
PMDC Step-1 Course
Review of CVS & Res
Prof. Saeed ShafiDean/Principal
Sahara Medical College/SFLT PAK.


L

A Newborb infant, presented with
respiratory distress. Gut sounds
heard on left hemichest.
What Congenital anomaly you
suspect?
How it can be diagnosed?
Embryological basis of anomaly?
Whats the incidence, management &
prognosis?

Learning Outcomes
1. Compare the neonate & adult chest of.
2. Compare clinical manifestations & anatomical
basis of mediastinal shift.
3. Why MI pain radiates to left arm?
4. Interpret anatomical basis of left dominant
heart.
5. Interpret anatomico-physiological basis of
tension pneumothorax.
6. What is clinical significance of CDH?
7. Interpret anatomical basis of clinical
manifestations of Thoracic outlet syndrome.


Development of Diaphragm
Septum Transversum (4th week)
Pleuro-peritoneal membranes(6th
week/42days)
Dorsal mesentry of esophagus
Muscular ingrowth from lateral body wall (9-12th week)

Development of Diaphragm
Development of crura fusion of mesenchyme from ST, PPM & DME
migration of myoblasts into dorsal mesentry of
esophagus
Costo-diaphragmatic recess
Innervation
Descent of Diaphragm

Development of Diaphragm

Development of Diaphragm
5W 6W12W

Development of Diaphragm
At birth

Positional changes of
Diaphragm
24days52days

Anomalies of Diaphragm

Anomalies of Diaphragm
Posterolateral Defect/Foramen of Bochdalek
Defective formation/fusion of Pleuro-peritoneal membranes
1:2200
85-90% left sided
Pulmonary Hypoplasia
Eventration of Diaphragm
Gastroschisis & Epigastric Hernia
Foramen of Morgagni / Retro-sternal Hernia
Congenital Hiatal Hernia
Accessory Diaphragm

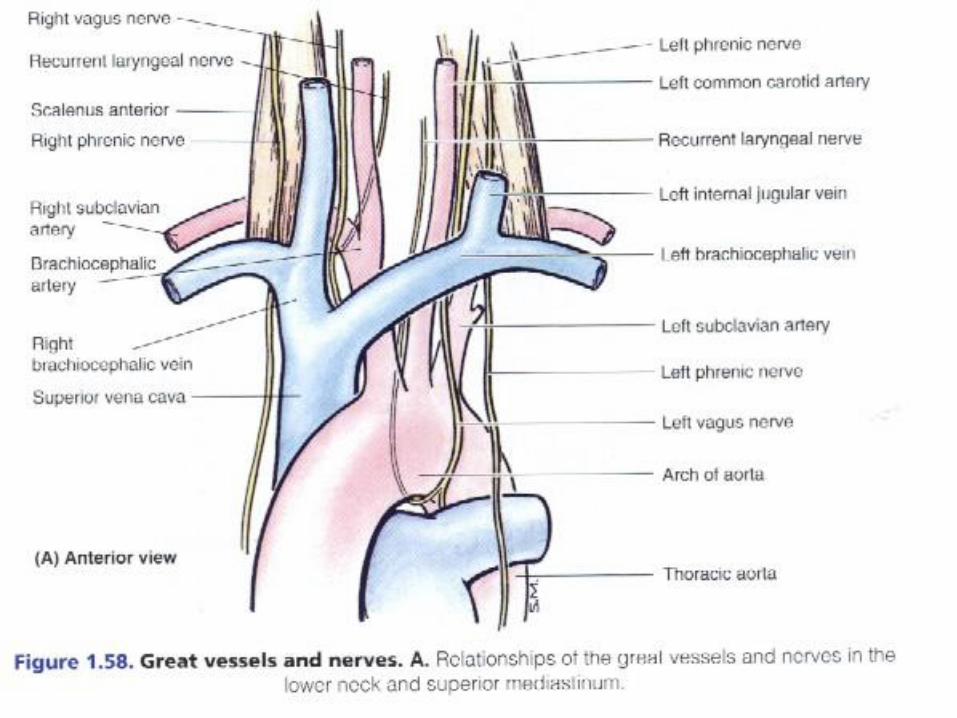
Functional anatomy of
mediastinum


The Mediastinum
Moore, Clinically
Oriented Anatomy,
3rd Edition


Subdivision of the Mediastinum
According to Anatomists


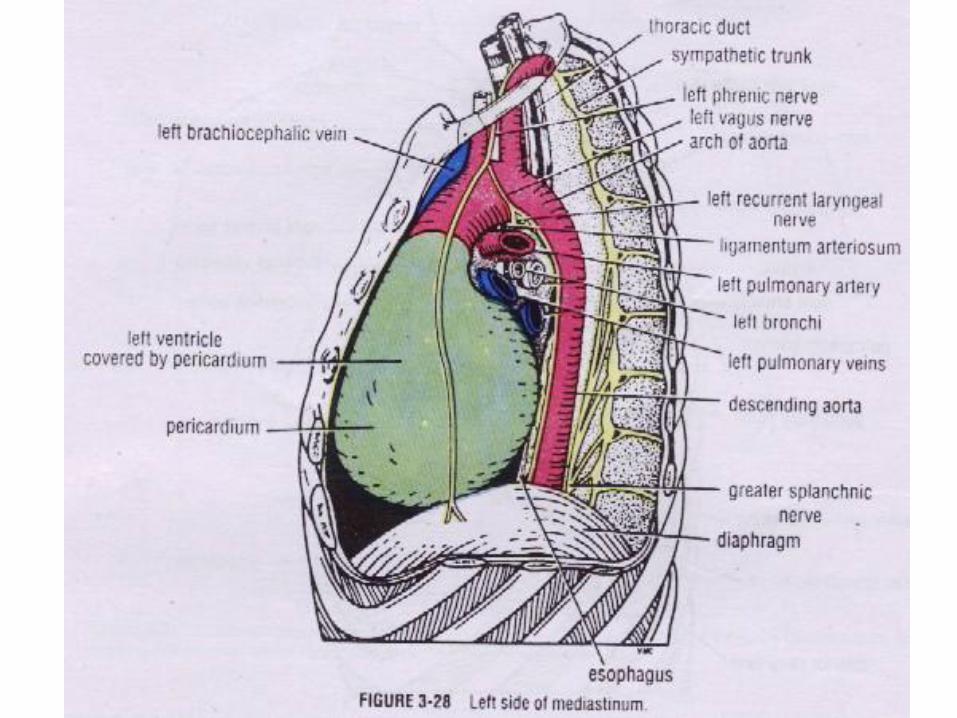

Contents of posterior
mediastinum• Viscus – esophagus
• Vessels
– Descending thoracic aorta
– Azygous and hemiazygous veins
– Thoracic duct (lymphatic)
• Nerves
– Sympathetic chain
– Splanchic nerves



Constrictions
• 3 anatomical and physiological
• Pharyngoesophageal junction
– Narrowest 15cm from incisor teeth
• Where crossed by aortic arch and left bronchus
– 25
• Where passes through opening in diaphragm
– 41cm from incisor teeth

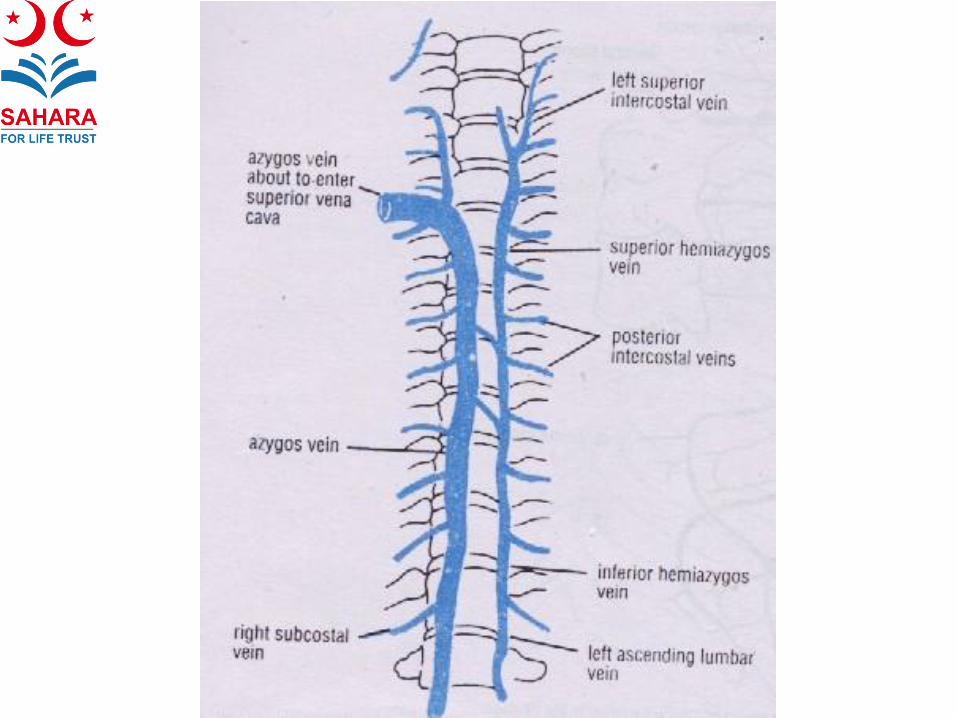
Azygos system of veins
• Consists of:
– Azygos vein
– Hemiazygos vein (inferior hemiazygos)
– Accessory hemiazygos vein (superior
hemiazygos)
• Drains thoracic wall and upper lumbar
regions


THE PLEURA & PERICARDIUM


• Pleura is a membrane that is single celled
• Normally it produces a small amount of fluid that fills gap between
parietal & visceral layers of pleura
WHAT IS PLEURA?

• Parietal & visceral layers of pleura separated from each other
by slit like space = pleural cavity
• Normally contains small amount of pleural fluid- covers surfaces
of pleura as a thin film- permits two layers to move on each
other with minimun friction
PLEURAL CAVITY


LAYERS OF PLEURA
PARIETAL PLEURA
• Lines thoracic wall
• Covers thoracic surface of diaphragm
• Lateral aspect of mediastinum
• Extends into root of neck
VISCERAL PLEURA
• Completely covers outer surfaces of lung
• Extends into depths of interlobar fissures
Two layers become continuous with each other by means of a
cuff of pleura that surrounds the structures entering &
leaving the lung at hilum

PARTS OF THE PARIETAL PLEURA
Divided into 4 parts
CERVICAL PLEURA
• Extends up into neck lining undersurface of
suprapleural membrane
• Reaches level 1-1.5inches above medial 1/3 of
clavicle
COSTAL PLEURA
• Lines inner surface of ribs, costal cartilages,
intercostal spaces, sides of vertebral bodies &
back of sternum
DIAPHRAGMATIC PLEURA
• Covers thoracic surface of diaphragm
MEDIASTINAL PLEURA
• Covers & forms lateral boundary of mediastinum
• At hilum of lung reflected – reflected as cuff around vessels
& bronchi- becomes continuous with visceral pleura

COSTODIAPHRAGMATIC RECESSES• Slit like spaces between costal & diaphragmatic pleura
separated by pleural fluid
• Quiet respiration : costal & diaphragmatic pleura are in
apposition to each other below lower border of lung
• Deep inspiration : margins of base of lung descend,
costal & diaphragmatic pleura separate
COSTOMEDIASTINAL RECESS
• Found along anterior margin of pleura
• Slit like space between costal & mediastinal pleura
• Separated by pleural fluid
RECESSES

NERVE SUPPLY OF PLEURA
PARIETAL PLEURA
Costal : intercostal nerves
Mediastinal : phrenic nerve
Diaphragmatic : domes – phrenic nerve; periphery
– lower 6 intercostal nerves
VISCERAL PLEURA
Pulmonary plexus

PERICARDIUM
Definition: Fibro-serous sac enclosing heart & great vessels
Lies within middle mediastinum, posterior to body of sternum & 2-6th costal
cartilage

FIBROUS PERICARDIUM
• Strong fibrous part of sac firmly
attached below central tendon of
diaphragm
• Fuses with outer surfaces of
great blood vessels passing
though it viz. aorta, pulmonary
trunk, SVC, IVC, pulmonary
veins
• Attached in front to sternum by
sternopericardial ligament

SEROUS PERICARDIUM
PARIETAL LAYER
• Lines fibrous pericardium
• Reflected around roots of great vessels to become
continuous with vicseral layer of serous pericardium
VISCERAL LAYER
• Closely applied to heart
• Often called epicardium
• Slit like space between parietal & visceral layers =
pericardial cavity filled with pericardial fluid (acts as
lubricant to facilitate movement of heart)

PERICARDIAL SINUSES
OBLIQUE SINUS
• Reflection of serous pericardium around large veins
TRANSVERSE SINUS
• Short passage lying between reflection of serous pericardium around
aorta & pulmonary trunk & reflection around the large veins

Clinical Anatomy of the
Cardiovascular System

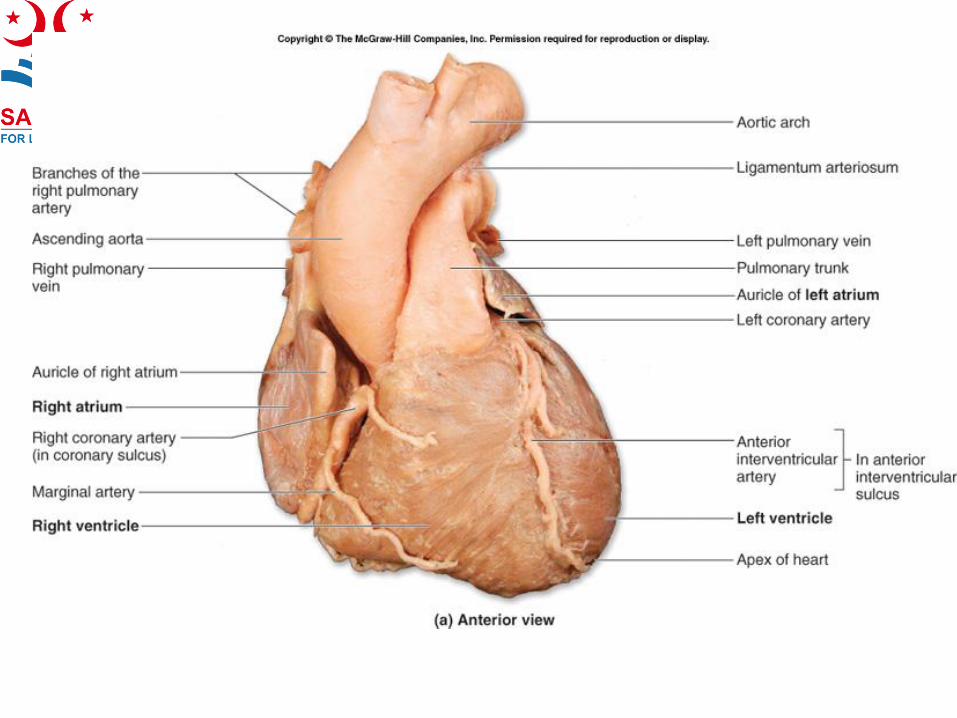
Heart
• Cardiac orientation

Anterior surface of the heart

Base of the heart.

Internal view of right atrium

Internal view of the right
ventricle

Internal view of the left
ventricle

Circuit diagram of circulation

X rays

Coronary circulation

Venous drainage

Coronary angiogram

Mechanism for perceiving heart
pain in T1-4 dermatomes

Major vessels within the middle mediastinum. A.
Anterior view. B. Posterior view.

Surface anatomy

Location of the heart valves and
auscultation points

Developmental anomalies of
heart

Echocardiogram



Plate 223
Innervation of
the Heart

CORONARY CIRCULATION

CORONARY ATERIES
• Heart is supplied by right and left coronary
arteries
• Both are branches of ascending aorta
arising from coronary sinuses, located at
the origin of the ascending aorta
• they run in the coronary sulcus



RIGHT CORONARY
ARTERY
• Arises from the anterior aortic sinus and
runs in the coronary sulcus
• Gives off a right marginal branch
• in the posterior interventricular groove and
continues as posterior interventricular
artery
• Its termination anastomoses with LAD

CORONARY ARTERIES
• The Right Coronary Artery
• In 60% cases it gives off an SA nodal
artery, which supplies SA node
• In summary right coronary artery supplies
the right atrium, right ventricle, posterior
1/3 of interventricular septum, SA and AV
nodes

LEFT CORONARY ARTERY
• It arises from the left posterior aortic sinus
and reach the coronary sulcus
• Divides into two terminal branches
• The larger anterior interventricular branch
(LAD) anastomoses with right coronary
artey
• The smaller circumflex branch run in
coronary sulcus

CORONARY ARTERIES
• Left Coronary Artery
• Left coronary artery supplies most of the
left ventricle, atrium and anterior 2/3rd of
interventricular septum
• It also supplies part of the right atrium and
may supply the SA node (10%)



CORONARY VEINS
• Venae cordis minimae
• Anterior cardiac veins
• Coronary sinus
– Great cardiac vein
– Middle cardiac vein
– Small cardiac vein
– Posterior vein of left ventricle / vein of left
atrium




VARIATIONS OF THE
CORONARY ARTERIES
• Right coronary artery is dominant in 90% of
cases
• Left coronary artery is dominant in 10% of
cases
• accessory coronary artery is present in 4%
of the cases


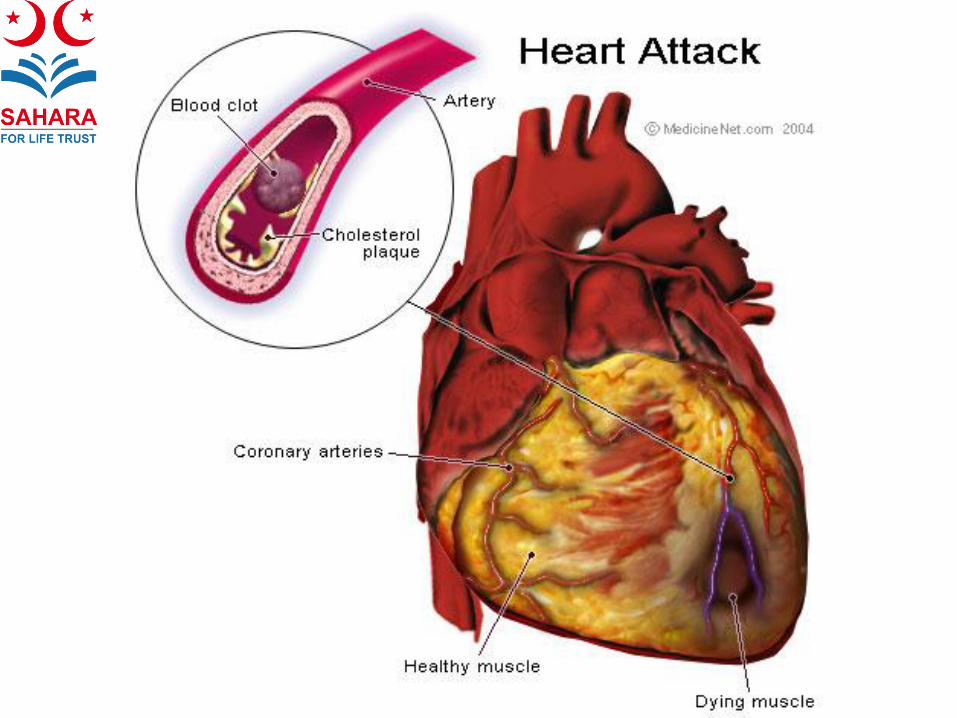
MYOCARDIAL INFARCTION
• Occlusion of a major branch of coronary artery
• The region of myocardium supplied by the occluded branch becomes infarctedand soon undergoes necrosis
• This necrosed area is called a myocardial infarct(MI)
• most common reason of the occlusion iscoronary atherosclerosis


ANGINA PECTORIS
• Clinical syndrome characterized by
substernal discomfort resulting from
myocardial ischemia
• Common causes are the stress and
strenuous exercise after a heavy meal
• It is relieved by 1 or 2 min of rest and
administration of sublingual nitroglycerin



Coronary interventions
• Echocardiography
• Angiography / angioplasty
• Thallium scan
• Coronary revascularization

CORONARY
ANGIOGRAPHY
• It is the method to visualize coronary
arteries by using radiopaque contrast
material
• Radiographs or cineradiographs are taken to
show the lumen of the artery and its
branches, as well as ant stenotic areas that
may be present



CORONARY BYPASS
GRAFT
• A coronary bypass graft shunts blood from the
aorta or a coronary artery to a branch of coronary
artery to increase the flow distal to the occlusion
• Usually a segment of internal thoracic artery or
great saphenous vein is used as a graft
• In Percutaneous transluminal coronary
angioplasy(PTA) the obstruction is opened by
using a catheter with a small inflatable balloon





PULMONARY CIRCULATION



Respiratory zone

PULMONARY VEINS
• They carry oxygenated blood from the
lungs to the left atrium
• A main vein drains each bronchopulmonary
segment
• The two pulmonary veins on each side,
superior and inferior ones, opens into the
posterior aspect of left atrium


BRONCHIAL ARTERIES &
BRONCHIAL VEINS
• They supply blood to the connective tissues
of the bronchial tree
• There are two left bronchial arteries arising
from thoracic aorta
• The single right bronchial artery
• The right bronchial vein drains into the
azygos vein and the left bronchial vein into
the accessory hemiazygos vein

PULMONARY
THROMBOEMBOLISM
• Thrombi are carried from distant site e.g., from leg
veins following fractures or DVT
• Thrombus is carried to lungs via right heart
• When this thrombus is lodged in somewhere
pulmonary arterial system, blood supply to that
area of the lung is compromised
• Depending upon the size of blood vessel and area
of lung involved, respiratory distress may lead to
daeth.


PULMONARY HYPERTENSION
• Pulmonary hypertension occurs when there
is elevated blood pressure in the blood
circulation of the lungs.
• CAUSES
• Congenital and valvular heart disease
• Chronic lung disease
• Pulmonary embolism


Thank you







