Combination of Verapamil and Beta Blockers in Systemic Hypertension
HENRY DARGIE, MB, JOHN CLELAND, MB, IAIN FINDLAY, MB, GORDON MURRAY, PhD, and GORDON MclNNES, MD
The efficacy and safety of verapamil and proprano- lol were examined in 14 hypertensive patients (mean age 51.2, range 30 to 65) in a double-blind, randomized, crossover study of verapamil, 360 mg, propranolol, 240 mg, these 2 formulations in combi- nation and placebo, each given for 4 weeks. Supine blood pressure, heart rate, atrioventricular conduc- tion (PR interval) and left ventricular function were measured. All treatments reduced diastolic blood pressure (mean f standard deviation) (p <O.OOl): placebo to 106.6 f 6.1 mm Hg; propranolol to 93.8 f 7.7; verapamil to 89.8 f 7.8; the combination to 84.1 f 6.1, but the effect of the combination was significantly greater than that of either drug alone (p <0.05). Heart rate at rest (placebo, 80.2 f 12.2 beats/min) was reduced by propranolol (63.3 f 9.4, p <O.OOl), but not by verapamil (79.0 f 8.9).
However, the addition of verapamil to propranolol led to a further reduction in heart rate (56.9 f 8.4, p <0.005). PR interval was prolonged significantly by the combination (185.5 f 35.3 ms) when com- pared with placebo (154.0 f 22.7); propranolol (159.1 f 21.2) and verapamil (165.5 f 32.4) (p <0.005 for each). The active drugs increased end- diastolic dimension and end-systolic dimension. For each variable, the effect of the combination was statistically significant (p <O.Ol). Fractional short- ening was not altered significantly by any of the treatments. Thus verapamil plus propranolol is a very effective antihypertensive combination but heart rate, atrioventricular conduction and left ven- tricular function may be affected adversely, necessi- tating careful monitoring of therapy.
(Am J Cardiol 1986;57:8OD-82D)
T he potential for calcium-channel blockers in the treatment of hypertension was recognized by Flecken- stein when he described the basic pharmacology of these compounds in 1977.l At that time fl blockers were being recognized clinically as effective antihyperten- sive agents and now are established not only as a first line treatment in moderate hypertension, but also as the basis for more complex regimens in patients resis- tant to monotherapy with either diuretics or ,8 blockers. Recently such calcium-channel blockers as verapamil and nifedipine have been shown to decrease blood pressure in patients with mild and moderate hyperten- sion2s3 with a potency approximately similar to that of /3 blockers. This similar effect on blood pressure occurs for different reasons. While the antihypertensive ef-
From the Department of Cardiology, Western Infirmary, De- partment of Statistics, The University, Glasgow, and University Department of Medicine, Gardiner Institute, Western Infirma- ry, Glasgow, United Kingdom.
Address for reprints: Henry Dargie, MB, Department of Cardiology, Western Infirmary, Glasgow Gil 6NT, United Kingdom.
feet of /3 blockers is still incompletely understood, the principal effect of the calcium-channel blocker is to reduce peripheral vascular resistance. Because this is the underlying hemodynamic abnormality in most pa- tients with essential hypertension, the mode of action of calcium-channel blockers in decreasing blood pres- sure seems attractive; moreover, the possibility of a beneficial drug interaction with /3 blockers would be an additional advantage. The combination of calcium- channel blockers such as verapamil with p blockers could have implications not only for blood pressure, but also for cardiac conduction and left ventricu- lar (LV) function. We investigated the effects of vera- pamil and propranolol alone and in combination on blood pressure, heart rate, LV function and cardiac conduction.
Methods Fourteen patients [9 women and 5 men, mean age
51.6, range 30 to 651, in whom diastolic blood pressure was 95 to 110 mm Hg on single drug therapy, took part in a double-blind, randomized, crossover study. All other drug treatments were discontinued before entry
SOD
into the study. The treatments were verapamil, 120 mg The calcium-channel blockers are a beterogenous 3 times a day, propranolol, 80 mg 3 times a day, verapa- group of compounds; verapamil, unlike nifedipine, mil, 120 mg 3 times a day plus propranolol, 80 mg 3 has additional properties in delaying conduction in the times a day, and placebo; each was given for 4 weeks. atrioventricular node,7 which is the basis for its SUC- On completion of each treatment, blood pressure at cessful use in supraventricular tachycardias. This rest and heart rate (supine and standing) were mea- property is shared by p blockers and in our study both sured using a Bosomat II automatic blood pressure propranolol and verapamil prolonged atrioventricular recorder (Bosch and Sohn). Heart rate and cardiac nodal conduction as inferred from the increase in PR rhythm were assessed by resting electrocardiogram interval. This effect was greater with the combination from which the PR interval was calculated and by 24- than either drug alone but no significant pauses or hour ambulatory electrocardiographic monitoring us- episodes of more serious conduction disturbances oc- ing the Oxford Medilog I recorder and the Reynolds curred. We would regard these observations as the medical “pathfinder” analyzer. LV internal dimen- expected consequence of the clinical pharmacologic sions were recorded using M-mode echocardiography profiles of verapamil and propranolol. Their clinical from which fractional shortening was calculated. The significance in patients with normal cardiac function results of the treatments were compared using repeat- as in this group of hypertensive patients is uncertain. ed measures analysis of variance and paired t tests. In patients with impaired IX function or disturbed
Results cardiac conduction, however, these effects could be of concern.
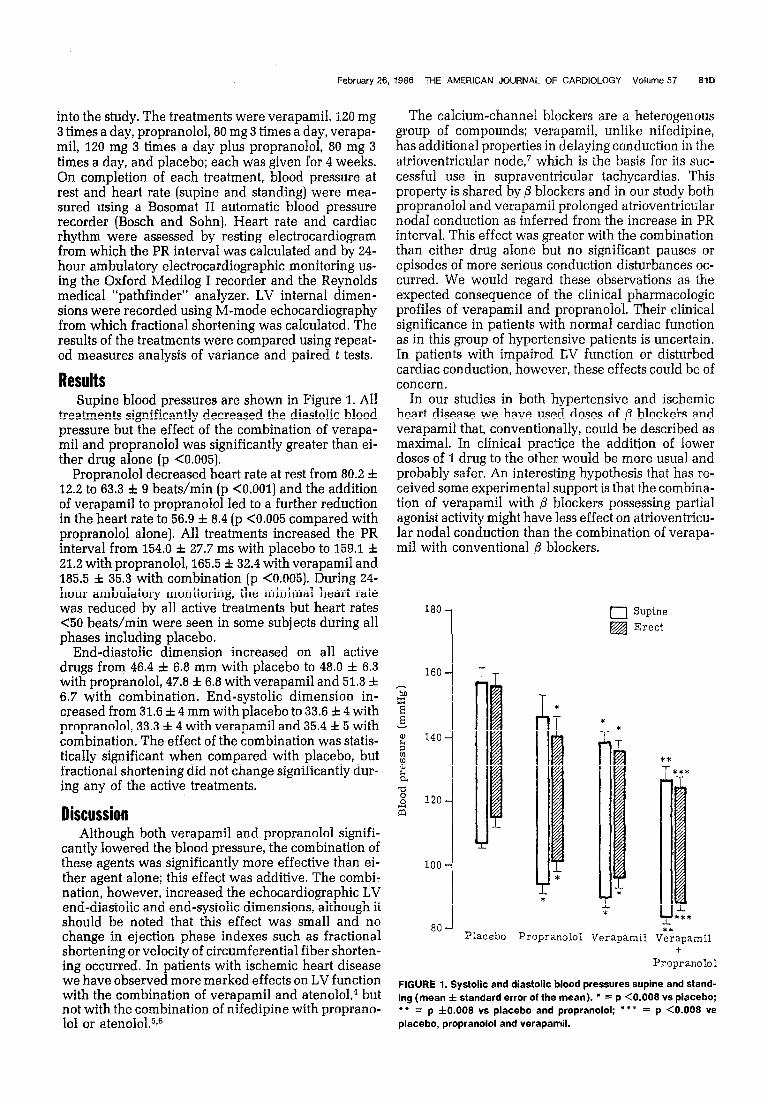
Supine blood pressures are shown in Figure 1. All In our studies in both hypertensive and ischemic treatments significantly decreased the diastolic blood heart disease we have used doses of @ blockers and pressure but the effect of the combination of verapa- verapamil that, conventionally, could be described as mil and propranolol was significantly greater than ei- maximal. In clinical practice the addition of lower ther drug alone (p <O.O05). doses of 1 drug to the other would be more usual and
Propranolol decreased heart rate at rest from 80.2 & probably safer. An interesting hypothesis that has re- 12.2 to 63.3 f 9 beats/min (p <O.OOl] and the addition ceived some experimental support is that the combina- of verapamil to propranolol led to a further reduction tion of verapamil with @ blockers possessing partial in the heart rate to 56.9 f 8.4 (p <0.005 compared with agonist activity might have less effect on atrioventricu- propranolol alone]. All treatments increased the PR lar nodal conduction than the combination of verapa- interval from 154.0 f 27.7 ms with placebo to 159.1 f mil with conventional p blockers. 21.2 with propranolol, 165.5 f 32.4 with verapamil and 185.5 f 35.3 with combination (p <0.005). During 24- hour ambulatory monitoring, the minimal heart rate was reduced by all active treatments but heart rates 180 <5O beats/min were seen in some subjects during all
0 Supine
phases including placebo. &j Erect
End-diastolic dimension increased on all active drugs from 46.4 f 6.8 mm with placebo to 48.0 f 6.3 with propranolol, 47.8 f 6.8 with verapamil and 51.3 f
160 J 6.7 with combination. End-systolic dimension in- xi
X creased from 31.6 f 4 mm with placebo to 33.6 f 4 with propranolol, 33.3 f 4 with verapamil and 35.4 & 5 with i 1; * * combination. The effect of the combination was statis- it 140
tically significant when compared with placebo, but 2 fractional shortening did not change significantly dur- d ***
ing any of the active treatments. a -0 8 120
Discussion iii
Although both verapamil and propranolol signifi- cantly lowered the blood pressure, the combination of f these agents was significantly more effective than ei- 100 ther agent alone; this effect was additive. The combi- * nation, however, increased the echocardiographic LV ; * end-diastolic and end-systolic dimensions, although it should be noted that this effect was small and no A***
change in ejection phase indexes such as fractional 80
Placebo Propranolol Verapamil V*eFapamil shortening or velocity of circumferential fiber shorten- +
ing occurred. In patients with ischemic heart disease Propranolol
we have observed more marked effects on LV function with the combination of verapamil and atenoloL4 but
FIGURE 1. Systolic and diastolic blood pressures supine and stand-
not with the combination of nifedipine with proprano- ing (mean f standard error of the mean). l = p <0.008 vs placebo; l * = p f0.008 vs placebo and propranolol; **+ = p <0.008 vs
February 26, 1986 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 57 810
101 or atenolol.5T6 placebo, propranolol and verapamil.

82D A SYMPOSIUM: CALCIUM ANTAGONISTS IN HYPERTENSION-FOCUS ON VERAPAMIL
In summary, the combination of propranolol and verapamil isvery effective in lowering blood pressure, but careful monitoring must be advised until the safety of this combination has been assessed in a large pa- tient population. The theoretical advantage of using a ,6 blocker with partial agonist activity should not be implemented clinically until proven in suitably de- signed clinical trials.
References 1. Fleckenstein A. Specific pharmacology of calcium in myocardium cardiac pacemakers and vascular smooth muscle. Annu Rev Pharmacol Toxic01
1977;17:149-166. 2. Lewis GJR, Morley KD, Lewis BM, Bones PJ. The treatment of hyperten- sion with verapamil. NZ Med J 1978;87:352-354. 3. Harris L, Dargie HJ, Lynch PG, Bulpitt CJ. Krikler DM. Blood pressure and heart rate in patients with ischaemic heart disease receiving nifedipine and propranoloi. Br Med J 1982;284:1148-1151. 4. Findlay IN, Gillen G, Elliott AT. Dargie HJ. The treatment of ongina pectoria with calcium channel and p-blockers: efficacy and effect on cardiac function. JACC 1984;3:482. 5. Dargie HJ, Lynch PC, Krikler DM, Harris L, Krikler S. Nifedipine and propranolol in angina pectoris: a beneficial drug interaction. Am J Med 1981;71:676-682. 6. Findlay IN, Dargie HJ. The effects of nifedipine, atenolof and that combi- nation on left ventricular function. Postgrad Med 1 1983;59:suppf 2:70-73. 7. Rowland E. Evans T, Krikler DM. Effect of nifedipine on otrioventriculor conduction as compared with verapamil. Br Heart f 1979;42:124-127.







