Sclérodermie systémique Pronostic
Pôle de Médecine Interne, Centre de référence pour les vascularites
nécrosantes et la sclérodermie systémique, hôpital Cochin, Assistance
publique-Hôpitaux de Paris, Paris
Université Paris Descartes, Inserm U1016, Institut Cochin, Paris
Luc Mouthon
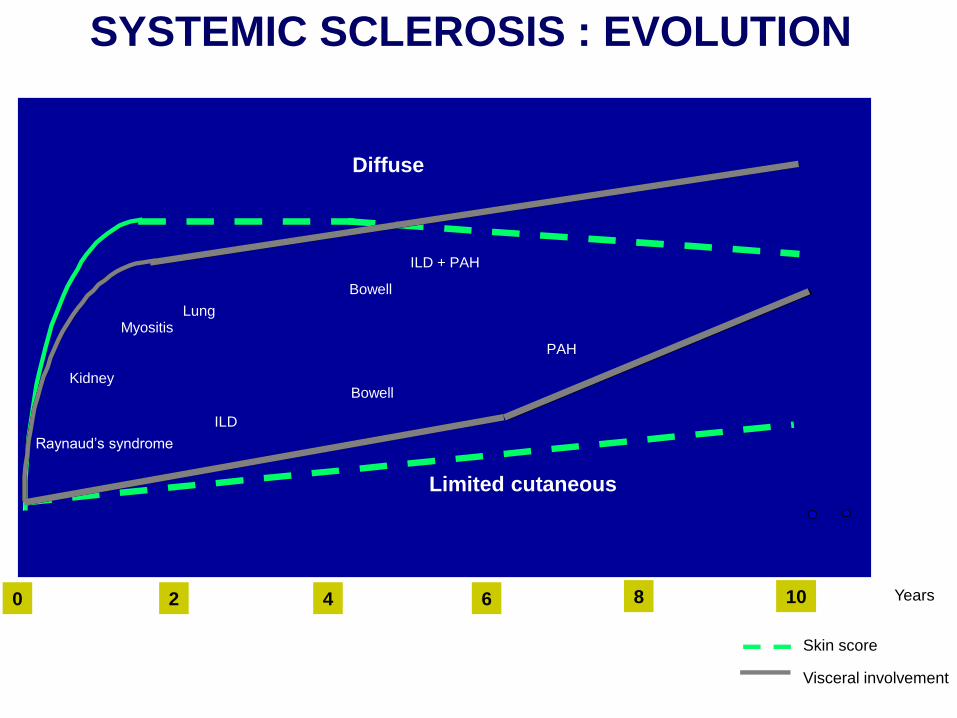
Skin score
Visceral involvement
SYSTEMIC SCLEROSIS : EVOLUTION
Diffuse
Limited cutaneous
0 10 2 4 6 8
Raynaud’s syndrome
Kidney
ILD + PAH
Myositis
Bowell
ILD
PAH
Bowell
0 10 2 4 6 8 Years
Lung
Elements pronostiques (I)
The 9 years survival rate was 38% with severe visceral involvement
72% without visceral involvement (p < 0.001)
Steen V, Arthritis Rheum 2000: 2437

Éléments pronostiques (II)
• Les séries récentes montrent une diminution de la mortalité – survie à 10 ans de 80% à 92% dans les formes
limités
– survie à 10 ans de 62 à 76% dans les formes diffuses
• Cela semble en grande partie liée à l’amélioration des traitements à visée vasculaire
• Caractères péjoratifs d’une atteinte viscérale en particulier pulmonaires, cardiaques et rénales.
Mortalité
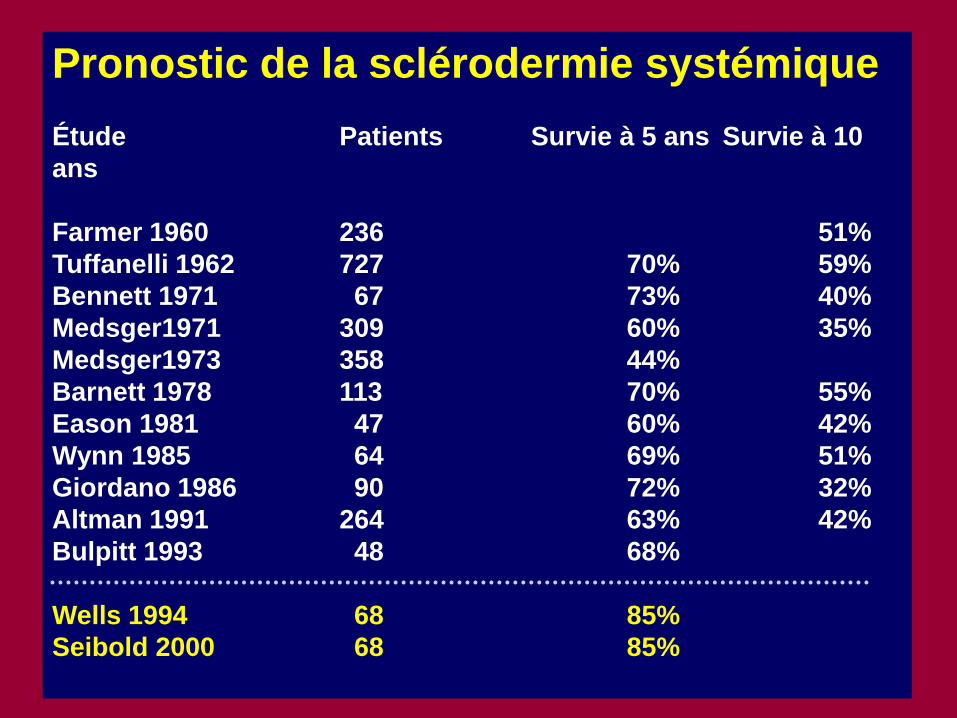
Pronostic de la sclérodermie systémique
Étude Patients Survie à 5 ans Survie à 10
ans
Farmer 1960 236 51%
Tuffanelli 1962 727 70% 59%
Bennett 1971 67 73% 40%
Medsger1971 309 60% 35%
Medsger1973 358 44%
Barnett 1978 113 70% 55%
Eason 1981 47 60% 42%
Wynn 1985 64 69% 51%
Giordano 1986 90 72% 32%
Altman 1991 264 63% 42%
Bulpitt 1993 48 68%
Wells 1994 68 85%
Seibold 2000 68 85%
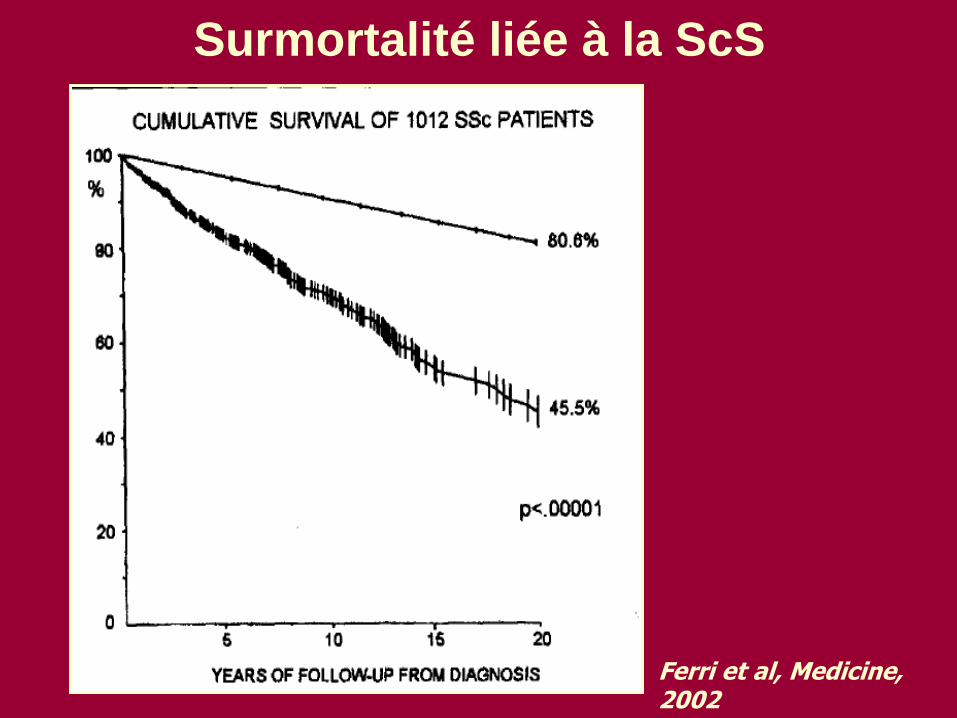
Surmortalité liée à la ScS
Ferri et al, Medicine, 2002
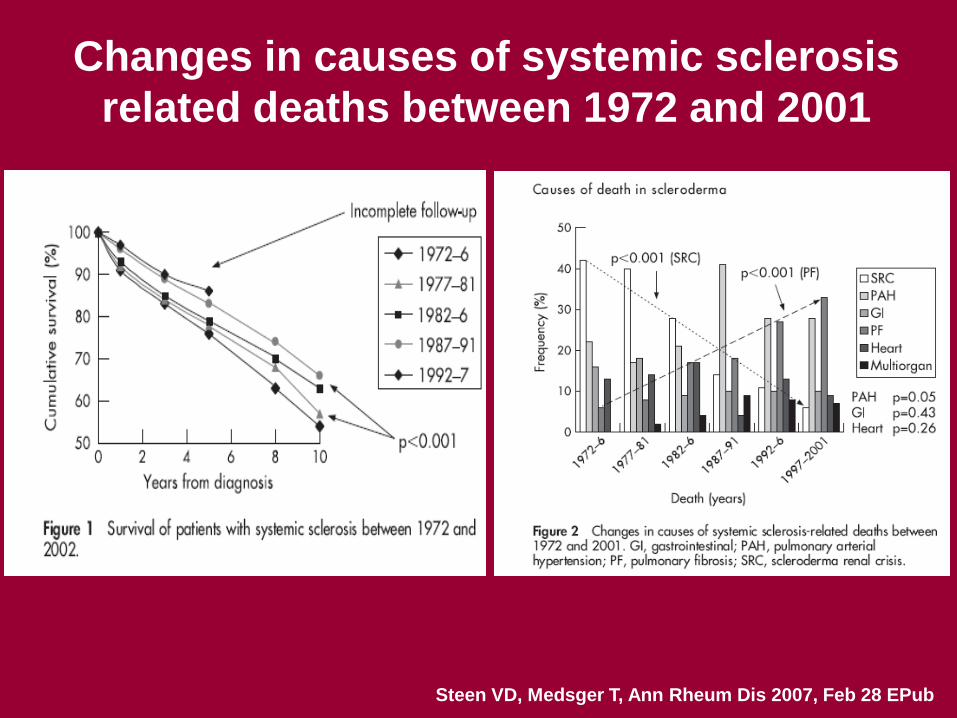
Changes in causes of systemic sclerosis
related deaths between 1972 and 2001
Steen VD, Medsger T, Ann Rheum Dis 2007, Feb 28 EPub
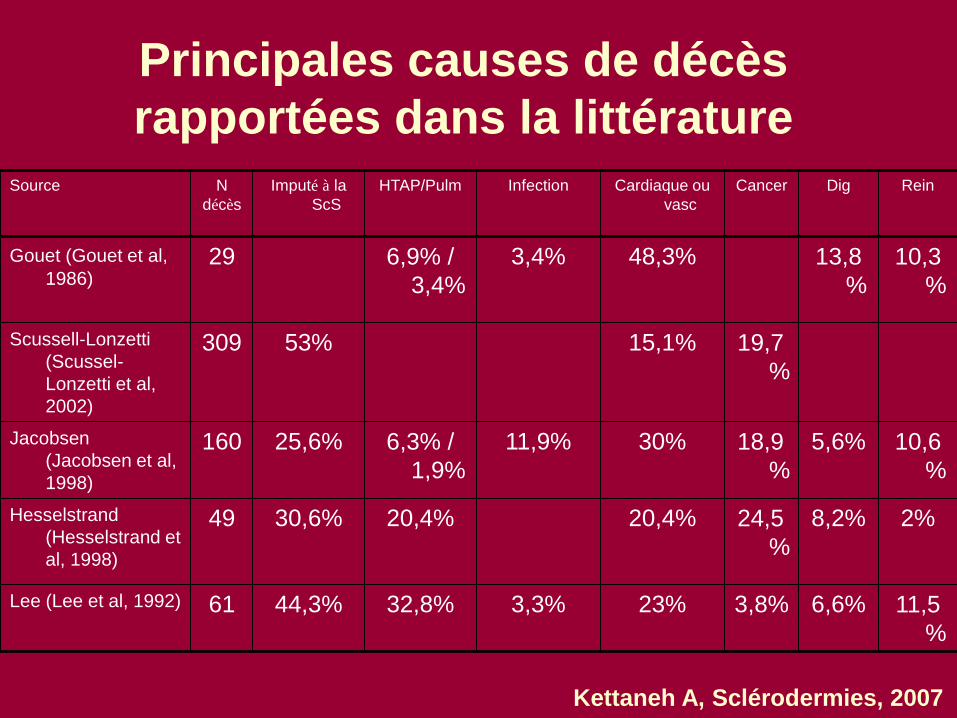
Principales causes de décès
rapportées dans la littérature
Source N
décès
Imputé à la
ScS
HTAP/Pulm Infection Cardiaque ou
vasc
Cancer Dig Rein
Gouet (Gouet et al,
1986) 29 6,9% /
3,4%
3,4% 48,3% 13,8
%
10,3
%
Scussell-Lonzetti
(Scussel-
Lonzetti et al,
2002)
309 53% 15,1% 19,7
%
Jacobsen
(Jacobsen et al,
1998)
160 25,6% 6,3% /
1,9%
11,9% 30% 18,9
%
5,6% 10,6
%
Hesselstrand
(Hesselstrand et
al, 1998)
49 30,6% 20,4% 20,4% 24,5
%
8,2% 2%
Lee (Lee et al, 1992) 61 44,3% 32,8% 3,3% 23% 3,8% 6,6% 11,5
%
Kettaneh A, Sclérodermies, 2007
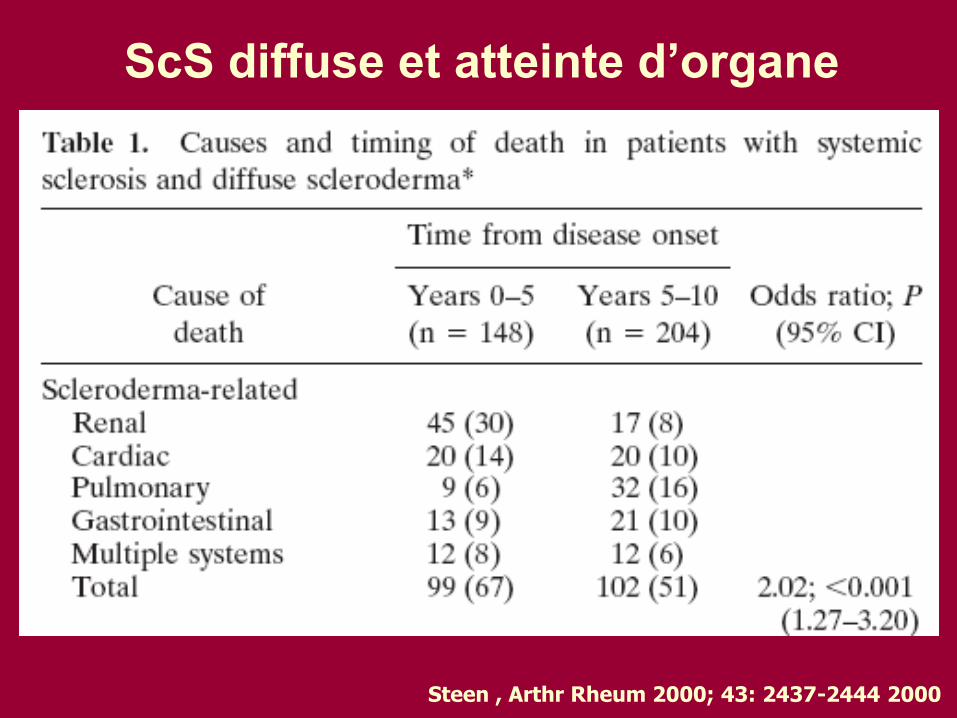
ScS diffuse et atteinte d’organe
Steen , Arthr Rheum 2000; 43: 2437-2444 2000
Autoanticorps
Survie à 10 ans des patients atteints de
ScS
- 93 % avec anticorps anticentromère
- 66 % avec Ac anti-Scl70
- 30 % chez les patients ayant des anti-
ARN polymérase.
Kuwana M, Arthritis Rheum 1994; 37: 75-83
Demographic and clinical factors associated
with in-hospital death among patients with
systemic sclerosis.
Data were obtained on all hospitalizations in South Carolina for patients who were ever hospitalized between 1996 and 2000 with a diagnosis of SSc.
Proportions of in-hospital deaths among blacks (23.0%) and others (27.7%) were higher than among whites (15.6%), a finding that remained after adjustment for other sociodemographic and clinical factors (black/white odds ratio: 1.70).
Black and other non-white patients with SSc appear to experience an elevated risk of death during their hospital stays.
Nietert PJ, J Rheumatol 2005
Race and association with disease manifestations and
mortality in scleroderma: a 20-year experience at the Johns
Hopkins Scleroderma Center and review of the literature (I).
Between 1990 and 2009, 409 African American and 1808 white patients with SSc were evaluated at a single university medical center.
African American patients presented to the center at a younger mean age than white patients (47 vs. 53 yr; p < 0.001).
Two-thirds of white patients manifested the limited cutaneous subset of disease, whereas the majority of African American patients manifested the diffuse cutaneous subset (p < 0.001).
The proportion seropositive for anticentromere antibody was nearly 3-fold greater among white patients, at 34%, compared to African American patients (12%; p < 0.001).
Nearly a third of African American (31%) patients had autoantibodies to topoisomerase, compared to 19% of white patients (p = 0.001).
Notably, African American patients experienced an increase in prevalence of cardiac (adjusted odds ratio [OR], 1.6; 95% confidence interval [CI], 1.3-2.2), renal (OR, 1.6; 95% CI, 1.2-2.1), digital ischemia (OR, 1.5; 95% CI, 1.4-2.2), muscle (OR, 1.7; 95% CI, 1.3-2.3), and restrictive lung (OR, 6.9; 95% CI, 5.1-9.4) disease.
Gelber AC et al, Medicine 2013
Race and association with disease manifestations and
mortality in scleroderma: a 20-year experience at the Johns
Hopkins Scleroderma Center and review of the literature (I).
• Overall, 700 (32%) patients died (159 African American; 541 white).
• Cumulative incidence of mortality at 10 years: 43% among African American patients vs 35% among white patients (log-rank p = 0.0011).
• Compared to white patients, African American patients experienced an 80% increase in risk of mortality (relative risk [RR], 1.8; 95% CI, 1.4-2.2), after adjustment for age at disease onset and disease duration.
• Adjustment by sex, disease subtype, SSc-specific autoantibody status, socioeconomic measures of educational attainment and health insurance status, diminished these risk estimates (RR, 1.3; 95% CI, 1.0-1.6).
• The heightened risk of mortality persisted in strata defined by age at disease onset, diffuse SSc, anticentromere seropositivity, decade of care at the center, and among women.
• These findings support the notion that race is related to a distinct phenotypic profile in scleroderma, and a more unfavorable prognosis among African Americans, warranting heightened diagnostic evaluation and vigilant care of these patients.
Gelber AC et al, Medicine 2013
Disease-related nutritional risk and mortality in systemic sclerosis
Single-centre prospective cohort study: 160 SSc patients (median age, 62 yr).
Nutritional risk assessed by the Malnutrition Universal Screening Tool (MUST), a screening tool that combines anthropometric parameters of nutritional status (body mass index [BMI] and percentage of unintentional weight loss [WL]) with the presence of an "acute disease" (disease activity score ≥3 according to Valentini's criteria).
Prevalence of high nutritional risk (MUST score ≥2): 24.4% [95%CI, 17.4-31.3].
Hazard analysis (median follow-up duration = 46 months [25th-75th percentile, 31-54]), high nutritional risk was significantly associated with mortality (HR = 8.3 [95%CI, 2.1-32.1]).
Performance of the model based on nutritional risk including disease activity (Harrell's c = 0.74 [95%CI, 0.59-0.89]) was superior to that based on active disease alone (HR = 6.3 [95%CI, 1.8-21.7]; Harrell's c = 0.68 [95%CI, 0.53-0.84]).
In SSc outpatients MUST significantly predicts mortality.
The combined assessment of nutritional parameters and disease activity significantly improves the evaluation of mortality risk.
Cereda E et al. Clin Nutr 2013
Pronostic en fonction du
type d’atteinte viscérale
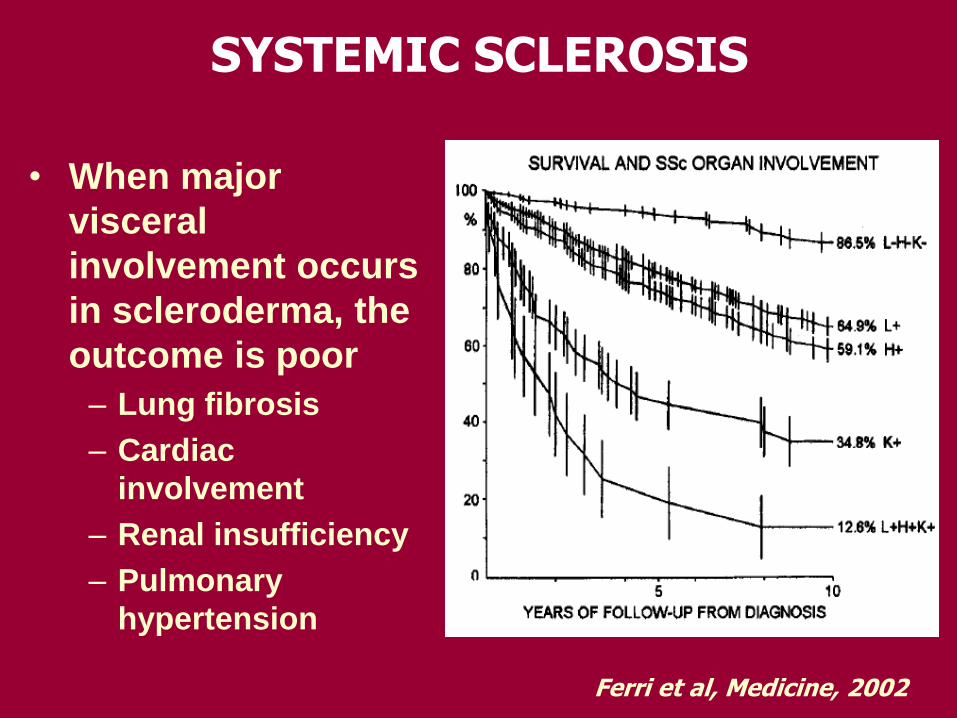
• When major
visceral
involvement occurs
in scleroderma, the
outcome is poor
– Lung fibrosis
– Cardiac
involvement
– Renal insufficiency
– Pulmonary
hypertension
SYSTEMIC SCLEROSIS
Ferri et al, Medicine, 2002
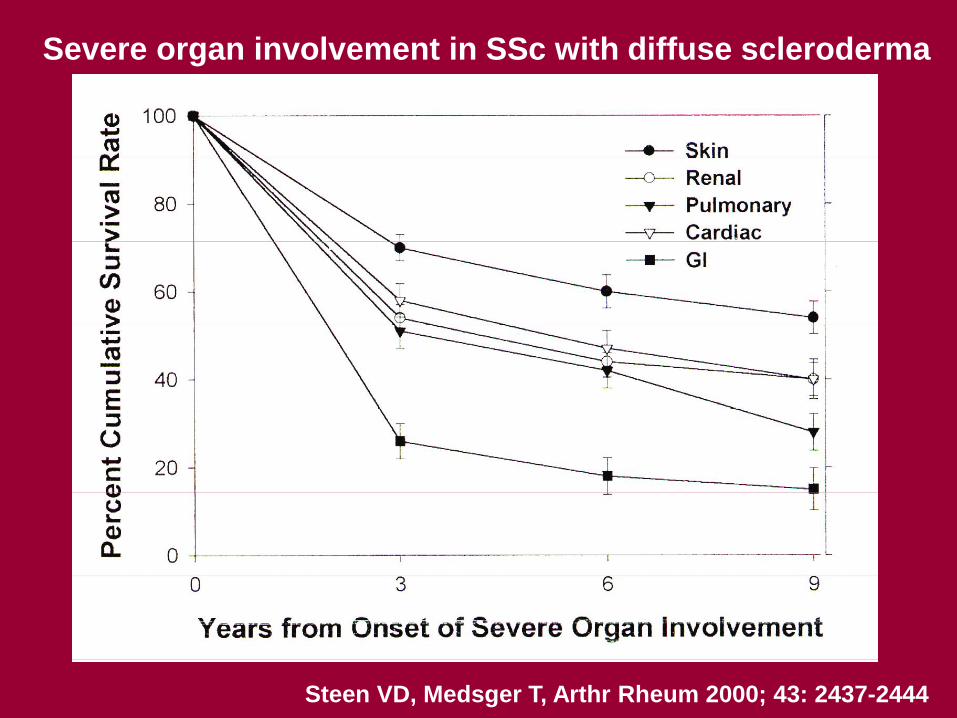
Severe organ involvement in SSc with diffuse scleroderma
Steen VD, Medsger T, Arthr Rheum 2000; 43: 2437-2444
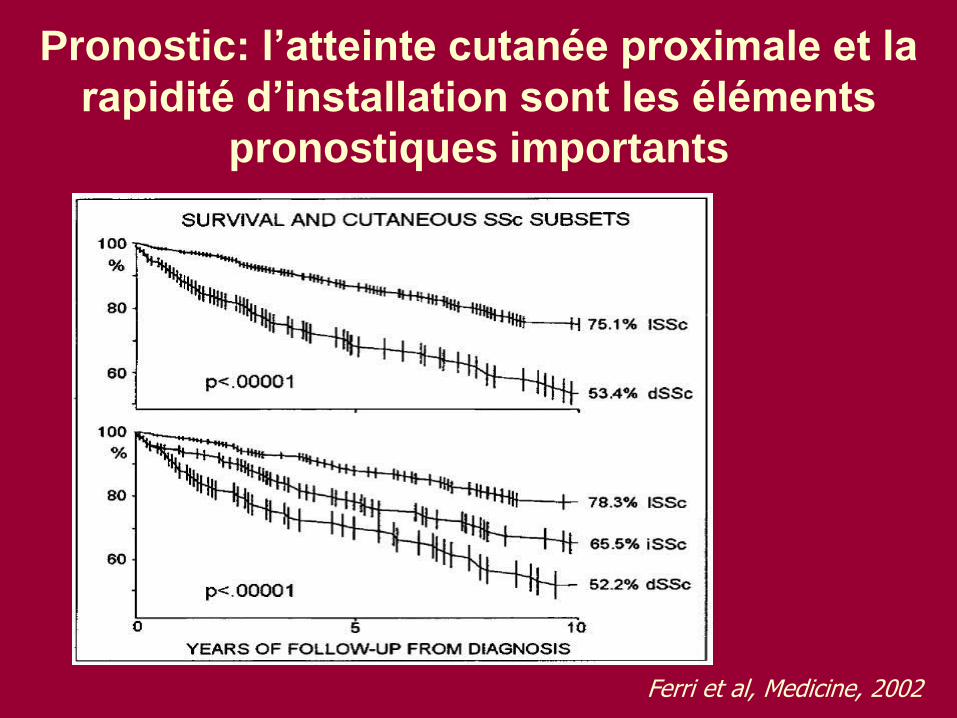
Pronostic: l’atteinte cutanée proximale et la
rapidité d’installation sont les éléments
pronostiques importants
Ferri et al, Medicine, 2002
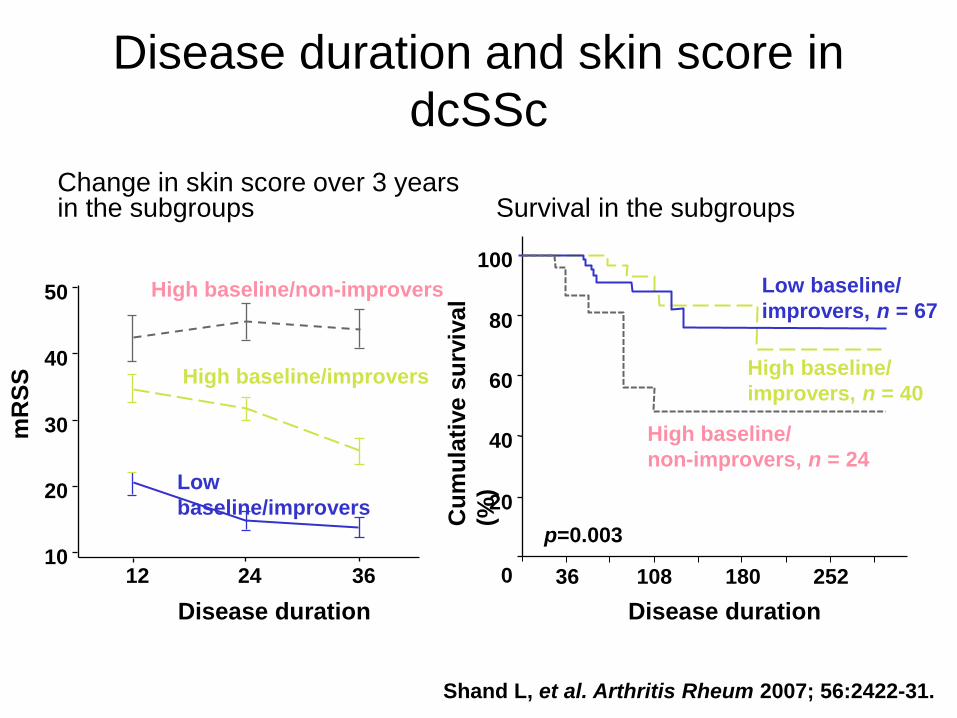
Shand L, et al. Arthritis Rheum 2007; 56:2422-31.
Disease duration and skin score in
dcSSc
Change in skin score over 3 years in the subgroups Survival in the subgroups
High baseline/improvers
Disease duration
12 24 36 10
20
30
40
50
Low
baseline/improvers
High baseline/non-improvers
mR
SS
High baseline/
improvers, n = 40
Low baseline/
improvers, n = 67
252 180 108 36 0
20
40
60
80
100
p=0.003
High baseline/
non-improvers, n = 24 C
um
ula
tive s
urv
ival
(%)
Disease duration
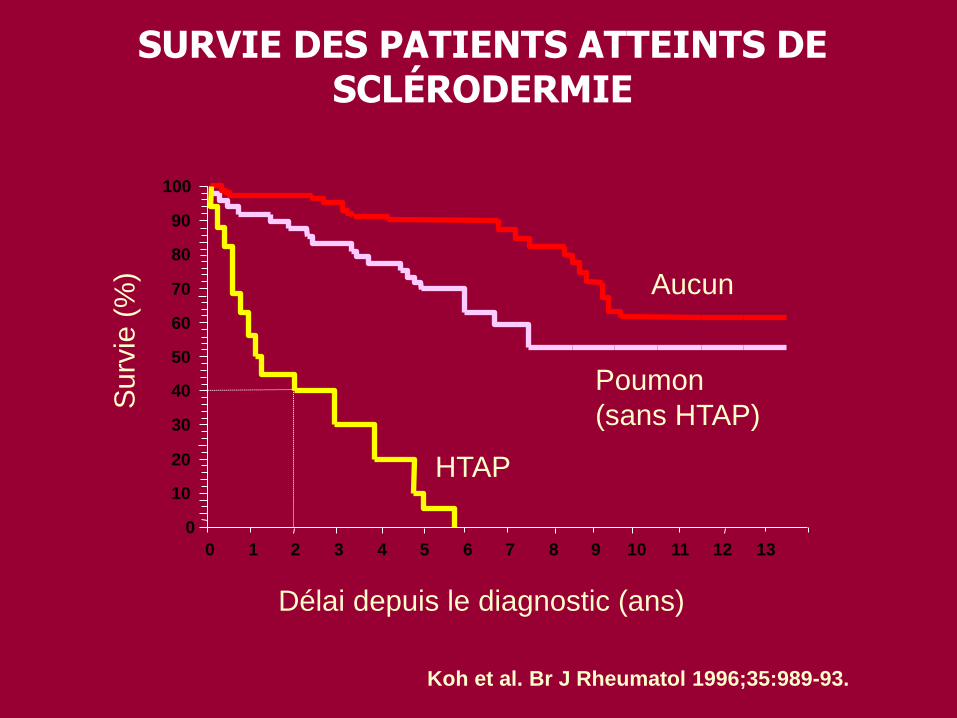
Koh et al. Br J Rheumatol 1996;35:989-93.
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13
Délai depuis le diagnostic (ans)
Surv
ie (
%)
HTAP
Poumon
(sans HTAP)
Aucun
SURVIE DES PATIENTS ATTEINTS DE SCLÉRODERMIE
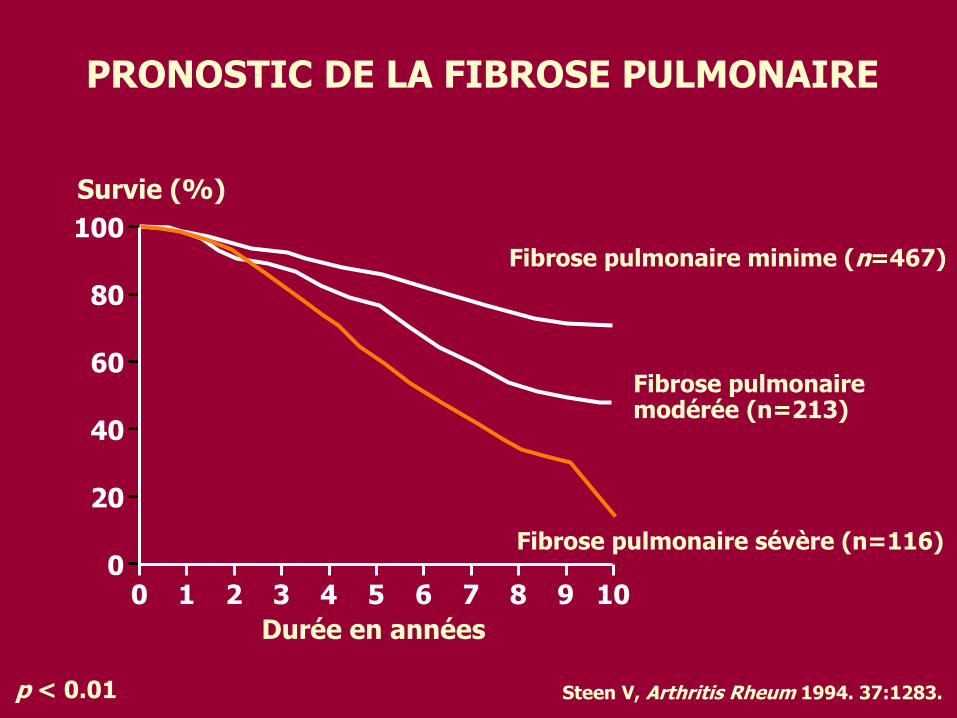
Steen V, Arthritis Rheum 1994. 37:1283.
PRONOSTIC DE LA FIBROSE PULMONAIRE
100
80
60
40
20
0 0 2 4 6 8 10
Durée en années
Survie (%)
1 3 5 7 9
Fibrose pulmonaire minime (n=467)
Fibrose pulmonaire modérée (n=213)
Fibrose pulmonaire sévère (n=116)
p < 0.01
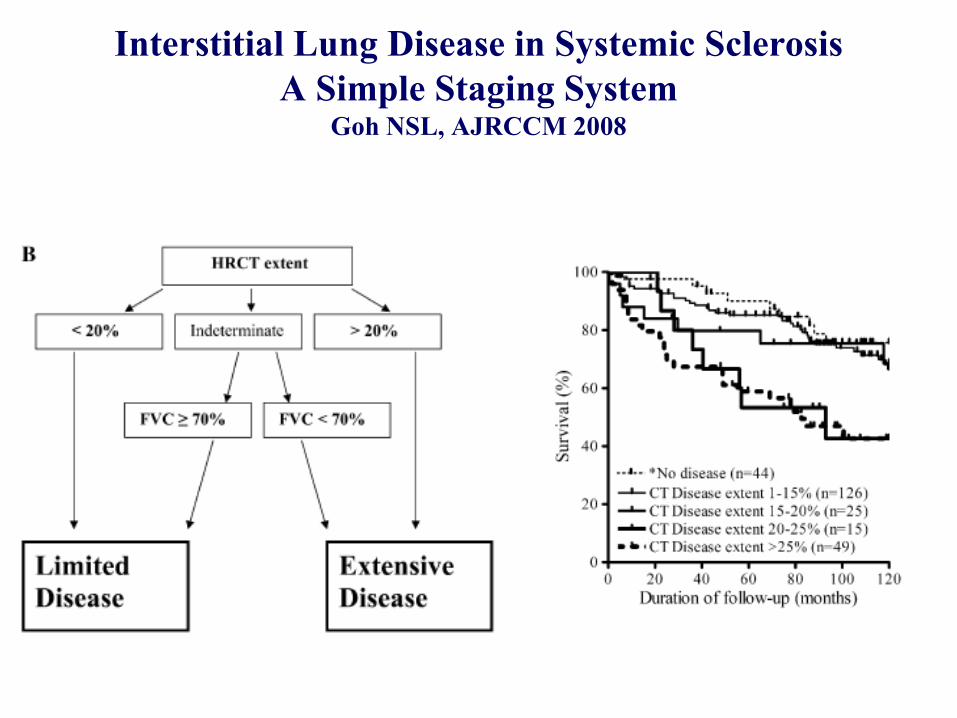
Interstitial Lung Disease in Systemic Sclerosis
A Simple Staging System Goh NSL, AJRCCM 2008
Pronostic de la PID Le pronostic des PID de la ScS est meilleur que celui de la fibrose pulmonaire idiopathique
Wells, AJRCCM 1994;149:1583-90
Race noire et asiatique, sexe masculin, atteinte cardiaque et les formes précoces de Scs sont le plus souvent associées à une forme sévère de PID (Jacobsen S et al. Clin Rheumatol 1997;16:384-90) mais ces données ne sont pas confirmées par d’autres études
Peters-golden M et al. Medicine 1984;63:221-31
Les principaux éléments permettant de définir le pronostic des PID associées à la ScS sont:
-PID d’emblée sévère
-PID rapidement progressive définie par une perte de 10% de CVF/CPT ou 15% de DLCO en 1 an
-Le type histologique de la PID n’a pas démontré de valeur pronostique au cours de la ScS
Bouros et al. AJRCCM
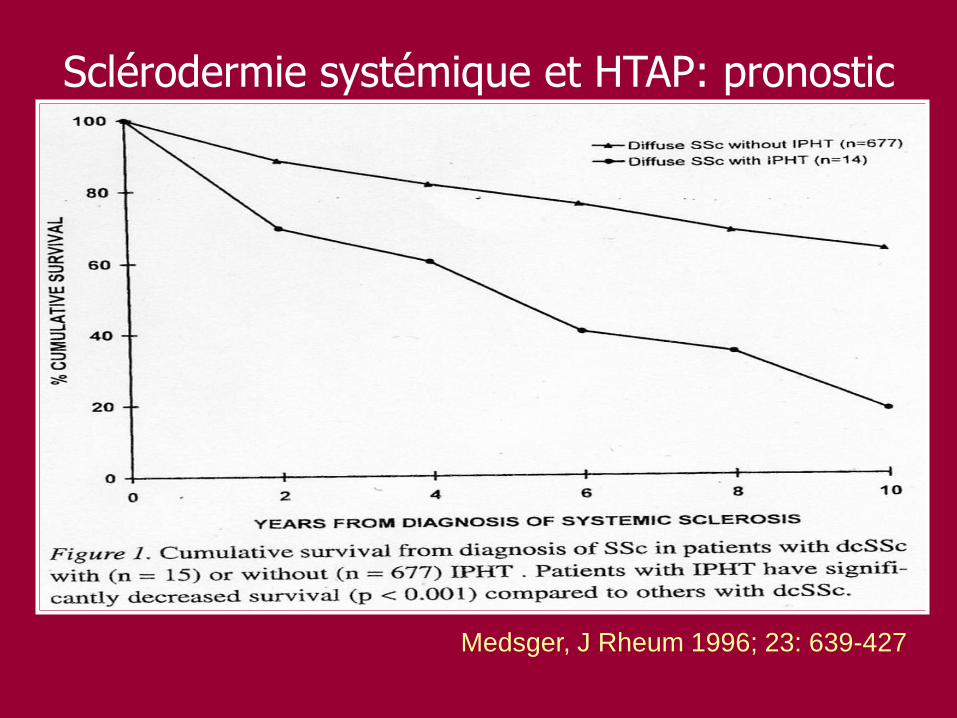
Medsger, J Rheum 1996; 23: 639-427
Sclérodermie systémique et HTAP: pronostic
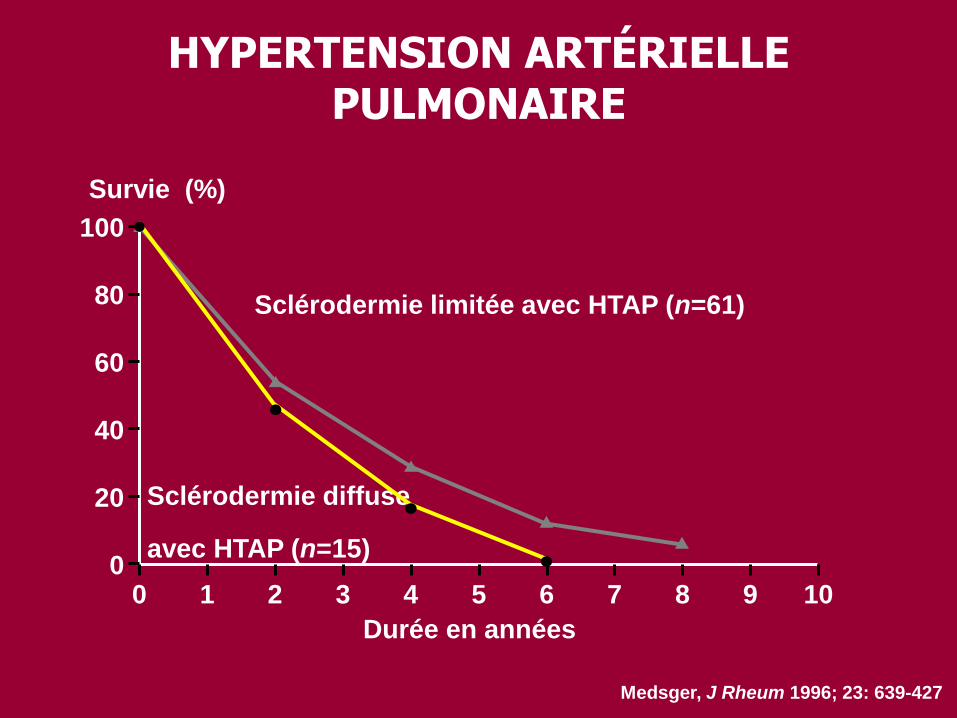
Medsger, J Rheum 1996; 23: 639-427
HYPERTENSION ARTÉRIELLE PULMONAIRE
100
80
60
40
20
0 0 2 4 6 8 10
Durée en années
Survie (%)
1 3 5 7 9
Sclérodermie limitée avec HTAP (n=61)
Sclérodermie diffuse
avec HTAP (n=15)
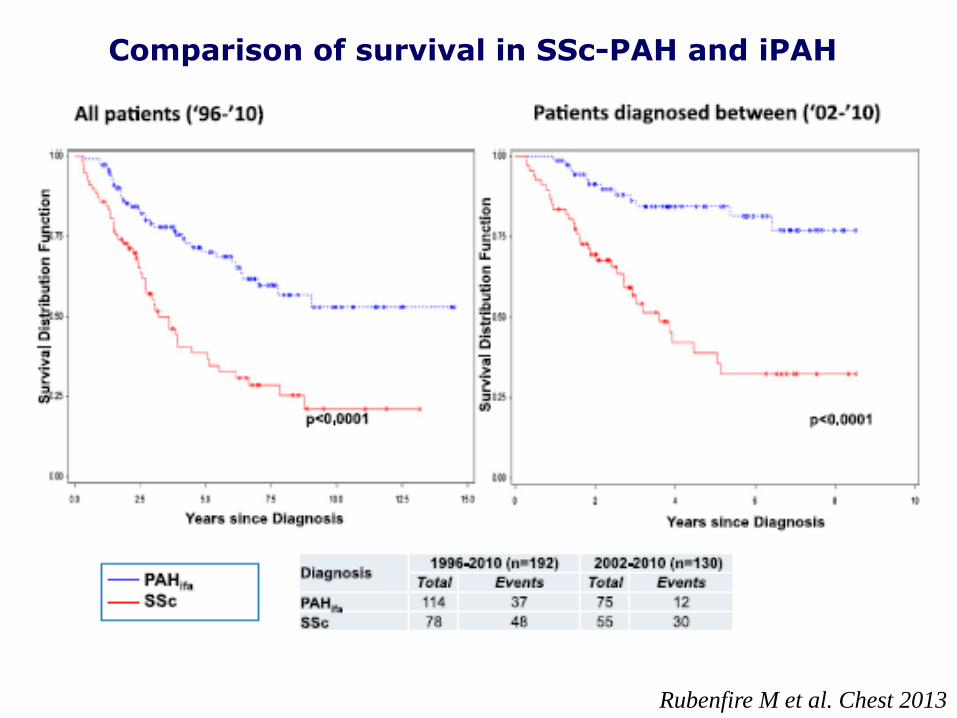
Comparison of survival in SSc-PAH and iPAH
Rubenfire M et al. Chest 2013
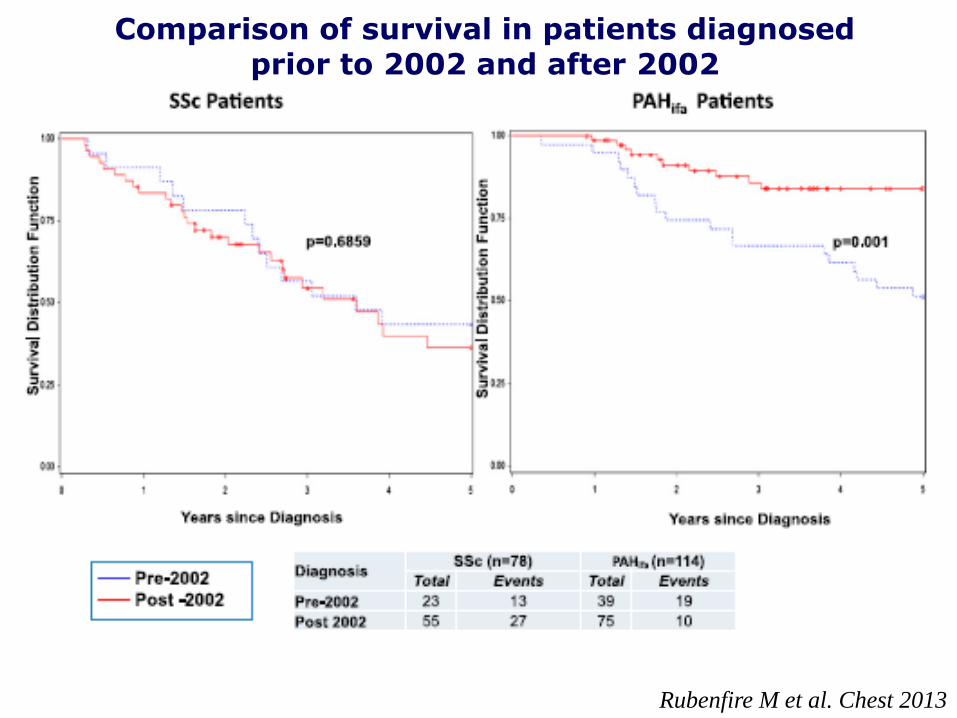
Comparison of survival in patients diagnosed prior to 2002 and after 2002
Rubenfire M et al. Chest 2013
3ème journée française de l’HTAP Paris – 20 et 21 Octobre 2005
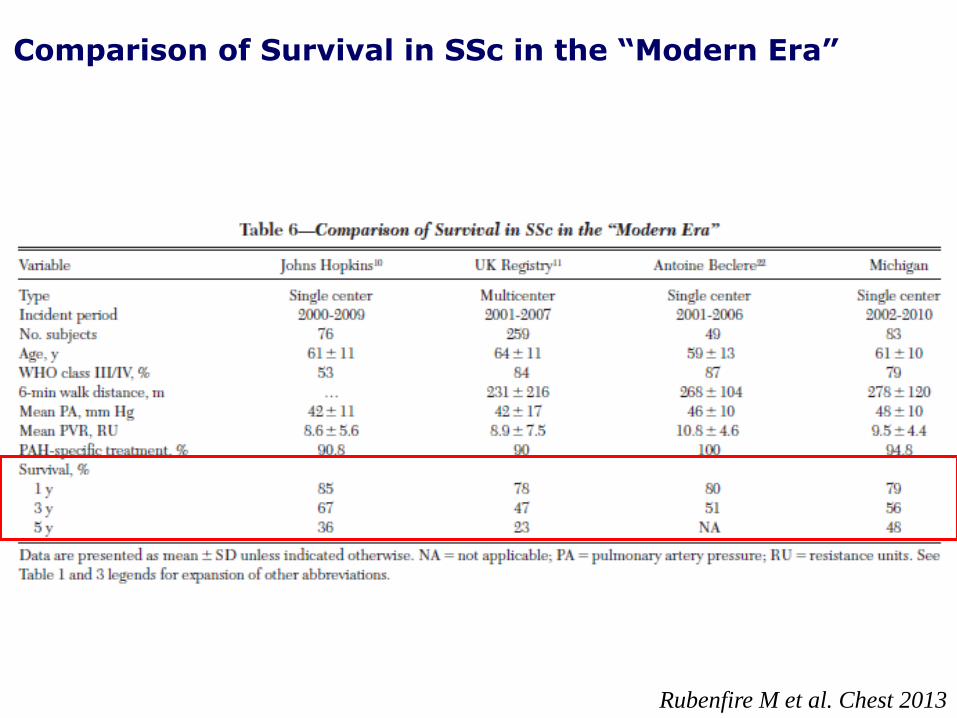
Comparison of Survival in SSc in the “Modern Era”
Rubenfire M et al. Chest 2013
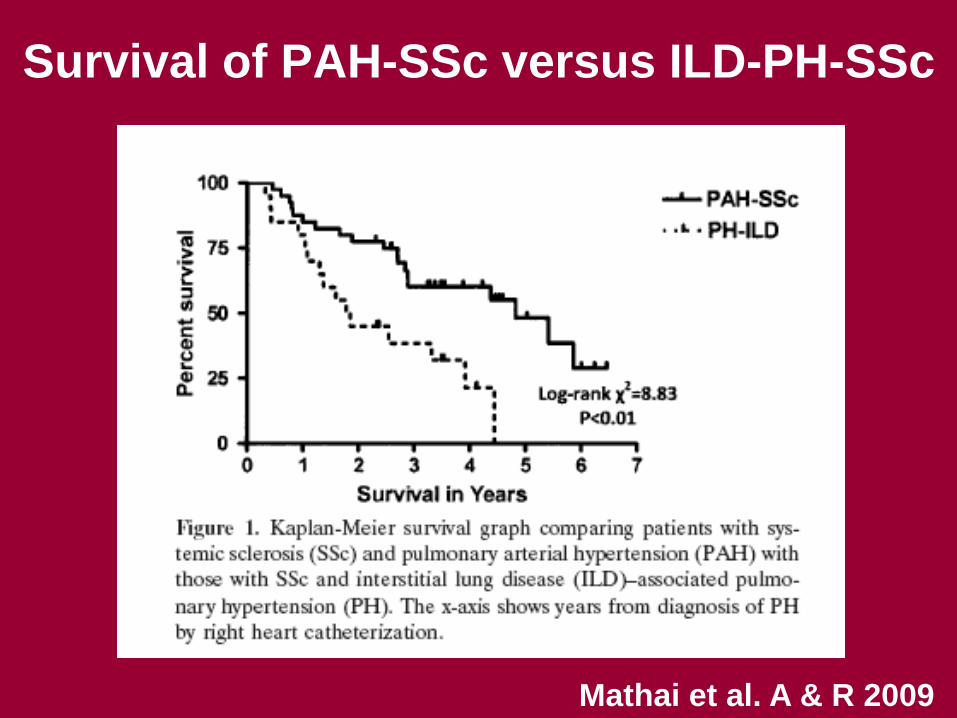
Survival of PAH-SSc versus ILD-PH-SSc
Mathai et al. A & R 2009
Outcomes in systemic sclerosis-related lung
disease after lung transplantation
• From 1998 to 2012, persons undergoing LT for SSc-LD were age and
gender matched in a 2:1 fashion to controls undergoing LT for nCTD-ILD.
• Survival was similar in 23 persons with SSc-LD and 46 controls who
underwent LT (P = 0.47).
• For the SSc-LD group, 1- and 5-year survival was 83% and 76% compared
with 91% and 64% in the nCTD-ILD group, respectively.
• There were no differences in bronchiolitis obliterans syndrome (P = 0.83).
Rates of acute rejection were less in SSc-ILD (P = 0.05).
• Esophageal dysfunction was not associated with worse outcomes (P>0.55).
• Persons with SSc-LD appear to have similar survival and bronchiolitis
obliterans syndrome as persons transplanted for nCTD-ILD. The risk of
acute rejection after transplantation may be reduced in persons with SSc-
LD. Esophageal involvement does not appear to impact outcomes.
Sottile PD et al. Transplantation 2013
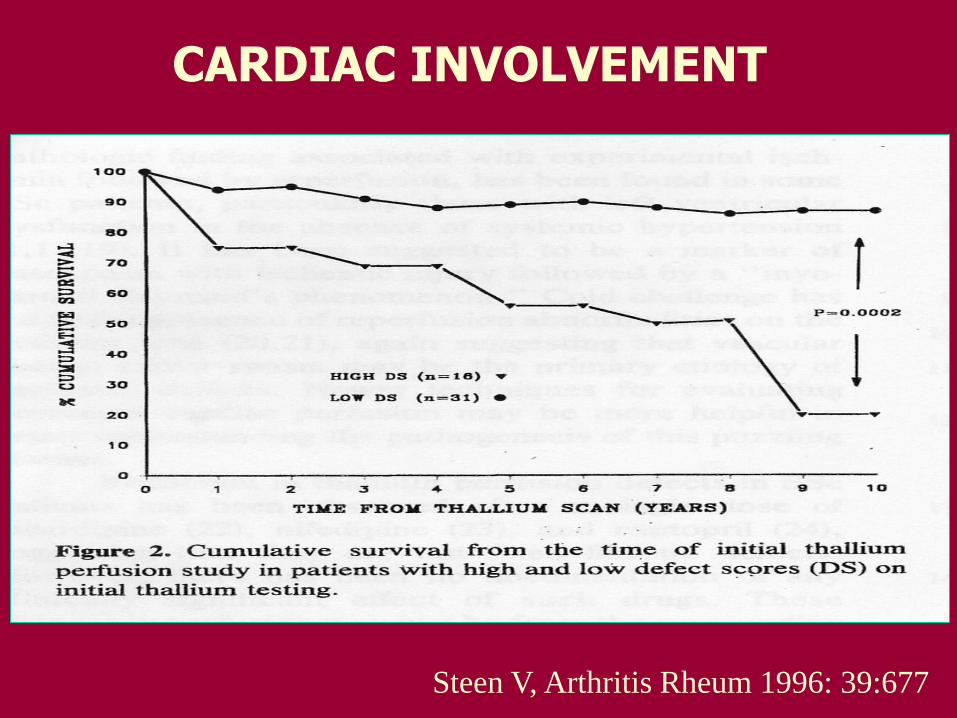
CARDIAC INVOLVEMENT
Steen V, Arthritis Rheum 1996: 39:677
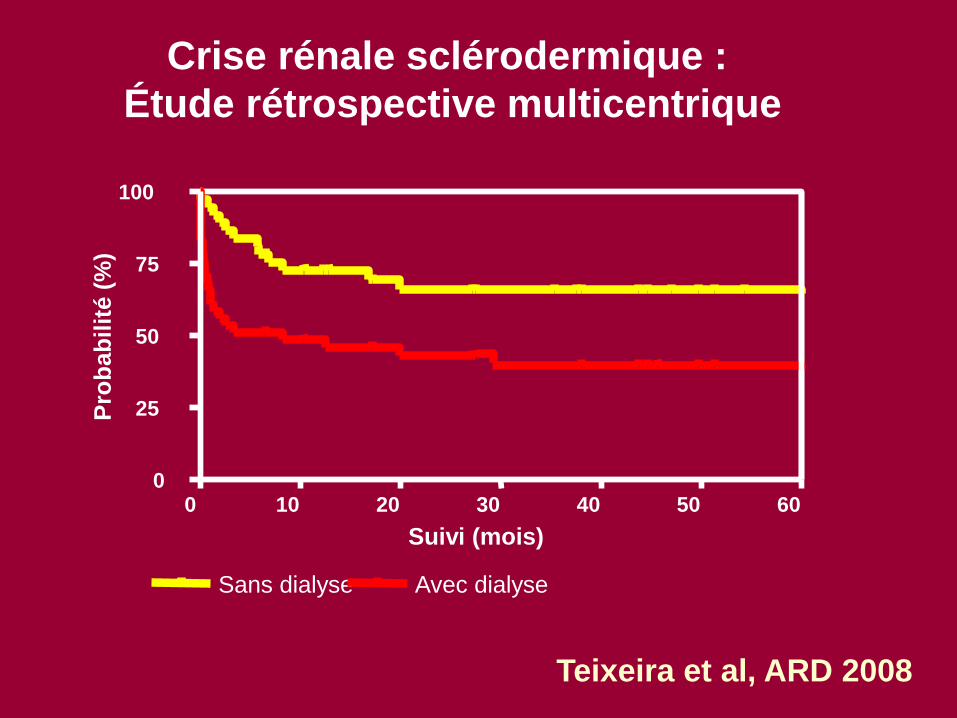
Crise rénale sclérodermique :
Étude rétrospective multicentrique
0 10 20 30 40 50 60 0
25
50
75
100
Sans dialyse Avec dialyse
Suivi (mois)
Pro
bab
ilit
é (
%)
Teixeira et al, ARD 2008
3ème journée française de l’HTAP Paris – 20 et 21 Octobre 2005
Factors predictive of renal crisis
Diffuse skin involvement
Rapid progression of skin thickening
Disease course < 4 years
Anti-RNA-polymerase III-antibodies
Newly manifested anaemia
Newly manifested cardiac involvement
Pericardial effusion
Heart insufficiency
Previous high-dose CS therapy
Steen VD. Am J Med 1984; 76:779-86.
Steen VD. Rheum Dis Clin North Am 2003; 29:315-33.
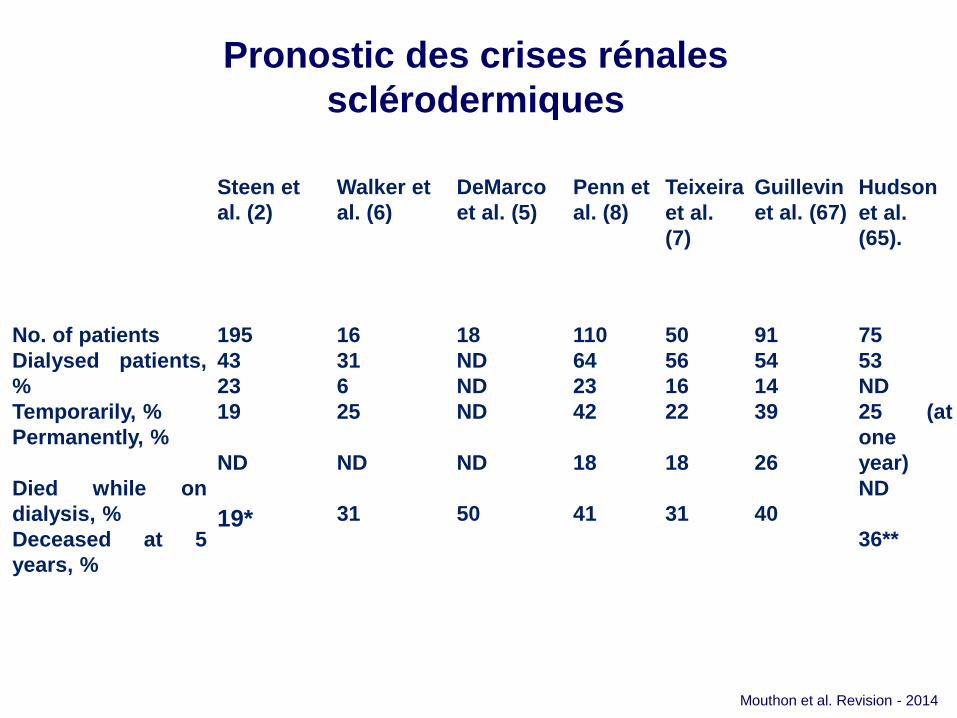
Pronostic des crises rénales
sclérodermiques
Steen et
al. (2)
Walker et
al. (6)
DeMarco
et al. (5)
Penn et
al. (8)
Teixeira
et al.
(7)
Guillevin
et al. (67)
Hudson
et al.
(65).
No. of patients
Dialysed patients,
%
Temporarily, %
Permanently, %
Died while on
dialysis, %
Deceased at 5
years, %
195
43
23
19
ND
19*
16
31
6
25
ND
31
18
ND
ND
ND
ND
50
110
64
23
42
18
41
50
56
16
22
18
31
91
54
14
39
26
40
75
53
ND
25 (at
one
year)
ND
36**
Mouthon et al. Revision - 2014
Mesure de l’activité de la
ScS
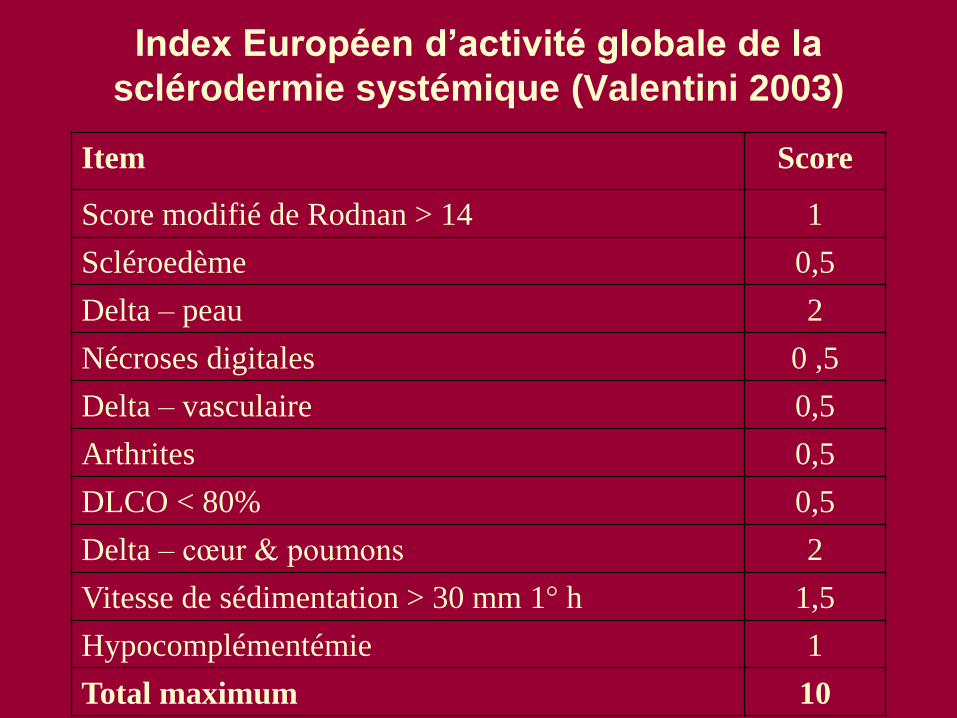
Index Européen d’activité globale de la
sclérodermie systémique (Valentini 2003)
Item Score
Score modifié de Rodnan > 14 1
Scléroedème 0,5
Delta – peau 2
Nécroses digitales 0 ,5
Delta – vasculaire 0,5
Arthrites 0,5
DLCO < 80% 0,5
Delta – cœur & poumons 2
Vitesse de sédimentation > 30 mm 1° h 1,5
Hypocomplémentémie 1
Total maximum 10

Organes Stade 0
(normal)
Stade 1
(discret)
Stade 2
(modéré)
Stade 3
(sévère)
Stade 4
(terminal)
Etat
général
Perte de poids
< 5%
Hématocrite >
37%
Hb > 12,2 g/dl
Perte de poids = 5
-10%
Hématocrite = 33 -
37%
Hb = 11 - 12,2 g/dl
Perte de poids =
10-15%
Hématocrite= 29-
32%
Hb = 9,7 – 10,9
g/dl
Perte de poids=
15-19%
Hématocrite = 25-
28%
Hb = 8,3-9,6 g/dl
Perte de poids
>20%
Hématocrite <
25%
Hb < 8,3 g/dl
Vasculaire
périphé
rique
Raynaud absent
ou ne
requérant
pas de
traitement
Raynaud requérant
un traitement
vasodilatateur
Cicatrices
pulpaires
ponctuelles
Ulcérations
digitales
Gangrène
digitale
Peau Score de
Rodnan
modifié = 0
Score de Rodnan
modifié = 1-14
Score de Rodnan
modifié = 15-
29
Score de Rodnan
modifié = 30-
39
Score de
Rodnan
modifié >
40
Articulation
s et
tendon
s
Distance index-
paume <
0,9 cm
Distance index-
paume = 1 -1,9
cm
Distance index-
paume = 2-3,9
cm
Distance index-
paume = 4 –
4,9 cm
Distance index-
paume > 5
cm
Muscles Force
musculaire
proximale
normale
Force musculaire
proximale peu
altérée
Faiblesse
musculaire
proximale
modérée
Faiblesse
musculaire
proximale
sévère
Nécessité
d’aides
pour
déambuler
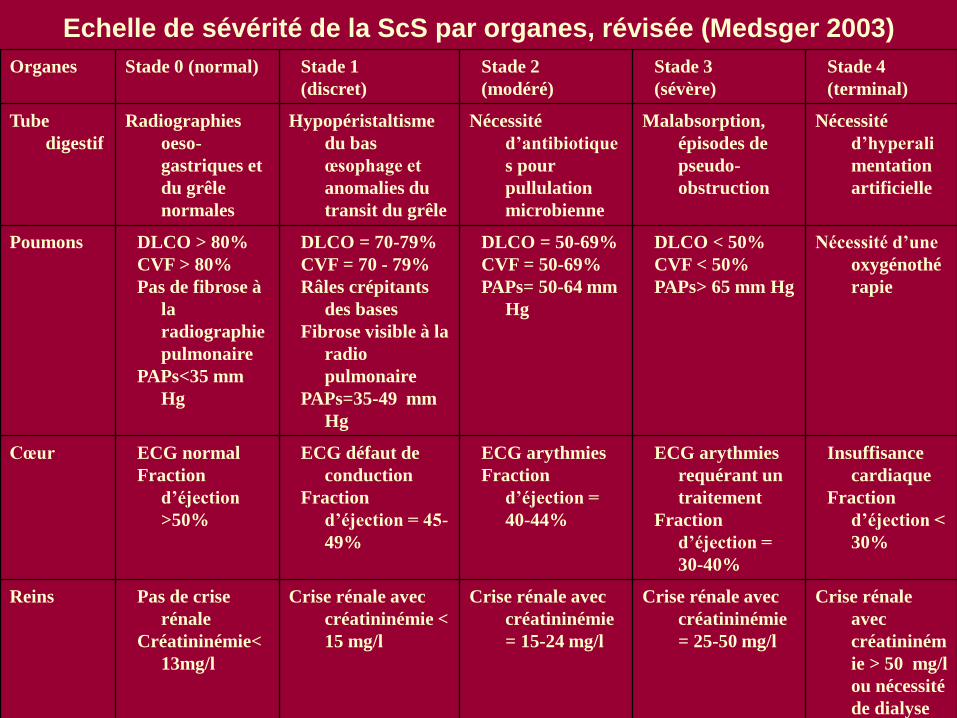
Echelle de sévérité de la ScS par organes, révisée (Medsger 2003)
Echelle de sévérité de la ScS par organes, révisée (Medsger 2003)
Organes Stade 0 (normal) Stade 1
(discret)
Stade 2
(modéré)
Stade 3
(sévère)
Stade 4
(terminal)
Tube
digestif
Radiographies
oeso-
gastriques et
du grêle
normales
Hypopéristaltisme
du bas
œsophage et
anomalies du
transit du grêle
Nécessité
d’antibiotique
s pour
pullulation
microbienne
Malabsorption,
épisodes de
pseudo-
obstruction
Nécessité
d’hyperali
mentation
artificielle
Poumons DLCO > 80%
CVF > 80%
Pas de fibrose à
la
radiographie
pulmonaire
PAPs<35 mm
Hg
DLCO = 70-79%
CVF = 70 - 79%
Râles crépitants
des bases
Fibrose visible à la
radio
pulmonaire
PAPs=35-49 mm
Hg
DLCO = 50-69%
CVF = 50-69%
PAPs= 50-64 mm
Hg
DLCO < 50%
CVF < 50%
PAPs> 65 mm Hg
Nécessité d’une
oxygénothé
rapie
Cœur ECG normal
Fraction
d’éjection
>50%
ECG défaut de
conduction
Fraction
d’éjection = 45-
49%
ECG arythmies
Fraction
d’éjection =
40-44%
ECG arythmies
requérant un
traitement
Fraction
d’éjection =
30-40%
Insuffisance
cardiaque
Fraction
d’éjection <
30%
Reins Pas de crise
rénale
Créatininémie<
13mg/l
Crise rénale avec
créatininémie <
15 mg/l
Crise rénale avec
créatininémie
= 15-24 mg/l
Crise rénale avec
créatininémie
= 25-50 mg/l
Crise rénale
avec
créatininém
ie > 50 mg/l
ou nécessité
de dialyse







