
Genes, Brain and Behavior (2011) 10: 418–423 doi: 10.1111/j.1601-183X.2011.00680.x
Bipolar disorder risk alleles in adult ADHD patients
E. T. Landaas†,‡,§, S. Johansson†,‡,§,A. Halmøy†,‡,††, K. J. Oedegaard‡,∗∗,††,O. B. Fasmer‡,∗∗,†† and J. Haavik∗,†,‡,††
†Department of Biomedicine, University of Bergen, ‡K.G.Jebsen Centre for Research on Neuropsychiatric Disorders,University of Bergen §Centre of Medical Genetics andMolecular Medicine, Haukeland University Hospital,**Department of Clinical Medicine, Section for Psychiatry,Faculty of Medicine, University of Bergen, and ††Division ofPsychiatry, Haukeland University Hospital, Bergen, Norway*Corresponding author: J. Haavik, Department of Biomedicine,University of Bergen, Bergen, Norway.E-mail: [email protected]
Attention-deficit/hyperactivity disorder (ADHD) has an
estimated prevalence of 3–5% in adults. Genome-wide
association (GWA) studies have not been performed
in adults with ADHD and studies in children have so
far been inconclusive, possibly because of the small
sample sizes. Larger GWA studies have been performed
on bipolar disorder (BD) and BD symptoms, and several
potential risk genes have been reported. ADHD and BD
share many clinical features and comorbidity between
these two disorders is common. We therefore wanted
to examine whether the reported BD genetic variants
in CACNA1C, ANK3, MYO5B, TSPAN8 and ZNF804A
loci are associated with ADHD or with scores on the
Mood Disorder Questionnaire (MDQ), a commonly used
screening instrument for bipolar spectrum disorders. We
studied 561 adult Norwegian ADHD patients and 711
controls from the general population. No significant
associations or trends were found between any of
the single nucleotide polymorphisms (SNPs) studied
and ADHD [odds ratios (ORs) ≤ 1.05]. However, a weak
association was found between rs1344706 in ZNF804A
(OR = 1.25; P = 0.05) and MDQ. In conclusion, it seems
unlikely that these six SNPs with strong evidence of
association in BD GWA studies are shared risk variants
between ADHD and BD.
Keywords: ADHD, ANK3, BD, CACNA1C, genetics, GWAstudies, MDQ, MYO5B, TSPAN8, ZNF804A
Received 21 October 2010, revised 11 January 2011,accepted for publication 25 January 2011
Attention-deficit/hyperactivity disorder (ADHD) is a neuropsy-chiatric disorder characterized by hyperactivity, impulsivityand inattention. Initially it was considered a childhood condi-tion, but it has become increasingly evident that symptoms
frequently persist into adulthood (Faraone et al. 2006), andthe prevalence of ADHD has been estimated to be inthe range of 3–5% in adults (Fayyad et al. 2007; Kessleret al. 2006).
Affective symptoms are common in adult ADHD patients,constitute an important feature of the disorder (Reimherret al. 2005), and it has been suggested that such symptomsshould be among the diagnostic criteria in adults (Wenderet al. 1981). Comorbidity with other psychiatric disorders isalso common in adult ADHD patients (Haavik et al. 2010;Mcgough et al. 2005; Sobanski et al. 2007), and one of thefrequently reported co-occurring diagnoses is bipolar disor-der (BD) (Wingo & Ghaemi 2007). In addition to affectivesymptoms, individuals with BD and ADHD show overlappingsymptoms such as impaired impulse control and dysreg-ulation of energy and activity levels (Skirrow et al. 2009).We have previously reported that approximately 12% of ouradult ADHD patients have self-reported comorbidity with BD(Halmoy et al. 2010). However, 51% of the patients screenedpositive on the Mood Disorder Questionnaire (MDQ), ascreening instrument for bipolar spectrum disorders (BSD)(Hirschfeld et al. 2000), showing that symptoms of maniaand hypomania are highly prevalent in adult ADHD patientsalso in the absence of a diagnosed BD. Neuroimaging studiesare also compatible with partially overlapping pathogeneticmechanisms in these conditions (Passarotti et al. 2010).
The heritability of childhood ADHD has been estimatedto be about 76% (Faraone et al. 2005). Although many link-age and candidate association studies have been performedin the search for susceptibility genes, findings have beeninconsistent and contradictory (Franke et al. 2009). Overrecent years, genome-wide association (GWA) studies haveresulted in a large number of genetic variants showing highlysignificant associations with traits in several medical spe-cialities (McCarthy 2010; Teslovich et al. 2010), althoughoften with relatively modest effect sizes. However, concern-ing ADHD, no gene region has been established at wholegenome significance so far (Franke et al. 2009). Althoughprogress has been slow even for most other common com-plex mental disorders, there have been some promisingresults, especially in BD, where the numbers of samplesstudied have been considerably larger than for ADHD.
As both BD and ADHD are highly heritable and often co-occur within families (Birmaher et al. 2010; Faraone et al.1997), one could hypothesize that the two disorders mightshare some common genetic risk factors (Hegerl et al. 2010).The aim of this study was to examine whether singlenucleotide polymorphism (SNP) alleles found associatedwith BD through recent GWA studies are more commonin patients with persistent ADHD than in controls recruitedfrom the general population. We chose to study six SNPs,of which five are located in or near the genes encodingankyrinG (ANK3) (Ferreira et al. 2008), myosin5B (MYO5B),
418 © 2011 The AuthorsGenes, Brain and Behavior © 2011 Blackwell Publishing Ltd and International Behavioural and Neural Genetics Society

Bipolar disorder risk alleles in adult ADHD patients
tetraspanin-8 (TSPAN8) and the alpha 1C subunit of anL-type voltage-dependent calcium channel (CACNA1C) (Sklaret al. 2008). The sixth SNP is located in the zinc fingerprotein 804A gene (ZNF804A), a gene that was first foundassociated with schizophrenia in a GWA study, but wasfurther found associated with BD, because the P-valuebecame genome-wide significant only after individuals withBD were included in the original patient sample (O’Donovanet al. 2008). Additionally, we wanted to test if there was anyassociation between these SNPs and scores on the MDQ.
Material and methods
SubjectsOur sample consists of 1272 Caucasians of Norwegian ancestry, allof more than 18 years of age. Of these, 561 were patients diagnosedwith ADHD according to ICD-10 research criteria (World HealthOrganization 1993), with two modifications: allowing the inattentivesubtype in DSM-IV as sufficient for the diagnosis and allowing for thepresence of comorbid psychiatric disorders, as long as the criteria forADHD were present before the appearance of the comorbid disorder(Johansson et al. 2008). These diagnostic criteria are very similarto the DSM-IV criteria for ADHD (American Psychiatric Association2000). The majority of the patients were recruited by responding toan invitation sent by letter to their addresses, as listed in a Norwegiannational registry of adult ADHD patients. The remainder was recruiteddirectly from psychiatrists or out-patient clinics (Johansson et al.2008). Patients who reported mental retardation were excludedfrom analyses. The control group consisted of 711 volunteers fromthe general population (aged 18–40 years) recruited from all acrossNorway for the purpose of this study (described in Halmoy et al.2010). Controls were unselected, i.e. no controls were excludedbased on the presence of life-time psychiatric disorders or otherrelated traits. A written informed consent was obtained from allparticipants and the study was approved by the Norwegian RegionalMedical Research Ethics Committee West IRB #3 (FWA00009490,IRB00001872).
MeasuresAll participants returned a questionnaire, where current and life-timepsychiatric morbidity was reported (Halmøy et al. 2010). Additionally,they filled in the MDQ, which is a screening instrument designed tofacilitate the recognition of BSD (Hirschfeld et al. 2000). A positivescore is defined as ≥7 (of 13) positive items concerning life-timesymptoms of mania and hypomania, co-occurrence of at least two ofthese symptoms and functional impairment caused by the symptomsrated as moderate to severe. MDQ has been validated for use in bothhealthy and psychiatrically ill individuals (Hirschfeld et al. 2000, 2003).For the quantitative MDQ analyses, all individuals with missing itemswere excluded, resulting in analyses of 503 ADHD patients (90%)and 681 controls (96%). A few individuals fulfilled the criteria forMDQ positive or negative despite having missing items, and thusthe dichotomous MDQ analyses included 517 ADHD patients (92%)and 691 controls (97%).
SNP selection and genotypingSelection of SNPs was based on a literature search as of January2010. SNPs that had been emphasized as likely to be associatedwith BD, at a level of genome-wide significance (P < 5.0 × 10−8)or near such values, either in BD GWA studies alone [rs9804190(Schulze et al. 2009); rs10994336 (Ferreira et al. 2008); rs1006737,rs1705236 and rs4939921 (Sklar et al. 2008)] or in combination withschizophrenia cases [rs1344706 in ZNF804A (O’Donovan et al. 2008)]were selected as candidates for genotyping in our sample. Only oneSNP, with the strongest P-value, was chosen for each locus tolimit multiple testing issues, except for the ANK3 locus where two
SNPs were selected as studies have pointed to two independentsignals. The DGKH (diacylglycerol kinase eta) SNP rs1012053 (Baumet al. 2008) failed in assay design and was not included in theanalysis.
Samples of either whole blood or saliva were obtained fromall participants, and the Oragene™ DNA Self-Collection Kit (DNAGenotek Inc., Ontario, Canada) was used for DNA extraction. TheDNA was aliquoted into 96-well plates, each of which contained DNAfrom both cases and controls and a minimum of two blank samplesand two internal controls. SNP genotyping was performed using theMassARRAY iPLEX System (Sequenom, San Diego, CA, USA). Thegenotyping rate was ≥0.99 for all SNPs, and the concordance rate,found through use of internal controls and duplicates, was 100%.
Statistical analysesThe clinical data and the distribution of the MDQ scores wereanalysed with descriptive methods using χ2 tables and t-testsperformed by the Statistical Package for Social Sciences version15.0.1 (SPSS Inc, Chicago, IL, USA). The genetic statistical analyseswere performed with the PLINK software version 1.07 (Purcell et al.2007), based on an additive allelic model and using linear/logisticregression with gender and ADHD status as covariates. Genotypedistributions for all SNPs were consistent with Hardy–Weinbergequilibrium, P ≥ 0.05. For the MassARRAY iPLEX analysis, twoindividuals were excluded because of low genotyping efficiency(missingness >0.3). These were further excluded from all clinicaland genetic analyses. All odds ratio (OR) estimates are presentedfor the allele found associated with increased BD risk in the BDGWA studies. A two-tailed level of P < 0.05 was chosen for nominalsignificance, and all P-values are presented without correction formultiple testing.
Power calculations in the total sample were performed with thegenetic power calculator (http://pngu.mgh.harvard.edu/∼purcell/gpc/cc2.html), using a disease prevalence of 0.034 for adult ADHD, asignificance level of 0.05 and assuming an additive allelic model. Weused the allele frequencies detected in our control sample, and theORs were obtained from the original GWA studies.
Results
Clinical characteristics of the sample
Sociodemographic and clinical characteristics of the 561 adultADHD patients and 711 controls from the general populationare summarized in Table 1. Significantly more patients thancontrols reported life-time episodes of depression or anxiety,with a frequency of 68.5% among the patients and 14.2% inthe control group. BD, problems with alcohol and problems
Table 1: Clinical characteristics of the sample
ADHD patients Controls
N 561 711Males, % (N) 51.7 (290) 40.1 (285)Age (SD) 34.1 (10.4) 29.6 (6.5)MDQ score, mean (SE)∗ 8.1 (0.18) 2.9 (0.12)MDQ positive, % (N)† 48.7 (252) 6.1 (42)Self-reported morbidity, % (N)
Depression/Anxiety 68.5 (401) 14.2 (128)BD 11.2 (63) 1.1 (10)Alcohol problems 23.1 (135) 2.1 (19)Problems with illegal drugs 26.4 (155) 2.2 (20)
∗Five hundred and three patients and 681 controls with nomissing items.†In total, 517 cases and 691 controls.
Genes, Brain and Behavior (2011) 10: 418–423 419
Landaas et al.
with illegal drugs were also much more common in theADHD group than among the controls. ADHD patients scoredsignificantly higher than controls on the MDQ, with a meanscore of 8.1 in the patients and 2.9 in the controls; 48.7%of the patients and 6.1% of the controls were classified asMDQ positive.
Genetic analyses
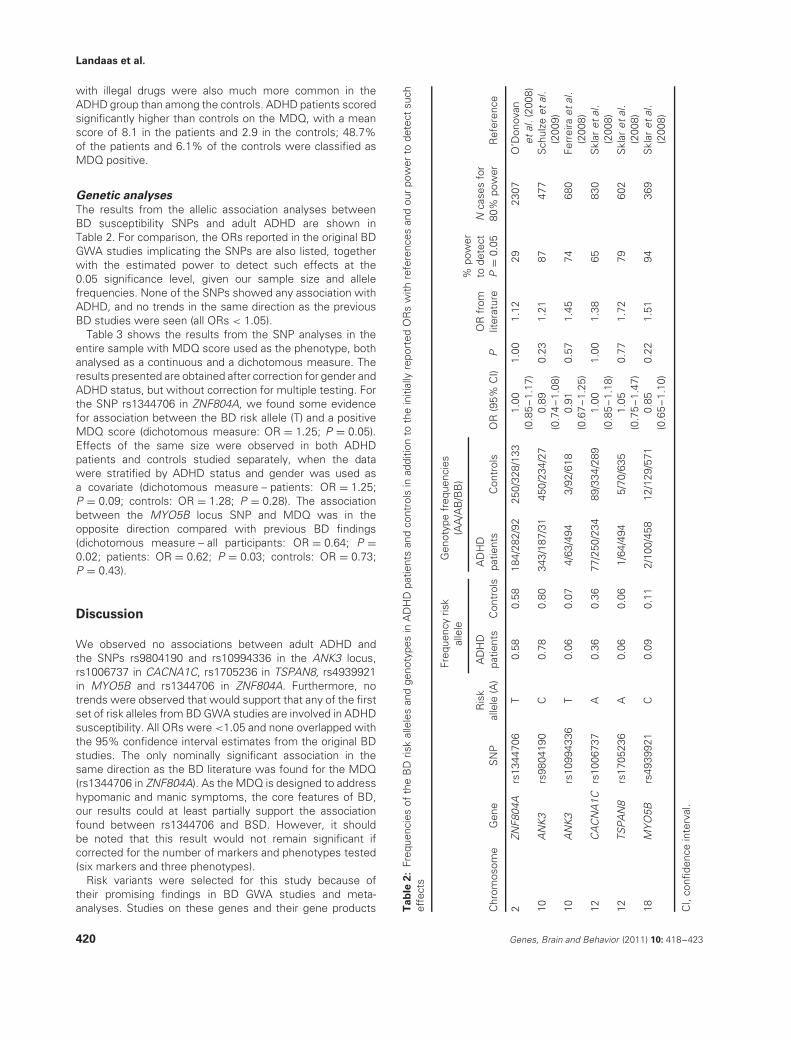
The results from the allelic association analyses betweenBD susceptibility SNPs and adult ADHD are shown inTable 2. For comparison, the ORs reported in the original BDGWA studies implicating the SNPs are also listed, togetherwith the estimated power to detect such effects at the0.05 significance level, given our sample size and allelefrequencies. None of the SNPs showed any association withADHD, and no trends in the same direction as the previousBD studies were seen (all ORs < 1.05).
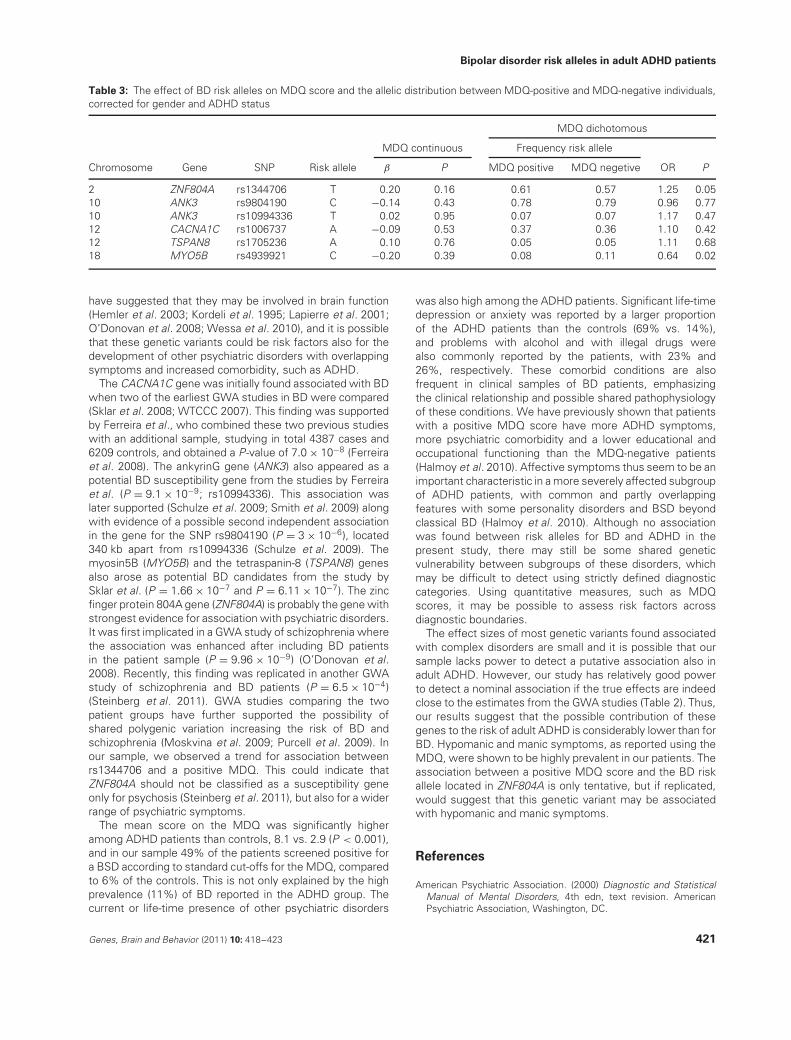
Table 3 shows the results from the SNP analyses in theentire sample with MDQ score used as the phenotype, bothanalysed as a continuous and a dichotomous measure. Theresults presented are obtained after correction for gender andADHD status, but without correction for multiple testing. Forthe SNP rs1344706 in ZNF804A, we found some evidencefor association between the BD risk allele (T) and a positiveMDQ score (dichotomous measure: OR = 1.25; P = 0.05).Effects of the same size were observed in both ADHDpatients and controls studied separately, when the datawere stratified by ADHD status and gender was used asa covariate (dichotomous measure – patients: OR = 1.25;P = 0.09; controls: OR = 1.28; P = 0.28). The associationbetween the MYO5B locus SNP and MDQ was in theopposite direction compared with previous BD findings(dichotomous measure – all participants: OR = 0.64; P =0.02; patients: OR = 0.62; P = 0.03; controls: OR = 0.73;P = 0.43).
Discussion
We observed no associations between adult ADHD andthe SNPs rs9804190 and rs10994336 in the ANK3 locus,rs1006737 in CACNA1C, rs1705236 in TSPAN8, rs4939921in MYO5B and rs1344706 in ZNF804A. Furthermore, notrends were observed that would support that any of the firstset of risk alleles from BD GWA studies are involved in ADHDsusceptibility. All ORs were <1.05 and none overlapped withthe 95% confidence interval estimates from the original BDstudies. The only nominally significant association in thesame direction as the BD literature was found for the MDQ(rs1344706 in ZNF804A). As the MDQ is designed to addresshypomanic and manic symptoms, the core features of BD,our results could at least partially support the associationfound between rs1344706 and BSD. However, it shouldbe noted that this result would not remain significant ifcorrected for the number of markers and phenotypes tested(six markers and three phenotypes).
Risk variants were selected for this study because oftheir promising findings in BD GWA studies and meta-analyses. Studies on these genes and their gene products T
ab
le2
:Fr
eque
ncie
sof
the
BD
risk
alle
les
and
geno
type
sin
AD
HD
patie
nts
and
cont
rols
inad
ditio
nto
the
initi
ally
repo
rted
OR
sw
ithre
fere
nces
and
our
pow
erto
dete
ctsu
chef
fect
s
Freq
uenc
yris
kal
lele
Gen
otyp
efr
eque
ncie
s(A
A/A
B/B
B)
Chr
omos
ome
Gen
eS
NP
Ris
kal
lele
(A)
AD
HD
patie
nts
Con
trol
sA
DH
Dpa
tient
sC
ontr
ols
OR
(95%
CI)
PO
Rfr
omlit
erat
ure
%po
wer
tode
tect
P=
0.05
Nca
ses
for
80%
pow
erR
efer
ence
2ZN
F804
Ars
1344
706
T0.
580.
5818
4/28
2/92
250/
328/
133
1.00
(0.8
5–1
.17)
1.00
1.12
2923
07O
’Don
ovan
etal
.(20
08)
10A
NK3
rs98
0419
0C
0.78
0.80
343/
187/
3145
0/23
4/27
0.89
(0.7
4–1
.08)
0.23
1.21
8747
7S
chul
zeet
al.
(200
9)10
AN
K3rs
1099
4336
T0.
060.
074/
63/4
943/
92/6
180.
91(0
.67
–1.2
5)0.
571.
4574
680
Ferr
eira
etal
.(2
008)
12C
AC
NA
1Crs
1006
737
A0.
360.
3677
/250
/234
89/3
34/2
891.
00(0
.85
–1.1
8)1.
001.
3865
830
Skl
aret
al.
(200
8)12
TSPA
N8
rs17
0523
6A
0.06
0.06
1/64
/494
5/70
/635
1.05
(0.7
5–1
.47)
0.77
1.72
7960
2S
klar
etal
.(2
008)
18M
YO5B
rs49
3992
1C
0.09
0.11
2/10
0/45
812
/129
/571
0.85
(0.6
5–1
.10)
0.22
1.51
9436
9S
klar
etal
.(2
008)
CI,
confi
denc
ein
terv
al.
420 Genes, Brain and Behavior (2011) 10: 418–423
Bipolar disorder risk alleles in adult ADHD patients
Table 3: The effect of BD risk alleles on MDQ score and the allelic distribution between MDQ-positive and MDQ-negative individuals,corrected for gender and ADHD status
MDQ dichotomous
MDQ continuous Frequency risk allele
Chromosome Gene SNP Risk allele β P MDQ positive MDQ negetive OR P
2 ZNF804A rs1344706 T 0.20 0.16 0.61 0.57 1.25 0.0510 ANK3 rs9804190 C −0.14 0.43 0.78 0.79 0.96 0.7710 ANK3 rs10994336 T 0.02 0.95 0.07 0.07 1.17 0.4712 CACNA1C rs1006737 A −0.09 0.53 0.37 0.36 1.10 0.4212 TSPAN8 rs1705236 A 0.10 0.76 0.05 0.05 1.11 0.6818 MYO5B rs4939921 C −0.20 0.39 0.08 0.11 0.64 0.02
have suggested that they may be involved in brain function(Hemler et al. 2003; Kordeli et al. 1995; Lapierre et al. 2001;O’Donovan et al. 2008; Wessa et al. 2010), and it is possiblethat these genetic variants could be risk factors also for thedevelopment of other psychiatric disorders with overlappingsymptoms and increased comorbidity, such as ADHD.
The CACNA1C gene was initially found associated with BDwhen two of the earliest GWA studies in BD were compared(Sklar et al. 2008; WTCCC 2007). This finding was supportedby Ferreira et al., who combined these two previous studieswith an additional sample, studying in total 4387 cases and6209 controls, and obtained a P-value of 7.0 × 10−8 (Ferreiraet al. 2008). The ankyrinG gene (ANK3) also appeared as apotential BD susceptibility gene from the studies by Ferreiraet al. (P = 9.1 × 10−9; rs10994336). This association waslater supported (Schulze et al. 2009; Smith et al. 2009) alongwith evidence of a possible second independent associationin the gene for the SNP rs9804190 (P = 3 × 10−6), located340 kb apart from rs10994336 (Schulze et al. 2009). Themyosin5B (MYO5B) and the tetraspanin-8 (TSPAN8) genesalso arose as potential BD candidates from the study bySklar et al. (P = 1.66 × 10−7 and P = 6.11 × 10−7). The zincfinger protein 804A gene (ZNF804A) is probably the gene withstrongest evidence for association with psychiatric disorders.It was first implicated in a GWA study of schizophrenia wherethe association was enhanced after including BD patientsin the patient sample (P = 9.96 × 10−9) (O’Donovan et al.2008). Recently, this finding was replicated in another GWAstudy of schizophrenia and BD patients (P = 6.5 × 10−4)(Steinberg et al. 2011). GWA studies comparing the twopatient groups have further supported the possibility ofshared polygenic variation increasing the risk of BD andschizophrenia (Moskvina et al. 2009; Purcell et al. 2009). Inour sample, we observed a trend for association betweenrs1344706 and a positive MDQ. This could indicate thatZNF804A should not be classified as a susceptibility geneonly for psychosis (Steinberg et al. 2011), but also for a widerrange of psychiatric symptoms.
The mean score on the MDQ was significantly higheramong ADHD patients than controls, 8.1 vs. 2.9 (P < 0.001),and in our sample 49% of the patients screened positive fora BSD according to standard cut-offs for the MDQ, comparedto 6% of the controls. This is not only explained by the highprevalence (11%) of BD reported in the ADHD group. Thecurrent or life-time presence of other psychiatric disorders
was also high among the ADHD patients. Significant life-timedepression or anxiety was reported by a larger proportionof the ADHD patients than the controls (69% vs. 14%),and problems with alcohol and with illegal drugs werealso commonly reported by the patients, with 23% and26%, respectively. These comorbid conditions are alsofrequent in clinical samples of BD patients, emphasizingthe clinical relationship and possible shared pathophysiologyof these conditions. We have previously shown that patientswith a positive MDQ score have more ADHD symptoms,more psychiatric comorbidity and a lower educational andoccupational functioning than the MDQ-negative patients(Halmoy et al. 2010). Affective symptoms thus seem to be animportant characteristic in a more severely affected subgroupof ADHD patients, with common and partly overlappingfeatures with some personality disorders and BSD beyondclassical BD (Halmoy et al. 2010). Although no associationwas found between risk alleles for BD and ADHD in thepresent study, there may still be some shared geneticvulnerability between subgroups of these disorders, whichmay be difficult to detect using strictly defined diagnosticcategories. Using quantitative measures, such as MDQscores, it may be possible to assess risk factors acrossdiagnostic boundaries.
The effect sizes of most genetic variants found associatedwith complex disorders are small and it is possible that oursample lacks power to detect a putative association also inadult ADHD. However, our study has relatively good powerto detect a nominal association if the true effects are indeedclose to the estimates from the GWA studies (Table 2). Thus,our results suggest that the possible contribution of thesegenes to the risk of adult ADHD is considerably lower than forBD. Hypomanic and manic symptoms, as reported using theMDQ, were shown to be highly prevalent in our patients. Theassociation between a positive MDQ score and the BD riskallele located in ZNF804A is only tentative, but if replicated,would suggest that this genetic variant may be associatedwith hypomanic and manic symptoms.
References
American Psychiatric Association. (2000) Diagnostic and StatisticalManual of Mental Disorders, 4th edn, text revision. AmericanPsychiatric Association, Washington, DC.
Genes, Brain and Behavior (2011) 10: 418–423 421
Landaas et al.
Baum, A.E., Akula, N., Cabanero, M., Cardona, I., Corona, W.,Klemens, B., Schulze, T.G., Cichon, S., Rietschel, M., Nothen,M.M., Georgi, A., Schumacher, J., Schwarz, M., Abou Jamra, R.,Hofels, S., Propping, P., Satagopan, J., Detera-Wadleigh, S.D.,Hardy, J. & McMahon, F.J. (2008) A genome-wide associationstudy implicates diacylglycerol kinase eta (DGKH) and severalother genes in the etiology of bipolar disorder. Mol Psychiatry 13,197–207.
Birmaher, B., Axelson, D., Goldstein, B., Monk, K., Kalas, C.,Obreja, M., Hickey, M.B., Iyengar, S., Brent, D., Shamseddeen, W.,Diler, R. & Kupfer, D. (2010) Psychiatric disorders in preschool off-spring of parents with bipolar disorder: the Pittsburgh BipolarOffspring Study (BIOS). Am J Psychiatry 167, 321–330.
Bridgman, P.C. (2004) Myosin-dependent transport in neurons.J Neurobiol 58, 164–174.
Faraone, S.V., Biederman, J., Mennin, D., Wozniak, J. & Spencer, T.(1997) Attention-deficit hyperactivity disorder with bipolar disorder:a familial subtype? J Am Acad Child Adolesc Psychiatry 36,1378–1387 (discussion).
Faraone, S.V., Biederman, J. & Mick, E. (2006) The age-dependentdecline of attention deficit hyperactivity disorder: a meta-analysisof follow-up studies. Psychol Med 36, 159–165.
Faraone, S.V., Perlis, R.H., Doyle, A.E., Smoller, J.W., Goralnick, J.J.,Holmgren, M.A. & Sklar, P. (2005) Molecular genetics of attention-deficit/hyperactivity disorder. Biol Psychiatry 57, 1313–1323.
Fayyad, J., De Graaf, R., Kessler, R., Alonso, J., Angermeyer, M.,Demyttenaere, K., De Girolamo, G., Haro, J.M., Karam, E.G.,Lara, C., Lepine, J.P., Ormel, J., Posada-Villa, J., Zaslavsky, A.M.& Jin, R. (2007) Cross-national prevalence and correlates ofadult attention-deficit hyperactivity disorder. Br J Psychiatry 190,402–409.
Ferreira, M.A., O’Donovan, M.C., Meng, Y.A. et al. (2008) Collabora-tive genome-wide association analysis supports a role for ANK3and CACNA1C in bipolar disorder. Nat Genet 40, 1056–1058.
Franke, B., Neale, B.M. & Faraone, S.V. (2009) Genome-wideassociation studies in ADHD. Hum Genet 126, 13–50.
Haavik, J., Halmoy, A., Lundervold, A.J. & Fasmer, O.B. (2010)Clinical assessment and diagnosis of adults with attention-deficit/hyperactivity disorder. Expert Rev Neurother 10,1569–1580.
Halmoy, A., Halleland, H., Dramsdahl, M., Bergsholm, P., Fasmer,O.B. & Haavik, J. (2010) Bipolar symptoms in adult attention-deficit/hyperactivity disorder: a cross-sectional study of 510clinically diagnosed patients and 417 population-based controls.J Clin Psychiatry 71, 48–57.
Hegerl, U., Himmerich, H., Engmann, B. & Hensch, T. (2010) Maniaand attention-deficit/hyperactivity disorder: common symptoma-tology, common pathophysiology and common treatment? CurrOpin Psychiatry 23, 1–7.
Hemler, M.E. (2003) Tetraspanin proteins mediate cellular pene-tration, invasion, and fusion events and define a novel type ofmembrane microdomain. Annu Rev Cell Dev Biol 19, 397–422.
Hirschfeld, R.M., Holzer, C., Calabrese, J.R., Weissman, M.,Reed, M., Davies, M., Frye, M.A., Keck, P., McElroy, S., Lewis, L.,Tierce, J., Wagner, K.D. & Hazard, E. (2003) Validity of the mooddisorder questionnaire: a general population study. Am J Psychiatry160, 178–180.
Hirschfeld, R.M., Williams, J.B., Spitzer, R.L., Calabrese, J.R.,Flynn, L., Keck, P.E. Jr. Lewis, L., McElroy, S.L., Post, R.M., Rap-port, D.J., Russell, J.M., Sachs, G.S. & Zajecka, J. (2000) Develop-ment and validation of a screening instrument for bipolar spectrumdisorder: the mood disorder questionnaire. Am J Psychiatry 157,1873–1875.
Johansson, S., Halleland, H., Halmoy, A., Jacobsen, K.K., Landaas,E.T., Dramsdahl, M., Fasmer, O.B., Bergsholm, P., Lundervold,A.J., Gillberg, C., Hugdahl, K., Knappskog, P.M. & Haavik, J.(2008) Genetic analyses of dopamine related genes in adult ADHDpatients suggest an association with the DRD5-microsatelliterepeat, but not with DRD4 or SLC6A3 VNTRs. Am J Med Genet BNeuropsychiatr Genet 147B, 1470–1475.
Kessler, R.C., Adler, L., Barkley, R., Biederman, J., Conners, C.K.,Demler, O., Faraone, S.V., Greenhill, L.L., Howes, M.J., Secnik, K.,Spencer, T., Ustun, T.B., Walters, E.E. & Zaslavsky, A.M. (2006)The prevalence and correlates of adult ADHD in the UnitedStates: results from the National comorbidity survey replication.Am J Psychiatry 163, 716–723.
Kordeli, E., Lambert, S. & Bennett, V. (1995) AnkyrinG. A new ankyringene with neural-specific isoforms localized at the axonal initialsegment and node of Ranvier. J Biol Chem 270, 2352–2359.
Lapierre, L.A., Kumar, R., Hales, C.M., Navarre, J., Bhartur, S.G.,Burnette, J.O., Provance, D.W. Jr, Mercer, J.A., Bahler, M. &Goldenring, J.R. (2001) Myosin vb is associated with plasmamembrane recycling systems. Mol Biol Cell 12, 1843–1857.
McCarthy, M.I. (2010) Genomics, type 2 diabetes, and obesity.N Engl J Med 363, 2339–2350.
McGough, J.J., Smalley, S.L., McCracken, J.T., Yang, M.,Del’Homme, M., Lynn, D.E. & Loo, S. (2005) Psychiatric comor-bidity in adult attention deficit hyperactivity disorder: findings frommultiplex families. Am J Psychiatry 162, 1621–1627.
Moskvina, V., Craddock, N., Holmans, P., Nikolov, I., Pahwa, J.S.,Green, E., Owen, M.J. & O’Donovan, M.C. (2009) Gene-wideanalyses of genome-wide association data sets: evidence formultiple common risk alleles for schizophrenia and bipolar disorderand for overlap in genetic risk. Mol Psychiatry 14, 252–260.
O’Donovan, M.C., Craddock, N., Norton, N. et al. (2008) Identifi-cation of loci associated with schizophrenia by genome-wideassociation and follow-up. Nat Genet 40, 1053–1055.
Passarotti, A.M., Sweeney, J.A. & Pavuluri, M.N. (2010) Emotionprocessing influences working memory circuits in pediatric bipolardisorder and attention-deficit/hyperactivity disorder. J Am AcadChild Adolesc Psychiatry 49, 1064–1080.
Purcell, S., Neale, B., Todd-Brown, K., Thomas, L., Ferreira, M.A.,Bender, D., Maller, J., Sklar, P., de Bakker, P.I., Daly, M.J. &Sham, P.C. (2007) PLINK: a tool set for whole-genome associationand population-based linkage analyses. Am J Hum Genet 81,559–575.
Purcell, S.M., Wray, N.R., Stone, J.L., Visscher, P.M., O’Donovan,M.C., Sullivan, P.F. & Sklar, P. (2009) Common polygenic variationcontributes to risk of schizophrenia and bipolar disorder. Nature460, 748–752.
Reimherr, F.W., Marchant, B.K., Strong, R.E., Hedges, D.W.,Adler, L., Spencer, T.J., West, S.A. & Soni, P. (2005) Emotionaldysregulation in adult ADHD and response to atomoxetine. BiolPsychiatry 58, 125–131.
Schulze, T.G., Detera-Wadleigh, S.D., Akula, N., Gupta, A.,Kassem, L., Steele, J., Pearl, J., Strohmaier, J., Breuer, R.,Schwarz, M., Propping, P., Nothen, M.M., Cichon, S., Schu-macher, J., Rietschel, M. & McMahon, F.J. (2009) Two variantsin Ankyrin 3 (ANK3) are independent genetic risk factors for bipolardisorder. Mol Psychiatry 14, 487–491.
Skirrow, C., McLoughlin, G., Kuntsi, J. & Asherson, P. (2009) Behav-ioral, neurocognitive and treatment overlap between attention-deficit/hyperactivity disorder and mood instability. Expert RevNeurother 9, 489–503.
Sklar, P., Smoller, J.W., Fan, J. et al. (2008) Whole-genome associa-tion study of bipolar disorder. Mol Psychiatry 13, 558–569.
Smith, E.N., Bloss, C.S., Badner, J.A. et al. (2009) Genome-wideassociation study of bipolar disorder in European American andAfrican American individuals. Mol Psychiatry 14, 755–763.
Sobanski, E., Bruggemann, D., Alm, B., Kern, S., Deschner, M.,Schubert, T., Philipsen, A. & Rietschel, M. (2007) Psychiatriccomorbidity and functional impairment in a clinically referredsample of adults with attention-deficit/hyperactivity disorder(ADHD). Eur Arch Psychiatry Clin Neurosci 257, 371–377.
Steinberg, S., Mors, O., Borglum, A.D. et al. (2011) Expanding therange of ZNF804A variants conferring risk of psychosis. MolPsychiatry 16, 59–66.
Teslovich, T.M., Musunuru, K., Smith, A.V. et al. G.W. (2010)Biological, clinical and population relevance of 95 loci for bloodlipids. Nature 466, 707–713.
422 Genes, Brain and Behavior (2011) 10: 418–423

Bipolar disorder risk alleles in adult ADHD patients
Wender, P.H., Reimherr, F.W. & Wood, D.R. (1981) Attention deficitdisorder (’minimal brain dysfunction’) in adults. A replication studyof diagnosis and drug treatment. Arch Gen Psychiatry 38, 449–456.
Wessa, M., Linke, J., Witt, S.H., Nieratschker, V., Esslinger, C.,Kirsch, P., Grimm, O., Hennerici, M.G., Gass, A., King, A.V. &Rietschel, M. (2010) The CACNA1C risk variant for bipolar disorderinfluences limbic activity. Mol Psychiatry 15, 1126–1127.
Wingo, A.P. & Ghaemi, S.N. (2007) A systematic review of rates anddiagnostic validity of comorbid adult attention-deficit/hyperactivitydisorder and bipolar disorder. J Clin Psychiatry 68, 1776–1784.
Wellcome Trust Case Control Consortium (WTCCC) (2007) Genome-wide association study of 14,000 cases of seven common diseasesand 3,000 shared controls. Nature 447, 661–678.
World Health Organization. 2003 The ICD-10 Classification of Mentaland Behavioural Disorders: Diagnostic criteria for Research. WorldHealth Organization, Geneva, Switzerland.
Acknowledgments
We are grateful to the patients and controls who participated inthis study. We thank Paal Borge and Ragnhild Nordenborg fortechnical assistance. This project was supported by the ResearchCouncil of Norway, Western Norway Regional Health Authority,the Norwegian ADHD Research Network and the University ofBergen.
Genes, Brain and Behavior (2011) 10: 418–423 423







