Download - Newborn mcq
MCQ OF NEWBORN
Abdulrahman Bashire
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 1
1) Newborn infants commonly have:-A. Capillary hemangioma on the forehead.B. Posterior cranial fontenalle.C. Metopic sutures.D. Impalpable coronal sutures.E. Skin tag in front of the ear.
Ans:- ABC2) The following should be investigated in five day old baby:-
A. Erythema ToxicumB. Cloudy corneaC. Divarication of rectiiD. Subconjunctival hemorrhageE. Preauricular skin tags
Ans:-BE
3) During morning rounds in the newborn nursery, you examine a healthy infant who hasblotchy erythematous macules that are 2 to 3 cm in diameter. The macules are scatteredover the trunk, face, and proximal extremities; the palms and soles are spared. Eachmacule has a 1- to 3-mm central vesicle or pustule.Of the following, the MOST likelyadditional finding in this patient is
A. pigmented macules located at sites of resolving pustules B. presence of lesions at birth C. pustules coalescing into bullae D. Wright stain of a smear of the vesicopustular contents revealing a predominance of eosinophils E. Wright stain of a smear of the vesicopustular contents revealing a predominance of polymorphonuclear neutrophils Preferred Response: DThe infant described in the vignette exhibits the classic presentation of erythema toxicumneonatorum. Tiny vesicles or pustules arise from blotchy erythematous macules, withlesions characteristically appearing at 24 to 48 hours after birth. The pustules do not coalesce intobullae. Wright staining of the pustular contents reveals a predominance of eosinophils, notneutrophils. Because the lesions are seen in healthy infants, it has been suggested that this benigncondition be renamed; suggested names include “benign neonatal rash” or “benign erythemaneonatorum.”
Transient neonatal pustular melanosis (TNPM) is another well-recognized benign dermaleruption of infancy in which pustular lesions spontaneously resolve into transient pigmentedmacules . TNPM may be present at birth, and examination of pustular contents reveals apredominance of neutrophils.
Infantile acropustulosis is a chronic or recurring benign condition manifested by intenselypruritic pustules on hands and feet. Characteristic papules and pustules may coalesce into bullae.
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 2
Infantile acropustulosis frequently is confused with scabies infestation. The lesions resolvespontaneously at 1 to 2 years of age.
4) You are examining a newborn who is the product of an uneventful pregnancy, labor, anddelivery. Apgar scores were 9 at both 1 and 5 minutes. Findings on the initial physicalexamination are unremarkable except for the presence of vesicopustules and frecklelikemacules (Item Q33A), some of which have a collarette of surrounding scale. Wright stainof a smear of the vesicopustular contents reveals a predominance of polymorphonuclearneutrophils.Of the following, the MOST likely diagnosis is
A. congenital candidiasis B. erythema toxicum neonatorum C. infantile acropustulosis D. miliaria rubra E. transient neonatal pustular melanosis Preferred Response: ECharacteristic lesions of transient neonatal pustular melanosis (TNPM) may be present at birth asvesicles, pustules, or ruptured vesicles or pustules that have a collarette of surrounding scale.Pigmented macules (Item C33A) often develop at the sites of resolving pustules or vesicles.Primary lesions usually disappear by 5 days of age; the secondary pigmented lesions may remainup to 3 months. TNPM occurs more commonly in African-American infants.Lesions can occur on palms and soles. Pustular contents reveal a predominance of neutrophils onWright stain examination, as reported for the newborn in the vignette. Infants who have congenital cutaneous candidiasis may present with scaling, erythematouspapules and pustules (Item C33B) at birth. Candida albicans can penetrate through the amnion andchorion to cause congenital infections. Scrapings from lesions prepared with potassium hydroxidedocument pseudohyphae (Item C33C) or budding yeast. Term infants who have erythema toxicum neonatorum exhibit vesicopustular lesions (ItemC33D) that usually overlie erythematous macules. Lesions of erythema toxicum rarely are presentat birth, and Wright stain of smears of pustular contents reveals a predominance of eosinophils.
Infantile acropustulosis presents as pustules or vesicles (Item C33E) localized to the handsand feet. It may be present at birth but more commonly develops in the first weeks and monthsafter birth, possibly continuing or recurring throughout infancy and early childhood. Lesions arevery similar to those of infantile scabies infestation. Pustular contents may reveal prominentneutrophils and occasional eosinophils without evidence of the mites, ova, or feces seen inscabies. An absence of hyperpigmentation in resolving lesions and a prolonged or recurringcourse distinguishes infantile acropustulosis from TNPM.
Miliaria rubra (prickly heat or heat rash) is caused by intraepidermal obstruction of the sweatducts. A secondary local inflammatory response is responsible for the erythema (Item C33F)associated with the papules and vesicles. Miliaria rubra occurs later than miliaria crystallina,usually beyond thefirst postnatal week. Hyperpigmented, frecklelike lesions are not expected inmiliaria rubra.
5) The following is true regarding changes in the fetal cardiovascular system after birth:A. There is normally immediate closure of the ductus arteriosus
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 3
B. Hypoxia-induced vasoconstriction is the mechanism of closure of the ductusarteriosus
C. The ligamentum teres is the remnant of the umbilical veinD. Regression of right ventricular hypertrophy occurs postnatallyE. Inferior vena caval pressure falls after birth
Ans:-CDEOcclusion of the umbilical cord removes this low resistance capillary bed from the circulation;breathing results in a marked decrease in pulmonary vascular resistance, hence there is increasedpulmonary blood flow returning to the left atrium raising the pressure in the left atrium causingthe foramen ovale to close. As pressure in the systemic circulation rises, shunt through the ductusarteriosus reverses. As the pO2 rises, synthesis of bradykinin and prostacyclins is inhibited, thuscausing closure of the ductus arteriosus. The ductus arteriosus can take up to 3 months to close innormal neonates.
6) Neonatal RDS:-A. Seen in most babies of birth weight < 2.5 kg.B. More common in infants of diabetic mothers.C. Associated with prolonged rupture of membrane.D. Less sever in babies of Afro-Caribiean origin than Caucasians.E. Exacerbated by hypothermia.
Ans:-BDE7) The following are causes of generalized hypotonia in 2 days old infants:-
A. PrematurityB. HypothyroidismC. Myotonic dystrophyD. Spinal dysraphyismE. Anterior horn cell disease
Ans:-ACE8) Regarding surfactant:-
A. Production begins at 30 weeksB. It is produced by Type II pneumocytes in the walls of the bronchiC. Testosterone stimulates surfactant productionD. Production is increased during a stressful event like hypothermiaE. Betamathasone given to the mother improves surfactant production in the
premature baby Ans:- E
Surfactant production begins at 20-22 weeks. It is produced by Type II pneumocytes which are inthe walls of the alveoli. The hormones testosterone and insulin inhibit surfactant production;hence hyaline membrane disease is more common in males than females and more common ininfants of diabetic mothers. Surfactant production is suppressed if the baby is hypothermic,hypoxic, acidotic or hypoglycemic.Although dexamethasone is more commonly used, betamethasone has an identical effect on lungmaturation
9) Concerning fetal lung development:-
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 4
A. Type ΙΙ pneumocytes are present at 24 week gestationB. Cuboidal cells are capable of gas transfer in uteroC. There is virtually no smooth muscle in the terminal & respiratory bronchioles at
6 month of ageD. The large airways are formed at 16 week gestationE. Alveoli are completely formed at birth
Ans:-AD10) Congenital CMV infection:-
A. Only 10% of affected pregnancies have resulting long term sequel at birthB. Diagnosis is by viral isolation from the urineC. Hearing loss can develop gradually over the first 5 yearsD. The affected newborn should be treated with ganciclovirE. Intracranial calcifications are seen in a periventricular distribution
Ans:- ABCECongenital CMV occurs in approximately 1% of all live births and only 10% of these infectionsresult in clinical symptoms. Severe clinical disease is associated with primary maternal infectionin pregnancy. Infection in early gestation carries a far greater risk of severe fetal disease. In CMVintra-cranial calcifications are in a periventricular distribution. Ganciclovir is only used if there isCNS involvement, chorioretinitis or pneumonitis.
11) The following conditions will present with cyanosis in the first week of life:A. Aortic stenosisB. Transposition of the great vesselsC. Hypoplastic left heart syndromeD. Fallot's tetralogyE. Fallot's pentalogy
Ans:- BAny cardiac lesion which allows a mixing of blood along with a right to left flow or any cardiaclesion wherein pulmonary perfusion is impaired results in cyanosis. Left heart problems oroutflow tract obstructions present as cardiac failure. Fallot's pentalogy includes an ASD alongwith the tetrad of infundibular pulmonary stenosis, RVH, over-riding of the aorta and a VSD.Babies with tetralogy of Fallot usually have a patent ductus arteriosus at birth that providesadditional pulmonary blood flow, so severe cyanosis is rare early after birth.As the ductus arteriosus closes, as it typically will in the first days of life, cyanosis can develop orbecome more severe.The degree of cyanosis is proportional to lung blood flow and thus depends upon the degree ofnarrowing of the outflow tract to the pulmonary arteries.
12) Pulmonary surfactantA. Is partly recycled by endocytosis into the synthesizing cellB. Is produced by type Ι alveolar cellsC. Reduction in pulmonary flow can cause a decrease in surfactant productionD. Synthesis is inhibited by thyroxineE. Synthesis is stimulated by glucocorticoids
Ans:- ACE
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 5
Dipalmityl- phosphotidyl choline is the main component of surfactant and is produced by Type-ΙΙalveolar cells (granular pneumocytes). Its half-life is 14 hours and its main function is to reducethe surface tension of the alveoli.
13) Lung surfactantA. Decreases the surface tension within an alveolusB. Causes an increase in chest wall complianceC. Is a glycoproteinD. Maintains the same surface tension for different sized alveoliE. Appears only after the 1st week of life
Ans:- ASurfactant is a dipalmitoyl-phosphatidyl choline and is a phospholipid, which prevents alveolarcollapse by reducing alveoli surface tension. It is produced by type-II pneumocytes and is seen atabout 24 weeks gestation. It causes an increase in lung compliance only (not chest wallcompliance).
14) The following organisms cause conjunctivitis:-A. Epstein Barr virusB. Chlamydia trachomatisC. AdenovirusD. Haemophilus influenzaeE. Neisseria gonorrhoeae
Ans:- BCDEChlamydia trachomatis causes conjunctivitis in 30-50% of neonates born to mothers withcervicitis. It is a purulent conjunctivitis, which develops 5-14 days after birth and isindistinguishable from gonococcal infection. It is diagnosed on a swab scraped over the lowereyelid (to allow cells to be collected – don’t forget it is an intracellular organism) by directfluorescent antibody, ELISA or PCR. Tetracycline ointment topically is combined with oralerythromycin – the oral antibiotic is to prevent relapse after ointment is discontinued and toprevent progression to pneumonia. Gonococcal conjunctivitis presents earlier than chlamydialdisease (usually within 2 days), is diagnosed on gram stain and culture and should be treated withIV penicillin and chloramphenicol eye drops. Don’t forget sexual health screening for the motherand informing public health of ophthalmia neonatorum. Adenovirus causes conjunctivitis insummer outbreaks; enterovirus, coxsackie and herpes simplex are other viral causes.
15) Concerning blood flow in the fetus:-A. Blood flow from right to left through the foramen ovaleB. Blood in the ascending aorta has higher oxygen content than in the descending
aortaC. The ductus arteriosus is closedD. Pulmonary pressure equal systemic pressureE. Hemoglobin may be 20 gm/dl
Ans:-ABE16) -In a healthy baby the transition from fetal to neonatal circulation involves:-
A. Functional closure of the foramen ovale in the first 24 hours
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 6
B. Blood flow in the ductus arteriosus continues from right to left until its closureC. Decrease in pulmonary artery resistance following closure of the ductus arteriosusD. The ductus arteriosus closes in response to decreased oxygen concentrationsE. The umbilical artery is a branch of the common iliac artery Ans:- A
Functional closure of the ductus arteriosus occurs soon after birth but anatomical closure can takeupto one week. As pulmonary pressures fall after birth, blood flow in the ductus is reversed iefrom left to right. The umbilical artery is a branch of the internal iliac artery.Factors influencing closure of the ductus include:- 1. Increased oxygen concentrations 2. Decreased prostaglandin levels 3. Drop in pulmonary artery pressuresN.B. Prostaglandin E2 keeps the ductus open.
17) A 10-day old male presents with bilious emesis. What is the most likely diagnosis?A. AppendicitisB. Pyloric stenosisC. Malrotation with midgut volvulusD. Feeding intolerance
Ans:- C18) A term newborn is delivered by emergent cesarean section because of intrauterine
growth restriction, oligohydramnios, and nonreassuring fetal heart rate monitoring inlabor. Delivery room resuscitation includes endotracheal intubation and assistedventilation with 100% oxygen, chest compressions, intravenous epinephrine, and volumeexpansion. Apgar scores are 1, 2, and 3 at 1, 5, and 10 minutes, respectively. An umbilicalcord arterial blood gas measurement documents a pH of 6.9 and a base deficit of 20mmol/L. At 12 hours of age, the infant demonstrates tonic-clonic convulsive activity ofthe arms and legs with a concomitant decrease in heart rate and bedside pulse oximetrysaturation. Of the following, the MOST likely cause for this infant's seizure is:-
A.Hypercalcemia.B. Hypercarbia.C.Hyperglycemia.D.Hypomagnesemia.E. Hypoxia.
Preferred Response: ESeizures are the most frequent sign of central nervous system injury in the newborn. Whenseizures occur in a newborn who has depressed neuromotor tone, reflexes, andcardiopulmonary function at birth that requires assisted ventilation, perinatal asphyxia is likely. Inthis event, Apgar scores typically are depressed to less than 3 at 5 or more minutes after birth,and there is a severely acidotic umbilical cord arterial pH (<7.0), with evidence of metabolicacidemia. Poor tolerance of labor and asphyxia are more common in fetuses that haveexperienced intrauterine growth restriction. Because the infant in the vignette has the previouslydescribed features, hypoxic-ischemic encephalopathy (HIE) must be considered as a cause forthe seizures.HIE is the most common cause of seizures occurring in the first 24 hours of postnatal life
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 7
and accounts for up to 67% of early neonatal seizures. Other causes of neonatal seizureinclude intracranial hemorrhage, cerebrovascular accidents (stroke), or hemorrhagic infarction(10% to 15%); intracranial malformation (<10%); transient hypoglycemia or hypocalcemia(<10%); drug withdrawal (<5%); and inborn errors of metabolism (<5%).When seizures occur beyond the first 24 hours after birth, especially in the absence of anyhistory of fetal or neonatal asphyxia, the evaluation should focus on potential causes other thanHIE. An additional cause for later seizures is infection (meningitis, encephalitis).Asphyxia may result in hypocalcemia and hypoglycemia; hyperglycemia and hypercalcemiaare not associated with HIE and do not typically cause seizures. Hypomagnesemia mayaccompany hypocalcemia in the infant of a diabetic mother, but it is not common followingasphyxia and is not associated with neonatal seizures. Hypercarbia may occur in the depressednewborn who has inadequate ventilation, but it is not associated with seizures unless there iscorresponding hypoxia.
19) A 2-week-old-male presents with lethargy and vomiting. His electrolytes reveal sodiumof 121 meq/L, potassium of 7.0-meq/l and blood glucose of 40 mg/dl. What is the mostlikely diagnosis?
A. DehydrationB. Congenital adrenal hyperplasiaC. Inborn error of metabolismD. Pyloric stenosis
Ans:- B20) The following cause the onset of persistent vomiting in 3 week old child:-
A. Disaccharidase intoleranceB. Duodenal atresiaC. Pyloric stenosisD. Hiatus herniaE. Lactose intolerance
Ans:-C21) The drug of choice for treating a newborn with presumed ductal-dependant cyanotic
congenital heart disease is:A. MorphineB. DobutamineC. Prostaglandin E1D. Indomethacin Ans:- C
The drug of choice for ductal dependent cyanotic heart disease is prostaglandin E1- with astarting infusion of 0.05 - 1ug/kg/min. There is a risk of apnea associated with its use so beprepared to intubate, other complications include seizures and fever. Patients with congenitalheart disease present with poor feeding, sweating with feeds, tachypnea, sudden onset ofcyanosis or pallor that may worsen with crying, lethargy, or failure to thrive. Patients withcyanotic congenital heart disease are hypoxic but typically have a minimal response to oxygentherapy; whereas patients with a pulmonary process causing hypoxia will have an increase in
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 8
their oxygen saturation when oxygen is administered. Indomethacin is used to close a patentductus.
22) How should a neonate with lethargy and a blood sugar of 20mg/dl be treated?A. Oral feeds with apple juiceB. 25% dextrose solutionC. 10% dextrose solutionD. 50% dextrose solution Ans:- C
Newborns with hypoglycemia should be treated with D10W solution with a range of 2-10cc/kg. Higher concentrations should not be used as they can cause vein sclerosis andintracranial hemorrhage. Infants and young children should be treated with D25 2-4cc/kg.
23) Neonatal convulsion can be caused by:-A. Maternal hyperparathyroidismB. Subdural hematomaC. Birth asphyxiaD. HyponatremiaE. Wilson's disease
Ans:-ABCD24) A 2-day-old female presents with abdominal distension and vomiting. She has not yet
passed a meconium stool. What is the most likely diagnosis?A. Hirschsprung DiseaseB. Malrotation with midgut volvulusC. Necrotizing enterocolitisD. Constipation Ans:-A
Suspect Hirschsprung Disease in a newborn who has not yet passed a meconium stool. Otherpossibilities include an imperforate anus or meconium plugging. Older children present with ahistory of chronic constipation. Hirschsprung disease is the absence of intramural ganglion cells inthe rectum which extends to the sigmoid colon in 77% of patients and involves the entire colon in15% of patients. The incidence is 1/5,000 live-births, with a male to female ratio of 4:1. Thediagnosis should be suspected if the patient presents with lack of meconium stool within the first24 to 48 hours of life. Vomiting and abdominal distension may also be present.
25) A 3-week-old female presents with persistent seizures despite aggressive managementwith benzodiazepines and phenobarbital. The mother reports giving her daughter somewater to "stop her from getting dehydrated." What is the most likely cause of her statusepilepticus?
A. HypoglycemiaB. Diabetes insipidusC. HyponatremiaD. Hypokalemi Ans:-C
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 9
Excessive free water intake can result in hyponatremic seizures. Infants less than 6 months of ageare particularly susceptible to these types of seizures and commonly have intractable seizuresrequiring intubation and hypothermia. Immediate treatment includes the administration of 3%saline 4cc/kg.
26) A 1-week-old male presents with some mild erythema around his umbilicus extendingonto the abdominal wall. Which of the following is the correct management for thispatient?
A. Reassurance and continue with alcohol wipes of umbilicusB. Topical antibiotic ointment and recheck the patient the next dayC. Discharge on cephalexin and recheck the next dayD. Perform a full septic workup and admit the patient Ans:- D
This patient has Omphalitis and should undergo a full septic evaluation, administration ofantibiotics and hospital admission. Surgical debridement may be required for severe cases.Omphalitis is inflammation and infection surrounding the umbilicus that can spread to the liver orperitoneum. Patients can present with symptoms ranging from mild erythema to necrosing lesionssurrounding the umbilicus on the abdominal wall. Fever may be present
27) A 5-day old, well-appearing male is brought to the ED by his mother today because shenoted that he has a cluster of vesicles on his scalp. Which of the following should be themanagement approach?
A. Skin biopsyB. IV acyclovir and a full septic workupC. Oral acyclovirD. Discharge, with next day follow up Ans:-B
This patient is at risk for herpes encephalitis and should undergo a complete septic workup and IVacyclovir should be initiated in the ED. Begin acyclovir (20mg/kg every 8 hours IV) if there is apositive maternal history of herpes, a vesicular rash, focal neurologic findings, CSF pleocytosis orelevated CSF protein without organisms on gram stain.
28) The following maternal condition can cause disease in the fetus/newborn:-A. HyperparathyroidismB. ITPC. Myasthenia gravisD. Diabetus mellitusE. Thyrotoxicosis
Ans:-ABCDE29) Which of the following heart rates is most suggestive of supraventricular tachycardia in
a newborn?A. 180 BPMB. 230 BPMC. 150 BPMD. 210 BPM
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 10
Ans:-BPALS defines SVT in infants as a heart rate of greater than 220 BPM. In older children theheart rate for SVT is greater than 180 BPM. The ECG demonstrates a narrow complextachycardia without discernible p waves or beat-to-beat variability. In the stable patient, vagalmaneuvers are the first treatment of choice (ice to the face, or blowing through an occludedstraw in older children). Adenosine given as centrally as possible is the first drug of choice (0.1mg/kg up to 6mg for the first dose and then 0.2mg/kg for the second dose up to 12 mg) Ifthis is not successful, then amiodarone 5mg/kg given over 20-60 minutes or procainamide15mg/kg given over 30-60 minutes are the next drugs of choice. Unstable patients shouldundergo cardioversion with 0.5-1J/kg followed by 2J/kg. If an IV is accessible, a dose ofadenosine can be given while setting up for the cardioversion.
30) Vaginal bleeding in a 3-day-old female is:A. Is always indicative of child abuseB. May be due to withdrawal of maternal hormonesC. Is suspicious for gonorrheaD. Is most commonly due to a vaginal foreign body-such as baby wipes Ans:- B
31) Cyanosis in the first week of life can be caused by:-A. Tetralogy of FallotB. Pulmonary stenosisC. Eisenmenger syndromeD. TAPVDE. Ebistein's anomaly
Ans:-ABDE32) A 3-week old male presenting to the emergency department with vomiting and altered
mental status and acidosis. What additional laboratory test should be included in yourevaluation?
A. Ammonia levelB. Cortisol levelC. Serum acetoneD. Thyroid function test Ans:- A
Suspect an inborn error of metabolism in patients who have an altered level of consciousness.These patients may or may not be acidotic depending on the type of inborn error that is present.Patients with a urea cycle defect typically have a normal blood gas but an elevated ammonialevel. Patients with organic acidemias will be acidotic but may or may not have an elevatedammonia level. Patients with galactosemia will have a normal blood gas and ammonia level butwill have reducing substances in the urine.
33) Which of the following are causes of shock in the newborn?A. InfectionB. Inborn errors of metabolismC. Child abuseD. Thyrotoxicosis
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 11
E. All of the above Ans:- E
34) In neonatal RDS (respiratory distress syndrome):A. Surfactant is useful in the treatment.B. It is rare in infants below 28 weeks gestation.C. Antenatal steroids are beneficial.D. Maternal opiate abuse increases the risk.E. Maternal diabetes increases the risk.
Ans:- ACE35) The risk of neonatal jaundice is increase by:
A. Prematurity.B. Trisomy 21.C. Elective caesarean section.D. Congenital hypothyroidism.E. Cephalahaematoma.
Ans:-ABDE36) At birth the blood volume is approximately:-
A. 65 ml/kg body weightB. 85 ml/kg body weightC. 110 ml/kg body weightD. 125 ml/kg body weightE. 150 ml/kg body weight Ans:- B
37) Newborn infants commonly have:-A. Papulovesicles over the trunk.B. Posterior fusion of the labia minora.C. An adherent foreskinD. Breast enlargementE. Shallow sacral dimple
Ans:-ACDE38) The following conditions signify disease in the newborn;-
A. Peeling of the skin of the hands and feetB. Blanched on one side of the body and pink on the opposite sideC. Pinhead lesion on the nose ( milia)D. Peripheral cyanosisE. Oedema of one arm
Ans:- ALL FALS39) Apreviously healthy full term infant have several episode of duskiness and feeding
difficulties during the second day of life . She is noted to have increasing jaundice, whichof the following tests will be the least helpful in making diagnosis:-
A. CSFB. Urine C/ SC. Total bilirubinD. Endotracheal aspirate C/SE. Venous blood
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 12
Ans:- D40) Difference between infant born to heroin-abusing mothers and infant born to
phenobarbitone-abusing mothers is that infant in the later group:-A. Don't have withdrawal symptomsB. Have withdrawal symptoms appearing earlier than heroin withdrawalC. Don't develop tremorD. Have high incidence of jaundiceE. Are usually term and full size Ans:- E
41) Which of the following organisms is the most frequent causes of neonatal meningitis:-A. GBSB. E . coliC. L . monocytogenesD. H .influenzaE. S. pneumoniae Ans:- A
42) One should be concerned about term infant who has not passed meconium stool:-A. During the process of birthB. Within few min of birthC. By 1-2 hour of lifeD. By 6-12 hour of lifeE. By 24 hour of life Ans:- E
43) The initial lesion of incontinentia pigmenti are:-A. Deeply pigmentedB. ScalyC. Waxy papulesD. Inflammatory bullaeE. Small vesicles
Ans:- D44) Factor that appear to lower threshold for neurologic damage and kernicterus from
unconjugated hyperbilirubinemia include all of the following except:-A. AcidosisB. AsphyxiaC. SepsisD. PostmaturityE. Hypothermia
Ans:- D45) Infant born to diabetic mothers are at risk of all of the following except:-
A. PolycythemiaB. Hyperglycemic dehydrationC. HypocalcemiaD. Congenital malformationE. Cardiomyopathy
Ans:- B
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 13
46) The Apt test is used for what purpose:-A. Crude test for carbon monoxide poisoningB. Semiquantitative test for lead poisoningC. Qualitative test for fetal hemoglobinD. Screening test for S hemoglobinE. Test for blood viscosity
Ans:- C47) Birth injury account for the majority of the following conditions detected in early
infancy:-A. Intraventricular hemorrhageB. CephalohematomaC. HydrocephalusD. Facial nerve palsyE. Pneumothorax
Ans:-BD48) In birth trauma:-
A. Erb's palsy involve C6,C7 & C8B. Klumpke's palsy involve C7,C8 &T1C. Facial nerve palsy lead to persistently closed eyeD. Sciatic nerve involvement is commonE. Cephalohematoma is characteristically present at birth
Ans:- BIn Erb-Duchenne paralysis, the injury is limited to the 5th and 6th cervical nerves. The infantloses the power to abduct the arm from the shoulder, rotate the arm externally, and supinate theforearm. The characteristic position consists of adduction and internal rotation of the arm withpronation of the forearm. Klumpke paralysis is a rare form of brachial palsy; injury to the 7thand 8th cervical nerves and the 1st thoracic nerve produces a paralyzed hand and ipsilateral ptosis,anhidrosis and miosis (Horner syndrome) if the sympathetic fibers of the 1st thoracic root arealso injured (which reflects damage to the stellate ganglion adjacent to T1.)
49) Birth injury:-A. Paralysis of the upper arm has better prognosis than paralysis of the lowerB. In nerve injury, neuroplasty is advised at the end of first year of lifeC. In phrenic nerve paralysis, spontaneous recovery is expectedD. Facial nerve paralysis will result from the nuclear agenesis of the facial nerve
Ans:-ACIf the paralysis persists without improvement for 3–6 mo, neuroplasty, neurolysis, end-to-endanastomosis, and nerve grafting offer hope for partial recovery. function usually returns in a fewmonths. Total disruption of nerves (neurotmesis) or root avulsion is the most severe, especially ifit involves C5–T1; microsurgical repair may be indicated. Fortunately, most (75%) injuries are atthe root level C5–C6, involve neurapraxia and axonotmesis, and should heal spontaneously.Botulism toxin may be used to treat biceps-triceps co-contractions.
50) The following are useful in the assessment of gestational age in preterm:-A. Presence of palmar creases
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 14
B. Breast sizeC. Sacral edemaD. The scarf signE. Muscle ton
Ans:-BDE51) Cephalohematoma:-
A. Must be differentiated from subperiosteal hemorrhageB. Is usually visible at birthC. May calcifyD. May be associated with underling fracture of the skullE. Should be managed surgically
Ans:-CD52) Caput succedaneum is characterized by all of the following except:-
A. Diffuse edematous swelling of the soft tissues of the scalp involving theportion presenting during vertex delivery
B. It may extend across the midlineC. It may extend across the suture linesD. Edema usually disappear within 2-3 monthsE. The scalp overlying the area may show mild bruising Ans:- D
53) In newborn with oral moniliasis the most common primary source of infectionA. Maternal source ( vaginal )B. Contaminated fomitesC. Following use of AgNO2D. Contact by hospital carriersE. Systemic antibiotic therapy
Ans:- A54) Meconium impaction is associated with:-
A. CretinismB. Cystic fibrosisC. ThrushD. HMDE. Trisomy 21 syndromes Ans;- B
55) Premature infant is delivered precipitiously and appear asphyxiated . The infant iscyanotic, there are no respiratory efforts,and the heart rate is 80 / min .The infant ismeconium stained and thick particulate meconium is noted in the amniotic fluid and ininfant mouth. At this point you should:-
A. Pass an umbilical artery catheter to measure the PH & PO2B. Start bag-mask ventilation with 100% oxygenC. Suction the oropharynx & trachea with ETT to remove the meconiumD. Intubate the trachea & begin the ventilation with 100 % oxygenE. Establish monitoring with ECG & pulse oximeter Ans:- C
56) Hypoglycemia has been observed in all of the following except;-
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 15
A. With LBW and RDSB. With anoxic injuryC. With hypothermiaD. Who are SGAE. With high PO2
Ans:- E57) All of the following are usually associated with cretinism except:-
A. ConstipationB. Prolonged jaundiceC. LethargyD. TetanyE. Hypotonia Ans:- D
58) All of the following are characteristic of single umbilical artery except:-A. Presence in about 5 of 1000 birthB. About 1/3 of such infants have congenital abnormalitiesC. 21 trisomy is frequently foundD. Among twin ,the rate of occurrence is 35 / 1000E. The associated congenital abnormalities may involve the genitourinary tract
Ans:- C59) Two minutes after normal term delivary:-
A. The ductus venosus will be closedB. The pulmonary arterial pressure will have fallenC. The pressure in the left atrium will have fallenD. The arterial oxygen tension will have risenE. Regular breathing will have begun
Ans :-ABDE60) Established neonatal resuscitation procedures include:-
A. Directing cold stream of oxygen at the noseB. Administration of drugs with respiratory stimulant propertiesC. Oropharyngeal suctionD. Bag and face mask ventilationE. Prompt cooling
Ans:-ACD61) The Apgar score :-
A. At 1 min is reliable measure of asphyxiaB. At 1 min is reliable measure of respiratory failureC. At 10 min is strongly correlated with later neurological deficitD. Includes the infant response to pharyngeal suction catheterE. Isn't application after 10 min of age
Ans:- BCD62) Criteria used in the Apgar score include :-
A. Core temperatureB. Heart rateC. Respiratory rate
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 16
D. Skin thicknessE. Muscle tone
Ans :-BE63) Pink newborn with HR of 88/min is actively gasping , he has good muscle tone and
respond to nasal catheter stimulation with facial grimace, the apgar score is:-A. 5B. 6C. 7D. 8E. 9
Ans:- D64) Mongolian spots are characterized by all of the following except:-
A. They are permanentB. They are usually of a slate blue pigmentationC. They are generally observed over the buttocksD. The area of pigmentation is well demarcatedE. They aren't associated with trisomy syndromes Ans:-A
65) All of the following physical signs may be useful in estimating the gestational age at birthexcept:-
A. There are only one or two transverse skin creases on the sole of the foot until36 week of gestation
B. The breast nodule is usually not palpable at 33 or 34 weeksC. The breast nodule is usually 4-10 mm in term infantD. The testes are descending and rugae cover the entire scrotal surface by 34
weeksE. The texture of scalp hair
Ans:- DThe testes are usually not completely descended until after 36 weeks & scrotal rugae are few andlimited the anterior and inferior aspect of relatively small scrotum . By 34 weeks the areolabecome raised and between 36-37 weeks the breast bud is 1 – 2 mm reaching size of 4-10 mm atterm. The transversr foot creases develop at 31 – 32 weeks .By 36 weeks creases cover theanterior two-third of the sole .
66) Newborn infant who remain centrally cyanosed after intubation and IPPV may have:-A. Diaphragmatic herniaB. Choanal atresiaC. Tension pneumothoraxD. Drug induced respiratory center impairmentE. Profound anaemia
Ans:-AC67) The following statement about pulmonary hypertension are true :-
A. It recognized complication of group B streptococcal sepsisB. Hyperventilation is an effective treatmentC. Tolazoline is potent pulmonary vasoconstriction
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 17
D. Radial arterial PaO2 is lower than umbilical artery PaO2E. Birth asphyxia is a risk factor
Ans:-ABE
68) Concerning air leak syndromes in the newborn:-A. Underwater seal drain is only required if the pneumothorax is under tensionB. In term baby with small pneumothorax giving oxygen at high concentration
can worsen itC. Increasing the I; E ratio in ventilated baby decrease the risk of pneumothoraxD. Pneumomediastenum is usually fatalE. They can be asymptomatic
Ans;- E69) Recognized problem of infants born at term SGA include:-
A. HypothermiaB. SepsisC. PolycythemiaD. HypoglycemiaE. Retinopathy of prematurity
Ans:-ABCD70) Complication of steroid therapy in the newborn include:-
A. LeucopeniaB. HypoglycemiaC. CataractD. SepsisE. Gastric perforation
Ans:-CDE71) Concerning NEC :-
A. Exchange transfusion is predisposing factorB. Clostridium welchii is implicated in the pathogenesisC. It is most common in infants born less than 1500 gmD. Oral antibiotics are usefulE. Complications include short bowel syndrome
Ans:-ACE72) The following congenital condition require immediate ( within first week) treatment
after birth:-A. TEFB. Cleft lipC. Spina bifidaD. ExomphalosE. Hydrcephalus
Ans:-ACD73) Preterm infant at increased risk from :-
A. Conjugated hyperbilirubinemiaB. Meconium aspirationC. Periventricular leucomalacia
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 18
D. Necrotizing enterocloitisE. Child abuse
Ans:- CDE74) Peri- or intraventricular cerebral hemorrhage
A. Occur in less than 10% of VLBW infantB. Arise most commonly in the first 72 hour after delivaryC. Is direct result of impaired vitamin K supplyD. Is the single most common cause of congenital cerebral palsyE. May result in rapidly evolving hydrocephalus
Ans:-BE75) Feature typical of physiological jaundice include:-
A. Recognizable jaundice in the first 48 hoursB. Peak plasma bilirubin at 4-5 daysC. Persistent beyond first weekD. IrritabilityE. Pale stool
Ans:- B76) Jaundice on day 1 is often caused by ;-
A. Metabolic disorderB. TORCH infectionC. Gastrointestinal obstructionD. HemolysisE. Physiological factor
Ans:-BD77) Persistant, conjugated hyperbilirubinaemia may be caused by:
A. Alpha-1-antitrypsin deficiency.B. Hypothyroidism.C. Haemolytic disease.D. Cytomegalovirus infection.E. Cystic fibrosis.
Ans:-ABDEExplanation:- all cases need further investigation.Causes of conjugated hyperbilirubinaemia in a neonte are:1)-Intrahepatic cholestasis -Infections. -Congenital infections (STORCH-syphlis, toxoplasma, rubella, cytomegalovirus, hepatitis, herpes virus infection) -Acquired infections- septicaemia, UTI. -Metabolic disorders –cystic fibrosis, alpha-1- antitrypsin deficiency, galactosaemia, fructosaemia, lysosomal storage disorders, peroxisomal disorders. -Endocrine disorders – hypothyroidism, hypopituitarism, hypoadrenalism. -Anatomical disorders – intrahepatic:bile duct hypoplasia. -Miscellaneous – idiopathic neonatal hepatitis, chromosomal abnormalities, trisomy 21, 18 and 13.2)-Extrahepatic cholestasis:- biliary atresia, choledochal cyst, spontaneous bile duct
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 19
perforation, inspissated bile syndrome.Unconjugated neonatal jaundice is normally physiological and resolves spontaneously.
78) All of the following are characteristic of jaundice associated with breast feeding except :-A. Significant elevation of unconjugated bilirubinB. Rapid fall in serum bilirubin after discontinuation of nursingC. Nursing can be resumed after several days without return of hyperbilirbinemiaD. Significant elevation of conjugated bilirubinE. Kernicterus has never been reported to occur as result of breast milk jaundice alone
Ans :- D79) Persistent jaundice during the first month of life may associated with all of the following
except:-A. Cytomegalic inclusion diseaseB. Congenital atresia of the bile ductC. GalactosemiaD. Rh incompatibilityE. Penicillin treatment
Ans:- E80) A 26-week gestation preterm infant is now 6 weeks old and weighs 1,250 g. He is
receiving full-volume enteral nutrition. The only significant finding on physicalexamination is pallor. He has anemia (hematocrit of 28% [0.28]; reticulocyte count of 8%[0.08]) and receives iron supplementation. He is receiving a formula that is high inpolyunsaturated fatty acids.Of the following, the MOST correct statement about his needfor vitamin E is that it
A. does not need to be supplemented in infancy B. has no effect on anemia C. needs to be supplemented now D. will be needed when the infant is 3 months old E. will prevent anemia Preferred Response: CHistorically, inadequate vitamin E, a high level of polyunsaturated fatty acids (PUFAs) in infantformula, and exposure to the oxidizing effects of iron supplementation contributed to a hemolyticanemia seen in preterm infants. In the United States and many developed countries, infantformulas now provide an adequate vitamin E:PUFA ratio to eliminate this risk. However, preterminfants continue to have low vitamin E levels due to limited stores, especially when the birth isextremely premature, and limited enteral feedings early in their postnatal neonatal intensive careunit course.The neonate who has anemia and is receiving iron supplementation, such as the infant describedin the vignette, requires the antioxidant effect of vitamin E to reduce red blood cell hemolysis. Atotal daily requirement of 10 to 25 IU of vitamin E meets the infant’s needs, only 50% of which isprovided by dietary formula. Of note, human milk also is an incomplete source of vitamin E.
81) Amniocentesis is useful in establishing the prenatal diagnosis of:-A. Down syndromeB. Meningomyelocele
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 20
C. Erythroblastosis fetalisD. Achondroplasia
Ans:-ABC82) USS can be used during pregnancy to:-
A. Determine crown rump lengthB. Determine fetal sexC. Determine biparietal diameterD. Accurately determine fetal weight
Ans ;-AC83) Gestation that produce multiple births:-
A. Are classified as high riskB. Are always delivered by cesarean sectionC. Can produce infant with discordance in body size at birthD. Aren't associated with the premature onset of labour
Ans:-AC84) For newborn infant, the least important factor to consider in assessing the risk of
kernicterus is:-A. Breast feedingB. AcidosisC. SepsisD. Albumin levelE. Moxalactam, cephalosporin type antibiotic
Ans:- A
85) The following maternal conditions are known to cause adverse effects on the neonate:A. Diabetes insipidus.B. Toxoplasmosis.C. Chronic myeloid leukaemia.D. SLE.E. Hyperthyroidism.
Ans:-BCDEExplanation:- Maternal SLE is a risk factor for neonatal lupus syndrome. The neonate presentswith clinical features of SLE due to transplacental passage of maternal Ab. The skin is frequentlyinvolved with malar rashes and there can be haematological and cardiac abnormalities. The mostfrequent heart abnormality is congenital heart block – 90% of mothers whose infants havecongenital heart block are anti-Ro(SSA)Ab positive.Toxoplasmosis leads to congenital infection by transplacental transmission. The rate oftransmission is +/- 60% of third trimester infections and 20%-30% during the first two trimesters.The ewborn presents with the classic triad of hydrocephalus, chorioretinitis, and cerebralcalcification.Maternal chronic myeloid leukaemia can have adverse effect on pregnancy – fetal/neonatalmortality is 16-38%. Pathology can be secondary to placental leukaemic infiltrates, anaemia andinfectious complications. Splenomegaly can restrict intrauterine growth and lead to prematuredelivery.
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 21
If hyperthyroidism is due to Grave’s disease or Hashimoto thyroiditis, the neonate may presentwith thyrotoxicosis due to the transplacental passage of TSI. These symptoms are frequentelyshort-lived i.e as long as the circulating antibodies persist in the baby’s circulation.
86) Each of the following statement about GBS infection in the newborn is true except:-A. Incidence is correlates inversely with the presence of maternal antibodiesB. The exotoxin has powerful pulmonary vasoconstrictive effectsC. The disease has two distinct pattern; early & late onsetD. Both the incidence & severity of the disease can be lessened by pretreatment of the
mother who is colonizedE. The risk of invasive disease isn't related to the amount of inoculum received by the
infant Ans:- E87) Newborn infant may present with bile stained vomiting and abdominal distension as the
result ofA. Oesophageal atresiaB. Duodenal atresiaC. Birth asphyxiaD. Electrolyte disturbanceE. Cystic fibrosis
Ans:-BCDE88) The following feature are consistent with newborn infant having oesophageal atresia and
tracheo-oesophageal fistula:-A. Maternal polyhydramnioseB. Passage of wide bore orogastric catheter into the stomachC. Plain x-ray evidence of air in the stomach and small bowelD. Plain x-ray evidence of hemivertebraE. Excessive mucus in the nostrils or mouth.
Ans:-ACDE89) Vitamin K
A. Is an essential cofactor for the synthesis of coagulation factor II , VII, IC, CB. Is readily transported across the placentaC. Is present in the breast milk at higher concentration than in cow milk.D. Given in single oral dose after delivary effectively prevent s hemorrhagic diseaseE. Related hemorrhage in the newborn is commoner when mother have taken
anticonvulsant during pregnancy Ans:-AE90) The following are recognizable causes of neonatal convulsion:-
A. Birth asphyxiaB. HypoglycemiaC. HypothermiaD. Opiate withdrawalE. Hypernatremia
Ans:-ABDE91) With regard to Apgar score:-
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 22
A. 2 points given to pulse of 88/minB. 1 point is given for irregular gaspsC. An initial satisfactory score gurarantees an eventual perinatal periodD. Score of 2 at 10 min carries worse prognosis than score of 2 at 5 minE. The lowest possible score is 1
Ans:-BD92) Intrauterine posture is commonly responsible for:-
A. Congenital dislocation of the hipB. PlagiocephalyC. Sternomastoid shorteningD. SyndactylyE. Mandibular asymmetry
Ans:-ABCE93) Established neonatal screening tests include:-
A. Umbilical cord blood analysis to detect phenylketonuriaB. Umbilical cord blood analysis to detect galactoseC. Umbilical cord blood analysis to detect sickle cell diseaseD. Capillary blood analysis at 6-8 days to detect elevated TSHE. Capillary blood analysis at 6-8 days to detect elevated immunoreactive trypsin
Ans:-CDE
94) Maternal condition that may have effect in the neonatal period include:-A. ITPB. Multiple sclerosisC. DMD. Varicella zosterE. Bornholm disease
Ans:-ACDE95) Neonatal polycythemia :-
A. Occur in small for date infant as response to placental insufficiencyB. Has an increased incidence if maternal diabetes is poorly controlledC. Carry an increased risk of cerebral venous sinus thrombosisD. Is recognizable feature of congenital hypothyroidismE. May occur as result of feto-maternal transfusion
Ans:-ABCD96) Polycythemia on the newborn is characterized by all of the following except:-
A. Increased the incidence in IDMB. Placental transfusion decreased by late clamping of the umbilical cordC. Clinical presentation that includes jitteriness & poor feedingD. Complication including heart failure & NECE. Elevated viscosity of whole blood
Ans;- B97) Causes of neonatal polycythemia include:-
A. Congenital rubella infection
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 23
B. Pre-eclampsiaC. Maternal diabtus mellitusD. Delayed clamping of umbilical cordE. Congenital adrenal hyperplasia
Ans:- BCDE98) Meconium aspiration pneumonia:-
A. Occur with equal frequency in term and preterm infantB. In infant required ventilation for this condition, combination of high PEEP and
rapid rate is advisableC. Has high risk of developing even if liquor is only thinly stainedD. High dose steroid are the mainstay of treatmentE. Antibiotic treatment is an important part of treatment
Ans :- all False99) The following statement are true regarding hemolytic disease of newborn ( HDN ):_
A. Hemolytic disease should be suspected if jaundice is noted in the first 24 hour oflife
B. HDN may occur if mother is group A +ve and the baby is group O+veC. If due to Rh –incompatibility the severity of the hemolysis typically increase with
each affected pregnancyD. HDN due to ABO incompatibility can be detected at 36 week gestation by
amniocentesisE. As long as the level of unconjugated bilirubin never rises above20 mg/dl there is no
dangerous of kernicterus Ans:-AC100) Full term infant has tachypnea with grunting , chest X ray show well expanded lung
with streaky shadows radiating from the bilateral hilar region , the most likely diagnosisis :-
A. TTNB. Congenital pneumoniaC. BPDD. Meconium aspirationE. Aspiration pneumonia
Ans:- A101) Condition associated with polyhydramniose include:-
A. Oesophageal atresiaB. Down's syndromeC. Renal agenesisD. Cord around the neckE. CNS malformation
Ans:- ABE102) The following are causes of polyhydramnios:
A. Maternal diabetes mellitus.B. Potter syndrome.C. Anencephaly.D. Oesophageal atresia.
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 24
E. Polycystic kidneys. Ans:-ACD
103) The following are causes of polyhydramniose:-A. Pottrer syndromeB. TEF and oesophageal atresiaC. Rh – incompatibilityD. AnencephalyE. Maternal diabetus
Ans:-BDE104) For necrotizing enterocloitis:-
A. Term baby are particularly at riskB. Perinatal asphyxia is risk factorC. Expressed breast milk from milk bank confer no protectionD. Failure of temperature control is late signE. High platelet count is frequently seen
Ans:- B105) You diagnose necrotizing enterocolitis in a preterm neonate who has abdominal
distention and blood in the stool. You decide that this infant should be placed on a 14-dayregimen of parenteral nutrition.Of the following, the micronutrient for which weeklymonitoring is MOST recommended during this infant’s parenteral nutrition therapy is
A. copper B. iron C. phosphorus D. selenium E. zinc Preferred Response: CParenteral nutrition (PN), the intravenous administration of carbohydrates, lipids, amino acids,and micronutrients, is an important component in the management of a variety of chronicdisorders, including surgical conditions (eg, omphalocele, gastroschisis, diaphragmatic hernia,short bowel syndrome), inflammatory conditions (eg, Crohn disease, ulcerative colitis,pseudomembranous colitis, pancreatitis, graft versus host disease), hypermetabolic states (eg,burns, trauma), and intestinal motility disorders (eg, pseudo-obstruction). PN is especiallyimportant in the support of very low-birthweight infants, who frequently have increased caloricrequirements, decreased oral intake, and immature intestinal motility. In addition to glucose, amino acids, sodium, potassium, and chloride, PN provides additionalmineral supplements, including calcium, phosphorus, magnesium, zinc, copper, selenium,chromium, manganese, molybdenum, and iodide. In preterm infants, the administration of bothcalcium and phosphorus is important to prevent metabolic bone disease.However, the amount of calcium and phosphorus that can be administered in PN must be limitedbecause of the risk of precipitation in the PN and formation of calcium-phosphorus complexesthat could embolize. It generally is thought that the chance of precipitation is high if the productof the concentrations (in mmol/L) of the calcium and phosphorus in PN is greater than 40.Because hypophosphatemia can have significant consequences (including impaired cardiacfunction, muscle weakness, and hemolysis), it is recommended that serum phosphorusconcentrations be assessed at least once weekly for patients receiving PN. The serum
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 25
concentrations of copper, iron, selenium, and zinc, which are trace elements, require only periodicassessment (eg, once a month or less).
106) An 1,800-g preterm infant is recovering from surgery for gastroschisis. Of thefollowing, the MOST correct statement regarding this infant’s immediate dailynutritional requirements is that he
A. can meet energy needs from fat through enteral feeding B. can meet protein needs for growth through enteral feeding C. requires lysine supplementation to promote protein synthesis D. requires more protein per kilogram than a term infant E. requires 2.5 g/kg per day of protein Preferred Response: DMilk remains the principal source of nutrition for infants, who consume 120 to 150 mL/kg per dayin the newborn period.Human milk has 67 kcal/100 mL, and most term infant formulas have a similar composition. Theenergy derived from ingesting milk comes primarily from fat calories (3.8 g/100 mL = 34kcal/100mL), followed by carbohydrates (lactose, 7 g/100 mL = 28 kcal/100 mL) and minimally fromprotein (1.3 g/100 mL = 5 kcal/100 mL). Conditions such as prematurity, lung disease, or surgerymay increase both caloric and specific nutrient requirements for newborns. The newborn described in the vignette can only take limited enteral nutrition and has anincreased need for both protein and calories to facilitate healing and growth. The normal 2 to 3g/kg per day of protein ingested by the term infant who is either formula- or breastfed isinadequate for this low-birthweight, preterm newborn. He will grow and heal best receiving 3.5 to4.0 g/kg per day of protein. The potential benefits of single amino-acid supplementation, suchas lysine, remain unknown.
107) Hypoxic-ischemic encephalopathy all are correct except:-A. Result from excessive use of oxytocinB. IUGR is be first indication of fetal hyoxiaC. Associated with increased beat to beat variabilityD. Prognosis depend on gestational ageE. Persistent of abnormal neurological sign at two week indicate poor prognosis
Ans:- C
108) polyhydramniose:-A. Is defined as an amniotic fluid volume of more than 500 mlB. Occur with increased frequency in diabetic pregnancyC. Is associated with renal agenesisD. Is associated with tracheo-oesophageal fistulaE. Is associated with increased risk of premature labor
Ans :-BDE109) Polyhydramnios is associated with all of the following condition except:-
A. Amniotic fluid volume between 500-2000 mlB. Maternal diabetes
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 26
C. TwinsD. Erythroblastosis fetalisE. Down syndrome
Ans:- A110) Condition associated with oligohydramnios include:-
A. Infantile polycystic kidneyB. Congenital heart diseaseC. IUGRD. High intestinal obstructionE. Posterior urethral valve
Ans:- ACE111) Regarding hyaline membrane disease ( HMD)
A. Can occur in infants of diabetic mother of 37-40 week gestationB. Infant born to mothers who are heroin addicts are at increased risk of HMDC. Light-for –date infant of 33 weeks gestation has greater risk of developing
HMD than 33 week infant of appropriate weightD. Administration of artificial surfactant is curativeE. Chest x-ray finding are markedly different between cases of HMD and Group
B streptococcal pneumonia Ans:- A
112) Hyaline membrane disease:-A. Is more common in babies of diabetic motherB. Is due to surfactant deficiencyC. Is not seen in term babiesD. Occur most commonly at 12 hour post-delivaryE. Always require ventilation
Ans:- AB113) The following symptoms in an infants in the first month of life should alert one to
possibility of hypothyroidism:A. Prolonged jaundiceB. VomitingC. DiarrheaD. Hoarse cryE. Voracious appetite
Ans:- AD
114) The following malformation can occur in children born to mother who have IDDM:A. Cleft lip/ palateB. Caudal regression syndromeC. Femoral hypoplasiaD. HolopresencaphalyE. Polydactyly
Ans:- BCDE115) With regard to RDS of the newborn
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 27
A. Meconium aspiration pneumonia is especially likely to be the cause if the infant ispreterm
B. HMD is unlikely to be the cause if the prepartum lecithin sphingomylin (L/S) ratioin amniotic fluid is > 2;1
C. Patchy opacities on chest X-ray are evidence in favour of diagnosis HMDD. In the artificial ventilation of infant with HMD , inflation pressure must never
exceed 30 cm of waterE. CPAP is an effective in treatment for Pneumothorax
Ans : B116) In RDS due to meconium aspiration
A. Antibiotic therapy is of crucial importanceB. Steroid therapy improve the prognosisC. There is high risk of PneumothoraxD. Chest X-ray typically shows ground glass opacityE. The infant may also suffer from cerebral oedema
Ans:-C117) Recognized association of small-for-date babies include
A. Maternal smoking in pregnancyB. Hemolytic disease due to ABO incompatibilityC. Pre-eclamptic toxaemiaD. Congenital rubella infectionE. Fetal alcohol syndrome
Ans:- ACDE118) Prolonged neonatal jaundice is recognized feature in infants with
A. CMV infectionB. Congenital hypothyroidismC. Untreated urinary tract infectionD. Tracheo-oesophageal fistulaE. Galactosemia
Ans:- ABCE119) In baby of 32 week gestation who has tachypnea and sternal recession at 4 hour of age:
A. The ductus arteriosus is likely to be patentB. Meconium aspiration pneumonia is likely to be diagnosisC. The L/S ratio is likely to be lowD. Fluid level on chest X-ray suggest pneumonia due to Group B streptococcusE. The presence of bowel shadows on the left side of the chest on X-ray is
diagnostic of Tracheo-oesophageal fistula Ans :-AC
120) The following condition characteristically cause jaundice within the first 24 hour of life:-A. G6PD deficiencyB. Congenital hypothyroidismC. Sever congenital CMV infectionD. Choledochal cystE. Primary tyrosinaemia
Ans:- AC
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 28
121) Hypothermia can cause the following in LBW infant:-A. Decrease synthesis of surfactantB. HypernatremiaC. HypoglycemiaD. Increased oxygen consumptionE. Hypercalcemia
Ans :- ACD122) The following substance are freely transmitted across the placenta:-
A. CarbimazoleB. DiazepamC. WarfarinD. PethidineE. IgM antibodies
Ans:-ABCD123) In congenital diaphragmatic hernia:-
A. Hernia most commonly occur on the leftB. Pulmonary hypoplasia is the major cause of deathC. Persistent fetal circulation occurs uncommonlyD. Associated congenital anomalies are commonE. Most present between 12-24 hours of life
Ans:- ABThe incidence of CDH is between 1/2,000 and 1/5,000 live births, with females affected twice asoften as males. Defects are more common on the left (85%) and are occasionally (<5%) bilateral.Pulmonary hypoplasia and malrotation of the intestine are part of the lesion, not associatedanomalies. Most cases of CDH are sporadic, but familial cases have been reported. Associatedanomalies have been reported in up to 30% of cases; these include central nervous system lesions,esophageal atresia, omphalocele, and cardiovascular lesions. CDH is recognized as part of severalchromosomal syndromes: Trisomy 21, Trisomy 13, Trisomy 18, Fryn, Brachmann–de Lange,Pallister-Killian, and Turner. Relative predictors of a poor prognosis include an associated majoranomaly, symptoms before 24 hr of age, severe pulmonary hypoplasia, herniation to thecontralateral lung, and the need for ECMO.
124) In the normal newborn infant in the first 24 hour of life:-A. Many significant heart defect may be clinically undetectableB. Normal arterial PaO2 help the ductus to closeC. Hypoxia causes pulmonary artery vasoconstrictionD. All children with murmur heard in the first 24 hour should be followed up for
at least 6 monthsE. The systolic blood pressure is between 40-80 mmHg
Ans:-ABCE125) A light –for-date full term baby is at particular risk from the following condition:-
A. HMDB. Physiological jaundiceC. Milk aspirationD. Hypoglycemia
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 29
E. Apnoeic attacke Ans:- D
126) Recurrent apnoea of prematurity:-A. Characteristically develop within the first 24 hour of lifeB. Is more likely to occur in infant of < 32 week gestationC. Usually respond to naloxoneD. Should be treated with 100% oxygen during attackE. May be accentuated by the presence of nasogastric tube
Ans:- BE127) In the management of HMD:
A. Tolazoline may lead to systemic hypertensionB. Early use of CPAP may reduce the need for subsequent ventilatory supportC. Antibiotic improve ventilation- perfusion ratioD. The illness may be expected to increase in the severity for the first 5 daysE. Corticosteroid used postnatally have beneficial effect on the course of the
disease Ans:- B
128) Characteristic finding in preterm baby include:-A. Chin reaching only to the tip of shoulderB. Full wrist flexionC. Flat on couch when lying proneD. Incomplete ankle dorsiflexionE. Incomplete knee extension with hip fully flexed
Ans:- C129) Drug effects on the fetus:-
A. Isotretinion can lead to CNS defects mainly if given in the third trimesterB. Phenytoin can lead to cleft lip, finger and toe abnormalities mainly if given in
the second trimesterC. Carbimazole cause goiter, mainly if given in the third trimesterD. Warfarine can lead to neonatal hemorrhage mainly if given in the first
trimesterE. Valproate can lead to neural tube defects mainly if given in the third trimester
Ans:- C130) The external criteria for the Dubowitz score for gestational age include:-
A. Breast sizeB. Skin textureC. External genitaliaD. Langue hairE. Nose firmness
Ans:-ABCD131) Problem of babies born to mothers with poorly controlled diabetus mellitus:
A. HypermagnesemiaB. PolycythemiaC. HypocalcemiaD. Sacral agenesis
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 30
E. Respiratory distress Ans:-BCDE
132) The following are recognised associations of maternal diabetes:A. Sacral agenesisB. Intrauterine growth retardationC. MacrosomiaD. Hyaline membrane diseaseE. Hypertrophic cardiomyopathy
Ans:-ABCDEComments:Overall, malformations occur in 6%, with an increased incidence of cardiac malformations, sacralagenesis, hyperplastic left colon. Intrauterine growth retardation is 3 times as common due tosmall vessel disease in the mother. More common is macrosomia, and this is related to the degreeof maternal hyperglycaemia. The glucose crosses the placenta while the insulin does not, so thefetus increases its production of insulin. This results in increased cell number andsize. 25% of IDM are greater than 4kg compared with only 8% of non-diabetics. This givesproblems with delivery such as CPD, shoulder dystosia resulting in an increased incidence of birthasphyxia and trauma.In the neonatal period, hypoglycaemia, respiratory distress and reversible hypotrophiccardiomyopathy and polychthaemia are all more common. Gestational diabetes is whencarbohydrate intolerance occurs only during pregnancy. It is commonest in obese women andthose from Afro-Caribbean and Asian ethnic groups. In these women there is no increase incongenital malformations, thoug macrosomia and other complications remain similar infrequency.
133) Characteristic finding in full term baby are:-A. Full knee extension with hips fully flexedB. Momentary neck extension when held sittingC. Chin reach beyond tip of shoulderD. Hip abducts and legs flat on couch when lying supineE. Full ankle dorsiflexion
Ans:- BE134) The external criteria for the Dubowitz score for gestational age include:-
A. Nipple formationB. Ear form & firmnessC. Skin colour & opacityD. Protruding tongueE. Planter creases
Ans:- ABCE
135) In fetal circulation:-A. 30% of the fetal cardiac output goes through the placentaB. Oxygenated blood from the placenta passes through the ductus arteriosus toward
the right atriumC. The oxygen saturation of blood in umbilical arteries is approximately 60%
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 31
D. Blood entering the heart from the inferior vena cava is diverted directly to the leftatrium via patent foramen ovale
E. There is one umbilical vein Ans:- CDE
136) The following disease can now be diagnosed prenatally:-A. PhenylketonuriaB. HomocystinuriaC. Sever combined immunodeficiencyD. Fanconi's anaemiaE. Lesh-Nyhan syndrome
Ans:- ABCDE137) Resuscitation of neonate with coarctation of aorta may require the use of :-
A. FrusemideB. BicarbonateC. IndomethacinD. DopamineE. Prostaglandin E
Ans:- ABDE138) Recognized causes of the floppy baby include:-
A. Trisomy 21B. Zellweger syndromeC. Becker muscular dystrophyD. Spinal muscular atrophyE. Hypothyroidism
Ans:- ABDE139) Which of the following may cause apnoea in preterm infant
A. HypocalcemiaB. HypoglycemiaC. RSV infectionD. CaffeineE. Intraventricular hemorrahage
Ans:- ABCE140) Failure of resuscitation of newborn may be due to :-
A. PDAB. VSDC. Congenital diaphragmatic herniaD. Pulmonary hypoplasiaE. HMD
Ans:-CD141) Feature of IUGR include:-
A. NeutropeniaB. HypoglycemiaC. Necrotizing EnterocolitisD. Weight loss > 10% of birth weight in first weekE. Thermal instability
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 32
Ans:- ABCE142) Newborn infant has breathing difficulty with central cyanosis .Nitrogen washout test
raised the PO2 to 15 kPa possible diagnosis include:-A. Fallot's tetralogyB. VSDC. PneumoniaD. Tricuspid atresiaE. HMD
Ans:- CE143) Newborn infant has central cyanosis and fit with slow & shallow breathing , Nitogen
washout test produce slight raise in the PO2 , the most likely cause of cyanosis is:-A. MethemoglobinemiaB. Cerebral disorderC. Persistent fetal circulationD. Congenital cyanotic heart diseaseE. Lung disease
Ans:- B144) The following disease can now be diagnosed prenatally:-
A. HypercholesterolemiaB. Polycystic kidney diseaseC. CystinosisD. Gaucher's diseaseE. Beta thalassaemia
Ans:-ABCDE145) Common causes of seizure in the neonatal period include:-
A. Intracranial hemorrhageB. Electrolyte disturbanceC. InfectionD. Drug withdrawalE. Febrile convulsion
Ans:- ABCD146) Neonatal convulsion may be caused by :-
A. HypomagnesaemiaB. HyperkalamiaC. Pyridoxine dependencyD. CephalohematomaE. HSV infection
Ans:- ACE
147) The following disease can now be diagnosed prenatally:-A. Sickle cell diseaseB. Maple syrup urine diseaseC. RetinoblastomaD. HypophosphaturiaE. Von-Willebrand disease
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 33
Ans:- ABCDE148) Which of the following statement regarding surfactant therapy is correct :-
A. The incidence of Pneumothorax is reducedB. The incidence of intraventricular hemorrhage is reducedC. Early therapy ( within 4 hour) is more beneficial than later administration ( after
12 hour)D. Prolonged courses of surfactant therapy confer advantagesE. The incidence of chronic lung disease is increased
Ans:- ABC149) Which of the following statement regarding periventricular hemorrhage are correct:
A. Most hemorrhage occur after the fourth day of lifeB. Over 80% of hemorrhage progress to ventricular dilatationC. Most cases of posthemorrhagic hydrocephalous are communicatingD. Early ventricular tapping improve the neurological outcomeE. Hemorrhage is usually caused by hypoglycemia
Ans:- C150) Complication of phototherapy include:-
A. DiarrheaB. Erythematosus rashC. HyponatremiaD. Skin discolorationE. Peripheral desqumation
Ans:- ABD151) Which of the following are characteristic haemodynamic changes encountered at birth:-
A. Increase the pulmonary vascular pressureB. Right to left flow through the ductus arteriosusC. Closure of the ductus arteriosusD. Increased right ventricular end diastolic pressureE. Reversal of flow across the foramen ovale
Ans:- C152) Feature suggestive of TEF with oesophageal atresia include:-
A. FTTB. Recurrent pneumoniaC. OligohydramnioseD. Large amount of mucus in the pharynx at delivaryE. Slow to establish feed
Ans:- D
153) The development of Pneumothorax is associated with :-A. Surfactant therapyB. Artificial paralysisC. Patient triggered ventilationD. Meconium aspirationE. Pulmonary interstitial emphysema
Ans:- DE
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 34
154) Cyanotic congenital heart disease in the newborn include:-A. TGAB. Pulmonary stenosisC. Fallot's tetrallogyD. VSDE. Tricuspid atresia
Ans:- AE155) The following congenital disorder require immediate ( within first week) treatment after
birth:-A. HemangiomaB. Imperforate anusC. Choanal atresiaD. HypospadiusE. Congenital diaphragmatic hernia
Ans:-BCE156) Causes of neonatal hypoglycemia include;-
A. Erythroblastosis fetalisB. Glycogen storage disease type IC. Maternal treatment with sodium valproateD. GalactosemiaE. Congenital adrenal hypoplasia
Ans:- ABDEPlasma glucose level of <40 mg/dL, During gestation, glucose is freely transferred across theplacenta by the process of facilitated diffusion. However, after birth, the infant must adjust to thesudden withdrawal of this transplacental supply. In all infants, there is a nadir in blood sugarbetween 1 and 3 hours of life. During the first 12-24 hours of life, newborns are at increased riskfor hypoglycemia because gluconeogenesis and especially ketogenesis are incompletelydeveloped. These factors are accentuated in preterm infants, infants of diabetic mothers, infantswith erythroblastosis fetalis, asphyxiated infants, and infants who are small or large for gestationalage.
Transient hypoglycemia causes:- prematurity, hypothermia, Birth asphyxia, sepsis,erythroblastosis fetalis, infants with Beckwith-Wiedemann syndrome, maternal diabetes,maternal glucose infusion in labor, and intrauterine growth restriction (IUGR)and maternaldrugs( b sympathomimetic and chlorpropamide).Persistent hypoglycemia may be due to: - inborn error of metabolism (Glycogen storagedisease type I , P & IV, maple syrup urine disease, Nesidioblastosis, galactosemia,andmitochondrial fatty acid oxidation defects such as MCAD deficiency. Hormonal deficiencysuc as congenital hypopituitrism,congenital glucagons deficiency and cortisol deficiencystates including congenital adrenal hypoplasia.Features on physical examination suggest the etiology of hypoglycemia:-
· Macrosomia: This occurs in infants of diabetic mothers, infants with severe congenitalhyperinsulinism, and infants with Beckwith-Wiedemann syndrome; recall that insulin is agrowth factor and that hyperinsulinism leads to macrosomia.
· Midline defects: Congenital pituitary deficiency can be associated with midline defectssuch as cleft lip, cleft palate, single central incisor, and micro-ophthalmia.
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 35
· Micropenis: Congenital gonadotropin deficiency and possible pituitary abnormalities causethis condition.
· Hepatomegaly: This is associated with glycogen storage diseases and fatty acid oxidationdisorders.
157) Healthy term neonate differ from adult in the following way:-A. Less complementB. Decrease IgG levelC. Fewer B lymphocytesD. Lower level of secretory IgAE. Higher level of C reactive protein
Ans:- AD158) Necrotizing enterocloitis is recognized complication of:-
A. PolycythemiaB. Umbilical arterial catheterizationC. Parenteral feedingD. Maternal Crohn's diseaseE. Birth asphyxia in term neonate
Ans:- ABE159) NEC is associated with:-
A. EpidemicB. ThrombocytopeniaC. MalabsorptionD. Bile stained aspirateE. Air in the portal tree on abdominal X –ray
Ans:- ABCDE160) The presenting feature of NEC include:-
A. ApnoeaB. BradycardiaC. Abdominal distensionD. Intramural gas on abdominal X rayE. Bloody stool Ans:- ABCDE
161) A 3-week-old breastfed infant presents to the emergency department with irritability,fever, jaundice, and hepatomegaly. A laboratory evaluation shows a normal complete bloodcount and a bilirubin concentration of 6.5 mg/dL (111.2 mcmol/L). A urinalysis is positive forreducing substances. A blood culture is positive for Escherichia coli. You initiate antibiotictherapy Of the following, the MOST appropriate dietary management of this patient is to
A. continue breastfeeding B. switch to a cow milk-based formula C. switch to a soy-based formula D. switch to a whey hydrolysate formula E. switch to an elemental formula Preferred Response: C
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 36
The clinical features of jaundice, hepatomegaly, and invasive Escherichia coli infection describedfor the neonate in the vignette suggest the possible diagnosis of galactosemia.Galactosemia is an autosomal recessive disorder most commonly caused by a deficiency of theenzyme galactose-1-phosphate uridyltransferase. The reducing substances in the urine representthe accumulation of galactose. In addition to recognizing and treating the gram-negative infectionin the infant, it is important to remove lactose, which is comprised of glucose and galactose,from the diet as soon as the diagnosis is suspected. Soy protein formulas are the first choice of nutrition for infants who have suspected or provengalactosemia because the carbohydrate source in these formulas is sucrose or corn syrup ratherthan lactose. Protein hydrolysate and elemental formulas also contain other carbohydrates thanlactose, but they can be more expensive and less readily available than soy formulas. Lactose isthe primary carbohydrate in human milk, cow milk-based formulas, and most whey hydrolysateformulas.
162) Hydrops fetalis may be associated with :-A. Rhesus isoimmunizationB. Paroxysmal supraventricular tachycardiaC. CMV infectionD. AchondroplasiaE. Renal vein thrombosis
Ans:- ABCDE
163) The following drugs are correctly paired with their potential teratogenic effect:-A. Alcohol & macrocephaly with congenital heart diseaseB. Phenytoin & meningomyeloceleC. Isotretinoic acid & cutis laxis syndromeD. Penicillamine & facial abnormalities with pinna defectsE. Lithium & Ebtein's anomaly
Ans:-BCDE
Warfarine Hypoplastic nasal bridge ,chrondroplasi puncta Isotretinoic acid facial , ear , cardiovascular abnormality Phenytoin Hypoplastic nail, IUGR, typical facies & may be associated withneural tube defect Tetracyclin Enamel hypoplasia Sodium Valproate Neural tube defect
164) The neonate of mother with SLE may demonstrate:-A. PolythycemiaB. RashC. NeutropeniaD. Atrial fibrillationE. Anti-Ro antibodies
Ans:- BCE165) Pulmonary hypoplasia is consequence of :-
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 37
A. Congenital varicella zosterB. AnencephalyC. Posterior urethral valveD. Congenital diaphragmatic herniaE. Exomphalos
Ans:- BCDE166) The following conditions may present with bile-stained vomiting in the first week of life:-
A. Duodenal atresiaB. Cystic fibrosisC. Inguinal herniaD. GERE. NEC
Ans:- ABCE167) Renal immaturity in normal neonate born at term is manifested as:-
A. Reduced number of nephronsB. Decreased glucose reabsorptionC. Increased glomerular filteration rateD. Decreased renal bicarbonate reabsorptionE. Decreased urea excretion
Ans:- BDE
168) The following maternal factors increase the incidence of surfactant deficient RDS:-A. Steroid therapyB. OpiateC. Placental insufficiency leading to IUGRD. DiabetusE. Alcoholism
Ans:- D169) Bacteria commonly isolated in case of neonatal meningitis include:-
A. Escherichia coliB. Haemophilus infuenzaeC. Group B streptococcusD. Staphylococcu epidermidisE. Neisseria meningitis
Ans:- AC170) In the infant of diabetic mother :-
A. The infants brain size is increased beyond normalB. The infant's liver size is increased beyond normalC. He can be small for gestational ageD. There is an increased incidence of polycythemiaE. He has an increased incidence of hypertrophic Cardiomyopathy
Ans:- BCDE171) Galactosaemia:-
A. Is caused by deficiency of the enzyme galactokinase
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 38
B. Causes jaundice in the newbornC. May present with cataract at birthD. Is associated with Escherichia coli septicemiaE. Is diagnosed as result of screening in the majority of cases.
Ans:- BCD172) SVT in neonate:-
A. Is the most common abnormal tachycardiaB. Reflect underlying congenital heart disease in the majority of casesC. Show regular rate of 160-220 beats /min on the ECGD. Recurrent episodes usually persist into adulthoodE. May be stopped with rapid I/V bolus of adenosine
Ans:- A E173) Neonates suffering withdrawal from in utero exposure to narcotics may show sign of
A. IrritabilityB. VomitingC. PhotophobiaD. HypotoniaE. Diarrhea
Ans:- ABCE174) Clinical feature of congenital hypothyroidism diagnosed in the newborn period include:-
A. Large tongueB. Presence of third fontenalleC. Umbilical herniaD. Loose stoolsE. High incidence of mental retardation
Ans:- A C
175) Causes of persistent neonatal unconjugated hyperbilirubinemia after 2 weeks include:-A. Rhesus incompatibilityB. HypothyroidismC. Breast milk jaundiceD. Rotor syndromeE. Sepsis
Ans:- ABCE176) Growth retardation babies are at increased risk of:-
A. PolycythemiaB. HMDC. HypoglycemiaD. Group B streptococcal infectionE. Sudden intrapartum death
Ans:- ACE177) Oesophageal atresia is associated with:-
A. Maternal polyhydramnioseB. Vertebral anomaliesC. Diaphragmatic hernia
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 39
D. Low birthweightE. Duplex collecting system
Ans:- ABDE178) Congenital Rubella:-
A. Is associated with cerebral calcificationB. Frequently lead to cataractC. Is associated with VSDD. Rarely occur following maternal infection in the third trimesterE. Should be prevented by vaccinating women found to be seronegative during the
first trimester Ans:- B D
179) Human breast milk contain:-A. Secretory IgAB. MacrophagesC. LysozymeD. Vitamin cE. Zinc
Ans:- ABCDE180) The following are recommended daily requirement for 1 month old child /hg of B wt:-
A. Fluids 150-180 ml orallyB. Calories 90-115 kcalC. Sodium 1.25-2.5 mmolD. Protein 2.2-3.5 gmE. Potassium 2.0-3.5 mmol
Ans:- ABCDE
181) Compared with cow's milk, human breast milk contains:A. Less sodium.B. Less calcium.C. Less protein.D. Less fat.E. Less carbohydrate.
Ans:-A B C
182) UK infants are routinely immunised against:A. Meningococcus type B.B. Diphtheria.C. Cholera.D. Polio.Pertussis.
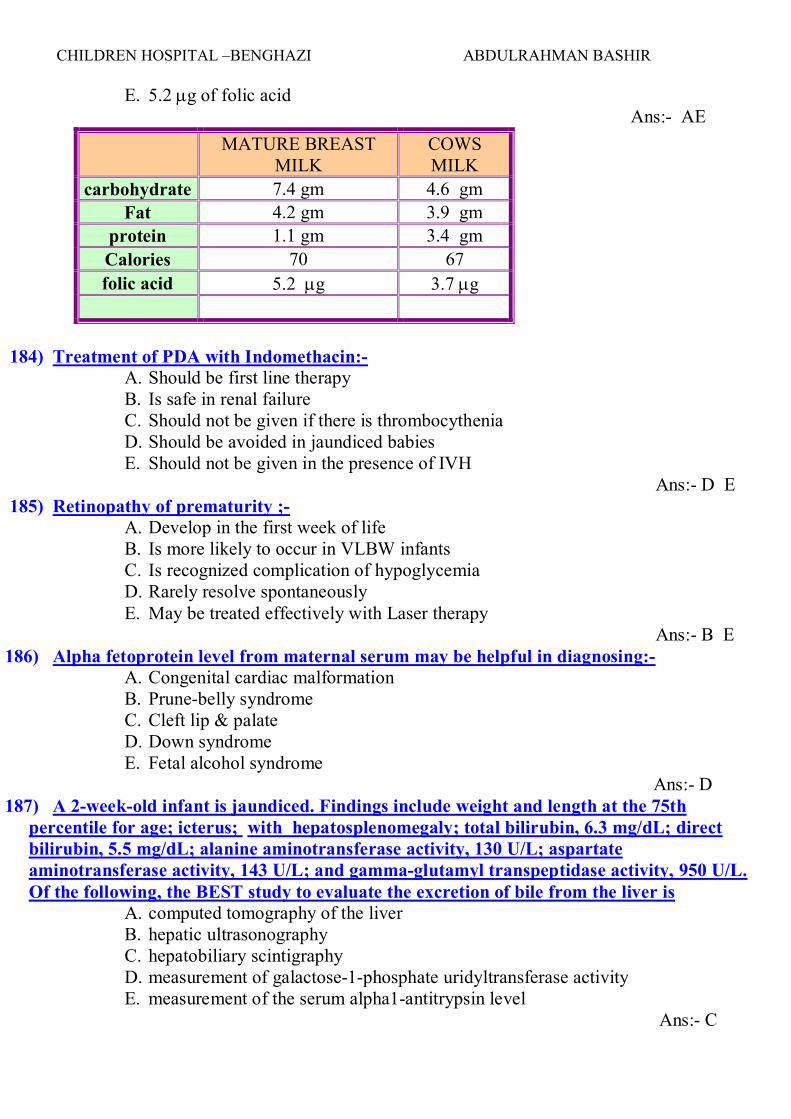
Ans:-B D E183) Mature breast milk contain per 100 ml;-
A. 60-75 kcalB. 8-10 gm of proteinC. 0.1-0.5 gm of fatD. 0.1-0.5 gm of carbohydrate
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 40
E. 5.2 mg of folic acid Ans:- AE
MATURE BREASTMILK
COWSMILK
carbohydrate 7.4 gm 4.6 gmFat 4.2 gm 3.9 gm
protein 1.1 gm 3.4 gmCalories 70 67folic acid 5.2 mg 3.7 mg
184) Treatment of PDA with Indomethacin:-A. Should be first line therapyB. Is safe in renal failureC. Should not be given if there is thrombocytheniaD. Should be avoided in jaundiced babiesE. Should not be given in the presence of IVH
Ans:- D E185) Retinopathy of prematurity ;-
A. Develop in the first week of lifeB. Is more likely to occur in VLBW infantsC. Is recognized complication of hypoglycemiaD. Rarely resolve spontaneouslyE. May be treated effectively with Laser therapy
Ans:- B E186) Alpha fetoprotein level from maternal serum may be helpful in diagnosing:-
A. Congenital cardiac malformationB. Prune-belly syndromeC. Cleft lip & palateD. Down syndromeE. Fetal alcohol syndrome
Ans:- D187) A 2-week-old infant is jaundiced. Findings include weight and length at the 75th
percentile for age; icterus; with hepatosplenomegaly; total bilirubin, 6.3 mg/dL; directbilirubin, 5.5 mg/dL; alanine aminotransferase activity, 130 U/L; aspartateaminotransferase activity, 143 U/L; and gamma-glutamyl transpeptidase activity, 950 U/L.Of the following, the BEST study to evaluate the excretion of bile from the liver is
A. computed tomography of the liverB. hepatic ultrasonographyC. hepatobiliary scintigraphyD. measurement of galactose-1-phosphate uridyltransferase activityE. measurement of the serum alpha1-antitrypsin level
Ans:- C
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 1
188) Which of the following constellations of features BEST describes the fetal alcoholsyndrome?
A. Elfin facies, irritability, and supravalvular aortic stenosisB. Growth deficiency with microcephaly, developmental delay, and short palpebral
fissuresC. Intrauterine growth retardation, triangular-shaped face, and clinodactyly of the
fifth fingerD. Short stature, webbed neck, and pulmonic stenosisE. Weakness, club feet, immobile face, and inadequate respirations
Ans:- B189) A female infant born to a 24-year-old woman has been diagnosed clinically as having
Down syndrome. The mother is concerned about her risk of having another child who has achromosomal abnormalityThe statement that you are MOST likely to include in yourdiscussion is that her risk
A. can be estimated by determination of maternal serum alpha-fetoprotein in allfuture pregnancies
B. cannot be estimated until her infant's chromosome complement has beendetermined
C. is increased for Down syndrome, but not for any other chromosomal abnormalityD. is no greater than that of any other woman her ageE. is not increased until she reaches the age of 35
Ans:- B190) During delivery of an infant who has an estimated gestational age of 42 weeks, you note
that the amniotic fluid looks like pea soup and contains thick particles of meconium. Of the following, the MOST important initial step in resuscitation of the infant is to :-
A. aspirate the gastric contentsB. determine the Apgar score initiate tracheal intubationC. provide positive pressure ventilationD. suction the hypopharynx
Ans:- D
191) In addition to irritability, sweating, and difficulty breathing with feeding, the symptomthat is MOST indicative of congestive heart failure in a 3-week-old infant is
A. ascitesB. coughC. cyanosisD. diminished feeding volumeE. pretibial edema
Ans:- D192) The decreased incidence of enteric infections noted in breastfed infants compared with
formula-fed infants is MOST likely due to theA. more alkaline stool pH in breastfed infantsB. nutritional benefits of human milk on the infant's immune systemC. predominance of Bacteroides and Clostridium in the gut of breastfed infantsD. presence of protective antibodies against enteric infection in human milk
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 42
E. sterility of human milk Ans:- D
193) A newborn who weighs 600 g and whose estimated gestational age is 24 weeks at birth isadmitted to the neonatal intensive care unit after successful resuscitation in the deliveryroom. Arterial blood gas measurements on room air are: pH, 7.35; PCO2, 42 mm Hg; PO2,68 mm Hg; base deficit, 2 mEq/L. Of the following, the MOST appropriate initialmanagement is to
A. begin intravenous vancomycinB. begin phototherapyC. initiate enteral feedingD. provide bicarbonate infusionE. provide glucose infusion
Ans:- E194) A 3-day-old infant presents to the emergency department with vomiting, lethargy,
hypotonia, and jaundice. Physical examination reveals hepatomegaly and neurologicdepression. A full sepsis evaluation is undertaken, and the Gram stain of the cerebrospinalfluid reveals gram-negative organisms. Of the following, the BEST additional laboratorytest to obtain is
A. erythrocyte galactose-1-phosphateB. liver glycogen contentC. plasma insulin levelD. plasma very long-chain fatty acids.E. stool porphyrins
Ans:- A195) You are examining a term newborn in the nursery. His weight is 3.27 kg (50th
percentile), and his length is 50.5 cm (50th percentile). The pregnancy, labor, and deliverywere unremarkable. There are no significant findings on physical examination. The MOSTlikely head circumference in this child, if it is consistent with his other growth parameters, is
A. 31 cmB. 33 cmC. 35 cmD. 37 cmE. 39 cm
Ans:- D196) previously healthy 5-day-old male who was born at home develops bruising and melena.
The pregnancy, delivery, and postnatal course were unremarkable. The infant isbreastfeeding vigorously every 2 hours. Findings on physical examination are unremarkableexcept for several large bruises. Laboratory testing reveals: hemoglobin, 81 g/L (8.1 g/dL);white blood cell count, 9.4 x 109/L (9,400/mm3); prothrombin time, 37 seconds; partialthromboplastin time, 98 seconds; platelet count, 242 x 109/L (242,000/mm3); and fibrinogen,2.34 g/L (234 mg/dL). Of the following, the MOST likely cause of the bleeding is
A. disseminated intravascular coagulationB. factor VIII deficiency hemophiliaC. liver diseaseD. vitamin K deficiency
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 43
E. von Willebrand disease Ans:- D
197) A newborn whose estimated gestational age is 42 weeks is stained with meconium.Tracheal intubation reveals meconium in the hypopharynx as well as below the vocal cords.The infant has respiratory distress. A chest radiograph is obtained. Of the following, theMOST likely radiographic finding is
A. coarse infiltratesB. decreased lung volumesC. mediastinal shiftD. pleural effusionE. reticulogranular pattern
Ans:- A198) A 20-year-old primigravida at 30 weeks of gestation has a blood pressure of 160/112 mm
Hg, serum total bilirubin level of 44.5 mcmol/L (2.6 mg/dL), serum alanineaminotransferase level of 150 U/L, and platelet count of 75 x 109/L (75,000/mm3). She ishospitalized for observation and electronic fetal heart rate monitoring. Of the following, theMOST ominous sign of fetal distress during monitoring would be
A. early decelerationsB. increased beat-to-beat variabilityC. late decelerationsD. spontaneous accelerationsE. variable decelerations
Ans:- C199) A term newborn presents with bilious vomiting shortly after birth. Her abdomen is
distended slightly, and facial features are characteristic of Down syndrome. She has passeda normal meconium stool. The pregnancy was complicated by polyhydramnios. Of thefollowing, the MOST likely diagnosis is
A. duodenal atresiaB. Hirschsprung diseaseC. meconium ileusD. midgut volvulusE. pyloric stenosis
Ans:- A200) An 18-year-old primigravida at 32 weeks' gestation has a blood pressure of 148/96 mm
Hg, proteinuria, oliguria, and visual disturbances. Labor is induced, and the infant isdelivered. His weight is 850 g (<10th percentile), crown-heel length is 38 cm (10thpercentile), and head circumference is 30 cm (50th percentile). Of the following, the MOSTlikely complication in this infant is
A. anemia of prematurityB. hyaline membrane diseaseC. hyperglycemiaD. meconium aspirationE. perinatal asphyxia
Ans:- E
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 44
201) An infant is born at 27 weeks' gestation following a pregnancy complicated by pretermlabor that progressed despite administration of a tocolytic agent. Of the following, themost appropriate INITIAL management is to
A. measure transcutaneous oxygen saturationB. perform endotracheal intubationC. place an umbilical arterial catheterD. place the infant in an open bed warmerE. provide nasal continuous positive airway pressure
Ans:- D202) Of the following, the MOST important determinant of neurodevelopmental outcome of
VLBW infants isA. antenatal obstetric managementB. infant genderC. length of gestationD. maternal educationE. socioeconomic status
Ans:- C
203) You are called to the newborn nursery to examine an infant who appears dysmorphic.On physical examination, the baby is normally grown and vigorous. You note overfoldedpinnae, deviation of the nose to one side (Item Q25A), and a small chin. The feet aremaintained in dorsiflexion (Item Q25B), but can be corrected passively. You review thepregnancy history. Of the following pregnancy complications, the one MOST likely to beassociated with this baby’s features is
A. maternal hypertension B. polyhydramnios C. preeclampsia D. transverse lie E. vaginal bleeding Preferred Response: DThe infant described in the vignette displays the characteristic features of a deformation sequence.Unlike malformations, which occur due to intrinsic problems within a developing structure,deformations are due to mechanical forces acting on an otherwise normally developing embryo orfetus. Causes of fetal deformation are many and include oligohydramnios, prolonged breechpositioning, a small or malformed uterus, fibroid tumors of the uterus, and multiple gestations.Often, the affected infant has a pugilistic facies, with deviation of the nose to one side. Limbpositioning defects are common.Barring any association with malformations or disruptions, the appearance of the affected infanttypically normalizes over time. Although maternal hypertension and preeclampsia can be associated with placentalinsufficiency and, ultimately, decreased fetal movement, typically they are not associatedwith fetal deformation. Polyhydramnios usually is associated with unrestricted fetal movement,and fetuses are not deformed. Vaginal bleeding has multiple potential causes, most of which arenot associated with deformation.
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 45
Transverse lie is the only pregnancy complication listed that is likely to be associated withdeformation due to unusual fetal position
204) A 10-day-old infant who weighed 1,750 g at birth and whose gestational age was 34 weeksis jaundiced. His total serum bilirubin concentration is 10.0 mg/dL and the direct fraction is0.8 mg/dL. He is receiving intermittent orogastric feeding of expressed human milk andsupplemental parenteral nutrition. Of the following, the MOST likely explanation for thesefindings is
A. Crigler-Najjar syndromeB. jaundice due to parenteral nutritionC. neonatal hepatitisD. physiologic jaundiceE. pyloric stenosis
Ans:- D205) Early hospital discharge is defined as the discharge of a newborn earlier than 48 hours
following vaginal delivery or 96 hours following cesarean delivery. Of the following, theMOST common reason for readmission to the hospital within 7 days following an earlydischarge is
A. bacterial sepsisB. congenital heart diseaseC. gastrointestinal malformationD. hyperbilirubinemiaE. metabolic disorders
Ans:- D206) A newborn infant is delivered by emergent cesarean section at 41 weeks' gestation
following a pregnancy complicated by a prolapsed umbilical cord and meconium-stainedamniotic fluid. At 6 hours of age, the infant has a generalized tonic-clonic seizure. Of thefollowing, the MOST likely explanation for this seizure is
A. hyponatremiaB. hypoxic-ischemic encephalopathyC. intracranial hemorrhageD. meningitisE. pyridoxine dependency
Ans:- B207) A 4-hour-old newborn has copious oral secretions and episodes of coughing, choking, and
cyanosis. The pregnancy was complicated by polyhydramnios. You suspect esophagealatresia with tracheoesophageal fistula.Of the following, the MOST helpful test to confirm the diagnosis is to
A. inject a contrast medium through an orogastric catheter and obtain a neckradiograph
B. obtain computed tomography of the neckC. perform flexible bronchoscopyD. place an endotracheal tube and examine the endotracheal fluidE. place an orogastric suction catheter and obtain a chest radiograph
Ans:- E
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 46
208) A newborn is delivered by emergent cesarean section because of fetal distress followingacute abruption of the placenta. The infant is resuscitated and transferred to the nursery.On physical examination, she appears pale, and her extremities are cold to touch. Thecapillary refill is 8 seconds. Results of an arterial blood gas analysis show a Po2 of 48 mmHg. Of the following, the MOST likely additional finding is
A. decreased bicarbonate concentrationB. hypercalcemiaC. hyperglycemiaD. hyponatremiaE. normal anion gap
Ans:- A209) Of the following, erythromycin prophylaxis is MOST likely to prevent ocular infection
due toA. Chlamydia trachomatisB. group B streptococciC. Neisseria gonorrhoeaeD. Staphylococcus aureusE. Trichomonas vaginalis
Ans:- C
210) A 1,300 g infant who is born at 34 weeks' gestation has a head circumference of 27 cmand crown-heel length of 40 cm. At 48 hours of age, she is irritable, tremulous, andinconsolable. Her systolic blood pressure is 65 mm Hg and heart rate is 180 beats/min. Herface appears normal, and her cry is high-pitched. Cranial ultrasonography reveals bilateralecho densities suggestive of periventricular leukomalacia. Of the following, the MOSTlikely explanation for the findings in this infant is maternal exposure to
A. alcoholB. barbituratesC. cocaineD. marijuanaE. opiates
Ans:- C211) A 4.3 kg infant is delivered to a woman whose diabetes mellitus is poorly controlled. Of
the following, the MOST likely neonatal manifestation of maternal diabetes isA. diabetic ketoacidosisB. Hirschsprung diseaseC. hypercalcemiaD. polycythemiaE. renal vein thrombosis
Ans:- D212) Of the following, the MOST helpful finding to distinguish GBS pneumonia from RDS is
A. a normal C-reactive protein levelB. an elevated erythrocyte sedimentation rateC. diffuse alveolar infiltrates on chest radiographyD. increased ratio of bands to segmented neutrophils
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 47
E. persistent hypoxemia on blood gas analysis Ans:- D
213) An 18-hour-old infant of a diabetic mother develops abdominal distension. Physicalexamination reveals a protuberant, firm, but nontender abdomen; patent anus; and nogrossly visible anomalies. The infant has passed no meconium stool since birth. A supineabdominal radiograph reveals multiple dilated loops of intestine.Of the following, a contrast enema would MOST likely confirm a diagnosis of
A. atresia of the colonB. Hirschsprung diseaseC. hypoplastic left colon syndromeD. meconium ileusE. midgut volvulus with malrotation
Ans:- C214) You are attending the emergency delivery by cesarean section of a primiparous woman.
The gestation was complicated by pregnancy-induced hypertension. Deep variable fetalheart rate decelerations were noted during labor. At delivery, the infant is acrocyanotic withpoor tone; spontaneous movement and minimal respiratory effort are present. Of thefollowing, your INITIAL management is to
A. ascertain the heart rate and assign a 1-minute Apgar scoreB. begin tactile stimulation and provide blow-by oxygen supplementationC. dry all skin surfaces and clear the oropharynxD. initiate bag-mask ventilationE. insert an umbilical catheter and administer naloxone
Ans:-C215) A vigorous, normal-appearing term male newborn has not voided by 18 hours after
delivery. Perinatal history is negative for maternal illness or medications. Amniotic fluidvolume was reportedly normal, and the delivery was uneventful, with Apgar scores of 6 and9 at 1 and 5 minutes, respectively. Of the following, the MOST likely reason why this 18-hour-old infant has not voided is
A. bilateral ureteropelvic junction obstructionB. intravascular volume depletionC. neurogenic bladderD. posterior urethral valveE. undocumented void in the delivery room
Ans:- E216) A 2-week-old neonate who was born at 32 weeks’ gestation has recovered from
respiratory distress syndrome. He has been tolerating increasing volumes of enteral feedingsvia gavage. Over the past several feedings, abdominal distension, gastric residuals, andstools that are positive for blood have been noted. Of the following, the radiographic findingMOST supportive of the diagnosis of necrotizing enterocolitis is
A. absence of luminal bowel gasB. generalized bowel distensionC. intraperitoneal fluidD. pneumatosis intestinalisE. thickening of the bowel wall
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 48
Ans:- D217) A term infant is placed under a radiant warmer, the skin is dried, and the oropharynx
and nose are suctioned. After tactile stimulation, there is minimal respiratory effort, duskycolor, and a heart rate of 86 beats/min. Bag/mask ventilation is performed for 30 secondswith 100% oxygen at a rate of 40 to 60 breaths/min. The heart rate increases to 100beats/min. Of the following, the NEXT best step is to: A. administer sodium bicarbonate B. continue bag/mask ventilation at a rate of 20 to 40 breaths/min C .continue ventilation and begin chest compressions D. observes for spontaneous respiration and discontinues ventilation E. perform endotracheal intubation
Ans:-D218) A 900 g male infant is delivered vaginally to a woman who had no prenatal care.
Of the following, the physical finding that is MOST consistent with prematurity rather thanintrauterine growth restriction is A. creases over entire sole of foot B. descended testes with deep rugae of the scrotum C. formed and firm pinna with instant recoil D. gelatinous translucent skin E. raised areola and 3 mm breast buds\
Ans:-D
219) A 1-day-old infant develops bilious vomiting and gastric distension. She has been afebrileand has been passing meconium-laden stools. Of the following, the most appropriateINITIAL step in the management of this infant is A. abdominal radiography to look for the “double-bubble” sign B .culture of a catheterized urine specimen C .insertion of a rectal tube for decompression D .placement of a nasogastric tube and initiation of intravenous fluid therapy E. upper gastrointestinal radiographic series to look for malrotation of the small bowel
Ans:- D220) While performing ultrasonography on a 31-week fetus, an obstetrician notes that the
fetal heart rate ranges from 62 to 66 beats/min. Fetal growth appears normal, and nostructural cardiac anomalies are identified. Fetal echocardiography reveals that the fetalatria appear to be contracting at 140 beats/min, with a ventricular rate of 65 beats/min. Ofthe following, the NEXT step in the management of this infant is to:-
A. administer beta-agonist drug therapy to the motherB. assess the cardiac status of the infant following labor and deliveryC. counsel the parents that intrauterine fetal death is likelyD. perform amniocentesis to confirm lung maturity and if mature, perform immediate
cesarean sectionE. repeat the fetal echocardiography and fetal ultrasonography in 1 week
Ans:-E221) The mother of a 2-week-old infant is concerned because her baby has not had a stool in 7 days.
She has been exclusively breastfeeding him every 2 to 3 hours since her milk came in, but the
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 49
baby has only passed flatus. The infant is gaining weight well. Results of physical examinationare normal.Of the following, the best course of INITIAL management for this infantis……………………………………
222) Term infant is cyanotic and requires intubation. Findings include: heart rate, 175beats/min; blood pressure, 60/30 mm Hg; increased right ventricular activity; single S2;short systolic murmur; and equal arm and leg pulses; chest radiography, normal heart sizeand pulmonary congestion. Arterial blood gases (right radial artery on 100% FIO2): pH,7.31; PO2, 43 torr; PCO2, 48 torr. Of the following, the MOST likely diagnosis is:- A. hyaline membrane disease B. hypoplastic left heart C. intrauterine constriction of the ductus arteriosus D. tetralogy of Fallot E. total anomalous pulmonary venous connection Ans:-E
223) A 7-day-old infant has copious purulent discharge from both eyes. The 17-year-oldmother currently complains of a yellowish vaginal discharge. The only medications receivedby the infant were vitamin K and topical erythromycin prophylaxis following delivery.Giemsa stain of a conjunctival scraping reveals intracytoplasmic inclusions. After obtainingappropriate diagnostic studies, the BEST management includes treatment with :- A. oral erythromycin B. oral penicillin C. topical erythromycin D. topical gentamicin E. topical sulfonamide Ans:-A
224) Of the following, the condition that is MOST likely to present with seizures during thefirst 24 hours of life is A .fetal alcohol syndrome B .herpes simplex infection C. hypoxic-ischemic encephalopathy D. organic acidemia E. urea cycle defect Ans:-C225) Maternal serum alpha fetoprotein measured at 12 weeks gestation
A. If normal then neural tube defect are excludedB. Is increased in twin pregnancyC. Is reduced in Turner syndromeD. Is increased in Down syndromeE. AFT is the main blood protein fraction in the first trimester
Ans :- BESerum a fetoprotein is usually measured at 16-18 week gestation, normal screening would notrule out neural tube defect or any other lesion such as twins, Turner's syndrome, Exomphalus,which can all have raised value .
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 50
226) A newborn presents with an early onset of dyspnea with chest retractions, expiratorygrunting and cyanosis following an uneventful normal preterm labor. On examination nocardiac murmurs are heard and the lungs appear clear. On a plain X-Ray there isevidence of prominent pulmonary vascular markings and fluid lines in the fissures. Thecyanosis improves with minimal oxygen. The most probable diagnosis is :-
a) Meconium aspiration syndrome b) Fetal aspiration syndrome c) Transient tachypnea of the newborn d) Persistent fetal circulation e) Hyaline membrane disease Ans:- CEXPLANATIONThe clinical case given above indicates the likely diagnosis of transient tachypnea of the newborn,(Choice C) which is otherwise called Respiratory distress syndrome type II. It is characterized bythe early onset of dyspnea with chest retractions, expiratory grunting and cyanosis. Neonatesusually recover within 3 days.The syndrome is believed to be secondary to slow absorption of fetal lung fluid resulting indecreased pulmonary compliance and tidal volume.The distinctive feature of transient tachypnea of the newborn from hyaline membrane disease(Choice E) are the infant’s sudden recovery and the absence of a radiographic reticulogranularpattern.In meconium aspiration syndrome (Choice A) the chest X-ray is characterized by patchy infiltrate,coarsestreaking of both lung fields and flattening of diaphragm. A normal chest X-ray in an infantwith severe hypoxia and no cardiac malformation suggests the diagnosis of persistent fetalcirculation. ( Choice D).Fetal aspiration syndrome(Choice B) is very common during prolonged labor and difficultdeliveries and mayinitiate vigorous respiratory movements in-utero because of interference with oxygen supply
227) A neonate on the 5th day of life was diagnosed to have developed severe meningitis.Serology of the CSF revealed that the causative organism was Haemophilus influenza.The neonate was started on chloramphenicol. After 36hrs the neonate started vomiting,and became flaccid. The baby was also found to be hypothermic. These symptoms areresult of the neonate having an immature
a) hepatic function b) immune system c) renal tubule system d) hypothalamic regulatory system e) peripheral neurological system Ans: AEXPLANATIONChloramphenicol is the drug of choice in Haemophilus influenza due to its high efficacy againstH.influenza.
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 51
Gray baby syndrome is the name given to chloramphenicol toxicity seen in characteristicallyneonates even at low therapeutic levels. The cause for this is that neonates have an immaturehepatic function and lack an effective glucoronic acid conjugation mechanism for degradation anddetoxification of chloramphenicol. So even at low therapeutic levels the drug accumulates in thebody causing toxicity which is manifested by vomiting, flaccidity, hypothermia, gray color andultimately shock and collapse.
1. Indomethacin give to preterm baby may cause :-A. HypernatremiaB. HyperkalemiaC. PolyuriaD. Hypoglycemia
Ans:- BContraindications to indomethacin include thrombocytopenia (<50,000/mm3),bleeding disorders, oliguria (<1 mL/kg/hr), necrotizing enterocolitis, isolatedintestinal perforation, and an elevated plasma creatinine level (>1.8 mg/dL).
2. Na- Valproate used in early pregnancy may result in fetal:-A. Cardiac anomalyB.C. Platelet dysfunctionD. Neural tube defect
Ans :-D
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 52
3. α fetoprotein increased in :-A. Turner syndromeB. Trisomy 13C. Rh isoimmunizationD. Spontaneous abortion
Ans:- A
4. During management of patient with sever meconium aspiration the following canbe used:-
A. IPPVB. CPAPC. NitroprussideD. Dexamethasone
Ans:-A
5. Hypoxic-ischemic encephalopathy all are correct except:-A. Result from excessive use of oxytocinB. IUGR is be first indication of fetal hypoxiaC. Associated with increased beat to beat variabilityD. Prognosis depend on gestational ageE. Persistent of abnormal neurological sign at two week indicate poor prognosis
Ans:- C6. Apgar score include the following except :-
A. Muscle toneB. Response to catheter in nostrilsC. Heart rateD. Respiratory rate
Ans:- D7. Intracranial hemorrhage :
A. Primary hemorrhage disorder give rise to intraventricular hemorrhageB. intraventricular hemorrhage is symptomatic immediately after birthC. neurosurgical intervention is indicated early in the ?course of the conditionD. benefit of reducing intracranial pressure have not been established
Ans:8. HMD:-
A. Pathological finding are rarely seen in infant dying early than 8 hour after birthB. In sever cases grunting is absentC. Death is rare in the 1st day of illnessD. X- ray finding are pathognomic
Ans:- AB C
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 53
Death is rare on the 1st day of illness, usually occurs between days 2 and 7, and is associated withalveolar air leaks (interstitial emphysema, pneumothorax), pulmonary hemorrhage, or IVH, On x-ray, the lungs may have a characteristic, but not pathognomonic appearance that includes a finereticular granularity of the parenchyma and air bronchograms, which are often more prominentearly in the left lower lobe because of superimposition of the cardiac shadow
9. About HMD all correct except :-A. Occur in 60% of infant (28 week of age)B. Increased frequency is associated with previous history of affected infantC. High oxygen lead to decreased surfactantD. Atelectasis lead to ventilated but not perfused alveoliE. HMD is accompanied by Rt → Lt shunt
Ans:- D10.All of the following are true except:-
A. TTN isn't seen in normal delivered infantB. Patient with TTN may have pleural effusionC. Meconium stained amniotic fluid is seen in 10% of live birthD. Meconium aspiration syndrome may lead to metabolic acidosisE. Patient with meconium aspiration may get beneficial from ECMO
Ans:- A11.natural thermal environment for 1-2 kg at 12 hour of age is :-
A. 37B. 36C. 34D. 38E. 32
Ans:- C12.To increase the Hb of newborn by 1gm/dl the amount of packed cell required will
be :-A. 2 cc/kgB. 4 cc/kgC. 5 cc/kgD. 9 cc/kgE. 15 cc/kg
Ans:- A13.About birth injury all are correct except
A. C1-C2 level is the commonest site of injuryB. In spinal injury , the patient may die before appearance of neurological signC. Erb's palsy infant loss power to abductionD. Erb's palsy infant, Bicep's reflex is absentE. Erb's palsy infant, preserve of hand grasp is favorable prognosis
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 54
Ans: A14.The following associated with polyhydramniose except;-
A. Indomethacin administrationB. Diaphragmatic herniaC. AchondroplasiaD. Adenomatoid cystic lungE. Trisomy 18
Ans:- A
15.Birth injury:-A. Paralysis of the upper arm has better prognosis than paralysis of the lowerB. In nerve injury, neuroplasty is advised at the end of first year of lifeC. In phrenic nerve paralysis, spontaneous recovery is expectedD. Facial nerve paralysis will result from the muscular agenesis of the facial nerve
Ans:-A C
16.All statement are true except:-A. IVH is uncommon in infant > 34 week gestationB. The incidence of VSD is high in VLBW infant ( PT > PDA)C. Hypoglycemia seen more commonly in patient with SGAD. Hypercarbia is risk factor for …..E. Decrease vitamin E may cause hemolytic anaemia
Ans:-
17.Breast milk composition all true except:-A. Protein 2gm/dlB. Carbohydrate 7 gm /dlC. Ca/Po4 33/15 mg/dlD. Fat 4 gm/dlE. Osmolality 290-300 mosm
Ans:-A
18.All statement are true except:-A. Prematurity is predisposing factor for birth asphyxiaB. Cephalohematoma is accompanied with discoloration of the scalpC. Sensation of central depression suggesting fracture accompanied
cephalohematomaD. Occipital bone fracture is fatalE. Subconjunctival hemorrhage is due to increase intrathoracic pressure
Ans:- B
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 55
19.Sign of ICH include all of the following except:-A. Enlarged headB. Fixed dilated pupilC. Neck stiffnessD. Persistent cyanosisE. Sweating
Ans:- E
20.Exchange transfusion in preterm baby may be complicated by:-A. HemoglobinuriaB. HemoglobinemiaC. ThrombocytopeniaD. IVH ??E. GVHD
Ans:-
21.For treatment of hyperbilirubinemia all are true except:-A. Phototherpy ( 250-320 nm) ??B. Intravenouse immunoglobulineC. Metalloporphyrins (Tin (Sn)-protoporphyrin ).D. Activated charcoal
Ans:- AClinical jaundice and indirect hyperbilirubinemia are reduced on exposure to a high intensity oflight in the visible spectrum. Bilirubin absorbs light maximally in the blue range (420–470 nm).
22.Necrotizing enterocloitis :-A. USS detect microbabbules of gas in the GIT wall is used recentlyB. Vitamine E is used in the treatment of NECC. Maternal intake of cocaine may predispose to NECD. Breast milk protect against NEC Ans:- CD
23.All of the following are correct except:-A. Generalized oedema occur with Hurler syndromeB. Cyanosis can be mask with paleC. Postmature tend to have pale skin than termD. Periodic respiration is common in the first 24 hourE. Wormian bone associated with cliedo dystosis
Ans:-D
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 56
24.The following fact give false positive ( low) Apgar score except:-A. Mg sulfateB. Congenital myopathyC. High fetal calcitonine levelD. ImmaturityE. Airway obstructed
Ans:-C
25.IDM:-A. Increased insulin level in infant born to mother with gestational diabetusB. Decrease level of FFAC. Decrease Epinephrine & Glucagons responseD. Cortisol & human growth hormone are normal Ans:- A BC D
26. Regarding thyroid problem during neonatal period all are false except:_A. Maternal thyrotoxicosis during pregnancy can be treated safely with propranolol
& thiouracilB. Mother should be kept mildly hypothyroidismC. Breast milk may mask neonatal hypothyroidismD. If the mother on thyroxine should stop breast feedingE. Carbimazole can be used safely in nursing mother
Ans:-E
27. Regarding Tetracyclin all are true except:-A. It is selectively concentrated in the teeth by chelating calciumB. It effect decidual teethC. It effect permanent teethD. Has no effect on eye ( CAUSE CATARACT)E. It depress skeletal growth
Ans:-D
28.Maternal vaccination during pregnancy can be given safely except:-A. BCGB. HBVC. Cholera vaccineD. TetanusE. Meningococcal vaccine
Ans:- A
ABDULRAHMAN BASHIRCHILDREN HOSPITAL –BENGHAZI 57
29.Hepatitis B infection all false except:-A. Increase incidence of malformed & stillbirthB. Increase the risk of prematurityC. Hepatitis B immunization & vaccine should be given in 1st weekD. 25% babies born to mother with HBsAg positive are HBsAg negativeE. Presence of HBeAg has no role in increase transplacentalcross infection Ans:-B
QUESTION NUMBER 1120







