User Guidelines
for
Self-Assessment Purposes
2017


SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 3
Introduction
Purpose of these guidelines: This guidelines is aimed at the end-users of the hospital Ac-
creditation Standards and of the accreditation methodology, for them to understand the phases and
the general activities that they must undertake throughout the accreditation process and how
should they assess their own level of compliance with the requirements included in the accreditation
standards.
Expected outcomes:
- Information for the hospitals on the concepts of quality management in health and of ac-
creditation;
- Proper knowledge by hospitals of the activities and responsibilities that they have to under-
take during the accreditation process;
- Achievement by hospitals of quality standards for hospitals and provision of instruments that
could be used for self-assessment purposes;
- Providing to the hospitals a clear instrument for self-assessment of own level of compliance
with the requirements included in the accreditation standards.
***
The current guidelines help to a better understanding, by the end-users of the principles of
quality in health and the philosophy underlying the accreditation process in health services, as well
of the results and benefits of accreditation. The second part of the guidelines reviews the accredita-
tion process, from the perspective of end-users (hospitals), underlining the administrative, meth-
odological or procedural and communication requirements, matching the rights and duties that
they have when undertaking this process, until it is resumed for re-accreditation purposes.
The main phases of this route are described: the request for accreditation and preparations
made for the user in order to get accredited, the evaluation process including the pre-visit, the visit
and the post-visit stage, the ongoing monitoring process undertaken in order to maintain the ac-
creditation level, which is initiated after the level of accreditation is communicated and which is
concluded through the registration within a new evaluation process, for re-accreditation purposes.
The final aim of this document is to inform the users and to bring them on board the ongoing
process of improving the quality of health services, as the outcomes could be measured through
the patients’ satisfaction degree, simultaneous with an increase in the measurable quality of medi-
cal services and with the an increase in the level of efficiency in the provision of health services.

4 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
The Co-ordinating group for
Standards Elaboration
Experts Group:
Mr. Vasile CEPOI - President of ANMCS
Mr. Sorin UNGUREANU - Assistant Director ANMCS
Mr. Marius FILIP - Director USSS Mrs. Nicoleta MANU - Head office
BSSSS Mr. Andrei ȘTEFAN - Counselor BSSSS Mrs. Adina GEANĂ - Expert ANMCS
Vasile Astărăstoae
Carmen Angheluță
Mariana Brudașcă
Daniel Burghelea
Ana-Maria Dădulescu
Adina Geană
Nirvana Georgescu
Daniela Marghidan
Doina Miron
Daniela Moșoiu
Antonia Nițescu
Georgel Rusu
Relu Chițac
Guide Authors:
Co-ordinator: dr. Vasile CEPOI,
Psih. Alexandru DICU
SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 5
1.1. Quality assessment - the philosophy underlying the accredi-
tation of hospital-based services.
Hospital-based services represent an atypical economic market, on one hand, as the health-
care market does not rely on the classical economic relation between supply and demand, where
“the supply creates the demand”. As regards demand, the patient has no possibility to take deci-
sions, as the doctor interposes himself/herself in the decision chain on care and treatment deemed
as most convenient; as regards supply, the service provider (the hospital) is not able to set the price.
The health services market is also atypical due to the fact that the “end-product” of these ser-
vices is intangible and difficult to measure and standardize - health, recovered or restored. More-
over, the patients’ expectation are different from their genuine needs for care, while various behav-
iours and habits, deemed useful by the patient, may interfere with his/her health.
The accreditation standards are considered, from a motivational perspective, to be the opti-
mal and achievable level and they are meant to encourage ongoing efforts for the improvement of
the activity within the accredited organizations.
Accreditation is a process in which the need to register and participate is determined by the
law.
The decision to issue accreditation for a specific hospital ensues an evaluation visit performed
by a team of evaluators, under normal circumstances, once every 5 years.
The choice for the precise moment when the actual visit should take place is subject to an
agreement between each registered hospital and the National Authority for Quality Management in
Health (ANMCS), over the entire 5-year period, representing an accreditation cycle.
Chapter 1. General presentation

6 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
According to A.N.M.C.S. understanding, the philosophy behind accreditation relies on the fol-
lowing relevant values:
The ANMCS accreditation programme starts from the assumption that hospitals are capable to
develop their strategies in order to fulfil the quality standards, without any need for stimuli of any
nature, as what is required is the mere reorganization of the existing resources: the financial, human
or organizational ones.
1.1.1 What is A.N.M.C.S.
National Authority for Quality Management in Health (ANMCS) is a public institution with a
legal capacity, specialized body of central public administration in the field of quality management
in the health sector, which operates as a subordinate body to the Government and under the coor-
dination of the Prime-Minister, through the Prime-Minister’s Chancery.
ANMCS deals with the accreditation of healthcare units, as these are established in consulta-
tion with the Ministry of Health. Healthcare units are those entities with or without a legal capacity
whose scope of work is represented by the provision of medical care, at any level: primary health-
care/GP healthcare, outpatient healthcare, hospital-based healthcare, no matter the type of owner-
ship. Accreditation is awarded over a 5 year period, after that the respective healthcare unit must
be re-accredited.

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 7
The ANMCS purpose consists from ensuring and ongoing improvement of quality in health ser-
vices and patient safety, through standardization and evaluation of health services and accreditation
of healthcare units.
ANMCS is financed through own revenues and subsidies provided by the state budget,
through the budget of the General Secretariat of the Government.
The mission of the National Authority for Quality Management in Health is to determine qual-
ity assurance and continuous improvement of the health services and patient safety through a
change in the culture of organizations operating in the health sector, standardization, evaluation of
health services and accreditation of healthcare units.
A.N.M.C.S. will disseminate the concept of quality to the professionals within the health sys-
tem, for the purpose of changing the organizational mind-set in order to ensure the implementation
of the quality management system.
The objectives of the National Authority for Quality Management in Health:
The horizon of the national quality system in health: Development in the health ser-
vices through quality, efficiency and performance.

8 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
1.1.2 What is accreditation?
Accreditation is the method which demonstrates that a healthcare unit makes efforts to
provide medical care that should satisfy the patients’ expectations, from the point of view
of results, as well as from the point of view of conditions and processes through which accreditation
is being awarded.
This activity is delivered by the National Authority for Quality Management in Health
(ANMCS), which verifies the manner in which medical services are provided and evaluates the de-
gree to which such services comply with the accreditation standards.
What is accreditation useful for?
Accreditation confirms that a medical unit has the required resources and professional skills in
order to provide health care according to the level of specialization stipulated in its structures. It
confirms that a healthcare unit is actually able to do what they state they could perform. Therefore,
patients will have a higher level of trust to use the services of an accredited healthcare unit com-
pared to those of a non-accredited one.
Accreditation is a process required for the state-owned healthcare providers, as well as for the
private ones, as long as they wish to enter contractual relations with the Health Insurance Houses.
How does the patient find out that he/she uses the service of an accredited health-
care unit?
The patient may find out if a healthcare unit is accredited or not from the hospital
website or from the Official Journal. Also, we will propose to our partners which are interested in
promoting the quality of health services, to the Ministry of Health, CNAS, professional colleges, pa-
tient associations a.s.o. To publish such information on their web-sites.
Which extra advantages are provided to the patient who is using the services of an
accredited unit?
The patient who uses the services of an accredited healthcare unit will be sure that he/
she is properly informed on his/her health issues, on the possibilities that the respective unit has to
deliver treatment and on the provision of continuous medical care until the situation is solved. An
accredited healthcare unit has the required conditions in order to apply best practice in the field
and to take all measures in order to avoid risks for the patient to suffer any injuries whatsoever dur-
ing the treatment applied within the respective hospital.
How long is the accreditation valid?
5 years
What happens during this period?
In order to support the healthcare units in the process of maintaining and optimizing
quality, ANMCS cooperates with the staff from within the accredited facility through-
out a process of ongoing monitoring of the activity, thus stimulating the preoccupation of profes-
sionals within the accredited healthcare units to remain consistent in complying with the rules that

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 9
they have established themselves in order to satisfy to the highest degree possible the patients’ ex-
pectations and in order to improve continuously the standards for the services provided.
What happens with a hospital which does not receive the accreditation?
Hospitals which do not acquire an accreditation will not be able to conclude a contract
with the Health Insurance House. A Hospital which is not accredited may also operate
without having a contractual relation with the public health insurance system. As long
as the patients accept to receive medical care within a non-accredited healthcare facility, and they
accept paying for such services, the unit will continue operating.
ACCREDITATION is a complex process. It starts by the bedded healthcare unit requesting
ANMCS to initiate a series of activities that result in its accreditation as an organisation that meets
particular quality standards.
After filing the application, three main stages ensue.
Stage 1: 9 months – the hospital prepares for evaluation.
Stage 2: 3 months – the evaluation team prepares the mission, carries out the evalua-
tion and post-evaluation visit, resulting in the evaluation report that forms the basis for
the accreditation decision.
Finally, Stage 3: 4 years – monitoring, after the determination of the accreditation
level. The purpose of this last stage is to ensure that the hospital maintains the accred-
ited level.
Throughout the process, the bedded healthcare unit will be comprehensively assessed, as a
provider of healthcare, treatment and services to its patients, based on its structure, staff qualifica-
tion and resources available and employed. Accreditation is an evaluation of the combination of fac-
tors described above, which work together and interact to improve, ensure and maintain the quality
of its activities.
For these reasons, the accreditation process looks at the entire organisation, and not at the
work of an individual department.
10 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
The accreditation of an organisation has the following features:
In this context, the ANMCS goal is to ensure and maximise relevant patient care safety and
quality standards.

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 11
Principles of accreditation
12 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
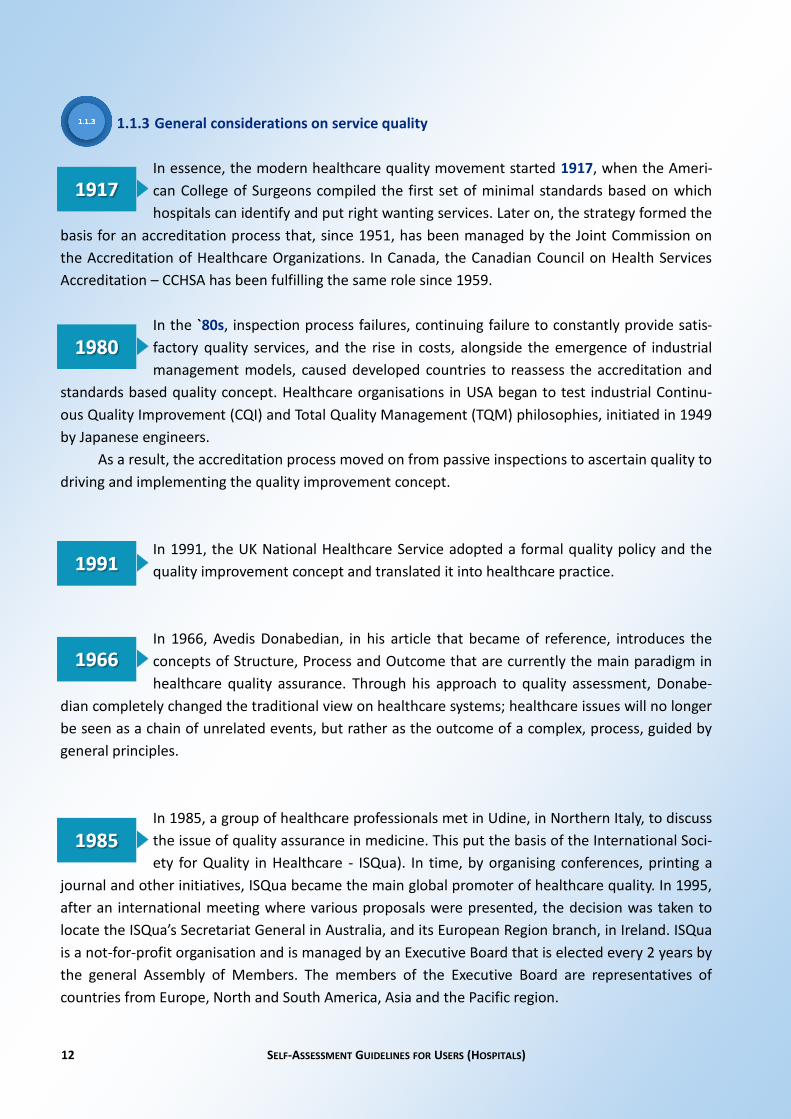
1.1.3 General considerations on service quality
In essence, the modern healthcare quality movement started 1917, when the Ameri-
can College of Surgeons compiled the first set of minimal standards based on which
hospitals can identify and put right wanting services. Later on, the strategy formed the
basis for an accreditation process that, since 1951, has been managed by the Joint Commission on
the Accreditation of Healthcare Organizations. In Canada, the Canadian Council on Health Services
Accreditation – CCHSA has been fulfilling the same role since 1959.
In the `80s, inspection process failures, continuing failure to constantly provide satis-
factory quality services, and the rise in costs, alongside the emergence of industrial
management models, caused developed countries to reassess the accreditation and
standards based quality concept. Healthcare organisations in USA began to test industrial Continu-
ous Quality Improvement (CQI) and Total Quality Management (TQM) philosophies, initiated in 1949
by Japanese engineers.
As a result, the accreditation process moved on from passive inspections to ascertain quality to
driving and implementing the quality improvement concept.
In 1991, the UK National Healthcare Service adopted a formal quality policy and the
quality improvement concept and translated it into healthcare practice.
In 1966, Avedis Donabedian, in his article that became of reference, introduces the
concepts of Structure, Process and Outcome that are currently the main paradigm in
healthcare quality assurance. Through his approach to quality assessment, Donabe-
dian completely changed the traditional view on healthcare systems; healthcare issues will no longer
be seen as a chain of unrelated events, but rather as the outcome of a complex, process, guided by
general principles.
In 1985, a group of healthcare professionals met in Udine, in Northern Italy, to discuss
the issue of quality assurance in medicine. This put the basis of the International Soci-
ety for Quality in Healthcare - ISQua). In time, by organising conferences, printing a
journal and other initiatives, ISQua became the main global promoter of healthcare quality. In 1995,
after an international meeting where various proposals were presented, the decision was taken to
locate the ISQua’s Secretariat General in Australia, and its European Region branch, in Ireland. ISQua
is a not-for-profit organisation and is managed by an Executive Board that is elected every 2 years by
the general Assembly of Members. The members of the Executive Board are representatives of
countries from Europe, North and South America, Asia and the Pacific region.

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 13
Based on quality philosophies, the quality management principles were stated. Adapted to the
hospital organisation, they are:
In some countries, the theoretical quality model is based on the minimum acceptable quality. In others, it is based on the highest expected level of quality, making up a number of desiderates.
The common principle of most accreditation processes is visiting the evaluated facility, apply-ing evaluation tools such as direct observation, questionnaires, checking existence of paperwork and looking for factual evidence of concern for quality and safety.
The standards, criteria and, above all the requirements (and then the measurable markers, called indicators), are dynamic elements of the accreditation system of values. In other words, that which today validates quality, tomorrow may become unsuitable or even contrary. For this reason,

14 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
these elements require constant assessment and adaptation to the developments in healthcare sys-tem.
Currently, accreditation no longer represents a sum of numeric data on all the standards. The
requirements also have binary values, meaning that one or another of the elements that combine to
define the overall snapshot of a hospital and is services may be in place or may be missing. On the
other hand, the evaluation visit itself is no longer a full inspection, limited to measuring normative
quantitative values.
Today, it is considered that the level of accreditation defines the level achieved by the organi-
sation in terms of quality management, on the one hand, and, on the other hand, the place that the
hospital has as provider on the healthcare market and its potential for development and continued
existence on this market.
The total quality management doctrine is based on the involvement of institutional manage-
ment in increasing customer satisfaction, staff participation in decision making and identification
various stages of processes that are may be improved. Through this approach, quality becomes the
focal point of the organisation’s development and evolution, including hospitals that, thus, gain ac-
cess to funding, in a market that is regulated by local and national healthcare and resource alloca-
tion polices.
1.2. Statement of terms and the use of the standardisation system in evaluation.
Accreditation is a process that entails external and, in principle, independent evaluation, car-
ried out by purposely trained persons – evaluators, followed by an analysis that determines the level
of accreditation, and results in the accreditation as such, followed by a period when the mainte-
nance of compliance with the accreditation requirements is monitored.
The accreditation of a hospital organisation is focused on three dimensions, namely the quality
management system, organisation of healthcare services and efforts to improve practices
(processes).
Thus, the accreditation looks at the hospital as a system of structures, activities and out-
comes, as an organisation.
The STANDARDS establish the ex-
pectations on a hospital’s performance,
structure and processes that should en-
sure (as outcomes) quality, safe and
compliant care, treatment and service s
for each patient. At the end of the day, a
standard is the value of the expected or
targeted quality.
Thus, the decision to accredit a
hospital means measuring the conformity with various standards.
The accreditation process covers all public and private healthcare facilities with beds: including
one day, acute conditions, chronic conditions, long term and recovery care.

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 15
Standards are designed to define the targeted, desired or expected
higher quality, in terms of an organisation’s processes and outcomes and
in direct relation with the patient’s satisfaction and health status benefits.
Standards are reunited in chapters named references (3 such refer-
ences are used in this cycle of accreditation), and are described by crite-
ria. While the standards are envisaged targets, the criteria are measurable
and define objectives to be achieved by complying with the standards.
Criteria are supplementary information, details or circumstances
related to a standard within a reference. Criteria are used in the accredi-
tation audit as a method for defining the evaluation framework and for
qualifying a referred element, for the purpose of making a judgement or
an appreciation on the conformity of a practice or activity.
Each criterion is defined by the concurrent existence of:
The requirements are what is requested for proving the criteria, so they
are activities performed by the users (hospitals) through which the ob-
jectives (criteria) are achieved. The criteria and requirements of stan-
dards are part of the standards.
Beyond them, in the process of measuring the compliance with the requirements, the indica-
tors are defined as concrete instruments proposed by ANMCS to measure the compliance of users
with the requirements of standards. They can be regarded as stages fulfilled to carry out the activi-
ties which the requirements imply. The indicators are not mandatory, are only the vision of
ANMCS regarding the measurement of compliance with the standard requirements.

16 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
The hospital may have its own way in which it should be compliant with the standard re-
quirements! Thus, it shall show the evaluators how and bring the evidence used to check them
(both the fulfilment of requirements and the way in which they are fulfilled).
The evaluation of performance is definitely an evaluation of success, and the accuracy of such
measurement is given by the use of specifically selected quality indicators. The indicators are part of
the set and measurement instruments while the standards are described and detailed through crite-
ria and characterised and concretely anchored by requirements.
The objectivity of this type of finding is given by the use of indicators specific to each criterion,
and the scalable consideration allows a nuance to the issuing of evaluation judgment.
The indicators have features which qualify them as measurements units intended to measure
an evolution in quantitative terms; they are quantifiable and reveal whether an activity was or not
efficiently and effectively managed and carried out.
The quality of an indicator is given by the fact that it constantly measures the same element of
a situation, regardless of the context.
Several categories or types of indicators applicable for the criteria and evaluation require-
ments are recognised:

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 17
They are expressed in absolute values or as numeric report, there being simple indicators and
composite indicators. The indicators shall be applicable to different dimensions of quality, being also
indicators measuring the effectiveness (relation between the results and initially proposed objec-
tives), the efficiency (relation between the results and used means to achieve them) and the avail-
ability or accessibility (service provided at the right time, in the right place, the right time and corre-
sponding intensity measure).
1.2.1. Selection and organisation of standards to be used during the accreditation proc-
ess.
The standards, criteria and requirements and measurement indicators are grouped into check-
lists (according to annex 1 to this guideline), grouping for a list exactly those standards, criteria and
requirements which are relevant for the subject/domain for which they are applicable.
The indicators proving the fulfilment of those requirements are mentioned in the checklists.
The checklists are instruments for data collection, containing indicator packages generally re-
ferring to a single activity, thus taking part in the development of the entire image of quality and
safety of services in the hospital.
The indicators were built on the principle of logical succession of the stages of an activity: first
of all an interrogation is made on the existence of an activity, then the degree of its development,
then the good or bad experience accumulated by the activity, and then the existence of a type of
evaluation of that activity and the existence of data and information on the evaluation and, finally,
any measures taken to correct the deficiencies.
Another used principle is to collect the same data, by the same indicators, from several
sources, so that there should be an indirect and remote verification of the verisimilitude of answers
received by the evaluators from their interlocutors in hospitals. The principle is met in social sci-
ences under the name of “quiz”. For this reason, the identical indicators were spread in several
checklists and even in several reference chapters.
1.2.2. Expected outcomes from the accreditation process.
General results from the perspective of the healthcare system:
Accreditation of hospitals enlisted in the process and obtaining and keeping a level of
accreditation positioning them with the accredited status.
Maintaining a minimum reasonable level of satisfaction of users to standards and accredita-
tion methodology.
Permanently obtaining a correct feedback regarding the level of standard updating in rela-
tion to the situation in the healthcare system.
18 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
Specific results from the hospital:
During the 9-month period from the registration in the accreditation process, the main results
which are expected from the hospitals are:
understanding and deepening the concept of quality management in healthcare, understanding the accreditation standards, criteria and their requirements, verification of the initial level of compliance with the standards, criteria, requirements, use of own department or person responsible for the quality management to improve the
compliance with the standards, where necessary, preparation of documents/records proving the compliance with the standard requirements
and fulfilment,
establishing the responsible persons by the hospital to communicate with the evaluation team, responsible persons with the required competences regarding the requirements for
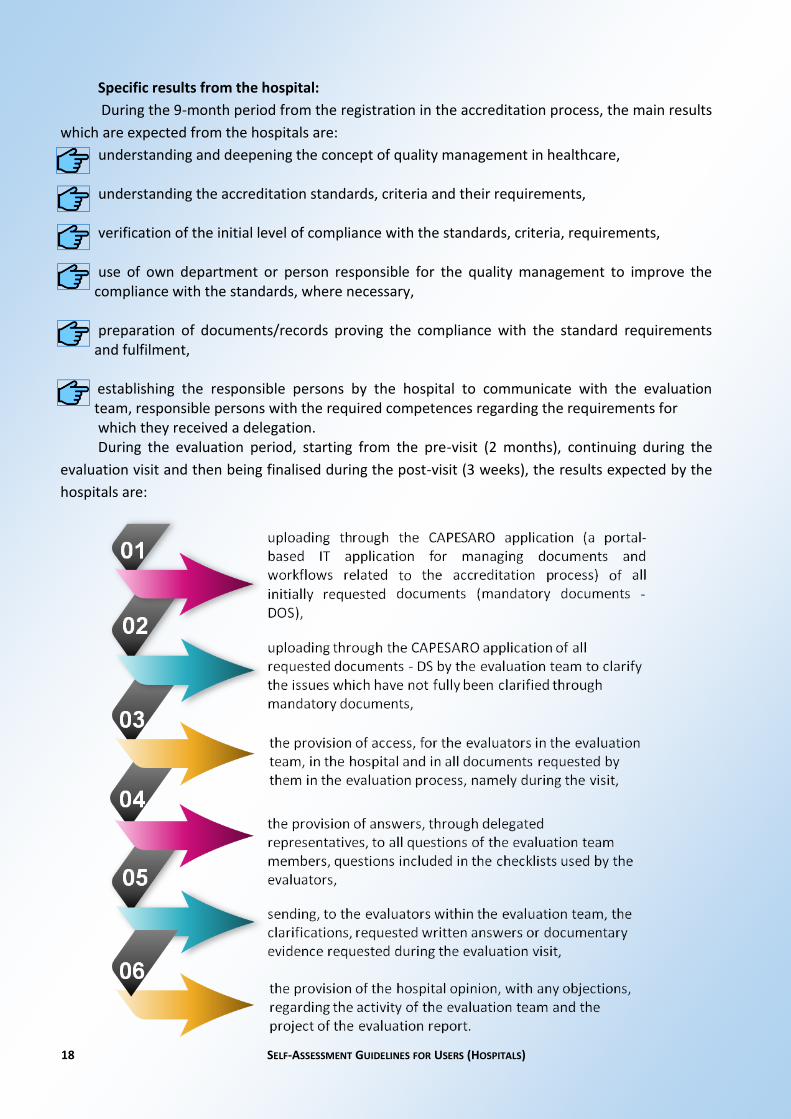
which they received a delegation. During the evaluation period, starting from the pre-visit (2 months), continuing during the
evaluation visit and then being finalised during the post-visit (3 weeks), the results expected by the
hospitals are:

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 19
After the establishment of the accreditation level, for the accredited hospitals and those with-
out a compliance plan, the maintenance of the level of compliance with the accreditation standards,
the results expected from the hospital being:
1.2.3. The conduct.
In relation to ANMCS and the external evaluators which are part of the evaluation team, the
hospital representatives must promptly answer all applications by submitting documents, providing
the access or the requested additional information.
In their entire activity, the hospitals must show interest and a permanent active concern for
increasing the quality of services and their positive reception by the patients, to increase the effi-
ciency of the medical procedure and the administrative procedure but also for the traceability and
predictability of its processes.

20 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
1.3. Beneficiaries of the accreditation process Stakeholders involved in the
accreditation process.
The beneficiaries of the accreditation process are first and foremost the hospitals registered
within the accreditation process. For them, due to the efforts of increasing the quality and the com-
pliance with ANMCS quality standards, the preparation of structure, organisation of healthcare ser-
vices, establishment and procedural processes and flows of activities, forecasting the impact or re-
sult., all these are benefits already from the stage of preparation for the accreditation. At the same
time, increasing the customers’ confidence in the provided services is the competitive benefit in the
community and in the fundraising and new patient market.
The most important beneficiaries of the accreditation process are yet the beneficiaries, for
which the increase in the level of service quality and the ensured degree of safety are arguments to
support the quality management system in healthcare.
For the hospital staff, the benefit is the increase in traceability and predictability of activities,
which contributes to the increase of occupational safety and determines the possibility of profes-
sional development and increase in competences at the workplace.
For the healthcare system and financiers/insurers, the accreditation is the guarantee of knowl-
edge, monitoring and mitigating the functional and institutional risks.
In the accreditation process, four parties are involved:
SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 21
2.1. Overview.
For the hospital, the process called accreditation is a continuous one, which starts with the
submission of the first application, the one of “accreditation”, designating, through it, the entry of
the hospital in the circuit of quality improvement, evaluation, accreditation, monitoring of the main-
tenance of the accreditation level and, at the end of the 5 years specific to an accreditation cycle,
resuming the process by submitting a new application for re-accreditation.
Therefore, there are 3 general stages:
The first stage is to prepare the hospital for accreditation. It starts once with the submission of
the application and lasts for 9 months.
The second stage is the one in which the accreditation is done, namely the evaluation of com-
pliance with the accreditation standards and establishment of the level of compliance with the stan-
dard requirements (“level of accreditation”). This stage lasts about 3 months, since the fulfilment of
the conditions for triggering the accreditation visit.
The last stage is the one for monitoring the maintenance of the level of compliance for the
hospitals without a compliance plan, namely the evaluation of the improvement of the compliance
level, at the end of the 6 month period, ordered by the conformity plan, for the hospitals who re-
ceived a conformity plan to obtain the level to be accredited. Subsequent to the fulfilment of re-
quirements in the compliance plan, the hospital is enrolled in the process to monitor the mainte-
nance of the level of compliance. This stage lasts about 4 years starting with the conclusion of the
evaluation period.
2.2. Overview of standards, criteria and requirements.
The standards are grouped into 3 important chapters called references. This edition of the
hospital accreditation standards contains 3 references, as follows:
Strategic and Organisational Management
Clinical Management
Medical Ethics and Patient’s Rights
These three are, as mentioned before, the three major concerns defining the quality of health-
care services, namely: organisation and structure, provision of healthcare services and patient's sat-
isfaction in relation to the received services and their provider.
Chapter 2. Accreditation process

22 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
From a strategic and organisational perspective, from the perspective of ANMCS, the hospi-
tals must relate to the following standards:
Strategy and strategic management of the organisation are consistent with the need for
healthcare services and the dynamics of the healthcare services market.
The organisational structure and management ensure the optimal development of all assis-
tance and healthcare granting processes.
The human resource management ensures the need for personnel according to the mission
undertaken by the hospital.
The financial and administrative management shall be liable for the strategic and opera-
tional objectives of the hospital.
The IT system meets the need for information and establishes their efficient use in the hospi-
tal.
The communication system existing in the hospital meets the needs of the organisation and
the beneficiaries.
The service quality management system is operational and ensures the development of all
processes related to the monitoring and improvement of quality.
The non-clinical risk management prevents damages and underlies the decision-making
process.
The care environment ensures the conditions required to carrying out the healthcare.
From the clinical perspective, the standards to which the hospitals need to relate are:
The provision of healthcare to patients is done according to their needs, hospital's mission
and available resources.
The initial evaluation aims at identifying the patients' needs in the context of knowing the
exposure to risk factors (environmental, social, economic, behavioural and biological) and
establishes the needed healthcare and care for them.
The medical practice addresses the patient in an integrated and specific manner, ensuring
the continuity of care and healthcare.
The hospital promotes the concept of “child’s friend”.

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 23
The para-clinical services correspond to the investigative needs.
The Nephrology Hospital or the hospital with Nephrology Departments ensures the continu-
ity of healthcare for patients with chronic kidney disease (BCR).
Radiotherapy and/or nuclear medicine provides specific treatment needs.
Palliative and terminal healthcare is addressed to patients with chronic progressive illness
and families and seeks to improve their quality of life by relieving suffering.
The pharmaceutical and medication management ensures the continuity of treatment and
patient’s safety.
The hospital has implemented good antibiotic therapy practices.
The management of healthcare associated infections respects the good practice in the field.
The hospital develops and implements a policy to ensure and improve the patient's safety.
The hospital implemented good transfusion and haemovigilance practices.
The clinical audit evaluates the effectiveness and efficiency of healthcare.
The patient's discharge and transfer is specifically organised, depending on his condition.
Related to the patients and their satisfaction, the standards to which they should relate are:
The hospital promotes the respect for the patient’s autonomy.
The hospital respects the principle of equity and social justice and the patients' rights.
The hospital promotes the principles of benediction and non-harm.
The detailed description of the standards as well as the mapping of the standards in the sec-
ond edition with those of the first edition can be found in the Accreditation Manual in the chapter
"Description of Accreditation Standards" and "Mapping".

24 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
The performance of a hospital organisation is detailed by measuring the compliance with the
standards. There are also standards for which only the presence or absence of conformity is re-
corded, or, as the case may be, the inapplicability of a standard.
For the first reference, there are 32 criteria and 113 requirements that set the level of compli-
ance with the strategic and structural standards.
For the second reference, there are more verified requirements, namely 168, for 53 criteria
describing the clinical management standards.
Finally, 9 criteria and 19 requirements determine how the hospital focuses on the patients'
perception on its services provided to them.
2.3. Steps undertaken by users in the accreditation process.
The actions to be undertaken by the hospital as part of the accreditation process are:
1. submits to ANMCS the request for the registration in the accreditation proc-
ess, 9 months prior to the expiration of the previous accreditation or to the
date of the evaluation visit.
2. uploads, in the CAPESARO application, the mandatory documents for the hos-
pital (DOS), before the start of the evaluation stage (which includes the pre-
visit, the actual visit and the post-visit)
3. pays the accreditation fee, before the start of the evaluation stage
1. in the pre-visit, answers to the requests for documents (DS) by uploading
them in the CAPESARO application, within 2 days from the receipt of such re-
quest
2. within maximum 2 days from the receipt of the of the visit timetable in draft
version, analyses it, proposes the agreed version and appoints, by means of
the hospital manager’s decision, the hospitals representatives who will answer
to the requests of the evaluation board.
3. ensures all the necessary conditions throughout the evaluation visit
4. during the evaluation visits, presents to the evaluation board the documents
requested by the evaluation team members
SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 25
5. makes available to the evaluation board all requested documents and answers
to the questions asked by the evaluation team members in order to verify the
compliance with the requirements of the hospital accreditation standards
6. fills in, during the evaluation visit, all the forms and questionnaires received
from the evaluation board, including the questionnaire for monitoring the ac-
creditation standards (which included the users’ feedback).
7. uploads in the CAPESARO application, during the post-visit stage, all clarifica-
tion documents requested by the team of external evaluators during the visit
or included in the evaluation report.
8. agrees, with or without objections, on the draft evaluation report, within maxi-
mum 5 days from its receipt
9. receives the evaluation report and registers it in the internal register, on the
day of its receipt from the evaluation board
10. sends feedback on the activity of the members of the evaluation board who
made the evaluation of the hospital, by filling in the questionnaire in the
CAPESARO application, after the receipt of the evaluation report
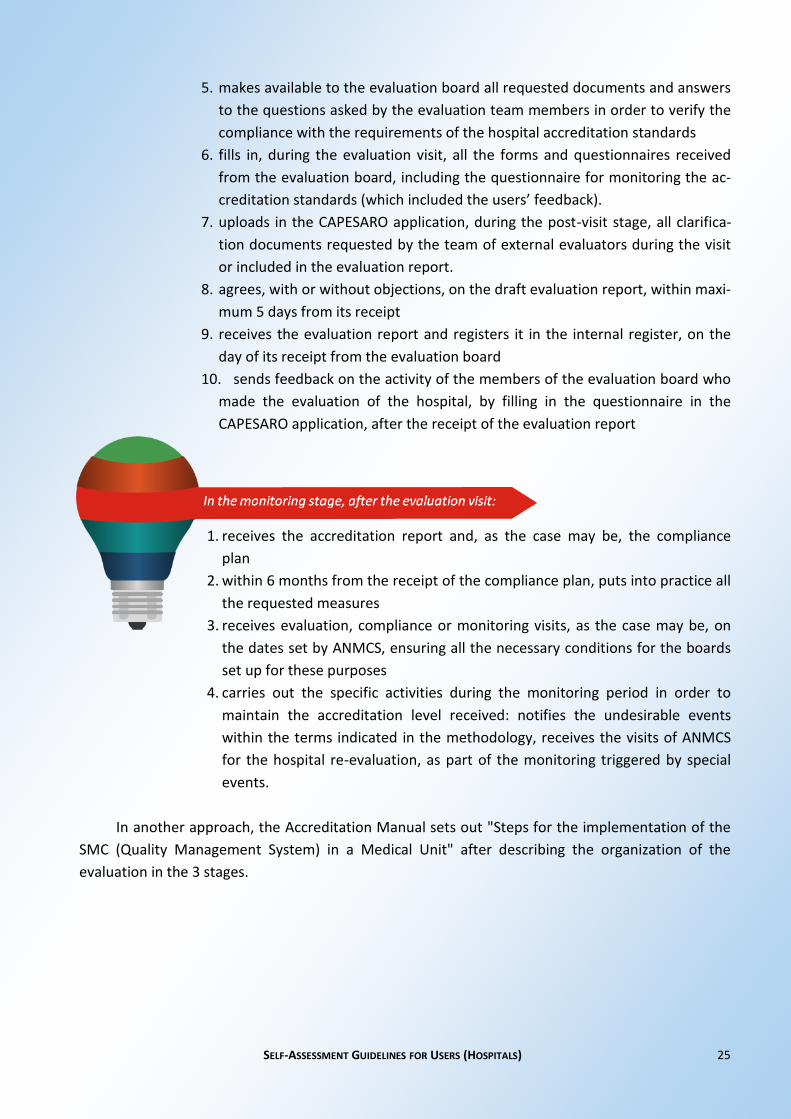
1. receives the accreditation report and, as the case may be, the compliance
plan
2. within 6 months from the receipt of the compliance plan, puts into practice all
the requested measures
3. receives evaluation, compliance or monitoring visits, as the case may be, on
the dates set by ANMCS, ensuring all the necessary conditions for the boards
set up for these purposes
4. carries out the specific activities during the monitoring period in order to
maintain the accreditation level received: notifies the undesirable events
within the terms indicated in the methodology, receives the visits of ANMCS
for the hospital re-evaluation, as part of the monitoring triggered by special
events.
In another approach, the Accreditation Manual sets out "Steps for the implementation of the
SMC (Quality Management System) in a Medical Unit" after describing the organization of the
evaluation in the 3 stages.

26 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
2.4. Description of the hospital evaluation process
The detailed assessment process can be found in the assessment section in the chapter on
accreditation of the Hospital Accreditation Manual.
Planning the visits
Evaluation visits are some of the most important processes of accreditation, which is why they
are the object of a thorough planning, including steps to be taken before as well as during the actual
visits. The first planning is made by means of the multi-annual plan, which sets the calendar of the
evaluation visits of the hospitals and which is approved by the A.N.M.C.S. Management Board. This
plan is updated permanently, as only hospitals who meet the requirements for the initiation of the
evaluation visits are planned for the assignment to an evaluation board.
Self-assessment
The self-assessment form for hospitals is enclosed to the present Guide and also available in
the CAPESARO application. It is a standard form which allows hospitals to assess their compliance to
the accreditation standards. It also includes instructions for filling the form. At the same time, the
CAPESARO application makes available a mechanism for calculating the estimated level of compli-
ance to the accreditation standards. This way, hospitals have the possibility of self-assessing their
level of quality in relation to A.N.M.C.S. standards.
Assigning the evaluation board
According to A.N.M.C.S. procedures for random selection of the members within the evalua-
tion boards, for those hospitals which meet the requirements for the initiation of the evaluation vis-
its, meaning:
they have submitted the request for accreditation,
they have submitted the documents on the structure and number of services which are to be
accredited,
they have submitted the mandatory documents and
have also delivered a self-assessment of the level of compliance by filling in the self-
assessment sheet
have paid the accreditation fee according to the minimal amount set down by
A.N.M.C.S.,

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 27
the number of the evaluation board members is established depending on the hospital structure
(number of locations, departments, beds, specialties etc.) and its classification.
Evaluation visit duration
The duration of an evaluation visit varies between 2 and 5 days and is calculated so that the
time needed by the members of the evaluation board to apply the checklists does not exceed the
normal work schedule of a working day, for each of the evaluators. If needed, in order not to ex-
ceed the 5 days maximum duration of an evaluation visit, the number of evaluators assigned in the
board can be supplemented.
Scheduling the evaluation visit
Once set the period of the evaluation visit, the evaluation board proposes to the hospital the
evaluation visit timetable, which sets the order, the location and the time of applying the checklists,
as well as the interlocutors with whom the lists are applied. This timetable is approved with or with-
out amendments by the hospital manager, and becomes effective once the kick-off meeting ends.
Evaluation report
After the evaluation visit, during the post-visit period, the evaluation board prepares the draft
evaluation report, based on the applied checklists. It is then submitted to the hospital for approval,
with or without objections. Objections must be sent in writing, through an official document signed
by the hospital manager and bearing a registration number. Within the term mentioned in the pro-
cedure, for each objection the evaluators shall formulate an opinion and prepare support docu-
ments, which are then sent to A.N.M.C.S. together with the hospital objections. Within the term
also mentioned in the A.N.M.C.S. regulations, the Committee for analysing objections meets, in or-
der to accept or reasonably reject the objections raised by the hospital. The decision of the Commit-
tee for analysing objections is then communicated to the members of the evaluation board in order
to write the Evaluation report, which is submitted to the hospital which registers and confirms its
receipt.
The evaluation report, together with the file with the evaluation documents, are the docu-
ments on the basis of which the accreditation level is set. Also, these are the documents used by
A.N.M.C.S. to draw up the accreditation report and eventually the compliance plan.

28 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
2.5. The evaluators and the evaluation board.
The healthcare service evaluator is an individual specialised in healthcare services
quality management who holds, pursuant to law, the graduation certificate for
healthcare services evaluators or for hospital evaluators training and/or improvement courses, as
appropriate.
Evaluators are specially trained persons who, on the basis of an agreement signed with
A.N.M.C.S., carry out the external and independent evaluation process, on behalf and for A.N.M.C.S.
The evaluation board is the team assigned by A.N.M.C.S., under the coordination of a presi-
dent, an employee of A.N.M.C.S., who has the responsibility to carry out all activities related to the
evaluation process (pre-visit, actual visit and post-visit) for a certain hospital, and also to draw up all
documents provided by the evaluation procedure of A.N.M.C.S., the document by which the evalua-
tion process is ended being the evaluation report.
The evaluation report is a collective document, drawn up and assumed by all members of the
evaluation board.
2.6. Training and profile of evaluators.
Evaluators follow an intense training programme. The first level refers to the initial training,
through the Training programme for evaluators, carried out by A.N.M.C.S., in partnership with the
National School of Public Health, Management and Professional Development in Bucharest
(SNSPMPDSB), the sole body which can provide initial and continuous training, as part of a protocol
signed with A.N.M.C.S. which agreed both on the training curriculum as well as the trainers.
The training curriculum and the training programme handbook for the healthcare services or
hospital evaluators were developed together with A.N.M.C.S. and with its approval.
Following this initial programme, in order to add additional information, a Specialization pro-
gramme for evaluators is organized, also in partnership with SNSPMPDSB, a programme intended to
cover the continuous training level for evaluators.
Beside these 2 special training programmes, which include both theory and practice, at
A.N.M.C.S. level, evaluators are included in specialized trainings where they analyse up-to-date in-
formation from the evaluation practice. These trainings also take the form of plenary sessions, with
the support of directors of different departments, support divisions and of the A.N.M.C.S. president.
Another level of training takes place within the evaluation board, being carried out by the president
of the board, which details, explains and presents the work instruments, the forms used as well as
the particularities of the hospital which is to be evaluated.
SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 29
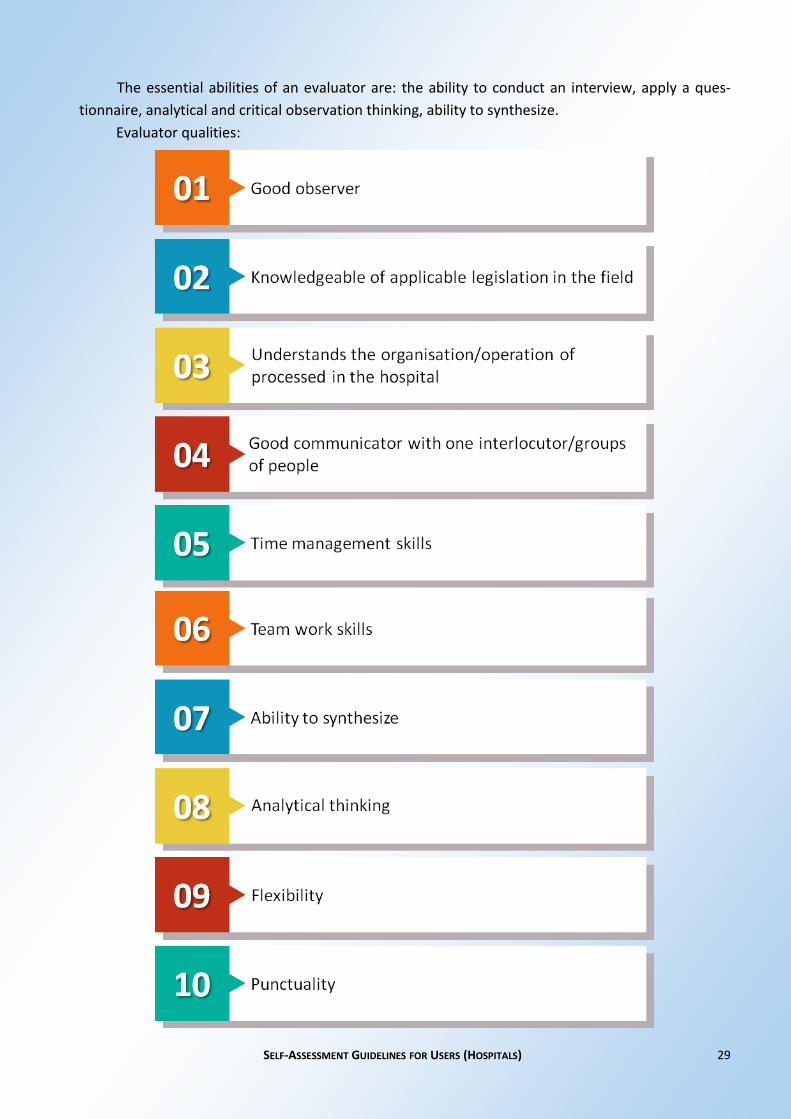
The essential abilities of an evaluator are: the ability to conduct an interview, apply a ques-
tionnaire, analytical and critical observation thinking, ability to synthesize.
Evaluator qualities:

30 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
2.7. Evaluation visit requirements.
Evaluation visit requirements:

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 31
2.8. What A.N.M.C.S. does in relation to the hospital.
before the start date of the accreditation procedure for the hospital, makes available
the Accreditation standards for hospitals;
after the hospital registration in the accreditation procedure, that is 9 months prior to
the date when the scheduling procedure of the evaluation visit starts, gives access to the
CAPESARO application;
after the submission of the hospital request to enter the accreditation procedure, 9
months prior to the date when the scheduling procedure of the evaluation visit starts,
makes available the accreditation manual and the self-assessment guide, which included
the self-assessment form;
once the hospital fills in and uploads in the CAPESARO application the self-assessment
form and the document presenting the identification data and the functional description
of the unit, within the 9 calendar month period from the request of the hospital of enter-
ing the accreditation procedure, calculates and informs the hospital management on the
amount of the accreditation fee;
after the payment, by the hospital, of the accreditation fee, A.N.N.C.S. sets the date of
the evaluation visit. 2 month prior to this date, the preliminary activities for the prepara-
tion of the evaluation visit start. In the pre-visit stage, specific instruments are applied by
the external evaluators of A.N.M.C.S.;
during the maximum 1 week period of the evaluation visit, but also in the 3 weeks fol-
lowing the visit (post-visit), monitors and supervises the activity of the evaluation board;
sends the Accreditation report to the hospital, with the following accreditation levels:
accredited; accredited with recommendations; conditional accreditation; accredited
with a compliance plan; not accredited. For the compliance plan, gives the hospital the
possi bility to prove the implementation of at least the requested measures, in a 6
month period from the receipt of the plan. At the end of the 6 month period, it starts
the compliance visit;
receives and answers possible appeals;

32 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
ensures the monitoring of hospitals on a 4 year period from the end of the evaluation
process (pre-visit, actual visit and post-visit);
in special situations, starts the monitoring visit following which it can decide to maintain
the accreditation or set a compliance plan
A.N.M.C.S. sends to hospitals:
2.9. Defining compliance levels.
Following the evaluation of hospital compliance with the accreditation standards, the follow-
ing accreditation levels can be established:
accredited; accredited with recommendations; conditional accreditation; accredited with a compliance plan; not-accredited.
SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 33
For the compliance plan, A.N.M.C.S. gives the hospital the possibility to prove the implementa-
tion of at least the requested measures, in a 6 month period from the receipt of the plan. At the end
of the 6 month period, A.N.M.C.S. starts the compliance visit
2.10. Monitoring the maintaining of the accreditation level, post-
evaluation.
Once it is granted one of the 3 levels of accreditation (considering that the compliance plan is
an intermediary stage, following which the hospital can be declared as being accredited or not-
accredited), the healthcare unit enters, according to the A.N.M.C.S., the monitoring period, which
lasts for about 4 years, until the re-commencement of the accreditation process, for the every 5
years re-accreditation.
During this time, hospitals shall follow the maintenance and the improvement of quality, im-
provement of processes, by regularly checking the level of compliance with the updated standards
at the time of the self-assessment process.
According to the A.N.M.C.S. methodology, the hospital shall send the requested notifications
and reports, within the terms communicated by A.N.M.C.S., including a form for the monitoring of
the compliance with the accreditation standards, every 3 months after the end of the evaluation
period, and also a form for the monitoring of special situations.
In special circumstances, A.N.M.C.S. starts the monitoring visit following which it can decide to
maintain the accreditation or set a compliance plan.

34 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
3.1. The rights of the hospital.
the right to be evaluated and accredited
According to the Romanian legislation for the healthcare system, every hospital has the right
to request the national body for the quality management in the healthcare system, A.N.M.C.S. to
evaluate the level of quality management, according to A.N.M.C.S. standards and, depending on the
evaluation result, to grant the accreditation for the level of compliance with the accreditation stan-
dards. This right can be requested in writing, being associated with the payment of a fee for the ser-
vices which shall be provided for the purposes of evaluation and accreditation.
right to be informed (standards to the level of accreditation requirements, process and
methodology)
In the accreditation process, hospitals shall be informed on the standards against which they
have to compare the quality of the services provided, with additional details, descriptions, as well as
the requirements for proving the criteria are met. They shall be made public on the A.N.M.C.S web-
site, together with the documents describing the accreditation process.
The accreditation process and the methodology, including the methods of measuring the level
of compliance to the accreditation standards, are also public, as they can be accessed on the
A.N.M.C.S. website as well as in the guidelines, manuals, methodologies and procedures made avail-
able to hospitals by A.N.M.C.S., so that they understand better the accreditation process.
right to be advised
Hospitals have the right to ask for feedback on the way in which they understood to meet
their obligations and carry out the activities assigned to them in the accreditation process. At the
same time, they can request for tailored explanations on what they have to do in order to follow the
accreditation timetable, without delays or errors.
Chapter 3: The hospital during the accreditation process

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 35
right to participate
Hospitals have the right to participate to any public debate, counsel, conference or meeting
organized by A.N.M.C.S. alone or in partnership, on the subject of quality and accreditation of
healthcare services.
right to challenge
Beside the right to appeal guaranteed by special laws, hospitals have the right to challenge any
of the documents or the opinions they consider as inconsistent with the reality of containing writing
or content errors. Depending on the stage they find themselves in in the accreditation process, hos-
pitals can submit their appeals to A.N.M.C.S. or the evaluation board. The terms and the interpreta-
tion for the settlement on each case are defined in specific methodologies and procedures. Depend-
ing on the type of the appeal, the answers are sent to hospitals within the terms provided in the
A.N.M.C.S. procedures and methodologies.
3.2. Hospital activities specific to the accreditation process.
carries out the self-assessment
At the beginning of the accreditation process, immediately after the submission of the accredi-
tation or re-accreditation request, hospitals receive the self-assessment form, which is a useful in-
strument to check the level of compliance to the accreditation standards.
Self-assessment can be repeated at any stage of the accreditation process, being necessary
before the start of the evaluation visit.
receives and facilitates the evaluators' visit
During the evaluation visit, hospitals have the obligation to receive and facilitate the access of
evaluators in the hospital. The hospital shall ensure the necessary conditions for the evaluators in
the evaluation process, by giving them access to documents, to the facilities necessary for the
evaluation and access to the staff in charge of specific activities which are to be evaluated. The hos-
pital shall facilitate the evaluators' access to the locations in which the activities and services subject
to the accreditation process are provided.

36 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
actively contributes to the development of the draft and final evaluation report
At the end of the evaluation visit, while the draft evaluation report is drawn up, the hospital
contributes by providing information or documents requested by the evaluation board during the
evaluation visit. Once the draft evaluation report is finalised, hospitals can express their opinions,
objections or points of view on the report, the members of the evaluation board being obliged to
analyse their opinion and make the necessary changes in the evaluation report, as the case may be.
intervenes for the meeting of different criteria during the post accreditation monitoring
process
Except for the case when the hospital, following evaluation, received a compliance plan, dur-
ing the post-evaluation monitoring period, of 4 years after accreditation, the hospital can improve
the level of quality of the already evaluated services and which allow for the improvement of the
level of compliance to the A.N.M.C.S. standards. Thus, following accreditation and taking advantage
of a specialized information from A.N.M.C.S., through its monitoring specialists, the hospital can use
the result of the accreditation process as a feedback for the improvement the level of quality.
3.3. Preparing for the evaluation visit.
The evaluation visit is an important step in the process, given that it makes a scan of the hospi-
tal at a certain time, from 3 perspectives: structure, processes and results. Before the evaluation
visit, the hospital must be informed on the concept of quality in healthcare services, quality man-
agement in hospitals, accreditation standards developed by A.N.M.C.S. and the accreditation meth-
odology.
The hospital must have a separate structure for quality management or a quality management
responsible and the internal organization must be in line with the legal provisions in force. The re-
quest for registration in the accreditation process must be submitted only after the unit has met the
minimum requirements.
At the same time, before the evaluation visit, the hospital must have in place specific proce-
dures, which are prepared, known by those involved, functional (implemented) and monitored, to-
gether with the evidence proving these.
The hospital must be able to prove that the activities evaluated from the quality point of view
are planned, implemented, monitored and adjusted when needed. The first check is done together
with the first self-assessment process, by filling in the self-assessment form.
The self-assessment form is the instrument made available to hospitals in order to get the
feedback needed for making the necessary adjustments before the commencement of the evalua-
tion visits. The use of this instrument can check the level of compliance with A.N.M.C.S. accredita-

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 37
tion standards, each time the hospital unit takes measures for quality improvement and wants to
adopt the same references as the evaluation board. At the same time, the indicators can be a good
mechanism for collecting examples of measuring the compliance with the standards requirement,
when the hospital has a different way of meeting the standards.
Another activity which is not related to quality management, but necessary for hospitals for
the preparation of the evaluation visit is the access and use of the CAPESARO application.
CAPESARO application is the IT instrument developed by A.N.M.C.S. by means of which the
institution collects information, centralizes documents and provides hospitals with different data or
work instruments (such as the self-assessment form). The access to the application is secured and
restricted only to those having a user account and a password, which ensures confidentiality, avail-
ability and speed, as data from hospital units, evaluators or A.N.M.C.S can be uploaded at any time
and from any location of the user.
CAPESARO application is also used by evaluators, who are given access to resources or data
regarding hospital units depending on the evaluation board they are assigned to. In times when the
accreditation standards and methodologies are subject to different changes and these changes are
being tested, experts or volunteers are given limited access to CAPESARO application, in order to
upload different documents or download information they need in their activity.
In addition, all manuals, guidelines, methodologies, procedures, work instruments or forms
can be found in the specific sections and can be downloaded from the application, depending on the
rights and the level of access of the user.

38 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
39 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
Table of Contents
Chapter 1. General presentation ..................................................................................... 5
1.1. Quality assessment - the philosophy underlying the accreditation
of hospital-based services. .............................................................................................. 5
1.1.1. What is A.N.M.C.S. .......................................................................................... 6
1.1.2. What is accreditation ...................................................................................... 8
1.1.3. General considerations on service quality .................................................... 12
1.2. Statement of terms and the use of the standards, criteria, requirements
and indicators during the evaluation . .......................................................................... 14
1.2.1. Selection and organisation of standards to be used during
the accreditation process. ...................................................................................... 17
1.2.2. Expected outcomes from the accreditation process. ................................... 17
1.2.3. The conduct. ................................................................................................. 19
1.3. Beneficiaries of the accreditation process Stakeholders involved in
the accreditation process. ............................................................................................ 20
Chapter 2: Accreditation process .................................................................................. 21
2.1. Overview. ............................................................................................................. 21
2.2. Overview of standards, criteria and requirements. ............................................ 21
2.3. Steps undertaken by users in the accreditation process..................................... 24
2.4. Description of the hospital evaluation process ................................................... 26
2.5. The evaluators and the evaluation board. .......................................................... 28
2.6. Training and profile of evaluators. ...................................................................... 28
2.7. Evaluation visit requirements. ............................................................................. 30
2.8. A.N.M.C.S. notice to hospital. .............................................................................. 31
2.9. Defining compliance levels. ................................................................................. 32
2.10. Monitoring the maintaining of the accreditation level, post-evaluation. ......... 33
Chapter 3: The hospital during the accreditation process ..................................... 34
3.1. The rights of the hospital. .................................................................................... 34
3.2. Hospital activities specific to the accreditation process. .................................... 35
3.3. Preparing for the evaluation visit. ....................................................................... 36
Glossary
Self-Assessment Tools
Appendix 1: FAE
Appendix 2: Master list
Appendix 3: Validation methods for suggested evidences (indicators)
Appendix 4: Overall rating
SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 40
Glossary
Accreditation - The action of recognition or acknowledgement by an external evaluation body
of the level of compliance with accreditation standards, resulted after an external and independent
technical evaluation, establishing the performance level of an organisation (healthcare organisation)
against those standards. See also ISQua accreditation.
ISQua accreditation - Public recognition by ISQua of the manner in which a body with the role
of external evaluator which develops standards in a healthcare system meets the ISQua
international standards or principles, after this body underwent an independent external evaluation
of its organisational performance, of the standards they developed and/or of the training/education
programmes on standards.
Threat - External factor which may exploit the vulnerability of an organisation by actions or
facts which cause imbalance or instability and generate life threatening situations, endanger the
bodily integrity or freedom of persons or values;
Risk analysis for physical security - Activity undertaken to identify threats and vulnerabilities
which may endanger people’s life, bodily integrity or freedom or may prejudice the values owned
by the organisation, in order to determine the impact and to evaluate security risks, underpinning
the necessary actions to limit or eliminate them;
Healthcare - All medical acts undertaken for diagnosis, therapeutic or rehabilitation and
recovery purposes
Audit - Systematic and independent examination and review of activities to determine
whether they match the objectives set and the accepted rules to reach them.
Good practices - Approach which may deliver the best outcomes, selected by a systematic
analysis process which proved it to be a good example or a success. It is further adapted to cater for
a given organisation.
Risk management framework - A set of components which provide the basis and the
organisation rules for the design, implementation, monitoring, review and continuing improvement
of risk management within the organisation. The framework should be integrated in the overall
strategic and operational policies and practices of the organisation.
Qualified - Holding the required certificates, trained and legally and professionally licensed to
perform specific activities.
Quality - Level of excellence, extent to which an organisation meets the needs and the
expectations of its customers (patients)
Research - Production of new knowledge, recognised as such, as a result of systematic,
sometimes random search, using field-specific methods an techniques, in order to advance
knowledge, with or without intention to achieve long-term economic or social benefits, with or
without intention to transfer them to enforcement sectors (fundamental, applied, experimental)
Certification - Formal recognition of compliance against approved standards, validated by
external evaluation.
Information circuit - Path taken by information or a category of information between issuer
and recipient
41 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
Customers - Natural or legal persons to whom the organisation provides services, goods or
works.
Code of conduct - Documented set of principles and recommendations, agreed to shape and
maintain certain behaviours, which provide all parties involved information on the responsibilities
and expectations generated by that code.
Hospital competence - Capacity to provide assistance and healthcare evaluated by: formal
professional competence (certification of training in the field) and practical competence (medical
team experience) and technical and physical resources necessary to provide assistance and
healthcare in place
Competence - Individual knowledge and skills, adequate to provide certain services and
guarantee that those knowledge and skills are assessed regularly.
Complexity - Number of medical specialties in a hospital
Community - Individuals, families, groups and organisations which interact, cooperate to
undertake joint activities and participate in solving common concerns which, in general, occur
within a common geographic area or environment.
Confidentiality - Guarantee of limitations of the right to use or distribute information received
from individuals or organisations.
Consent - Assent or approval given by a customer (patient), his/her caregivers, guardians or
guardianship supervisory authority.
Dose constraint - Dose constraint is a restriction imposed to the doses a person may receive
from a given source and a useful tool for optimisation of radiation protection.
Dose constraint relies on a prospective evaluation of doses, using well managed practices or
the rationale of a professional, and is not a dose limit.
A threshold dose level or dose output, maintained at the lowest reasonable level, to allow
delivery of diagnostic information required, considering social and economic factors, it is a
protection improvement tool.
Interdisciplinary consultation - It relies on transfer of concepts and methodologies from two
or more fields (domains, specialties), to the treating physician, in order to solve certain problems
which cannot be properly researched by one field/speciality. Interdisciplinarity involves clarification
of new working practices and assumptions for each specialty involved, and integrated interaction for
the unitary diagnosis and treatment of a certain condition.
Continuity of care - Extent to which patient healthcare is coordinated between practitioners
and organisations in time
Contract - Formal agreement stipulating the terms and conditions for services received or
provided from or to another organisation. The contract and contracted services are monitored and
coordinated.
Criterion - A specific step which must be taken or an activity which must be carried out to
meet a requirement or a standard.
Culture - A shared system of values, beliefs and behaviours.
Data - Unorganised facts or aspects which may generate information.
DDD - Defined Daily Dose = (according to WHO) the assumed average maintenance dose per
day for a drug used for its main indication in adults. DDD is a statistical measure of active substance
consumption defined by the World Health Organisation (WHO). It is used to standardise comparison

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 42
of active substance consumption between various drugs or various healthcare environments.
Dependency - Individual’s incapacity to adopt certain behaviours or to undertake alone,
without the help of another person, actions which allow him/her to achieve an acceptable level of
satisfaction of basic needs. (Nursing Guide with evaluation and care techniques for basic needs -
coordinator Lucreția Titircă, Viața Medicală Românească Publishing House, Bucharest, 2013)
Executive Director - A person holding a management position in an organisation, appointed by
the management body of the organisation. Other titles, such as manager, director or general
manager may be used.
Scope - Field of activity (medical, social, economic, scientific, cultural etc.) in which various
types of services provided by the organisation are delivered under certain conditions and
limitations.
Human Resources record - All information about an employee of the institution (staff
member). It includes human resources management data such as: holidays, recommendations,
performance reviews, qualifications, employment registration and conditions.
Rights - Something that can be claimed by a person, as a rightfully, fair, legal or moral
entitlement. A formal description of the services customers may expect and claim from an
organisation.
Multidisciplinary team - A multidisciplinary team includes professionals from various medical
specialties, who bring together their own working methodologies to build a diagnosis or treatment
procedure which adds up the activity of all team members to reach a common outcome. Under
multidisciplinary relations, cooperation between scientific fields may be “mutual and cumulative,
but not interactive”.
Multidisciplinarity is a non-integrative combination of scientific specialties where each
specialty maintains its working methodologies and assumptions without adopting changes or
developments from other specialties, within multidisciplinary relations.
Pluridisciplinary team - A team of professionals from various professions (physician,
psychologist, social worker, spiritual guide) who cooperate by systemic transgressive interference
focused on the patient and on the quality of the patient’s overall condition.
Pluridisciplinarity relies on the use of independent methods and theories from various
disciplines and their application to shape, structure and understand various phenomena and
processes which transcend healthcare, but start from it. Pluridisciplinarity occurs when a general
assumption applies creatively to other scientific fields and generates a new set of systems, laws,
relations and structures.
Education - Systematic learning and training of necessary activities to develop, acquire or
change knowledge, attitudes, values and skills.
Effectiveness - Extent to which services, interventions or actions are provided according to
existing good practices to reach objectives and accomplish best results. A dimension of quality.
Ethics/ Ethical - Set of recognised principles guiding professional and moral conduct.
Evaluation - Appraisal of success in reaching expected objectives and outcomes regarding the
organisation, services, programmes or customers.
External evaluation of the organisation - Highly objective appraisal performed by a
recognised body of professionals who are not employed by the organisation and who evaluate as
objectively as possible the performance of a user against the quality standards applicable.
43 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
Quality assessment - Planned and systematic collection and analysis of data related to a
service, usually focused on the specifications related to its content and operation and to customer-
oriented outcomes.
Evaluator - External professional with expertise in the field who may appraise the organisation
performance against agreed standards.
Adverse event - Any medical incident which may occur during healthcare activities, or outside
such activities (unfavourable and unintended response)/event considered, which represents an
unintentional and undesired harm, injury, illness, temporary or permanent disability or even death
of the patient, associated to healthcare provision
Undesirable event - Any event endangering patient’s life or safety
Sentinel event - Adverse event involving serious harm to patient’s health with long-term
consequences, permanent disability or patient death which reflects serious deficiencies in the
healthcare provider’s policies and procedures, lack of interest for safety and an organisation at risk
in service provision. Such an event signals the need for immediate investigation and adoption of
adequate corrective actions
"Near miss" event - Incident or potential incident, which was avoided and did not cause harm,
although it could have caused harm.
Function examination - Medical investigation of the health condition by evaluation, using
specialised devices, of the functioning parameters of various organs/organ systems in the human
body:
– respiratory function (spirometry), cardiovascular system (EKG- electrocardiogram), kidney
function (probes?), gastric secretion, liver function, bile ducts, pancreas (intubation or fibroscopy-
endoscopy: oesophagus, gastroscopy, colonoscopy), visual analyser (visual acuity), acoustic-
vestibular analyser (audiometry), nervous system (EEG - electroencephalogram).
It requires the use of specialist equipment, and it is performed upon request of a specialist
physician.
Data mining - A process used to analyse large sets of data and extract relevant information
using mathematical and statistical methods.
Reliability - Extent to which results are validated by repeated measurements made by
different persons or at different times by the same person, when what is being measured did not
change in the interval between measurements.
Information flow - Quantity of information passed between issuer and beneficiary along the
information circuit, characterised by certain properties - length, speed, reliability, cost, etc
Provider of healthcare services - Legal organisation, entity or group of entities, with or
without legal personality, which provide healthcare services, primary assistance, community
assistance, services for acute patients, specialist healthcare services etc.
Risk management - A systematic process of identification, evaluation and actions to prevent
or manage within the organisation health or safety risks at clinical, administrative, property or
occupational levels.
Guideline - Thematic document including guiding principles and actions on a certain topic.
Practice Guide - A document on a certain theme which presents tools describing processes
based on clinical trials or endorsed by experts as most efficient in the evaluation and/or treatment
of a patient with a certain symptom, condition or diagnosis, or which describes a specific procedure.
SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 44
Level of dependency - Level of dependency or severity of dependency of a care beneficiary -
the level of autonomy compared to a person who, without the help of another person, may
undertake alone the necessary actions to satisfy his/her basic needs.
This may be determined after the evaluation of the independence / dependency function of
each basic need. (Nursing Guide with evaluation and care techniques for basic needs - coordinator
Lucreția Titircă, Viața Medicală Românească Publishing House, Bucharest, 2013)
Population groups with clinical-biologic particularities: children, elderly, pregnant women,
people with disabilities etc. - Groups of people who live in the same geographic area and have
various properties / common/similar specificities in terms of their health condition and of clinical or
biological criteria.
Governance - Function which determines the direction, the objectives and the development
policy of an organisation in order to accomplish its mission and which allows monitoring of
achievements and policy implementation.
Diagnostic nuclear imaging (performed in Nuclear Medicine laboratories, uses the physical
properties of certain radioactive isotopes): myocardial, brain, lung scintigraphy, bone scintigraphy,
kidney scintigraphy, Spect-CT, positron emission tomography (PET), hybrid PET- CT versions (PET
scanner – computed tomography) or PET-RM (PET scanner – magnetic resonance)
Security incident - Event occurring with an uncontrolled evolution, which generates
unwanted consequences on persons and/or assets and/or activities within an organisation and
which requires immediate action to reinstate the previous situation;
Incidents - Unusual, unexpected events which may involve an element of risk or may have a
negative impact on customers, groups, staff or organisation.
Independence - Reaching an acceptable level in basic needs satisfaction (including
physiological and psychological needs) by actions undertaken by the individual himself/herself,
without the help of another person. (Nursing Guide with evaluation and care techniques for basic
needs - coordinator Lucreția Titircă, Viața Medicală Românească Publishing House, Bucharest, 2013)
Indicator - Performance measurement tool used to monitor, evaluate and improve the quality
of services. Indicators are related to structure, process and outcomes. They are calculated according
to a compliance ratio, for example they have a numerator and a denominator so that they and be
compared and used as benchmarks.
Data integrity - The meaning of data is not different from the meaning registered in the
source document; data are not accidentally or intentionally.
Interoperability - Capacity of different entities / systems / software applications to exchange
data through a common set of procedures so that they answer specifically to certain problems or
fields of activity.
Preventive maintenance - A planned, scheduled, cyclic process of functional evaluation of
equipment, performed before using new equipment and regularly throughout the equipment life
cycle. The purpose is to maintain equipment performance according to manufacturer specifications.
It includes a verification of safety of equipment use.
Healthcare - All specific care activities to cater for the basic needs of each patient,
complementary to nursing
Records - Documents certifying results obtained or providing evidence of activities performed,
which are the result of key processes, for example human resources records, customer records,
45 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
customer reports.
Procedure justification - Analysis of specific benefits of patient care, against risks (e.g.:
exposure to ionising radiation); it is performed individually, considering economic, social factors,
costs etc. and existence of other specific procedures (e.g.: no exposure to radiation); if the
procedure cannot be justified, it shall not be performed.
Clinical laboratory - A medical specialty department within a hospital, which, based on
biological samples collected from the human (generally blood samples) performs biochemical
investigations to place the results within specific parameters of diagnostic relevance. E.g.
haematology, biochemistry, bacteriology, immunology, cytology; pathology laboratory
Radiology and Medical Imaging Laboratory - Medical specialty department performing
investigations:
- X-ray investigations: radiography, fluoroscopy, tomodensitometry or computed tomography
with or without contrast, mammography, DEXA bone densitometry;
- ultrasound: abdominal-pelvic ultrasound, fetal morphology, cardiovascular ultrasound,
thyroid ultrasound, musculoskeletal ultrasound, mammary glands and genitals, eye ultrasound,
transesophageal ultrasound, transfontanellar ultrasound;
- Nuclear Magnetic Resonance (NMR)
Networking - Connections, contacts, collaborators/partners and collaboration/work
relationships with others.
Management - Science and technique of organisation and management, all organisation,
leadership and management activities of any type of organised activity or economic unit for
manufacturing, services or trade (including medical services).
Stages: setting targets or goals, by planning and budgeting, definition of processes to reach
these objectives and allocation of resources to implement these plans. Take actions to implement
the plans by organising, employment of personnel, control and problem-solving.
Information management - Information management and control system including data
which are organised, interpreted and usable. The information may be written, audio, video or
pictures.
Security action - Basic component of a security solution, corresponding to one or several
threats and vulnerabilities identified by the risk analysis, whose purpose is to reduce related risks;
Feedback mechanism - How an organisation checks the effect caused by its actions or services
by direct liaison with their beneficiaries
Security mechanisms - Solutions which include several security actions, operating according to
predefined scenarios, to secure one or several facilities, when they are located within the same
perimeter;
High-risk drugs - Drugs which are dangerous for the human body (may lead to death,
miscarriage, permanent or temporary, local or general health damage etc., due to failure to non-
compliance with the dose prescribed or due to substances which may cause allergies or toxic
reactions when associated with other substances present in food)
Mentoring - Guidance and continuing training programme for evaluators and external users
where training is provided by unmediated assistance (face-to-face and distance learning) of a
mentor
Mission - General written statement of an organisation’s position and goals. The mission
SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 46
differentiates organisations.
Dangerous substances - Also called harmful agents – any chemical, physical or biological
factor present in the work environment (occupational environment) which may endanger employee
health.
Nursing - International term used by the World Health Organisation for the specific function of
licensed nurse, which helps sick or healthy individuals perform those activities which contribute to
maintaining or recovering their health.
Objective - A goal which should be achieved if the organisation is to reach its purposes. It is
the translation of goals at a specific, concrete level, where results may be measured.
Objectives of care - Description of behaviour expected as a response of patient’s health to a
treatment, a result we want to achieve following interventions. (Nursing Guide with evaluation and
care techniques for basic needs - coordinator Lucreția Titircă, Viața Medicală Românească
Publishing House, Bucharest, 2013)
Procedure optimisation - Amendment of procedural parameters so that they respond best to
the purpose of the procedure, with least side effects and/or related risks.
In radiodiagnosis, obtaining a good quality image with minimal exposure to ionising radiation;
in radiotherapy, accurate release of desired dose in the target volume, with minimal exposure of
peritumoral healthy tissues and/or radiosensitive organs.
Management body - Natural persons, groups or agencies with authority and responsibility for
setting the strategic guidelines and the organisation operation. Also known as Board, Committee,
Commissioners Committee.
External evaluation body - Acknowledged body in the field which provides an independent
evaluation of an organisation’s performance, against specific quality standards for the functions of
that organisation.
Accredited Dosimetry Body - A body responsible with benchmarking and verification of
individual dosimetry surveillance instruments and reading or interpreting their indications, or for
radioactivity measurements in the human body or in biological samples, or for dose evaluation and
determination, accredited by the National Commission for Nuclear Activities Control.
Organisation - It comprises all structures/locations under the management of the organisation
management body/owner, to who it reports.
Induction - A process by which employees become familiar with all work-related aspects and
their responsibilities.
High Performance - Exceeding own results, obtaining top results by using state-of-the-art
technologies and mastering best practices in the field, development of practices with results
exceeding those obtained to date by top professionals
Personnel - Employees of an organisation
PLAN A detailed document which identifies the needs, the list of strategies to cover those
needs and sets targets and objectives. The document may include descriptions, policies and
procedures, practice guides, protocols or a combination thereof (JCI 5th edition)
Operational Plan - Organisation’s management document explaining how to transpose into
practice the organisation’s strategy.
It is a result f strategic planning and it includes the necessary processes, actions and resources
to achieve the objectives set by the strategy.
47 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
Strategic Plan - A formal plan formal setting the overall goals and aiming at positioning and
adjusting the organisation according to its environment.
Patient Care Plan - A written document summing up the stages of the nursing process which
informs each member of the healthcare team on the patient and the interventions performed.
Regardless the nursing theory used for the patient care plan, it should include: the nursing
diagnosis, the objectives of care, nurse interventions and evaluation of interventions.
The nursing process is turned into action by using the patient care plan.
Complaint - Oral or written description of a problem, aspect or dissatisfaction with the
services received.
Policies - Documented statements formalising the task and concept approach according to the
objectives of the organisation.
Radiodiagnosis practice - Getting a medical diagnosis based on a radiologic examination.
Radiologic examination uses radiology and medical imaging methods as well as diagnostic nuclear
imaging.
Radiologic procedure - Medical diagnostic or treatment procedure using ionising X, gamma,
electron, neutron radiation etc.
Procedures - Sets of written instructions which communicated approved and recommended
steps for a specific action or set of actions so that results are predictable and responsibilities are
clear and assumed.
IT procedures - All elements establishing the means of collection, registration, submission,
processing and archiving of a category of information, mentioning operations to be performed, their
sequence, support, formulas, models and treatment of information used.
Process - Series of interdependent activities and communications leading to delivery of
services.
Care process - An organised and planned process, a rational method to plan and promote
individualised interventions in order to obtain a good health condition for the individual, family and
community. It is a scientific method of solving the individual’s current and potential problems, based
on the physiologic, psychological, socio-cultural and spiritual needs of the individual. It focuses on
the particular responses of each individual (or group of individuals), to a real or potential health
change. (Nursing Guide with evaluation and care techniques for basic needs - coordinator Lucreția
Titircă, Viața Medicală Românească Publishing House, Bucharest, 2013)
Programme - Official organised system or plan, which guides actions toward a specific goal.
(JCI 5th edition)
Physical protection - All measures aimed at preventing, identifying and responding to theft,
sabotage, unauthorised access, unauthorised activities related to nuclear and radiologic equipment,
nuclear materials and other sources of ionising radiation; (similar information/Law 182/art. 15, i): all
classified information security and protection activities, by physical check measures and devices and
technical means)
CARE PROTOCOL - A plan which identifies all patient’s care needs, lists the strategies used o
cover these needs, identifies treatment targets and objectives. The care plan specifies the criteria
against which certain interventions should be finalised and documents how the patient reaches the
targets during his/her care programme. The care plan relies on data collected during patient
evaluation. The care plan template may differ from one organisation to another. The plan is guided
SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 48
by specific practice guides, by protocols and combined guides and protocol, and by specific policies
and procedures.
Interventional Radiology - Performance of medical procedures (invasive and minimum
invasive, intraoperative) using imaging technologies for guidance. Practitioners may be radiologists
or clinicians of various specialties (cardiology, urology, orthopedics, vascular surgery, general
surgery, neurosurgery, thoracic surgery, pediatric surgery). Equipment used in interventional
radiology: angiography equipment, C-arm fluoroscopy equipment, extracorporeal lithotriptor,
dedicated imaging equipment for intraoperative ultrasound explorations. Hybrid imaging systems
(PET-CT or PET - MR) may only be used by physicians with both specialties, Radiology/ Medical
Imaging licensed for CT or MRI and Nuclear Medicine
Duty - Duty and obligation to undertake tasks or activities. This duty cannot be delegated and
it should be transparent for all parties involved.
Responsiveness - Being able to offer respect to others, customer-orientation, encourage the
customer to participate and obtain customer agreement. A dimension of quality.
Recruitment and Selection - Processes used to attract, select and appoint personnel and
evaluators.
Public recognition - Independent external public recognition/acknowledgement.
Results - Consequences of an action, operation, service or intervention.
Risk - Likelihood or possibility that danger, loss or prejudice should occur. This may be related
to staff and public health and welfare, to property, reputation, organisation’s operation
environment, financial stability, market share and other valuables.
Risk related to medical care in the hospital - Likelihood of prejudice generated while the
patient is within hospital premises with other causes than those related to nursing or healthcare
Clinical risk - Likelihood of prejudice generated by a medical diagnostic or therapeutic
intervention or due to inaccurate appraisal of patient condition and needs
Infectious risk - Likelihood of prejudice as a consequence of major epidemiologic factors
(microorganism, microorganism, environmental factors) and of secondary factors (climate, social
factors) leading to possible biologic contamination. Treating physicians identify infectious risk
patients and take action to limit the risk.
Scalability - Scalability of a data processing system consists in its capacity of similar behaviour,
without faults, when the volume of data processed increases and/or when it is capable to provide
better results with additional resources (usually, hardware)
Goals - General statements describing the results an organisation wants and providing the
necessary guidelines for daily activities and decisions. Goals support the organisation’s mission.
Dependency score - Score obtained after an evaluation of basic deficit needs to determine the
patient’s dependency level.
Nuclear security - All technical and organisational measures to ensure smooth operation of
nuclear equipment, to prevent and limit its damage and ensure protection of personnel subject to
professional exposure, of population, environment and assets against exposure to ionising radiation
or radioactive contamination exceeding the limits allowed by the legislation in force;
Services - Action serving or benefiting someone; work delivered for or to somebody’s interest.
The American Marketing Association defines services as: activity offered for sale, which
provides advantages and satisfaction without entailing a physical exchange in the form of goods.
49 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
Safety - Trust that potential risks are avoided and unintentional results are avoided or
minimised.
Nuclear safety - All physical protection and nuclear guarantee control measures.
A set of technical and organisational measures to:
- Ensure safe operation of nuclear equipment;
- Prevent and limit their damage;
- Ensure personnel, public and environmental protection against radiation of radioactive
contamination
Nurse call - Central system whereby any patient may ask medical personnel assistance when
he/she needs help
Medical staff alert in case of major emergencies - Alert system used by medical staff to alert
emergency intervention team (UPU sau ATI)
Document control system - A planned system to check how important documents, especially
policies and procedures, are issued, amended and used within the organisation. The system needs
each document to have a unique identification, to include the date of issuance, updates and
authorisation. Issuance of documents within the organisation is controlled and all copies of each
document are accessible and can be tracked. Use of outdated documents is prevented.
Security system - Integrated set of organisational, technical and procedural actions aiming at
securing physical security for an organisation or facility;
Information systems - Electronic and manual data and information planning, organisation,
analysis and control systems.
IT system - It may defined as the set of data, information, information flows and circuits,
information processing procedures and means designed to contribute to setting and achieving the
objectives of the organisation.
Stakeholder - Individuals, organisations or groups which have an interest or participate in a
service. Shareholders or members of the management board of an organisation.
Standard - Desired and achievable level of performance used to measure current
performance.
Strategy - Long-term management document designed to set objectives and plan the course
of action to be implemented.
GOVERNANCE STRUCTURE - It may vary from one hospital to another. Usually this category
includes: hospital owners (in case of private hospitals), a group of persons supervising how the
hospital is managed, responsible for high quality healthcare service provision (JCI)
Nursing research surveys - For the purposes of this document, nursing research surveys are
research undertaken in the hospital where in which nurses were involved in cooperation with
University research departments; for development of Bachelor, Master’s or PhD thesis; for
development of specialist books, articles or papers presented in scientific events.
Sustainability - Quality of anthropic activity to unfold without exhausting available resources,
therefore without compromising possibilities to satisfy future needs. At macroeconomic level, it
entails a balance between growth and available resources (including identification of alternative
resources).
From the standards perspective, it is the extent to which a healthcare system provides
infrastructure, workforce, facilities and equipment, innovation and responsiveness to emerging
50 SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS)
needs, e.g. research, monitoring. It is a dimension of quality.
Dashboard - An instrument including overall information on the activities to be undertaken
Medical technology - (WHO definition) “devices, medicines, medical and surgical procedures –
and related knowledge – used in the prevention, diagnosis, treatment of infections, rehabilitation
and organisational support systems providing healthcare”
Validity - Relation between data obtained and the purpose for which they were requested or
extent to which they reflect what they intend to measure.
Values - Principles, beliefs or philosophies guiding behaviour which may involve social or
ethical issues.
Performance review - Continuous process whereby a manager and another staff member
review staff performance, set performance objectives and evaluate progress made to achieve them.
Vision - Describes what the organisation wants to be.
Vulnerability - Characteristic acquired, with or without intention, by a person, facility, values
etc., which may be used or may deliberately or unconsciously lead to prejudice against that entity.

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 51

SELF-ASSESSMENT GUIDELINES FOR USERS (HOSPITALS) 52
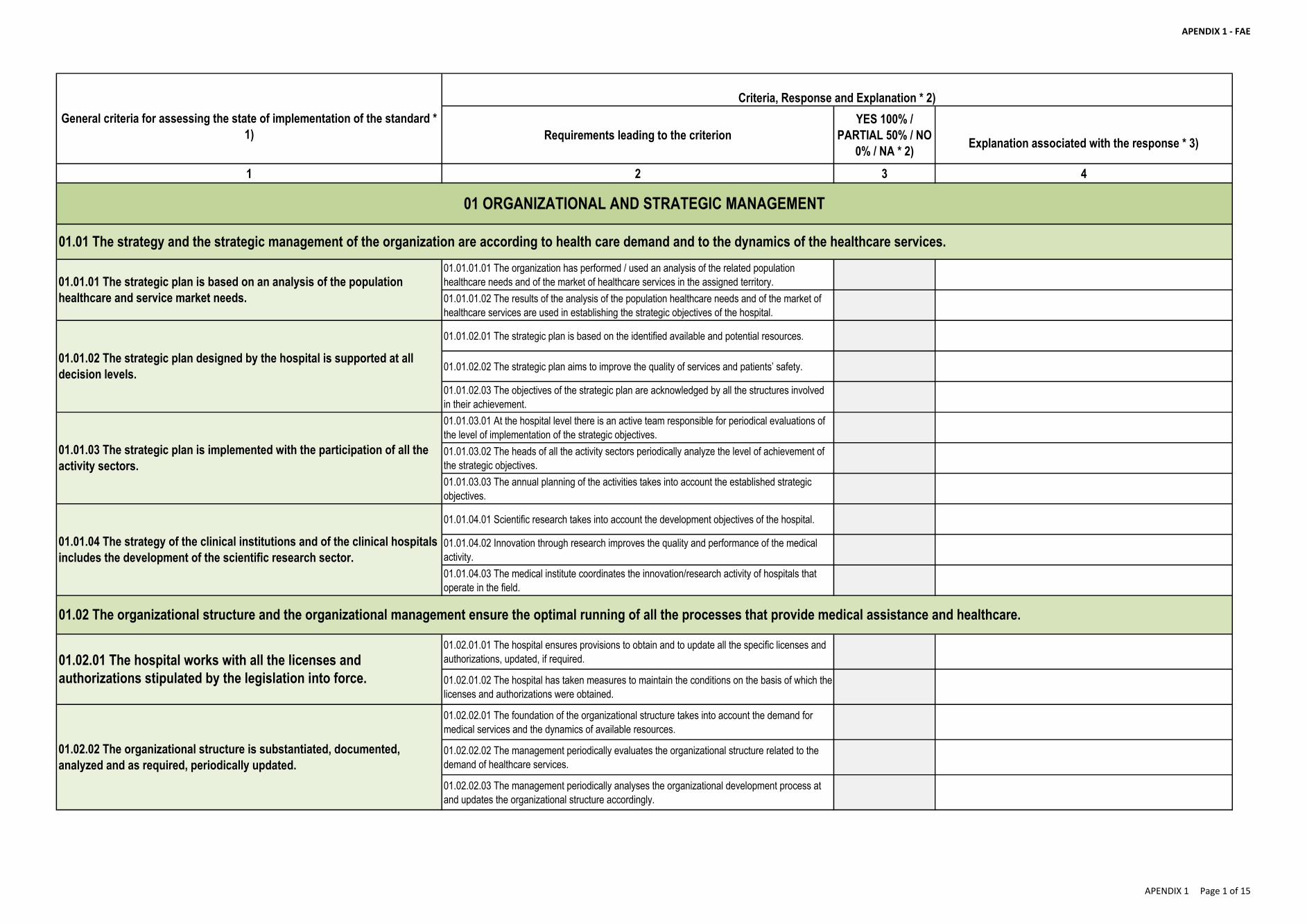
APENDIX 1 - FAE
Requirements leading to the criterion
YES 100% /
PARTIAL 50% / NO
0% / NA * 2)Explanation associated with the response * 3)
1 2 3 4
01.01.01.01 The organization has performed / used an analysis of the related population
healthcare needs and of the market of healthcare services in the assigned territory.
01.01.01.02 The results of the analysis of the population healthcare needs and of the market of
healthcare services are used in establishing the strategic objectives of the hospital.
01.01.02.01 The strategic plan is based on the identified available and potential resources.
01.01.02.02 The strategic plan aims to improve the quality of services and patients’ safety.
01.01.02.03 The objectives of the strategic plan are acknowledged by all the structures involved
in their achievement.
01.01.03.01 At the hospital level there is an active team responsible for periodical evaluations of
the level of implementation of the strategic objectives.
01.01.03.02 The heads of all the activity sectors periodically analyze the level of achievement of
the strategic objectives.
01.01.03.03 The annual planning of the activities takes into account the established strategic
objectives.
01.01.04.01 Scientific research takes into account the development objectives of the hospital.
01.01.04.02 Innovation through research improves the quality and performance of the medical
activity.
01.01.04.03 The medical institute coordinates the innovation/research activity of hospitals that
operate in the field.
01.02.01.01 The hospital ensures provisions to obtain and to update all the specific licenses and
authorizations, updated, if required.
01.02.01.02 The hospital has taken measures to maintain the conditions on the basis of which the
licenses and authorizations were obtained.
01.02.02.01 The foundation of the organizational structure takes into account the demand for
medical services and the dynamics of available resources.
01.02.02.02 The management periodically evaluates the organizational structure related to the
demand of healthcare services.
01.02.02.03 The management periodically analyses the organizational development process at
and updates the organizational structure accordingly.
01.02.02 The organizational structure is substantiated, documented,
analyzed and as required, periodically updated.
01.02.01 The hospital works with all the licenses and
authorizations stipulated by the legislation into force.
01.01.01 The strategic plan is based on an analysis of the population
healthcare and service market needs.
01.01.02 The strategic plan designed by the hospital is supported at all
decision levels.
01.01.03 The strategic plan is implemented with the participation of all the
activity sectors.
01.01.04 The strategy of the clinical institutions and of the clinical hospitals
includes the development of the scientific research sector.
01.01 The strategy and the strategic management of the organization are according to health care demand and to the dynamics of the healthcare services.
01 ORGANIZATIONAL AND STRATEGIC MANAGEMENT
Criteria, Response and Explanation * 2)
General criteria for assessing the state of implementation of the standard *
1)
01.02 The organizational structure and the organizational management ensure the optimal running of all the processes that provide medical assistance and healthcare.
APENDIX 1 Page 1 of 15
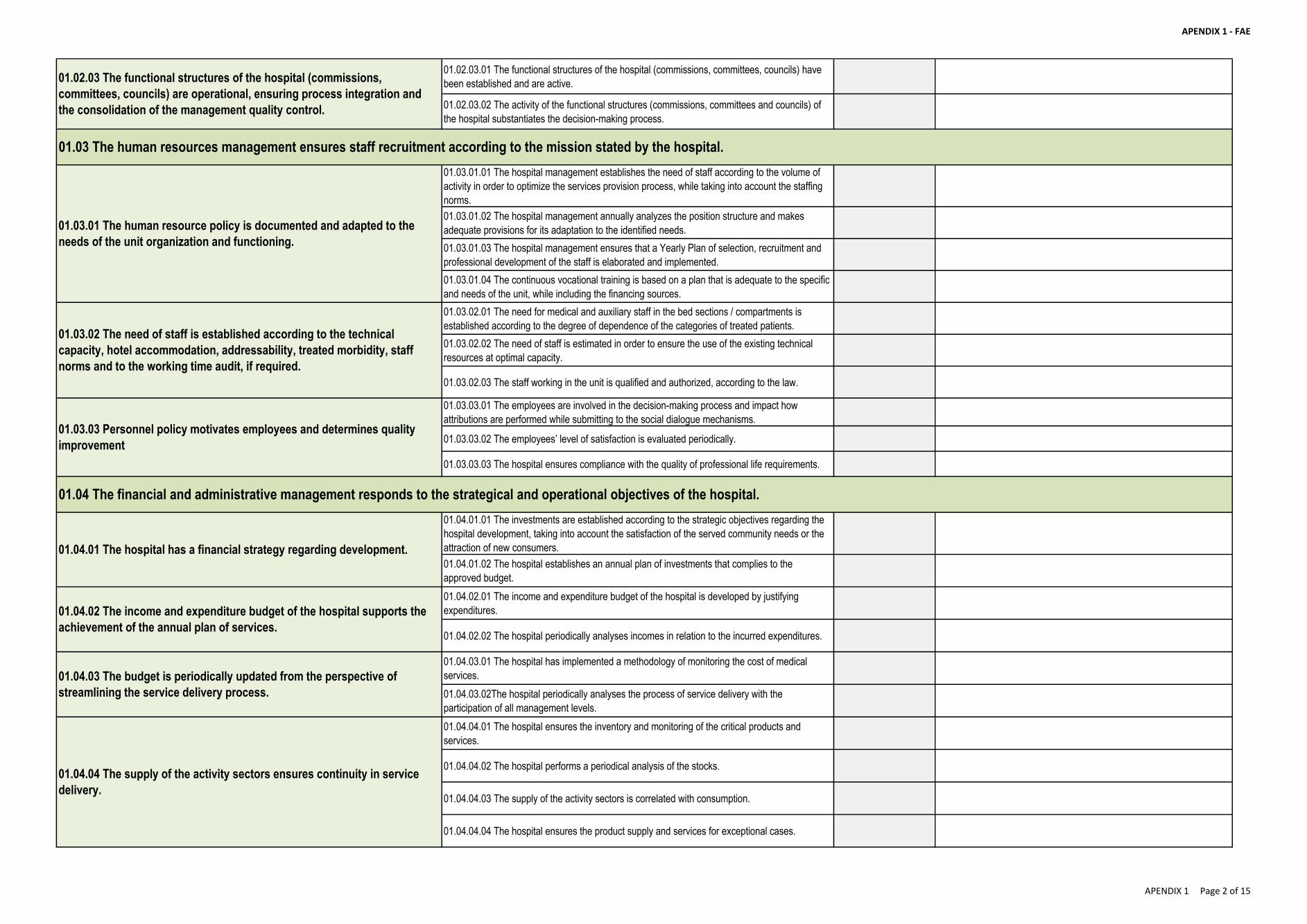
APENDIX 1 - FAE
01.02.03.01 The functional structures of the hospital (commissions, committees, councils) have
been established and are active.
01.02.03.02 The activity of the functional structures (commissions, committees and councils) of
the hospital substantiates the decision-making process.
01.03.01.01 The hospital management establishes the need of staff according to the volume of
activity in order to optimize the services provision process, while taking into account the staffing
norms.
01.03.01.02 The hospital management annually analyzes the position structure and makes
adequate provisions for its adaptation to the identified needs.
01.03.01.03 The hospital management ensures that a Yearly Plan of selection, recruitment and
professional development of the staff is elaborated and implemented.
01.03.01.04 The continuous vocational training is based on a plan that is adequate to the specific
and needs of the unit, while including the financing sources.
01.03.02.01 The need for medical and auxiliary staff in the bed sections / compartments is
established according to the degree of dependence of the categories of treated patients.
01.03.02.02 The need of staff is estimated in order to ensure the use of the existing technical
resources at optimal capacity.
01.03.02.03 The staff working in the unit is qualified and authorized, according to the law.
01.03.03.01 The employees are involved in the decision-making process and impact how
attributions are performed while submitting to the social dialogue mechanisms.
01.03.03.02 The employees’ level of satisfaction is evaluated periodically.
01.03.03.03 The hospital ensures compliance with the quality of professional life requirements.
01.04.01.01 The investments are established according to the strategic objectives regarding the
hospital development, taking into account the satisfaction of the served community needs or the
attraction of new consumers.
01.04.01.02 The hospital establishes an annual plan of investments that complies to the
approved budget.
01.04.02.01 The income and expenditure budget of the hospital is developed by justifying
expenditures.
01.04.02.02 The hospital periodically analyses incomes in relation to the incurred expenditures.
01.04.03.01 The hospital has implemented a methodology of monitoring the cost of medical
services.
01.04.03.02The hospital periodically analyses the process of service delivery with the
participation of all management levels.
01.04.04.01 The hospital ensures the inventory and monitoring of the critical products and
services.
01.04.04.02 The hospital performs a periodical analysis of the stocks.
01.04.04.03 The supply of the activity sectors is correlated with consumption.
01.04.04.04 The hospital ensures the product supply and services for exceptional cases.
01.02.03 The functional structures of the hospital (commissions,
committees, councils) are operational, ensuring process integration and
the consolidation of the management quality control.
01.04 The financial and administrative management responds to the strategical and operational objectives of the hospital.
01.03 The human resources management ensures staff recruitment according to the mission stated by the hospital.
01.03.01 The human resource policy is documented and adapted to the
needs of the unit organization and functioning.
01.03.02 The need of staff is established according to the technical
capacity, hotel accommodation, addressability, treated morbidity, staff
norms and to the working time audit, if required.
01.03.03 Personnel policy motivates employees and determines quality
improvement
01.04.01 The hospital has a financial strategy regarding development.
01.04.02 The income and expenditure budget of the hospital supports the
achievement of the annual plan of services.
01.04.03 The budget is periodically updated from the perspective of
streamlining the service delivery process.
01.04.04 The supply of the activity sectors ensures continuity in service
delivery.
APENDIX 1 Page 2 of 15
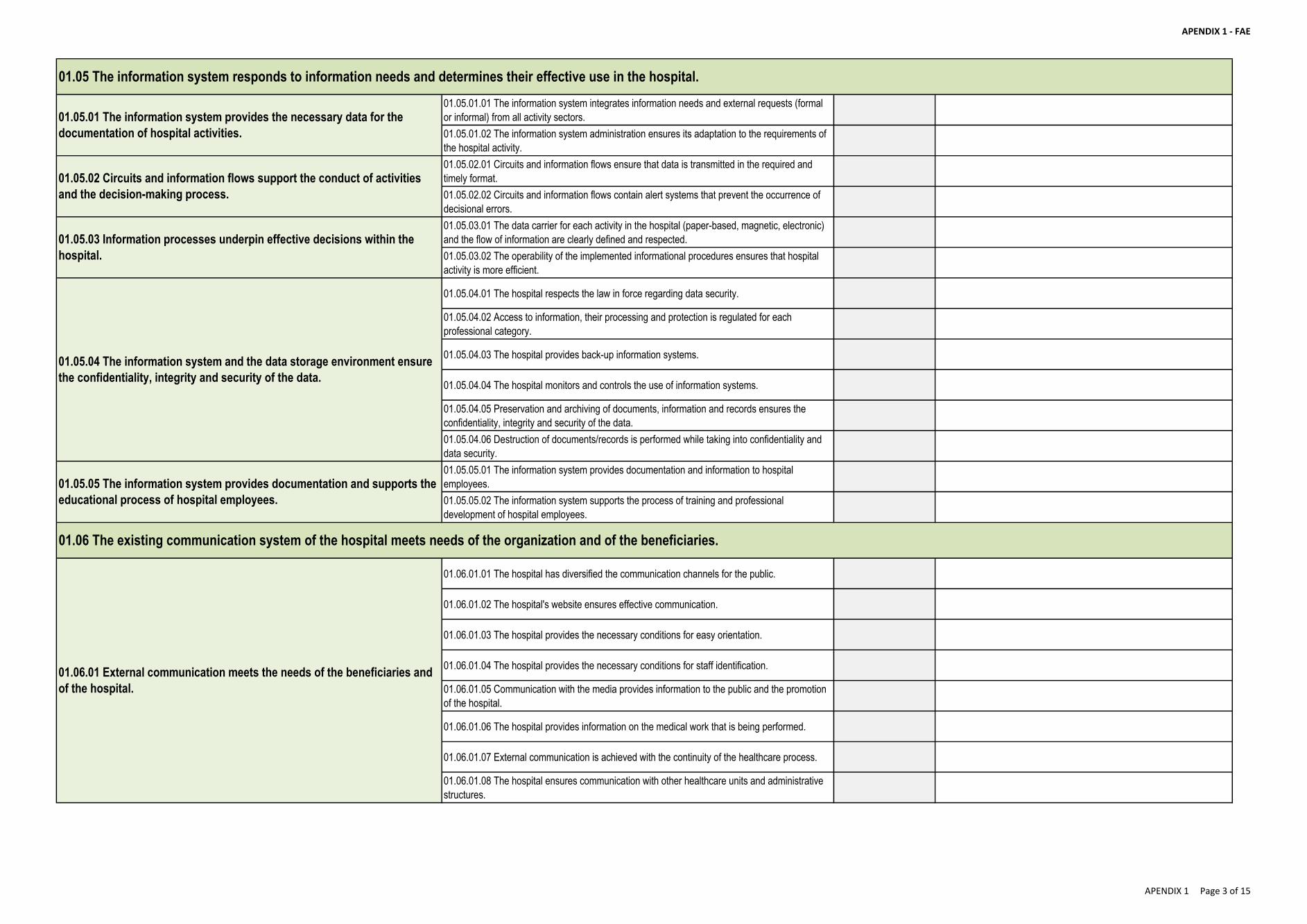
APENDIX 1 - FAE
01.05.01.01 The information system integrates information needs and external requests (formal
or informal) from all activity sectors.
01.05.01.02 The information system administration ensures its adaptation to the requirements of
the hospital activity.
01.05.02.01 Circuits and information flows ensure that data is transmitted in the required and
timely format.
01.05.02.02 Circuits and information flows contain alert systems that prevent the occurrence of
decisional errors.
01.05.03.01 The data carrier for each activity in the hospital (paper-based, magnetic, electronic)
and the flow of information are clearly defined and respected.
01.05.03.02 The operability of the implemented informational procedures ensures that hospital
activity is more efficient.
01.05.04.01 The hospital respects the law in force regarding data security.
01.05.04.02 Access to information, their processing and protection is regulated for each
professional category.
01.05.04.03 The hospital provides back-up information systems.
01.05.04.04 The hospital monitors and controls the use of information systems.
01.05.04.05 Preservation and archiving of documents, information and records ensures the
confidentiality, integrity and security of the data.
01.05.04.06 Destruction of documents/records is performed while taking into confidentiality and
data security.
01.05.05.01 The information system provides documentation and information to hospital
employees.
01.05.05.02 The information system supports the process of training and professional
development of hospital employees.
01.06.01.01 The hospital has diversified the communication channels for the public.
01.06.01.02 The hospital's website ensures effective communication.
01.06.01.03 The hospital provides the necessary conditions for easy orientation.
01.06.01.04 The hospital provides the necessary conditions for staff identification.
01.06.01.05 Communication with the media provides information to the public and the promotion
of the hospital.
01.06.01.06 The hospital provides information on the medical work that is being performed.
01.06.01.07 External communication is achieved with the continuity of the healthcare process.
01.06.01.08 The hospital ensures communication with other healthcare units and administrative
structures.
01.06 The existing communication system of the hospital meets needs of the organization and of the beneficiaries.
01.05.05 The information system provides documentation and supports the
educational process of hospital employees.
01.06.01 External communication meets the needs of the beneficiaries and
of the hospital.
01.05 The information system responds to information needs and determines their effective use in the hospital.
01.05.04 The information system and the data storage environment ensure
the confidentiality, integrity and security of the data.
01.05.01 The information system provides the necessary data for the
documentation of hospital activities.
01.05.02 Circuits and information flows support the conduct of activities
and the decision-making process.
01.05.03 Information processes underpin effective decisions within the
hospital.
APENDIX 1 Page 3 of 15
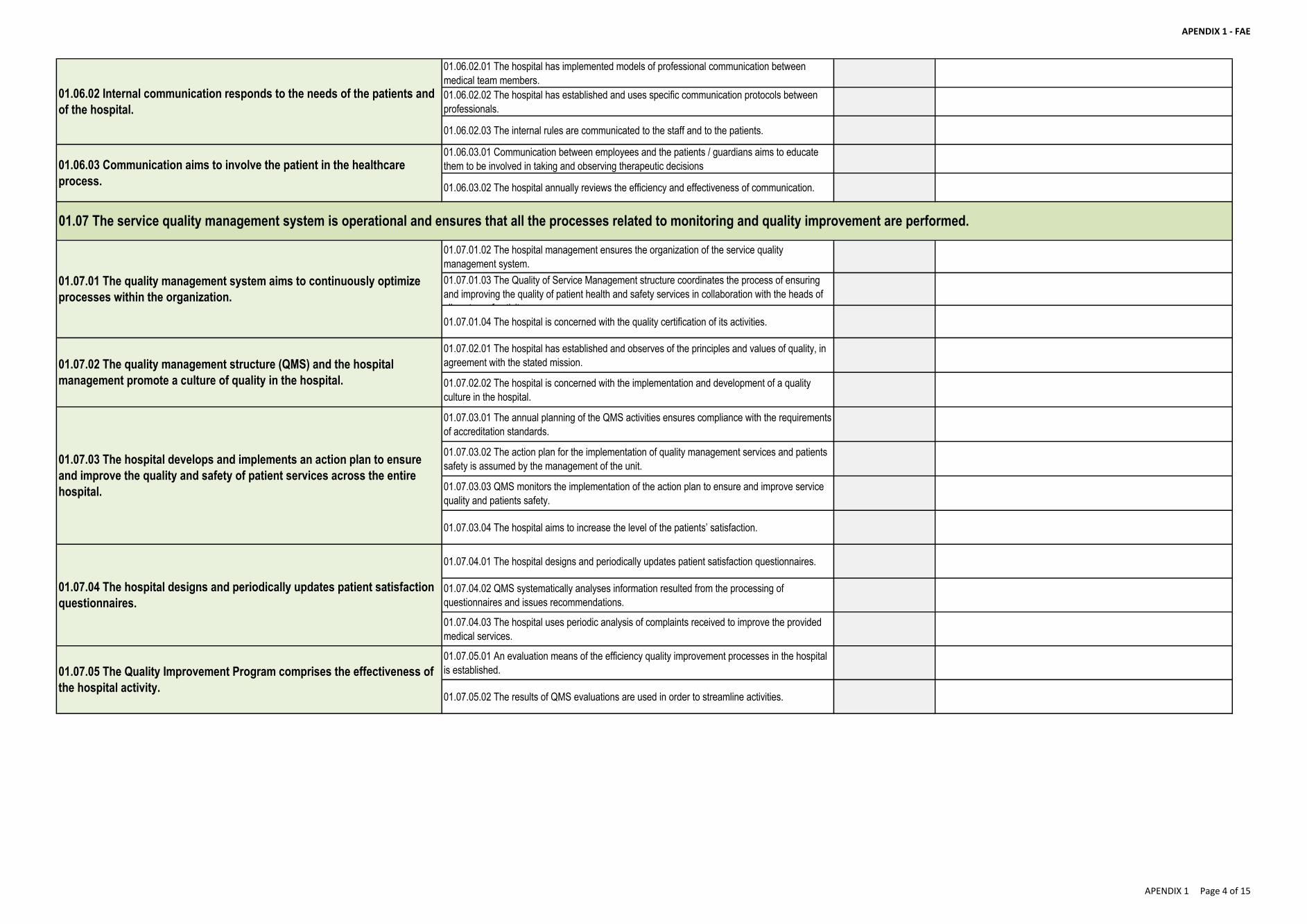
APENDIX 1 - FAE
01.06.02.01 The hospital has implemented models of professional communication between
medical team members.
01.06.02.02 The hospital has established and uses specific communication protocols between
professionals.
01.06.02.03 The internal rules are communicated to the staff and to the patients.
01.06.03.01 Communication between employees and the patients / guardians aims to educate
them to be involved in taking and observing therapeutic decisions
01.06.03.02 The hospital annually reviews the efficiency and effectiveness of communication.
01.07.01.02 The hospital management ensures the organization of the service quality
management system.
01.07.01.03 The Quality of Service Management structure coordinates the process of ensuring
and improving the quality of patient health and safety services in collaboration with the heads of
all sectors of activity.
01.07.01.04 The hospital is concerned with the quality certification of its activities.
01.07.02.01 The hospital has established and observes of the principles and values of quality, in
agreement with the stated mission.
01.07.02.02 The hospital is concerned with the implementation and development of a quality
culture in the hospital.
01.07.03.01 The annual planning of the QMS activities ensures compliance with the requirements
of accreditation standards.
01.07.03.02 The action plan for the implementation of quality management services and patients
safety is assumed by the management of the unit.
01.07.03.03 QMS monitors the implementation of the action plan to ensure and improve service
quality and patients safety.
01.07.03.04 The hospital aims to increase the level of the patients’ satisfaction.
01.07.04.01 The hospital designs and periodically updates patient satisfaction questionnaires.
01.07.04.02 QMS systematically analyses information resulted from the processing of
questionnaires and issues recommendations.
01.07.04.03 The hospital uses periodic analysis of complaints received to improve the provided
medical services.
01.07.05.01 An evaluation means of the efficiency quality improvement processes in the hospital
is established.
01.07.05.02 The results of QMS evaluations are used in order to streamline activities.
01.07.01 The quality management system aims to continuously optimize
processes within the organization.
01.07.02 The quality management structure (QMS) and the hospital
management promote a culture of quality in the hospital.
01.06.02 Internal communication responds to the needs of the patients and
of the hospital.
01.06.03 Communication aims to involve the patient in the healthcare
process.
01.07.03 The hospital develops and implements an action plan to ensure
and improve the quality and safety of patient services across the entire
hospital.
01.07.04 The hospital designs and periodically updates patient satisfaction
questionnaires.
01.07.05 The Quality Improvement Program comprises the effectiveness of
the hospital activity.
01.07 The service quality management system is operational and ensures that all the processes related to monitoring and quality improvement are performed.
APENDIX 1 Page 4 of 15
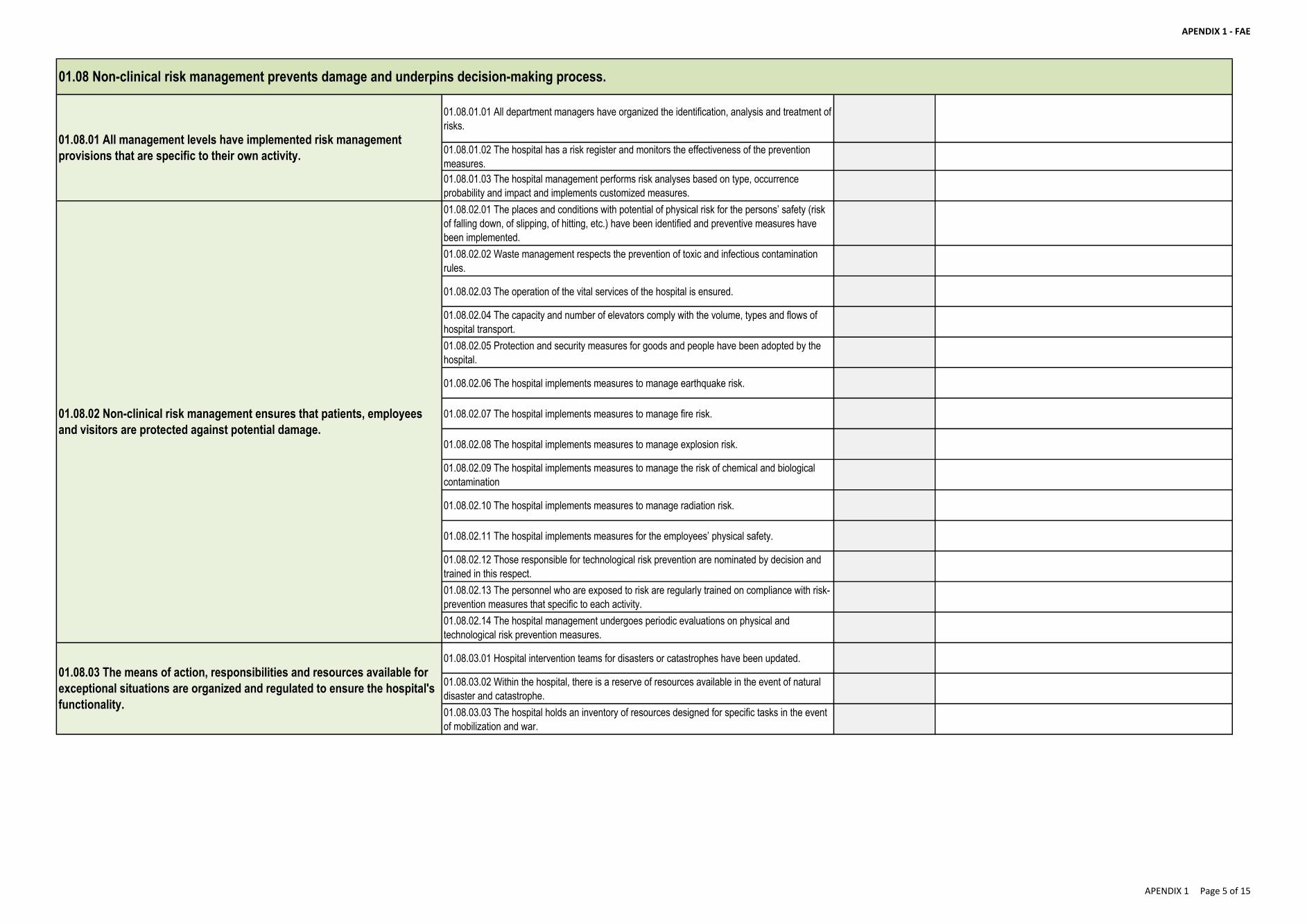
APENDIX 1 - FAE
01.08.01.01 All department managers have organized the identification, analysis and treatment of
risks.
01.08.01.02 The hospital has a risk register and monitors the effectiveness of the prevention
measures.
01.08.01.03 The hospital management performs risk analyses based on type, occurrence
probability and impact and implements customized measures.
01.08.02.01 The places and conditions with potential of physical risk for the persons’ safety (risk
of falling down, of slipping, of hitting, etc.) have been identified and preventive measures have
been implemented.
01.08.02.02 Waste management respects the prevention of toxic and infectious contamination
rules.
01.08.02.03 The operation of the vital services of the hospital is ensured.
01.08.02.04 The capacity and number of elevators comply with the volume, types and flows of
hospital transport.
01.08.02.05 Protection and security measures for goods and people have been adopted by the
hospital.
01.08.02.06 The hospital implements measures to manage earthquake risk.
01.08.02.07 The hospital implements measures to manage fire risk.
01.08.02.08 The hospital implements measures to manage explosion risk.
01.08.02.09 The hospital implements measures to manage the risk of chemical and biological
contamination
01.08.02.10 The hospital implements measures to manage radiation risk.
01.08.02.11 The hospital implements measures for the employees’ physical safety.
01.08.02.12 Those responsible for technological risk prevention are nominated by decision and
trained in this respect.
01.08.02.13 The personnel who are exposed to risk are regularly trained on compliance with risk-
prevention measures that specific to each activity.
01.08.02.14 The hospital management undergoes periodic evaluations on physical and
technological risk prevention measures.
01.08.03.01 Hospital intervention teams for disasters or catastrophes have been updated.
01.08.03.02 Within the hospital, there is a reserve of resources available in the event of natural
disaster and catastrophe.
01.08.03.03 The hospital holds an inventory of resources designed for specific tasks in the event
of mobilization and war.
01.08.01 All management levels have implemented risk management
provisions that are specific to their own activity.
01.08.02 Non-clinical risk management ensures that patients, employees
and visitors are protected against potential damage.
01.08.03 The means of action, responsibilities and resources available for
exceptional situations are organized and regulated to ensure the hospital's
functionality.
01.08 Non-clinical risk management prevents damage and underpins decision-making process.
APENDIX 1 Page 5 of 15
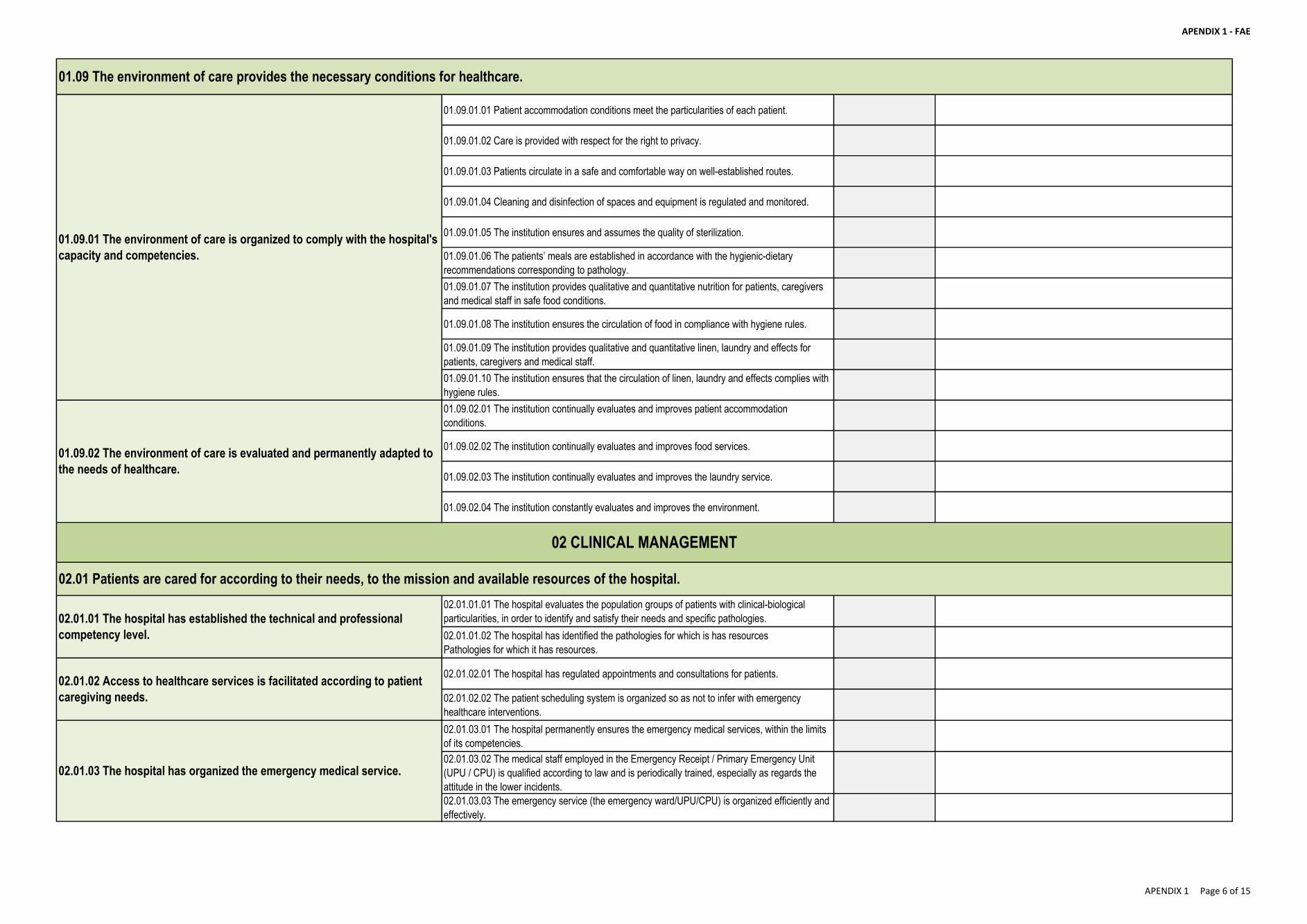
APENDIX 1 - FAE
01.09.01.01 Patient accommodation conditions meet the particularities of each patient.
01.09.01.02 Care is provided with respect for the right to privacy.
01.09.01.03 Patients circulate in a safe and comfortable way on well-established routes.
01.09.01.04 Cleaning and disinfection of spaces and equipment is regulated and monitored.
01.09.01.05 The institution ensures and assumes the quality of sterilization.
01.09.01.06 The patients’ meals are established in accordance with the hygienic-dietary
recommendations corresponding to pathology.
01.09.01.07 The institution provides qualitative and quantitative nutrition for patients, caregivers
and medical staff in safe food conditions.
01.09.01.08 The institution ensures the circulation of food in compliance with hygiene rules.
01.09.01.09 The institution provides qualitative and quantitative linen, laundry and effects for
patients, caregivers and medical staff.
01.09.01.10 The institution ensures that the circulation of linen, laundry and effects complies with
hygiene rules.
01.09.02.01 The institution continually evaluates and improves patient accommodation
conditions.
01.09.02.02 The institution continually evaluates and improves food services.
01.09.02.03 The institution continually evaluates and improves the laundry service.
01.09.02.04 The institution constantly evaluates and improves the environment.
02.01.01.01 The hospital evaluates the population groups of patients with clinical-biological
particularities, in order to identify and satisfy their needs and specific pathologies.
02.01.01.02 The hospital has identified the pathologies for which is has resources
Pathologies for which it has resources.
02.01.02.01 The hospital has regulated appointments and consultations for patients.
02.01.02.02 The patient scheduling system is organized so as not to infer with emergency
healthcare interventions.
02.01.03.01 The hospital permanently ensures the emergency medical services, within the limits
of its competencies.
02.01.03.02 The medical staff employed in the Emergency Receipt / Primary Emergency Unit
(UPU / CPU) is qualified according to law and is periodically trained, especially as regards the
attitude in the lower incidents.
02.01.03.03 The emergency service (the emergency ward/UPU/CPU) is organized efficiently and
effectively.
01.09 The environment of care provides the necessary conditions for healthcare.
02 CLINICAL MANAGEMENT
02.01 Patients are cared for according to their needs, to the mission and available resources of the hospital.
01.09.02 The environment of care is evaluated and permanently adapted to
the needs of healthcare.
02.01.01 The hospital has established the technical and professional
competency level.
02.01.02 Access to healthcare services is facilitated according to patient
caregiving needs.
02.01.03 The hospital has organized the emergency medical service.
01.09.01 The environment of care is organized to comply with the hospital's
capacity and competencies.
APENDIX 1 Page 6 of 15
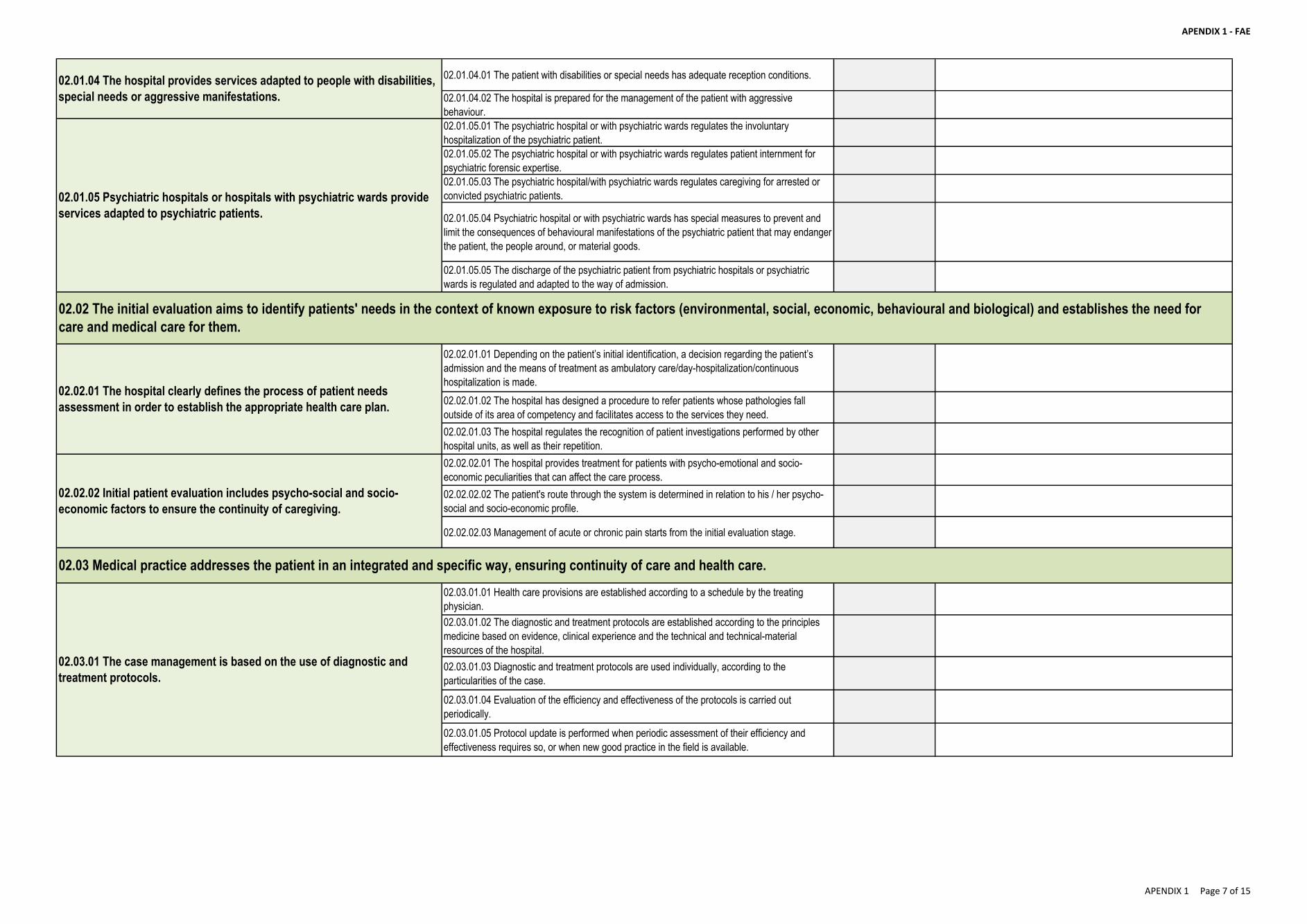
APENDIX 1 - FAE
02.01.04.01 The patient with disabilities or special needs has adequate reception conditions.
02.01.04.02 The hospital is prepared for the management of the patient with aggressive
behaviour.
02.01.05.01 The psychiatric hospital or with psychiatric wards regulates the involuntary
hospitalization of the psychiatric patient.
02.01.05.02 The psychiatric hospital or with psychiatric wards regulates patient internment for
psychiatric forensic expertise.
02.01.05.03 The psychiatric hospital/with psychiatric wards regulates caregiving for arrested or
convicted psychiatric patients.
02.01.05.04 Psychiatric hospital or with psychiatric wards has special measures to prevent and
limit the consequences of behavioural manifestations of the psychiatric patient that may endanger
the patient, the people around, or material goods.
02.01.05.05 The discharge of the psychiatric patient from psychiatric hospitals or psychiatric
wards is regulated and adapted to the way of admission.
02.02.01.01 Depending on the patient’s initial identification, a decision regarding the patient’s
admission and the means of treatment as ambulatory care/day-hospitalization/continuous
hospitalization is made.
02.02.01.02 The hospital has designed a procedure to refer patients whose pathologies fall
outside of its area of competency and facilitates access to the services they need.
02.02.01.03 The hospital regulates the recognition of patient investigations performed by other
hospital units, as well as their repetition.
02.02.02.01 The hospital provides treatment for patients with psycho-emotional and socio-
economic peculiarities that can affect the care process.
02.02.02.02 The patient's route through the system is determined in relation to his / her psycho-
social and socio-economic profile.
02.02.02.03 Management of acute or chronic pain starts from the initial evaluation stage.
02.03.01.01 Health care provisions are established according to a schedule by the treating
physician.
02.03.01.02 The diagnostic and treatment protocols are established according to the principles
medicine based on evidence, clinical experience and the technical and technical-material
resources of the hospital.
02.03.01.03 Diagnostic and treatment protocols are used individually, according to the
particularities of the case.
02.03.01.04 Evaluation of the efficiency and effectiveness of the protocols is carried out
periodically.
02.03.01.05 Protocol update is performed when periodic assessment of their efficiency and
effectiveness requires so, or when new good practice in the field is available.
02.03.01 The case management is based on the use of diagnostic and
treatment protocols.
02.01.04 The hospital provides services adapted to people with disabilities,
special needs or aggressive manifestations.
02.01.05 Psychiatric hospitals or hospitals with psychiatric wards provide
services adapted to psychiatric patients.
02.02.01 The hospital clearly defines the process of patient needs
assessment in order to establish the appropriate health care plan.
02.02.02 Initial patient evaluation includes psycho-social and socio-
economic factors to ensure the continuity of caregiving.
02.03 Medical practice addresses the patient in an integrated and specific way, ensuring continuity of care and health care.
02.02 The initial evaluation aims to identify patients' needs in the context of known exposure to risk factors (environmental, social, economic, behavioural and biological) and establishes the need for
care and medical care for them.
APENDIX 1 Page 7 of 15
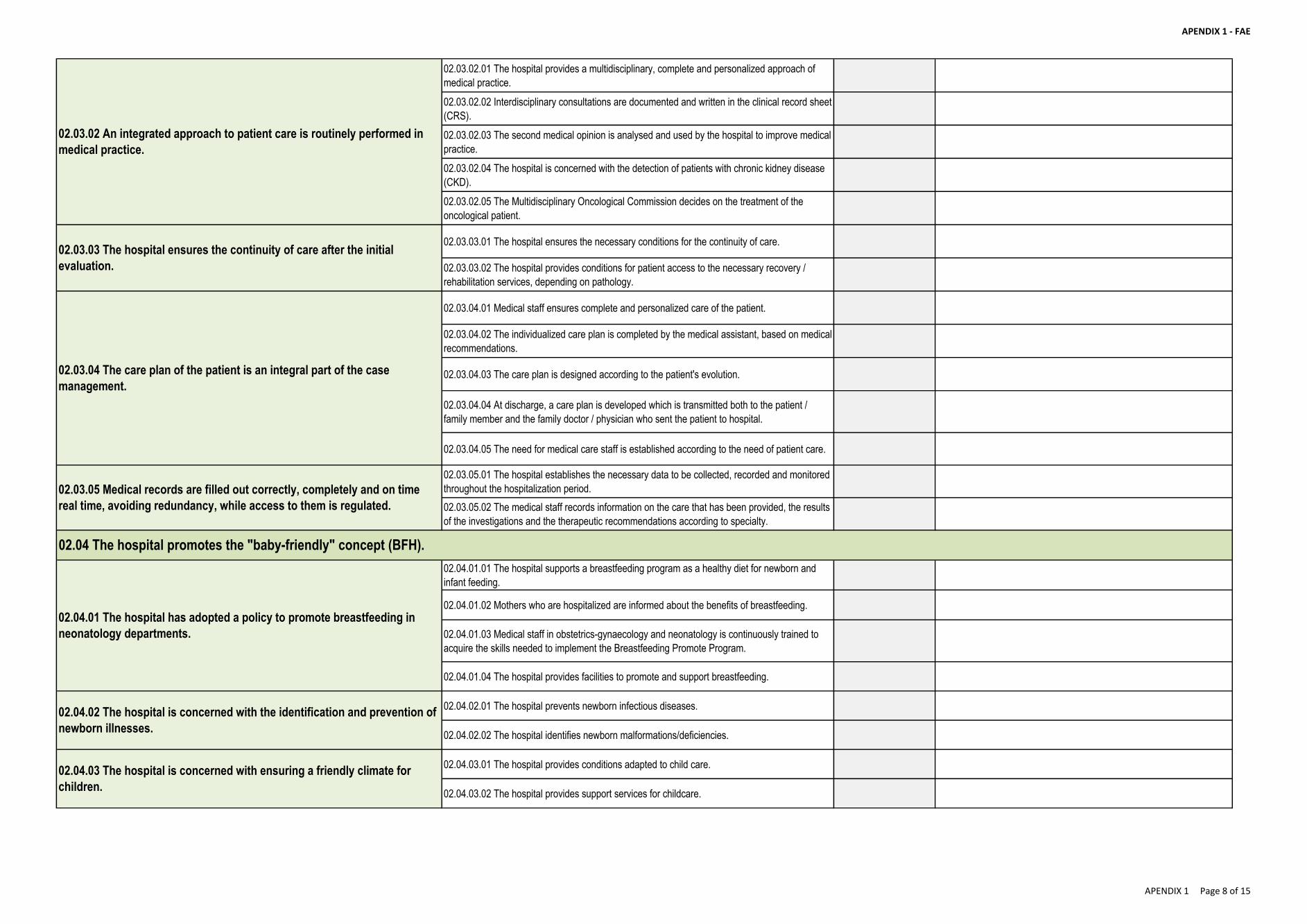
APENDIX 1 - FAE
02.03.02.01 The hospital provides a multidisciplinary, complete and personalized approach of
medical practice.
02.03.02.02 Interdisciplinary consultations are documented and written in the clinical record sheet
(CRS).
02.03.02.03 The second medical opinion is analysed and used by the hospital to improve medical
practice.
02.03.02.04 The hospital is concerned with the detection of patients with chronic kidney disease
(CKD).
02.03.02.05 The Multidisciplinary Oncological Commission decides on the treatment of the
oncological patient.
02.03.03.01 The hospital ensures the necessary conditions for the continuity of care.
02.03.03.02 The hospital provides conditions for patient access to the necessary recovery /
rehabilitation services, depending on pathology.
02.03.04.01 Medical staff ensures complete and personalized care of the patient.
02.03.04.02 The individualized care plan is completed by the medical assistant, based on medical
recommendations.
02.03.04.03 The care plan is designed according to the patient's evolution.
02.03.04.04 At discharge, a care plan is developed which is transmitted both to the patient /
family member and the family doctor / physician who sent the patient to hospital.
02.03.04.05 The need for medical care staff is established according to the need of patient care.
02.03.05.01 The hospital establishes the necessary data to be collected, recorded and monitored
throughout the hospitalization period.
02.03.05.02 The medical staff records information on the care that has been provided, the results
of the investigations and the therapeutic recommendations according to specialty.
02.04.01.01 The hospital supports a breastfeeding program as a healthy diet for newborn and
infant feeding.
02.04.01.02 Mothers who are hospitalized are informed about the benefits of breastfeeding.
02.04.01.03 Medical staff in obstetrics-gynaecology and neonatology is continuously trained to
acquire the skills needed to implement the Breastfeeding Promote Program.
02.04.01.04 The hospital provides facilities to promote and support breastfeeding.
02.04.02.01 The hospital prevents newborn infectious diseases.
02.04.02.02 The hospital identifies newborn malformations/deficiencies.
02.04.03.01 The hospital provides conditions adapted to child care.
02.04.03.02 The hospital provides support services for childcare.
02.03.02 An integrated approach to patient care is routinely performed in
medical practice.
02.03.03 The hospital ensures the continuity of care after the initial
evaluation.
02.03.04 The care plan of the patient is an integral part of the case
management.
02.03.05 Medical records are filled out correctly, completely and on time
real time, avoiding redundancy, while access to them is regulated.
02.04.01 The hospital has adopted a policy to promote breastfeeding in
neonatology departments.
02.04.02 The hospital is concerned with the identification and prevention of
newborn illnesses.
02.04.03 The hospital is concerned with ensuring a friendly climate for
children.
02.04 The hospital promotes the "baby-friendly" concept (BFH).
APENDIX 1 Page 8 of 15
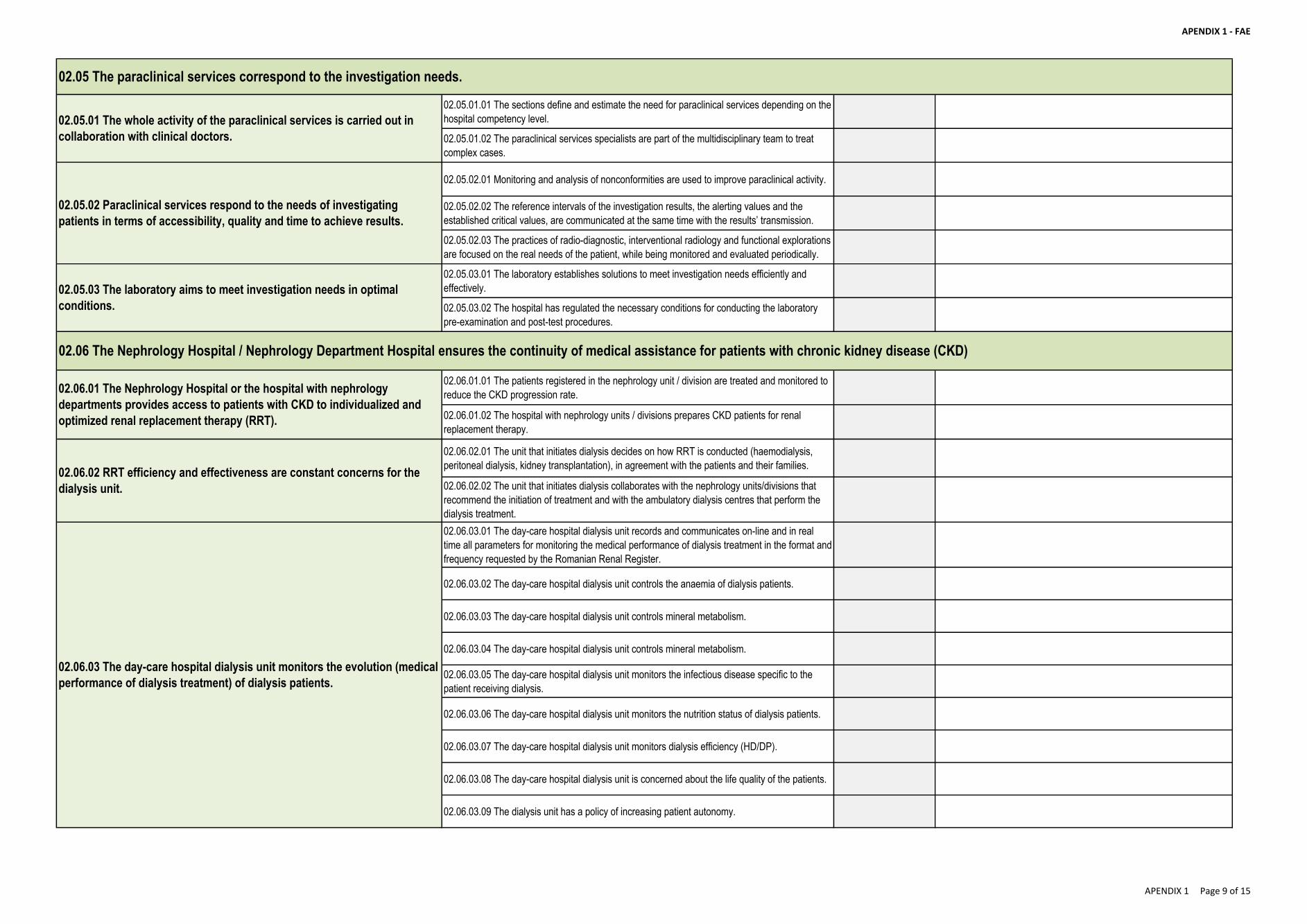
APENDIX 1 - FAE
02.05.01.01 The sections define and estimate the need for paraclinical services depending on the
hospital competency level.
02.05.01.02 The paraclinical services specialists are part of the multidisciplinary team to treat
complex cases.
02.05.02.01 Monitoring and analysis of nonconformities are used to improve paraclinical activity.
02.05.02.02 The reference intervals of the investigation results, the alerting values and the
established critical values, are communicated at the same time with the results’ transmission.
02.05.02.03 The practices of radio-diagnostic, interventional radiology and functional explorations
are focused on the real needs of the patient, while being monitored and evaluated periodically.
02.05.03.01 The laboratory establishes solutions to meet investigation needs efficiently and
effectively.
02.05.03.02 The hospital has regulated the necessary conditions for conducting the laboratory
pre-examination and post-test procedures.
02.06.01.01 The patients registered in the nephrology unit / division are treated and monitored to
reduce the CKD progression rate.
02.06.01.02 The hospital with nephrology units / divisions prepares CKD patients for renal
replacement therapy.
02.06.02.01 The unit that initiates dialysis decides on how RRT is conducted (haemodialysis,
peritoneal dialysis, kidney transplantation), in agreement with the patients and their families.
02.06.02.02 The unit that initiates dialysis collaborates with the nephrology units/divisions that
recommend the initiation of treatment and with the ambulatory dialysis centres that perform the
dialysis treatment.
02.06.03.01 The day-care hospital dialysis unit records and communicates on-line and in real
time all parameters for monitoring the medical performance of dialysis treatment in the format and
frequency requested by the Romanian Renal Register.
02.06.03.02 The day-care hospital dialysis unit controls the anaemia of dialysis patients.
02.06.03.03 The day-care hospital dialysis unit controls mineral metabolism.
02.06.03.04 The day-care hospital dialysis unit controls mineral metabolism.
02.06.03.05 The day-care hospital dialysis unit monitors the infectious disease specific to the
patient receiving dialysis.
02.06.03.06 The day-care hospital dialysis unit monitors the nutrition status of dialysis patients.
02.06.03.07 The day-care hospital dialysis unit monitors dialysis efficiency (HD/DP).
02.06.03.08 The day-care hospital dialysis unit is concerned about the life quality of the patients.
02.06.03.09 The dialysis unit has a policy of increasing patient autonomy.
02.05 The paraclinical services correspond to the investigation needs.
02.05.03 The laboratory aims to meet investigation needs in optimal
conditions.
02.06.01 The Nephrology Hospital or the hospital with nephrology
departments provides access to patients with CKD to individualized and
optimized renal replacement therapy (RRT).
02.06.02 RRT efficiency and effectiveness are constant concerns for the
dialysis unit.
02.06.03 The day-care hospital dialysis unit monitors the evolution (medical
performance of dialysis treatment) of dialysis patients.
02.05.01 The whole activity of the paraclinical services is carried out in
collaboration with clinical doctors.
02.05.02 Paraclinical services respond to the needs of investigating
patients in terms of accessibility, quality and time to achieve results.
02.06 The Nephrology Hospital / Nephrology Department Hospital ensures the continuity of medical assistance for patients with chronic kidney disease (CKD)
APENDIX 1 Page 9 of 15
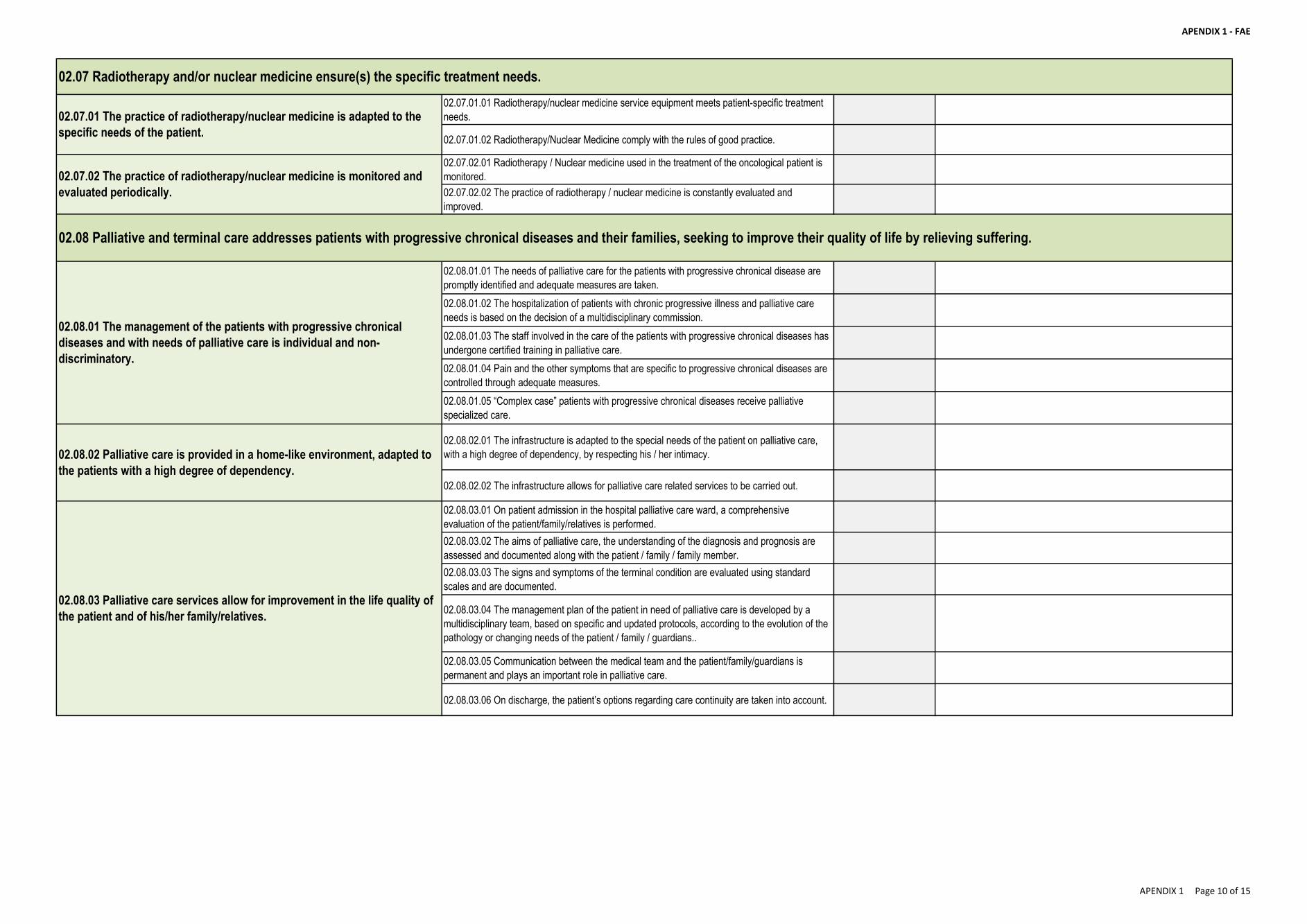
APENDIX 1 - FAE
02.07.01.01 Radiotherapy/nuclear medicine service equipment meets patient-specific treatment
needs.
02.07.01.02 Radiotherapy/Nuclear Medicine comply with the rules of good practice.
02.07.02.01 Radiotherapy / Nuclear medicine used in the treatment of the oncological patient is
monitored.
02.07.02.02 The practice of radiotherapy / nuclear medicine is constantly evaluated and
improved.
02.08.01.01 The needs of palliative care for the patients with progressive chronical disease are
promptly identified and adequate measures are taken.
02.08.01.02 The hospitalization of patients with chronic progressive illness and palliative care
needs is based on the decision of a multidisciplinary commission.
02.08.01.03 The staff involved in the care of the patients with progressive chronical diseases has
undergone certified training in palliative care.
02.08.01.04 Pain and the other symptoms that are specific to progressive chronical diseases are
controlled through adequate measures.
02.08.01.05 “Complex case” patients with progressive chronical diseases receive palliative
specialized care.
02.08.02.01 The infrastructure is adapted to the special needs of the patient on palliative care,
with a high degree of dependency, by respecting his / her intimacy.
02.08.02.02 The infrastructure allows for palliative care related services to be carried out.
02.08.03.01 On patient admission in the hospital palliative care ward, a comprehensive
evaluation of the patient/family/relatives is performed.
02.08.03.02 The aims of palliative care, the understanding of the diagnosis and prognosis are
assessed and documented along with the patient / family / family member.
02.08.03.03 The signs and symptoms of the terminal condition are evaluated using standard
scales and are documented.
02.08.03.04 The management plan of the patient in need of palliative care is developed by a
multidisciplinary team, based on specific and updated protocols, according to the evolution of the
pathology or changing needs of the patient / family / guardians..
02.08.03.05 Communication between the medical team and the patient/family/guardians is
permanent and plays an important role in palliative care.
02.08.03.06 On discharge, the patient’s options regarding care continuity are taken into account.
02.07.01 The practice of radiotherapy/nuclear medicine is adapted to the
specific needs of the patient.
02.07.02 The practice of radiotherapy/nuclear medicine is monitored and
evaluated periodically.
02.08.01 The management of the patients with progressive chronical
diseases and with needs of palliative care is individual and non-
discriminatory.
02.08.02 Palliative care is provided in a home-like environment, adapted to
the patients with a high degree of dependency.
02.08.03 Palliative care services allow for improvement in the life quality of
the patient and of his/her family/relatives.
02.08 Palliative and terminal care addresses patients with progressive chronical diseases and their families, seeking to improve their quality of life by relieving suffering.
02.07 Radiotherapy and/or nuclear medicine ensure(s) the specific treatment needs.
APENDIX 1 Page 10 of 15
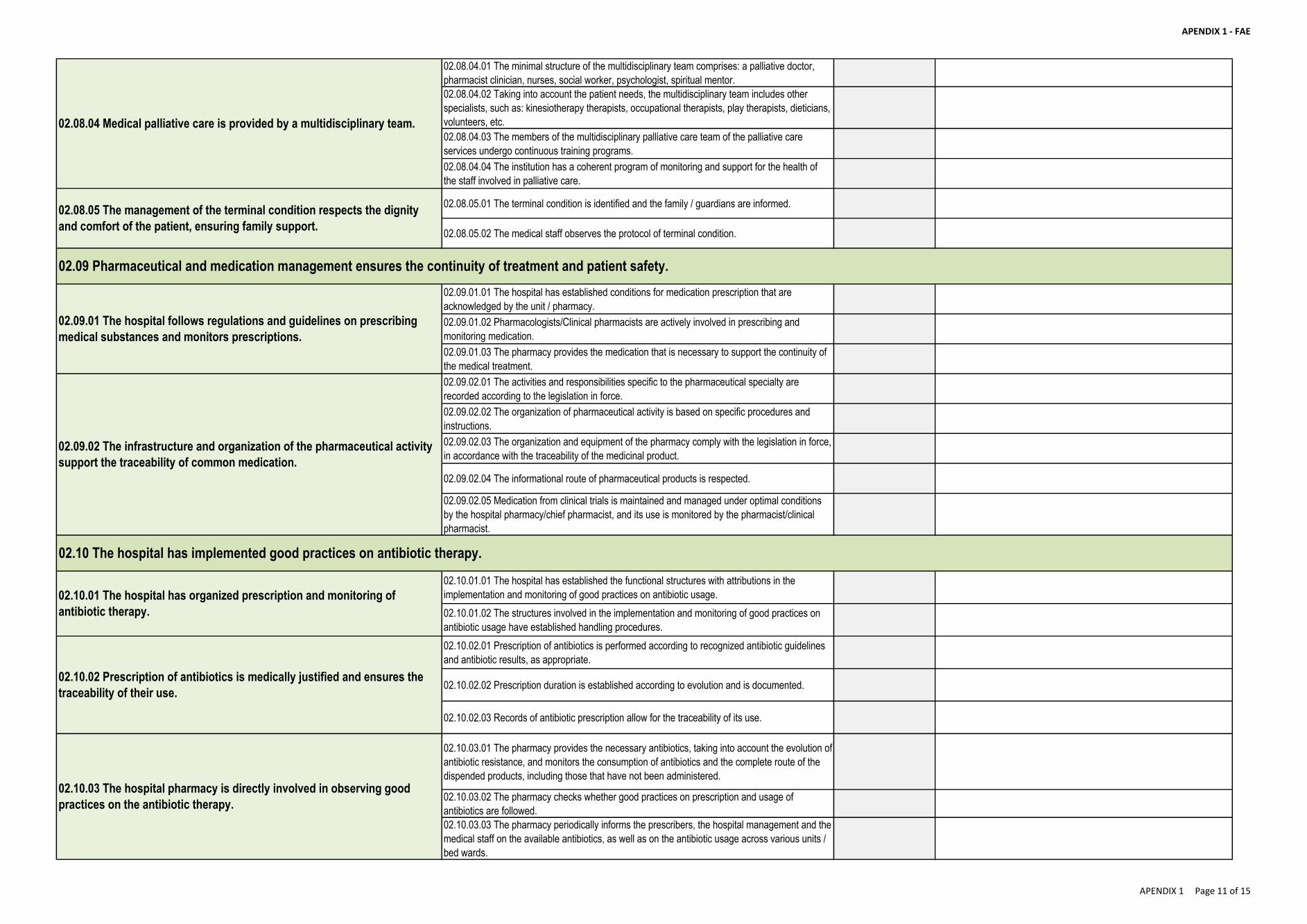
APENDIX 1 - FAE
02.08.04.01 The minimal structure of the multidisciplinary team comprises: a palliative doctor,
pharmacist clinician, nurses, social worker, psychologist, spiritual mentor.
02.08.04.02 Taking into account the patient needs, the multidisciplinary team includes other
specialists, such as: kinesiotherapy therapists, occupational therapists, play therapists, dieticians,
volunteers, etc.
02.08.04.03 The members of the multidisciplinary palliative care team of the palliative care
services undergo continuous training programs.
02.08.04.04 The institution has a coherent program of monitoring and support for the health of
the staff involved in palliative care.
02.08.05.01 The terminal condition is identified and the family / guardians are informed.
02.08.05.02 The medical staff observes the protocol of terminal condition.
02.09.01.01 The hospital has established conditions for medication prescription that are
acknowledged by the unit / pharmacy.
02.09.01.02 Pharmacologists/Clinical pharmacists are actively involved in prescribing and
monitoring medication.
02.09.01.03 The pharmacy provides the medication that is necessary to support the continuity of
the medical treatment.
02.09.02.01 The activities and responsibilities specific to the pharmaceutical specialty are
recorded according to the legislation in force.
02.09.02.02 The organization of pharmaceutical activity is based on specific procedures and
instructions.
02.09.02.03 The organization and equipment of the pharmacy comply with the legislation in force,
in accordance with the traceability of the medicinal product.
02.09.02.04 The informational route of pharmaceutical products is respected.
02.09.02.05 Medication from clinical trials is maintained and managed under optimal conditions
by the hospital pharmacy/chief pharmacist, and its use is monitored by the pharmacist/clinical
pharmacist.
02.10.01.01 The hospital has established the functional structures with attributions in the
implementation and monitoring of good practices on antibiotic usage.
02.10.01.02 The structures involved in the implementation and monitoring of good practices on
antibiotic usage have established handling procedures.
02.10.02.01 Prescription of antibiotics is performed according to recognized antibiotic guidelines
and antibiotic results, as appropriate.
02.10.02.02 Prescription duration is established according to evolution and is documented.
02.10.02.03 Records of antibiotic prescription allow for the traceability of its use.
02.10.03.01 The pharmacy provides the necessary antibiotics, taking into account the evolution of
antibiotic resistance, and monitors the consumption of antibiotics and the complete route of the
dispended products, including those that have not been administered.
02.10.03.02 The pharmacy checks whether good practices on prescription and usage of
antibiotics are followed.
02.10.03.03 The pharmacy periodically informs the prescribers, the hospital management and the
medical staff on the available antibiotics, as well as on the antibiotic usage across various units /
bed wards.
02.10.01 The hospital has organized prescription and monitoring of
antibiotic therapy.
02.10.02 Prescription of antibiotics is medically justified and ensures the
traceability of their use.
02.10.03 The hospital pharmacy is directly involved in observing good
practices on the antibiotic therapy.
02.09 Pharmaceutical and medication management ensures the continuity of treatment and patient safety.
02.08.04 Medical palliative care is provided by a multidisciplinary team.
02.08.05 The management of the terminal condition respects the dignity
and comfort of the patient, ensuring family support.
02.10 The hospital has implemented good practices on antibiotic therapy.
02.09.01 The hospital follows regulations and guidelines on prescribing
medical substances and monitors prescriptions.
02.09.02 The infrastructure and organization of the pharmaceutical activity
support the traceability of common medication.
APENDIX 1 Page 11 of 15
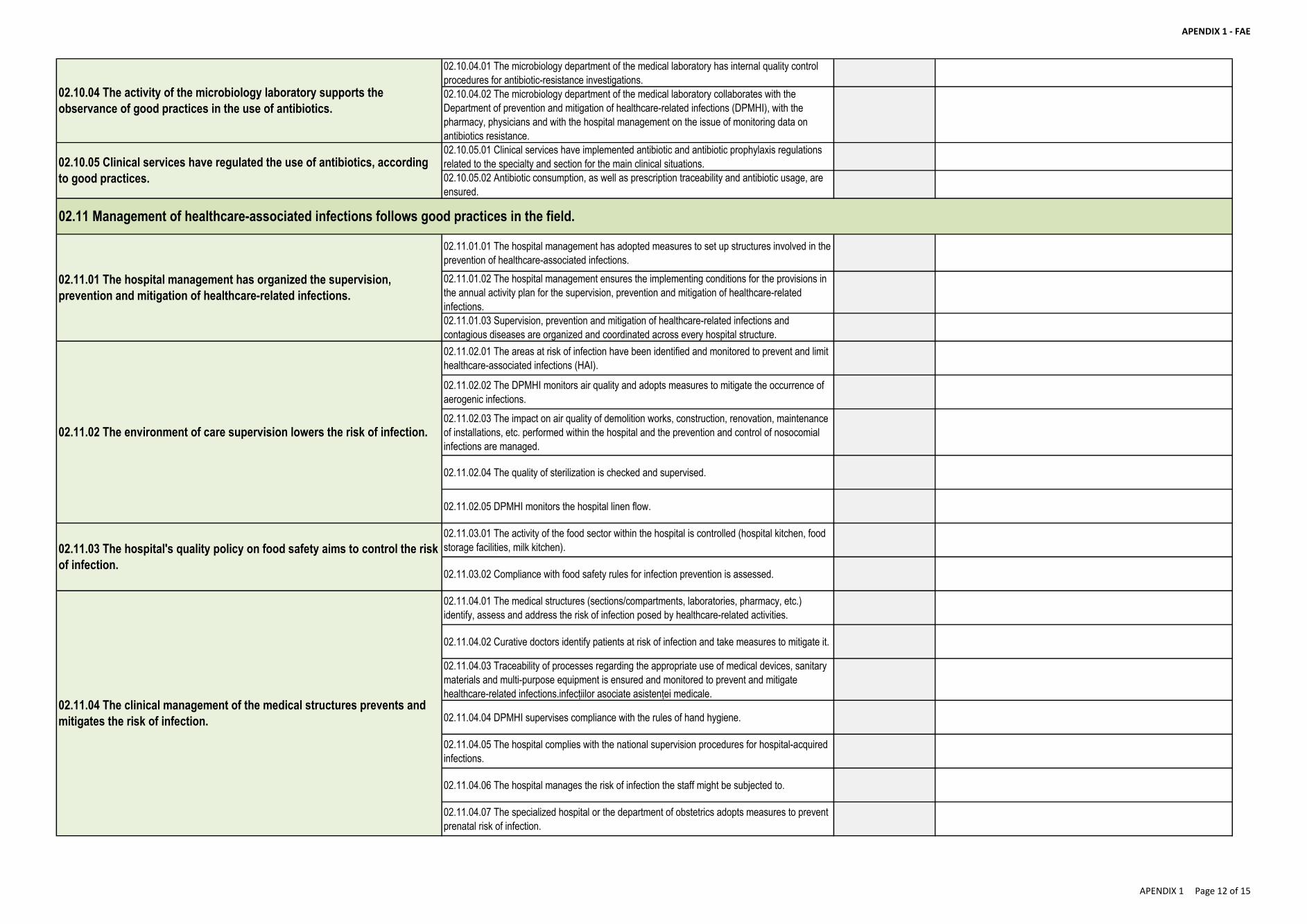
APENDIX 1 - FAE
02.10.04.01 The microbiology department of the medical laboratory has internal quality control
procedures for antibiotic-resistance investigations.
02.10.04.02 The microbiology department of the medical laboratory collaborates with the
Department of prevention and mitigation of healthcare-related infections (DPMHI), with the
pharmacy, physicians and with the hospital management on the issue of monitoring data on
antibiotics resistance.
02.10.05.01 Clinical services have implemented antibiotic and antibiotic prophylaxis regulations
related to the specialty and section for the main clinical situations.
02.10.05.02 Antibiotic consumption, as well as prescription traceability and antibiotic usage, are
ensured.
02.11.01.01 The hospital management has adopted measures to set up structures involved in the
prevention of healthcare-associated infections.
02.11.01.02 The hospital management ensures the implementing conditions for the provisions in
the annual activity plan for the supervision, prevention and mitigation of healthcare-related
infections.
02.11.01.03 Supervision, prevention and mitigation of healthcare-related infections and
contagious diseases are organized and coordinated across every hospital structure.
02.11.02.01 The areas at risk of infection have been identified and monitored to prevent and limit
healthcare-associated infections (HAI).
02.11.02.02 The DPMHI monitors air quality and adopts measures to mitigate the occurrence of
aerogenic infections.
02.11.02.03 The impact on air quality of demolition works, construction, renovation, maintenance
of installations, etc. performed within the hospital and the prevention and control of nosocomial
infections are managed.
02.11.02.04 The quality of sterilization is checked and supervised.
02.11.02.05 DPMHI monitors the hospital linen flow.
02.11.03.01 The activity of the food sector within the hospital is controlled (hospital kitchen, food
storage facilities, milk kitchen).
02.11.03.02 Compliance with food safety rules for infection prevention is assessed.
02.11.04.01 The medical structures (sections/compartments, laboratories, pharmacy, etc.)
identify, assess and address the risk of infection posed by healthcare-related activities.
02.11.04.02 Curative doctors identify patients at risk of infection and take measures to mitigate it.
02.11.04.03 Traceability of processes regarding the appropriate use of medical devices, sanitary
materials and multi-purpose equipment is ensured and monitored to prevent and mitigate
healthcare-related infections.infecțiilor asociate asistenței medicale.
02.11.04.04 DPMHI supervises compliance with the rules of hand hygiene.
02.11.04.05 The hospital complies with the national supervision procedures for hospital-acquired
infections.
02.11.04.06 The hospital manages the risk of infection the staff might be subjected to.
02.11.04.07 The specialized hospital or the department of obstetrics adopts measures to prevent
prenatal risk of infection.
02.11.03 The hospital's quality policy on food safety aims to control the risk
of infection.
02.11.04 The clinical management of the medical structures prevents and
mitigates the risk of infection.
02.10.04 The activity of the microbiology laboratory supports the
observance of good practices in the use of antibiotics.
02.10.05 Clinical services have regulated the use of antibiotics, according
to good practices.
02.11 Management of healthcare-associated infections follows good practices in the field.
02.11.01 The hospital management has organized the supervision,
prevention and mitigation of healthcare-related infections.
02.11.02 The environment of care supervision lowers the risk of infection.
APENDIX 1 Page 12 of 15
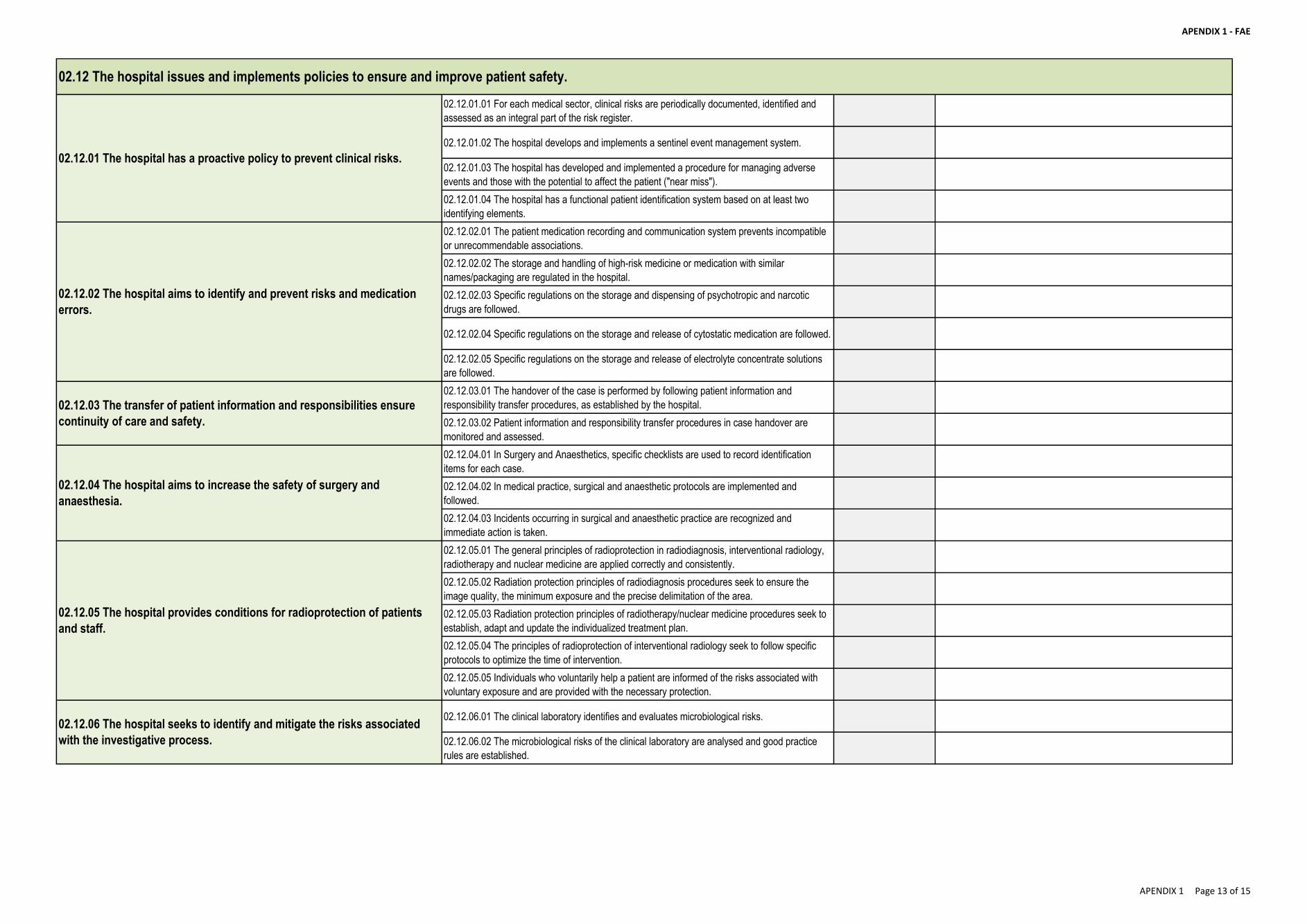
APENDIX 1 - FAE
02.12.01.01 For each medical sector, clinical risks are periodically documented, identified and
assessed as an integral part of the risk register.
02.12.01.02 The hospital develops and implements a sentinel event management system.
02.12.01.03 The hospital has developed and implemented a procedure for managing adverse
events and those with the potential to affect the patient ("near miss").
02.12.01.04 The hospital has a functional patient identification system based on at least two
identifying elements.
02.12.02.01 The patient medication recording and communication system prevents incompatible
or unrecommendable associations.
02.12.02.02 The storage and handling of high-risk medicine or medication with similar
names/packaging are regulated in the hospital.
02.12.02.03 Specific regulations on the storage and dispensing of psychotropic and narcotic
drugs are followed.
02.12.02.04 Specific regulations on the storage and release of cytostatic medication are followed.
02.12.02.05 Specific regulations on the storage and release of electrolyte concentrate solutions
are followed.
02.12.03.01 The handover of the case is performed by following patient information and
responsibility transfer procedures, as established by the hospital.
02.12.03.02 Patient information and responsibility transfer procedures in case handover are
monitored and assessed.
02.12.04.01 In Surgery and Anaesthetics, specific checklists are used to record identification
items for each case.
02.12.04.02 In medical practice, surgical and anaesthetic protocols are implemented and
followed.
02.12.04.03 Incidents occurring in surgical and anaesthetic practice are recognized and
immediate action is taken.
02.12.05.01 The general principles of radioprotection in radiodiagnosis, interventional radiology,
radiotherapy and nuclear medicine are applied correctly and consistently.
02.12.05.02 Radiation protection principles of radiodiagnosis procedures seek to ensure the
image quality, the minimum exposure and the precise delimitation of the area.
02.12.05.03 Radiation protection principles of radiotherapy/nuclear medicine procedures seek to
establish, adapt and update the individualized treatment plan.
02.12.05.04 The principles of radioprotection of interventional radiology seek to follow specific
protocols to optimize the time of intervention.
02.12.05.05 Individuals who voluntarily help a patient are informed of the risks associated with
voluntary exposure and are provided with the necessary protection.
02.12.06.01 The clinical laboratory identifies and evaluates microbiological risks.
02.12.06.02 The microbiological risks of the clinical laboratory are analysed and good practice
rules are established.
02.12.02 The hospital aims to identify and prevent risks and medication
errors.
02.12.03 The transfer of patient information and responsibilities ensure
continuity of care and safety.
02.12.04 The hospital aims to increase the safety of surgery and
anaesthesia.
02.12.01 The hospital has a proactive policy to prevent clinical risks.
02.12 The hospital issues and implements policies to ensure and improve patient safety.
02.12.05 The hospital provides conditions for radioprotection of patients
and staff.
02.12.06 The hospital seeks to identify and mitigate the risks associated
with the investigative process.
APENDIX 1 Page 13 of 15
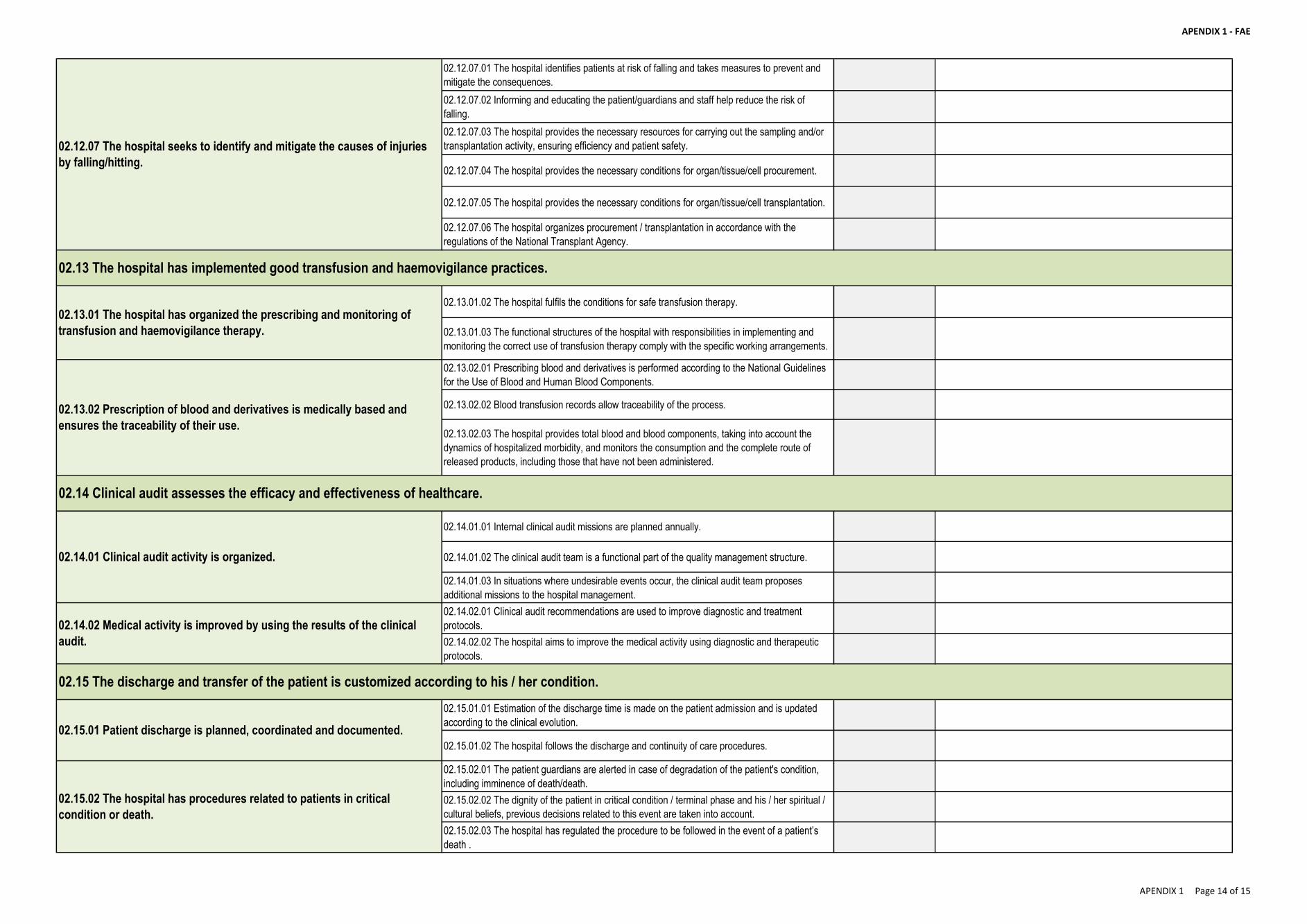
APENDIX 1 - FAE
02.12.07.01 The hospital identifies patients at risk of falling and takes measures to prevent and
mitigate the consequences.
02.12.07.02 Informing and educating the patient/guardians and staff help reduce the risk of
falling.
02.12.07.03 The hospital provides the necessary resources for carrying out the sampling and/or
transplantation activity, ensuring efficiency and patient safety.
02.12.07.04 The hospital provides the necessary conditions for organ/tissue/cell procurement.
02.12.07.05 The hospital provides the necessary conditions for organ/tissue/cell transplantation.
02.12.07.06 The hospital organizes procurement / transplantation in accordance with the
regulations of the National Transplant Agency.
02.13.01.02 The hospital fulfils the conditions for safe transfusion therapy.
02.13.01.03 The functional structures of the hospital with responsibilities in implementing and
monitoring the correct use of transfusion therapy comply with the specific working arrangements.
02.13.02.01 Prescribing blood and derivatives is performed according to the National Guidelines
for the Use of Blood and Human Blood Components.
02.13.02.02 Blood transfusion records allow traceability of the process.
02.13.02.03 The hospital provides total blood and blood components, taking into account the
dynamics of hospitalized morbidity, and monitors the consumption and the complete route of
released products, including those that have not been administered.
02.14.01.01 Internal clinical audit missions are planned annually.
02.14.01.02 The clinical audit team is a functional part of the quality management structure.
02.14.01.03 In situations where undesirable events occur, the clinical audit team proposes
additional missions to the hospital management.
02.14.02.01 Clinical audit recommendations are used to improve diagnostic and treatment
protocols.
02.14.02.02 The hospital aims to improve the medical activity using diagnostic and therapeutic
protocols.
02.15.01.01 Estimation of the discharge time is made on the patient admission and is updated
according to the clinical evolution.
02.15.01.02 The hospital follows the discharge and continuity of care procedures.
02.15.02.01 The patient guardians are alerted in case of degradation of the patient's condition,
including imminence of death/death.
02.15.02.02 The dignity of the patient in critical condition / terminal phase and his / her spiritual /
cultural beliefs, previous decisions related to this event are taken into account.
02.15.02.03 The hospital has regulated the procedure to be followed in the event of a patient’s
death .
02.12.07 The hospital seeks to identify and mitigate the causes of injuries
by falling/hitting.
02.14.02 Medical activity is improved by using the results of the clinical
audit.
02.15.01 Patient discharge is planned, coordinated and documented.
02.15.02 The hospital has procedures related to patients in critical
condition or death.
02.15 The discharge and transfer of the patient is customized according to his / her condition.
02.13.01 The hospital has organized the prescribing and monitoring of
transfusion and haemovigilance therapy.
02.13.02 Prescription of blood and derivatives is medically based and
ensures the traceability of their use.
02.14.01 Clinical audit activity is organized.
02.14 Clinical audit assesses the efficacy and effectiveness of healthcare.
02.13 The hospital has implemented good transfusion and haemovigilance practices.
APENDIX 1 Page 14 of 15
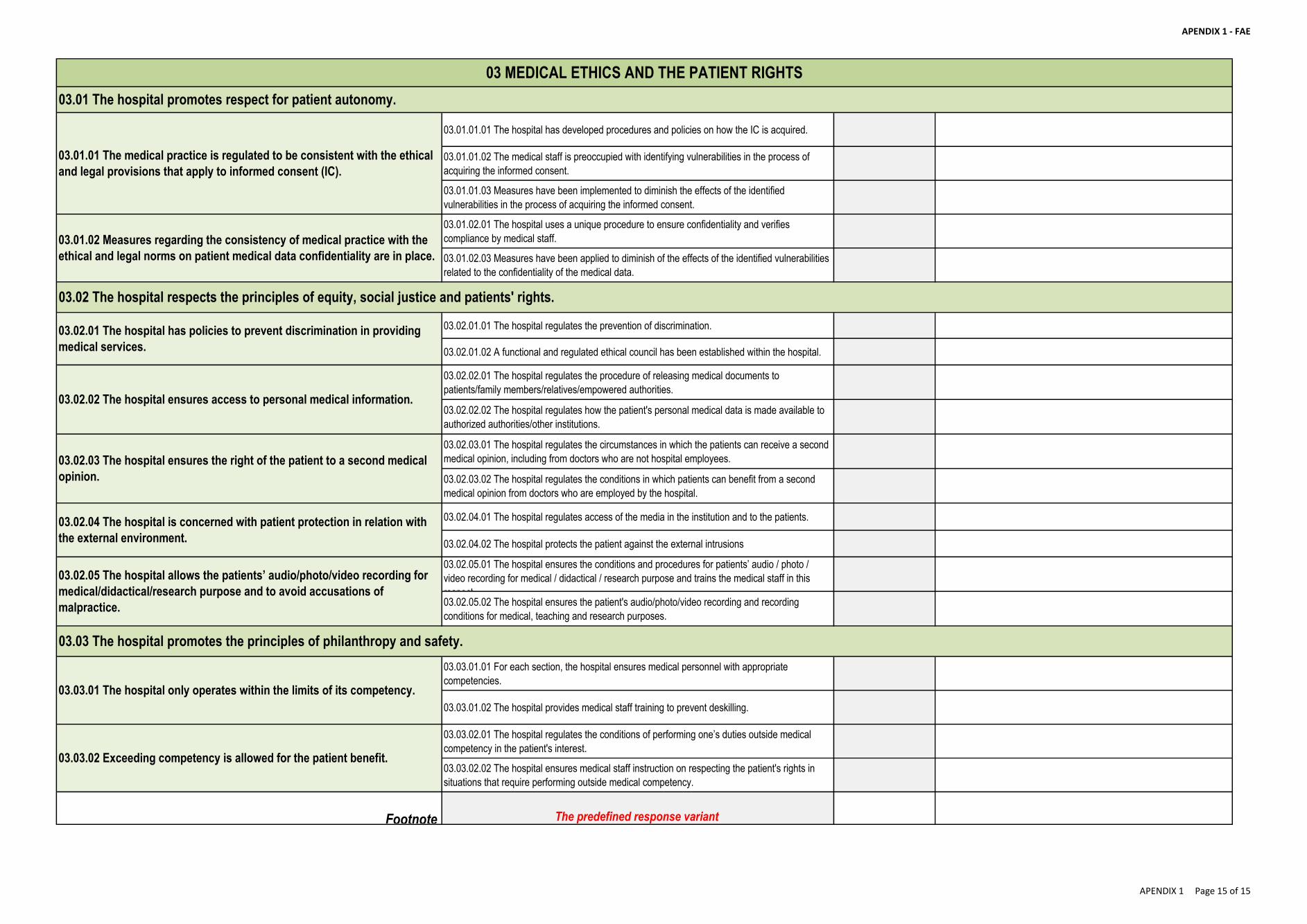
APENDIX 1 - FAE
03.01.01.01 The hospital has developed procedures and policies on how the IC is acquired.
03.01.01.02 The medical staff is preoccupied with identifying vulnerabilities in the process of
acquiring the informed consent.
03.01.01.03 Measures have been implemented to diminish the effects of the identified
vulnerabilities in the process of acquiring the informed consent.
03.01.02.01 The hospital uses a unique procedure to ensure confidentiality and verifies
compliance by medical staff.
03.01.02.03 Measures have been applied to diminish of the effects of the identified vulnerabilities
related to the confidentiality of the medical data.
03.02.01.01 The hospital regulates the prevention of discrimination.
03.02.01.02 A functional and regulated ethical council has been established within the hospital.
03.02.02.01 The hospital regulates the procedure of releasing medical documents to
patients/family members/relatives/empowered authorities.
03.02.02.02 The hospital regulates how the patient's personal medical data is made available to
authorized authorities/other institutions.
03.02.03.01 The hospital regulates the circumstances in which the patients can receive a second
medical opinion, including from doctors who are not hospital employees.
03.02.03.02 The hospital regulates the conditions in which patients can benefit from a second
medical opinion from doctors who are employed by the hospital.
03.02.04.01 The hospital regulates access of the media in the institution and to the patients.
03.02.04.02 The hospital protects the patient against the external intrusions
03.02.05.01 The hospital ensures the conditions and procedures for patients’ audio / photo /
video recording for medical / didactical / research purpose and trains the medical staff in this
respect. 03.02.05.02 The hospital ensures the patient's audio/photo/video recording and recording
conditions for medical, teaching and research purposes.
03.03.01.01 For each section, the hospital ensures medical personnel with appropriate
competencies.
03.03.01.02 The hospital provides medical staff training to prevent deskilling.
03.03.02.01 The hospital regulates the conditions of performing one’s duties outside medical
competency in the patient's interest.
03.03.02.02 The hospital ensures medical staff instruction on respecting the patient's rights in
situations that require performing outside medical competency.
Footnote The predefined response variant
03.02.04 The hospital is concerned with patient protection in relation with
the external environment.
03.02.05 The hospital allows the patients’ audio/photo/video recording for
medical/didactical/research purpose and to avoid accusations of
malpractice.
03.03.01 The hospital only operates within the limits of its competency.
03.03.02 Exceeding competency is allowed for the patient benefit.
03.03 The hospital promotes the principles of philanthropy and safety.
03.01.01 The medical practice is regulated to be consistent with the ethical
and legal provisions that apply to informed consent (IC).
03.01.02 Measures regarding the consistency of medical practice with the
ethical and legal norms on patient medical data confidentiality are in place.
03.02.01 The hospital has policies to prevent discrimination in providing
medical services.
03.02.02 The hospital ensures access to personal medical information.
03.02.03 The hospital ensures the right of the patient to a second medical
opinion.
03.02 The hospital respects the principles of equity, social justice and patients' rights.
03 MEDICAL ETHICS AND THE PATIENT RIGHTS
03.01 The hospital promotes respect for patient autonomy.
APENDIX 1 Page 15 of 15
APENDIX 2 - Master list
Standards for the
hospital accreditation
2017
APENDIX 2 Page 1 of 99
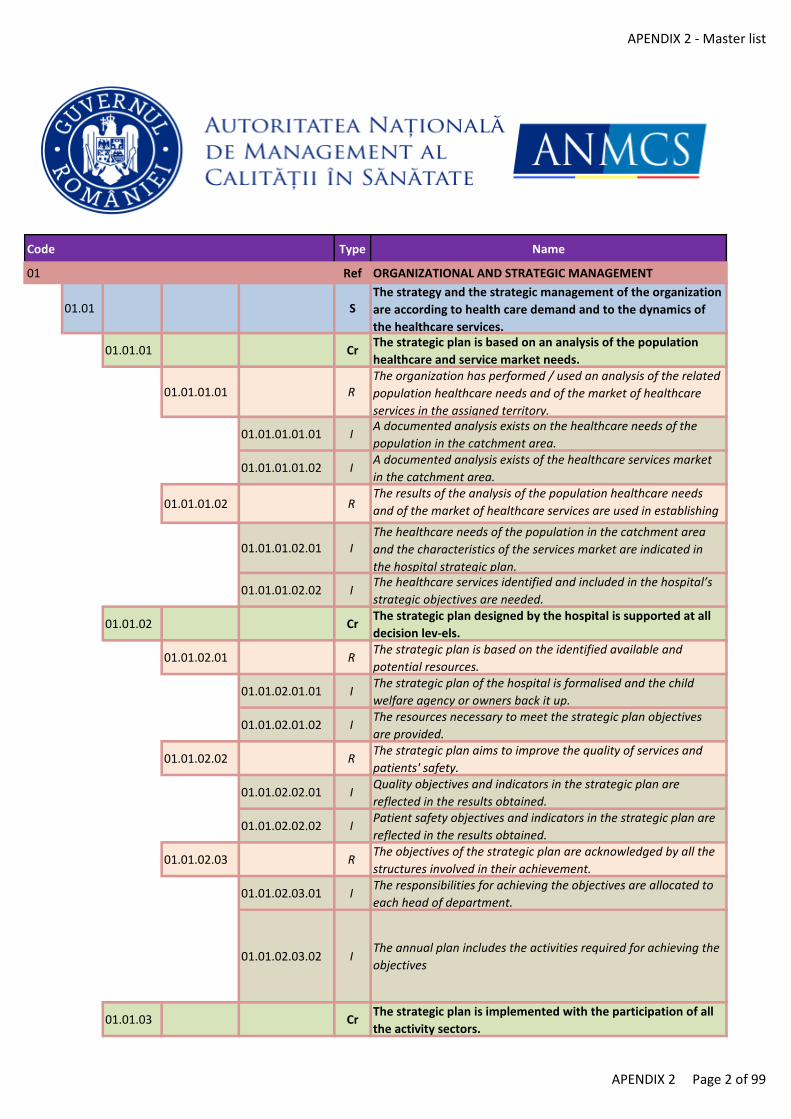
APENDIX 2 - Master list
Code Type Name
01 Ref ORGANIZATIONAL AND STRATEGIC MANAGEMENT
01.01 SThe strategy and the strategic management of the organization
are according to health care demand and to the dynamics of
the healthcare services.
01.01.01 CrThe strategic plan is based on an analysis of the population
healthcare and service market needs.
01.01.01.01 RThe organization has performed / used an analysis of the related
population healthcare needs and of the market of healthcare
services in the assigned territory.
01.01.01.01.01 IA documented analysis exists on the healthcare needs of the
population in the catchment area.
01.01.01.01.02 IA documented analysis exists of the healthcare services market
in the catchment area.
01.01.01.02 RThe results of the analysis of the population healthcare needs
and of the market of healthcare services are used in establishing
the strategic objectives of the hospital.
01.01.01.02.01 IThe healthcare needs of the population in the catchment area
and the characteristics of the services market are indicated in
the hospital strategic plan.
01.01.01.02.02 IThe healthcare services identified and included in the hospital’s
strategic objectives are needed.
01.01.02 CrThe strategic plan designed by the hospital is supported at all
decision lev-els.
01.01.02.01 RThe strategic plan is based on the identified available and
potential resources.
01.01.02.01.01 IThe strategic plan of the hospital is formalised and the child
welfare agency or owners back it up.
01.01.02.01.02 IThe resources necessary to meet the strategic plan objectives
are provided.
01.01.02.02 RThe strategic plan aims to improve the quality of services and
patients' safety.
01.01.02.02.01 IQuality objectives and indicators in the strategic plan are
reflected in the results obtained.
01.01.02.02.02 IPatient safety objectives and indicators in the strategic plan are
reflected in the results obtained.
01.01.02.03 RThe objectives of the strategic plan are acknowledged by all the
structures involved in their achievement.
01.01.02.03.01 IThe responsibilities for achieving the objectives are allocated to
each head of department.
01.01.02.03.02 IThe annual plan includes the activities required for achieving the
objectives
01.01.03 CrThe strategic plan is implemented with the participation of all
the activity sectors.
APENDIX 2 Page 2 of 99
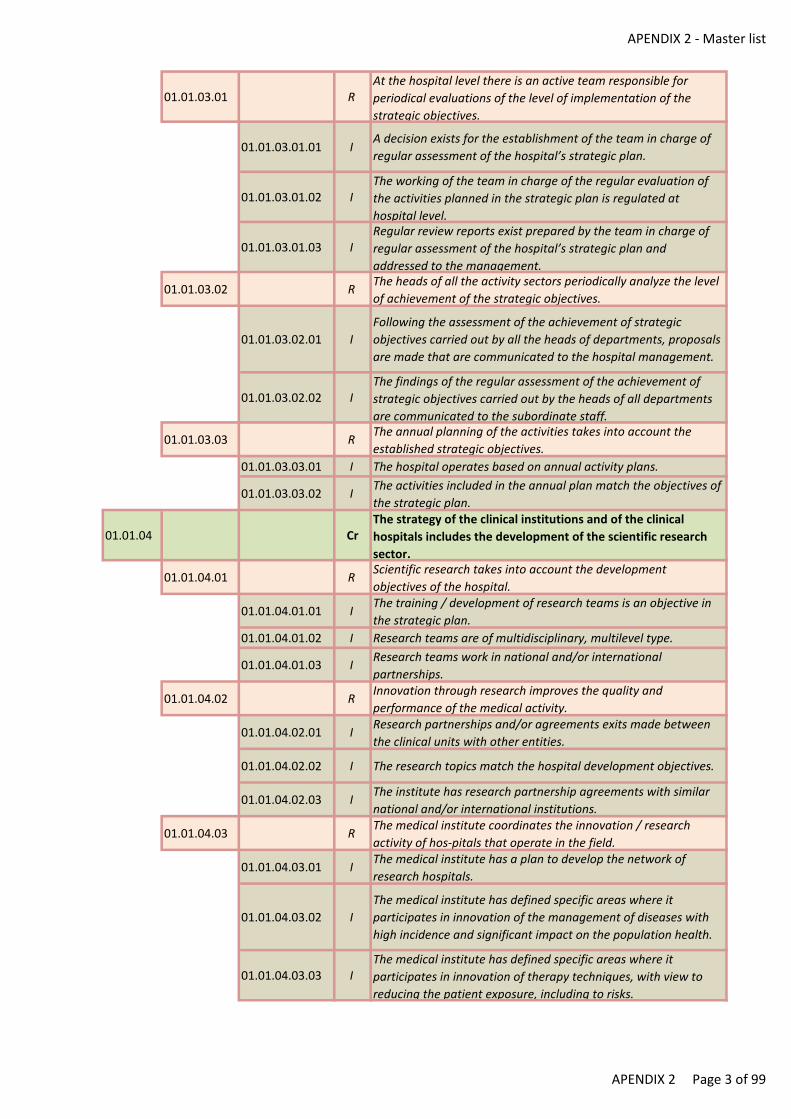
APENDIX 2 - Master list
01.01.03.01 RAt the hospital level there is an active team responsible for
periodical evaluations of the level of implementation of the
strategic objectives.
01.01.03.01.01 IA decision exists for the establishment of the team in charge of
regular assessment of the hospital’s strategic plan.
01.01.03.01.02 IThe working of the team in charge of the regular evaluation of
the activities planned in the strategic plan is regulated at
hospital level.
01.01.03.01.03 IRegular review reports exist prepared by the team in charge of
regular assessment of the hospital’s strategic plan and
addressed to the management.
01.01.03.02 RThe heads of all the activity sectors periodically analyze the level
of achievement of the strategic objectives.
01.01.03.02.01 I
Following the assessment of the achievement of strategic
objectives carried out by all the heads of departments, proposals
are made that are communicated to the hospital management.
01.01.03.02.02 IThe findings of the regular assessment of the achievement of
strategic objectives carried out by the heads of all departments
are communicated to the subordinate staff.
01.01.03.03 RThe annual planning of the activities takes into account the
established strategic objectives.
01.01.03.03.01 I The hospital operates based on annual activity plans.
01.01.03.03.02 IThe activities included in the annual plan match the objectives of
the strategic plan.
01.01.04 CrThe strategy of the clinical institutions and of the clinical
hospitals includes the development of the scientific research
sector.
01.01.04.01 RScientific research takes into account the development
objectives of the hospital.
01.01.04.01.01 IThe training / development of research teams is an objective in
the strategic plan.
01.01.04.01.02 I Research teams are of multidisciplinary, multilevel type.
01.01.04.01.03 IResearch teams work in national and/or international
partnerships.
01.01.04.02 RInnovation through research improves the quality and
performance of the medical activity.
01.01.04.02.01 IResearch partnerships and/or agreements exits made between
the clinical units with other entities.
01.01.04.02.02 I The research topics match the hospital development objectives.
01.01.04.02.03 IThe institute has research partnership agreements with similar
national and/or international institutions.
01.01.04.03 RThe medical institute coordinates the innovation / research
activity of hos-pitals that operate in the field.
01.01.04.03.01 IThe medical institute has a plan to develop the network of
research hospitals.
01.01.04.03.02 I
The medical institute has defined specific areas where it
participates in innovation of the management of diseases with
high incidence and significant impact on the population health.
01.01.04.03.03 IThe medical institute has defined specific areas where it
participates in innovation of therapy techniques, with view to
reducing the patient exposure, including to risks.
APENDIX 2 Page 3 of 99
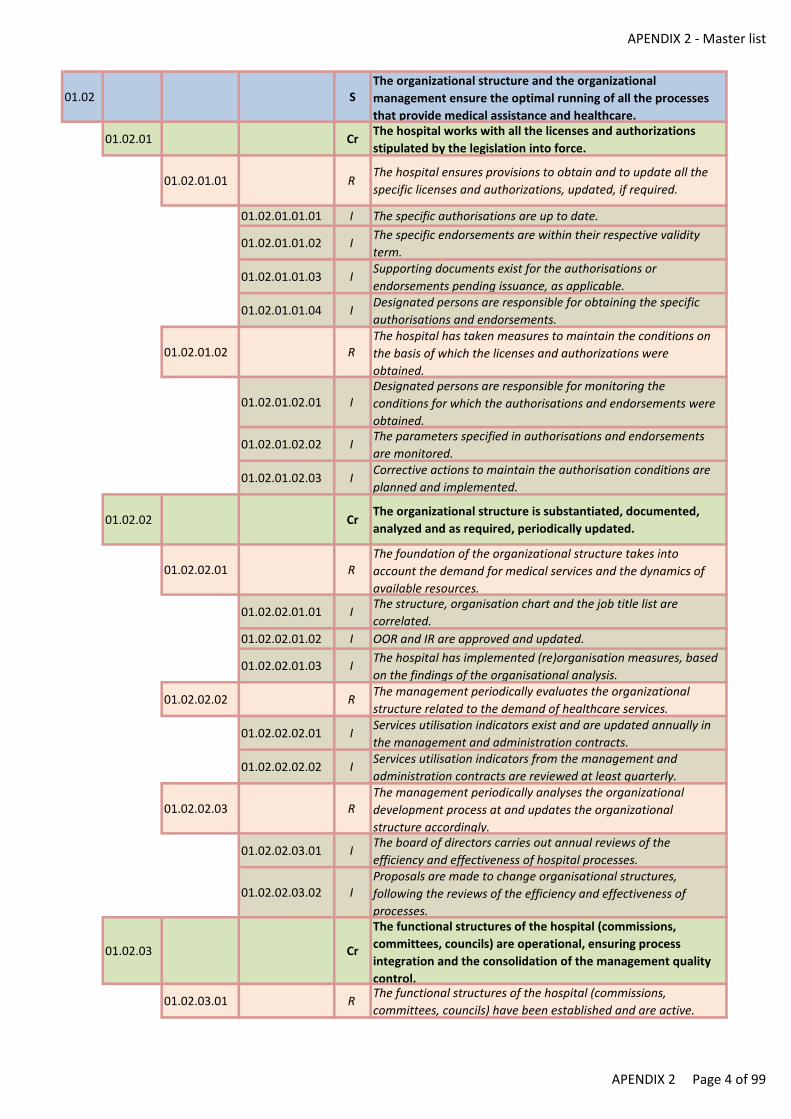
APENDIX 2 - Master list
01.02 SThe organizational structure and the organizational
management ensure the optimal running of all the processes
that provide medical assistance and healthcare.
01.02.01 CrThe hospital works with all the licenses and authorizations
stipulated by the legislation into force.
01.02.01.01 RThe hospital ensures provisions to obtain and to update all the
specific licenses and authorizations, updated, if required.
01.02.01.01.01 I The specific authorisations are up to date.
01.02.01.01.02 IThe specific endorsements are within their respective validity
term.
01.02.01.01.03 ISupporting documents exist for the authorisations or
endorsements pending issuance, as applicable.
01.02.01.01.04 IDesignated persons are responsible for obtaining the specific
authorisations and endorsements.
01.02.01.02 RThe hospital has taken measures to maintain the conditions on
the basis of which the licenses and authorizations were
obtained.
01.02.01.02.01 IDesignated persons are responsible for monitoring the
conditions for which the authorisations and endorsements were
obtained.
01.02.01.02.02 IThe parameters specified in authorisations and endorsements
are monitored.
01.02.01.02.03 ICorrective actions to maintain the authorisation conditions are
planned and implemented.
01.02.02 CrThe organizational structure is substantiated, documented,
analyzed and as required, periodically updated.
01.02.02.01 RThe foundation of the organizational structure takes into
account the demand for medical services and the dynamics of
available resources.
01.02.02.01.01 IThe structure, organisation chart and the job title list are
correlated.
01.02.02.01.02 I OOR and IR are approved and updated.
01.02.02.01.03 IThe hospital has implemented (re)organisation measures, based
on the findings of the organisational analysis.
01.02.02.02 RThe management periodically evaluates the organizational
structure related to the demand of healthcare services.
01.02.02.02.01 IServices utilisation indicators exist and are updated annually in
the management and administration contracts.
01.02.02.02.02 IServices utilisation indicators from the management and
administration contracts are reviewed at least quarterly.
01.02.02.03 RThe management periodically analyses the organizational
development process at and updates the organizational
structure accordingly.
01.02.02.03.01 IThe board of directors carries out annual reviews of the
efficiency and effectiveness of hospital processes.
01.02.02.03.02 IProposals are made to change organisational structures,
following the reviews of the efficiency and effectiveness of
processes.
01.02.03 Cr
The functional structures of the hospital (commissions,
committees, councils) are operational, ensuring process
integration and the consolidation of the management quality
control.
01.02.03.01 RThe functional structures of the hospital (commissions,
committees, councils) have been established and are active.
APENDIX 2 Page 4 of 99
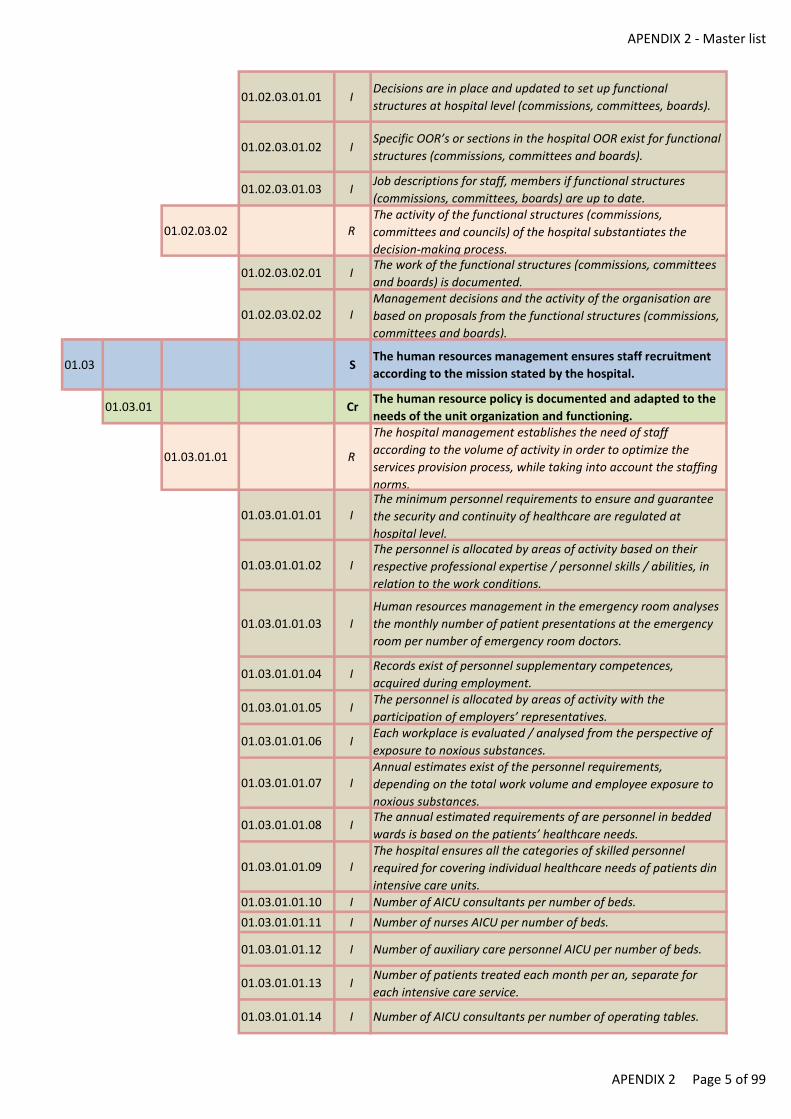
APENDIX 2 - Master list
01.02.03.01.01 IDecisions are in place and updated to set up functional
structures at hospital level (commissions, committees, boards).
01.02.03.01.02 ISpecific OOR’s or sections in the hospital OOR exist for functional
structures (commissions, committees and boards).
01.02.03.01.03 IJob descriptions for staff, members if functional structures
(commissions, committees, boards) are up to date.
01.02.03.02 RThe activity of the functional structures (commissions,
committees and councils) of the hospital substantiates the
decision-making process.
01.02.03.02.01 IThe work of the functional structures (commissions, committees
and boards) is documented.
01.02.03.02.02 IManagement decisions and the activity of the organisation are
based on proposals from the functional structures (commissions,
committees and boards).
01.03 SThe human resources management ensures staff recruitment
according to the mission stated by the hospital.
01.03.01 CrThe human resource policy is documented and adapted to the
needs of the unit organization and functioning.
01.03.01.01 R
The hospital management establishes the need of staff
according to the volume of activity in order to optimize the
services provision process, while taking into account the staffing
norms.
01.03.01.01.01 IThe minimum personnel requirements to ensure and guarantee
the security and continuity of healthcare are regulated at
hospital level.
01.03.01.01.02 IThe personnel is allocated by areas of activity based on their
respective professional expertise / personnel skills / abilities, in
relation to the work conditions.
01.03.01.01.03 I
Human resources management in the emergency room analyses
the monthly number of patient presentations at the emergency
room per number of emergency room doctors.
01.03.01.01.04 IRecords exist of personnel supplementary competences,
acquired during employment.
01.03.01.01.05 IThe personnel is allocated by areas of activity with the
participation of employers’ representatives.
01.03.01.01.06 IEach workplace is evaluated / analysed from the perspective of
exposure to noxious substances.
01.03.01.01.07 IAnnual estimates exist of the personnel requirements,
depending on the total work volume and employee exposure to
noxious substances.
01.03.01.01.08 IThe annual estimated requirements of are personnel in bedded
wards is based on the patients’ healthcare needs.
01.03.01.01.09 IThe hospital ensures all the categories of skilled personnel
required for covering individual healthcare needs of patients din
intensive care units.
01.03.01.01.10 I Number of AICU consultants per number of beds.
01.03.01.01.11 I Number of nurses AICU per number of beds.
01.03.01.01.12 I Number of auxiliary care personnel AICU per number of beds.
01.03.01.01.13 INumber of patients treated each month per an, separate for
each intensive care service.
01.03.01.01.14 I Number of AICU consultants per number of operating tables.
APENDIX 2 Page 5 of 99
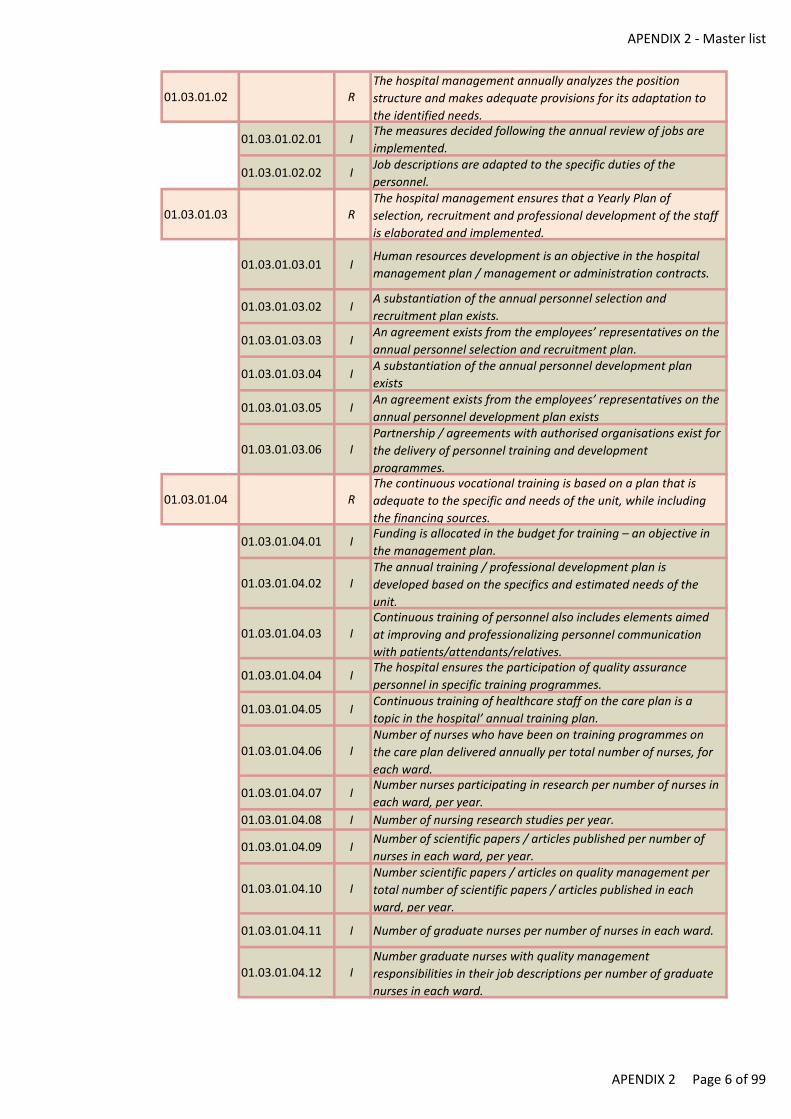
APENDIX 2 - Master list
01.03.01.02 RThe hospital management annually analyzes the position
structure and makes adequate provisions for its adaptation to
the identified needs.
01.03.01.02.01 IThe measures decided following the annual review of jobs are
implemented.
01.03.01.02.02 IJob descriptions are adapted to the specific duties of the
personnel.
01.03.01.03 RThe hospital management ensures that a Yearly Plan of
selection, recruitment and professional development of the staff
is elaborated and implemented.
01.03.01.03.01 IHuman resources development is an objective in the hospital
management plan / management or administration contracts.
01.03.01.03.02 IA substantiation of the annual personnel selection and
recruitment plan exists.
01.03.01.03.03 IAn agreement exists from the employees’ representatives on the
annual personnel selection and recruitment plan.
01.03.01.03.04 IA substantiation of the annual personnel development plan
exists
01.03.01.03.05 IAn agreement exists from the employees’ representatives on the
annual personnel development plan exists
01.03.01.03.06 IPartnership / agreements with authorised organisations exist for
the delivery of personnel training and development
programmes.
01.03.01.04 RThe continuous vocational training is based on a plan that is
adequate to the specific and needs of the unit, while including
the financing sources.
01.03.01.04.01 IFunding is allocated in the budget for training – an objective in
the management plan.
01.03.01.04.02 IThe annual training / professional development plan is
developed based on the specifics and estimated needs of the
unit.
01.03.01.04.03 IContinuous training of personnel also includes elements aimed
at improving and professionalizing personnel communication
with patients/attendants/relatives.
01.03.01.04.04 IThe hospital ensures the participation of quality assurance
personnel in specific training programmes.
01.03.01.04.05 IContinuous training of healthcare staff on the care plan is a
topic in the hospital’ annual training plan.
01.03.01.04.06 INumber of nurses who have been on training programmes on
the care plan delivered annually per total number of nurses, for
each ward.
01.03.01.04.07 INumber nurses participating in research per number of nurses in
each ward, per year.
01.03.01.04.08 I Number of nursing research studies per year.
01.03.01.04.09 INumber of scientific papers / articles published per number of
nurses in each ward, per year.
01.03.01.04.10 INumber scientific papers / articles on quality management per
total number of scientific papers / articles published in each
ward, per year.
01.03.01.04.11 I Number of graduate nurses per number of nurses in each ward.
01.03.01.04.12 INumber graduate nurses with quality management
responsibilities in their job descriptions per number of graduate
nurses in each ward.
APENDIX 2 Page 6 of 99
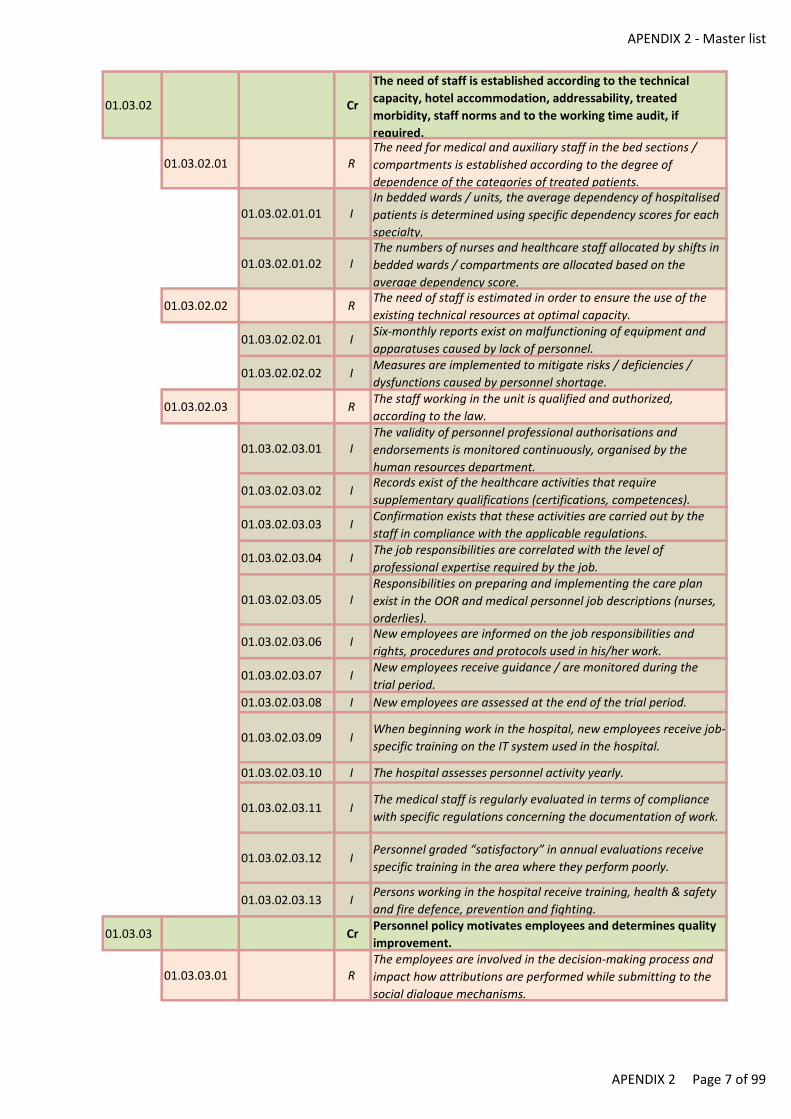
APENDIX 2 - Master list
01.03.02 Cr
The need of staff is established according to the technical
capacity, hotel accommodation, addressability, treated
morbidity, staff norms and to the working time audit, if
required.
01.03.02.01 RThe need for medical and auxiliary staff in the bed sections /
compartments is established according to the degree of
dependence of the categories of treated patients.
01.03.02.01.01 IIn bedded wards / units, the average dependency of hospitalised
patients is determined using specific dependency scores for each
specialty.
01.03.02.01.02 IThe numbers of nurses and healthcare staff allocated by shifts in
bedded wards / compartments are allocated based on the
average dependency score.
01.03.02.02 RThe need of staff is estimated in order to ensure the use of the
existing technical resources at optimal capacity.
01.03.02.02.01 ISix-monthly reports exist on malfunctioning of equipment and
apparatuses caused by lack of personnel.
01.03.02.02.02 IMeasures are implemented to mitigate risks / deficiencies /
dysfunctions caused by personnel shortage.
01.03.02.03 RThe staff working in the unit is qualified and authorized,
according to the law.
01.03.02.03.01 IThe validity of personnel professional authorisations and
endorsements is monitored continuously, organised by the
human resources department.
01.03.02.03.02 IRecords exist of the healthcare activities that require
supplementary qualifications (certifications, competences).
01.03.02.03.03 IConfirmation exists that these activities are carried out by the
staff in compliance with the applicable regulations.
01.03.02.03.04 IThe job responsibilities are correlated with the level of
professional expertise required by the job.
01.03.02.03.05 IResponsibilities on preparing and implementing the care plan
exist in the OOR and medical personnel job descriptions (nurses,
orderlies).
01.03.02.03.06 INew employees are informed on the job responsibilities and
rights, procedures and protocols used in his/her work.
01.03.02.03.07 INew employees receive guidance / are monitored during the
trial period.
01.03.02.03.08 I New employees are assessed at the end of the trial period.
01.03.02.03.09 IWhen beginning work in the hospital, new employees receive job-
specific training on the IT system used in the hospital.
01.03.02.03.10 I The hospital assesses personnel activity yearly.
01.03.02.03.11 IThe medical staff is regularly evaluated in terms of compliance
with specific regulations concerning the documentation of work.
01.03.02.03.12 IPersonnel graded “satisfactory” in annual evaluations receive
specific training in the area where they perform poorly.
01.03.02.03.13 IPersons working in the hospital receive training, health & safety
and fire defence, prevention and fighting.
01.03.03 CrPersonnel policy motivates employees and determines quality
improvement.
01.03.03.01 RThe employees are involved in the decision-making process and
impact how attributions are performed while submitting to the
social dialogue mechanisms.
APENDIX 2 Page 7 of 99
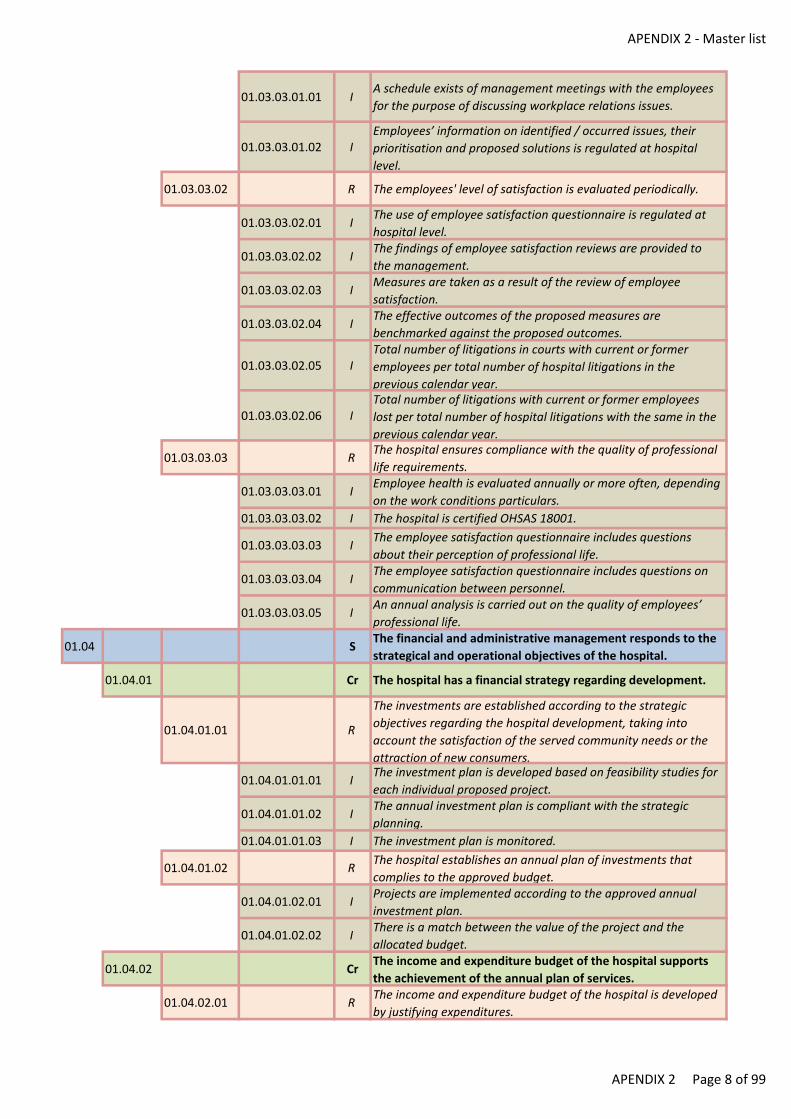
APENDIX 2 - Master list
01.03.03.01.01 IA schedule exists of management meetings with the employees
for the purpose of discussing workplace relations issues.
01.03.03.01.02 IEmployees’ information on identified / occurred issues, their
prioritisation and proposed solutions is regulated at hospital
level.
01.03.03.02 R The employees' level of satisfaction is evaluated periodically.
01.03.03.02.01 IThe use of employee satisfaction questionnaire is regulated at
hospital level.
01.03.03.02.02 IThe findings of employee satisfaction reviews are provided to
the management.
01.03.03.02.03 IMeasures are taken as a result of the review of employee
satisfaction.
01.03.03.02.04 IThe effective outcomes of the proposed measures are
benchmarked against the proposed outcomes.
01.03.03.02.05 ITotal number of litigations in courts with current or former
employees per total number of hospital litigations in the
previous calendar year.
01.03.03.02.06 ITotal number of litigations with current or former employees
lost per total number of hospital litigations with the same in the
previous calendar year.
01.03.03.03 RThe hospital ensures compliance with the quality of professional
life requirements.
01.03.03.03.01 IEmployee health is evaluated annually or more often, depending
on the work conditions particulars.
01.03.03.03.02 I The hospital is certified OHSAS 18001.
01.03.03.03.03 IThe employee satisfaction questionnaire includes questions
about their perception of professional life.
01.03.03.03.04 IThe employee satisfaction questionnaire includes questions on
communication between personnel.
01.03.03.03.05 IAn annual analysis is carried out on the quality of employees’
professional life.
01.04 SThe financial and administrative management responds to the
strategical and operational objectives of the hospital.
01.04.01 Cr The hospital has a financial strategy regarding development.
01.04.01.01 R
The investments are established according to the strategic
objectives regarding the hospital development, taking into
account the satisfaction of the served community needs or the
attraction of new consumers.
01.04.01.01.01 IThe investment plan is developed based on feasibility studies for
each individual proposed project.
01.04.01.01.02 IThe annual investment plan is compliant with the strategic
planning.
01.04.01.01.03 I The investment plan is monitored.
01.04.01.02 RThe hospital establishes an annual plan of investments that
complies to the approved budget.
01.04.01.02.01 IProjects are implemented according to the approved annual
investment plan.
01.04.01.02.02 IThere is a match between the value of the project and the
allocated budget.
01.04.02 CrThe income and expenditure budget of the hospital supports
the achievement of the annual plan of services.
01.04.02.01 RThe income and expenditure budget of the hospital is developed
by justifying expenditures.
APENDIX 2 Page 8 of 99
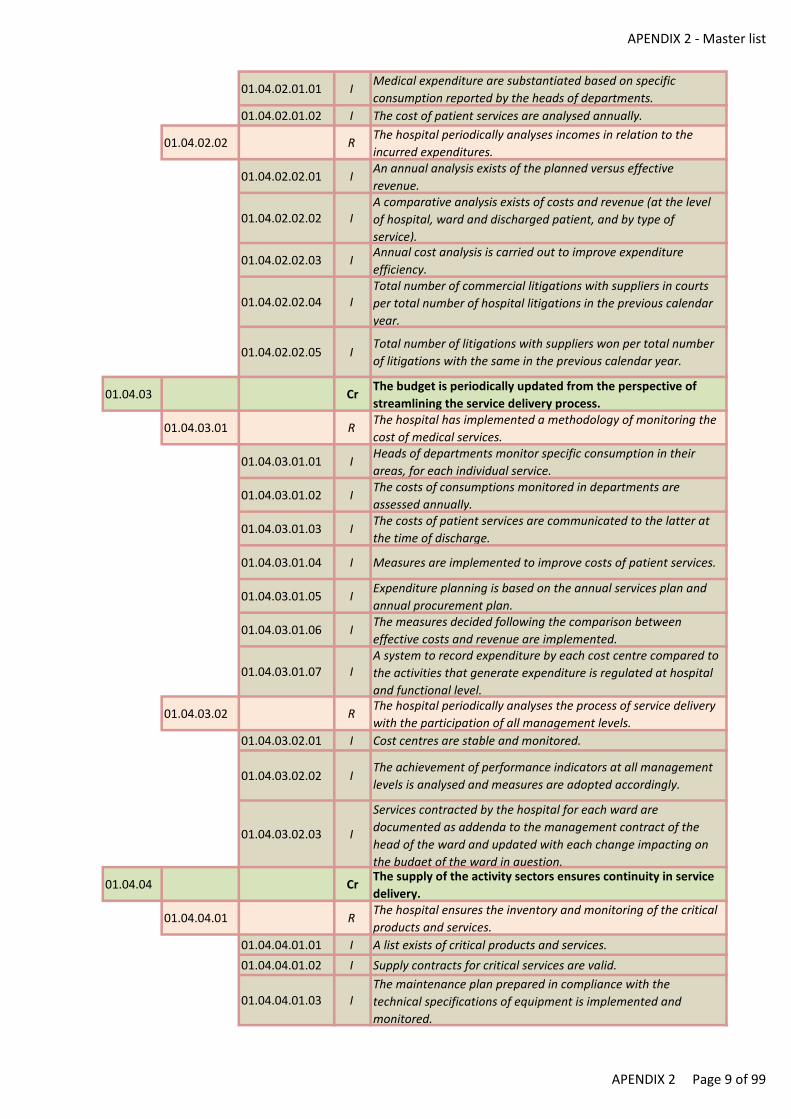
APENDIX 2 - Master list
01.04.02.01.01 IMedical expenditure are substantiated based on specific
consumption reported by the heads of departments.
01.04.02.01.02 I The cost of patient services are analysed annually.
01.04.02.02 RThe hospital periodically analyses incomes in relation to the
incurred expenditures.
01.04.02.02.01 IAn annual analysis exists of the planned versus effective
revenue.
01.04.02.02.02 IA comparative analysis exists of costs and revenue (at the level
of hospital, ward and discharged patient, and by type of
service).
01.04.02.02.03 IAnnual cost analysis is carried out to improve expenditure
efficiency.
01.04.02.02.04 ITotal number of commercial litigations with suppliers in courts
per total number of hospital litigations in the previous calendar
year.
01.04.02.02.05 ITotal number of litigations with suppliers won per total number
of litigations with the same in the previous calendar year.
01.04.03 CrThe budget is periodically updated from the perspective of
streamlining the service delivery process.
01.04.03.01 RThe hospital has implemented a methodology of monitoring the
cost of medical services.
01.04.03.01.01 IHeads of departments monitor specific consumption in their
areas, for each individual service.
01.04.03.01.02 IThe costs of consumptions monitored in departments are
assessed annually.
01.04.03.01.03 IThe costs of patient services are communicated to the latter at
the time of discharge.
01.04.03.01.04 I Measures are implemented to improve costs of patient services.
01.04.03.01.05 IExpenditure planning is based on the annual services plan and
annual procurement plan.
01.04.03.01.06 IThe measures decided following the comparison between
effective costs and revenue are implemented.
01.04.03.01.07 IA system to record expenditure by each cost centre compared to
the activities that generate expenditure is regulated at hospital
and functional level.
01.04.03.02 RThe hospital periodically analyses the process of service delivery
with the participation of all management levels.
01.04.03.02.01 I Cost centres are stable and monitored.
01.04.03.02.02 IThe achievement of performance indicators at all management
levels is analysed and measures are adopted accordingly.
01.04.03.02.03 I
Services contracted by the hospital for each ward are
documented as addenda to the management contract of the
head of the ward and updated with each change impacting on
the budget of the ward in question.
01.04.04 CrThe supply of the activity sectors ensures continuity in service
delivery.
01.04.04.01 RThe hospital ensures the inventory and monitoring of the critical
products and services.
01.04.04.01.01 I A list exists of critical products and services.
01.04.04.01.02 I Supply contracts for critical services are valid.
01.04.04.01.03 IThe maintenance plan prepared in compliance with the
technical specifications of equipment is implemented and
monitored.
APENDIX 2 Page 9 of 99
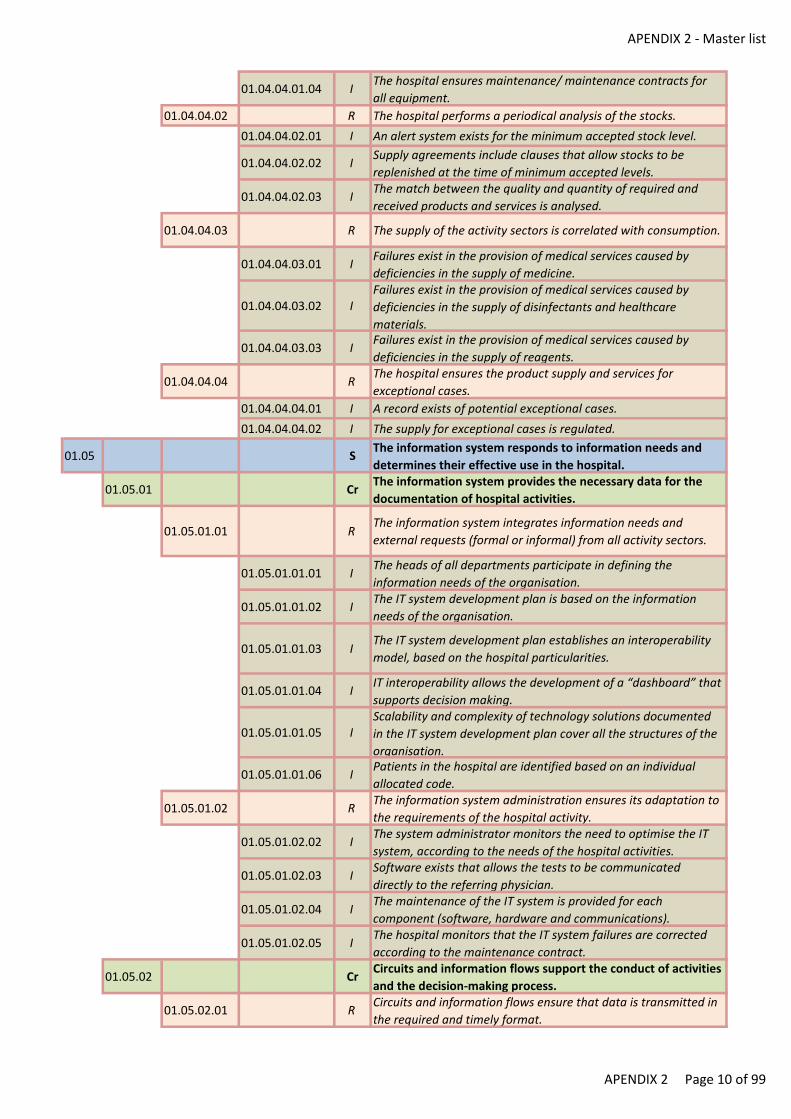
APENDIX 2 - Master list
01.04.04.01.04 IThe hospital ensures maintenance/ maintenance contracts for
all equipment.
01.04.04.02 R The hospital performs a periodical analysis of the stocks.
01.04.04.02.01 I An alert system exists for the minimum accepted stock level.
01.04.04.02.02 ISupply agreements include clauses that allow stocks to be
replenished at the time of minimum accepted levels.
01.04.04.02.03 IThe match between the quality and quantity of required and
received products and services is analysed.
01.04.04.03 R The supply of the activity sectors is correlated with consumption.
01.04.04.03.01 IFailures exist in the provision of medical services caused by
deficiencies in the supply of medicine.
01.04.04.03.02 IFailures exist in the provision of medical services caused by
deficiencies in the supply of disinfectants and healthcare
materials.
01.04.04.03.03 IFailures exist in the provision of medical services caused by
deficiencies in the supply of reagents.
01.04.04.04 RThe hospital ensures the product supply and services for
exceptional cases.
01.04.04.04.01 I A record exists of potential exceptional cases.
01.04.04.04.02 I The supply for exceptional cases is regulated.
01.05 SThe information system responds to information needs and
determines their effective use in the hospital.
01.05.01 CrThe information system provides the necessary data for the
documentation of hospital activities.
01.05.01.01 RThe information system integrates information needs and
external requests (formal or informal) from all activity sectors.
01.05.01.01.01 IThe heads of all departments participate in defining the
information needs of the organisation.
01.05.01.01.02 IThe IT system development plan is based on the information
needs of the organisation.
01.05.01.01.03 IThe IT system development plan establishes an interoperability
model, based on the hospital particularities.
01.05.01.01.04 IIT interoperability allows the development of a “dashboard” that
supports decision making.
01.05.01.01.05 IScalability and complexity of technology solutions documented
in the IT system development plan cover all the structures of the
organisation.
01.05.01.01.06 IPatients in the hospital are identified based on an individual
allocated code.
01.05.01.02 RThe information system administration ensures its adaptation to
the requirements of the hospital activity.
01.05.01.02.02 IThe system administrator monitors the need to optimise the IT
system, according to the needs of the hospital activities.
01.05.01.02.03 ISoftware exists that allows the tests to be communicated
directly to the referring physician.
01.05.01.02.04 IThe maintenance of the IT system is provided for each
component (software, hardware and communications).
01.05.01.02.05 IThe hospital monitors that the IT system failures are corrected
according to the maintenance contract.
01.05.02 CrCircuits and information flows support the conduct of activities
and the decision-making process.
01.05.02.01 RCircuits and information flows ensure that data is transmitted in
the required and timely format.
APENDIX 2 Page 10 of 99

APENDIX 2 - Master list
01.05.02.01.01 I The hospital has implemented a document management system.
01.05.02.01.02 IThe documents issued at hospital level in response to internal
and/or external requests are duly registered
01.05.02.01.03 IThe hospital personnel have real time access to data and
information required for discharging their responsibilities.
01.05.02.01.04 I The hospital has organised patients’ registration system.
01.05.02.02 RCircuits and information flows contain alert systems that prevent
the occurrence of decisional errors.
01.05.02.02.01 IInformation access levels are defined for each category of
personnel.
01.05.02.02.02 I Accidental / intentional virus alert is in place.
01.05.02.02.03 IInformation integrity is regulated and ensured by the use of
successive verification filters
01.05.02.02.04 IThe annual internal audit report includes findings on the
operation of information technology.
01.05.03 CrInformation processes underpin effective decisions within the
hospital.
01.05.03.01 RThe data carrier for each activity in the hospital (paper-based,
magnetic, electronic) and the flow of information are clearly
defined and respected.
01.05.03.01.01 IThe hospital has defined a consistent method for recording each
category of information.
01.05.03.01.02 I Data is recorded in real time.
01.05.03.01.03 I At hospital level, the document flow is regulated.
01.05.03.02 RThe operability of the implemented informational procedures
ensures that hospital activity is more efficient.
01.05.03.02.01 I Operational procedures exist by category of activities.
01.05.03.02.02 IA six-monthly analysis of compliance with operational
procedures is carried out.
01.05.03.02.03 I Persons are designated to verify documents according to a plan.
01.05.03.02.04 IMonthly records exist for interventions and development of IT
applications.
01.05.03.02.05 IThe IT system risks in relation to its reliability, complexity and
scalability are identified and dealt with.
01.05.04 CrThe information system and the data storage environment
ensure the confidentiality, integrity and security of the data.
01.05.04.01 R The hospital respects the law in force regarding data security.
01.05.04.01.01 I The hospital is registered as personal data operator.
01.05.04.01.02 IThe patients’ personal/medical data is transmitted in
confidentiality.
01.05.04.01.03 IThe hospital applies a specific rule for requests for medical data
received from patients/relatives.
01.05.04.01.04 IA method is in place for ensuring data propriety in relation with
third party collaborators.
01.05.04.01.05 I The hospital is certified ISO/IEC 27001.
01.05.04.01.06 I Data collection and management is regulated at hospital level.
01.05.04.02 RAccess to information, their processing and protection is
regulated for each professional category.
01.05.04.02.01 IAccess to computer system data is regulated and enforced at
hospital level.
APENDIX 2 Page 11 of 99
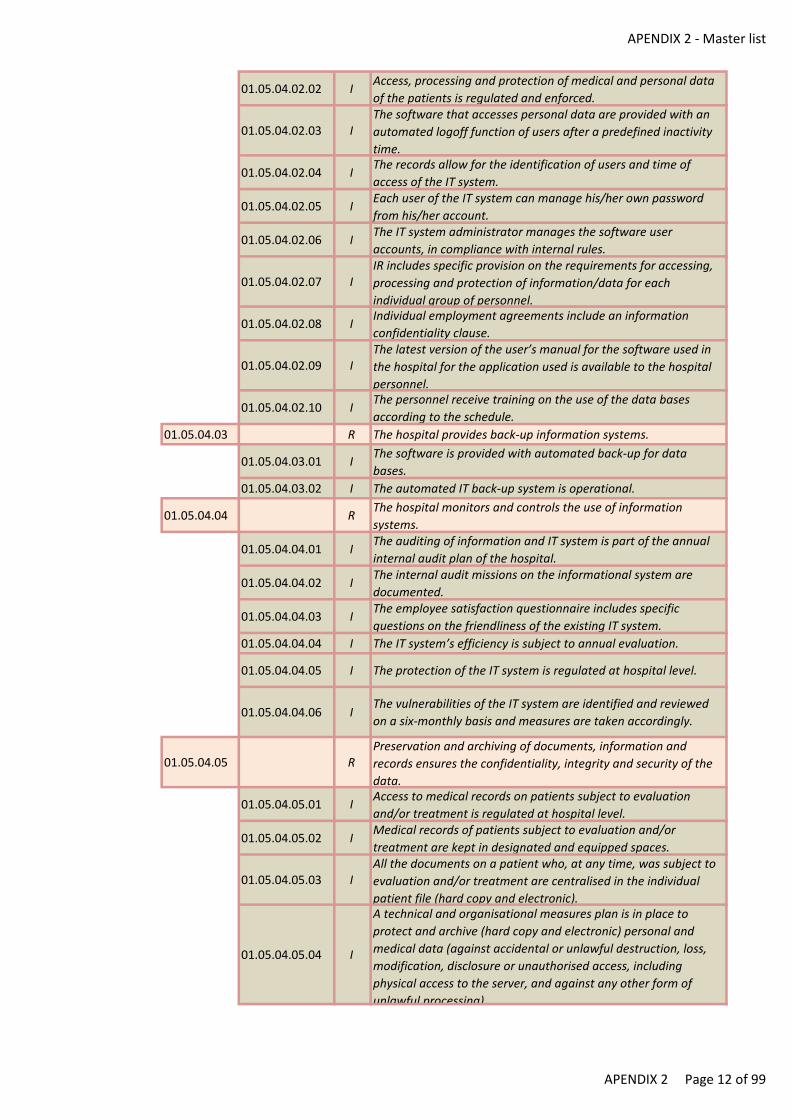
APENDIX 2 - Master list
01.05.04.02.02 IAccess, processing and protection of medical and personal data
of the patients is regulated and enforced.
01.05.04.02.03 IThe software that accesses personal data are provided with an
automated logoff function of users after a predefined inactivity
time.
01.05.04.02.04 IThe records allow for the identification of users and time of
access of the IT system.
01.05.04.02.05 IEach user of the IT system can manage his/her own password
from his/her account.
01.05.04.02.06 IThe IT system administrator manages the software user
accounts, in compliance with internal rules.
01.05.04.02.07 IIR includes specific provision on the requirements for accessing,
processing and protection of information/data for each
individual group of personnel.
01.05.04.02.08 IIndividual employment agreements include an information
confidentiality clause.
01.05.04.02.09 IThe latest version of the user’s manual for the software used in
the hospital for the application used is available to the hospital
personnel.
01.05.04.02.10 IThe personnel receive training on the use of the data bases
according to the schedule.
01.05.04.03 R The hospital provides back-up information systems.
01.05.04.03.01 IThe software is provided with automated back-up for data
bases.
01.05.04.03.02 I The automated IT back-up system is operational.
01.05.04.04 RThe hospital monitors and controls the use of information
systems.
01.05.04.04.01 IThe auditing of information and IT system is part of the annual
internal audit plan of the hospital.
01.05.04.04.02 IThe internal audit missions on the informational system are
documented.
01.05.04.04.03 IThe employee satisfaction questionnaire includes specific
questions on the friendliness of the existing IT system.
01.05.04.04.04 I The IT system’s efficiency is subject to annual evaluation.
01.05.04.04.05 I The protection of the IT system is regulated at hospital level.
01.05.04.04.06 IThe vulnerabilities of the IT system are identified and reviewed
on a six-monthly basis and measures are taken accordingly.
01.05.04.05 RPreservation and archiving of documents, information and
records ensures the confidentiality, integrity and security of the
data.
01.05.04.05.01 IAccess to medical records on patients subject to evaluation
and/or treatment is regulated at hospital level.
01.05.04.05.02 IMedical records of patients subject to evaluation and/or
treatment are kept in designated and equipped spaces.
01.05.04.05.03 IAll the documents on a patient who, at any time, was subject to
evaluation and/or treatment are centralised in the individual
patient file (hard copy and electronic).
01.05.04.05.04 I
A technical and organisational measures plan is in place to
protect and archive (hard copy and electronic) personal and
medical data (against accidental or unlawful destruction, loss,
modification, disclosure or unauthorised access, including
physical access to the server, and against any other form of
unlawful processing).
APENDIX 2 Page 12 of 99
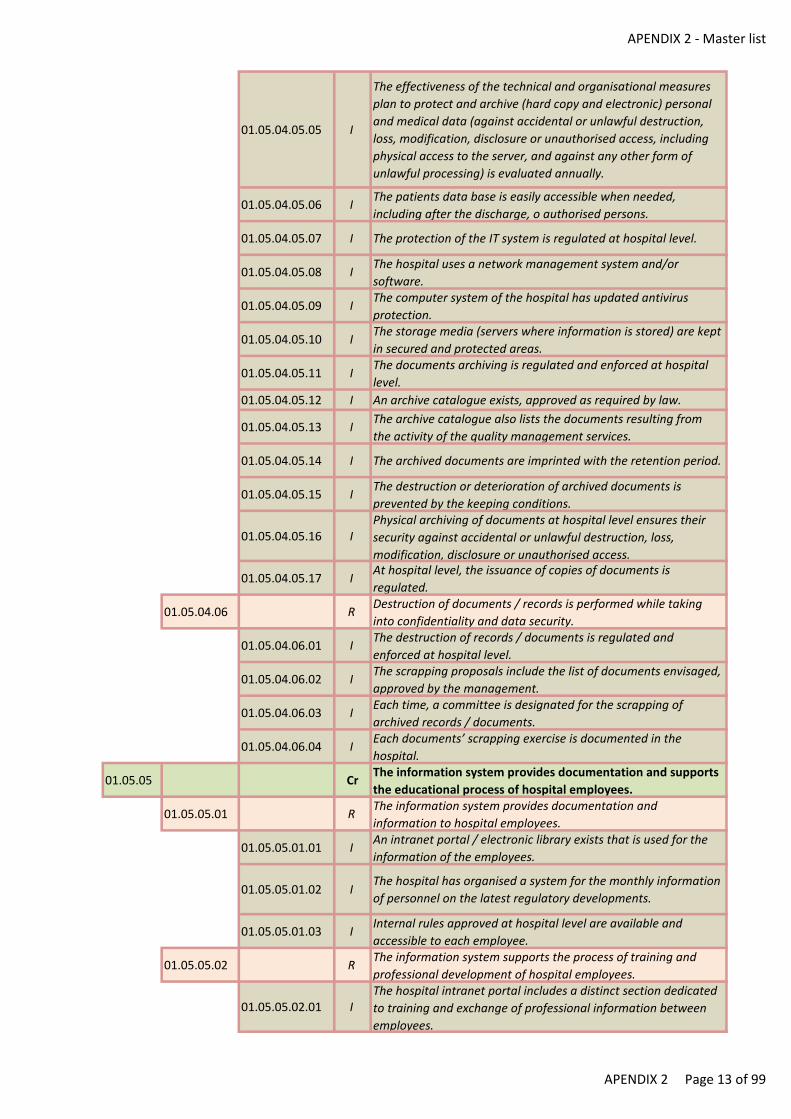
APENDIX 2 - Master list
01.05.04.05.05 I
The effectiveness of the technical and organisational measures
plan to protect and archive (hard copy and electronic) personal
and medical data (against accidental or unlawful destruction,
loss, modification, disclosure or unauthorised access, including
physical access to the server, and against any other form of
unlawful processing) is evaluated annually.
01.05.04.05.06 IThe patients data base is easily accessible when needed,
including after the discharge, o authorised persons.
01.05.04.05.07 I The protection of the IT system is regulated at hospital level.
01.05.04.05.08 IThe hospital uses a network management system and/or
software.
01.05.04.05.09 IThe computer system of the hospital has updated antivirus
protection.
01.05.04.05.10 IThe storage media (servers where information is stored) are kept
in secured and protected areas.
01.05.04.05.11 IThe documents archiving is regulated and enforced at hospital
level.
01.05.04.05.12 I An archive catalogue exists, approved as required by law.
01.05.04.05.13 IThe archive catalogue also lists the documents resulting from
the activity of the quality management services.
01.05.04.05.14 I The archived documents are imprinted with the retention period.
01.05.04.05.15 IThe destruction or deterioration of archived documents is
prevented by the keeping conditions.
01.05.04.05.16 IPhysical archiving of documents at hospital level ensures their
security against accidental or unlawful destruction, loss,
modification, disclosure or unauthorised access.
01.05.04.05.17 IAt hospital level, the issuance of copies of documents is
regulated.
01.05.04.06 RDestruction of documents / records is performed while taking
into confidentiality and data security.
01.05.04.06.01 IThe destruction of records / documents is regulated and
enforced at hospital level.
01.05.04.06.02 IThe scrapping proposals include the list of documents envisaged,
approved by the management.
01.05.04.06.03 IEach time, a committee is designated for the scrapping of
archived records / documents.
01.05.04.06.04 IEach documents’ scrapping exercise is documented in the
hospital.
01.05.05 CrThe information system provides documentation and supports
the educational process of hospital employees.
01.05.05.01 RThe information system provides documentation and
information to hospital employees.
01.05.05.01.01 IAn intranet portal / electronic library exists that is used for the
information of the employees.
01.05.05.01.02 IThe hospital has organised a system for the monthly information
of personnel on the latest regulatory developments.
01.05.05.01.03 IInternal rules approved at hospital level are available and
accessible to each employee.
01.05.05.02 RThe information system supports the process of training and
professional development of hospital employees.
01.05.05.02.01 IThe hospital intranet portal includes a distinct section dedicated
to training and exchange of professional information between
employees.
APENDIX 2 Page 13 of 99
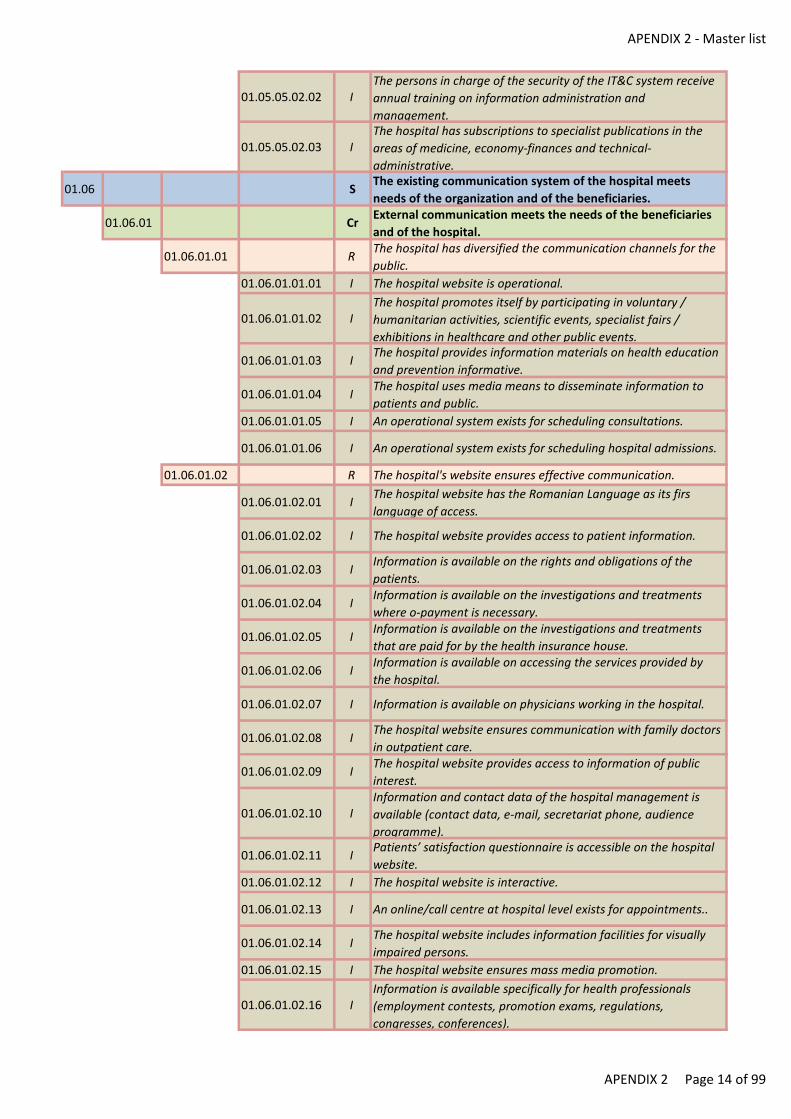
APENDIX 2 - Master list
01.05.05.02.02 IThe persons in charge of the security of the IT&C system receive
annual training on information administration and
management.
01.05.05.02.03 IThe hospital has subscriptions to specialist publications in the
areas of medicine, economy-finances and technical-
administrative.
01.06 SThe existing communication system of the hospital meets
needs of the organization and of the beneficiaries.
01.06.01 CrExternal communication meets the needs of the beneficiaries
and of the hospital.
01.06.01.01 RThe hospital has diversified the communication channels for the
public.
01.06.01.01.01 I The hospital website is operational.
01.06.01.01.02 IThe hospital promotes itself by participating in voluntary /
humanitarian activities, scientific events, specialist fairs /
exhibitions in healthcare and other public events.
01.06.01.01.03 IThe hospital provides information materials on health education
and prevention informative.
01.06.01.01.04 IThe hospital uses media means to disseminate information to
patients and public.
01.06.01.01.05 I An operational system exists for scheduling consultations.
01.06.01.01.06 I An operational system exists for scheduling hospital admissions.
01.06.01.02 R The hospital's website ensures effective communication.
01.06.01.02.01 IThe hospital website has the Romanian Language as its firs
language of access.
01.06.01.02.02 I The hospital website provides access to patient information.
01.06.01.02.03 IInformation is available on the rights and obligations of the
patients.
01.06.01.02.04 IInformation is available on the investigations and treatments
where o-payment is necessary.
01.06.01.02.05 IInformation is available on the investigations and treatments
that are paid for by the health insurance house.
01.06.01.02.06 IInformation is available on accessing the services provided by
the hospital.
01.06.01.02.07 I Information is available on physicians working in the hospital.
01.06.01.02.08 IThe hospital website ensures communication with family doctors
in outpatient care.
01.06.01.02.09 IThe hospital website provides access to information of public
interest.
01.06.01.02.10 IInformation and contact data of the hospital management is
available (contact data, e-mail, secretariat phone, audience
programme).
01.06.01.02.11 IPatients’ satisfaction questionnaire is accessible on the hospital
website.
01.06.01.02.12 I The hospital website is interactive.
01.06.01.02.13 I An online/call centre at hospital level exists for appointments..
01.06.01.02.14 IThe hospital website includes information facilities for visually
impaired persons.
01.06.01.02.15 I The hospital website ensures mass media promotion.
01.06.01.02.16 IInformation is available specifically for health professionals
(employment contests, promotion exams, regulations,
congresses, conferences).
APENDIX 2 Page 14 of 99
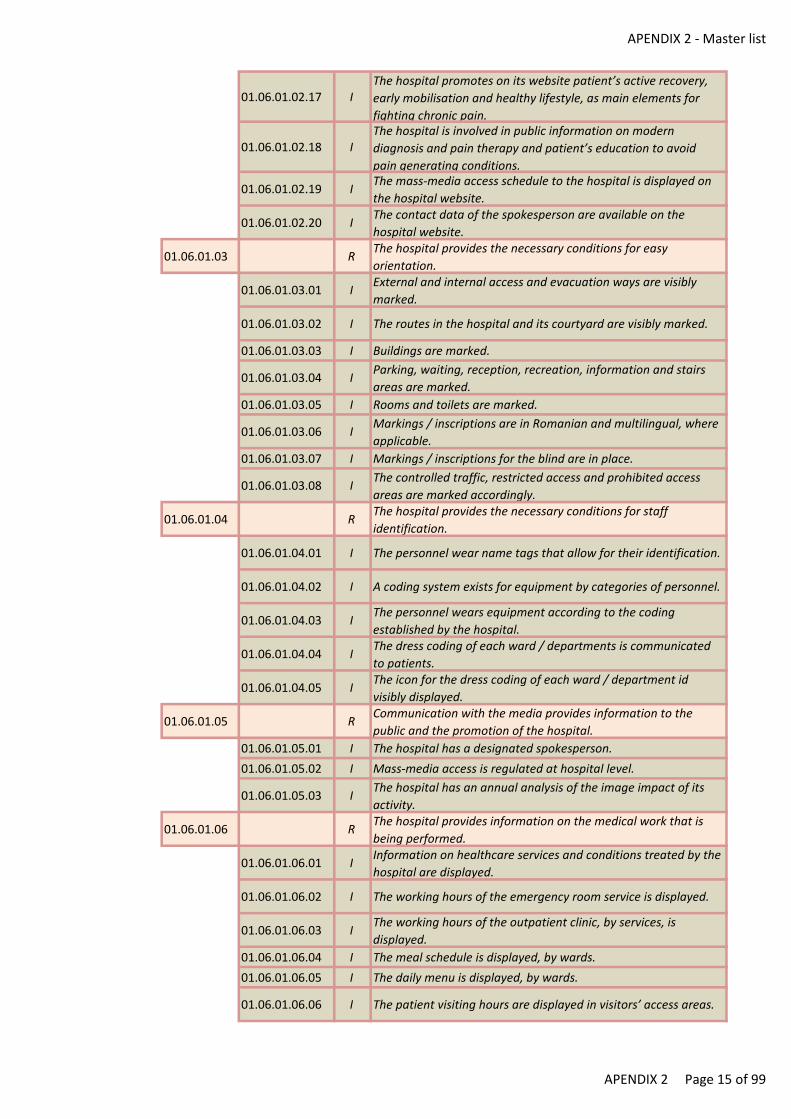
APENDIX 2 - Master list
01.06.01.02.17 IThe hospital promotes on its website patient’s active recovery,
early mobilisation and healthy lifestyle, as main elements for
fighting chronic pain.
01.06.01.02.18 IThe hospital is involved in public information on modern
diagnosis and pain therapy and patient’s education to avoid
pain generating conditions.
01.06.01.02.19 IThe mass-media access schedule to the hospital is displayed on
the hospital website.
01.06.01.02.20 IThe contact data of the spokesperson are available on the
hospital website.
01.06.01.03 RThe hospital provides the necessary conditions for easy
orientation.
01.06.01.03.01 IExternal and internal access and evacuation ways are visibly
marked.
01.06.01.03.02 I The routes in the hospital and its courtyard are visibly marked.
01.06.01.03.03 I Buildings are marked.
01.06.01.03.04 IParking, waiting, reception, recreation, information and stairs
areas are marked.
01.06.01.03.05 I Rooms and toilets are marked.
01.06.01.03.06 IMarkings / inscriptions are in Romanian and multilingual, where
applicable.
01.06.01.03.07 I Markings / inscriptions for the blind are in place.
01.06.01.03.08 IThe controlled traffic, restricted access and prohibited access
areas are marked accordingly.
01.06.01.04 RThe hospital provides the necessary conditions for staff
identification.
01.06.01.04.01 I The personnel wear name tags that allow for their identification.
01.06.01.04.02 I A coding system exists for equipment by categories of personnel.
01.06.01.04.03 IThe personnel wears equipment according to the coding
established by the hospital.
01.06.01.04.04 IThe dress coding of each ward / departments is communicated
to patients.
01.06.01.04.05 IThe icon for the dress coding of each ward / department id
visibly displayed.
01.06.01.05 RCommunication with the media provides information to the
public and the promotion of the hospital.
01.06.01.05.01 I The hospital has a designated spokesperson.
01.06.01.05.02 I Mass-media access is regulated at hospital level.
01.06.01.05.03 IThe hospital has an annual analysis of the image impact of its
activity.
01.06.01.06 RThe hospital provides information on the medical work that is
being performed.
01.06.01.06.01 IInformation on healthcare services and conditions treated by the
hospital are displayed.
01.06.01.06.02 I The working hours of the emergency room service is displayed.
01.06.01.06.03 IThe working hours of the outpatient clinic, by services, is
displayed.
01.06.01.06.04 I The meal schedule is displayed, by wards.
01.06.01.06.05 I The daily menu is displayed, by wards.
01.06.01.06.06 I The patient visiting hours are displayed in visitors’ access areas.
APENDIX 2 Page 15 of 99

APENDIX 2 - Master list
01.06.01.07 RExternal communication is achieved with the continuity of the
healthcare process.
01.06.01.07.01 IThe hospital records patients/relatives’ contact data, with their
agreement, as applicable.
01.06.01.07.02 IRecords are available of the physicians and medical and related
services in the area.
01.06.01.07.03 IThe lists of suppliers in the area that provide recovery, home
care and palliative healthcare services is displayed.
01.06.01.07.04 IThe hospital ensures physicians’ access to the electronic file of
the patient (DES).
01.06.01.08 RThe hospital ensures communication with other healthcare units
and administrative structures.
01.06.01.08.01 IThe hospital is involved in partnerships for the education of
patients/attendants/relatives.
01.06.01.08.02 IA list of healthcare establishments and administrative units with
which the hospital cooperates is available.
01.06.01.08.03 IThe situations are identified where communication with other
healthcare establishments and administrative units is required.
01.06.01.08.04 IMethods for communication with other healthcare
establishments and administrative units are established,
depending on the situation.
01.06.01.08.05 IThe hospital ensures the permanent operation of the
infrastructure required for consulting with external medical staff
extern.
01.06.01.08.06 IThe hospital has a functional infrastructure for external
interpersonal communication – telemedicine.
01.06.01.08.07 I
Based on a schedule and as and when needed, the hospital
provides information to healthcare establishments in the
catchment area on its level of competence and capacity to treat
patients.
01.06.01.08.08 IThe institutionalised communication channels with patients’
associations are operational.
01.06.02 CrInternal communication responds to the needs of the patients
and of the hospital.
01.06.02.01 RThe hospital has implemented models of professional
communication between medical team members.
01.06.02.01.01 IThe methods for communication between the members of the
medical teams are regulated at hospital level.
01.06.02.01.02 IInterpersonal communication of employees is included in the
annual personnel evaluation criteria.
01.06.02.02 RThe hospital has established and uses specific communication
protocols between professionals.
01.06.02.02.01 IMedical risk situations that require specific communication are
defined.
01.06.02.02.02 IPriority communication of investigations’ results and/or need for
treatment / intervention in cases when a patient’s life is in
danger is regulated at hospital level.
01.06.02.02.03 ICommunication in risk / crisis situations is regulated at hospital
level.
01.06.02.03 RThe internal rules are communicated to the staff and to the
patients.
01.06.02.03.01 IRules of conduct in the emergency room are displayed are
displayed in areas accessible to patients/relatives.
01.06.02.03.02 IRights and obligations of the patient are legibly printed and
displayed in areas accessible to patients/relatives at emergency
room.
APENDIX 2 Page 16 of 99
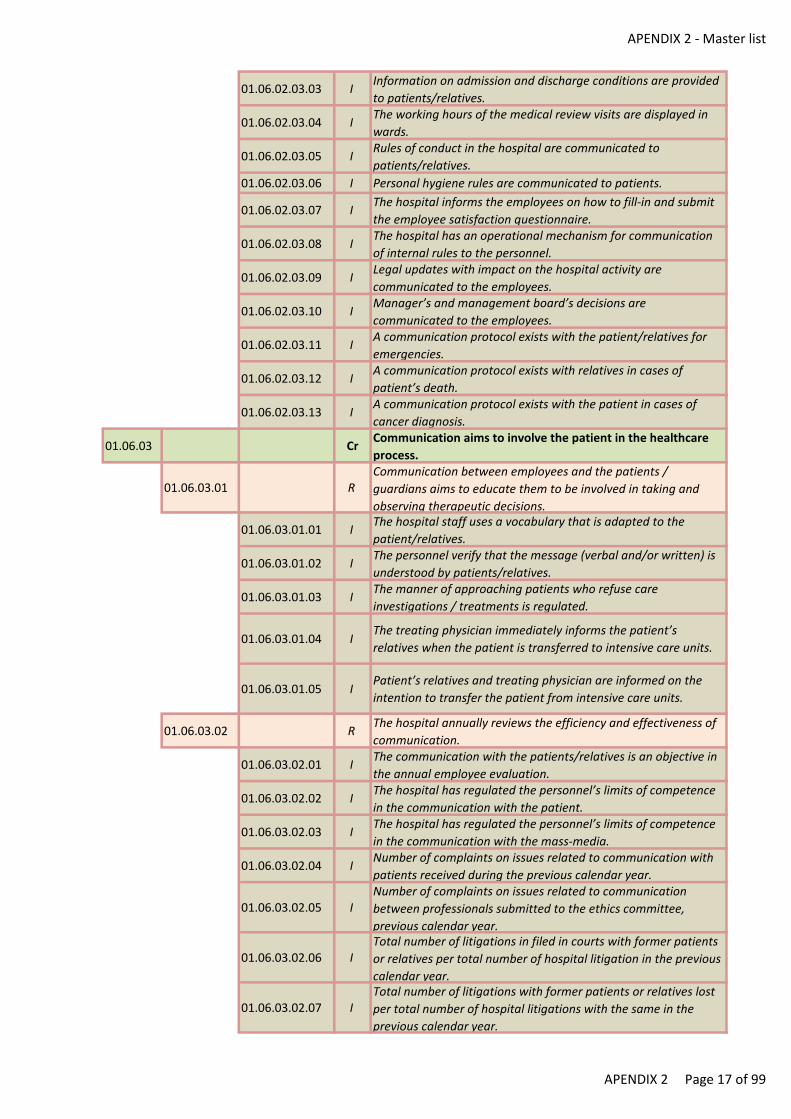
APENDIX 2 - Master list
01.06.02.03.03 IInformation on admission and discharge conditions are provided
to patients/relatives.
01.06.02.03.04 IThe working hours of the medical review visits are displayed in
wards.
01.06.02.03.05 IRules of conduct in the hospital are communicated to
patients/relatives.
01.06.02.03.06 I Personal hygiene rules are communicated to patients.
01.06.02.03.07 IThe hospital informs the employees on how to fill-in and submit
the employee satisfaction questionnaire.
01.06.02.03.08 IThe hospital has an operational mechanism for communication
of internal rules to the personnel.
01.06.02.03.09 ILegal updates with impact on the hospital activity are
communicated to the employees.
01.06.02.03.10 IManager’s and management board’s decisions are
communicated to the employees.
01.06.02.03.11 IA communication protocol exists with the patient/relatives for
emergencies.
01.06.02.03.12 IA communication protocol exists with relatives in cases of
patient’s death.
01.06.02.03.13 IA communication protocol exists with the patient in cases of
cancer diagnosis.
01.06.03 CrCommunication aims to involve the patient in the healthcare
process.
01.06.03.01 RCommunication between employees and the patients /
guardians aims to educate them to be involved in taking and
observing therapeutic decisions.
01.06.03.01.01 IThe hospital staff uses a vocabulary that is adapted to the
patient/relatives.
01.06.03.01.02 IThe personnel verify that the message (verbal and/or written) is
understood by patients/relatives.
01.06.03.01.03 IThe manner of approaching patients who refuse care
investigations / treatments is regulated.
01.06.03.01.04 IThe treating physician immediately informs the patient’s
relatives when the patient is transferred to intensive care units.
01.06.03.01.05 IPatient’s relatives and treating physician are informed on the
intention to transfer the patient from intensive care units.
01.06.03.02 RThe hospital annually reviews the efficiency and effectiveness of
communication.
01.06.03.02.01 IThe communication with the patients/relatives is an objective in
the annual employee evaluation.
01.06.03.02.02 IThe hospital has regulated the personnel’s limits of competence
in the communication with the patient.
01.06.03.02.03 IThe hospital has regulated the personnel’s limits of competence
in the communication with the mass-media.
01.06.03.02.04 INumber of complaints on issues related to communication with
patients received during the previous calendar year.
01.06.03.02.05 INumber of complaints on issues related to communication
between professionals submitted to the ethics committee,
previous calendar year.
01.06.03.02.06 ITotal number of litigations in filed in courts with former patients
or relatives per total number of hospital litigation in the previous
calendar year.
01.06.03.02.07 ITotal number of litigations with former patients or relatives lost
per total number of hospital litigations with the same in the
previous calendar year.
APENDIX 2 Page 17 of 99
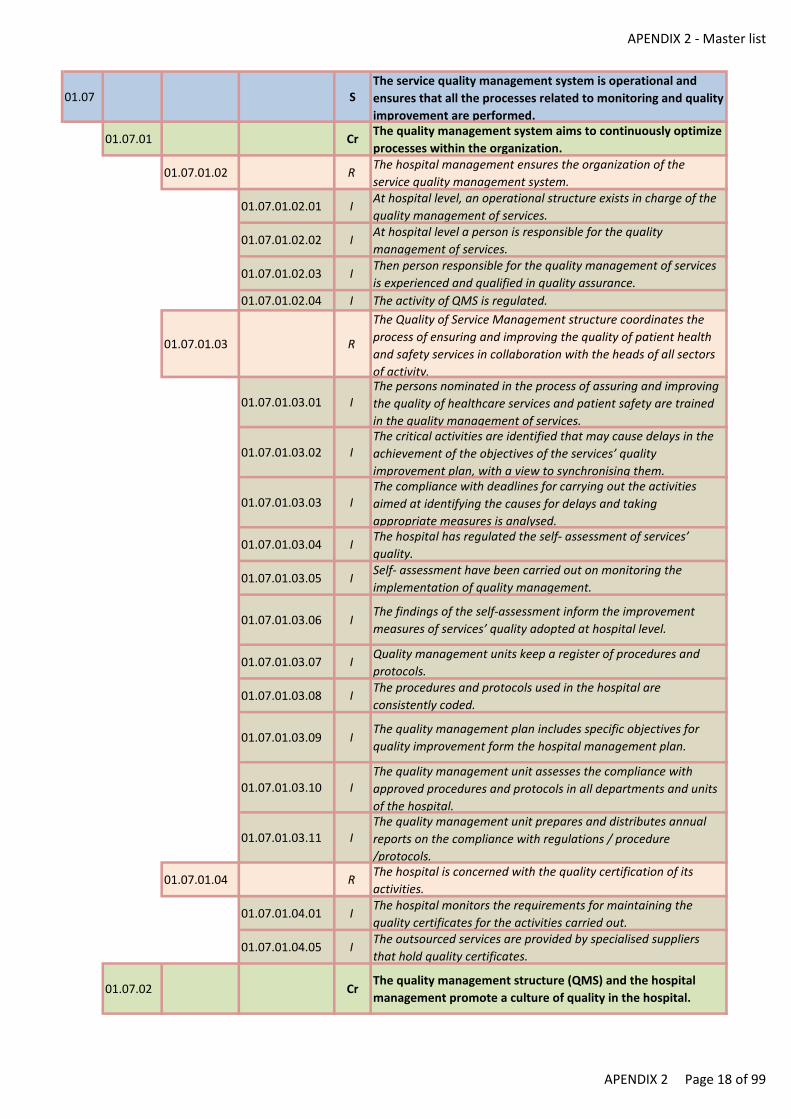
APENDIX 2 - Master list
01.07 SThe service quality management system is operational and
ensures that all the processes related to monitoring and quality
improvement are performed.
01.07.01 CrThe quality management system aims to continuously optimize
processes within the organization.
01.07.01.02 RThe hospital management ensures the organization of the
service quality management system.
01.07.01.02.01 IAt hospital level, an operational structure exists in charge of the
quality management of services.
01.07.01.02.02 IAt hospital level a person is responsible for the quality
management of services.
01.07.01.02.03 IThen person responsible for the quality management of services
is experienced and qualified in quality assurance.
01.07.01.02.04 I The activity of QMS is regulated.
01.07.01.03 R
The Quality of Service Management structure coordinates the
process of ensuring and improving the quality of patient health
and safety services in collaboration with the heads of all sectors
of activity.
01.07.01.03.01 IThe persons nominated in the process of assuring and improving
the quality of healthcare services and patient safety are trained
in the quality management of services.
01.07.01.03.02 IThe critical activities are identified that may cause delays in the
achievement of the objectives of the services’ quality
improvement plan, with a view to synchronising them.
01.07.01.03.03 IThe compliance with deadlines for carrying out the activities
aimed at identifying the causes for delays and taking
appropriate measures is analysed.
01.07.01.03.04 IThe hospital has regulated the self- assessment of services’
quality.
01.07.01.03.05 ISelf- assessment have been carried out on monitoring the
implementation of quality management.
01.07.01.03.06 IThe findings of the self-assessment inform the improvement
measures of services’ quality adopted at hospital level.
01.07.01.03.07 IQuality management units keep a register of procedures and
protocols.
01.07.01.03.08 IThe procedures and protocols used in the hospital are
consistently coded.
01.07.01.03.09 IThe quality management plan includes specific objectives for
quality improvement form the hospital management plan.
01.07.01.03.10 IThe quality management unit assesses the compliance with
approved procedures and protocols in all departments and units
of the hospital.
01.07.01.03.11 IThe quality management unit prepares and distributes annual
reports on the compliance with regulations / procedure
/protocols.
01.07.01.04 RThe hospital is concerned with the quality certification of its
activities.
01.07.01.04.01 IThe hospital monitors the requirements for maintaining the
quality certificates for the activities carried out.
01.07.01.04.05 IThe outsourced services are provided by specialised suppliers
that hold quality certificates.
01.07.02 CrThe quality management structure (QMS) and the hospital
management promote a culture of quality in the hospital.
APENDIX 2 Page 18 of 99
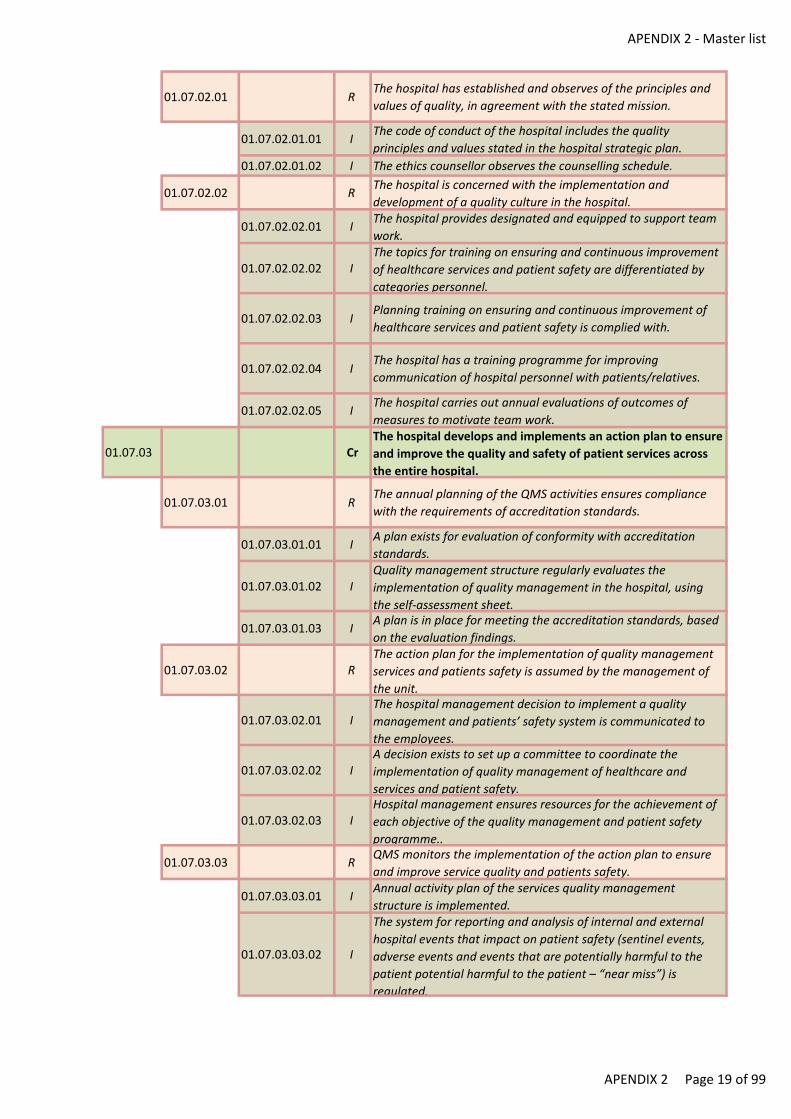
APENDIX 2 - Master list
01.07.02.01 RThe hospital has established and observes of the principles and
values of quality, in agreement with the stated mission.
01.07.02.01.01 IThe code of conduct of the hospital includes the quality
principles and values stated in the hospital strategic plan.
01.07.02.01.02 I The ethics counsellor observes the counselling schedule.
01.07.02.02 RThe hospital is concerned with the implementation and
development of a quality culture in the hospital.
01.07.02.02.01 IThe hospital provides designated and equipped to support team
work.
01.07.02.02.02 IThe topics for training on ensuring and continuous improvement
of healthcare services and patient safety are differentiated by
categories personnel.
01.07.02.02.03 IPlanning training on ensuring and continuous improvement of
healthcare services and patient safety is complied with.
01.07.02.02.04 IThe hospital has a training programme for improving
communication of hospital personnel with patients/relatives.
01.07.02.02.05 IThe hospital carries out annual evaluations of outcomes of
measures to motivate team work.
01.07.03 CrThe hospital develops and implements an action plan to ensure
and improve the quality and safety of patient services across
the entire hospital.
01.07.03.01 RThe annual planning of the QMS activities ensures compliance
with the requirements of accreditation standards.
01.07.03.01.01 IA plan exists for evaluation of conformity with accreditation
standards.
01.07.03.01.02 IQuality management structure regularly evaluates the
implementation of quality management in the hospital, using
the self-assessment sheet.
01.07.03.01.03 IA plan is in place for meeting the accreditation standards, based
on the evaluation findings.
01.07.03.02 RThe action plan for the implementation of quality management
services and patients safety is assumed by the management of
the unit.
01.07.03.02.01 IThe hospital management decision to implement a quality
management and patients’ safety system is communicated to
the employees.
01.07.03.02.02 IA decision exists to set up a committee to coordinate the
implementation of quality management of healthcare and
services and patient safety.
01.07.03.02.03 IHospital management ensures resources for the achievement of
each objective of the quality management and patient safety
programme..
01.07.03.03 RQMS monitors the implementation of the action plan to ensure
and improve service quality and patients safety.
01.07.03.03.01 IAnnual activity plan of the services quality management
structure is implemented.
01.07.03.03.02 I
The system for reporting and analysis of internal and external
hospital events that impact on patient safety (sentinel events,
adverse events and events that are potentially harmful to the
patient potential harmful to the patient – “near miss”) is
regulated.
APENDIX 2 Page 19 of 99
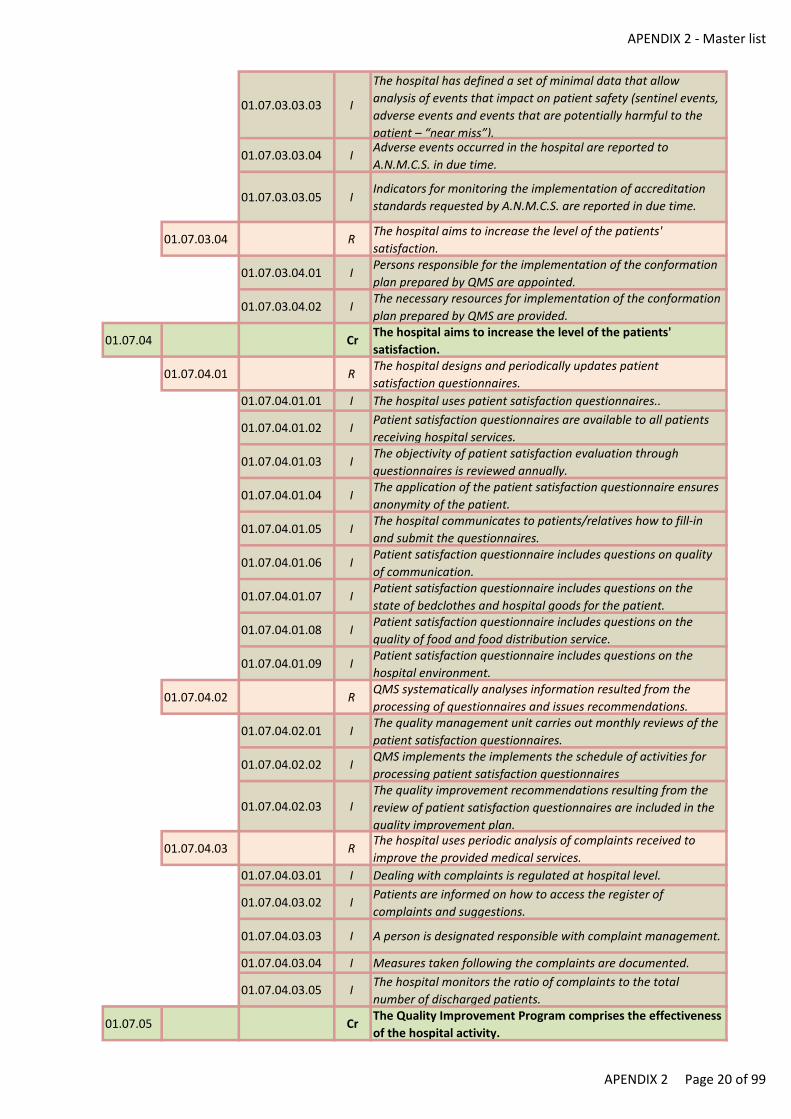
APENDIX 2 - Master list
01.07.03.03.03 I
The hospital has defined a set of minimal data that allow
analysis of events that impact on patient safety (sentinel events,
adverse events and events that are potentially harmful to the
patient – “near miss”).
01.07.03.03.04 IAdverse events occurred in the hospital are reported to
A.N.M.C.S. in due time.
01.07.03.03.05 IIndicators for monitoring the implementation of accreditation
standards requested by A.N.M.C.S. are reported in due time.
01.07.03.04 RThe hospital aims to increase the level of the patients'
satisfaction.
01.07.03.04.01 IPersons responsible for the implementation of the conformation
plan prepared by QMS are appointed.
01.07.03.04.02 IThe necessary resources for implementation of the conformation
plan prepared by QMS are provided.
01.07.04 CrThe hospital aims to increase the level of the patients'
satisfaction.
01.07.04.01 RThe hospital designs and periodically updates patient
satisfaction questionnaires.
01.07.04.01.01 I The hospital uses patient satisfaction questionnaires..
01.07.04.01.02 IPatient satisfaction questionnaires are available to all patients
receiving hospital services.
01.07.04.01.03 IThe objectivity of patient satisfaction evaluation through
questionnaires is reviewed annually.
01.07.04.01.04 IThe application of the patient satisfaction questionnaire ensures
anonymity of the patient.
01.07.04.01.05 IThe hospital communicates to patients/relatives how to fill-in
and submit the questionnaires.
01.07.04.01.06 IPatient satisfaction questionnaire includes questions on quality
of communication.
01.07.04.01.07 IPatient satisfaction questionnaire includes questions on the
state of bedclothes and hospital goods for the patient.
01.07.04.01.08 IPatient satisfaction questionnaire includes questions on the
quality of food and food distribution service.
01.07.04.01.09 IPatient satisfaction questionnaire includes questions on the
hospital environment.
01.07.04.02 RQMS systematically analyses information resulted from the
processing of questionnaires and issues recommendations.
01.07.04.02.01 IThe quality management unit carries out monthly reviews of the
patient satisfaction questionnaires.
01.07.04.02.02 IQMS implements the implements the schedule of activities for
processing patient satisfaction questionnaires
01.07.04.02.03 IThe quality improvement recommendations resulting from the
review of patient satisfaction questionnaires are included in the
quality improvement plan.
01.07.04.03 RThe hospital uses periodic analysis of complaints received to
improve the provided medical services.
01.07.04.03.01 I Dealing with complaints is regulated at hospital level.
01.07.04.03.02 IPatients are informed on how to access the register of
complaints and suggestions.
01.07.04.03.03 I A person is designated responsible with complaint management.
01.07.04.03.04 I Measures taken following the complaints are documented.
01.07.04.03.05 IThe hospital monitors the ratio of complaints to the total
number of discharged patients.
01.07.05 CrThe Quality Improvement Program comprises the effectiveness
of the hospital activity.
APENDIX 2 Page 20 of 99
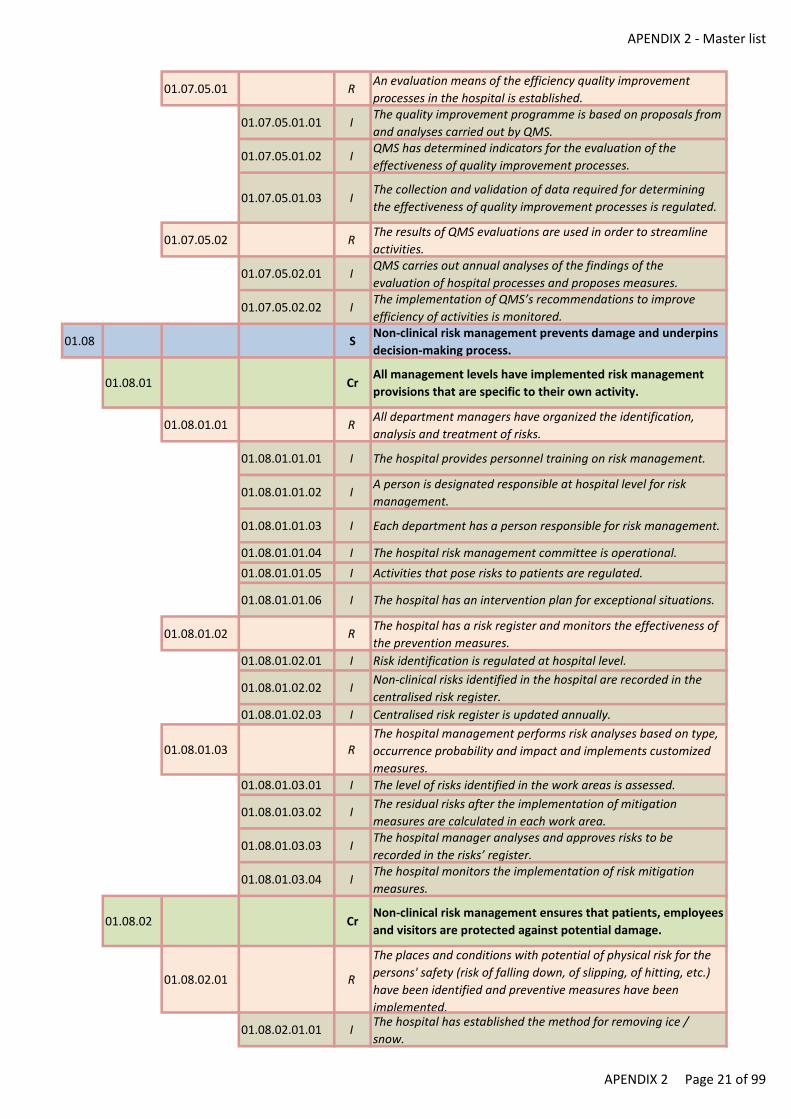
APENDIX 2 - Master list
01.07.05.01 RAn evaluation means of the efficiency quality improvement
processes in the hospital is established.
01.07.05.01.01 IThe quality improvement programme is based on proposals from
and analyses carried out by QMS.
01.07.05.01.02 IQMS has determined indicators for the evaluation of the
effectiveness of quality improvement processes.
01.07.05.01.03 IThe collection and validation of data required for determining
the effectiveness of quality improvement processes is regulated.
01.07.05.02 RThe results of QMS evaluations are used in order to streamline
activities.
01.07.05.02.01 IQMS carries out annual analyses of the findings of the
evaluation of hospital processes and proposes measures.
01.07.05.02.02 IThe implementation of QMS’s recommendations to improve
efficiency of activities is monitored.
01.08 SNon-clinical risk management prevents damage and underpins
decision-making process.
01.08.01 CrAll management levels have implemented risk management
provisions that are specific to their own activity.
01.08.01.01 RAll department managers have organized the identification,
analysis and treatment of risks.
01.08.01.01.01 I The hospital provides personnel training on risk management.
01.08.01.01.02 IA person is designated responsible at hospital level for risk
management.
01.08.01.01.03 I Each department has a person responsible for risk management.
01.08.01.01.04 I The hospital risk management committee is operational.
01.08.01.01.05 I Activities that pose risks to patients are regulated.
01.08.01.01.06 I The hospital has an intervention plan for exceptional situations.
01.08.01.02 RThe hospital has a risk register and monitors the effectiveness of
the prevention measures.
01.08.01.02.01 I Risk identification is regulated at hospital level.
01.08.01.02.02 INon-clinical risks identified in the hospital are recorded in the
centralised risk register.
01.08.01.02.03 I Centralised risk register is updated annually.
01.08.01.03 RThe hospital management performs risk analyses based on type,
occurrence probability and impact and implements customized
measures.
01.08.01.03.01 I The level of risks identified in the work areas is assessed.
01.08.01.03.02 IThe residual risks after the implementation of mitigation
measures are calculated in each work area.
01.08.01.03.03 IThe hospital manager analyses and approves risks to be
recorded in the risks’ register.
01.08.01.03.04 IThe hospital monitors the implementation of risk mitigation
measures.
01.08.02 CrNon-clinical risk management ensures that patients, employees
and visitors are protected against potential damage.
01.08.02.01 R
The places and conditions with potential of physical risk for the
persons' safety (risk of falling down, of slipping, of hitting, etc.)
have been identified and preventive measures have been
implemented.
01.08.02.01.01 IThe hospital has established the method for removing ice /
snow.
APENDIX 2 Page 21 of 99
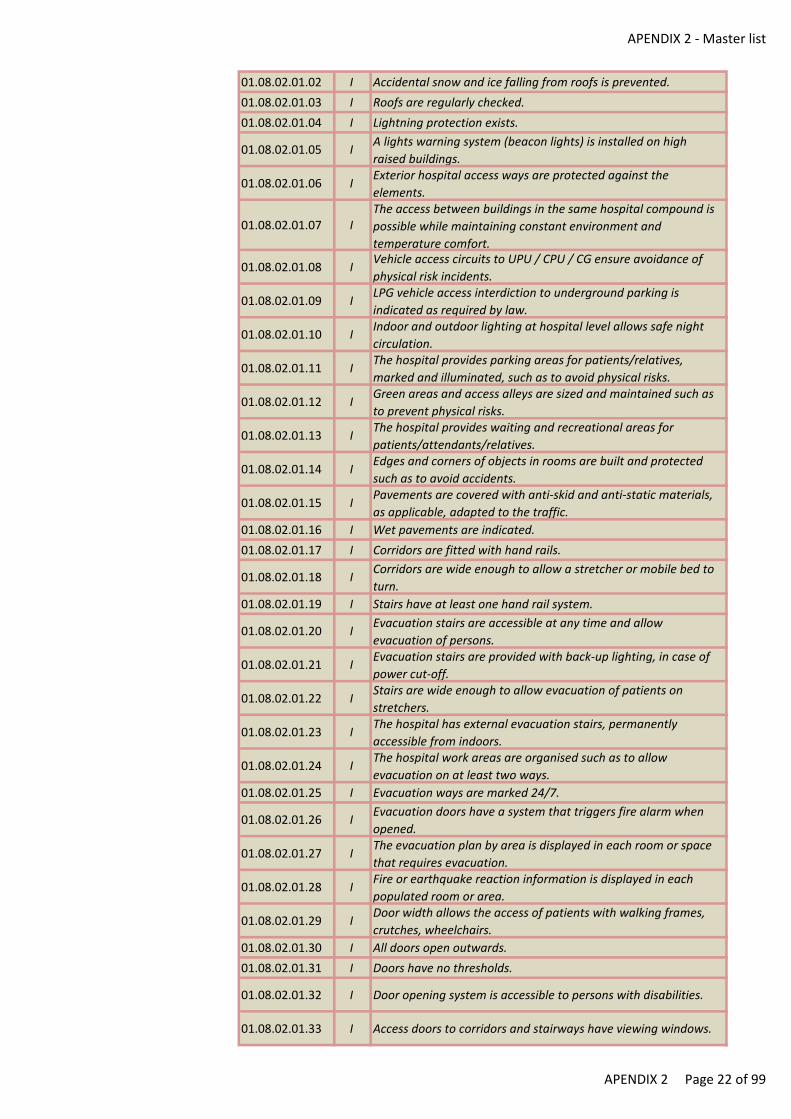
APENDIX 2 - Master list
01.08.02.01.02 I Accidental snow and ice falling from roofs is prevented.
01.08.02.01.03 I Roofs are regularly checked.
01.08.02.01.04 I Lightning protection exists.
01.08.02.01.05 IA lights warning system (beacon lights) is installed on high
raised buildings.
01.08.02.01.06 IExterior hospital access ways are protected against the
elements.
01.08.02.01.07 IThe access between buildings in the same hospital compound is
possible while maintaining constant environment and
temperature comfort.
01.08.02.01.08 IVehicle access circuits to UPU / CPU / CG ensure avoidance of
physical risk incidents.
01.08.02.01.09 ILPG vehicle access interdiction to underground parking is
indicated as required by law.
01.08.02.01.10 IIndoor and outdoor lighting at hospital level allows safe night
circulation.
01.08.02.01.11 IThe hospital provides parking areas for patients/relatives,
marked and illuminated, such as to avoid physical risks.
01.08.02.01.12 IGreen areas and access alleys are sized and maintained such as
to prevent physical risks.
01.08.02.01.13 IThe hospital provides waiting and recreational areas for
patients/attendants/relatives.
01.08.02.01.14 IEdges and corners of objects in rooms are built and protected
such as to avoid accidents.
01.08.02.01.15 IPavements are covered with anti-skid and anti-static materials,
as applicable, adapted to the traffic.
01.08.02.01.16 I Wet pavements are indicated.
01.08.02.01.17 I Corridors are fitted with hand rails.
01.08.02.01.18 ICorridors are wide enough to allow a stretcher or mobile bed to
turn.
01.08.02.01.19 I Stairs have at least one hand rail system.
01.08.02.01.20 IEvacuation stairs are accessible at any time and allow
evacuation of persons.
01.08.02.01.21 IEvacuation stairs are provided with back-up lighting, in case of
power cut-off.
01.08.02.01.22 IStairs are wide enough to allow evacuation of patients on
stretchers.
01.08.02.01.23 IThe hospital has external evacuation stairs, permanently
accessible from indoors.
01.08.02.01.24 IThe hospital work areas are organised such as to allow
evacuation on at least two ways.
01.08.02.01.25 I Evacuation ways are marked 24/7.
01.08.02.01.26 IEvacuation doors have a system that triggers fire alarm when
opened.
01.08.02.01.27 IThe evacuation plan by area is displayed in each room or space
that requires evacuation.
01.08.02.01.28 IFire or earthquake reaction information is displayed in each
populated room or area.
01.08.02.01.29 IDoor width allows the access of patients with walking frames,
crutches, wheelchairs.
01.08.02.01.30 I All doors open outwards.
01.08.02.01.31 I Doors have no thresholds.
01.08.02.01.32 I Door opening system is accessible to persons with disabilities.
01.08.02.01.33 I Access doors to corridors and stairways have viewing windows.
APENDIX 2 Page 22 of 99
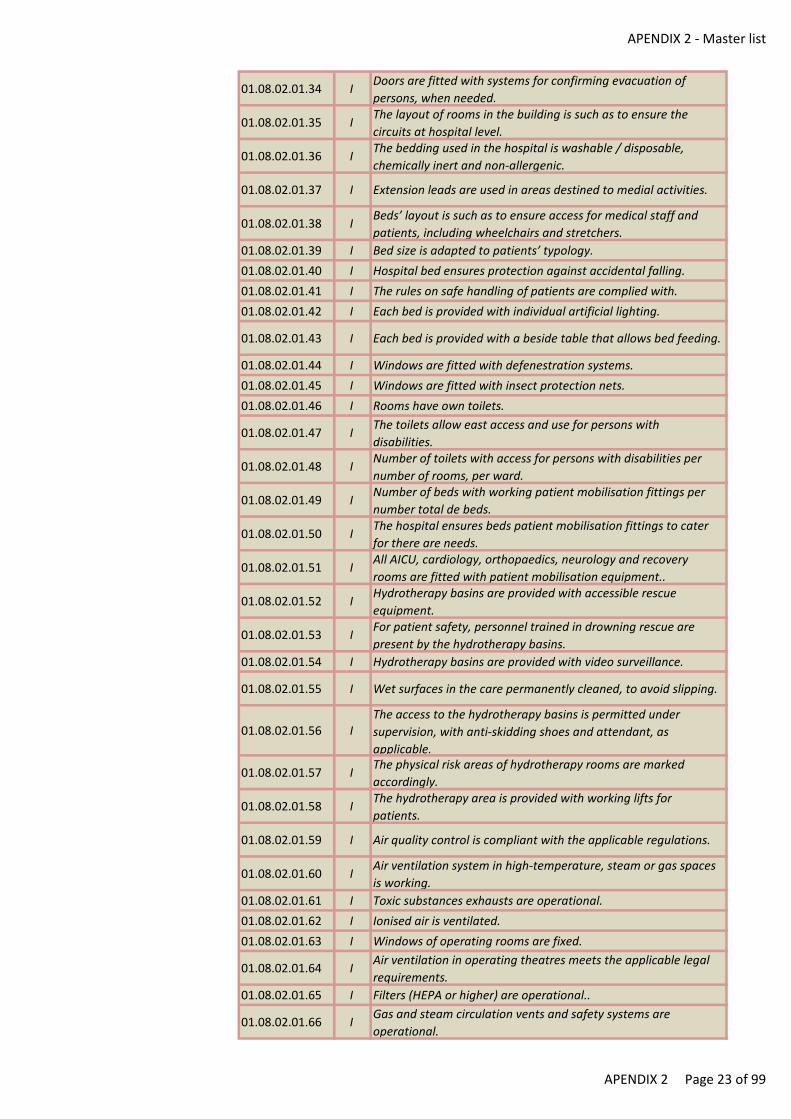
APENDIX 2 - Master list
01.08.02.01.34 IDoors are fitted with systems for confirming evacuation of
persons, when needed.
01.08.02.01.35 IThe layout of rooms in the building is such as to ensure the
circuits at hospital level.
01.08.02.01.36 IThe bedding used in the hospital is washable / disposable,
chemically inert and non-allergenic.
01.08.02.01.37 I Extension leads are used in areas destined to medial activities.
01.08.02.01.38 IBeds’ layout is such as to ensure access for medical staff and
patients, including wheelchairs and stretchers.
01.08.02.01.39 I Bed size is adapted to patients’ typology.
01.08.02.01.40 I Hospital bed ensures protection against accidental falling.
01.08.02.01.41 I The rules on safe handling of patients are complied with.
01.08.02.01.42 I Each bed is provided with individual artificial lighting.
01.08.02.01.43 I Each bed is provided with a beside table that allows bed feeding.
01.08.02.01.44 I Windows are fitted with defenestration systems.
01.08.02.01.45 I Windows are fitted with insect protection nets.
01.08.02.01.46 I Rooms have own toilets.
01.08.02.01.47 IThe toilets allow east access and use for persons with
disabilities.
01.08.02.01.48 INumber of toilets with access for persons with disabilities per
number of rooms, per ward.
01.08.02.01.49 INumber of beds with working patient mobilisation fittings per
number total de beds.
01.08.02.01.50 IThe hospital ensures beds patient mobilisation fittings to cater
for there are needs.
01.08.02.01.51 IAll AICU, cardiology, orthopaedics, neurology and recovery
rooms are fitted with patient mobilisation equipment..
01.08.02.01.52 IHydrotherapy basins are provided with accessible rescue
equipment.
01.08.02.01.53 IFor patient safety, personnel trained in drowning rescue are
present by the hydrotherapy basins.
01.08.02.01.54 I Hydrotherapy basins are provided with video surveillance.
01.08.02.01.55 I Wet surfaces in the care permanently cleaned, to avoid slipping.
01.08.02.01.56 IThe access to the hydrotherapy basins is permitted under
supervision, with anti-skidding shoes and attendant, as
applicable.
01.08.02.01.57 IThe physical risk areas of hydrotherapy rooms are marked
accordingly.
01.08.02.01.58 IThe hydrotherapy area is provided with working lifts for
patients.
01.08.02.01.59 I Air quality control is compliant with the applicable regulations.
01.08.02.01.60 IAir ventilation system in high-temperature, steam or gas spaces
is working.
01.08.02.01.61 I Toxic substances exhausts are operational.
01.08.02.01.62 I Ionised air is ventilated.
01.08.02.01.63 I Windows of operating rooms are fixed.
01.08.02.01.64 IAir ventilation in operating theatres meets the applicable legal
requirements.
01.08.02.01.65 I Filters (HEPA or higher) are operational..
01.08.02.01.66 IGas and steam circulation vents and safety systems are
operational.
APENDIX 2 Page 23 of 99
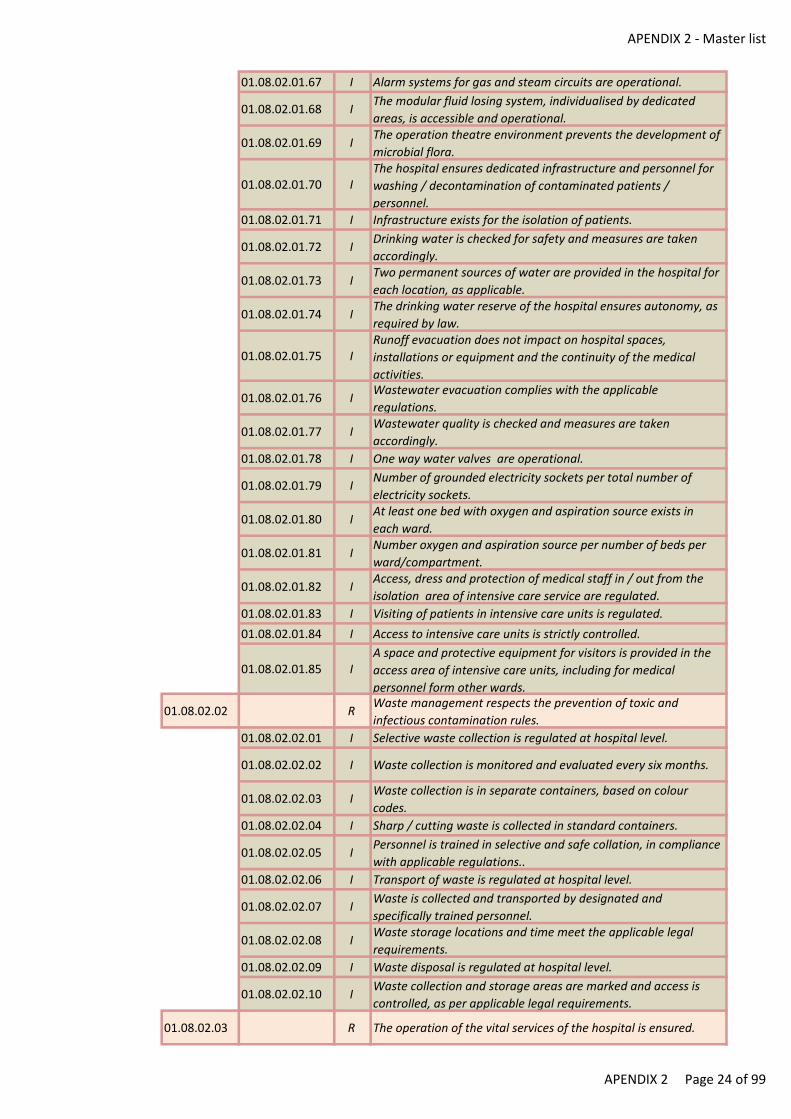
APENDIX 2 - Master list
01.08.02.01.67 I Alarm systems for gas and steam circuits are operational.
01.08.02.01.68 IThe modular fluid losing system, individualised by dedicated
areas, is accessible and operational.
01.08.02.01.69 IThe operation theatre environment prevents the development of
microbial flora.
01.08.02.01.70 IThe hospital ensures dedicated infrastructure and personnel for
washing / decontamination of contaminated patients /
personnel.
01.08.02.01.71 I Infrastructure exists for the isolation of patients.
01.08.02.01.72 IDrinking water is checked for safety and measures are taken
accordingly.
01.08.02.01.73 ITwo permanent sources of water are provided in the hospital for
each location, as applicable.
01.08.02.01.74 IThe drinking water reserve of the hospital ensures autonomy, as
required by law.
01.08.02.01.75 IRunoff evacuation does not impact on hospital spaces,
installations or equipment and the continuity of the medical
activities.
01.08.02.01.76 IWastewater evacuation complies with the applicable
regulations.
01.08.02.01.77 IWastewater quality is checked and measures are taken
accordingly.
01.08.02.01.78 I One way water valves are operational.
01.08.02.01.79 INumber of grounded electricity sockets per total number of
electricity sockets.
01.08.02.01.80 IAt least one bed with oxygen and aspiration source exists in
each ward.
01.08.02.01.81 INumber oxygen and aspiration source per number of beds per
ward/compartment.
01.08.02.01.82 IAccess, dress and protection of medical staff in / out from the
isolation area of intensive care service are regulated.
01.08.02.01.83 I Visiting of patients in intensive care units is regulated.
01.08.02.01.84 I Access to intensive care units is strictly controlled.
01.08.02.01.85 IA space and protective equipment for visitors is provided in the
access area of intensive care units, including for medical
personnel form other wards.
01.08.02.02 RWaste management respects the prevention of toxic and
infectious contamination rules.
01.08.02.02.01 I Selective waste collection is regulated at hospital level.
01.08.02.02.02 I Waste collection is monitored and evaluated every six months.
01.08.02.02.03 IWaste collection is in separate containers, based on colour
codes.
01.08.02.02.04 I Sharp / cutting waste is collected in standard containers.
01.08.02.02.05 IPersonnel is trained in selective and safe collation, in compliance
with applicable regulations..
01.08.02.02.06 I Transport of waste is regulated at hospital level.
01.08.02.02.07 IWaste is collected and transported by designated and
specifically trained personnel.
01.08.02.02.08 IWaste storage locations and time meet the applicable legal
requirements.
01.08.02.02.09 I Waste disposal is regulated at hospital level.
01.08.02.02.10 IWaste collection and storage areas are marked and access is
controlled, as per applicable legal requirements.
01.08.02.03 R The operation of the vital services of the hospital is ensured.
APENDIX 2 Page 24 of 99
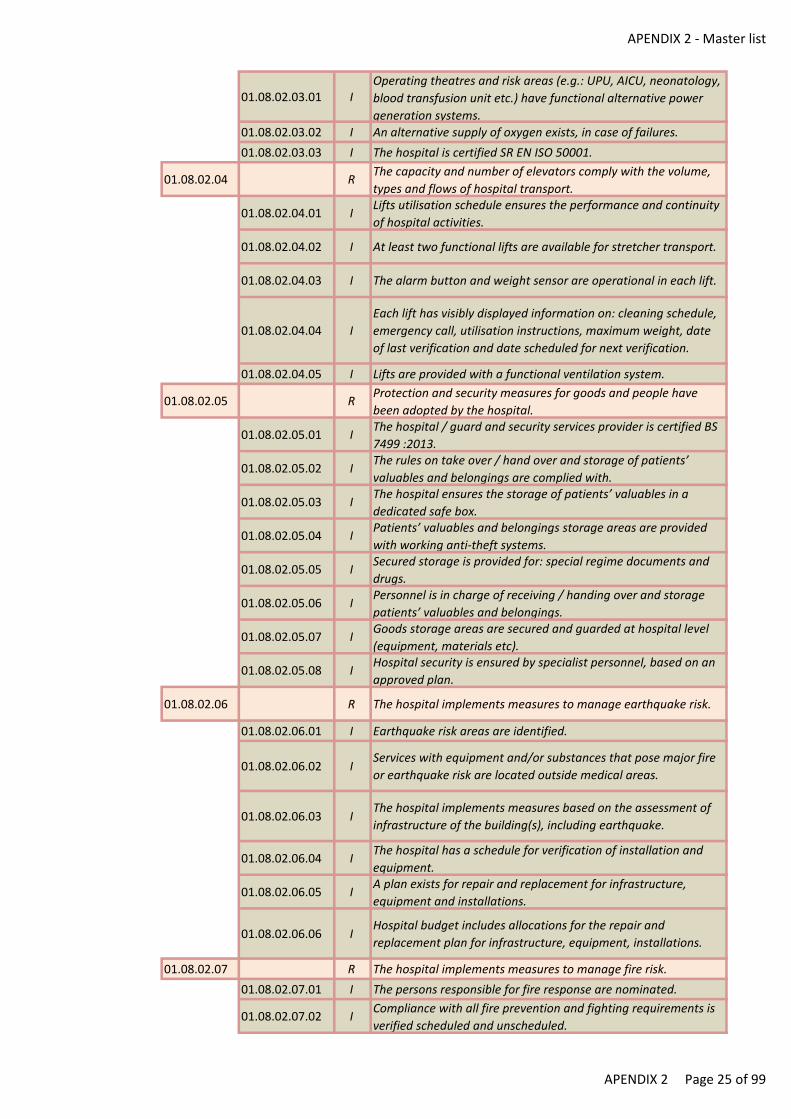
APENDIX 2 - Master list
01.08.02.03.01 IOperating theatres and risk areas (e.g.: UPU, AICU, neonatology,
blood transfusion unit etc.) have functional alternative power
generation systems.
01.08.02.03.02 I An alternative supply of oxygen exists, in case of failures.
01.08.02.03.03 I The hospital is certified SR EN ISO 50001.
01.08.02.04 RThe capacity and number of elevators comply with the volume,
types and flows of hospital transport.
01.08.02.04.01 ILifts utilisation schedule ensures the performance and continuity
of hospital activities.
01.08.02.04.02 I At least two functional lifts are available for stretcher transport.
01.08.02.04.03 I The alarm button and weight sensor are operational in each lift.
01.08.02.04.04 I
Each lift has visibly displayed information on: cleaning schedule,
emergency call, utilisation instructions, maximum weight, date
of last verification and date scheduled for next verification.
01.08.02.04.05 I Lifts are provided with a functional ventilation system.
01.08.02.05 RProtection and security measures for goods and people have
been adopted by the hospital.
01.08.02.05.01 IThe hospital / guard and security services provider is certified BS
7499 :2013.
01.08.02.05.02 IThe rules on take over / hand over and storage of patients’
valuables and belongings are complied with.
01.08.02.05.03 IThe hospital ensures the storage of patients’ valuables in a
dedicated safe box.
01.08.02.05.04 IPatients’ valuables and belongings storage areas are provided
with working anti-theft systems.
01.08.02.05.05 ISecured storage is provided for: special regime documents and
drugs.
01.08.02.05.06 IPersonnel is in charge of receiving / handing over and storage
patients’ valuables and belongings.
01.08.02.05.07 IGoods storage areas are secured and guarded at hospital level
(equipment, materials etc).
01.08.02.05.08 IHospital security is ensured by specialist personnel, based on an
approved plan.
01.08.02.06 R The hospital implements measures to manage earthquake risk.
01.08.02.06.01 I Earthquake risk areas are identified.
01.08.02.06.02 IServices with equipment and/or substances that pose major fire
or earthquake risk are located outside medical areas.
01.08.02.06.03 IThe hospital implements measures based on the assessment of
infrastructure of the building(s), including earthquake.
01.08.02.06.04 IThe hospital has a schedule for verification of installation and
equipment.
01.08.02.06.05 IA plan exists for repair and replacement for infrastructure,
equipment and installations.
01.08.02.06.06 IHospital budget includes allocations for the repair and
replacement plan for infrastructure, equipment, installations.
01.08.02.07 R The hospital implements measures to manage fire risk.
01.08.02.07.01 I The persons responsible for fire response are nominated.
01.08.02.07.02 ICompliance with all fire prevention and fighting requirements is
verified scheduled and unscheduled.
APENDIX 2 Page 25 of 99
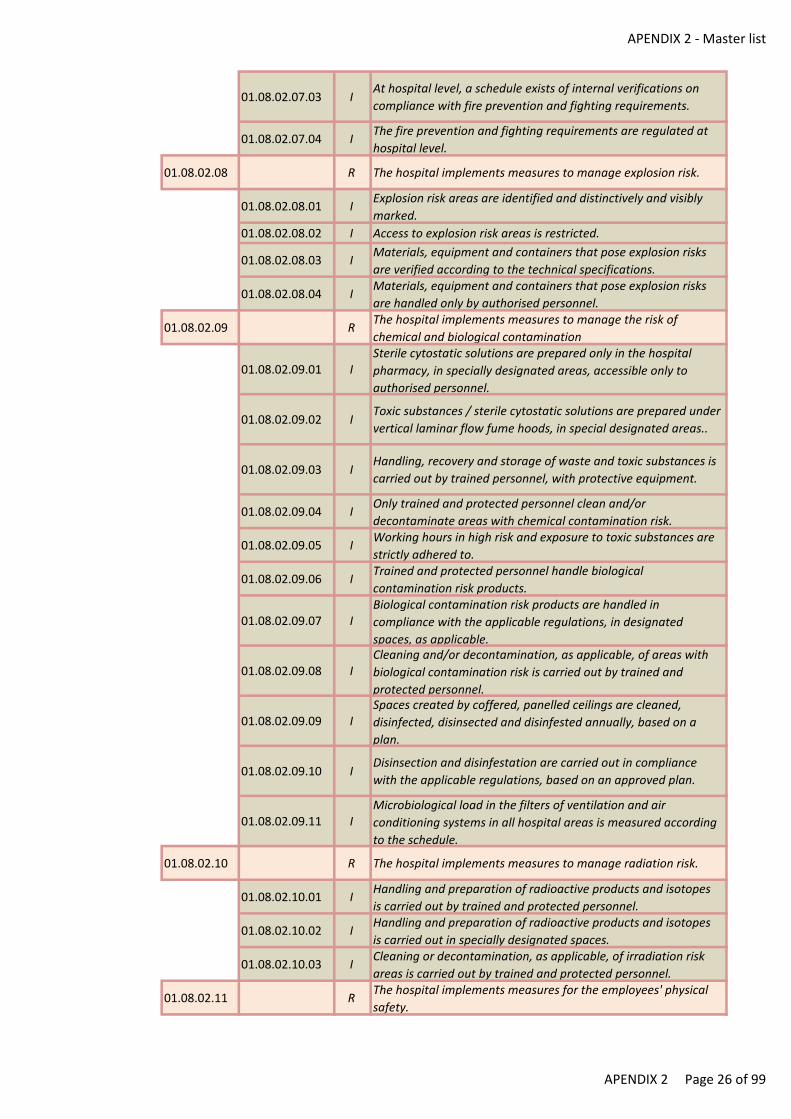
APENDIX 2 - Master list
01.08.02.07.03 IAt hospital level, a schedule exists of internal verifications on
compliance with fire prevention and fighting requirements.
01.08.02.07.04 IThe fire prevention and fighting requirements are regulated at
hospital level.
01.08.02.08 R The hospital implements measures to manage explosion risk.
01.08.02.08.01 IExplosion risk areas are identified and distinctively and visibly
marked.
01.08.02.08.02 I Access to explosion risk areas is restricted.
01.08.02.08.03 IMaterials, equipment and containers that pose explosion risks
are verified according to the technical specifications.
01.08.02.08.04 IMaterials, equipment and containers that pose explosion risks
are handled only by authorised personnel.
01.08.02.09 RThe hospital implements measures to manage the risk of
chemical and biological contamination
01.08.02.09.01 ISterile cytostatic solutions are prepared only in the hospital
pharmacy, in specially designated areas, accessible only to
authorised personnel.
01.08.02.09.02 IToxic substances / sterile cytostatic solutions are prepared under
vertical laminar flow fume hoods, in special designated areas..
01.08.02.09.03 IHandling, recovery and storage of waste and toxic substances is
carried out by trained personnel, with protective equipment.
01.08.02.09.04 IOnly trained and protected personnel clean and/or
decontaminate areas with chemical contamination risk.
01.08.02.09.05 IWorking hours in high risk and exposure to toxic substances are
strictly adhered to.
01.08.02.09.06 ITrained and protected personnel handle biological
contamination risk products.
01.08.02.09.07 IBiological contamination risk products are handled in
compliance with the applicable regulations, in designated
spaces, as applicable.
01.08.02.09.08 ICleaning and/or decontamination, as applicable, of areas with
biological contamination risk is carried out by trained and
protected personnel.
01.08.02.09.09 ISpaces created by coffered, panelled ceilings are cleaned,
disinfected, disinsected and disinfested annually, based on a
plan.
01.08.02.09.10 IDisinsection and disinfestation are carried out in compliance
with the applicable regulations, based on an approved plan.
01.08.02.09.11 IMicrobiological load in the filters of ventilation and air
conditioning systems in all hospital areas is measured according
to the schedule.
01.08.02.10 R The hospital implements measures to manage radiation risk.
01.08.02.10.01 IHandling and preparation of radioactive products and isotopes
is carried out by trained and protected personnel.
01.08.02.10.02 IHandling and preparation of radioactive products and isotopes
is carried out in specially designated spaces.
01.08.02.10.03 ICleaning or decontamination, as applicable, of irradiation risk
areas is carried out by trained and protected personnel.
01.08.02.11 RThe hospital implements measures for the employees' physical
safety.
APENDIX 2 Page 26 of 99
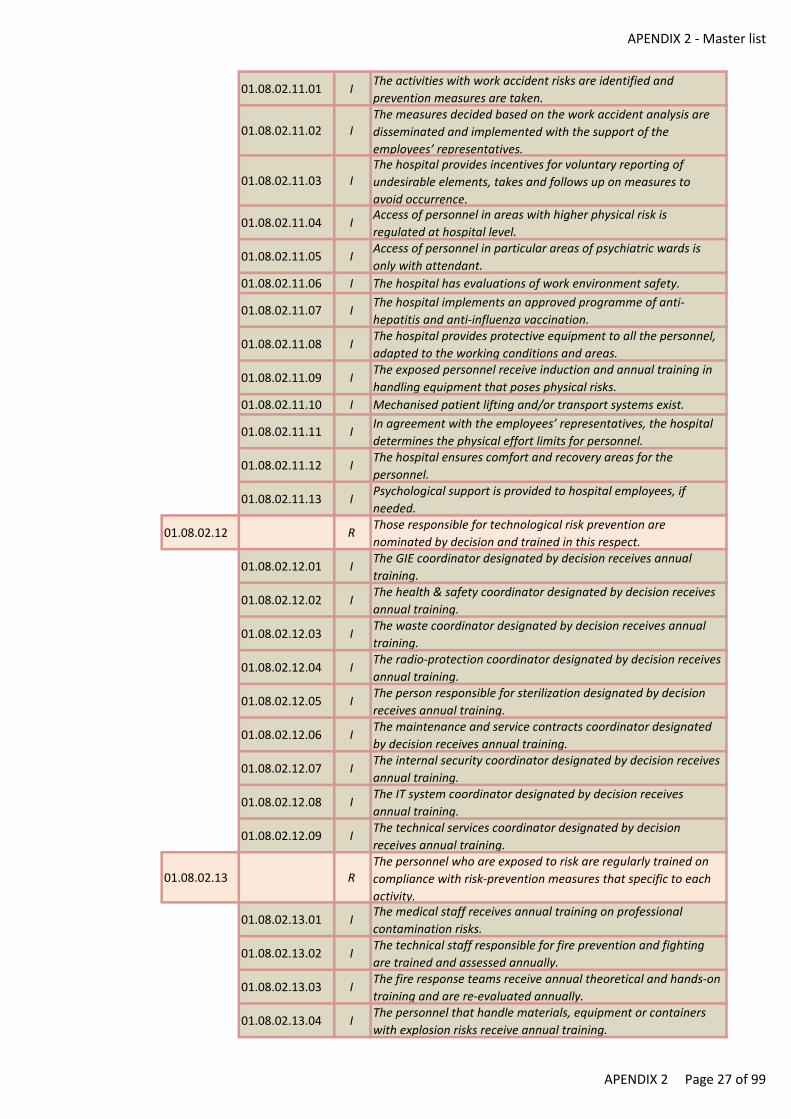
APENDIX 2 - Master list
01.08.02.11.01 IThe activities with work accident risks are identified and
prevention measures are taken.
01.08.02.11.02 IThe measures decided based on the work accident analysis are
disseminated and implemented with the support of the
employees’ representatives.
01.08.02.11.03 IThe hospital provides incentives for voluntary reporting of
undesirable elements, takes and follows up on measures to
avoid occurrence.
01.08.02.11.04 IAccess of personnel in areas with higher physical risk is
regulated at hospital level.
01.08.02.11.05 IAccess of personnel in particular areas of psychiatric wards is
only with attendant.
01.08.02.11.06 I The hospital has evaluations of work environment safety.
01.08.02.11.07 IThe hospital implements an approved programme of anti-
hepatitis and anti-influenza vaccination.
01.08.02.11.08 IThe hospital provides protective equipment to all the personnel,
adapted to the working conditions and areas.
01.08.02.11.09 IThe exposed personnel receive induction and annual training in
handling equipment that poses physical risks.
01.08.02.11.10 I Mechanised patient lifting and/or transport systems exist.
01.08.02.11.11 IIn agreement with the employees’ representatives, the hospital
determines the physical effort limits for personnel.
01.08.02.11.12 IThe hospital ensures comfort and recovery areas for the
personnel.
01.08.02.11.13 IPsychological support is provided to hospital employees, if
needed.
01.08.02.12 RThose responsible for technological risk prevention are
nominated by decision and trained in this respect.
01.08.02.12.01 IThe GIE coordinator designated by decision receives annual
training.
01.08.02.12.02 IThe health & safety coordinator designated by decision receives
annual training.
01.08.02.12.03 IThe waste coordinator designated by decision receives annual
training.
01.08.02.12.04 IThe radio-protection coordinator designated by decision receives
annual training.
01.08.02.12.05 IThe person responsible for sterilization designated by decision
receives annual training.
01.08.02.12.06 IThe maintenance and service contracts coordinator designated
by decision receives annual training.
01.08.02.12.07 IThe internal security coordinator designated by decision receives
annual training.
01.08.02.12.08 IThe IT system coordinator designated by decision receives
annual training.
01.08.02.12.09 IThe technical services coordinator designated by decision
receives annual training.
01.08.02.13 RThe personnel who are exposed to risk are regularly trained on
compliance with risk-prevention measures that specific to each
activity.
01.08.02.13.01 IThe medical staff receives annual training on professional
contamination risks.
01.08.02.13.02 IThe technical staff responsible for fire prevention and fighting
are trained and assessed annually.
01.08.02.13.03 IThe fire response teams receive annual theoretical and hands-on
training and are re-evaluated annually.
01.08.02.13.04 IThe personnel that handle materials, equipment or containers
with explosion risks receive annual training.
APENDIX 2 Page 27 of 99
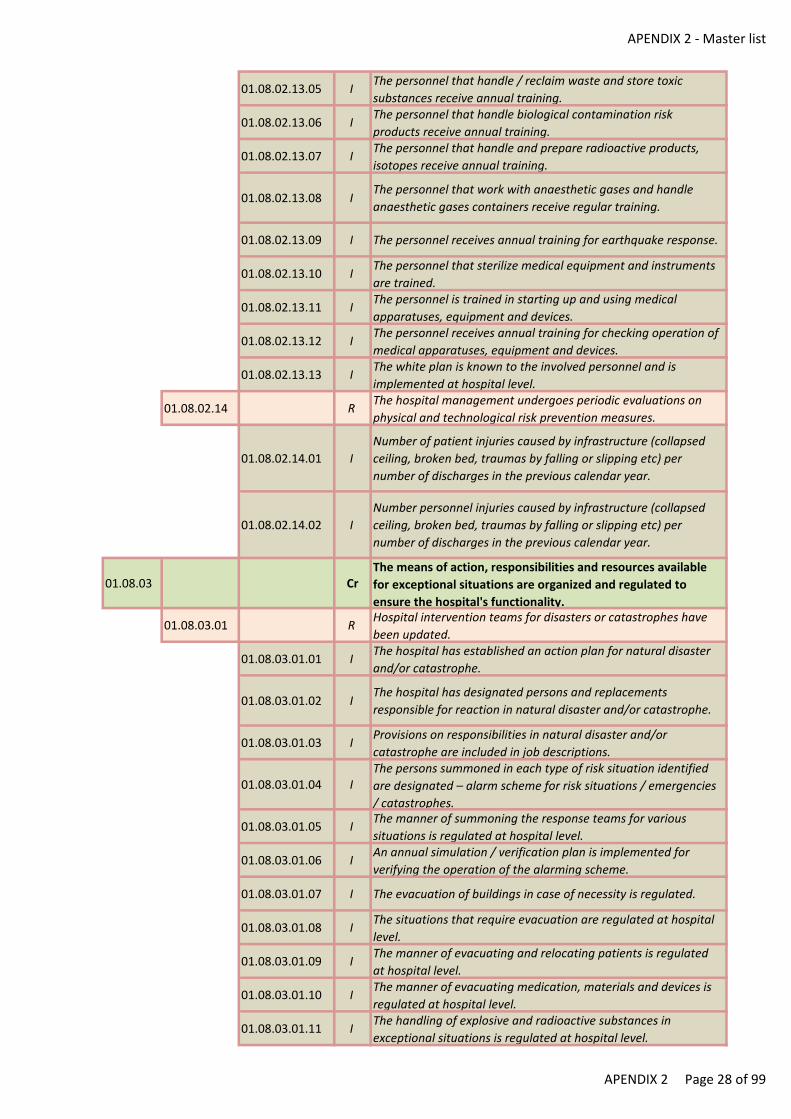
APENDIX 2 - Master list
01.08.02.13.05 IThe personnel that handle / reclaim waste and store toxic
substances receive annual training.
01.08.02.13.06 IThe personnel that handle biological contamination risk
products receive annual training.
01.08.02.13.07 IThe personnel that handle and prepare radioactive products,
isotopes receive annual training.
01.08.02.13.08 IThe personnel that work with anaesthetic gases and handle
anaesthetic gases containers receive regular training.
01.08.02.13.09 I The personnel receives annual training for earthquake response.
01.08.02.13.10 IThe personnel that sterilize medical equipment and instruments
are trained.
01.08.02.13.11 IThe personnel is trained in starting up and using medical
apparatuses, equipment and devices.
01.08.02.13.12 IThe personnel receives annual training for checking operation of
medical apparatuses, equipment and devices.
01.08.02.13.13 IThe white plan is known to the involved personnel and is
implemented at hospital level.
01.08.02.14 RThe hospital management undergoes periodic evaluations on
physical and technological risk prevention measures.
01.08.02.14.01 I
Number of patient injuries caused by infrastructure (collapsed
ceiling, broken bed, traumas by falling or slipping etc) per
number of discharges in the previous calendar year.
01.08.02.14.02 I
Number personnel injuries caused by infrastructure (collapsed
ceiling, broken bed, traumas by falling or slipping etc) per
number of discharges in the previous calendar year.
01.08.03 CrThe means of action, responsibilities and resources available
for exceptional situations are organized and regulated to
ensure the hospital's functionality.
01.08.03.01 RHospital intervention teams for disasters or catastrophes have
been updated.
01.08.03.01.01 IThe hospital has established an action plan for natural disaster
and/or catastrophe.
01.08.03.01.02 IThe hospital has designated persons and replacements
responsible for reaction in natural disaster and/or catastrophe.
01.08.03.01.03 IProvisions on responsibilities in natural disaster and/or
catastrophe are included in job descriptions.
01.08.03.01.04 IThe persons summoned in each type of risk situation identified
are designated – alarm scheme for risk situations / emergencies
/ catastrophes.
01.08.03.01.05 IThe manner of summoning the response teams for various
situations is regulated at hospital level.
01.08.03.01.06 IAn annual simulation / verification plan is implemented for
verifying the operation of the alarming scheme.
01.08.03.01.07 I The evacuation of buildings in case of necessity is regulated.
01.08.03.01.08 IThe situations that require evacuation are regulated at hospital
level.
01.08.03.01.09 IThe manner of evacuating and relocating patients is regulated
at hospital level.
01.08.03.01.10 IThe manner of evacuating medication, materials and devices is
regulated at hospital level.
01.08.03.01.11 IThe handling of explosive and radioactive substances in
exceptional situations is regulated at hospital level.
APENDIX 2 Page 28 of 99
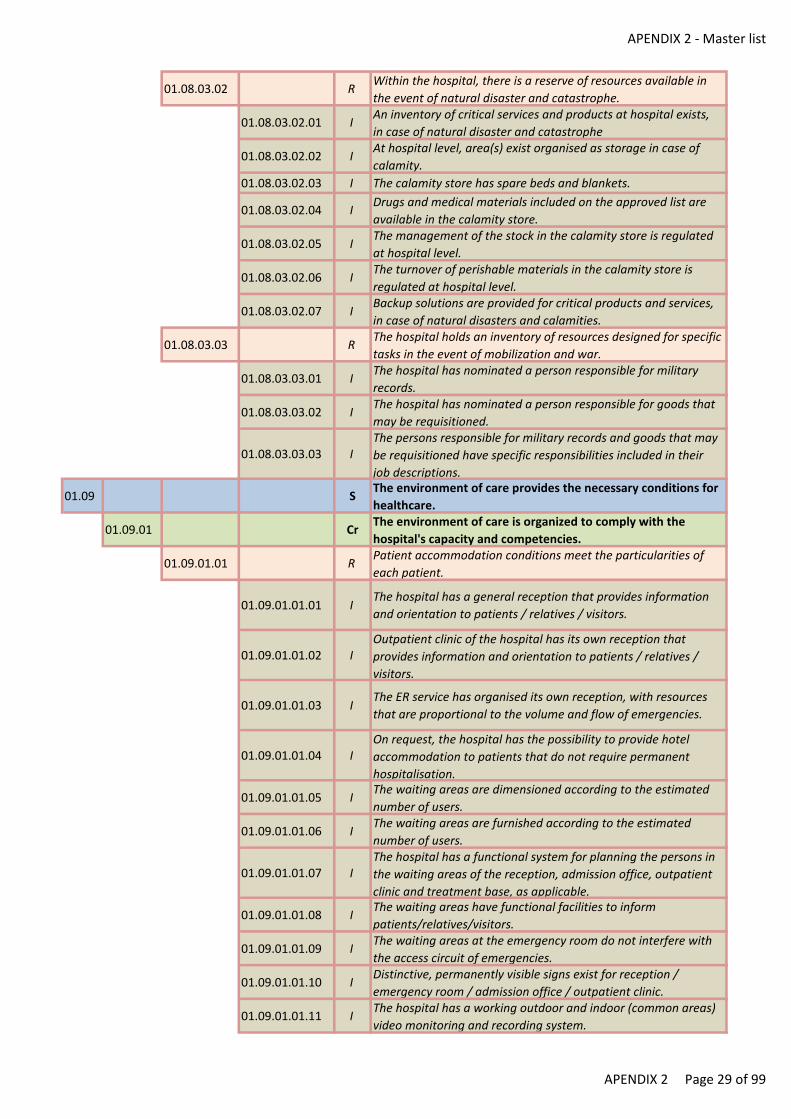
APENDIX 2 - Master list
01.08.03.02 RWithin the hospital, there is a reserve of resources available in
the event of natural disaster and catastrophe.
01.08.03.02.01 IAn inventory of critical services and products at hospital exists,
in case of natural disaster and catastrophe
01.08.03.02.02 IAt hospital level, area(s) exist organised as storage in case of
calamity.
01.08.03.02.03 I The calamity store has spare beds and blankets.
01.08.03.02.04 IDrugs and medical materials included on the approved list are
available in the calamity store.
01.08.03.02.05 IThe management of the stock in the calamity store is regulated
at hospital level.
01.08.03.02.06 IThe turnover of perishable materials in the calamity store is
regulated at hospital level.
01.08.03.02.07 IBackup solutions are provided for critical products and services,
in case of natural disasters and calamities.
01.08.03.03 RThe hospital holds an inventory of resources designed for specific
tasks in the event of mobilization and war.
01.08.03.03.01 IThe hospital has nominated a person responsible for military
records.
01.08.03.03.02 IThe hospital has nominated a person responsible for goods that
may be requisitioned.
01.08.03.03.03 IThe persons responsible for military records and goods that may
be requisitioned have specific responsibilities included in their
job descriptions.
01.09 SThe environment of care provides the necessary conditions for
healthcare.
01.09.01 CrThe environment of care is organized to comply with the
hospital's capacity and competencies.
01.09.01.01 RPatient accommodation conditions meet the particularities of
each patient.
01.09.01.01.01 IThe hospital has a general reception that provides information
and orientation to patients / relatives / visitors.
01.09.01.01.02 IOutpatient clinic of the hospital has its own reception that
provides information and orientation to patients / relatives /
visitors.
01.09.01.01.03 IThe ER service has organised its own reception, with resources
that are proportional to the volume and flow of emergencies.
01.09.01.01.04 IOn request, the hospital has the possibility to provide hotel
accommodation to patients that do not require permanent
hospitalisation.
01.09.01.01.05 IThe waiting areas are dimensioned according to the estimated
number of users.
01.09.01.01.06 IThe waiting areas are furnished according to the estimated
number of users.
01.09.01.01.07 IThe hospital has a functional system for planning the persons in
the waiting areas of the reception, admission office, outpatient
clinic and treatment base, as applicable.
01.09.01.01.08 IThe waiting areas have functional facilities to inform
patients/relatives/visitors.
01.09.01.01.09 IThe waiting areas at the emergency room do not interfere with
the access circuit of emergencies.
01.09.01.01.10 IDistinctive, permanently visible signs exist for reception /
emergency room / admission office / outpatient clinic.
01.09.01.01.11 IThe hospital has a working outdoor and indoor (common areas)
video monitoring and recording system.
APENDIX 2 Page 29 of 99
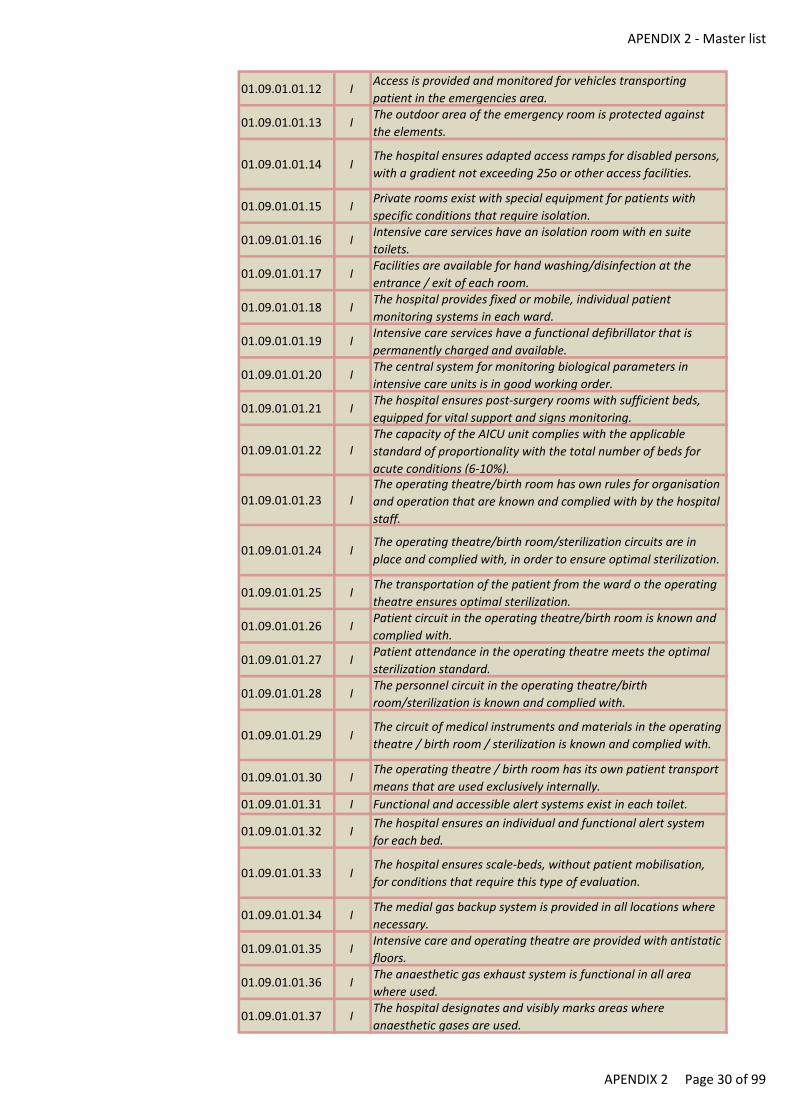
APENDIX 2 - Master list
01.09.01.01.12 IAccess is provided and monitored for vehicles transporting
patient in the emergencies area.
01.09.01.01.13 IThe outdoor area of the emergency room is protected against
the elements.
01.09.01.01.14 IThe hospital ensures adapted access ramps for disabled persons,
with a gradient not exceeding 25o or other access facilities.
01.09.01.01.15 IPrivate rooms exist with special equipment for patients with
specific conditions that require isolation.
01.09.01.01.16 IIntensive care services have an isolation room with en suite
toilets.
01.09.01.01.17 IFacilities are available for hand washing/disinfection at the
entrance / exit of each room.
01.09.01.01.18 IThe hospital provides fixed or mobile, individual patient
monitoring systems in each ward.
01.09.01.01.19 IIntensive care services have a functional defibrillator that is
permanently charged and available.
01.09.01.01.20 IThe central system for monitoring biological parameters in
intensive care units is in good working order.
01.09.01.01.21 IThe hospital ensures post-surgery rooms with sufficient beds,
equipped for vital support and signs monitoring.
01.09.01.01.22 IThe capacity of the AICU unit complies with the applicable
standard of proportionality with the total number of beds for
acute conditions (6-10%).
01.09.01.01.23 IThe operating theatre/birth room has own rules for organisation
and operation that are known and complied with by the hospital
staff.
01.09.01.01.24 IThe operating theatre/birth room/sterilization circuits are in
place and complied with, in order to ensure optimal sterilization.
01.09.01.01.25 IThe transportation of the patient from the ward o the operating
theatre ensures optimal sterilization.
01.09.01.01.26 IPatient circuit in the operating theatre/birth room is known and
complied with.
01.09.01.01.27 IPatient attendance in the operating theatre meets the optimal
sterilization standard.
01.09.01.01.28 IThe personnel circuit in the operating theatre/birth
room/sterilization is known and complied with.
01.09.01.01.29 IThe circuit of medical instruments and materials in the operating
theatre / birth room / sterilization is known and complied with.
01.09.01.01.30 IThe operating theatre / birth room has its own patient transport
means that are used exclusively internally.
01.09.01.01.31 I Functional and accessible alert systems exist in each toilet.
01.09.01.01.32 IThe hospital ensures an individual and functional alert system
for each bed.
01.09.01.01.33 IThe hospital ensures scale-beds, without patient mobilisation,
for conditions that require this type of evaluation.
01.09.01.01.34 IThe medial gas backup system is provided in all locations where
necessary.
01.09.01.01.35 IIntensive care and operating theatre are provided with antistatic
floors.
01.09.01.01.36 IThe anaesthetic gas exhaust system is functional in all area
where used.
01.09.01.01.37 IThe hospital designates and visibly marks areas where
anaesthetic gases are used.
APENDIX 2 Page 30 of 99
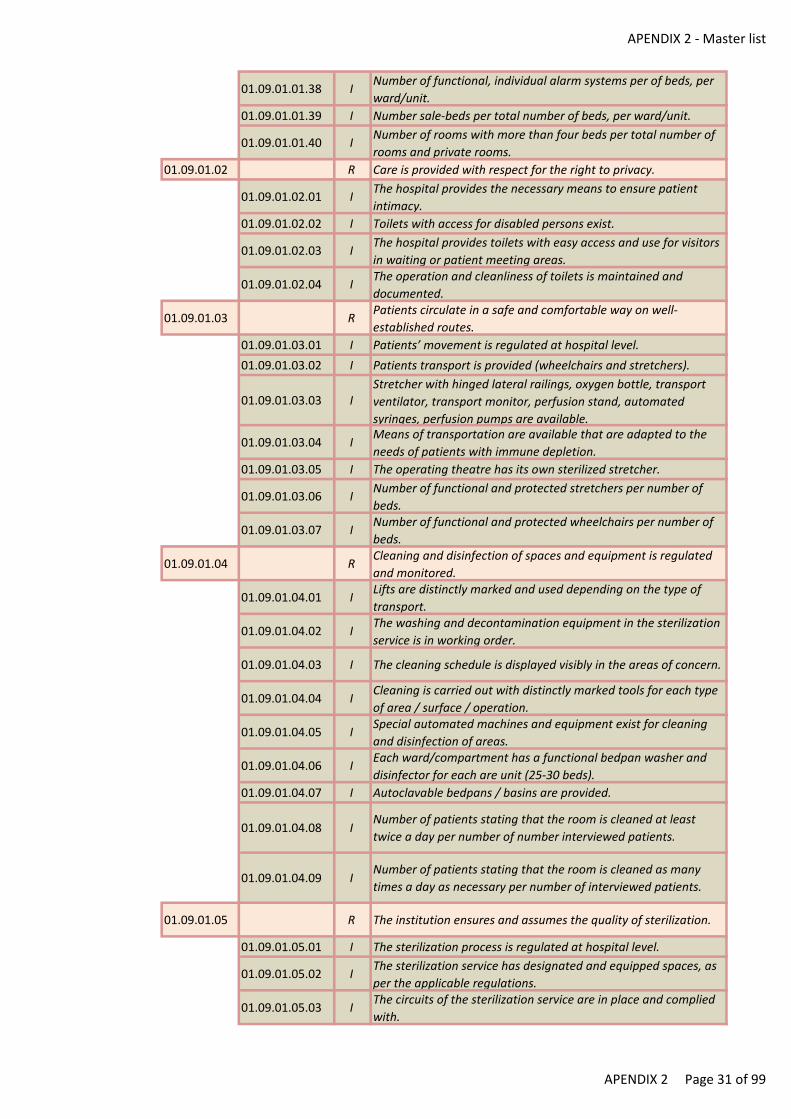
APENDIX 2 - Master list
01.09.01.01.38 INumber of functional, individual alarm systems per of beds, per
ward/unit.
01.09.01.01.39 I Number sale-beds per total number of beds, per ward/unit.
01.09.01.01.40 INumber of rooms with more than four beds per total number of
rooms and private rooms.
01.09.01.02 R Care is provided with respect for the right to privacy.
01.09.01.02.01 IThe hospital provides the necessary means to ensure patient
intimacy.
01.09.01.02.02 I Toilets with access for disabled persons exist.
01.09.01.02.03 IThe hospital provides toilets with easy access and use for visitors
in waiting or patient meeting areas.
01.09.01.02.04 IThe operation and cleanliness of toilets is maintained and
documented.
01.09.01.03 RPatients circulate in a safe and comfortable way on well-
established routes.
01.09.01.03.01 I Patients’ movement is regulated at hospital level.
01.09.01.03.02 I Patients transport is provided (wheelchairs and stretchers).
01.09.01.03.03 IStretcher with hinged lateral railings, oxygen bottle, transport
ventilator, transport monitor, perfusion stand, automated
syringes, perfusion pumps are available.
01.09.01.03.04 IMeans of transportation are available that are adapted to the
needs of patients with immune depletion.
01.09.01.03.05 I The operating theatre has its own sterilized stretcher.
01.09.01.03.06 INumber of functional and protected stretchers per number of
beds.
01.09.01.03.07 INumber of functional and protected wheelchairs per number of
beds.
01.09.01.04 RCleaning and disinfection of spaces and equipment is regulated
and monitored.
01.09.01.04.01 ILifts are distinctly marked and used depending on the type of
transport.
01.09.01.04.02 IThe washing and decontamination equipment in the sterilization
service is in working order.
01.09.01.04.03 I The cleaning schedule is displayed visibly in the areas of concern.
01.09.01.04.04 ICleaning is carried out with distinctly marked tools for each type
of area / surface / operation.
01.09.01.04.05 ISpecial automated machines and equipment exist for cleaning
and disinfection of areas.
01.09.01.04.06 IEach ward/compartment has a functional bedpan washer and
disinfector for each are unit (25-30 beds).
01.09.01.04.07 I Autoclavable bedpans / basins are provided.
01.09.01.04.08 INumber of patients stating that the room is cleaned at least
twice a day per number of number interviewed patients.
01.09.01.04.09 INumber of patients stating that the room is cleaned as many
times a day as necessary per number of interviewed patients.
01.09.01.05 R The institution ensures and assumes the quality of sterilization.
01.09.01.05.01 I The sterilization process is regulated at hospital level.
01.09.01.05.02 IThe sterilization service has designated and equipped spaces, as
per the applicable regulations.
01.09.01.05.03 IThe circuits of the sterilization service are in place and complied
with.
APENDIX 2 Page 31 of 99
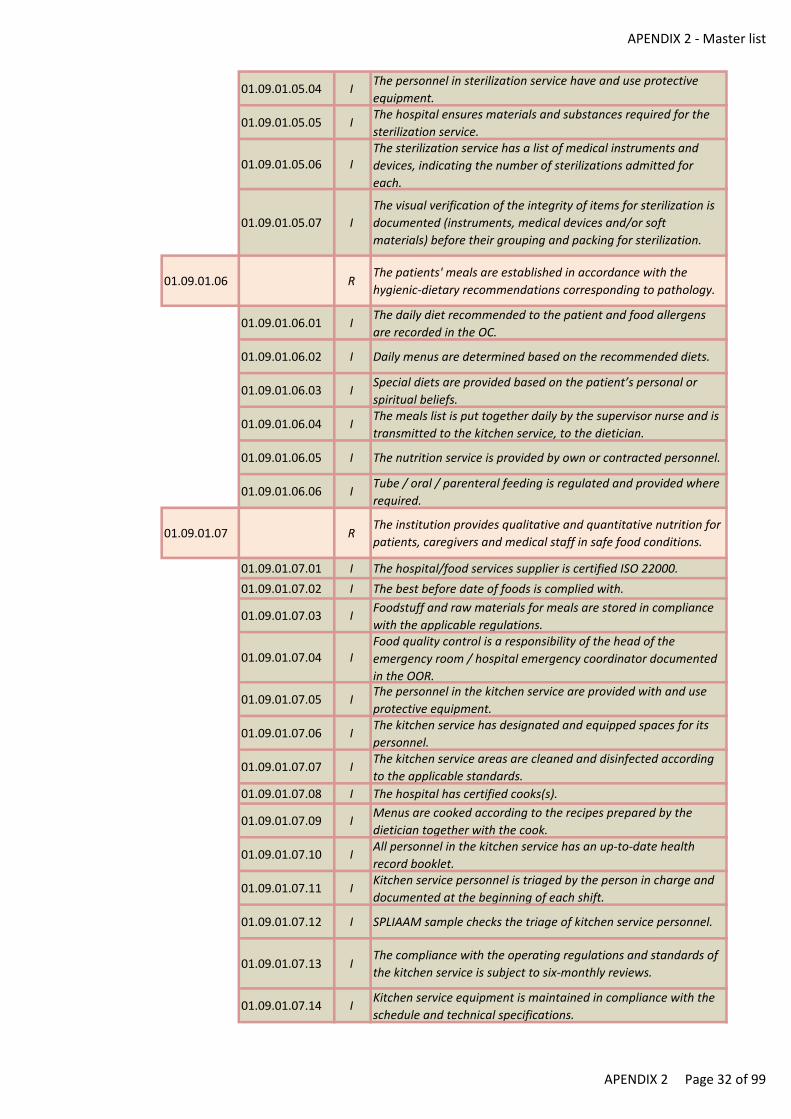
APENDIX 2 - Master list
01.09.01.05.04 IThe personnel in sterilization service have and use protective
equipment.
01.09.01.05.05 IThe hospital ensures materials and substances required for the
sterilization service.
01.09.01.05.06 IThe sterilization service has a list of medical instruments and
devices, indicating the number of sterilizations admitted for
each.
01.09.01.05.07 I
The visual verification of the integrity of items for sterilization is
documented (instruments, medical devices and/or soft
materials) before their grouping and packing for sterilization.
01.09.01.06 RThe patients' meals are established in accordance with the
hygienic-dietary recommendations corresponding to pathology.
01.09.01.06.01 IThe daily diet recommended to the patient and food allergens
are recorded in the OC.
01.09.01.06.02 I Daily menus are determined based on the recommended diets.
01.09.01.06.03 ISpecial diets are provided based on the patient’s personal or
spiritual beliefs.
01.09.01.06.04 IThe meals list is put together daily by the supervisor nurse and is
transmitted to the kitchen service, to the dietician.
01.09.01.06.05 I The nutrition service is provided by own or contracted personnel.
01.09.01.06.06 ITube / oral / parenteral feeding is regulated and provided where
required.
01.09.01.07 RThe institution provides qualitative and quantitative nutrition for
patients, caregivers and medical staff in safe food conditions.
01.09.01.07.01 I The hospital/food services supplier is certified ISO 22000.
01.09.01.07.02 I The best before date of foods is complied with.
01.09.01.07.03 IFoodstuff and raw materials for meals are stored in compliance
with the applicable regulations.
01.09.01.07.04 IFood quality control is a responsibility of the head of the
emergency room / hospital emergency coordinator documented
in the OOR.
01.09.01.07.05 IThe personnel in the kitchen service are provided with and use
protective equipment.
01.09.01.07.06 IThe kitchen service has designated and equipped spaces for its
personnel.
01.09.01.07.07 IThe kitchen service areas are cleaned and disinfected according
to the applicable standards.
01.09.01.07.08 I The hospital has certified cooks(s).
01.09.01.07.09 IMenus are cooked according to the recipes prepared by the
dietician together with the cook.
01.09.01.07.10 IAll personnel in the kitchen service has an up-to-date health
record booklet.
01.09.01.07.11 IKitchen service personnel is triaged by the person in charge and
documented at the beginning of each shift.
01.09.01.07.12 I SPLIAAM sample checks the triage of kitchen service personnel.
01.09.01.07.13 IThe compliance with the operating regulations and standards of
the kitchen service is subject to six-monthly reviews.
01.09.01.07.14 IKitchen service equipment is maintained in compliance with the
schedule and technical specifications.
APENDIX 2 Page 32 of 99
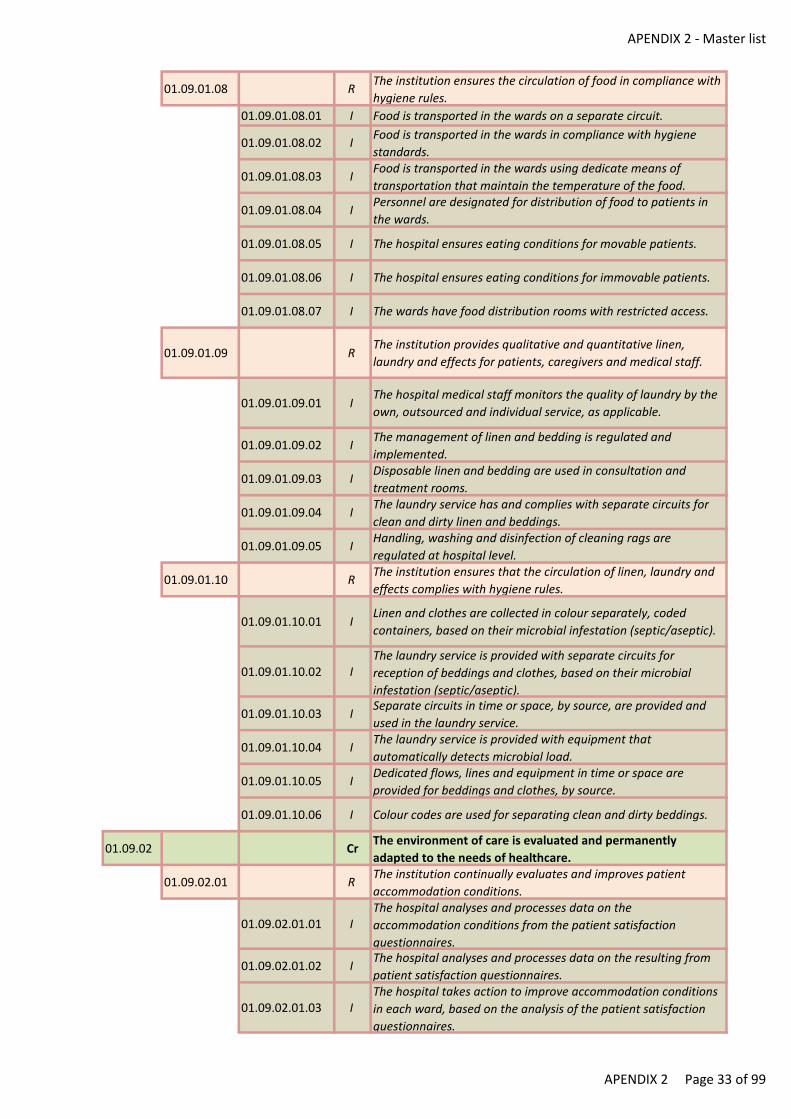
APENDIX 2 - Master list
01.09.01.08 RThe institution ensures the circulation of food in compliance with
hygiene rules.
01.09.01.08.01 I Food is transported in the wards on a separate circuit.
01.09.01.08.02 IFood is transported in the wards in compliance with hygiene
standards.
01.09.01.08.03 IFood is transported in the wards using dedicate means of
transportation that maintain the temperature of the food.
01.09.01.08.04 IPersonnel are designated for distribution of food to patients in
the wards.
01.09.01.08.05 I The hospital ensures eating conditions for movable patients.
01.09.01.08.06 I The hospital ensures eating conditions for immovable patients.
01.09.01.08.07 I The wards have food distribution rooms with restricted access.
01.09.01.09 RThe institution provides qualitative and quantitative linen,
laundry and effects for patients, caregivers and medical staff.
01.09.01.09.01 IThe hospital medical staff monitors the quality of laundry by the
own, outsourced and individual service, as applicable.
01.09.01.09.02 IThe management of linen and bedding is regulated and
implemented.
01.09.01.09.03 IDisposable linen and bedding are used in consultation and
treatment rooms.
01.09.01.09.04 IThe laundry service has and complies with separate circuits for
clean and dirty linen and beddings.
01.09.01.09.05 IHandling, washing and disinfection of cleaning rags are
regulated at hospital level.
01.09.01.10 RThe institution ensures that the circulation of linen, laundry and
effects complies with hygiene rules.
01.09.01.10.01 ILinen and clothes are collected in colour separately, coded
containers, based on their microbial infestation (septic/aseptic).
01.09.01.10.02 IThe laundry service is provided with separate circuits for
reception of beddings and clothes, based on their microbial
infestation (septic/aseptic).
01.09.01.10.03 ISeparate circuits in time or space, by source, are provided and
used in the laundry service.
01.09.01.10.04 IThe laundry service is provided with equipment that
automatically detects microbial load.
01.09.01.10.05 IDedicated flows, lines and equipment in time or space are
provided for beddings and clothes, by source.
01.09.01.10.06 I Colour codes are used for separating clean and dirty beddings.
01.09.02 CrThe environment of care is evaluated and permanently
adapted to the needs of healthcare.
01.09.02.01 RThe institution continually evaluates and improves patient
accommodation conditions.
01.09.02.01.01 IThe hospital analyses and processes data on the
accommodation conditions from the patient satisfaction
questionnaires.
01.09.02.01.02 IThe hospital analyses and processes data on the resulting from
patient satisfaction questionnaires.
01.09.02.01.03 IThe hospital takes action to improve accommodation conditions
in each ward, based on the analysis of the patient satisfaction
questionnaires.
APENDIX 2 Page 33 of 99
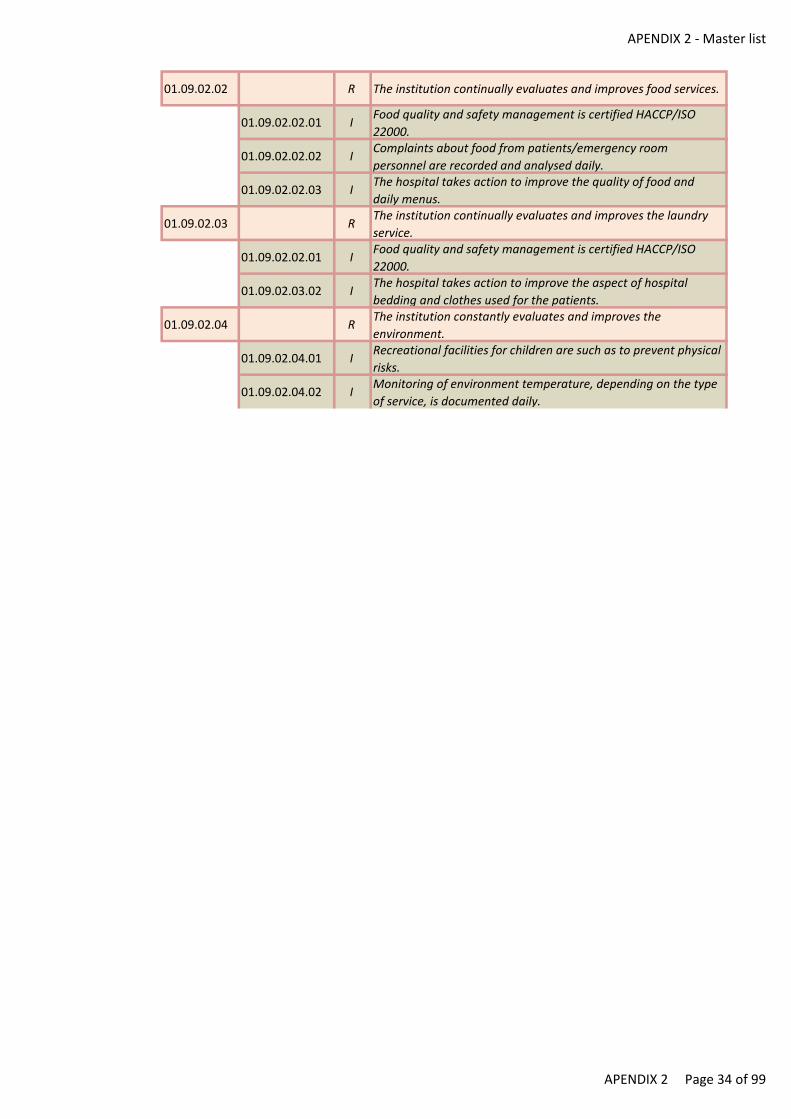
APENDIX 2 - Master list
01.09.02.02 R The institution continually evaluates and improves food services.
01.09.02.02.01 IFood quality and safety management is certified HACCP/ISO
22000.
01.09.02.02.02 IComplaints about food from patients/emergency room
personnel are recorded and analysed daily.
01.09.02.02.03 IThe hospital takes action to improve the quality of food and
daily menus.
01.09.02.03 RThe institution continually evaluates and improves the laundry
service.
01.09.02.02.01 IFood quality and safety management is certified HACCP/ISO
22000.
01.09.02.03.02 IThe hospital takes action to improve the aspect of hospital
bedding and clothes used for the patients.
01.09.02.04 RThe institution constantly evaluates and improves the
environment.
01.09.02.04.01 IRecreational facilities for children are such as to prevent physical
risks.
01.09.02.04.02 IMonitoring of environment temperature, depending on the type
of service, is documented daily.
APENDIX 2 Page 34 of 99
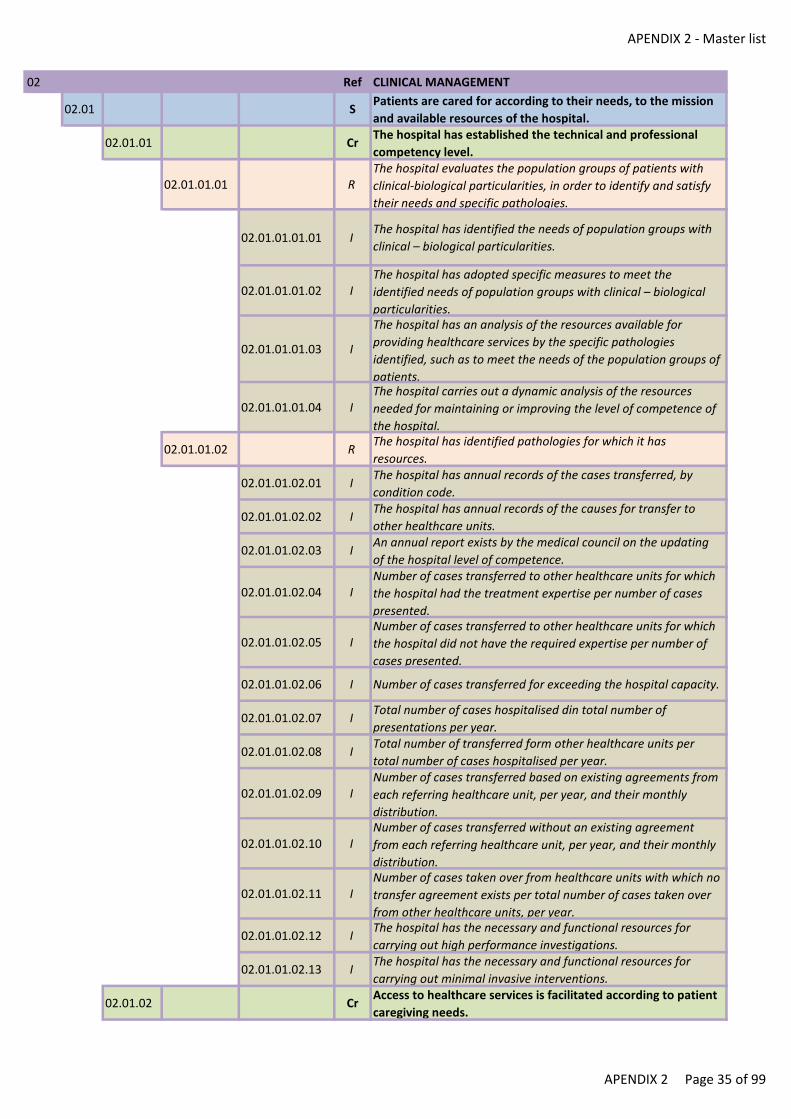
APENDIX 2 - Master list
02 Ref CLINICAL MANAGEMENT
02.01 SPatients are cared for according to their needs, to the mission
and available resources of the hospital.
02.01.01 CrThe hospital has established the technical and professional
competency level.
02.01.01.01 RThe hospital evaluates the population groups of patients with
clinical-biological particularities, in order to identify and satisfy
their needs and specific pathologies.
02.01.01.01.01 IThe hospital has identified the needs of population groups with
clinical – biological particularities.
02.01.01.01.02 IThe hospital has adopted specific measures to meet the
identified needs of population groups with clinical – biological
particularities.
02.01.01.01.03 I
The hospital has an analysis of the resources available for
providing healthcare services by the specific pathologies
identified, such as to meet the needs of the population groups of
patients.
02.01.01.01.04 IThe hospital carries out a dynamic analysis of the resources
needed for maintaining or improving the level of competence of
the hospital.
02.01.01.02 RThe hospital has identified pathologies for which it has
resources.
02.01.01.02.01 IThe hospital has annual records of the cases transferred, by
condition code.
02.01.01.02.02 IThe hospital has annual records of the causes for transfer to
other healthcare units.
02.01.01.02.03 IAn annual report exists by the medical council on the updating
of the hospital level of competence.
02.01.01.02.04 INumber of cases transferred to other healthcare units for which
the hospital had the treatment expertise per number of cases
presented.
02.01.01.02.05 INumber of cases transferred to other healthcare units for which
the hospital did not have the required expertise per number of
cases presented.
02.01.01.02.06 I Number of cases transferred for exceeding the hospital capacity.
02.01.01.02.07 ITotal number of cases hospitalised din total number of
presentations per year.
02.01.01.02.08 ITotal number of transferred form other healthcare units per
total number of cases hospitalised per year.
02.01.01.02.09 INumber of cases transferred based on existing agreements from
each referring healthcare unit, per year, and their monthly
distribution.
02.01.01.02.10 INumber of cases transferred without an existing agreement
from each referring healthcare unit, per year, and their monthly
distribution.
02.01.01.02.11 INumber of cases taken over from healthcare units with which no
transfer agreement exists per total number of cases taken over
from other healthcare units, per year.
02.01.01.02.12 IThe hospital has the necessary and functional resources for
carrying out high performance investigations.
02.01.01.02.13 IThe hospital has the necessary and functional resources for
carrying out minimal invasive interventions.
02.01.02 CrAccess to healthcare services is facilitated according to patient
caregiving needs.
APENDIX 2 Page 35 of 99
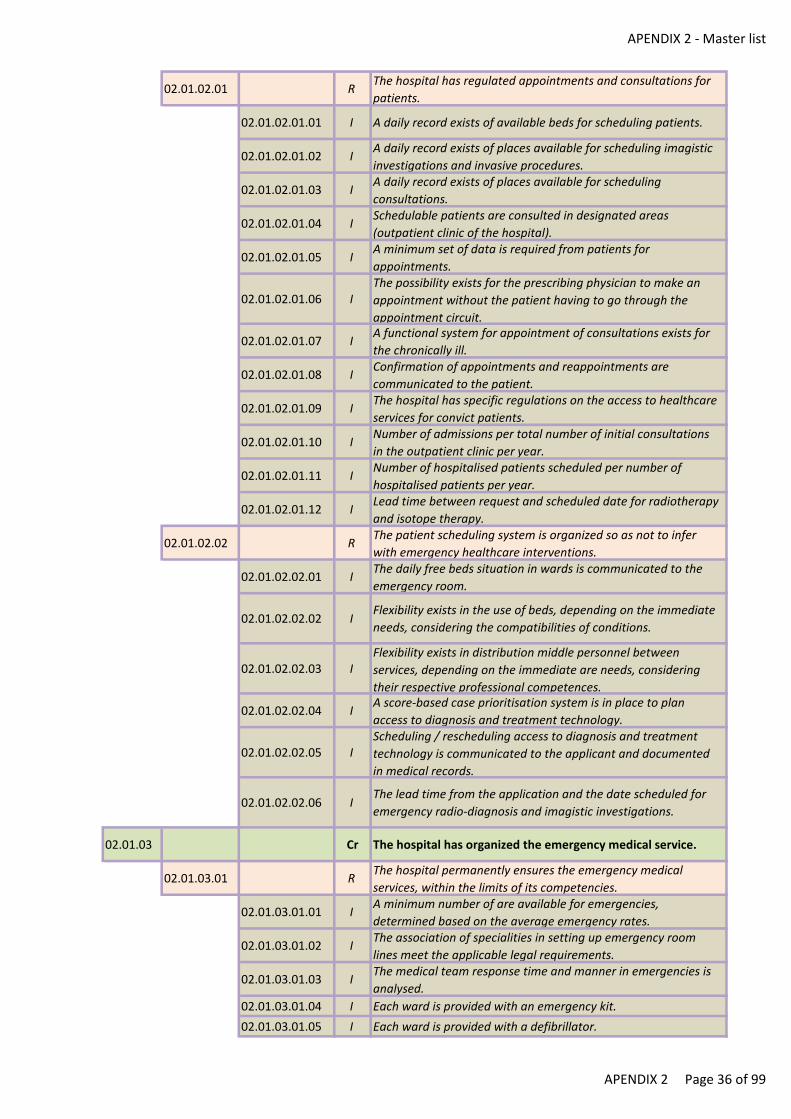
APENDIX 2 - Master list
02.01.02.01 RThe hospital has regulated appointments and consultations for
patients.
02.01.02.01.01 I A daily record exists of available beds for scheduling patients.
02.01.02.01.02 IA daily record exists of places available for scheduling imagistic
investigations and invasive procedures.
02.01.02.01.03 IA daily record exists of places available for scheduling
consultations.
02.01.02.01.04 ISchedulable patients are consulted in designated areas
(outpatient clinic of the hospital).
02.01.02.01.05 IA minimum set of data is required from patients for
appointments.
02.01.02.01.06 IThe possibility exists for the prescribing physician to make an
appointment without the patient having to go through the
appointment circuit.
02.01.02.01.07 IA functional system for appointment of consultations exists for
the chronically ill.
02.01.02.01.08 IConfirmation of appointments and reappointments are
communicated to the patient.
02.01.02.01.09 IThe hospital has specific regulations on the access to healthcare
services for convict patients.
02.01.02.01.10 INumber of admissions per total number of initial consultations
in the outpatient clinic per year.
02.01.02.01.11 INumber of hospitalised patients scheduled per number of
hospitalised patients per year.
02.01.02.01.12 ILead time between request and scheduled date for radiotherapy
and isotope therapy.
02.01.02.02 RThe patient scheduling system is organized so as not to infer
with emergency healthcare interventions.
02.01.02.02.01 IThe daily free beds situation in wards is communicated to the
emergency room.
02.01.02.02.02 IFlexibility exists in the use of beds, depending on the immediate
needs, considering the compatibilities of conditions.
02.01.02.02.03 IFlexibility exists in distribution middle personnel between
services, depending on the immediate are needs, considering
their respective professional competences.
02.01.02.02.04 IA score-based case prioritisation system is in place to plan
access to diagnosis and treatment technology.
02.01.02.02.05 IScheduling / rescheduling access to diagnosis and treatment
technology is communicated to the applicant and documented
in medical records.
02.01.02.02.06 IThe lead time from the application and the date scheduled for
emergency radio-diagnosis and imagistic investigations.
02.01.03 Cr The hospital has organized the emergency medical service.
02.01.03.01 RThe hospital permanently ensures the emergency medical
services, within the limits of its competencies.
02.01.03.01.01 IA minimum number of are available for emergencies,
determined based on the average emergency rates.
02.01.03.01.02 IThe association of specialities in setting up emergency room
lines meet the applicable legal requirements.
02.01.03.01.03 IThe medical team response time and manner in emergencies is
analysed.
02.01.03.01.04 I Each ward is provided with an emergency kit.
02.01.03.01.05 I Each ward is provided with a defibrillator.
APENDIX 2 Page 36 of 99
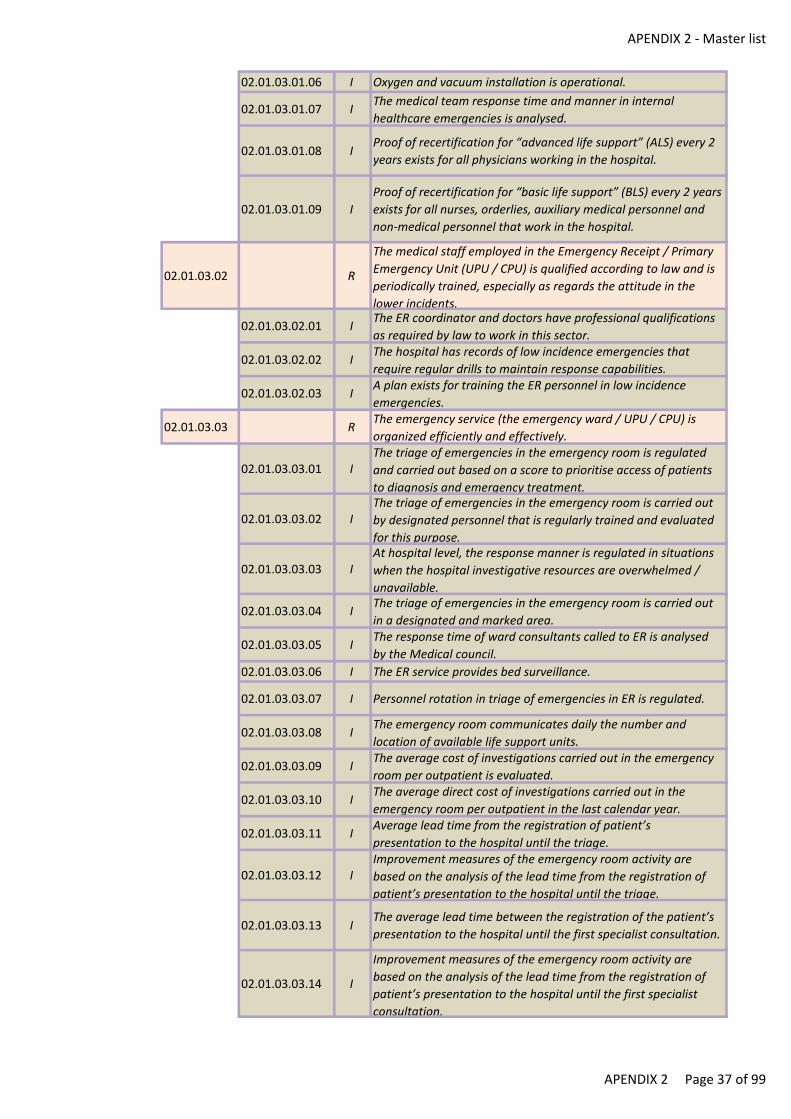
APENDIX 2 - Master list
02.01.03.01.06 I Oxygen and vacuum installation is operational.
02.01.03.01.07 IThe medical team response time and manner in internal
healthcare emergencies is analysed.
02.01.03.01.08 IProof of recertification for “advanced life support” (ALS) every 2
years exists for all physicians working in the hospital.
02.01.03.01.09 I
Proof of recertification for “basic life support” (BLS) every 2 years
exists for all nurses, orderlies, auxiliary medical personnel and
non-medical personnel that work in the hospital.
02.01.03.02 R
The medical staff employed in the Emergency Receipt / Primary
Emergency Unit (UPU / CPU) is qualified according to law and is
periodically trained, especially as regards the attitude in the
lower incidents.
02.01.03.02.01 IThe ER coordinator and doctors have professional qualifications
as required by law to work in this sector.
02.01.03.02.02 IThe hospital has records of low incidence emergencies that
require regular drills to maintain response capabilities.
02.01.03.02.03 IA plan exists for training the ER personnel in low incidence
emergencies.
02.01.03.03 RThe emergency service (the emergency ward / UPU / CPU) is
organized efficiently and effectively.
02.01.03.03.01 IThe triage of emergencies in the emergency room is regulated
and carried out based on a score to prioritise access of patients
to diagnosis and emergency treatment.
02.01.03.03.02 IThe triage of emergencies in the emergency room is carried out
by designated personnel that is regularly trained and evaluated
for this purpose.
02.01.03.03.03 IAt hospital level, the response manner is regulated in situations
when the hospital investigative resources are overwhelmed /
unavailable.
02.01.03.03.04 IThe triage of emergencies in the emergency room is carried out
in a designated and marked area.
02.01.03.03.05 IThe response time of ward consultants called to ER is analysed
by the Medical council.
02.01.03.03.06 I The ER service provides bed surveillance.
02.01.03.03.07 I Personnel rotation in triage of emergencies in ER is regulated.
02.01.03.03.08 IThe emergency room communicates daily the number and
location of available life support units.
02.01.03.03.09 IThe average cost of investigations carried out in the emergency
room per outpatient is evaluated.
02.01.03.03.10 IThe average direct cost of investigations carried out in the
emergency room per outpatient in the last calendar year.
02.01.03.03.11 IAverage lead time from the registration of patient’s
presentation to the hospital until the triage.
02.01.03.03.12 IImprovement measures of the emergency room activity are
based on the analysis of the lead time from the registration of
patient’s presentation to the hospital until the triage.
02.01.03.03.13 IThe average lead time between the registration of the patient’s
presentation to the hospital until the first specialist consultation.
02.01.03.03.14 I
Improvement measures of the emergency room activity are
based on the analysis of the lead time from the registration of
patient’s presentation to the hospital until the first specialist
consultation.
APENDIX 2 Page 37 of 99
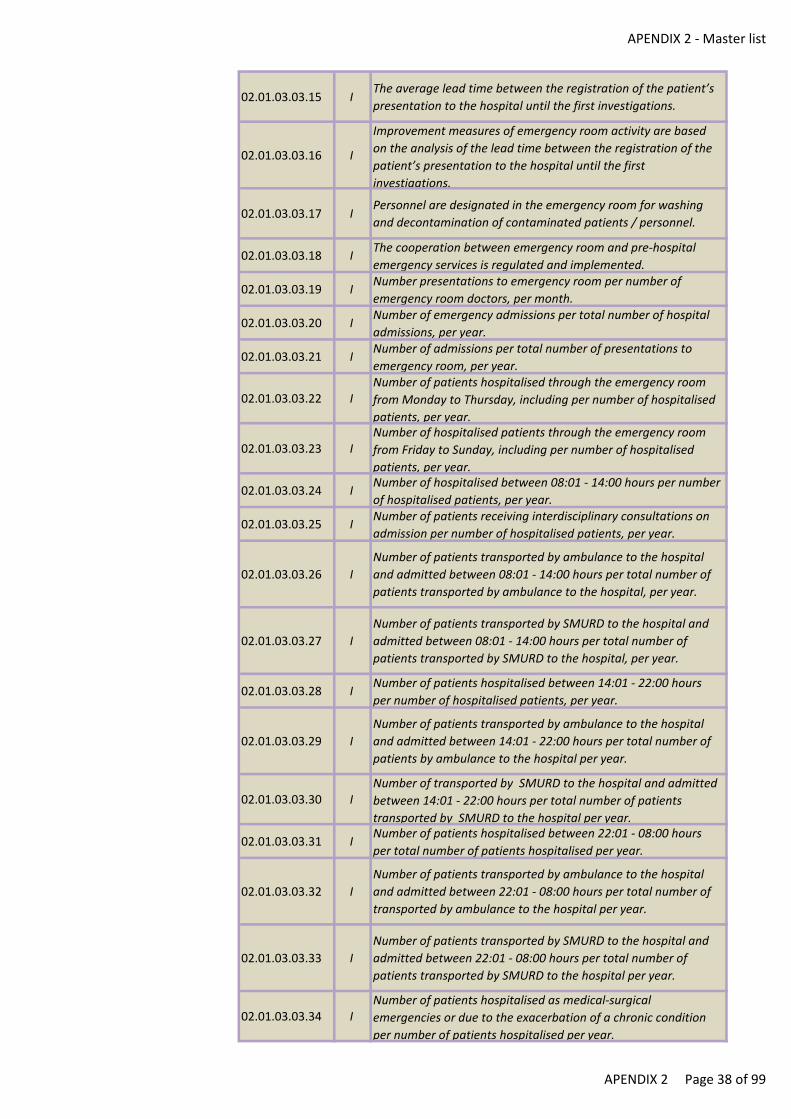
APENDIX 2 - Master list
02.01.03.03.15 IThe average lead time between the registration of the patient’s
presentation to the hospital until the first investigations.
02.01.03.03.16 I
Improvement measures of emergency room activity are based
on the analysis of the lead time between the registration of the
patient’s presentation to the hospital until the first
investigations.
02.01.03.03.17 IPersonnel are designated in the emergency room for washing
and decontamination of contaminated patients / personnel.
02.01.03.03.18 IThe cooperation between emergency room and pre-hospital
emergency services is regulated and implemented.
02.01.03.03.19 INumber presentations to emergency room per number of
emergency room doctors, per month.
02.01.03.03.20 INumber of emergency admissions per total number of hospital
admissions, per year.
02.01.03.03.21 INumber of admissions per total number of presentations to
emergency room, per year.
02.01.03.03.22 INumber of patients hospitalised through the emergency room
from Monday to Thursday, including per number of hospitalised
patients, per year.
02.01.03.03.23 INumber of hospitalised patients through the emergency room
from Friday to Sunday, including per number of hospitalised
patients, per year.
02.01.03.03.24 INumber of hospitalised between 08:01 - 14:00 hours per number
of hospitalised patients, per year.
02.01.03.03.25 INumber of patients receiving interdisciplinary consultations on
admission per number of hospitalised patients, per year.
02.01.03.03.26 I
Number of patients transported by ambulance to the hospital
and admitted between 08:01 - 14:00 hours per total number of
patients transported by ambulance to the hospital, per year.
02.01.03.03.27 I
Number of patients transported by SMURD to the hospital and
admitted between 08:01 - 14:00 hours per total number of
patients transported by SMURD to the hospital, per year.
02.01.03.03.28 INumber of patients hospitalised between 14:01 - 22:00 hours
per number of hospitalised patients, per year.
02.01.03.03.29 I
Number of patients transported by ambulance to the hospital
and admitted between 14:01 - 22:00 hours per total number of
patients by ambulance to the hospital per year.
02.01.03.03.30 INumber of transported by SMURD to the hospital and admitted
between 14:01 - 22:00 hours per total number of patients
transported by SMURD to the hospital per year.
02.01.03.03.31 INumber of patients hospitalised between 22:01 - 08:00 hours
per total number of patients hospitalised per year.
02.01.03.03.32 I
Number of patients transported by ambulance to the hospital
and admitted between 22:01 - 08:00 hours per total number of
transported by ambulance to the hospital per year.
02.01.03.03.33 I
Number of patients transported by SMURD to the hospital and
admitted between 22:01 - 08:00 hours per total number of
patients transported by SMURD to the hospital per year.
02.01.03.03.34 INumber of patients hospitalised as medical-surgical
emergencies or due to the exacerbation of a chronic condition
per number of patients hospitalised per year.
APENDIX 2 Page 38 of 99
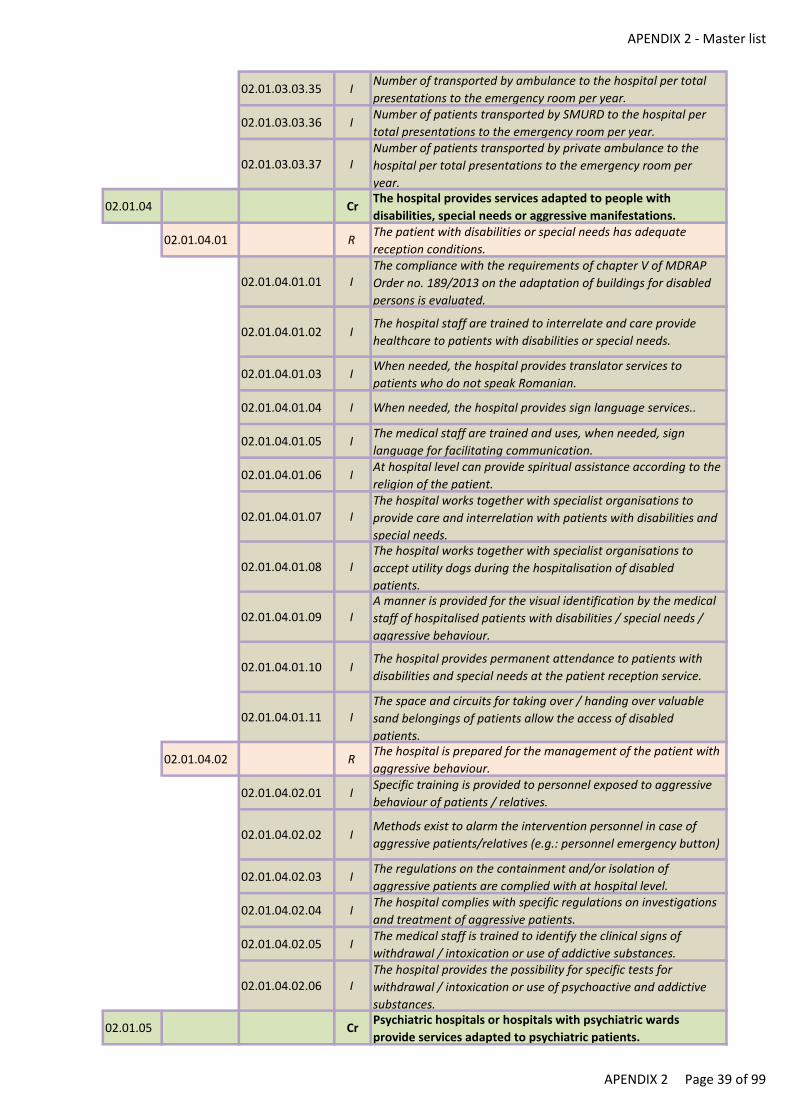
APENDIX 2 - Master list
02.01.03.03.35 INumber of transported by ambulance to the hospital per total
presentations to the emergency room per year.
02.01.03.03.36 INumber of patients transported by SMURD to the hospital per
total presentations to the emergency room per year.
02.01.03.03.37 INumber of patients transported by private ambulance to the
hospital per total presentations to the emergency room per
year.
02.01.04 CrThe hospital provides services adapted to people with
disabilities, special needs or aggressive manifestations.
02.01.04.01 RThe patient with disabilities or special needs has adequate
reception conditions.
02.01.04.01.01 IThe compliance with the requirements of chapter V of MDRAP
Order no. 189/2013 on the adaptation of buildings for disabled
persons is evaluated.
02.01.04.01.02 IThe hospital staff are trained to interrelate and care provide
healthcare to patients with disabilities or special needs.
02.01.04.01.03 IWhen needed, the hospital provides translator services to
patients who do not speak Romanian.
02.01.04.01.04 I When needed, the hospital provides sign language services..
02.01.04.01.05 IThe medical staff are trained and uses, when needed, sign
language for facilitating communication.
02.01.04.01.06 IAt hospital level can provide spiritual assistance according to the
religion of the patient.
02.01.04.01.07 IThe hospital works together with specialist organisations to
provide care and interrelation with patients with disabilities and
special needs.
02.01.04.01.08 IThe hospital works together with specialist organisations to
accept utility dogs during the hospitalisation of disabled
patients.
02.01.04.01.09 IA manner is provided for the visual identification by the medical
staff of hospitalised patients with disabilities / special needs /
aggressive behaviour.
02.01.04.01.10 IThe hospital provides permanent attendance to patients with
disabilities and special needs at the patient reception service.
02.01.04.01.11 IThe space and circuits for taking over / handing over valuable
sand belongings of patients allow the access of disabled
patients.
02.01.04.02 RThe hospital is prepared for the management of the patient with
aggressive behaviour.
02.01.04.02.01 ISpecific training is provided to personnel exposed to aggressive
behaviour of patients / relatives.
02.01.04.02.02 IMethods exist to alarm the intervention personnel in case of
aggressive patients/relatives (e.g.: personnel emergency button)
02.01.04.02.03 IThe regulations on the containment and/or isolation of
aggressive patients are complied with at hospital level.
02.01.04.02.04 IThe hospital complies with specific regulations on investigations
and treatment of aggressive patients.
02.01.04.02.05 IThe medical staff is trained to identify the clinical signs of
withdrawal / intoxication or use of addictive substances.
02.01.04.02.06 IThe hospital provides the possibility for specific tests for
withdrawal / intoxication or use of psychoactive and addictive
substances.
02.01.05 CrPsychiatric hospitals or hospitals with psychiatric wards
provide services adapted to psychiatric patients.
APENDIX 2 Page 39 of 99
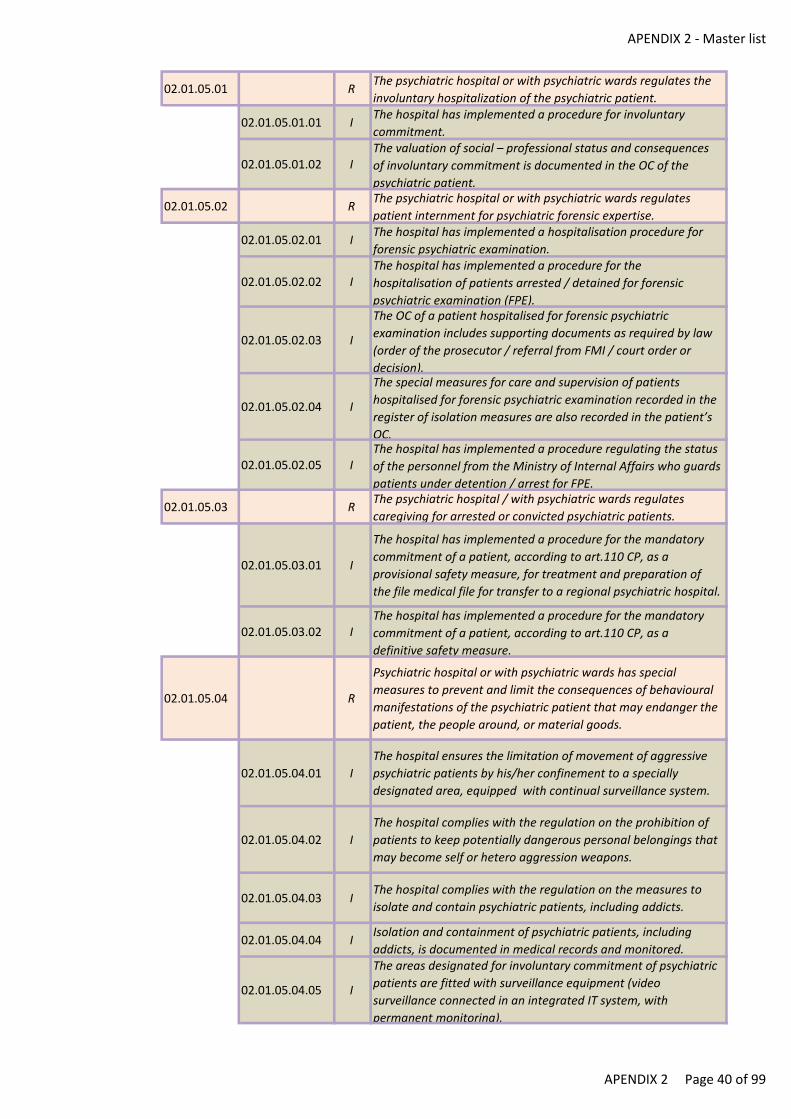
APENDIX 2 - Master list
02.01.05.01 RThe psychiatric hospital or with psychiatric wards regulates the
involuntary hospitalization of the psychiatric patient.
02.01.05.01.01 IThe hospital has implemented a procedure for involuntary
commitment.
02.01.05.01.02 IThe valuation of social – professional status and consequences
of involuntary commitment is documented in the OC of the
psychiatric patient.
02.01.05.02 RThe psychiatric hospital or with psychiatric wards regulates
patient internment for psychiatric forensic expertise.
02.01.05.02.01 IThe hospital has implemented a hospitalisation procedure for
forensic psychiatric examination.
02.01.05.02.02 IThe hospital has implemented a procedure for the
hospitalisation of patients arrested / detained for forensic
psychiatric examination (FPE).
02.01.05.02.03 I
The OC of a patient hospitalised for forensic psychiatric
examination includes supporting documents as required by law
(order of the prosecutor / referral from FMI / court order or
decision).
02.01.05.02.04 I
The special measures for care and supervision of patients
hospitalised for forensic psychiatric examination recorded in the
register of isolation measures are also recorded in the patient’s
OC.
02.01.05.02.05 IThe hospital has implemented a procedure regulating the status
of the personnel from the Ministry of Internal Affairs who guards
patients under detention / arrest for FPE.
02.01.05.03 RThe psychiatric hospital / with psychiatric wards regulates
caregiving for arrested or convicted psychiatric patients.
02.01.05.03.01 I
The hospital has implemented a procedure for the mandatory
commitment of a patient, according to art.110 CP, as a
provisional safety measure, for treatment and preparation of
the file medical file for transfer to a regional psychiatric hospital.
02.01.05.03.02 IThe hospital has implemented a procedure for the mandatory
commitment of a patient, according to art.110 CP, as a
definitive safety measure.
02.01.05.04 R
Psychiatric hospital or with psychiatric wards has special
measures to prevent and limit the consequences of behavioural
manifestations of the psychiatric patient that may endanger the
patient, the people around, or material goods.
02.01.05.04.01 I
The hospital ensures the limitation of movement of aggressive
psychiatric patients by his/her confinement to a specially
designated area, equipped with continual surveillance system.
02.01.05.04.02 I
The hospital complies with the regulation on the prohibition of
patients to keep potentially dangerous personal belongings that
may become self or hetero aggression weapons.
02.01.05.04.03 IThe hospital complies with the regulation on the measures to
isolate and contain psychiatric patients, including addicts.
02.01.05.04.04 IIsolation and containment of psychiatric patients, including
addicts, is documented in medical records and monitored.
02.01.05.04.05 I
The areas designated for involuntary commitment of psychiatric
patients are fitted with surveillance equipment (video
surveillance connected in an integrated IT system, with
permanent monitoring).
APENDIX 2 Page 40 of 99

APENDIX 2 - Master list
02.01.05.04.06 IAggressive patients are immobilised using a system of cuffs (for
the four limbs and torso), according to the applicable regulation,
for a limited period of time.
02.01.05.04.07 Iaggressive patients are isolated in a special designated room, at
the recommendation of the doctor. for a limited period of time.
02.01.05.04.08 IThe doctor’s decision to immobilise/isolate an aggressive patient
is documented in the OC.
02.01.05.05 RThe discharge of the psychiatric patient from psychiatric
hospitals or psychiatric wards is regulated and adapted to the
way of admission.
02.01.05.05.01 IThe hospital complies with the procedure for the discharge and
attendance of the involuntary committed patient by a relatives.
02.01.05.05.02 IThe hospital complies with the discharge procedure and
attendance provided to patients committed as a provisional or
definitive safety measure.
02.01.05.05.03 I
The patient admitted on the grounds of art.110 CP is discharged
immediately after the receipt of the sentence replacing the
involuntary commitment with that provided for under art.109
CP, namely compulsory outpatient treatment.
02.02 S
The initial evaluation aims to identify patients' needs in the
context of known exposure to risk factors (environmental,
social, economic, behavioural and biological) and establishes
the need for care and medical care for them.
02.02.01 CrThe hospital clearly defines the process of patient needs
assessment in order to establish the appropriate health care
plan.
02.02.01.01 R
Depending on the patient's initial identification, a decision
regarding the patient's admission and the means of treatment
as ambulatory care / day-hospitalization / continuous
hospitalization is made.
02.02.01.01.01 IDoctors are trained in the consistent application of the criteria
for dealing with the case (outpatient clinic/day
hospitalisation/continuous hospitalisation).
02.02.01.01.02 IThe medical council carries out monthly evaluations of the
compliance with the criteria for dealing with the case, based on
the reviews of the heads of wards.
02.02.01.01.03 IInitial evaluation of the patients also includes the individual
infection risks and is documented in medical records.
02.02.01.01.04 IPatient evaluation – depending on his/her immediate care needs
(transportation on the ward, diet, type of bed, type of mattress
etc) – is documented in the OC.
02.02.01.01.05 IGeneral and, as applicable, local cleaning and disinfection of
open wounds of transferred patients is regulated and
implemented.
02.02.01.02 RThe hospital has designed a procedure to refer patients whose
pathologies fall outside of its area of competency and facilitates
access to the services they need.
02.02.01.02.01 IRecords exist of the categories of patients who exceeded the
competence of the hospital.
02.02.01.02.02 I
Working cooperation agreements exist with other healthcare
units for the transfer of patients or their access to healthcare
services, where the hospital’s competence / capability to deal
with the case is exceeded.
APENDIX 2 Page 41 of 99
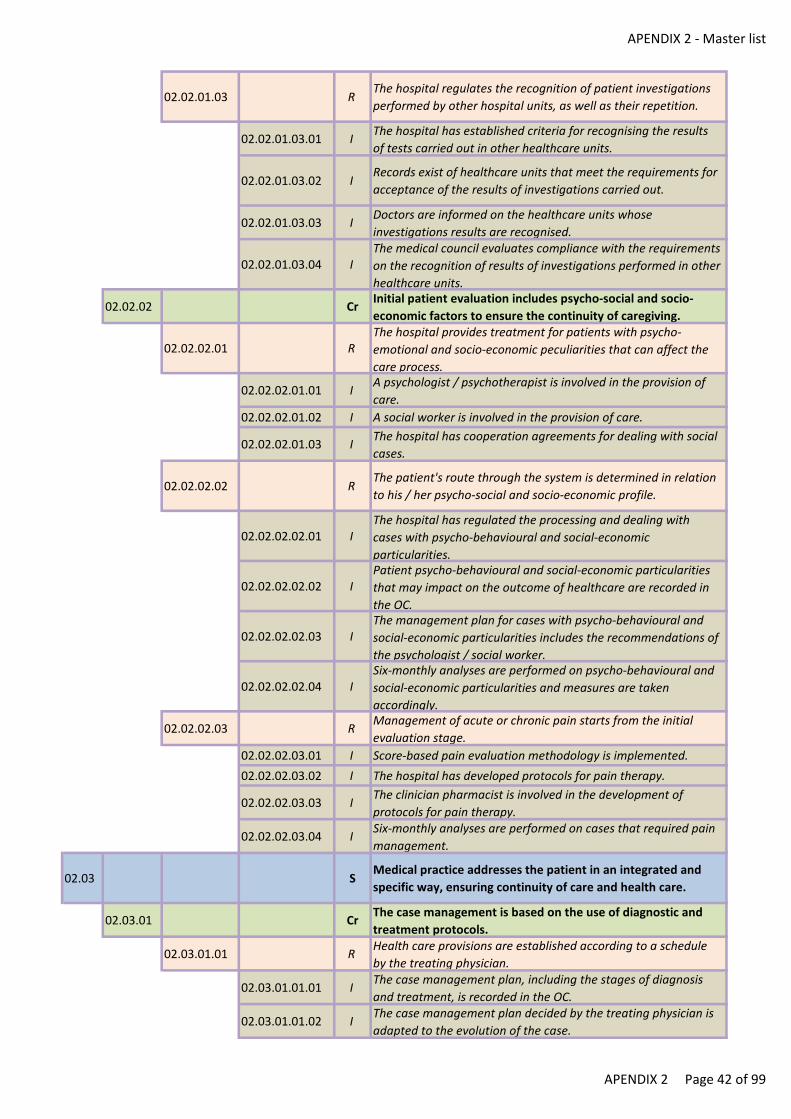
APENDIX 2 - Master list
02.02.01.03 RThe hospital regulates the recognition of patient investigations
performed by other hospital units, as well as their repetition.
02.02.01.03.01 IThe hospital has established criteria for recognising the results
of tests carried out in other healthcare units.
02.02.01.03.02 IRecords exist of healthcare units that meet the requirements for
acceptance of the results of investigations carried out.
02.02.01.03.03 IDoctors are informed on the healthcare units whose
investigations results are recognised.
02.02.01.03.04 IThe medical council evaluates compliance with the requirements
on the recognition of results of investigations performed in other
healthcare units.
02.02.02 CrInitial patient evaluation includes psycho-social and socio-
economic factors to ensure the continuity of caregiving.
02.02.02.01 RThe hospital provides treatment for patients with psycho-
emotional and socio-economic peculiarities that can affect the
care process.
02.02.02.01.01 IA psychologist / psychotherapist is involved in the provision of
care.
02.02.02.01.02 I A social worker is involved in the provision of care.
02.02.02.01.03 IThe hospital has cooperation agreements for dealing with social
cases.
02.02.02.02 RThe patient's route through the system is determined in relation
to his / her psycho-social and socio-economic profile.
02.02.02.02.01 IThe hospital has regulated the processing and dealing with
cases with psycho-behavioural and social-economic
particularities.
02.02.02.02.02 IPatient psycho-behavioural and social-economic particularities
that may impact on the outcome of healthcare are recorded in
the OC.
02.02.02.02.03 IThe management plan for cases with psycho-behavioural and
social-economic particularities includes the recommendations of
the psychologist / social worker.
02.02.02.02.04 ISix-monthly analyses are performed on psycho-behavioural and
social-economic particularities and measures are taken
accordingly.
02.02.02.03 RManagement of acute or chronic pain starts from the initial
evaluation stage.
02.02.02.03.01 I Score-based pain evaluation methodology is implemented.
02.02.02.03.02 I The hospital has developed protocols for pain therapy.
02.02.02.03.03 IThe clinician pharmacist is involved in the development of
protocols for pain therapy.
02.02.02.03.04 ISix-monthly analyses are performed on cases that required pain
management.
02.03 SMedical practice addresses the patient in an integrated and
specific way, ensuring continuity of care and health care.
02.03.01 CrThe case management is based on the use of diagnostic and
treatment protocols.
02.03.01.01 RHealth care provisions are established according to a schedule
by the treating physician.
02.03.01.01.01 IThe case management plan, including the stages of diagnosis
and treatment, is recorded in the OC.
02.03.01.01.02 IThe case management plan decided by the treating physician is
adapted to the evolution of the case.
APENDIX 2 Page 42 of 99
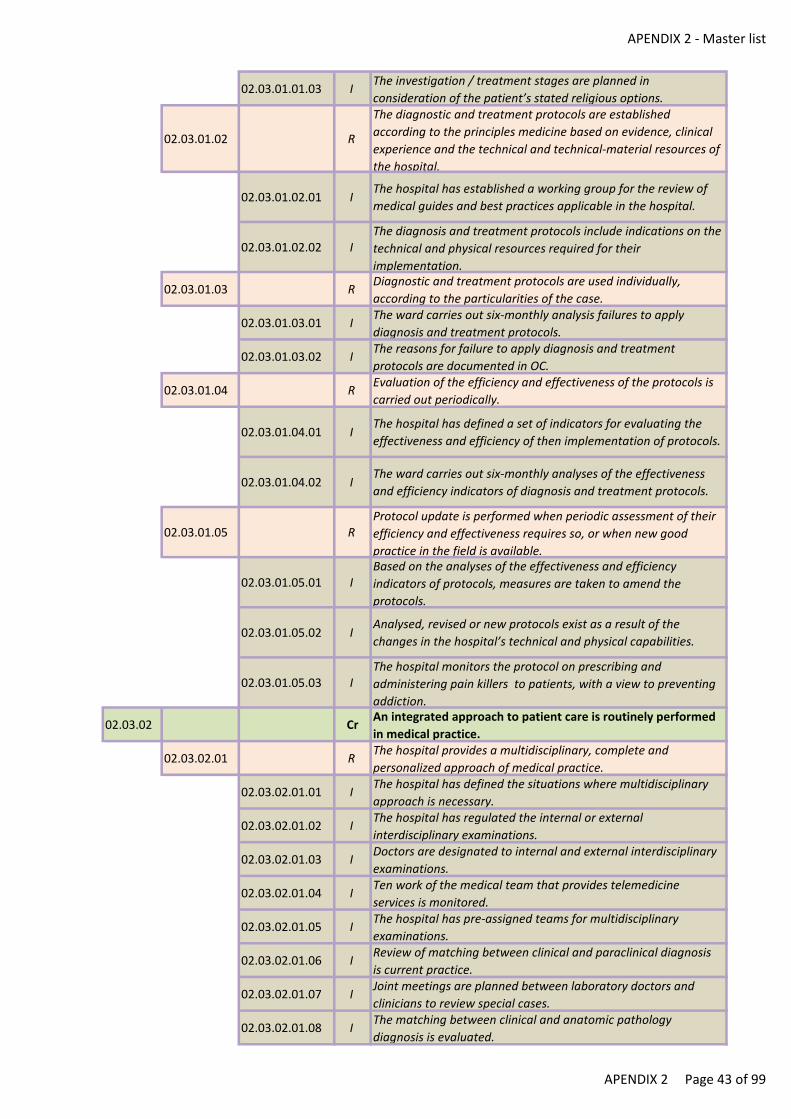
APENDIX 2 - Master list
02.03.01.01.03 IThe investigation / treatment stages are planned in
consideration of the patient’s stated religious options.
02.03.01.02 R
The diagnostic and treatment protocols are established
according to the principles medicine based on evidence, clinical
experience and the technical and technical-material resources of
the hospital.
02.03.01.02.01 IThe hospital has established a working group for the review of
medical guides and best practices applicable in the hospital.
02.03.01.02.02 IThe diagnosis and treatment protocols include indications on the
technical and physical resources required for their
implementation.
02.03.01.03 RDiagnostic and treatment protocols are used individually,
according to the particularities of the case.
02.03.01.03.01 IThe ward carries out six-monthly analysis failures to apply
diagnosis and treatment protocols.
02.03.01.03.02 IThe reasons for failure to apply diagnosis and treatment
protocols are documented in OC.
02.03.01.04 REvaluation of the efficiency and effectiveness of the protocols is
carried out periodically.
02.03.01.04.01 IThe hospital has defined a set of indicators for evaluating the
effectiveness and efficiency of then implementation of protocols.
02.03.01.04.02 IThe ward carries out six-monthly analyses of the effectiveness
and efficiency indicators of diagnosis and treatment protocols.
02.03.01.05 RProtocol update is performed when periodic assessment of their
efficiency and effectiveness requires so, or when new good
practice in the field is available.
02.03.01.05.01 IBased on the analyses of the effectiveness and efficiency
indicators of protocols, measures are taken to amend the
protocols.
02.03.01.05.02 IAnalysed, revised or new protocols exist as a result of the
changes in the hospital’s technical and physical capabilities.
02.03.01.05.03 IThe hospital monitors the protocol on prescribing and
administering pain killers to patients, with a view to preventing
addiction.
02.03.02 CrAn integrated approach to patient care is routinely performed
in medical practice.
02.03.02.01 RThe hospital provides a multidisciplinary, complete and
personalized approach of medical practice.
02.03.02.01.01 IThe hospital has defined the situations where multidisciplinary
approach is necessary.
02.03.02.01.02 IThe hospital has regulated the internal or external
interdisciplinary examinations.
02.03.02.01.03 IDoctors are designated to internal and external interdisciplinary
examinations.
02.03.02.01.04 ITen work of the medical team that provides telemedicine
services is monitored.
02.03.02.01.05 IThe hospital has pre-assigned teams for multidisciplinary
examinations.
02.03.02.01.06 IReview of matching between clinical and paraclinical diagnosis
is current practice.
02.03.02.01.07 IJoint meetings are planned between laboratory doctors and
clinicians to review special cases.
02.03.02.01.08 IThe matching between clinical and anatomic pathology
diagnosis is evaluated.
APENDIX 2 Page 43 of 99
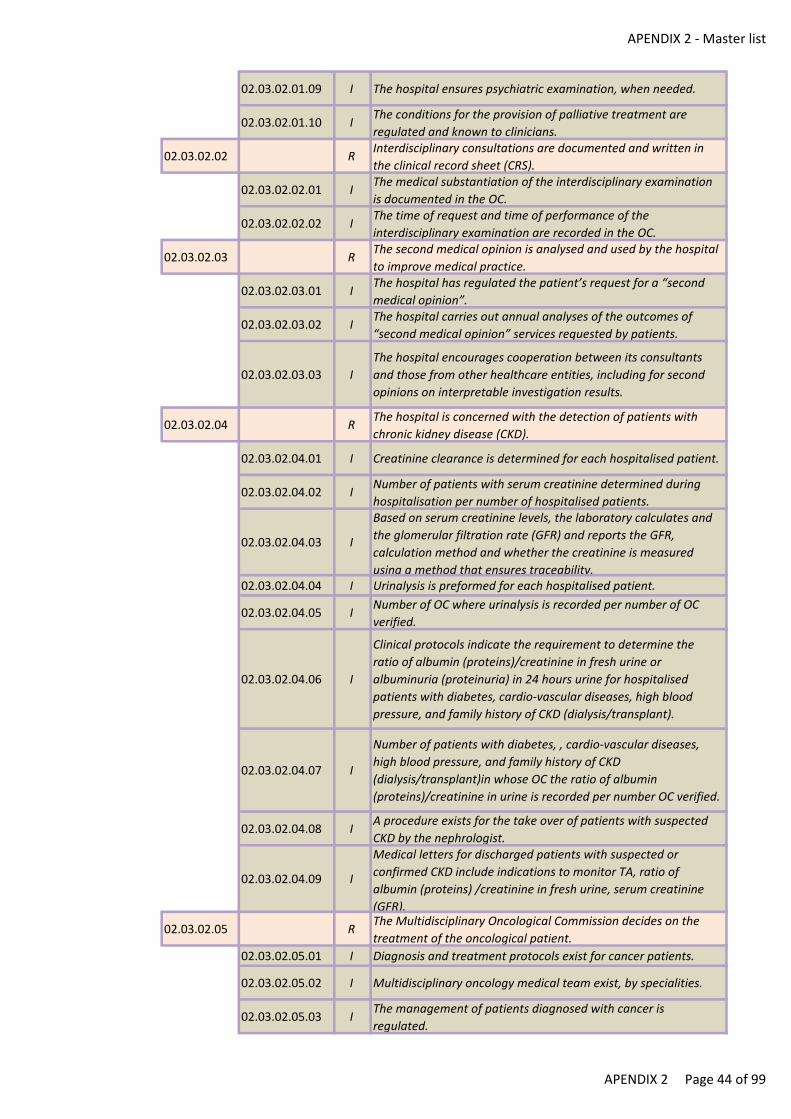
APENDIX 2 - Master list
02.03.02.01.09 I The hospital ensures psychiatric examination, when needed.
02.03.02.01.10 IThe conditions for the provision of palliative treatment are
regulated and known to clinicians.
02.03.02.02 RInterdisciplinary consultations are documented and written in
the clinical record sheet (CRS).
02.03.02.02.01 IThe medical substantiation of the interdisciplinary examination
is documented in the OC.
02.03.02.02.02 IThe time of request and time of performance of the
interdisciplinary examination are recorded in the OC.
02.03.02.03 RThe second medical opinion is analysed and used by the hospital
to improve medical practice.
02.03.02.03.01 IThe hospital has regulated the patient’s request for a “second
medical opinion”.
02.03.02.03.02 IThe hospital carries out annual analyses of the outcomes of
“second medical opinion” services requested by patients.
02.03.02.03.03 I
The hospital encourages cooperation between its consultants
and those from other healthcare entities, including for second
opinions on interpretable investigation results.
02.03.02.04 RThe hospital is concerned with the detection of patients with
chronic kidney disease (CKD).
02.03.02.04.01 I Creatinine clearance is determined for each hospitalised patient.
02.03.02.04.02 INumber of patients with serum creatinine determined during
hospitalisation per number of hospitalised patients.
02.03.02.04.03 I
Based on serum creatinine levels, the laboratory calculates and
the glomerular filtration rate (GFR) and reports the GFR,
calculation method and whether the creatinine is measured
using a method that ensures traceability. 02.03.02.04.04 I Urinalysis is preformed for each hospitalised patient.
02.03.02.04.05 INumber of OC where urinalysis is recorded per number of OC
verified.
02.03.02.04.06 I
Clinical protocols indicate the requirement to determine the
ratio of albumin (proteins)/creatinine in fresh urine or
albuminuria (proteinuria) in 24 hours urine for hospitalised
patients with diabetes, cardio-vascular diseases, high blood
pressure, and family history of CKD (dialysis/transplant).
02.03.02.04.07 I
Number of patients with diabetes, , cardio-vascular diseases,
high blood pressure, and family history of CKD
(dialysis/transplant)in whose OC the ratio of albumin
(proteins)/creatinine in urine is recorded per number OC verified.
02.03.02.04.08 IA procedure exists for the take over of patients with suspected
CKD by the nephrologist.
02.03.02.04.09 I
Medical letters for discharged patients with suspected or
confirmed CKD include indications to monitor TA, ratio of
albumin (proteins) /creatinine in fresh urine, serum creatinine
(GFR).
02.03.02.05 RThe Multidisciplinary Oncological Commission decides on the
treatment of the oncological patient.
02.03.02.05.01 I Diagnosis and treatment protocols exist for cancer patients.
02.03.02.05.02 I Multidisciplinary oncology medical team exist, by specialities.
02.03.02.05.03 IThe management of patients diagnosed with cancer is
regulated.
APENDIX 2 Page 44 of 99
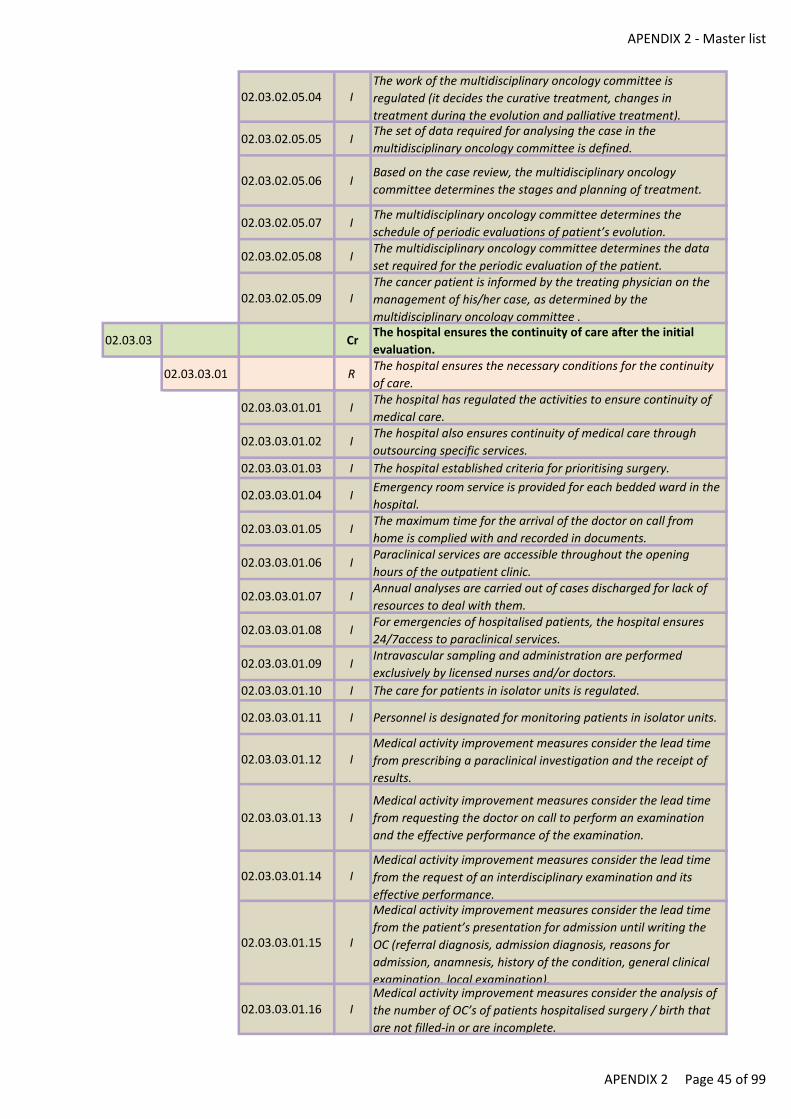
APENDIX 2 - Master list
02.03.02.05.04 IThe work of the multidisciplinary oncology committee is
regulated (it decides the curative treatment, changes in
treatment during the evolution and palliative treatment).
02.03.02.05.05 IThe set of data required for analysing the case in the
multidisciplinary oncology committee is defined.
02.03.02.05.06 IBased on the case review, the multidisciplinary oncology
committee determines the stages and planning of treatment.
02.03.02.05.07 IThe multidisciplinary oncology committee determines the
schedule of periodic evaluations of patient’s evolution.
02.03.02.05.08 IThe multidisciplinary oncology committee determines the data
set required for the periodic evaluation of the patient.
02.03.02.05.09 IThe cancer patient is informed by the treating physician on the
management of his/her case, as determined by the
multidisciplinary oncology committee .
02.03.03 CrThe hospital ensures the continuity of care after the initial
evaluation.
02.03.03.01 RThe hospital ensures the necessary conditions for the continuity
of care.
02.03.03.01.01 IThe hospital has regulated the activities to ensure continuity of
medical care.
02.03.03.01.02 IThe hospital also ensures continuity of medical care through
outsourcing specific services.
02.03.03.01.03 I The hospital established criteria for prioritising surgery.
02.03.03.01.04 IEmergency room service is provided for each bedded ward in the
hospital.
02.03.03.01.05 IThe maximum time for the arrival of the doctor on call from
home is complied with and recorded in documents.
02.03.03.01.06 IParaclinical services are accessible throughout the opening
hours of the outpatient clinic.
02.03.03.01.07 IAnnual analyses are carried out of cases discharged for lack of
resources to deal with them.
02.03.03.01.08 IFor emergencies of hospitalised patients, the hospital ensures
24/7access to paraclinical services.
02.03.03.01.09 IIntravascular sampling and administration are performed
exclusively by licensed nurses and/or doctors.
02.03.03.01.10 I The care for patients in isolator units is regulated.
02.03.03.01.11 I Personnel is designated for monitoring patients in isolator units.
02.03.03.01.12 IMedical activity improvement measures consider the lead time
from prescribing a paraclinical investigation and the receipt of
results.
02.03.03.01.13 I
Medical activity improvement measures consider the lead time
from requesting the doctor on call to perform an examination
and the effective performance of the examination.
02.03.03.01.14 IMedical activity improvement measures consider the lead time
from the request of an interdisciplinary examination and its
effective performance.
02.03.03.01.15 I
Medical activity improvement measures consider the lead time
from the patient’s presentation for admission until writing the
OC (referral diagnosis, admission diagnosis, reasons for
admission, anamnesis, history of the condition, general clinical
examination, local examination).
02.03.03.01.16 IMedical activity improvement measures consider the analysis of
the number of OC’s of patients hospitalised surgery / birth that
are not filled-in or are incomplete.
APENDIX 2 Page 45 of 99
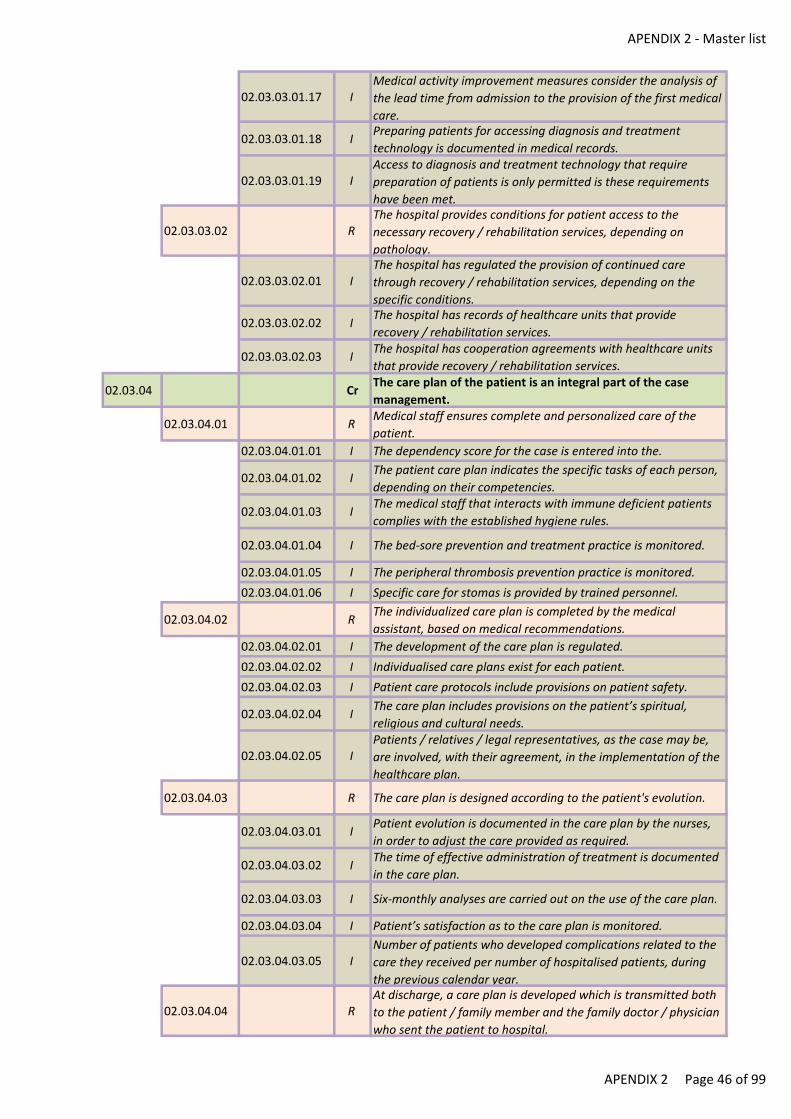
APENDIX 2 - Master list
02.03.03.01.17 IMedical activity improvement measures consider the analysis of
the lead time from admission to the provision of the first medical
care.
02.03.03.01.18 IPreparing patients for accessing diagnosis and treatment
technology is documented in medical records.
02.03.03.01.19 IAccess to diagnosis and treatment technology that require
preparation of patients is only permitted is these requirements
have been met.
02.03.03.02 RThe hospital provides conditions for patient access to the
necessary recovery / rehabilitation services, depending on
pathology.
02.03.03.02.01 IThe hospital has regulated the provision of continued care
through recovery / rehabilitation services, depending on the
specific conditions.
02.03.03.02.02 IThe hospital has records of healthcare units that provide
recovery / rehabilitation services.
02.03.03.02.03 IThe hospital has cooperation agreements with healthcare units
that provide recovery / rehabilitation services.
02.03.04 CrThe care plan of the patient is an integral part of the case
management.
02.03.04.01 RMedical staff ensures complete and personalized care of the
patient.
02.03.04.01.01 I The dependency score for the case is entered into the.
02.03.04.01.02 IThe patient care plan indicates the specific tasks of each person,
depending on their competencies.
02.03.04.01.03 IThe medical staff that interacts with immune deficient patients
complies with the established hygiene rules.
02.03.04.01.04 I The bed-sore prevention and treatment practice is monitored.
02.03.04.01.05 I The peripheral thrombosis prevention practice is monitored.
02.03.04.01.06 I Specific care for stomas is provided by trained personnel.
02.03.04.02 RThe individualized care plan is completed by the medical
assistant, based on medical recommendations.
02.03.04.02.01 I The development of the care plan is regulated.
02.03.04.02.02 I Individualised care plans exist for each patient.
02.03.04.02.03 I Patient care protocols include provisions on patient safety.
02.03.04.02.04 IThe care plan includes provisions on the patient’s spiritual,
religious and cultural needs.
02.03.04.02.05 IPatients / relatives / legal representatives, as the case may be,
are involved, with their agreement, in the implementation of the
healthcare plan.
02.03.04.03 R The care plan is designed according to the patient's evolution.
02.03.04.03.01 IPatient evolution is documented in the care plan by the nurses,
in order to adjust the care provided as required.
02.03.04.03.02 IThe time of effective administration of treatment is documented
in the care plan.
02.03.04.03.03 I Six-monthly analyses are carried out on the use of the care plan.
02.03.04.03.04 I Patient’s satisfaction as to the care plan is monitored.
02.03.04.03.05 INumber of patients who developed complications related to the
care they received per number of hospitalised patients, during
the previous calendar year.
02.03.04.04 RAt discharge, a care plan is developed which is transmitted both
to the patient / family member and the family doctor / physician
who sent the patient to hospital.
APENDIX 2 Page 46 of 99
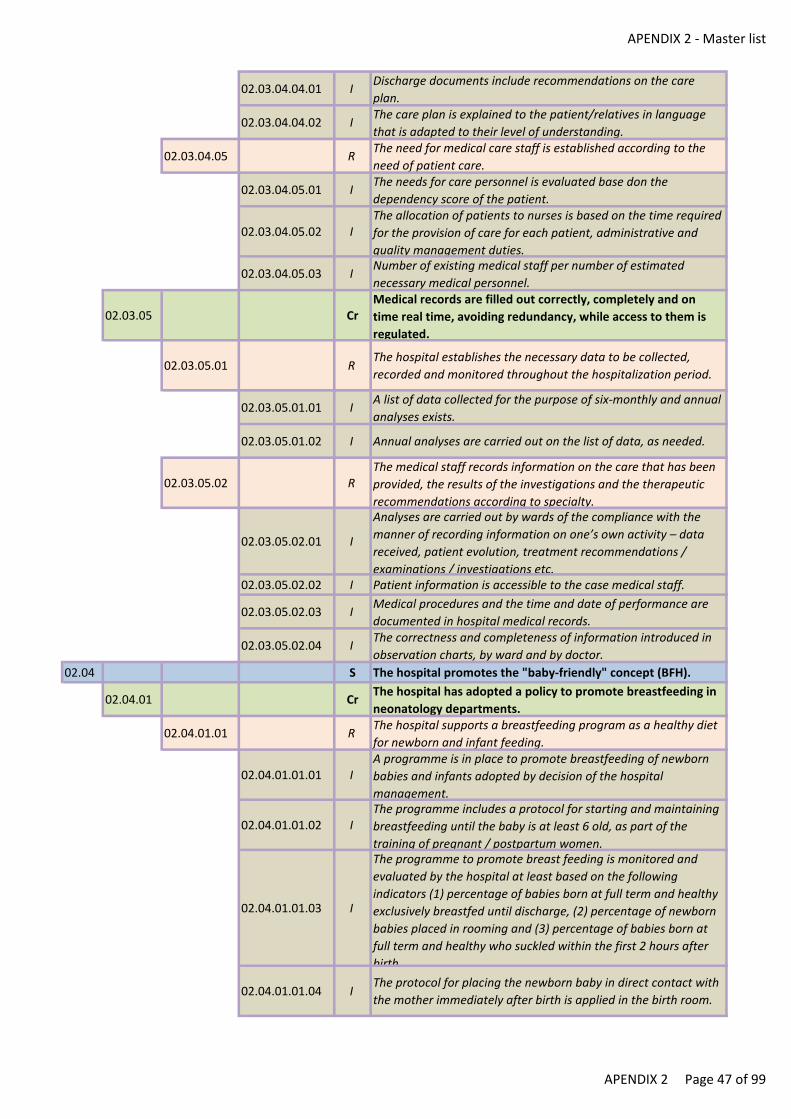
APENDIX 2 - Master list
02.03.04.04.01 IDischarge documents include recommendations on the care
plan.
02.03.04.04.02 IThe care plan is explained to the patient/relatives in language
that is adapted to their level of understanding.
02.03.04.05 RThe need for medical care staff is established according to the
need of patient care.
02.03.04.05.01 IThe needs for care personnel is evaluated base don the
dependency score of the patient.
02.03.04.05.02 IThe allocation of patients to nurses is based on the time required
for the provision of care for each patient, administrative and
quality management duties.
02.03.04.05.03 INumber of existing medical staff per number of estimated
necessary medical personnel.
02.03.05 CrMedical records are filled out correctly, completely and on
time real time, avoiding redundancy, while access to them is
regulated.
02.03.05.01 RThe hospital establishes the necessary data to be collected,
recorded and monitored throughout the hospitalization period.
02.03.05.01.01 IA list of data collected for the purpose of six-monthly and annual
analyses exists.
02.03.05.01.02 I Annual analyses are carried out on the list of data, as needed.
02.03.05.02 RThe medical staff records information on the care that has been
provided, the results of the investigations and the therapeutic
recommendations according to specialty.
02.03.05.02.01 I
Analyses are carried out by wards of the compliance with the
manner of recording information on one’s own activity – data
received, patient evolution, treatment recommendations /
examinations / investigations etc.02.03.05.02.02 I Patient information is accessible to the case medical staff.
02.03.05.02.03 IMedical procedures and the time and date of performance are
documented in hospital medical records.
02.03.05.02.04 IThe correctness and completeness of information introduced in
observation charts, by ward and by doctor.
02.04 S The hospital promotes the "baby-friendly" concept (BFH).
02.04.01 CrThe hospital has adopted a policy to promote breastfeeding in
neonatology departments.
02.04.01.01 RThe hospital supports a breastfeeding program as a healthy diet
for newborn and infant feeding.
02.04.01.01.01 IA programme is in place to promote breastfeeding of newborn
babies and infants adopted by decision of the hospital
management.
02.04.01.01.02 IThe programme includes a protocol for starting and maintaining
breastfeeding until the baby is at least 6 old, as part of the
training of pregnant / postpartum women.
02.04.01.01.03 I
The programme to promote breast feeding is monitored and
evaluated by the hospital at least based on the following
indicators (1) percentage of babies born at full term and healthy
exclusively breastfed until discharge, (2) percentage of newborn
babies placed in rooming and (3) percentage of babies born at
full term and healthy who suckled within the first 2 hours after
birth.
02.04.01.01.04 IThe protocol for placing the newborn baby in direct contact with
the mother immediately after birth is applied in the birth room.
APENDIX 2 Page 47 of 99
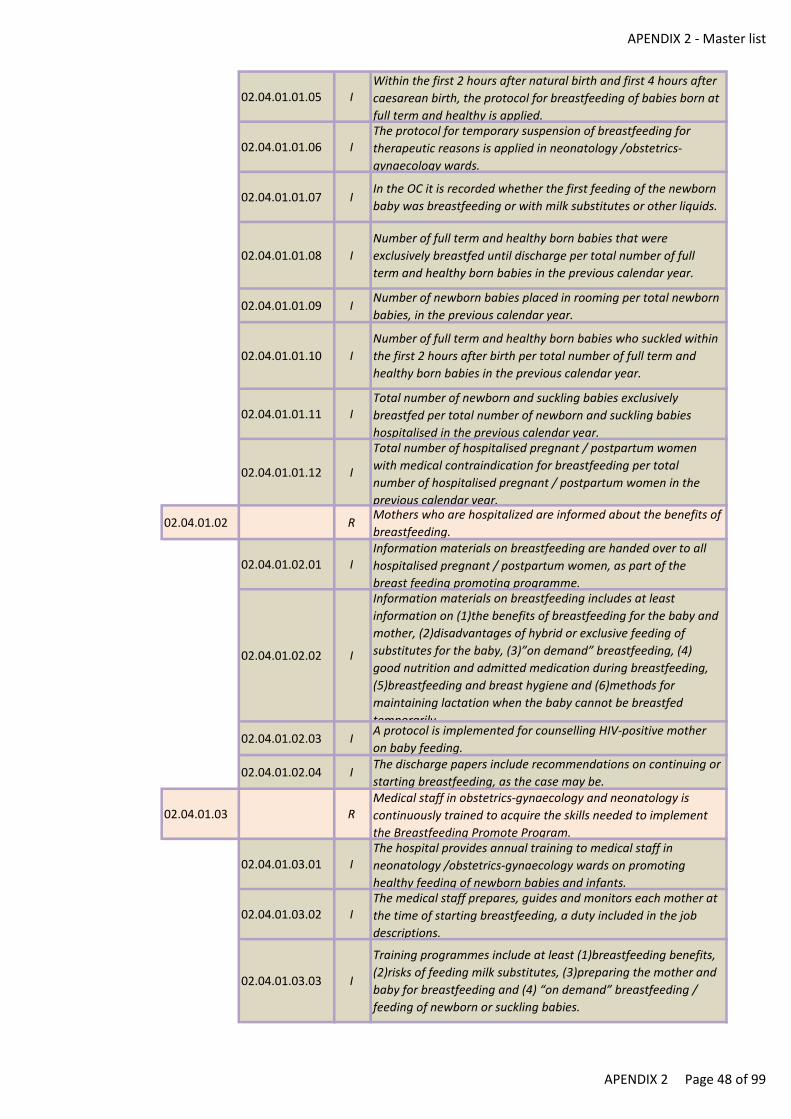
APENDIX 2 - Master list
02.04.01.01.05 IWithin the first 2 hours after natural birth and first 4 hours after
caesarean birth, the protocol for breastfeeding of babies born at
full term and healthy is applied.
02.04.01.01.06 IThe protocol for temporary suspension of breastfeeding for
therapeutic reasons is applied in neonatology /obstetrics-
gynaecology wards.
02.04.01.01.07 IIn the OC it is recorded whether the first feeding of the newborn
baby was breastfeeding or with milk substitutes or other liquids.
02.04.01.01.08 I
Number of full term and healthy born babies that were
exclusively breastfed until discharge per total number of full
term and healthy born babies in the previous calendar year.
02.04.01.01.09 INumber of newborn babies placed in rooming per total newborn
babies, in the previous calendar year.
02.04.01.01.10 I
Number of full term and healthy born babies who suckled within
the first 2 hours after birth per total number of full term and
healthy born babies in the previous calendar year.
02.04.01.01.11 ITotal number of newborn and suckling babies exclusively
breastfed per total number of newborn and suckling babies
hospitalised in the previous calendar year.
02.04.01.01.12 I
Total number of hospitalised pregnant / postpartum women
with medical contraindication for breastfeeding per total
number of hospitalised pregnant / postpartum women in the
previous calendar year.
02.04.01.02 RMothers who are hospitalized are informed about the benefits of
breastfeeding.
02.04.01.02.01 IInformation materials on breastfeeding are handed over to all
hospitalised pregnant / postpartum women, as part of the
breast feeding promoting programme.
02.04.01.02.02 I
Information materials on breastfeeding includes at least
information on (1)the benefits of breastfeeding for the baby and
mother, (2)disadvantages of hybrid or exclusive feeding of
substitutes for the baby, (3)”on demand” breastfeeding, (4)
good nutrition and admitted medication during breastfeeding,
(5)breastfeeding and breast hygiene and (6)methods for
maintaining lactation when the baby cannot be breastfed
temporarily.
02.04.01.02.03 IA protocol is implemented for counselling HIV-positive mother
on baby feeding.
02.04.01.02.04 IThe discharge papers include recommendations on continuing or
starting breastfeeding, as the case may be.
02.04.01.03 RMedical staff in obstetrics-gynaecology and neonatology is
continuously trained to acquire the skills needed to implement
the Breastfeeding Promote Program.
02.04.01.03.01 IThe hospital provides annual training to medical staff in
neonatology /obstetrics-gynaecology wards on promoting
healthy feeding of newborn babies and infants.
02.04.01.03.02 IThe medical staff prepares, guides and monitors each mother at
the time of starting breastfeeding, a duty included in the job
descriptions.
02.04.01.03.03 I
Training programmes include at least (1)breastfeeding benefits,
(2)risks of feeding milk substitutes, (3)preparing the mother and
baby for breastfeeding and (4) “on demand” breastfeeding /
feeding of newborn or suckling babies.
APENDIX 2 Page 48 of 99
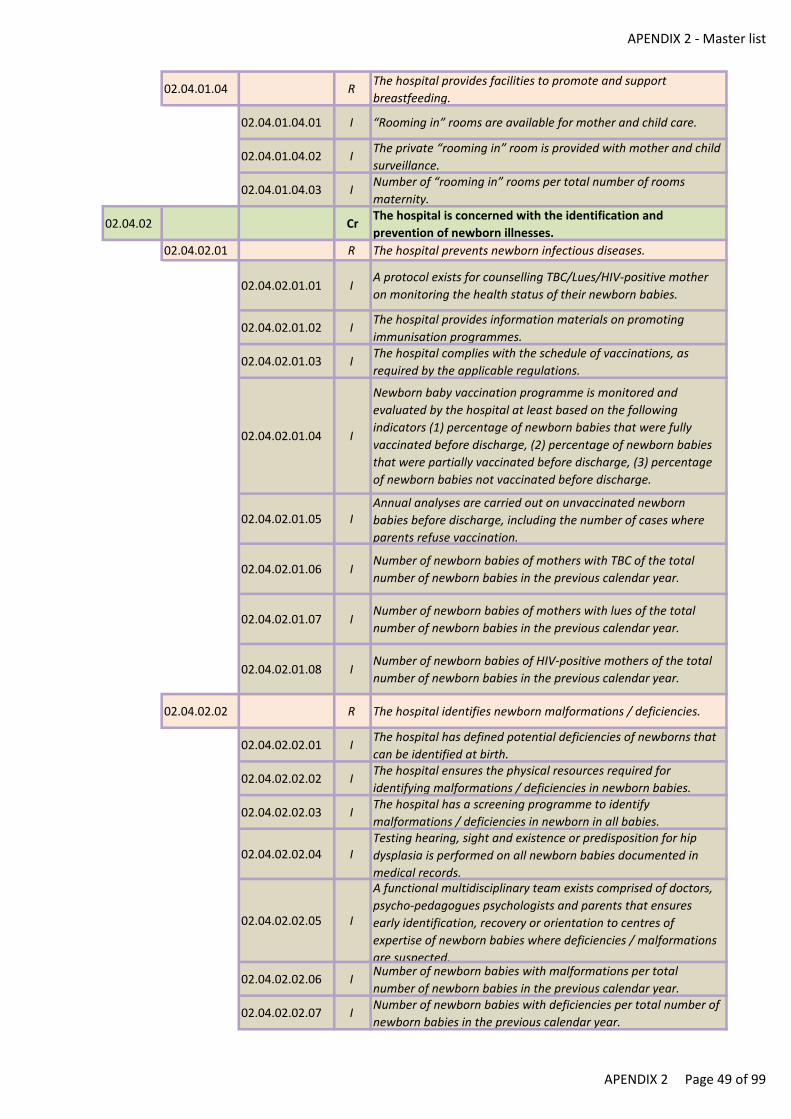
APENDIX 2 - Master list
02.04.01.04 RThe hospital provides facilities to promote and support
breastfeeding.
02.04.01.04.01 I “Rooming in” rooms are available for mother and child care.
02.04.01.04.02 IThe private “rooming in” room is provided with mother and child
surveillance.
02.04.01.04.03 INumber of “rooming in” rooms per total number of rooms
maternity.
02.04.02 CrThe hospital is concerned with the identification and
prevention of newborn illnesses.
02.04.02.01 R The hospital prevents newborn infectious diseases.
02.04.02.01.01 IA protocol exists for counselling TBC/Lues/HIV-positive mother
on monitoring the health status of their newborn babies.
02.04.02.01.02 IThe hospital provides information materials on promoting
immunisation programmes.
02.04.02.01.03 IThe hospital complies with the schedule of vaccinations, as
required by the applicable regulations.
02.04.02.01.04 I
Newborn baby vaccination programme is monitored and
evaluated by the hospital at least based on the following
indicators (1) percentage of newborn babies that were fully
vaccinated before discharge, (2) percentage of newborn babies
that were partially vaccinated before discharge, (3) percentage
of newborn babies not vaccinated before discharge.
02.04.02.01.05 IAnnual analyses are carried out on unvaccinated newborn
babies before discharge, including the number of cases where
parents refuse vaccination.
02.04.02.01.06 INumber of newborn babies of mothers with TBC of the total
number of newborn babies in the previous calendar year.
02.04.02.01.07 INumber of newborn babies of mothers with lues of the total
number of newborn babies in the previous calendar year.
02.04.02.01.08 INumber of newborn babies of HIV-positive mothers of the total
number of newborn babies in the previous calendar year.
02.04.02.02 R The hospital identifies newborn malformations / deficiencies.
02.04.02.02.01 IThe hospital has defined potential deficiencies of newborns that
can be identified at birth.
02.04.02.02.02 IThe hospital ensures the physical resources required for
identifying malformations / deficiencies in newborn babies.
02.04.02.02.03 IThe hospital has a screening programme to identify
malformations / deficiencies in newborn in all babies.
02.04.02.02.04 ITesting hearing, sight and existence or predisposition for hip
dysplasia is performed on all newborn babies documented in
medical records.
02.04.02.02.05 I
A functional multidisciplinary team exists comprised of doctors,
psycho-pedagogues psychologists and parents that ensures
early identification, recovery or orientation to centres of
expertise of newborn babies where deficiencies / malformations
are suspected.
02.04.02.02.06 INumber of newborn babies with malformations per total
number of newborn babies in the previous calendar year.
02.04.02.02.07 INumber of newborn babies with deficiencies per total number of
newborn babies in the previous calendar year.
APENDIX 2 Page 49 of 99
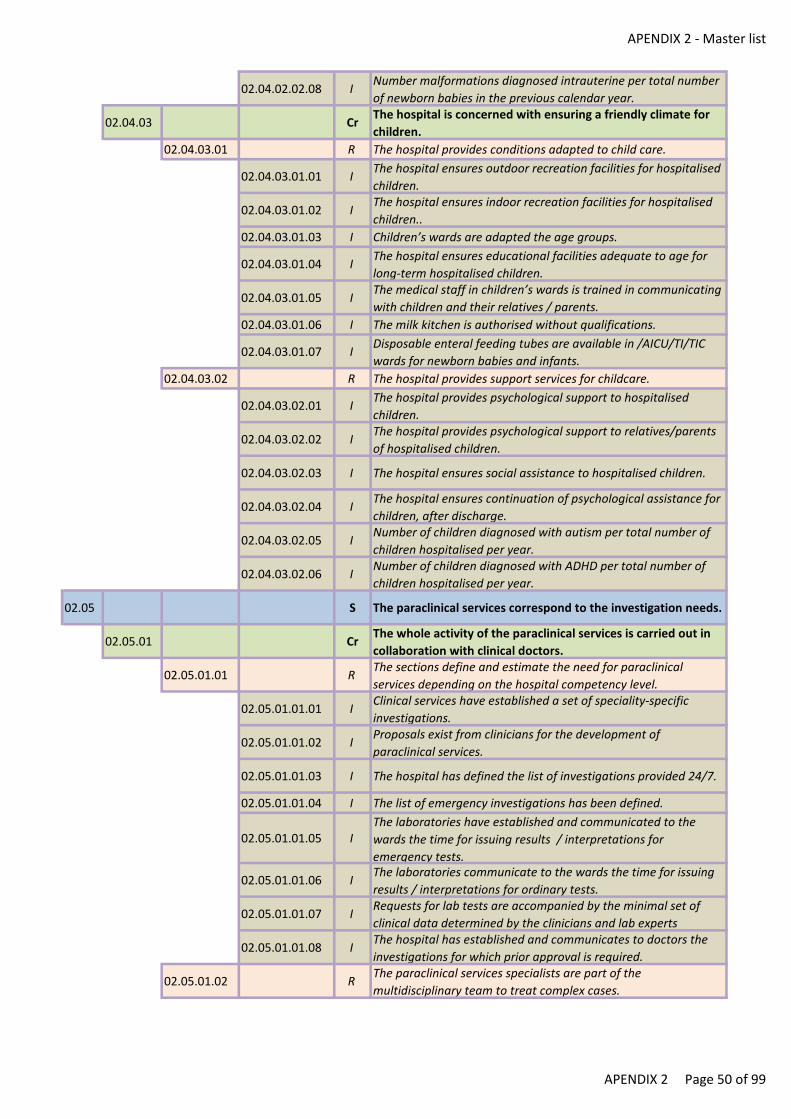
APENDIX 2 - Master list
02.04.02.02.08 INumber malformations diagnosed intrauterine per total number
of newborn babies in the previous calendar year.
02.04.03 CrThe hospital is concerned with ensuring a friendly climate for
children.
02.04.03.01 R The hospital provides conditions adapted to child care.
02.04.03.01.01 IThe hospital ensures outdoor recreation facilities for hospitalised
children.
02.04.03.01.02 IThe hospital ensures indoor recreation facilities for hospitalised
children..
02.04.03.01.03 I Children’s wards are adapted the age groups.
02.04.03.01.04 IThe hospital ensures educational facilities adequate to age for
long-term hospitalised children.
02.04.03.01.05 IThe medical staff in children’s wards is trained in communicating
with children and their relatives / parents.
02.04.03.01.06 I The milk kitchen is authorised without qualifications.
02.04.03.01.07 IDisposable enteral feeding tubes are available in /AICU/TI/TIC
wards for newborn babies and infants.
02.04.03.02 R The hospital provides support services for childcare.
02.04.03.02.01 IThe hospital provides psychological support to hospitalised
children.
02.04.03.02.02 IThe hospital provides psychological support to relatives/parents
of hospitalised children.
02.04.03.02.03 I The hospital ensures social assistance to hospitalised children.
02.04.03.02.04 IThe hospital ensures continuation of psychological assistance for
children, after discharge.
02.04.03.02.05 INumber of children diagnosed with autism per total number of
children hospitalised per year.
02.04.03.02.06 INumber of children diagnosed with ADHD per total number of
children hospitalised per year.
02.05 S The paraclinical services correspond to the investigation needs.
02.05.01 CrThe whole activity of the paraclinical services is carried out in
collaboration with clinical doctors.
02.05.01.01 RThe sections define and estimate the need for paraclinical
services depending on the hospital competency level.
02.05.01.01.01 IClinical services have established a set of speciality-specific
investigations.
02.05.01.01.02 IProposals exist from clinicians for the development of
paraclinical services.
02.05.01.01.03 I The hospital has defined the list of investigations provided 24/7.
02.05.01.01.04 I The list of emergency investigations has been defined.
02.05.01.01.05 IThe laboratories have established and communicated to the
wards the time for issuing results / interpretations for
emergency tests.
02.05.01.01.06 IThe laboratories communicate to the wards the time for issuing
results / interpretations for ordinary tests.
02.05.01.01.07 IRequests for lab tests are accompanied by the minimal set of
clinical data determined by the clinicians and lab experts
02.05.01.01.08 IThe hospital has established and communicates to doctors the
investigations for which prior approval is required.
02.05.01.02 RThe paraclinical services specialists are part of the
multidisciplinary team to treat complex cases.
APENDIX 2 Page 50 of 99
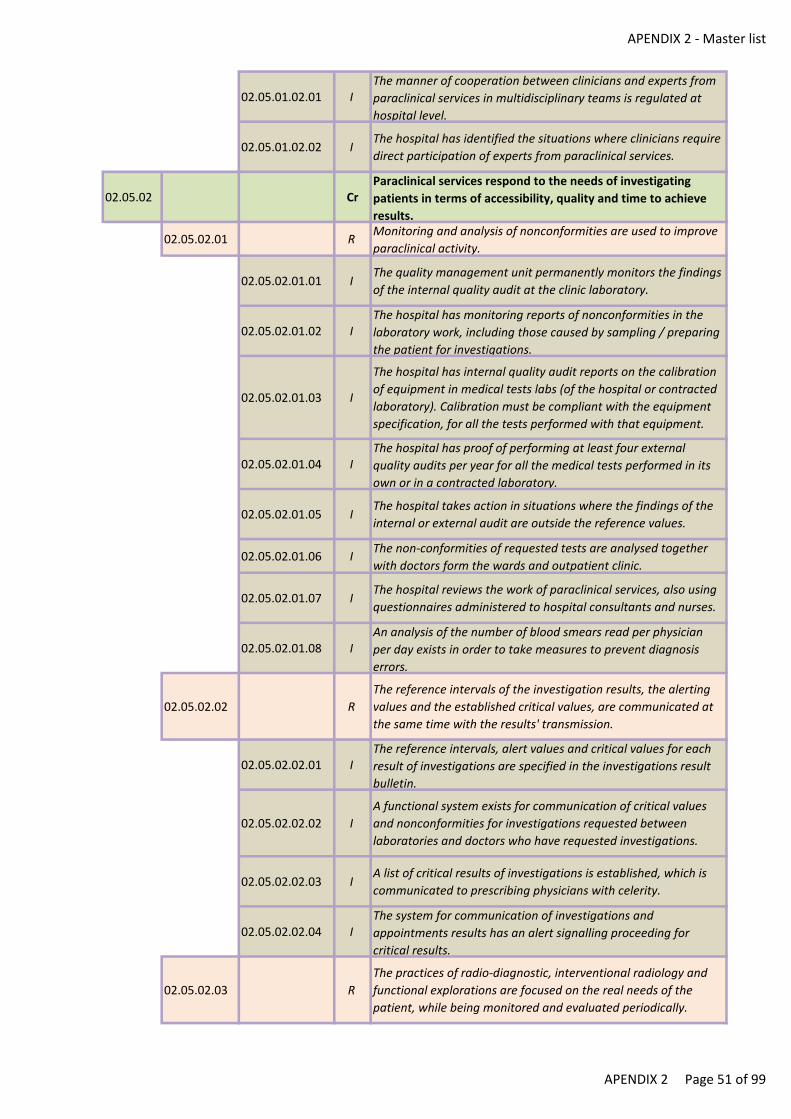
APENDIX 2 - Master list
02.05.01.02.01 IThe manner of cooperation between clinicians and experts from
paraclinical services in multidisciplinary teams is regulated at
hospital level.
02.05.01.02.02 IThe hospital has identified the situations where clinicians require
direct participation of experts from paraclinical services.
02.05.02 CrParaclinical services respond to the needs of investigating
patients in terms of accessibility, quality and time to achieve
results.
02.05.02.01 RMonitoring and analysis of nonconformities are used to improve
paraclinical activity.
02.05.02.01.01 IThe quality management unit permanently monitors the findings
of the internal quality audit at the clinic laboratory.
02.05.02.01.02 IThe hospital has monitoring reports of nonconformities in the
laboratory work, including those caused by sampling / preparing
the patient for investigations.
02.05.02.01.03 I
The hospital has internal quality audit reports on the calibration
of equipment in medical tests labs (of the hospital or contracted
laboratory). Calibration must be compliant with the equipment
specification, for all the tests performed with that equipment.
02.05.02.01.04 IThe hospital has proof of performing at least four external
quality audits per year for all the medical tests performed in its
own or in a contracted laboratory.
02.05.02.01.05 IThe hospital takes action in situations where the findings of the
internal or external audit are outside the reference values.
02.05.02.01.06 IThe non-conformities of requested tests are analysed together
with doctors form the wards and outpatient clinic.
02.05.02.01.07 IThe hospital reviews the work of paraclinical services, also using
questionnaires administered to hospital consultants and nurses.
02.05.02.01.08 IAn analysis of the number of blood smears read per physician
per day exists in order to take measures to prevent diagnosis
errors.
02.05.02.02 R
The reference intervals of the investigation results, the alerting
values and the established critical values, are communicated at
the same time with the results' transmission.
02.05.02.02.01 IThe reference intervals, alert values and critical values for each
result of investigations are specified in the investigations result
bulletin.
02.05.02.02.02 I
A functional system exists for communication of critical values
and nonconformities for investigations requested between
laboratories and doctors who have requested investigations.
02.05.02.02.03 IA list of critical results of investigations is established, which is
communicated to prescribing physicians with celerity.
02.05.02.02.04 IThe system for communication of investigations and
appointments results has an alert signalling proceeding for
critical results.
02.05.02.03 R
The practices of radio-diagnostic, interventional radiology and
functional explorations are focused on the real needs of the
patient, while being monitored and evaluated periodically.
APENDIX 2 Page 51 of 99
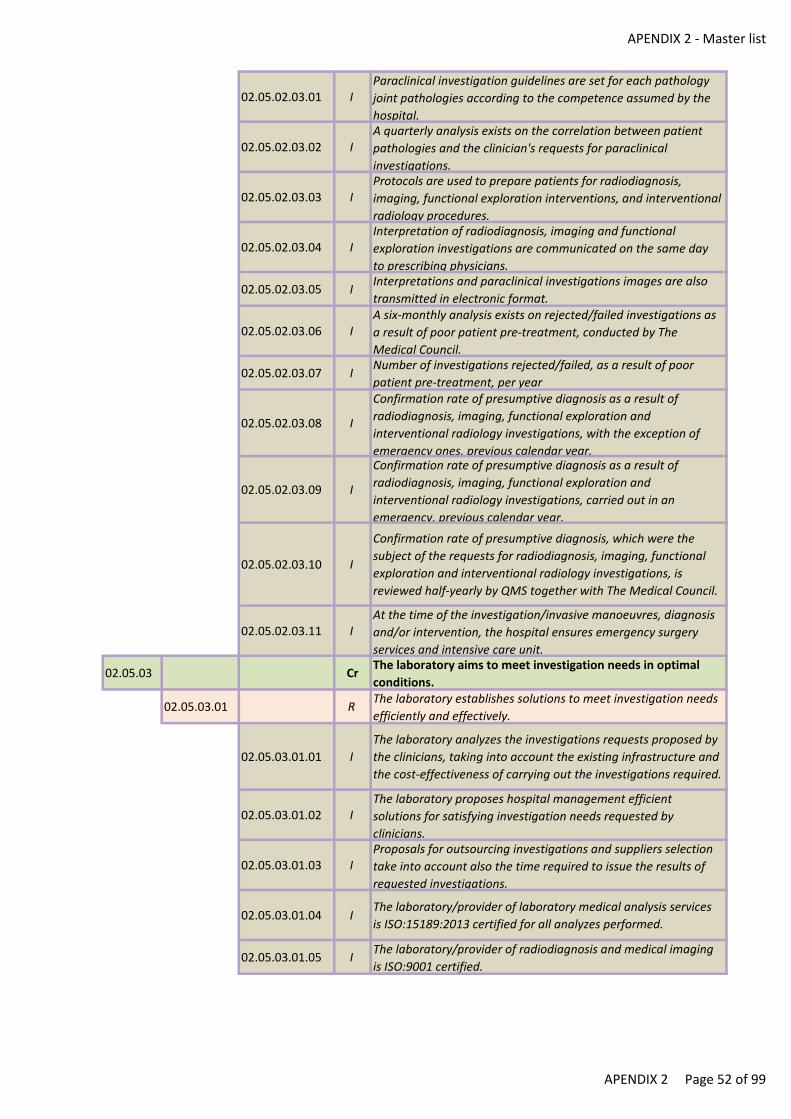
APENDIX 2 - Master list
02.05.02.03.01 IParaclinical investigation guidelines are set for each pathology
joint pathologies according to the competence assumed by the
hospital.
02.05.02.03.02 IA quarterly analysis exists on the correlation between patient
pathologies and the clinician's requests for paraclinical
investigations.
02.05.02.03.03 IProtocols are used to prepare patients for radiodiagnosis,
imaging, functional exploration interventions, and interventional
radiology procedures.
02.05.02.03.04 IInterpretation of radiodiagnosis, imaging and functional
exploration investigations are communicated on the same day
to prescribing physicians.
02.05.02.03.05 IInterpretations and paraclinical investigations images are also
transmitted in electronic format.
02.05.02.03.06 IA six-monthly analysis exists on rejected/failed investigations as
a result of poor patient pre-treatment, conducted by The
Medical Council.
02.05.02.03.07 INumber of investigations rejected/failed, as a result of poor
patient pre-treatment, per year
02.05.02.03.08 I
Confirmation rate of presumptive diagnosis as a result of
radiodiagnosis, imaging, functional exploration and
interventional radiology investigations, with the exception of
emergency ones, previous calendar year.
02.05.02.03.09 I
Confirmation rate of presumptive diagnosis as a result of
radiodiagnosis, imaging, functional exploration and
interventional radiology investigations, carried out in an
emergency, previous calendar year.
02.05.02.03.10 I
Confirmation rate of presumptive diagnosis, which were the
subject of the requests for radiodiagnosis, imaging, functional
exploration and interventional radiology investigations, is
reviewed half-yearly by QMS together with The Medical Council.
02.05.02.03.11 IAt the time of the investigation/invasive manoeuvres, diagnosis
and/or intervention, the hospital ensures emergency surgery
services and intensive care unit.
02.05.03 CrThe laboratory aims to meet investigation needs in optimal
conditions.
02.05.03.01 RThe laboratory establishes solutions to meet investigation needs
efficiently and effectively.
02.05.03.01.01 I
The laboratory analyzes the investigations requests proposed by
the clinicians, taking into account the existing infrastructure and
the cost-effectiveness of carrying out the investigations required.
02.05.03.01.02 IThe laboratory proposes hospital management efficient
solutions for satisfying investigation needs requested by
clinicians.
02.05.03.01.03 IProposals for outsourcing investigations and suppliers selection
take into account also the time required to issue the results of
requested investigations.
02.05.03.01.04 IThe laboratory/provider of laboratory medical analysis services
is ISO:15189:2013 certified for all analyzes performed.
02.05.03.01.05 IThe laboratory/provider of radiodiagnosis and medical imaging
is ISO:9001 certified.
APENDIX 2 Page 52 of 99
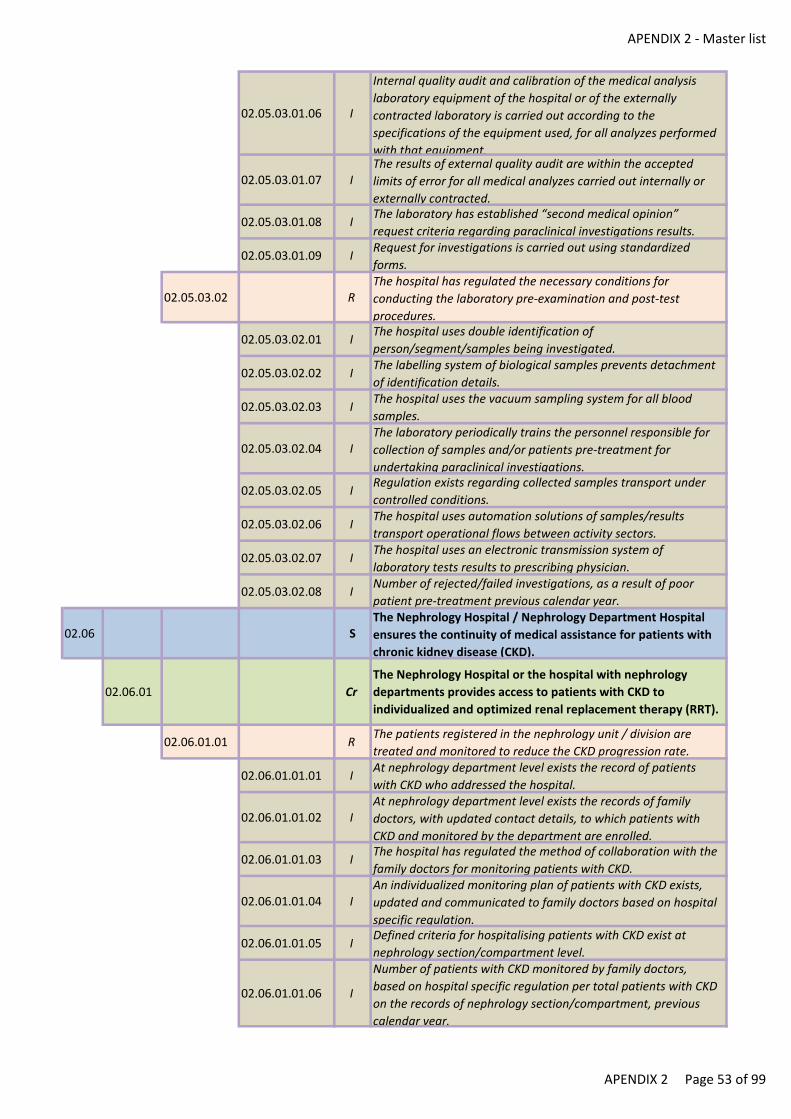
APENDIX 2 - Master list
02.05.03.01.06 I
Internal quality audit and calibration of the medical analysis
laboratory equipment of the hospital or of the externally
contracted laboratory is carried out according to the
specifications of the equipment used, for all analyzes performed
with that equipment.
02.05.03.01.07 IThe results of external quality audit are within the accepted
limits of error for all medical analyzes carried out internally or
externally contracted.
02.05.03.01.08 IThe laboratory has established “second medical opinion”
request criteria regarding paraclinical investigations results.
02.05.03.01.09 IRequest for investigations is carried out using standardized
forms.
02.05.03.02 RThe hospital has regulated the necessary conditions for
conducting the laboratory pre-examination and post-test
procedures.
02.05.03.02.01 IThe hospital uses double identification of
person/segment/samples being investigated.
02.05.03.02.02 IThe labelling system of biological samples prevents detachment
of identification details.
02.05.03.02.03 IThe hospital uses the vacuum sampling system for all blood
samples.
02.05.03.02.04 IThe laboratory periodically trains the personnel responsible for
collection of samples and/or patients pre-treatment for
undertaking paraclinical investigations.
02.05.03.02.05 IRegulation exists regarding collected samples transport under
controlled conditions.
02.05.03.02.06 IThe hospital uses automation solutions of samples/results
transport operational flows between activity sectors.
02.05.03.02.07 IThe hospital uses an electronic transmission system of
laboratory tests results to prescribing physician.
02.05.03.02.08 INumber of rejected/failed investigations, as a result of poor
patient pre-treatment previous calendar year.
02.06 SThe Nephrology Hospital / Nephrology Department Hospital
ensures the continuity of medical assistance for patients with
chronic kidney disease (CKD).
02.06.01 Cr
The Nephrology Hospital or the hospital with nephrology
departments provides access to patients with CKD to
individualized and optimized renal replacement therapy (RRT).
02.06.01.01 RThe patients registered in the nephrology unit / division are
treated and monitored to reduce the CKD progression rate.
02.06.01.01.01 IAt nephrology department level exists the record of patients
with CKD who addressed the hospital.
02.06.01.01.02 IAt nephrology department level exists the records of family
doctors, with updated contact details, to which patients with
CKD and monitored by the department are enrolled.
02.06.01.01.03 IThe hospital has regulated the method of collaboration with the
family doctors for monitoring patients with CKD.
02.06.01.01.04 IAn individualized monitoring plan of patients with CKD exists,
updated and communicated to family doctors based on hospital
specific regulation.
02.06.01.01.05 IDefined criteria for hospitalising patients with CKD exist at
nephrology section/compartment level.
02.06.01.01.06 I
Number of patients with CKD monitored by family doctors,
based on hospital specific regulation per total patients with CKD
on the records of nephrology section/compartment, previous
calendar year.
APENDIX 2 Page 53 of 99

APENDIX 2 - Master list
02.06.01.01.07 INumber of patients with CKD hospitalised in an emergency per
total number of patients with CKD hospitalised, previous
calendar year.
02.06.01.02 RThe hospital with nephrology units / divisions prepares CKD
patients for renal replacement therapy.
02.06.01.02.01 IThe hospital nephrology section/compartment has collaboration
protocols with transplant centres.
02.06.01.02.02 IPatients with CKD on the records of nephrology department are
being investigated in view of transplant.
02.06.01.02.03 I
Number of patients with GFR under 20mL/min, who are being
investigated for kidney transplant per total number of patients
with GFR under 20mL/min, on the records of nephrology
section/compartment, previous calendar year.
02.06.01.02.04 ICollaboration protocol exists for performing arterio-venous
fistula with vascular surgery services/surgeon with competence
in vascular surgery.
02.06.01.02.05 IA planning of patients with GFR between 15-20mL/min exists,
for performing arterio-venous fistula.
02.06.01.02.06 I
Number of patients on the records of nephrology
section/compartment who started dialysis on arterio-venous
fistula per total number of patients initiated in dialysis in the
hospital dialysis unit, previous calendar year.
02.06.01.02.07 I
Number of patients with GFR below 30mL/min, serologically
evaluated for viral infections (VHB, VHC, HIV) per number of
patients with GFR under 30mL/min, previous calendar year.
02.06.01.02.08 INumber of patients with GFR below 30mL/min vaccinated anti-
HBV per total patients with GFR under 30mL/min, previous
calendar year.
02.06.01.02.09 I
Number of hematologically balanced (Hb >10/dL) patients on
the records of nephrology department at the initiation of dialysis
per number total patients on the records of nephrology
department to which dialysis was initiated in the previous full
calendar year.
02.06.01.02.10 I
Number of patients on the records of nephrology department
with PTH between 200-500pg/mL, at the initiation of dialysis,
per total number of patients on the records of nephrology
department, to which dialysis was initiated, in the previous full
calendar year.
02.06.02 CrRRT efficiency and effectiveness are constant concerns for the
dialysis unit.
02.06.02.01 R
The unit that initiates dialysis decides on how RRT is conducted
(haemodialysis, peritoneal dialysis, kidney transplantation), in
agreement with the patients and their families.
02.06.02.01.01 I
Number of patients who started haemodialysis treatment per
number of patients on the records of nephrology department
who started KFST, in the previous full calendar year.
02.06.02.01.02 I
Number of patients who started treatment through peritoneal
dialysis per number of patients on the records of nephrology
department who started KFST, in the previous full calendar year.
02.06.02.01.03 I
Number of patients with kidney transplant indications registered
with transplant centres per number of patients with GFR under
20mL/min on the records of nephrology department, in the
previous full calendar year.
APENDIX 2 Page 54 of 99
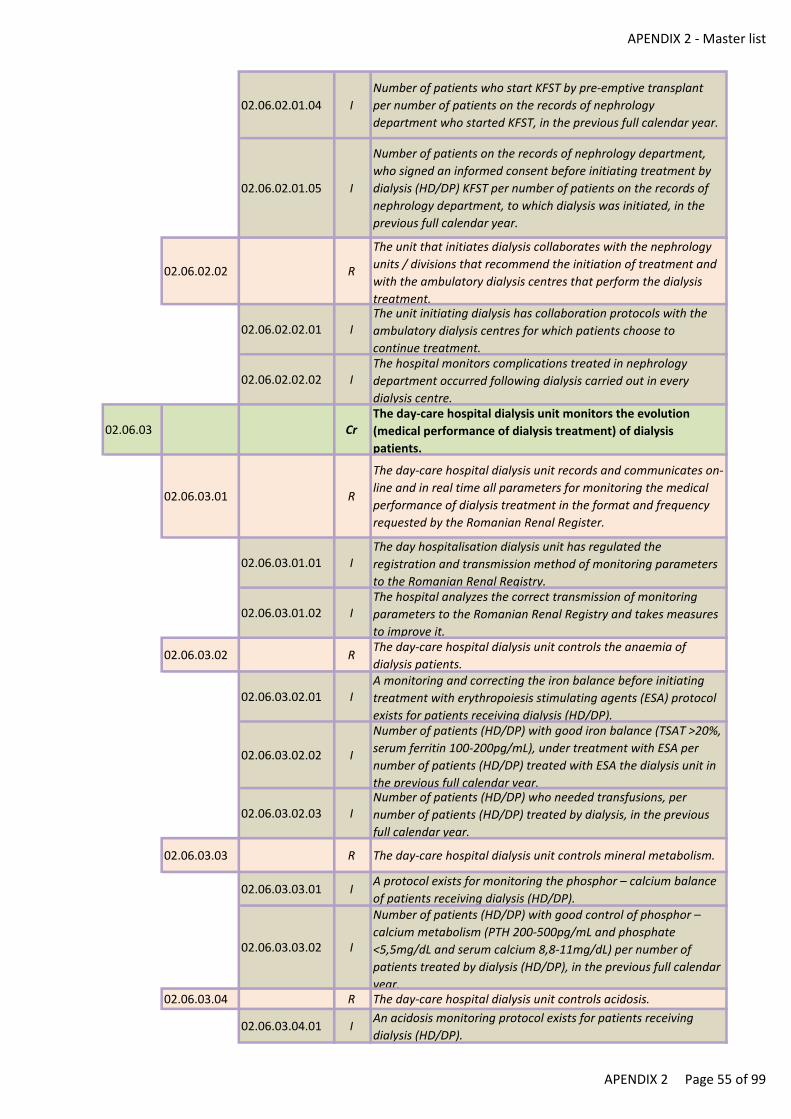
APENDIX 2 - Master list
02.06.02.01.04 I
Number of patients who start KFST by pre-emptive transplant
per number of patients on the records of nephrology
department who started KFST, in the previous full calendar year.
02.06.02.01.05 I
Number of patients on the records of nephrology department,
who signed an informed consent before initiating treatment by
dialysis (HD/DP) KFST per number of patients on the records of
nephrology department, to which dialysis was initiated, in the
previous full calendar year.
02.06.02.02 R
The unit that initiates dialysis collaborates with the nephrology
units / divisions that recommend the initiation of treatment and
with the ambulatory dialysis centres that perform the dialysis
treatment.
02.06.02.02.01 IThe unit initiating dialysis has collaboration protocols with the
ambulatory dialysis centres for which patients choose to
continue treatment.
02.06.02.02.02 IThe hospital monitors complications treated in nephrology
department occurred following dialysis carried out in every
dialysis centre.
02.06.03 CrThe day-care hospital dialysis unit monitors the evolution
(medical performance of dialysis treatment) of dialysis
patients.
02.06.03.01 R
The day-care hospital dialysis unit records and communicates on-
line and in real time all parameters for monitoring the medical
performance of dialysis treatment in the format and frequency
requested by the Romanian Renal Register.
02.06.03.01.01 IThe day hospitalisation dialysis unit has regulated the
registration and transmission method of monitoring parameters
to the Romanian Renal Registry.
02.06.03.01.02 IThe hospital analyzes the correct transmission of monitoring
parameters to the Romanian Renal Registry and takes measures
to improve it.
02.06.03.02 RThe day-care hospital dialysis unit controls the anaemia of
dialysis patients.
02.06.03.02.01 IA monitoring and correcting the iron balance before initiating
treatment with erythropoiesis stimulating agents (ESA) protocol
exists for patients receiving dialysis (HD/DP).
02.06.03.02.02 I
Number of patients (HD/DP) with good iron balance (TSAT >20%,
serum ferritin 100-200pg/mL), under treatment with ESA per
number of patients (HD/DP) treated with ESA the dialysis unit in
the previous full calendar year.
02.06.03.02.03 INumber of patients (HD/DP) who needed transfusions, per
number of patients (HD/DP) treated by dialysis, in the previous
full calendar year.
02.06.03.03 R The day-care hospital dialysis unit controls mineral metabolism.
02.06.03.03.01 IA protocol exists for monitoring the phosphor – calcium balance
of patients receiving dialysis (HD/DP).
02.06.03.03.02 I
Number of patients (HD/DP) with good control of phosphor –
calcium metabolism (PTH 200-500pg/mL and phosphate
<5,5mg/dL and serum calcium 8,8-11mg/dL) per number of
patients treated by dialysis (HD/DP), in the previous full calendar
year.02.06.03.04 R The day-care hospital dialysis unit controls acidosis.
02.06.03.04.01 IAn acidosis monitoring protocol exists for patients receiving
dialysis (HD/DP).
APENDIX 2 Page 55 of 99
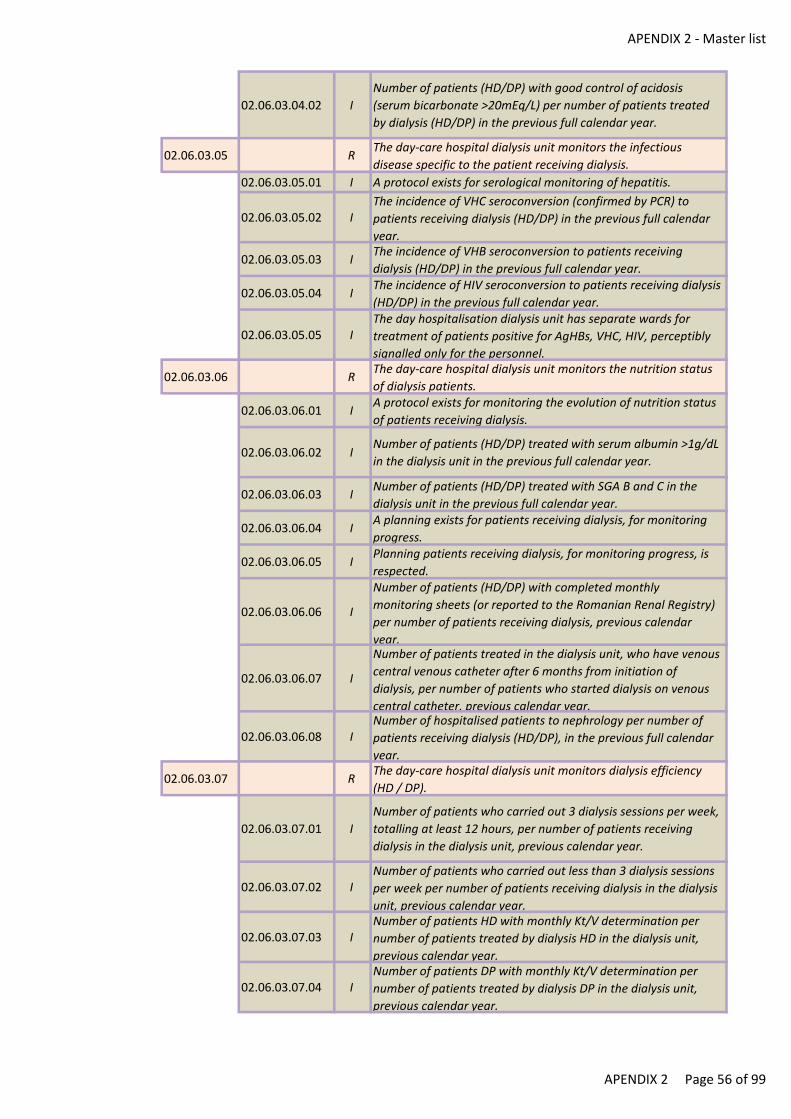
APENDIX 2 - Master list
02.06.03.04.02 I
Number of patients (HD/DP) with good control of acidosis
(serum bicarbonate >20mEq/L) per number of patients treated
by dialysis (HD/DP) in the previous full calendar year.
02.06.03.05 RThe day-care hospital dialysis unit monitors the infectious
disease specific to the patient receiving dialysis.
02.06.03.05.01 I A protocol exists for serological monitoring of hepatitis.
02.06.03.05.02 IThe incidence of VHC seroconversion (confirmed by PCR) to
patients receiving dialysis (HD/DP) in the previous full calendar
year.
02.06.03.05.03 IThe incidence of VHB seroconversion to patients receiving
dialysis (HD/DP) in the previous full calendar year.
02.06.03.05.04 IThe incidence of HIV seroconversion to patients receiving dialysis
(HD/DP) in the previous full calendar year.
02.06.03.05.05 IThe day hospitalisation dialysis unit has separate wards for
treatment of patients positive for AgHBs, VHC, HIV, perceptibly
signalled only for the personnel.
02.06.03.06 RThe day-care hospital dialysis unit monitors the nutrition status
of dialysis patients.
02.06.03.06.01 IA protocol exists for monitoring the evolution of nutrition status
of patients receiving dialysis.
02.06.03.06.02 INumber of patients (HD/DP) treated with serum albumin >1g/dL
in the dialysis unit in the previous full calendar year.
02.06.03.06.03 INumber of patients (HD/DP) treated with SGA B and C in the
dialysis unit in the previous full calendar year.
02.06.03.06.04 IA planning exists for patients receiving dialysis, for monitoring
progress.
02.06.03.06.05 IPlanning patients receiving dialysis, for monitoring progress, is
respected.
02.06.03.06.06 I
Number of patients (HD/DP) with completed monthly
monitoring sheets (or reported to the Romanian Renal Registry)
per number of patients receiving dialysis, previous calendar
year.
02.06.03.06.07 I
Number of patients treated in the dialysis unit, who have venous
central venous catheter after 6 months from initiation of
dialysis, per number of patients who started dialysis on venous
central catheter, previous calendar year.
02.06.03.06.08 INumber of hospitalised patients to nephrology per number of
patients receiving dialysis (HD/DP), in the previous full calendar
year.
02.06.03.07 RThe day-care hospital dialysis unit monitors dialysis efficiency
(HD / DP).
02.06.03.07.01 I
Number of patients who carried out 3 dialysis sessions per week,
totalling at least 12 hours, per number of patients receiving
dialysis in the dialysis unit, previous calendar year.
02.06.03.07.02 INumber of patients who carried out less than 3 dialysis sessions
per week per number of patients receiving dialysis in the dialysis
unit, previous calendar year.
02.06.03.07.03 INumber of patients HD with monthly Kt/V determination per
number of patients treated by dialysis HD in the dialysis unit,
previous calendar year.
02.06.03.07.04 INumber of patients DP with monthly Kt/V determination per
number of patients treated by dialysis DP in the dialysis unit,
previous calendar year.
APENDIX 2 Page 56 of 99
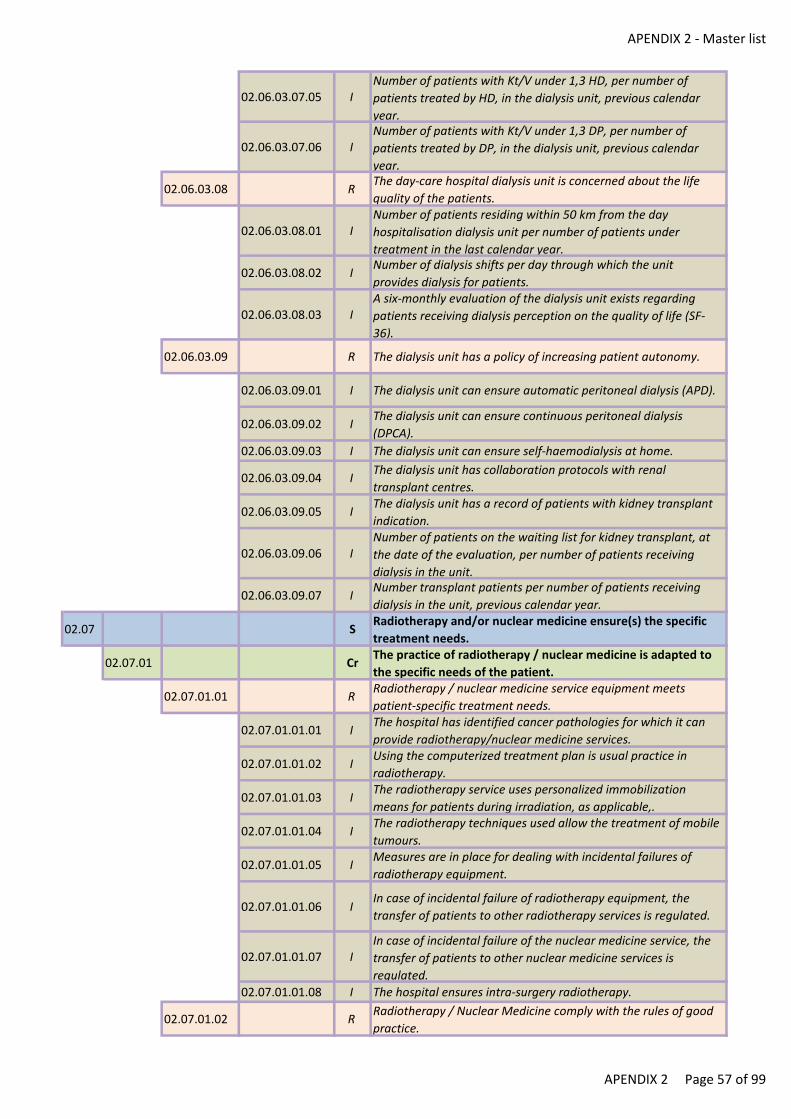
APENDIX 2 - Master list
02.06.03.07.05 INumber of patients with Kt/V under 1,3 HD, per number of
patients treated by HD, in the dialysis unit, previous calendar
year.
02.06.03.07.06 INumber of patients with Kt/V under 1,3 DP, per number of
patients treated by DP, in the dialysis unit, previous calendar
year.
02.06.03.08 RThe day-care hospital dialysis unit is concerned about the life
quality of the patients.
02.06.03.08.01 INumber of patients residing within 50 km from the day
hospitalisation dialysis unit per number of patients under
treatment in the last calendar year.
02.06.03.08.02 INumber of dialysis shifts per day through which the unit
provides dialysis for patients.
02.06.03.08.03 IA six-monthly evaluation of the dialysis unit exists regarding
patients receiving dialysis perception on the quality of life (SF-
36).
02.06.03.09 R The dialysis unit has a policy of increasing patient autonomy.
02.06.03.09.01 I The dialysis unit can ensure automatic peritoneal dialysis (APD).
02.06.03.09.02 IThe dialysis unit can ensure continuous peritoneal dialysis
(DPCA).
02.06.03.09.03 I The dialysis unit can ensure self-haemodialysis at home.
02.06.03.09.04 IThe dialysis unit has collaboration protocols with renal
transplant centres.
02.06.03.09.05 IThe dialysis unit has a record of patients with kidney transplant
indication.
02.06.03.09.06 INumber of patients on the waiting list for kidney transplant, at
the date of the evaluation, per number of patients receiving
dialysis in the unit.
02.06.03.09.07 INumber transplant patients per number of patients receiving
dialysis in the unit, previous calendar year.
02.07 SRadiotherapy and/or nuclear medicine ensure(s) the specific
treatment needs.
02.07.01 CrThe practice of radiotherapy / nuclear medicine is adapted to
the specific needs of the patient.
02.07.01.01 RRadiotherapy / nuclear medicine service equipment meets
patient-specific treatment needs.
02.07.01.01.01 IThe hospital has identified cancer pathologies for which it can
provide radiotherapy/nuclear medicine services.
02.07.01.01.02 IUsing the computerized treatment plan is usual practice in
radiotherapy.
02.07.01.01.03 IThe radiotherapy service uses personalized immobilization
means for patients during irradiation, as applicable,.
02.07.01.01.04 IThe radiotherapy techniques used allow the treatment of mobile
tumours.
02.07.01.01.05 IMeasures are in place for dealing with incidental failures of
radiotherapy equipment.
02.07.01.01.06 IIn case of incidental failure of radiotherapy equipment, the
transfer of patients to other radiotherapy services is regulated.
02.07.01.01.07 IIn case of incidental failure of the nuclear medicine service, the
transfer of patients to other nuclear medicine services is
regulated.
02.07.01.01.08 I The hospital ensures intra-surgery radiotherapy.
02.07.01.02 RRadiotherapy / Nuclear Medicine comply with the rules of good
practice.
APENDIX 2 Page 57 of 99
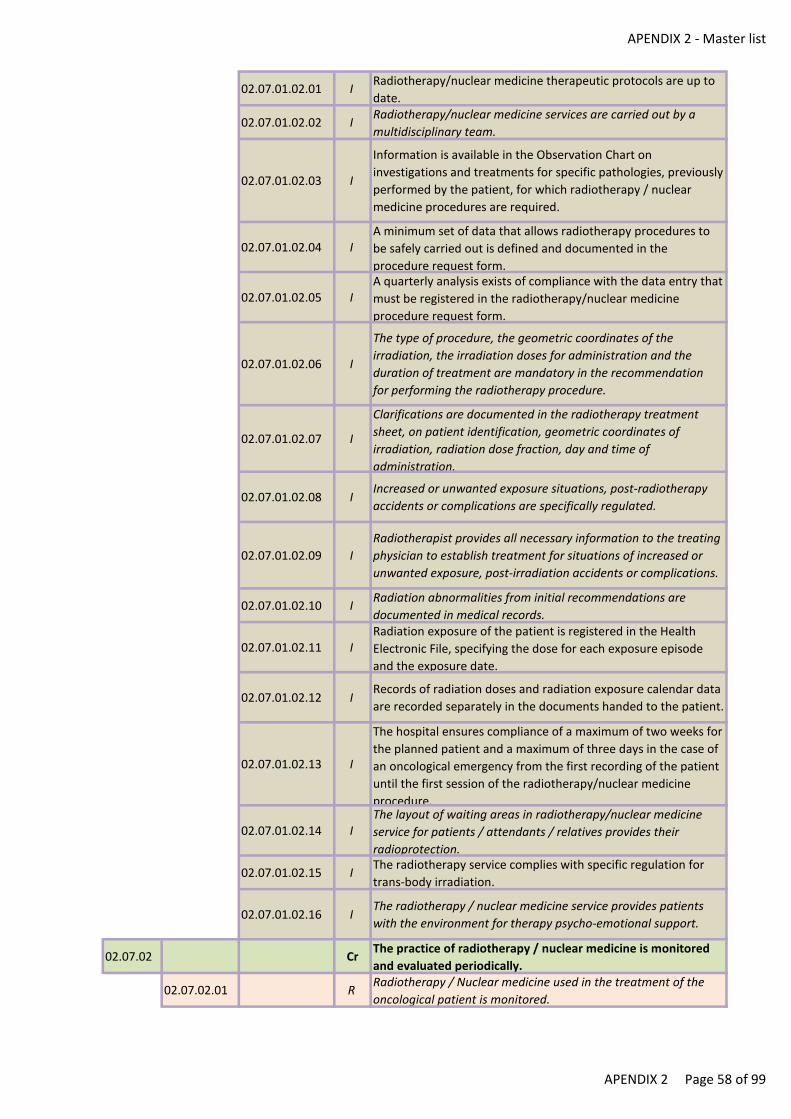
APENDIX 2 - Master list
02.07.01.02.01 IRadiotherapy/nuclear medicine therapeutic protocols are up to
date.
02.07.01.02.02 IRadiotherapy/nuclear medicine services are carried out by a
multidisciplinary team.
02.07.01.02.03 I
Information is available in the Observation Chart on
investigations and treatments for specific pathologies, previously
performed by the patient, for which radiotherapy / nuclear
medicine procedures are required.
02.07.01.02.04 IA minimum set of data that allows radiotherapy procedures to
be safely carried out is defined and documented in the
procedure request form.
02.07.01.02.05 IA quarterly analysis exists of compliance with the data entry that
must be registered in the radiotherapy/nuclear medicine
procedure request form.
02.07.01.02.06 I
The type of procedure, the geometric coordinates of the
irradiation, the irradiation doses for administration and the
duration of treatment are mandatory in the recommendation
for performing the radiotherapy procedure.
02.07.01.02.07 I
Clarifications are documented in the radiotherapy treatment
sheet, on patient identification, geometric coordinates of
irradiation, radiation dose fraction, day and time of
administration.
02.07.01.02.08 IIncreased or unwanted exposure situations, post-radiotherapy
accidents or complications are specifically regulated.
02.07.01.02.09 I
Radiotherapist provides all necessary information to the treating
physician to establish treatment for situations of increased or
unwanted exposure, post-irradiation accidents or complications.
02.07.01.02.10 IRadiation abnormalities from initial recommendations are
documented in medical records.
02.07.01.02.11 IRadiation exposure of the patient is registered in the Health
Electronic File, specifying the dose for each exposure episode
and the exposure date.
02.07.01.02.12 IRecords of radiation doses and radiation exposure calendar data
are recorded separately in the documents handed to the patient.
02.07.01.02.13 I
The hospital ensures compliance of a maximum of two weeks for
the planned patient and a maximum of three days in the case of
an oncological emergency from the first recording of the patient
until the first session of the radiotherapy/nuclear medicine
procedure.
02.07.01.02.14 IThe layout of waiting areas in radiotherapy/nuclear medicine
service for patients / attendants / relatives provides their
radioprotection.
02.07.01.02.15 IThe radiotherapy service complies with specific regulation for
trans-body irradiation.
02.07.01.02.16 IThe radiotherapy / nuclear medicine service provides patients
with the environment for therapy psycho-emotional support.
02.07.02 CrThe practice of radiotherapy / nuclear medicine is monitored
and evaluated periodically.
02.07.02.01 RRadiotherapy / Nuclear medicine used in the treatment of the
oncological patient is monitored.
APENDIX 2 Page 58 of 99
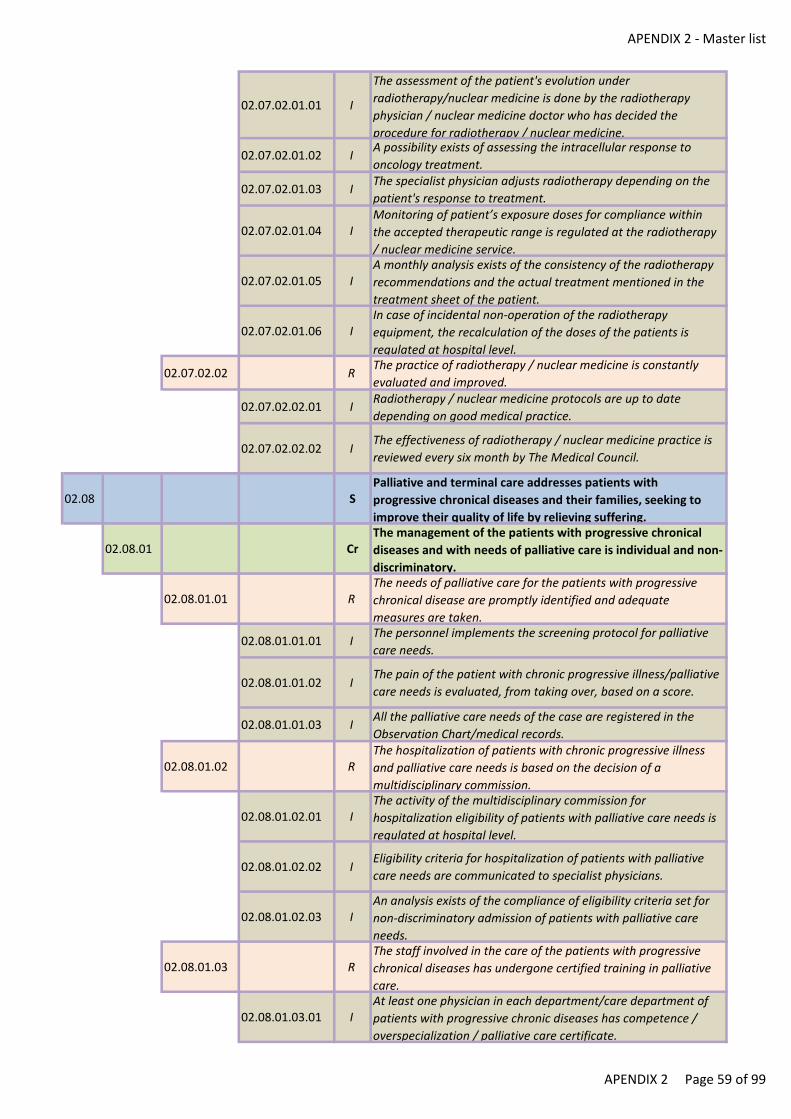
APENDIX 2 - Master list
02.07.02.01.01 I
The assessment of the patient's evolution under
radiotherapy/nuclear medicine is done by the radiotherapy
physician / nuclear medicine doctor who has decided the
procedure for radiotherapy / nuclear medicine.
02.07.02.01.02 IA possibility exists of assessing the intracellular response to
oncology treatment.
02.07.02.01.03 IThe specialist physician adjusts radiotherapy depending on the
patient's response to treatment.
02.07.02.01.04 IMonitoring of patient’s exposure doses for compliance within
the accepted therapeutic range is regulated at the radiotherapy
/ nuclear medicine service.
02.07.02.01.05 IA monthly analysis exists of the consistency of the radiotherapy
recommendations and the actual treatment mentioned in the
treatment sheet of the patient.
02.07.02.01.06 IIn case of incidental non-operation of the radiotherapy
equipment, the recalculation of the doses of the patients is
regulated at hospital level.
02.07.02.02 RThe practice of radiotherapy / nuclear medicine is constantly
evaluated and improved.
02.07.02.02.01 IRadiotherapy / nuclear medicine protocols are up to date
depending on good medical practice.
02.07.02.02.02 IThe effectiveness of radiotherapy / nuclear medicine practice is
reviewed every six month by The Medical Council.
02.08 SPalliative and terminal care addresses patients with
progressive chronical diseases and their families, seeking to
improve their quality of life by relieving suffering.
02.08.01 CrThe management of the patients with progressive chronical
diseases and with needs of palliative care is individual and non-
discriminatory.
02.08.01.01 RThe needs of palliative care for the patients with progressive
chronical disease are promptly identified and adequate
measures are taken.
02.08.01.01.01 IThe personnel implements the screening protocol for palliative
care needs.
02.08.01.01.02 IThe pain of the patient with chronic progressive illness/palliative
care needs is evaluated, from taking over, based on a score.
02.08.01.01.03 IAll the palliative care needs of the case are registered in the
Observation Chart/medical records.
02.08.01.02 RThe hospitalization of patients with chronic progressive illness
and palliative care needs is based on the decision of a
multidisciplinary commission.
02.08.01.02.01 IThe activity of the multidisciplinary commission for
hospitalization eligibility of patients with palliative care needs is
regulated at hospital level.
02.08.01.02.02 IEligibility criteria for hospitalization of patients with palliative
care needs are communicated to specialist physicians.
02.08.01.02.03 IAn analysis exists of the compliance of eligibility criteria set for
non-discriminatory admission of patients with palliative care
needs.
02.08.01.03 RThe staff involved in the care of the patients with progressive
chronical diseases has undergone certified training in palliative
care.
02.08.01.03.01 IAt least one physician in each department/care department of
patients with progressive chronic diseases has competence /
overspecialization / palliative care certificate.
APENDIX 2 Page 59 of 99
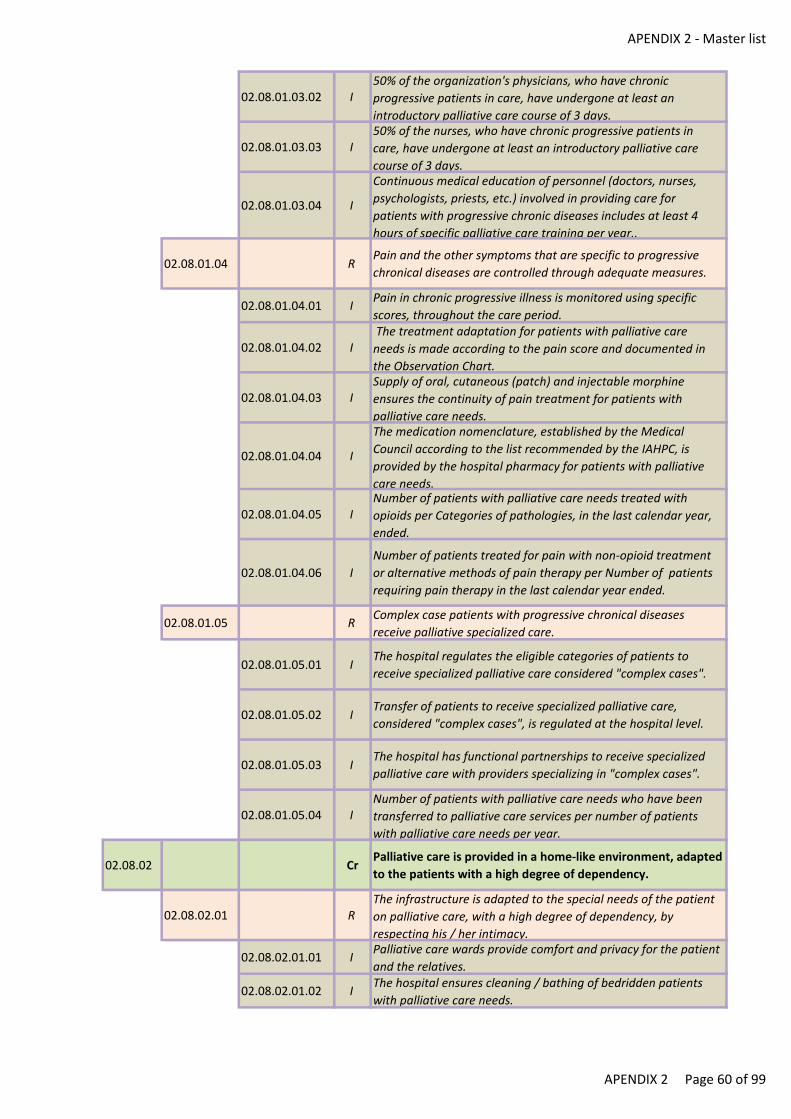
APENDIX 2 - Master list
02.08.01.03.02 I50% of the organization's physicians, who have chronic
progressive patients in care, have undergone at least an
introductory palliative care course of 3 days.
02.08.01.03.03 I50% of the nurses, who have chronic progressive patients in
care, have undergone at least an introductory palliative care
course of 3 days.
02.08.01.03.04 I
Continuous medical education of personnel (doctors, nurses,
psychologists, priests, etc.) involved in providing care for
patients with progressive chronic diseases includes at least 4
hours of specific palliative care training per year..
02.08.01.04 RPain and the other symptoms that are specific to progressive
chronical diseases are controlled through adequate measures.
02.08.01.04.01 IPain in chronic progressive illness is monitored using specific
scores, throughout the care period.
02.08.01.04.02 I The treatment adaptation for patients with palliative care
needs is made according to the pain score and documented in
the Observation Chart.
02.08.01.04.03 ISupply of oral, cutaneous (patch) and injectable morphine
ensures the continuity of pain treatment for patients with
palliative care needs.
02.08.01.04.04 I
The medication nomenclature, established by the Medical
Council according to the list recommended by the IAHPC, is
provided by the hospital pharmacy for patients with palliative
care needs.
02.08.01.04.05 INumber of patients with palliative care needs treated with
opioids per Categories of pathologies, in the last calendar year,
ended.
02.08.01.04.06 I
Number of patients treated for pain with non-opioid treatment
or alternative methods of pain therapy per Number of patients
requiring pain therapy in the last calendar year ended.
02.08.01.05 RComplex case patients with progressive chronical diseases
receive palliative specialized care.
02.08.01.05.01 IThe hospital regulates the eligible categories of patients to
receive specialized palliative care considered "complex cases".
02.08.01.05.02 ITransfer of patients to receive specialized palliative care,
considered "complex cases", is regulated at the hospital level.
02.08.01.05.03 IThe hospital has functional partnerships to receive specialized
palliative care with providers specializing in "complex cases".
02.08.01.05.04 INumber of patients with palliative care needs who have been
transferred to palliative care services per number of patients
with palliative care needs per year.
02.08.02 CrPalliative care is provided in a home-like environment, adapted
to the patients with a high degree of dependency.
02.08.02.01 RThe infrastructure is adapted to the special needs of the patient
on palliative care, with a high degree of dependency, by
respecting his / her intimacy.
02.08.02.01.01 IPalliative care wards provide comfort and privacy for the patient
and the relatives.
02.08.02.01.02 IThe hospital ensures cleaning / bathing of bedridden patients
with palliative care needs.
APENDIX 2 Page 60 of 99

APENDIX 2 - Master list
02.08.02.01.03 IThe hospital provides the possibility of accommodation for
relatives, during the hospitalisation of patients with palliative
care needs.
02.08.02.02 RThe infrastructure allows for palliative care related services to be
carried out.
02.08.02.02.01 IAreas exist for interdisciplinary meetings and continuing medical
education for palliative care units.
02.08.02.02.02 IEquipped and supervised day areas exist for socialisation of
patients/relatives in palliative care.
02.08.02.02.03 IAreas exist for counselling of patient and family in palliative
care.
02.08.02.02.04 IAreas exist for complementary therapies – aromatherapy, kineto-
therapy, volunteers etc. dedicated to palliative care.
02.08.02.02.05 IPalliative care unit has a “cold room” or access to similar
services.
02.08.02.02.06 IPalliative care unit has specific facilities: mobile beds, anti-bed
sore mattresses (minimum 1 to 3 beds), lifts, walking frames,
food tables, mobile wc, wheelchairs.
02.08.02.02.07 I
The palliative sector complies with the minimum mandatory
endowment: secretion aspirator, glucometer, tonometer,
stethoscope, thermometer, oxygen station/ oxygen
concentrator, pulse oximeter, automatic / injectable syringes.
02.08.03 CrPalliative care services allow for improvement in the life quality
of the patient and of his / her family / guardians.
02.08.03.01 ROn patient admission in the hospital palliative care ward, a
comprehensive evaluation of the patient / family / guardians is
performed.
02.08.03.01.01 IThe adapted Observation Chart for palliative care includes
integrated psychosocial assessment elements of the patient,
family, relatives, as applicable.
02.08.03.01.02 IThe findings of the assessment / the management plan of the
patient with palliative care needs include the needs in the
physical, psycho-emotional, social and spiritual areas.
02.08.03.01.03 IThe pain impact on the quality of life of the patient with
palliative care needs is assessed and recorded in the Observation
Chart.
02.08.03.02 RThe aims of palliative care, the understanding of the diagnosis
and prognosis are assessed and documented along with the
patient / family / family member.
02.08.03.02.01 I
Expectations related to care of the patient with chronic
progressive illness / palliative care needs and / or his family are
recorded in medical records and analyzed annually or whenever
appropriate.
02.08.03.02.02 I
The treating physician documents his appreciation regarding the
degree of understanding of the patient with palliative care
needs in relation to the diagnosis and prognosis communicated
to him in the Observation Chart.
02.08.03.02.03 I
The treating physician documents his appreciation regarding the
degree of understanding of the family / relatives in relation to
the diagnosis and prognosis of the patient with progressive
chronic disease / palliative care needs in the Observation Chart.
02.08.03.03 RThe signs and symptoms of the terminal condition are evaluated
using standard scales and are documented.
02.08.03.03.01 IThe intensity assessment of terminal status symptoms is done
using a specific score.
APENDIX 2 Page 61 of 99
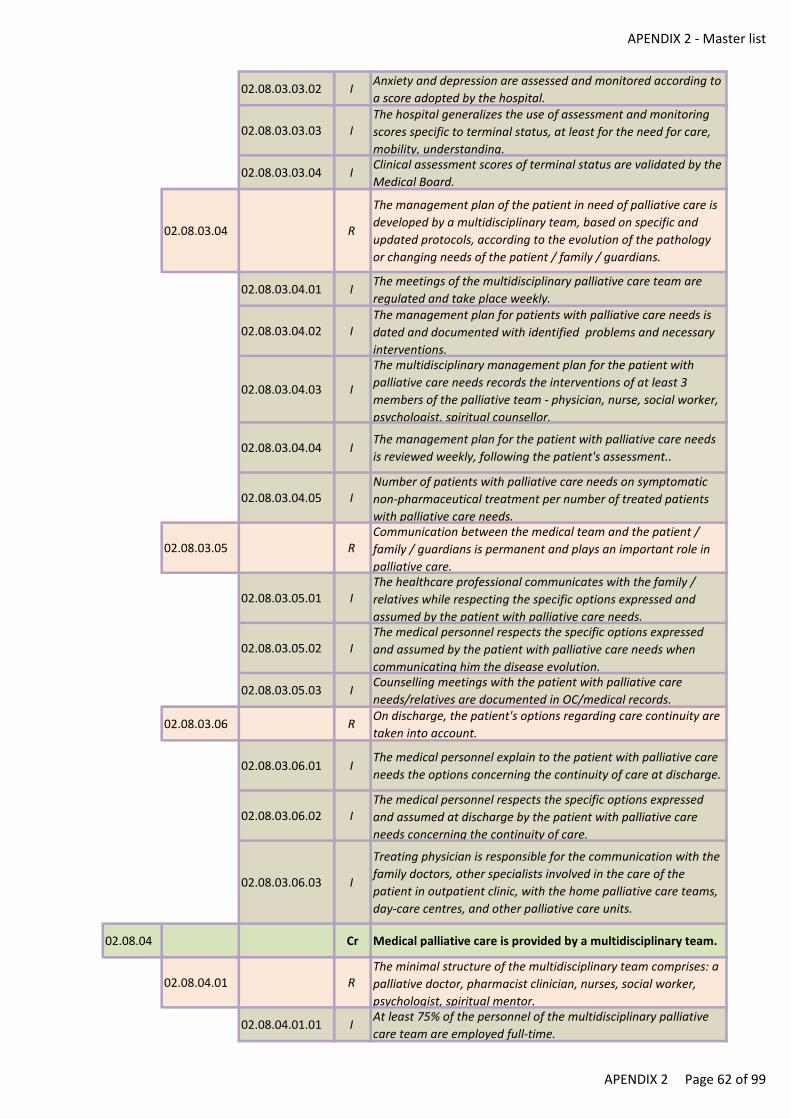
APENDIX 2 - Master list
02.08.03.03.02 IAnxiety and depression are assessed and monitored according to
a score adopted by the hospital.
02.08.03.03.03 IThe hospital generalizes the use of assessment and monitoring
scores specific to terminal status, at least for the need for care,
mobility, understanding.
02.08.03.03.04 IClinical assessment scores of terminal status are validated by the
Medical Board.
02.08.03.04 R
The management plan of the patient in need of palliative care is
developed by a multidisciplinary team, based on specific and
updated protocols, according to the evolution of the pathology
or changing needs of the patient / family / guardians.
02.08.03.04.01 IThe meetings of the multidisciplinary palliative care team are
regulated and take place weekly.
02.08.03.04.02 IThe management plan for patients with palliative care needs is
dated and documented with identified problems and necessary
interventions.
02.08.03.04.03 I
The multidisciplinary management plan for the patient with
palliative care needs records the interventions of at least 3
members of the palliative team - physician, nurse, social worker,
psychologist, spiritual counsellor.
02.08.03.04.04 IThe management plan for the patient with palliative care needs
is reviewed weekly, following the patient's assessment..
02.08.03.04.05 INumber of patients with palliative care needs on symptomatic
non-pharmaceutical treatment per number of treated patients
with palliative care needs.
02.08.03.05 RCommunication between the medical team and the patient /
family / guardians is permanent and plays an important role in
palliative care.
02.08.03.05.01 IThe healthcare professional communicates with the family /
relatives while respecting the specific options expressed and
assumed by the patient with palliative care needs.
02.08.03.05.02 IThe medical personnel respects the specific options expressed
and assumed by the patient with palliative care needs when
communicating him the disease evolution.
02.08.03.05.03 ICounselling meetings with the patient with palliative care
needs/relatives are documented in OC/medical records.
02.08.03.06 ROn discharge, the patient's options regarding care continuity are
taken into account.
02.08.03.06.01 IThe medical personnel explain to the patient with palliative care
needs the options concerning the continuity of care at discharge.
02.08.03.06.02 IThe medical personnel respects the specific options expressed
and assumed at discharge by the patient with palliative care
needs concerning the continuity of care.
02.08.03.06.03 I
Treating physician is responsible for the communication with the
family doctors, other specialists involved in the care of the
patient in outpatient clinic, with the home palliative care teams,
day-care centres, and other palliative care units.
02.08.04 Cr Medical palliative care is provided by a multidisciplinary team.
02.08.04.01 RThe minimal structure of the multidisciplinary team comprises: a
palliative doctor, pharmacist clinician, nurses, social worker,
psychologist, spiritual mentor.
02.08.04.01.01 IAt least 75% of the personnel of the multidisciplinary palliative
care team are employed full-time.
APENDIX 2 Page 62 of 99
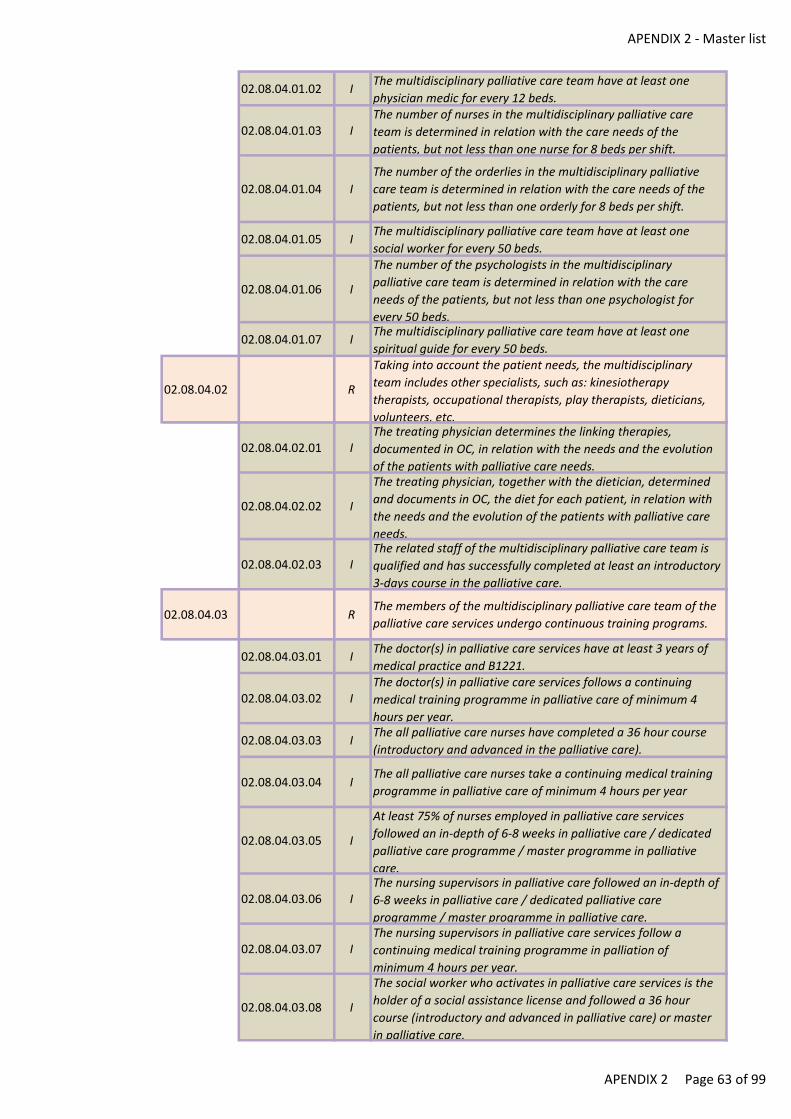
APENDIX 2 - Master list
02.08.04.01.02 IThe multidisciplinary palliative care team have at least one
physician medic for every 12 beds.
02.08.04.01.03 IThe number of nurses in the multidisciplinary palliative care
team is determined in relation with the care needs of the
patients, but not less than one nurse for 8 beds per shift.
02.08.04.01.04 I
The number of the orderlies in the multidisciplinary palliative
care team is determined in relation with the care needs of the
patients, but not less than one orderly for 8 beds per shift.
02.08.04.01.05 IThe multidisciplinary palliative care team have at least one
social worker for every 50 beds.
02.08.04.01.06 I
The number of the psychologists in the multidisciplinary
palliative care team is determined in relation with the care
needs of the patients, but not less than one psychologist for
every 50 beds.
02.08.04.01.07 IThe multidisciplinary palliative care team have at least one
spiritual guide for every 50 beds.
02.08.04.02 R
Taking into account the patient needs, the multidisciplinary
team includes other specialists, such as: kinesiotherapy
therapists, occupational therapists, play therapists, dieticians,
volunteers, etc.
02.08.04.02.01 IThe treating physician determines the linking therapies,
documented in OC, in relation with the needs and the evolution
of the patients with palliative care needs.
02.08.04.02.02 I
The treating physician, together with the dietician, determined
and documents in OC, the diet for each patient, in relation with
the needs and the evolution of the patients with palliative care
needs.
02.08.04.02.03 IThe related staff of the multidisciplinary palliative care team is
qualified and has successfully completed at least an introductory
3-days course in the palliative care.
02.08.04.03 RThe members of the multidisciplinary palliative care team of the
palliative care services undergo continuous training programs.
02.08.04.03.01 IThe doctor(s) in palliative care services have at least 3 years of
medical practice and B1221.
02.08.04.03.02 IThe doctor(s) in palliative care services follows a continuing
medical training programme in palliative care of minimum 4
hours per year.
02.08.04.03.03 IThe all palliative care nurses have completed a 36 hour course
(introductory and advanced in the palliative care).
02.08.04.03.04 IThe all palliative care nurses take a continuing medical training
programme in palliative care of minimum 4 hours per year
02.08.04.03.05 I
At least 75% of nurses employed in palliative care services
followed an in-depth of 6-8 weeks in palliative care / dedicated
palliative care programme / master programme in palliative
care.
02.08.04.03.06 IThe nursing supervisors in palliative care followed an in-depth of
6-8 weeks in palliative care / dedicated palliative care
programme / master programme in palliative care.
02.08.04.03.07 IThe nursing supervisors in palliative care services follow a
continuing medical training programme in palliation of
minimum 4 hours per year.
02.08.04.03.08 I
The social worker who activates in palliative care services is the
holder of a social assistance license and followed a 36 hour
course (introductory and advanced in palliative care) or master
in palliative care.
APENDIX 2 Page 63 of 99
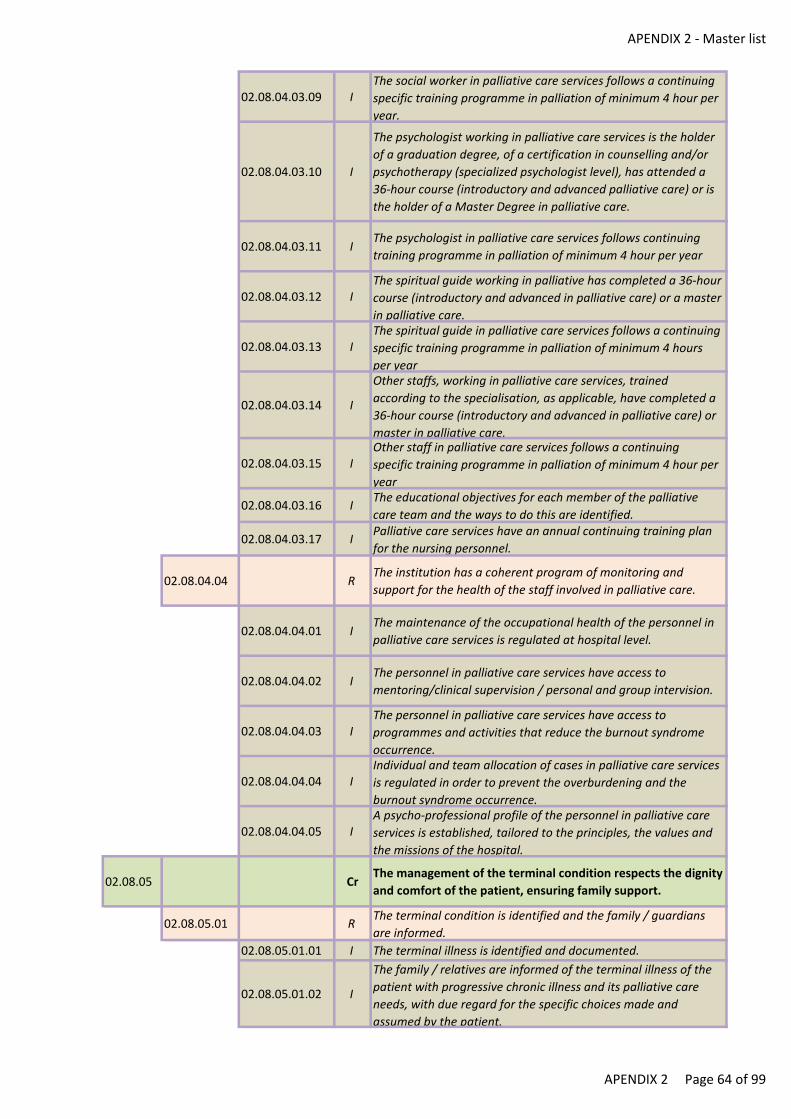
APENDIX 2 - Master list
02.08.04.03.09 IThe social worker in palliative care services follows a continuing
specific training programme in palliation of minimum 4 hour per
year.
02.08.04.03.10 I
The psychologist working in palliative care services is the holder
of a graduation degree, of a certification in counselling and/or
psychotherapy (specialized psychologist level), has attended a
36-hour course (introductory and advanced palliative care) or is
the holder of a Master Degree in palliative care.
02.08.04.03.11 IThe psychologist in palliative care services follows continuing
training programme in palliation of minimum 4 hour per year
02.08.04.03.12 IThe spiritual guide working in palliative has completed a 36-hour
course (introductory and advanced in palliative care) or a master
in palliative care.
02.08.04.03.13 IThe spiritual guide in palliative care services follows a continuing
specific training programme in palliation of minimum 4 hours
per year
02.08.04.03.14 I
Other staffs, working in palliative care services, trained
according to the specialisation, as applicable, have completed a
36-hour course (introductory and advanced in palliative care) or
master in palliative care.
02.08.04.03.15 IOther staff in palliative care services follows a continuing
specific training programme in palliation of minimum 4 hour per
year
02.08.04.03.16 IThe educational objectives for each member of the palliative
care team and the ways to do this are identified.
02.08.04.03.17 IPalliative care services have an annual continuing training plan
for the nursing personnel.
02.08.04.04 RThe institution has a coherent program of monitoring and
support for the health of the staff involved in palliative care.
02.08.04.04.01 IThe maintenance of the occupational health of the personnel in
palliative care services is regulated at hospital level.
02.08.04.04.02 IThe personnel in palliative care services have access to
mentoring/clinical supervision / personal and group intervision.
02.08.04.04.03 IThe personnel in palliative care services have access to
programmes and activities that reduce the burnout syndrome
occurrence.
02.08.04.04.04 IIndividual and team allocation of cases in palliative care services
is regulated in order to prevent the overburdening and the
burnout syndrome occurrence.
02.08.04.04.05 IA psycho-professional profile of the personnel in palliative care
services is established, tailored to the principles, the values and
the missions of the hospital.
02.08.05 CrThe management of the terminal condition respects the dignity
and comfort of the patient, ensuring family support.
02.08.05.01 RThe terminal condition is identified and the family / guardians
are informed.
02.08.05.01.01 I The terminal illness is identified and documented.
02.08.05.01.02 I
The family / relatives are informed of the terminal illness of the
patient with progressive chronic illness and its palliative care
needs, with due regard for the specific choices made and
assumed by the patient.
APENDIX 2 Page 64 of 99
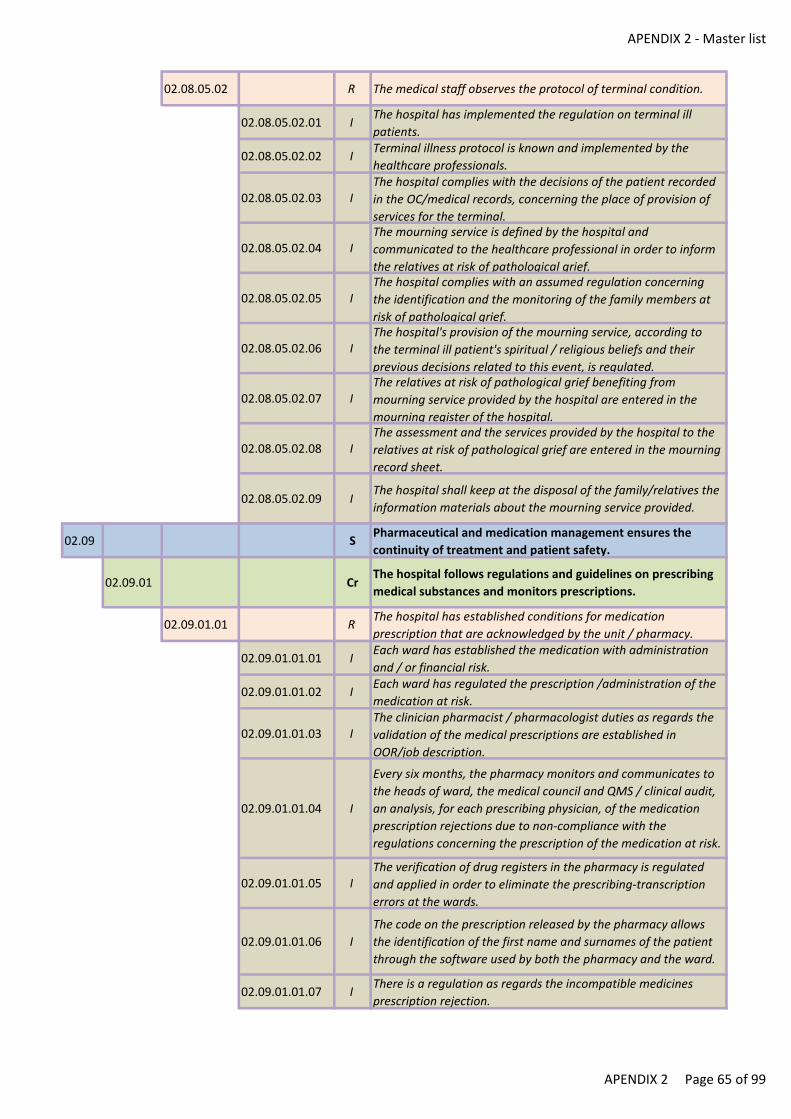
APENDIX 2 - Master list
02.08.05.02 R The medical staff observes the protocol of terminal condition.
02.08.05.02.01 IThe hospital has implemented the regulation on terminal ill
patients.
02.08.05.02.02 ITerminal illness protocol is known and implemented by the
healthcare professionals.
02.08.05.02.03 IThe hospital complies with the decisions of the patient recorded
in the OC/medical records, concerning the place of provision of
services for the terminal.
02.08.05.02.04 IThe mourning service is defined by the hospital and
communicated to the healthcare professional in order to inform
the relatives at risk of pathological grief.
02.08.05.02.05 IThe hospital complies with an assumed regulation concerning
the identification and the monitoring of the family members at
risk of pathological grief.
02.08.05.02.06 IThe hospital's provision of the mourning service, according to
the terminal ill patient's spiritual / religious beliefs and their
previous decisions related to this event, is regulated.
02.08.05.02.07 IThe relatives at risk of pathological grief benefiting from
mourning service provided by the hospital are entered in the
mourning register of the hospital.
02.08.05.02.08 IThe assessment and the services provided by the hospital to the
relatives at risk of pathological grief are entered in the mourning
record sheet.
02.08.05.02.09 IThe hospital shall keep at the disposal of the family/relatives the
information materials about the mourning service provided.
02.09 SPharmaceutical and medication management ensures the
continuity of treatment and patient safety.
02.09.01 CrThe hospital follows regulations and guidelines on prescribing
medical substances and monitors prescriptions.
02.09.01.01 RThe hospital has established conditions for medication
prescription that are acknowledged by the unit / pharmacy.
02.09.01.01.01 IEach ward has established the medication with administration
and / or financial risk.
02.09.01.01.02 IEach ward has regulated the prescription /administration of the
medication at risk.
02.09.01.01.03 IThe clinician pharmacist / pharmacologist duties as regards the
validation of the medical prescriptions are established in
OOR/job description.
02.09.01.01.04 I
Every six months, the pharmacy monitors and communicates to
the heads of ward, the medical council and QMS / clinical audit,
an analysis, for each prescribing physician, of the medication
prescription rejections due to non-compliance with the
regulations concerning the prescription of the medication at risk.
02.09.01.01.05 IThe verification of drug registers in the pharmacy is regulated
and applied in order to eliminate the prescribing-transcription
errors at the wards.
02.09.01.01.06 I
The code on the prescription released by the pharmacy allows
the identification of the first name and surnames of the patient
through the software used by both the pharmacy and the ward.
02.09.01.01.07 IThere is a regulation as regards the incompatible medicines
prescription rejection.
APENDIX 2 Page 65 of 99
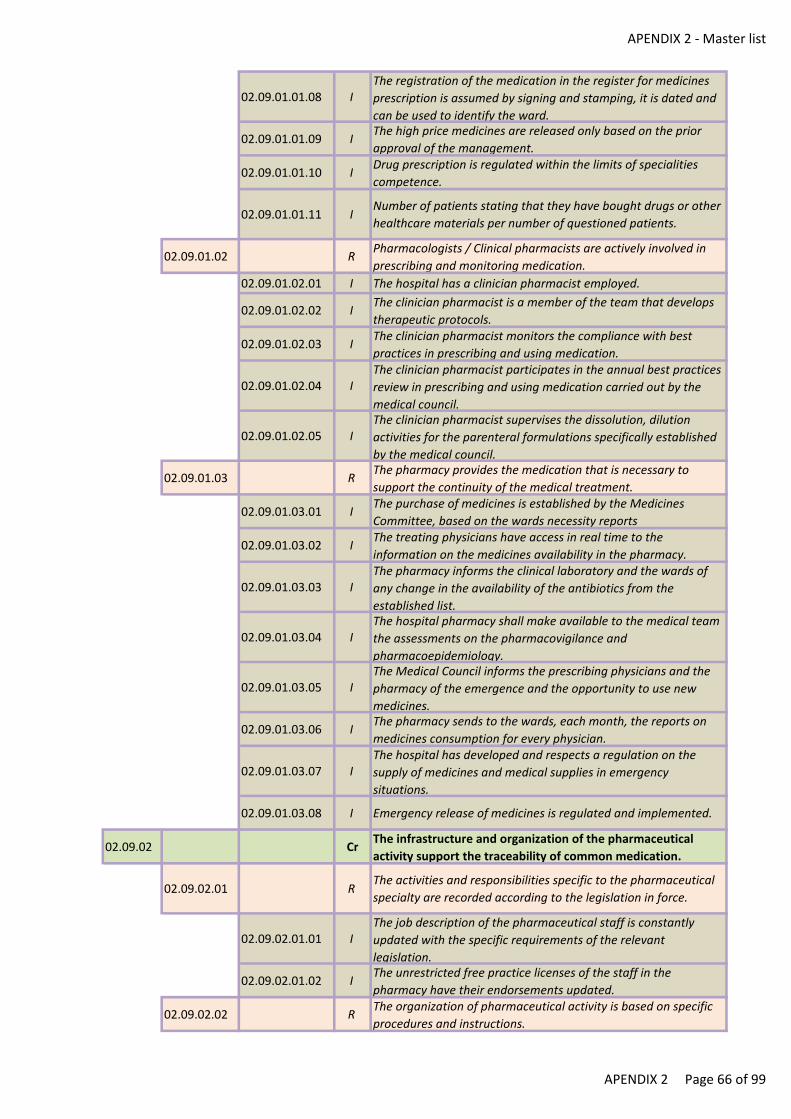
APENDIX 2 - Master list
02.09.01.01.08 IThe registration of the medication in the register for medicines
prescription is assumed by signing and stamping, it is dated and
can be used to identify the ward.
02.09.01.01.09 IThe high price medicines are released only based on the prior
approval of the management.
02.09.01.01.10 IDrug prescription is regulated within the limits of specialities
competence.
02.09.01.01.11 INumber of patients stating that they have bought drugs or other
healthcare materials per number of questioned patients.
02.09.01.02 RPharmacologists / Clinical pharmacists are actively involved in
prescribing and monitoring medication.
02.09.01.02.01 I The hospital has a clinician pharmacist employed.
02.09.01.02.02 IThe clinician pharmacist is a member of the team that develops
therapeutic protocols.
02.09.01.02.03 IThe clinician pharmacist monitors the compliance with best
practices in prescribing and using medication.
02.09.01.02.04 IThe clinician pharmacist participates in the annual best practices
review in prescribing and using medication carried out by the
medical council.
02.09.01.02.05 IThe clinician pharmacist supervises the dissolution, dilution
activities for the parenteral formulations specifically established
by the medical council.
02.09.01.03 RThe pharmacy provides the medication that is necessary to
support the continuity of the medical treatment.
02.09.01.03.01 IThe purchase of medicines is established by the Medicines
Committee, based on the wards necessity reports
02.09.01.03.02 IThe treating physicians have access in real time to the
information on the medicines availability in the pharmacy.
02.09.01.03.03 IThe pharmacy informs the clinical laboratory and the wards of
any change in the availability of the antibiotics from the
established list.
02.09.01.03.04 IThe hospital pharmacy shall make available to the medical team
the assessments on the pharmacovigilance and
pharmacoepidemiology.
02.09.01.03.05 IThe Medical Council informs the prescribing physicians and the
pharmacy of the emergence and the opportunity to use new
medicines.
02.09.01.03.06 IThe pharmacy sends to the wards, each month, the reports on
medicines consumption for every physician.
02.09.01.03.07 IThe hospital has developed and respects a regulation on the
supply of medicines and medical supplies in emergency
situations.
02.09.01.03.08 I Emergency release of medicines is regulated and implemented.
02.09.02 CrThe infrastructure and organization of the pharmaceutical
activity support the traceability of common medication.
02.09.02.01 RThe activities and responsibilities specific to the pharmaceutical
specialty are recorded according to the legislation in force.
02.09.02.01.01 IThe job description of the pharmaceutical staff is constantly
updated with the specific requirements of the relevant
legislation.
02.09.02.01.02 IThe unrestricted free practice licenses of the staff in the
pharmacy have their endorsements updated.
02.09.02.02 RThe organization of pharmaceutical activity is based on specific
procedures and instructions.
APENDIX 2 Page 66 of 99
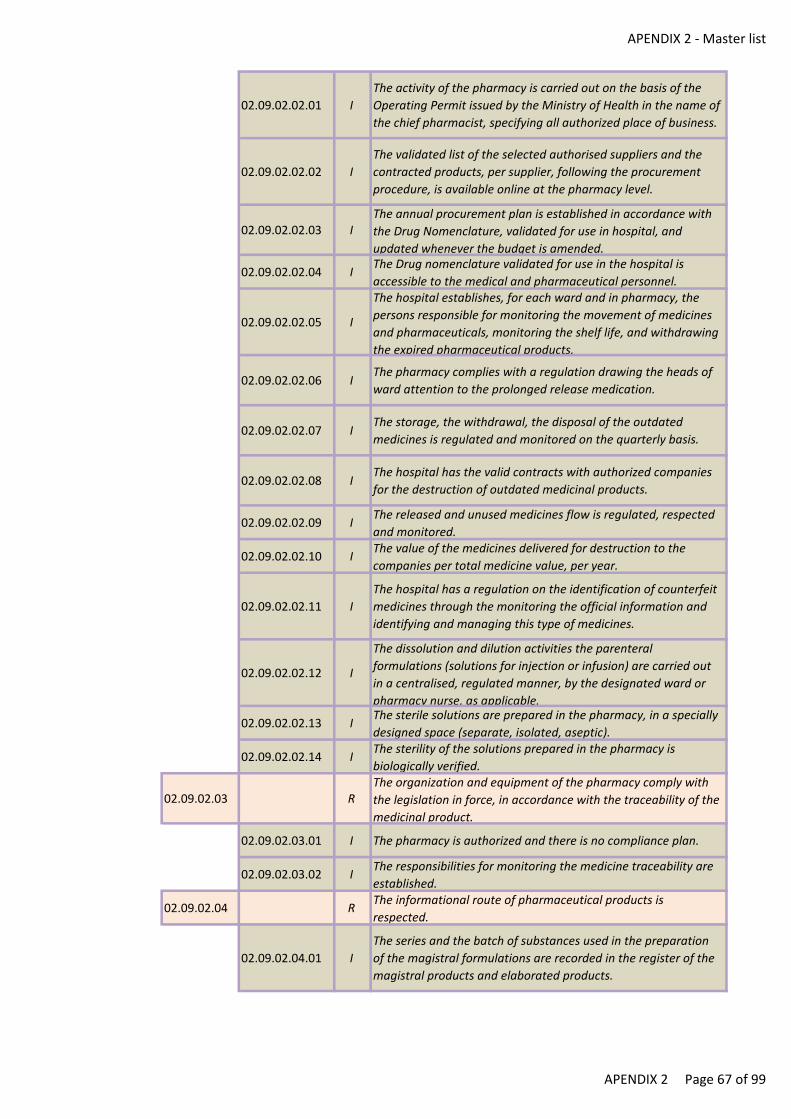
APENDIX 2 - Master list
02.09.02.02.01 I
The activity of the pharmacy is carried out on the basis of the
Operating Permit issued by the Ministry of Health in the name of
the chief pharmacist, specifying all authorized place of business.
02.09.02.02.02 I
The validated list of the selected authorised suppliers and the
contracted products, per supplier, following the procurement
procedure, is available online at the pharmacy level.
02.09.02.02.03 IThe annual procurement plan is established in accordance with
the Drug Nomenclature, validated for use in hospital, and
updated whenever the budget is amended.
02.09.02.02.04 IThe Drug nomenclature validated for use in the hospital is
accessible to the medical and pharmaceutical personnel.
02.09.02.02.05 I
The hospital establishes, for each ward and in pharmacy, the
persons responsible for monitoring the movement of medicines
and pharmaceuticals, monitoring the shelf life, and withdrawing
the expired pharmaceutical products.
02.09.02.02.06 IThe pharmacy complies with a regulation drawing the heads of
ward attention to the prolonged release medication.
02.09.02.02.07 IThe storage, the withdrawal, the disposal of the outdated
medicines is regulated and monitored on the quarterly basis.
02.09.02.02.08 IThe hospital has the valid contracts with authorized companies
for the destruction of outdated medicinal products.
02.09.02.02.09 IThe released and unused medicines flow is regulated, respected
and monitored.
02.09.02.02.10 IThe value of the medicines delivered for destruction to the
companies per total medicine value, per year.
02.09.02.02.11 I
The hospital has a regulation on the identification of counterfeit
medicines through the monitoring the official information and
identifying and managing this type of medicines.
02.09.02.02.12 I
The dissolution and dilution activities the parenteral
formulations (solutions for injection or infusion) are carried out
in a centralised, regulated manner, by the designated ward or
pharmacy nurse, as applicable.
02.09.02.02.13 IThe sterile solutions are prepared in the pharmacy, in a specially
designed space (separate, isolated, aseptic).
02.09.02.02.14 IThe sterility of the solutions prepared in the pharmacy is
biologically verified.
02.09.02.03 RThe organization and equipment of the pharmacy comply with
the legislation in force, in accordance with the traceability of the
medicinal product.
02.09.02.03.01 I The pharmacy is authorized and there is no compliance plan.
02.09.02.03.02 IThe responsibilities for monitoring the medicine traceability are
established.
02.09.02.04 RThe informational route of pharmaceutical products is
respected.
02.09.02.04.01 I
The series and the batch of substances used in the preparation
of the magistral formulations are recorded in the register of the
magistral products and elaborated products.
APENDIX 2 Page 67 of 99
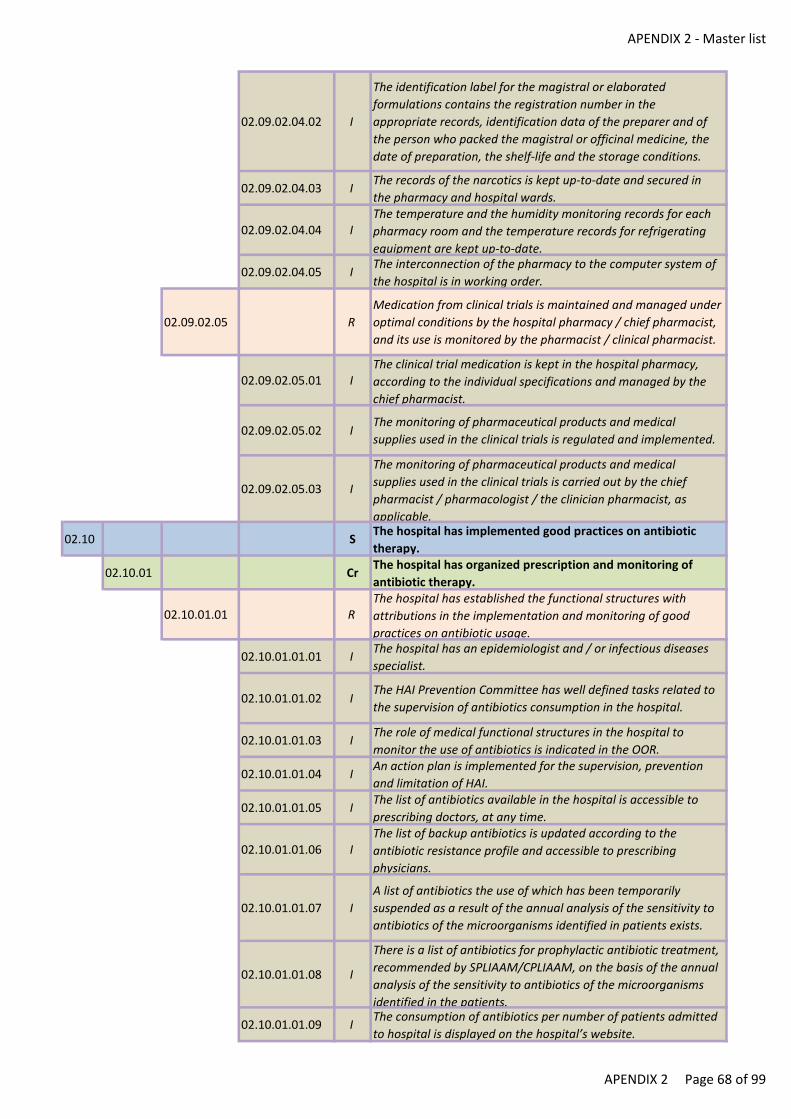
APENDIX 2 - Master list
02.09.02.04.02 I
The identification label for the magistral or elaborated
formulations contains the registration number in the
appropriate records, identification data of the preparer and of
the person who packed the magistral or officinal medicine, the
date of preparation, the shelf-life and the storage conditions.
02.09.02.04.03 IThe records of the narcotics is kept up-to-date and secured in
the pharmacy and hospital wards.
02.09.02.04.04 IThe temperature and the humidity monitoring records for each
pharmacy room and the temperature records for refrigerating
equipment are kept up-to-date.
02.09.02.04.05 IThe interconnection of the pharmacy to the computer system of
the hospital is in working order.
02.09.02.05 R
Medication from clinical trials is maintained and managed under
optimal conditions by the hospital pharmacy / chief pharmacist,
and its use is monitored by the pharmacist / clinical pharmacist.
02.09.02.05.01 IThe clinical trial medication is kept in the hospital pharmacy,
according to the individual specifications and managed by the
chief pharmacist.
02.09.02.05.02 IThe monitoring of pharmaceutical products and medical
supplies used in the clinical trials is regulated and implemented.
02.09.02.05.03 I
The monitoring of pharmaceutical products and medical
supplies used in the clinical trials is carried out by the chief
pharmacist / pharmacologist / the clinician pharmacist, as
applicable.
02.10 SThe hospital has implemented good practices on antibiotic
therapy.
02.10.01 CrThe hospital has organized prescription and monitoring of
antibiotic therapy.
02.10.01.01 RThe hospital has established the functional structures with
attributions in the implementation and monitoring of good
practices on antibiotic usage.
02.10.01.01.01 IThe hospital has an epidemiologist and / or infectious diseases
specialist.
02.10.01.01.02 IThe HAI Prevention Committee has well defined tasks related to
the supervision of antibiotics consumption in the hospital.
02.10.01.01.03 IThe role of medical functional structures in the hospital to
monitor the use of antibiotics is indicated in the OOR.
02.10.01.01.04 IAn action plan is implemented for the supervision, prevention
and limitation of HAI.
02.10.01.01.05 IThe list of antibiotics available in the hospital is accessible to
prescribing doctors, at any time.
02.10.01.01.06 IThe list of backup antibiotics is updated according to the
antibiotic resistance profile and accessible to prescribing
physicians.
02.10.01.01.07 I
A list of antibiotics the use of which has been temporarily
suspended as a result of the annual analysis of the sensitivity to
antibiotics of the microorganisms identified in patients exists.
02.10.01.01.08 I
There is a list of antibiotics for prophylactic antibiotic treatment,
recommended by SPLIAAM/CPLIAAM, on the basis of the annual
analysis of the sensitivity to antibiotics of the microorganisms
identified in the patients.
02.10.01.01.09 IThe consumption of antibiotics per number of patients admitted
to hospital is displayed on the hospital’s website.
APENDIX 2 Page 68 of 99
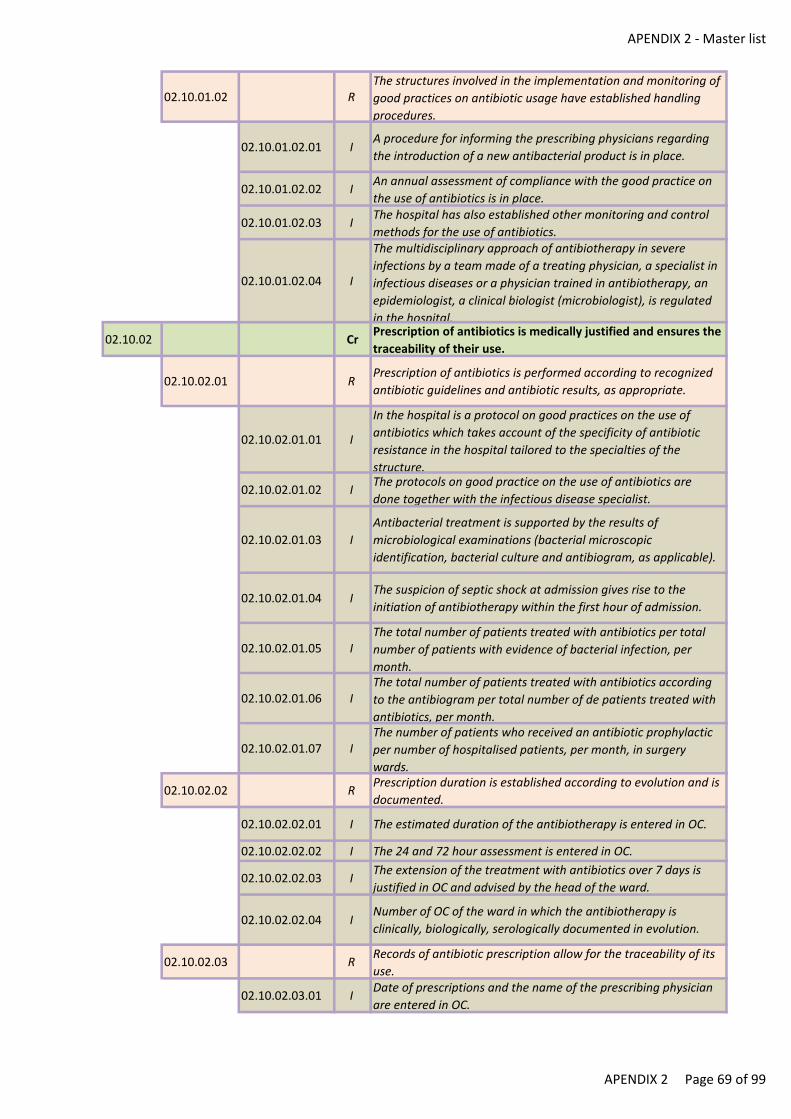
APENDIX 2 - Master list
02.10.01.02 RThe structures involved in the implementation and monitoring of
good practices on antibiotic usage have established handling
procedures.
02.10.01.02.01 IA procedure for informing the prescribing physicians regarding
the introduction of a new antibacterial product is in place.
02.10.01.02.02 IAn annual assessment of compliance with the good practice on
the use of antibiotics is in place.
02.10.01.02.03 IThe hospital has also established other monitoring and control
methods for the use of antibiotics.
02.10.01.02.04 I
The multidisciplinary approach of antibiotherapy in severe
infections by a team made of a treating physician, a specialist in
infectious diseases or a physician trained in antibiotherapy, an
epidemiologist, a clinical biologist (microbiologist), is regulated
in the hospital.
02.10.02 CrPrescription of antibiotics is medically justified and ensures the
traceability of their use.
02.10.02.01 RPrescription of antibiotics is performed according to recognized
antibiotic guidelines and antibiotic results, as appropriate.
02.10.02.01.01 I
In the hospital is a protocol on good practices on the use of
antibiotics which takes account of the specificity of antibiotic
resistance in the hospital tailored to the specialties of the
structure.
02.10.02.01.02 IThe protocols on good practice on the use of antibiotics are
done together with the infectious disease specialist.
02.10.02.01.03 I
Antibacterial treatment is supported by the results of
microbiological examinations (bacterial microscopic
identification, bacterial culture and antibiogram, as applicable).
02.10.02.01.04 IThe suspicion of septic shock at admission gives rise to the
initiation of antibiotherapy within the first hour of admission.
02.10.02.01.05 IThe total number of patients treated with antibiotics per total
number of patients with evidence of bacterial infection, per
month.
02.10.02.01.06 IThe total number of patients treated with antibiotics according
to the antibiogram per total number of de patients treated with
antibiotics, per month.
02.10.02.01.07 IThe number of patients who received an antibiotic prophylactic
per number of hospitalised patients, per month, in surgery
wards.
02.10.02.02 RPrescription duration is established according to evolution and is
documented.
02.10.02.02.01 I The estimated duration of the antibiotherapy is entered in OC.
02.10.02.02.02 I The 24 and 72 hour assessment is entered in OC.
02.10.02.02.03 IThe extension of the treatment with antibiotics over 7 days is
justified in OC and advised by the head of the ward.
02.10.02.02.04 INumber of OC of the ward in which the antibiotherapy is
clinically, biologically, serologically documented in evolution.
02.10.02.03 RRecords of antibiotic prescription allow for the traceability of its
use.
02.10.02.03.01 IDate of prescriptions and the name of the prescribing physician
are entered in OC.
APENDIX 2 Page 69 of 99
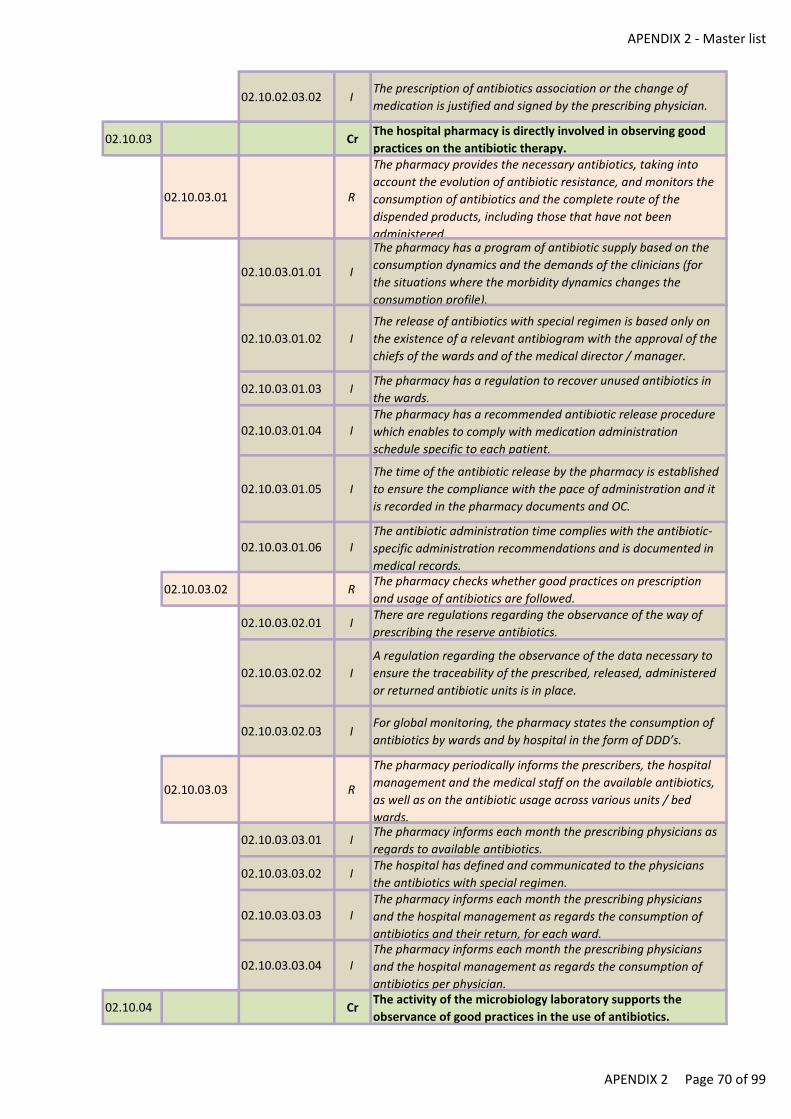
APENDIX 2 - Master list
02.10.02.03.02 IThe prescription of antibiotics association or the change of
medication is justified and signed by the prescribing physician.
02.10.03 CrThe hospital pharmacy is directly involved in observing good
practices on the antibiotic therapy.
02.10.03.01 R
The pharmacy provides the necessary antibiotics, taking into
account the evolution of antibiotic resistance, and monitors the
consumption of antibiotics and the complete route of the
dispended products, including those that have not been
administered.
02.10.03.01.01 I
The pharmacy has a program of antibiotic supply based on the
consumption dynamics and the demands of the clinicians (for
the situations where the morbidity dynamics changes the
consumption profile).
02.10.03.01.02 I
The release of antibiotics with special regimen is based only on
the existence of a relevant antibiogram with the approval of the
chiefs of the wards and of the medical director / manager.
02.10.03.01.03 IThe pharmacy has a regulation to recover unused antibiotics in
the wards.
02.10.03.01.04 IThe pharmacy has a recommended antibiotic release procedure
which enables to comply with medication administration
schedule specific to each patient.
02.10.03.01.05 I
The time of the antibiotic release by the pharmacy is established
to ensure the compliance with the pace of administration and it
is recorded in the pharmacy documents and OC.
02.10.03.01.06 IThe antibiotic administration time complies with the antibiotic-
specific administration recommendations and is documented in
medical records.
02.10.03.02 RThe pharmacy checks whether good practices on prescription
and usage of antibiotics are followed.
02.10.03.02.01 IThere are regulations regarding the observance of the way of
prescribing the reserve antibiotics.
02.10.03.02.02 I
A regulation regarding the observance of the data necessary to
ensure the traceability of the prescribed, released, administered
or returned antibiotic units is in place.
02.10.03.02.03 IFor global monitoring, the pharmacy states the consumption of
antibiotics by wards and by hospital in the form of DDD’s.
02.10.03.03 R
The pharmacy periodically informs the prescribers, the hospital
management and the medical staff on the available antibiotics,
as well as on the antibiotic usage across various units / bed
wards.
02.10.03.03.01 IThe pharmacy informs each month the prescribing physicians as
regards to available antibiotics.
02.10.03.03.02 IThe hospital has defined and communicated to the physicians
the antibiotics with special regimen.
02.10.03.03.03 IThe pharmacy informs each month the prescribing physicians
and the hospital management as regards the consumption of
antibiotics and their return, for each ward.
02.10.03.03.04 IThe pharmacy informs each month the prescribing physicians
and the hospital management as regards the consumption of
antibiotics per physician.
02.10.04 CrThe activity of the microbiology laboratory supports the
observance of good practices in the use of antibiotics.
APENDIX 2 Page 70 of 99
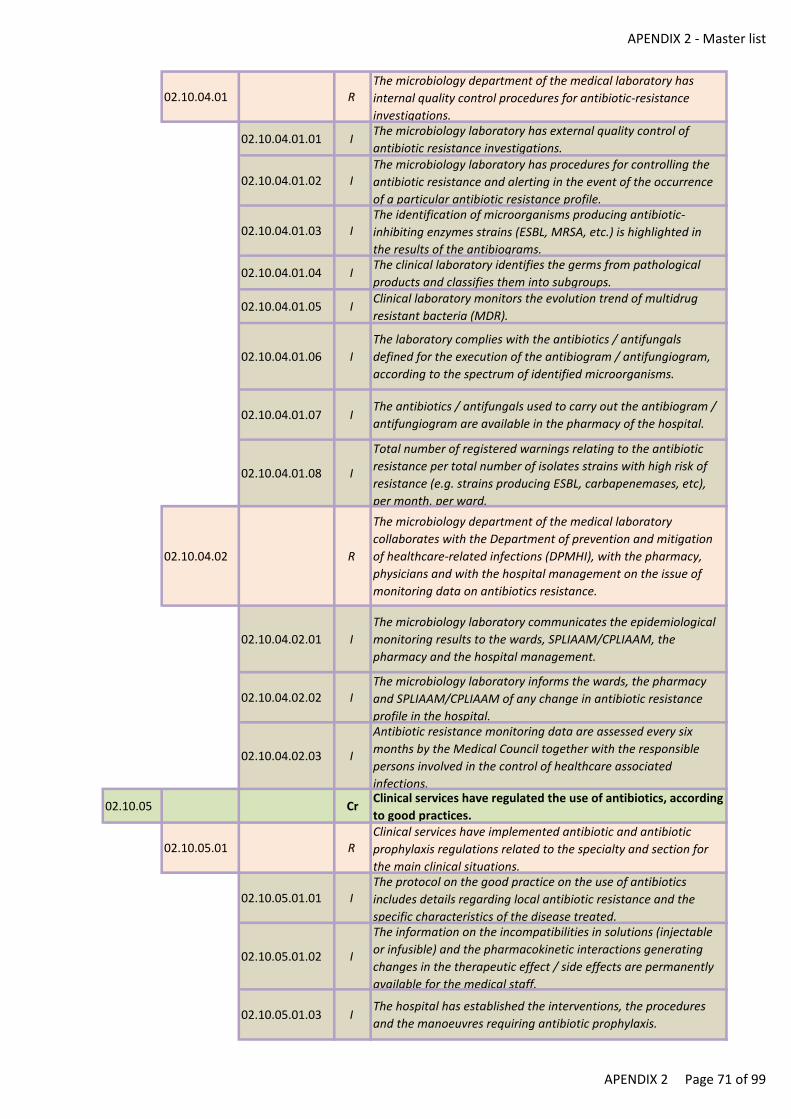
APENDIX 2 - Master list
02.10.04.01 RThe microbiology department of the medical laboratory has
internal quality control procedures for antibiotic-resistance
investigations.
02.10.04.01.01 IThe microbiology laboratory has external quality control of
antibiotic resistance investigations.
02.10.04.01.02 IThe microbiology laboratory has procedures for controlling the
antibiotic resistance and alerting in the event of the occurrence
of a particular antibiotic resistance profile.
02.10.04.01.03 IThe identification of microorganisms producing antibiotic-
inhibiting enzymes strains (ESBL, MRSA, etc.) is highlighted in
the results of the antibiograms.
02.10.04.01.04 IThe clinical laboratory identifies the germs from pathological
products and classifies them into subgroups.
02.10.04.01.05 IClinical laboratory monitors the evolution trend of multidrug
resistant bacteria (MDR).
02.10.04.01.06 I
The laboratory complies with the antibiotics / antifungals
defined for the execution of the antibiogram / antifungiogram,
according to the spectrum of identified microorganisms.
02.10.04.01.07 IThe antibiotics / antifungals used to carry out the antibiogram /
antifungiogram are available in the pharmacy of the hospital.
02.10.04.01.08 I
Total number of registered warnings relating to the antibiotic
resistance per total number of isolates strains with high risk of
resistance (e.g. strains producing ESBL, carbapenemases, etc),
per month, per ward.
02.10.04.02 R
The microbiology department of the medical laboratory
collaborates with the Department of prevention and mitigation
of healthcare-related infections (DPMHI), with the pharmacy,
physicians and with the hospital management on the issue of
monitoring data on antibiotics resistance.
02.10.04.02.01 I
The microbiology laboratory communicates the epidemiological
monitoring results to the wards, SPLIAAM/CPLIAAM, the
pharmacy and the hospital management.
02.10.04.02.02 IThe microbiology laboratory informs the wards, the pharmacy
and SPLIAAM/CPLIAAM of any change in antibiotic resistance
profile in the hospital.
02.10.04.02.03 I
Antibiotic resistance monitoring data are assessed every six
months by the Medical Council together with the responsible
persons involved in the control of healthcare associated
infections.
02.10.05 CrClinical services have regulated the use of antibiotics, according
to good practices.
02.10.05.01 RClinical services have implemented antibiotic and antibiotic
prophylaxis regulations related to the specialty and section for
the main clinical situations.
02.10.05.01.01 IThe protocol on the good practice on the use of antibiotics
includes details regarding local antibiotic resistance and the
specific characteristics of the disease treated.
02.10.05.01.02 I
The information on the incompatibilities in solutions (injectable
or infusible) and the pharmacokinetic interactions generating
changes in the therapeutic effect / side effects are permanently
available for the medical staff.
02.10.05.01.03 IThe hospital has established the interventions, the procedures
and the manoeuvres requiring antibiotic prophylaxis.
APENDIX 2 Page 71 of 99
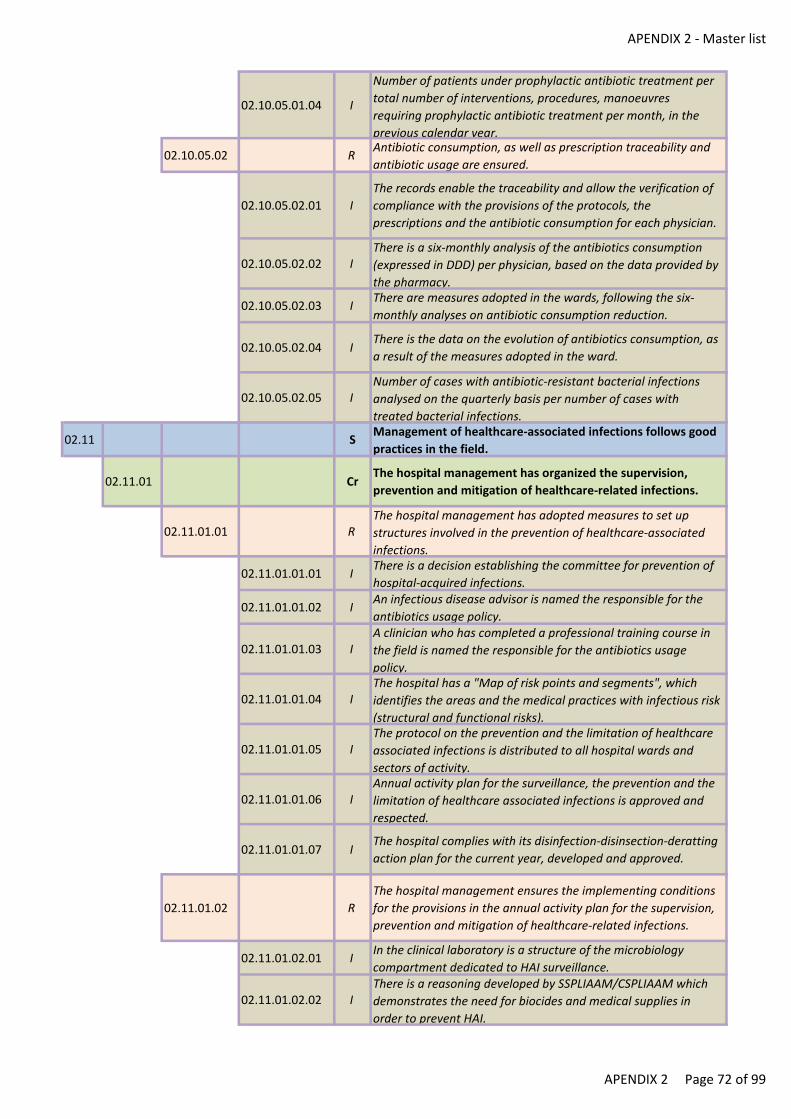
APENDIX 2 - Master list
02.10.05.01.04 I
Number of patients under prophylactic antibiotic treatment per
total number of interventions, procedures, manoeuvres
requiring prophylactic antibiotic treatment per month, in the
previous calendar year.
02.10.05.02 RAntibiotic consumption, as well as prescription traceability and
antibiotic usage are ensured.
02.10.05.02.01 I
The records enable the traceability and allow the verification of
compliance with the provisions of the protocols, the
prescriptions and the antibiotic consumption for each physician.
02.10.05.02.02 IThere is a six-monthly analysis of the antibiotics consumption
(expressed in DDD) per physician, based on the data provided by
the pharmacy.
02.10.05.02.03 IThere are measures adopted in the wards, following the six-
monthly analyses on antibiotic consumption reduction.
02.10.05.02.04 IThere is the data on the evolution of antibiotics consumption, as
a result of the measures adopted in the ward.
02.10.05.02.05 INumber of cases with antibiotic-resistant bacterial infections
analysed on the quarterly basis per number of cases with
treated bacterial infections.
02.11 SManagement of healthcare-associated infections follows good
practices in the field.
02.11.01 CrThe hospital management has organized the supervision,
prevention and mitigation of healthcare-related infections.
02.11.01.01 RThe hospital management has adopted measures to set up
structures involved in the prevention of healthcare-associated
infections.
02.11.01.01.01 IThere is a decision establishing the committee for prevention of
hospital-acquired infections.
02.11.01.01.02 IAn infectious disease advisor is named the responsible for the
antibiotics usage policy.
02.11.01.01.03 IA clinician who has completed a professional training course in
the field is named the responsible for the antibiotics usage
policy.
02.11.01.01.04 IThe hospital has a "Map of risk points and segments", which
identifies the areas and the medical practices with infectious risk
(structural and functional risks).
02.11.01.01.05 IThe protocol on the prevention and the limitation of healthcare
associated infections is distributed to all hospital wards and
sectors of activity.
02.11.01.01.06 IAnnual activity plan for the surveillance, the prevention and the
limitation of healthcare associated infections is approved and
respected.
02.11.01.01.07 IThe hospital complies with its disinfection-disinsection-deratting
action plan for the current year, developed and approved.
02.11.01.02 R
The hospital management ensures the implementing conditions
for the provisions in the annual activity plan for the supervision,
prevention and mitigation of healthcare-related infections.
02.11.01.02.01 IIn the clinical laboratory is a structure of the microbiology
compartment dedicated to HAI surveillance.
02.11.01.02.02 IThere is a reasoning developed by SSPLIAAM/CSPLIAAM which
demonstrates the need for biocides and medical supplies in
order to prevent HAI.
APENDIX 2 Page 72 of 99

APENDIX 2 - Master list
02.11.01.02.03 IThe quantities of biocides and materials for HAI prevention is
decided by the Biocides Biocide and Medical Supplies
Commission in collaboration with SSPLIAAM/CSPLIAAM.
02.11.01.02.04 IAnnual procurement plan contains the quantities of biocides and
medical supplies for preventing HAI.
02.11.01.02.05 IThe budget allocated to the biocides and medical supplies
procurement ensures the HAI prevention.
02.11.01.02.06 IThe amount allocated for HAI prevention expenditures in the
budget per number of cases settled, in the previous calendar
year.
02.11.01.02.07 IThe biocides consumption performed per planned consumption,
in the previous full calendar year.
02.11.01.03 RSupervision, prevention and mitigation of healthcare-related
infections and contagious diseases are organized and
coordinated across every hospital structure.
02.11.01.03.01 IThe registry for the monitoring of healthcare associated
infections is in place.
02.11.01.03.02 IA record exists in the ward / department on the accidental
exposure cases to the biological products.
02.11.01.03.03 IThe procedure for disinfection of the rooms in which were
hospitalized the patients infected / colonised with multi-
resistant bacteria is implemented.
02.11.01.03.04 IThe procedure for the beds and the beddings disinfection is
implemented.
02.11.01.03.05 IThe conditions for the beds and the beddings sterilising are in
place
02.11.01.03.06 IThe sanctions for non-compliance with the procedures and
protocols for HAI prevention and limitation are set out in IR.
02.11.01.03.07 IThe verification of career status for the healthcare professional
is regulated and implemented.
02.11.01.03.08 IThe anaesthesia and the assisted breathing of the infectious-
contagious patient are regulated.
02.11.01.03.09 IThe Healthcare Associated Infections Committee analyses each
month the all cases of HAI with multi-resistant microorganisms.
02.11.01.03.10 I
The Healthcare Associated Infections Committee has a half-
yearly review of compliance with HAI prevention and limiting
procedures and protocols and takes action accordingly.
02.11.01.03.11 I
The programme for improving hand hygiene, implemented by
the hospital, set out the action plan, the responsible persons, the
indicators and the resources needed to accomplish it.
02.11.01.03.12 IThe programme for improving hand hygiene, implemented by
the hospital, set out the training of the personnel according to
the specificity of their activity.
02.11.01.03.13 IThe programme for improving hand hygiene, implemented by
the hospital, is assessed and revised annually.
02.11.01.03.14 IThe healthcare professionals are trained to address the patients
for whom a “clean area” microclimate needs to be provided.
02.11.01.03.15 IThe surgical interventions’ planning is regulated and is made on
the basis of the infection hazard and the emergency level.
02.11.01.03.16 IThe number of hands sanitation samples, with a positive result
out of the total hands sanitation samples collected from each
work sector, per year.
APENDIX 2 Page 73 of 99
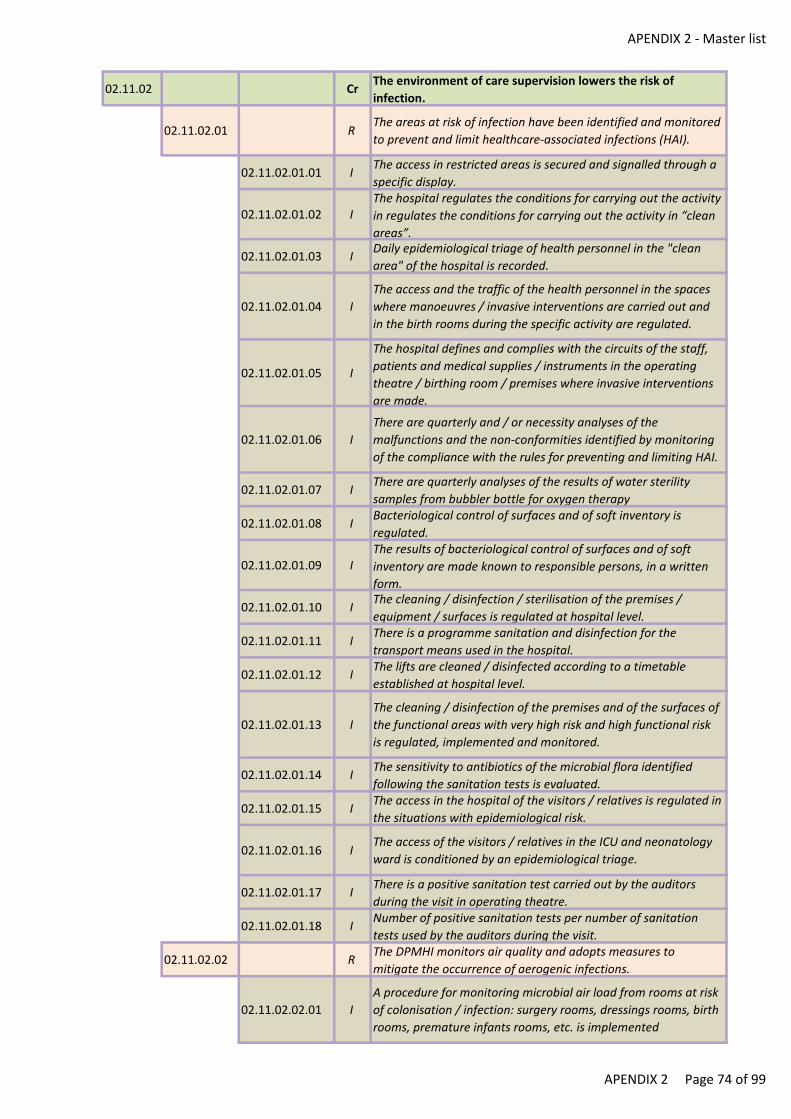
APENDIX 2 - Master list
02.11.02 CrThe environment of care supervision lowers the risk of
infection.
02.11.02.01 RThe areas at risk of infection have been identified and monitored
to prevent and limit healthcare-associated infections (HAI).
02.11.02.01.01 IThe access in restricted areas is secured and signalled through a
specific display.
02.11.02.01.02 IThe hospital regulates the conditions for carrying out the activity
in regulates the conditions for carrying out the activity in “clean
areas”.
02.11.02.01.03 IDaily epidemiological triage of health personnel in the "clean
area" of the hospital is recorded.
02.11.02.01.04 I
The access and the traffic of the health personnel in the spaces
where manoeuvres / invasive interventions are carried out and
in the birth rooms during the specific activity are regulated.
02.11.02.01.05 I
The hospital defines and complies with the circuits of the staff,
patients and medical supplies / instruments in the operating
theatre / birthing room / premises where invasive interventions
are made.
02.11.02.01.06 I
There are quarterly and / or necessity analyses of the
malfunctions and the non-conformities identified by monitoring
of the compliance with the rules for preventing and limiting HAI.
02.11.02.01.07 IThere are quarterly analyses of the results of water sterility
samples from bubbler bottle for oxygen therapy
02.11.02.01.08 IBacteriological control of surfaces and of soft inventory is
regulated.
02.11.02.01.09 IThe results of bacteriological control of surfaces and of soft
inventory are made known to responsible persons, in a written
form.
02.11.02.01.10 IThe cleaning / disinfection / sterilisation of the premises /
equipment / surfaces is regulated at hospital level.
02.11.02.01.11 IThere is a programme sanitation and disinfection for the
transport means used in the hospital.
02.11.02.01.12 IThe lifts are cleaned / disinfected according to a timetable
established at hospital level.
02.11.02.01.13 I
The cleaning / disinfection of the premises and of the surfaces of
the functional areas with very high risk and high functional risk
is regulated, implemented and monitored.
02.11.02.01.14 IThe sensitivity to antibiotics of the microbial flora identified
following the sanitation tests is evaluated.
02.11.02.01.15 IThe access in the hospital of the visitors / relatives is regulated in
the situations with epidemiological risk.
02.11.02.01.16 IThe access of the visitors / relatives in the ICU and neonatology
ward is conditioned by an epidemiological triage.
02.11.02.01.17 IThere is a positive sanitation test carried out by the auditors
during the visit in operating theatre.
02.11.02.01.18 INumber of positive sanitation tests per number of sanitation
tests used by the auditors during the visit.
02.11.02.02 RThe DPMHI monitors air quality and adopts measures to
mitigate the occurrence of aerogenic infections.
02.11.02.02.01 I
A procedure for monitoring microbial air load from rooms at risk
of colonisation / infection: surgery rooms, dressings rooms, birth
rooms, premature infants rooms, etc. is implemented
APENDIX 2 Page 74 of 99
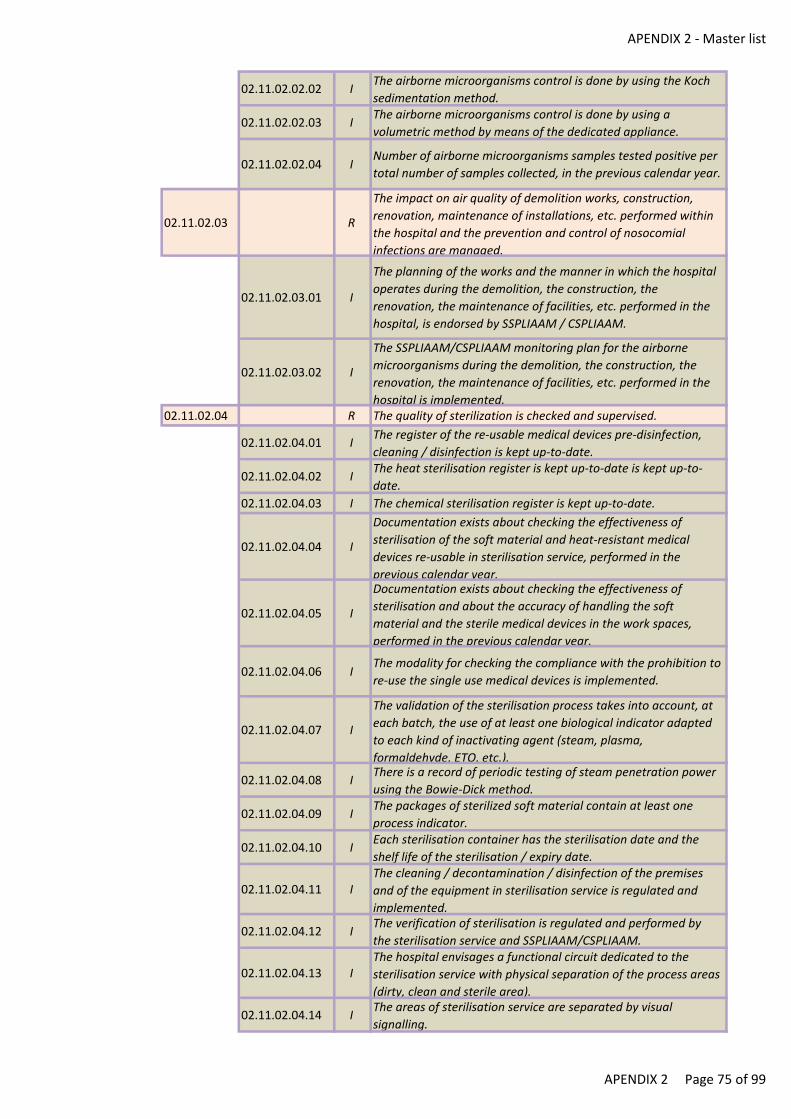
APENDIX 2 - Master list
02.11.02.02.02 IThe airborne microorganisms control is done by using the Koch
sedimentation method.
02.11.02.02.03 IThe airborne microorganisms control is done by using a
volumetric method by means of the dedicated appliance.
02.11.02.02.04 INumber of airborne microorganisms samples tested positive per
total number of samples collected, in the previous calendar year.
02.11.02.03 R
The impact on air quality of demolition works, construction,
renovation, maintenance of installations, etc. performed within
the hospital and the prevention and control of nosocomial
infections are managed.
02.11.02.03.01 I
The planning of the works and the manner in which the hospital
operates during the demolition, the construction, the
renovation, the maintenance of facilities, etc. performed in the
hospital, is endorsed by SSPLIAAM / CSPLIAAM.
02.11.02.03.02 I
The SSPLIAAM/CSPLIAAM monitoring plan for the airborne
microorganisms during the demolition, the construction, the
renovation, the maintenance of facilities, etc. performed in the
hospital is implemented.02.11.02.04 R The quality of sterilization is checked and supervised.
02.11.02.04.01 IThe register of the re-usable medical devices pre-disinfection,
cleaning / disinfection is kept up-to-date.
02.11.02.04.02 IThe heat sterilisation register is kept up-to-date is kept up-to-
date.
02.11.02.04.03 I The chemical sterilisation register is kept up-to-date.
02.11.02.04.04 I
Documentation exists about checking the effectiveness of
sterilisation of the soft material and heat-resistant medical
devices re-usable in sterilisation service, performed in the
previous calendar year.
02.11.02.04.05 I
Documentation exists about checking the effectiveness of
sterilisation and about the accuracy of handling the soft
material and the sterile medical devices in the work spaces,
performed in the previous calendar year.
02.11.02.04.06 IThe modality for checking the compliance with the prohibition to
re-use the single use medical devices is implemented.
02.11.02.04.07 I
The validation of the sterilisation process takes into account, at
each batch, the use of at least one biological indicator adapted
to each kind of inactivating agent (steam, plasma,
formaldehyde, ETO, etc.).
02.11.02.04.08 IThere is a record of periodic testing of steam penetration power
using the Bowie-Dick method.
02.11.02.04.09 IThe packages of sterilized soft material contain at least one
process indicator.
02.11.02.04.10 IEach sterilisation container has the sterilisation date and the
shelf life of the sterilisation / expiry date.
02.11.02.04.11 IThe cleaning / decontamination / disinfection of the premises
and of the equipment in sterilisation service is regulated and
implemented.
02.11.02.04.12 IThe verification of sterilisation is regulated and performed by
the sterilisation service and SSPLIAAM/CSPLIAAM.
02.11.02.04.13 IThe hospital envisages a functional circuit dedicated to the
sterilisation service with physical separation of the process areas
(dirty, clean and sterile area).
02.11.02.04.14 IThe areas of sterilisation service are separated by visual
signalling.
APENDIX 2 Page 75 of 99
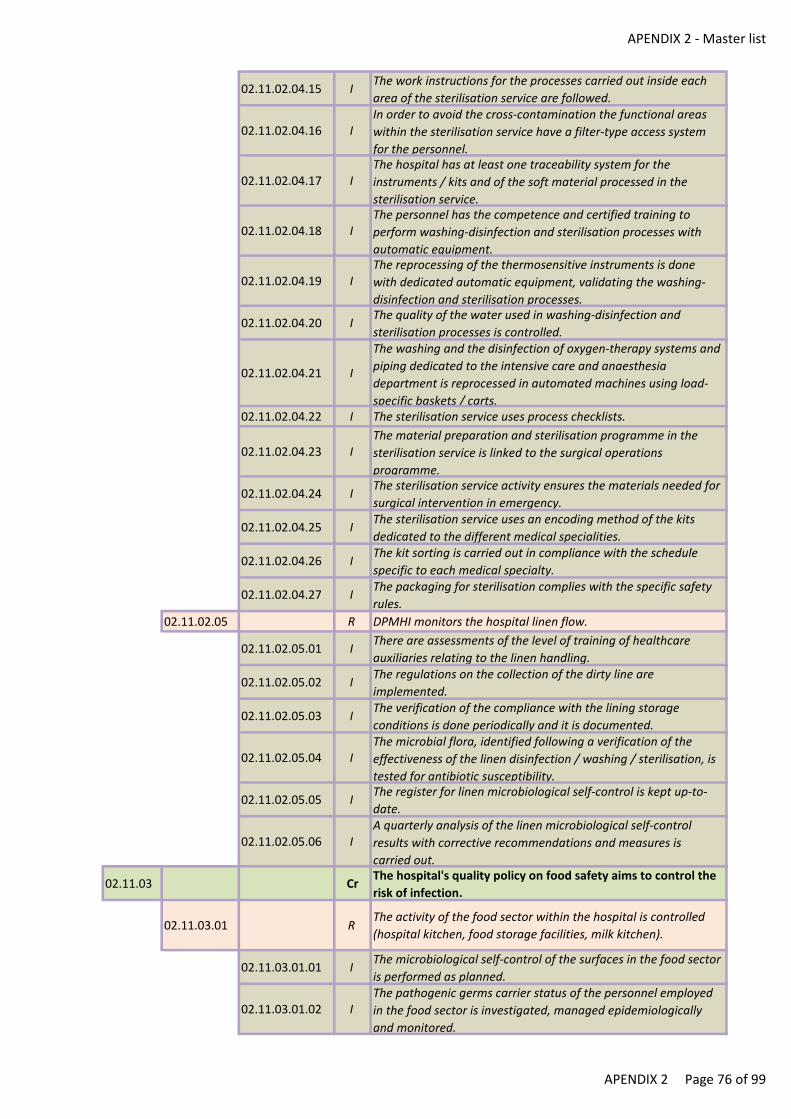
APENDIX 2 - Master list
02.11.02.04.15 IThe work instructions for the processes carried out inside each
area of the sterilisation service are followed.
02.11.02.04.16 IIn order to avoid the cross-contamination the functional areas
within the sterilisation service have a filter-type access system
for the personnel.
02.11.02.04.17 IThe hospital has at least one traceability system for the
instruments / kits and of the soft material processed in the
sterilisation service.
02.11.02.04.18 IThe personnel has the competence and certified training to
perform washing-disinfection and sterilisation processes with
automatic equipment.
02.11.02.04.19 IThe reprocessing of the thermosensitive instruments is done
with dedicated automatic equipment, validating the washing-
disinfection and sterilisation processes.
02.11.02.04.20 IThe quality of the water used in washing-disinfection and
sterilisation processes is controlled.
02.11.02.04.21 I
The washing and the disinfection of oxygen-therapy systems and
piping dedicated to the intensive care and anaesthesia
department is reprocessed in automated machines using load-
specific baskets / carts.02.11.02.04.22 I The sterilisation service uses process checklists.
02.11.02.04.23 IThe material preparation and sterilisation programme in the
sterilisation service is linked to the surgical operations
programme.
02.11.02.04.24 IThe sterilisation service activity ensures the materials needed for
surgical intervention in emergency.
02.11.02.04.25 IThe sterilisation service uses an encoding method of the kits
dedicated to the different medical specialities.
02.11.02.04.26 IThe kit sorting is carried out in compliance with the schedule
specific to each medical specialty.
02.11.02.04.27 IThe packaging for sterilisation complies with the specific safety
rules.
02.11.02.05 R DPMHI monitors the hospital linen flow.
02.11.02.05.01 IThere are assessments of the level of training of healthcare
auxiliaries relating to the linen handling.
02.11.02.05.02 IThe regulations on the collection of the dirty line are
implemented.
02.11.02.05.03 IThe verification of the compliance with the lining storage
conditions is done periodically and it is documented.
02.11.02.05.04 IThe microbial flora, identified following a verification of the
effectiveness of the linen disinfection / washing / sterilisation, is
tested for antibiotic susceptibility.
02.11.02.05.05 IThe register for linen microbiological self-control is kept up-to-
date.
02.11.02.05.06 IA quarterly analysis of the linen microbiological self-control
results with corrective recommendations and measures is
carried out.
02.11.03 CrThe hospital's quality policy on food safety aims to control the
risk of infection.
02.11.03.01 RThe activity of the food sector within the hospital is controlled
(hospital kitchen, food storage facilities, milk kitchen).
02.11.03.01.01 IThe microbiological self-control of the surfaces in the food sector
is performed as planned.
02.11.03.01.02 IThe pathogenic germs carrier status of the personnel employed
in the food sector is investigated, managed epidemiologically
and monitored.
APENDIX 2 Page 76 of 99
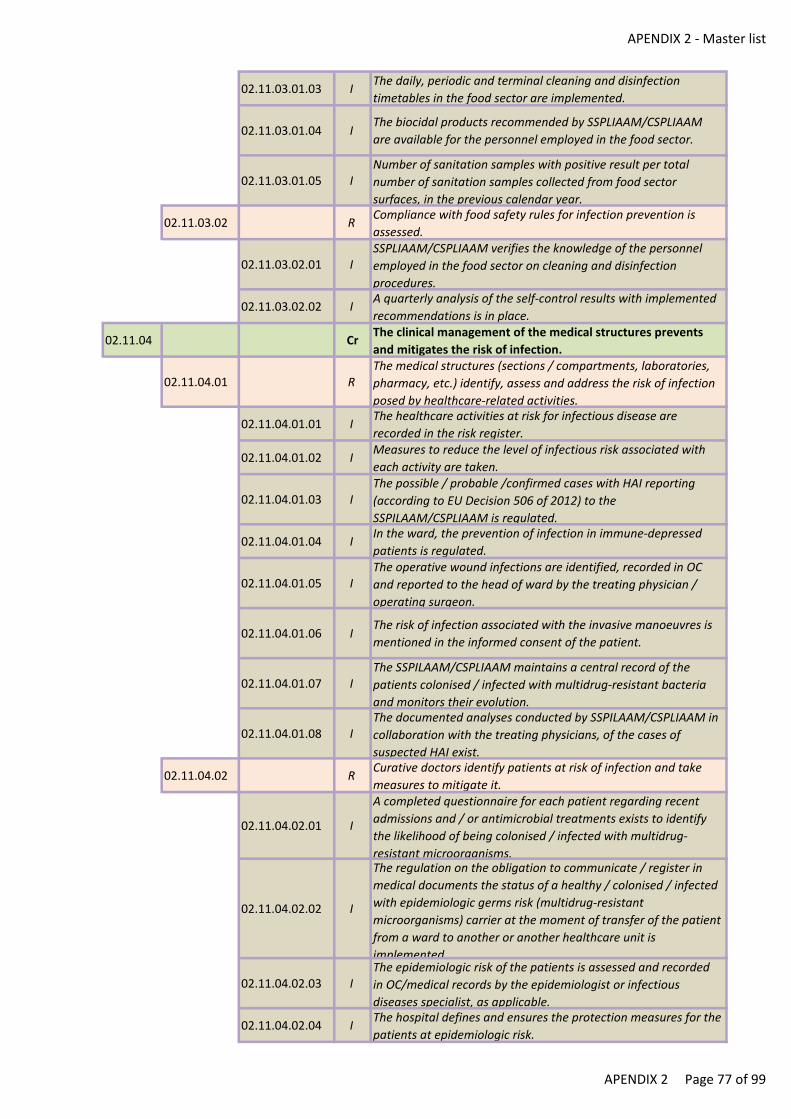
APENDIX 2 - Master list
02.11.03.01.03 IThe daily, periodic and terminal cleaning and disinfection
timetables in the food sector are implemented.
02.11.03.01.04 IThe biocidal products recommended by SSPLIAAM/CSPLIAAM
are available for the personnel employed in the food sector.
02.11.03.01.05 INumber of sanitation samples with positive result per total
number of sanitation samples collected from food sector
surfaces, in the previous calendar year.
02.11.03.02 RCompliance with food safety rules for infection prevention is
assessed.
02.11.03.02.01 ISSPLIAAM/CSPLIAAM verifies the knowledge of the personnel
employed in the food sector on cleaning and disinfection
procedures.
02.11.03.02.02 IA quarterly analysis of the self-control results with implemented
recommendations is in place.
02.11.04 CrThe clinical management of the medical structures prevents
and mitigates the risk of infection.
02.11.04.01 RThe medical structures (sections / compartments, laboratories,
pharmacy, etc.) identify, assess and address the risk of infection
posed by healthcare-related activities.
02.11.04.01.01 IThe healthcare activities at risk for infectious disease are
recorded in the risk register.
02.11.04.01.02 IMeasures to reduce the level of infectious risk associated with
each activity are taken.
02.11.04.01.03 IThe possible / probable /confirmed cases with HAI reporting
(according to EU Decision 506 of 2012) to the
SSPILAAM/CSPLIAAM is regulated.
02.11.04.01.04 IIn the ward, the prevention of infection in immune-depressed
patients is regulated.
02.11.04.01.05 IThe operative wound infections are identified, recorded in OC
and reported to the head of ward by the treating physician /
operating surgeon.
02.11.04.01.06 IThe risk of infection associated with the invasive manoeuvres is
mentioned in the informed consent of the patient.
02.11.04.01.07 IThe SSPILAAM/CSPLIAAM maintains a central record of the
patients colonised / infected with multidrug-resistant bacteria
and monitors their evolution.
02.11.04.01.08 IThe documented analyses conducted by SSPILAAM/CSPLIAAM in
collaboration with the treating physicians, of the cases of
suspected HAI exist.
02.11.04.02 RCurative doctors identify patients at risk of infection and take
measures to mitigate it.
02.11.04.02.01 I
A completed questionnaire for each patient regarding recent
admissions and / or antimicrobial treatments exists to identify
the likelihood of being colonised / infected with multidrug-
resistant microorganisms.
02.11.04.02.02 I
The regulation on the obligation to communicate / register in
medical documents the status of a healthy / colonised / infected
with epidemiologic germs risk (multidrug-resistant
microorganisms) carrier at the moment of transfer of the patient
from a ward to another or another healthcare unit is
implemented.
02.11.04.02.03 IThe epidemiologic risk of the patients is assessed and recorded
in OC/medical records by the epidemiologist or infectious
diseases specialist, as applicable.
02.11.04.02.04 IThe hospital defines and ensures the protection measures for the
patients at epidemiologic risk.
APENDIX 2 Page 77 of 99
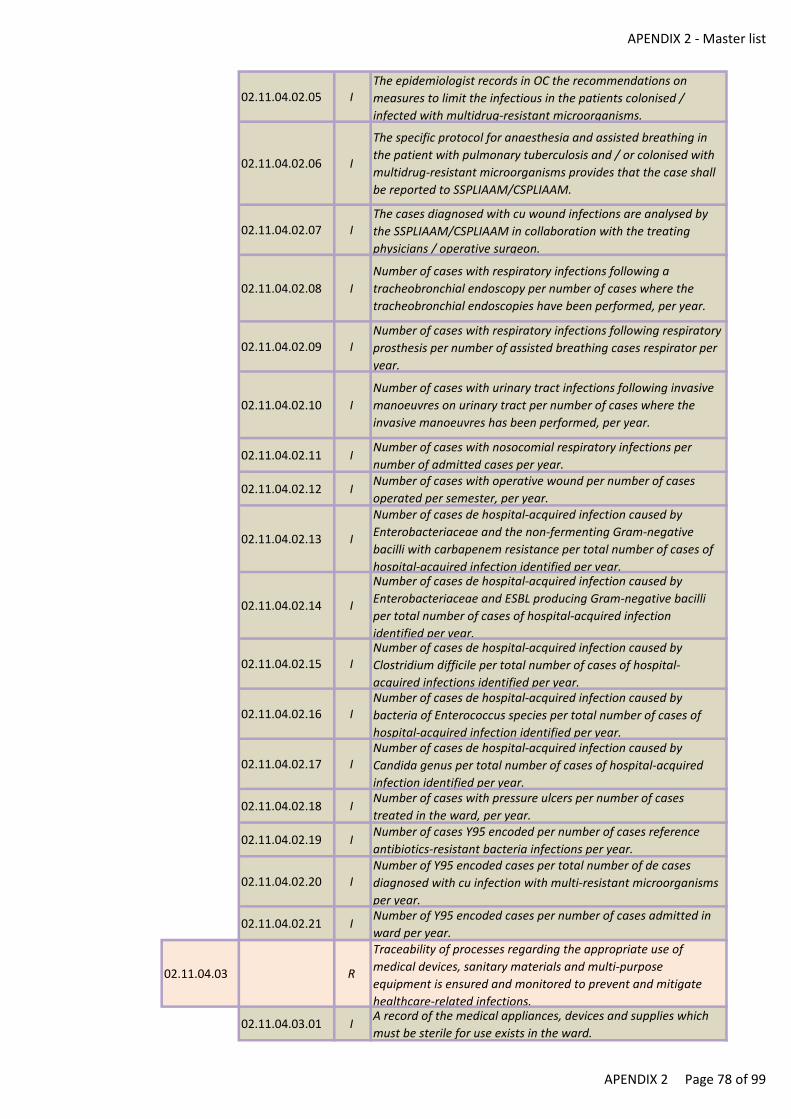
APENDIX 2 - Master list
02.11.04.02.05 IThe epidemiologist records in OC the recommendations on
measures to limit the infectious in the patients colonised /
infected with multidrug-resistant microorganisms.
02.11.04.02.06 I
The specific protocol for anaesthesia and assisted breathing in
the patient with pulmonary tuberculosis and / or colonised with
multidrug-resistant microorganisms provides that the case shall
be reported to SSPLIAAM/CSPLIAAM.
02.11.04.02.07 IThe cases diagnosed with cu wound infections are analysed by
the SSPLIAAM/CSPLIAAM in collaboration with the treating
physicians / operative surgeon.
02.11.04.02.08 I
Number of cases with respiratory infections following a
tracheobronchial endoscopy per number of cases where the
tracheobronchial endoscopies have been performed, per year.
02.11.04.02.09 INumber of cases with respiratory infections following respiratory
prosthesis per number of assisted breathing cases respirator per
year.
02.11.04.02.10 I
Number of cases with urinary tract infections following invasive
manoeuvres on urinary tract per number of cases where the
invasive manoeuvres has been performed, per year.
02.11.04.02.11 INumber of cases with nosocomial respiratory infections per
number of admitted cases per year.
02.11.04.02.12 INumber of cases with operative wound per number of cases
operated per semester, per year.
02.11.04.02.13 I
Number of cases de hospital-acquired infection caused by
Enterobacteriaceae and the non-fermenting Gram-negative
bacilli with carbapenem resistance per total number of cases of
hospital-acquired infection identified per year.
02.11.04.02.14 I
Number of cases de hospital-acquired infection caused by
Enterobacteriaceae and ESBL producing Gram-negative bacilli
per total number of cases of hospital-acquired infection
identified per year.
02.11.04.02.15 INumber of cases de hospital-acquired infection caused by
Clostridium difficile per total number of cases of hospital-
acquired infections identified per year.
02.11.04.02.16 INumber of cases de hospital-acquired infection caused by
bacteria of Enterococcus species per total number of cases of
hospital-acquired infection identified per year.
02.11.04.02.17 INumber of cases de hospital-acquired infection caused by
Candida genus per total number of cases of hospital-acquired
infection identified per year.
02.11.04.02.18 INumber of cases with pressure ulcers per number of cases
treated in the ward, per year.
02.11.04.02.19 INumber of cases Y95 encoded per number of cases reference
antibiotics-resistant bacteria infections per year.
02.11.04.02.20 INumber of Y95 encoded cases per total number of de cases
diagnosed with cu infection with multi-resistant microorganisms
per year.
02.11.04.02.21 INumber of Y95 encoded cases per number of cases admitted in
ward per year.
02.11.04.03 R
Traceability of processes regarding the appropriate use of
medical devices, sanitary materials and multi-purpose
equipment is ensured and monitored to prevent and mitigate
healthcare-related infections.
02.11.04.03.01 IA record of the medical appliances, devices and supplies which
must be sterile for use exists in the ward.
APENDIX 2 Page 78 of 99
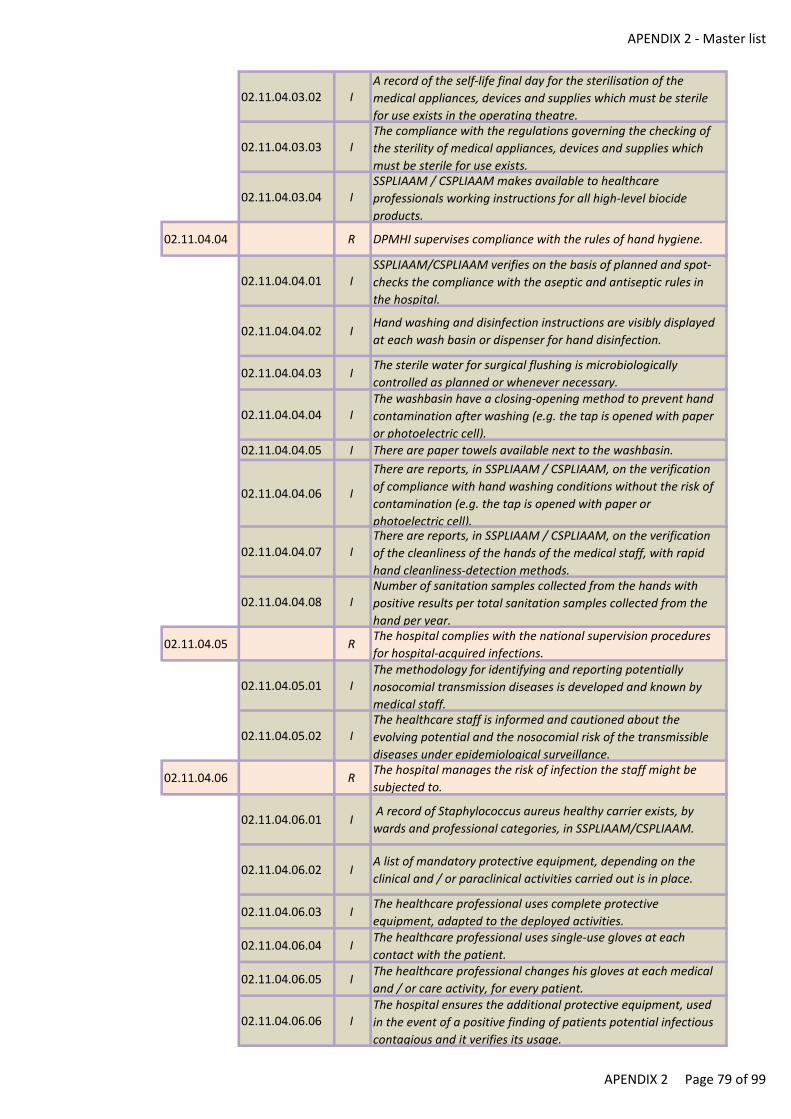
APENDIX 2 - Master list
02.11.04.03.02 IA record of the self-life final day for the sterilisation of the
medical appliances, devices and supplies which must be sterile
for use exists in the operating theatre.
02.11.04.03.03 IThe compliance with the regulations governing the checking of
the sterility of medical appliances, devices and supplies which
must be sterile for use exists.
02.11.04.03.04 ISSPLIAAM / CSPLIAAM makes available to healthcare
professionals working instructions for all high-level biocide
products.
02.11.04.04 R DPMHI supervises compliance with the rules of hand hygiene.
02.11.04.04.01 ISSPLIAAM/CSPLIAAM verifies on the basis of planned and spot-
checks the compliance with the aseptic and antiseptic rules in
the hospital.
02.11.04.04.02 IHand washing and disinfection instructions are visibly displayed
at each wash basin or dispenser for hand disinfection.
02.11.04.04.03 IThe sterile water for surgical flushing is microbiologically
controlled as planned or whenever necessary.
02.11.04.04.04 IThe washbasin have a closing-opening method to prevent hand
contamination after washing (e.g. the tap is opened with paper
or photoelectric cell).
02.11.04.04.05 I There are paper towels available next to the washbasin.
02.11.04.04.06 I
There are reports, in SSPLIAAM / CSPLIAAM, on the verification
of compliance with hand washing conditions without the risk of
contamination (e.g. the tap is opened with paper or
photoelectric cell).
02.11.04.04.07 IThere are reports, in SSPLIAAM / CSPLIAAM, on the verification
of the cleanliness of the hands of the medical staff, with rapid
hand cleanliness-detection methods.
02.11.04.04.08 INumber of sanitation samples collected from the hands with
positive results per total sanitation samples collected from the
hand per year.
02.11.04.05 RThe hospital complies with the national supervision procedures
for hospital-acquired infections.
02.11.04.05.01 IThe methodology for identifying and reporting potentially
nosocomial transmission diseases is developed and known by
medical staff.
02.11.04.05.02 IThe healthcare staff is informed and cautioned about the
evolving potential and the nosocomial risk of the transmissible
diseases under epidemiological surveillance.
02.11.04.06 RThe hospital manages the risk of infection the staff might be
subjected to.
02.11.04.06.01 I A record of Staphylococcus aureus healthy carrier exists, by
wards and professional categories, in SSPLIAAM/CSPLIAAM.
02.11.04.06.02 IA list of mandatory protective equipment, depending on the
clinical and / or paraclinical activities carried out is in place.
02.11.04.06.03 IThe healthcare professional uses complete protective
equipment, adapted to the deployed activities.
02.11.04.06.04 IThe healthcare professional uses single-use gloves at each
contact with the patient.
02.11.04.06.05 IThe healthcare professional changes his gloves at each medical
and / or care activity, for every patient.
02.11.04.06.06 IThe hospital ensures the additional protective equipment, used
in the event of a positive finding of patients potential infectious
contagious and it verifies its usage.
APENDIX 2 Page 79 of 99
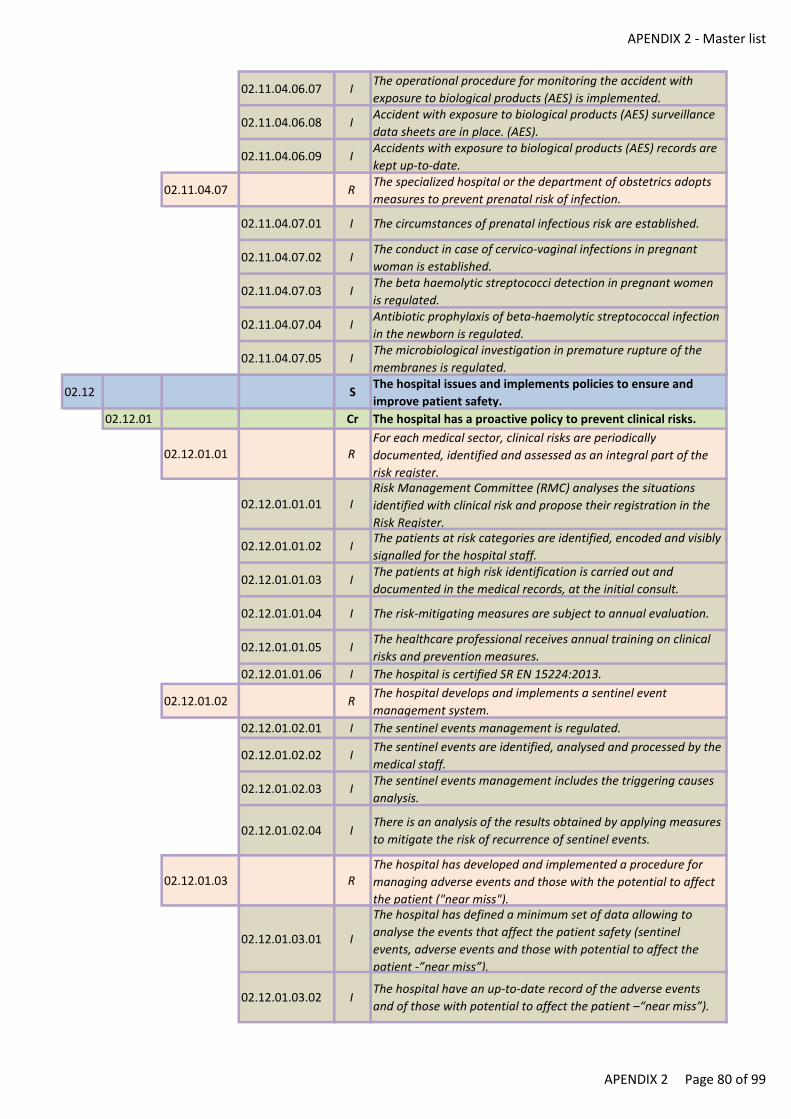
APENDIX 2 - Master list
02.11.04.06.07 IThe operational procedure for monitoring the accident with
exposure to biological products (AES) is implemented.
02.11.04.06.08 IAccident with exposure to biological products (AES) surveillance
data sheets are in place. (AES).
02.11.04.06.09 IAccidents with exposure to biological products (AES) records are
kept up-to-date.
02.11.04.07 RThe specialized hospital or the department of obstetrics adopts
measures to prevent prenatal risk of infection.
02.11.04.07.01 I The circumstances of prenatal infectious risk are established.
02.11.04.07.02 IThe conduct in case of cervico-vaginal infections in pregnant
woman is established.
02.11.04.07.03 IThe beta haemolytic streptococci detection in pregnant women
is regulated.
02.11.04.07.04 IAntibiotic prophylaxis of beta-haemolytic streptococcal infection
in the newborn is regulated.
02.11.04.07.05 IThe microbiological investigation in premature rupture of the
membranes is regulated.
02.12 SThe hospital issues and implements policies to ensure and
improve patient safety.
02.12.01 Cr The hospital has a proactive policy to prevent clinical risks.
02.12.01.01 RFor each medical sector, clinical risks are periodically
documented, identified and assessed as an integral part of the
risk register.
02.12.01.01.01 IRisk Management Committee (RMC) analyses the situations
identified with clinical risk and propose their registration in the
Risk Register.
02.12.01.01.02 IThe patients at risk categories are identified, encoded and visibly
signalled for the hospital staff.
02.12.01.01.03 IThe patients at high risk identification is carried out and
documented in the medical records, at the initial consult.
02.12.01.01.04 I The risk-mitigating measures are subject to annual evaluation.
02.12.01.01.05 IThe healthcare professional receives annual training on clinical
risks and prevention measures.
02.12.01.01.06 I The hospital is certified SR EN 15224:2013.
02.12.01.02 RThe hospital develops and implements a sentinel event
management system.
02.12.01.02.01 I The sentinel events management is regulated.
02.12.01.02.02 IThe sentinel events are identified, analysed and processed by the
medical staff.
02.12.01.02.03 IThe sentinel events management includes the triggering causes
analysis.
02.12.01.02.04 IThere is an analysis of the results obtained by applying measures
to mitigate the risk of recurrence of sentinel events.
02.12.01.03 RThe hospital has developed and implemented a procedure for
managing adverse events and those with the potential to affect
the patient ("near miss").
02.12.01.03.01 I
The hospital has defined a minimum set of data allowing to
analyse the events that affect the patient safety (sentinel
events, adverse events and those with potential to affect the
patient -”near miss”).
02.12.01.03.02 IThe hospital have an up-to-date record of the adverse events
and of those with potential to affect the patient –“near miss”).
APENDIX 2 Page 80 of 99
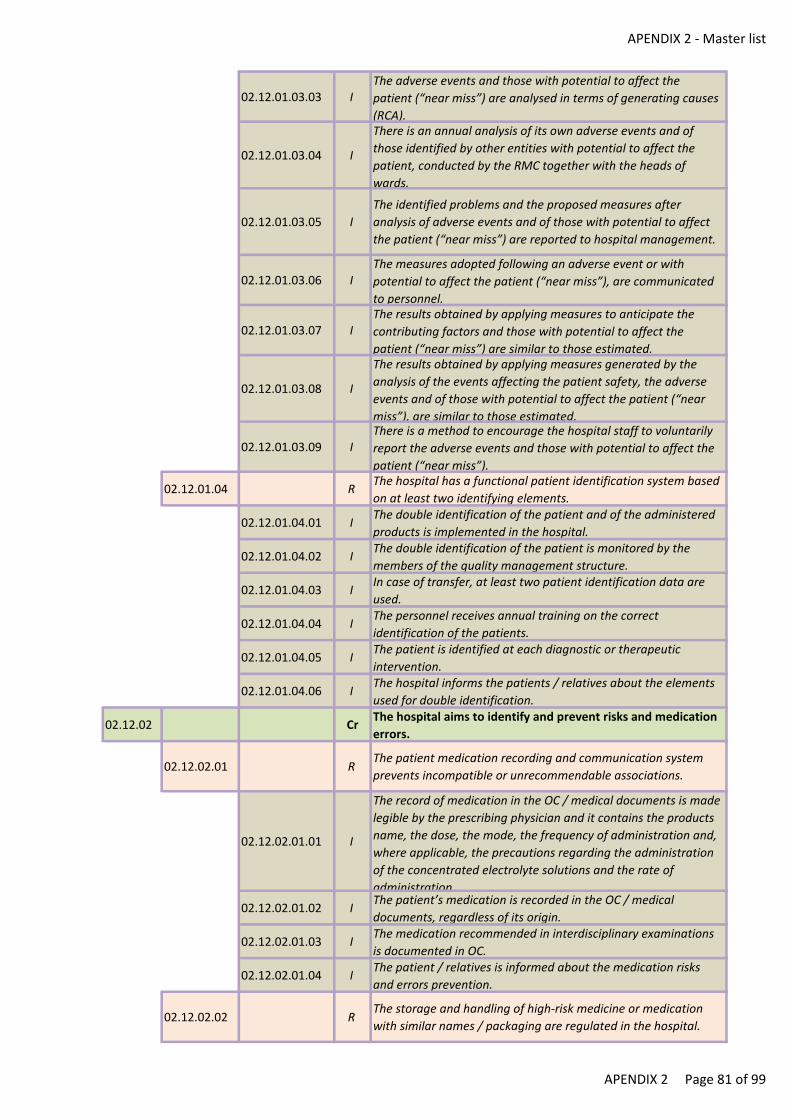
APENDIX 2 - Master list
02.12.01.03.03 IThe adverse events and those with potential to affect the
patient (“near miss”) are analysed in terms of generating causes
(RCA).
02.12.01.03.04 I
There is an annual analysis of its own adverse events and of
those identified by other entities with potential to affect the
patient, conducted by the RMC together with the heads of
wards.
02.12.01.03.05 I
The identified problems and the proposed measures after
analysis of adverse events and of those with potential to affect
the patient (“near miss”) are reported to hospital management.
02.12.01.03.06 IThe measures adopted following an adverse event or with
potential to affect the patient (“near miss”), are communicated
to personnel.
02.12.01.03.07 IThe results obtained by applying measures to anticipate the
contributing factors and those with potential to affect the
patient (“near miss”) are similar to those estimated.
02.12.01.03.08 I
The results obtained by applying measures generated by the
analysis of the events affecting the patient safety, the adverse
events and of those with potential to affect the patient (“near
miss”), are similar to those estimated.
02.12.01.03.09 IThere is a method to encourage the hospital staff to voluntarily
report the adverse events and those with potential to affect the
patient (“near miss”).
02.12.01.04 RThe hospital has a functional patient identification system based
on at least two identifying elements.
02.12.01.04.01 IThe double identification of the patient and of the administered
products is implemented in the hospital.
02.12.01.04.02 IThe double identification of the patient is monitored by the
members of the quality management structure.
02.12.01.04.03 IIn case of transfer, at least two patient identification data are
used.
02.12.01.04.04 IThe personnel receives annual training on the correct
identification of the patients.
02.12.01.04.05 IThe patient is identified at each diagnostic or therapeutic
intervention.
02.12.01.04.06 IThe hospital informs the patients / relatives about the elements
used for double identification.
02.12.02 CrThe hospital aims to identify and prevent risks and medication
errors.
02.12.02.01 RThe patient medication recording and communication system
prevents incompatible or unrecommendable associations.
02.12.02.01.01 I
The record of medication in the OC / medical documents is made
legible by the prescribing physician and it contains the products
name, the dose, the mode, the frequency of administration and,
where applicable, the precautions regarding the administration
of the concentrated electrolyte solutions and the rate of
administration.
02.12.02.01.02 IThe patient’s medication is recorded in the OC / medical
documents, regardless of its origin.
02.12.02.01.03 IThe medication recommended in interdisciplinary examinations
is documented in OC.
02.12.02.01.04 IThe patient / relatives is informed about the medication risks
and errors prevention.
02.12.02.02 RThe storage and handling of high-risk medicine or medication
with similar names / packaging are regulated in the hospital.
APENDIX 2 Page 81 of 99
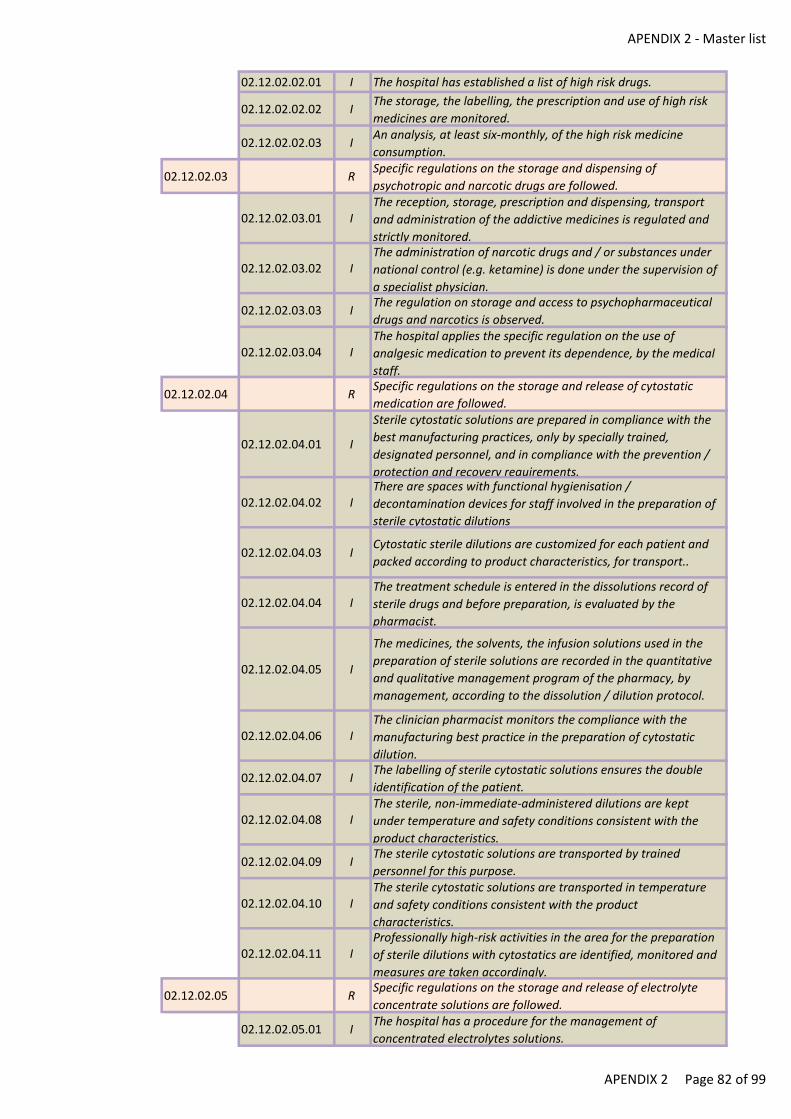
APENDIX 2 - Master list
02.12.02.02.01 I The hospital has established a list of high risk drugs.
02.12.02.02.02 IThe storage, the labelling, the prescription and use of high risk
medicines are monitored.
02.12.02.02.03 IAn analysis, at least six-monthly, of the high risk medicine
consumption.
02.12.02.03 RSpecific regulations on the storage and dispensing of
psychotropic and narcotic drugs are followed.
02.12.02.03.01 IThe reception, storage, prescription and dispensing, transport
and administration of the addictive medicines is regulated and
strictly monitored.
02.12.02.03.02 IThe administration of narcotic drugs and / or substances under
national control (e.g. ketamine) is done under the supervision of
a specialist physician.
02.12.02.03.03 IThe regulation on storage and access to psychopharmaceutical
drugs and narcotics is observed.
02.12.02.03.04 IThe hospital applies the specific regulation on the use of
analgesic medication to prevent its dependence, by the medical
staff.
02.12.02.04 RSpecific regulations on the storage and release of cytostatic
medication are followed.
02.12.02.04.01 I
Sterile cytostatic solutions are prepared in compliance with the
best manufacturing practices, only by specially trained,
designated personnel, and in compliance with the prevention /
protection and recovery requirements.
02.12.02.04.02 IThere are spaces with functional hygienisation /
decontamination devices for staff involved in the preparation of
sterile cytostatic dilutions
02.12.02.04.03 ICytostatic sterile dilutions are customized for each patient and
packed according to product characteristics, for transport..
02.12.02.04.04 IThe treatment schedule is entered in the dissolutions record of
sterile drugs and before preparation, is evaluated by the
pharmacist.
02.12.02.04.05 I
The medicines, the solvents, the infusion solutions used in the
preparation of sterile solutions are recorded in the quantitative
and qualitative management program of the pharmacy, by
management, according to the dissolution / dilution protocol.
02.12.02.04.06 IThe clinician pharmacist monitors the compliance with the
manufacturing best practice in the preparation of cytostatic
dilution.
02.12.02.04.07 IThe labelling of sterile cytostatic solutions ensures the double
identification of the patient.
02.12.02.04.08 IThe sterile, non-immediate-administered dilutions are kept
under temperature and safety conditions consistent with the
product characteristics.
02.12.02.04.09 IThe sterile cytostatic solutions are transported by trained
personnel for this purpose.
02.12.02.04.10 IThe sterile cytostatic solutions are transported in temperature
and safety conditions consistent with the product
characteristics.
02.12.02.04.11 IProfessionally high-risk activities in the area for the preparation
of sterile dilutions with cytostatics are identified, monitored and
measures are taken accordingly.
02.12.02.05 RSpecific regulations on the storage and release of electrolyte
concentrate solutions are followed.
02.12.02.05.01 IThe hospital has a procedure for the management of
concentrated electrolytes solutions.
APENDIX 2 Page 82 of 99
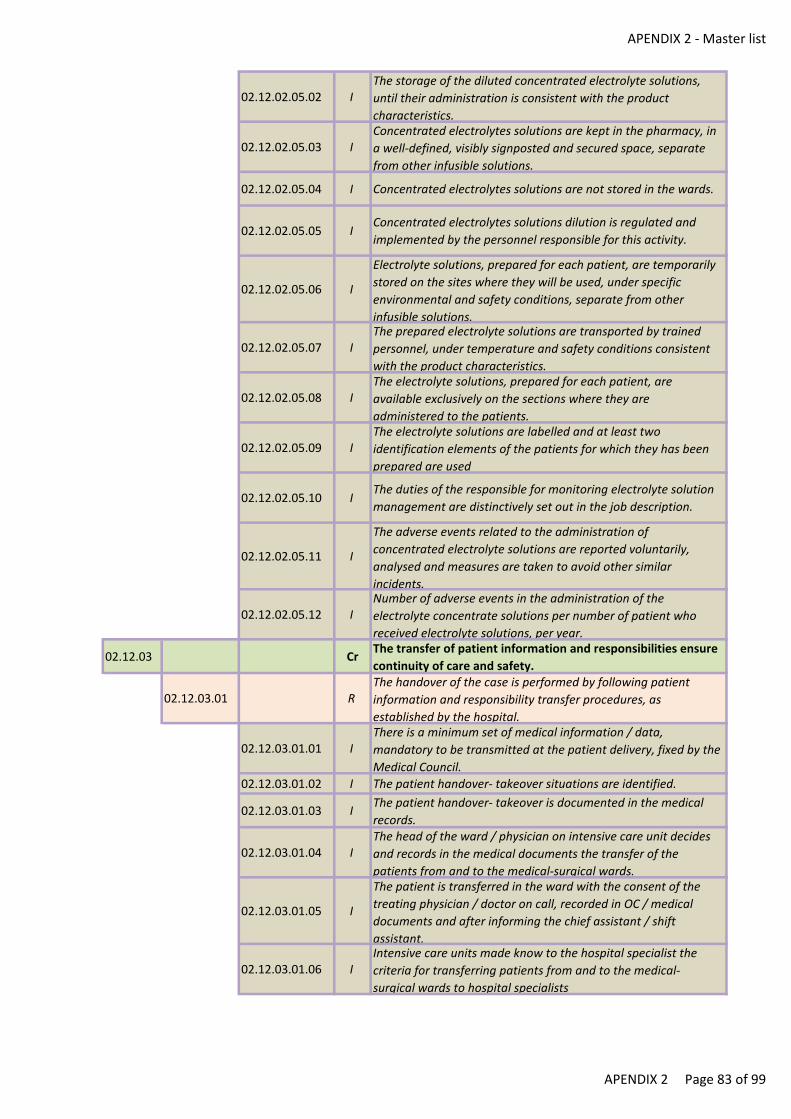
APENDIX 2 - Master list
02.12.02.05.02 IThe storage of the diluted concentrated electrolyte solutions,
until their administration is consistent with the product
characteristics.
02.12.02.05.03 IConcentrated electrolytes solutions are kept in the pharmacy, in
a well-defined, visibly signposted and secured space, separate
from other infusible solutions.
02.12.02.05.04 I Concentrated electrolytes solutions are not stored in the wards.
02.12.02.05.05 IConcentrated electrolytes solutions dilution is regulated and
implemented by the personnel responsible for this activity.
02.12.02.05.06 I
Electrolyte solutions, prepared for each patient, are temporarily
stored on the sites where they will be used, under specific
environmental and safety conditions, separate from other
infusible solutions.
02.12.02.05.07 IThe prepared electrolyte solutions are transported by trained
personnel, under temperature and safety conditions consistent
with the product characteristics.
02.12.02.05.08 IThe electrolyte solutions, prepared for each patient, are
available exclusively on the sections where they are
administered to the patients.
02.12.02.05.09 IThe electrolyte solutions are labelled and at least two
identification elements of the patients for which they has been
prepared are used
02.12.02.05.10 IThe duties of the responsible for monitoring electrolyte solution
management are distinctively set out in the job description.
02.12.02.05.11 I
The adverse events related to the administration of
concentrated electrolyte solutions are reported voluntarily,
analysed and measures are taken to avoid other similar
incidents.
02.12.02.05.12 INumber of adverse events in the administration of the
electrolyte concentrate solutions per number of patient who
received electrolyte solutions, per year.
02.12.03 CrThe transfer of patient information and responsibilities ensure
continuity of care and safety.
02.12.03.01 RThe handover of the case is performed by following patient
information and responsibility transfer procedures, as
established by the hospital.
02.12.03.01.01 IThere is a minimum set of medical information / data,
mandatory to be transmitted at the patient delivery, fixed by the
Medical Council.
02.12.03.01.02 I The patient handover- takeover situations are identified.
02.12.03.01.03 IThe patient handover- takeover is documented in the medical
records.
02.12.03.01.04 IThe head of the ward / physician on intensive care unit decides
and records in the medical documents the transfer of the
patients from and to the medical-surgical wards.
02.12.03.01.05 I
The patient is transferred in the ward with the consent of the
treating physician / doctor on call, recorded in OC / medical
documents and after informing the chief assistant / shift
assistant.
02.12.03.01.06 IIntensive care units made know to the hospital specialist the
criteria for transferring patients from and to the medical-
surgical wards to hospital specialists
APENDIX 2 Page 83 of 99
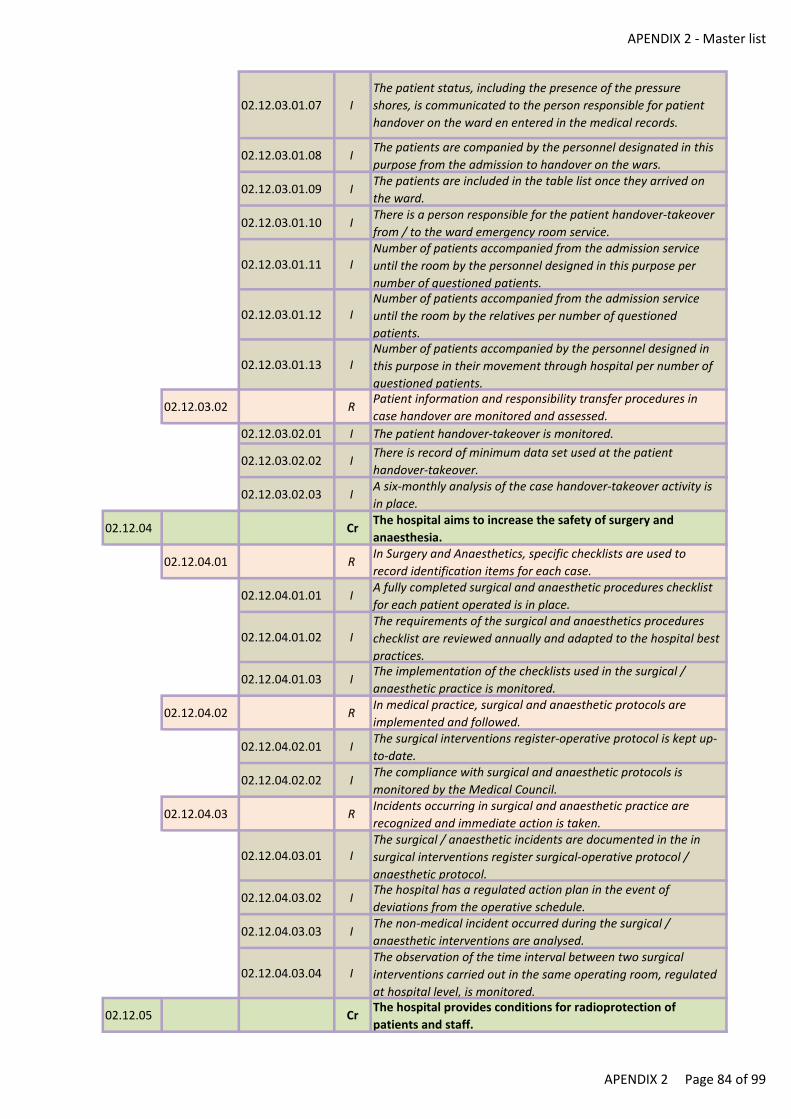
APENDIX 2 - Master list
02.12.03.01.07 I
The patient status, including the presence of the pressure
shores, is communicated to the person responsible for patient
handover on the ward en entered in the medical records.
02.12.03.01.08 IThe patients are companied by the personnel designated in this
purpose from the admission to handover on the wars.
02.12.03.01.09 IThe patients are included in the table list once they arrived on
the ward.
02.12.03.01.10 IThere is a person responsible for the patient handover-takeover
from / to the ward emergency room service.
02.12.03.01.11 INumber of patients accompanied from the admission service
until the room by the personnel designed in this purpose per
number of questioned patients.
02.12.03.01.12 INumber of patients accompanied from the admission service
until the room by the relatives per number of questioned
patients.
02.12.03.01.13 INumber of patients accompanied by the personnel designed in
this purpose in their movement through hospital per number of
questioned patients.
02.12.03.02 RPatient information and responsibility transfer procedures in
case handover are monitored and assessed.
02.12.03.02.01 I The patient handover-takeover is monitored.
02.12.03.02.02 IThere is record of minimum data set used at the patient
handover-takeover.
02.12.03.02.03 IA six-monthly analysis of the case handover-takeover activity is
in place.
02.12.04 CrThe hospital aims to increase the safety of surgery and
anaesthesia.
02.12.04.01 RIn Surgery and Anaesthetics, specific checklists are used to
record identification items for each case.
02.12.04.01.01 IA fully completed surgical and anaesthetic procedures checklist
for each patient operated is in place.
02.12.04.01.02 IThe requirements of the surgical and anaesthetics procedures
checklist are reviewed annually and adapted to the hospital best
practices.
02.12.04.01.03 IThe implementation of the checklists used in the surgical /
anaesthetic practice is monitored.
02.12.04.02 RIn medical practice, surgical and anaesthetic protocols are
implemented and followed.
02.12.04.02.01 IThe surgical interventions register-operative protocol is kept up-
to-date.
02.12.04.02.02 IThe compliance with surgical and anaesthetic protocols is
monitored by the Medical Council.
02.12.04.03 RIncidents occurring in surgical and anaesthetic practice are
recognized and immediate action is taken.
02.12.04.03.01 IThe surgical / anaesthetic incidents are documented in the in
surgical interventions register surgical-operative protocol /
anaesthetic protocol.
02.12.04.03.02 IThe hospital has a regulated action plan in the event of
deviations from the operative schedule.
02.12.04.03.03 IThe non-medical incident occurred during the surgical /
anaesthetic interventions are analysed.
02.12.04.03.04 IThe observation of the time interval between two surgical
interventions carried out in the same operating room, regulated
at hospital level, is monitored.
02.12.05 CrThe hospital provides conditions for radioprotection of
patients and staff.
APENDIX 2 Page 84 of 99
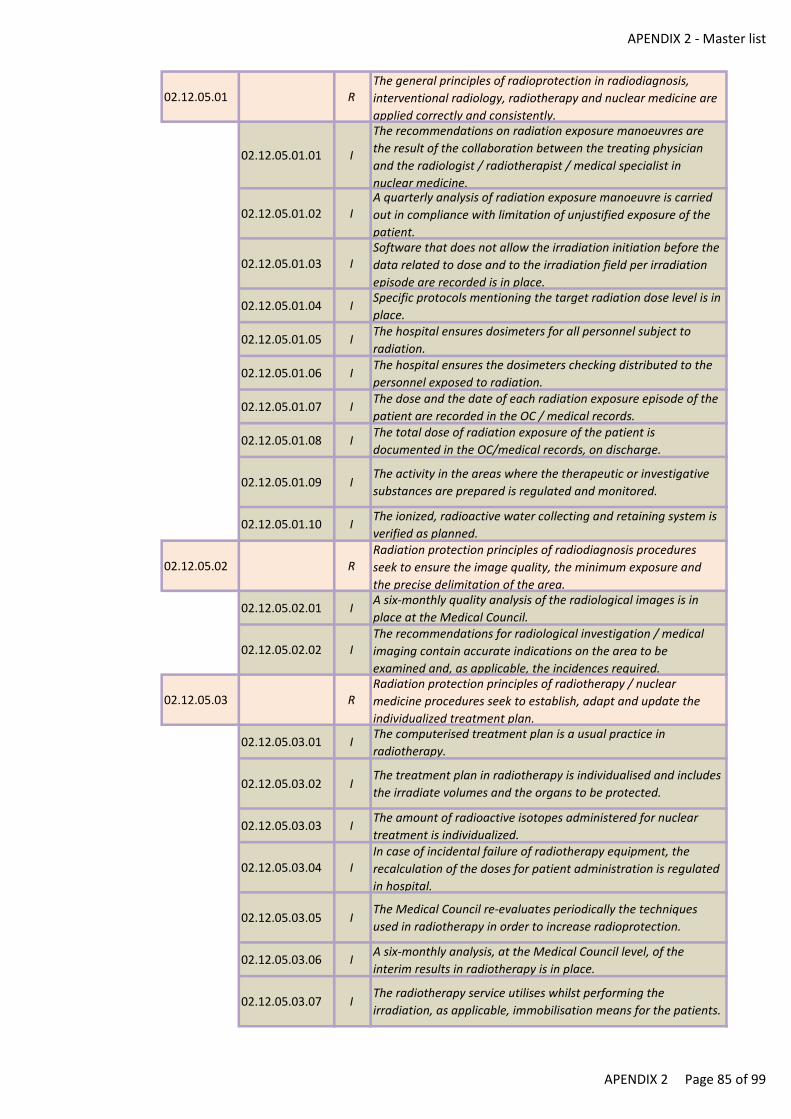
APENDIX 2 - Master list
02.12.05.01 RThe general principles of radioprotection in radiodiagnosis,
interventional radiology, radiotherapy and nuclear medicine are
applied correctly and consistently.
02.12.05.01.01 I
The recommendations on radiation exposure manoeuvres are
the result of the collaboration between the treating physician
and the radiologist / radiotherapist / medical specialist in
nuclear medicine.
02.12.05.01.02 IA quarterly analysis of radiation exposure manoeuvre is carried
out in compliance with limitation of unjustified exposure of the
patient.
02.12.05.01.03 ISoftware that does not allow the irradiation initiation before the
data related to dose and to the irradiation field per irradiation
episode are recorded is in place.
02.12.05.01.04 ISpecific protocols mentioning the target radiation dose level is in
place.
02.12.05.01.05 IThe hospital ensures dosimeters for all personnel subject to
radiation.
02.12.05.01.06 IThe hospital ensures the dosimeters checking distributed to the
personnel exposed to radiation.
02.12.05.01.07 IThe dose and the date of each radiation exposure episode of the
patient are recorded in the OC / medical records.
02.12.05.01.08 IThe total dose of radiation exposure of the patient is
documented in the OC/medical records, on discharge.
02.12.05.01.09 IThe activity in the areas where the therapeutic or investigative
substances are prepared is regulated and monitored.
02.12.05.01.10 IThe ionized, radioactive water collecting and retaining system is
verified as planned.
02.12.05.02 RRadiation protection principles of radiodiagnosis procedures
seek to ensure the image quality, the minimum exposure and
the precise delimitation of the area.
02.12.05.02.01 IA six-monthly quality analysis of the radiological images is in
place at the Medical Council.
02.12.05.02.02 IThe recommendations for radiological investigation / medical
imaging contain accurate indications on the area to be
examined and, as applicable, the incidences required.
02.12.05.03 RRadiation protection principles of radiotherapy / nuclear
medicine procedures seek to establish, adapt and update the
individualized treatment plan.
02.12.05.03.01 IThe computerised treatment plan is a usual practice in
radiotherapy.
02.12.05.03.02 IThe treatment plan in radiotherapy is individualised and includes
the irradiate volumes and the organs to be protected.
02.12.05.03.03 IThe amount of radioactive isotopes administered for nuclear
treatment is individualized.
02.12.05.03.04 IIn case of incidental failure of radiotherapy equipment, the
recalculation of the doses for patient administration is regulated
in hospital.
02.12.05.03.05 IThe Medical Council re-evaluates periodically the techniques
used in radiotherapy in order to increase radioprotection.
02.12.05.03.06 IA six-monthly analysis, at the Medical Council level, of the
interim results in radiotherapy is in place.
02.12.05.03.07 IThe radiotherapy service utilises whilst performing the
irradiation, as applicable, immobilisation means for the patients.
APENDIX 2 Page 85 of 99
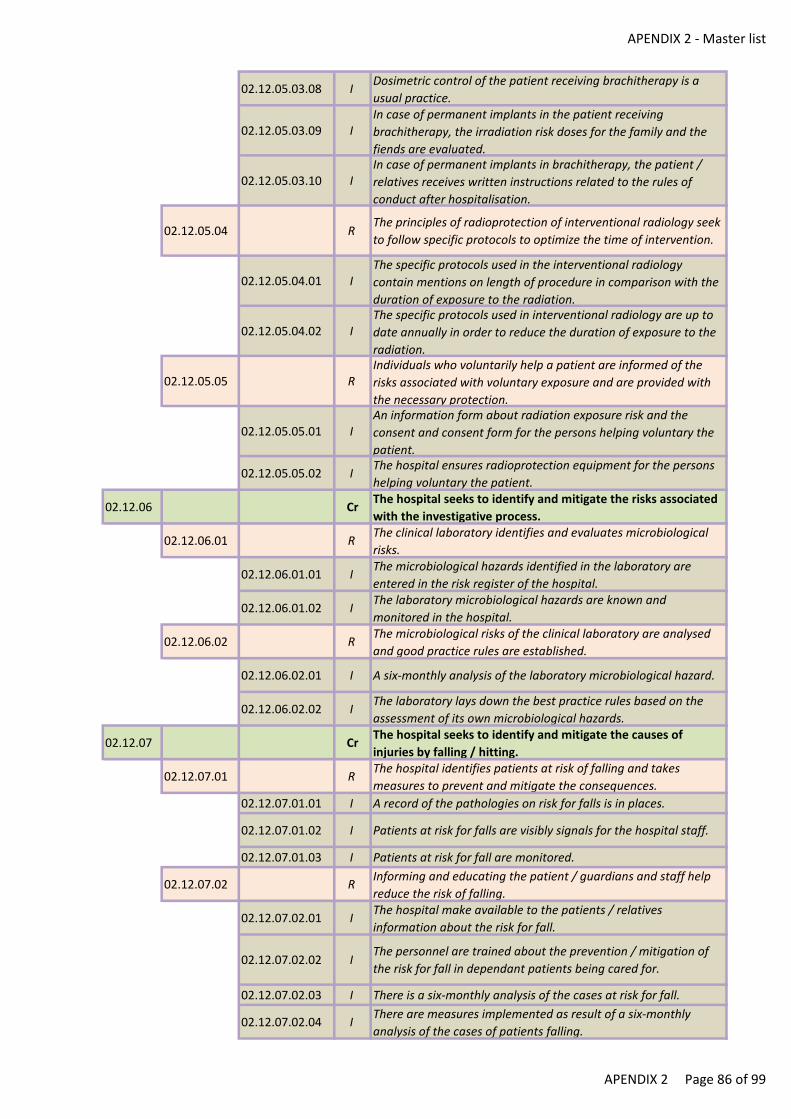
APENDIX 2 - Master list
02.12.05.03.08 IDosimetric control of the patient receiving brachitherapy is a
usual practice.
02.12.05.03.09 IIn case of permanent implants in the patient receiving
brachitherapy, the irradiation risk doses for the family and the
fiends are evaluated.
02.12.05.03.10 IIn case of permanent implants in brachitherapy, the patient /
relatives receives written instructions related to the rules of
conduct after hospitalisation.
02.12.05.04 RThe principles of radioprotection of interventional radiology seek
to follow specific protocols to optimize the time of intervention.
02.12.05.04.01 IThe specific protocols used in the interventional radiology
contain mentions on length of procedure in comparison with the
duration of exposure to the radiation.
02.12.05.04.02 IThe specific protocols used in interventional radiology are up to
date annually in order to reduce the duration of exposure to the
radiation.
02.12.05.05 RIndividuals who voluntarily help a patient are informed of the
risks associated with voluntary exposure and are provided with
the necessary protection.
02.12.05.05.01 IAn information form about radiation exposure risk and the
consent and consent form for the persons helping voluntary the
patient.
02.12.05.05.02 IThe hospital ensures radioprotection equipment for the persons
helping voluntary the patient.
02.12.06 CrThe hospital seeks to identify and mitigate the risks associated
with the investigative process.
02.12.06.01 RThe clinical laboratory identifies and evaluates microbiological
risks.
02.12.06.01.01 IThe microbiological hazards identified in the laboratory are
entered in the risk register of the hospital.
02.12.06.01.02 IThe laboratory microbiological hazards are known and
monitored in the hospital.
02.12.06.02 RThe microbiological risks of the clinical laboratory are analysed
and good practice rules are established.
02.12.06.02.01 I A six-monthly analysis of the laboratory microbiological hazard.
02.12.06.02.02 IThe laboratory lays down the best practice rules based on the
assessment of its own microbiological hazards.
02.12.07 CrThe hospital seeks to identify and mitigate the causes of
injuries by falling / hitting.
02.12.07.01 RThe hospital identifies patients at risk of falling and takes
measures to prevent and mitigate the consequences.
02.12.07.01.01 I A record of the pathologies on risk for falls is in places.
02.12.07.01.02 I Patients at risk for falls are visibly signals for the hospital staff.
02.12.07.01.03 I Patients at risk for fall are monitored.
02.12.07.02 RInforming and educating the patient / guardians and staff help
reduce the risk of falling.
02.12.07.02.01 IThe hospital make available to the patients / relatives
information about the risk for fall.
02.12.07.02.02 IThe personnel are trained about the prevention / mitigation of
the risk for fall in dependant patients being cared for.
02.12.07.02.03 I There is a six-monthly analysis of the cases at risk for fall.
02.12.07.02.04 IThere are measures implemented as result of a six-monthly
analysis of the cases of patients falling.
APENDIX 2 Page 86 of 99
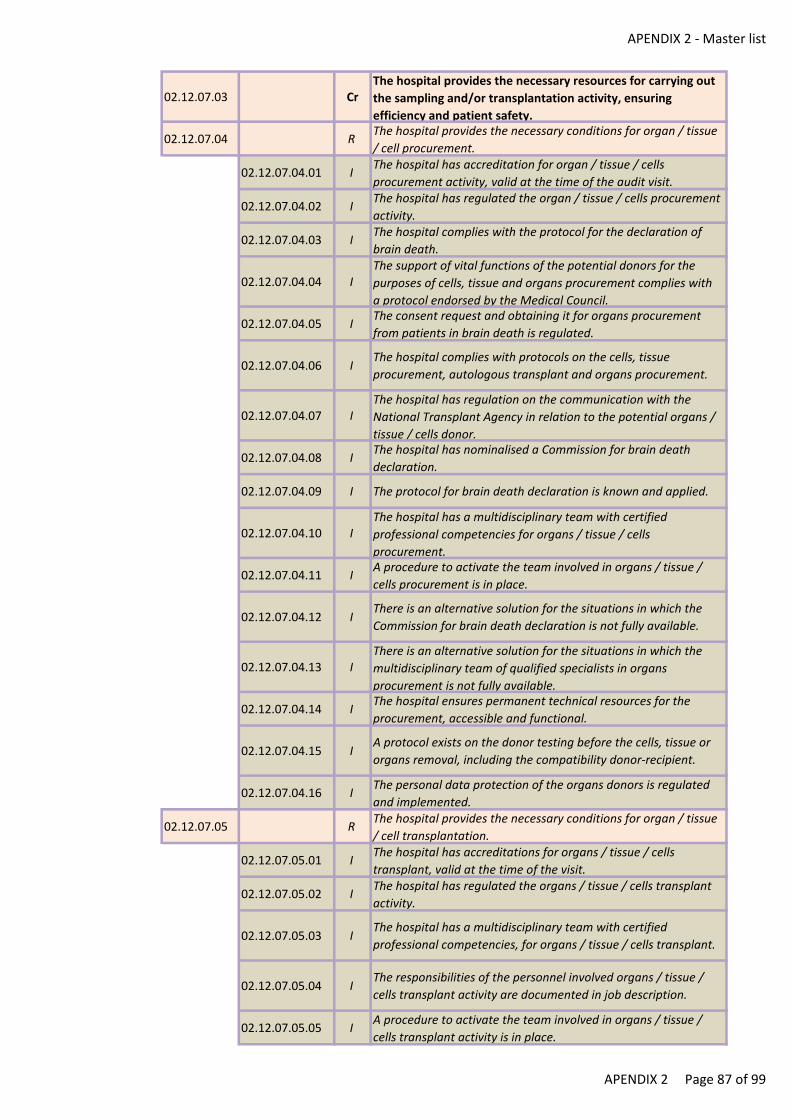
APENDIX 2 - Master list
02.12.07.03 CrThe hospital provides the necessary resources for carrying out
the sampling and/or transplantation activity, ensuring
efficiency and patient safety.
02.12.07.04 RThe hospital provides the necessary conditions for organ / tissue
/ cell procurement.
02.12.07.04.01 IThe hospital has accreditation for organ / tissue / cells
procurement activity, valid at the time of the audit visit.
02.12.07.04.02 IThe hospital has regulated the organ / tissue / cells procurement
activity.
02.12.07.04.03 IThe hospital complies with the protocol for the declaration of
brain death.
02.12.07.04.04 IThe support of vital functions of the potential donors for the
purposes of cells, tissue and organs procurement complies with
a protocol endorsed by the Medical Council.
02.12.07.04.05 IThe consent request and obtaining it for organs procurement
from patients in brain death is regulated.
02.12.07.04.06 IThe hospital complies with protocols on the cells, tissue
procurement, autologous transplant and organs procurement.
02.12.07.04.07 IThe hospital has regulation on the communication with the
National Transplant Agency in relation to the potential organs /
tissue / cells donor.
02.12.07.04.08 IThe hospital has nominalised a Commission for brain death
declaration.
02.12.07.04.09 I The protocol for brain death declaration is known and applied.
02.12.07.04.10 IThe hospital has a multidisciplinary team with certified
professional competencies for organs / tissue / cells
procurement.
02.12.07.04.11 IA procedure to activate the team involved in organs / tissue /
cells procurement is in place.
02.12.07.04.12 IThere is an alternative solution for the situations in which the
Commission for brain death declaration is not fully available.
02.12.07.04.13 IThere is an alternative solution for the situations in which the
multidisciplinary team of qualified specialists in organs
procurement is not fully available.
02.12.07.04.14 IThe hospital ensures permanent technical resources for the
procurement, accessible and functional.
02.12.07.04.15 IA protocol exists on the donor testing before the cells, tissue or
organs removal, including the compatibility donor-recipient.
02.12.07.04.16 IThe personal data protection of the organs donors is regulated
and implemented.
02.12.07.05 RThe hospital provides the necessary conditions for organ / tissue
/ cell transplantation.
02.12.07.05.01 IThe hospital has accreditations for organs / tissue / cells
transplant, valid at the time of the visit.
02.12.07.05.02 IThe hospital has regulated the organs / tissue / cells transplant
activity.
02.12.07.05.03 IThe hospital has a multidisciplinary team with certified
professional competencies, for organs / tissue / cells transplant.
02.12.07.05.04 IThe responsibilities of the personnel involved organs / tissue /
cells transplant activity are documented in job description.
02.12.07.05.05 IA procedure to activate the team involved in organs / tissue /
cells transplant activity is in place.
APENDIX 2 Page 87 of 99

APENDIX 2 - Master list
02.12.07.05.06 IThere is an alternative solution for the situations in which the
multidisciplinary team of qualified specialists in organs / tissue /
cells transplant is not fully available.
02.12.07.06 RThe hospital organizes procurement / transplantation in
accordance with the regulations of the National Transplant
Agency.
02.12.07.06.01 IThe hospital has established indicators for monitoring the
organs / tissue / cell procurement / transplant activity.
02.12.07.06.02 IA database of the current status of all patients transplanted in
the hospital is in place.
02.12.07.06.03 IThere is an annual analysis of the survival rate of all patients
transplanted in the hospital, by pathology.
02.12.07.06.04 INumber of transplanted patients deceased before discharge per
total number of transplanted patients per year.
02.12.07.06.05 INumber of transplant patients deceased after discharge per
total number of transplant patients per year.
02.13 SThe hospital has implemented good transfusion and
haemovigilance practices.
02.13.01 CrThe hospital has organized the prescribing and monitoring of
transfusion and haemovigilance therapy.
02.13.01.02 R The hospital fulfils the conditions for safe transfusion therapy.
02.13.01.02.01 I The hospital has an authorised blood transfusion unit.
02.13.01.02.02 IAn annual continuing plan exists for the training of healthcare
professional in transfusion operations.
02.13.01.02.03 IA record exists of critical item of the blood transfusion unit,
including technical specifications thereof.
02.13.01.02.04 IThe critical items stock of the blood transfusion unit is provided
in accordance with the regulation.
02.13.01.02.05 IRecords exist of the critical equipment of the blood transfusion
unit, including technical specifications thereof.
02.13.01.02.06 I Qualification plans exist for critical equipment.
02.13.01.02.07 I Qualification reports exist for critical equipment.
02.13.01.02.08 IValidation reports exist for the procedures applied in the use of
critical equipment.
02.13.01.02.09 IPlans exist for the verification, calibration, maintenance and
requalification of the critical equipment in the blood transfusion
unit.
02.13.01.02.10 I
The verification, the calibration, the maintenance and the
requalification of the critical equipment in the blood transfusion
unit are carried out according to the schedules and documented
in dedicated records.
02.13.01.02.11 I
The hospital has regulated the qualification, maintenance,
calibration and validation of procedures, the repair and
requalification of critical equipment in the blood transfusion
unit.
02.13.01.02.12 I
In the blood transfusion unit, the refrigerators, the freezers, the
platelet agitators have a visual and auditory alarm system,
alternative emergency power system (electric generator) and
automatic temperature monitoring system.
02.13.01.02.13 IThe hospital has an emergency plan to ensure the continuity of
the blood transfusion unit, in the event of personnel, equipment
failure and of other critical items.
APENDIX 2 Page 88 of 99
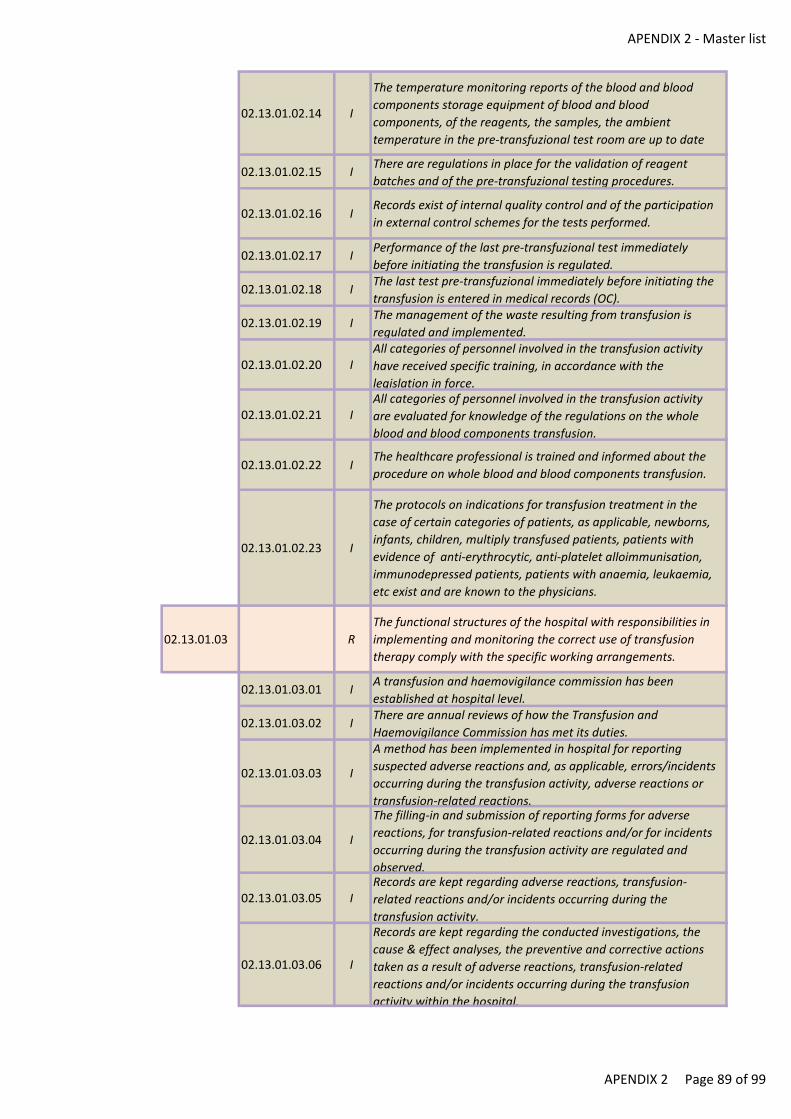
APENDIX 2 - Master list
02.13.01.02.14 I
The temperature monitoring reports of the blood and blood
components storage equipment of blood and blood
components, of the reagents, the samples, the ambient
temperature in the pre-transfuzional test room are up to date
02.13.01.02.15 IThere are regulations in place for the validation of reagent
batches and of the pre-transfuzional testing procedures.
02.13.01.02.16 IRecords exist of internal quality control and of the participation
in external control schemes for the tests performed.
02.13.01.02.17 IPerformance of the last pre-transfuzional test immediately
before initiating the transfusion is regulated.
02.13.01.02.18 IThe last test pre-transfuzional immediately before initiating the
transfusion is entered in medical records (OC).
02.13.01.02.19 IThe management of the waste resulting from transfusion is
regulated and implemented.
02.13.01.02.20 IAll categories of personnel involved in the transfusion activity
have received specific training, in accordance with the
legislation in force.
02.13.01.02.21 IAll categories of personnel involved in the transfusion activity
are evaluated for knowledge of the regulations on the whole
blood and blood components transfusion.
02.13.01.02.22 IThe healthcare professional is trained and informed about the
procedure on whole blood and blood components transfusion.
02.13.01.02.23 I
The protocols on indications for transfusion treatment in the
case of certain categories of patients, as applicable, newborns,
infants, children, multiply transfused patients, patients with
evidence of anti-erythrocytic, anti-platelet alloimmunisation,
immunodepressed patients, patients with anaemia, leukaemia,
etc exist and are known to the physicians.
02.13.01.03 R
The functional structures of the hospital with responsibilities in
implementing and monitoring the correct use of transfusion
therapy comply with the specific working arrangements.
02.13.01.03.01 IA transfusion and haemovigilance commission has been
established at hospital level.
02.13.01.03.02 IThere are annual reviews of how the Transfusion and
Haemovigilance Commission has met its duties.
02.13.01.03.03 I
A method has been implemented in hospital for reporting
suspected adverse reactions and, as applicable, errors/incidents
occurring during the transfusion activity, adverse reactions or
transfusion-related reactions.
02.13.01.03.04 I
The filling-in and submission of reporting forms for adverse
reactions, for transfusion-related reactions and/or for incidents
occurring during the transfusion activity are regulated and
observed.
02.13.01.03.05 IRecords are kept regarding adverse reactions, transfusion-
related reactions and/or incidents occurring during the
transfusion activity.
02.13.01.03.06 I
Records are kept regarding the conducted investigations, the
cause & effect analyses, the preventive and corrective actions
taken as a result of adverse reactions, transfusion-related
reactions and/or incidents occurring during the transfusion
activity within the hospital.
APENDIX 2 Page 89 of 99
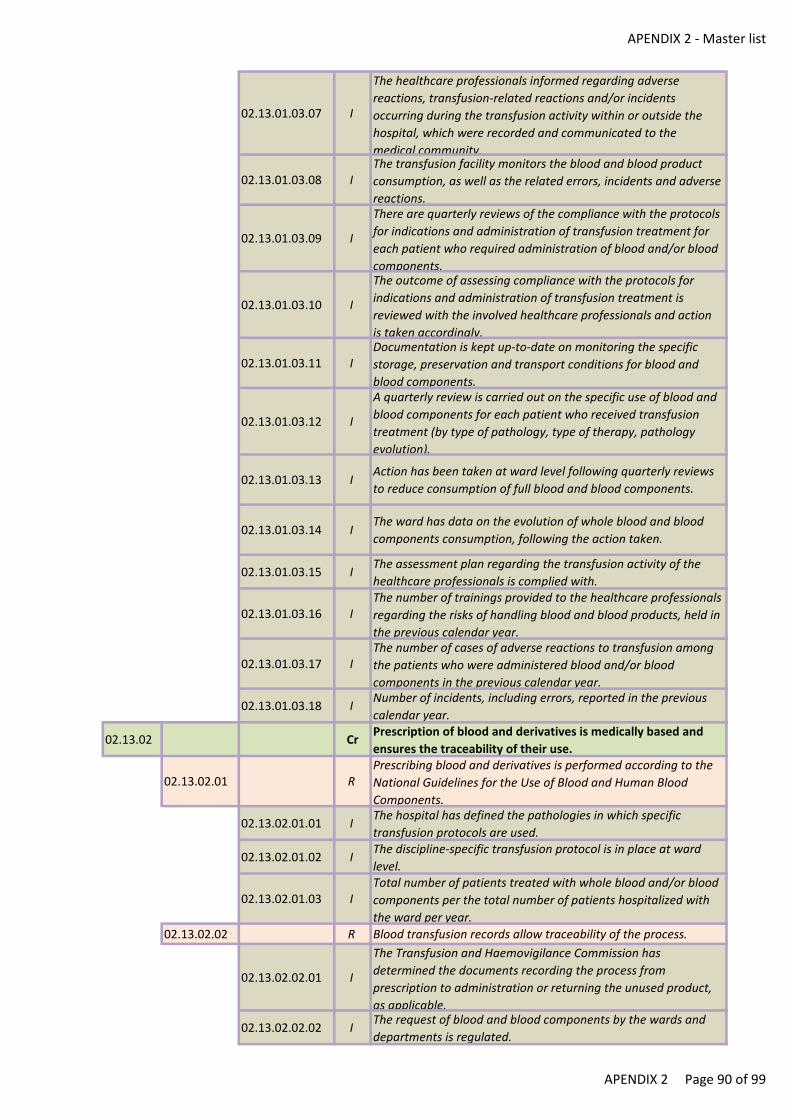
APENDIX 2 - Master list
02.13.01.03.07 I
The healthcare professionals informed regarding adverse
reactions, transfusion-related reactions and/or incidents
occurring during the transfusion activity within or outside the
hospital, which were recorded and communicated to the
medical community.
02.13.01.03.08 IThe transfusion facility monitors the blood and blood product
consumption, as well as the related errors, incidents and adverse
reactions.
02.13.01.03.09 I
There are quarterly reviews of the compliance with the protocols
for indications and administration of transfusion treatment for
each patient who required administration of blood and/or blood
components.
02.13.01.03.10 I
The outcome of assessing compliance with the protocols for
indications and administration of transfusion treatment is
reviewed with the involved healthcare professionals and action
is taken accordingly.
02.13.01.03.11 IDocumentation is kept up-to-date on monitoring the specific
storage, preservation and transport conditions for blood and
blood components.
02.13.01.03.12 I
A quarterly review is carried out on the specific use of blood and
blood components for each patient who received transfusion
treatment (by type of pathology, type of therapy, pathology
evolution).
02.13.01.03.13 IAction has been taken at ward level following quarterly reviews
to reduce consumption of full blood and blood components.
02.13.01.03.14 IThe ward has data on the evolution of whole blood and blood
components consumption, following the action taken.
02.13.01.03.15 IThe assessment plan regarding the transfusion activity of the
healthcare professionals is complied with.
02.13.01.03.16 IThe number of trainings provided to the healthcare professionals
regarding the risks of handling blood and blood products, held in
the previous calendar year.
02.13.01.03.17 IThe number of cases of adverse reactions to transfusion among
the patients who were administered blood and/or blood
components in the previous calendar year.
02.13.01.03.18 INumber of incidents, including errors, reported in the previous
calendar year.
02.13.02 CrPrescription of blood and derivatives is medically based and
ensures the traceability of their use.
02.13.02.01 RPrescribing blood and derivatives is performed according to the
National Guidelines for the Use of Blood and Human Blood
Components.
02.13.02.01.01 IThe hospital has defined the pathologies in which specific
transfusion protocols are used.
02.13.02.01.02 IThe discipline-specific transfusion protocol is in place at ward
level.
02.13.02.01.03 ITotal number of patients treated with whole blood and/or blood
components per the total number of patients hospitalized with
the ward per year.
02.13.02.02 R Blood transfusion records allow traceability of the process.
02.13.02.02.01 I
The Transfusion and Haemovigilance Commission has
determined the documents recording the process from
prescription to administration or returning the unused product,
as applicable.
02.13.02.02.02 IThe request of blood and blood components by the wards and
departments is regulated.
APENDIX 2 Page 90 of 99
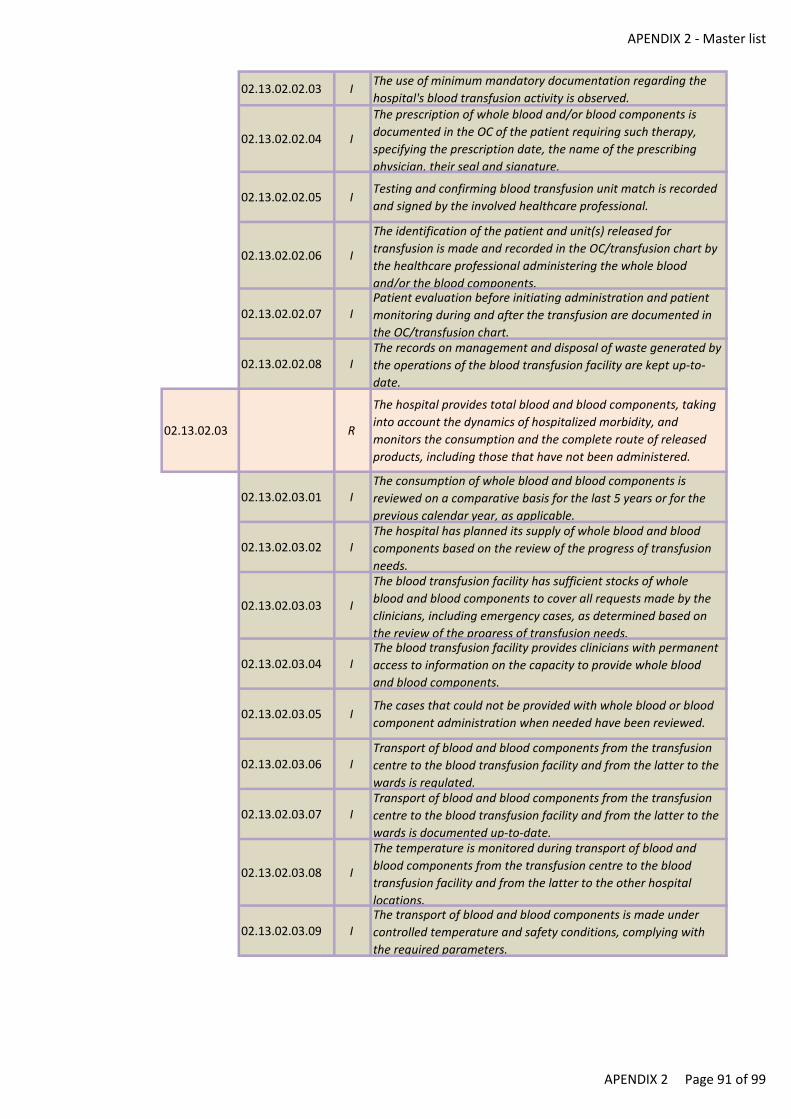
APENDIX 2 - Master list
02.13.02.02.03 IThe use of minimum mandatory documentation regarding the
hospital's blood transfusion activity is observed.
02.13.02.02.04 I
The prescription of whole blood and/or blood components is
documented in the OC of the patient requiring such therapy,
specifying the prescription date, the name of the prescribing
physician, their seal and signature.
02.13.02.02.05 ITesting and confirming blood transfusion unit match is recorded
and signed by the involved healthcare professional.
02.13.02.02.06 I
The identification of the patient and unit(s) released for
transfusion is made and recorded in the OC/transfusion chart by
the healthcare professional administering the whole blood
and/or the blood components.
02.13.02.02.07 IPatient evaluation before initiating administration and patient
monitoring during and after the transfusion are documented in
the OC/transfusion chart.
02.13.02.02.08 IThe records on management and disposal of waste generated by
the operations of the blood transfusion facility are kept up-to-
date.
02.13.02.03 R
The hospital provides total blood and blood components, taking
into account the dynamics of hospitalized morbidity, and
monitors the consumption and the complete route of released
products, including those that have not been administered.
02.13.02.03.01 IThe consumption of whole blood and blood components is
reviewed on a comparative basis for the last 5 years or for the
previous calendar year, as applicable.
02.13.02.03.02 IThe hospital has planned its supply of whole blood and blood
components based on the review of the progress of transfusion
needs.
02.13.02.03.03 I
The blood transfusion facility has sufficient stocks of whole
blood and blood components to cover all requests made by the
clinicians, including emergency cases, as determined based on
the review of the progress of transfusion needs.
02.13.02.03.04 IThe blood transfusion facility provides clinicians with permanent
access to information on the capacity to provide whole blood
and blood components.
02.13.02.03.05 IThe cases that could not be provided with whole blood or blood
component administration when needed have been reviewed.
02.13.02.03.06 ITransport of blood and blood components from the transfusion
centre to the blood transfusion facility and from the latter to the
wards is regulated.
02.13.02.03.07 ITransport of blood and blood components from the transfusion
centre to the blood transfusion facility and from the latter to the
wards is documented up-to-date.
02.13.02.03.08 I
The temperature is monitored during transport of blood and
blood components from the transfusion centre to the blood
transfusion facility and from the latter to the other hospital
locations.
02.13.02.03.09 IThe transport of blood and blood components is made under
controlled temperature and safety conditions, complying with
the required parameters.
APENDIX 2 Page 91 of 99
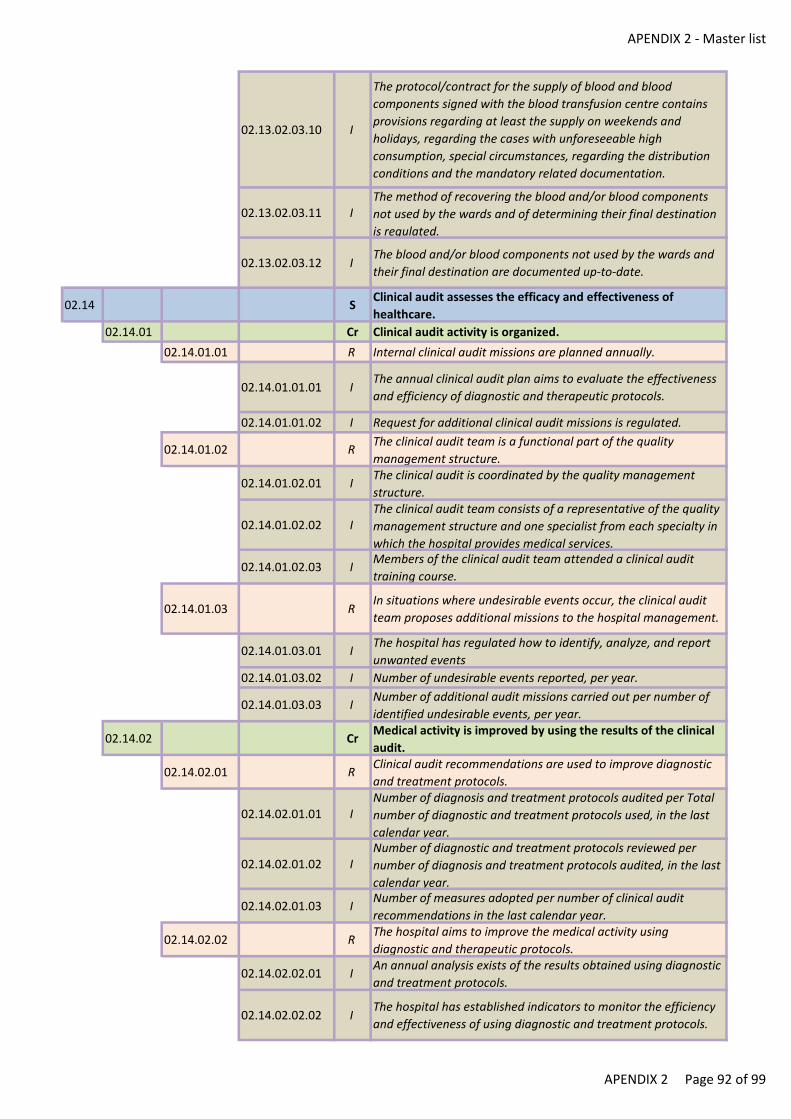
APENDIX 2 - Master list
02.13.02.03.10 I
The protocol/contract for the supply of blood and blood
components signed with the blood transfusion centre contains
provisions regarding at least the supply on weekends and
holidays, regarding the cases with unforeseeable high
consumption, special circumstances, regarding the distribution
conditions and the mandatory related documentation.
02.13.02.03.11 IThe method of recovering the blood and/or blood components
not used by the wards and of determining their final destination
is regulated.
02.13.02.03.12 IThe blood and/or blood components not used by the wards and
their final destination are documented up-to-date.
02.14 SClinical audit assesses the efficacy and effectiveness of
healthcare.
02.14.01 Cr Clinical audit activity is organized.
02.14.01.01 R Internal clinical audit missions are planned annually.
02.14.01.01.01 IThe annual clinical audit plan aims to evaluate the effectiveness
and efficiency of diagnostic and therapeutic protocols.
02.14.01.01.02 I Request for additional clinical audit missions is regulated.
02.14.01.02 RThe clinical audit team is a functional part of the quality
management structure.
02.14.01.02.01 IThe clinical audit is coordinated by the quality management
structure.
02.14.01.02.02 IThe clinical audit team consists of a representative of the quality
management structure and one specialist from each specialty in
which the hospital provides medical services.
02.14.01.02.03 IMembers of the clinical audit team attended a clinical audit
training course.
02.14.01.03 RIn situations where undesirable events occur, the clinical audit
team proposes additional missions to the hospital management.
02.14.01.03.01 IThe hospital has regulated how to identify, analyze, and report
unwanted events
02.14.01.03.02 I Number of undesirable events reported, per year.
02.14.01.03.03 INumber of additional audit missions carried out per number of
identified undesirable events, per year.
02.14.02 CrMedical activity is improved by using the results of the clinical
audit.
02.14.02.01 RClinical audit recommendations are used to improve diagnostic
and treatment protocols.
02.14.02.01.01 INumber of diagnosis and treatment protocols audited per Total
number of diagnostic and treatment protocols used, in the last
calendar year.
02.14.02.01.02 INumber of diagnostic and treatment protocols reviewed per
number of diagnosis and treatment protocols audited, in the last
calendar year.
02.14.02.01.03 INumber of measures adopted per number of clinical audit
recommendations in the last calendar year.
02.14.02.02 RThe hospital aims to improve the medical activity using
diagnostic and therapeutic protocols.
02.14.02.02.01 IAn annual analysis exists of the results obtained using diagnostic
and treatment protocols.
02.14.02.02.02 IThe hospital has established indicators to monitor the efficiency
and effectiveness of using diagnostic and treatment protocols.
APENDIX 2 Page 92 of 99
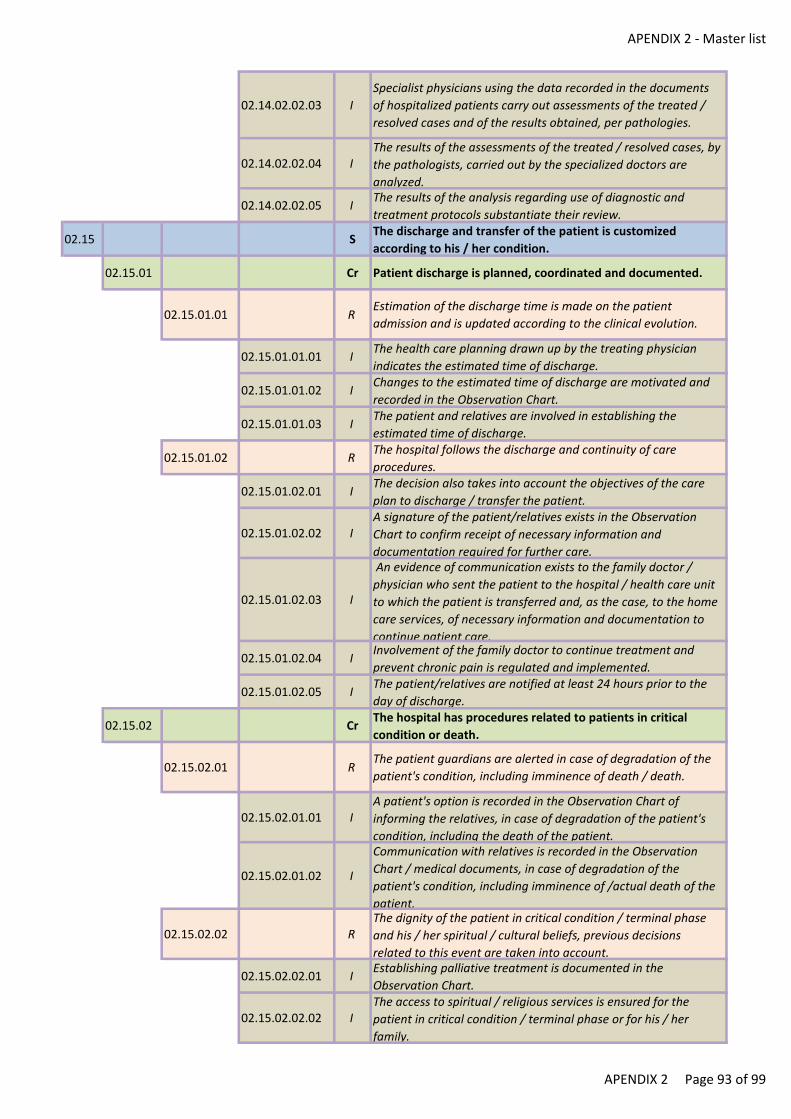
APENDIX 2 - Master list
02.14.02.02.03 I
Specialist physicians using the data recorded in the documents
of hospitalized patients carry out assessments of the treated /
resolved cases and of the results obtained, per pathologies.
02.14.02.02.04 IThe results of the assessments of the treated / resolved cases, by
the pathologists, carried out by the specialized doctors are
analyzed.
02.14.02.02.05 IThe results of the analysis regarding use of diagnostic and
treatment protocols substantiate their review.
02.15 SThe discharge and transfer of the patient is customized
according to his / her condition.
02.15.01 Cr Patient discharge is planned, coordinated and documented.
02.15.01.01 REstimation of the discharge time is made on the patient
admission and is updated according to the clinical evolution.
02.15.01.01.01 IThe health care planning drawn up by the treating physician
indicates the estimated time of discharge.
02.15.01.01.02 IChanges to the estimated time of discharge are motivated and
recorded in the Observation Chart.
02.15.01.01.03 IThe patient and relatives are involved in establishing the
estimated time of discharge.
02.15.01.02 RThe hospital follows the discharge and continuity of care
procedures.
02.15.01.02.01 IThe decision also takes into account the objectives of the care
plan to discharge / transfer the patient.
02.15.01.02.02 IA signature of the patient/relatives exists in the Observation
Chart to confirm receipt of necessary information and
documentation required for further care.
02.15.01.02.03 I
An evidence of communication exists to the family doctor /
physician who sent the patient to the hospital / health care unit
to which the patient is transferred and, as the case, to the home
care services, of necessary information and documentation to
continue patient care.
02.15.01.02.04 IInvolvement of the family doctor to continue treatment and
prevent chronic pain is regulated and implemented.
02.15.01.02.05 IThe patient/relatives are notified at least 24 hours prior to the
day of discharge.
02.15.02 CrThe hospital has procedures related to patients in critical
condition or death.
02.15.02.01 RThe patient guardians are alerted in case of degradation of the
patient's condition, including imminence of death / death.
02.15.02.01.01 IA patient's option is recorded in the Observation Chart of
informing the relatives, in case of degradation of the patient's
condition, including the death of the patient.
02.15.02.01.02 I
Communication with relatives is recorded in the Observation
Chart / medical documents, in case of degradation of the
patient's condition, including imminence of /actual death of the
patient.
02.15.02.02 RThe dignity of the patient in critical condition / terminal phase
and his / her spiritual / cultural beliefs, previous decisions
related to this event are taken into account.
02.15.02.02.01 IEstablishing palliative treatment is documented in the
Observation Chart.
02.15.02.02.02 IThe access to spiritual / religious services is ensured for the
patient in critical condition / terminal phase or for his / her
family.
APENDIX 2 Page 93 of 99
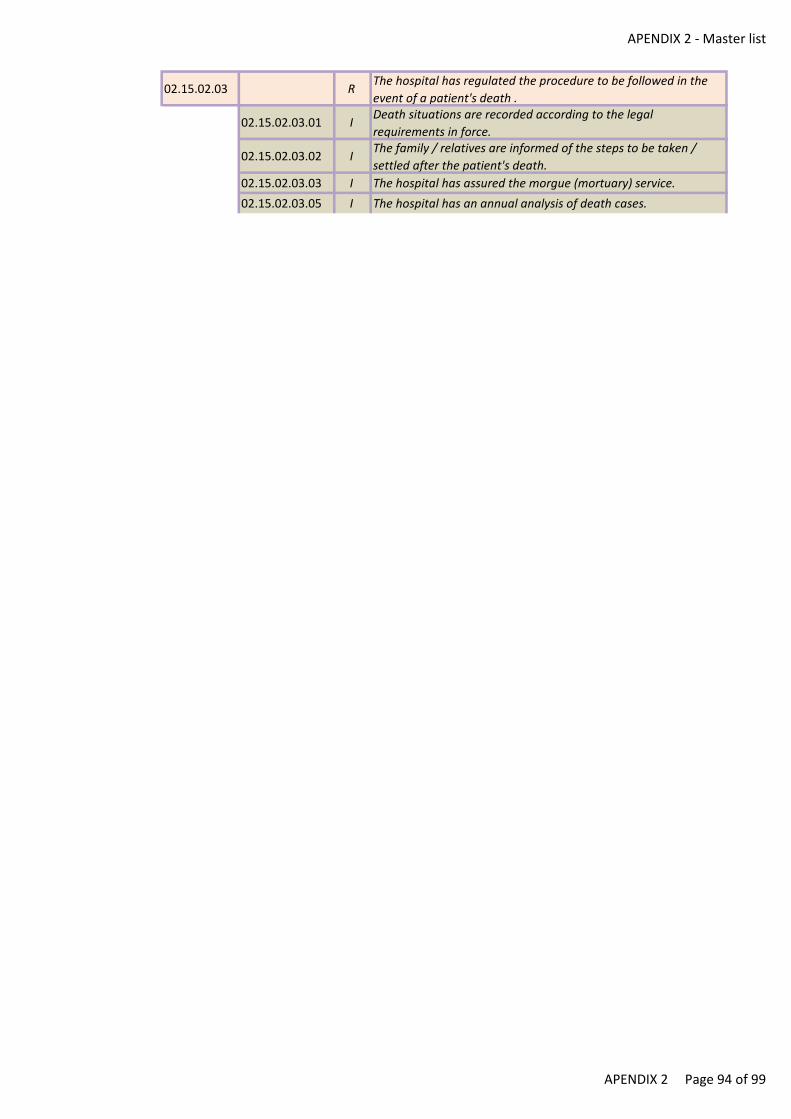
APENDIX 2 - Master list
02.15.02.03 RThe hospital has regulated the procedure to be followed in the
event of a patient's death .
02.15.02.03.01 IDeath situations are recorded according to the legal
requirements in force.
02.15.02.03.02 IThe family / relatives are informed of the steps to be taken /
settled after the patient's death.
02.15.02.03.03 I The hospital has assured the morgue (mortuary) service.
02.15.02.03.05 I The hospital has an annual analysis of death cases.
APENDIX 2 Page 94 of 99
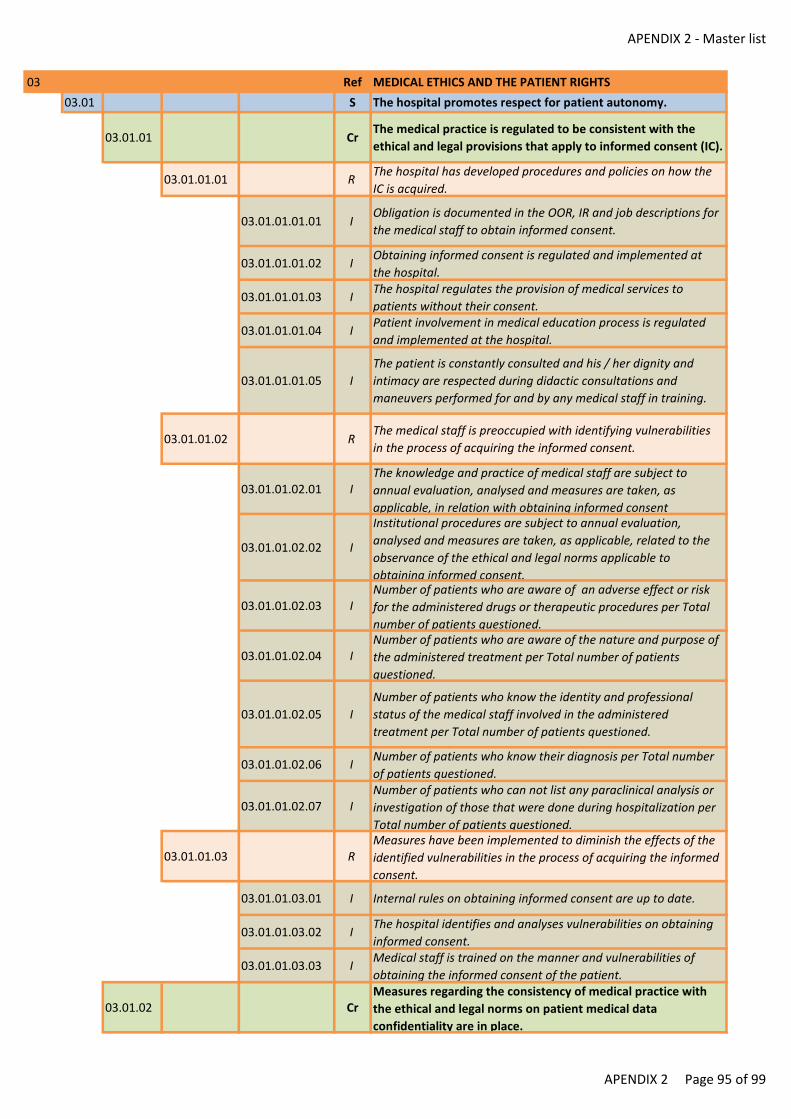
APENDIX 2 - Master list
03 Ref MEDICAL ETHICS AND THE PATIENT RIGHTS
03.01 S The hospital promotes respect for patient autonomy.
03.01.01 CrThe medical practice is regulated to be consistent with the
ethical and legal provisions that apply to informed consent (IC).
03.01.01.01 RThe hospital has developed procedures and policies on how the
IC is acquired.
03.01.01.01.01 IObligation is documented in the OOR, IR and job descriptions for
the medical staff to obtain informed consent.
03.01.01.01.02 IObtaining informed consent is regulated and implemented at
the hospital.
03.01.01.01.03 IThe hospital regulates the provision of medical services to
patients without their consent.
03.01.01.01.04 IPatient involvement in medical education process is regulated
and implemented at the hospital.
03.01.01.01.05 I
The patient is constantly consulted and his / her dignity and
intimacy are respected during didactic consultations and
maneuvers performed for and by any medical staff in training.
03.01.01.02 RThe medical staff is preoccupied with identifying vulnerabilities
in the process of acquiring the informed consent.
03.01.01.02.01 IThe knowledge and practice of medical staff are subject to
annual evaluation, analysed and measures are taken, as
applicable, in relation with obtaining informed consent
03.01.01.02.02 I
Institutional procedures are subject to annual evaluation,
analysed and measures are taken, as applicable, related to the
observance of the ethical and legal norms applicable to
obtaining informed consent.
03.01.01.02.03 INumber of patients who are aware of an adverse effect or risk
for the administered drugs or therapeutic procedures per Total
number of patients questioned.
03.01.01.02.04 INumber of patients who are aware of the nature and purpose of
the administered treatment per Total number of patients
questioned.
03.01.01.02.05 I
Number of patients who know the identity and professional
status of the medical staff involved in the administered
treatment per Total number of patients questioned.
03.01.01.02.06 INumber of patients who know their diagnosis per Total number
of patients questioned.
03.01.01.02.07 INumber of patients who can not list any paraclinical analysis or
investigation of those that were done during hospitalization per
Total number of patients questioned.
03.01.01.03 RMeasures have been implemented to diminish the effects of the
identified vulnerabilities in the process of acquiring the informed
consent.
03.01.01.03.01 I Internal rules on obtaining informed consent are up to date.
03.01.01.03.02 IThe hospital identifies and analyses vulnerabilities on obtaining
informed consent.
03.01.01.03.03 IMedical staff is trained on the manner and vulnerabilities of
obtaining the informed consent of the patient.
03.01.02 CrMeasures regarding the consistency of medical practice with
the ethical and legal norms on patient medical data
confidentiality are in place.
APENDIX 2 Page 95 of 99
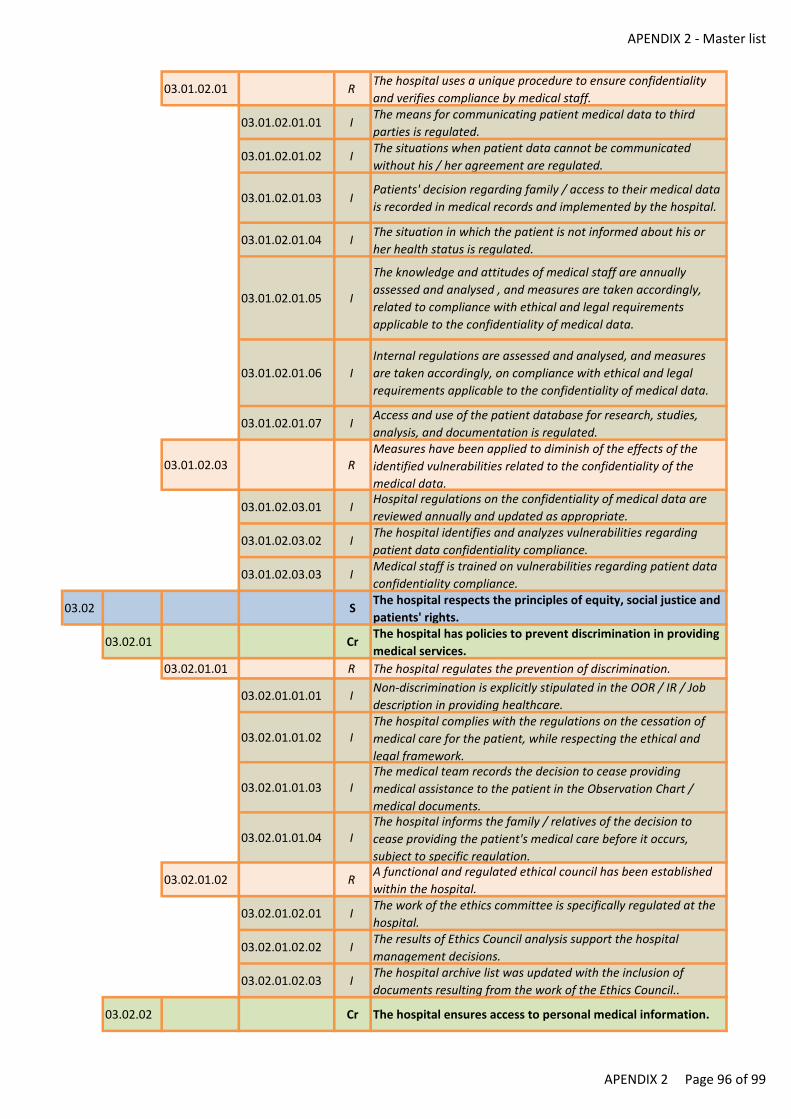
APENDIX 2 - Master list
03.01.02.01 RThe hospital uses a unique procedure to ensure confidentiality
and verifies compliance by medical staff.
03.01.02.01.01 IThe means for communicating patient medical data to third
parties is regulated.
03.01.02.01.02 IThe situations when patient data cannot be communicated
without his / her agreement are regulated.
03.01.02.01.03 IPatients' decision regarding family / access to their medical data
is recorded in medical records and implemented by the hospital.
03.01.02.01.04 IThe situation in which the patient is not informed about his or
her health status is regulated.
03.01.02.01.05 I
The knowledge and attitudes of medical staff are annually
assessed and analysed , and measures are taken accordingly,
related to compliance with ethical and legal requirements
applicable to the confidentiality of medical data.
03.01.02.01.06 I
Internal regulations are assessed and analysed, and measures
are taken accordingly, on compliance with ethical and legal
requirements applicable to the confidentiality of medical data.
03.01.02.01.07 IAccess and use of the patient database for research, studies,
analysis, and documentation is regulated.
03.01.02.03 RMeasures have been applied to diminish of the effects of the
identified vulnerabilities related to the confidentiality of the
medical data.
03.01.02.03.01 IHospital regulations on the confidentiality of medical data are
reviewed annually and updated as appropriate.
03.01.02.03.02 IThe hospital identifies and analyzes vulnerabilities regarding
patient data confidentiality compliance.
03.01.02.03.03 IMedical staff is trained on vulnerabilities regarding patient data
confidentiality compliance.
03.02 SThe hospital respects the principles of equity, social justice and
patients' rights.
03.02.01 CrThe hospital has policies to prevent discrimination in providing
medical services.
03.02.01.01 R The hospital regulates the prevention of discrimination.
03.02.01.01.01 INon-discrimination is explicitly stipulated in the OOR / IR / Job
description in providing healthcare.
03.02.01.01.02 IThe hospital complies with the regulations on the cessation of
medical care for the patient, while respecting the ethical and
legal framework.
03.02.01.01.03 IThe medical team records the decision to cease providing
medical assistance to the patient in the Observation Chart /
medical documents.
03.02.01.01.04 IThe hospital informs the family / relatives of the decision to
cease providing the patient's medical care before it occurs,
subject to specific regulation.
03.02.01.02 RA functional and regulated ethical council has been established
within the hospital.
03.02.01.02.01 IThe work of the ethics committee is specifically regulated at the
hospital.
03.02.01.02.02 IThe results of Ethics Council analysis support the hospital
management decisions.
03.02.01.02.03 IThe hospital archive list was updated with the inclusion of
documents resulting from the work of the Ethics Council..
03.02.02 Cr The hospital ensures access to personal medical information.
APENDIX 2 Page 96 of 99
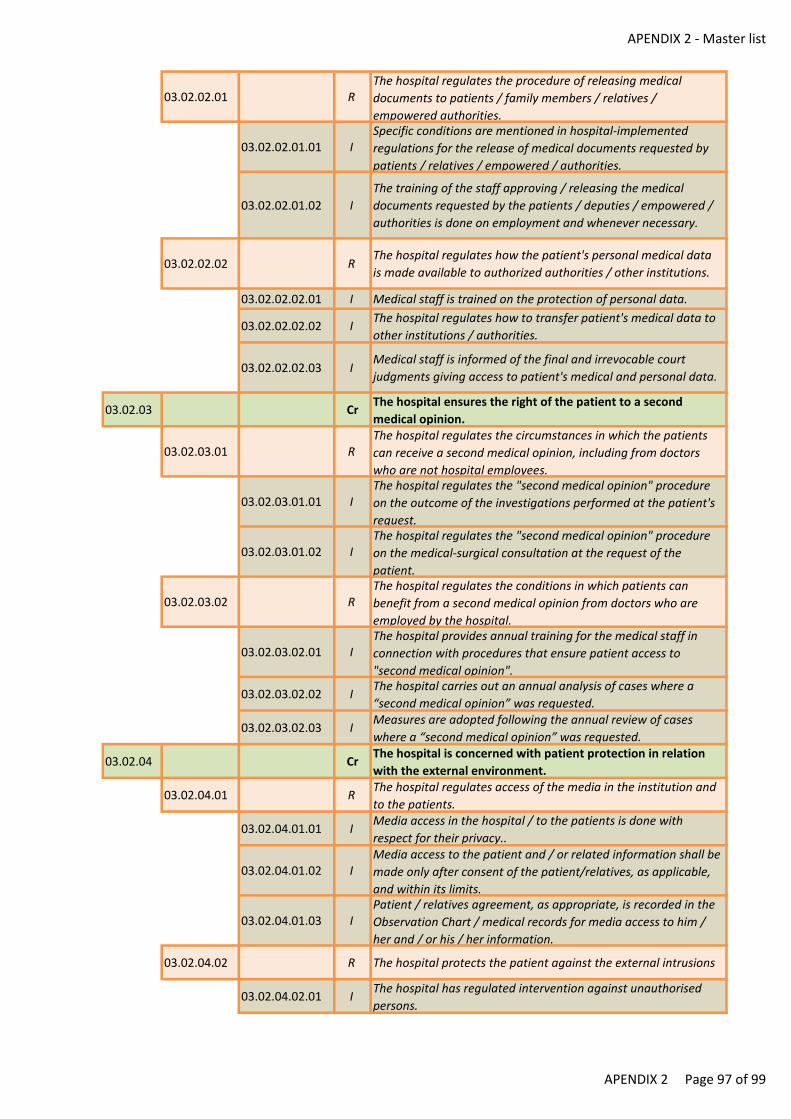
APENDIX 2 - Master list
03.02.02.01 RThe hospital regulates the procedure of releasing medical
documents to patients / family members / relatives /
empowered authorities.
03.02.02.01.01 ISpecific conditions are mentioned in hospital-implemented
regulations for the release of medical documents requested by
patients / relatives / empowered / authorities.
03.02.02.01.02 I
The training of the staff approving / releasing the medical
documents requested by the patients / deputies / empowered /
authorities is done on employment and whenever necessary.
03.02.02.02 RThe hospital regulates how the patient's personal medical data
is made available to authorized authorities / other institutions.
03.02.02.02.01 I Medical staff is trained on the protection of personal data.
03.02.02.02.02 IThe hospital regulates how to transfer patient's medical data to
other institutions / authorities.
03.02.02.02.03 IMedical staff is informed of the final and irrevocable court
judgments giving access to patient's medical and personal data.
03.02.03 CrThe hospital ensures the right of the patient to a second
medical opinion.
03.02.03.01 RThe hospital regulates the circumstances in which the patients
can receive a second medical opinion, including from doctors
who are not hospital employees.
03.02.03.01.01 IThe hospital regulates the "second medical opinion" procedure
on the outcome of the investigations performed at the patient's
request.
03.02.03.01.02 IThe hospital regulates the "second medical opinion" procedure
on the medical-surgical consultation at the request of the
patient.
03.02.03.02 RThe hospital regulates the conditions in which patients can
benefit from a second medical opinion from doctors who are
employed by the hospital.
03.02.03.02.01 IThe hospital provides annual training for the medical staff in
connection with procedures that ensure patient access to
"second medical opinion".
03.02.03.02.02 IThe hospital carries out an annual analysis of cases where a
“second medical opinion” was requested.
03.02.03.02.03 IMeasures are adopted following the annual review of cases
where a “second medical opinion” was requested.
03.02.04 CrThe hospital is concerned with patient protection in relation
with the external environment.
03.02.04.01 RThe hospital regulates access of the media in the institution and
to the patients.
03.02.04.01.01 IMedia access in the hospital / to the patients is done with
respect for their privacy..
03.02.04.01.02 IMedia access to the patient and / or related information shall be
made only after consent of the patient/relatives, as applicable,
and within its limits.
03.02.04.01.03 IPatient / relatives agreement, as appropriate, is recorded in the
Observation Chart / medical records for media access to him /
her and / or his / her information.
03.02.04.02 R The hospital protects the patient against the external intrusions
03.02.04.02.01 IThe hospital has regulated intervention against unauthorised
persons.
APENDIX 2 Page 97 of 99
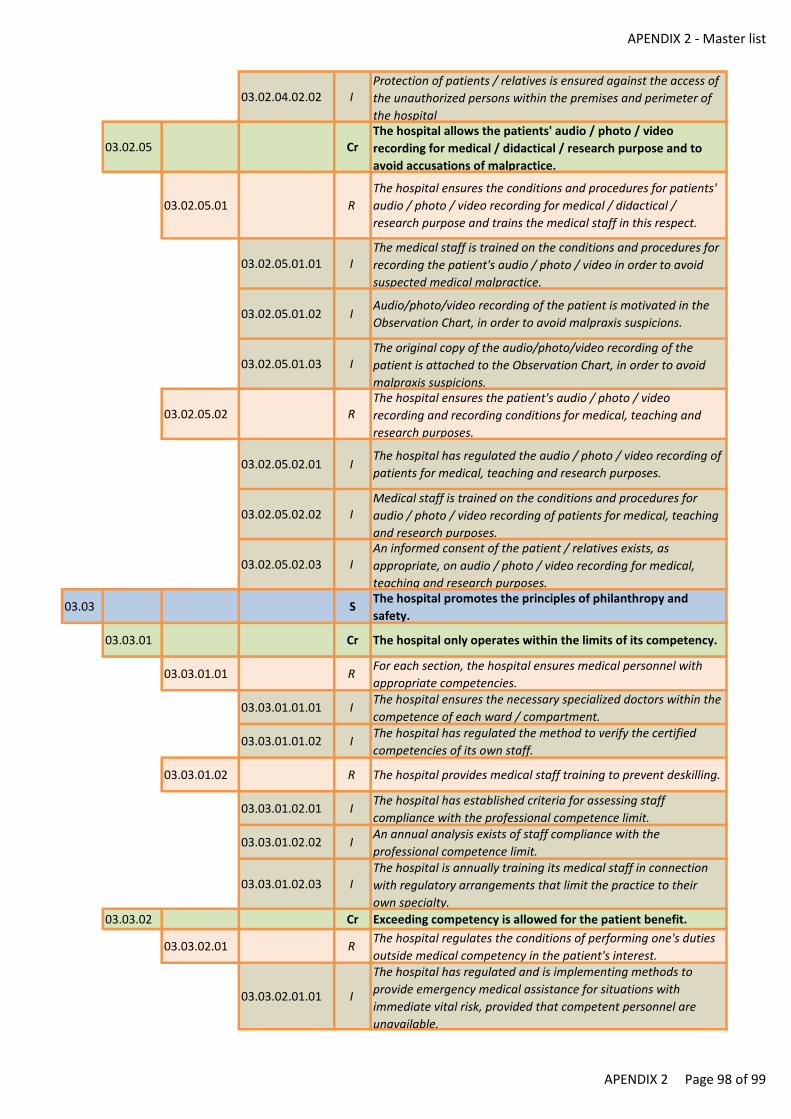
APENDIX 2 - Master list
03.02.04.02.02 IProtection of patients / relatives is ensured against the access of
the unauthorized persons within the premises and perimeter of
the hospital
03.02.05 CrThe hospital allows the patients' audio / photo / video
recording for medical / didactical / research purpose and to
avoid accusations of malpractice.
03.02.05.01 R
The hospital ensures the conditions and procedures for patients'
audio / photo / video recording for medical / didactical /
research purpose and trains the medical staff in this respect.
03.02.05.01.01 IThe medical staff is trained on the conditions and procedures for
recording the patient's audio / photo / video in order to avoid
suspected medical malpractice.
03.02.05.01.02 IAudio/photo/video recording of the patient is motivated in the
Observation Chart, in order to avoid malpraxis suspicions.
03.02.05.01.03 IThe original copy of the audio/photo/video recording of the
patient is attached to the Observation Chart, in order to avoid
malpraxis suspicions.
03.02.05.02 RThe hospital ensures the patient's audio / photo / video
recording and recording conditions for medical, teaching and
research purposes.
03.02.05.02.01 IThe hospital has regulated the audio / photo / video recording of
patients for medical, teaching and research purposes.
03.02.05.02.02 IMedical staff is trained on the conditions and procedures for
audio / photo / video recording of patients for medical, teaching
and research purposes.
03.02.05.02.03 IAn informed consent of the patient / relatives exists, as
appropriate, on audio / photo / video recording for medical,
teaching and research purposes.
03.03 SThe hospital promotes the principles of philanthropy and
safety.
03.03.01 Cr The hospital only operates within the limits of its competency.
03.03.01.01 RFor each section, the hospital ensures medical personnel with
appropriate competencies.
03.03.01.01.01 IThe hospital ensures the necessary specialized doctors within the
competence of each ward / compartment.
03.03.01.01.02 IThe hospital has regulated the method to verify the certified
competencies of its own staff.
03.03.01.02 R The hospital provides medical staff training to prevent deskilling.
03.03.01.02.01 IThe hospital has established criteria for assessing staff
compliance with the professional competence limit.
03.03.01.02.02 IAn annual analysis exists of staff compliance with the
professional competence limit.
03.03.01.02.03 IThe hospital is annually training its medical staff in connection
with regulatory arrangements that limit the practice to their
own specialty.
03.03.02 Cr Exceeding competency is allowed for the patient benefit.
03.03.02.01 RThe hospital regulates the conditions of performing one's duties
outside medical competency in the patient's interest.
03.03.02.01.01 I
The hospital has regulated and is implementing methods to
provide emergency medical assistance for situations with
immediate vital risk, provided that competent personnel are
unavailable.
APENDIX 2 Page 98 of 99
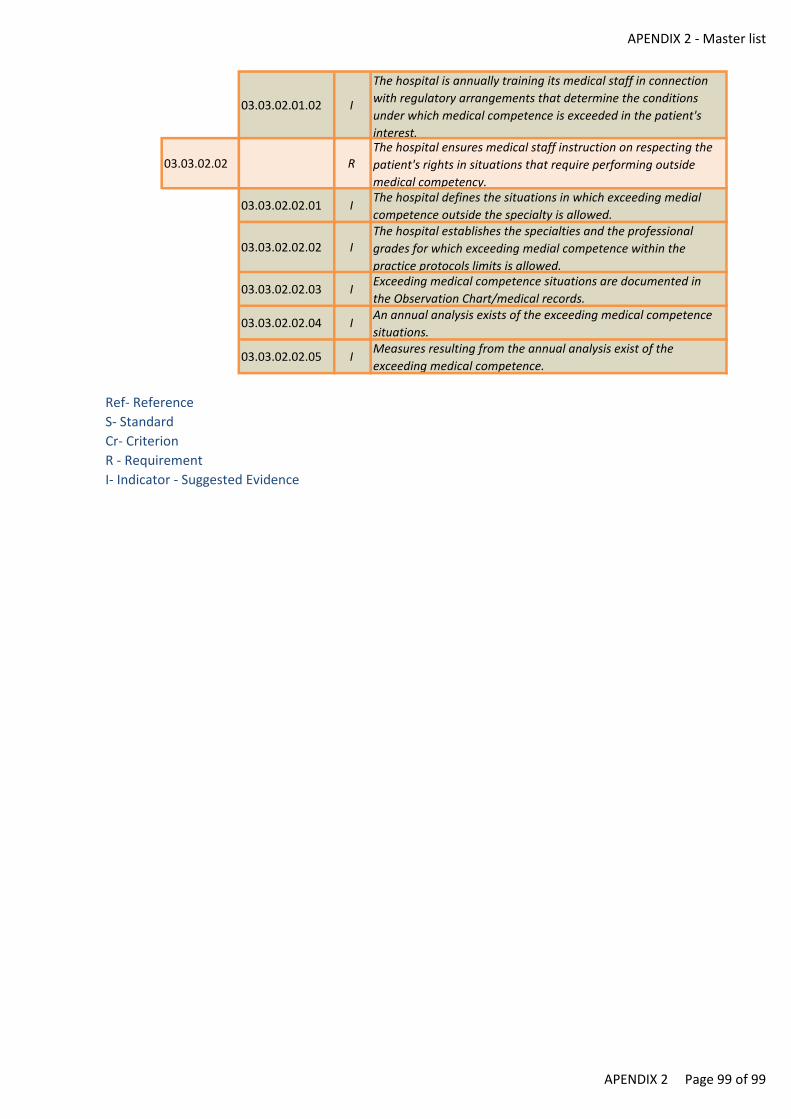
APENDIX 2 - Master list
03.03.02.01.02 I
The hospital is annually training its medical staff in connection
with regulatory arrangements that determine the conditions
under which medical competence is exceeded in the patient's
interest.
03.03.02.02 RThe hospital ensures medical staff instruction on respecting the
patient's rights in situations that require performing outside
medical competency.
03.03.02.02.01 IThe hospital defines the situations in which exceeding medial
competence outside the specialty is allowed.
03.03.02.02.02 IThe hospital establishes the specialties and the professional
grades for which exceeding medial competence within the
practice protocols limits is allowed.
03.03.02.02.03 IExceeding medical competence situations are documented in
the Observation Chart/medical records.
03.03.02.02.04 IAn annual analysis exists of the exceeding medical competence
situations.
03.03.02.02.05 IMeasures resulting from the annual analysis exist of the
exceeding medical competence.
Ref- Reference
S- Standard
Cr- Criterion
R - Requirement
I- Indicator - Suggested Evidence
APENDIX 2 Page 99 of 99
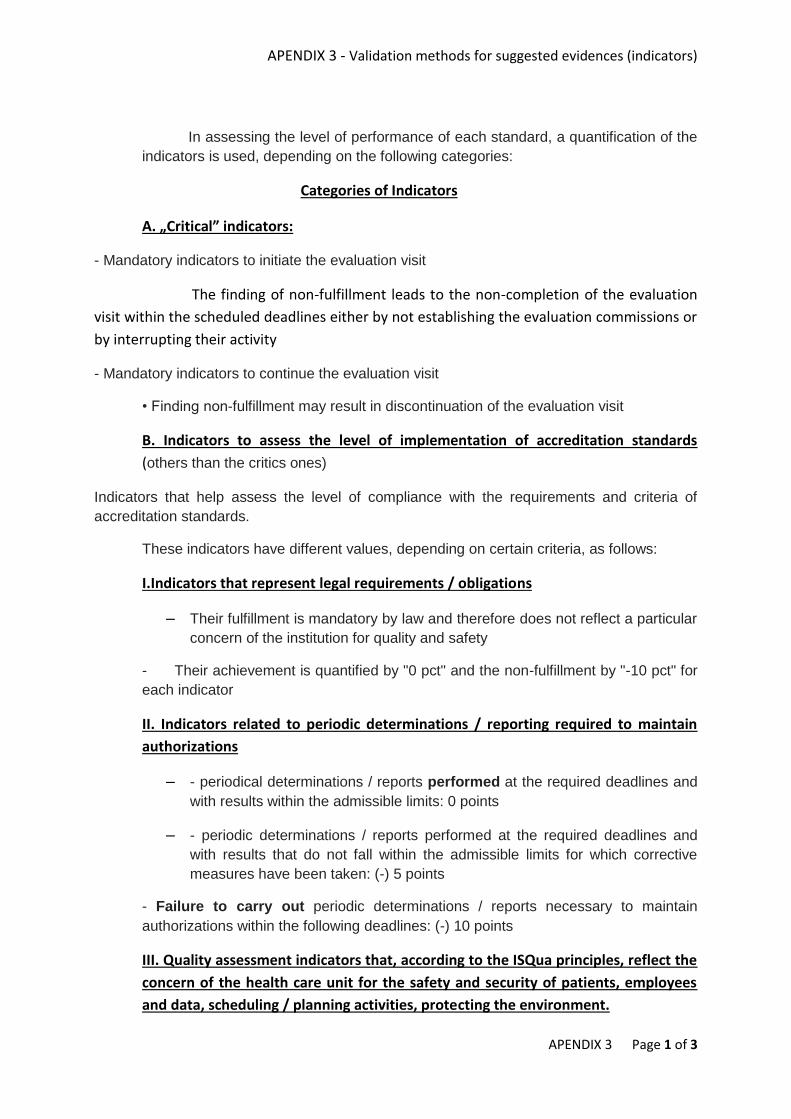
APENDIX 3 - Validation methods for suggested evidences (indicators)
APENDIX 3 Page 1 of 3
In assessing the level of performance of each standard, a quantification of the
indicators is used, depending on the following categories:
Categories of Indicators
A. „Critical” indicators:
- Mandatory indicators to initiate the evaluation visit
The finding of non-fulfillment leads to the non-completion of the evaluation
visit within the scheduled deadlines either by not establishing the evaluation commissions or
by interrupting their activity
- Mandatory indicators to continue the evaluation visit
• Finding non-fulfillment may result in discontinuation of the evaluation visit
B. Indicators to assess the level of implementation of accreditation standards
(others than the critics ones)
Indicators that help assess the level of compliance with the requirements and criteria of
accreditation standards.
These indicators have different values, depending on certain criteria, as follows:
I.Indicators that represent legal requirements / obligations
– Their fulfillment is mandatory by law and therefore does not reflect a particular
concern of the institution for quality and safety
- Their achievement is quantified by "0 pct" and the non-fulfillment by "-10 pct" for
each indicator
II. Indicators related to periodic determinations / reporting required to maintain
authorizations
– - periodical determinations / reports performed at the required deadlines and
with results within the admissible limits: 0 points
– - periodic determinations / reports performed at the required deadlines and
with results that do not fall within the admissible limits for which corrective
measures have been taken: (-) 5 points
- Failure to carry out periodic determinations / reports necessary to maintain
authorizations within the following deadlines: (-) 10 points
III. Quality assessment indicators that, according to the ISQua principles, reflect the
concern of the health care unit for the safety and security of patients, employees
and data, scheduling / planning activities, protecting the environment.
APENDIX 3 - Validation methods for suggested evidences (indicators)
APENDIX 3 Page 2 of 3
Within them two subcategories of indicators are identified:
a.Risk indicators
- indicators whose failure reflects deficiencies that may endanger the safety of
patients, staff, data and the environment (other than those critical)
- fulfillment is scored by 0 points, failure by (-10) points
– b. "Quality" indicators themselves:
– • The performance of these indicators is scored on a scale of 0 points to 10
points, depending on their relevance and the complexity of the resources
usable in their realization, as follows:
– • Indicators whose performance is "10 points":
- IAAM (associate infections to medical assitence) indicators
- Indicators for drug administration
- Indicators for the safety of surgical interventions
- Indicators for the safety of blood and blood products administration
- Indicators on healthcare in ITI
- Indicators for double identification
- Indicators relating to diagnostic technology risk
- Indicators related to the therapeutic technological risk
- Physical safety of the patient - falling (from the bed, from the trolley / trolley,
sliding on the pavement), lifts
- Food security
- indicators related to patient protection in case of internal events (fire,
collapse, internal flood, gas leakage, oxygen / water / water supply / ambient
temperature stop, ambient temperature
- Indicators regarding the hospital's reactive capacity in critical external
situations of the hospital (other than natural ones (collective accidents,
epidemics, war, etc.)
- Indicators related to natural hazards (earthquake, floods, etc.)
- Indicators relating to the use of employee protection equipment, employees'
in-service triage, regular employee health assessments, employee injury
prevention (immunizations)
- Indicators relating to data security and security
• - Programming / planning of activities
• - Indicators for the evaluation of procedures / protocols
• - Indicators related to patient route planning
• - Indicators regarding compliance with management / scheduling
• - Protecting the environment
APENDIX 3 - Validation methods for suggested evidences (indicators)
APENDIX 3 Page 3 of 3
• o Indicators on waste management
• o Indicators on waste water safety
• 0 – 9 points
– Indicators related to analyzes required for medical and managerial decision-
making, staff training / periodic training, continuing medical education, activity
monitoring - Score: 9 points
– - Indicators on the continuity of health care - 8 points
– - Indicators relating to patient information and informed consent: Score: 7
points
– - Indicators on patient rights compliance, measures from patient / employee
satisfaction score Score: 6 points
– - Indicators related to solving social problems of patients, providing services
related to medical activity (psychologist, physiokinetotherapy, spiritual
assistance, social services, mourning service etc.) Score: 5 points
– - Indicators of modern means of informing patients, communicating with
external physicians, planning and arranging external medical services
(medical recovery, home services, arranging transfer to another medical unit,
providing other medical opinion, etc.) Score: 4 points
– - Indicators related to process traceability, current maintenance activities,
maintenance, security and protection measures, facility facility for patients /
employees Score: 3 points
– - Indicators for display instructions, rights, information for patients Score: 2
points
– Indicators referring to the submission of a document (minutes, formal data -
job descriptions, etc.) Score: 1 point
The sum of the points obtained from the indicators of a standard, reported as a percentage to
the maximum possible value to be achieved for that standard, is the percentage of
compliance with that standard.
APENDIX 4 - Overall rating
APENDIX 4 Page 1 of 10
EVALUATION AND ACCREDITATION PROCEDURE FOR HOSPITALS
The terms and notions used herein have the following meaning:
a) Reference (R) – the groups of standards, criteria and requirements, all of them having the same
scope;
b) Standard (S) – represents the level of performance achievable and measurable, agreed upon by
professionals, which can be observed by the population to whom it is addressed. It consists of a set
of criteria and requirements which define the expectations related to the performance, structure and
the processes in a hospital.
c) Criterion (Cr) – the specific objective to be achieved to reach the standard.
d) Requirement (R) – action that must be undertaken for the specific objective to be achieved.
The hospital evaluation and accreditation procedure and methodology shall comply with the
following principles:
a) To ensure and permanently improve the quality of healthcare services and patient safety;
b) To ensure non-discriminatory patient access to healthcare services according to needs, within the
limits of the hospital mission and resources;
c) To respect human dignity, the principles of medical ethics and deontology and care for patients’
health;
d) Organisational management focused on supporting patient-centred clinical activity;
e) Integrated, inter- and multidisciplinary patient approach in case management;
f) To promote effectiveness and efficiency by developing the concept of professional practice
evaluation by clinical audit and by streamlining the decision-making process;
g) To promote organisational culture development through standards;
h) Environmental protection;
i) Transparency and openness, by efficient and ongoing information on the accreditation process,
direct communication with the accreditation beneficiaries in all stages of the evaluation process,
including in the development of the final version of the accreditation report;
j) Independence, objectivity, confidentiality and impartiality of the evaluation and accreditation
process;
k) Integrity and professionalism of evaluators.
National Authority for Quality Management in Health (A.N.M.C.S.) publishes on its website the
references, standards, criteria, requirements and verification tools.
APENDIX 4 - Overall rating
APENDIX 4 Page 2 of 10
The documents used in the evaluation and accreditation process, the deadlines and the manner of
their transmission, as well as the conditions for the postponement, cancellation or interruption of
the evaluation visit are established by an order of the President of A.N.M.C.S.
The evaluation and accreditation procedure shall include the following main stages:
a) Evaluation preparation stage;
b) Evaluation stage;
c) Accreditation stage.
The evaluation preparation stage, coordinated by the specialist structures of the National
Authority of Quality Management in Health, hereinafter called A.N.M.C.S., includes the following
main activities:
a) Hospital registration for the accreditation procedure with A.N.M.C.S., by filling in and submitting
the template form developed by the specialist structures of A.N.M.C.S. The accredited hospitals
shall submit the registration application within one year, but no less than 9 months before the
validity of the accreditation certificate expires, and those submitting for the first time the
registration application for the accreditation procedure within one year from the publication of the
order to which this annex is an integral part shall be evaluated according to the provisions of this
order;
b) Identification by A.N.M.C.S. of the necessary human resources for the evaluation visit and
planning of the evaluation visit;
c) Communication by A.N.M.C.S. of the response to the application, of the estimated period
for the performance of the evaluation visit and of the amount of the accreditation fee, estimated
based on the statements in the hospital identification form. The evaluation visit duration, which
underpins the estimation of the amount of the accreditation fee, shall be calculated according to the
visit duration calculation form, hereinafter called FCD, whose template is approved by order of the
A.N.M.C.S. president;
d) In case of structure changes occurred after the submission of the accreditation
application, FCD shall be updated and shall determine a recalculation of the fee according to the new
structure;
e) The accreditation fee calculation method and formula shall be established according to the
provisions of the Order of the Minister of Health and of the President of the Authority of Quality
Management in Health no. 1.350/668/2016 approving the accreditation fee calculation method, valid
for the accreditation cycle related to the period 2017-2021;
f) Communication by A.N.M.C.S., at least 9 months prior to the period planned or the
performance of the evaluation visit, of the initiation of the evaluation preparation stage, and of the
deadline within which the hospital should make available for A.N.M.C.S. the mandatory documents
requested, hereinafter called DOS, and the additional documents necessary for the evaluation and
accreditation process, hereinafter called DS;
APENDIX 4 - Overall rating
APENDIX 4 Page 3 of 10
g) DOS means documents certifying the legality of the hospital operations, internal
regulations on activities with major impact on patient and staff safety, hospital structure and the
proof of payment of the accreditation fee. The means of accreditation fee payment are set by order
of the A.N.M.C.S. president;
h) Analysis of DOS and DS by the specialist structures of A.N.M.C.S.;
i) If, the analysis performed according to the provisions of letter h) finds that the mandatory
requirements have been fulfilled, the evaluation visit shall be performed in the period initially
announced, and A.N.M.C.S. shall set up and approve the evaluation committee for accreditation
purposes, depending on the hospital specificity. The evaluation committee shall be set up according
to the provisions of the Order of the President of the Authority of Quality Management in Health no.
136/20151 approving the Operational Procedure for random distribution in the memberships of the
hospital evaluation committees of evaluators included in the A.N.M.C.S.’s Register of Healthcare
Services Evaluators specialised in hospital evaluation, and for the appointment of committee
presidents. The information on the membership of the evaluation committee and on the visit period
shall be published by A.N.M.C.S. on the institution website;
j) After the committee membership has been set, A.N.M.C.S. shall conclude contracts with
the members of the evaluation team, and they shall be trained by A.N.M.C.S. staff;
k) If the analysis performed according to the provisions of letter h) indicates that the hospital
does not meet the minimum mandatory requirements to start the evaluation visit, A.N.M.C.S. shall
submit the hospital a request to complete the documentation, within 30 calendar days after the
request receipt;
l) In case the documentation is complete upon expiry of the 30-day deadline, the provisions
of letters h) and i) shall apply;
m) In case the documentation is not complete upon expiry of the 30-day deadline, the
evaluation visit shall be postponed by A.N.M.C.S., and the hospital shall be responsible for the
consequences of non-accreditation. The visit shall be re-planned according to A.N.M.C.S. resources.
2) The evaluation stage, coordinated by the evaluation committee, shall include the pre-visit, the
actual visit and the post-visit.
a) The pre-visit shall include the following main activities:
i) Communication with the hospital and development of a report on DOS and DS
compliance which shall be submitted to A.N.M.C.S.;
ii) Based on the report mentioned at letter a), A.N.M.C.S. may decide to cancel the
evaluation visit;
iii) Development of the evaluation visit plan and it communication to the hospital;
b) The actual visit to the hospital includes the following main activities:
i) The kick-off meeting, with the participation of hospital representatives, in order to
establish in detail how the hospital visit will take place;
APENDIX 4 - Overall rating
APENDIX 4 Page 4 of 10
ii) The information meeting at the beginning of each day, with the participation of
hospital representatives;
iii) Reaching the specific objectives allocated to each evaluator within the evaluation
committee, by using the data collection techniques and instruments and by appraising the processes
within the hospital;
iv) Final information meeting, with the participation of hospital representatives, in
order to present the preliminary conclusions of the evaluation visit;
v) The draft evaluation report shall be commenced during the evaluation visit, and
each evaluation has the obligation to include in the draft report their own interim conclusions and to
archive the documents developed or received during the evaluation stage, which shall be submitted
to A.N.M.C.S. together with the evaluation report;
vi) Filling in the special situations form, for those situations which hinder the
evaluation process, whereby the evaluation committee requests A.N.M.C.S. to suspend the
evaluation visit. The A.N.M.C.S. president may decide to suspend the evaluation visit. In this
case, the entire activity of the hospital shall be considered non-compliant. The accreditation
process may be re-commenced, upon request of the hospital, with the approval of the
A.N.M.C.S. Management Board, according to the provisions of Art. 4 of this procedure;
vii) Filling in the special situations form, in case of identifying deficiencies which
endanger patient or hospital personnel safety, by which the evaluation committee notifies
such findings to A.N.M.C.S. The A.N.M.C.S. president may decide to suspend the evaluation
visit. In this case, the accreditation process may be re-commenced, with the approval of the
A.N.M.C.S. Management Board, according to the provisions of Art. 4 of this procedure.
c) The post-visit shall include the following main activities:
i) Development of the draft evaluation report by the members of the evaluation
committee and its submission to the evaluated hospital, within maximum 5 working days after the
actual visit to the hospital has been finalised;
ii) Within maximum 5 working days after having received the draft evaluation report,
the hospital shall formulate in writing objections on certain aspects included in the report, as
applicable;
iii) Analysis by A.N.M.C.S. staff, within maximum 5 working days after receipt, of the
objections formulated by the hospital and submission of conclusions to the evaluation
committee members;
iv) Development of the evaluation report by the evaluation committee members,
within maximum 5 working days after having received the conclusions, and its communication to the
hospital. The hospital may formulate no other objections against the evaluation report.
3) The accreditation stage shall include the following main activities:
APENDIX 4 - Overall rating
APENDIX 4 Page 5 of 10
a) The assessment of hospitals by the Evaluation and Accreditation Unit of the documents
generated in the evaluation process and the elaboration of the Accreditation Report with
classification according to accreditation categories, as follows:
I. Category I - Accredited
II. Category II - Accredited with recommendations
III. Category III - Accredited with reservations
IV. Category IV – Accredited with low confidence
V. Category V - Decision to prolong the accreditation process
VI. Category VI – not accredited
For enrollment in any accreditation category, sanitary facilities must meet the
following general minimum requirements:
a. each standard is met in excess of 51%;
b. the following critical patient safety indicators are met in 100%:
1.the existence of all authorizations or endorsements required by law
i. absence of infrastructure deficiencies and circuits that expose patients, employees or visitors to major risks (eg failure to observe the rules for the handling and storage of explosive materials, hazardous waste, fall prevention, electric shock, etc);
ii. Control of access to areas at risk of contamination (operator block, birth block,
ATI sections / compartments, neonatology, etc.)
The classification in the accreditation category is done by cumulative fulfillment of the
following three criteria, the category level being given by the criterion with the lowest
value / the lowest level:
1. total score - is the percentage expression of the number of points obtained, relative
to the maximum number of points to be obtained by that health unit.
Obtaining the overall score on compliance with accreditation standards is based on the
following criteria:
- indicators that represent legal requirements / obligations, the fulfillment of which is
mandatory by law and therefore does not reflect a particular concern of the institution
for quality and safety - their achievement is scored by 0 points, the failure to (-10) points
APENDIX 4 - Overall rating
APENDIX 4 Page 6 of 10
- Indicators pertaining to periodic determinations / reporting required to maintain
authorizations, which are quantified as follows:
- periodical determinations/reports performed at the required deadlines and with results within the admissible limits: 0 points - periodical determinations/reports performed at the required deadlines and with results that do not fall within the admissible limits for which corrective measures have been taken: (-) 5 points
- Failure to carry out periodic determinations / reports necessary to maintain
authorizations within the following deadlines: (-) 10 points
- Quality assessment indicators that, in accordance with WHO requirements and
ISQua principles, reflect the concern of the healthcare unit for the safety and security of
patients, employees and data, the scheduling / planning of activities, the environmental
protection to be quantified on a scale from 0 to + 10, depending on:
relevance for service quality and patient safety reflecting the level of risk associated with
failure to meet the indicator
the difficulty of accomplishing - the complexity of the resources and the activities necessary to accomplish it
level of accomplishment
2. the number of indicators (-10) obtained, as a percentage of the total number of value
indicators (-10) applicable to the sanitary unit. Value indicators (-10) are indicators that
represent legal obligations or indicators whose failure reflects serious hospital
deficiencies that pose or threaten the safety of patients, staff, data and the
environment.
3. the existence or non-existence of a plan for compliance with The Sanitary Operating
authorization (ASF) assumed by the management of the sanitary unit and approved by
the guardianship or patronage authority, in the case of private hospitals, the realization
of the time taken to accomplish it.
I. Category I – Accredited
- Criteria:
- total score over 90%
- there are no dotted indicators with (-10)
- ASF without compliance plan
Hospitals in this category are accredited without recommendations and are
encouraged, through their coverage by ANMCS, to maintain and improve the approach.
APENDIX 4 - Overall rating
APENDIX 4 Page 7 of 10
They can be rewarded by the public health insurance system under the service contract.
They can be nominated by the Minister of Health as a methodological tool for the
quality management for the other hospitals in the administrative-territorial area in
which they operate.
II. Category II – Accredited with recommendations:
- Criteria:
- total score between 70 - 89.99%;
- are scored (-10) less than 10% of the possible markers of this value applicable to that
sanitary unit;
- the compliance plan for ASF is assumed by the hospital and approved by the
guardianship or patronage authority to be completed within 12 months of receiving the
accreditation report.
If the compliance plan is fulfilled within the assumed period, the hospital may remain in
this category until the end of the 5-year period or may request the ANMCS a re-
evaluation for classification in category I. In the event of non-compliance with the
assumed interval, it may request its extension by up to 12 months , in which case it will
be classified in the following category.
III. Category III – Accredited with reservations:
This category includes Category II hospitals that have requested a prolongation of the
compliance plan or hospitals that, following the assessment, meet the following
classification criteria:
- total score between 51-69,99%;
- are indicated by (-10) between 10% and 30% of the possible markers of this
value applicable to that sanitary unit;
- the ASF compliance plan is assumed by the hospital and approved by the
tutelage or patronage authority to be completed within 24 months of receiving the
accreditation report.
If the compliance plan is fulfilled in the assumed period, the hospitals may remain in
the category given by the other criteria until the 5-year period or they can request the
ANMCS to reassess them in order to be in higher categories. In case of non-compliance
with the assumed interval, the hospitals will be classified in category IV.

APENDIX 4 - Overall rating
APENDIX 4 Page 8 of 10
IV. Category IV – Accredited with low confidence
This category includes hospitals meeting any of the first two criteria of categories I, II
or III but who have not undertaken to comply with the compliance plan or have
undertaken to comply with it within 24 months of receive the accreditation report or
have exceeded the period of 24 months originally assumed.
These hospitals may request the ANMCS, when communicating full compliance with the
non-conformities in the compliance plan to ASF, to be in the accreditation category set
by the other criteria.
V. Category V - Decision to prolong the accreditation process:
Within this category, for a maximum of 6 months after receiving the accreditation
report, hospitals that meet the following criteria:
- total score bigger then 51%;
- at most 2 standards with a score of less than 51% and / or between 30%
and 50% of the possible markers (-10) applicable to that sanitary unit are scored by this
value.
- non-acceptance or any assumed interval for the compliance with the ASF
compliance plan.
During this period, the hospital, considered in the accreditation procedure,
must meet the criteria for classification in one of categories I, II, III or IV, otherwise, at
the end of the 6 months, it will be declared non-accredited.
VI. Category VI – not accredited
This category includes:
- hospitals that, after the evaluation process, have scored altogether less than 51% or
- had more than two standards met in less than 50% or
- had more than 50% of the possible indicators to be scored by (-10) applicable to that
sanitary unit, labeled with this value, or
- Category V hospitals that did not meet the criteria for admission to one of the
accreditation categories within 6 months of receiving the accreditation report.
APENDIX 4 - Overall rating
APENDIX 4 Page 9 of 10
Hospitals in this category may enter a new accreditation procedure in the next
accreditation cycle, in compliance with the legal provisions in force at the time of applying
for registration, or in the same accreditation cycle at the decision of the Ministry of Health.
b) Issuance of the Order of A.N.M.C.S. President on the accreditation or non-accreditation of the
hospital, as applicable, and its communication to the hospital
The accreditation certificate shall be issued to those hospitals which obtained accreditation, within
maximum 90 working days after the Order of A.N.M.C.S. President on the accreditation has been
communicated to the hospital.
Methods Used for Hospital Accreditation:
(1) The internal evaluation (self-assessment) by the hospital consists in the analysis of services
provided, of the performance and monitoring indicators and in the communication of its conclusions
to A.N.M.C.S., as well as submission of other specific information requested by A.N.M.C.S.
throughout the evaluation process.
(2) The external evaluation consists in the stages provided by Art. 3 of this procedure.
The data collection techniques used in the evaluation and accreditation process are:
a) Analysis of documents provided by the hospital;
b) Direct observation – on the spot observation to note compliance with predefined requirements or
how activities are carried out, without interference by evaluators;
c) Focus groups – a quality research technique, by which the members of a group made of hospital
representatives and the evaluation committee members express their viewpoints on the topics
under discussion, within a limited period of time;
d) Interview – aims at data collection by direct discussion, during the actual visit;
e) Simulation of processes to identify clinical risks.
(2) Validation of data collected consists in their verification by the evaluation committee, by
examination, recalculation, comparison and agreement to confirm the reality of the data collected.
The main instruments used for hospital accreditation are:
a) Hospital identification form – a template document developed by the specialist structures of
A.N.M.C.S., requesting the hospital to provide information on the identification data and on its
organisational and operational structure;
b) List of mandatory documents requested - a template document developed by the specialist
structures of A.N.M.C.S., requesting the hospital to submit the documents whose existence and
compliance are a prerequisite for the initiation of the evaluation stage;
APENDIX 4 - Overall rating
APENDIX 4 Page 10 of 10
c) List of additional documents necessary for the evaluation and accreditation process - a template
document developed by the specialist structures of A.N.M.C.S., requesting the hospital to submit the
documents whose existence is necessary for the initiation of the evaluation stage;
d) Self-assessment form – a template document developed by the specialist structures of A.N.M.C.S.,
requesting the hospital to submit information on meeting the requirements of the accreditation
standards in successive stages of the evaluation and accreditation process;
e) Compliance Plan for evaluation purposes – a document submitted by A.N.M.C.S. to the hospital
under accreditation procedure, communicating the hospital any non-compliance which prevents the
initiation of the evaluation procedure.
f) The evaluation visit timetable – a document including the hours and the objectives to be
evaluated;
g) Meetings minutes – a documents including the important aspects discussed by evaluators and
representatives of the hospital under evaluation;
h) Checklist – a template document developed by the specialist structures of A.N.M.C.S., used for
data collection purposes;
i) List of documents requested during the actual evaluation – a template document developed by the
specialist structures of A.N.M.C.S., including the additional documents requested by evaluators form
the hospital representatives during the evaluation process;
j) Questionnaire – an instrument developed by the specialist structures of A.N.M.C.S., applied at
individual level only after having obtained the consent and after having guaranteed confidentiality
and anonymity;
k) Identification and non-compliance form – a template document developed by the specialist
structures of A.N.M.C.S. and filled in by evaluators, who note, during the evaluation visit, facts
disturbing the visit;
l) Special situations form – an unilateral document drafted by the evaluation committee to indicate
facts which hinder the evaluation visit or endanger patient or hospital personnel safety, submitted to
the A.N.M.C.S. president, which may lead to the suspension of the evaluation visit;
m) Draft evaluation report – a written communication submitted by the evaluation committee to the
hospital, on the results of the evaluation visit for accreditation purposes, submitted to the hospital to
formulate possible objections;
n) Evaluation Report – a written communication submitted by the evaluation committee to the
hospital, on the results of the evaluation visit for accreditation purposes, submitted to the hospital
after having analysed and solved any possible objections;
o) Accreditation Report – a document developed by the specialist structures of A.N.M.C.S.
underpinning the issuance of the accreditation or non-accreditation order of the A.N.M.C.S.
president, as applicable.







