POTENTIALLY INAPPROPRIATE MEDICATIONS FOR THE GERIATRIC
POPULATIONIN THE PRACTICE OF DENTISTRY
Arwa Farag, BDS, DMSc, DipABOM, DipABOP, FRCSEdApril 6th, 2017

DISCLOSURES
GRANT/RESEARCH SUPPORT: NOVARTIS, GLAXOSMITHKLINE, BIOGEN
IDEC, PROCTER & GAMBEL, & PRIVO

I WILL BE DISCUSSING “OFF-LABEL” USES OF THE FOLLOWING FDA APPROVED
MEDICATIONS:
DOXEPIN, GABAPENTIN, PREGABALIN, DULOXETINE& MILNACIPRAN
CONSUMPTION OF MEDICATIONS IN GERIATRIC POPULATION
Geriatrics adult population aged 65 & above
Represent 13% of the US population but consume
• 40% of prescription drugs• 35% of all OTC drugs
Task force on Aging Research: Meds & Errors. https://www.ascp.com/sites/default/files/file_Task_Force_2009_FINAL-3.pdf Accessed June 15,2015
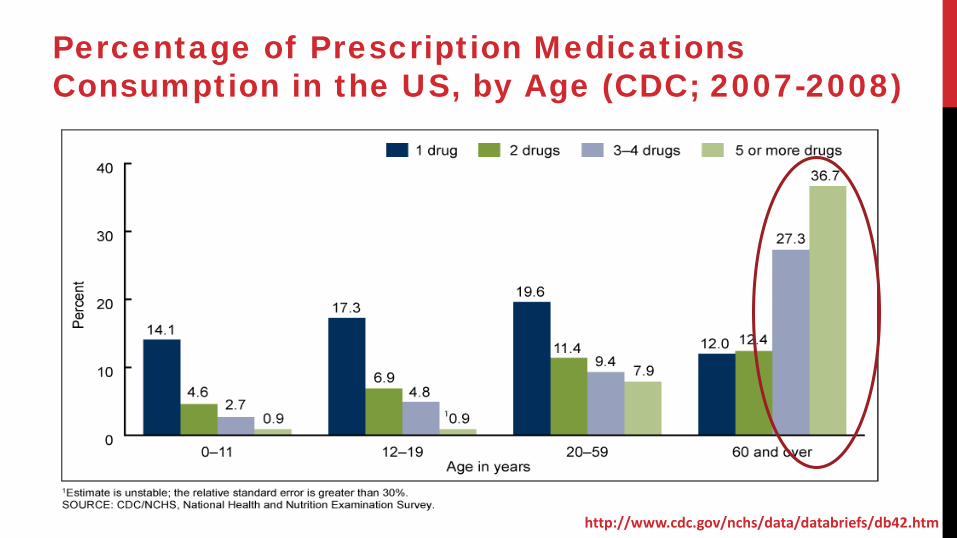
http://www.cdc.gov/nchs/data/databriefs/db42.htm
Percentage of Prescription Medications Consumption in the US, by Age (CDC; 2007-2008)
INCREASED RISK FOR ADE & DRUG INTERACTIONS
• Co-existence of health-related comorbidities
• Polypharmacy
• Pharmacokinetic activities diminished • GI absorption, drug distribution, hepatic metabolism & renal clearance
• Pharmacodynamic functions compromised• drug-receptor interaction, signal transduction, protein transcription &
cellular response
Akhtar S, Ramani R. Anesthesiol Clin 2015;33(3):457-69Wehling M. J Am Geriatr Soc 2011;59(2):376-7
AS DENTISTS, WHY SHOULD WE CARE?
ARE THERE GUIDELINES?

The Centers for Medicare/Medicaid Services (CMS) uses the National Committee for Quality
Assurance (NCQA) & Pharmacy Quality Alliance (PQA)
• Evaluate the quality of care provided to their beneficiaries
• Monitor the use of high-risk medications in the elderly
Both are based on the AGS Beers Criteria
http://www.ncqa.org/hedis-quality-measurement/hedis-measures/hedis-2016/hedis-2016-ndc-license/hedis-2016-final-ndc-lists
http://pqaalliance.org/images/uploads/files/2017_HRM.pdf
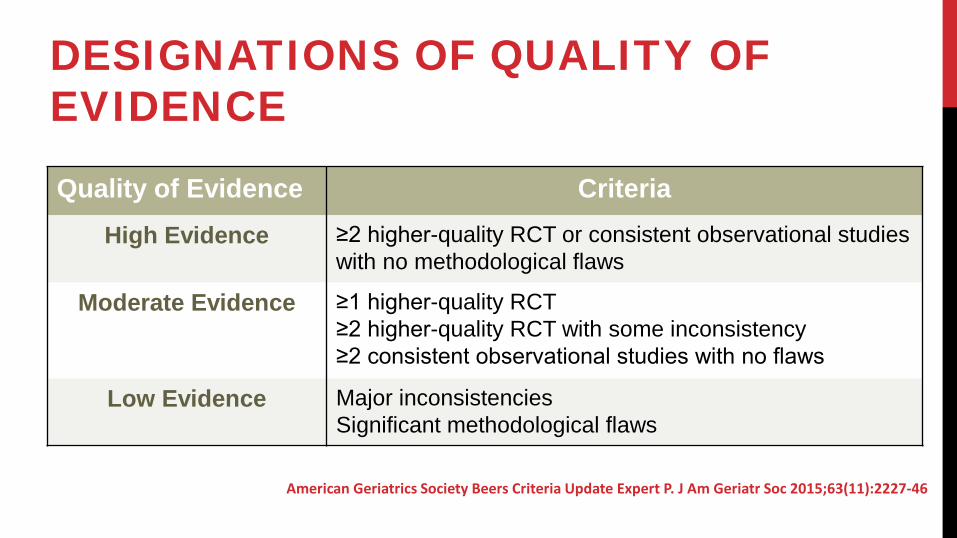
DESIGNATIONS OF QUALITY OF EVIDENCE
Quality of Evidence CriteriaHigh Evidence ≥2 higher-quality RCT or consistent observational studies
with no methodological flaws
Moderate Evidence ≥1 higher-quality RCT≥2 higher-quality RCT with some inconsistency ≥2 consistent observational studies with no flaws
Low Evidence Major inconsistenciesSignificant methodological flaws
American Geriatrics Society Beers Criteria Update Expert P. J Am Geriatr Soc 2015;63(11):2227-46
DESIGNATIONS OF STRENGTH OF RECOMMENDATION
Strength of Recommendation
Rational
Strong Harms, risks & adverse events clearly outweigh benefits
Weak Inadequate evidence to determine net harms, adverse events & risks
American Geriatrics Society Beers Criteria Update Expert P. J Am Geriatr Soc 2015;63(11):2227-46

TRICYCLIC ANTIDEPRESSANTS
TRICYCLIC ANTIDEPRESSANTSIndication • Depression, anxiety disorders, PTSD, & panic attacks• Chronic neuropathic pain
Amitriptyline, nortriptyline, doxepin & imipramine
In the H & N region• Post-herpetic neuropathy• Persistent dento-alveolar pain (PDAP)• Burning mouth syndrome
Attal N, et al. Eur J Neurol 2010;17(9):1113-e88Finnerup NB,et al. Pain 2005;118(3):289-305List T, et al. J Orofac Pain 2003;17(4):301-10
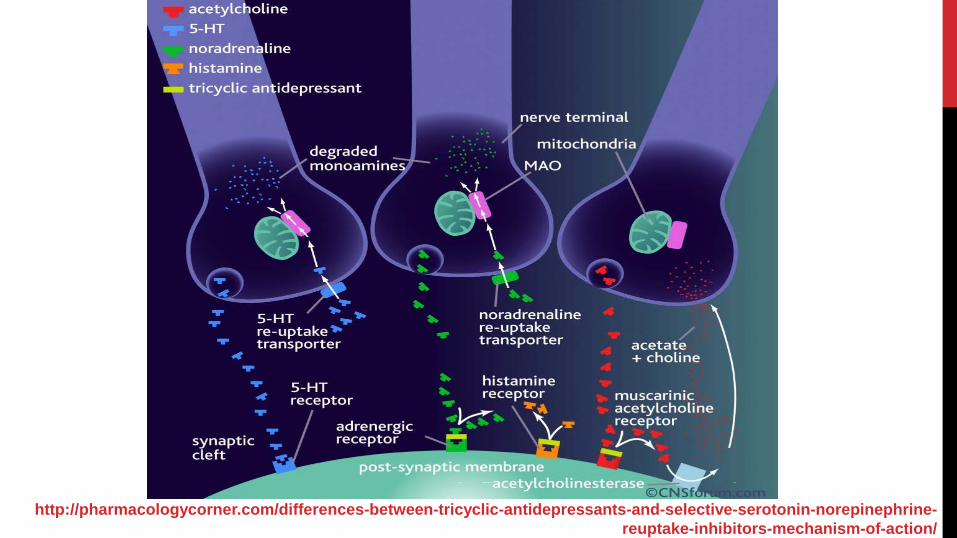
http://pharmacologycorner.com/differences-between-tricyclic-antidepressants-and-selective-serotonin-norepinephrine-reuptake-inhibitors-mechanism-of-action/
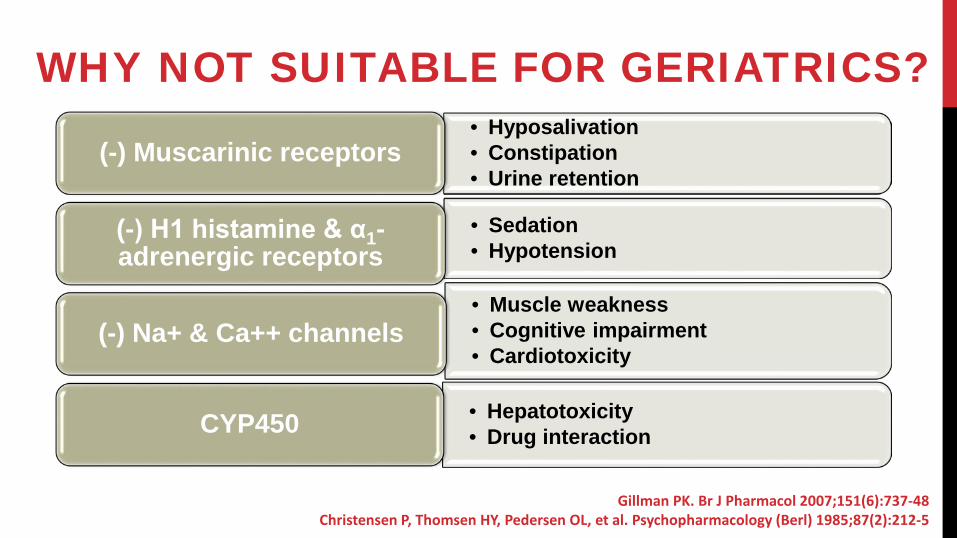
WHY NOT SUITABLE FOR GERIATRICS? • Hyposalivation• Constipation• Urine retention
(-) Muscarinic receptors
• Sedation• Hypotension
(-) H1 histamine & α1-adrenergic receptors
• Muscle weakness• Cognitive impairment• Cardiotoxicity
(-) Na+ & Ca++ channels
• Hepatotoxicity• Drug interactionCYP450
Gillman PK. Br J Pharmacol 2007;151(6):737-48Christensen P, Thomsen HY, Pedersen OL, et al. Psychopharmacology (Berl) 1985;87(2):212-5
TRICYCLIC ANTIDEPRESSANTS
Beers Criteria
STOPP List
AvoidEvidence HighRecomdStrong
Coupland C, et al.. BMJ 2011;343:d4551Nelson JC, Devanand DP. J Am Geriatr Soc 2011;59(4):577-85
Scharf M, et al. J Clin Psychiatry 2008;69(10):1557-64
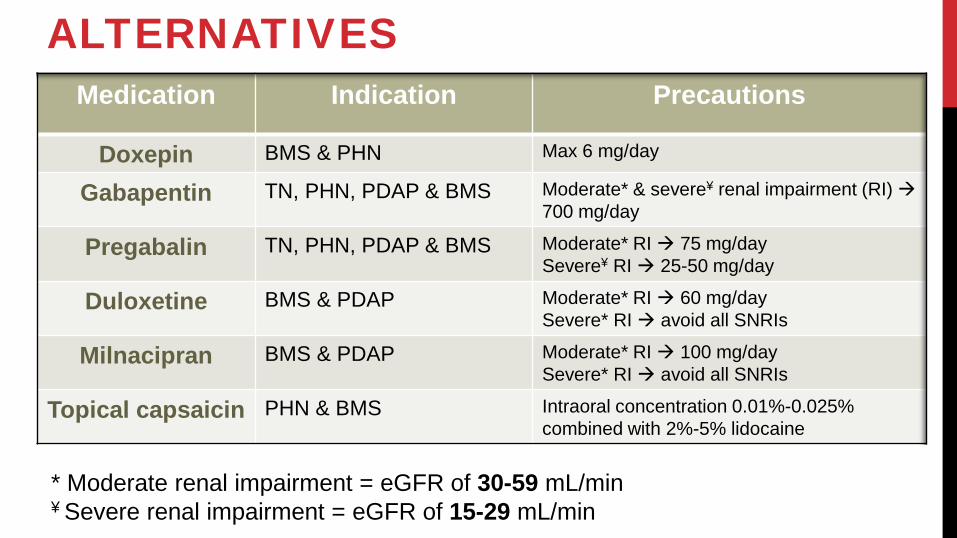
ALTERNATIVESMedication Indication Precautions
Doxepin BMS & PHN Max 6 mg/day
Gabapentin TN, PHN, PDAP & BMS Moderate* & severe¥ renal impairment (RI) 700 mg/day
Pregabalin TN, PHN, PDAP & BMS Moderate* RI 75 mg/daySevere¥ RI 25-50 mg/day
Duloxetine BMS & PDAP Moderate* RI 60 mg/daySevere* RI avoid all SNRIs
Milnacipran BMS & PDAP Moderate* RI 100 mg/daySevere* RI avoid all SNRIs
Topical capsaicin PHN & BMS Intraoral concentration 0.01%-0.025% combined with 2%-5% lidocaine
* Moderate renal impairment = eGFR of 30-59 mL/min¥ Severe renal impairment = eGFR of 15-29 mL/min

BENZODIAZEPINES
BENZODIAZEPINES
Indications• Sedative, hypnotic, anticonvulsant & anxiolytic
• Anxiety disorders, PAs, muscle spasms, seizures & insomnias
• In the H & N region• BMS, PDAP & some TMDs
Clonazepam & sometimes diazepam
Heckmann SM, Kirchner E, Grushka M, Wichmann MG, Hummel T. Laryngoscope 2012;122(4):813-6Gremeau-Richard C, Woda A, Navez ML, et al. Pain 2004;108(1-2):51-7
Martin WJ, & Forouzanfar T. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111(5):627-33
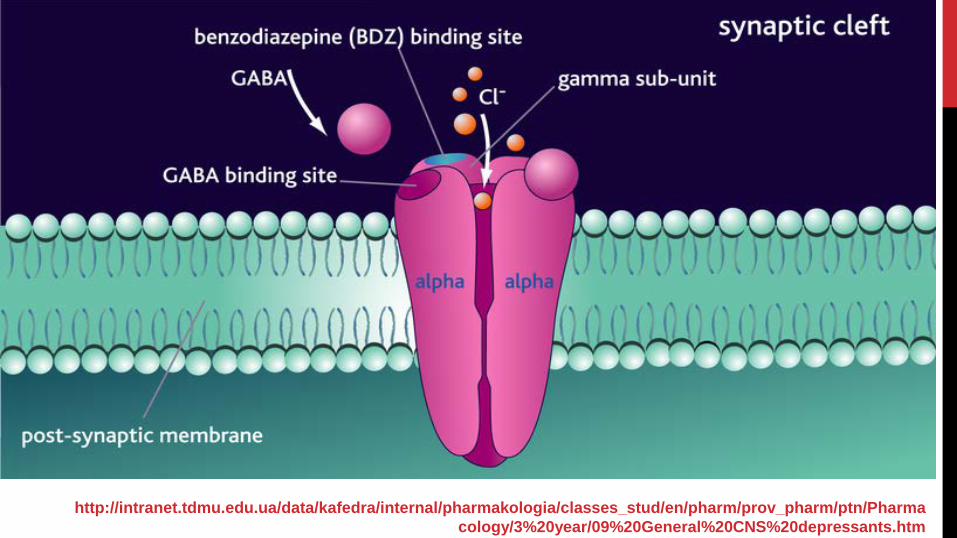
http://intranet.tdmu.edu.ua/data/kafedra/internal/pharmakologia/classes_stud/en/pharm/prov_pharm/ptn/Pharmacology/3%20year/09%20General%20CNS%20depressants.htm
BENZODIAZEPINES
Beers Criteria
STOPP List
AvoidEvidenceModerate
Recomd Strong
llain H, Bentue-Ferrer D, Polard E, Akwa Y, Patat A. Drugs Aging 2005;22(9):749-65Finkle WD, Der JS, Greenland S, et al. J Am Geriatr Soc 2011;59(10):1883-90
Paterniti S, Dufouil C, Alperovitch. J Clin Psychopharmacol 2002;22(3):285-93

WHY NOT SUITABLE FOR GERIATRICS?
• Increased susceptibility to drug interaction• Increased susceptibility to AEs:
• cognitive impairment, dizziness, delirium, fatigue, falls, & mind cloudiness
WHY?• CYP3A4 interactions• long-acting agents:
• clonazepam T ½ 21-70 hours• diazepam T ½ 19-60 hours
Berlin A, Dahlstrom H. Eur J Clin Pharmacol 1975;9(2-3):155-9Cloyd JC, Lalonde RL, Beniak TE, Novack GD. Epilepsia 1998;39(5):520-6
Kaplan SA, Jack ML, Alexander K, Weinfeld RE. J Pharm Sci 1973;62(11):1789-96 Riss J, Cloyd J, Gates J, Collins S. Acta Neurol Scand 2008;118(2):69-86
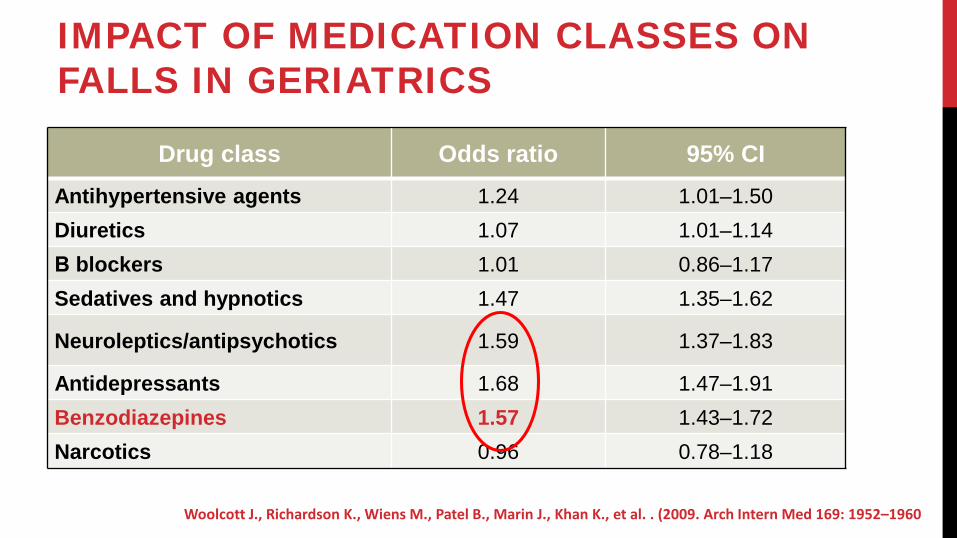
IMPACT OF MEDICATION CLASSES ON FALLS IN GERIATRICS
Drug class Odds ratio 95% CIAntihypertensive agents 1.24 1.01–1.50Diuretics 1.07 1.01–1.14Β blockers 1.01 0.86–1.17Sedatives and hypnotics 1.47 1.35–1.62
Neuroleptics/antipsychotics 1.59 1.37–1.83
Antidepressants 1.68 1.47–1.91Benzodiazepines 1.57 1.43–1.72Narcotics 0.96 0.78–1.18
Woolcott J., Richardson K., Wiens M., Patel B., Marin J., Khan K., et al. . (2009. Arch Intern Med 169: 1952–1960
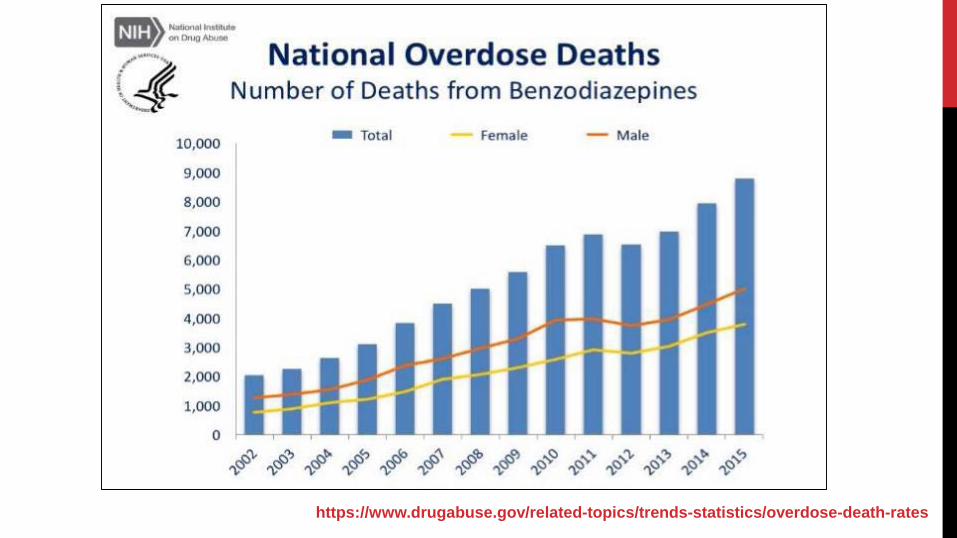
https://www.drugabuse.gov/related-topics/trends-statistics/overdose-death-rates
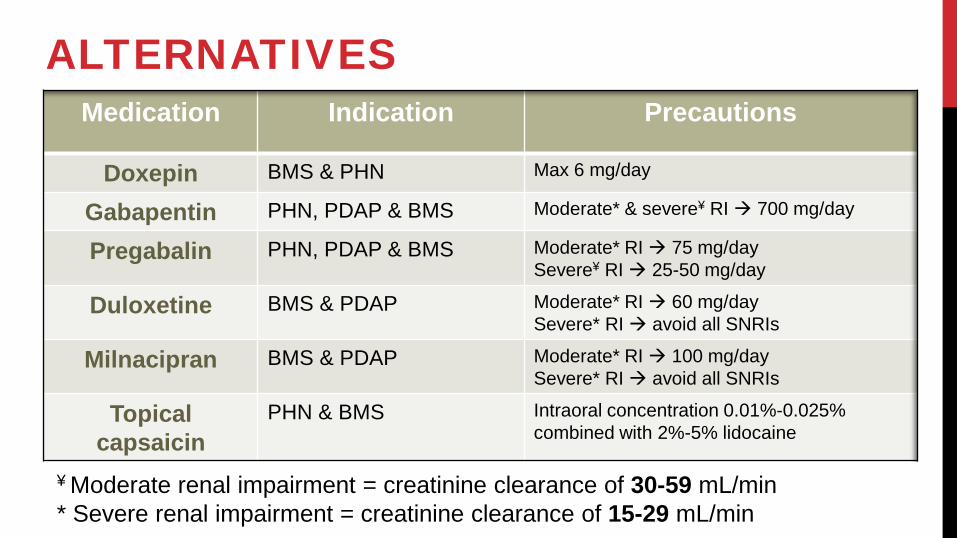
ALTERNATIVES
¥ Moderate renal impairment = creatinine clearance of 30-59 mL/min* Severe renal impairment = creatinine clearance of 15-29 mL/min
Medication Indication Precautions
Doxepin BMS & PHN Max 6 mg/day
Gabapentin PHN, PDAP & BMS Moderate* & severe¥ RI 700 mg/day
Pregabalin PHN, PDAP & BMS Moderate* RI 75 mg/daySevere¥ RI 25-50 mg/day
Duloxetine BMS & PDAP Moderate* RI 60 mg/daySevere* RI avoid all SNRIs
Milnacipran BMS & PDAP Moderate* RI 100 mg/daySevere* RI avoid all SNRIs
Topical capsaicin
PHN & BMS Intraoral concentration 0.01%-0.025% combined with 2%-5% lidocaine

SKELETAL MUSCLE RELAXANTS
SKELETAL MUSCLE RELAXANTS
Indication in the H & N region
• Regional myofascial pain & myospasm
• Tension type headache & tardive dyskinesia
Cyclobenzaprine, carisoprodol, metaxalone & methocarbamol
Mechanism of action• Incompletely elucidated CNS conductivity (brain stem & spinal cord)
• cyclobenzaprine inhibit alpha motor neurons activity + TCA
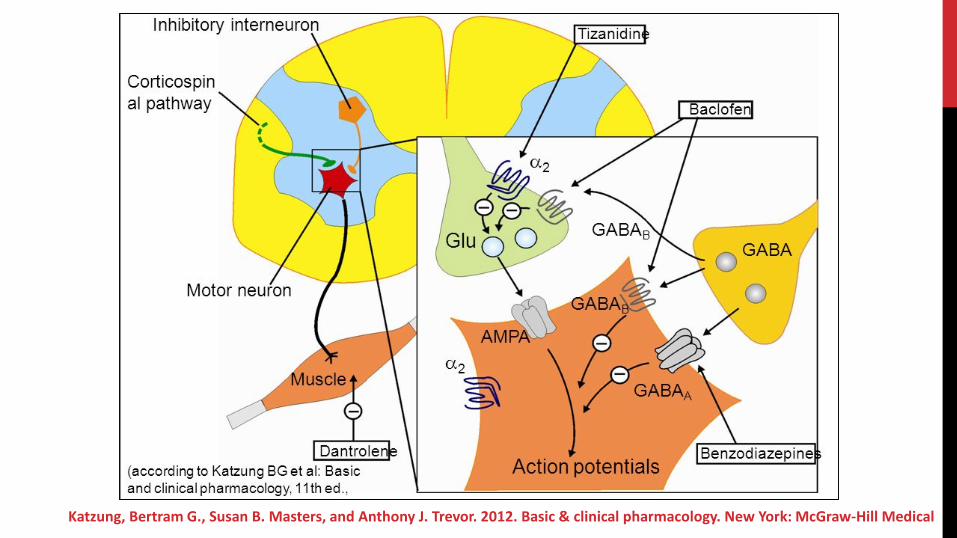
Katzung, Bertram G., Susan B. Masters, and Anthony J. Trevor. 2012. Basic & clinical pharmacology. New York: McGraw-Hill Medical
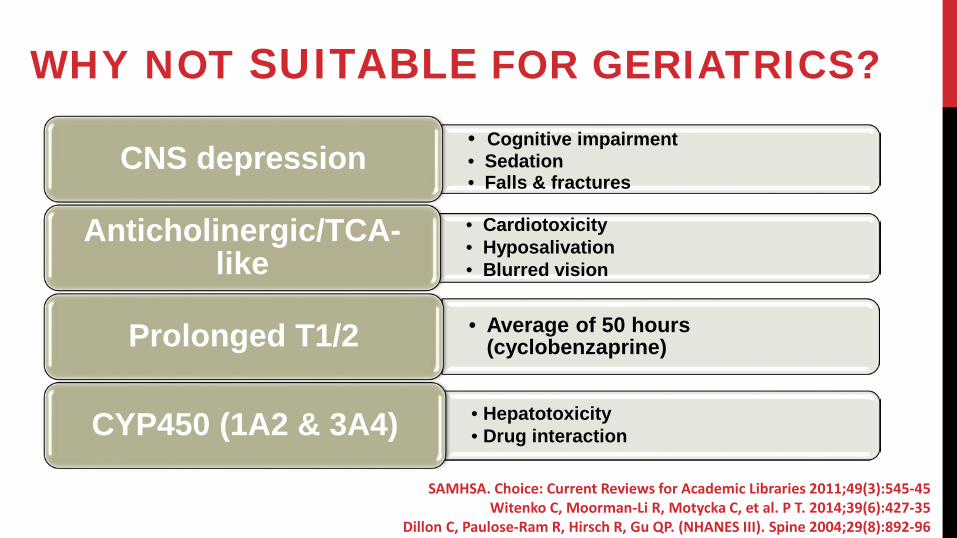
WHY NOT SUITABLE FOR GERIATRICS? • Cognitive impairment• Sedation• Falls & fractures
CNS depression
• Cardiotoxicity• Hyposalivation• Blurred vision
Anticholinergic/TCA-like
• Average of 50 hours (cyclobenzaprine)Prolonged T1/2
• Hepatotoxicity• Drug interactionCYP450 (1A2 & 3A4)
SAMHSA. Choice: Current Reviews for Academic Libraries 2011;49(3):545-45Witenko C, Moorman-Li R, Motycka C, et al. P T. 2014;39(6):427-35
Dillon C, Paulose-Ram R, Hirsch R, Gu QP. (NHANES III). Spine 2004;29(8):892-96
Annually, ≈15% (300,000) of muscle relaxants prescribed in the US are given to patients over the age of 65
MS relaxants are associated with a 50% increased risk of ADEs majority related to CNS depression
& sedation [RR=2.04 (95% CI, 1.23–3.37)]
SKELETAL MUSCLE RELAXANTS
Beers Criteria
STOPP List
AvoidEvidence Moderate
Recomd Strong
Rudolph JL, Salow MJ, Angelini MC, McGlinchey RE. Arch Intern Med 2008;168(5):508-13American Geriatrics Society Beers Criteria Update Expert P. J Am Geriatr Soc 2015;63(11):2227-46
- Uncovering & addressing the underlying problem
• Depression, anxiety, posture, parafunctional movements
- Conservative interventional modalities
• Posture adjustment, physical therapy, passive & active muscle stretching exercises, oral appliance therapy, heat or cold application, low-level laser therapy, trigger point injections, acupuncture, & cognitive behavioral therapy
ALTERNATIVES
Alexandra Martin, et al. Arch Intern Med. 2006;166(10):1092-1097Christian JB, et al. Consult Pharm 2004;19:1011-28
ALTERNATIVELioresal• Agonist of GABA-B receptor
• Antagonist of neuronal Na+ channels
Dosage
• Start at 5 mg TID
• Increase gradually to max 40 mg/day*
Heetla HW, et al. Arch Phys Med Rehabil 2014;95(11):2199-206Zakrzewska JM. Expert Opin Pharmacother 2010;11(8):1239-54
Sommer C.. Schmerz 2002;16(5):381-8List T, Axelsson S. J Oral Rehabil 2010;37(6):430-51
Nicol CF. Headache 1969;9(1):54-7
Effectiveness• Moderate effectiveness in regional
myofascial pain
• Second-line therapy for refractory TN
Less side effects• Minimal uptake across the BBB
• Limited CYP450 interactions
Anticonvulsants
ANTICONVULSANTSIndication in the H & N region• Trigeminal neuralgia• Glossopharyngeal neuralgia & PHN (moderate success) • PDAP (limited success)
Carbamazepine & oxcarbazepine
Mechanism of action• Blocks voltage activated Na+ channels
Nicol CF. Headache 1969;9(1):54-7Campbell FG, Graham JG, Zilkha KJ. J Neurol Neurosurg Psychiatry 1966;29(3):265-7
Martin WJ, Forouzanfar T. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111(5):627-33
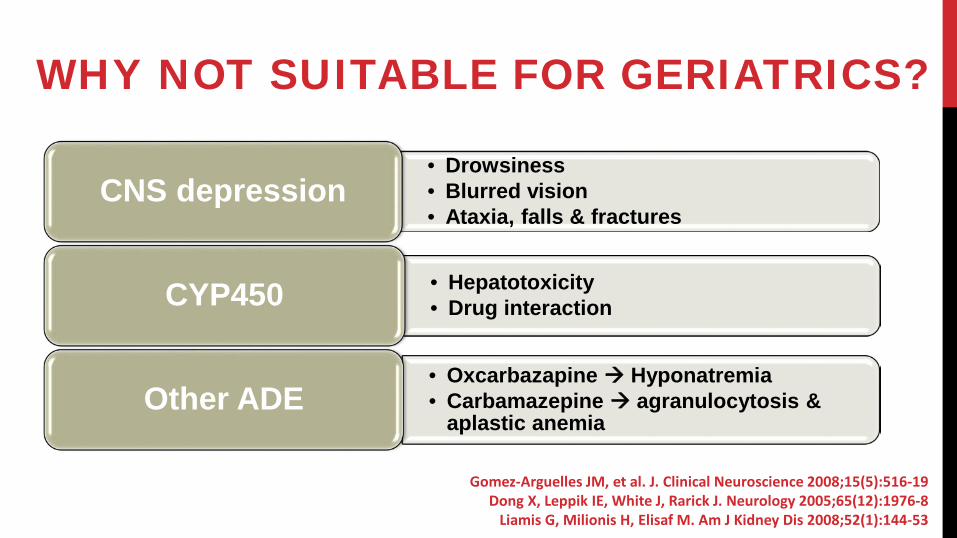
WHY NOT SUITABLE FOR GERIATRICS?
• Drowsiness• Blurred vision• Ataxia, falls & fractures
CNS depression
• Hepatotoxicity• Drug interactionCYP450
• Oxcarbazapine Hyponatremia• Carbamazepine agranulocytosis &
aplastic anemiaOther ADE
Gomez-Arguelles JM, et al. J. Clinical Neuroscience 2008;15(5):516-19Dong X, Leppik IE, White J, Rarick J. Neurology 2005;65(12):1976-8
Liamis G, Milionis H, Elisaf M. Am J Kidney Dis 2008;52(1):144-53
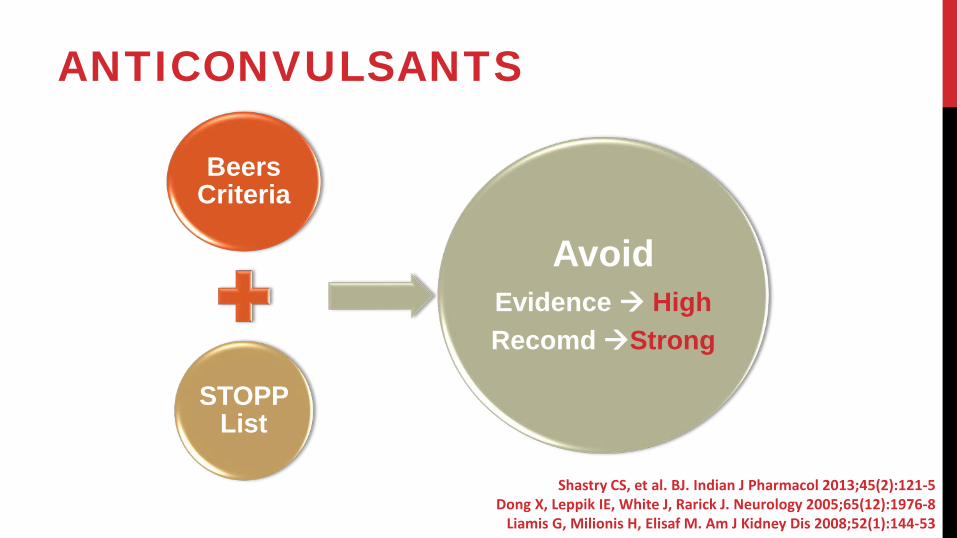
ANTICONVULSANTS
Beers Criteria
STOPP List
AvoidEvidence HighRecomdStrong
Shastry CS, et al. BJ. Indian J Pharmacol 2013;45(2):121-5Dong X, Leppik IE, White J, Rarick J. Neurology 2005;65(12):1976-8
Liamis G, Milionis H, Elisaf M. Am J Kidney Dis 2008;52(1):144-53
Safety & tolerability carbamazepine was associated with:Early onset of ADE, higher discontinuation rate & higher risk
of serious ADE
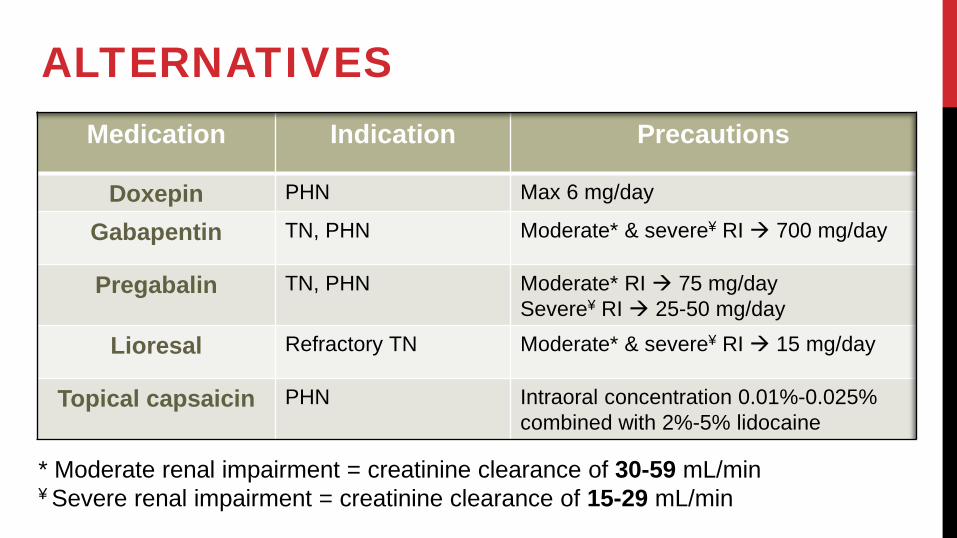
ALTERNATIVES
* Moderate renal impairment = creatinine clearance of 30-59 mL/min¥ Severe renal impairment = creatinine clearance of 15-29 mL/min
Medication Indication Precautions
Doxepin PHN Max 6 mg/day
Gabapentin TN, PHN Moderate* & severe¥ RI 700 mg/day
Pregabalin TN, PHN Moderate* RI 75 mg/daySevere¥ RI 25-50 mg/day
Lioresal Refractory TN Moderate* & severe¥ RI 15 mg/day
Topical capsaicin PHN Intraoral concentration 0.01%-0.025% combined with 2%-5% lidocaine

LONG-TERM USE OF NSAIDS
NSAIDSIndications in Dentistry
- Odontogenic infections, traumas or invasive dental procedures
Ibuprofen, ketoprofen, meloxicam, piroxicam & nabumetone
- Acute TMJ pain symptoms & some chronic myofascial pain
Naproxen & diclofenac
- Chronic paroxysmal hemicrania and hemicrania continua
Indomethacin
Scrivani SJ, David A. Keith DA, Kaban LB. N Engl J Med 2008; 359:2693-2705Dodick DW et al, Curr Pain Headache Rep. 2004 Feb;8(1):19-26

WHY NOT SUITABLE FOR GERIATRICS?
• Renal dysfunction• GI ulcers• GI bleeding
Cox1 inhibition
• Hypertension• Cardiovascular events
TXA2–mediated vasoconstriction
Smalley WE, Ray WA, Daugherty JR et al. Am J Epidemiol. 1995, 141:539–545Komhoff M, Grone HJ, Klein T, Seyberth HW, Nusing RM. Am J Physiol. 1997,272:F460–F468
Mukherjee D, Nissen SE, Topol E. JAMA, 2001, 286:954–959 Solomon DH, Schneeweiss S, Levin R, Avorn J. Hypertension, 2004; 44:140–145
The use of non-selective NSAIDs & selective COX 2 NSAIDs was associated with 40% & 70% increase in
relative risk of atrial fibrillation or flutter
LONG-TERM NSAIDS
Beers Criteria
STOPP List
Avoid Chronic Use
Evidence ModerateRecom Strong
Shastry CS, et al. BJ. Indian J Pharmacol 2013;45(2):121-5Dong X, Leppik IE, White J, Rarick J. Neurology 2005;65(12):1976-8
Liamis G, Milionis H, Elisaf M. Am J Kidney Dis 2008;52(1):144-53
NO REAL ALTERNATIVE• Avoid long-term use
• Cautions if other perpetuating factors existed
• systemic corticosteroids, anticoagulants, antiplatelets, etc..
• Ibuprfen is the safest followed by naproxen, etodolac & diclofenac
• ensure no heart failure or eGFR <30 mL/min• Indomethacin & ketorolac highest risk of ADE
• Antacids (PPIs & H2 blockers) may reduce, but eliminate this risk
• Opioids may be a safer alternative in selected cases???
Schmidt M, Christiansen CF, Mehnert F, et al. BMJ. 2011;343:d3450Abdulla A, Adams N, Bone M et al. Age Ageing 2013;42(Suppl 1):i1–i57
American Geriatrics Society Beers Criteria Update Expert P. J Am Geriatr Soc 2015;63(11):2227-46
GENERAL GUIDELINES FOR PRESCRIBING FOR GERIATRICS • Carry out a regular medication review • Avoid drugs that have known deleterious effects in elderly • Start with topical application• Use the recommended dosages for elderly patients• Use simple drug regimens• Consider non-pharmacological treatments • Limit the number of people prescribing for each patient• Avoid treating adverse drug reactions with further drugs
Milton J., Hill-Smith I, Jackson S., Prescribing for older people. BMJ. 2008 Mar 15; 336(7644): 606–609

FUTURE UPDATES & DEBATE POINTS
Medication Beers Criteria STOPP ListSystemic steroids No mention Osteoporosis
Short-term use of opioids
Prefer using opioids over NSAIDS
Increase risk of cognitive impairment,
falls & fractures
Gallagher P1, O'Mahony D. Age Ageing. 2008 Nov;37(6):673-9
THANK YOU
QUESTIONS?







