
Visya – www.cliniquevision.com
M. ASSOULINE, L. BESSEDE Centre IénaVision, PARIS. Clinique de la Vision, PARIS. [email protected] [email protected]
Comparison of four multifocal implants to compensate for presbyopia during cataract surgery INTRODUCTION There are a number of different IOL models available for cataract patients that may differ in:
material (hydrophilic or hydrophobic acrylic, silicone, PMMA);
design (plate haptics or loop haptics);
optical properties (aspherical implants slightly improve night vision in younger subjects);
optional yellow filter (designed to protect the retina and the macula from the toxic effects of UV rays and blue light).
In practice, the visual performance of these implants depends mainly on their optical qualities (standard monofocal, aspherical, toric, multifocal). Recent advances in multifocal implant designs have revolutionized cataract surgery, offering patients a truly spectacle-independent postoperative life. Not only will they have the opportunity to have perfect distance vision, which is a typical feature of standard monofocal implants, but also excellent near vision at 35 cm (reading), and with the most recent implants, satisfactory intermediate vision at 70 cm (computer work, reading sheet music, using smartphone/tablet, etc.). However, an informal survey has revealed that while experts in the field and surgeons who implant more than 200 multifocal IOLs per year have adopted the latest-generation multifocal implants for 50 to 70% of their patients, most cataract surgeons, particularly those not performing LASIK surgeries on a regular basis, are very reluctant to use these implants routinely. Instead, they implant them sparingly and only in patients who specifically request these IOLs. This explains why multifocal implants still account for less than 6% of the French market. This figure is difficult to explain considering that 80% of patients have no contraindication to these implants and in light of their functional advantages in terms of quality of life.
Modern cataract surgery is a refractive surgery and must expand to include presbyopia correction:
for patients who have knowledge or experience with refractive laser surgery or intraocular cataract lenses;
for surgeons who regard it as a more sophisticated and rewarding personal accomplishment, as well as an opportunity to provide a remarkable medical service to patients who place their trust in surgeons;
and to match the competing options, since developing and adopting innovations to new implants is faster.
"Expert" surgeons who use multifocal implants widely in their practice:
have changed their approach to cataract surgery to a refractive one (no post-operative glasses, using toric implants, monovision, and relaxing incisions);
have realized the benefits that multifocal implants have on the medical service provided to patients;
offer the surgery to younger patients, from 60 years of age for instance, but without upper age limit (up to 85 years old);
use multifocal implants to develop their surgical practice, thus gaining a competitive advantage by improving the medical services they provide;
Patients are more and more demanding:
if they've heard of presbyopia or astigmatism correction as part of cataract surgery (media, internet, neighbors, friends and family, or in the waiting room);
if they don't understand why they still have to wear eyeglasses or contact lenses permanently after surgery while their neighbors or friends and family don't have to after their operations;
and are also very grateful to surgeons for taking the time to choose the best visual correction for their specific needs.
THE SWITCH TO MULTIFOCAL IMPLANTS – WHY AND HOW? Multifocal implants are a better way to correct:
presbyopia;
astigmatism if a toric version is available;
patients' refractive expectations, whether stated explicitly or not. They also improve the functional results of cataract surgery:
better uncorrected acuity;
enhanced visual autonomy;
better quality of life. Finally, they improve patients' impression of the quality of medical service provided:
satisfaction because of personalized care;
appreciation of the surgeon's expertise and the results;
boost the surgeon's brand and act as a recruiting agent.
STRICTER QUALITY PROCEDURES APPLY TO MULTIFOCAL IMPLANTS Switching to and prescribing multifocal implants requires a stricter approach to quality, especially when it comes to your training and communicating with patients. All steps of a successful "conversion" to multifocal implants are equally important because the promises made to patients limit the surgeons' margin of error.
Understand the optics and PhysIOLogy of vision relating to multifocal implants thoroughly.
Be convinced of the benefits of these implants, both for your patients and yourself.
Talk to practitioners who are used to multifocal implants.
Attend one of their pre- and post-operative consultations.
Have a detailed discussion with patients who have benefited from multifocal implants as well as patients who have not.
Learn about the real costs of post-operative prescription eyeglasses.
Integrate information on multifocal implants into the standard information given to patients.
Systematically discuss multifocal implants with each patient.
Highlight the advantages in terms of effectiveness and comfort.
Reassure patients that the implants are perfectly safe.
Mention the rare contraindications, screened during pre-operative tests.
Before the operation, do not evade the postoperative quality of vision, the need for learning (neuro-adaptation) and the potential need for adjustment (less than 0.5% of cases) for perfect refractive results.
Be clear on financial questions.
Offer additional information before the patient decides.
Give patients time to consider the options and make up their own mind.
Apply the necessary pre- and post-operative protocols properly.
Support patients after surgery for as long as is necessary for perfectly satisfactory results.
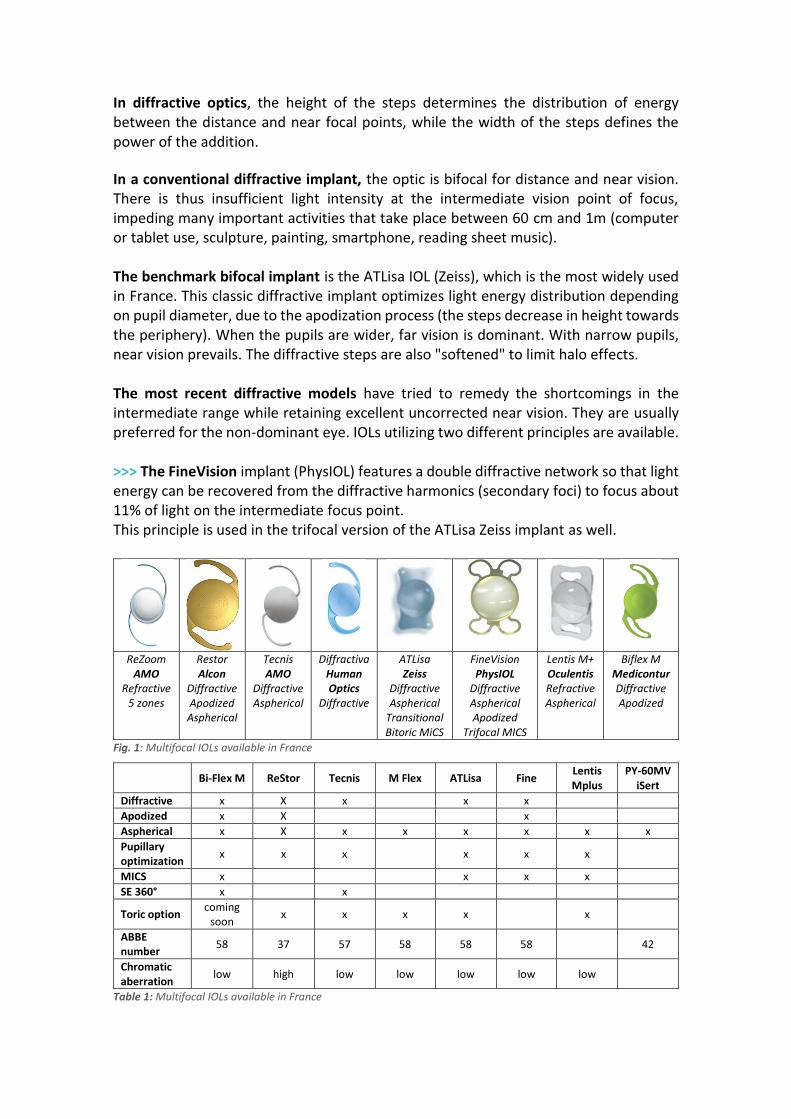
AVAILABLE MULTIFOCAL IMPLANTS Multifocal implants can be divided into 5 groups based on the design of their optic (Fig 1):
single diffractive bifocal (apodized or not): e.g. ATLisa Bifocal (Zeiss);
double diffractive (trifocal): e.g. FineVision (PhysIOL);
diffractive/refractive (improved depth of field): e.g. Bi-Flex 677M (Medicontur);
concentric multizone refractive: e.g. ReZoom (AMO);
sectorial aspherical refractive: e.g. Lentis Mplus (Oculentis / Topcon).
Diffractive multifocal implants include a microstructure of concentric steps similar to Fresnel lenses used in flexible flat magnifying lenses or in lighthouse lenses.
In diffractive optics, the height of the steps determines the distribution of energy between the distance and near focal points, while the width of the steps defines the power of the addition.
In a conventional diffractive implant, the optic is bifocal for distance and near vision. There is thus insufficient light intensity at the intermediate vision point of focus, impeding many important activities that take place between 60 cm and 1m (computer or tablet use, sculpture, painting, smartphone, reading sheet music). The benchmark bifocal implant is the ATLisa IOL (Zeiss), which is the most widely used in France. This classic diffractive implant optimizes light energy distribution depending on pupil diameter, due to the apodization process (the steps decrease in height towards the periphery). When the pupils are wider, far vision is dominant. With narrow pupils, near vision prevails. The diffractive steps are also "softened" to limit halo effects. The most recent diffractive models have tried to remedy the shortcomings in the intermediate range while retaining excellent uncorrected near vision. They are usually preferred for the non-dominant eye. IOLs utilizing two different principles are available. >>> The FineVision implant (PhysIOL) features a double diffractive network so that light energy can be recovered from the diffractive harmonics (secondary foci) to focus about 11% of light on the intermediate focus point. This principle is used in the trifocal version of the ATLisa Zeiss implant as well.
ReZoom AMO
Refractive 5 zones
Restor Alcon
Diffractive Apodized
Aspherical
Tecnis AMO
Diffractive Aspherical
Diffractiva Human Optics
Diffractive
ATLisa Zeiss
Diffractive Aspherical
Transitional Bitoric MiCS
FineVision PhysIOL
Diffractive Aspherical Apodized
Trifocal MICS
Lentis M+ Oculentis Refractive Aspherical
Biflex M Medicontur Diffractive Apodized
Fig. 1: Multifocal IOLs available in France
Bi-Flex M ReStor Tecnis M Flex ATLisa Fine Lentis Mplus
PY-60MV iSert
Diffractive x X x x x
Apodized x X x
Aspherical x X x x x x x x
Pupillary optimization
x x x x x x
MICS x x x x
SE 360° x x
Toric option coming
soon x x x x x
ABBE number
58 37 57 58 58 58 42
Chromatic aberration
low high low low low low low
Table 1: Multifocal IOLs available in France
>>> The Bi-Flex 677M implant (Medicontur) features a diffractive/refractive system. The manufacturing method has been improved to reach the nanometer scale in precision, thus each diffractive step has an aspherical curve modification to increase depth of field (PAD technology). Refractive multifocal implants feature several juxtaposed concentric optical zones of different optical power. The most recent model (Lentis Mplus) is aspherical. The optic includes an addition zone with a curvature concentric to the main optic for far vision, but with a segmented form (lower section). The large optic zone dedicated to distance vision (more than two thirds of the surface depending on pupil diameter) preserves distance vision in all light conditions. The aspherical transition, comparable to that of the presbyLasik, improves intermediate vision at 65 cm while maintaining appropriate near vision. These models are preferably chosen for the dominant eye. These systems sometimes cause some minor inconveniences that do not result in significant visual limitations and which usually disappear in one to three months.
The second, "phantom" image must be neutralized through cerebral adaptation. This may require a learning period of a few days to a few months, depending on the patient (neuroadaptation).
In case of bright light (e.g. car headlights at night) implanted patients may see halos of light.
Near vision requires sufficient lighting for small characters. Certain multifocal implants (Lentis Mplus, Bi-Flex M) are also available in toric versions, but must be ordered well in advance (4 to 6 weeks). Multifocal implants usually are not fully reimbursed by health insurance. For the most recent multifocal and/or toric implants, patients or their supplementary insurance companies need to pay in part. WHAT CAN WE EXPECT FROM THE LATEST MULTIFOCAL IMPLANTS? We compared three recent multifocal implants (designed to compensate intermediate vision more efficiently) to a benchmark bifocal implant in a consecutive series of 874 eyes, operated by a single surgeon. All of the functional results were measured by the same orthoptist, independent of the surgeon. The specifications of an ideal implant include several characteristics making it possible to compare the various models available on the market. We analyzed the following parameters: >>> Injectability
size of the incision;
unfolding;
spontaneous positioning of the optic;
ease of unfolding of loops and placement in the capsular bag;
centration: spontaneous and/or guided by the surgeon;
damage to implant during injection;
compatibility with sulcus fixation method in the event of capsular rupture.
>>> Vision
Corrected visual acuity;
Uncorrected visual acuity (distance at 3 m, intermediate at 65cm and near at 35cm);
Subjective monocular and binocular defocus curves (visual acuity measured at 3m with the best distance correction and with the addition of lenses from +2.00 D to -3.50 D in increments of 0.50 D);
Spectacle independence;
Refractive stability;
Change to binocular balance (angle kappa);
Posterior capsular opacification (survival analysis of Nd:YAG laser rate). >>> Patient satisfaction
Quality of vision (halos, dysphotopsia, glare, night vision);
Preference (implantation of different models in each eye);
Quality of life. All of the implants can be injected without difficulty through a 1.8 mm incision using the disposable Medicell device. Implants with plate haptics (ATLisa and Lentis) are easier to control during the injection process: in particular, they are noticeably less likely to be pinched by the plunger than implants with haptics (Medicontur and FineVision). Even though loop haptics are sometimes partially damaged, this does not affect the implantation negatively due to the IOL design. These problems persist occasionally, despite thorough, visual and audial (snap closure) checking of the haptics positioning in the cartridge. All of the implants (except Medicontur) can be implanted directly into the capsular bag without additional manipulation other than a gentle anteroposterior push on the center of the optic. Because of its 90° haptic loop design, the Medicontur implant requires a half-turn rotation around its axis to release the leading haptic and guide it towards the capsular equator. This inconvenience is justified by a significantly increased equatorial contact angle (90° for a 9 mm capsular bag, compared to 40 to 70° for conventional implants), in order to prevent posterior capsular opacification.
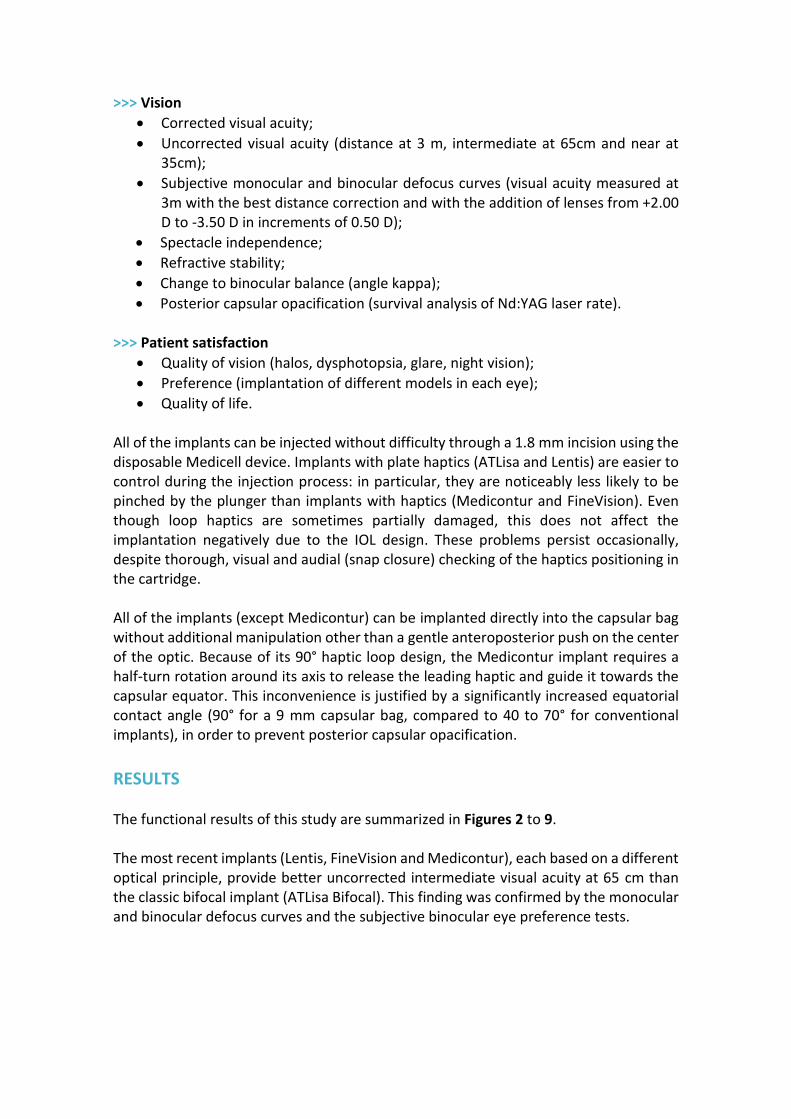
RESULTS The functional results of this study are summarized in Figures 2 to 9. The most recent implants (Lentis, FineVision and Medicontur), each based on a different optical principle, provide better uncorrected intermediate visual acuity at 65 cm than the classic bifocal implant (ATLisa Bifocal). This finding was confirmed by the monocular and binocular defocus curves and the subjective binocular eye preference tests.
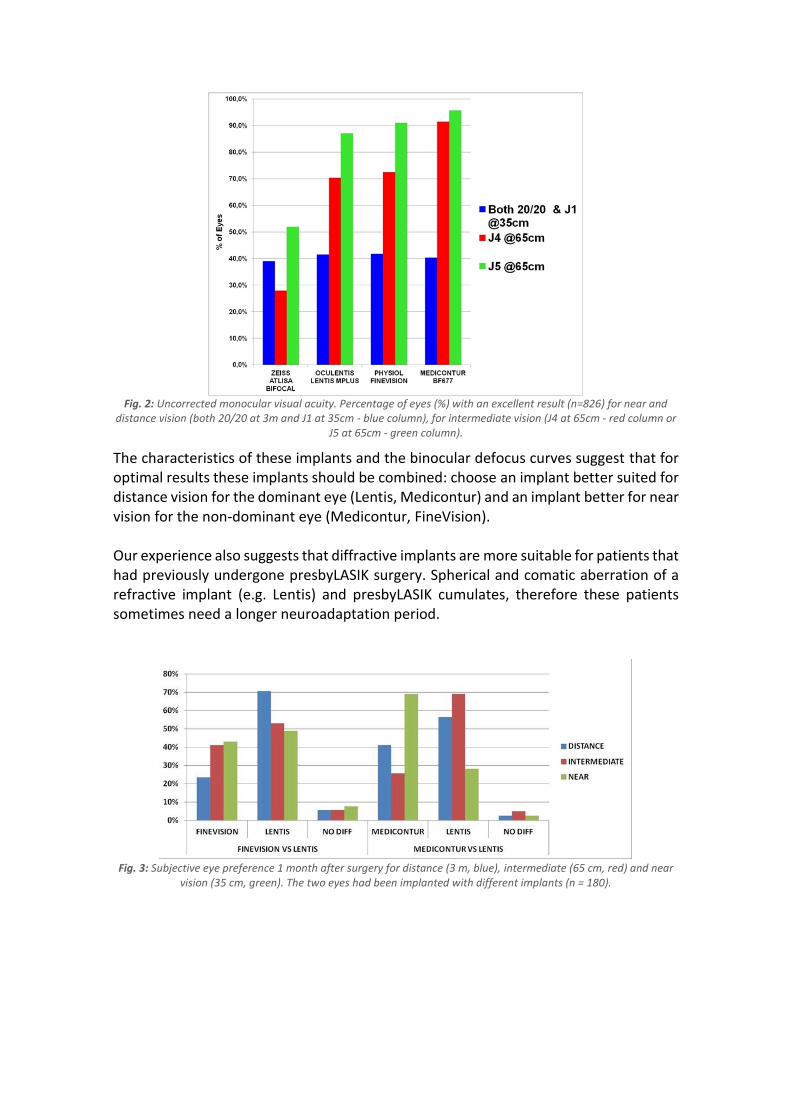
Fig. 2: Uncorrected monocular visual acuity. Percentage of eyes (%) with an excellent result (n=826) for near and
distance vision (both 20/20 at 3m and J1 at 35cm - blue column), for intermediate vision (J4 at 65cm - red column or J5 at 65cm - green column).
The characteristics of these implants and the binocular defocus curves suggest that for optimal results these implants should be combined: choose an implant better suited for distance vision for the dominant eye (Lentis, Medicontur) and an implant better for near vision for the non-dominant eye (Medicontur, FineVision). Our experience also suggests that diffractive implants are more suitable for patients that had previously undergone presbyLASIK surgery. Spherical and comatic aberration of a refractive implant (e.g. Lentis) and presbyLASIK cumulates, therefore these patients sometimes need a longer neuroadaptation period.
Fig. 3: Subjective eye preference 1 month after surgery for distance (3 m, blue), intermediate (65 cm, red) and near
vision (35 cm, green). The two eyes had been implanted with different implants (n = 180).
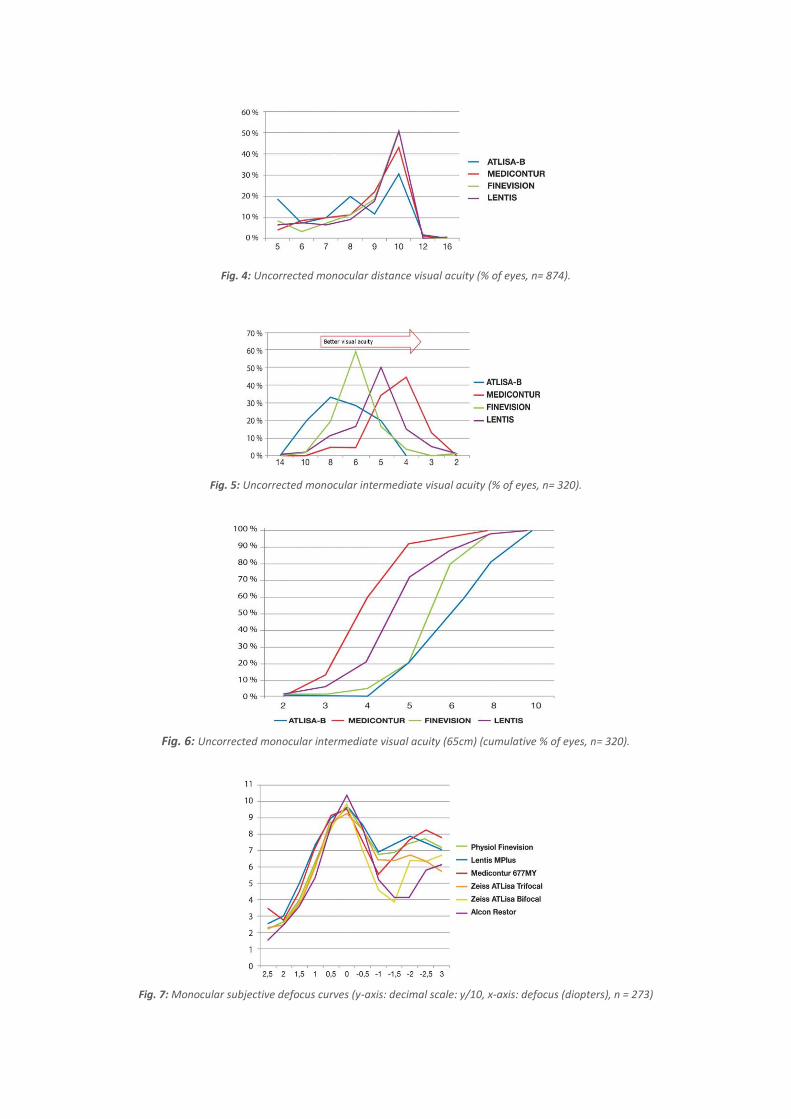
Fig. 4: Uncorrected monocular distance visual acuity (% of eyes, n= 874).
Fig. 5: Uncorrected monocular intermediate visual acuity (% of eyes, n= 320).
Fig. 6: Uncorrected monocular intermediate visual acuity (65cm) (cumulative % of eyes, n= 320).
Fig. 7: Monocular subjective defocus curves (y-axis: decimal scale: y/10, x-axis: defocus (diopters), n = 273)
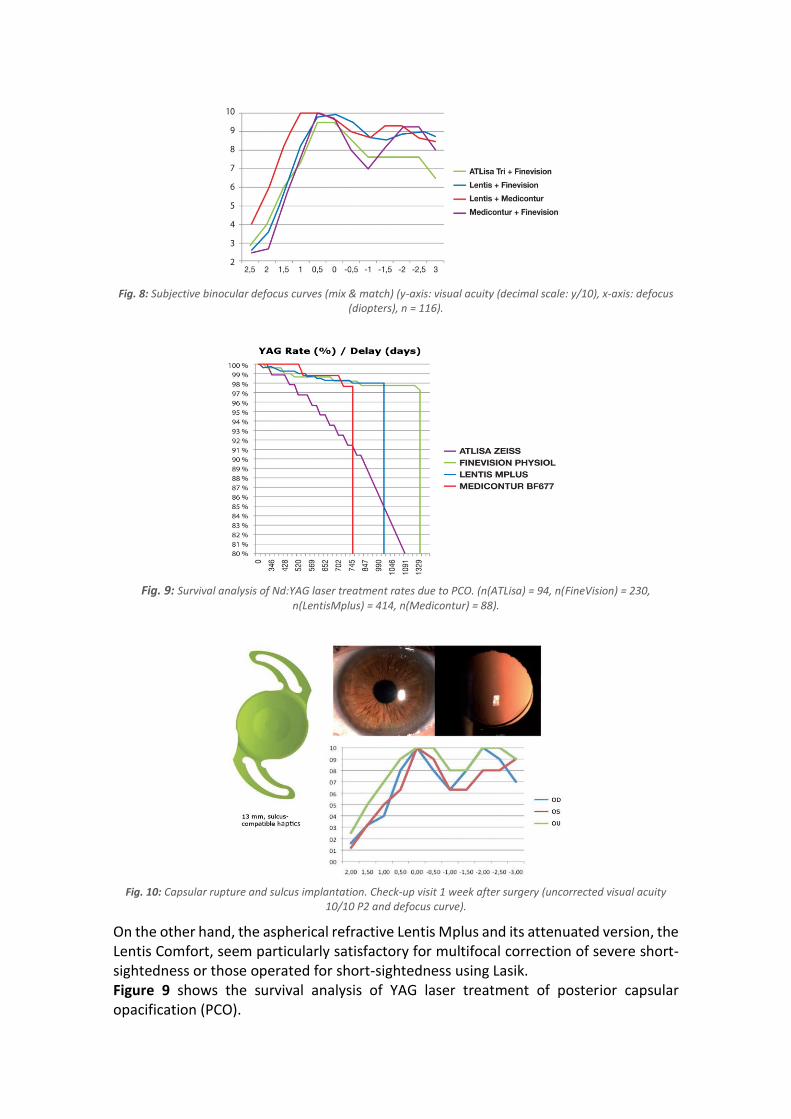
Fig. 8: Subjective binocular defocus curves (mix & match) (y-axis: visual acuity (decimal scale: y/10), x-axis: defocus
(diopters), n = 116).
Fig. 9: Survival analysis of Nd:YAG laser treatment rates due to PCO. (n(ATLisa) = 94, n(FineVision) = 230,
n(LentisMplus) = 414, n(Medicontur) = 88).
Fig. 10: Capsular rupture and sulcus implantation. Check-up visit 1 week after surgery (uncorrected visual acuity
10/10 P2 and defocus curve).
On the other hand, the aspherical refractive Lentis Mplus and its attenuated version, the Lentis Comfort, seem particularly satisfactory for multifocal correction of severe short-sightedness or those operated for short-sightedness using Lasik. Figure 9 shows the survival analysis of YAG laser treatment of posterior capsular opacification (PCO).
The three most recent models, all made from hydrophilic acrylic materials, also provide far better PCO prevention because of their better adapted geometry: 5° haptic angulation and 360° square edge in the case of the FineVision and Medicontur IOLs; and large overall diameter and significant volume in the case of Lentis Mplus.
COMPLICATIONS WITH THE MULTIFOCAL IMPLANTS IN THIS SERIES In connection with the cataract surgery of 874 eyes of this series during which multifocal IOLs were implanted, we recorded the following non-serious complications: >>> Around twenty cases of implant damage during injection, usually to the haptic (partial rupture) and less frequently to the optic (microrupture) of the implants (all models), with no effect on stability or visual function. >>> Five capsular ruptures. We were able to implant the planned multifocal IOL in all cases: in the capsular bag in 3 cases (ATLisa bifocal implant, FineVision implant, Lentis implant) and in the sulcus in 2 cases (Lentis and Medicontur implants). The Lentis Mplus implant placed in the sulcus moved slightly off center but this did not cause significant visual problems. Figure 10 shows that the Medicontur implant, which has a 13 mm large overall diameter, is perfectly centered, with normal functional result one week after surgery and stable 3 months after the operation. >>> 8 cases of clinically significant macular edema (none after capsular rupture), resolved by a single topic treatment, except for one case of recurring edema that required an injection of Ozurdex for over a year in a young patient operated for a traumatic cataract with zonular dehiscence (final visual acuity 7/10) and 4 cases of epimacular membrane requiring vitreoretinal surgery with good functional recovery. >>> 4 cases of significant subjective dissatisfaction lasting more than 3 months. One of these patients had a non-systematic, diffuse visual field deficit. Further tests revealed a cerebral pathology of hypertensive origin that was missed during the preoperative OCT examination. This patient's subjective satisfaction notably increased after 6 months, however, he had an uncorrected monocular visual acuity of 8/10 P4 on each side. >>> 4 cases of explantation due to the refractive error of the implant (2 cases after refractive surgery, and 2 cases due to distribution error) replaced with a multifocal implant. >>> 12 cases of complementary refractive treatment using limbal relaxing incisions to complement astigmatism correction.
>>> 2 cases of therapeutic photoablation by excimer laser for treating asymptomatic Cogan's dystrophy interfering with vision, which were documented photographically. >>> No cases of supplementary refractive treatment with Lasik or excimer laser. No cases requested the implant be exchanged or explanted.
CONCLUSION No ophthalmic surgeon, even a non-refractive surgeon, would prescribe eyeglasses or contact lenses without indicating the addition or the cylinder. It is thus difficult to understand why spherical intraocular implants are still the norm these days instead of being the exception... The objective and subjective results show that the latest multifocal implants consistently and safely improve patients’ visual autonomy and quality of life. This should be encouraging enough for ophthalmic surgeons to change their routines. Study presented in part at the ESCRS Annual Meeting (London, September 2014) and the ESCRS Winter Symposium (Istanbul, February 2015). The author is a consultant for Medicontur and PhysIOL.







