Download - Cranial meninges

CRANIAL MENINGES
Rajasri Manimaran
Group 2

Protection of the Brain
• The Skull
• Cranial meninges
• Cerebrospinal fluid
• Blood brain barrier
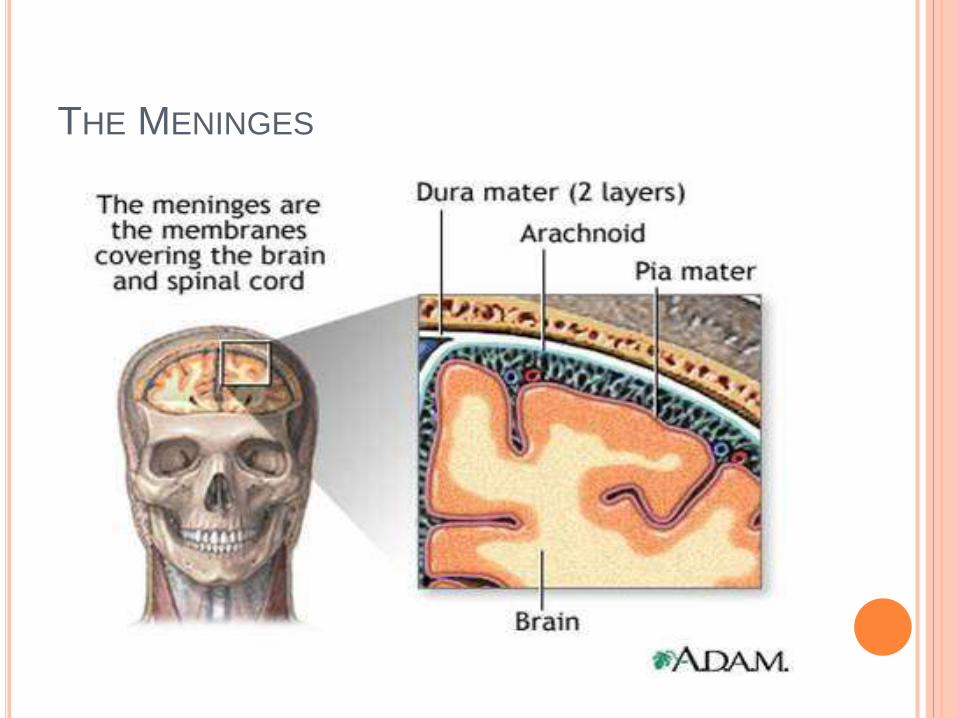
THE MENINGES
1. Dura Mater - Composed of two layers:a) Periosteal – outer layer, attaches to
bone.
b) Meningeal – inner layer, closer to brain.
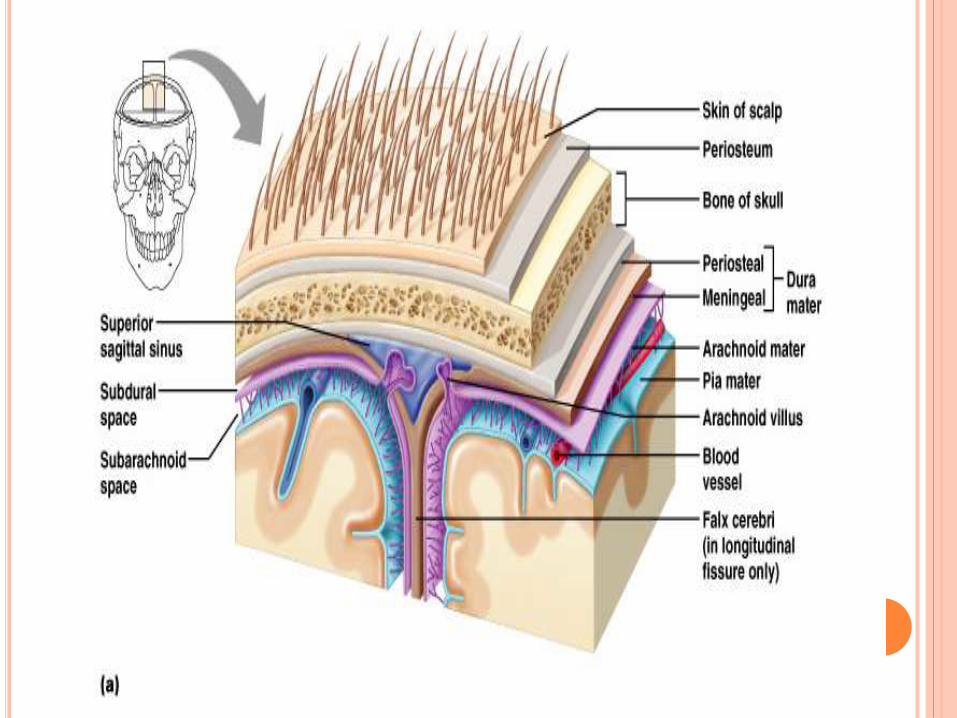
Cranial Meninges - 3 layer protective membrane
Two layers fused, except to enclose the dural sinuses
3. Pia Mater - delicate, follows convolutions.
2. Arachnoid Layer - ‘spider’ web like.
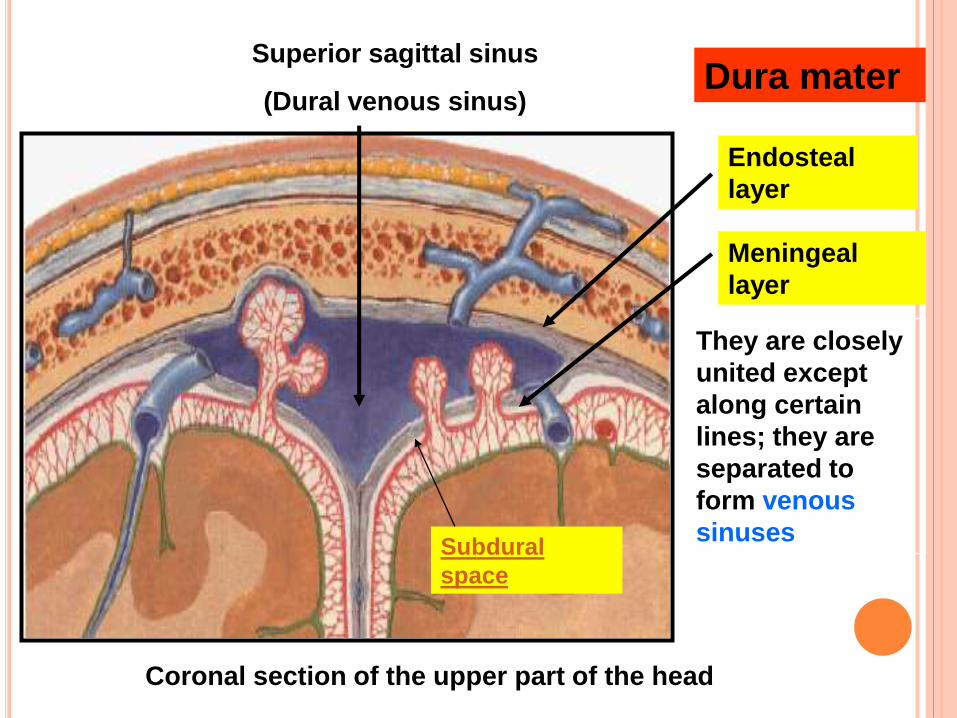
Coronal section of the upper part of the head
Endosteal
layer
Meningeal
layer
They are closely
united except
along certain
lines; they are
separated to
form venous
sinuses
Superior sagittal sinus
(Dural venous sinus)Dura mater
Subdural
space
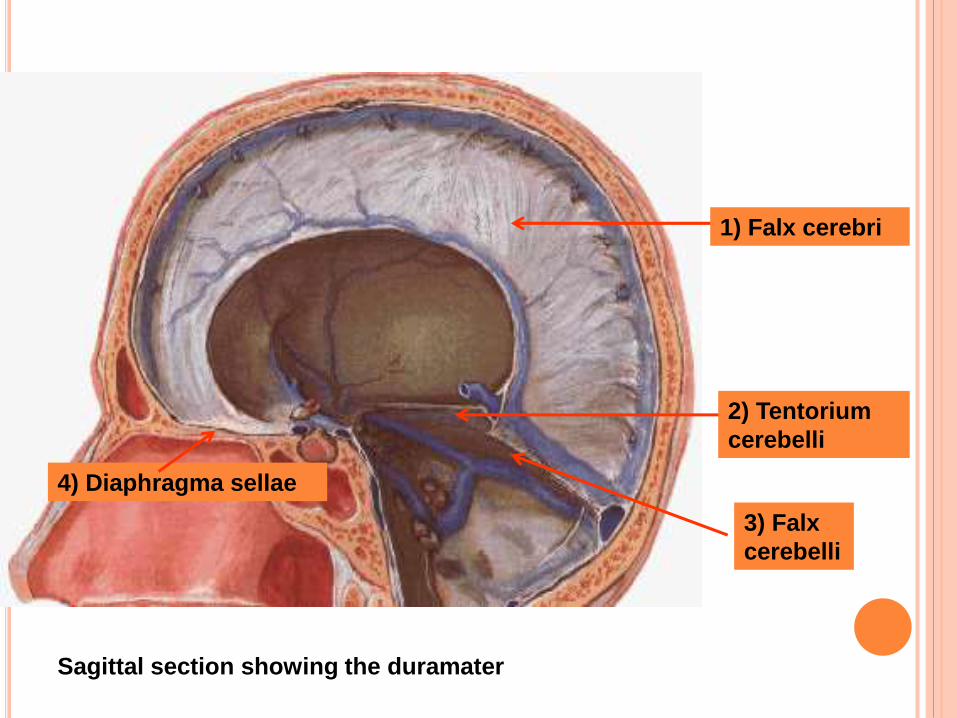
Sagittal section showing the duramater
1) Falx cerebri
2) Tentorium
cerebelli
3) Falx
cerebelli
4) Diaphragma sellae


DURAL NERVE SUPPLY
Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura.
The dura is sensitive to stretching, which produces the sensation of headache.
DURAL BLOOD SUPPLY
The middle meningeal artery supplies most of the blood for the dura mater, though the meningeal branches of the posterior and anterior ethmoidalartery also contribute.

ARACHNOID MATER
Subdural spacePotential space between dura and arachnoid
mater.
Cranial Meningeal Spaces Epidural space
Potential space superior to dura.
Subarachnoid spaceFilled with CSF
Contains the blood vessels supplying brain.
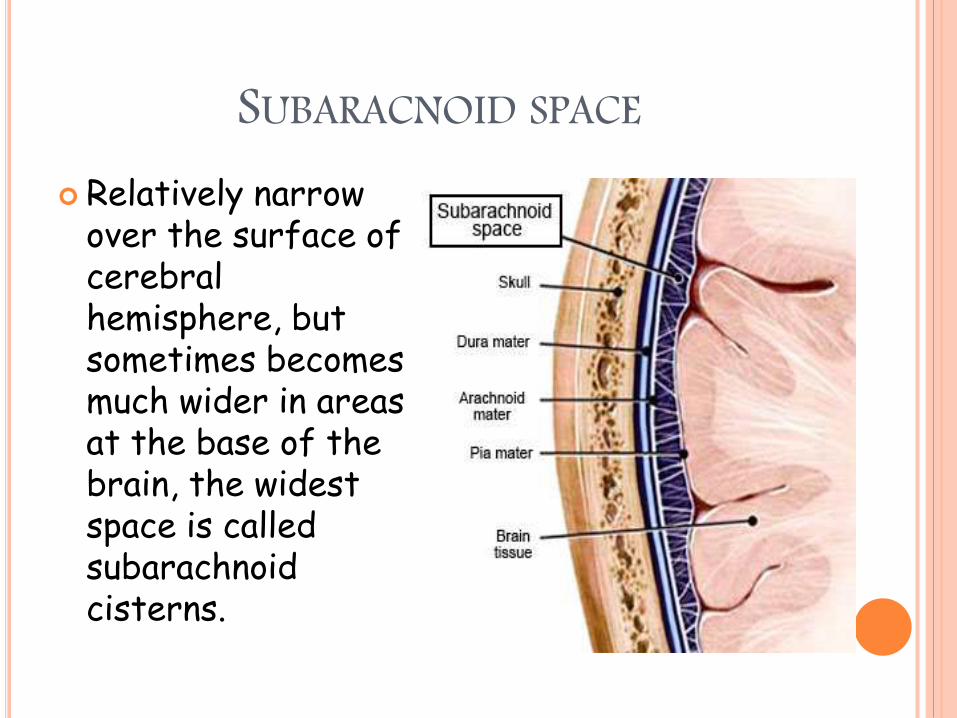
SUBARACNOID SPACE Relatively narrow
over the surface of cerebral hemisphere, but sometimes becomes much wider in areas at the base of the brain, the widest space is called subarachnoid cisterns.

Median sagittal section to show the subarachnoid cisterns
& circulation of CSF
Superior
cistern
Interpeduncular
cistern
Cerebellomedullary
cistern
Chiasmatic
cistern
Pontine
cistern
PIA MATER
Pia mater functions to cover and protect the central nervous system (CNS), to protect the blood vessels and enclose the venous sinuses near the CNS, to contain the cerebrospinal fluid (CSF) and to form partitions with the skull.
The CSF, pia mater, and other layers of the meninges work together as a protection device for the brain, with the CSF often referred to as the fourth layer of the meninges.

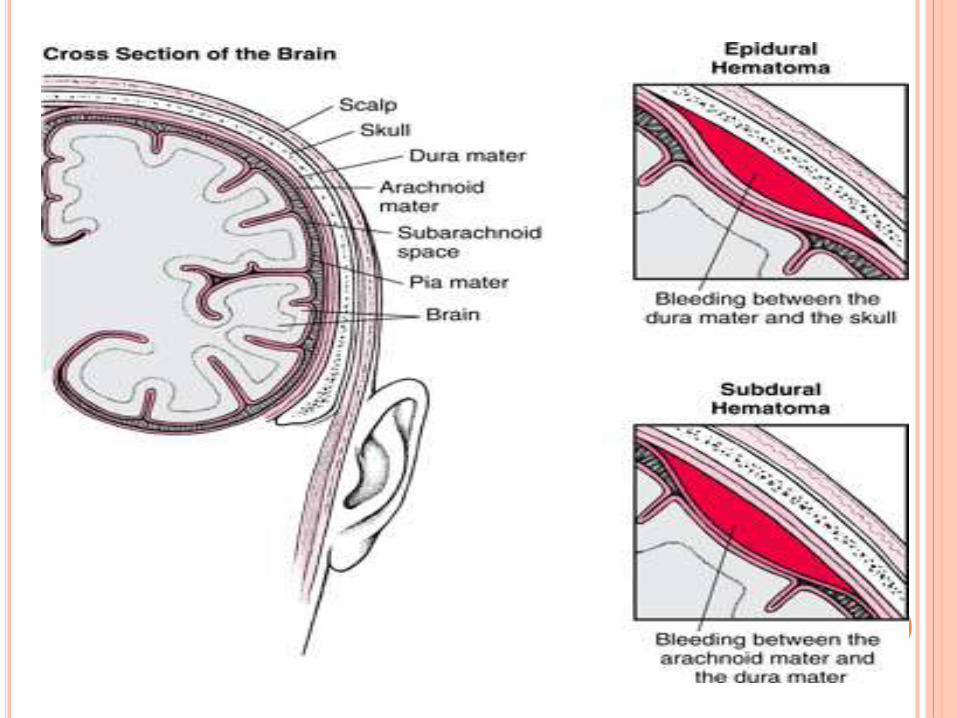
PATHOLOGYThere are three types of hemorrhage involving the
meninges: An epidural hematoma arise after an accident or
spontaneously A subdural hematoma is a hematoma (collection
of blood) located in a separation of the arachnoid from the dura mater. The small veins that connect the dura mater and the arachnoid are torn, usually during an accident, and blood leaks into this area
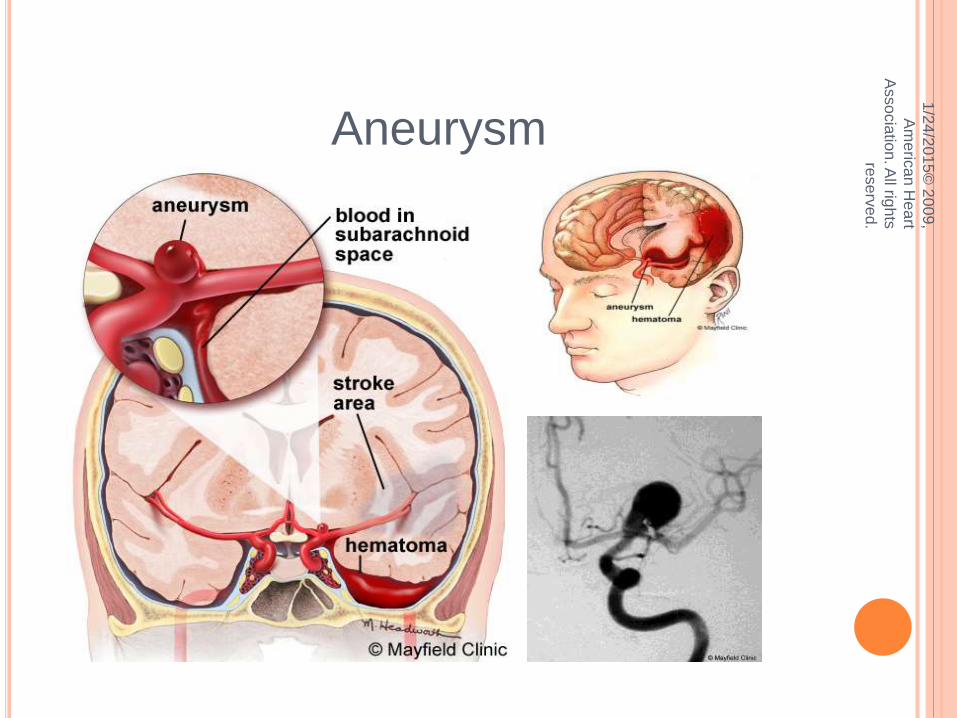
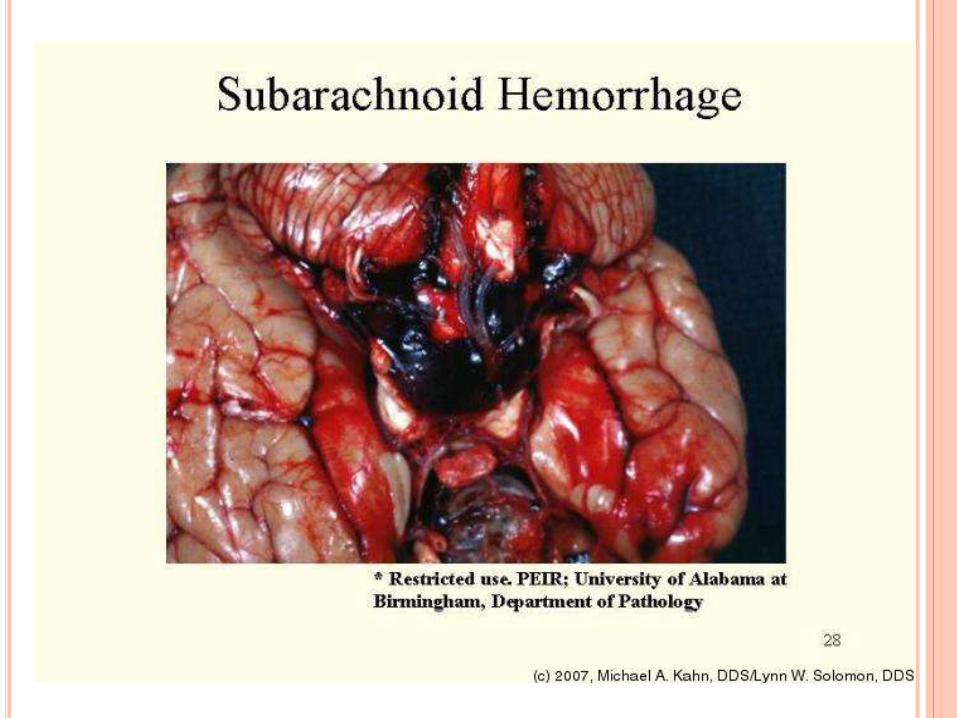
A subarachnoid hemorrhage is acute bleeding under the arachnoid; it may occur spontaneously or as a result of trauma.

Other medical conditions that affect the meninges include meningitis (usually from fungal, bacterial, or viral infection) and meningiomas that arise from the meninges, or from meningealcarcinomatoses (tumors) that form elsewhere in the body and metastasize to the meninges.
CRANIAL VENOUS SINUSES
The dural venous sinuses (also called dural sinuses, cerebral sinuses, or cranial sinuses) are venous channels found between layers of dura mater in the brain.
They receive blood from internal and external veins of the brain, receive cerebrospinal fluid (CSF) from the subarachnoid space, and ultimately empty into the internal jugular vein.

Name Drains to
Inferior sagittal sinus Straight sinus
Superior sagittal sinusTypically becomes right transverse
sinus or confluence of sinuses
Straight sinusTypically becomes left transverse sinus
or confluence of sinuses
Occipital sinus Confluence of sinuses
Confluence of sinuses Right and Left transverse sinuses
Sphenoparietal sinuses Cavernous sinuses
Cavernous sinuses Superior and inferior petrosal sinuses
Superior petrosal sinus Transverse sinuses
Transverse sinuses Sigmoid sinus
Inferior petrosal sinus Sigmoid sinus
Sigmoid sinuses Internal jugular vein
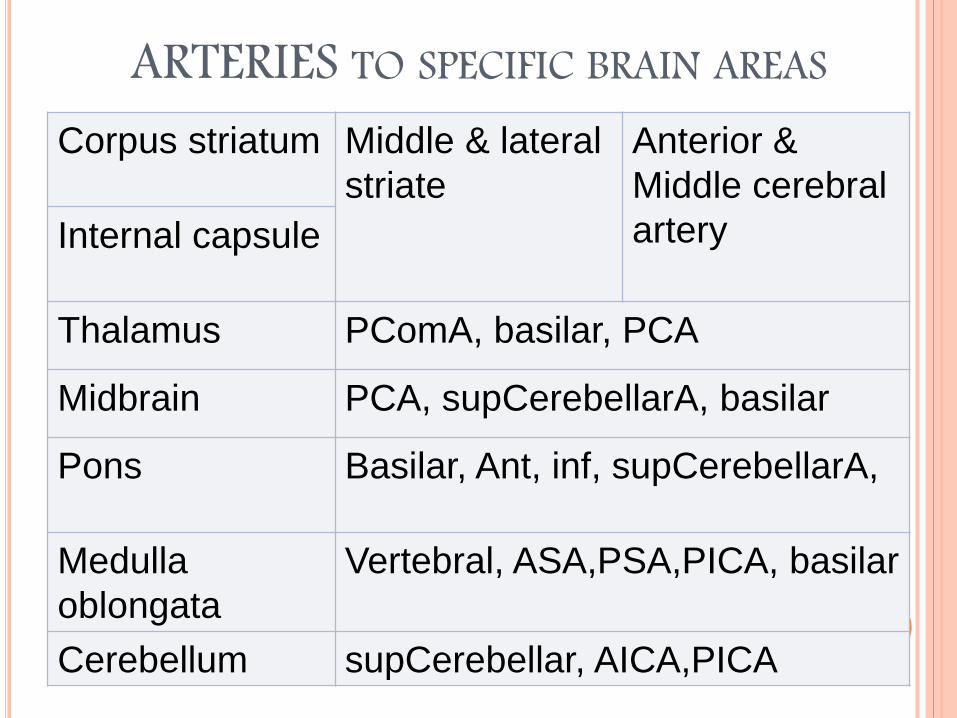
ARTERIES TO SPECIFIC BRAIN AREASCorpus striatum Middle & lateral
striate
Anterior &
Middle cerebral
arteryInternal capsule
Thalamus PComA, basilar, PCA
Midbrain PCA, supCerebellarA, basilar
Pons Basilar, Ant, inf, supCerebellarA,
Medulla
oblongata
Vertebral, ASA,PSA,PICA, basilar
Cerebellum supCerebellar, AICA,PICA
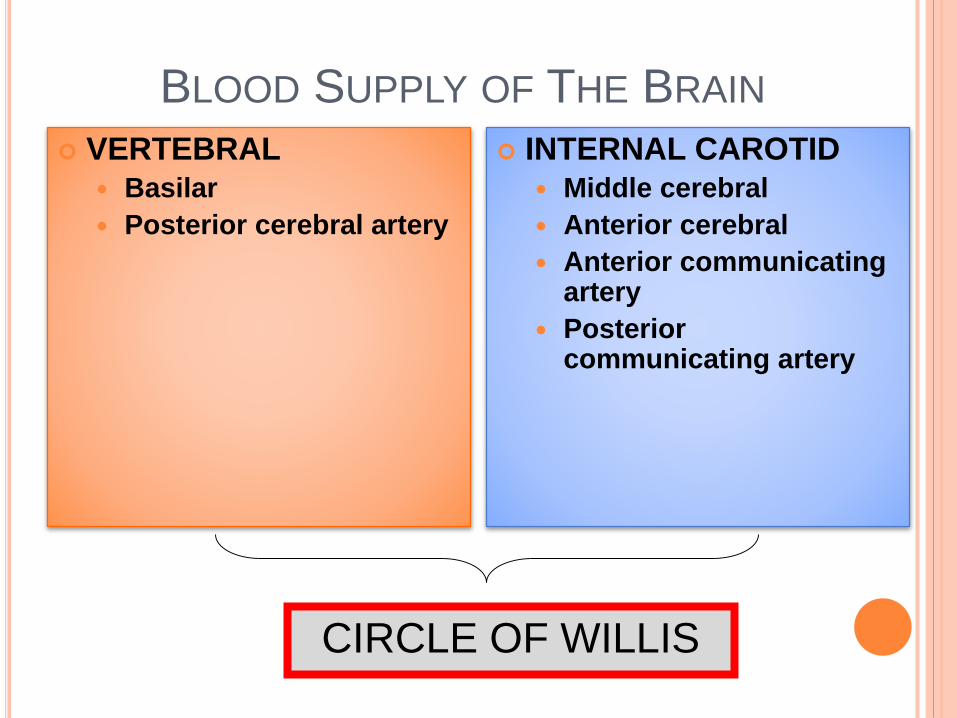
BLOOD SUPPLY OF THE BRAIN
VERTEBRAL
Basilar
Posterior cerebral artery
INTERNAL CAROTID
Middle cerebral
Anterior cerebral
Anterior communicating artery
Posterior communicating artery
CIRCLE OF WILLIS


Subarachnoid hemorrhage
1/2
4/2
015
© 2
00
9,
Am
eric
an
Hea
rt
Asso
cia
tion. A
ll righ
ts
rese
rve
d.
Aneurysm

SYMPTOMS
Headache (sudden onset, greater severity)
Nausea and vomitting
Loss or impairment of consciousness (may progress to coma and death)
Confusion and irritability
Meningial irritation and nuchal rigidity (stiff neck)
Focal neurological deficits (may indicate site of lesions).

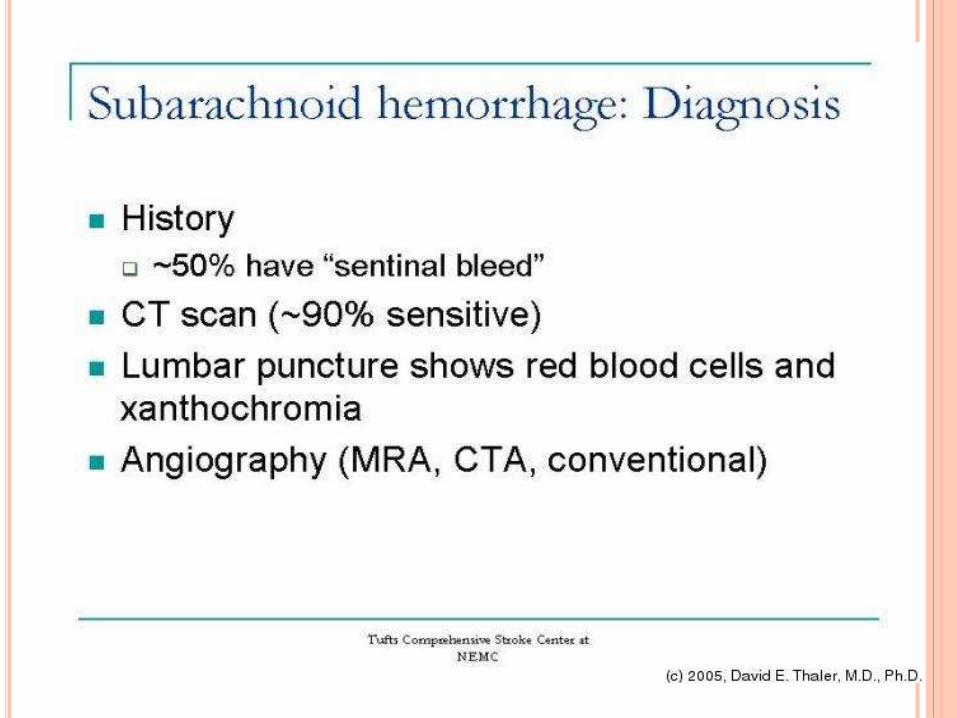
DIFFERENTIAL DIAGNOSIS
Meningitis
Migraine
Intracerebral hemorrhage
Ischemic stroke


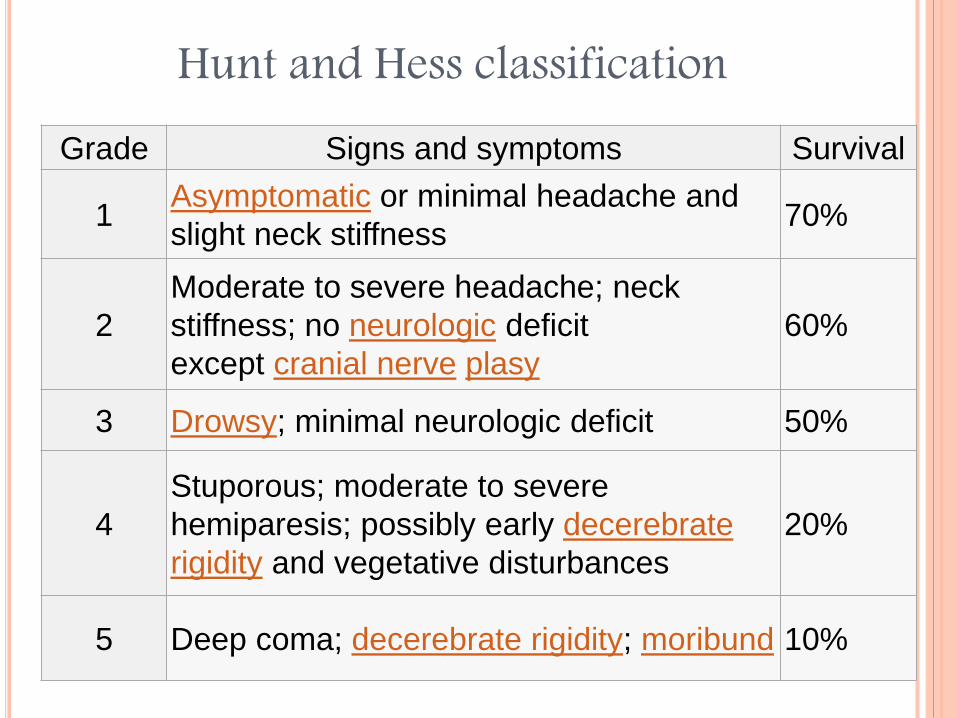
Grade Signs and symptoms Survival
1Asymptomatic or minimal headache and
slight neck stiffness70%
2
Moderate to severe headache; neck
stiffness; no neurologic deficit
except cranial nerve plasy
60%
3 Drowsy; minimal neurologic deficit 50%
4
Stuporous; moderate to severe
hemiparesis; possibly early decerebrate
rigidity and vegetative disturbances
20%
5 Deep coma; decerebrate rigidity; moribund 10%
Hunt and Hess classification
TREATMENT
Stabilizing patient.
Prevention of rebleeding by obliterating the bleeding source.
prevention of a phenomenon known as vasospasm and,
prevention and treatment of complications.
PREVENTING RE-BLEEDING
Up to 14% of SAH patients may experience re-bleeding within 2 hours of the initial hemorrhage
Re-bleeding was more common in those with a systolic blood pressure >160mm Hg
Anti-fibrinolytic therapy may reduce re-bleeding but has not been shown to improve outcomes
1/2
4/2
015
© 2
00
9,
Am
eric
an
Hea
rt
Asso
cia
tion. A
ll righ
ts
rese
rve
d.

SURGICAL AND ENDOVASCULARMANAGEMENT OF SAH
Surgery – clip aneurysm baseEndovascular – coilingShould be performed within 2 days of
hemorrhage.
1/2
4/2
015
© 2
00
9,
Am
eric
an
Hea
rt
Asso
cia
tion. A
ll righ
ts
rese
rve
d.

1/2
4/2
015
© 2
00
9,
Am
eric
an
Hea
rt
Asso
cia
tion. A
ll righ
ts
rese
rve
d.
Clipping

LEFT IMAGE ARROW -ANGIO WITH LARGE ANEURYSM
RIGHT IMAGE ARROW – ANGIO SHOWING ANEURYSM POST CLIPPING
1/2
4/2
015
© 2
00
9,
Am
eric
an
Hea
rt
Asso
cia
tion. A
ll righ
ts
rese
rve
d.
Angio Image Courtsey: The University of Texas Health Science Center at San Antonio – Department of Neurosurgery

SURGICAL AND ENDOVASCULARMANAGEMENT OF SAH
Combined morbidity and mortality was significantly greater in surgically treated patients than in those treated with endovascular techniques (30.9% vs. 23.5%; absolute risk reduction 7.4%)
During the short follow-up period, the re-bleeding rate for coiling was 2.9% versus 0.9% for surgery
There have been no randomized comparisons of coiling versus clipping for unruptured aneurysms
1/2
4/2
015
© 2
00
9,
Am
eric
an
Hea
rt
Asso
cia
tion. A
ll righ
ts
rese
rve
d.

1/2
4/2
015
© 2
00
9,
Am
eric
an
Hea
rt
Asso
cia
tion. A
ll righ
ts
rese
rve
d.
Coiling

COIL SYSTEM EMBOLIZATION: IMMEDIATE RESULT 1
/24
/2015
© 2
00
9,
Am
eric
an
Hea
rt
Asso
cia
tion. A
ll righ
ts
rese
rve
d.
Angio showing large ICA aneurysmSame aneurysm - Post GDC Coiling
Angio Image Courtsey: The University of Texas Health Science Center at San Antonio – Department of Neurosurgery


PREVENTING VASOSPASM
The use of calcium channel blockers, thought to be able to prevent the spasm of blood vessels by preventing calcium from entering smooth muscle cells, has been proposed for the prevention of vasospasm.
The oral calcium channel blocker nimodipine improves outcome if administered between the fourth and twenty-first day after the hemorrhage.

PREVENTING OTHER COMPLICATIONS
If medication don’t help, then angiography may be attempted to identify the sites of vasospasms and administer vasodilator medication (drugs that relax the blood vessel wall) directly into the artery.
Angioplasty (opening the constricted area with a balloon) may also be performed.
SUMMARY AND CONCLUSIONS
The current standard of practice calls for microsurgical clipping or endovascular coiling of the aneurysm neck whenever possible
Treatment morbidity is determined by numerous factors, including patient, aneurysm, and institutional factors
1/2
4/2
015
© 2
00
9,
Am
eric
an
Hea
rt
Asso
cia
tion. A
ll righ
ts
rese
rve
d.
SUMMARY AND CONCLUSIONS
Favorable outcomes are more likely in institutions that treat high volumes of patients with SAH, in institutions that offer endovascular services, and in selected patients whose aneurysms are coiled rather than clipped
Optimal treatment requires availability of both experienced cerebrovascular surgeons and endovascular surgeons working in a collaborative effort to evaluate each case of SAH
1/2
4/2
015
© 2
00
9,
Am
eric
an
Hea
rt
Asso
cia
tion. A
ll righ
ts
rese
rve
d.








