
Cancer Therapy: Clinical
CTLA4 Blockade Induces Frequent Tumor Infiltration by ActivatedLymphocytes Regardless of Clinical Responses in Humans
Rong Rong Huang1, Jason Jalil2, James S. Economou3,4, Bartosz Chmielowski2, Richard C. Koya3,Stephen Mok3, Hooman Sazegar2, Elizabeth Seja2, Arturo Villanueva2, Jesus Gomez-Navarro5,John A. Glaspy2,4, Alistair J. Cochran1, and Antoni Ribas2,3,4
AbstractBackground: CTLA4 blocking monoclonal antibodies provide durable clinical benefit in a subset of
patients with advanced melanoma mediated by intratumoral lymphocytic infiltrates. A key question is
defining whether the intratumoral infiltration (ITI) is a differentiating factor between patients with and
without tumor responses.
Methods: Paired baseline and postdosing tumor biopsy specimens were prospectively collected from 19
patients with metastatic melanoma, including 3 patients with an objective tumor response, receiving the
anti-CTLA4 antibody tremelimumab within a clinical trial with primary endpoint of quantitating CD8þ
cytotoxic T-lymphocyte (CTL) infiltration in tumors. Samples were analyzed for cell density by automated
imaging capture and further characterized for functional lymphocyte properties by assessing the cell
activation markers HLA-DR and CD45RO, the cell proliferation marker Ki67, and the regulatory T-cell
marker FOXP3.
Results: There was a highly significant increase in ITI by CD8þ cells in biopsy samples taken after
tremelimumab treatment. This included increases between 1-fold and 100-fold changes in 14 of 18
evaluable cases regardless of clinical tumor response or progression. There was no difference between the
absolute number, location, or cell density of infiltrating cells between clinical responders and patients with
nonresponding lesions that showed acquired intratumoral infiltrates. There were similar levels of expres-
sion of T-cell activation markers (CD45RO, HLA-DR) in both groups and no difference in markers for cell
replication (Ki67) or the suppressor cell marker FOXP3.
Conclusion: CTLA4 blockade induces frequent increases in ITI by T cells despite which only a minority
of patients have objective tumor responses. Clin Cancer Res; 17(12); 4101–9. �2011 AACR.
Introduction
Costimulatory and co-inhibitory molecules are keyplayers in the activation step of the adaptive immunesystem and regulate the expansion and effector functionsof antigen-specific T cells (1). CTLA4 has a pivotal role inthis interaction, dampening immune responses to self-antigens (2). Ipilimumab, a fully human IgG1 anti-CTLA4
antibody (formerly MDX-010; Bristol-Myers Squibb), hasshown improvement in overall survival relative to a peptidevaccine in a phase 3 randomized clinical trial in patientswith metastatic melanoma previously treated with stan-dard-of-care therapies (3), presenting the therapeutic activ-ity of this class of antibodies. Despite this success, theclinical experience shows that the objective response rateof patients with metastatic melanoma treated with ipili-mumab, or the IgG2 anti-CTLA4 antibody tremelimumab(formerly CP-675,206; Pfizer), is low, in the range of 5% to15%, and they both have similar rates of inflammatory andautoimmune toxicities (grade �3) in approximately 20%of patients in pivotal phase 2 trials in second-line therapyfor melanoma (4, 5). However, most patients with objec-tive tumor regression have durable responses, the longestongoing since 2001 (6). The proof of concept of antitumoractivity and patient benefit with CTLA4 blockade have beenachieved, but there is a clear need to determine whatdifferentiates patients who respond from those who showtumor progression.
Multiple groups have studied how anti-CTLA4 antibo-dies impact the human immune system and the mechan-isms that determine tumor response or progression.
Authors' Affiliations: Departments of 1Pathology and Laboratory Med-icine, 2Medicine, Division of Hematology/Oncology, and 3Surgery, Divisionof Surgical Oncology, and 4Jonsson Comprehensive Cancer Center,University of California, Los Angeles (UCLA), Los Angeles, California;and 5Pfizer Global Research and Development, New London, Connecticut
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Current address for J. Gomez-Navarro: Millennium-Takeda, Boston, Mas-sachusetts.
Corresponding Author: Antoni Ribas, Division of Hematology-Oncology,11-934 Factor Building, UCLA Medical Center, 10833 Le Conte Avenue,Los Angeles, CA 90095. Phone: 310-206-3928; Fax: 310-825-2493.E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-11-0407
�2011 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org 4101
Research. on July 15, 2018. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 10, 2011; DOI: 10.1158/1078-0432.CCR-11-0407

Analysis of the effects of anti-CTLA4 antibodies in patientshas been mainly based on the study of peripheral bloodsamples (7–18). Studying the effects of CTLA4 blockingantibodies in tumor samples allows analysis of the inter-action between an activated immune system and its cancercell targets. Preclinical models suggest a key role for CTLA4both in the infiltration of T lymphocytes into peripheraltissues including tumors and in the modulation of theduration of the interaction between T cells and cells pre-senting with cognate antigens (19, 20). These data predictthat the use of CTLA4 blocking antibodies should increaseintratumoral infiltration (ITI) by lymphocytes and retaintumor antigen–specific T cells within tumors. Clinical datato date show lymphocytic ITI in tumor biopsies of patientresponding after the administration of anti-CTLA4 anti-bodies (16, 17, 21, 22).
In a prior study, we analyzed 15 tumor biopsy samplestaken at different time points from 7 patients treated withtremelimumab, with lesions biopsied when there wasclinical evidence of either response or progression (22).Clinically responding lesions had diffuse intratumoralinfiltrates by CD8þ T cells that were markedly increasedin cases for whom comparison with a baseline biopsy wasavailable. These T-cell infiltrates were massive at the peakof the response at around 1 to 2 months after the firstantibody infusion, occupying much of the biopsiedregressing lesions. Interestingly, expression of FOXP3and indoleamine-2,3-dioxygenase, 2 proteins associatedwith immunosuppressive cells in the tumor microenvir-onment [regulatory T cells (Treg) and plasmacytoiddendritic cells, respectively], were actually increased inthe regressing lesions, particularly at the sites of immunecell–melanoma cell interaction (22). The retrospectivenature of that analysis (22) may have induced bias;patients with responding tumors were prone to be biop-sied at one stage of the response whereas those withdisease progression were primarily biopsied when the
therapy effects may be overwhelmed by melanomaprogression.
Therefore, a key question remains whether the presenceor degreeof ITI of T cells differentiates betweenpatientswithand without objective tumor responses in prospectivelyconducted tumor biopsy samples taken at a defined timepoint. Therefore, we conducted a clinical trial with pairedbaseline and postdosing tumor biopsy specimens collectedwithin 1 and 2 months from the first dose of the CTLA4blocking antibody.Ourmain finding is a remarkable induc-tion of immune cell infiltrates by CD4þ andmostly CD8þ Tcells after the administration of tremelimumab. This waspresent both in lesions that went on to objective tumorresponse and in half of the lesions that progressed.
Materials and Methods
Clinical trial designThirty-two patients with measurable advanced mela-
noma (stages IIIc–IV) with metastatic lesions amenableto outpatient biopsies were enrolled in this phase II clinicaltrial (UCLA IRB# 06-06-093 IND# 100453, clinical trialregistration NCT00471887). Patients received single-agenttremelimumab at 15 mg/kg every 3 months with baselineand approximately day 30 to 60 postdosing biopsies.Samples were coded with the study denomination of GAand a patient-specific number. Adverse events attributed totremelimumab were graded according to the NCI commontoxicity criteria version 2.0 (23). Patients who experiencedthe following adverse events at any time during the pre-vious cycle were considered to have a dose limiting toxicity(DLT) and treatment with tremelimumab was discontin-ued: grade 4 treatment-related adverse event; grade 3 orhigher hypersensitivity reaction; grade 2 or higher colitis;and/or autoimmune reaction in a critical organ (brain, eye,liver, thyroid, hypophysis). Objective clinical responseswere recorded following a modified Response EvaluationCriteria in Solid Tumors (RECIST; ref. 24), wherein skinand subcutaneous lesions evaluable only by physical exam-ination were considered measurable if adequately recordedusing a photographic camera with a measuring tape orruler; there was no minimum size restriction for theselesions.
Sample procurement and immunohistochemicalquantitation of CD4þ and CD8þ cells
Biopsies samples were formalin-fixed and paraffin-embedded and stained for immunohistochemistry (IHC)as previously described (22) with anti-CD4 (clone 4B12;NeoMarkers) and anti-CD8 (clone C8/144B’; Dako). TheSimple-PCI Imaging System (version 5.2.1.1609; CompixInc. Imaging System) was utilized to quantitatively evaluateT-cell infiltration. The frequency of intratumoral and peri-tumoral lymphocytes was assessed by analyzing 10 tumorareas from each sample at 200�magnification. The densitywas compared between pretreatment and posttreatmentbiopsies. All samples were analyzed without the knowledgeof the patients’ clinical outcomes.
Translational Significance
After 10 years of clinical development, it is stillunclear how anti-CTLA4 blocking monoclonal antibo-dies mediate antitumor responses and why only a fewpatients have durable responses. The anticipatedmechanism of action is the stimulation of a cytotoxicT-lymphocyte (CTL) response against the cancer, whichrequires studying such cells within tumors. We docu-mented, using paired tumor biopsy samples frompatients treated with the CTLA4 blocking antibodytremelimumab, a remarkable intratumoral infiltrationby activated CTLs in most patients regardless of having atumor response. This evidence suggests that the keydeterminant of tumor response or resistance residesin the interaction between CTLs and their tumor targets,as opposed to the more frequently studied effects ofCTLA4 blocking antibodies on cells or proteins detect-able in the blood.
Huang et al.
Clin Cancer Res; 17(12) June 15, 2011 Clinical Cancer Research4102
Research. on July 15, 2018. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 10, 2011; DOI: 10.1158/1078-0432.CCR-11-0407
Immunohistochemical staining for T-cell activation,proliferation, and regulatory markersPostdosing biopsy specimens with significant increase in
T-cell infiltrates were stained by immunohistochemicaldouble staining with anti-HLA-DR (clone TAL, 1B5; Dako)and anti-CD45RO (clone UCHL1; Dako), and single stain-ing with Ki67 (clone MIB-1; Dako) or anti-FOXP3 (clone236A/E7; Abcam).
Statistical analysisThe statistical design of this clinical trial was based on the
assumption of a 20% or higher probability of increasedCD8þ infiltration in posttreatment biopsies detected byIHC. This assumption was based on the lower boundary ofchange in CD8þ infiltration from our prior studies (22).Two scores using semiquantitative analysis of immunohis-tochemical data (0 to 2þ, 1þ to 3þ) were assessed. Abinomial test was used at 5% level of significance. If thetrue probability of infiltration increased by at least 2 scorelevels in at least 50% of the tremelimumab-treated patients,then 20 to 21 evaluable patients would provide 90% powerto reject the null hypothesis. The Mann–Whitney rank-sumtest was used to compare values obtained from assessmentof the pre- and posttreatment samples. Analyses were doneusing the SigmaPlot software package, and all tests were 2-sided with the significance level set at P ¼ 0.05.
Results
Patient characteristics, clinical response, andtoxicitiesThirty-two patients were enrolled (Table 1). Themajority
of patients had M1c metastatic melanoma (visceral metas-tasis and/or high lactate dehydrogenase level) and morethan half of the patients had received prior systemic ther-apy, most frequently a chemotherapy-containing regimen.There were 9 patients with clinically relevant toxicitiesprospectively defined as DLTs that precluded continueddosing with tremelimumab. One patient had immunethrombocytopenia purpura (ITP), which developed within1 week after the first dose; grade 3 colitis in 5 patients, 2during the first cycle and the other 3 while on chronicmaintenance dosing; 1 patient with a grade 3 skin rash inthe first cycle; and 2 with grade 2 hypophysitis, both duringthe second or later cycles. Three patients had an objectiveand durable tumor response, all with a complete responseof in-transit metastasis (patients GA18, GA29, and GA33).One additional patient had an objective response in supra-clavicular and laterocervical lymph nodes meeting partialresponse criteria, followed by slow disease progression ofnodal metastasies 7 months after initiating dosing withtremelimumab (patient GA5). This patient died from anunrelated cause (infectious osteomyelitis after an acciden-tal wound) 20 months after starting tremelimumab, withactive nodal metastases of melanoma localized in thesupraclavicular area but without widespread systemicmetastasis. There are 7 patients alive beyond 2 years, the3 patients with a complete response (35þ, 30þ and 28þ
months from study start), and 4 patients who are alive withmetastatic melanoma (follow-up between 29þ to 41þmonths) despite not having an objective response to tre-melimumab (patients GA7, GA19, GA26, and GA32).
Biopsy sample procurementPaired tumor biopsy samples before and after the first
infusion with tremelimumab were obtained in 21 of the 32patients enrolled in this clinical trial. Reasons for obtainingonly a baseline biopsy were absence of melanoma in thebiopsy specimen in 1 case, toxicity within the first cycleresulting in inability to return for the postdosing biopsy in
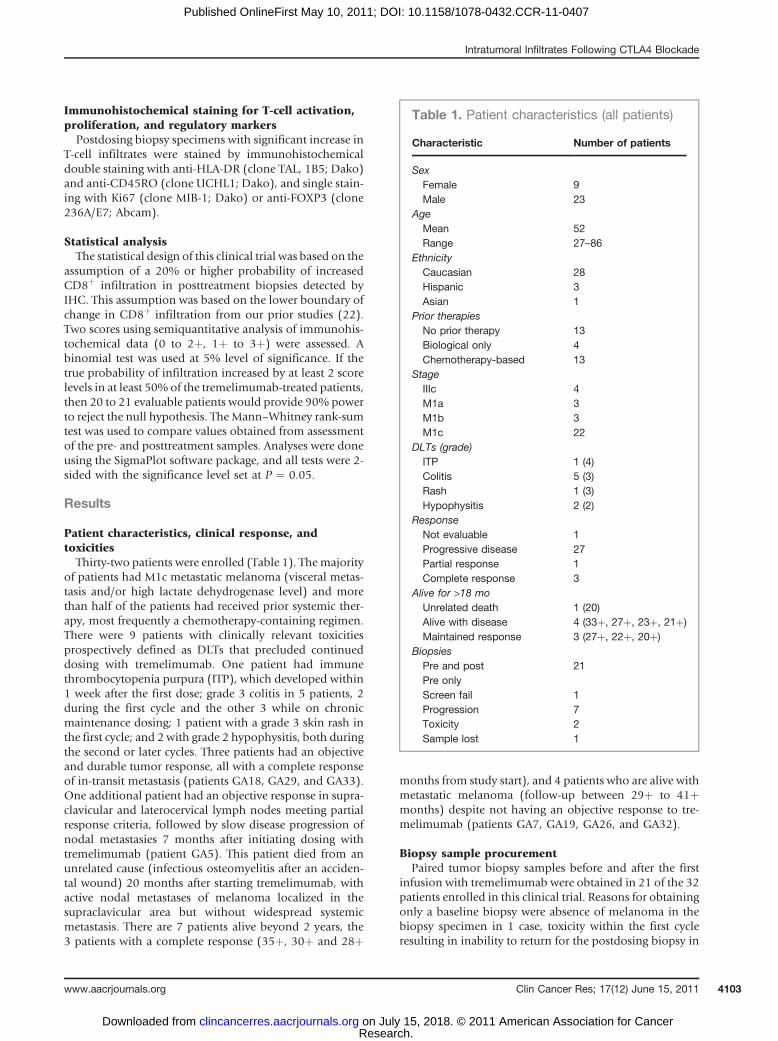
Table 1. Patient characteristics (all patients)
Characteristic Number of patients
SexFemale 9Male 23
AgeMean 52Range 27–86
EthnicityCaucasian 28Hispanic 3Asian 1
Prior therapiesNo prior therapy 13Biological only 4Chemotherapy-based 13
StageIIIc 4M1a 3M1b 3M1c 22
DLTs (grade)ITP 1 (4)Colitis 5 (3)Rash 1 (3)Hypophysitis 2 (2)
ResponseNot evaluable 1Progressive disease 27Partial response 1Complete response 3
Alive for >18 moUnrelated death 1 (20)Alive with disease 4 (33þ, 27þ, 23þ, 21þ)Maintained response 3 (27þ, 22þ, 20þ)
BiopsiesPre and post 21Pre onlyScreen fail 1Progression 7Toxicity 2Sample lost 1
Intratumoral Infiltrates Following CTLA4 Blockade
www.aacrjournals.org Clin Cancer Res; 17(12) June 15, 2011 4103
Research. on July 15, 2018. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 10, 2011; DOI: 10.1158/1078-0432.CCR-11-0407
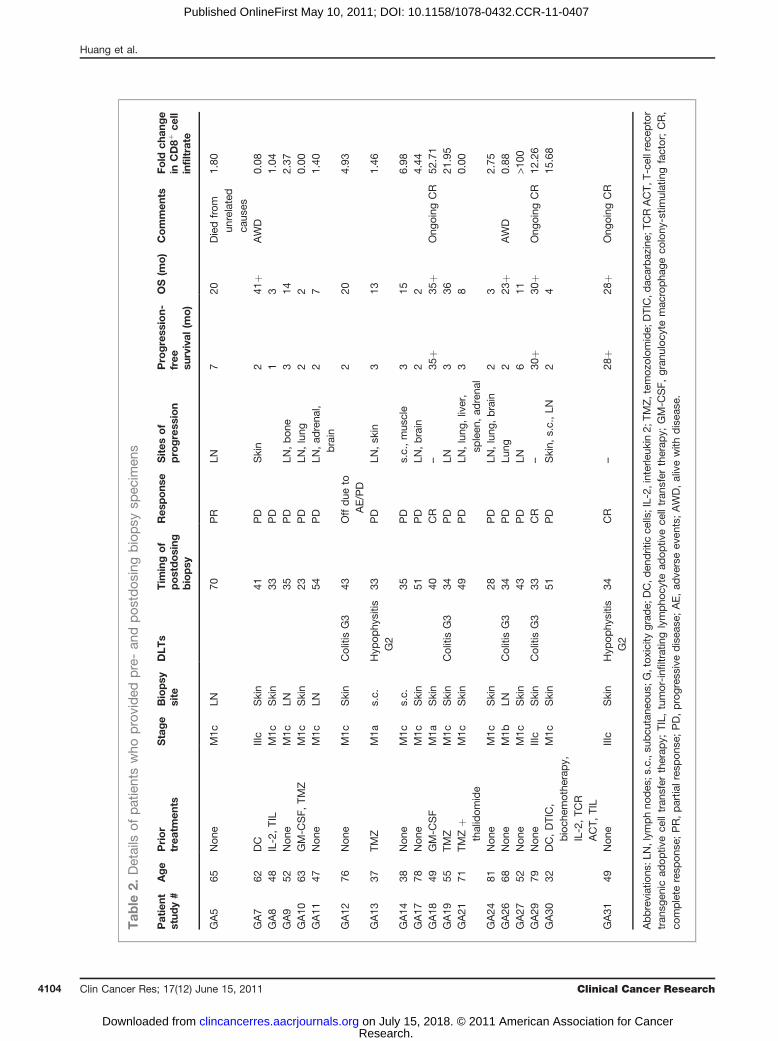
Tab
le2.
Details
ofpatientswho
provided
pre-an
dpos
tdos
ingbiopsy
spec
imen
s
Patient
stud
y#
Age
Prior
trea
tmen
tsStage
Biopsy
site
DLT
sTim
ingof
postdosing
biopsy
Res
pons
eSites
of
progress
ion
Progress
ion-
free
survival
(mo)
OS(m
o)
Commen
tsFo
ldch
ange
inCD8þ
cell
infiltrate
GA5
65Non
eM1c
LN70
PR
LN7
20Diedfrom
unrelated
caus
es
1.80
GA7
62DC
IIIc
Skin
41PD
Skin
241
þAWD
0.08
GA8
48IL-2,TIL
M1c
Skin
33PD
13
1.04
GA9
52Non
eM1c
LN35
PD
LN,bon
e3
142.37
GA10
63GM-C
SF,
TMZ
M1c
Skin
23PD
LN,lung
22
0.00
GA11
47Non
eM1c
LN54
PD
LN,ad
rena
l,brain
27
1.40
GA12
76Non
eM1c
Skin
ColitisG3
43Offdue
toAE/PD
220
4.93
GA13
37TM
ZM1a
s.c.
Hyp
ophy
sitis
G2
33PD
LN,sk
in3
131.46
GA14
38Non
eM1c
s.c.
35PD
s.c.,mus
cle
315
6.98
GA17
78Non
eM1c
Skin
51PD
LN,brain
22
4.44
GA18
49GM-C
SF
M1a
Skin
40CR
–35
þ35
þOng
oing
CR
52.71
GA19
55TM
ZM1c
Skin
ColitisG3
34PD
LN3
3621
.95
GA21
71TM
Zþ
thalidom
ide
M1c
Skin
49PD
LN,lung
,liver,
spleen
,ad
rena
l3
80.00
GA24
81Non
eM1c
Skin
28PD
LN,lung
,brain
23
2.75
GA26
68Non
eM1b
LNColitisG3
34PD
Lung
223
þAWD
0.88
GA27
52Non
eM1c
Skin
43PD
LN6
11>1
00GA29
79Non
eIIIc
Skin
ColitisG3
33CR
–30
þ30
þOng
oing
CR
12.26
GA30
32DC,DTIC,
bioch
emothe
rapy,
IL-2,TC
RACT,
TIL
M1c
Skin
51PD
Skin,
s.c.,LN
24
15.68
GA31
49Non
eIIIc
Skin
Hyp
ophy
sitis
G2
34CR
–28
þ28
þOng
oing
CR
Abbreviations
:LN,lym
phno
des
;s.c.,su
bcu
tane
ous;
G,tox
icity
grad
e;DC,d
endritic
cells;IL-2,
interle
ukin
2;TM
Z,tem
ozolom
ide;
DTIC,d
acarbaz
ine;
TCRACT,
T-ce
llrece
ptor
tran
sgen
icad
optiv
ece
lltran
sfer
therap
y;TIL,
tumor-infiltratin
glympho
cyte
adop
tivece
lltran
sfer
therap
y;GM-C
SF,
gran
uloc
ytemac
ropha
geco
lony
-stim
ulatingfactor;CR,
complete
resp
onse
;PR,partia
lres
pon
se;PD,progres
sive
disea
se;AE,ad
verseev
ents;AWD,alivewith
disea
se.
Huang et al.
Clin Cancer Res; 17(12) June 15, 2011 Clinical Cancer Research4104
Research. on July 15, 2018. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 10, 2011; DOI: 10.1158/1078-0432.CCR-11-0407
2 patients (ITP and colitis), and early disease progression in7 patients who withdrew consent before the proposedpostdosing biopsy. The postdosing sample from 1 of the21 patients with paired biopsies could not be retrieved foranalysis (patient GA32). The postdosing biopsy specimenfrom patient GA25 did not contain melanoma. The pre-senting characteristics and outcome of the remaining 19patients with pre- and postdosing biopsies available foranalysis are presented in Table 2.
Tumor infiltration by T lymphocytesUp to 10 randomly selected fields per sample were
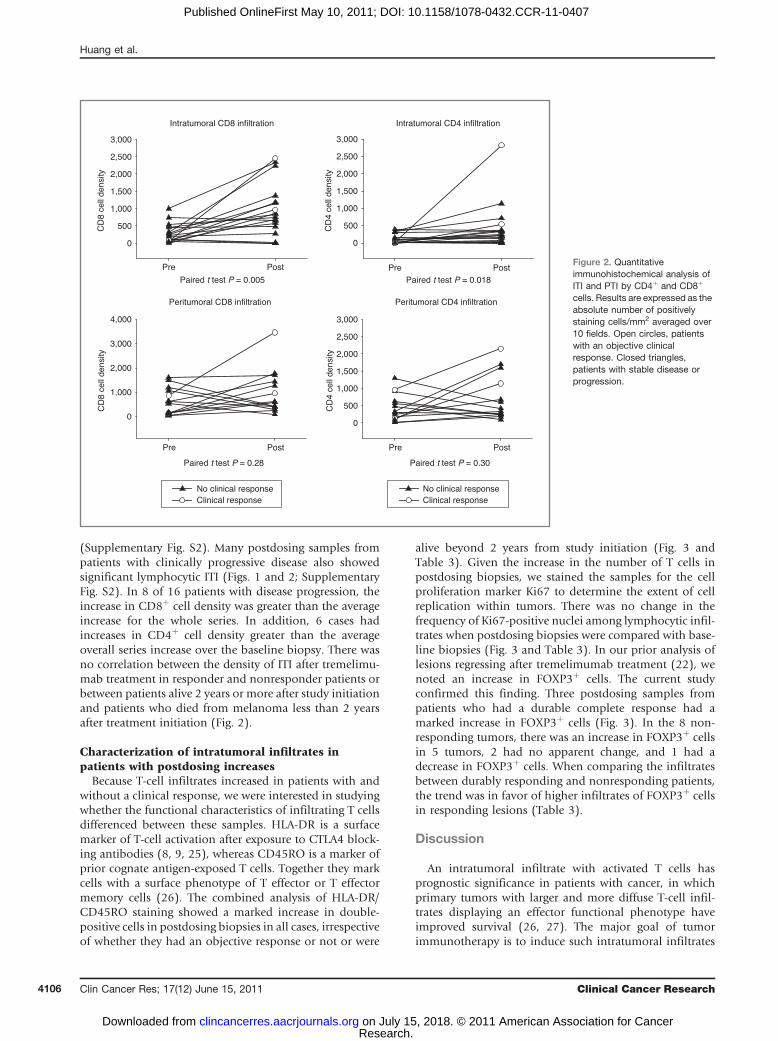
analyzed for ITI (when T cells were mixed within themelanoma cells) and peritumoral infiltration (PTI, whenT-cell infiltrates are located peripheral to the tumor massand in collagen bundles that dissected the tumor mass).Overall, there was a marked and highly statistically sig-nificant increase in ITI by CD8þ cells in biopsy samplestaken after tremelimumab treatment (Figs. 1 and 2). Themean pretreatment CD8þ cell count was 289 cells/mm2
(SEM ¼ 61), and the postdosing density of these cellsincreased to 955 (SEM ¼ 191, P ¼ 0.005; Fig. 2). Thedifference in ITI for CD4þ cells was also significantlyincreased but at a lower magnitude (mean predosing104 � 32 vs. mean postdosing 428 � 156, P ¼ 0.018;Fig. 2). Analysis of PTI by lymphocytes was not feasible in 5cases with metastatic melanoma to the lymph nodes
because the great majority of peritumoral cells were nodallymphocytes. Among the remaining cases, there were nosignificant changes in PTI by CD8þ or CD4þ cells (Sup-plementary Fig. S1), as there was no evidence of tumoradjacent infiltration by T cells in skin biopsies beyond themetastases (data not shown).
Analysis of tumor-infiltrating lymphocytes dependingon clinical response
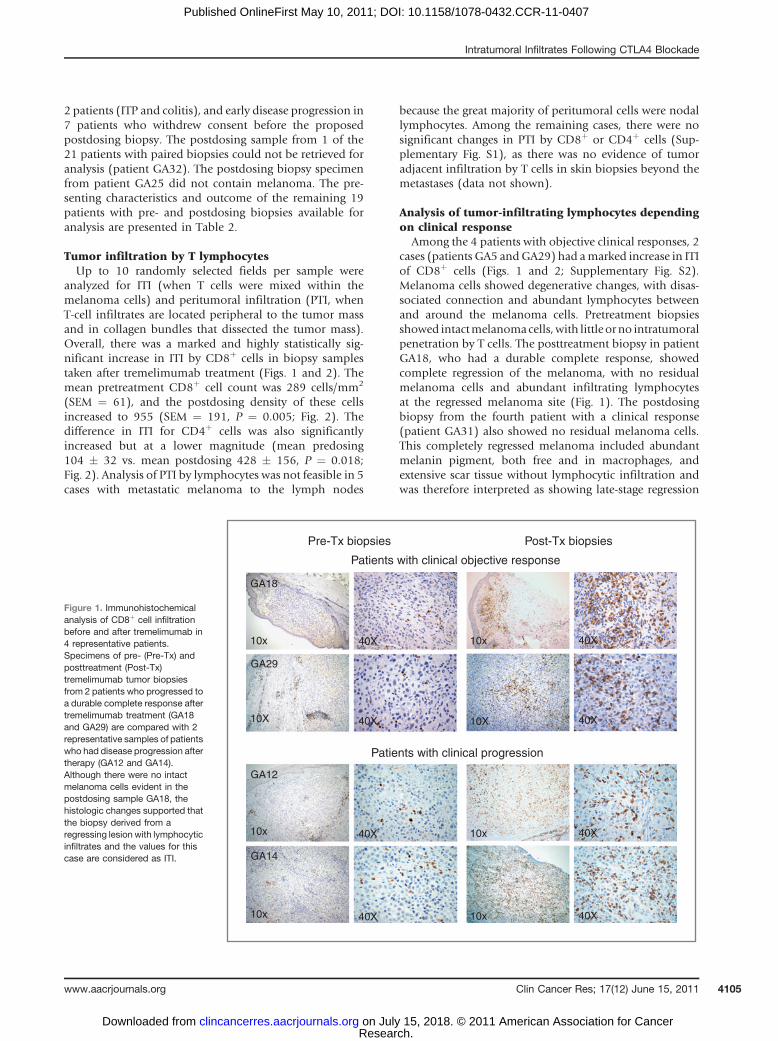
Among the 4 patients with objective clinical responses, 2cases (patients GA5 andGA29) had amarked increase in ITIof CD8þ cells (Figs. 1 and 2; Supplementary Fig. S2).Melanoma cells showed degenerative changes, with disas-sociated connection and abundant lymphocytes betweenand around the melanoma cells. Pretreatment biopsiesshowed intactmelanomacells,with little orno intratumoralpenetration by T cells. The posttreatment biopsy in patientGA18, who had a durable complete response, showedcomplete regression of the melanoma, with no residualmelanoma cells and abundant infiltrating lymphocytesat the regressed melanoma site (Fig. 1). The postdosingbiopsy from the fourth patient with a clinical response(patient GA31) also showed no residual melanoma cells.This completely regressed melanoma included abundantmelanin pigment, both free and in macrophages, andextensive scar tissue without lymphocytic infiltration andwas therefore interpreted as showing late-stage regression
Figure 1. Immunohistochemicalanalysis of CD8þ cell infiltrationbefore and after tremelimumab in4 representative patients.Specimens of pre- (Pre-Tx) andposttreatment (Post-Tx)tremelimumab tumor biopsiesfrom 2 patients who progressed toa durable complete response aftertremelimumab treatment (GA18and GA29) are compared with 2representative samples of patientswho had disease progression aftertherapy (GA12 and GA14).Although there were no intactmelanoma cells evident in thepostdosing sample GA18, thehistologic changes supported thatthe biopsy derived from aregressing lesion with lymphocyticinfiltrates and the values for thiscase are considered as ITI.
GA18
10x
Pre-Tx biopsies Post-Tx biopsies
40X10x40X
GA12
GA14
10x
10x 40X
40X10x
10x40X
40X
10X 40X10X40X
GA29
Patients with clinical progression
Patients with clinical objective response
Intratumoral Infiltrates Following CTLA4 Blockade
www.aacrjournals.org Clin Cancer Res; 17(12) June 15, 2011 4105
Research. on July 15, 2018. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 10, 2011; DOI: 10.1158/1078-0432.CCR-11-0407
(Supplementary Fig. S2). Many postdosing samples frompatients with clinically progressive disease also showedsignificant lymphocytic ITI (Figs. 1 and 2; SupplementaryFig. S2). In 8 of 16 patients with disease progression, theincrease in CD8þ cell density was greater than the averageincrease for the whole series. In addition, 6 cases hadincreases in CD4þ cell density greater than the averageoverall series increase over the baseline biopsy. There wasno correlation between the density of ITI after tremelimu-mab treatment in responder and nonresponder patients orbetween patients alive 2 years or more after study initiationand patients who died from melanoma less than 2 yearsafter treatment initiation (Fig. 2).
Characterization of intratumoral infiltrates inpatients with postdosing increases
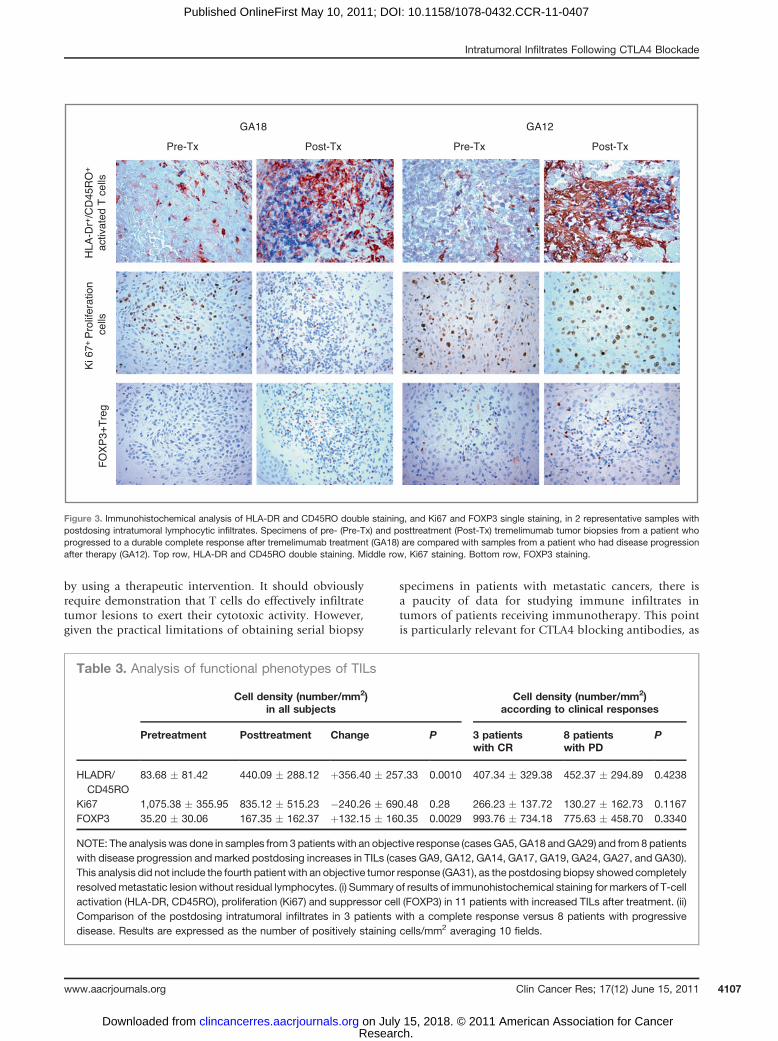
Because T-cell infiltrates increased in patients with andwithout a clinical response, we were interested in studyingwhether the functional characteristics of infiltrating T cellsdifferenced between these samples. HLA-DR is a surfacemarker of T-cell activation after exposure to CTLA4 block-ing antibodies (8, 9, 25), whereas CD45RO is a marker ofprior cognate antigen-exposed T cells. Together they markcells with a surface phenotype of T effector or T effectormemory cells (26). The combined analysis of HLA-DR/CD45RO staining showed a marked increase in double-positive cells in postdosing biopsies in all cases, irrespectiveof whether they had an objective response or not or were
alive beyond 2 years from study initiation (Fig. 3 andTable 3). Given the increase in the number of T cells inpostdosing biopsies, we stained the samples for the cellproliferation marker Ki67 to determine the extent of cellreplication within tumors. There was no change in thefrequency of Ki67-positive nuclei among lymphocytic infil-trates when postdosing biopsies were compared with base-line biopsies (Fig. 3 and Table 3). In our prior analysis oflesions regressing after tremelimumab treatment (22), wenoted an increase in FOXP3þ cells. The current studyconfirmed this finding. Three postdosing samples frompatients who had a durable complete response had amarked increase in FOXP3þ cells (Fig. 3). In the 8 non-responding tumors, there was an increase in FOXP3þ cellsin 5 tumors, 2 had no apparent change, and 1 had adecrease in FOXP3þ cells. When comparing the infiltratesbetween durably responding and nonresponding patients,the trend was in favor of higher infiltrates of FOXP3þ cellsin responding lesions (Table 3).
Discussion
An intratumoral infiltrate with activated T cells hasprognostic significance in patients with cancer, in whichprimary tumors with larger and more diffuse T-cell infil-trates displaying an effector functional phenotype haveimproved survival (26, 27). The major goal of tumorimmunotherapy is to induce such intratumoral infiltrates
Intratumoral CD8 infiltration
Pre Post
CD
8 ce
ll de
nsity
0
500
1,000
1,500
2,000
2,500
3,000
Paired t test P = 0.005
Intratumoral CD4 infiltration
Pre Post
CD
4 ce
ll de
nsity
0
500
1,000
1,500
2,000
2,500
3,000
Paired t test P = 0.018
Peritumoral CD8 infiltration
Pre Post
CD
8 ce
ll de
nsity
0
1,000
2,000
3,000
4,000
Paired t test P = 0.28
Clinical responseNo clinical response
Peritumoral CD4 infiltration
Pre Post
CD
4 ce
ll de
nsity
0
500
1,000
1,500
2,000
2,500
3,000
Paired t test P = 0.30
Clinical responseNo clinical response
Figure 2. Quantitativeimmunohistochemical analysis ofITI and PTI by CD4þ and CD8þ
cells. Results are expressed as theabsolute number of positivelystaining cells/mm2 averaged over10 fields. Open circles, patientswith an objective clinicalresponse. Closed triangles,patients with stable disease orprogression.
Huang et al.
Clin Cancer Res; 17(12) June 15, 2011 Clinical Cancer Research4106
Research. on July 15, 2018. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 10, 2011; DOI: 10.1158/1078-0432.CCR-11-0407
by using a therapeutic intervention. It should obviouslyrequire demonstration that T cells do effectively infiltratetumor lesions to exert their cytotoxic activity. However,given the practical limitations of obtaining serial biopsy
specimens in patients with metastatic cancers, there isa paucity of data for studying immune infiltrates intumors of patients receiving immunotherapy. This pointis particularly relevant for CTLA4 blocking antibodies, as
GA18
Pre-Tx Post-Tx
GA12
Pre-Tx Post-Tx
HLA
-Dr+
/CD
45R
O+
activ
ated
T c
ells
Ki 6
7+ P
rolif
erat
ion
cells
FO
XP
3+T
reg
Figure 3. Immunohistochemical analysis of HLA-DR and CD45RO double staining, and Ki67 and FOXP3 single staining, in 2 representative samples withpostdosing intratumoral lymphocytic infiltrates. Specimens of pre- (Pre-Tx) and posttreatment (Post-Tx) tremelimumab tumor biopsies from a patient whoprogressed to a durable complete response after tremelimumab treatment (GA18) are compared with samples from a patient who had disease progressionafter therapy (GA12). Top row, HLA-DR and CD45RO double staining. Middle row, Ki67 staining. Bottom row, FOXP3 staining.
Table 3. Analysis of functional phenotypes of TILs
Cell density (number/mm2)in all subjects
Cell density (number/mm2)according to clinical responses
Pretreatment Posttreatment Change P 3 patientswith CR
8 patientswith PD
P
HLADR/CD45RO
83.68 � 81.42 440.09 � 288.12 þ356.40 � 257.33 0.0010 407.34 � 329.38 452.37 � 294.89 0.4238
Ki67 1,075.38 � 355.95 835.12 � 515.23 �240.26 � 690.48 0.28 266.23 � 137.72 130.27 � 162.73 0.1167FOXP3 35.20 � 30.06 167.35 � 162.37 þ132.15 � 160.35 0.0029 993.76 � 734.18 775.63 � 458.70 0.3340
NOTE: The analysis was done in samples from 3 patients with an objective response (casesGA5, GA18 andGA29) and from 8 patientswith disease progression and marked postdosing increases in TILs (cases GA9, GA12, GA14, GA17, GA19, GA24, GA27, and GA30).This analysis did not include the fourth patient with an objective tumor response (GA31), as the postdosing biopsy showed completelyresolvedmetastatic lesion without residual lymphocytes. (i) Summary of results of immunohistochemical staining for markers of T-cellactivation (HLA-DR, CD45RO), proliferation (Ki67) and suppressor cell (FOXP3) in 11 patients with increased TILs after treatment. (ii)Comparison of the postdosing intratumoral infiltrates in 3 patients with a complete response versus 8 patients with progressivedisease. Results are expressed as the number of positively staining cells/mm2 averaging 10 fields.
Intratumoral Infiltrates Following CTLA4 Blockade
www.aacrjournals.org Clin Cancer Res; 17(12) June 15, 2011 4107
Research. on July 15, 2018. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 10, 2011; DOI: 10.1158/1078-0432.CCR-11-0407

preclinical data suggest that the mechanism of tumorregression should be mediated by the intratumoral accu-mulation of T cells, with little evidence of changes in thesystemic circulation. In the current studies, we analyzedtumor biopsy specimens from patients receiving anti-CTLA4 antibodies for the treatment of advanced mela-noma. The main goal was to compare baseline andpostdosing samples for the presence and functional char-acteristics of lymphocytic infiltrates. Contrary to conclu-sions based on prior experience with biopsies conductedlate in the treatment with tremelimumab (22), the currentstudies with biopsies at 1 to 2 months after the first doseof tremelimumab show sharp increases in tumor-infil-trating lymphocyte (TIL) in half of the patients whoshowed disease progression. Quantitative analysis ofthe T-cell infiltrates did not differentiate clinical respon-ders and nonresponders. Additional analyses to deter-mine whether there was a difference in the functionalityof these cells by using phenotypic markers also indicatethat the cellular infiltrate induced by tremelimumab doesnot differ significantly between clinical responders andnonclinical responders.
Postdosing intratumoral lymphocyte infiltrates could beas a result of cell mobilization and increased ITI induced byCTLA4 blockade, a possibility supported by some precli-nical models (19, 20, 28). Alternatively, the increase maybe due to active tumor antigen–specific lymphocyte pro-liferation with release of the so-called CTLA4 cell-cyclecheckpoint with G1 arrest (29–32). The dominant effectof CTLA4-inhibiting lymphocyte replication is evidencedby studies in CTLA4 knockout mice, which die within daysof postnatal antigen exposure due to massive lymphocyteproliferation and peripheral tissue infiltration (33, 34). Tostudy whether active lymphocyte replication within tumorscaused the postdosing increase in TILs, we compared pre-and postdosing samples for the nuclear expression of thecell replication marker Ki67. The data showed no suchchange, suggesting that tumors are not the site of lympho-cyte replication after CTLA4 blockade. This information iscomplemented by our recent experience in using wholebody imaging with positron emitting tomography (PET) tostudy tumor and lymphoid organs for a differential uptakeof radiolabeled PET traces in patients treated with treme-limumab (35). After treatment with tremelimumab, therewas increased 30-deoxy-3’-[18F]fluorothymidine ([18F]FLT)uptake in the spleen in most patients, which is reflective ofcell replication in this large lymphoid organ (35). The PETimaging data, together with the morphologic data from theanalysis of tumors presented herein, suggest that tremeli-mumab induces lymphocyte replication in lymphoidorgans that, in turn, leads to increased infiltration oftumors inmost patients, whether or not they have a clinicaltumor response. Because the changes in intratumoral T-cell
infiltrates are well beyond what can be detected in blood orin normal tissues, lymphocyte trafficking changes are themost likely explanation for the observed results in thisbiopsy series.
Studies analyzing immune parameters after CTLA4blockade have not yet provided a reproducible explanationof why clinical tumor responses are infrequent despiteevidence of immune activation in most patients. Multiplestudies reported lymphocyte activation in blood (7–10,12–16, 18, 36), and our current data confirm immuneactivation within tumors (17). It is difficult to reconcile thefrequent immune responses to CTLA4 blockade with infre-quent clinical evidence of tumor regression. Reportedmechanisms of tumor escape to tumor immunotherapyinclude downregulation of MHC and tumor antigen–pro-cessing and antigen-presenting machinery (37), or theeffects of oncogenes on sensitivity or resistance to apoptosisinduced by immune effector cells (38–40).
In conclusion, postdosing melanoma tumor biopsy spe-cimens from more than half of patients treated with theCTLA4 antagonistic antibody tremelimumab showincreased T-lymphocyte infiltrates. This increase is pro-nounced in patients who show an objective tumorresponse but is indistinguishable quantitatively and phe-notypically from infiltrates in half of the patients whoshowed disease progression. These data indicate that, inmost patients, therapeutic CTLA4 blockade induces thedesired immune stimulation resulting in T-cell infiltrationof tumors. Because only a minority have clinical responses,then differences on how tumors respond to the T cellinfiltrates is likely to be a major cause of resistance toanti-CTLA4 antibodies.
Disclosure of Potential Conflicts of Interest
J. Gomez-Navarro was an employee of Pfizer Inc. at the time of this work.A. Ribas received honoraria from Pfizer for the participation in advisoryboards during the conduct of this study.
Acknowledgments
We thank the manuscript review by Dr. Margaret Marshall from PfizerInc., New London, CT.
Grant Support
This work was funded in part by Pfizer Inc., the Melanoma ResearchFoundation, the NIH grant 2U54 CA119347, The Fred L. Hartley FamilyFoundation, the Jonsson Cancer Center Foundation and the Caltech-UCLAJoint Center for Translational Medicine (all to A. Ribas).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received February 25, 2011; revised April 19, 2011; accepted April 21,2011; published OnlineFirst May 10, 2011.
References1. Chen L. Co-inhibitory molecules of the B7-CD28 family in the control
of T-cell immunity. Nat Rev Immunol 2004;4:336–47.2. Chambers CA, Kuhns MS, Egen JG, Allison JP. CTLA-4-mediated
inhibition in regulation of T cell responses: mechanisms and
Huang et al.
Clin Cancer Res; 17(12) June 15, 2011 Clinical Cancer Research4108
Research. on July 15, 2018. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 10, 2011; DOI: 10.1158/1078-0432.CCR-11-0407
manipulation in tumor immunotherapy. Annu Rev Immunol2001;19:565–94.
3. Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, HaanenJB, et al. Improved survival with ipilimumab in patients with metastaticmelanoma. N Engl J Med 2010;363:711–23.
4. Kirkwood JM, Lorigan P, Hersey P, Hauschild A, Robert C,McDermottD, et al. Phase II trial of tremelimumab (CP-675,206) in patients withadvanced refractory or relapsed melanoma. Clin Cancer Res2010;16:1042–8.
5. O’Day SJ, Maio M, Chiarion-Sileni V, Gajewski TF, Pehamberger H,Bondarenko IN, et al. Efficacy and safety of ipilimumab monotherapyin patients with pretreated advanced melanoma: a multicenter single-arm phase II study. Ann Oncol 2010;21:1712–7.
6. Ribas A. Clinical development of the anti-CTLA-4 antibody tremeli-mumab. Semin Oncol 2010;37:450–4.
7. PhanGQ, Yang JC, Sherry RM, HwuP, Topalian SL, SchwartzentruberDJ, et al. Cancer regression and autoimmunity induced by cytotoxic Tlymphocyte-associated antigen 4 blockade in patients with metastaticmelanoma. Proc Natl Acad Sci U S A 2003;100:8372–7.
8. Maker AV, Attia P, Rosenberg SA. Analysis of the cellular mechanismof antitumor responses and autoimmunity in patients treated withCTLA-4 blockade. J Immunol 2005;175:7746–54.
9. Sanderson K, Scotland R, Lee P, Liu D, Groshen S, Snively J, et al.Autoimmunity in a phase I trial of a fully human anti-cytotoxic T-lymphocyte antigen-4 monoclonal antibody with multiple melanomapeptides and Montanide ISA 51 for patients with resected stages IIIand IV melanoma. J Clin Oncol 2005;23:741–50.
10. Comin-Anduix B, Lee Y, Jalil J, Algazi A, de la Rocha P, Camacho LH,et al. Detailed analysis of immunologic effects of the cytotoxic Tlymphocyte-associated antigen 4-blocking monoclonal antibody tre-melimumab in peripheral blood of patients with melanoma. J TranslMed 2008;6:22.
11. Ribas A, Glaspy JA, Lee Y, Dissette VB, Seja E, Vu HT, et al. Role ofdendritic cell phenotype, determinant spreading, and negative costi-mulatory blockade in dendritic cell-based melanoma immunotherapy.J Immunother 2004;27:354–67.
12. Klein O, Ebert LM, Nicholaou T, Browning J, Russell SE, ZuberM, et al.Melan-A-specific cytotoxic T cells are associated with tumor regres-sion and autoimmunity following treatment with anti-CTLA-4. ClinCancer Res 2009;15:2507–13.
13. Yuan J, Gnjatic S, Li H, Powel S, Gallardo HF, Ritter E, et al. CTLA-4blockade enhances polyfunctional NY-ESO-1 specific T cellresponses in metastatic melanoma patients with clinical benefit. ProcNatl Acad Sci U S A 2008;105:20410–5.
14. Fong L, Kwek SS, O’Brien S, Kavanagh B, McNeel DG, Weinberg V,et al. Potentiating endogenous antitumor immunity to prostate cancerthrough combination immunotherapy with CTLA4 blockade and GM-CSF. Cancer Res 2009;69:609–15.
15. Kavanagh B, O’Brien S, Lee D, Hou Y,Weinberg V, Rini B, et al. CTLA4blockade expands FoxP3þ regulatory and activated effector CD4þ Tcells in a dose-dependent fashion. Blood 2008;112:1175–83.
16. Hodi FS, Butler M, Oble DA, Seiden MV, Haluska FG, Kruse A, et al.Immunologic and clinical effects of antibody blockade of cytotoxic Tlymphocyte-associated antigen 4 in previously vaccinated cancerpatients. Proc Natl Acad Sci U S A 2008;105:3005–10.
17. Liakou CI, Kamat A, Tang DN, Chen H, Sun J, Troncoso P, et al. CTLA-4 blockade increases IFNgamma-producing CD4þICOShi cells to shiftthe ratio of effector to regulatory T cells in cancer patients. Proc NatlAcad Sci U S A 2008;105:14987–92.
18. Menard C, Ghiringhelli F, Roux S, Chaput N, Mateus C, Grohmann U,et al. Ctla-4 blockade confers lymphocyte resistance to regulatory T-cells in advanced melanoma: surrogate marker of efficacy oftremelimumab? Clin Cancer Res 2008;14:5242–9.
19. Schneider H, Downey J, Smith A, Zinselmeyer BH, Rush C, BrewerJM, et al. Reversal of the TCR stop signal by CTLA-4. Science2006;313:1972–5.
20. Paterson AM, Sharpe AH. Taming tissue-specific T cells: CTLA-4 reinsin self-reactive T cells. Nat Immunol 2010;11:109–11.
21. Hodi FS, MihmMC, Soiffer RJ, Haluska FG, Butler M, SeidenMV, et al.Biologic activity of cytotoxic T lymphocyte-associated antigen 4antibody blockade in previously vaccinated metastatic melanomaand ovarian carcinoma patients. Proc Natl Acad Sci U S A 2003;100:4712–7.
22. Ribas A, Comin-Anduix B, Economou JS, Donahue TR, de la Rocha P,Morris LF, et al. Intratumoral immune cell infiltrates, FoxP3, andindoleamine 2,3-dioxygenase in patients with melanoma undergoingCTLA4 blockade. Clin Cancer Res 2009;15:390–9.
23. CTEP Web site. Criteria NCT.The Revised Common Toxicity Criteria:Version 2.0. Bethesda, MD: Cancer Therapy Evaluation Program;1999.Available from: http://ctep.info.nih.gov.
24. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS,Rubinstein L, et al. New guidelines to evaluate the response totreatment in solid tumors [see comments]. J Natl Cancer Inst2000;92:205–16.
25. Comin-Anduix B, Gualberto A, Glaspy JA, Seja E, Ontiveros M,Reardon DL, et al. Definition of an immunologic response using themajor histocompatibility complex tetramer and enzyme-linked immu-nospot assays. Clin Cancer Res 2006;12:107–16.
26. Pages F, Berger A, Camus M, Sanchez-Cabo F, Costes A, Molidor R,et al. Effector memory T cells, early metastasis, and survival incolorectal cancer. N Engl J Med 2005;353:2654–66.
27. Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A,Mlecnik B, Lagorce-Pages C, et al. Type, density, and location of immune cells withinhuman colorectal tumors predict clinical outcome. Science 2006;313:1960–4.
28. Schneider H, Valk E, Leung R, Rudd CE. CTLA-4 activation ofphosphatidylinositol 3-kinase (PI 3-K) and protein kinase B (PKB/AKT) sustains T-cell anergy without cell death. PLoS One 2008;3:e3842.
29. Krummel MF, Allison JP. CTLA-4 engagement inhibits IL-2 accumula-tion and cell cycle progression upon activation of resting T cells. J ExpMed 1996;183:2533–40.
30. Marengere LE, Waterhouse P, Duncan GS, Mittrucker HW, Feng GS,Mak TW. Regulation of T cell receptor signaling by tyrosine phos-phatase SYP association with CTLA-4. Science 1996;272:1170–3.
31. Lee KM, Chuang E, Griffin M, Khattri R, Hong DK, Zhang W, et al.Molecular basis of T cell inactivation by CTLA-4. Science1998;282:2263–6.
32. Greenwald RJ, Boussiotis VA, Lorsbach RB, Abbas AK, Sharpe AH.CTLA-4 regulates induction of anergy in vivo. Immunity 2001;14:145–55.
33. Waterhouse P, Penninger JM, Timms E,WakehamA, Shahinian A, LeeKP, et al. Lymphoproliferative disorders with early lethality in micedeficient in Ctla-4. Science 1995;270:985–8.
34. Tivol EA, Borriello F, Schweitzer AN, LynchWP, Bluestone JA, SharpeAH. Loss of CTLA-4 leads to massive lymphoproliferation and fatalmultiorgan tissue destruction, revealing a critical negative regulatoryrole of CTLA-4. Immunity 1995;3:541–7.
35. Ribas A, Benz MR, Allen-Auerbach MS, Radu C, Chmielowski B, SejaE, et al. Imaging of CTLA4 blockade-induced cell replication with (18)F-FLT PET in patients with advanced melanoma treated with treme-limumab. J Nucl Med 2010;51:340–6.
36. Reuben JM, Lee BN, Li C, Gomez-Navarro J, Bozon VA, Parker CA,et al. Biologic and immunomodulatory events after CTLA-4 blockadewith ticilimumab in patients with advanced malignant melanoma.Cancer 2006;106:2437–44.
37. Ferrone S, Marincola FM. Loss of HLA class I antigens by melanomacells: molecular mechanisms, functional significance and clinicalrelevance. Immunol Today 1995;16:487–94.
38. Spaner DE. Amplifying cancer vaccine responses bymodifying patho-genic gene programs in tumor cells. J Leukoc Biol 2004;76:338–51.
39. Parsa AT, Waldron JS, Panner A, Crane CA, Parney IF, Barry JJ, et al.Loss of tumor suppressor PTEN function increases B7-H1 expressionand immunoresistance in glioma. Nat Med 2007;13:84–8.
40. Begley J, Ribas A. Targeted therapies to improve tumor immunother-apy. Clin Cancer Res 2008;14:4385–91.
Intratumoral Infiltrates Following CTLA4 Blockade
www.aacrjournals.org Clin Cancer Res; 17(12) June 15, 2011 4109
Research. on July 15, 2018. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 10, 2011; DOI: 10.1158/1078-0432.CCR-11-0407
2011;17:4101-4109. Published OnlineFirst May 10, 2011.Clin Cancer Res Rong Rong Huang, Jason Jalil, James S. Economou, et al. HumansActivated Lymphocytes Regardless of Clinical Responses in CTLA4 Blockade Induces Frequent Tumor Infiltration by
Updated version
10.1158/1078-0432.CCR-11-0407doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2011/06/17/1078-0432.CCR-11-0407.DC1Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/17/12/4101.full#ref-list-1
This article cites 39 articles, 22 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/17/12/4101.full#related-urls
This article has been cited by 16 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/17/12/4101To request permission to re-use all or part of this article, use this link
Research. on July 15, 2018. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst May 10, 2011; DOI: 10.1158/1078-0432.CCR-11-0407







