A Regulatory Perspective of End Points to Measure Safety and Efficacy of Drugs
Hormone Refractory Prostate CancerHormone Refractory Prostate Cancer
Bhupinder S. Mann, MBBSMedical OfficerDODP CDER FDA
Objectives
End points utilized for granting approval
Comments on difficulties encountered in measuring safety and efficacy of drugs for treatment of advanced HRPC
Approval of a New Drug
Substantial evidence of effectiveness
Adequate and well-controlled clinical investigations
End Points (Before 1992)
Required to represent clinical benefit
Direct measures of benefit, e.g. Improvement in survival Improvement of symptoms
Accepted surrogates for benefit, e.g. Durable complete responses in acute
leukemia
Accelerated Approval (1992) Surrogate endpoints that are
reasonably likely to predict clinical benefit
The drug
A benefit over available therapy
Post-approval studies Demonstrate that the drug does provide
clinical benefit
End pointsAccepted for drug approval Approved drugs for treatment of
advanced HRPC
Docetaxel (2004) Zoledronic acid (2003) Mitoxantrone (1996)
Estramustine (1981)
Overall Survival (OS)Safety and efficacy
Overall Survival
A direct measure of efficacy
A reassuring measure of safety
Docetaxel May 2004
Docetaxel in combination with prednisone is indicated for the treatment of patients with androgen independent (hormone refractory) metastatic prostate cancer
Demonstration of efficacy Well controlled clinical trial Significant prolongation in OS
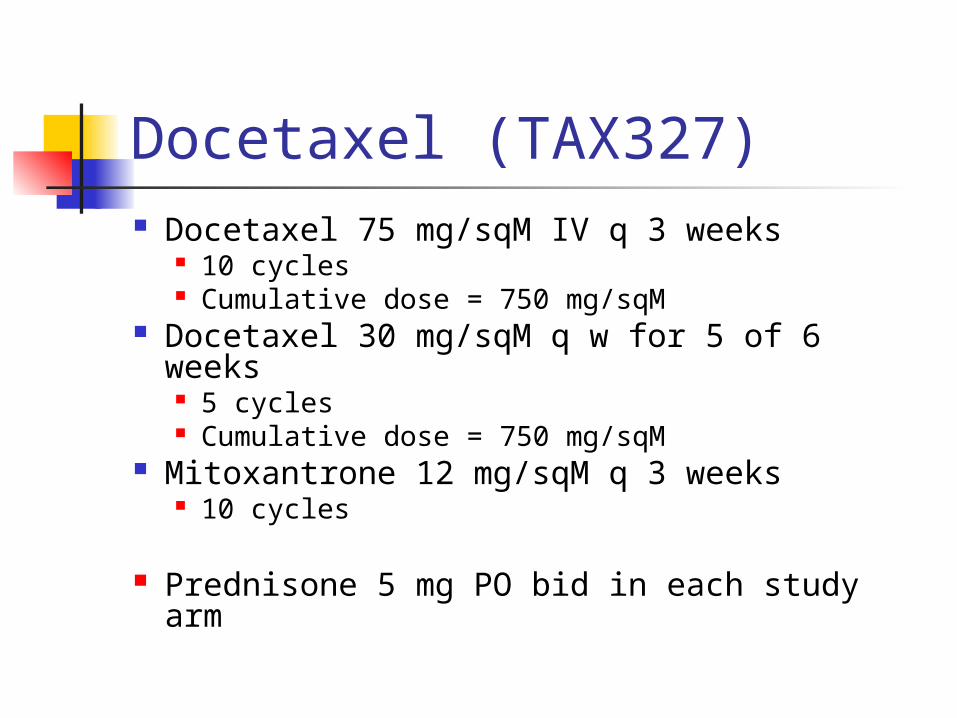
Docetaxel (TAX327) Docetaxel 75 mg/sqM IV q 3 weeks
10 cycles Cumulative dose = 750 mg/sqM
Docetaxel 30 mg/sqM q w for 5 of 6 weeks 5 cycles Cumulative dose = 750 mg/sqM
Mitoxantrone 12 mg/sqM q 3 weeks 10 cycles
Prednisone 5 mg PO bid in each study arm
Docetaxel (TAX327)
Patients=1,006
Primary efficacy end point Overall Survival Time from randomization to death
from any cause
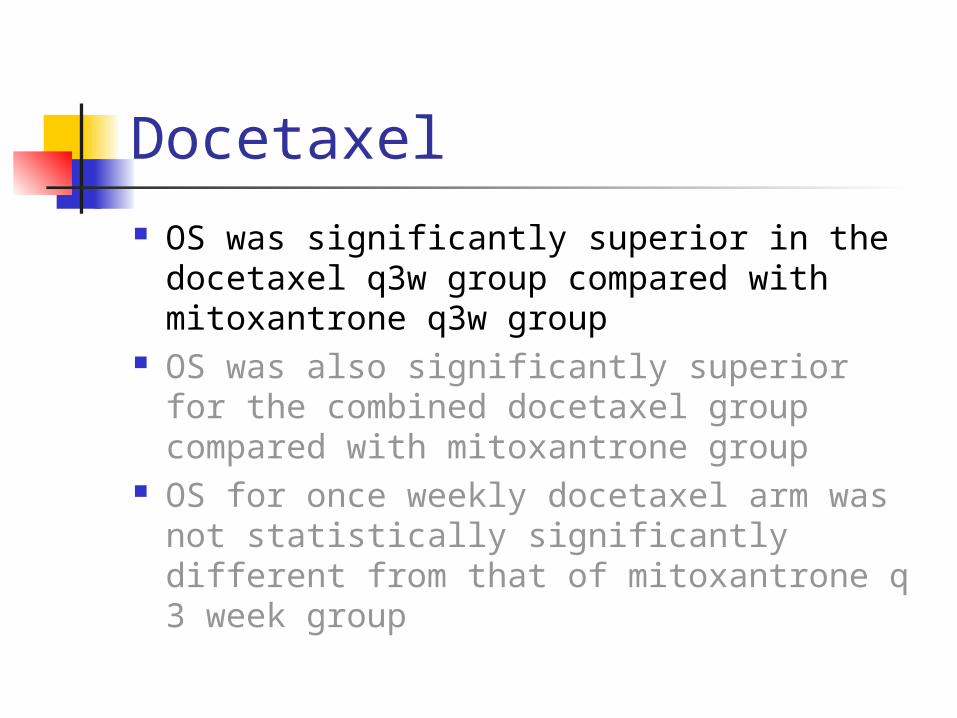
Docetaxel OS was significantly superior in the
docetaxel q3w group compared with mitoxantrone q3w group
OS was also significantly superior for the combined docetaxel group compared with mitoxantrone group
OS for once weekly docetaxel arm was not statistically significantly different from that of mitoxantrone q 3 week group
Docetaxel
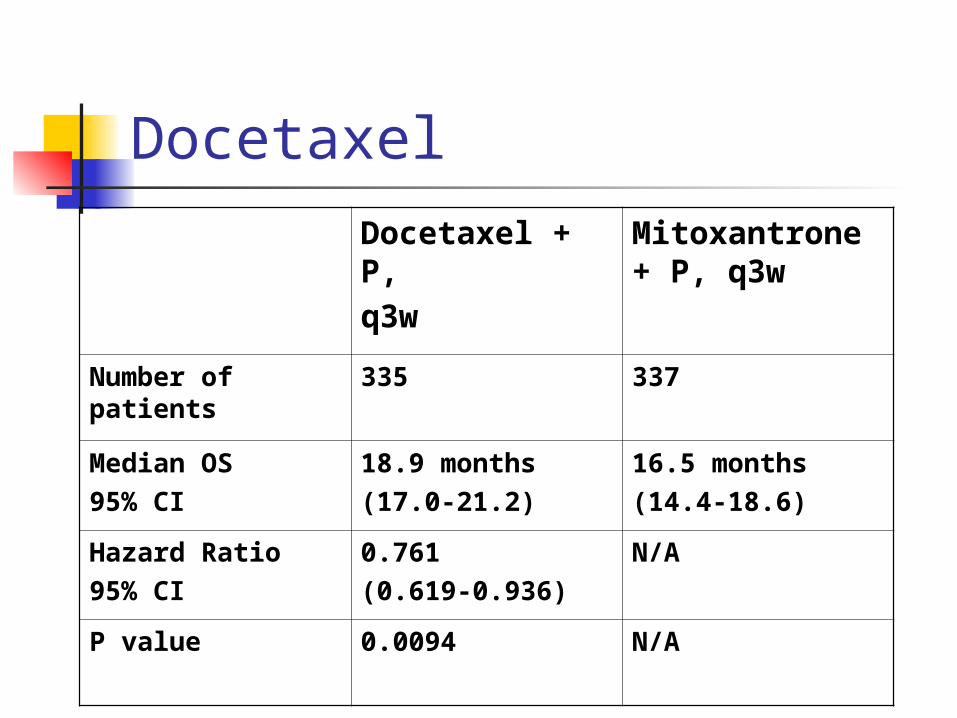
Docetaxel + P,q3w
Mitoxantrone + P, q3w
Number of patients
335 337
Median OS 95% CI
18.9 months(17.0-21.2)
16.5 months(14.4-18.6)
Hazard Ratio95% CI
0.761(0.619-0.936)
N/A
P value 0.0094 N/A
Demonstration of efficacyImprovement in symptoms and other
indices FDA accepted end points
Symptom measures Non-survival morbidity indices
Approvals based on non-survival end points Mitoxantrone Zoledronic acid
Mitoxantrone
November 1996
For use in combination with corticosteroids as initial chemotherapy for treatment of patients with pain related to advanced hormone refractory prostate cancer
Mitoxantrone Pivotal trial- open label, Phase III
161 symptomatic patients
End point- Palliative Response Prospectively defined A 2-point improvement on a 6-point pain
intensity scale Accompanied by a stable analgesic score Duration- at least 6 weeks
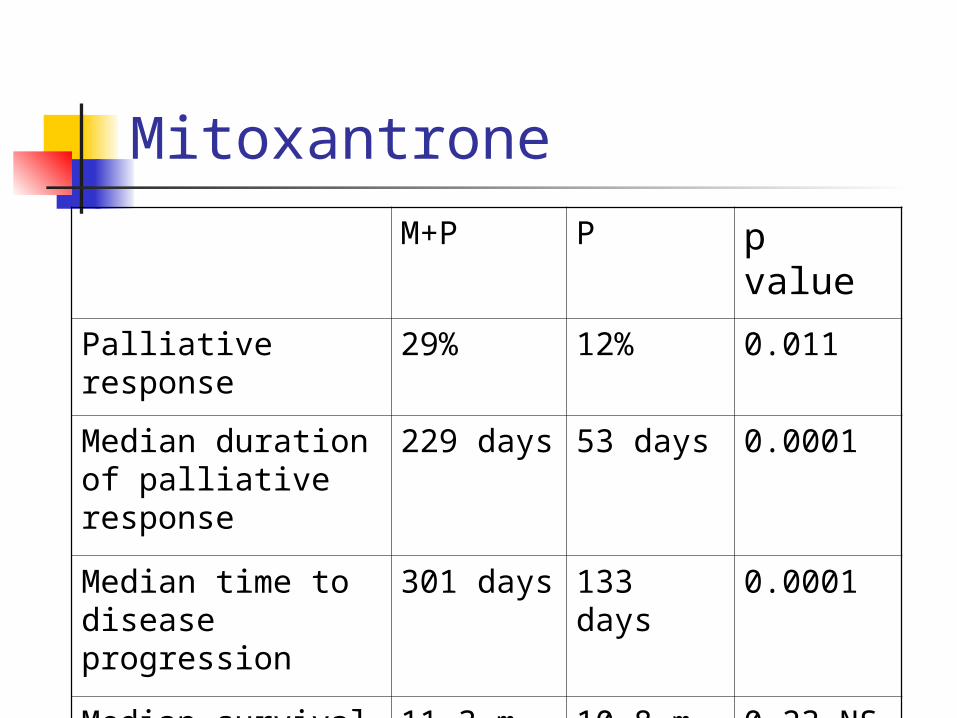
Mitoxantrone
M+P P p valuePalliative response
29% 12% 0.011
Median duration of palliative response
229 days 53 days 0.0001
Median time to disease progression
301 days 133 days 0.0001
Median survival time
11.3 m 10.8 m 0.23 NS
Decrease of ≥ 75% in PSA
27% 5% 0.011
Zoledronic acid
2003
Treatment of patients with progressive bone metastases from prostate cancer
Zoledronic acid
End point used- Composite end point based on
skeletal related events (SREs) Diverse disease manifestations Increased power
Previously used in lytic bone disease in multiple myeloma and breast cancer
Zoledronic acid SRE included in the composite end point
Pathological bone fractures Spinal cord compression Surgery to bone Radiation therapy to bone (including
Radioactive Isotopes)
A change in antineoplastic therapy due to increased pain
Added for prostate cancer trial
Demonstration of efficacySRE end point A decrease in the proportion of patients
with at least one SRE 33% vs. 44% Difference 11%, p 0.021
An increase in the median time to first SRE NR vs. 321 days HR 0.67, p 0.011
Evaluating Treatments for Advanced Prostate Cancer
Difficulties stem from several factors
Disease characteristics Patient population Prevalent clinical practice
Advanced HRPCDisease of heterogeneous natural history
Variable clinical course Diverse clinical manifestations Difficult treatment decisions
Traditional efficacy end points Limited utility
HRPCPSA only progression
Disease symptom None
Bone scan Negative
Survival Relatively long
HRPCSymptomatic progressive disease
Disease related symptoms Worsening of performance status Impaired quality of life
Survival Shortened
Clinical benefit of treatment Established
Patient Population
Competing causes of mortality
Advanced patient age Comorbid conditions
End points Problems confounding interpretation
PSA driven treatment changes
Missing clinical data
End points Problems confounding interpretation
PSA based end points may be acceptable surrogates for anti-tumor activity, eg in Phase II clinical trials
Reliable use of PSA based end points in Phase III comparative clinical trials remains to be defined
Acknowledgements
Ramzi Dagher, MDDonna Griebel, MDJohn Johnson, MD
Richard Pazdur, MDDianne D SpillmanGrant Williams, MD







