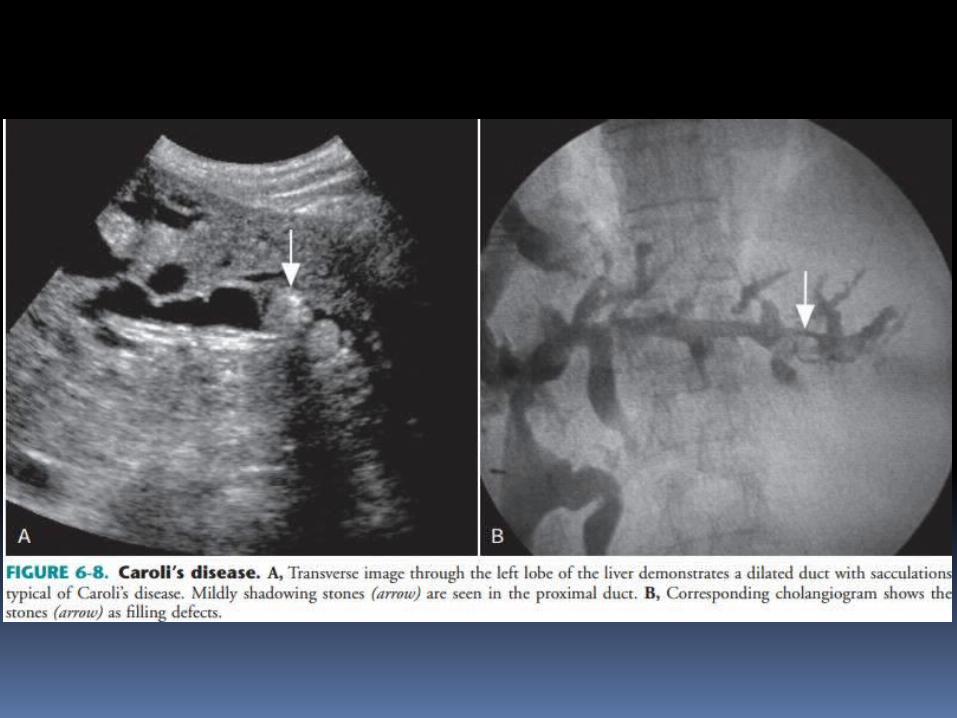
Caroli’s Disease
Caroli’s disease is a rare congenital disease of the intrahepatic biliary tree that results from malformation of the ductal plates, the primordial cells that give rise to the intrahepatic bile ducts.
Caroli’s disease has been associated with cystic renal disease, most often renal tubular ectasia (medullary sponge kidneys).
Caroli’s disease leads to saccular dilation or less often fusiform dilation of the intrahepatic biliary tree, resulting in biliary stasis, stone formation, and bouts of cholangitis and sepsis.
Cholangiocarcinoma develops in 7% of patients with Caroli’s disease.
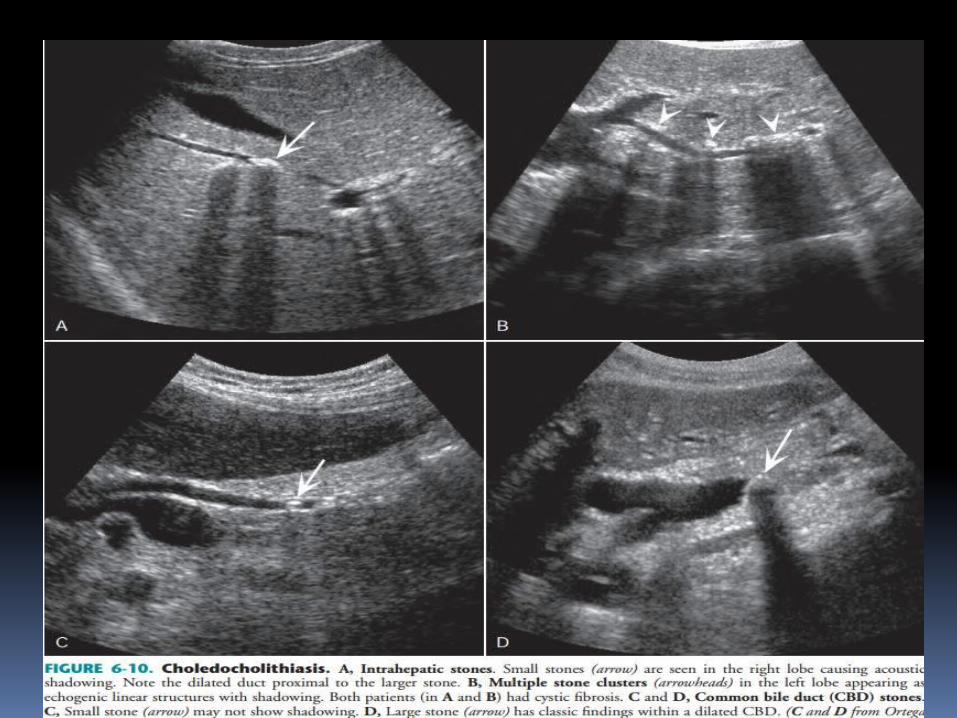
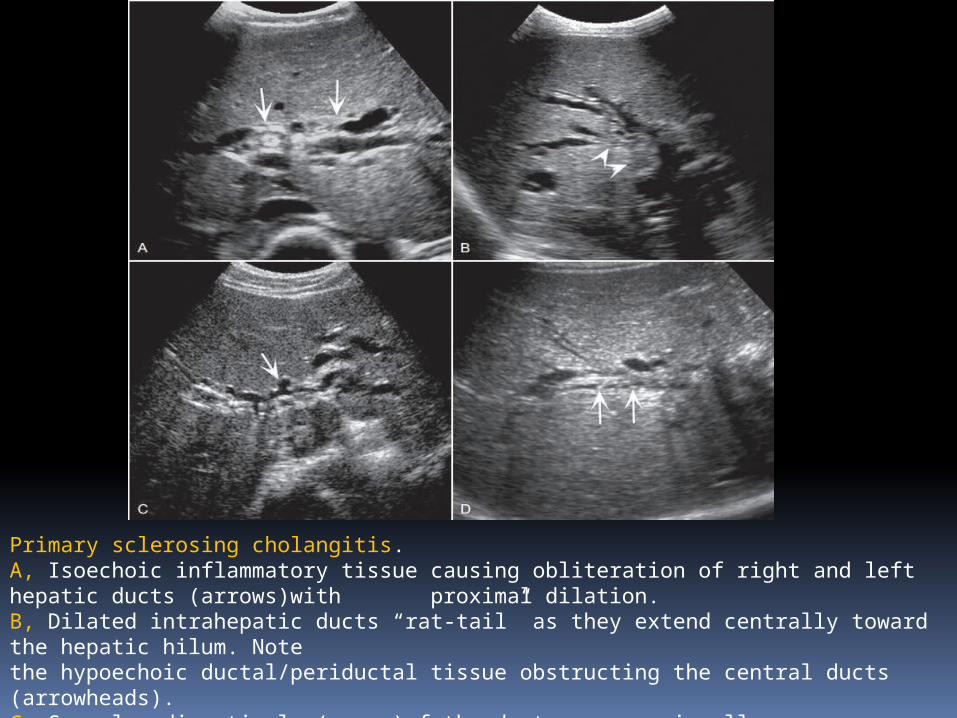
Primary sclerosing cholangitis. A, Isoechoic inflammatory tissue causing obliteration of right and left hepatic ducts (arrows)with proximal dilation.B, Dilated intrahepatic ducts “rat-tail” as they extend centrally toward the hepatic hilum. Note the hypoechoic ductal/periductal tissue obstructing the central ducts (arrowheads). C, Saccular diverticula (arrow)of the duct are occasionally seen. D, Minute intraductal stones (arrows)are seen in irregular, mildly dilated ducts.
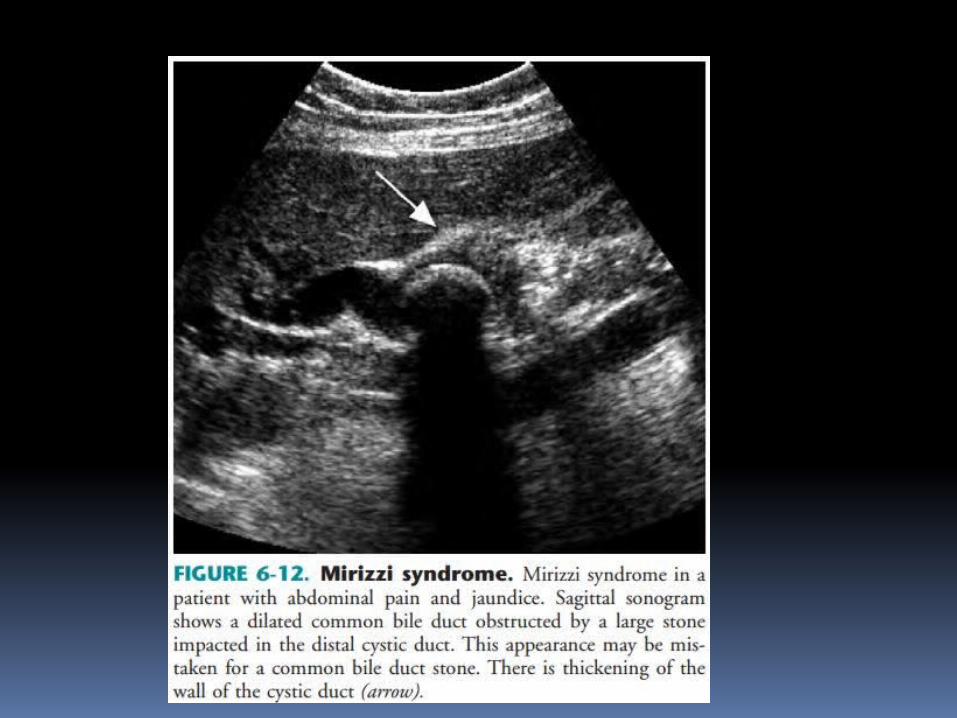
Mirizzi Syndrome
Mirizzi syndrome describes a clinical syndrome of jaundice with pain and fever resulting from obstruction of the common hepatic duct caused by a stone impacted in the cystic duct.
It occurs most often when the cystic duct and CHD run a parallel course.
Mirizzi syndrome should be considered on sonography when biliary obstruction with dilation of the biliary ducts to the CHD level is seen with acute or chronic cholecystitis.
A stone impacted in the cystic duct with surrounding edema at the level of the obstruction is confirmatory.
Biliary Tree Infection
Acute (Bacterial) Cholangitis
The clinical presentation is usually that of (1) fever (~90%), (2) right upper quadrant (RUQ) pain (~70%), and (3) jaundice (~60%), the classic Charcot’s triad.
The sonographic findings of bacterial cholangitis include the following :
• Dilation of the biliary tree
• Choledocholithiasis and possibly sludge
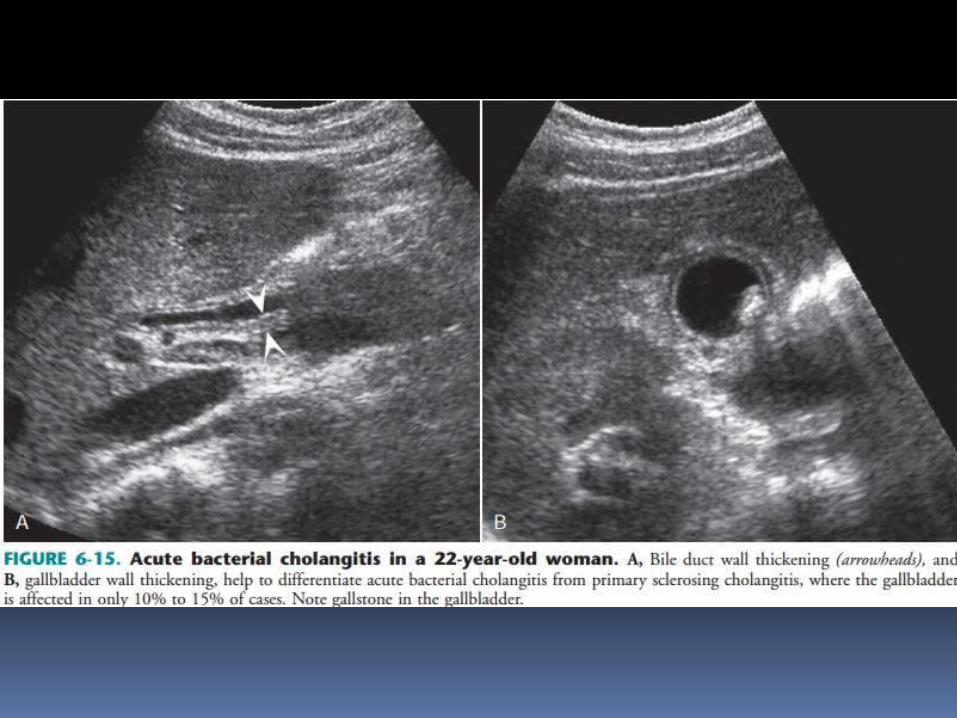
• Bile duct wall thickening
• Hepatic abscesses
Cholangiocarcinoma
Cholangiocarcinomas are classified based on the anatomic location:
1. intrahepatic, also called peripheral (~10%); 2. hilar, also called Klatskin’s (~60%)3. distal(~30%).
Approximately 90% of cholangiocarcinomas are adenocarcinomas, with squamous carcinomas the next most common subtype.
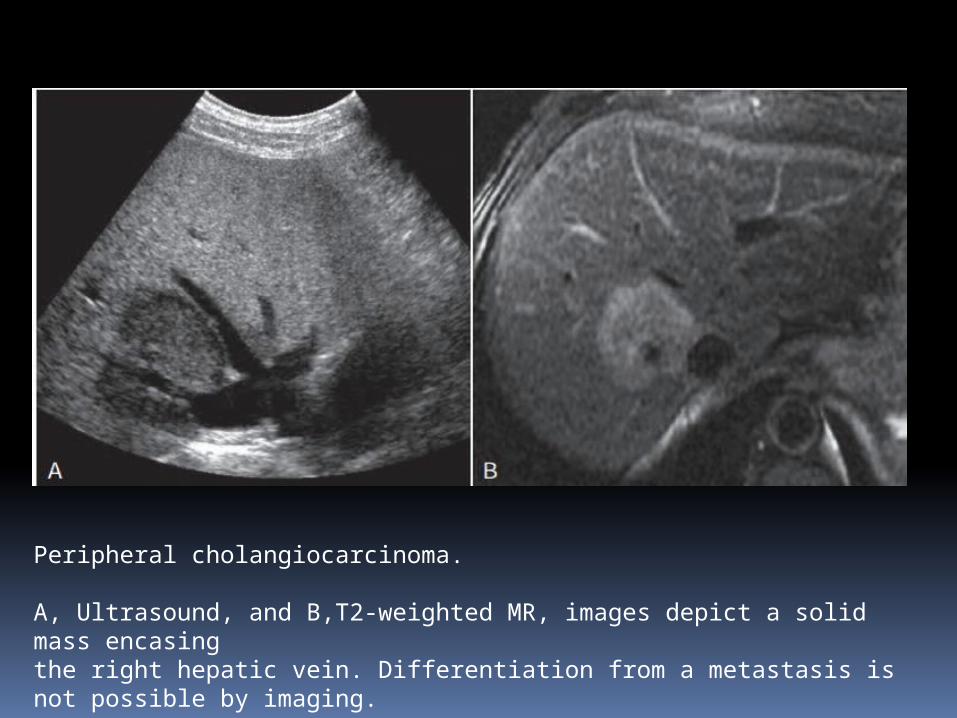
Peripheral cholangiocarcinoma.
A, Ultrasound, and B,T2-weighted MR, images depict a solid mass encasing the right hepatic vein. Differentiation from a metastasis is not possible by imaging.

THANK YOU







