End TB strategy target setting
Philippe Glaziou
Manila, December 2014
Outline
• Rationale for global projections post-2015• TB burden assessment• Country targets
– Short-term (3-5 years)– Long-term (≥10 years)
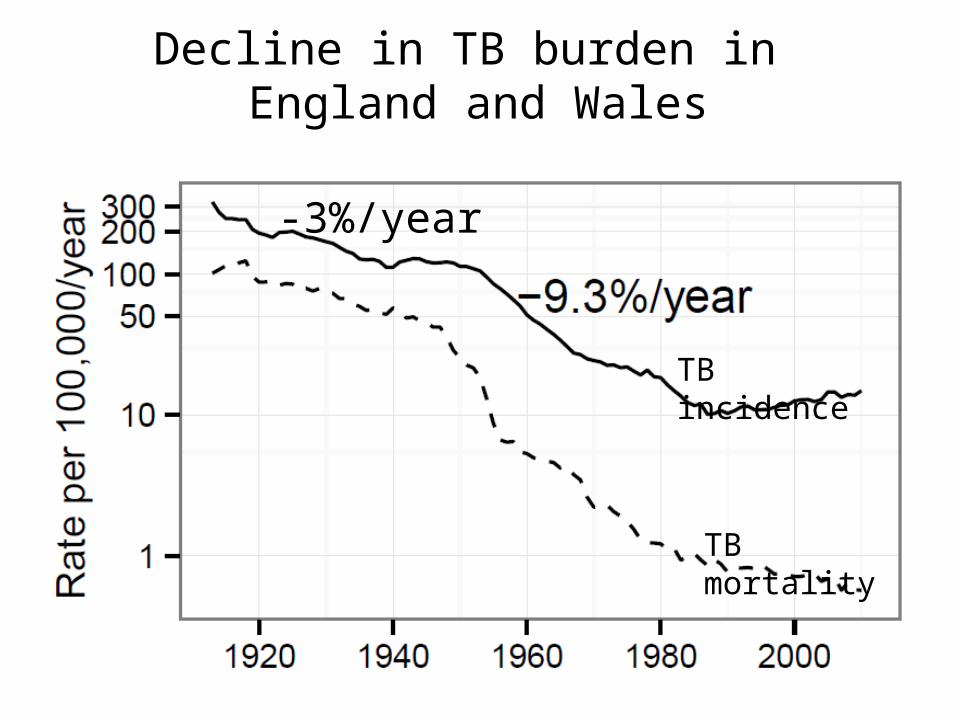
Decline in TB burden in England and Wales
TB mortality
TB incidence
-3%/year
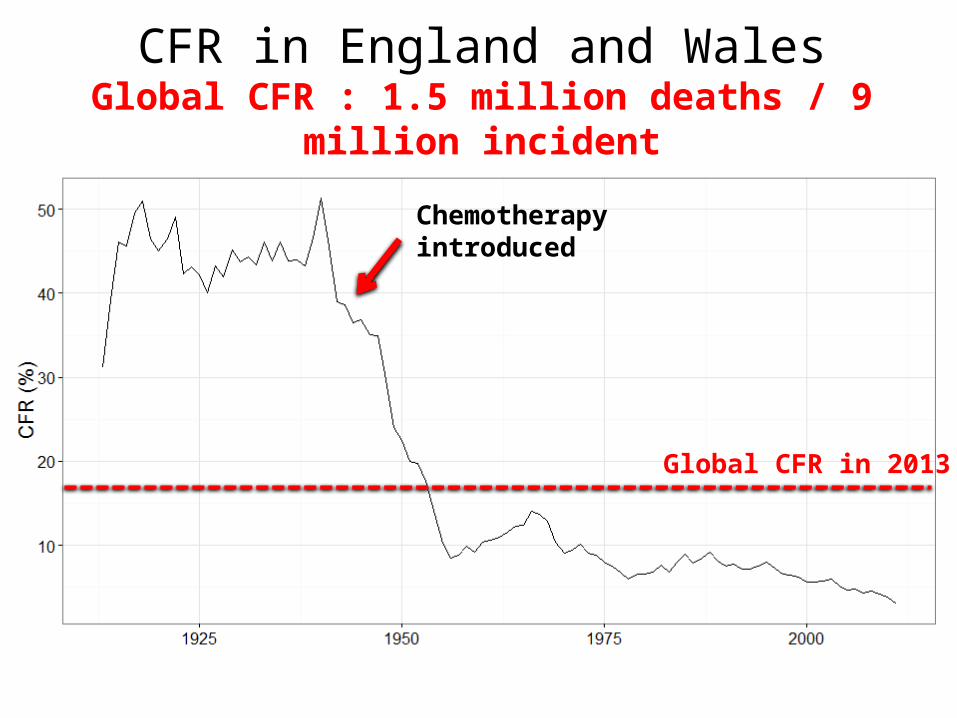
CFR in England and WalesGlobal CFR : 1.5 million deaths / 9 million incident
Chemotherapyintroduced
Global CFR in 2013
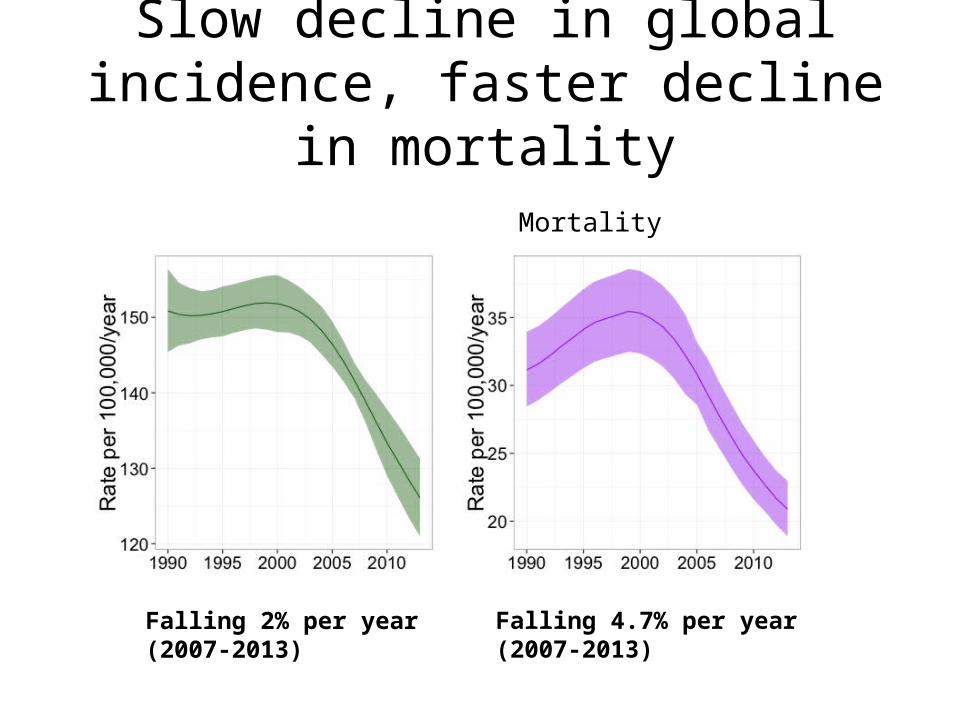
Slow decline in global incidence, faster decline in mortality
Incidence Mortality (including HIV)
Falling 2% per year(2007-2013)
Falling 4.7% per year(2007-2013)
Why is global TB incidence declining so slowly?
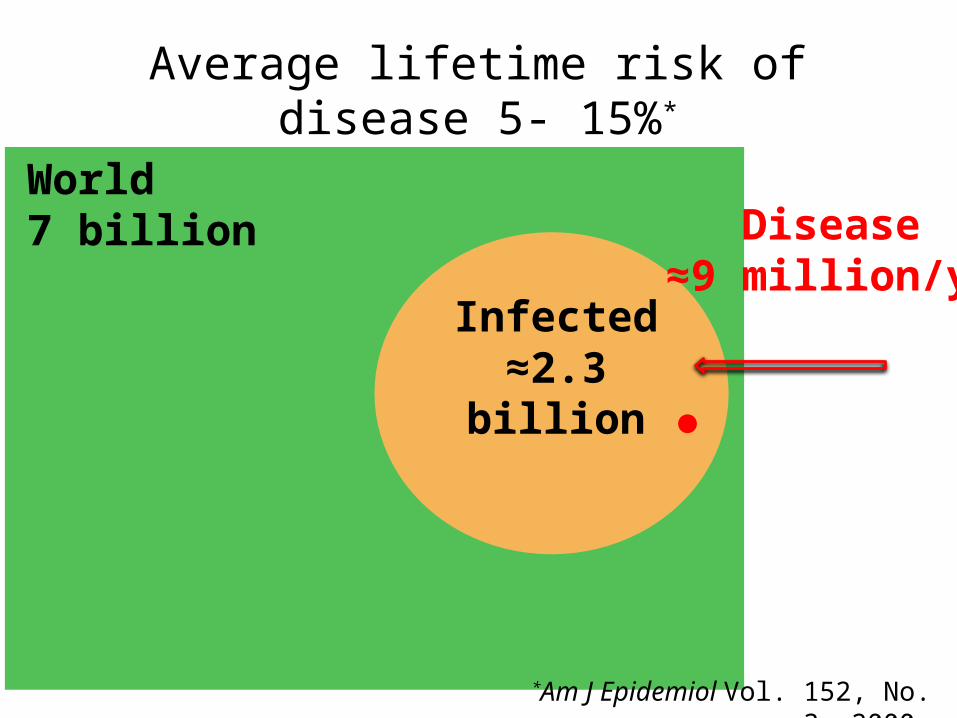
Average lifetime risk of disease 5- 15%*
World7 billion
Infected≈2.3 billion
Disease≈9 million/yr
*Am J Epidemiol Vol. 152, No. 3, 2000
Tools required for mitigating infection
• Mass Screening and Treatment may stop transmission but not TB reactivation
• Mass Prophylactic Treatment– IPT prevents 70% of reactivation in HIV-neg
Safety on a mass scale? (4-7/100,000 fatal hepatitis)Millard PS et al. West J Med. 1996 Jun;164(6):486-91.
• Mass Post-Exposure Vaccination
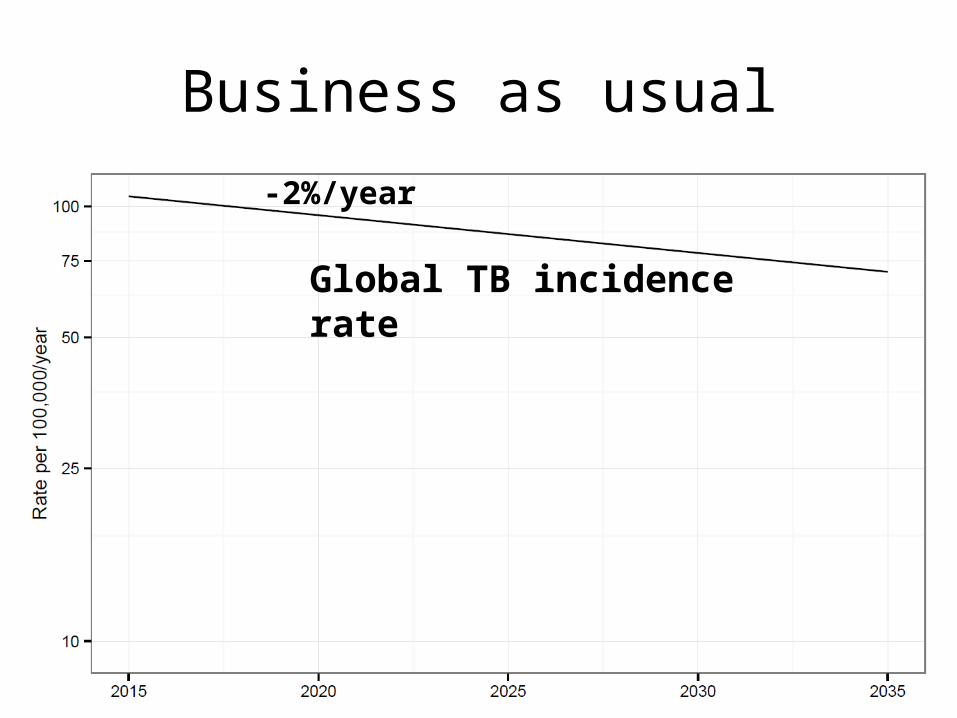
Business as usual
Global TB incidence rate
-2%/year
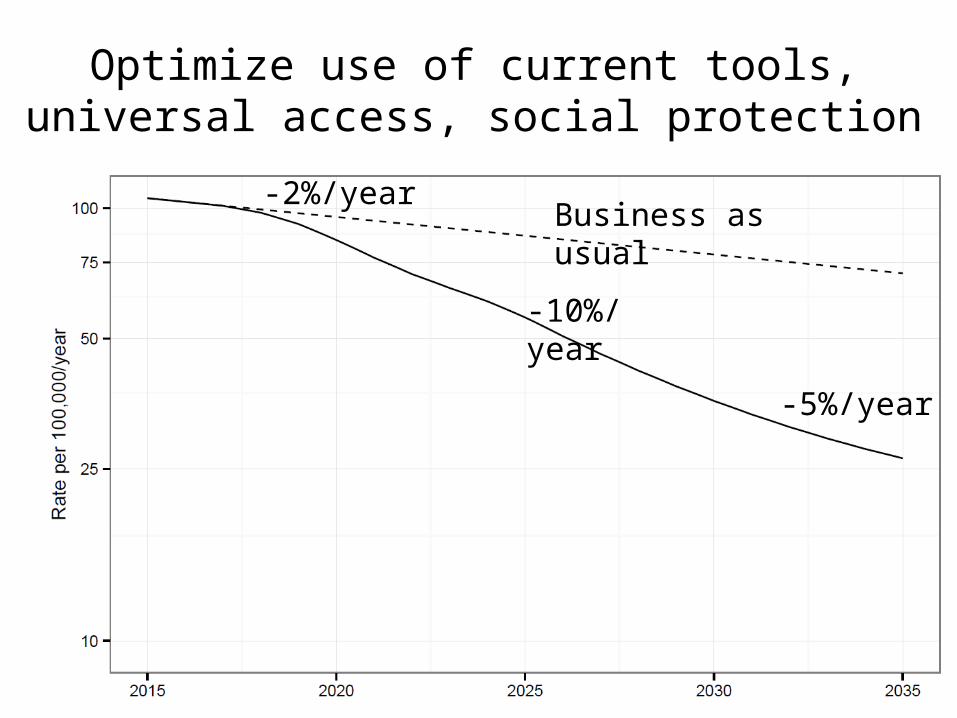
Optimize use of current tools, universal access, social protection
Business as usual
-10%/year
-5%/year
-2%/year
R&D pipelines
• No point of care test yet• 2 new drugs, little epi impact anticipated• 15 vaccines in development• New vaccine not likely until 2024
(AERAS)

Beyond 2025
Potential impact of vaccine– Introduced in 2025– 60% post-exposure efficacy– 95% coverage reached after 10 years– Assess year by which epidemic of TB could be
"ended"
~27+ billion
TB disease
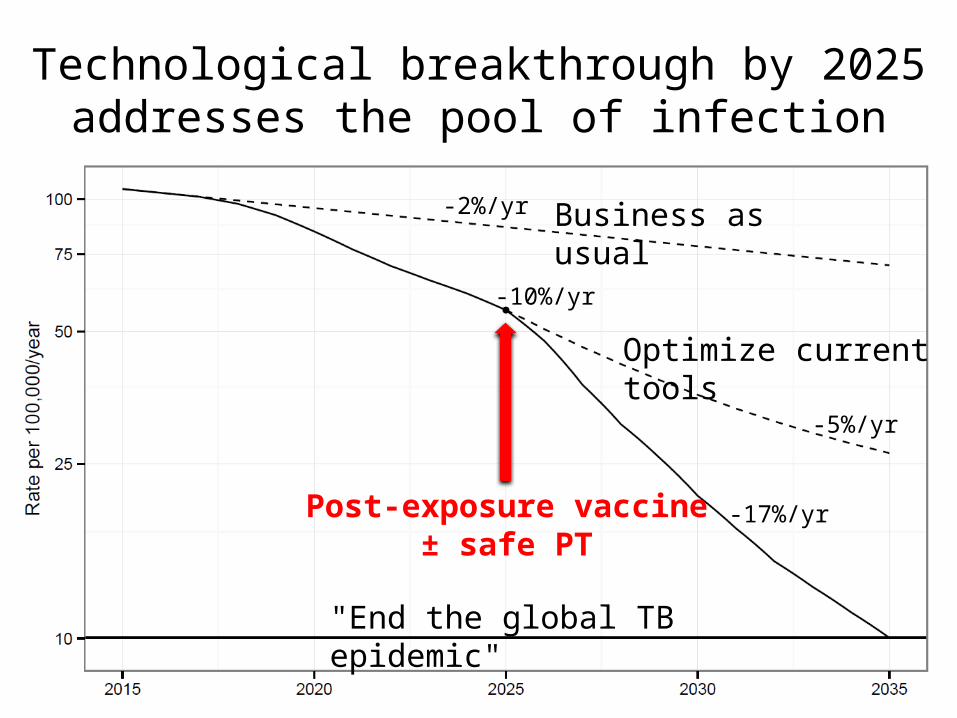
Technological breakthrough by 2025 addresses the pool of infection
Business as usual
Optimize current tools
Post-exposure vaccine± safe PT
"End the global TB epidemic"
-10%/yr
-2%/yr
-5%/yr
-17%/yr
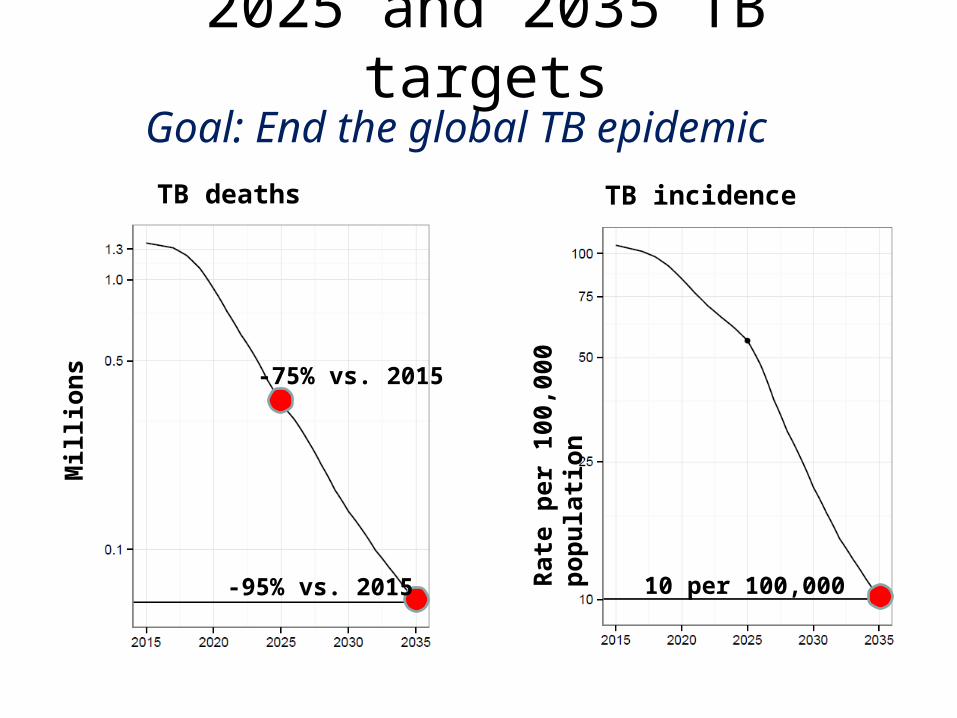
Goal: End the global TB epidemic
2025 and 2035 TB targets
TB incidence TB deaths
Rat
e p
er 1
00,0
00 p
op
ula
tio
n
Mill
ion
s
10 per 100,000
-75% vs. 2015
-95% vs. 2015
Estimating TB incidence
• National incidence surveys impractical• Best documented through state-of-the
art TB surveillance. Estimates are uncertain due to– Under-reporting– Under-diagnosis
• Estimation from tuberculin surveys not satisfactory
• Prevalence surveys
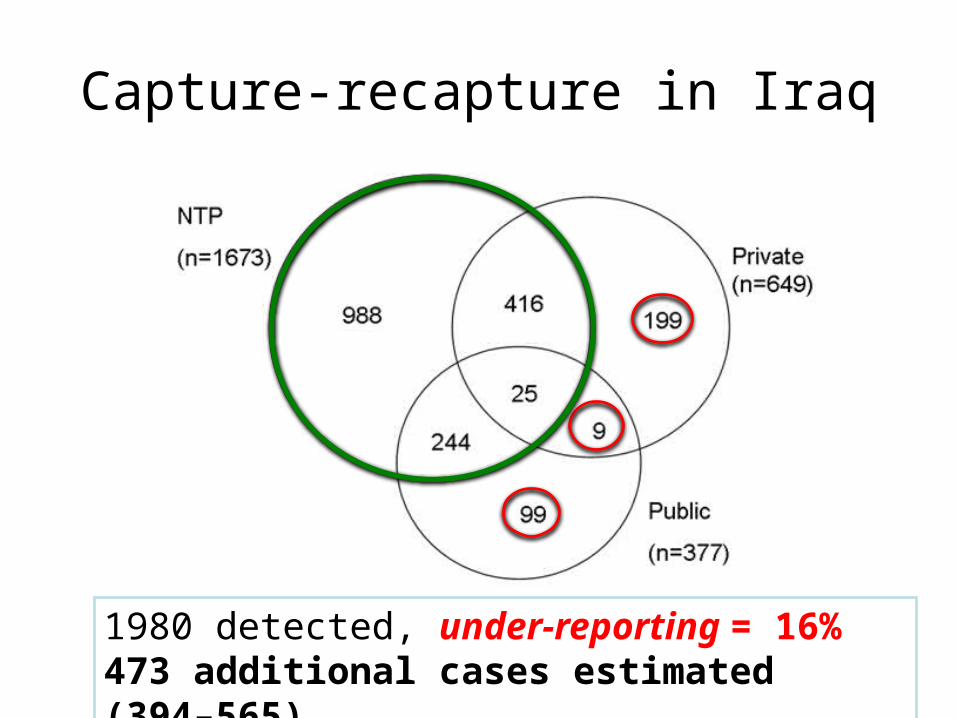
Capture-recapture in Iraq
1980 detected, under-reporting = 16%473 additional cases estimated (394–565)
How else can we estimate incidence?
- From results of prevalence surveys
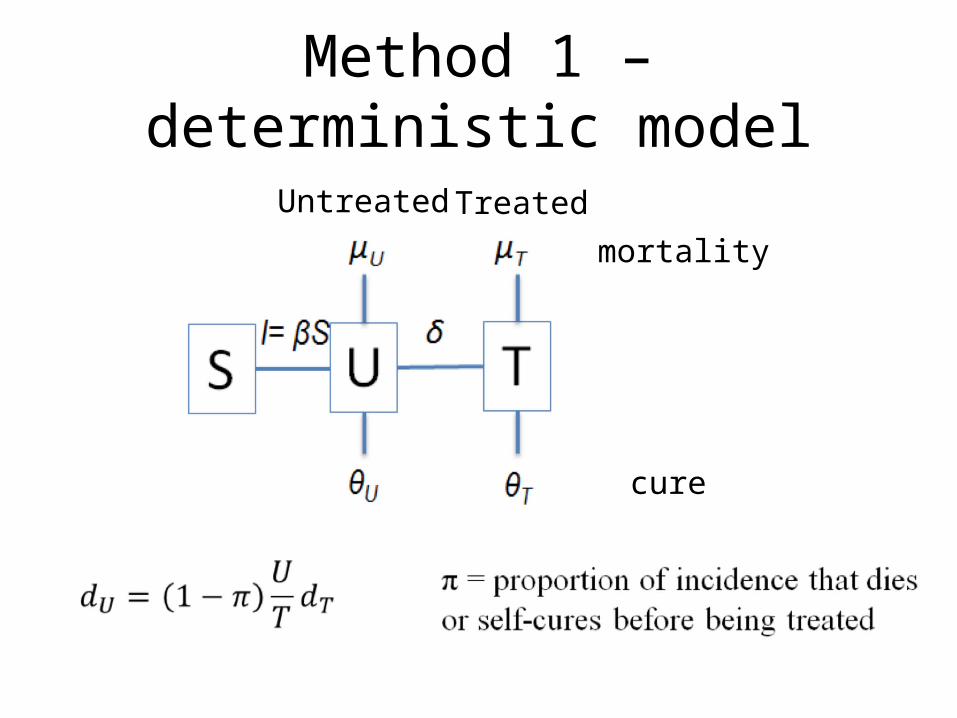
mortality
cure
Untreated Treated
Method 1 – deterministic model
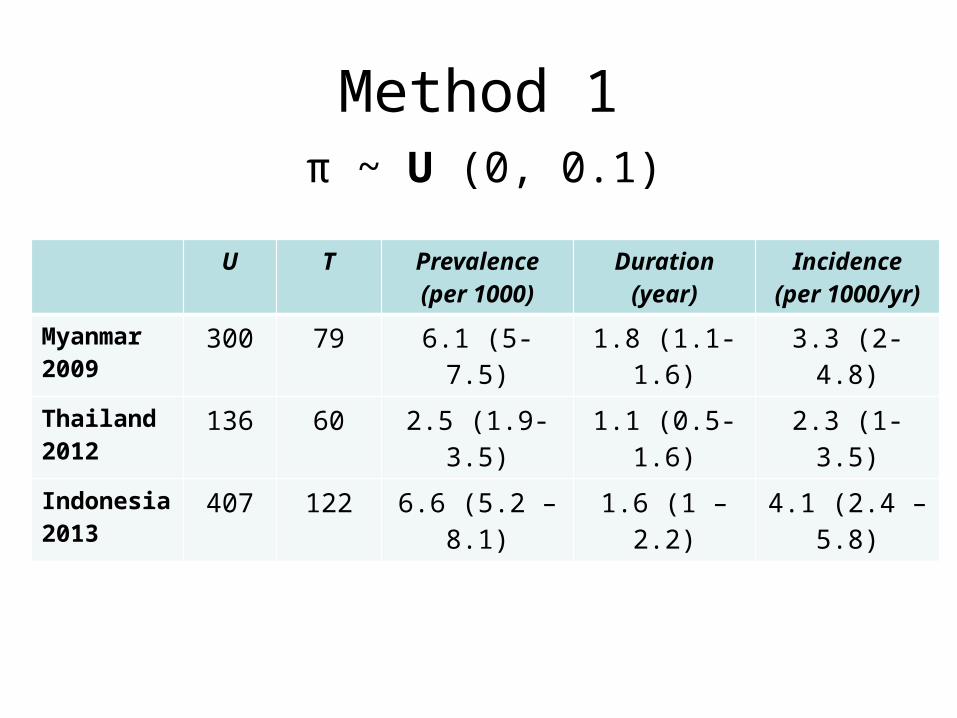
Method 1
U T Prevalence(per 1000)
Duration(year)
Incidence(per 1000/yr)
Myanmar 2009
300 79 6.1 (5-7.5) 1.8 (1.1-1.6) 3.3 (2-4.8)
Thailand 2012
136 60 2.5 (1.9-3.5) 1.1 (0.5-1.6) 2.3 (1-3.5)
Indonesia2013
407 122 6.6 (5.2 – 8.1) 1.6 (1 – 2.2) 4.1 (2.4 – 5.8)
π ~ U (0, 0.1)
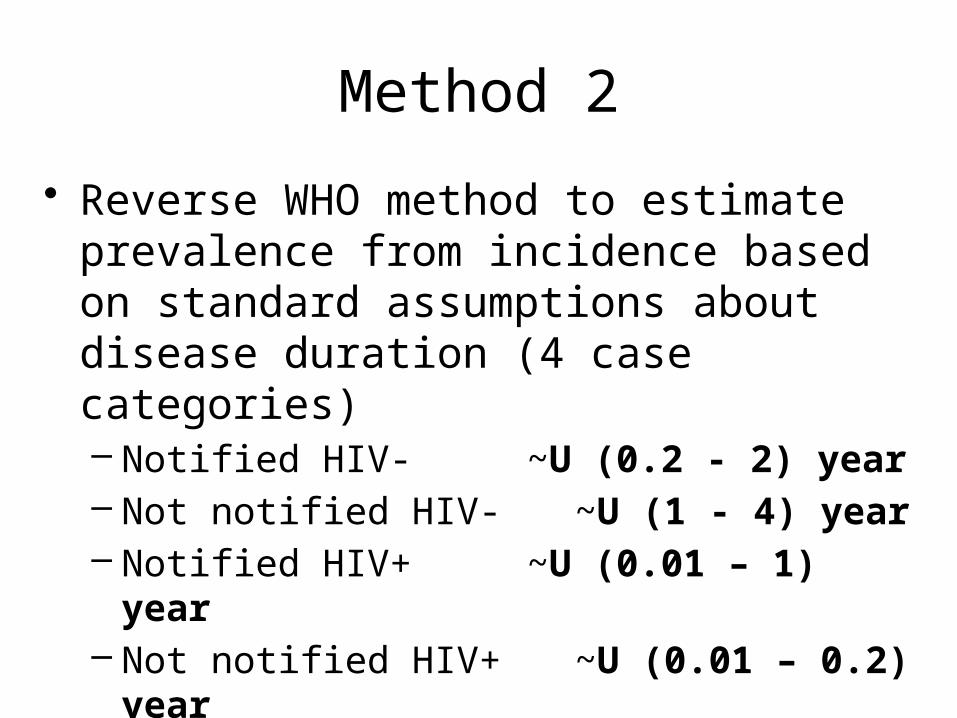
Method 2
• Reverse WHO method to estimate prevalence from incidence based on standard assumptions about disease duration (4 case categories)– Notified HIV- ~U (0.2 - 2) year– Not notified HIV- ~U (1 - 4) year– Notified HIV+ ~U (0.01 – 1) year– Not notified HIV+ ~U (0.01 – 0.2) year

Incidence in Indonesia (2013), ensemble model
Method 2(duration)
Method 1(dynamic)
Ensemble402 (276 - 552) per 100,000/year
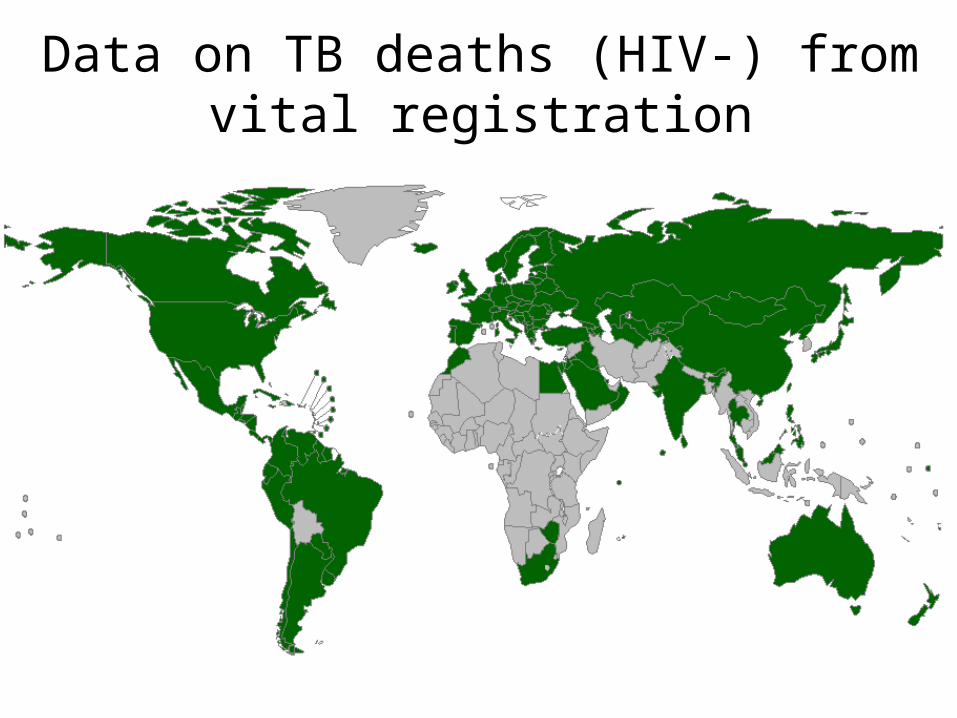
Data on TB deaths (HIV-) from vital registration
Sources of data
• Best sources of data on TB burden are – TB notifications when data meet quality criteria
and under-reporting low and documented– TB mortality from Vital Registration with COD– Prevalence from national prevalence surveys
• Impact assessment methods tailored to the existing data
• 2015: meeting the WHO task force on TB impact measurement to review methods to evaluate the 2015 targets achievement
Short-term targetting (3-5 years)
• Monitor progress towards set target• Use a directly measured indicator
– Not incidence, not CDR, because in most cases it will not be possible to state whether the country is on track
– Mortality if Vital Registrations or sample VR– Prevalence if repeat survey within the
programme cycle– Case notifications– Treatment success
Adaptation at country level
• Short-term targets (2016-2020)– Based on a thorough epi analysis, standards
and benchmarks for surveillance– Assessment of planned actions
• Long-term targets (2025, 2035)– Project incidence and CFR over time– Target for catastrophic cost achieved if
universal access is achieved
In conclusion
• Ambitious post-2015 global targets• Country adoption of targets:
– Evaluate surveillance system– Projections
• Short-term, programme planning based on measurable indicators
• Long-term, based on indicators that will become measurable
– Acceleration of the decline in incidence– Improvements over the case fatality ratio (% of incident
cases who die from TB) faster decline of TB mortality







