
Slowing of Mitral Valve Annular Calcium in Systemic Hypertension by Nifedipine and Comparisons with Enalapril and Atenolol
Federico Cacciapuoti, MD, Nicolb Perrone, MD, Rosalba Diaspro, MD, Domenico Galzerano, MD, Salvatore Gentile, MD, and Bartolomeo Lapiello, MD
Mitral annular calcium (MAC) is a condition that often occurs in patients with systemic hyperteu sion. To evaluate the effectiveness of nifedipine in preventing MAC, 223 patients with systemic hy- pertension of recent onset and without MAC were selected and randomly enrolled in 3 groups: group l(76 patients) received nifedipine; group 2 (72 patients) received enalapril; and group 3 (75 pa tients) received atenolol. After 5 years, these treatments significantly reduced systolic (p ~0.001) and diastolic (p ~0.05) blood pressure (BP) in 3 treated groups. M-mode echocardiom phy revealed MAC only in 2 patients in the nifedi- pine group (2.6%), in 13 in the enalapril group (Is%) and in 15 in the atenolol group (20%). The degree of MAC was mild (<5 mm) in the 2 patients in group 1, in 5 of the 13 in group 2, and in 6 of the 15 in the group 3, whereas it was severe (~5 mm) in the remaini* 6 in the enalapril group and in the other 9 in the atenolol group. There was also a significant correlation in the degree of MAC, left atrial enlargement and mitral regurgita tion. In addition, atrial fibrillation and atrioventric- ular conduction defects were associated with SB vere MAC. These results indicate that nifedipine is an effective drug both in the long-term manage ment of systemic hypertension and in preventing or delaying MAC.
(AmJCardiol1993;72:1039-1042)
From the Department of Geriatrics of the Faculty of Medicine, II Uni- versity of Naples, Italy. Manuscript received March 6, 1993; revised manuscript received June 7, 1993, and accepted June 8.
Address for reprints: Federico Cacciapuoti, MD, Cattedra di Tera- pia Medica, II Ateneo di Napoli, Piazza L. Miraglia, 2 80138 Naples, Italy.
M itral annular calcium (MAC) is a condition that frequently occurs in elderly subjects and particularly in patients with systemic hyper-
tension and diabetes mellitus.1-3 Although the signifi- cance of the association between MAC and systemic hy- pertension is unclear, Roberts suggested that conditions increasing the pressure of mitral valve closure induce MAC.4 In fact, during left ventricular systole the peak force to which the mitral valve is exposed is equal to the product of the mitral orifice area and the left ven- tricular force. Therefore, when this ventricular peak force increases, as occurs in systemic hypertension, the mitral valve undergoes increased stress. The posterior mitral leaflet is more exposed to mitral stress than the anterior leaflet because of its perpendicular position to the vector of left ventricular outflow force. This in- creased force may be transferred to the mitral annulus, inducing MAC.‘v5 Calcium-chelating agents and inhibi- tors of calcium influx into cells, such as calcium antago- gonists, may interfere in the development of MAC. However, calcium antagonists are also an effective drug class in long-term systemic hypertension management.6,7 Therefore, in the present study we prospectively evalu- ated the effectiveness of nifedipine in preventing MAC during the long-term treatment of patients with systemic hypertension.
METHODS Study population: Between May 1984 and Decem-
ber 1985, 237 patients (168 men and 69 women), age range 37 to 62 years (mean age 48 * 7) were selected among 2,624 patients with systemic hypertension. Crite- ria for selection were (1) high systemic blood pressure (BP) (systolic BP 2160 mm Hg and diastolic BP 190 mm Hg); (2) recent onset of systemic hypertension (16 months); (3) absence in the clinical history of other ma- jor atherosclerosis risk factors (diabetes mellitus, dyslip- idemia, cigarette smoking); (4) absence of history and clinical signs of congenital or acquired mitral valve dis- ease and other cardiac disease; (5) absence of echocar- diographic findings of MAC; and (6) absence of elec- trocardiographic and echocardiographic signs of left ventricular hypertrophy, left atrial enlargement and cor- onary artery disease. After a 2-week washout, fasting plasma glucose levels, total cholesterol, high-density li- poprotein and low-density lipoprotein cholesterol and serum triglyceride concentrations were measured. At the same time, patients underwent 1Zlead electrocardio- graphic recording, 24-hour systemic BP monitoring and
1038 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 NOVEMBER 1.1993

M-mode, 2-dimensional, Doppler and color Doppler echocardiography. For color Doppler, a commercially available instrument by Advanced Technology Labora- tories (Ultramark 9), with a phased-array 3 MHz trans- ducer was used.
Echocardiographic examination: Two-dimensional echocardiographic examination was performed as de- scribed.8 Parasternal short-axis view at the midventricu- lar level was used to derive the M-mode measurements of left ventricular end-systolic and end-diastolic dimen- sions. Ventricular septum and free left ventricular wall thicknesses were also measured by this approach. Mean left ventricular wall thickness was calculated as half the sum of the septal and free wall thickness. Left ventricu- lar hypertrophy was diagnosed when this mean value was Zl3 mm. The parastemal long-axis approach, at the aortic root level, was used to obtain M-mode left atrial dimensions. Left atria1 enlargement was defmed as left
atria1 size of >4.0 cm, as measured from the leading edge of the posterior aortic wall to the leading edge of the posterior left atrial wal1.9
Detedonofmi&alamu&calcification:Mitralvalve apparatus was examined by M-mode, 2-dimensional and color techniques. For the latter, parastemal long-axis and apical 4-chamber views were used. MAC was defined by the M-mode technique as dense echoes behind the posterior leaflet of the mitral valve, moving parallel and anterior to the endocardium of the posterior left ven- tricular wall, and best detected with a sweep horn the aortic root to the left ventricular cavity (Figure 1). The degree of MAC was measured in millimeters at its widest point behind the echoes originating from the mi- tral valve and was defined as mild when <5 mm and se- vere when >5 nnn10 Finally, to detine the characteris- tics of diastolic mitral flow and to evaluate the presence of mitral valve regurgitation, Doppler and color Doppler
FlGURE 1. W?, bode echocardii performed at level of the mitral leaflets; rim, 2dimeasional echocardiography by apical 4-chamber approach. An increased bri&tness and thickness of the mitral amudus (ANN.) due to calcinosis (CALC) is evident. AML q atrial mitral leaflet: ANNULD q annulus; IVS = interventricular septum; LA q Left atrium; LV = Left ventikle; M q mitral valve; RV = fight veatrike.
FlGURE 2. Mean values r 1 SD and statisti- cal significance of the systolic and diastolic -presoure reamled in basal condictioes and in 3 treated groups at final evaluation. ATEN. = atenolol group; BASAL = basal vaC ues; ENAL = enalapril group; NIF. q nifedi- pine WP.
BLOOO PRESSURE
x p(e.65 m p ( e&31
WR NlF. EtR. ATEN.
MITRAL ANNULAR CALCIUM 1039

transmitral flow velocities during systole and diastole were recorded from the apical 4-chamber approach, with the sample volume placed at level of the mitral leaflets.
Patient mbmbation: After basal examination, se- lected patients were randomly enrolled in 3 groups: group 1 (82 patients) received nifedipine orally (20 mg twice daily); group 2 (76 patients) was treated with the angiotensin-converting enzyme inhibitor enalapril (20 mg once daily); and group 3 (79 patients) was treated with the P-blocker atenolol(lO0 mg once daily). The di- uretic chlorthalidone (12.5 mg/day) was added when the single antihypertensive drug was inadequate in reducing high systemic BP levels. This drug was necessary in 8 patients in group 1, in 7 in group 2 and in 6 in group 3. All patients underwent the same biochemical, elec- trocardiographic and echocardiographic examinations at each return visit, performed every 6 months and lasting 5 years. During the study, 5 patients in group 1 (6%), 3
in group 2 (3.9%) and 4 in group 3 (3.8%) withdrew because of adverse effects. In addition, 1 patient in the nifedipine group and 1 in the enalapril group died from unrelated disease. . . Stab&cd analysis: Values in systemic BP, left ven- tricular dimensions, left ventricular wall thickness, left atrial size and biochemical data were expressed as mean I!I 1 SD. These means were compared with those of bas- al measurements, using the Student’s t test for unpaired data. MAC was identified and its percent incidence was calculated in 3 groups. Results obtained were compared using the &i-square test and differences were considered significant at p <0.05. The h4AC dimensions were also measured to detine their degree. Finally, the presence and incidence of some cardiac complications such as left atrial enlargement, mitral valve insufliciency, atrial fibril- lation and atrioventricular conduction disturbances were detined.
SLOOD GLUCOSE TOTFlL CHOLESTEROL 110
1 263 258
HOL CHOLESTEROL LOL CHOLESTEROL
170 1
TRIGLYCERIDE’ 2887 I
NIFEOIPINE
ENRLRPRIL
RTENOLOL
FlGURE 3. Mean values f 1 SD among the basal levels of fast- ing blood glucose, total choles terol, hiiensity lipoprotein (HDL) cholesterol, low&n&y lipoprotein (LJBL) cholesterol, tkt@yceriaes, and values ob- tained in 3 treated gwwps at theendoftbestudy.
1040 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 NOVEMBER 1,1993
RESULTS Two hundred twenty-three patients completed the
study: 76 from the nifedipine group, 72 from the enala- pril group and 75 from the atenolol group.
Hemodynamk and biochemical data: Three differ- ent treatments significantly reduced (p <O.OOl) basal val- ues of systolic BP (182 + 14 vs 155 -t 9 mm Hg; 156 + 8 and 154 + 9 mm Hg, respectively) (Figure 2). Dia- stolic BP was also significantly (p ~0.05) decreased in 3 groups (97 f 5 vs 82 t- 3 mm Hg; 81 + 4 and 82 + 5 mm Hg) (Figure 2). Fasting plasma glucose levels were normal at baseline conditions and at final evalua- tion (Figure 3). Total cholesterol, high-density lipopro- tein and low-density lipoprotein cholesterol and triglyc- eride plasma concentrations also remained unchanged in 3 treated groups (Figure 3). Left ventricular diameters were unchanged after 5 years of treatment, whereas left ventricular wall thickness slightly increased.
Development of mitral annular cakbwsis: At the end of the trial, MAC was seen in 2 of the 76 patients who received nifedipine, with an incidence of 2.6% (Ta- ble I). By contrast, this tinding was evident in 13 of the 72 patients (18%) in the enalapril group (p ~0.01) and in 15 of the 75 (20%) in the atenolol group (p ~0.01) (Table I). The total number of MAC seen in patients who received enalapril and atenolol (groups 2 and 3)
was 28 mm, with a 19% incidence. This value was sig- nificantly higher (p ~0.01) than that found in the nifed- ipine group (2.6%). The degree of MAC was defined as mild (~5 mm) in 2 patients with this tinding in the nifedipine group, in 5 of the 13 patients in the enalapril group and in 6 of the 15 in the atenolol group. In con- trast, MAC was defined as severe (>5 mm) in the re- maining 8 patients in the enalapril group and in the other 9 in the atenolol group (Table I).
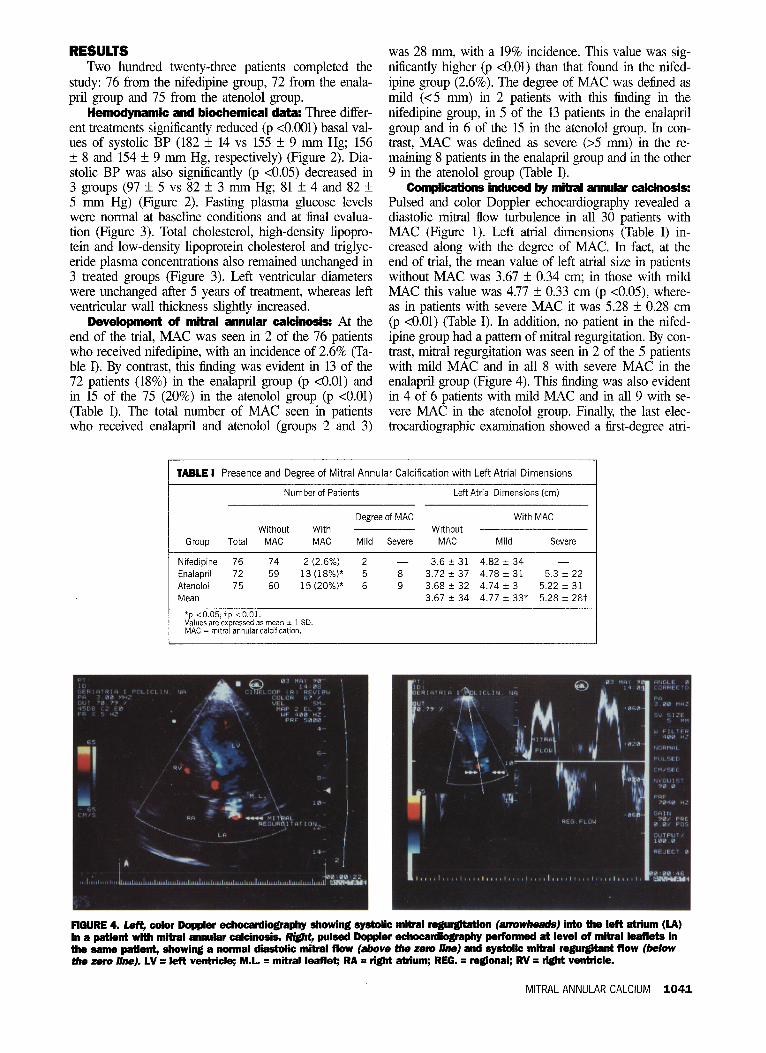
Con@kalions induced by mitral znsudw cakinosis: Pulsed and color Doppler echocardiography revealed a diastolic mitral flow turbulence in all 30 patients with MAC (Figure 1). Left atria1 dimensions (Table I) in- creased along with the degree of MAC. In fact, at the end of trial, the mean value of left atrial size in patients without MAC was 3.67 f 0.34 cm; in those with mild MAC this value was 4.77 k 0.33 cm (p <0.05), where- as in patients with severe MAC it was 5.28 + 0.28 cm (p <O.Ol) (Table I). In addition, no patient in the nifed- ipine group had a pattern of mitral regurgitation. By con- trast, mitral regurgitation was seen in 2 of the 5 patients with mild MAC and in all 8 with severe MAC in the enalapril group (Figure 4). This linding was also evident in 4 of 6 patients with mild MAC and in all 9 with se- vere MAC in the atenolol group. Finally, the last elec- trocardiographic examination showed a tirst-degree ani-
TABLE I Presence and Degree of Mitral Annular Calcification with Left Atrial Dimensions I Number of Patients Left Atrial Dimensions (cm)
Degree of MAC With MAC Without With Without
Group Total MAC MAC Mild Severe MAC Mild Severe
Nifedipine 76 74 2 (2.6%) 2 - 3.6 t 31 4.82 t 34 Enalapril 72 59 13(18%)* 5 8 3.72 -c 37 4.78 -c 31 5.3 + 22 Atenoloi 75 60 15 (20%)* 6 9 3.68 rk 32 4.74 + 3 5.22 + 31 Mean 3.67 + 34 4.77 + 33* 5.28 + 287
*p <0.05; tp <O.Ol. Values are expressed as mea” 2 1 SD. MAC = mitral annular calcification.
FIBURE 4. L&, color Boppk echocardiography showing systolic mitral regurgitation (atrwwI~&sj into the left atrium (LA) in a patient with mitral annular cakinosis. Rim, pulsed Doppler echocardiography performed at level of mitral leaflets in the same patient, showing a normal diastolic mitral flow (a&eve Be zolb /ine) and systolic mitral regurgitant flow (below the zero /in& LV q left ventricle; ML q mitral leaflet; RA = tight atrium; REG. = regIonal; RV = right ventricle.
MITRAL ANNULAR CALCIUM 1041

oventricular block in 2 patients with severe MAC in the enalapril group, and atrial fibrillation in 3 of those with this degree of MAC in the atenolol group.
DISCUSSION The significant reduction in high systemic BP in-
duced by. 3 treatments and lasting for 5 years certainly reduced the theoretical incidence of MAC, which one would expect if patients were untreated. Nevertheless, the smaller incidence of MAC recorded in the nifedi- pine group compared with those recorded in the other 2 groups may be dependent on the specific action mecha- nism of the nifedipine. Currently, no peculiar protective effect of the calcium antagonists on the mitral annulus is known. However, MAC is a degenerative lesion simi- lar to the age-dependent arterial calcinosis described by Fleckenstein et al.11-13 These investigators demonstrated that the calcium antagonist verapamil was able to pro- vide long-term protection of the arterial wall against age-induced calcium overload. Furthermore, Lichtlen14 and Knorr and Kazda,r5 reported similar results with nifedipine. We agree that the calcium antagonist nifedi- pine may interfere with the pathogenetic process induc- ing MAC by means of a specific anticalcinotic mecha- nism, different from its antihypertensive effect.
Acknowledgment: We are grateful’ to Eduardo Pel- legrino for technical assistance.
1. Savage DD, Garrison RJ, Castelli WP, McNamara PM, Anderson JS, Kannel BW, Feinleib M. Prevalence of submitral (annular) calcium and its correlates in a
general population-based sample (the Framingham Study). Am J Cardiol 1983;51: 1375-1378. 2. Rob&s WC, Perloff JK. Mitral valvulx disease: a clinic-pathological survey of the conditions causing the mitral valve to function abnormally. Ann Intern Med 1972;71:939T-915. 3. Cacciapuoti F, D&pro R, D’Avino M, Lama D, Coppola F, Bianchi U, Var- ricchio M. Calcifications of the mitral annulus as a marker of atherosclerosis in the elderly. Arch Gerontol Geriafr 1991;(suppl 2):339-344. 4. Roberts WC, Dangel JC, Bulkley BH. Non-rheumatic valvular cardiac disease: A clinicopathologic survey of 27 different condictions causing valwlar dysfunctions. In: Brest AM, ed. Cardiovascular Clinics. vol 5. No. 2. Philadelphia: FA Davis, 1973:333446. 5. Wailer BF, Roberts WC. Cardiovascular disease in the elderly. An analysis of 40 necmscopy patients aged 90 years or over. Am J Cardiol 1983;51:4031121. 6. Fleckenstein A, Frey M, Fleckenstein-Gmn G. Antihypertensive and arterial an- ticalcinotic effects of calcium antagonist. Am .I Cardiol 1986;57:1D-1OD. 7. Murphy MV, &riven AJ, Dollcry CT. Role. of n&=&pine in the treatment of hypertension. Br Med J 1983;287:257-262. 8. Tajik AJ, Seward JB, Hagler DJ, Mair DD, Lie JT. Twc-dimensional real time ultrasonic imaging of the heart and great vessels: technique, image orientation, stmc- ture, identification and validation. Mayo Clin Proc 1978;53:271-303. 9. Feigenbaum H. Echocardiography. 3rd ed. Philadelphia: Lea & Febiger, 1981:173. 10. Mellino M, Salcedo E, Lewer HM, Vasudevan G, Kramer JR. Echccardio- graphic-quantified severity of mitral ammlus calcification: prognostic correlation to related hemcdynamic, valvular, rhythm, and conduction abnormalities. Am Heart J 1982;103:322-325. 11. Fleckenstein A, Frey M, Fleckenstein-Gmn G. Protection by calcium antago- nists against experimental arterial calcinosis. Ix Pyorala K, eds. Secondary Pre- vention of Coronary Heart Disease. Workshop of the Internat Society and Fe&a- tion of Cardiology, Titisee, Oct. 1983. Stuttgart: G Thieme Verlag, 1983:1l%122. 12. Fleckenstein A, Fleckenstein-Gmn G, Frey M, Zom J. Future directions in the use of calcium antagonists. Am J Cardiol 1987;59:177B-187B. 13. Fleckenstein A, Frey M, Zom J, Fleckenstein-Gmn G. Calcium, a neglected key factor in hypertension and arteriosclerosis. Experimental vasopmtection with calcium antagonists or ACE inhibitors. In: Laragh JH, Brenner BM, eds. Hyper- tension: Pathophysiology, Diagnosis, and Management, New York: Raven Press, 1990:471-509. 14. Lichtlen P. Antisclemtic effects of nifedipine: the INTACT study. In: New Trends, Aspects, and Long-Term Benefits of Calcium Antagonists-Focus on Adalat. Proceedings of a Symposium in Vancouver, April 1989. 15. Knorr AM, Kazda S. Influence of nifedipine on experimental arteriosclerosis. Cardiovasc Drug Ther 1990;4:1027-1032.
1042 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 NOVEMBER I,1993







