
Hypertension in Pregnancy
Education Consultants SSM Healthcare – 2014

Objectives
1. Describe the classification of hypertensive disorders of pregnancy.
2. Describe the pathophysiology of preeclampsia. 3. Discuss patient assessment for preeclampsia. 4. Summarize the management of mild and
severe preeclampsia. 5. Describe the use of magnesium sulfate for
seizure prophylaxis. 6. Review the management of eclamptic seizures.

Hypertensive Disorders of Pregnancy . . .
Complicate 10% of all pregnancies Accounted for 15.7% of maternal mortality in the U.S. from 1991-1999

Current Terminology and Classification of Hypertension in Pregnancy
National High Blood Pressure Education Program Working Group on High Blood Pressure in Pregnancy (2000)
ACOG Practice Bulletin Number 33: Diagnosis and Management of Preeclampsia and Eclampsia (2002)
Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (2004)
ACOG Task Force on Hypertension in Pregnancy (2013) Hypertension in Pregnancy

Hypertension is Defined as . . .
Systolic blood pressure ≥ 140 mmHg or Diastolic blood pressure ≥ 90 mmHg Based on at least two measurements taken
4-6 hour apart (or 2 separate visits) Accurate and consistent BP assessment is
important

Classification of Blood Pressure for Adults Normal – SBP <120 and DBP <80 Prehypertension – 120–139 or 80–89 Hypertension Stage 1 – 140–159 or 90–99 Hypertension Stage 2 – >160 or >100
Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (2004)

Classification of Hypertensive Disorders in Pregnancy Gestational hypertension Preeclampsia-Eclampsia Chronic hypertension Chronic hypertension with superimposed
preeclampsia

Gestational Hypertension
New onset blood pressure elevation after 20 weeks of gestation in the absence of proteinuria or other systemic findings indicative of preeclampsia
Incidence Nulliparous women 6%-18% Multiparous women 6%-8% Markedly increased in twin gestations Higher rates of induction of labor and cesarean
birth

Preeclampsia/Eclampsia
Preeclampsia is a pregnancy specific hypertensive disease with multisystem involvement
Usually occurs after 20 weeks gestation Incidence
Nulliparous women 3%-7% Multiparous women 0.8%-5% Markedly increased in twin gestations
Eclampsia is the convulsive phase of the disorder

Preeclampsia/Eclampsia
Risk Factors for Preeclampsia
Primiparity Previous preeclamptic pregnancy Chronic HTN or chronic renal disease or both History of thrombophilia Mutifetal pregnancy In vitro fertilization Family history of preeclampsia Type I or Type II diabetes mellitus Obesity Systemic lupus erythematosus Advanced maternal age (older than 40 years)

Chronic Hypertension
Hypertension that predates pregnancy Or, is detected before 20 weeks of gestation

Chronic Hypertension with Superimposed Preeclampsia Chronic hypertension in association with
preeclampsia Prognosis much worse than for either condition
alone
Maternal Mortality Rate from Preeclampsia or Eclampsia
1.8 per 100,000 The incidence of preeclampsia has increased by 25%
in the U.S. in the past two decades Hypertension is directly responsible for 17.6% of
maternal deaths in the U.S. (ACOG, 2002) Large racial disparity, African-American women are
more likely to die of preeclampsia than are women of all other races
Outcome is usually dependent on gestational age at the onset and the severity of the disease process

Maternal Complications
Placental abruption Thrombocytopenia Disseminated intravascular coagulation (DIC) Cerebral hemorrhage Hepatic failure Subcapsular hematoma of the liver → rupture Acute renal failure Pulmonary edema ARDS Cesarean birth
Fetal/Neonatal Complications
Placental insufficiency Intrauterine growth restriction Hypoxia Intrauterine fetal demise
Acute insult with placental abruption Acute insult with maternal seizure Preterm birth Oligohydramnios

Normal Physiology of Pregnancy
50% increase in blood volume 35-50% increase in cardiac output Increased uterine blood flow
From 50 mL to 600 mL per minute

Uncomplicated Pregnancies Become a Markedly Vasodilated State Peripheral resistance decreases by 25%
Vessels develop resistance to the pressor effects of angiotensin II
Increased prostaglandin synthesis with an increase in the potent vasodilator prostacyclin
Increased nitric oxide synthase Increased production of the endothelium-derived
relaxing factor

Changes Also Occur in the Renal System Renal blood flow and
glomerular filtration rate increase, activating the renin-aldosterone system and resulting in a falling BP

Resulting in …
BP decreasing in the first 2 trimesters BP usually falling 10 mm Hg by mid-pregnancy,
then slowly approaching pre-pregnancy levels in the 3rd trimester

Etiology of Preeclampsia
Preeclampsia is a multisystemic disease that affects all organ systems and is far more than high blood pressure and renal dysfunction.
Despite considerable research, the etiology of
preeclampsia remains unclear.

The Prevailing Theory
The placenta is evident as the root cause of preeclampsia.
It is proposed that an immunologically initiated reduction in trophoblast invasion leads to failed vascular remodeling of the maternal spiral arteries that perfuse the placenta.
Altered placental function (placental hypoxia and ischemia) leads to the maternal disease.

Pathophysiology of Preeclampsia Occurs in Two Stages
1. Alterations in Placental Perfusion 2. Maternal Syndrome

The Link Between the Two Stages Includes a cascade of secondary effector
mechanisms including: Altered proangiogenic and antiangiogenic
factor balance Increase maternal oxidative stress Endothelial dysfunction Immunologic dysfunction
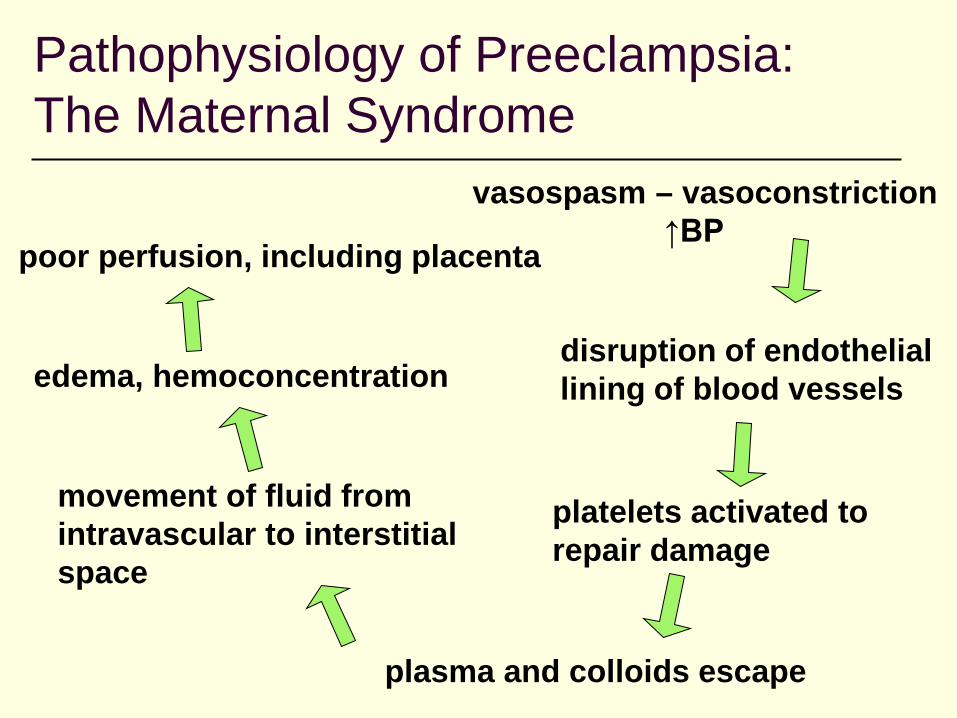
Pathophysiology of Preeclampsia: The Maternal Syndrome
vasospasm – vasoconstriction ↑BP
disruption of endothelial lining of blood vessels
plasma and colloids escape
platelets activated to repair damage
movement of fluid from intravascular to interstitial space
edema, hemoconcentration
poor perfusion, including placenta

Effects of Vasospasm and Vasoconstriction
normal RBCs & platelets
platelets agglutinate, fibrin forms
Hemolysis – damage or destruction of RBCs – schistocytes & burr cells

Vessel Damage
leakage of plasma & colloids into interstitial space

Renal Involvement
Glomerular endothelial damage & fibrin deposition leads to ischemia
↓ Renal blood flow and ↓ glomerular filtration rate Proteinuria ↓ Uric acid clearance, ↑ serum uric acid
↓ Creatinine clearance, ↑ serum creatinine
Oliguria Acute renal failure

Liver Involvement
Hepatic dysfunction is part of HELLP syndrome Late hepatic changes are consistent with hepatic
infarction and hepatocellular necrosis Signs of liver failure: malaise, nausea, epigastric
pain, hypoglycemia, hemolysis, anemia Hepatic changes can lead
to subcapsular hematoma which can result in liver rupture

CNS Involvement
Vasoconstriction results in widespread microvascular cerebral changes and ischemia
Cerebral edema Hyperreflexia Headache Nausea & vomiting CVA May induce seizures –
the eclamptic phase

Other Organ System Involvement
Pulmonary Pulmonary edema – endothelial injury leading to fluid
leakage and potential volume overload Ophthalmic Involvement
Retinal arteriolar spasms – scotoma, photophobia, blurring, or double vision
Coagulation Involvement Coagulation Involvement Endothelial damage consumes
platelets

Symptoms of Preeclampsia
Swelling of the face or hands Headache that will not go away Visual disturbances Pain in upper right quadrant Nausea or vomiting Sudden weight gain Difficulty breathing

Severe Preeclampsia

Management of Preeclampsia
Delivery is the only cure Deliver when most optimal for mother and fetus Little data to suggest any therapy alters the
underlying pathophysiology Interventions designed to safeguard mother
while allowing time for fetal maturity

Management of Preeclampsia
Careful monitoring Hospitalization frequently advised Ongoing assessment: symptoms, VS, DTRs,
fetal well-being (NST, BPP, Growth evaluation) Control of BP
Antihypertensive therapy warranted for BP ≥160/110 or rapidly rising
In pregnant adolescent, may use at DBP 100 Prevention of eclamptic seizures Timely delivery

Management of Mild Gestational HTN or Preeclampsia

Management of Severe Preeclampsia at <34 Weeks


Systematic Nursing Assessment is Essential Cardiovascular CNS Renal GI/Hepatic Fetal well-being Psychosocial

Hospital Safety Measures Low lighting Quiet environment (limit phone, TV, visitors) Airway, O2, suction at bedside Emergency medications available

In the Event of Eclampsia … Prevent maternal injury Lateral positioning Maintain airway – do not insert a tongue blade Suction Oxygen Give adequate magnesium sulfate Fetal assessment and labor assessment Seizure and blood pressure control first then
plan for delivery

HELLP Syndrome
A laboratory, not a clinical diagnosis Appears in 2%-12% of preeclamptic women Hemolysis
Peripheral smear with burr cells Elevated bilirubin level
Elevated Liver Enzymes Elevated AST and ALT
Low Platelets >100,000/mm3

HELLP Syndrome
More common in older, Caucasian, multiparous women
About 90% of women report a history of malaise for several days
About 65% of women have epigastric or right upper quadrant abdominal pain
About 50% of women develop nausea and vomiting

Fetal Assessment
Fetal activity, kick counts FHR pattern, continuous monitoring FHR variability Review NST and BPP Review growth curves per
ultrasound. IUGR often precedes preeclampsia.
Notify nursery & pediatrician Potential for neonatal
hypermagnesemia

Medications
Magnesium sulfate Antihypertensives – avoid ↓ BP < 140/90 Steroids for fetal lung maturity or for HELLP
syndrome Diuretics – only in pulmonary edema Avoid sedatives and valium

Magnesium Sulfate
Elevated magnesium levels depress the CNS Also acts as a cerebral vasodilator to counteract
the cerebral hypoxia and increases blood flow to the brain
Affects the neuromuscular and neurocellular signal transmission, which inhibits seizure activity
Also decreases levels of the neurotransmitter, acetylcholine

Magnesium Sulfate
4-6 g loading dose IV over 15-30 minutes 1-3 g continuous IV Always give IVPB with a pump Monitor for side effects and toxicity Cautious use of narcotics or CNS depressants Antidote: Calcium gluconate
Available at bedside 10 ml of 10% solution (equal to 1 g) slow IV
push over 3-10 minutes

Magnesium Sulfate on the FBP Bolus of 2 grams in 50 mL Bolus of 4 grams in 100 mL Bolus of 6 grams in 150 mL For any bolus . . . Set the rate at 300 mL/hr
(this equates to 1 gm/5 minutes) 2 grams in 50 mL will infuse in 10 minutes 4 grams in 100 mL will infuse in 20 minutes 6 grams in 150 mL will infuse in 30 minutes
Nurse remains at the bedside . . . VS every 15 minutes with oxygen saturation
monitoring

Magnesium Sulfate on the FBP
Maintenance 20 grams in 500 mL 1 gram/hr 25 mL/hr 2 grams /hr 50 mL/hr 3 grams/hr 75 mL/hr
Reminder card for your ID badge . . .

Side Effects
Flushing Sweating Lower maternal temperature Nausea and Vomiting Headache Blurred vision Shortness of breath, chest pain, &
pulmonary edema

Side Effects/Signs of Toxicity
Respiratory depression (respirations < 12/min) Shortness of breath, chest pain, abnormal
breath sounds, cough pulmonary edema Hypotension Bradyarrhythmias Muscle weakness Diminished/absent DTRs CNS depression – somnolence, marked
lethargy

Magnesium Sulfate
Nursing Care Monitor for toxicity Assess VS (respiratory rate), DTRs, and urine
output before and during administration Continuous fetal assessment
Institute for Safe Medication Practices – List of High-Alert Medications
High-alert medications are drugs that bear a heightened risk of causing significant patient harm when they are used in error.

Magnesium Sulfate
Half-life with normal renal function = 4 hours 90% excreted in 24 hours Signs of moderate toxicity include respiratory
depression and arrhythmia If respiratory alterations occur, turn off before
notifying physician Possible alternative – Phenytoin (Dilantin)

Magnesium Toxicity
Normal 1.7-2.1 mg/dl Therapeutic range 4.8 – 9.6 (5-8) Loss of DTRs 8-12 Feelings of warmth, flushing 9-12 Somnolence 10-12 Slurred speech 10-12 Muscular paralysis 15-17 Respiratory difficulty 15-17 Cardiac arrest 20-35
Sibai, B.M. (2002).

Deep Tendon Reflexes
Imperative nursing function with Magnesium Sulfate administration
Determine need for magnesium therapy Evaluate efficacy of magnesium therapy Prevent toxicity from magnesium therapy
DTRs function as a window into the CNS.

Tips on Taps (Checking DTRs) Assess biceps and patellar reflexes and ankle clonus Ensure relaxation of the limb Feel the tendon (if you can’t feel it, don’t tap) Tap lightly Reinforce the reflex, rather than tapping harder Assess upper and lower extremities in the same session Interpret the results 0 to 4 Assigning plus or minus notations creates problems

Biceps DTR
Elbow at a 90° angle Arm slightly bent
down Grasp the elbow Press thumb against
the biceps brachii tendon
Strike your thumb – vary your thumb pressure with each blow

Patellar Reflex
Put your hand under the knee (thigh) and lift it from the bed. Tap the patellar tendon directly.

Responding to DTRs
Hyperreflexia (3 or 4) A sign the disease has affected the cortex, the
pt needs magnesium started or increased Normoreflexia (2)
Proper dosing achieved Hyporeflexia or areflexia (1 or 0)
Decrease or discontinue infusion, with physician order
If respiratory depression, turn off infusion even before calling physician
Nursing Actions to Promote Safety
All loading doses, dosage changes and new infusion bags started must have pump settings checked by two registered nurses – document in EPIC
Purple tape is placed around each bag, on the tubing by the attachment to the pump, and on the tubing by the attachment to the mainline
When the magnesium infusion is discontinued the bag should be disconnected from the mainline

Antihypertensives in Preeclampsia
Hydralazine (Apresoline) - Vasodilator Labetalol hydrochloride – Beta-blocker Methyldopa (Aldomet) – Maintenance therapy Nifedipine (Procardia) – Calcium-channel
blocker – relaxes arterial smooth muscle – use with caution if patient is also getting magnesium sulfate due to possible potentiation of CNS effects

For Urgent BP Control in Pregnancy

Common Oral Antihypertensive Agents in Pregnancy

Labetalol hydrochloride Hypertension: initial, 100 mg ORALLY twice daily Maintenance, 200-400 mg ORALLY twice daily Hypertension: IV to ORAL conversion, initial, 200 mg
ORALLY, followed in 6-12 hr by 200-400 mg ORALLY depending on BP response
Hypertension (Severe): Repeated IV injection: Initial dose of 20 mg (0.25 mg/kg) by slow injection over 2 minutes; repeat injections of 40 or 80 mg at 10 minute intervals as indicated; MAXIMUM dose is 300 mg; maximum effects occur within 5 minutes of injection
Hypertension (Severe): May be used as a continuous infusion of 1mg/kg per hour as needed.
Watch for a delayed effect of sudden maternal hypotension. Use with caution in women with asthma.

Hydralazine (Apresoline)
Essential hypertension – emergency therapy: 20 to 40 mg/dose IM/IV bolus as needed
Pregnancy: 5 mg IV over 1-2 minutes, may give another 5-10 mg after 20 minutes
Maximal effect in 20 minutes Recheck BP every 5 minutes

Nifedipine (Procardia)
Calcium channel blocker Uses: Hypertension and angina, off label for
preterm labor Dosage: Extended release 30 mg – 60 mg
daily Acute hypertension: Short acting 10 mg PO,
repeat every 20-30 minutes to a maximum of 30 mg
Warnings/Precautions: Can cause hypotension and fluid retention

Other Issues
Fluid management – 100-125 mL per hour (?) Analgesia and anesthesia Method of delivery and timing of delivery Potential transfer issues Prolonged bedrest Psychosocial and emotional support Postpartum management

Postpartum Management
Continue intense assessment and interventions for 24-48 hours Seizure activity and pulmonary edema are
common In HELLP, increasing platelets indicate
improvement more than BP or output Increased potential for uterine atony,
hemorrhage, and volume depletion Remember, NSAIDS can contribute to
elevated BP

Postpartum Hypertension
Preeclampsia can first develop in the postpartum period
Thus mandating instruction at discharge regarding symptoms that should be reported

Final Reminder – Goals of Therapy
1.Ensure maternal safety
2.Deliver a healthy newborn
Nurses do make a difference!

References ACOG. (2013). Hypertension in pregnancy. Gilbert, E., & Harmon, J. (2003). High risk
pregnancy and delivery (3rd ed.). St. Louis: Mosby. Lowdermilk, D.L., & Perry, S.E. (2004). Maternity
and Women’s Health Care (8th ed.). St. Louis, Missouri: Mosby.
Sibai, B.M. (2007). Hypertension. In S.G. Gabbe, J.R. Niebyl, & J.L. Simpson (Eds.), Obstetrics: Normal and problem pregnancies (5th ed, pp. 863-912). New York: Churchill Livingstone.
Simpson, K.R., & Creehan, P.A. (Eds.). (2014). AWHONNs, perinatal nursing (4th ed.). Philadelphia: Lippincott.







