
Report - Internship in a Community Pharmacy
Student Exchange program
Apotheek Born
02/10/2016 – 31/10/2016
Kristína Krajčovičová
5th year of study, practical training
Faculty of Pharmacy, Comenius University, Bratislava, Slovakia
2th October 2016 – Sunday
The day of my arrival from belgian city Mons (where I have done 2 months of my intenship
in a community Pharmacy) to Sittard station. I had a short stay (only for few hours) in
Maastricht and than I retook direct train to Sittard where Mr. Sikkes have been already
waiting. Firstly, we went wind-surfing on belgian lake near borders (me, I was only
observing) and then we arrived home.
3th October 2016 - Monday
Meeting with a doctor
My first task in a Pharmacy was to look at the medical history of few patients. We had 5
patients whose treatement we needed to discuss with their generalist. It consists of elderly
patients with more than 5 medecines. According to their medical history of the last year and
their health problems, we were searching for interactions, contraindications, overdosing,
duplicitating of medecines or other therapeutical problems.
My responsibility was, at first to class molecules according to their ATC groups and to
prepare my questions.
I could see how NCARE system works (the system which shows interactions, CI or missing
thearapy)
Examples of problems, questions:
Elderly patients without supplement of vit. D
ACE-inhibitor + codeine – Does the patient suffer froma dry cough? No, codeine was
prescribed as a pain-killer.
Doxisosine + B-blocator – Doesn´t the patient posses some problems because of this
combination?
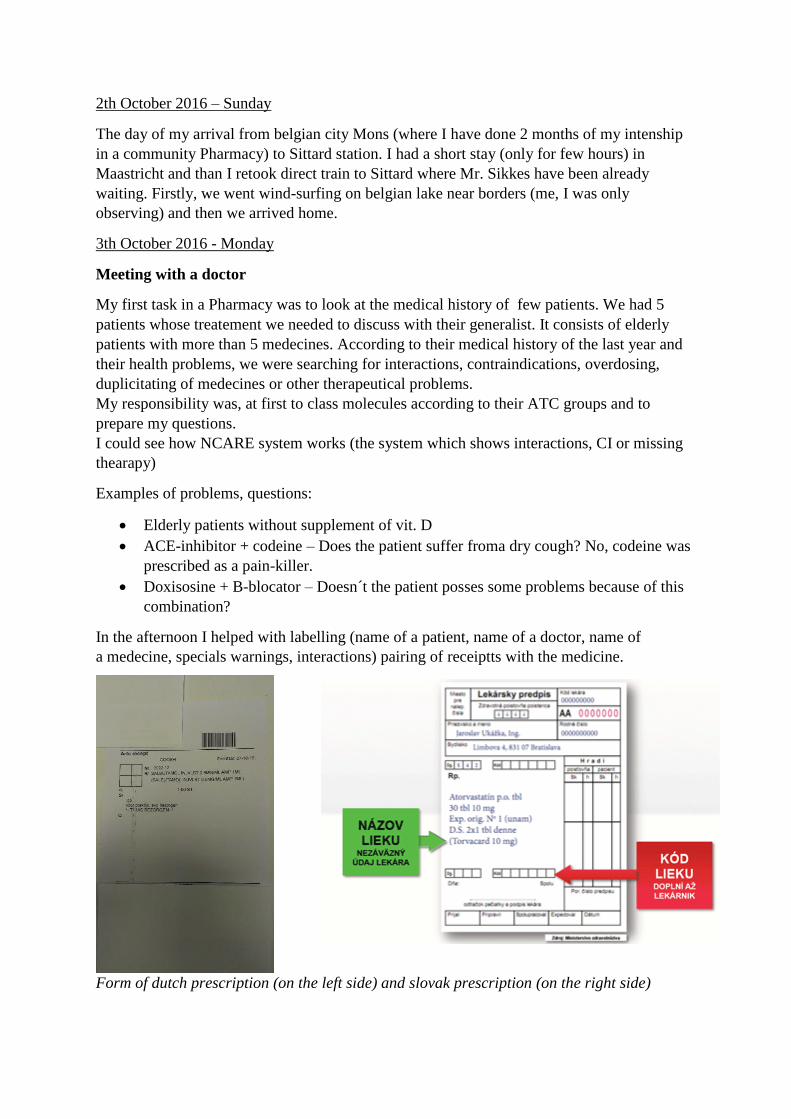
In the afternoon I helped with labelling (name of a patient, name of a doctor, name of
a medecine, specials warnings, interactions) pairing of receiptts with the medicine.
Form of dutch prescription (on the left side) and slovak prescription (on the right side)

At the end of my first day, I controlled dosage and drug interactions with Mr. Sikkes
(especially methotrexate - 1x/week, at once take).
And after work, short bike trip in the surronding
4th October 2016 - Tuesday
Introduction to the work in the Pharmacy
Rossetta explained me the system of work in a Pharmacy – how the receipt looks like, what
is „smart filling“, 2 possibilities of receiving receiptt – in printed version from a patient or by
electronic system, what we need to control, the system of ranging the medicines, how to pair
medecine with the receipt and required control of prepared treatement for a patient. There is
at least double control – the first one during choosing the right medecine (according to the
prescription). The last step before delivering the medicine to the patient is the packing or
preparing for blister. Patients can come to take their treatement at the Pharmacy , at the
branch Pharmacy or their is also the possibility of delivering medicine at home (manly for
elderly patients).
When the new therapy is on, the first time, patient is well informed about taking the
medicine. The second time, he receive the questionnary and is asked if he observes any
problem during treatement.
With Rossetta we went to Grevenbicht where I´ve been also solving therapeutical problem of
a patient, man of 53 years old who has a problem with cold hands, muscle stiffness. His
treatement conssist of: pantoprolol, clopidogrel, ASA, metoprolol, perindopril and
simvastatine. According do SPC, we concluded that metoprolol as B-bloc. can be responsible
for cold hands and simvastatine can cause muscle stiffness (undesired effect - myalgia).
In the afternoon, Nastacha explained me the system of ordering, preparaing received orders
for smart filling. They received one order every day in the early morning (once per day) – in
contrast with Slovakia, where the most of pharmacies received their orders 3 or more times
per day. I learnt more about using the information system in the Pharmacy – where to control
the location of a medicine, how to control the stocks, how to print PIL etc.
For received derivates of opium, it is necessary to control the number of received products,
sign the document of incomming opioids and control the stocks of these products.
I helped with delivering of the medecines in a branch Pharmacy.
With Mr. Sikkes, we discussed what the parallel export means, what the grossery must do
before libere these medicines to trade (change PIL into official language and translate outer
package of a medicine by sticking a label on it).

Kind of a stick English translation
To stock in a fridge
Do not swallow
Inhalation by mouth/ nose
Eye drops
May influence your reaction time
Shake before use
To deliver at home
Opium receipt
To Obbicht (branch Pharmacy)
Therapeutic education needed
Blister is necessary
First use
To use 1 month after openning

Ask us for help, advice
5th October 2016 – Wednesday
In the morning, I helped assistants with arranging received order, controlling the stock of
opium drugs and put them on their place. I also labelled medicines, controlled rightness of the
dosage and strength.
Afterwards, I had a preparation to do.
Preparation
Antiepileptic capsules
Phenobarbitalum 22,48 g
Phenytoinum 30,00 g
Cellulosum micro 43,02 g
D.t.d. No 300
Capsules No 0 were used.
I participated on a meeting in the Pharmacy – main themes that were discussed – how to get
more people on smart filling? Note always the dosage on a label. etc.
Searching information about some molecules/ medicines:
Levetiracetam
anticonvulsant
Dulaglitid
= oral antidiabetic
It is a GLP1 receptor agonist. Dulaglutide has been shown to cause thyroid cancer in rats.
Tafluprost
Is used for treatement of increased pressure in eye (ocular hypertension), open angle glaucoma.
It is an analog of PG.
Mebeverine
= anticholinergic
Indication: irritable bowel syndrome, chronic irritable colon, spastic constipation, mucous colitis. It is
a musculotropic antispasmodic with a direct action on the smooth muscle of GIT, without affecting
normal gut motility.
At the end of this day, we played tennis (me, I tried to play) with Mr. Sikkes and his friends.
6th October 2016 – Thursday
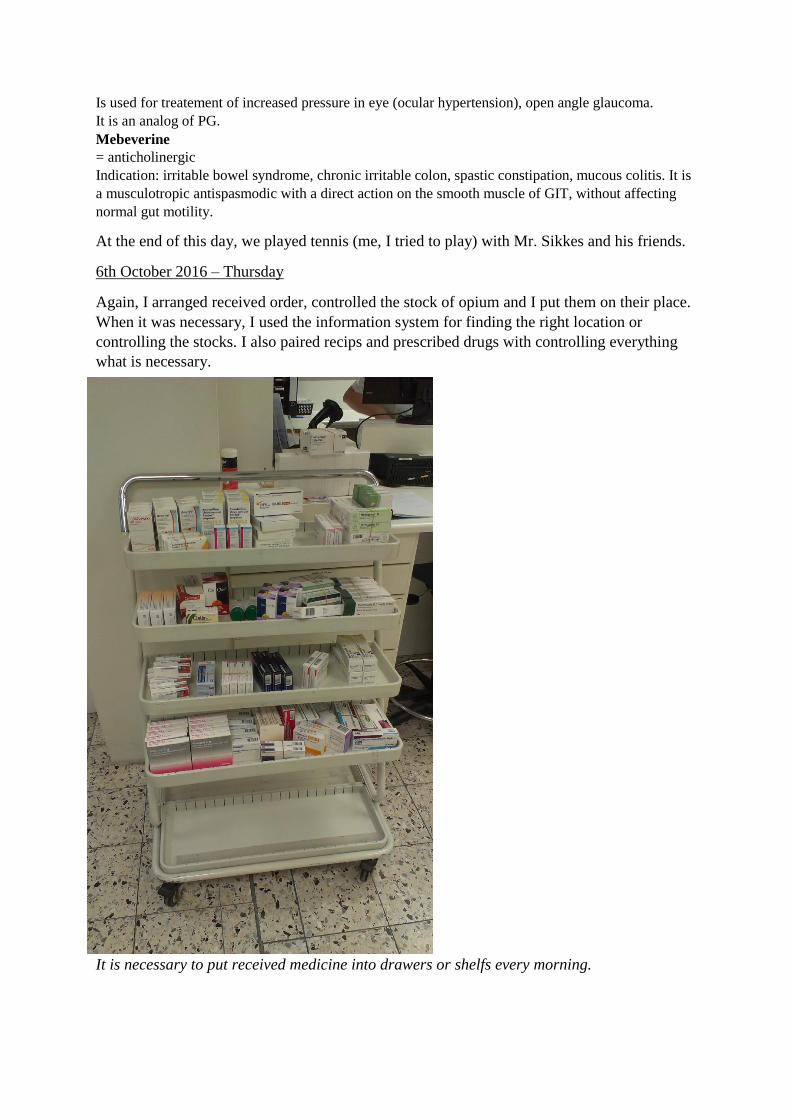
Again, I arranged received order, controlled the stock of opium and I put them on their place.
When it was necessary, I used the information system for finding the right location or
controlling the stocks. I also paired recips and prescribed drugs with controlling everything
what is necessary.
It is necessary to put received medicine into drawers or shelfs every morning.

Searching for information:
Sulfametazoltrimetoprim = Bactrimel
It´s an antibiotic, combination of sulfamethoxazole which block. Synth. Of dihydrofolic acid
by competing with PABA, and trimethoprim that reversibly inhibate dihydrofolate reductase,
whch produce tetrahydrofolic acid from dihydrofolic acid.
This combination is used for:
Urinary tract infections
Acute otitis media
Acute exacerbations of chronic bronchitide in adults
Shigellosis
Pneumonia
Traveler´s diarrhea in adults
Mupirocine = Bactroban (creme)
It´s an ATB that acts by inhibiting of synthesis of bact. Prot. – by reversibly and specifically
binding to bacterial isoleucyl-transfer RNA synthetase. Mupirocine is used again infections
caused by S. Aureus, S. Pyrogenes.
Hydroxychloroquine sulfate = Plaquenil
Has an antimalarial action – Plasmodium vivax, P. Malariae, P. Ovale, P. Falciparium. Is
used against lupus erythematosus, rheumatoid arthritis.
Bupropion
It´s an antidepressant. Inhibits re-uptake of NAD and DOP without inhib. Of 5-HT re-uptake.
Mycophenolat mofetil
Is an immunosupressant that is used to prevent organ rejection after transplantation – kidney,
liver, heart.
7th October 2016
Participation at doctor assistants´ lesson and visit in Pharmacy assistants´s practical lab
With Mr. Sikkes, I participated at the lesson talking about pain killers – their classement,
dossage, side effects, CI
1) Non-opioid
a) Paracetamol group
Paracetamol 500mg
Normal dosage: 3x/day
Max dosage: 4x/day 2 tbl
<2 weeks without medical advice
b) NSAID group
ASA
Diclofenac
Ibuprofen
Naproxen
c) Opioid
The most of the afternoon, I spent by labelling of drugs.

Preaparing medicines for their delivery to patients – according to the receipt, typers had to
choose the right medicine (preference of inssurance), strength and then print labels. Labels
are than sticked at the packages (the cross on a pachage means, that this package has been
already open). The choice of right medicine is controlled by computer system.
At the end of the day, I controlled medical prescription – right datas, right molecule, right
strength.
Flucloxaciline
Peniciline ATB
Carbasolatcalcium
NSAID
Mercaptopurine
Is used in a treatement of acute lymphatic leukemia. Competes with G and hypoxanthin for
HGPRTase.
11th October – Saturday
This was my first week-end in Holland, so I decided to visite the city Valkenburg and to get
there typicly dutch – by bike. The landscape was beautiful, bit hilly, sun was shinning, no
rain, I walked in Valkenburg and drank a tea on a terrace.
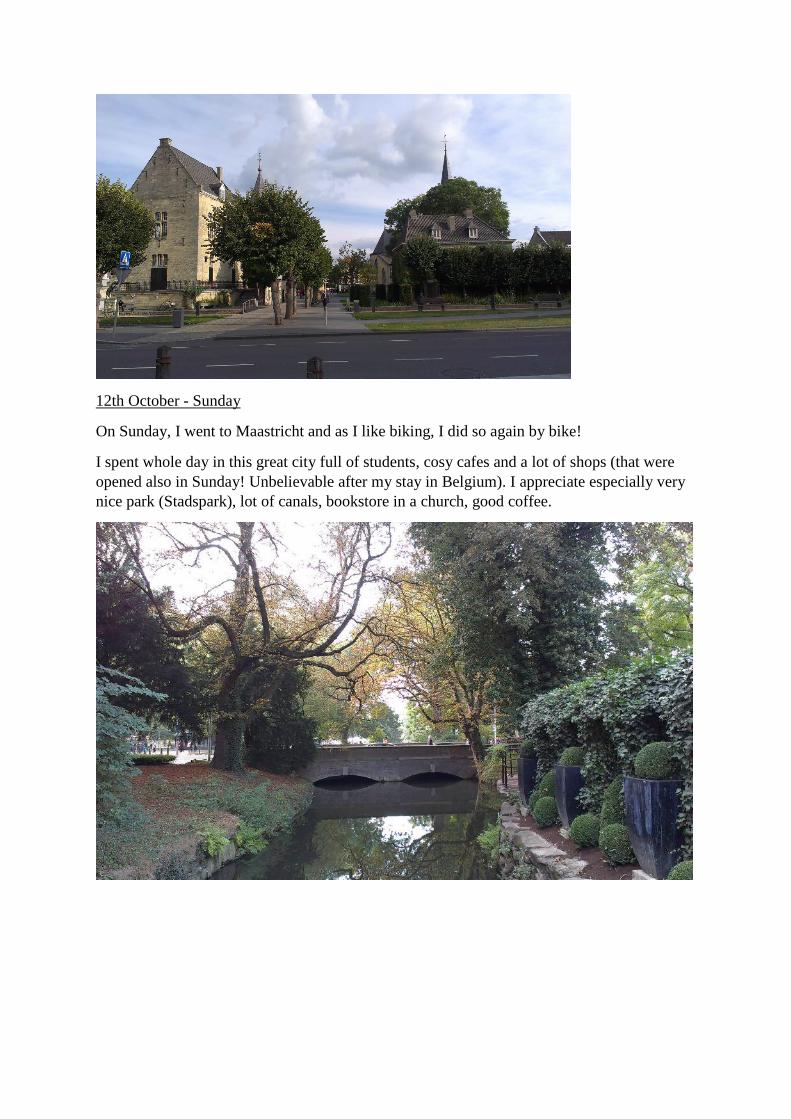
12th October - Sunday
On Sunday, I went to Maastricht and as I like biking, I did so again by bike!
I spent whole day in this great city full of students, cosy cafes and a lot of shops (that were
opened also in Sunday! Unbelievable after my stay in Belgium). I appreciate especially very
nice park (Stadspark), lot of canals, bookstore in a church, good coffee.
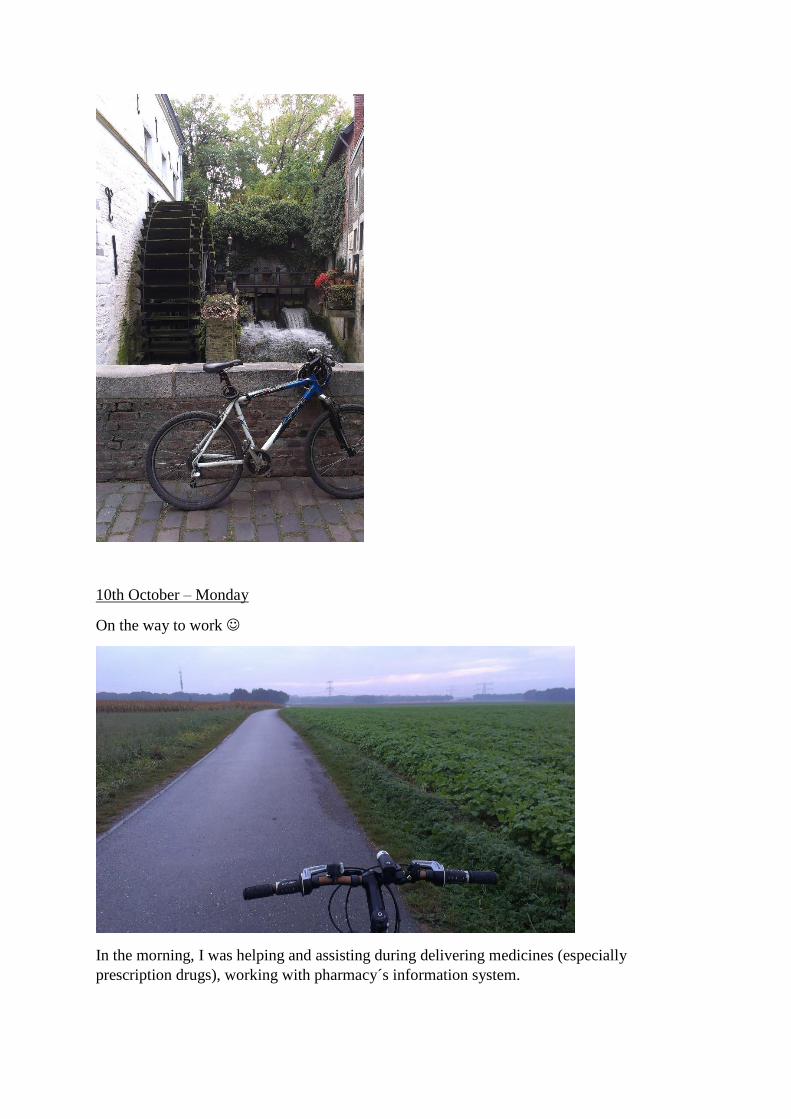
10th October – Monday
On the way to work
In the morning, I was helping and assisting during delivering medicines (especially
prescription drugs), working with pharmacy´s information system.
I was seeking for information about glycopyrronium – the doctor prescribed glycopyronnium
against excessive sweating (hyperhydrosis/polyhydrosis/sudorrhea), this indication is not
mentioned in a PIL – patient asked us if he nevertheless can take this medicine.
Glycopyrronium (oral tablets)
It is an anticholinergic (antimuscarinic) agent that exerts its mode of action by
competitive antagonismof ACh at postagnglionic cholinergic nerves.
According to EMA, glyccopyronium is not indicated in case of hyperhydrosis
UK – „There is weak evidence from case series that oral glyccopyronium bromide
tablets reduce sweating in people with hyperhydrosis. Hyperhydrosis responded to
oral glycopyrronium bromide tablets in 67%-90% of participants.“
FDA – Robinul (R) 5g powder for solution for Iontophoresis is used for the
treatement of excessive sweating. This is the only form of glycoppyronium, registred
in USA, which is indicated for this desease. No oral tablets regestrated for this
purpose.
Conclusion: Treatement of hyperhydrosis is an off label use of glycopyrronium.
I familirisated with a protocol that is required for patients who takes NSAID regullary – by
answering at questions, patient gain the score, behalf of the score, the additional treatement
with bloc. H+ pump can be recommended (score >3).
Filled document and total score.
During helping with delivering medicines, Yvonne told me more about advices that should be
given to a patient using hydrocortisone+miconazole creme – for 2 weeks, than continue only
with miconazol for next 1 week (eradication of mycosis without steroid hormone).
Another new information for me: during taking of nitrofurantoin – the color of urine can be
changed (because of the metabolit that is libere into the urine).
When I didn´t have any other responsibilities, I was seeking for information about medicines
that can cause discoloration of urine.
http://emedicine.medscape.com/article/2172371-overview
Urine Discoloration With the popularity of social media and its increasing use in medicine, commentary on urine color and health has recently been surfacing. Additionally, numerous internet medical reference pages list various urine colors and their potential etiologies, and a dedicated site even gives an overview of each. Nonetheless, an excellent 2012 review article by Aycock and Kass on abnormal urine color provides a contemporary insight into an issue explored in the same journal by Raymond and Yarger nearly a quarter century prior. This article outlines some of the more common causes of abnormal urine color.
Normal urine color and clarity
The yellow coloration of urine results from urobilin (or urochrome) that is produced as a product of bilirubin degradation. Specifically, urobilinogen metabolized from bile by intestinal bacteria is reabsorbed and oxidized, producing urobilin that is then renally excreted. Normal urine color ranges from light yellow to golden. This normal variance generally fluctuates based on urine output per hydration and fluid intake in the absence of diuretics. That being said, conditions such as diabetes with glucosuria may lead to osmotic diuresis that dilutes urine and increases its volume. Conversely, ingesting pigments contained in various foods and medications, such as those in multivitamins, may cause the urine to appear darker and more concentrated.
Normal urine is clear but may appear hazy if very concentrated in the face of reduced urine output. The presence of white blood cells, or pyuria, as in infection or inflammation, can also give the urine a turbid appearance. The presence of ejaculate in the urine, whether in the first postcoital void or in the presence of retrograde ejaculation secondary to medications, procedures, or neurologic issues, may also lead to cloudy urine. Proteinuria in such instances can also lead to the development of bubbles as the urine is agitated upon reaching water in the commode. This can also happen to some degree with normal urination. However, the consistent presence of a froth or foam in the commode when urinating may indicate pathologic proteinuria.
Abnormal urine
Orange urine
Generally, orange urine discoloration results from medication use. The most common culprits are rifampin, isoniazid, and phenazopyridine. Additionally, riboflavin, sulfasalazine, and warfarin (in the absence of hematuria) have also been implicated. An additional cause of benign orange urine discoloration is the overconsumption of carrots, which may also lead to similar changes in skin appearance. Otherwise, any factors that may cause red urine can also produce orange urine, usually depending on hydration status, considering their proximity on the color spectrum.
Red urine
As with the yellow coloration of normal urine, red urine can range in intensity from a pink lemonade color (clear light pink) to that of tomato soup (active thick bleeding) to a deep opaque merlot color (liquefying clot). Hematuria, or blood in the urine, is likely the most common cause of red urine. Directly visualizing erythrocytes via microscopy is the best means of identifying true hematuria, as dipstick testing can produce false-positive results. The presence of heme in the urine also produces red discoloration and generates a positive dipstick reading; however, this should not be considered hematuria in the absence of microscopic confirmation.

The differential diagnoses for gross hematuria are broad and include, but are not limited to, infection, stone disease, malignancy, trauma, fistula, medical renal disease, and contamination (eg, due to menstruation). Gross hematuria warrants a thorough diagnostic evaluation owing to the poor prognosis associated with some of its underlying etiologies.
Red urine discoloration due to hemoglobinuria may present in hemolytic disorders, as in “march hematuria” observed in troops. Likewise, myoglobinuria due to myocyte destruction (eg, caused by rhabdomyolysis after crush injury) can also result in red urine discoloration. Similarly, the disordered heme production inporphyria can result in red urine discoloration that may change to brown or purple with sunlight exposure.
As with the difference between red and orange discoloration, urine color can vary from red to brown with hydration status.
Numerous medications can cause red urine discoloration. Most commonly, rifampin, isoniazid, or phenazopyridine is the culprit, with tears and other bodily fluids generally also discolored. Others include chlorpromazine, thioridazine, senna, and laxatives with a phenolphthalein component. A report of hydroxocobalamin producing red urine discoloration after use in cyanide poisoning has also been documented. Both mercury and lead poisoning have also been implicated in red urine discoloration.
Other more benign causes of red urine discoloration are related to the ingestion of certain pigment-containing foods. Consumption of a large amount of beets can result in red urine with no observable erythrocytes on microscopy or heme on dipstick testing. Heavy consumption of rhubarb or carrots can also cause red urine discoloration.
Brown urine
Brown urine discoloration can stem from numerous causes of red urine. Old clot sediment can appear brown when suspended in urine of a certain concentration. Likewise, myoglobinuria and hemoglobinuria often appear brown in color. To this accord, a report of “rust-colored urine” after intense hand drumming has been published. Medical renal disease can also produce brown urine discoloration. One classic example is the “muddy brown urine” observed in acute tubular necrosis.
The commonly used antibiotics nitrofurantoin and metronidazole can lead to brown urine discoloration. Chloroquine and primaquine have also been implicated. Certain laxatives, as noted elsewhere, can also be causative. Additionally, the consumption of fava beans and aloe has been believed to cause urine to turn brown.
A more serious cause of brown urine is liver failure with elevated circulating levels of bilirubin, which may first be evident in jaundice with yellowing of the skin and sclera. A rarely reported but serious cause of brown urine is metastatic melanoma. This can lead to brown or even black urine if melanocytes implant within the urinary tract and slough into the urine and when melanin itself is cleared renally.[9] Like differences between other urine colors, causes of black urine discoloration can also produce brown urine discoloration with differing urine concentrations.
Black urine
As with other urine color changes, black urine discoloration can stem from causes of red or brown urine depending on urine concentration and the intensity of the color change etiology. Other causes of black urine include laxatives derived from senna leaves and cascara bark, as well as sorbitol, the naturally occurring sugar commonly used as an artificial sweetener. Alpha-methyldopa and L-dopa have also been associated with black discoloration of urine.
Poisoning with phenol has been noted to produce black urine, as has copper poisoning. Ingestion of iodine has also been implicated. A skeletal muscle relaxant, methocarbamol, can also lead to black urine discoloration that varies to blue or green with changes in urine concentration. As mentioned above, melanoma can create black urine. Alkaptonuria, a genetic condition, can also result in urine darkening upon air exposure due to the accumulation of byproducts that result from disordered tyrosine processing. As noted above, the disordered hemoglobin production in porphyria can also produce red or brown urine that may appear black after exposure to sunlight.
Purple urine
Purple discoloration is rare. One cause, as with other discolorations, is porphyria when urine is exposed to sunlight. Purple urine bag syndrome has also been associated with purple discoloration of catheter tubing and urine collection bags. This condition stems from bacteria, usually gram-negative species, in the urine

that metabolize indole into 2 components and stain the catheter hardware. Otherwise, conditions that cause blue urine discoloration in the presence of red urine discoloration could theoretically have the same outcome.
Blue urine
Iatrogenic causes are likely the most common reason for blue urine discoloration. The intravenous injection of methylene blue or indigo carmine produces blue urine discoloration. Likewise, ingestion of a sufficient amount of methylene blue, whether isolated or as a component of other medications, home remedies, or supplements, can also create blue discoloration. Conditions with disordered tryptophan processing can result in its urinary excretion, with subsequent bacterial metabolism and blue urine discoloration. Generally, frank blue urine discoloration is rare per the presence of urochrome and the high likelihood that the two combined will cause a green urine color.
Green urine
Causes of blue urine discoloration can also produce a green urine hue when combined with the yellow color urochrome produces. Additionally, consumption of foods and supplements that contain green pigmentation can also provide the same effect. Large amounts of asparagus or black licorice have been noted to cause green urine discoloration. Some medications that have been implicated include promethazine, cimetidine, amitriptyline, metoclopramide, and indomethacin. Additionally, drugs that contain phenol can be metabolized in such a manner that green urine discoloration results.
Certain medical conditions can also lead to green urine discoloration. Urinary tract infection with Pseudomonas species has been observed to produce a green hue in urine. Additionally, fistulas into the urinary tract that facilitate the passage of bile into the urine stream permit its green pigment to stain the urine. Metabolic conditions that cause blue urine discoloration, like the other causes mentioned, can also result in urine appearing green.
White urine
White urine, also called albinuria, is most commonly due to sediment. The presence of mineral crystals (eg, from calcium or phosphate precipitation) can lead to a white or snowy-appearing urine. Other causes of white urine include infection, with funguria often resulting in white sediment from the fungus itself or resultant pyuria. Similarly, substantial bacterial infection can result in pyuria that appears white, as can mycobacterial infection, such as that with tuberculosis involving the urinary tract. Lymphatic drainage into the urinary tract, or chyluria, is another source of white urine discoloration. Mucus in the urine can also cause it to appear white in color. Regardless of the cause, the appearance of white urine generally warrants a thorough diagnostic workup.

11th October – Tuesday
I started with ranging received order and pairing medical prescriptions with medicines,
labelling of medicines and medical devices, printing of PILs, packaging, if necessary, adding
additional information (stock in a fridge/for external use only/speed of action can be affected/
for inhalation by nose or by mounth...)
I preparated an ATB sirop – 2x Amoxicilline Sandoz Forte 250mg/5ml. (add 92ml of Aqua
purificata).
Steril box for preparing ATB sirops.
I controlled prescriptions and medicine, I was working with the Pharmacy´s information
system – the datas of patient, the right molecule and strenght, subscribing prepared
prescription into the system for finding the final localisation.
I continued working with patient medical history and Ncontrol system – controlling the
dosage, interactions, containdications, missing therapy...
Women, 70 years
Currently treatement:
Omeprazol 40mg 1x/day 1tbl
ASA 80mg 1x/day 1tbl
Hydrochlorothiazide 25mg 1x/day 1 tbl
Perindopril 4mg 2x/day 1 tbl
Betahistin 16mg 1x/day 1tbl
Creatinine: 59
Clereance: >60
Questions, notes:
Supplementation with vit. D? (patient 70 years)
In the past, she took Maalox, sukralfat and omeprazol ad the same time – peptic ulcus?
If ulcus – change ASA for another antiagregant?
The dosage of perindopril – isn´t it too high? Or take 8mg at the same time?
What is the exact indication perindopril and hydrochlorotiazide are used for? Hypertesion/
heart failure?
Which is the indication that betahistine is used for? Can´t we stop the therapy?
What´s the level of LDL – Isn´t the therapy with statine necessary?
Tolbutamid = oral antidiabetic
12th October – Wednesday
For warm-up, I arranged received order, prepared prescriptions and medicines and controlled
prescriptions at the same time.
Drawers with medicines on the ground flour, another drawers are in the basement.

Betahistine = antivertiginose, against Manier desease
Pimozid - antipsychotic
Dutasteride/tamsulozine
- Treatement of benign prostatic hyperplasia
Dutasteride = 5alpha-reductase inhib – what lower the level of testosterone
Tamsulozine = alpha-block. – relax muscle in the prostate and bladder
Aripiprazol
Indication: schizophrenia, approved off-label by FDA: bipolar disorders, irritability associated with
autistic disorder.
Atovaquon/proguanil
= preventing/treating malaria
Solifenacin/tamsulozin
Treatement of storage symptoms associated with BPH.
Quetiapin
= antipsychotic
Atypical antipsychotic, antagonist at D2 R and 5-HT2 R.
Side effects: antag. H1 – somnolence; antag. Alpha 1 – ortostatic hypertension.
Trimethoprim
= ATB
Blocks the production of tetrahydrofolic ac. From dihydrofolic ac. – reversibly inhibits dihydrofolate
reductase.
It is used as a treatement of initial episodesof uncomplicated urinary tract infections due to:
E coli
Proteus mirabilis
Klebsiella pneumoniae
Enterobacter species
Coagulase negative Staphyloccocus specie – S. saprophyticus
13th October 2016 – Thursday
I took care of received order that had to be put on place – drawers or shelfs.
I assisted with delivering medicine to the patients, with pairing prescriptions – medicines and
with labelling.
I learnt a bit more about the financing and reimbursement of medicines in Netherlands and
also about START and STOPP criterias for different indications.
I was interested in system of financing and reimbursement of medicines in Netherlands, so
here is an article:
http://www.gabionline.net/Country-Focus/The-Netherlands/Policies-and-Legislation
Policies and Legislation Posted 12/08/2011 In The Netherlands generic pricing is regulated in the same way as originator medicines and has been subject to many policy
and legislative changes over the past years, including the Drug Price Act (WGP), the Health Care Market Regulation Act
(WMG), Claw-back (De Geus measure), Covenant Years 2004–2007 and Pharmaceutical Care Transaction Agreements.
Generic medicines prices in The Netherlands are also subject to a reference pricing system and in recent years have been
influenced by the preference policy (preferentiebeleid) introduced by a number of healthcare insurers.
The Dutch government has stimulated physicians to prescribe by International Non-Proprietary Names (INN) using an
electronic prescription system. Physician prescribing is regularly evaluated and medicine lists have been developed to
rationalise prescribing practices.
Pharmacists are required to carry out generic substitution, without need for reference to the physician. However, since they
receive a fixed margin, the highest price medicine is more profitable for the pharmacist.
Patients have no incentives to buy generic medicines.
Pricing
In The Netherlands, with respect to reimbursement, generics are subject to the same laws and regulations in as branded
medicines.
Medicine prices in The Netherlands were at the average of EU prices in 2005.
Between 1996 and June 2008, under pressure from an active government, the prices of prescription medicines were reduced
by 45%.
In 2009 the prices of generic medicines were 60% lower compared with prices at the end of 2007, mainly as a result of the
preference policy that many healthcare insurers enforce.
Drug Price Act
The Drug Price Act (Wet Geneesmiddelenprijzen, WGP) was introduced in The Netherlands in 1996. This act introduced
maximum prices for medicines below the level of reference pricings. The WGP procedure is also used to set the prices of
generics.
The maximum price is based on the average price of both originator and generic medicines having the same active
ingredient, strength and dosage form in Belgium, France, Germany and the UK, adjusted twice yearly. This led to a 15% fall
in medicine prices.
Under the influence of lower maximum prices, the price level of medicines has dropped an annual average of 3–4% in recent
years.
Health Care Market Regulation Act
The Health Care Market Regulation Act (Wet Marktordening Gezondheidszorg, WMG) came into effect on 1 October 2006,
replacing the Health Care Charges Act (Wet Tarieven Gezondheidszorg, WTG).
The Dutch Health Care Authority (Nederlandse Zorgautoriteit, NZa) determines, according to this act, the fixed fee per
prescription that may be charged by pharmacies, and the rate that pharmacists receive for dispensing prescriptions.
The fixed fee per prescription was set at Euros 6.00 in 2008 and pharmacists’ reimbursement at Euros 8.90 per patient per
quarter regardless of the number of prescriptions.
Claw-back (De Geus measure)
In 1998, claw-back was introduced, which made it compulsory for pharmacies to pass on part of the purchase benefits as a
price benefit to patients and thus healthcare insurance companies. From 1999 onwards, pharmacies were obligated to grant
patients and healthcare insurers an effective 3% discount.

Adjustment of the claw-back scheme in 1999 and 2002 increased claw-back by 6.82% to a maximum of Euros 6.80 per
dispensed prescription.
Covenant Years 2004–2007
Covenants have been agreed between the Ministry of Health, Welfare and Sport (Volksgezondheid, Welzijn en Sport, VWS),
the Royal Dutch Association for the Advancement of Pharmacy (Koninklijke Nederlandse Maatschappij ter bevordering der
Pharmacie, KNMP) and the Association of Dutch Health Insurers (Zorgverzekeraars Nederland, ZN), in consultation with
the Association of the Generic Medicines Industry in The Netherlands (Bond van de Generieke Geneesmiddelenindustrie
Nederland, Bogin).
The covenant agreement in 2004 reduced the prices of generic medicines to 40% under the list price. New generic medicines
were also priced 40% below the reference product.
In 2005, the 2004 covenant was extended for an additional year, and Nefarma, the representative organisation of proprietary
suppliers, also joined the medicines covenant.
In 2006 and 2007 covenants reduced the prices of prescription medicines for which similar generic drugs were available.
Pharmaceutical Care Transaction Agreement 2008–2009
On 17 September 2007, the VWS, again closed an agreement with Bogin, KNMP, Nefarma and the ZN. The parties agreed
that the prices of generic medicines should be reduced by a further 10% in 2008 and that new generic medicines should be
placed on the market for half the price of the original brand name medicine. Moreover, it was agreed that the claw-back of
6.82% would be temporarily increased during the months of December 2007 through June 2008 with a transitional surcharge
to 11.3%.
Preference policy
In July 2005 the preference policy (preferentiebeleid) was introduced by a number of healthcare insurers. This means that
healthcare insurers will only reimburse, in most cases, one of a few variants within a certain medicine cluster. In most cases
this means that only the most inexpensive variants are reimbursed.
Under the influence of the preference policy, generic medicines prices decreased by an average of 85%. In a few cases, the
price was even reduced by more than 90%.
Reference pricing (RP)
In 1991, a reference pricing system (RPS) by therapeutic class was introduced irrespective of patent status. Medicines with a
comparable therapeutic effect were grouped if they had the same mechanism of action and a similar route of administration
for treating the same indication in the same age group. For each active substance in a homogenous group, the average price
per daily dose of originator medicines and one (the cheapest) generic medicine is calculated.
The RP is then set as the median of the distribution across all active substances in the group. In 1999, RPs were recalculated
taking into account actual prices.
Incentives for physicians
Since 1995, the Dutch government has stimulated physicians to prescribe by International Non-Proprietary Names (INN)
using an electronic prescription system.
The Netherlands has a tradition of developing and implementing prescribing guidelines and treatment protocols that promote
the efficient use of medicines.
Local pharmaco-therapeutic discussions take place periodically between physicians and community pharmacists to evaluate
medicine prescribing and dispensing.
Medicine lists have been developed to rationalise prescribing practices.
Incentives for pharmacists
The Netherlands government actively encourages generic medicine substitution by pharmacists.
If the physician prescribes a branded originator medicine that is out of patent, generic substitution is required, without need
for reference to the physician.
In the past, pharmacists were encouraged to dispense generics instead of the more expensive branded medicines because
they were allowed to keep one third of the difference between the price of the brand and that of the generic dispensed. This
incentive was removed in the covenant of February 2004, which has lead to a voluntary reduction in the price of generics.
There is now little financial incentive for pharmacists to dispense generics. Nevertheless, pharmacists have agreed under the
covenants of 2004, 2005 and 2006–2007 to continue to make optimum use of generics.

Health insurance funds have introduced the preference policy which means that only certain (cheaper) medicines within a
medicine cluster will be reimbursed.
Pharmacists receive a fixed dispensing fee per prescription = non-biased dispensing, the pharmacists tends to dispense the
medicine with the highest profit margin.
Incentives for patients
Patients do not have a financial incentive to buy generic medicines in The Netherlands as there is no patient co-payment
system.
In 2007, Dutch patients paid an average of 5.6% of the cost of medicines out of their own pocket.
Policy analysis
Key factors aiding the development of the generic medicines market
The financial attractiveness of generic substitution by pharmacists sustains generic medicines use.
The generic medicines market is driven by the lower prices of generic medicines.
A range of financial and non-financial incentives for physicians support generic prescribing.
Key factors hindering the development of the generic medicines market
Market entry requires pricing and reimbursement approval. This provides a mechanism to check justification for price
and reimbursement status. However, this process delays market entry of generic medicines and prevents level playing
field across countries.
Healthcare insurance companies have introduced the preference policy driving down prices and forcing out generic
suppliers whose products have not been selected for reimbursement, thereby reducing generic competition.
The RPS provides a financial incentive for patients to demand cheaper generic medicines. However, it does not stimulate
generic medicines use if originator medicines reduce their price below level of reference price.
INN prescribing is encouraged, however, there are no budget sanctions for doctors who do not comply.
Medical students are not taught to prescribe by international non-proprietary name (INN).
There is little financial incentive for pharmacists to dispense generics.
Patients have no incentives to buy generic medicines.
14th October 2016 – Friday
In the morning, I was controling dates of expiration of medicine and medical devices. Those,
which have already been expired, we took them off the stocks, and each medicine that will
expire in the next 3 monts have been signed by the yellow paper.
I continued and finished with medical histories of 5 patients, I noticed all my questions and
queries.
With Rosetta, we controled all receiptts from the morning – right dosage, interactions,
contraindications. What I noticed:
*Patients taking methotrexate (all tablets at same time 1xweek!!!) has to take aso ac. Folic –
a day after methotrexate, never the same day.
*irbesartan + diclofenac = interaction – this combination may reduce kidney function
*oxycodon – max. 40mg/day
*Paroxetine (SSRI) + NSAIDs – increased risk for stomach
*DM: hydrochlorotiazide more than 25mg – decreased glc tolerance

* azithromycine: Chlamidia – 1,0 g 1x/day only for 1 day! But for the others indications
500mg 1x/day for 3 days
*rivaroxaban (Xarelto) – works immediately
* levofloxacine – 1.day = 500mg; 4 days = 125mg
*chloramphenicol eye drops – each 2-3 hours
*tramadol – max. 4x50mg
As every day, I was pairing receiptts and medicines, controlling them.
When I was free, I was searching for some information about molecules and their indication
that I didn´t know very well.
15th and 16th October 2016 – Week-end
I spent whole week-end in one of the most beautiful cities that I have ever visited – Utrecht.
Thanks to Nienke, who borrow me her bike, I could get everywhere I wanted to go quiet fast.
I biked a lot along the cannals, saw few markets (beautiful flower market) and in the evening
I did Trajectum Lumen.
Next day, I visited University campus, castle in Bunnik and with two other dutch students
(Iris and Ben), we climbed on a Dom´s tour. At the end of my trip, we had a beer in a cafe
which is situated in a church.
One of Utrecht´s canals, Dom´s garden, view of a Dom´s tower and pub in a Church.

17th October 2016 – Monday
In the morning, I continued with controlling dates of expiration of medicine (those that
I didn´t controle on Friday) and I prepared medicine for delivering to patients.
With Mr. Sikkes, I was delivering medicine to patients with giving them advices and further
information about right dosage and usage of their medicines (english speaking patients, for
the rest I was assisting and Mr. Sikkes traducted me everything). We were asking patients
about their therapy, about complications and their satisfaction with their treatement.
I loaded receiptts to the electronic system.
Again, I looked up for information about some medicines, their dosage, indications,
pharmacologic action (mostly at drugs.com)
Bumetanide
Bumetanide is use for treating swelling caused by excess body water associated with heart
failure/kidney disease. It´s a loop diuretic with rapid onset and short duration of action. Its
site of action is ascending limb of the loop of Henle where it acts by inhibiting Na+ and Cl-
reabsorption.
Dabigatran = Pradaxa
Dabigatran is direct trombin inhibitor that is used for reducing the risk of stroke and serious
blood clots in patients with atrial fibrilation. It´s direct oral anticoagulant that inhibit both –
free and fibrin-bound thrombin. It is administrated as dabagitran etexilate which is lacking
anticoagulant activity.
Pipamperon
Pipamperon is an antipsychotic, neuroleptic.
Chlorprothixen
Chlorprothixen is typical antipsychtic drug form tricyclic class (group of thioxantanes) that
blocks 5-HT2, D1, D2, D3, H1, M and alfa1 receptors.
Topiramate = Topamax
Topiramate is used for treating seizures and preventing migraine. It´s prescribed as initial
monotherapy in the case of epilepsy. It acts by blocking Na+ voltage dependant channels
what increase activity of GABA.
18th October 2016 – Tuesday
As always, I arranged received order and prepared medicines, medical devices. I controlled
them and by the help of the information system, I gave the location of prepared receiptts.
I finished with the control of dates of expiration of medicines and medical devices.
In the afternoon I was mostly searching for the information about PAH.
Finally,I controlled medical prescriptions – patient´s datas and if the right medicine, dosage,
strength has been given.
Nepafenac
For treating pain and swelling associated with cataract surgery.
= NSAID
In the form of ophtalmic suspension
Nepafenac is converted to amfenac = NSAID, block COX.

Dorzolamide/ timolol
For treating ocular hypertension (patients with open ngle glaucoma/ ocular hypertension who
inssuficiently respond to beta-block.)
Dorzolamide = topical carbonic anhydrase II inhibtor
Timolol = topical beta-block. – beta1 and beta2 non selective
They reduce aqueus humor secretion.
19th October 2016 – Wednesday
I arranged received order and prepared medicines for their receiptts, besides I controlled
rightness of dosages, strength and interactions. If necessary I searched the PIL for medicines.
I started to write an article about PAH, their impacts on human organisme, metabolisme,
interactions with medicaments and contamination of food suplement, acceptable values,
sources...
20th October 2016 – Thursday
I had another individual preparation to make:
Preparation
Nystatinum 2,0 g
Hydrocortisonum acetatum 1,0 g
Zinkoxydi vaselinum 10% ad 100,0 gAnalytic control – controlling the texture of prepared
ointement by laying thin film of ointement between two glasses.

I was helping with matching prescriptions and medicines and making them ready for
delivery.
*Sumatriptan = max. 100mg/24h
Lanreotide
Treating certain patients with acromegalia, to treat certain type of cancer – neuroendocrine
tumorfrom the GIT/ pancreas.
= somatostatine analog;synthetic octapeptid analog of somatostatine which is a peptide
inhibitor of multipleendocrine, neuroendocrine and exocrine mechanisms.
Displays a greater affinity for somatostatine type 2 (SSTR2) and type 5 (SSTR5) R found in
pituitary gland, pancreas, and growth hormone (GH) secreting neoplasms of pituitary
glandand a lesser affinity for somatostat. R 1, 3, 4.
Reduces GH secretion and also reduces the levels of insuline-like growth factor 1.
Tacrolimus = Protopic – ointement
= macrolide immunosupresant produced by Streptomyces tsukubaensis
Treating of atopic dermatitis.
Inhibits T-lymphocyte activation by first binding to an intracellular protein, FKBP-12.
A complex of tacrolimus-FKBP-12, calcium, calmodulin and calcineurin is formedand the
phosphatase activity is inhibited. It prevents the dephosphorylationand translocationof
nuclear factor of activated T-cells (NF-AT), a nuclear factorthought initiate gene transcription
for the formation of lymphokines (interleukine-2 and gama-interferon). Alson inhibits
transcription for genes of IL-3, IL-4, IL-5, GM-CSF, TNF-alpha (these all are involved in the
early stages of T-cell activation).Has been shown to inhibit the release of pre-formed
mediatersfrom skin mast cells and basophiles and to down-regulate the expression of Fc ERI
on Langerhans cells.
Strattera = atomoxetine
Dexamphetamine sulfate
=sympathomimetic amine with central stimulant and annorectic activity
Treating narcolepsy, children with refracting hyperkinetic states.
21th October 2016 – Friday
The article about PAH is almost finished, it took me a mainly part of the morning.
For the rest of a time, I labelled medicines and made them ready for patients. If necessary,
I controlled the dosage according to PILs.
I assisted during delivering of prescription medicines in Obbicht.
In the evening, I went to Sittard for visiting October fest.
22th October 2016 – Saturday
Another free day, so I biked a lot again – from Geleen to Urmond (because of the windmill
that is there) and then throught Stein to Elsloo (beautiful parc around castle and very nice
city) and long way until Oisbeerk (to see another windmile) and finally throught Doenrade to
Sittard and Geleen.
Windmill in Urmond

Windmill in Oirsbeek
At the end of the day, I spent very nice evening with Sikkes´ family and another visite of
Octoberfest with Nienke.
23th October 2016 - Sunday
I was wondering for long time, what to do on Sunday – because there is a lot of things to do,
but less of time. So the possibilities were – Dutch Design Week in Eindhoven (but I can do it
also next week-end on the way to Amsterdam), Liége (but in Belgium I was during last 2
months) and finally I decided to go to Aachen, german city near borders.
It was very good choice – nice weather (I took a coffee on a terrace), historical center with
a cathedral which was as a first monument in Germany subscribed into the world heritage of
UNESCO, hilly parc from which you have a view of a city and delicious Printen – typical
biscuits for this city. Only worry was – if my bike will be on a station in Sittard even when
I will come back, bike was there so I consider this day as a big success.
24th October 2016 – Monday
This was a beginning of my last week in the Pharmacy.
The day started very nice – with Mr. Sikkes, we run 10km nerby Stein (we were lucky with
the weather – no rain during running), just after we had a tea and some biscuits with Rudy
and than we came to the Pharmacy.
I finished my article about PAHs.

Determination of levels of 4 PAHs generated during home grilling
Results from Albert Colijn, written by Kristína Krajčovičová.
There exist a lot of methods how to prepare tasty meat. Because the raw meat is edible only
in few cases, we prefer thermal treatment such as boiling, frying, baking, smoking or grilling
(contact electric grill, charcoal grilling, fuel grilling). Grilling is the method that require
exposure of high temperature what results into the forming of Polyaromatic hydrocarbons
(PAH). (1)
PAH are organic components that are generated during incomplete burning of organic
materiel by the action of high temperature (baking, grilling, barbecuing, frying…). They are
composed of 2 or more fused aromatic rings. They consist of carbon and hydrogen and do
not contain any heteroatoms. There exist hordes of different PAHs but 16 of them show
clear evidence of mutagenecity or genotoxicity (according to SCF – Scientific Committee of
Food and JECFA - FAO/WHO Expert Committee on Food Additives). Those 16 are namely:
Benz[a]anthracene, Benzo[b]fluoranthene, Benzo[j]fluoranthene, Benzo[k]fluoranthene,
Benzo[ghi]perylene, Benzo[a]pyrene, Chrysene, Cyclopenta[cd]pyrene,
Dibenz[a,h]anthracene, Dibenzo[a,e]pyrene, Dibenzo[a,h]pyrene, Dibenzo[a,i]pyrene,
Dibenzo[a,l]pyrene, Indeno[1,2,3-cd]pyrene, 5-methylchrysene, Benzo[c]fluorene. (2)
PAH are considered as principals atmospheric cancerogenic polluants. They were detected
in the water, in the air, in the soil, what means that also fish living in polluted water or
plants growing in polluted soil contain these cancerogenic substances.
Food represents the highest source of PAHs for a human, non-smoker. Following sources are
mainly cigarette fume, oil refining, house heating, traffic gaz. Beside, these sources of PAHs
that are formed directly or inderictly by the human behaviour against nature, they exist also
naturals resources, such as volcans’ erruption, forest fire and also biosynthetis of PAHs by
bacterias and plants. (3) They are in grilled and smoked products, fats and oils, in dry fruits,
cereals etc.
In 2008, EFSA decided to use 4 differents PAHs (benzo[a]pyrene, chrysene,
benz[a]anthracene and benzo[b]fluoranthene) as markers of occurrence of PAH in food. The
sum of these 4 components is expressed by the term PAH4 and permit more exactly
controlling of PAH’s values in food (2)
Regarding at the formule of PAH, e.g. benzo(a)pyrene, it is evident that these components
are highly liposoluble. Exposure to PAHs occurs by 3 routes – respiratory tract,
gastrointestinal tract and skin contact. PAHs can be absorpt by lung, intestine or skin.
Consequently, they are transported by blood or lymphatic way and stocked in the liver,
kidney or fat tissue. The accumulation is mainly in mitochondries and the nucleus, that can
result to the damage of DNA. Their elimination is done by faeces and urine. (3)
PAHs begin to be cancerogenic just after enter the organism because of their transformation
to cancerogenic forms. Human organism try to form more hydrophylic (water-soluble)
substances for enable the elimination of these toxines.
The metabolisation of benzo(a)pyrene consists of 2 phases. The first one is oxydation by
CYP450 especially CYP1A1, CYP1A2 and CYP1B1 to form a variety of products,
including Benzo[a]pyrene 7,8-oxide. Benzo[a]pyrene 7,8-oxide is metabolized by Epoxide
hydrolase 1 that opens the epoxide ring to produce Benzo[a]pyrene-7,8-diol. After another
reaction with CYP450, the ultimate cancerogene benzopyrene diol epoxide is formed.
Epoxydes are intermediate metabolites that can bind covalently at DNA bases and so they
can form DNA-adducts, what is explication of their cancerogenity. They can also bind to
protein such as albumin or haemoglobin. The aim of the second phase is formation of a
conjugate. The epoxyde formed during the first phase is now conjugated with glutathion
catalysed by glutathio-S-transferase. Glutation is considered as detoxification enzyme
because conjugate of PAH is not able to bind to DNA and so to cause its damage. (3) (4)
PAH components are known to have enzyme-inducing effects, especially on the CYP450
family of enzymes, including CYP1A. (5)
The exposure to PAHs can be analysed by monitoring their metabolites in urine. For benzo(a)pyrene, metabolites such as: 1-, 2- hydroxyphenanthrene, 9-, 3-, 4-hydroxyphenanthrene and 1-hydroxypyrene was measured in post-shift urine samples of workers who were in contact with PAHs. (6) The exposure of organism against PAH depends among other things on dietary composition. For mean consumers, the value of received PAH4 is 1168 ng/day (19.5 ng/kg b.w. per day) and 2068 ng/day (34.5 ng/kg b.w. per day) for high dietary consumers. SCF estimated a maximum daily intake of benzo[a]pyrene from food of approximately 6-8 ng/kg b.w. per day for a person weighing 70 kg. (7)
EFSA doesn’t determined acceptable values for PAHs in grilled meat. Values are available for
oils and fats, smoked meats and smoked meat products , muscle meat of smoked fish and
smoked fishery products , muscle meat of fish , crustaceans, cephalopods , bivalve molluscs ,
processed cereal-based foods and baby foods for infants and young children, Infant
formulae and follow-on formulae, including infant milk and follow-on milk, dietary foods for
special medical purposes intended specifically for infants. (8)
There exist already a large number of studies that compare impact of different types of
heating preparation on the concentration of PAH. Experiment at fish shows, that the highest
amount of PAH is in the fish prepared by frying, lower concentration are reached by grilling
and the lowest by boiling.(9) Studies also show, that right choice of marinnade can
influence the generation of PAHs. Acidic marinade, containing 1,2% of lemon juice reduce
the appearance of PAHs by 70%. The duration of marinating does not significantly change
the level of PAHs. (10)
The beer can also play a role in preserving the formation of PAHs in grilled meat. Marinades
containing black beer showed the highest inhibitory effect on the formation of PAH,
followed by marinade with non-alcoholic Pilsner beer and the lowest inhibitory effect was
observed with marinade from Pilsner beer. (11)

According to EFSA (European Food Safety Authority), the concentration of PAHs created
during home cooking practices of meat, such as barbecuing, could be lowered by preventing
fat dropping into the flames.
In laboratory Born, we often determine the concentration of benzo(a)pyrene in herbs and
herbs extract as a *marker of a herbal quality. As mentioned above, there is no exact value
for acceptable level of benzo(a)pyrene in grilled meat in Netherlands (for herbs it’s 10 µg/kg
= 10 ppb BaP).
*We decided to mesure the level of 4PAH, namely: Benz[a]anthracene, Chrysene,
Benzo[b]fluoranthene and benzo[a]pyrene in grilled meat. The meat was stored for 24 hours
in a freezer, than removed and treated on a grill using … . We left the meat enough longtime
at the grill for being black outwardly but still juicy in the middle. Afterwards, the meat was
devided into 2 pieces called sample 1 and sample 2, 4 grams and 9 grams respectively. The
difference was in the level of the burning. Sample 1 was more black than sample 2, we
expected higher value of 4PAH in the sample 1 than in the sample 2.
PAH sample 1 Sample 2 Average
µg/kg µg/kg µg/kg
Benzo(a)anthraceen 75 49 62
Chryseen 188 43 116
Benzo(b)fluoranthreen 22 10 16
Benzo(a)pyreen 46 21 34
PAH4 331 123

References:
1. A. Farhadian, S. Jinap, H.N. Hanifash, I.S. Zaidul Effects of meat preheating and
wrapping on the levels of polycyclic aromatic hydrocarbons in charcoal-grilled meat.
Food Chemistry, Volume 124, Issue 1, 1 Jaunuary 2011, p. 141-146, [cit. 18.10.2016]
http://www.sciencedirect.com/science/article/pii/S0308814610006990
2. According to EFSA
EFSA opinion on suitable indicators for both the occurrence and toxicity of polycyclic
aromatic hydrocarbons (PAHs) in food
3. Lecture by Olivier Laprevote, UE3 Pharmacocinétique, toxicology et champignons
macromycetes toxiques, Universite Paris Descartes, Faculte des sciences biologique
et Pharmacologiques, 2013
4. https://lsresearch.thomsonreuters.com/maps/2304/ [cit. 20.10.2016]
5. Katarzyna Skupinska et al. Polycyclic aromatic hydrocarbons: Physiochemical
properties, environmental appearance and impact on living organisms. Acta Poloniae
Pharmaceutica. Vol. 61 No 3 pp. 233-240, 2004 [cit. 19.10.2016]
6. Rossbach, B., Preuss, R., Letzel, S. et al. Int Arch Occup Environ Health (2007) 81: 221.
doi:10.1007/s00420-007-0209-9 [cit. 19.102016]
7. Scientific Opinion of the Panel on Contaminants in the Food Chain on a request from
the European Commission on Polycyclic Aromatic Hydrocarbons in Food. The EFSA
Journal (2008) 724, 1–114
8. COMMISSION REGULATION (EC) No 1881/2006 of 19 December 2006 setting maximum
levels for certain contaminants in foodstuffs (Text with EEA relevance) (OJ L 364, 20.12.2006,
p. 5) [cit. 18.10.2016]
9. Olatunji OS, Fatoki OS, Opeolu BO, Ximba BJ. Benzo[a]pyrene and
Benzo[k]fluoranthene in Some Processed Fish and Fish Products. Tchounwou PB, ed.
International Journal of Environmental Research and Public Health. 2015;12(1):940-
951. doi:10.3390/ijerph120100940.
10. Farhadian, , S. Jinap, , A. Faridah, , I.S.M. Zaidul. Effects of marinating on the
formation of polycyclic aromatic hydrocarbons (benzo[a]pyrene,
benzo[b]fluoranthene and fluoranthene) in grilled beef meat. Food Control, Volume
28, Issue 2, December 2012, Pages 420-425 A.
11. Effect of Beer Marinades on Formation of Polycyclic Aromatic Hydrocarbons in
Charcoal-Grilled Pork, Olga Viegas, Iria Yebra-Pimentel, Elena Martínez-Carballo,
Jesus Simal-Gandara, and Isabel M. P. L. V. O. Ferreira. Journal of Agricultural and
Food Chemistry 2014 62 (12), 2638-2643
DOI: 10.1021/jf404966w
I was prepairing medicines for their delivery to patients.
I searched for exact indication of methylfenidate (widely prescribed in Netherlands)
Adults – treating narcolepsy 20-30mg/day (but very individual), devided into 2-3 takes, 30-45
min before meals
Children – treating ADHD
25th October – Tuesday
My first task was to prepare 100 capsules of 10mg ASA for a baby of 5 months.
Preparation
Acidum acetylsalicylicum 10,0 mg
Cellulosum microcrystallicum q.s.
D.t.d. No C (centum)
And as always, I was helping assistants with everything that was necessary.
I was finding some information about:
Olodaterol
Long actinc beta2-R agonist. Treatement of COPD
Feneticiline
Peniciline ATB with narrow spectrum of action
26th October – Wednesday
I started the day by ranginning received order and helping assistants with receiptts and than
I had a preparation to do.
Preparation
Hair creme
Acidum salicylicum 10,0 g
Cetiol V decylis oleas 25,0 g
Cremor lanette ad 100,0 g
Firstly, I filled necessary documents – why is individual preparation necessary and a
protocol.
* Ac. Salicylic irritate respiratory system, after adding creme into the mixture of ac. Sal. And
cetiol, it is necessary to mix very longtime so that the liquid phase can involve into the creme.
Rosseta showed me the system of maintaining the quality, what it involves, how to work with
the system, what are tasks that should be completed in oncoming time.
Conclusion of my internship:
Here, I´d like to discuss what this internship gave to me, what I learnt and which differencies
between Slovak and Dutch system I can see.
The first difference that I realised, was the size of the Pharmacy (2 stories + basement and
laboratory for analysis of substances). In my pinion, slovak Pharmacies are in most of cases
smaller with dominance of Pharmacists and not assistants, as I could observed.
In Netherlands, there is a possibility to receive medical prescription by electronic way and the
form is completely different.
Doctor can prescribe only few tablets (or other forms) and not the whole package, so in the
Pharamcy, they are allowed to divide packages.
In most of the cases, generics are used, that is caused by their lower price. Inssurance
companies require the product with the lowest price, original medicine is given in the case
that doctor say so, or the pacient inssist on it, but in this case, patient has to pay the original
one.
The prescription for anticonception pills is necessary only for the first time, patients (women)
don´t have to see the doctor every year.
From my subjective view, the scale of vitamines and food supplements is smaller than in
Slovakia.
At the beginning of a therapy (the first time that patient take a medicine), patient receives
printed information about this medicine (it is not the same one as PIL). When the therapy
continues, it means the 2nd time when patient come for his medicine, Pharmacist or
Pharmaceutical Assistant is obliged to ask question about the treatement – complications,
side effects, satisfactions...
Pharmacist can visite patients at his home and discuss his therapy.
Pharmacists (in community pharmacy) talk with general practitioners about polypragmatic
patients that results into more efficient therapy.

From my subjectiv point of view, I would say that opioid analgetics, methotrexate and
methylfenidate for pediatric population are more prescribed here than in Slovakia (this
opinion can be cause by lacking experience).







