Colorectal Cancer Services Multidisciplinary Team William Harvey Hospital
Operational Policy Documentation
September 2010
Prepared by Mr Pradeep S Basnyat
Status:
Expiry Date:
Version Number:
Publication Date: September 2010
DOCUMENTATION
Document Location
The master electronic version of this document is kept by Mr Pradeep S Basnyat at William Harvey Hospital. Hardcopies are available on appropriate inpatient and outpatient areas. It is also available from Cancer Service Nurse (CNS) Ruth Burns and Maggie Moore from 1
st October 2010. This policy
will be circulated to all members of the Colorectal MDT. Access to the document is also possible via the Trust’s Intranet/website
Revision History
Date Version Status Author Summary of Changes
2008 Mr Nagesh Rao
2010 Mr Pradeep s Basnyat Changed according to new colorectal measures
Approvals Record
This document has been agreed by all Core Members of the Colorectal MDT and has been signed off by the Colorecal MDT Lead Clinician and Trust’s Lead Cancer Clinician and visiting Consultant Clinical Oncologist. Signed copies of this approval are filed and kept by William Harvey Hospital (WHH), Queen Elizabeth The Queen Mother Hospital (QEQMH), East Kent Hospitals University NHS Foundation Trust.
Approval
Date Name / Title Signature
Mr PS Basnyat MDT (MDT Lead WHH)
Mr G Harinath (Colorectal Surgeon)
Dr Catherine Harper-Wynne (Medical Oncologist)
Dr Julia Hall (Clinical Oncologist)
Dr A Santhakumaran (Radiologists)
Dr N Bagla (Histopathologists)
Dr G Vittay (Histopathologists)
Dr Arun Dhiman (Gastroenterologists and Lead Colonoscopists)
Mr George Stavellas (MDT Lead QEQM)
Mr Samer Doughan (Lead QEQM)
NSSG and Cross-Cutting Group Policy Documentation developed and managed by the Kent & Medway Cancer Network is referenced and incorporated into this policy document and the approvals and sign-off process of the original documents is managed by the Kent & Medway Cancer Network.
Enquiries
All enquiries relating to this document should be addressed to:
Addressee: Mr PS Basnyat
Telephone: 01233 616677
Email: [email protected]
Addressee: Mr George Stavellas
Telephone: 01843 225544 Ext 62329
Email: [email protected]
Addressee: Mr Samer Doughan
Telephone: 01843 225544 Ext 65300
Email: [email protected]
Addressee:
Telephone:
Email:
MEASURES ADDRESSED BY THIS EVIDENCE ITEM
This item of evidence is submitted against the following measures:
MDT LEADERSHIP
10-2D-101 Single Named Lead Clinician
MDT STRUCTURE
10-2D-102 Named Core Team memebers
MDT SPECIALISING IN ANAL CANCER
10-2D-103 Named Consultant Surgical Core Member(s) for Anal Cancer
MDT SPECIALISING IN ANAL CANCER
10-2D-103 Named Consultant Surgical Core Member(s) for Anal Cancer
10-2D-104 Named Consultant Clinical Oncology Core Member(s) for Anal Cancer
10-2D-105 Named MDT for Anal Cancer
10-2D-106 Team Attendance at NSSG Meetings
MDT MEETINGS
10-2D-107 Meet Weekly and record Core Attendance and protocols for Referral to Next Scheduled Meeting
10-2D-108 MDT Agreed Cover Arrangements for Core Memebers
10-2D-109 Core Members (or cover) Present for at Least 2/3 of Meetings
OPERATIONAL POLICIES
10-2D-110 Annual Meeting to Discuss Operational Policy
10-2D-111 Policy for all New patients to be reviewed by MDT
10-2D-112 Policy for Communication of Diagnosis to GP
10-2D-113 Operational Policy for Named Key Worker
10-2D-114 Core Histopathology Member Taking Part in Histopathology EQA
Management of Surgical Emergencies Potentially Due to Colorectal Cancer
10-2D-115 MDT/NSSG Agreed Guidelines on Management of Surgical Emergencies
10-2D-116 MDT/NSSG Agreed Secondary to Tertiary Referral Policy
Colorectal Stenting
10-2D-117 MDT/NSSG Agreed List of Personnel Judged Competent for Colorectal Stenting
MDT NURSE SPECIALIST MEASURES
10-2D-118 MDT/NSSG Core Nurse Member Completed Specialist Study
10-2D-119 Agreed List of Responsibilities for Core Nurse Members
10-2D-120 Agreed List of Additional Responsibilities for One Core Nurse Members
10-2D-121 Attendance at National Advanced Communication Skills Training Programme
Extended Membership of MDT
10-2D-122 Extended Membership of MDT
10-2D-123 Patients Permanent Consultation Record
10-2D-124 Patient Experience Excercise
10-2D-125 Presentation and Discussion of Patient Experience Survey
10-2D-126 Provision of Written Patient Information
TREATMENT PLANNING DECISION
10-2D-127 Agree and Record Individual Treatment Plans
CLINICAL GUIDELINES
10-2D-128 MDT/NSSG Agreed Network Clinical Guidelines for Colorectal Cancer
10-2D-129 MDT/NSSG Agreed Network Guidelines for the Clinical Management of Anal Cancer
10-2D-130 MDT/NSSG Agreed Network Guidelines on the Resection of Liver Metastasis
10-2D-131 MDT/NSSG Agreed Network Referral Guidelines between Teams for Anal Cancer
10-2D-132 MDT/NSSG Agreed Network Referral Guidelines between Teams for the Resection of Liver Metastasis
10-2D-133 MDT/NSSG Agreed Network Investigation Protocol for Colorectal Cancer
10-2D-134 MDT/Network Agreed Collection of Minimum Dataset
10-2D-135 MDT/NSSG Agreed Policy for the Electronic Collection of Specific Portion of MDS
10-2D-136 MDT/NSSG Agreed Participation in Network Audit
10-2D-137 MDT Present Results from Participation in Audit to NSSG
CANCER RESEARCH NETWORK
10-2D-138 MDT/NSSG Agreed List of Approved Trials
10-2D-139 MDT/NSSG remedial Action from MDTs Recruitment Results
MDT WORKLOAD
10-2D-140 MDT to Discuss 60 or more New Cases per Year
10-2D-141 20 or more Operative Procedures per Core Individual Surgical Member per Year
OPERATIONAL POLICY SPECIFIC TO ANAL CANCER MDTs
10-2D-142 No more than 2 Clinical Oncologists Practising Radiology in Radiology Department and they should be Core Members
LAPAROSCOPIC COLORECTAL CANCER SURGERY MEASURES
10-2D-143 Policy on the choice of Laparoscopic Colorectal Cancer Surgery (Applicable to all colorectal MDTs)
10-2D-144 Training in Laparoscopic Colorectal Cancer Surgery (Applicable to all colorectal MDTs)
10-2D-145 Referral Guidelines for Laparoscopic Colorectal Cancer Surgery (Applicable to Colorectal MDTs without trained or exempt members)
MDT LEADERSHIP
10-2D-101 Single Named Lead Clinician
The single named lead clinician for the WHH Colorectal MDT is Mr Pradeep S Basnyat. The responsibilities of the position, agreed with Dr Brett Pereira (Trust Cancer Lead Clinician) are listed below: Updated Roles and Responsibilities of MDT Lead Clinicians : August 2010 Role in MDT:
• Chair – Lead and chair the MDT and ensure membership is appropriate (IOG and Quality Measure compliant) and objectives as laid out in the Manual of Cancer Measures and in the national Cancer Action Team document ‘characteristics of an Effective MDT’ are met
• Policies – Be responsible for ensuring that the team has policies and protocols in place which are IOG, Cancer Quality Measure, DOG and Trust compliant
• Annual Operational Policy – Ensure that the team has a robust operational policy relating to the delivery of Cancer Services and that the policy is reviewed at least on an annual basis with appropriate changes to process agreed to ensure best practice
• MDT membership – Ensure that MDT members function in line with the operational policy and specialists work together in teams such that all decisions are multidisciplinary and effective regarding the patients pathway in cancer management
• Training – ensure appropriate skills and training of MDT members such as Advanced Communication Skills Training as appropriate
• Cancer Pathways – Ensure that all patients with Cancer are managed in line with the operational policy and disease site specific pathways of care agreed with the relevant DOG
• Clinical Trials – Support entry of eligible patients into clinical trials where appropriate and with full informed consent in partnership with the research team
• MDT Attendance – Ensure the MDT meets regularly and that attendance is documented and core member’s attendance is maintained in line with Quality Measures.
• MDT Documentation: Be responsible for ensuring that MDM discussions are appropriately documented, validated and circulated to all team members.
• MDT Data Collection and Audit: Be responsible for ensuring that the MDM collects validated data to support.
• - The collection of the cancer minimum data set
• - Cancer registration
• - Relevant DOG agreed clinical audit data sets
• - National Cancer Databases as required
• Meetings: Ensure that besides the regular meetings to discuss patients the MDT meets at least twice a year and that:
• - The outcomes of audit programmes are discussed and appropriate action plans agreed
• - The meeting takes the opportunity for teaching
• - Analysis of breach reports and embed process to ensure best practice delivery of cancer pathway to achieve National Cancer targets
Role in Peer Review Process:
• Lead the MDT through the annual self (and as appropriate external) assessment process for Peer Review
• Ensure Operational Policy is up to date and reviewed with the team
• Ensure appropriate audits and patient surveys completed and action points
MDT STRUCTURE
10-2D-102 Named Core Team memebers
WHH Core Team Members
Name Title/Responsibility Mr Pradeep S Basnyat Lead Clinician of the MDT Mr Gandrasuppalli Harinath Colorectal Surgeon Mr Nebil Behar Locum Colorectal Surgeon Dr Julia Hall Clinical Oncologist (responsible for radiotherapy for Rectal Cancer) Dr Catherine Harper-Wynne Medical Oncologist (responsible for chemotherapy) Dr A Santhakumaran Radiologists
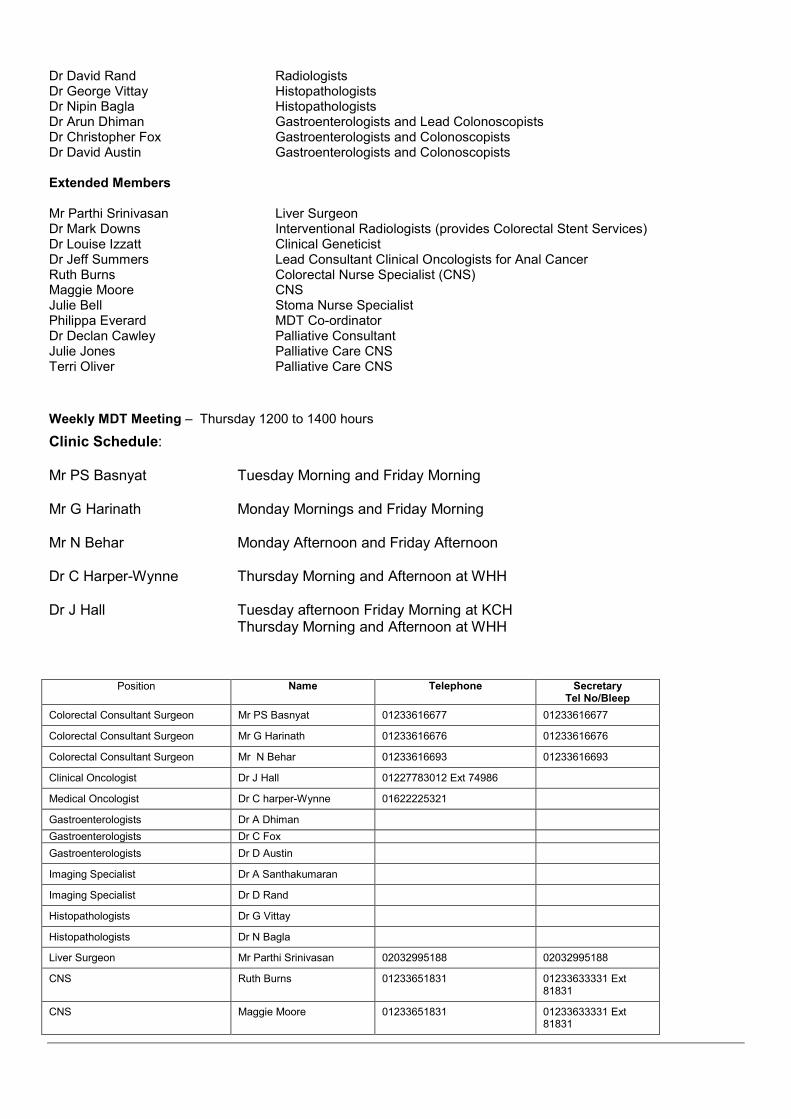
Dr David Rand Radiologists Dr George Vittay Histopathologists Dr Nipin Bagla Histopathologists Dr Arun Dhiman Gastroenterologists and Lead Colonoscopists Dr Christopher Fox Gastroenterologists and Colonoscopists Dr David Austin Gastroenterologists and Colonoscopists Extended Members Mr Parthi Srinivasan Liver Surgeon Dr Mark Downs Interventional Radiologists (provides Colorectal Stent Services) Dr Louise Izzatt Clinical Geneticist Dr Jeff Summers Lead Consultant Clinical Oncologists for Anal Cancer Ruth Burns Colorectal Nurse Specialist (CNS) Maggie Moore CNS Julie Bell Stoma Nurse Specialist Philippa Everard MDT Co-ordinator Dr Declan Cawley Palliative Consultant Julie Jones Palliative Care CNS Terri Oliver Palliative Care CNS
Weekly MDT Meeting – Thursday 1200 to 1400 hours
Clinic Schedule: Mr PS Basnyat Tuesday Morning and Friday Morning Mr G Harinath Monday Mornings and Friday Morning Mr N Behar Monday Afternoon and Friday Afternoon Dr C Harper-Wynne Thursday Morning and Afternoon at WHH Dr J Hall Tuesday afternoon Friday Morning at KCH
Thursday Morning and Afternoon at WHH
Position Name Telephone Secretary Tel No/Bleep
Colorectal Consultant Surgeon Mr PS Basnyat 01233616677 01233616677
Colorectal Consultant Surgeon Mr G Harinath 01233616676 01233616676
Colorectal Consultant Surgeon Mr N Behar 01233616693 01233616693
Clinical Oncologist Dr J Hall 01227783012 Ext 74986
Medical Oncologist Dr C harper-Wynne 01622225321
Gastroenterologists Dr A Dhiman
Gastroenterologists Dr C Fox
Gastroenterologists Dr D Austin
Imaging Specialist Dr A Santhakumaran
Imaging Specialist Dr D Rand
Histopathologists Dr G Vittay
Histopathologists Dr N Bagla
Liver Surgeon Mr Parthi Srinivasan 02032995188 02032995188
CNS Ruth Burns 01233651831 01233633331 Ext 81831
CNS Maggie Moore 01233651831 01233633331 Ext 81831
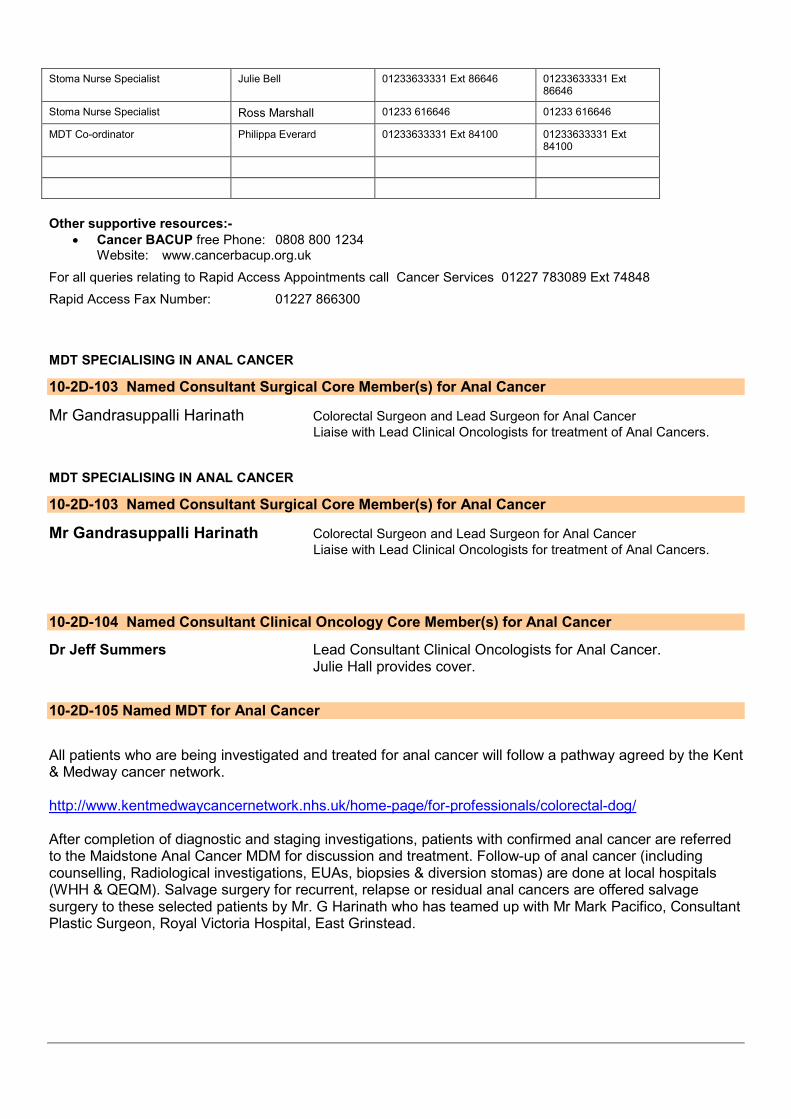
Stoma Nurse Specialist Julie Bell 01233633331 Ext 86646 01233633331 Ext 86646
Stoma Nurse Specialist Ross Marshall 01233 616646 01233 616646
MDT Co-ordinator Philippa Everard 01233633331 Ext 84100 01233633331 Ext 84100
Other supportive resources:-
• Cancer BACUP free Phone: 0808 800 1234 Website: www.cancerbacup.org.uk
For all queries relating to Rapid Access Appointments call Cancer Services 01227 783089 Ext 74848
Rapid Access Fax Number: 01227 866300 MDT SPECIALISING IN ANAL CANCER
10-2D-103 Named Consultant Surgical Core Member(s) for Anal Cancer
Mr Gandrasuppalli Harinath Colorectal Surgeon and Lead Surgeon for Anal Cancer
Liaise with Lead Clinical Oncologists for treatment of Anal Cancers. MDT SPECIALISING IN ANAL CANCER
10-2D-103 Named Consultant Surgical Core Member(s) for Anal Cancer
Mr Gandrasuppalli Harinath Colorectal Surgeon and Lead Surgeon for Anal Cancer
Liaise with Lead Clinical Oncologists for treatment of Anal Cancers.
10-2D-104 Named Consultant Clinical Oncology Core Member(s) for Anal Cancer
Dr Jeff Summers Lead Consultant Clinical Oncologists for Anal Cancer. Julie Hall provides cover.
10-2D-105 Named MDT for Anal Cancer
All patients who are being investigated and treated for anal cancer will follow a pathway agreed by the Kent & Medway cancer network. http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/ After completion of diagnostic and staging investigations, patients with confirmed anal cancer are referred to the Maidstone Anal Cancer MDM for discussion and treatment. Follow-up of anal cancer (including counselling, Radiological investigations, EUAs, biopsies & diversion stomas) are done at local hospitals (WHH & QEQM). Salvage surgery for recurrent, relapse or residual anal cancers are offered salvage surgery to these selected patients by Mr. G Harinath who has teamed up with Mr Mark Pacifico, Consultant Plastic Surgeon, Royal Victoria Hospital, East Grinstead.
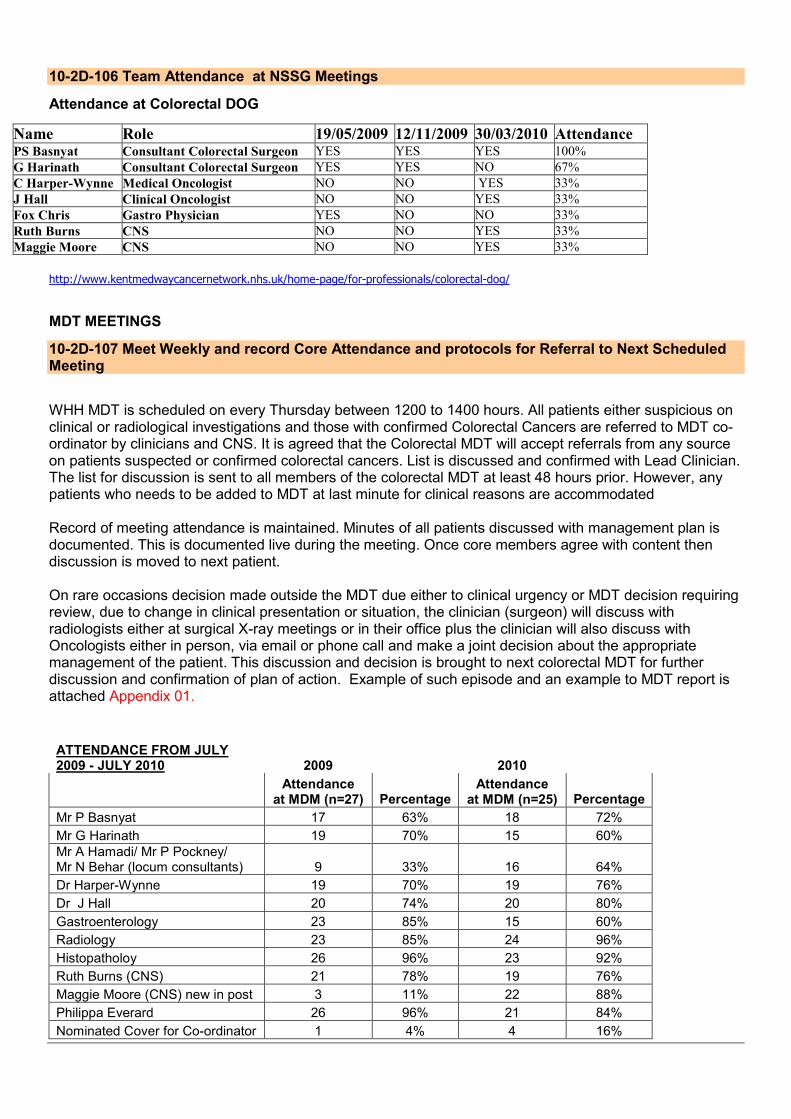
10-2D-106 Team Attendance at NSSG Meetings
Attendance at Colorectal DOG
Name Role 19/05/2009 12/11/2009 30/03/2010 Attendance PS Basnyat Consultant Colorectal Surgeon YES YES YES 100%
G Harinath Consultant Colorectal Surgeon YES YES NO 67%
C Harper-Wynne Medical Oncologist NO NO YES 33%
J Hall Clinical Oncologist NO NO YES 33%
Fox Chris Gastro Physician YES NO NO 33%
Ruth Burns CNS NO NO YES 33%
Maggie Moore CNS NO NO YES 33%
http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
MDT MEETINGS
10-2D-107 Meet Weekly and record Core Attendance and protocols for Referral to Next Scheduled Meeting
WHH MDT is scheduled on every Thursday between 1200 to 1400 hours. All patients either suspicious on clinical or radiological investigations and those with confirmed Colorectal Cancers are referred to MDT co-ordinator by clinicians and CNS. It is agreed that the Colorectal MDT will accept referrals from any source on patients suspected or confirmed colorectal cancers. List is discussed and confirmed with Lead Clinician. The list for discussion is sent to all members of the colorectal MDT at least 48 hours prior. However, any patients who needs to be added to MDT at last minute for clinical reasons are accommodated Record of meeting attendance is maintained. Minutes of all patients discussed with management plan is documented. This is documented live during the meeting. Once core members agree with content then discussion is moved to next patient. On rare occasions decision made outside the MDT due either to clinical urgency or MDT decision requiring review, due to change in clinical presentation or situation, the clinician (surgeon) will discuss with radiologists either at surgical X-ray meetings or in their office plus the clinician will also discuss with Oncologists either in person, via email or phone call and make a joint decision about the appropriate management of the patient. This discussion and decision is brought to next colorectal MDT for further discussion and confirmation of plan of action. Example of such episode and an example to MDT report is attached Appendix 01.
ATTENDANCE FROM JULY 2009 - JULY 2010 2009 2010
Attendance
at MDM (n=27) Percentage Attendance
at MDM (n=25) Percentage
Mr P Basnyat 17 63% 18 72%
Mr G Harinath 19 70% 15 60%
Mr A Hamadi/ Mr P Pockney/ Mr N Behar (locum consultants) 9 33% 16 64%
Dr Harper-Wynne 19 70% 19 76%
Dr J Hall 20 74% 20 80%
Gastroenterology 23 85% 15 60%
Radiology 23 85% 24 96%
Histopatholoy 26 96% 23 92%
Ruth Burns (CNS) 21 78% 19 76%
Maggie Moore (CNS) new in post 3 11% 22 88%
Philippa Everard 26 96% 21 84%
Nominated Cover for Co-ordinator 1 4% 4 16%
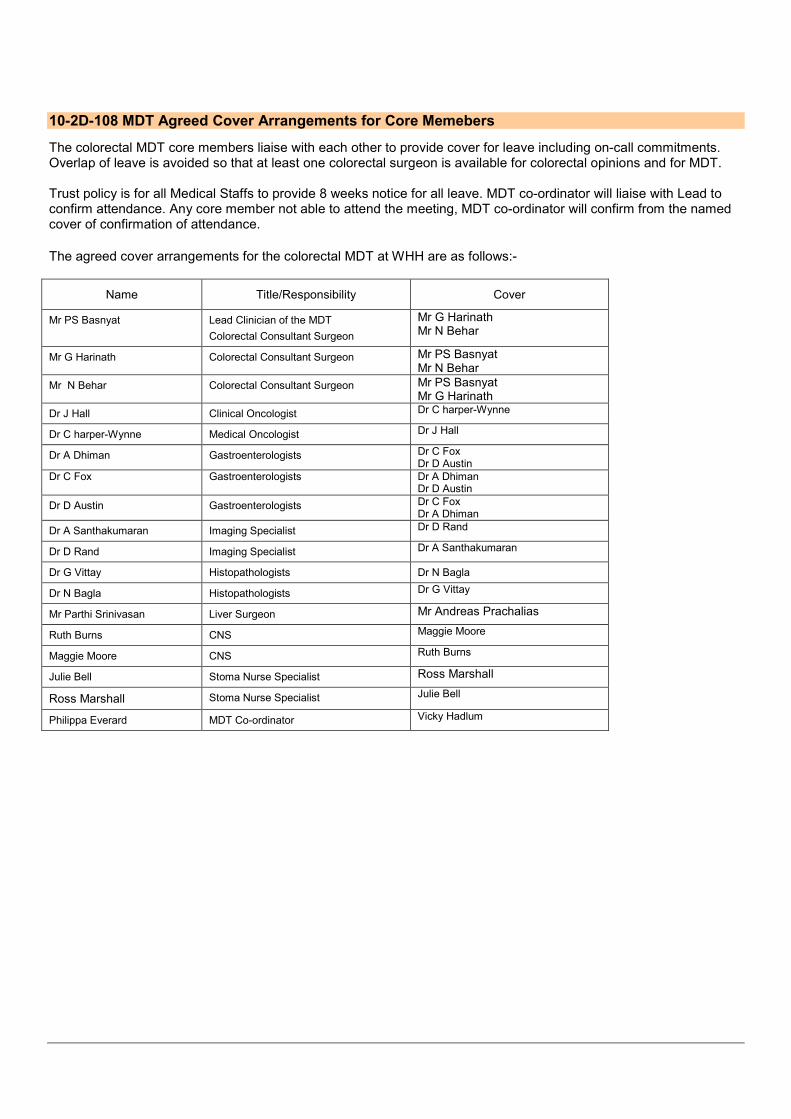
10-2D-108 MDT Agreed Cover Arrangements for Core Memebers
The colorectal MDT core members liaise with each other to provide cover for leave including on-call commitments. Overlap of leave is avoided so that at least one colorectal surgeon is available for colorectal opinions and for MDT. Trust policy is for all Medical Staffs to provide 8 weeks notice for all leave. MDT co-ordinator will liaise with Lead to confirm attendance. Any core member not able to attend the meeting, MDT co-ordinator will confirm from the named cover of confirmation of attendance.
The agreed cover arrangements for the colorectal MDT at WHH are as follows:-
Name Title/Responsibility Cover
Mr PS Basnyat Lead Clinician of the MDT
Colorectal Consultant Surgeon
Mr G Harinath Mr N Behar
Mr G Harinath Colorectal Consultant Surgeon Mr PS Basnyat Mr N Behar
Mr N Behar Colorectal Consultant Surgeon Mr PS Basnyat Mr G Harinath
Dr J Hall Clinical Oncologist Dr C harper-Wynne
Dr C harper-Wynne Medical Oncologist Dr J Hall
Dr A Dhiman Gastroenterologists Dr C Fox Dr D Austin
Dr C Fox Gastroenterologists Dr A Dhiman Dr D Austin
Dr D Austin Gastroenterologists Dr C Fox Dr A Dhiman
Dr A Santhakumaran Imaging Specialist Dr D Rand
Dr D Rand Imaging Specialist Dr A Santhakumaran
Dr G Vittay Histopathologists Dr N Bagla
Dr N Bagla Histopathologists Dr G Vittay
Mr Parthi Srinivasan Liver Surgeon Mr Andreas Prachalias
Ruth Burns CNS Maggie Moore
Maggie Moore CNS Ruth Burns
Julie Bell Stoma Nurse Specialist Ross Marshall
Ross Marshall Stoma Nurse Specialist Julie Bell
Philippa Everard MDT Co-ordinator Vicky Hadlum

10-2D-109 Core Members (or cover) Present for at Least 2/3 of Meetings
Attach is the attendance of individual member and cover for the colorectal MDT. Therefore, Mr Basnyat would have covered for Mr Harinath and locum consultants. Gastroenterology, Radiology and Histopathology, individual attendance and their covers attendance is documented.
ATTENDANCE FROM JULY 2009 - JULY 2010 2009 2010
Attendance
at MDM (n=27) Percentage Attendance
at MDM (n=25) Percentage
Mr P Basnyat 17 63% 18 72%
Mr G Harinath 19 70% 15 60%
Mr A Hamadi/ Mr P Pockney/ Mr N Behar (locum consultants) 9 33% 16 64%
Dr Harper-Wynne 19 70% 19 76%
Dr J Hall 20 74% 20 80%
Gastroenterology 23 85% 15 60%
Radiology 23 85% 24 96%
Histopatholoy 26 96% 23 92%
Ruth Burns (CNS) 21 78% 19 76%
Maggie Moore (CNS) new in post 3 11% 22 88%
Philippa Everard 26 96% 21 84%
Nominated Cover for Co-ordinator 1 4% 4 16%
OPERATIONAL POLICIES
10-2D-110 Annual Meeting to Discuss Operational Policy
Operational Policy meeting between QEQM and WHH was attended by Mr P Basnyat on 7th June 2010.
Minutes of the meeting is attached as Appendix 02.
10-2D-111 Policy for all New patients to be reviewed by MDT
Patients to be discussed at colorectal MDT meetings Colorectal & Anal Cancer cases (proven & suspected). Exceptionally other patients may be discussed, such as patients with high grade dysplasia in colorectal biopsies or polypectomy specimens, those with strong family history or patients with pelvic or small bowel cancer that involve the colon and rectum, especially when clinicians feel there is a need for discussion within the MDT. Colorectal cancer patients discussed fall in 3 main categories:
1. Pre operative or newly diagnosed colorectal or anal cancer patients (1st primary or subsequent colorectal primaries [metachronous]).
• All patients with a new cancer diagnosis are reviewed in the MDT meeting to discuss diagnosis & staging [biopsies and radiological imaging] as well as treatment options.
• Include discussion about patient fitness, choice of radical cancer resection (e.g. right hemicolectomy).
• Curative or Palliative treatment are discussed.
• Colorectal Stent if appropriate is considered
• Referral for preoperative radiotherapy (short or long course) in rectal cancer, preoperative chemotherapy, preoperative radio-chemotherapy and radio-chemotherapy as an alternative definitive treatment.
• Discussion may also include local treatment options including referral for TEM (Transanal endoscopic microsurgery) or referral to palliative care.
• Polyps that need resection or surveillance are discussed
• Anal cancer patients are referred to the Maidstone Anal Cancer MDT. 2. Post operative patients, including patients who have had emergency surgery and have been staged post operatively:
• Operative findings are discussed. Comparison are made with pre-operative staging and histology.
• Plan for adjuvant chemotherapy or postoperative radiotherapy
• Plans for radiological imaging (e.g. PET scans in patients with potentially resectable liver secondaries) to enable discussion regarding continuing management.
• Referral to the palliative care team.
3. Recurrent Cancer patients
• Enable discussion surrounding continuing treatment (salvage surgery, radiotherapy or chemotherapy) or referral to The Palliative Care Team (Pilgrims Hospice Clinical Nurse Specialists)
Referral / Submission of cases to be discussed at colorectal MDT meeting.
• Details of patients who have a suspected colorectal cancer are
• given to the MDT co-ordinator and CNS who will arrange for the patient to be discussed at the MDT with the relevant histopathology and imaging results
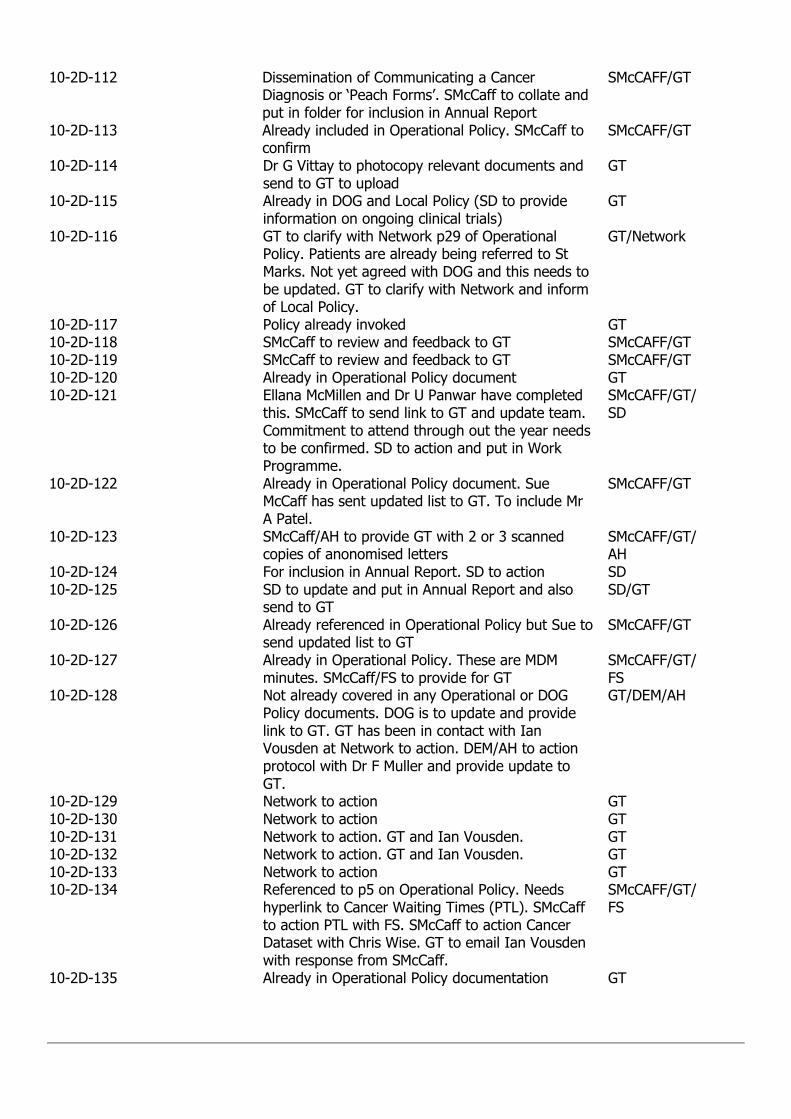
• Clinicians (surgeons, oncologists, gastroenterologists, colorectal CNS) are responsible for ensuring that an MDT referral form is submitted to the MDT Co-ordinator. (Appendix 3).
• Deadlines for inclusion in meeting: Referrals from all sources must be made to the MDT co-ordinator and/or Colorectal CNS (who will pass it on to the co-ordinator) by Monday 12:00 Noon (QEQM-KCH Colorectal MDT meeting) and by Tuesday 12:00 Noon for WHH colorectal MDT meeting. The MDT co-ordinator generates an MDT list of patients to be discussed at the next meeting. The order of the list is generally the order in which patients are discussed. However, if clinical need arises then patients are allowed to be added even at the last minute after discussion with the Lead.
• Informing Pathology and Radiology Department: This is the responsibility of the MDT co-ordinator. Pathologists and the radiologists are responsible for reviewing the slides and imaging respectively prior to the MDT meeting.
Source of Referral
• Out patient clinics including Surgical, Oncological, Gastroenterology all other clinical clinics.
• Endoscopy department after colonoscopic examination
• Bowel Screening Pathway. Appendix 4
• Radiology Department if bowel abnormality is picked up on imaging
• Pathology department if Histology is suspicious or confirms cancer
• Any other clinicians within the Trust Method of of Referral
• MDT Referral Form
• Phone
• Fax
10-2D-112 Policy for Communication of Diagnosis to GP
• All new diagnoses of colorectal cancer are to be discussed with the GP or practice by the end of The next working day
• MDT minutes are typed live and posted to GP’s on the day of the MDM
• Patients are arranged to be reviewed in out patient clinic under surgeon who will be performing the operation
• The CNS will meet with the patient when they receive the diagnosis (See Appendix 8) The CNS Will then phone / fax the GP to let them know the diagnosis and management plan.
• Any significant change to the management plan decided at the MDT will be communicated to the GP within 7 days by post.
• For GPs who wish to communicate by email, this is an acceptable alternative.
• For patients in peripheral clinics the consultant will let the CNS know what has been Communicated with the patient. The CNS will then contact the patient by phone and offer to meet with them if the patient wishes. The CNS will contact the GP as above. Information packs for these patients are available and will be provided by the consultant.
• Provision of information to referring GPs and other PCOs on the appropriateness and timeliness of urgent suspected cancer GP referrals. Cancer Data Co-ordinators on each site are responsible for giving a monthly report to the MDT lead on the cancer yield in the various categories of referral. The appropriateness of rapid access GP referrals will be prospectively audited by the Cancer Data Co-ordinators via the cancer tracking forms.
Key worker communicating cancer diagnosis audit has been completed. 80% compliance was noted in the audit undertaken by the CNS. (see appendix 4). The audit also looked at timeliness of diagnosis forms to GP.
10-2D-113 Operational Policy for Named Key Worker
The Kent and Medway Cancer Network Operational Policy for the named Key Worker has been uploaded to
http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/ Appendix 5
10-2D-114 Core Histopathology Member Taking Part in Histopathology EQA
Diagnostic Histopathology Service
• The Trust operates a consultant led service which is provided by the Pathology Department at the WHH, which serves all the trust.
• The designated Colorectal Pathologists are Dr. George Vittay and Dr. Nipin Bagla.
• Colorectal specimens are processed according to the Minimum Data Sets and reported by designated consultants.
• This department has responsibility for informing the MDT co-ordinator of any patients with a histology confirming colorectal cancer. This is normally done by giving the MDT co-ordinator access to a shared hard drive containing all histology results, which are updated on a weekly basis.
Histopathologists who have participated in South Thames (East) General Histopathology EQA Scheme are Dr G Vittay, Dr Nipin Bagla, Dr S Anjarwalla, Dr K Skendros and Dr M perenyei. Hard copy of the Certificate Appendix 6.
Management of Surgical Emergencies Potentially Due to Colorectal Cancer
10-2D-115 MDT/NSSG Agreed Guidelines on Management of Surgical Emergencies
Emergency Admission of Colorectal Patients
As agreed by the Association of Coloproctology for Great Britain and Ireland, patients admitted through the accident and emergency department with suspected colorectal cancer that require emergency surgery, will be operated on by the general surgeon on call. However, where that surgeon is not a core colorectal MDM member, it has been agreed that telephone advice may, if required, be obtained from any of the Trust’s colorectal surgeons if on-call at a different site within East Kent. Patients requiring colonic stenting will, after resuscitation, be transferred to KCH for stenting by Dr Mark Downes. Such patients, whilst at KCH, will remain under the care of Dr Frank Muller or Mr Amjad kushal (locum colorectal surgeon). All emergency patients will be referred to the colorectal MDT. Subsequent management and follow up will be taken over by one of the colorectal surgeon who is the core member of the MDT. Patients will be referred to the colorectal nurse specialist within 24 hours (for MDT discussion) or on Monday morning if this is a weekend admission.
Colorectal cancers presenting as an emergency are managed in line with the Network agreed guidance.
http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
10-2D-116 MDT/NSSG Agreed Secondary to Tertiary Referral Policy
In line with the Network agreed guidance all patients with Liver metastasis are discussed in MDT when Liver surgeons are present. In Liver surgeons absence, these patients are refereed to Liver MDT at Kings Hospital London. All Lung metastasis after discussion at local MDT are referred to Lung MDT. Those requiring more extensive surgery either for primary colorectal cancer or recurrence (pelvic exenteration) are referred to St Mark’s Hospital London. Those requiring TEMs procedure for local rectal tumours are referred to either king’s hospital London or St Richard’s Hospital Chichester. http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
Colorectal Stenting
10-2D-117 MDT/NSSG Agreed List of Personnel Judged Competent for Colorectal Stenting
Patients requiring colonic stenting will, after resuscitation, be transferred to KCH for stenting by Dr Mark Downes. Such patients, whilst at KCH, will remain under the care of Dr Frank Muller (gastroenterologists) or Mr Amjad Kushal (locum colorectal surgeon). Propective data of Sefl-expanding Metal Stenting for Malignant Colonic Tumours a Prospective Study was presented in February 2010 at Association of Surgeons In training Meeting, Hull. Mr Kushal is a colorectal surgeon who is skilled in colonoscopy and works in a JAG accredited unit at
Endoscopy Department Kent and Canterbury Hospital. Dr Downes has 30 years experience in interventional radiology. He is also an elected Fellow of the Cardiovascular and Interventional Radiology Society of Europe (CIRSE) which is only granted on evidence of sustained expertise. These will provide as competent for colorectal stenting.
http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
MDT NURSE SPECIALIST MEASURES
10-2D-118 MDT/NSSG Core Nurse Member Completed Specialist Study
The CNS team has also undergone changes and now has two part time CNS’s, this is a day less per week than a year ago (one with level 3 cancer qualification). However, a new surgical care practitioner is running the cancer follow up clinic. An oncology social worker is now in post. Cross site CNS meetings have been started and take place every 2 months to standardize nursing roles and work patterns across all three sites. Ruth Burns CNS qualifications:
• Bachelor of Science Full time Honours programme in Nursing Studies 16
th September 1993
South Bank University London
• Oncological Nursing Course 27th November 1995
• Applied Human Studies, Community Health LEO Level 3 February 2002 Bradford College
10-2D-119 Agreed List of Responsibilities for Core Nurse Members
Responsibilities of CNS
• The CNS will usually be present when a patient receives a diagnosis of colorectal cancer.
• The CNS if possible will spend time with the patient and their relatives.
• The CNS will make arrangements to contact the patient and family if appropriate at a later date.
• The CNS will be responsible for ensuring that patient information is available.
• The CNS will provide a card with contact details. The patient and carers will be encouraged to make contact if there are any concerns.
• The CNS will liaise with the MDT as appropriate..
• The CNS will usually be the key worker.
• The CNS will provide information packs to be made available to consultants who attend peripheral clinics.
• CNS will be contributing to the MDT discussion
• CNS will provide expert nursing advise and support to other health professionals in the nurse’s specialist area of practice Appendix 5
10-2D-120 Agreed List of Additional Responsibilities for One Core Nurse Members
Same as above responsibilities (Appendix 5). Two CNS are Ruth Burns and Maggie Moore at WHH. Maggie Moore is a recent appointee and they both cross cover each other.
10-2D-121 Attendance at National Advanced Communication Skills Training Programme
ADVANCE COMMUNICATION COURSE
Attended Enrolled
Mr P Basnyat yes
Mr G Harinath yes
Mr N Behar (locum) yes
Dr C Harper-Wynne yes
Dr J Hall yes
Ruth Burns (CNS) yes
Maggie Moore (CNS) yes
Zoe Clark (BS Nurse) yes
Extended Membership of MDT
10-2D-122 Extended Membership of MDT
Mr Parthi Srinivasan Liver Surgeon Dr Mark Downs Interventional Radiologists (provides Colorectal Stent Services) Mr Amjad Kushal Colorectal Surgeon (locum provided Colorectal Stent Services) Dr Frank Muller Gastroenterologists (provides Colorectal Stent Services) Dr Louise Izzatt Clinical Geneticist Dr Jeff Summers Lead Consultant Clinical Oncologists for Anal Cancer Dr Arun Dhiman Gastroenterologists Dr Christopher Fox Gastroenterologists Dr David Austin Gastroenterologists Ms Juliet King Thoracic Surgeon Ruth Burns Colorectal Nurse Specialist (CNS) Maggie Moore CNS Julie Bell Stoma Nurse Specialist Philippa Everard MDT Co-ordinator Dr Declan Cawley Palliative Consultant Julie Jones Palliative Care CNS Terri Oliver Palliative Care CNS
• There are no psychiatrist or clinical psychologist as extended member, however, we have access to psychiatrists and counsellor within the trust. Patients are provided with East Kent Hospitals University NHS Trust Cancer and Supportive Care Counselling Service for Patients leaflet.
There are arrangements in place to access a Social Worker when required
10-2D-123 Patients Permanent Consultation Record
Patients are given the opportunity of all clinic letters written to their GPs, both from surgical clinics and oncology clinics. Copies of colonoscopy reports are also given to patient. Patients are also offered all consultation records undertaken during their journey.
CNS are patients main source of contact.
10-2D-124 Patient Experience Excercise
‘Survery on the follow up of colorectal cancer patients’ Presented at DoG meeting, Kings Hill Conference Centre; November 2008 Local MDT in the work plan is committed to undertake patient satisfaction survey.
10-2D-125 Presentation and Discussion of Patient Experience Survey
Local MDT in the work plan is committed to undertake patient satisfaction survey. Results of which will be discussed at MDT meeting and appropriate action implemented. This is part of WHH Colorectal MDT Work Plan.
10-2D-126 Provision of Written Patient Information
Information provided to patient by CNS are (all these leaflets are included in the pack given to patients):
• NHS Kent and Medway cancer Network ‘Your Local cancer Services’
• Beating Bowel Cancer Leaflets: your pathway, your operation, your recipe for recovery, patient support
• Cancerbackup and Macmillan Book: Understanding Colon Cancer
• Cancerbackup and Macmillan Book: Help with the Cost of Cancer
• East Kent Hospitals University NHS Trust An introduction to the Colorectal Cancer Multidisciplinary Team
• East Kent Hospitals University NHS Trust Information Leaflet for Patients/Visitors
• East Kent Hospitals University NHS Trust Cancer and Supportive Care Counselling Service for Patients
• Leaflet information including contact details of CNSs
TREATMENT PLANNING DECISION
10-2D-127 Agree and Record Individual Treatment Plans
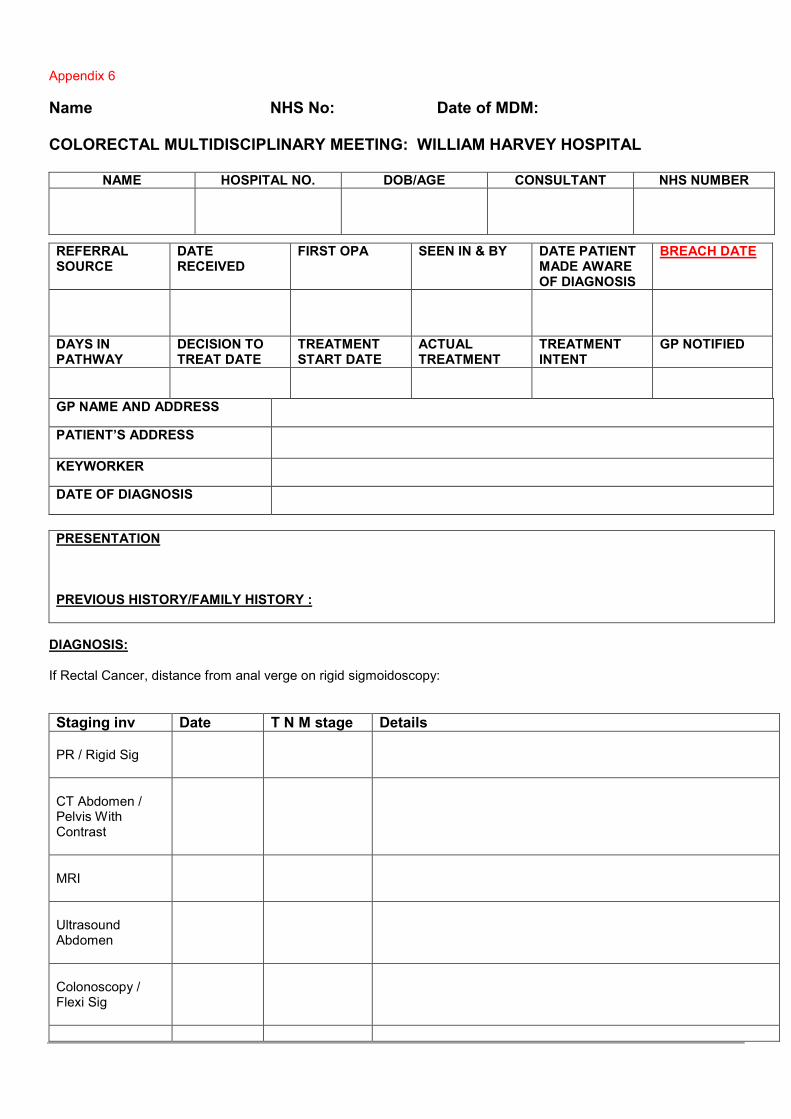
MDT meeting at WHH is scheduled every Thursday between 1200 to 1400 hours. Agreed individual patient’s management plans as per MDT meetings are recorded in a standard format. Appendix 6
Recording of the minutes of individual patients is live at MDT meetings. Recod includes details of patients identity, clinical presentation including associated co-morbidities, the MDT treatment planning decision. An anonymised example of the record of the meeting and individual treatment plan is attached as Appendix 7. Anal cancer patients are investigated and staged locally. These patients are discussed at local MDT and then referred to Network nominated anal cancer MDT at Maidstone. However, if the patient has a confirmed diagnosis of Anal Cancer and staging investigation is complete then the clinician has the provision of referring these cases to designated network Anal cancer MDT before local MDT discussion to avoid any delay in the pathway. CLINICAL GUIDELINES
10-2D-128 MDT/NSSG Agreed Network Clinical Guidelines for Colorectal Cancer
East Kent Hospitals University NHS Trust Local Colorectal MDT has agreed and signed up to the Kent & Medway Cancer Network The Management of Bowel Cancer ‘A Pathway of Care’. The pathway involves colorectal cancer in general, anal cancer and resection of liver metastasis. http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
10-2D-129 MDT/NSSG Agreed Network Guidelines for the Clinical Management of Anal Cancer
East Kent Hospitals University NHS Trust Local Colorectal MDT has agreed and signed up to the Kent & Medway Cancer Network The Management of Bowel Cancer ‘A Pathway of Care’. The pathway involves anal cancer. http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
As discussed previously, after completion of diagnostic and staging investigations, patients with confirmed anal cancer are referred to the Maidstone Anal Cancer MDM for discussion and treatment. Follow-up of anal cancer (including counselling, Radiological investigations, EUAs, biopsies & diversion stomas) are done at local hospitals (WHH & QEQM). Salvage surgery for recurrent, relapse or residual anal cancers are offered salvage surgery to these selected patients by Mr. G Harinath who has teamed up with Mr Mark Pacifico, Consultant Plastic Surgeon, Royal Victoria Hospital, East Grinstead.

10-2D-130 MDT/NSSG Agreed Network Guidelines on the Resection of Liver Metastasis
East Kent Hospitals University NHS Trust Local Colorectal MDT has agreed and signed up to the Kent & Medway Cancer Network The Management of Bowel Cancer ‘A Pathway of Care’. The pathway involves resection of liver metastasis. http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
In line with the Network agreed guidance all patients with Liver metastasis are discussed in MDT when Liver surgeons are present. Mr Parthi Srinivasan, Liver Surgeon from King’s Hospital London attend WHH MDT last Thursday of the month. In Liver surgeons absence, these patients are refereed to Liver MDT at Kings Hospital London. Those requiring urgent review are also referred directly to Liver MDT rather than waiting for last Thursday of the month. Communication between local MDT and Liver MDT is well established and runs successfully. Appendix 8
10-2D-131 MDT/NSSG Agreed Network Referral Guidelines between Teams for Anal Cancer
East Kent Hospitals University NHS Trust Local Colorectal MDT has agreed and signed up to the Kent & Medway Cancer Network The Management of Bowel Cancer ‘A Pathway of Care’. The pathway involves anal cancer. http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
As discussed previously, after completion of diagnostic and staging investigations, patients with confirmed anal cancer are referred to the Maidstone Anal Cancer MDM for discussion and treatment. Lead Consultant Clinical Oncologists for Anal Cancer for the network is Dr Jeff Summers. Mr. G Harinath is local colorectal surgeon who is the Lead for Anal Cancer. Mr Mark Pacifico, Consultant Plastic Surgeon, Royal Victoria Hospital, East Grinstead provides plastic surgery cover. Appendix 9
10-2D-132 MDT/NSSG Agreed Network Referral Guidelines between Teams for the Resection of Liver Metastasis
East Kent Hospitals University NHS Trust Local Colorectal MDT has agreed and signed up to the Kent & Medway Cancer Network The Management of Bowel Cancer ‘A Pathway of Care’. The pathway involves resection of liver metastasis. http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
In line with the Network agreed guidance all patients with Liver metastasis are discussed in MDT when Liver surgeons are present. Mr Parthi Srinivasan, Liver Surgeon from King’s Hospital London attend WHH MDT last Thursday of the month. In Liver surgeons absence, these patients are refereed to Liver MDT at Kings Hospital London. Those requiring urgent review are also referred directly to Liver MDT rather than waiting for last Thursday of the month. Communication between local MDT and Liver MDT is well established and runs successfully. Appendix 8
10-2D-133 MDT/NSSG Agreed Network Investigation Protocol for Colorectal Cancer
East Kent Hospitals University NHS Trust Local Colorectal MDT has agreed and signed up to the Kent & Medway Cancer Network The Management of Bowel Cancer ‘A Pathway of Care’. http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
DATA COLLECTION
10-2D-134 MDT/Network Agreed Collection of Minimum Dataset
Local MDT maintains minimum dataset by the Network. 31 and 62 day targets: These targets are closely monitored by the MDT via the Infoflex system. Rapid access tracking forms are completed at the first clinic appointment and then become the responsibility of the patient tracker who books the first diagnostic investigation and then hands over to the MDT co-ordinator. The MDT endeavours to comply with the 31 and 62 day targets. Potential breaches are escalated to the cancer directorate Clinical Service Manager Appendix 10 http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/data-set-documents/
10-2D-135 MDT/NSSG Agreed Policy for the Electronic Collection of Specific Portion of MDS
Minutes of the MDT discussion are recorded live electronically. A copy of the MDT minutes is circulated to all members via e-mail within 24 hours by the MDT co-ordinator
http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/data-set-documents/
10-2D-136 MDT/NSSG Agreed Participation in Network Audit
William Harvey Colorectal Department has taken part in following Audit projects which have been presented at the Network meetings. Some of the work has been presented in International Meetings and published in Peer Review Journal. 1. “Quality of Rectal Cancer Resection in East Kent NHS Hospitals Trust”. Presented at the March 2008 DoG Meeting, Kings Hill Conference Centre. 2. ‘Survery on the follow up of colorectal cancer patients’ Presented at DoG meeting, Kings Hill Conference Centre; November 2008 3. “Quality of Operative Documentation on Colorectal Cancers”. This was presented at the March 2009 DoG Meeting, Kings Hill Conference Centre. 4. ‘Managing colorectal cancers: Problems in secondary care’ Presented at the Dog Meeting, Kings Hill Conference Centre; May 2009 5. ‘Audit on the compliance of pathology reporting in Kent Medway Cancer Network’ Presented at the DoG meeting, Kings Hill Conference Centre November 2009 6. Research Grant from Colorectal DOG. Audit of 7 hospitals in the region for compliance on Colonoscopy Guidelines. Project has been completed. Data and results have been presented and published in peer review journals. a. Chivers K, Seunarine B, Shoaib A, Basnyat P, Taffinder N. Why wait for a colonoscopy? An easy cure. Br J Surg 2006; 93(Suppl1): 24. b. Chivers KC, Basnyat PS, Taffinder N. How compliant do we want to be with the colonoscopy surveillance guidelines?. Colorectal Disease 2007;9(9):830-33 c. Chivers KC, Basnyat PS, Taffinder N. The impact of national guidelines on the waiting list for colonoscopy: a quantitative clinical audit. Colorectal Disease July 2010;12(7):632-639. Article first published online: 10 April 2009, DOI:10.1111/j.1463-1318.2000.01871.x 7. Singh S, Arif A, Fox C, Basnyat PS. Complication after pre-operative India ink tattooing in a colonic lesion. Digestive Surgery. 2006;23(5-6);303 8. Rao G N, Basnyat P, Taffinder N, Hudson C, Insall R. Reducing surgical outpatient waiting is not the solution to meet the 2005 colorectal cancer target. Colorectal Disease February 2006;8:135-139.
10-2D-137 MDT Present Results from Participation in Audit to NSSG
As above, William Harvey Colorectal Department has taken part in following Audit projects which has been presented at the Network meetings. Some of the work has been presented in International Meetings and published in Peer Review Journal. 1. “Quality of Rectal Cancer Resection in East Kent NHS Hospitals Trust”. Presented at the March 2008 DoG Meeting, Kings Hill Conference Centre. 2. ‘Survery on the follow up of colorectal cancer patients’ Presented at DoG meeting, Kings Hill Conference Centre; November 2008 3. “Quality of Operative Documentation on Colorectal Cancers”. This was presented at the March 2009 DoG Meeting, Kings Hill Conference Centre. 4. ‘Managing colorectal cancers: Problems in secondary care’ Presented at the Dog Meeting, Kings Hill Conference Centre; May 2009 5. ‘Audit on the compliance of pathology reporting in Kent Medway Cancer Network’ Presented at the DoG meeting, Kings Hill Conference Centre November 2009 6. Research Grant from Colorectal DOG. Audit of 7 hospitals in the region for compliance on Colonoscopy Guidelines. Project has been completed. Data and results have been presented and published in peer review journals. a. Chivers K, Seunarine B, Shoaib A, Basnyat P, Taffinder N. Why wait for a colonoscopy? An easy cure. Br J Surg 2006; 93(Suppl1): 24. b. Chivers KC, Basnyat PS, Taffinder N. How compliant do we want to be with the colonoscopy surveillance guidelines?. Colorectal Disease 2007;9(9):830-33 c. Chivers KC, Basnyat PS, Taffinder N. The impact of national guidelines on the waiting list for colonoscopy: a quantitative clinical audit. Colorectal Disease July 2010;12(7):632-639. Article first published online: 10 April 2009, DOI:10.1111/j.1463-1318.2000.01871.x 7. Singh S, Arif A, Fox C, Basnyat PS. Complication after pre-operative India ink tattooing in a colonic lesion. Digestive Surgery. 2006;23(5-6);303 8. Rao G N, Basnyat P, Taffinder N, Hudson C, Insall R. Reducing surgical outpatient waiting is not the solution to meet the 2005 colorectal cancer target. Colorectal Disease February 2006;8:135-139.
CANCER RESEARCH NETWORK
10-2D-138 MDT/NSSG Agreed List of Approved Trials
Patients may be considered for research trials. This will be after discussion with the oncologist / colorectal surgeons. Dr Catherine Harper-Wynne and Julia Hall are Medical Oncologist and Clinical Oncologists respectively. Clinical trials coordinator is Paula Whichelo.
Colorectal Current List of Trials: NSCCG A National Study of Colorectal Cancer Genetics.
Patient selection: Patients with newly diagnosed with colorectal adenocarcinoma, and those treated within the last five years, under the age of 70 at diagnosis.
QUASAR 2 Multicentre International study capecitabine +/- bevacizumab as adjuvant treatment of colorectal cancer.
SCOT Short Course Oncology Therapy - A study of Adjuvant Chemotherapy in colorectal cancer by the
CACTUS & QUASAR 3 Groups. PICCOLO A randomized clinical trial of treatment for fluorouracil-resistant advanced colorectal cancer
comparing standard single-agent irinotecan versus irinotecan plus panitumumab and versus irinotecan plus ciclosporin. Closed June 2010
http://www.kentmedwaycancernetwork.nhs.uk/home-page/kmcrn/rats/colorectal/
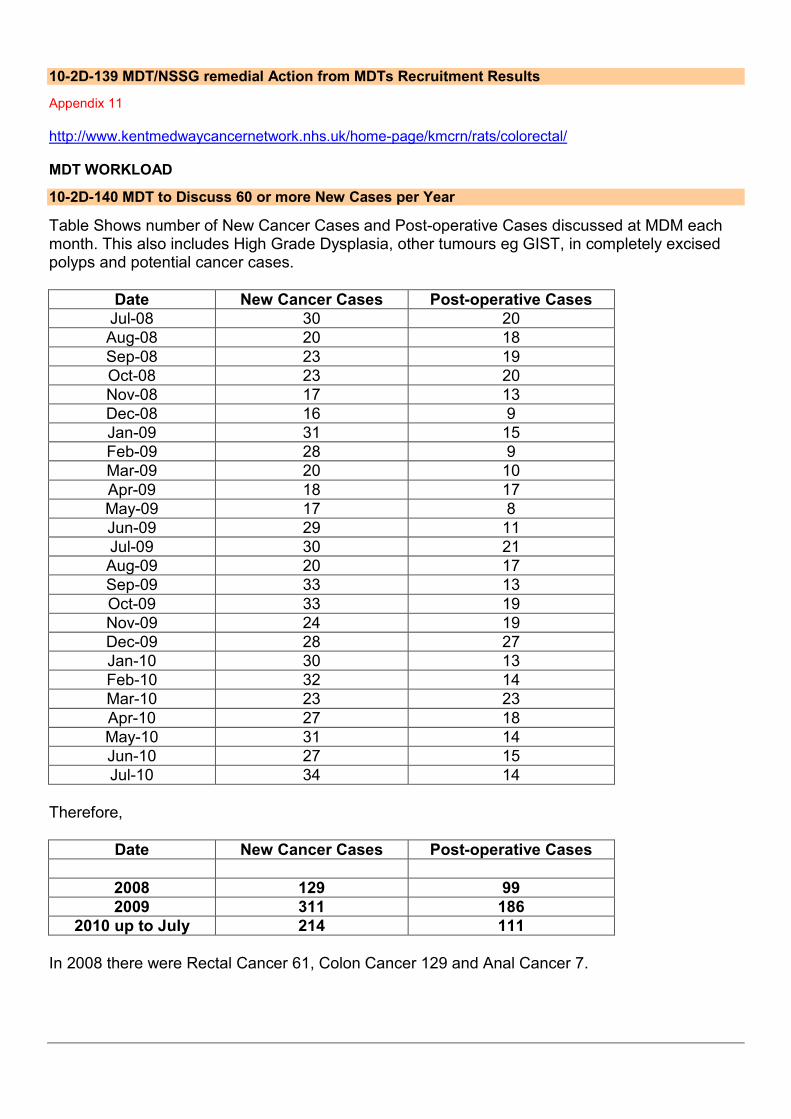
10-2D-139 MDT/NSSG remedial Action from MDTs Recruitment Results
Appendix 11 http://www.kentmedwaycancernetwork.nhs.uk/home-page/kmcrn/rats/colorectal/ MDT WORKLOAD
10-2D-140 MDT to Discuss 60 or more New Cases per Year
Table Shows number of New Cancer Cases and Post-operative Cases discussed at MDM each month. This also includes High Grade Dysplasia, other tumours eg GIST, in completely excised polyps and potential cancer cases.
Date New Cancer Cases Post-operative Cases
Jul-08 30 20
Aug-08 20 18
Sep-08 23 19
Oct-08 23 20
Nov-08 17 13
Dec-08 16 9
Jan-09 31 15
Feb-09 28 9
Mar-09 20 10
Apr-09 18 17
May-09 17 8
Jun-09 29 11
Jul-09 30 21
Aug-09 20 17
Sep-09 33 13
Oct-09 33 19
Nov-09 24 19
Dec-09 28 27
Jan-10 30 13
Feb-10 32 14
Mar-10 23 23
Apr-10 27 18
May-10 31 14
Jun-10 27 15
Jul-10 34 14
Therefore,
Date New Cancer Cases Post-operative Cases
2008 129 99
2009 311 186
2010 up to July 214 111
In 2008 there were Rectal Cancer 61, Colon Cancer 129 and Anal Cancer 7.

10-2D-141 20 or more Operative Procedures per Core Individual Surgical Member per Year
PS Basnyat
G Harinath
Locum Consultants
July 2008 7 8 5
August 2008 6 2 10
September 2008 5 8 6
October 2008 7 6 7
November 2008 5 7 1
December 2008
5 3 1
January 2009 5 5 5
February 2009 2 3 4
March 2009 6 2 2
April 2009 6 9 2
May 2009 2 3 3
June 2009 5 2 4
July 2009 7 10 4
August 2009 5 11 1
September 2009 7 6 0
October 2009 14 4 1
November 2009 8 10 1
December 2009
7 6 14
January 2010 6 4 3
February 2010 6 2 6
March 2010 8 5 10
April 2010 7 6 5
May 2010 5 4 5
June 2010 7 7 1
July 2010 3 4 7
Cancer operations by consultant as identified at MDM
PS Basnyat G Harinath Locum (combined)
Average operations per month
07/08-06/09 61 60 50 14.2
07/08-06/10 90 79 58 18.9
OPERATIONAL POLICY SPECIFIC TO ANAL CANCER MDTs
10-2D-142 No more than 2 Clinical Oncologists Practising Radiology in Radiology Department and they should be Core Members
East Kent Hospitals University NHS Trust Local Colorectal MDT has agreed and signed up to the Kent & Medway Cancer Network The Management of Bowel Cancer ‘A Pathway of Care’. The pathway involves anal cancer. As discussed previously, patients with confirmed anal cancer are referred to the Maidstone Anal Cancer MDM for discussion and treatment. Lead Consultant Clinical Oncologists for Anal Cancer for the network is Dr Jeff Summers. http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
LAPAROSCOPIC COLORECTAL CANCER SURGERY MEASURES
10-2D-143 Policy on the choice of Laparoscopic Colorectal Cancer Surgery (Applicable to all colorectal MDTs)
Laproscopic Surgery is offered to all suitable colorectal cancer patients at William Harvey Hospital. Mr P Basnyat is an established Laparoscopic Colorectal Surgeon (since 2006) and provides Laparoscopic Surgery to all patients allocated to his list. Mr Harinath is currently undertaking Laparoscopic Colorectal Surgery Training. He is registered with LAPCO, which is the National Laparoscopic Training Programme for laparoscopic colorectal surgery. He is expected to offer laparoscopic colorectal surgery by November 2010. All three locum consultants that were appointed at WHH in the last one year were trained in laparoscopic colorectal surgery and were able to offer this service. http://www.kentmedwaycancernetwork.nhs.uk/home-page/for-professionals/colorectal-dog/
10-2D-144 Training in Laparoscopic Colorectal Cancer Surgery (Applicable to all colorectal MDTs)
Mr P Basnyat is an established Laparoscopic Colorectal Surgeon (since 2006) and provides Laparoscopic Surgery to all patients allocated to his list. Mr Basnyat’s training involved 23rd and 24th May 2006 Laparoscopic Colo-rectal Surgery Course at The Royal Surrey County Hospital, 22nd and 23rd June 2006 Colorectal Masterclass Elancourt France and Laparoscopic Colorectal Course 15th and 16th February 2007 at European Surgical Institute Hamburg, Germany. His training was supervised by Mr Henk Wegstapel which included viewing of 10 procedures and performing 4 Laparoscopic Colorectal Surgery under supervision. Mr Harinath is currently undertaking Laparoscopic Colorectal Surgery Training. He is registered with LAPCO, which is the National Laparoscopic Training Programme for laparoscopic colorectal surgery. He is expected to offer laparoscopic colorectal surgery by November 2010.
10-2D-145 Referral Guidelines for Laparoscopic Colorectal Cancer Surgery (Applicable to Colorectal MDTs without trained or exempt members)
Not Applicable as we provide Laparoscopic colorectal Surgery at WHH.
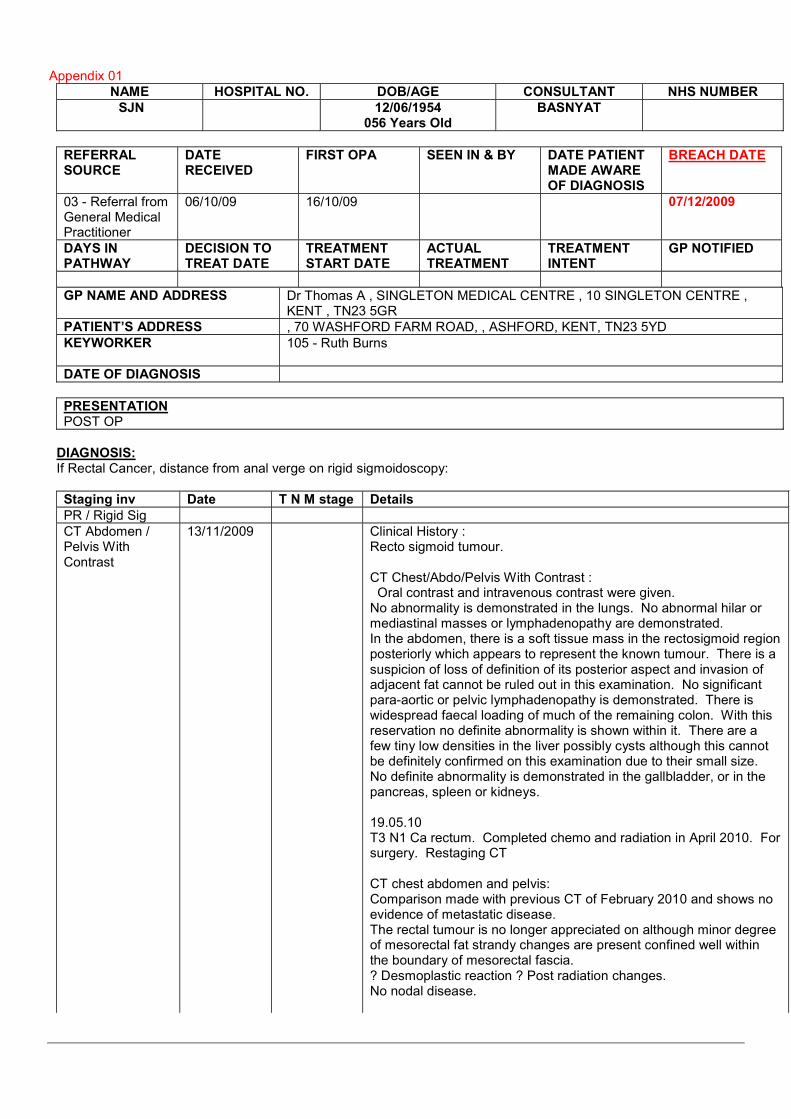
Appendix 01
NAME HOSPITAL NO. DOB/AGE CONSULTANT NHS NUMBER
SJN 12/06/1954 056 Years Old
BASNYAT
REFERRAL SOURCE
DATE RECEIVED
FIRST OPA SEEN IN & BY DATE PATIENT MADE AWARE OF DIAGNOSIS
BREACH DATE
03 - Referral from General Medical Practitioner
06/10/09 16/10/09 07/12/2009
DAYS IN PATHWAY
DECISION TO TREAT DATE
TREATMENT START DATE
ACTUAL TREATMENT
TREATMENT INTENT
GP NOTIFIED
GP NAME AND ADDRESS Dr Thomas A , SINGLETON MEDICAL CENTRE , 10 SINGLETON CENTRE , KENT , TN23 5GR
PATIENT’S ADDRESS , 70 WASHFORD FARM ROAD, , ASHFORD, KENT, TN23 5YD
KEYWORKER 105 - Ruth Burns
DATE OF DIAGNOSIS
PRESENTATION POST OP
DIAGNOSIS: If Rectal Cancer, distance from anal verge on rigid sigmoidoscopy:
Staging inv Date T N M stage Details
PR / Rigid Sig
CT Abdomen / Pelvis With Contrast
13/11/2009 Clinical History : Recto sigmoid tumour. CT Chest/Abdo/Pelvis With Contrast : Oral contrast and intravenous contrast were given. No abnormality is demonstrated in the lungs. No abnormal hilar or mediastinal masses or lymphadenopathy are demonstrated. In the abdomen, there is a soft tissue mass in the rectosigmoid region posteriorly which appears to represent the known tumour. There is a suspicion of loss of definition of its posterior aspect and invasion of adjacent fat cannot be ruled out in this examination. No significant para-aortic or pelvic lymphadenopathy is demonstrated. There is widespread faecal loading of much of the remaining colon. With this reservation no definite abnormality is shown within it. There are a few tiny low densities in the liver possibly cysts although this cannot be definitely confirmed on this examination due to their small size. No definite abnormality is demonstrated in the gallbladder, or in the pancreas, spleen or kidneys. 19.05.10 T3 N1 Ca rectum. Completed chemo and radiation in April 2010. For surgery. Restaging CT CT chest abdomen and pelvis: Comparison made with previous CT of February 2010 and shows no evidence of metastatic disease. The rectal tumour is no longer appreciated on although minor degree of mesorectal fat strandy changes are present confined well within the boundary of mesorectal fascia. ? Desmoplastic reaction ? Post radiation changes. No nodal disease.
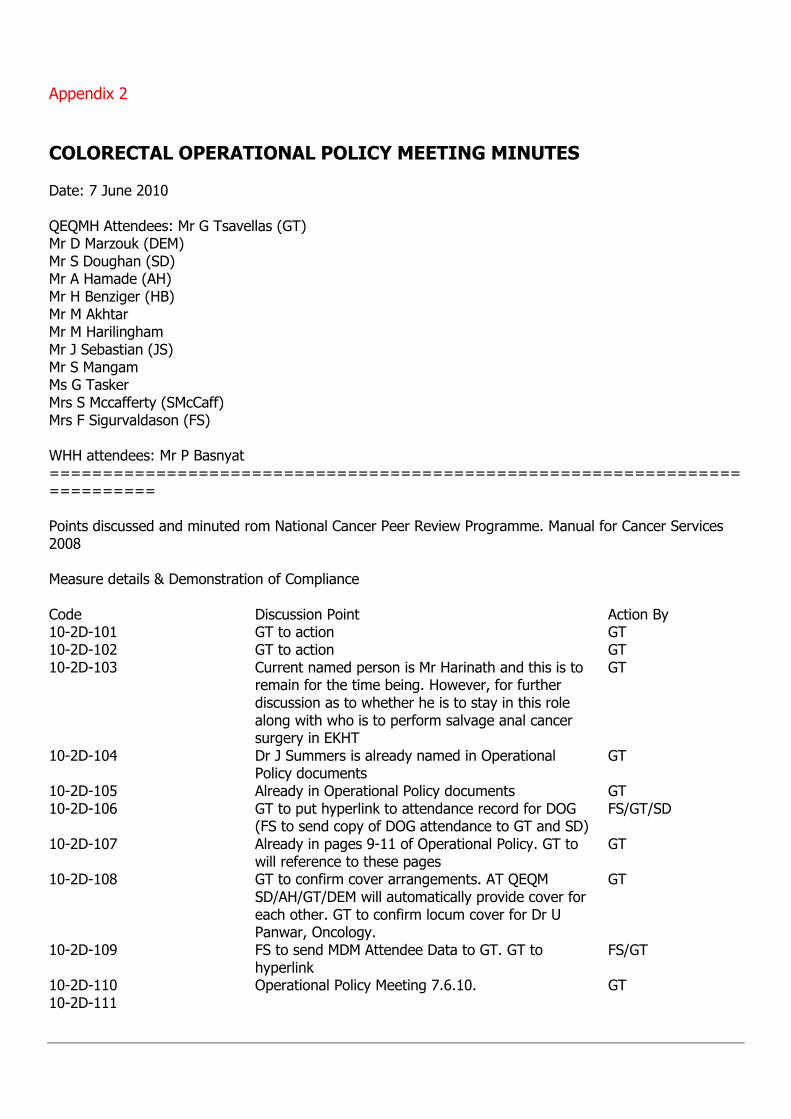
Appendix 2
COLORECTAL OPERATIONAL POLICY MEETING MINUTES Date: 7 June 2010 QEQMH Attendees: Mr G Tsavellas (GT) Mr D Marzouk (DEM) Mr S Doughan (SD) Mr A Hamade (AH) Mr H Benziger (HB) Mr M Akhtar Mr M Harilingham Mr J Sebastian (JS) Mr S Mangam Ms G Tasker Mrs S Mccafferty (SMcCaff) Mrs F Sigurvaldason (FS) WHH attendees: Mr P Basnyat =========================================================================== Points discussed and minuted rom National Cancer Peer Review Programme. Manual for Cancer Services 2008 Measure details & Demonstration of Compliance Code Discussion Point Action By 10-2D-101 GT to action GT 10-2D-102 GT to action GT 10-2D-103 Current named person is Mr Harinath and this is to
remain for the time being. However, for further discussion as to whether he is to stay in this role along with who is to perform salvage anal cancer surgery in EKHT
GT
10-2D-104 Dr J Summers is already named in Operational Policy documents
GT
10-2D-105 Already in Operational Policy documents GT 10-2D-106 GT to put hyperlink to attendance record for DOG
(FS to send copy of DOG attendance to GT and SD) FS/GT/SD
10-2D-107 Already in pages 9-11 of Operational Policy. GT to will reference to these pages
GT
10-2D-108 GT to confirm cover arrangements. AT QEQM SD/AH/GT/DEM will automatically provide cover for each other. GT to confirm locum cover for Dr U Panwar, Oncology.
GT
10-2D-109 FS to send MDM Attendee Data to GT. GT to hyperlink
FS/GT
10-2D-110 Operational Policy Meeting 7.6.10. GT 10-2D-111
10-2D-112 Dissemination of Communicating a Cancer Diagnosis or ‘Peach Forms’. SMcCaff to collate and put in folder for inclusion in Annual Report
SMcCAFF/GT
10-2D-113 Already included in Operational Policy. SMcCaff to confirm
SMcCAFF/GT
10-2D-114 Dr G Vittay to photocopy relevant documents and send to GT to upload
GT
10-2D-115 Already in DOG and Local Policy (SD to provide information on ongoing clinical trials)
GT
10-2D-116 GT to clarify with Network p29 of Operational Policy. Patients are already being referred to St Marks. Not yet agreed with DOG and this needs to be updated. GT to clarify with Network and inform of Local Policy.
GT/Network
10-2D-117 Policy already invoked GT 10-2D-118 SMcCaff to review and feedback to GT SMcCAFF/GT 10-2D-119 SMcCaff to review and feedback to GT SMcCAFF/GT 10-2D-120 Already in Operational Policy document GT 10-2D-121 Ellana McMillen and Dr U Panwar have completed
this. SMcCaff to send link to GT and update team. Commitment to attend through out the year needs to be confirmed. SD to action and put in Work Programme.
SMcCAFF/GT/SD
10-2D-122 Already in Operational Policy document. Sue McCaff has sent updated list to GT. To include Mr A Patel.
SMcCAFF/GT
10-2D-123 SMcCaff/AH to provide GT with 2 or 3 scanned copies of anonomised letters
SMcCAFF/GT/AH
10-2D-124 For inclusion in Annual Report. SD to action SD 10-2D-125 SD to update and put in Annual Report and also
send to GT SD/GT
10-2D-126 Already referenced in Operational Policy but Sue to send updated list to GT
SMcCAFF/GT
10-2D-127 Already in Operational Policy. These are MDM minutes. SMcCaff/FS to provide for GT
SMcCAFF/GT/FS
10-2D-128 Not already covered in any Operational or DOG Policy documents. DOG is to update and provide link to GT. GT has been in contact with Ian Vousden at Network to action. DEM/AH to action protocol with Dr F Muller and provide update to GT.
GT/DEM/AH
10-2D-129 Network to action GT 10-2D-130 Network to action GT 10-2D-131 Network to action. GT and Ian Vousden. GT 10-2D-132 Network to action. GT and Ian Vousden. GT 10-2D-133 Network to action GT 10-2D-134 Referenced to p5 on Operational Policy. Needs
hyperlink to Cancer Waiting Times (PTL). SMcCaff to action PTL with FS. SMcCaff to action Cancer Dataset with Chris Wise. GT to email Ian Vousden with response from SMcCaff.
SMcCAFF/GT/FS
10-2D-135 Already in Operational Policy documentation GT

10-2D-136 Already prepared and presented to DOG by DEM. DEM to send copies to SD and GT for inclusion in documentation. Work Plan to state ongoing continuation of work audit. GT to upload
DEM/SD/GT
10-2D-137 See 136 above 10-2D-138 SD has names to upload in to report. GT has
emailed Dr Panwar. SD/
10-2D-139 See 138 above 10-2D-140 Chris Jacobs has provided data. FS to send to GT
and cc SD for inclusion in Annual Report GT/SD/FS
10-2D-141 Paul Williams (WHH Pathology) to provide diagnosis + surgeon between Jan08-Dec08 and Jan09-Dec09. Also to include Mr Khushal. JS to action.
JS/GT
10-2D-142 Not applicable to Colorectal MDM 10-2D-143 Already on p46 of high level document. To be
further discussed (Laws and Muller) GT
10-2D-144 AH to document and write to relevant Directorate. Core team members are exempt as they have already performed in excess of 20 lap cases and therefore conform. PB to confirm if Mr Harinath has completed the requisite number of lap cases.
AH/PB/GT
10-2D-145 Not applicable to Colorectal MDM
DATE OF NEXT MEETING: TBA
APPENDIX 3
East Kent Hospitals NHS Trust ……………… Hospital
PATIENT REFERRAL FORM FOR COLORECTAL MULTIDISCIPLINARY TEAM MEETING
Name Date of Birth Hospital No. Consultant NHS No.
Current Background/Presenting Features/Reason for referral
Past Medical History Relevant Medication The following test results are required for the meeting:
Test ���� Date Performed if known Ref. No. where known
CT scan
Ultrasound
Barium Enema
MRI
PET Scan
Histology (Please specify)
Other
Request made by ………………………(Print Name)……………………. Date ………………. Position ……………………………………… Please return to: QEQM Fiona O’Neil, MDT Co-ordinator Ext. 65198. WHH Philipa Everard MDT Co-ordinator Ext 84100
(Electronic versions of this form available on request from)
Appendix 4
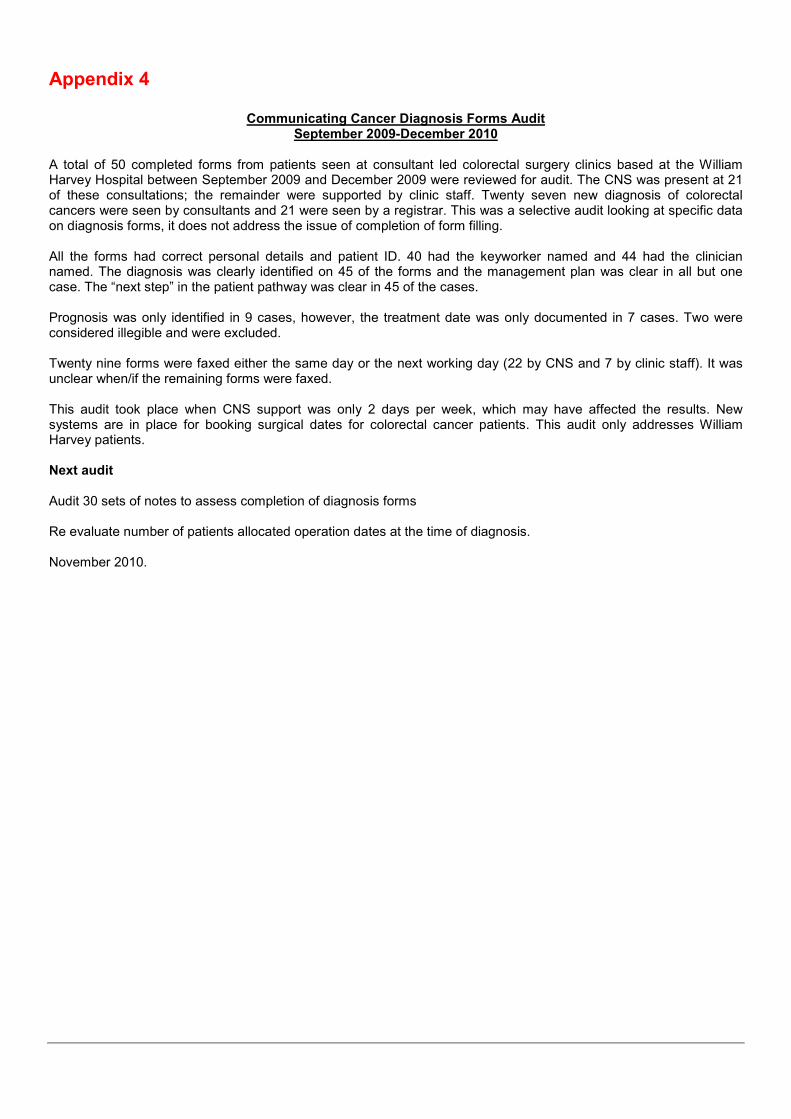
Communicating Cancer Diagnosis Forms Audit September 2009-December 2010
A total of 50 completed forms from patients seen at consultant led colorectal surgery clinics based at the William Harvey Hospital between September 2009 and December 2009 were reviewed for audit. The CNS was present at 21 of these consultations; the remainder were supported by clinic staff. Twenty seven new diagnosis of colorectal cancers were seen by consultants and 21 were seen by a registrar. This was a selective audit looking at specific data on diagnosis forms, it does not address the issue of completion of form filling. All the forms had correct personal details and patient ID. 40 had the keyworker named and 44 had the clinician named. The diagnosis was clearly identified on 45 of the forms and the management plan was clear in all but one case. The “next step” in the patient pathway was clear in 45 of the cases. Prognosis was only identified in 9 cases, however, the treatment date was only documented in 7 cases. Two were considered illegible and were excluded. Twenty nine forms were faxed either the same day or the next working day (22 by CNS and 7 by clinic staff). It was unclear when/if the remaining forms were faxed. This audit took place when CNS support was only 2 days per week, which may have affected the results. New systems are in place for booking surgical dates for colorectal cancer patients. This audit only addresses William Harvey patients. Next audit Audit 30 sets of notes to assess completion of diagnosis forms Re evaluate number of patients allocated operation dates at the time of diagnosis. November 2010.

Appendix 5
2D-218
Colorectal Keyworker Operational Policy East Kent Macmillan Colorectal Clinical Nurse Specialists Contents Introduction The Role of the Key Worker Key Transitional Times in Patient Pathway Allocating the Key Worker for Colorectal Cancer Patients References and Acknowledgements Introduction The concept of a ‘key worker’ for patients’ with a diagnosis of cancer was first identified by the National Institute for Clinical Excellence (NICE) in their ‘Improving Supportive and Palliative Care for Adults with Cancer’ guidance (2004). This guidance defines the key worker as: “Person who, with the patient’s consent and agreement, takes a key role in co-ordinating the patient’s care and promoting continuity, ensuring the patient knows who to access for information and advice.” The Role of the Key Worker The NICE 2004 guidance suggests the key worker role may include:
• ‘Orchestrating assessments to ensure patients’ needs are elicitied
• Ensuring care plans have been agreed with patients
• Ensuring findings from assessments and care plans are communicated to others involved in patient care
• Ensuring patients know who to contact when help or advice is needed, whether this is the key worker or other appropriate personnel
• Mangaing Transition of care’ Key Transitional Times in Patient Pathway ‘Improving Supportive and Palliative Care for Adults with Cancer’ guidance (2004)acknowledges the named key worker is likely to change at key transitional points in the patients’ cancer pathway. Within this guidance seven key points in the patient pathway are indentified:
1. Around the time of diagnosis 2. Commencement of treatment 3. Completion of the primary treatment plan 4. Disease recurrence
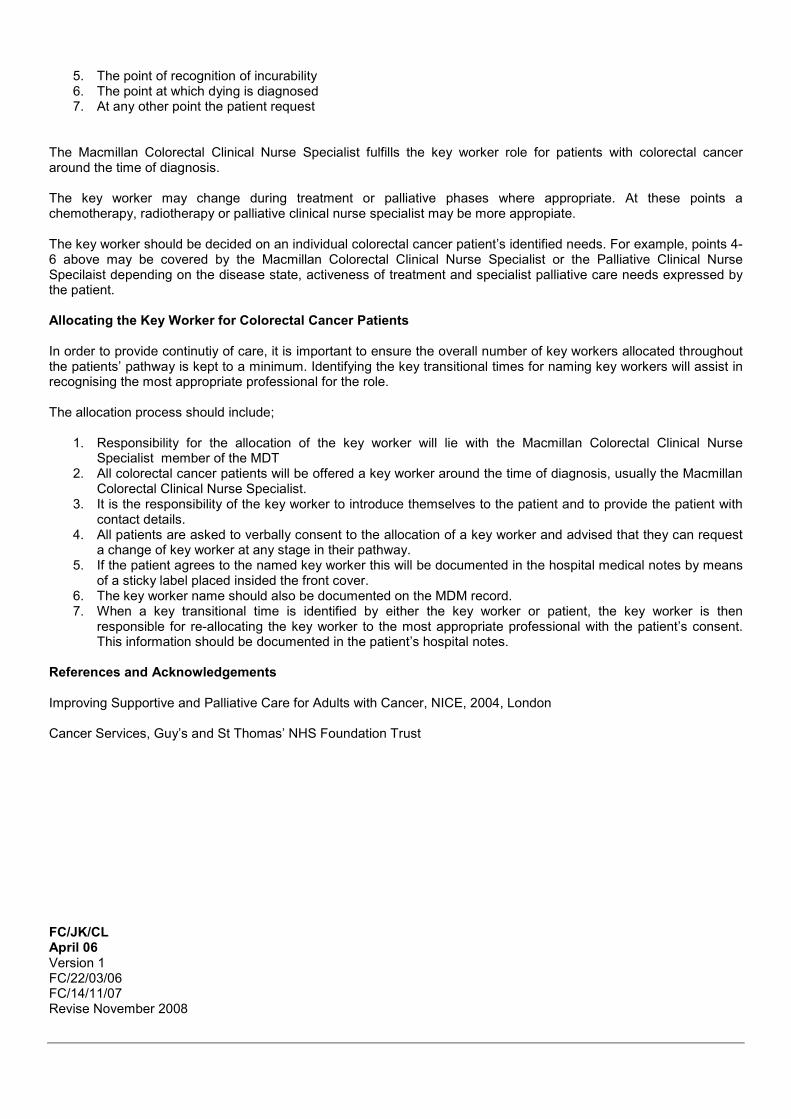
5. The point of recognition of incurability 6. The point at which dying is diagnosed 7. At any other point the patient request
The Macmillan Colorectal Clinical Nurse Specialist fulfills the key worker role for patients with colorectal cancer around the time of diagnosis. The key worker may change during treatment or palliative phases where appropriate. At these points a chemotherapy, radiotherapy or palliative clinical nurse specialist may be more appropiate. The key worker should be decided on an individual colorectal cancer patient’s identified needs. For example, points 4-6 above may be covered by the Macmillan Colorectal Clinical Nurse Specialist or the Palliative Clinical Nurse Specilaist depending on the disease state, activeness of treatment and specialist palliative care needs expressed by the patient. Allocating the Key Worker for Colorectal Cancer Patients In order to provide continutiy of care, it is important to ensure the overall number of key workers allocated throughout the patients’ pathway is kept to a minimum. Identifying the key transitional times for naming key workers will assist in recognising the most appropriate professional for the role. The allocation process should include;
1. Responsibility for the allocation of the key worker will lie with the Macmillan Colorectal Clinical Nurse Specialist member of the MDT
2. All colorectal cancer patients will be offered a key worker around the time of diagnosis, usually the Macmillan Colorectal Clinical Nurse Specialist.
3. It is the responsibility of the key worker to introduce themselves to the patient and to provide the patient with contact details.
4. All patients are asked to verbally consent to the allocation of a key worker and advised that they can request a change of key worker at any stage in their pathway.
5. If the patient agrees to the named key worker this will be documented in the hospital medical notes by means of a sticky label placed insided the front cover.
6. The key worker name should also be documented on the MDM record. 7. When a key transitional time is identified by either the key worker or patient, the key worker is then
responsible for re-allocating the key worker to the most appropriate professional with the patient’s consent. This information should be documented in the patient’s hospital notes.
References and Acknowledgements Improving Supportive and Palliative Care for Adults with Cancer, NICE, 2004, London Cancer Services, Guy’s and St Thomas’ NHS Foundation Trust
FC/JK/CL April 06 Version 1 FC/22/03/06 FC/14/11/07 Revise November 2008
Appendix 6
Name NHS No: Date of MDM: COLORECTAL MULTIDISCIPLINARY MEETING: WILLIAM HARVEY HOSPITAL
NAME HOSPITAL NO. DOB/AGE CONSULTANT NHS NUMBER
REFERRAL SOURCE
DATE RECEIVED
FIRST OPA SEEN IN & BY DATE PATIENT MADE AWARE OF DIAGNOSIS
BREACH DATE
DAYS IN PATHWAY
DECISION TO TREAT DATE
TREATMENT START DATE
ACTUAL TREATMENT
TREATMENT INTENT
GP NOTIFIED
GP NAME AND ADDRESS
PATIENT’S ADDRESS
KEYWORKER
DATE OF DIAGNOSIS
PRESENTATION PREVIOUS HISTORY/FAMILY HISTORY :
DIAGNOSIS: If Rectal Cancer, distance from anal verge on rigid sigmoidoscopy:
Staging inv Date T N M stage Details PR / Rigid Sig
CT Abdomen / Pelvis With Contrast
MRI
Ultrasound Abdomen
Colonoscopy / Flexi Sig
Barium Enema
PET Scan
Other (specify)
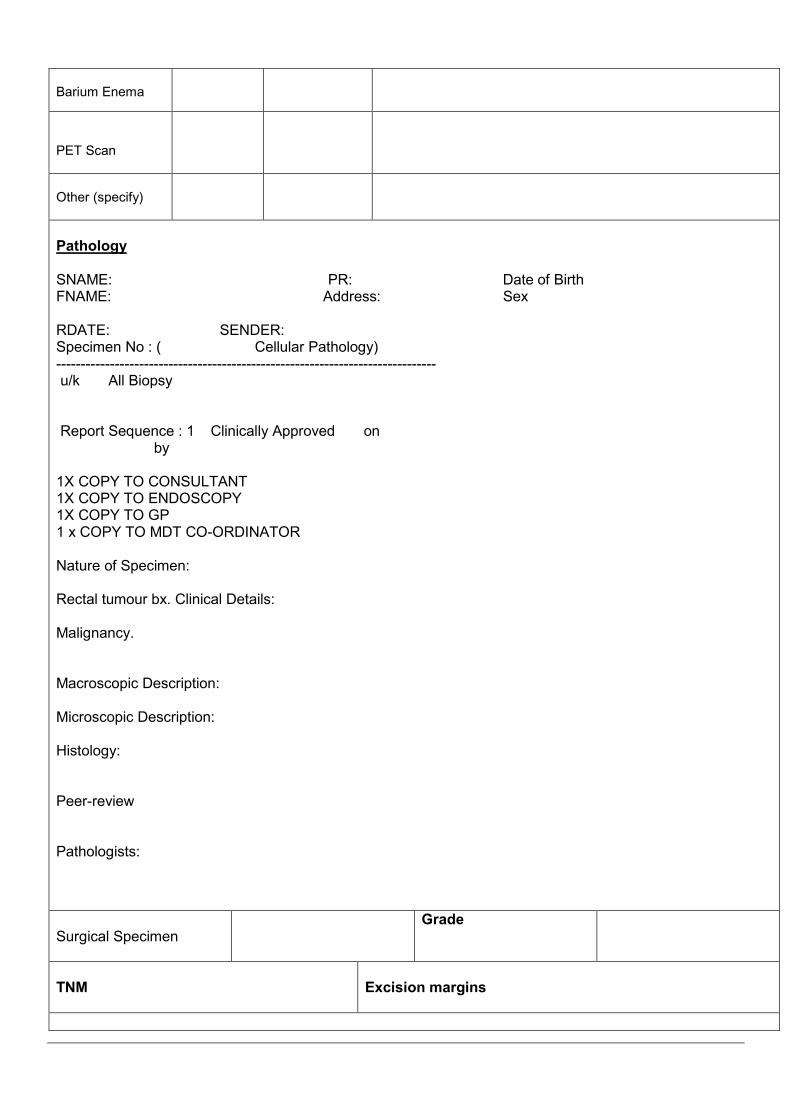
Pathology SNAME: PR: Date of Birth FNAME: Address: Sex RDATE: SENDER: Specimen No : ( Cellular Pathology) ------------------------------------------------------------------------------ u/k All Biopsy Report Sequence : 1 Clinically Approved on by 1X COPY TO CONSULTANT 1X COPY TO ENDOSCOPY 1X COPY TO GP 1 x COPY TO MDT CO-ORDINATOR Nature of Specimen: Rectal tumour bx. Clinical Details: Malignancy. Macroscopic Description: Microscopic Description: Histology: Peer-review Pathologists:
Surgical Specimen
Grade
TNM
Excision margins
Duke's Stage:
Distal clearance
mms
Circumference resection margin:
mms
Number of lymph nodes examined
Number lymph nodes positive
Quirkes’ grading of TME quality:
Doughnuts Distal: Doughnuts Proximal:
MDM ACTIONs
Date of MDM:
Actions:
Managing Consultant’s Signature: ___________________________ Managing Consultant’s Name:
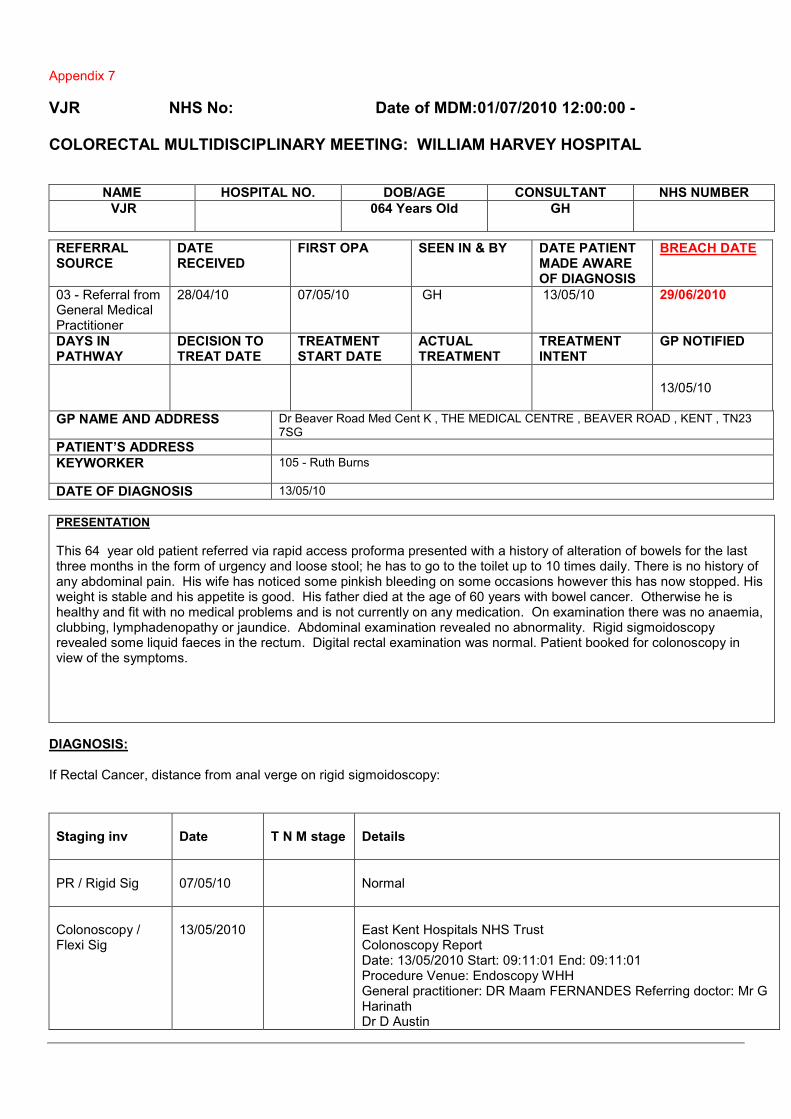
Appendix 7
VJR NHS No: Date of MDM:01/07/2010 12:00:00 - COLORECTAL MULTIDISCIPLINARY MEETING: WILLIAM HARVEY HOSPITAL
NAME HOSPITAL NO. DOB/AGE CONSULTANT NHS NUMBER
VJR 064 Years Old GH
REFERRAL SOURCE
DATE RECEIVED
FIRST OPA SEEN IN & BY DATE PATIENT MADE AWARE OF DIAGNOSIS
BREACH DATE
03 - Referral from General Medical Practitioner
28/04/10 07/05/10 GH 13/05/10 29/06/2010
DAYS IN PATHWAY
DECISION TO TREAT DATE
TREATMENT START DATE
ACTUAL TREATMENT
TREATMENT INTENT
GP NOTIFIED
13/05/10
GP NAME AND ADDRESS Dr Beaver Road Med Cent K , THE MEDICAL CENTRE , BEAVER ROAD , KENT , TN23 7SG
PATIENT’S ADDRESS
KEYWORKER 105 - Ruth Burns
DATE OF DIAGNOSIS 13/05/10
PRESENTATION
This 64 year old patient referred via rapid access proforma presented with a history of alteration of bowels for the last three months in the form of urgency and loose stool; he has to go to the toilet up to 10 times daily. There is no history of any abdominal pain. His wife has noticed some pinkish bleeding on some occasions however this has now stopped. His weight is stable and his appetite is good. His father died at the age of 60 years with bowel cancer. Otherwise he is healthy and fit with no medical problems and is not currently on any medication. On examination there was no anaemia, clubbing, lymphadenopathy or jaundice. Abdominal examination revealed no abnormality. Rigid sigmoidoscopy revealed some liquid faeces in the rectum. Digital rectal examination was normal. Patient booked for colonoscopy in view of the symptoms.
DIAGNOSIS: If Rectal Cancer, distance from anal verge on rigid sigmoidoscopy:
Staging inv
Date
T N M stage
Details
PR / Rigid Sig
07/05/10
Normal
Colonoscopy / Flexi Sig
13/05/2010
East Kent Hospitals NHS Trust Colonoscopy Report Date: 13/05/2010 Start: 09:11:01 End: 09:11:01 Procedure Venue: Endoscopy WHH General practitioner: DR Maam FERNANDES Referring doctor: Mr G Harinath Dr D Austin
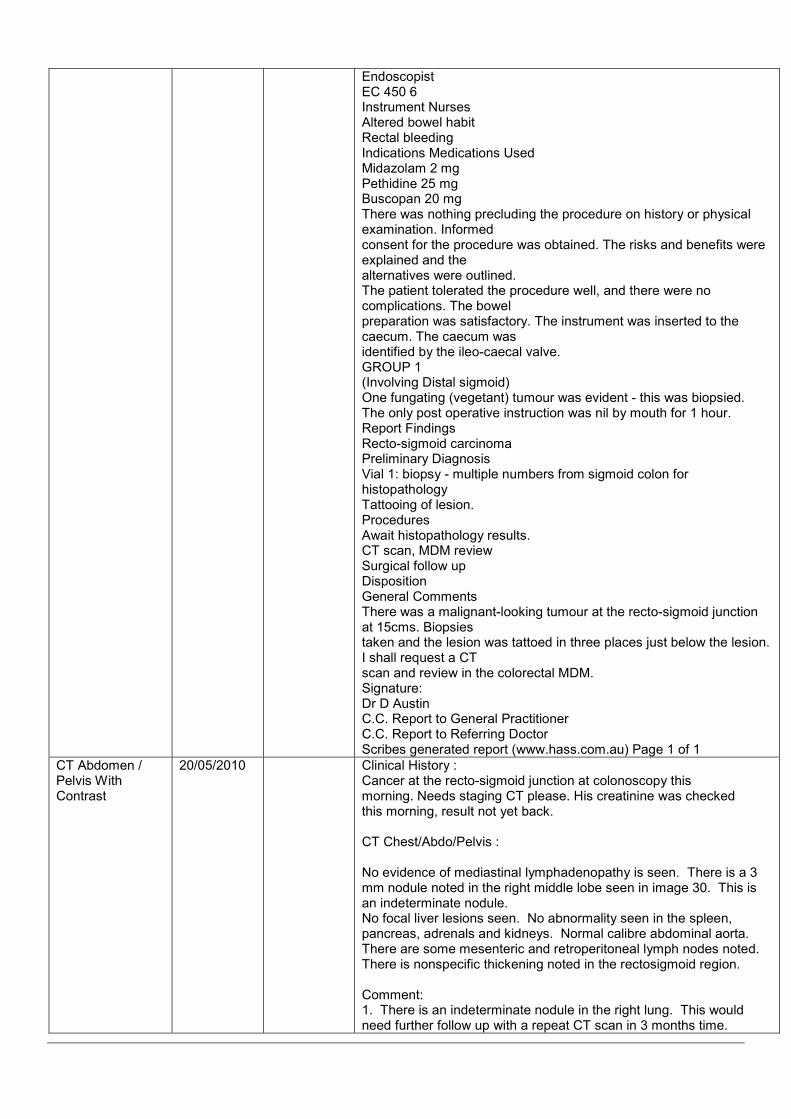
Endoscopist EC 450 6 Instrument Nurses Altered bowel habit Rectal bleeding Indications Medications Used Midazolam 2 mg Pethidine 25 mg Buscopan 20 mg There was nothing precluding the procedure on history or physical examination. Informed consent for the procedure was obtained. The risks and benefits were explained and the alternatives were outlined. The patient tolerated the procedure well, and there were no complications. The bowel preparation was satisfactory. The instrument was inserted to the caecum. The caecum was identified by the ileo-caecal valve. GROUP 1 (Involving Distal sigmoid) One fungating (vegetant) tumour was evident - this was biopsied. The only post operative instruction was nil by mouth for 1 hour. Report Findings Recto-sigmoid carcinoma Preliminary Diagnosis Vial 1: biopsy - multiple numbers from sigmoid colon for histopathology Tattooing of lesion. Procedures Await histopathology results. CT scan, MDM review Surgical follow up Disposition General Comments There was a malignant-looking tumour at the recto-sigmoid junction at 15cms. Biopsies taken and the lesion was tattoed in three places just below the lesion. I shall request a CT scan and review in the colorectal MDM. Signature: Dr D Austin C.C. Report to General Practitioner C.C. Report to Referring Doctor Scribes generated report (www.hass.com.au) Page 1 of 1
CT Abdomen / Pelvis With Contrast
20/05/2010 Clinical History : Cancer at the recto-sigmoid junction at colonoscopy this morning. Needs staging CT please. His creatinine was checked this morning, result not yet back. CT Chest/Abdo/Pelvis : No evidence of mediastinal lymphadenopathy is seen. There is a 3 mm nodule noted in the right middle lobe seen in image 30. This is an indeterminate nodule. No focal liver lesions seen. No abnormality seen in the spleen, pancreas, adrenals and kidneys. Normal calibre abdominal aorta. There are some mesenteric and retroperitoneal lymph nodes noted. There is nonspecific thickening noted in the rectosigmoid region. Comment: 1. There is an indeterminate nodule in the right lung. This would need further follow up with a repeat CT scan in 3 months time.
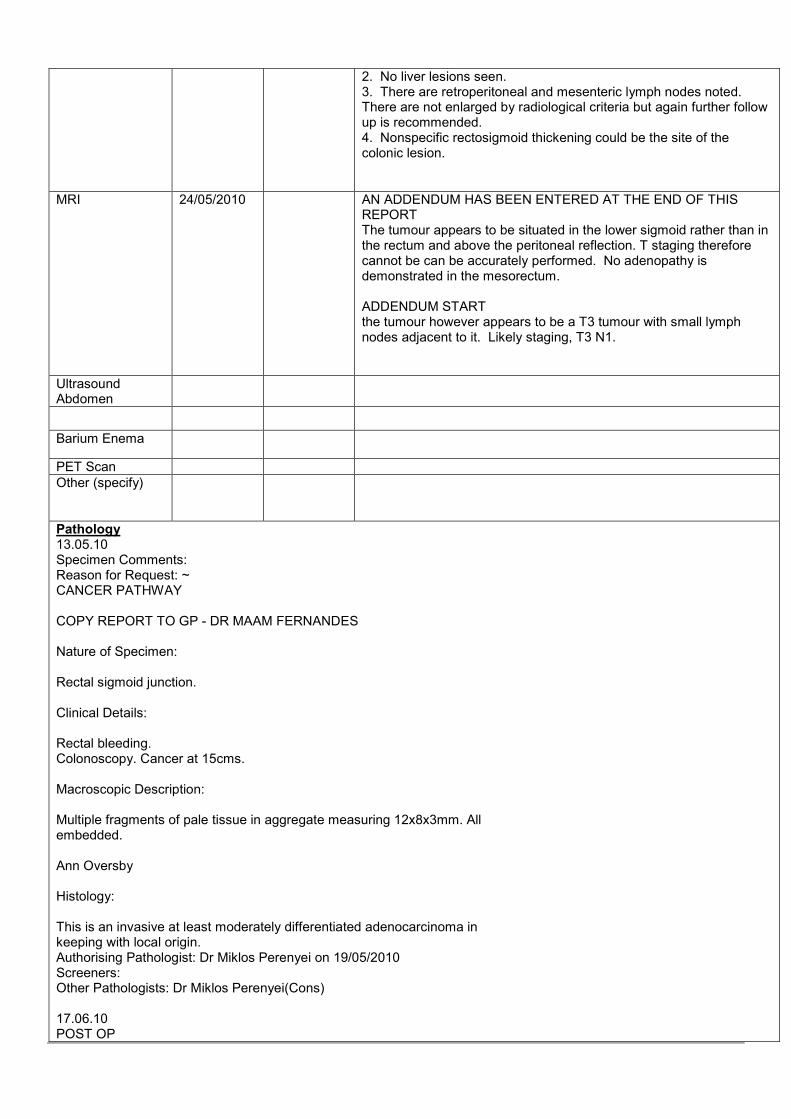
2. No liver lesions seen. 3. There are retroperitoneal and mesenteric lymph nodes noted. There are not enlarged by radiological criteria but again further follow up is recommended. 4. Nonspecific rectosigmoid thickening could be the site of the colonic lesion.
MRI 24/05/2010 AN ADDENDUM HAS BEEN ENTERED AT THE END OF THIS REPORT The tumour appears to be situated in the lower sigmoid rather than in the rectum and above the peritoneal reflection. T staging therefore cannot be can be accurately performed. No adenopathy is demonstrated in the mesorectum. ADDENDUM START the tumour however appears to be a T3 tumour with small lymph nodes adjacent to it. Likely staging, T3 N1.
Ultrasound Abdomen
Barium Enema
PET Scan
Other (specify)
Pathology 13.05.10 Specimen Comments: Reason for Request: ~ CANCER PATHWAY COPY REPORT TO GP - DR MAAM FERNANDES Nature of Specimen: Rectal sigmoid junction. Clinical Details: Rectal bleeding. Colonoscopy. Cancer at 15cms. Macroscopic Description: Multiple fragments of pale tissue in aggregate measuring 12x8x3mm. All embedded. Ann Oversby Histology: This is an invasive at least moderately differentiated adenocarcinoma in keeping with local origin. Authorising Pathologist: Dr Miklos Perenyei on 19/05/2010 Screeners: Other Pathologists: Dr Miklos Perenyei(Cons) 17.06.10 POST OP

Specimen Comments: Reason for Request: ~ East Kent Hospitals Trust COLORECTAL RESECTION HISTOPATHOLOGY REPORT PH _________________________________________________________________________________________________ Surname R Forenames VJ Date of birth NHS No Sex M Clinician GH Name of GP Unknown Clinician Patient location Intensive Treatment Unit Date specimen taken 17/06/2010 Date of receipt 18/06/2010 Hospital No Pathologist Dr Nipin Bagla Hospital William Harvey Hospital _________________________________________________________________________________________________ CLINICAL DETAILS Specimen type Anterior resection Previous biopsy Adenocarcinoma (biopsy No: PH) Rectosigmoid - high ant.resection + part of additional sigmoid resected. NATURE OF SPECIMEN: 1-2 Rectosigmoid. MACROSCOPIC DESCRIPTION: Specimen 1 - sigmoid + rectum - Anterior resection 100 x 20 mm. Whole specimen is above anterior peritoneal reflection. Posterior mesorectal excision is smooth and bulky Quirk 3. Flat superficial ulcerated tumour 20 x 20 x 20 mm is situated 40 mm from distal and 60 mm from proximal margin. Tumour is not stricturing and occupies anterior half of the circumference. On sectioning the tumour invades through the muscularis propria focally. Macroscopically involved lymph nodes are seen which are at least 5 mm from the posterior resection margin. Rest of the bowel is unremarkable. A second piece of fully peritonealised sigmoid colon is present which is 60 mm in length and shows diverticular disease on opening. There is no further tumour. A - distal margin TS, B - distal margin, C, D and E - deepest part of tumour, F and G - lymph nodes closest to posterior RM, H and I - high tie lymph nodes, J to U - node in each block, V to W - the second sigmoid segment. Tissue remains. Specimen 2 - doughnuts - Sutured doughnut 20 mm in diameter. Part embedded in A. Stapled doughnut 16 mm in diameter. Part embedded in B. Dr N Bagla MACROSCOPY Site of tumour Rectum Maximum tumour diameter 20mm Tumour perforation No Distance to nearer cut end 40 mm (not involved) Distance to proximal margin 60 mm (not involved) Distance to distal margin 40 mm (not involved) Relation to peritoneal reflection Above Involves anterior quadrant Yes Mesorectal assessment Mesorectal fascia Location of doughnuts Proximal and Distal Specimen length 100mm MICROSCOPY Tumour type Poorly differentiated - Adenocarcinoma, NOS Local invasion Tumour cells have breached the peritoneal surface
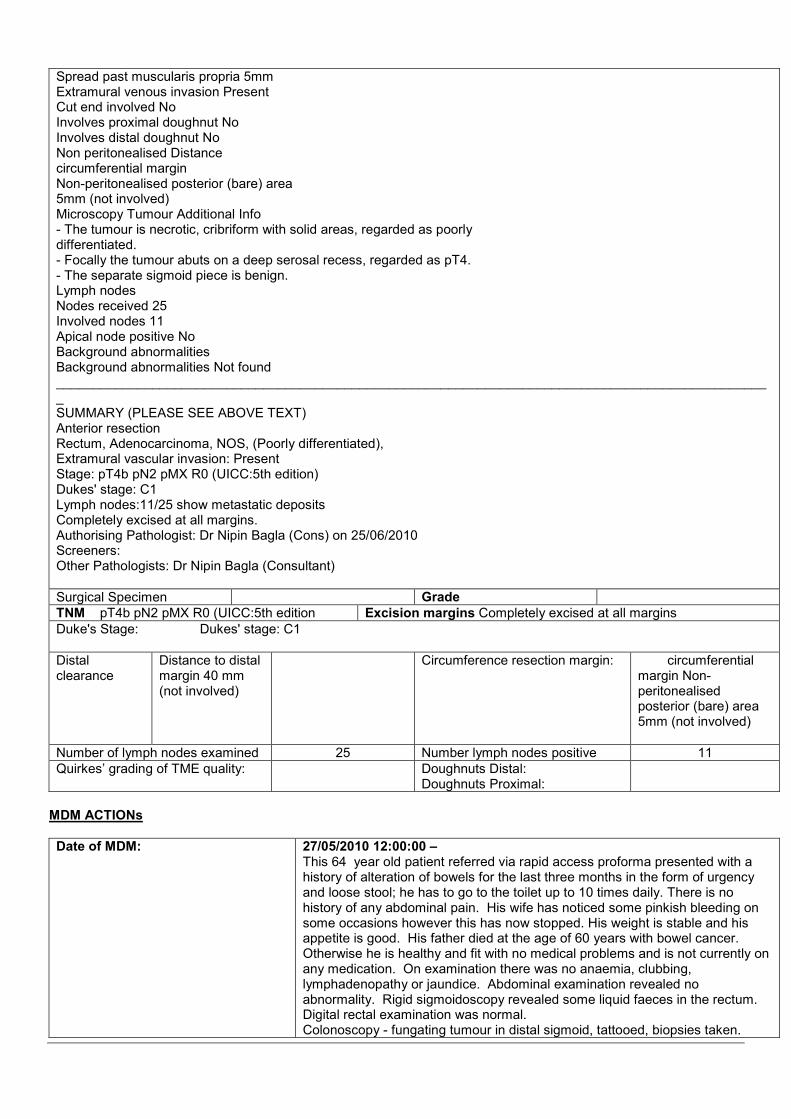
Spread past muscularis propria 5mm Extramural venous invasion Present Cut end involved No Involves proximal doughnut No Involves distal doughnut No Non peritonealised Distance circumferential margin Non-peritonealised posterior (bare) area 5mm (not involved) Microscopy Tumour Additional Info - The tumour is necrotic, cribriform with solid areas, regarded as poorly differentiated. - Focally the tumour abuts on a deep serosal recess, regarded as pT4. - The separate sigmoid piece is benign. Lymph nodes Nodes received 25 Involved nodes 11 Apical node positive No Background abnormalities Background abnormalities Not found _________________________________________________________________________________________________ SUMMARY (PLEASE SEE ABOVE TEXT) Anterior resection Rectum, Adenocarcinoma, NOS, (Poorly differentiated), Extramural vascular invasion: Present Stage: pT4b pN2 pMX R0 (UICC:5th edition) Dukes' stage: C1 Lymph nodes:11/25 show metastatic deposits Completely excised at all margins. Authorising Pathologist: Dr Nipin Bagla (Cons) on 25/06/2010 Screeners: Other Pathologists: Dr Nipin Bagla (Consultant)
Surgical Specimen Grade
TNM pT4b pN2 pMX R0 (UICC:5th edition Excision margins Completely excised at all margins
Duke's Stage: Dukes' stage: C1
Distal clearance
Distance to distal margin 40 mm (not involved)
Circumference resection margin:
circumferential margin Non-peritonealised posterior (bare) area 5mm (not involved)
Number of lymph nodes examined 25 Number lymph nodes positive 11
Quirkes’ grading of TME quality: Doughnuts Distal: Doughnuts Proximal:
MDM ACTIONs
Date of MDM:
27/05/2010 12:00:00 – This 64 year old patient referred via rapid access proforma presented with a history of alteration of bowels for the last three months in the form of urgency and loose stool; he has to go to the toilet up to 10 times daily. There is no history of any abdominal pain. His wife has noticed some pinkish bleeding on some occasions however this has now stopped. His weight is stable and his appetite is good. His father died at the age of 60 years with bowel cancer. Otherwise he is healthy and fit with no medical problems and is not currently on any medication. On examination there was no anaemia, clubbing, lymphadenopathy or jaundice. Abdominal examination revealed no abnormality. Rigid sigmoidoscopy revealed some liquid faeces in the rectum. Digital rectal examination was normal. Colonoscopy - fungating tumour in distal sigmoid, tattooed, biopsies taken.
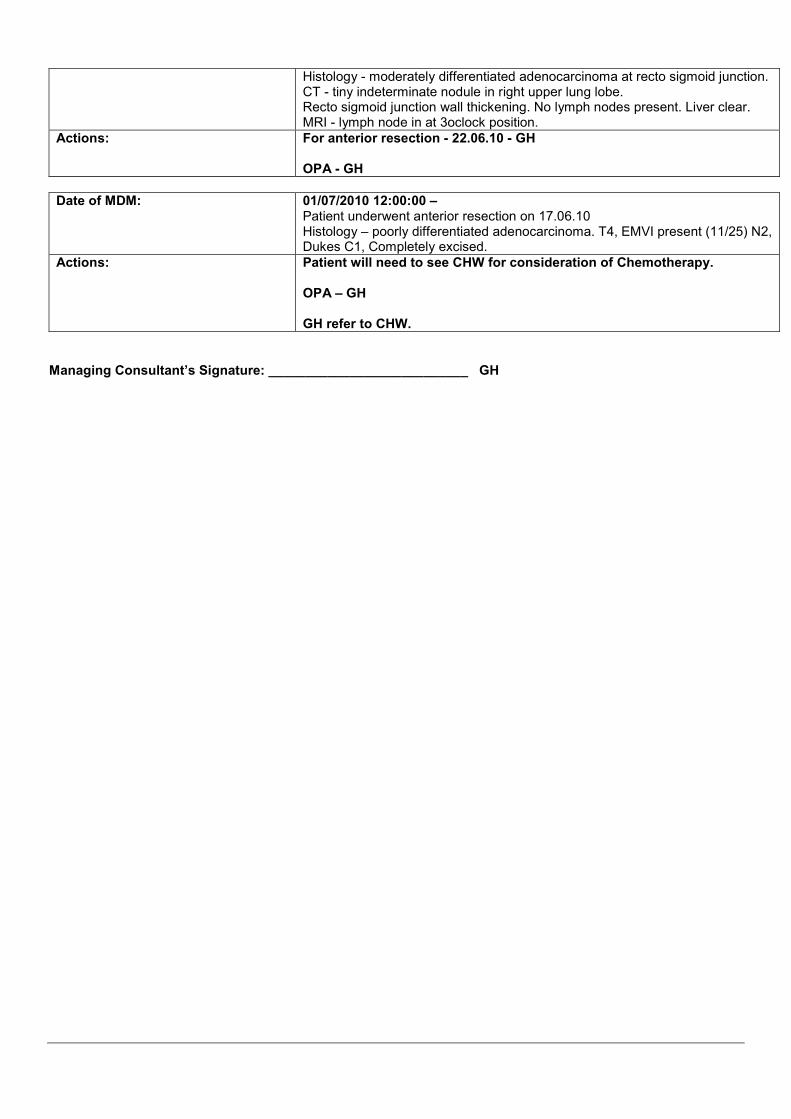
Histology - moderately differentiated adenocarcinoma at recto sigmoid junction. CT - tiny indeterminate nodule in right upper lung lobe. Recto sigmoid junction wall thickening. No lymph nodes present. Liver clear. MRI - lymph node in at 3oclock position.
Actions:
For anterior resection - 22.06.10 - GH OPA - GH
Date of MDM:
01/07/2010 12:00:00 – Patient underwent anterior resection on 17.06.10 Histology – poorly differentiated adenocarcinoma. T4, EMVI present (11/25) N2, Dukes C1, Completely excised.
Actions:
Patient will need to see CHW for consideration of Chemotherapy. OPA – GH GH refer to CHW.
Managing Consultant’s Signature: ___________________________ GH

Appendix 8
Patients With Potentially Resectable Liver Metastasis Extracted from The Management of Bowel Cancer “A Pathway of Care” Kent and Medway Cancer Network 2008
Secondary Care
Tertiary Care (King’s)
Potentially resectable liver mets - refer to King’s
Joint MDM at which King’s surgeons are present (or in discussion with King’s)
Synchronous disease?
Pt has metachronous disease
Follow up
OPERABLE?
Primary tumour removed?
Is synchronous surgery possible?
Is 2-stage surgery possible?
Is primary resectable?
Surgery @ King’s
Has Pt had previous chemotherapy?
OPERABLE?
Offer ChemoRx & Review @ MDM
Offer 2nd line ChemoRx and review @ MDM
? offer non-surgical therapy
Adjuvant ChemoRx
Review & restage by King’s MDT
OPERABLE?
Surgery @ King’s with pre & post operative MDM outcomes sent to referrer
Is surgery available locally?
Surgery @ King’s
Primary surgery performed locally
Adjuvant chemoRx offered locally
N
Y
N
N
N Y
Y
Y
N
Y
N Y
Y
Y
N
N
Y
N Y
N

Appendix 9
Patients With Anal Cancers
Extracted from The Management of Bowel Cancer “A Pathway of Care” Kent and Medway Cancer Network 2008
Secondary Care (Continued from pathway on P4)
MDT
Confirmed Anal Cancer
� Biopsy � Local
excision � EUA
staging
Tertiary Care
Anal Intraepithelial Neoplasia
Local FU
Invasive disease T1N0M0 Anal Margin
Local FU
Others
Refer to MKOC
MDT
Unsuitable for radical treatment
Fit for travel
Palliative radiotherapy
UN-Fit for travel
Suitable for radical treatment
Chemoradiotherapy
Suitable Outpatient
Care
Suitable Inpatient Care
FOLLOW UP - SEE TEXT FOR FULLER DETAILS, INCLUDING SURVEILLANCE.
� Right person at right time in the right place avoiding prolonged & multi-speciality follow up. � Consider consortium follow-up systems that includes Specialist Palliative Care +/- primary / secondary / tertiary care
nurses. � Patients who recur should be fast tracked back into a relevant MDT. � Patients will have unlimited access to specialist nurses within an appropriate setting (Specialist Palliative Care +/-
primary / secondary / tertiary care)
6/52 Clinical Oncologist Review
3/12 Surgical review: EUA + Bx
Salvage APR Persistent disease
Pathological Complete Remission Local FU
Colorectal CNS notification
Specialist Palliative Care
(See text)
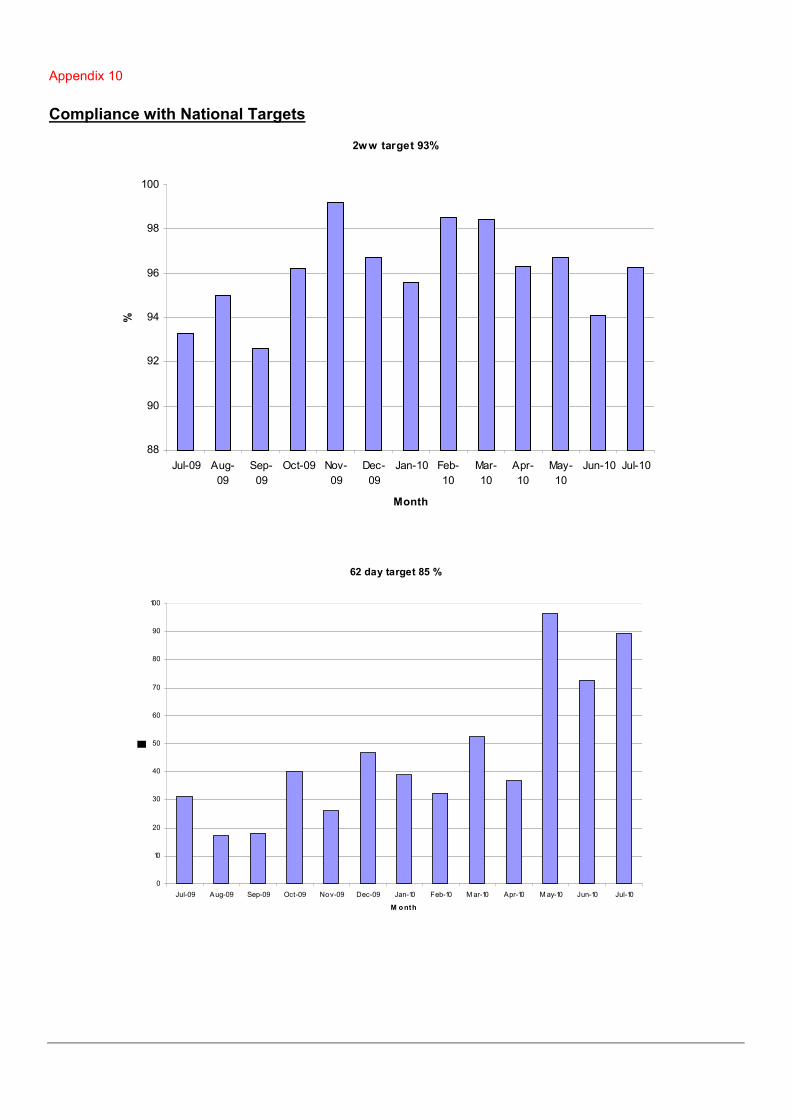
Appendix 10 Compliance with National Targets
2ww target 93%
88
90
92
94
96
98
100
Jul-09 Aug-
09
Sep-
09
Oct-09 Nov-
09
Dec-
09
Jan-10 Feb-
10
Mar-
10
Apr-
10
May-
10
Jun-10 Jul-10
Month
%
62 day target 85 %
0
10
20
30
40
50
60
70
80
90
100
Jul-09 Aug-09 Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 M ar-10 Apr-10 M ay-10 Jun-10 Jul-10
M onth
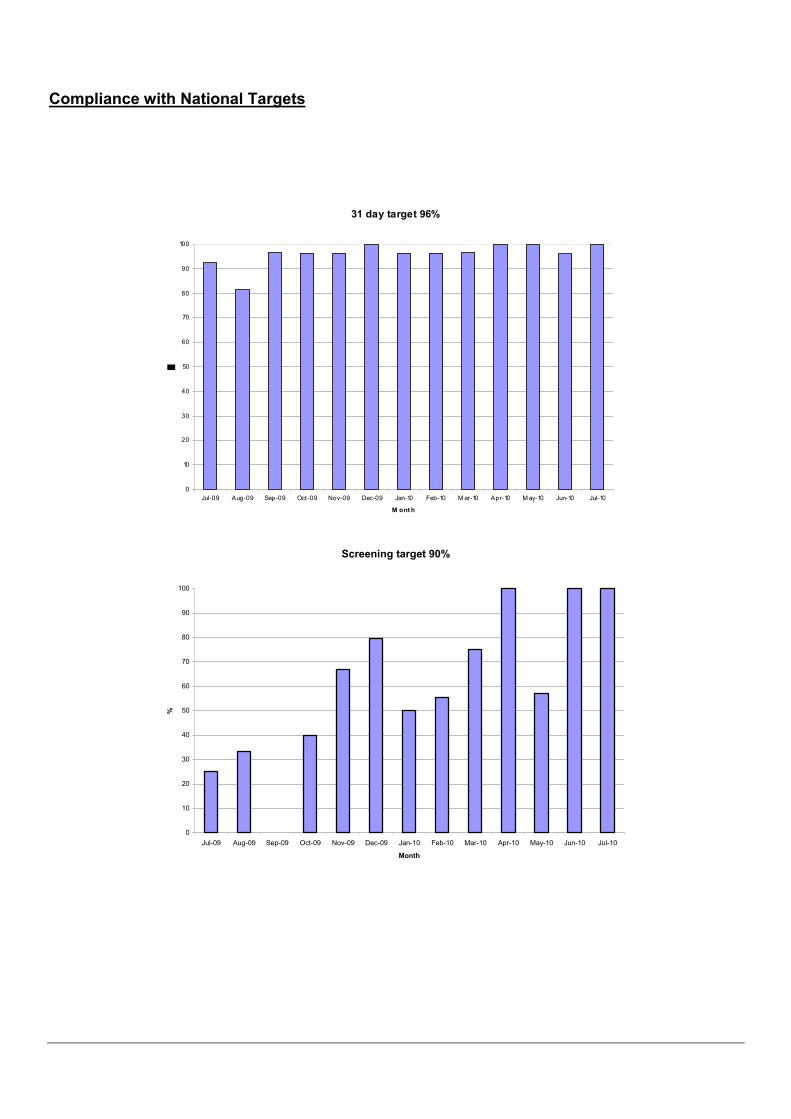
Compliance with National Targets
31 day target 96%
0
10
20
30
40
50
60
70
80
90
100
Jul-09 Aug-09 Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 M ar-10 Apr-10 M ay-10 Jun-10 Jul-10
M ont h
Screening target 90%
0
10
20
30
40
50
60
70
80
90
100
Jul-09 Aug-09 Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 Mar-10 Apr-10 May-10 Jun-10 Jul-10
Month
%

Appendix 11
Actual (01/04/2010 - 30/06/2010) vs Forecast Recruitment (01/04/2010 - 31/03/2011)
Study Acronym D&G EKHUFT MTW MFT
Network Actual Recruitment Qtr 1
Actual recruitment Qtr 1
Forecast recruitment 12 months
Actual recruitment Qtr 1
Forecast recruitment 12 months
Actual recruitment Qtr 1
Forecast recruitment 12 months
Actual recruitment Qtr 1
Forecast recruitment 12 months
Actual recruitment Qtr 1
COIN B 2 1
CREST 0 1
ENROL 5 1
FOCUS3 2 12
FOXTROT 0 3
NEW EPOC 0 4
PICCOLO 3 2 1 2
SCOT 3 3 0 3 3 5 0 1
Total RCT 5 5 3 5 6 26 5 2
NSCCG 0 10 0 6 0 12 0 8
Total Non RCT 0 10 0 6 0 12 0 8
Overall Total 5 15 3 11 6 38 5 10







