
Injury, Int. J. Care Injured 32 (2001) 71–73
Case report
Fracture of the clavicle associated with a rotatory atlantoaxialsubluxation
R. Nannapaneni a, F.P. Nath a, S.L. Papastefanou b,*a Department of Neurosurgery, Middlesbrough General Hospital, Ayresome Green Lane, Middlesbrough, Cle6eland TS5 5AZ, UK
b Department of Orthopedic Surgery, Middlesbrough General Hospital, Ayresome Green Lane, Middlesbrough, Cle6eland TS5 5AZ, UK
Accepted 23 May 2000
www.elsevier.com/locate/injury
Muscle spasm following a clavicular fracture in chil-dren is not uncommon. However, this may mask anassociated atlanto-axial rotatory subluxation (AARS).Awareness of this possible association allows for earlydiagnosis and effective conservative management.
1. Presentation of cases
1.1. Case 1
A 6-year-old girl tripped over a football and landedon her right shoulder. Clinical examination revealed afracture of the right clavicle with torticollis. An X-rayof the right shoulder confirmed the angulated midshaftfracture of the clavicle. The patient was discharged withanalgesics and a broad arm sling.
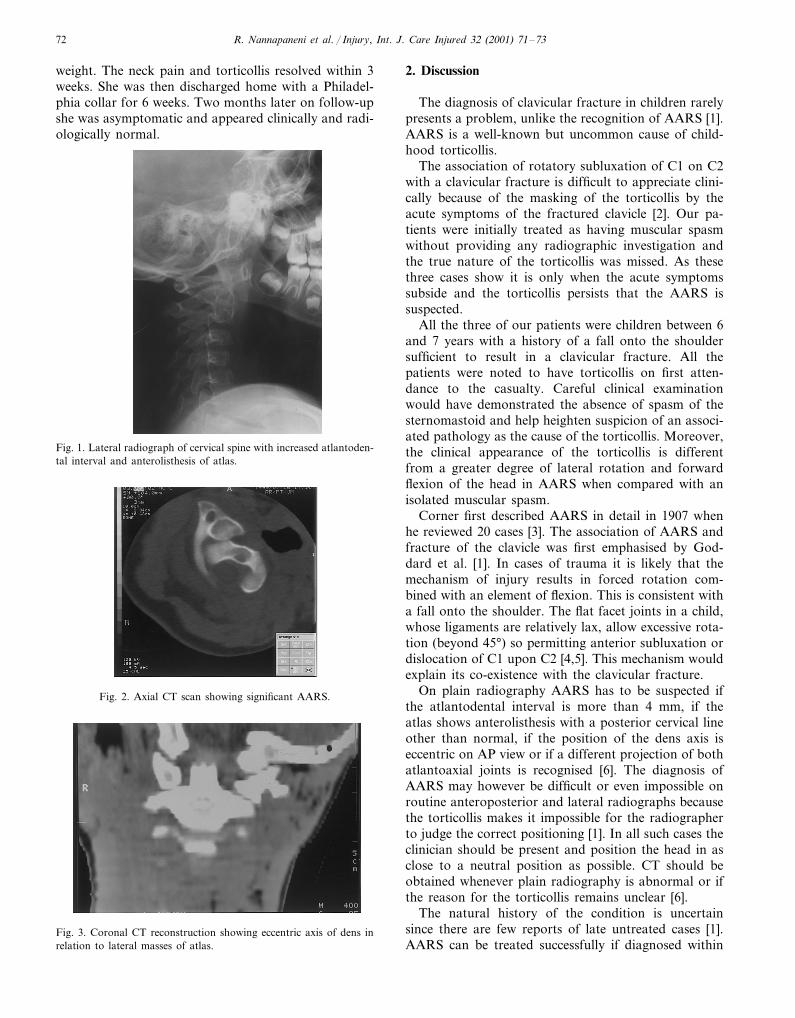
She returned to the casualty department the next daywith headache and vomiting. She was sent home onanalgesics. Following a further re-attendance the nextday she was noted to have a ‘Cock–Robin position’.Although the motion of the cervical spine was severelyrestricted in all directions with marked nuchal musclespasm, the results of the neurological examination werenormal. X-rays of the cervical spine then showedAARS (Fig. 1), which was confirmed, on computedtomography (CT) scan (Figs. 2 and 3).
She was treated conservatively with continuous haltertraction using 4-lb weight. The neck pain and torticollisresolved within 4 days. She was discharged home witha Philadelphia collar for 6 weeks. On follow-up 3months later the patient was free from pain and torti-collis and had resumed normal activity.
1.2. Case 2
A 7-year-old boy fell from a push-bike with thehandle hitting his shoulder, sustaining a fracture of theright clavicle. He was noted to have a torticollis withthe head turned to the left. X-ray of the right shoulderconfirmed the fracture of the clavicle. The torticolliswas considered to be the result of a protective mecha-nism involving spasm of the sternomastoid. He wasdischarged on analgesics and a collar-and-cuff sling.
Four days later he re-attended the casualty depart-ment with persistent torticollis. Examination revealedtenderness over the upper cervical spine. Cervical spineX-rays showed AARS, which was confirmed on CTscan. He was managed conservatively with halter trac-tion and analgesia. The subluxation reduced over 7days and he was discharged home in a Philadelphiacollar for 6 weeks. On follow-up 2 months later heappeared clinically and radiologically normal, with afull range of neck movements.
1.3. Case 3
A 7-year-old girl fell on her shoulder when an over-weight adult tripped and fell over her. On attendance tothe casualty she was noted to have a fracture of herright clavicle with torticollis. She also had pins andneedles in the right arm, but this subsided with physio-therapy over 1 week. She was discharged home with acollar-and-cuff sling.
The torticollis persisted with pain in the upper cervi-cal spine. She re-attended 6 weeks following injury withincreasing neck pain. Cervical spine X-rays showedatlantoaxial rotatory subluxation. She was treated con-servatively with continuous halter traction using 6-lb
* Corresponding author. Tel.: +44-1642-850850; fax: +44-1642-854136.
0020-1383/01/$ - see front matter © 2001 Elsevier Science Ltd. All rights reserved.PII: S 0020 -1383 (00 )00114 -5
R. Nannapaneni et al. / Injury, Int. J. Care Injured 32 (2001) 71–7372
weight. The neck pain and torticollis resolved within 3weeks. She was then discharged home with a Philadel-phia collar for 6 weeks. Two months later on follow-upshe was asymptomatic and appeared clinically and radi-ologically normal.
2. Discussion
The diagnosis of clavicular fracture in children rarelypresents a problem, unlike the recognition of AARS [1].AARS is a well-known but uncommon cause of child-hood torticollis.
The association of rotatory subluxation of C1 on C2with a clavicular fracture is difficult to appreciate clini-cally because of the masking of the torticollis by theacute symptoms of the fractured clavicle [2]. Our pa-tients were initially treated as having muscular spasmwithout providing any radiographic investigation andthe true nature of the torticollis was missed. As thesethree cases show it is only when the acute symptomssubside and the torticollis persists that the AARS issuspected.
All the three of our patients were children between 6and 7 years with a history of a fall onto the shouldersufficient to result in a clavicular fracture. All thepatients were noted to have torticollis on first atten-dance to the casualty. Careful clinical examinationwould have demonstrated the absence of spasm of thesternomastoid and help heighten suspicion of an associ-ated pathology as the cause of the torticollis. Moreover,the clinical appearance of the torticollis is differentfrom a greater degree of lateral rotation and forwardflexion of the head in AARS when compared with anisolated muscular spasm.
Corner first described AARS in detail in 1907 whenhe reviewed 20 cases [3]. The association of AARS andfracture of the clavicle was first emphasised by God-dard et al. [1]. In cases of trauma it is likely that themechanism of injury results in forced rotation com-bined with an element of flexion. This is consistent witha fall onto the shoulder. The flat facet joints in a child,whose ligaments are relatively lax, allow excessive rota-tion (beyond 45°) so permitting anterior subluxation ordislocation of C1 upon C2 [4,5]. This mechanism wouldexplain its co-existence with the clavicular fracture.
On plain radiography AARS has to be suspected ifthe atlantodental interval is more than 4 mm, if theatlas shows anterolisthesis with a posterior cervical lineother than normal, if the position of the dens axis iseccentric on AP view or if a different projection of bothatlantoaxial joints is recognised [6]. The diagnosis ofAARS may however be difficult or even impossible onroutine anteroposterior and lateral radiographs becausethe torticollis makes it impossible for the radiographerto judge the correct positioning [1]. In all such cases theclinician should be present and position the head in asclose to a neutral position as possible. CT should beobtained whenever plain radiography is abnormal or ifthe reason for the torticollis remains unclear [6].
The natural history of the condition is uncertainsince there are few reports of late untreated cases [1].AARS can be treated successfully if diagnosed within
Fig. 1. Lateral radiograph of cervical spine with increased atlantoden-tal interval and anterolisthesis of atlas.
Fig. 2. Axial CT scan showing significant AARS.
Fig. 3. Coronal CT reconstruction showing eccentric axis of dens inrelation to lateral masses of atlas.

R. Nannapaneni et al. / Injury, Int. J. Care Injured 32 (2001) 71–73 73
the first month. Failure to do so risks the developmentof neurological dysfunction and a chronic AARS whichcan only be treated by surgical fusion and this results inlimited upper cervical spine function [6]. Our patientsillustrate the relative ease of treatment if the fixed rotatorysubluxation is diagnosed early with only halter tractionbeing required to reduce and maintain the subluxation.
Lack of awareness of the association of AARS witha fractured clavicle may place undue reliance on conven-tional radiographs thus missing the AARS. Carefulclinical examination is paramount. It is important toexplain the presence of torticollis and be absolutelysatisfied with the radiographs and not assume it to be dueto protective sternomastoid spasm related to clavicularfracture. When doubt persists, CT scanning should bedone to exclude AARS.
References
[1] Goddard NJ, Stabler J, Alert JS. Atlanto-axial rotatory fixationand fracture of the clavicle. An association and a classification. JBone Jt Surg (Br) 1990;72(1):72–5.
[2] Al-Etani H, D’Astous J, Letts M, Hahn M, Yeadon A. Maskedrotatory subluxation of the atlas associated with fracture of theclavicle: a clinical and biomechanical analysis. Am J Orthop1998;27(5):375–80.
[3] Corner EM. Rotatory dislocation of the atlas. Ann Surg1907;14:9–26.
[4] Jacobsen G, Adler DC. Examination of the atlantoaxial jointfollowing injury with particular emphasis on rotational subluxa-tion. Am J Radiol 1956;76:1081–94.
[5] Wortzman G, Dewar FP. Rotatory fixation of the atlantoaxialjoint: rotational atlantoaxial subluxation. Radiology1968;90:479–87.
[6] Schwarz N. The fate of missed atlanto-axial rotatory subluxationin children. Arch Orthop Trauma Surg 1998;117(4–5):288–9.
.







