dosing and monitoring: children and adolescents buspar: 20–60 carbamazepine: ... hydroxyzine...
TRANSCRIPT
34 • PsychoPharmacology Bulletin: Vol. 48 · No. 2
Educational REviEw
Dosing and Monitoring: Children and Adolescents
By Glenn S. Hirsch
IntroductIon
American culture places a great value on our children. In accordance with this, parents seek out the best health care, wanting to ensure the well-being of their children. Despite this, physicians have been forced to treat children with medica-tions lacking FDA indications for pediatric use. Off-label use to treat childhood disorders has been the rule rather than the exception, with clinicians relying on limited literature or clinical lore to make important medical decisions.
The treatment of psychiatric disorders in children has been no exception. Medications approved for adults gradually make their way into the armamen-tarium of child and adolescent psychiatrists, often without adequate dosing guidelines. The past two decades have seen a dramatic increase in the number of studies looking specifically at pediatric psychopharmacology, but there have been difficulties in obtaining funding for such work. Pediatric studies have also been hampered by the lack of understanding of the biologic nature of many psychiatric disorders.
Numerous factors have worked together to begin changing these problems. In 1994, the FDA enacted the Pediatric Labeling Regulation, which encouraged pharmaceutical firms to submit applications for a change in labeling for pediatric indications if a review of the literature showed that enough data existed to war-rant a pediatric indication.
As part of the Food and Drug Administration Modernization Act of 1997 (enacted in 1998), pediatric exclusivity could be extended by 6 months for medi-cations whose manufacturers submitted pediatric studies in compliance with the act’s regulations. In addition, the Pediatric Rule, effective April 1999, required certain manufacturers—namely those of products that would either be used in a “substantial” number of pediatric patients or provide children a meaningful
Journal name: Psychopharmacology BulletinVolume no: 48Issue no: 2Year: 2018Article designation: Educational ReviewRunning heading title: Dosing and Monitoring: Children and Adolescents
Dr. Hirsch is Vice Chair for Clinical Affairs, Department of Child and Adolescent Psychiatry and Child Study Center of the Hassenfeld Children’s Hospital at NYU Langone and Associate Professor of Child and Adolescent Psychiatry, Psychiatry, and Pediatrics.To whom correspondence should be addressed: James M. La Rossa Jr., Publisher, 2205 Rockefeller Lane, Bldg. B, Redondo Beach, CA 90278. Phone: 310.374.1300; Fax: 424.398.0067; E-mail: [email protected]
Psychopharmacol Bull. 2018;48(2):34–92.
PB-Child & Adolescent Dosing.indd 34 05-02-2018 16:02:25
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
35Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
therapeutic benefit over existing treatments—to conduct studies that would be adequate to provide labeling for pediatric indications.
In addition, the NIMH funded the Research Units in Pediatric Psychopharmacology (RUPP) network. RUPP is composed of research units in academic centers across the country devoted to conduct-ing studies to test the efficacy and safety of medications commonly used by practitioners to treat children and adolescents but not yet adequately tested.
The number of pediatric studies and submissions to the FDA has subsequently increased dramatically. Clearly this has allowed new fund-ing sources to assist in the development of pharmacological trials. It has also assisted in allaying the resistance that is often seen toward treatment studies in young children. As public awareness of psychiatric disorders has grown, resistance toward research has begun to diminish.
As our knowledge of pediatric psychopharmacology increa ses, it becomes increasingly difficult to keep track of the available options for treatment. While it is beyond the scope of this book to cover all the factors that make the treatment of children different from that of adults, we have attempted to compile a practical guide for those “in the trenches.” Medications commonly used in children and adolescents, as well as general dosing guidelines, have been provided.
In addition to the dosing and monitoring tables that follow, there are a number of overarching “principles” to keep in mind in treating this vul-nerable population. The latest recommendations for use of psychotro-pic medication from the American Academy of Child and Adolescent Psychiatry (AACAP) greatly expanded guidelines for clinicians. These guidelines for dosing and monitoring in children and adolescents will follow the AACAP’s lead.
Psychiatrists, pediatric neurologists, and pediatricians whose patients may present on a medication they are less familiar with will hopefully find this guide helpful.
We hope the following will enhance the ease with which you practice, and we look forward to your suggestions for future updates.
— Editorial Director, James M. La Rossa Jr.,contributed to the 2018 update of this work
PB-Child & Adolescent Dosing.indd 35 05-02-2018 16:02:25
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
36Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
TABLE 1
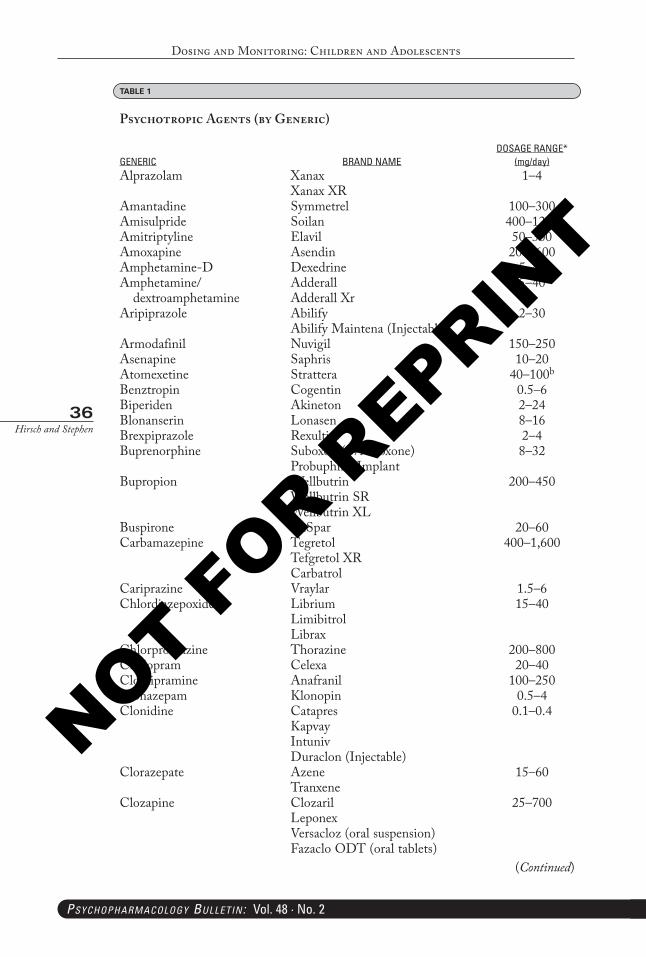
Psychotropic Agents (by Generic)
GENERIC BRAND NAMEDOSAGE RANGE*
(mg/day)Alprazolam Xanax
Xanax XR1–4
Amantadine Symmetrel 100–300Amisulpride Soilan 400–1200Amitriptyline Elavil 50–300Amoxapine Asendin 200–600Amphetamine-D Dexedrine 5–40Amphetamine/
dextroamphetamineAdderallAdderall Xr
5–40
Aripiprazole AbilifyAbilify Maintena (Injectable)
2–30
Armodafinil Nuvigil 150–250Asenapine Saphris 10–20Atomexetine Strattera 40–100b
Benztropin Cogentin 0.5–6Biperiden Akineton 2–24Blonanserin Lonasen 8–16Brexpiprazole Rexulti 2–4Buprenorphine Suboxon (w/Naloxone)
Probuphine Implant8–32
Bupropion WellbutrinWellbutrin SRWellbutrin XL
200–450
Buspirone BuSpar 20–60Carbamazepine Tegretol
Tefgretol XRCarbatrol
400–1,600
Cariprazine Vraylar 1.5–6Chlordiazepoxide Librium
LimibitrolLibrax
15–40
Chlorpromazine Thorazine 200–800Citalopram Celexa 20–40Clomipramine Anafranil 100–250Clonazepam Klonopin 0.5–4Clonidine Catapres
KapvayIntunivDuraclon (Injectable)
0.1–0.4
Clorazepate AzeneTranxene
15–60
Clozapine ClozarilLeponexVersacloz (oral suspension)Fazaclo ODT (oral tablets)
25–700
(Continued)
PB-Child & Adolescent Dosing.indd 36 05-02-2018 16:02:25
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
37Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
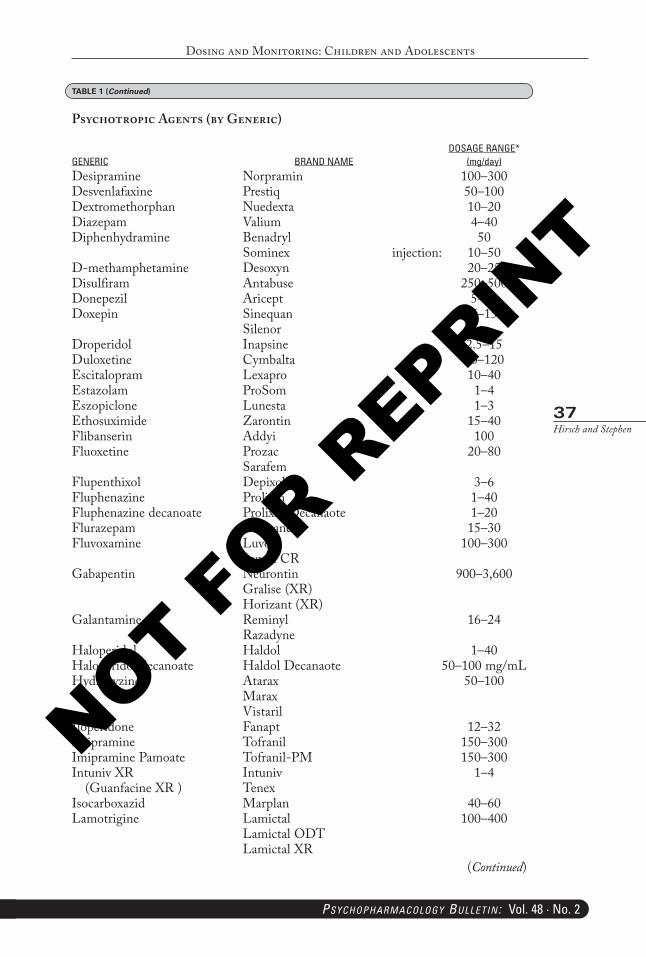
GENERIC BRAND NAMEDOSAGE RANGE*
(mg/day)Desipramine Norpramin 100–300Desvenlafaxine Prestiq 50–100Dextromethorphan Nuedexta 10–20Diazepam Valium 4–40Diphenhydramine Benadryl
Sominex injection:50
10–50D-methamphetamine Desoxyn 20–25Disulfiram Antabuse 250–500Donepezil Aricept 5–10Doxepin Sinequan
Silenor75–150
Droperidol Inapsine 2.5–15Duloxetine Cymbalta 60–120Escitalopram Lexapro 10–40Estazolam ProSom 1–4Eszopiclone Lunesta 1–3Ethosuximide Zarontin 15–40Flibanserin Addyi 100Fluoxetine Prozac
Sarafem20–80
Flupenthixol Depixol 3–6Fluphenazine Prolixin 1–40Fluphenazine decanoate Prolixin Decanaote 1–20Flurazepam Dalmane 15–30Fluvoxamine Luvox
Luvox CR100–300
Gabapentin NeurontinGralise (XR)Horizant (XR)
900–3,600
Galantamine ReminylRazadyne
16–24
Haloperidol Haldol 1–40Haloperidol decanoate Haldol Decanaote 50–100 mg/mLHydroxyzine Atarax
MaraxVistaril
50–100
Iloperidone Fanapt 12–32Imipramine Tofranil 150–300Imipramine Pamoate Tofranil-PM 150–300Intuniv XR
(Guanfacine XR )IntunivTenex
1–4
Isocarboxazid Marplan 40–60Lamotrigine Lamictal
Lamictal ODTLamictal XR
100–400
TABLE 1 (Continued)
Psychotropic Agents (by Generic)
(Continued)
PB-Child & Adolescent Dosing.indd 37 05-02-2018 16:02:25
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
38Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
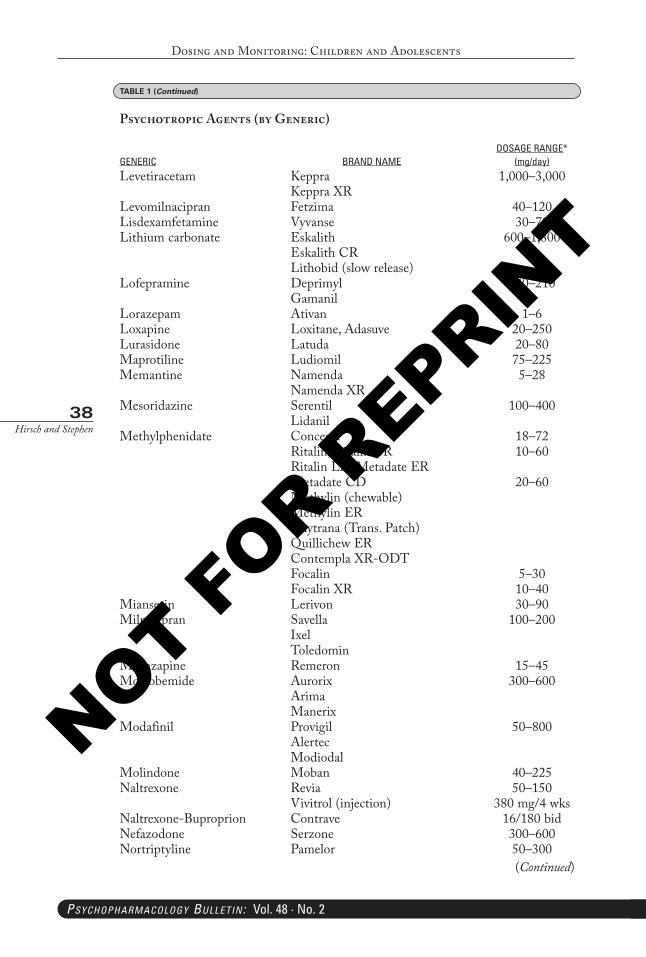
GENERIC BRAND NAMEDOSAGE RANGE*
(mg/day)Levetiracetam Keppra
Keppra XR1,000–3,000
Levomilnacipran Fetzima 40–120Lisdexamfetamine Vyvanse 30–70Lithium carbonate Eskalith
Eskalith CRLithobid (slow release)
600–1,800
Lofepramine DeprimylGamanil
140–210
Lorazepam Ativan 1–6Loxapine Loxitane, Adasuve 20–250Lurasidone Latuda 20–80Maprotiline Ludiomil 75–225Memantine Namenda
Namenda XR5–28
Mesoridazine SerentilLidanil
100–400
Methylphenidate ConcertaRitalin, Ritalin-SRRitalin LA, Metadate ER Metadate CD Methylin (chewable)Methylin ERDaytrana (Trans. Patch)Quillichew ERContempla XR-ODTFocalinFocalin XR
18–7210–60
20–60
5–3010–40
Mianserin Lerivon 30–90Milnacipran Savella
IxelToledomin
100–200
Mirtazapine Remeron 15–45Moclobemide Aurorix
ArimaManerix
300–600
Modafinil ProvigilAlertecModiodal
50–800
Molindone Moban 40–225Naltrexone Revia
Vivitrol (injection)50–150
380 mg/4 wksNaltrexone-Buproprion Contrave 16/180 bidNefazodone Serzone 300–600Nortriptyline Pamelor 50–300
TABLE 1 (Continued)
Psychotropic Agents (by Generic)
(Continued)
PB-Child & Adolescent Dosing.indd 38 05-02-2018 16:02:26
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
39Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
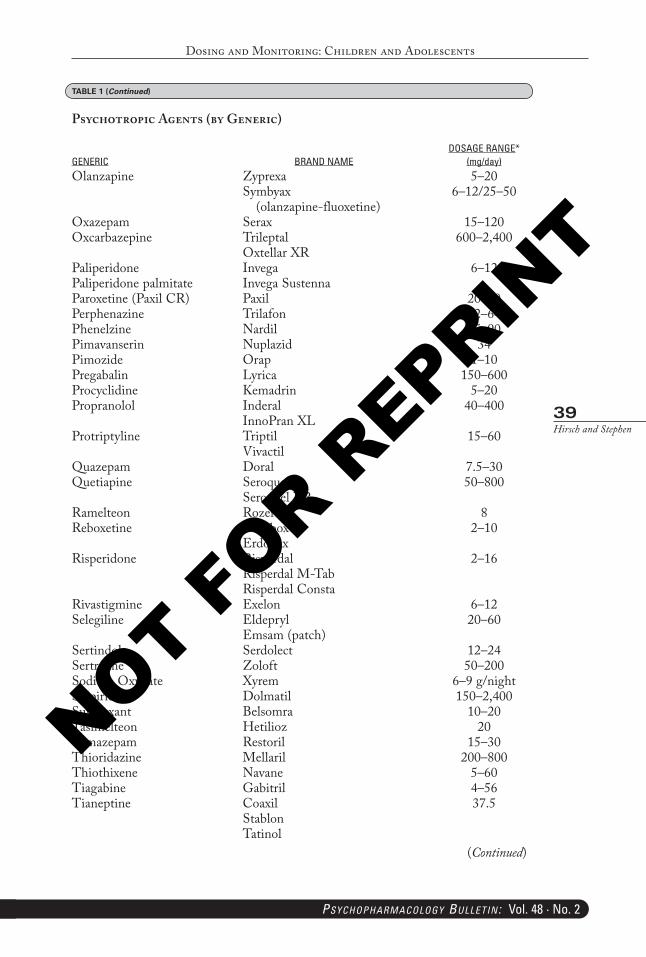
GENERIC BRAND NAMEDOSAGE RANGE*
(mg/day)Olanzapine Zyprexa
Symbyax (olanzapine-fluoxetine)
5–206–12/25–50
Oxazepam Serax 15–120Oxcarbazepine Trileptal
Oxtellar XR600–2,400
Paliperidone Paliperidone palmitate
InvegaInvega Sustenna
6–12
Paroxetine (Paxil CR) Paxil 20–50Perphenazine Trilafon 12–64Phenelzine Nardil 45–90Pimavanserin Nuplazid 34Pimozide Orap 1–10Pregabalin Lyrica 150–600Procyclidine Kemadrin 5–20Propranolol Inderal
InnoPran XL40–400
Protriptyline TriptilVivactil
15–60
Quazepam Doral 7.5–30Quetiapine Seroquel
Seroquel XR50–800
Ramelteon Rozerem 8Reboxetine Norebox
Erdonax2–10
Risperidone RisperdalRisperdal M-TabRisperdal Consta
2–16
Rivastigmine Exelon 6–12Selegiline Eldepryl
Emsam (patch)20–60
Sertindole Serdolect 12–24Sertraline Zoloft 50–200Sodium Oxybate Xyrem 6–9 g/nightSulpiride Dolmatil 150–2,400Suvorexant Belsomra 10–20Tasimelteon Hetilioz 20Temazepam Restoril 15–30Thioridazine Mellaril 200–800Thiothixene Navane 5–60Tiagabine Gabitril 4–56Tianeptine Coaxil
StablonTatinol
37.5
TABLE 1 (Continued)
Psychotropic Agents (by Generic)
(Continued)
PB-Child & Adolescent Dosing.indd 39 05-02-2018 16:02:26
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
40Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
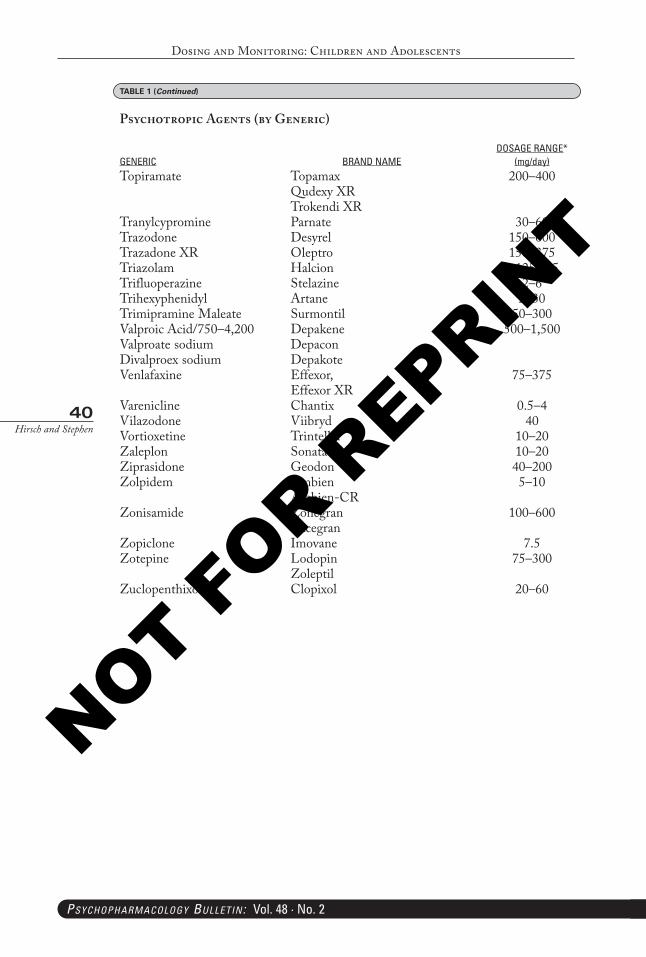
GENERIC BRAND NAMEDOSAGE RANGE*
(mg/day)Topiramate Topamax
Qudexy XRTrokendi XR
200–400
Tranylcypromine Parnate 30–60Trazodone Desyrel 150–600Trazadone XR Oleptro 150–375Triazolam Halcion 0.125–0.5Trifluoperazine Stelazine 2–6Trihexyphenidyl Artane 2–30Trimipramine Maleate Surmontil 50–300Valproic Acid/750–4,200 Valproate sodiumDivalproex sodium
DepakeneDepaconDepakote
500–1,500
Venlafaxine Effexor,Effexor XR
75–375
Varenicline Chantix 0.5–4Vilazodone Viibryd 40Vortioxetine Trintellix 10–20Zaleplon Sonata 10–20Ziprasidone Geodon 40–200Zolpidem Ambien
Ambien-CR5–10
Zonisamide ZonegranExcegran
100–600
Zopiclone Imovane 7.5Zotepine Lodopin
Zoleptil75–300
Zuclopenthixol Clopixol 20–60
TABLE 1 (Continued)
Psychotropic Agents (by Generic)
PB-Child & Adolescent Dosing.indd 40 05-02-2018 16:02:26
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
41Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Psyc
ho
tr
oPI
c c
rIt
erIa
fo
r c
hIl
dr
en a
nd
ad
ole
scen
ts (
ta
bles
2–7
)TA
BLE
2
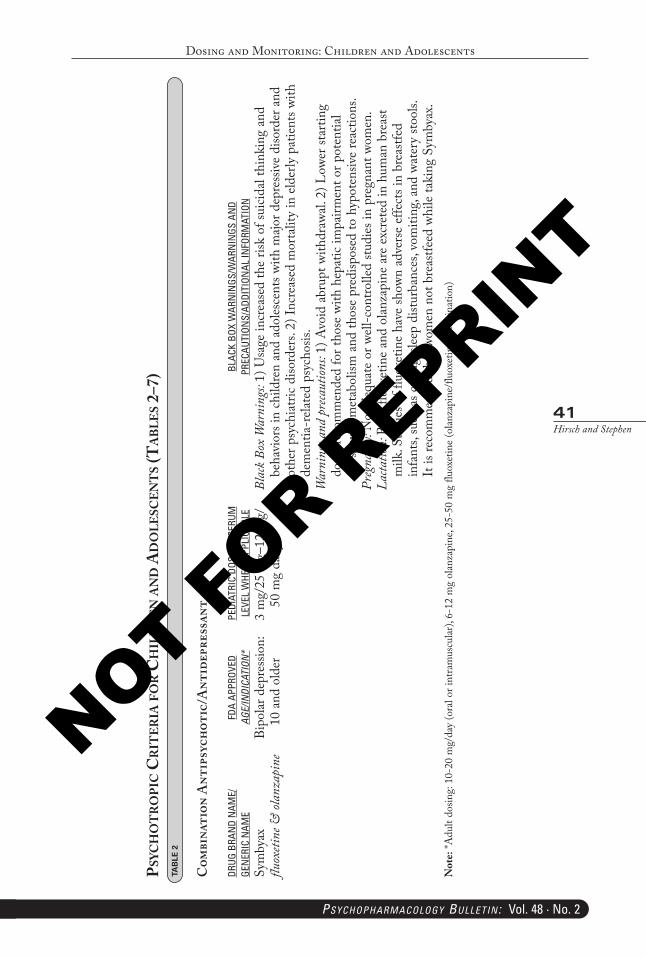
Com
bina
tion
Ant
ipsy
chot
ic/A
ntid
epre
ssan
t
DRUG
BRA
ND
NAM
E/GE
NER
IC N
AME
FDA
APPR
OVED
AGE/INDICATION*
PEDI
ATRI
C DO
SAGE
/SER
UM
LEVE
L W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
Sym
byax
fluox
etine
& ol
anza
pine
Bipo
lar d
epre
ssio
n:
10 a
nd o
lder
3 m
g/25
mg–
12 m
g/
50 m
g da
ilyBl
ack B
ox W
arni
ngs:
1) U
sage
incr
ease
d th
e ris
k of
suici
dal t
hink
ing
and
beha
vior
s in
child
ren
and
adol
esce
nts w
ith m
ajor d
epre
ssiv
e di
sord
er a
nd
othe
r psy
chia
tric
diso
rder
s. 2)
Incr
ease
d m
orta
lity
in e
lder
ly p
atie
nts w
ith
dem
entia
-rela
ted
psyc
hosis
.W
arni
ngs a
nd p
reca
ution
s: 1)
Avo
id a
brup
t with
draw
al. 2
) Low
er st
artin
g do
ses r
ecom
men
ded
for t
hose
with
hep
atic
impa
irmen
t or p
oten
tial
for s
lowe
d m
etab
olism
and
thos
e pr
edisp
osed
to h
ypot
ensiv
e re
actio
ns.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant w
omen
.La
ctatio
n: B
oth
fluox
etin
e an
d ol
anza
pine
are
exc
rete
d in
hum
an b
reas
t m
ilk. S
tudi
es o
f flu
oxet
ine
have
show
n ad
vers
e ef
fect
s in
brea
stfed
in
fant
s, su
ch a
s cry
ing,
sleep
dist
urba
nces
, vom
iting
, and
wat
ery
stool
s. It
is re
com
men
ded
that
wom
en n
ot b
reas
tfeed
whi
le ta
king
Sym
byax
.N
ote:
*Adu
lt do
sing:
10-
20 m
g/da
y (o
ral o
r int
ram
uscu
lar),
6-12
mg
olan
zapi
ne, 2
5-50
mg
fluox
etin
e (o
lanza
pine
/fluo
xetin
e co
mbi
natio
n)
PB-Child & Adolescent Dosing.indd 41 05-02-2018 16:02:26
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
42Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
TAB
LE 3
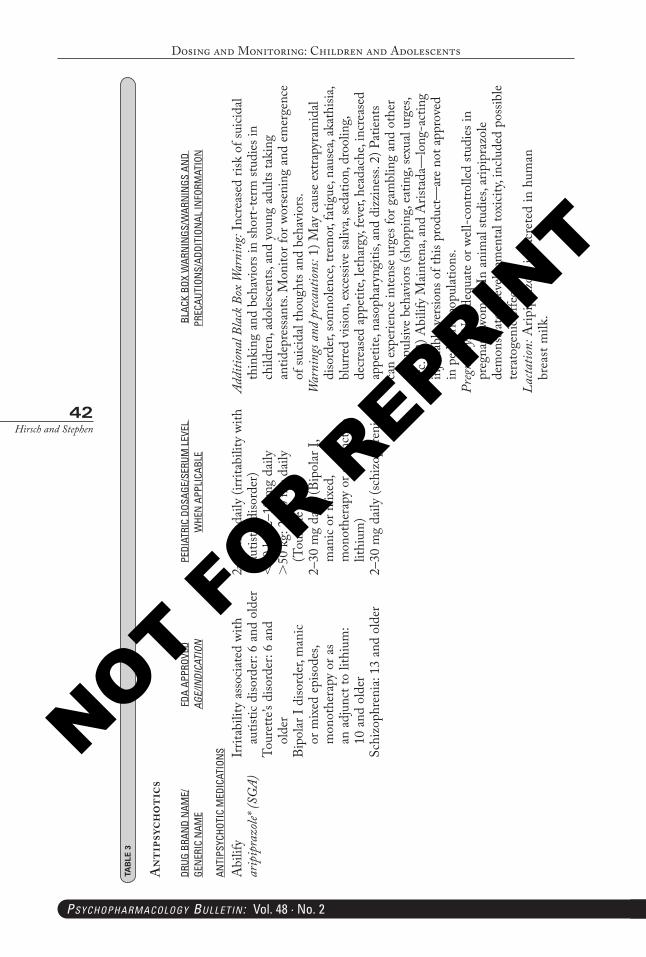
Ant
ipsy
chot
ics
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
ANTI
PSYC
HOTI
C M
EDIC
ATIO
NS
Abi
lify
arip
ipra
zole*
(SG
A)Ir
ritab
ility
ass
ocia
ted
with
au
tistic
diso
rder
: 6 a
nd o
lder
Tour
ette
’s di
sord
er: 6
and
ol
der
Bipo
lar I
diso
rder
, man
ic or
mix
ed e
piso
des,
mon
othe
rapy
or a
s an
adj
unct
to li
thiu
m:
10 a
nd o
lder
Schi
zoph
reni
a: 13
and
old
er
2–15
mg
daily
(irr
itabi
lity
with
au
tistic
diso
rder
)<
50 k
g: 2
–10
mg
daily
>50
kg:
2–2
0 m
g da
ily
(Tou
rette
’s)2–
30 m
g da
ily (B
ipol
ar I,
m
anic
or m
ixed
, m
onot
hera
py o
r adj
unct
to
lithi
um)
2–30
mg
daily
(sch
izop
hren
ia)
Addi
tiona
l Bla
ck B
ox W
arni
ng: I
ncre
ased
risk
of s
uicid
al th
inki
ng a
nd b
ehav
iors
in sh
ort-
term
stud
ies i
n ch
ildre
n, a
doles
cent
s, an
d yo
ung
adul
ts ta
king
an
tidep
ress
ants.
Mon
itor f
or w
orse
ning
and
em
erge
nce
of su
icida
l tho
ught
s and
beh
avio
rs.
War
ning
s and
pre
caut
ions:
1) M
ay c
ause
ext
rapy
ram
idal
diso
rder
, som
nolen
ce, t
rem
or, f
atig
ue, n
ause
a, ak
athi
sia,
blur
red
visio
n, e
xces
sive
saliv
a, se
datio
n, d
rool
ing,
decr
ease
d ap
petit
e, let
harg
y, fe
ver,
head
ache
, inc
reas
ed
appe
tite,
naso
phar
yngi
tis, a
nd d
izzi
ness
. 2) P
atie
nts
can
expe
rienc
e in
tens
e ur
ges f
or g
ambl
ing
and
othe
r co
mpu
lsive
beh
avio
rs (s
hopp
ing,
eatin
g, se
xual
urge
s, et
c.). 3
) Abi
lify
Mai
nten
a, an
d A
rista
da—
long
-act
ing
injec
tabl
e ve
rsio
ns o
f thi
s pro
duct
—ar
e no
t app
rove
d in
ped
iatri
c po
pulat
ions
.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pr
egna
nt w
omen
. In
anim
al stu
dies
, arip
ipra
zole
dem
onstr
ated
dev
elopm
enta
l tox
icity,
inclu
ded
poss
ible
tera
toge
nic
effe
cts.
Lacta
tion:
Arip
ipra
zole
is e
xcre
ted
in h
uman
br
east
milk
.
PB-Child & Adolescent Dosing.indd 42 05-02-2018 16:02:26
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
43Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
(Con
tinue
d)
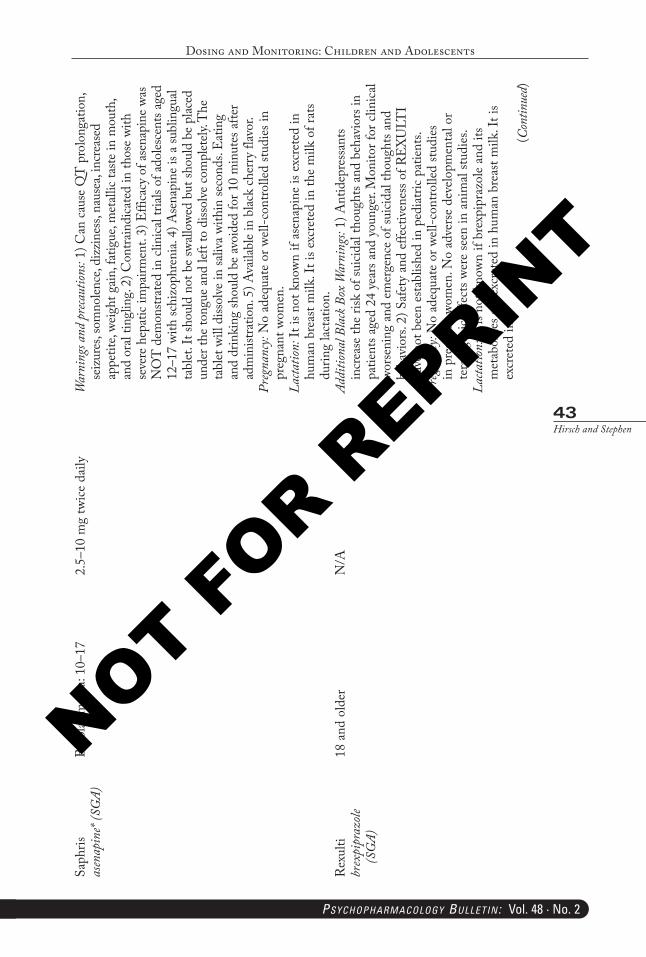
Saph
risas
enap
ine*
(SG
A)Bi
polar
man
ia: 1
0–17
2.5–
10 m
g tw
ice d
aily
War
ning
s and
pre
caut
ions:
1) C
an ca
use
QT
pro
long
atio
n,
seizu
res,
som
nolen
ce, d
izzin
ess,
naus
ea, i
ncre
ased
ap
petit
e, we
ight
gain
, fat
igue
, met
allic
taste
in m
outh
, an
d or
al tin
glin
g. 2)
Con
train
dica
ted
in th
ose
with
se
vere
hep
atic
impa
irmen
t. 3)
Effi
cacy
of a
sena
pine
was
N
OT
dem
onstr
ated
in c
linica
l tria
ls of
adol
esce
nts a
ged
12–1
7 wi
th sc
hizo
phre
nia.
4) A
sena
pine
is a
subl
ingu
al ta
blet
. It s
houl
d no
t be
swall
owed
but
shou
ld b
e pl
aced
un
der t
he to
ngue
and
left
to d
issol
ve co
mpl
etely
. The
ta
blet
will
diss
olve
in sa
liva
with
in se
cond
s. Ea
ting
and
drin
king
shou
ld b
e av
oide
d fo
r 10
min
utes
afte
r ad
min
istra
tion.
5) A
vaila
ble
in b
lack
cher
ry fl
avor
.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pr
egna
nt w
omen
.La
ctatio
n: It
is n
ot k
nown
if a
sena
pine
is e
xcre
ted
in
hum
an b
reas
t milk
. It i
s exc
rete
d in
the
milk
of r
ats
durin
g lac
tatio
n.R
exul
tibr
expi
praz
ole
(SG
A)
18 a
nd o
lder
N/A
Addi
tiona
l Bla
ck B
ox W
arni
ngs:
1) A
ntid
epre
ssan
ts in
crea
se th
e ris
k of
suici
dal t
houg
hts a
nd b
ehav
iors
in
patie
nts a
ged
24 y
ears
and
you
nger
. Mon
itor f
or c
linica
l wo
rseni
ng a
nd e
mer
genc
e of
suici
dal t
houg
hts a
nd
beha
vior
s. 2)
Saf
ety
and
effe
ctive
ness
of R
EXU
LTI
have
not
bee
n es
tabl
ished
in p
ediat
ric p
atien
ts.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es
in p
regn
ant w
omen
. No
adve
rse
deve
lopm
enta
l or
tera
toge
nic
effe
cts w
ere
seen
in a
nim
al stu
dies
.La
ctatio
n: It
is n
ot k
nown
if b
rexp
ipra
zole
and
its
met
abol
ites a
re e
xcre
ted
in h
uman
bre
ast m
ilk. I
t is
excr
eted
in
PB-Child & Adolescent Dosing.indd 43 05-02-2018 16:02:26
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
44Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
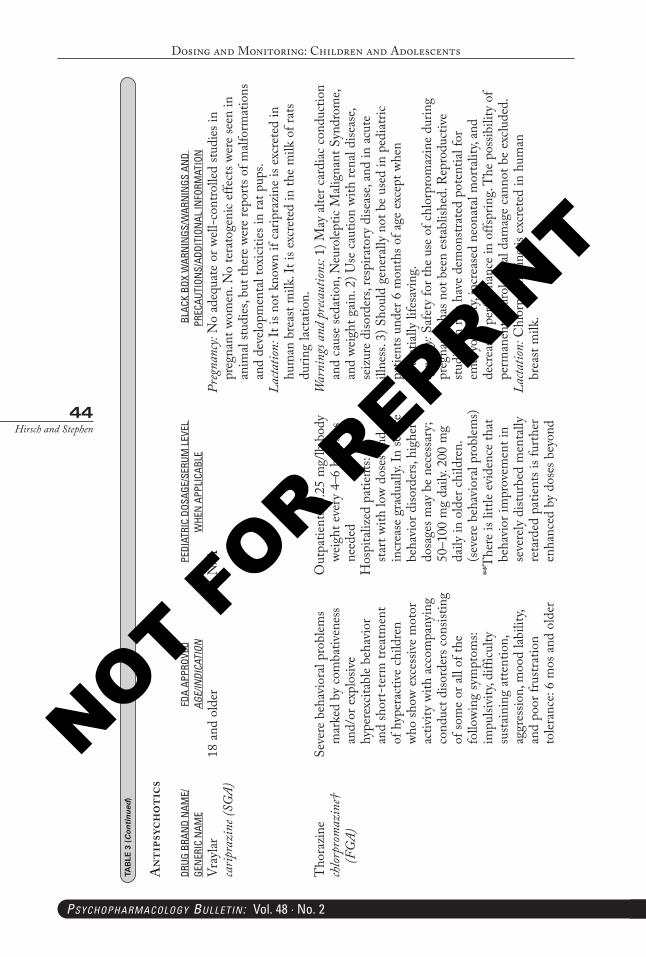
Vray
lar
carip
razi
ne (S
GA)
18 a
nd o
lder
N/A
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in
preg
nant
wom
en. N
o te
rato
geni
c effe
cts w
ere
seen
in
anim
al stu
dies
, but
ther
e we
re re
ports
of m
alfor
mat
ions
an
d de
velo
pmen
tal t
oxici
ties i
n ra
t pup
s.La
ctatio
n: It
is n
ot k
nown
if c
arip
razi
ne is
exc
rete
d in
hu
man
bre
ast m
ilk. I
t is e
xcre
ted
in th
e m
ilk o
f rat
s du
ring
lacta
tion.
Tho
razi
ne
chlor
prom
azin
e†
(FG
A)
Seve
re b
ehav
iora
l pro
blem
s m
arke
d by
com
bativ
enes
s an
d/or
exp
losiv
e hy
pere
xcita
ble
beha
vior
an
d sh
ort-
term
trea
tmen
t of
hyp
erac
tive
child
ren
who
show
exc
essiv
e m
otor
ac
tivity
with
acc
ompa
nyin
g co
nduc
t diso
rder
s con
sistin
g of
som
e or
all
of th
e fo
llowi
ng sy
mpt
oms:
impu
lsivi
ty, d
ifficu
lty
susta
inin
g at
tent
ion,
ag
gres
sion,
moo
d lab
ility,
an
d po
or fr
ustra
tion
toler
ance
: 6 m
os a
nd o
lder
Out
patie
nts:
0.25
mg/
lb b
ody
weig
ht e
very
4–6
hou
rs a
s ne
eded
Hos
pita
lized
pat
ient
s: sta
rt wi
th lo
w do
ses a
nd
incr
ease
gra
duall
y. In
seve
re
beha
vior
diso
rder
s, hi
gher
do
sage
s may
be
nece
ssar
y;
50–1
00 m
g da
ily. 2
00 m
g da
ily in
old
er c
hild
ren.
(se
vere
beh
avio
ral p
robl
ems)
**The
re is
littl
e ev
iden
ce th
at
beha
vior
impr
ovem
ent i
n se
vere
ly d
istur
bed
men
tally
re
tard
ed p
atie
nts i
s fur
ther
en
hanc
ed b
y do
ses b
eyon
d
War
ning
s and
pre
caut
ions:
1) M
ay a
lter c
ardi
ac c
ondu
ctio
n an
d ca
use
seda
tion,
Neu
rolep
tic M
align
ant S
yndr
ome,
and
weig
ht g
ain.
2) U
se c
autio
n wi
th re
nal d
iseas
e, se
izur
e di
sord
ers,
resp
irato
ry d
iseas
e, an
d in
acu
te
illne
ss. 3
) Sho
uld
gene
rally
not
be
used
in p
edia
tric
patie
nts u
nder
6 m
onth
s of a
ge e
xcep
t whe
n po
tent
ially
life
savi
ng.
Preg
nanc
y: Sa
fety
for t
he u
se o
f chl
orpr
omaz
ine
durin
g pr
egna
ncy
has n
ot b
een
esta
blish
ed. R
epro
duct
ive
studi
es in
rats
have
dem
onstr
ated
pot
entia
l for
em
bryo
toxi
city,
incr
ease
d ne
onat
al m
orta
lity,
and
decr
ease
d pe
rform
ance
in o
ffspr
ing.
The
pos
sibili
ty o
f pe
rman
ent n
euro
logi
cal d
amag
e ca
nnot
be
exclu
ded.
Lacta
tion:
Chl
orpr
omaz
ine
is ex
cret
ed in
hum
an
brea
st m
ilk.
TAB
LE 3
(Continued
)
Ant
ipsy
chot
ics
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 44 05-02-2018 16:02:26
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
45Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
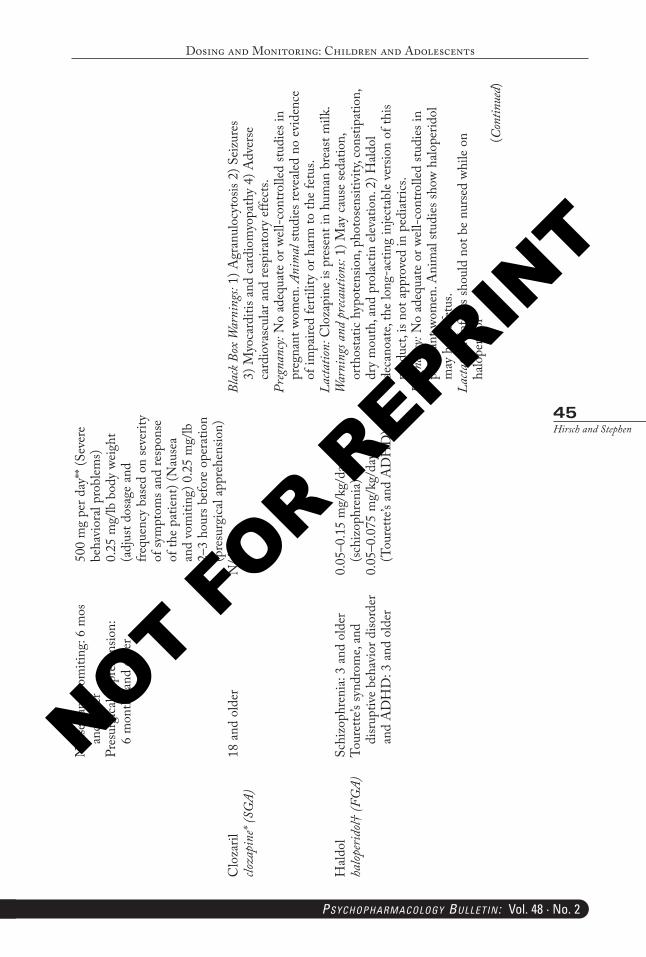
Nau
sea
and
vom
iting
: 6 m
os
and
olde
rPr
esur
gica
l app
rehe
nsio
n:
6 m
onth
s and
old
er
500
mg
per d
ay**
(Sev
ere
beha
vior
al pr
oblem
s) 0.
25 m
g/lb
bod
y we
ight
(a
djus
t dos
age
and
frequ
ency
bas
ed o
n se
verit
y of
sym
ptom
s and
resp
onse
of
the
patie
nt) (
Nau
sea
and
vom
iting
) 0.2
5 m
g/lb
2–
3 ho
urs b
efor
e op
erat
ion
(pre
surg
ical a
ppre
hens
ion)
Clo
zaril
clo
zapi
ne* (
SGA)
18 a
nd o
lder
N/A
Blac
k Box
War
ning
s: 1)
Agr
anul
ocyt
osis
2) S
eizu
res
3) M
yoca
rditi
s and
car
diom
yopa
thy
4) A
dver
se
card
iova
scul
ar a
nd re
spira
tory
effe
cts.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in
preg
nant
wom
en. A
nim
al st
udie
s rev
ealed
no
evid
ence
of
impa
ired
ferti
lity
or h
arm
to th
e fe
tus.
Lacta
tion:
Clo
zapi
ne is
pre
sent
in h
uman
bre
ast m
ilk.
Hald
ol
halop
erid
ol† (F
GA)
Schi
zoph
reni
a: 3
and
olde
rTo
uret
te’s
synd
rom
e, an
d di
srup
tive
beha
vior
diso
rder
an
d A
DH
D: 3
and
old
er
0.05
–0.1
5 m
g/kg
/day
(sc
hizo
phre
nia)
0.05
–0.0
75 m
g/kg
/day
(T
oure
tte’s
and
AD
HD
)
War
ning
s and
pre
caut
ions:
1) M
ay c
ause
seda
tion,
or
thos
tatic
hyp
oten
sion,
pho
tose
nsiti
vity,
con
stipa
tion,
dr
y m
outh
, and
pro
lactin
ele
vatio
n. 2
) Hald
ol
deca
noat
e, th
e lo
ng-a
ctin
g in
jecta
ble
vers
ion
of th
is pr
oduc
t, is
not a
ppro
ved
in p
edia
trics
.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pr
egna
nt w
omen
. Ani
mal
studi
es sh
ow h
alope
ridol
m
ay h
arm
fetu
s.La
ctatio
n: In
fant
s sho
uld
not b
e nu
rsed
whi
le on
ha
lope
ridol
(Con
tinue
d)
PB-Child & Adolescent Dosing.indd 45 05-02-2018 16:02:26
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
46Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
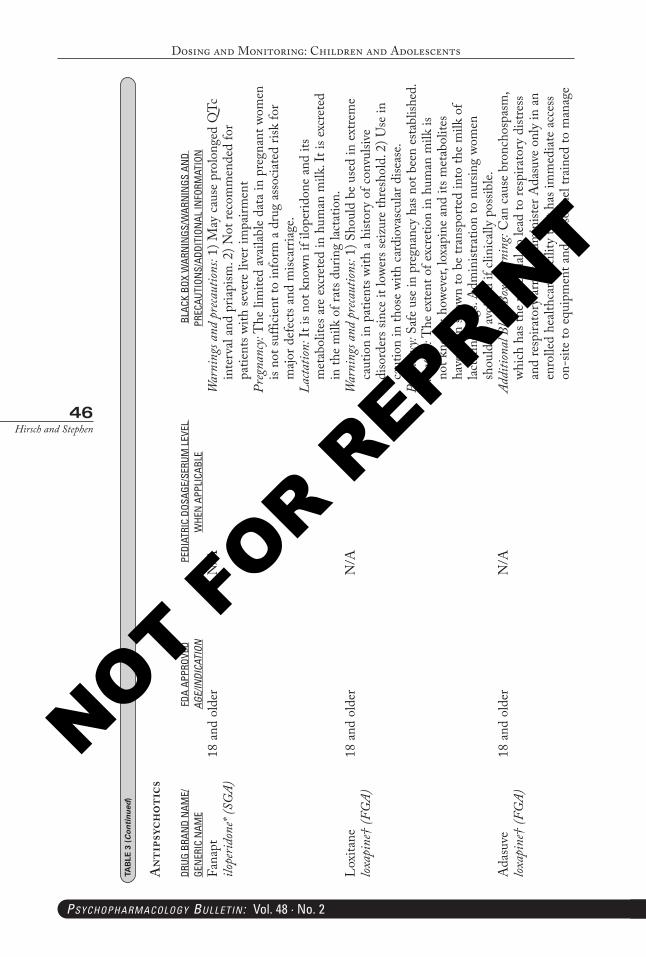
Fana
pt
ilope
ridon
e* (S
GA)
18 a
nd o
lder
N/A
War
ning
s and
pre
caut
ions:
1) M
ay c
ause
pro
long
ed Q
Tc
inte
rval
and
pria
pism
. 2) N
ot re
com
men
ded
for
patie
nts w
ith se
vere
live
r im
pairm
ent
Preg
nanc
y: T
he li
mite
d av
ailab
le da
ta in
pre
gnan
t wom
en
is no
t suf
ficie
nt to
info
rm a
dru
g as
socia
ted
risk
for
majo
r def
ects
and
misc
arria
ge.
Lacta
tion:
It is
not
kno
wn if
ilop
erid
one
and
its
met
abol
ites a
re e
xcre
ted
in h
uman
milk
. It i
s exc
rete
d in
the
milk
of r
ats d
urin
g lac
tatio
n.Lo
xita
ne
loxap
ine†
(FG
A)18
and
old
erN
/AW
arni
ngs a
nd p
reca
ution
s: 1)
Sho
uld
be u
sed
in e
xtre
me
caut
ion
in p
atie
nts w
ith a
hist
ory
of c
onvu
lsive
di
sord
ers s
ince
it lo
wers
seiz
ure
thre
shol
d. 2
) Use
in
caut
ion
in th
ose
with
car
diov
ascu
lar d
iseas
e.Pr
egna
ncy:
Safe
use
in p
regn
ancy
has
not
bee
n es
tabl
ished
.La
ctatio
n: T
he e
xten
t of e
xcre
tion
in h
uman
milk
is
not k
nown
; how
ever
, lox
apin
e an
d its
met
abol
ites
have
bee
n sh
own
to b
e tra
nspo
rted
into
the
milk
of
lacta
ting
dogs
. Adm
inist
ratio
n to
nur
sing
wom
en
shou
ld b
e av
oide
d if
clini
cally
pos
sible.
Ada
suve
lox
apin
e† (F
GA)
18 a
nd o
lder
N/A
Addi
tiona
l Bla
ck B
ox W
arni
ng: C
an c
ause
bro
ncho
spas
m,
which
has
the
pote
ntia
l to
lead
to re
spira
tory
dist
ress
an
d re
spira
tory
arre
st. A
dmin
ister
Ada
suve
onl
y in
an
enro
lled
healt
hcar
e fa
cility
that
has
imm
edia
te a
cces
s on
-site
to e
quip
men
t and
per
sonn
el tra
ined
to m
anag
e
TAB
LE 3
(Continued
)
Ant
ipsy
chot
ics
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 46 05-02-2018 16:02:26
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
47Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
(Con
tinue
d)
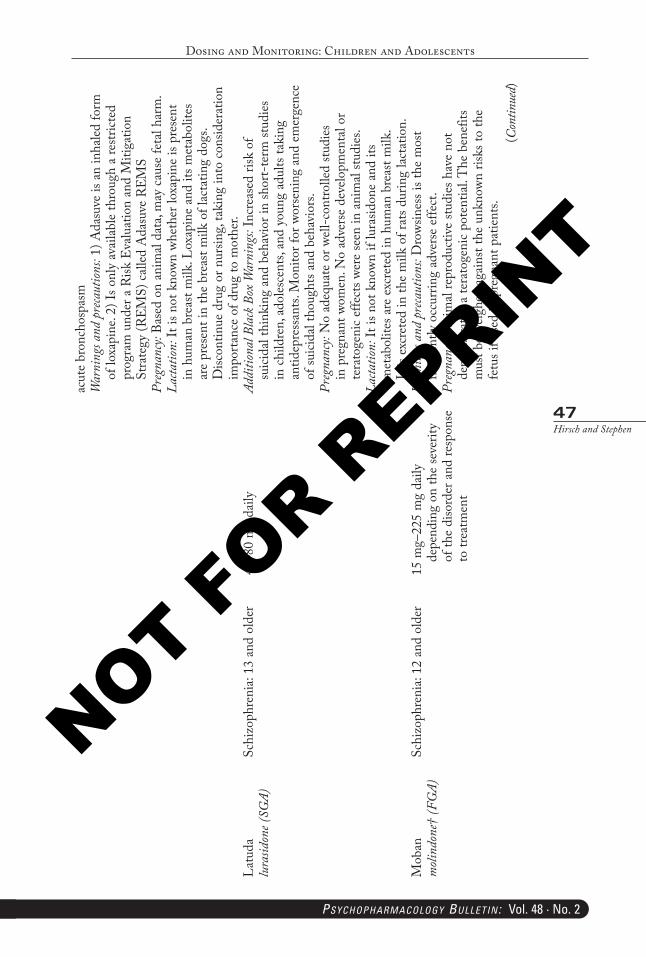
acut
e br
onch
ospa
smW
arni
ngs a
nd p
reca
ution
s: 1)
Ada
suve
is a
n in
haled
form
of
loxa
pine
. 2) I
s onl
y av
ailab
le th
roug
h a
restr
icted
pr
ogra
m u
nder
a R
isk E
valu
atio
n an
d M
itiga
tion
Stra
tegy
(REM
S) c
alled
Ada
suve
REM
SPr
egna
ncy:
Base
d on
ani
mal
data
, may
cau
se fe
tal h
arm
.La
ctatio
n: It
is n
ot k
nown
whe
ther
loxa
pine
is p
rese
nt
in h
uman
bre
ast m
ilk. L
oxap
ine
and
its m
etab
olite
s ar
e pr
esen
t in
the
brea
st m
ilk o
f lac
tatin
g do
gs.
Disc
ontin
ue d
rug
or n
ursin
g, ta
king
into
con
sider
atio
n im
porta
nce
of d
rug
to m
othe
r.La
tuda
lu
rasid
one (
SGA)
Schi
zoph
reni
a: 13
and
old
er40
–80
mg
daily
Addi
tiona
l Bla
ck B
ox W
arni
ngs:
Incr
ease
d ris
k of
su
icida
l thi
nkin
g an
d be
havi
or in
shor
t-te
rm st
udie
s in
chi
ldre
n, a
doles
cent
s, an
d yo
ung
adul
ts ta
king
an
tidep
ress
ants.
Mon
itor f
or w
orse
ning
and
em
erge
nce
of su
icida
l tho
ught
s and
beh
avio
rs.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in
pre
gnan
t wom
en. N
o ad
vers
e de
velo
pmen
tal o
r te
rato
geni
c ef
fect
s wer
e se
en in
ani
mal
studi
es.
Lacta
tion:
It is
not
kno
wn if
lura
sidon
e an
d its
m
etab
olite
s are
exc
rete
d in
hum
an b
reas
t milk
. It
is e
xcre
ted
in th
e m
ilk o
f rat
s dur
ing
lacta
tion.
Mob
an
moli
ndon
e† (F
GA)
Schi
zoph
reni
a: 12
and
old
er15
mg–
225
mg
daily
de
pend
ing
on th
e se
verit
y of
the
diso
rder
and
resp
onse
to
trea
tmen
t
War
ning
s and
pre
caut
ions:
Dro
wsin
ess i
s the
mos
t fre
quen
tly o
ccur
ring
adve
rse
effe
ct.
Preg
nanc
y: A
nim
al re
prod
uctiv
e stu
dies
hav
e no
t de
mon
strat
ed a
tera
toge
nic
pote
ntia
l. The
ben
efits
m
ust b
e we
ighe
d ag
ains
t the
unk
nown
risk
s to
the
fetu
s if u
sed
in p
regn
ant p
atie
nts.
PB-Child & Adolescent Dosing.indd 47 05-02-2018 16:02:26
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
48Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
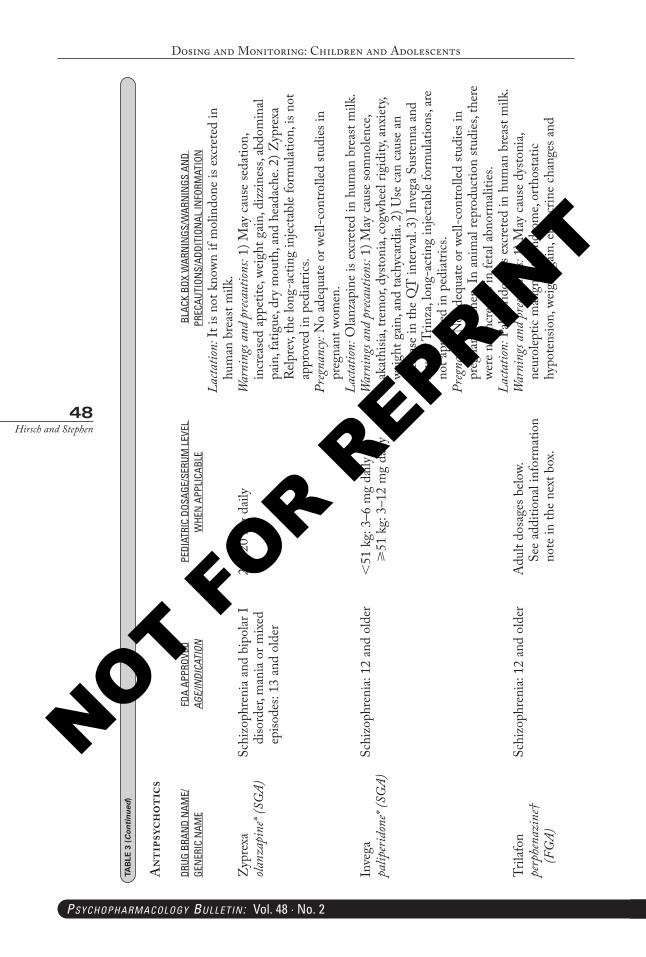
Lacta
tion:
It is
not
kno
wn if
mol
indo
ne is
exc
rete
d in
hu
man
bre
ast m
ilk.
Zyp
rexa
ola
nzap
ine*
(SG
A)Sc
hizo
phre
nia
and
bipo
lar I
diso
rder
, man
ia o
r mix
ed
episo
des:
13 a
nd o
lder
2.5–
20 m
g da
ilyW
arni
ngs a
nd p
reca
ution
s: 1)
May
cau
se se
datio
n,
incr
ease
d ap
petit
e, we
ight
gai
n, d
izzi
ness
, abd
omin
al pa
in, f
atig
ue, d
ry m
outh
, and
hea
dach
e. 2)
Zyp
rexa
R
elpre
v, th
e lo
ng-a
ctin
g in
jecta
ble
form
ulat
ion,
is n
ot
appr
oved
in p
edia
trics
.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pr
egna
nt w
omen
.La
ctatio
n: O
lanza
pine
is e
xcre
ted
in h
uman
bre
ast m
ilk.
Inve
ga
palip
erid
one*
(SG
A)Sc
hizo
phre
nia:
12 a
nd o
lder
<51
kg:
3–6
mg
daily
⩾
51 k
g: 3
–12
mg
daily
War
ning
s and
pre
caut
ions:
1) M
ay c
ause
som
nolen
ce,
akat
hisia
, tre
mor
, dys
toni
a, co
gwhe
el rig
idity
, anx
iety,
we
ight
gai
n, a
nd ta
chyc
ardi
a. 2)
Use
can
cau
se a
n in
crea
se in
the
QT
inte
rval.
3) I
nveg
a Su
stenn
a an
d In
vega
Trin
za, l
ong-
actin
g in
jecta
ble
form
ulat
ions
, are
no
t app
rove
d in
ped
iatri
cs.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in
preg
nant
wom
en. I
n an
imal
repr
oduc
tion
studi
es, t
here
we
re n
o in
crea
ses i
n fe
tal a
bnor
mali
ties.
Lacta
tion:
Pali
perid
one
is ex
cret
ed in
hum
an b
reas
t milk
.Tr
ilafo
n pe
rphe
nazi
ne†
(FG
A)
Schi
zoph
reni
a: 12
and
old
erA
dult
dosa
ges b
elow.
Se
e ad
ditio
nal i
nfor
mat
ion
note
in th
e ne
xt b
ox.
War
ning
s and
pre
caut
ions:
1) M
ay c
ause
dys
toni
a, ne
urol
eptic
mali
gnan
t syn
drom
e, or
thos
tatic
hy
pote
nsio
n, w
eigh
t gai
n, e
ndoc
rine
chan
ges a
nd
TAB
LE 3
(Continued
)
Ant
ipsy
chot
ics
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 48 05-02-2018 16:02:26
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
49Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
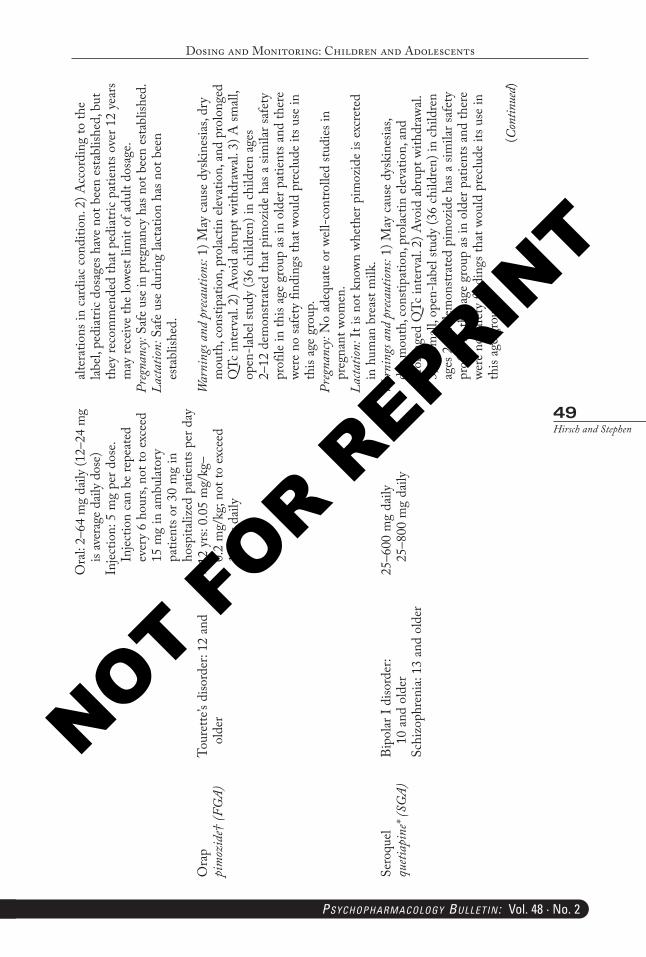
Ora
l: 2–
64 m
g da
ily (1
2–24
mg
is av
erag
e dail
y do
se)
Injec
tion:
5 m
g pe
r dos
e. In
jectio
n ca
n be
repe
ated
ev
ery
6 ho
urs,
not t
o ex
ceed
15
mg
in a
mbu
lator
y pa
tient
s or 3
0 m
g in
ho
spita
lized
pat
ient
s per
day
alter
atio
ns in
car
diac
con
ditio
n. 2
) Acc
ordi
ng to
the
label,
ped
iatri
c do
sage
s hav
e no
t bee
n es
tabl
ished
, but
th
ey re
com
men
ded
that
ped
iatri
c pat
ient
s ove
r 12
year
s m
ay re
ceiv
e th
e lo
west
limit
of a
dult
dosa
ge.
Preg
nanc
y: Sa
fe u
se in
pre
gnan
cy h
as n
ot b
een
esta
blish
ed.
Lacta
tion:
Saf
e us
e du
ring
lacta
tion
has n
ot b
een
esta
blish
ed.
Ora
p pi
moz
ide†
(FG
A)To
uret
te’s
diso
rder
: 12
and
olde
r⩾
12 y
rs: 0
.05
mg/
kg–
0.2
mg/
kg; n
ot to
exc
eed
10 m
g da
ily
War
ning
s and
pre
caut
ions:
1) M
ay c
ause
dys
kine
sias,
dry
mou
th, c
onsti
patio
n, p
rolac
tin e
leva
tion,
and
pro
long
ed
QTc
inte
rval.
2) A
void
abr
upt w
ithdr
awal.
3) A
small
, op
en-la
bel s
tudy
(36
child
ren)
in c
hild
ren
ages
2–
12 d
emon
strat
ed th
at p
imoz
ide
has a
sim
ilar s
afet
y pr
ofile
in th
is ag
e gr
oup
as in
old
er p
atie
nts a
nd th
ere
were
no
safe
ty fi
ndin
gs th
at w
ould
pre
clude
its u
se in
th
is ag
e gr
oup.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in
preg
nant
wom
en.
Lacta
tion:
It is
not
kno
wn w
heth
er p
imoz
ide
is ex
cret
ed
in h
uman
bre
ast m
ilk.
Sero
quel
queti
apin
e* (S
GA)
Bipo
lar I
diso
rder
: 10
and
old
erSc
hizo
phre
nia:
13 a
nd o
lder
25–6
00 m
g da
ily
25–8
00 m
g da
ilyW
arni
ngs a
nd p
reca
ution
s: 1)
May
cau
se d
yski
nesia
s, dr
y m
outh
, con
stipa
tion,
pro
lactin
ele
vatio
n, a
nd
prol
onge
d Q
Tc in
terv
al. 2
) Avo
id a
brup
t with
draw
al.
3) A
small
, ope
n-lab
el stu
dy (3
6 ch
ildre
n) in
chi
ldre
n ag
es 2
–12
dem
onstr
ated
pim
ozid
e ha
s a si
mila
r saf
ety
prof
ile in
this
age
grou
p as
in o
lder
pat
ient
s and
ther
e we
re n
o sa
fety
find
ings
that
wou
ld p
reclu
de it
s use
in
this
age
grou
p.(C
ontin
ued)
PB-Child & Adolescent Dosing.indd 49 05-02-2018 16:02:27
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
50Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in
preg
nant
wom
en.
Lacta
tion:
It is
not
kno
wn w
heth
er p
imoz
ide
is ex
cret
ed
in h
uman
bre
ast m
ilk.
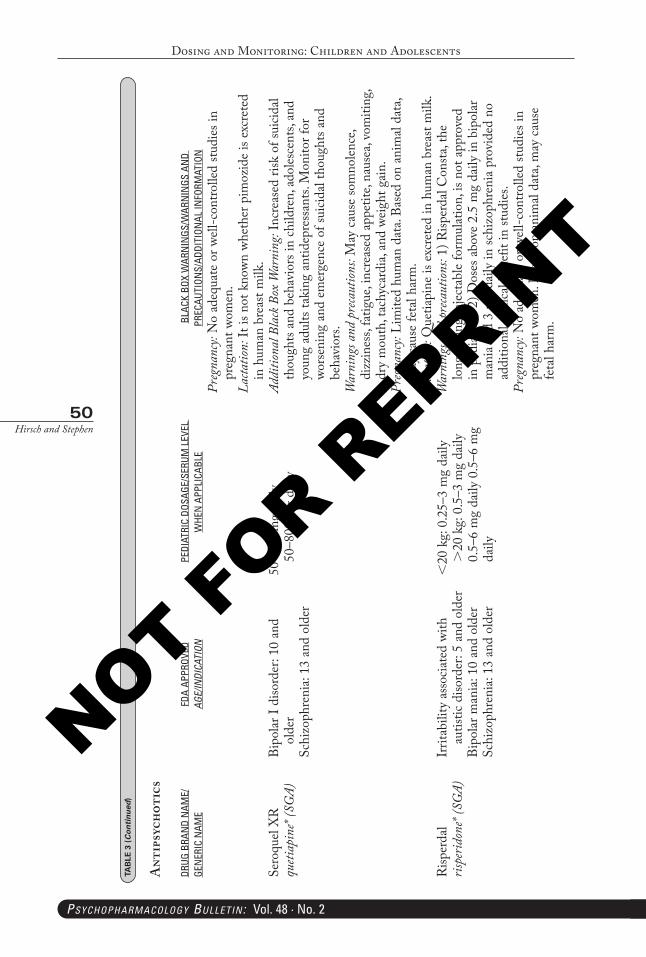
Sero
quel
XR
queti
apin
e* (S
GA)
Bipo
lar I
diso
rder
: 10
and
olde
rSc
hizo
phre
nia:
13 a
nd o
lder
50–6
00 m
g da
ily
50–8
00 m
g da
ilyAd
ditio
nal B
lack
Box
War
ning
: Inc
reas
ed ri
sk o
f sui
cidal
thou
ghts
and
beha
vior
s in
child
ren,
ado
lesce
nts,
and
youn
g ad
ults
taki
ng a
ntid
epre
ssan
ts. M
onito
r for
wo
rsen
ing
and
emer
genc
e of
suici
dal t
houg
hts a
nd
beha
vior
s.W
arni
ngs a
nd p
reca
ution
s: M
ay c
ause
som
nolen
ce,
dizz
ines
s, fa
tigue
, inc
reas
ed a
ppet
ite, n
ause
a, vo
miti
ng,
dry
mou
th, t
achy
card
ia, a
nd w
eigh
t gai
n.Pr
egna
ncy:
Lim
ited
hum
an d
ata.
Base
d on
ani
mal
data
, m
ay c
ause
feta
l har
m.
Lacta
tion:
Que
tiapi
ne is
exc
rete
d in
hum
an b
reas
t milk
.R
isper
dal
rispe
ridon
e* (S
GA)
Irrit
abili
ty a
ssoc
iate
d wi
th
autis
tic d
isord
er: 5
and
old
erBi
polar
man
ia: 1
0 an
d ol
der
Schi
zoph
reni
a: 13
and
old
er
<20
kg:
0.2
5–3
mg
daily
>
20 k
g: 0
.5–3
mg
daily
0.
5–6
mg
daily
0.5
–6 m
g da
ily
War
ning
s and
pre
caut
ions:
1) R
isper
dal C
onsta
, the
lo
ng-a
ctin
g in
jecta
ble
form
ulat
ion,
is n
ot a
ppro
ved
in p
edia
trics
. 2) D
oses
abo
ve 2
.5 m
g da
ily in
bip
olar
m
ania
and
3 m
g da
ily in
schi
zoph
reni
a pr
ovid
ed n
o ad
ditio
nal c
linica
l ben
efit
in st
udie
s.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pr
egna
nt w
omen
. Bas
ed o
n an
imal
data
, may
cau
se
feta
l har
m.
TAB
LE 3
(Continued
)
Ant
ipsy
chot
ics
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 50 05-02-2018 16:02:27
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
51Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
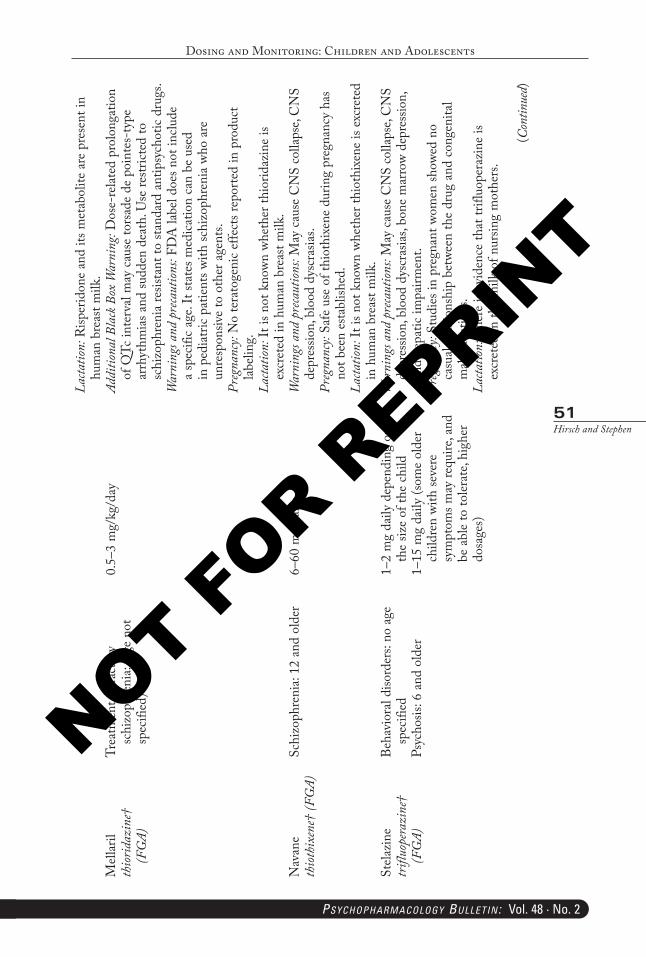
Lacta
tion:
Risp
erid
one
and
its m
etab
olite
are
pre
sent
in
hum
an b
reas
t milk
.M
ellar
ilth
iorid
azin
e†
(FG
A)
Trea
tmen
t ref
ract
ory
schi
zoph
reni
a: (a
ge n
ot
spec
ified
)
0.5–
3 m
g/kg
/day
Addi
tiona
l Bla
ck B
ox W
arni
ng: D
ose-
relat
ed p
rolo
ngat
ion
of Q
Tc in
terv
al m
ay c
ause
tors
ade
de p
oint
es-t
ype
arrh
ythm
ias a
nd su
dden
dea
th. U
se re
strict
ed to
sc
hizo
phre
nia
resis
tant
to st
anda
rd a
ntip
sych
otic
drug
s.W
arni
ngs a
nd p
reca
ution
s: FD
A la
bel d
oes n
ot in
clude
a
spec
ific
age.
It st
ates
med
icatio
n ca
n be
use
d in
ped
iatri
c pa
tient
s with
schi
zoph
reni
a wh
o ar
e un
resp
onsiv
e to
oth
er a
gent
s.Pr
egna
ncy:
No
tera
toge
nic
effe
cts r
epor
ted
in p
rodu
ct
labeli
ng.
Lacta
tion:
It is
not
kno
wn w
heth
er th
iorid
azin
e is
excr
eted
in h
uman
bre
ast m
ilk.
Nav
ane
thiot
hixe
ne†
(FG
A)Sc
hizo
phre
nia:
12 a
nd o
lder
6–60
mg
daily
War
ning
s and
pre
caut
ions:
May
cau
se C
NS
colla
pse,
CN
S de
pres
sion,
blo
od d
yscr
asia
s.Pr
egna
ncy:
Safe
use
of t
hiot
hixe
ne d
urin
g pr
egna
ncy
has
not b
een
esta
blish
ed.
Lacta
tion:
It is
not
kno
wn w
heth
er th
ioth
ixen
e is
excr
eted
in
hum
an b
reas
t milk
.St
elazi
ne
trifl
uope
razi
ne†
(FG
A)
Beha
vior
al di
sord
ers:
no a
ge
spec
ified
Psyc
hosis
: 6 a
nd o
lder
1–2
mg
daily
dep
endi
ng o
n th
e siz
e of
the
child
1–15
mg
daily
(som
e ol
der
child
ren
with
seve
re
sym
ptom
s may
requ
ire, a
nd
be a
ble
to to
lerat
e, hi
gher
do
sage
s)
War
ning
s and
pre
caut
ions:
May
cau
se C
NS
colla
pse,
CN
S de
pres
sion,
blo
od d
yscr
asia
s, bo
ne m
arro
w de
pres
sion,
an
d he
patic
impa
irmen
t.Pr
egna
ncy:
Stud
ies i
n pr
egna
nt w
omen
show
ed n
o ca
sual
relat
ions
hip
betw
een
the
drug
and
con
geni
tal
malf
orm
atio
ns.
Lacta
tion:
The
re is
evi
denc
e th
at tr
ifluo
pera
zine
is
excr
eted
in th
e m
ilk o
f nur
sing
mot
hers
.
(Con
tinue
d)
PB-Child & Adolescent Dosing.indd 51 05-02-2018 16:02:27
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
52Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
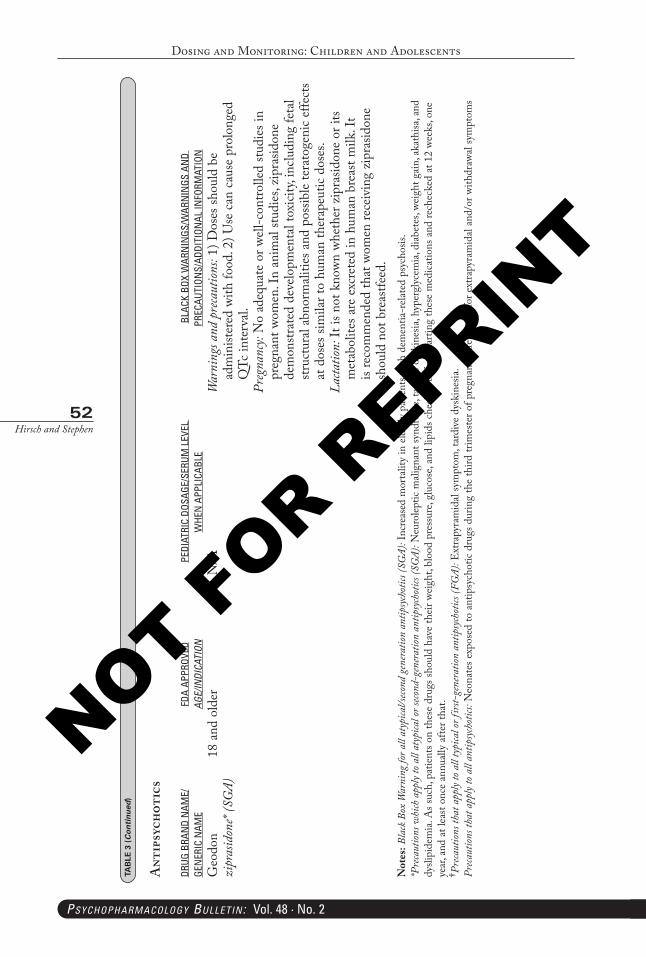
Geo
don
zipr
asid
one*
(SG
A)18
and
old
erN
/AW
arni
ngs a
nd p
reca
ution
s: 1)
Dos
es sh
ould
be
adm
inist
ered
with
food
. 2) U
se c
an c
ause
pro
long
ed
QTc
inte
rval.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in
preg
nant
wom
en. I
n an
imal
studi
es, z
ipra
sidon
e de
mon
strat
ed d
evelo
pmen
tal t
oxici
ty, in
cludi
ng fe
tal
struc
tura
l abn
orm
alitie
s and
pos
sible
tera
toge
nic
effe
cts
at d
oses
sim
ilar t
o hu
man
ther
apeu
tic d
oses
.La
ctatio
n: It
is n
ot k
nown
whe
ther
zip
rasid
one
or it
s m
etab
olite
s are
exc
rete
d in
hum
an b
reas
t milk
. It
is re
com
men
ded
that
wom
en re
ceiv
ing
zipr
asid
one
shou
ld n
ot b
reas
tfeed
.N
otes
: Bla
ck B
ox W
arni
ng fo
r all
atyp
ical/s
econd
gene
ratio
n an
tipsy
chot
ics (S
GA)
: Inc
reas
ed m
orta
lity
in e
lder
ly p
atie
nts w
ith d
emen
tia-r
elate
d ps
ycho
sis.
*Pre
caut
ions w
hich
app
ly to
all
atyp
ical o
r seco
nd-g
ener
ation
ant
ipsy
chot
ics (S
GA)
: Neu
rolep
tic m
align
ant s
yndr
ome,
tard
ive
dysk
ines
ia, h
yper
glyc
emia
, dia
bete
s, we
ight
gai
n, a
kath
isa, a
nd
dysli
pide
mia
. As s
uch,
pat
ient
s on
thes
e dr
ugs s
houl
d ha
ve th
eir w
eigh
t, bl
ood
pres
sure
, glu
cose
, and
lipi
ds c
heck
ed b
efor
e sta
rting
thes
e m
edica
tions
and
rech
ecke
d at
12
week
s, on
e ye
ar, a
nd a
t lea
st on
ce a
nnua
lly a
fter t
hat.
† Preca
ution
s tha
t app
ly to
all
typi
cal o
r firs
t-ge
nera
tion
antip
sych
otics
(FG
A): E
xtra
pyra
mid
al sy
mpt
om, t
ardi
ve d
yski
nesia
.Pr
ecaut
ions t
hat a
pply
to a
ll an
tipsy
chot
ics: N
eona
tes e
xpos
ed to
ant
ipsy
chot
ic dr
ugs d
urin
g th
e th
ird tr
imes
ter o
f pre
gnan
cy a
re a
t risk
for e
xtra
pyra
mid
al an
d/or
with
draw
al sy
mpt
oms
TAB
LE 3
(Continued
)
Ant
ipsy
chot
ics
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 52 05-02-2018 16:02:27
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
53Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
TAB
LE 4
Ant
idep
ress
ants
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM
LEVE
L W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
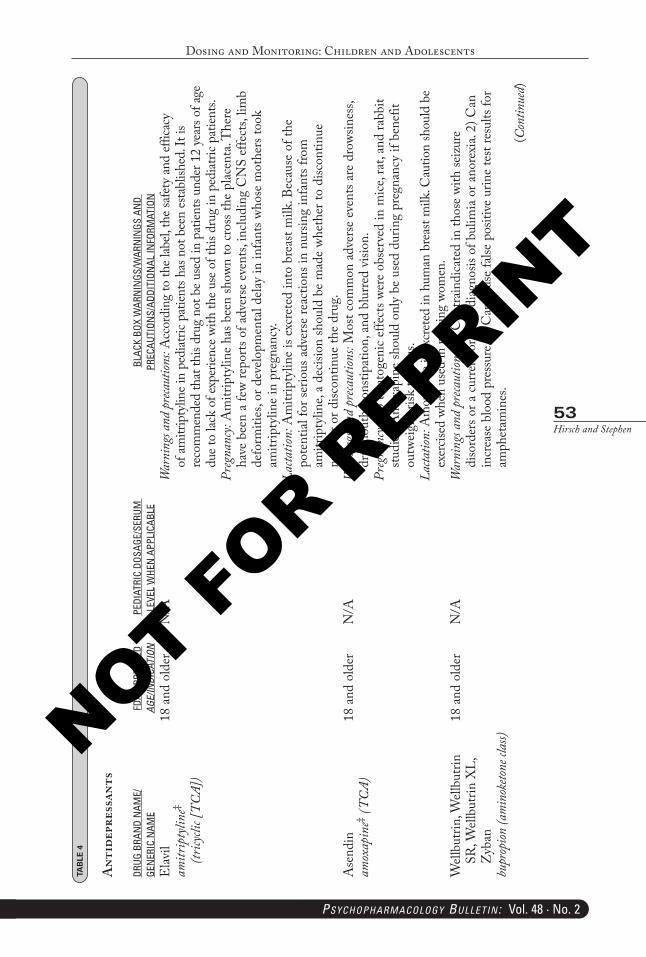
Elav
il am
itrip
tylin
e‡ (tr
icycli
c [TC
A])
18 a
nd o
lder
N/A
War
ning
s and
preca
ution
s: A
ccor
ding
to th
e lab
el, th
e saf
ety a
nd ef
ficac
y of
amitr
ipty
line i
n pe
diat
ric p
atien
ts ha
s not
bee
n es
tabl
ished
. It i
s re
com
men
ded
that
this
drug
not
be u
sed
in p
atien
ts un
der 1
2 ye
ars o
f age
du
e to
lack
of ex
perie
nce w
ith th
e use
of t
his d
rug
in p
ediat
ric p
atien
ts.Pr
egna
ncy:
Am
itrip
tylin
e ha
s bee
n sh
own
to c
ross
the
plac
enta
. The
re
have
bee
n a
few
repo
rts o
f adv
erse
eve
nts,
inclu
ding
CN
S ef
fect
s, lim
b de
form
ities
, or d
evelo
pmen
tal d
elay
in in
fant
s who
se m
othe
rs to
ok
amitr
ipty
line
in p
regn
ancy
.La
ctatio
n: A
mitr
ipty
line
is ex
cret
ed in
to b
reas
t milk
. Bec
ause
of t
he
pote
ntia
l for
serio
us a
dver
se re
actio
ns in
nur
sing
infa
nts f
rom
am
itrip
tylin
e, a
decis
ion
shou
ld b
e m
ade
whet
her t
o di
scon
tinue
nu
rsin
g or
disc
ontin
ue th
e dr
ug.
Ase
ndin
am
oxap
ine‡ (
TCA)
18 a
nd o
lder
N/A
War
ning
s and
pre
caut
ions:
Mos
t com
mon
adv
erse
eve
nts a
re d
rows
ines
s, dr
y m
outh
, con
stipa
tion,
and
blu
rred
visio
n.Pr
egna
ncy:
No
tera
toge
nic
effe
cts w
ere
obse
rved
in m
ice, r
at, a
nd ra
bbit
studi
es. A
mox
apin
e sh
ould
onl
y be
use
d du
ring
preg
nanc
y if
bene
fit
outw
eigh
s risk
to fe
tus.
Lacta
tion:
Am
oxap
ine i
s exc
rete
d in
hum
an b
reas
t milk
. Cau
tion
shou
ld b
e ex
ercis
ed w
hen
used
in n
ursin
g wo
men
.W
ellbu
trin,
Well
butri
n SR
, Well
butri
n X
L,
Zyb
anbu
prop
ion (a
min
oketo
ne cl
ass)
18 a
nd o
lder
N/A
War
ning
s and
pre
caut
ions:
1) C
ontra
indi
cate
d in
thos
e wi
th se
izur
e di
sord
ers o
r a cu
rrent
or p
rior d
iagno
sis o
f bul
imia
or a
nore
xia.
2) C
an
incr
ease
blo
od p
ress
ure.
3) C
an c
ause
false
pos
itive
urin
e te
st re
sults
for
amph
etam
ines
.(C
ontin
ued)
PB-Child & Adolescent Dosing.indd 53 05-02-2018 16:02:27
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
54Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
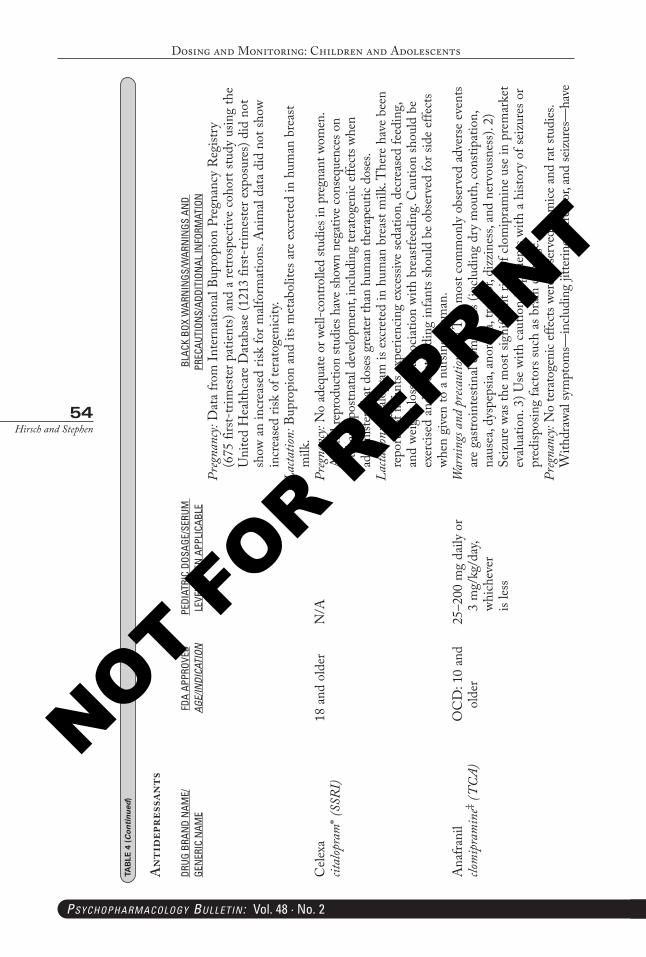
Preg
nanc
y: D
ata
from
Inte
rnat
iona
l Bup
ropi
on P
regn
ancy
Reg
istry
(6
75 fi
rst-
trim
este
r pat
ient
s) an
d a
retro
spec
tive
coho
rt stu
dy u
sing
the
Uni
ted
Hea
lthca
re D
atab
ase
(121
3 fir
st-tri
mes
ter e
xpos
ures
) did
not
sh
ow a
n in
crea
sed
risk
for m
alfor
mat
ions
. Ani
mal
data
did
not
show
in
crea
sed
risk
of te
rato
geni
city.
Lacta
tion:
Bup
ropi
on a
nd it
s met
abol
ites a
re e
xcre
ted
in h
uman
bre
ast
milk
.C
elexa
cital
opra
m* (
SSRI
)18
and
old
erN
/APr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pre
gnan
t wom
en.
Ani
mal
repr
oduc
tion
studi
es h
ave s
hown
neg
ative
cons
eque
nces
on
feta
l and
pos
tnat
al de
velo
pmen
t, in
cludi
ng te
rato
geni
c effe
cts w
hen
adm
inist
ered
at d
oses
gre
ater
than
hum
an th
erap
eutic
dos
es.
Lacta
tion:
Cita
lopr
am is
exc
rete
d in
hum
an b
reas
t milk
. The
re h
ave
been
re
ports
of i
nfan
ts ex
perie
ncin
g ex
cess
ive
seda
tion,
dec
reas
ed fe
edin
g, an
d we
ight
loss
in a
ssoc
iatio
n wi
th b
reas
tfeed
ing.
Cau
tion
shou
ld b
e ex
ercis
ed a
nd b
reas
tfeed
ing
infa
nts s
houl
d be
obs
erve
d fo
r sid
e ef
fect
s wh
en g
iven
to a
nur
sing
wom
an.
Ana
frani
lclo
mip
ram
ine‡ (
TCA)
OC
D: 1
0 an
d ol
der
25–2
00 m
g da
ily o
r 3
mg/
kg/d
ay,
which
ever
is
less
War
ning
s and
pre
caut
ions:
1) T
he m
ost c
omm
only
obs
erve
d ad
vers
e ev
ents
are
gastr
oint
estin
al co
mpl
aint
s (in
cludi
ng d
ry m
outh
, con
stipa
tion,
na
usea
, dys
peps
ia, a
nore
xia,
trem
or, d
izzi
ness
, and
ner
vous
ness
). 2)
Se
izur
e wa
s the
mos
t sig
nific
ant r
isk o
f clo
mip
ram
ine
use
in p
rem
arke
t ev
aluat
ion.
3) U
se w
ith c
autio
n in
pat
ient
s with
a h
istor
y of
seiz
ures
or
pred
ispos
ing
fact
ors s
uch
as b
rain
dam
age.
Preg
nanc
y: N
o te
rato
geni
c effe
cts w
ere o
bser
ved
in m
ice an
d ra
t stu
dies
. W
ithdr
awal
sym
ptom
s—in
cludi
ng ji
tterin
ess,
trem
or, a
nd se
izure
s—ha
ve
TAB
LE 4
(Continued
)
Ant
idep
ress
ants
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM
LEVE
L W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 54 05-02-2018 16:02:27
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
55Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
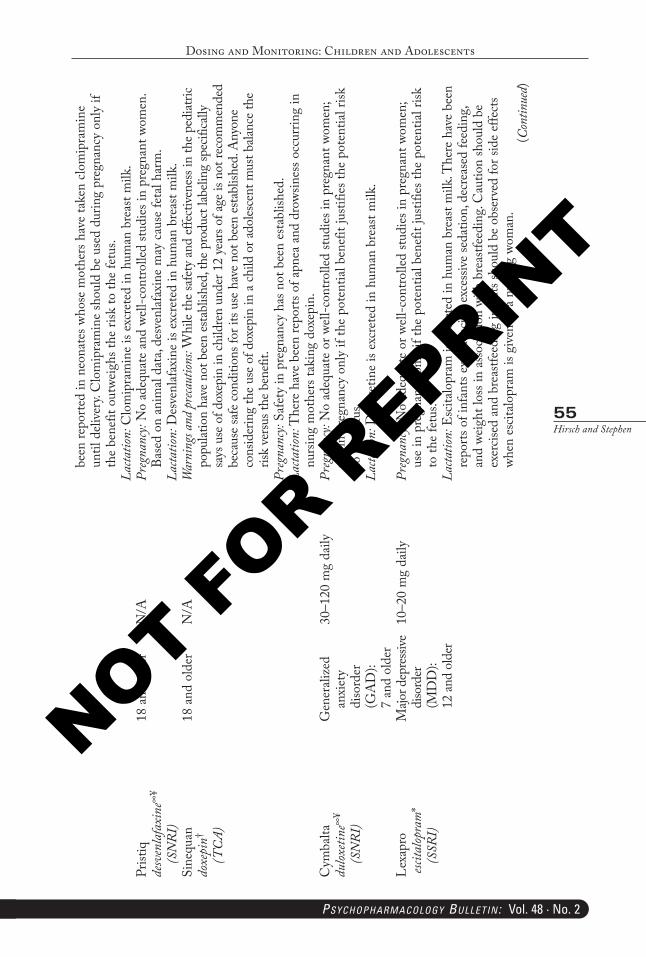
been
repo
rted
in n
eona
tes w
hose
mot
hers
hav
e ta
ken
clom
ipra
min
e un
til d
elive
ry. C
lom
ipra
min
e sh
ould
be
used
dur
ing
preg
nanc
y on
ly if
th
e be
nefit
out
weig
hs th
e ris
k to
the
fetu
s.La
ctatio
n: C
lom
ipra
min
e is
excr
eted
in h
uman
bre
ast m
ilk.
Prist
iqde
sven
lafa
xine
∞¥
(SN
RI)
18 a
nd o
lder
N/A
Preg
nanc
y: N
o ad
equa
te a
nd w
ell-c
ontro
lled
studi
es in
pre
gnan
t wom
en.
Base
d on
ani
mal
data
, des
venl
afax
ine
may
cau
se fe
tal h
arm
.La
ctatio
n: D
esve
nlaf
axin
e is
excr
eted
in h
uman
bre
ast m
ilk.
Sine
quan
do
xepi
n† (T
CA)
18 a
nd o
lder
N/A
War
ning
s and
prec
autio
ns: W
hile
the s
afet
y an
d ef
fect
ivene
ss in
the p
ediat
ric
popu
latio
n ha
ve n
ot b
een
esta
blish
ed, t
he p
rodu
ct la
belin
g sp
ecifi
cally
sa
ys u
se o
f dox
epin
in ch
ildre
n un
der 1
2 ye
ars o
f age
is n
ot re
com
men
ded
beca
use s
afe c
ondi
tions
for i
ts us
e hav
e not
bee
n es
tabl
ished
. Any
one
cons
ider
ing
the u
se o
f dox
epin
in a
child
or a
doles
cent
mus
t bala
nce t
he
risk
versu
s the
ben
efit.
Preg
nanc
y: Sa
fety
in p
regn
ancy
has
not
bee
n es
tabl
ished
.La
ctatio
n: T
here
hav
e be
en re
ports
of a
pnea
and
dro
wsin
ess o
ccur
ring
in
nurs
ing
mot
hers
taki
ng d
oxep
in.
Cym
balta
du
loxeti
ne∞
¥ (S
NRI
)
Gen
erali
zed
anxi
ety
diso
rder
(G
AD
):
7 an
d ol
der
30–1
20 m
g da
ilyPr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pre
gnan
t wom
en;
use
in p
regn
ancy
onl
y if
the
pote
ntia
l ben
efit
justi
fies t
he p
oten
tial r
isk
to th
e fe
tus.
Lacta
tion:
Dul
oxet
ine
is ex
cret
ed in
hum
an b
reas
t milk
.
Lexa
pro
escit
alop
ram
* (S
SRI)
Majo
r dep
ressi
ve
diso
rder
(M
DD
):
12 an
d ol
der
10–2
0 m
g da
ilyPr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pre
gnan
t wom
en;
use
in p
regn
ancy
onl
y if
the
pote
ntia
l ben
efit
justi
fies t
he p
oten
tial r
isk
to th
e fe
tus.
Lacta
tion:
Esc
italo
pram
is e
xcre
ted
in h
uman
bre
ast m
ilk. T
here
hav
e be
en
repo
rts o
f inf
ants
expe
rienc
ing
exce
ssive
seda
tion,
dec
reas
ed fe
edin
g, an
d we
ight
loss
in a
ssoc
iatio
n wi
th b
reas
tfeed
ing.
Cau
tion
shou
ld b
e ex
ercis
ed a
nd b
reas
tfeed
ing
infa
nts s
houl
d be
obs
erve
d fo
r sid
e ef
fect
s wh
en e
scita
lopr
am is
give
n to
a n
ursin
g wo
man
.(C
ontin
ued)
PB-Child & Adolescent Dosing.indd 55 05-02-2018 16:02:27
NOT FOR R
EPRINT
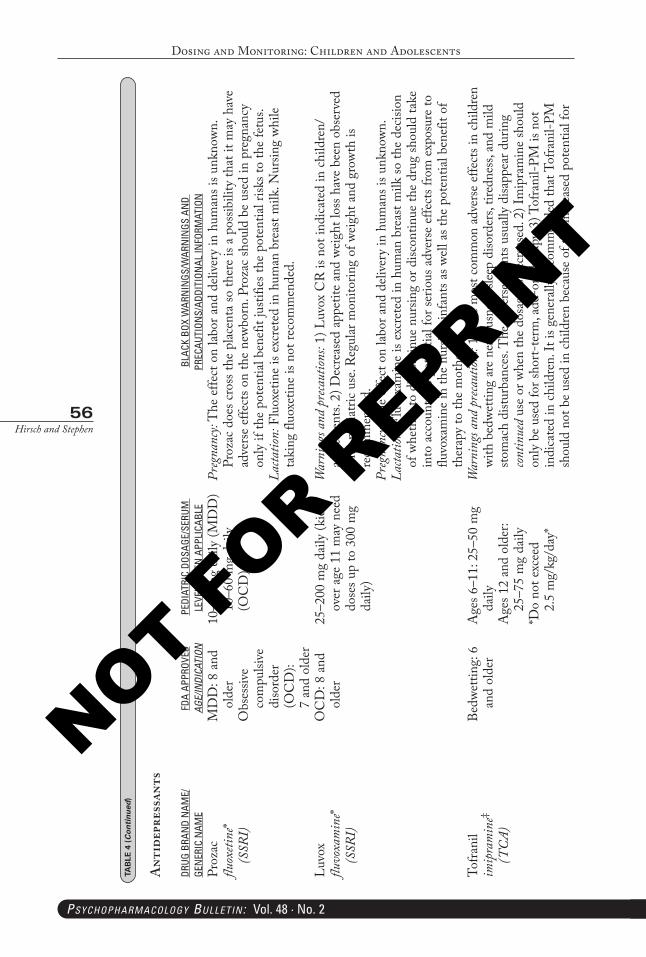
Dosing and Monitoring: Children and Adolescents
56Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Proz
ac
fluox
etine
* (S
SRI)
MD
D: 8
and
ol
der
Obs
essiv
e co
mpu
lsive
di
sord
er
(OC
D):
7
and
olde
r
10–2
0 m
g da
ily (M
DD
) 10
–60
mg
daily
(O
CD
)
Preg
nanc
y: T
he e
ffect
on
labor
and
deli
very
in h
uman
s is u
nkno
wn.
Proz
ac d
oes c
ross
the
plac
enta
so th
ere
is a
poss
ibili
ty th
at it
may
hav
e ad
vers
e ef
fect
s on
the
newb
orn.
Pro
zac
shou
ld b
e us
ed in
pre
gnan
cy
only
if th
e po
tent
ial b
enef
it ju
stifie
s the
pot
entia
l risk
s to
the
fetu
s.La
ctatio
n: F
luox
etin
e is
excr
eted
in h
uman
bre
ast m
ilk. N
ursin
g wh
ile
taki
ng fl
uoxe
tine
is no
t rec
omm
ende
d.
Luvo
x flu
voxa
min
e*
(SSR
I)
OC
D: 8
and
ol
der
25–2
00 m
g da
ily (k
ids
over
age
11
may
nee
d do
ses u
p to
300
mg
daily
)
War
ning
s and
pre
caut
ions:
1) L
uvox
CR
is n
ot in
dica
ted
in c
hild
ren/
adol
esce
nts.
2) D
ecre
ased
app
etite
and
wei
ght l
oss h
ave
been
obs
erve
d wi
th p
edia
tric
use.
Reg
ular
mon
itorin
g of
wei
ght a
nd g
row
th is
re
com
men
ded.
Preg
nanc
y: T
he e
ffect
on
labor
and
deli
very
in h
uman
s is u
nkno
wn.
Lacta
tion:
Flu
voxa
min
e is
excr
eted
in h
uman
bre
ast m
ilk so
the
decis
ion
of w
heth
er to
disc
ontin
ue n
ursin
g or
disc
ontin
ue th
e dr
ug sh
ould
take
in
to a
ccou
nt th
e po
tent
ial f
or se
rious
adv
erse
effe
cts f
rom
exp
osur
e to
flu
voxa
min
e in
the
nurs
ing
infa
nts a
s well
as t
he p
oten
tial b
enef
it of
th
erap
y to
the
mot
her.
Tofra
nil
imip
ram
ine‡
(TC
A)
Bedw
ettin
g: 6
an
d ol
der
Age
s 6–1
1: 2
5–50
mg
daily
Age
s 12
and
olde
r:
25–7
5 m
g da
ily*D
o no
t exc
eed
2.
5 m
g/kg
/day
*
War
ning
s and
pre
caut
ions:
1) T
he m
ost c
omm
on a
dver
se e
ffect
s in
child
ren
with
bed
wetti
ng a
re n
ervo
usne
ss, s
leep
diso
rder
s, tir
edne
ss, a
nd m
ild
stom
ach
distu
rban
ces.
The
adv
erse
eve
nts u
suall
y di
sapp
ear d
urin
g co
ntin
ued
use
or w
hen
the
dosa
ge is
dec
reas
ed. 2
) Im
ipra
min
e sh
ould
on
ly b
e us
ed fo
r sho
rt-te
rm, a
dd-o
n th
erap
y. 3)
Tof
rani
l-PM
is n
ot
indi
cate
d in
child
ren.
It is
gen
erall
y re
com
men
ded
that
Tof
rani
l-PM
sh
ould
not
be
used
in ch
ildre
n be
caus
e of
the
incr
ease
d po
tent
ial fo
r
TAB
LE 4
(Continued
)
Ant
idep
ress
ants
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM
LEVE
L W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 56 05-02-2018 16:02:27
NOT FOR R
EPRINT
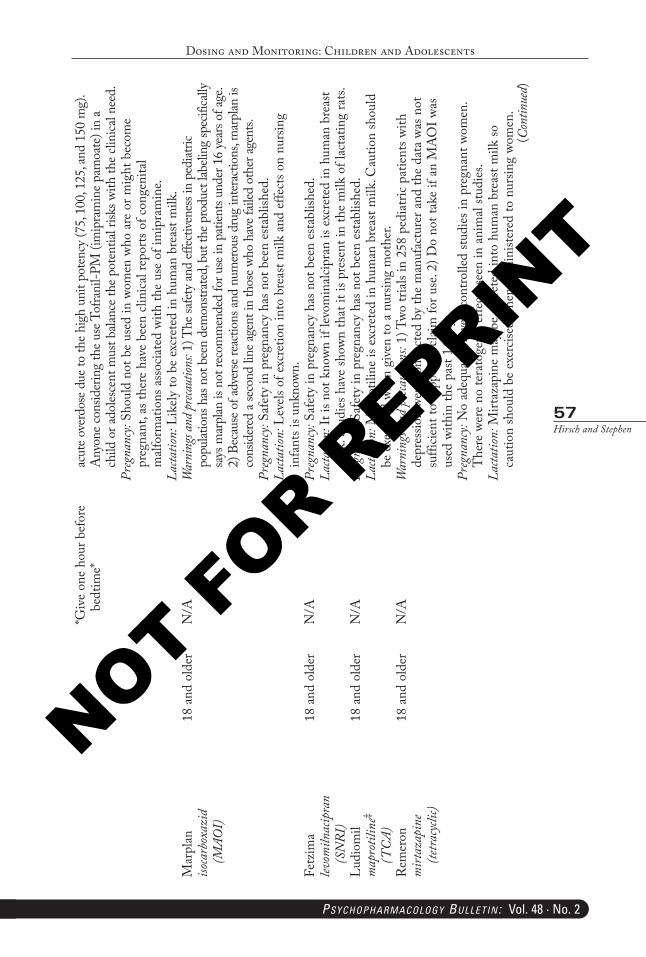
Dosing and Monitoring: Children and Adolescents
57Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
*Giv
e on
e ho
ur b
efor
e be
dtim
e*ac
ute o
verd
ose d
ue to
the h
igh
unit
pote
ncy (
75, 1
00, 1
25, a
nd 1
50 m
g).
Any
one c
onsid
erin
g th
e use
Tof
rani
l-PM
(im
ipra
min
e pam
oate
) in
a ch
ild o
r ado
lesce
nt m
ust b
alanc
e the
pot
entia
l risk
s with
the c
linica
l nee
d.Pr
egna
ncy:
Shou
ld n
ot b
e us
ed in
wom
en w
ho a
re o
r mig
ht b
ecom
e pr
egna
nt, a
s the
re h
ave
been
clin
ical r
epor
ts of
con
geni
tal
malf
orm
atio
ns a
ssoc
iate
d wi
th th
e us
e of
imip
ram
ine.
Lacta
tion:
Lik
ely
to b
e ex
cret
ed in
hum
an b
reas
t milk
.M
arpl
an
isoca
rbox
azid
(M
AOI)
18 a
nd o
lder
N/A
War
ning
s and
preca
ution
s: 1)
The
safe
ty an
d ef
fecti
vene
ss in
ped
iatric
po
pulat
ions
has
not
bee
n de
mon
strat
ed, b
ut th
e pro
duct
labeli
ng sp
ecifi
cally
sa
ys m
arpl
an is
not
reco
mm
ende
d fo
r use
in p
atien
ts un
der 1
6 ye
ars o
f age
. 2)
Bec
ause
of a
dver
se re
actio
ns an
d nu
mer
ous d
rug
inte
racti
ons,
mar
plan
is
cons
ider
ed a
seco
nd li
ne ag
ent i
n th
ose w
ho h
ave f
ailed
oth
er ag
ents.
Preg
nanc
y: Sa
fety
in p
regn
ancy
has
not
bee
n es
tabl
ished
.La
ctatio
n: L
evels
of e
xcre
tion
into
bre
ast m
ilk a
nd e
ffect
s on
nurs
ing
infa
nts i
s unk
nown
.Fe
tzim
a lev
omiln
acip
ran
(S
NRI
)
18 a
nd o
lder
N/A
Preg
nanc
y: Sa
fety
in p
regn
ancy
has
not
bee
n es
tabl
ished
.La
ctatio
n: It
is n
ot k
nown
if le
vom
inalc
ipra
n is
excr
eted
in h
uman
bre
ast
milk
. Stu
dies
hav
e sh
own
that
it is
pre
sent
in th
e m
ilk o
f lac
tatin
g ra
ts.Lu
diom
il m
apro
tilin
e‡ (T
CA)
18 a
nd o
lder
N/A
Preg
nanc
y: Sa
fety
in p
regn
ancy
has
not
bee
n es
tabl
ished
.La
ctatio
n: M
apro
tilin
e is
excr
eted
in h
uman
bre
ast m
ilk. C
autio
n sh
ould
be
exe
rcise
d wh
en g
iven
to a
nur
sing
mot
her.
Rem
eron
m
irtaz
apin
e (te
tracy
clic)
18 a
nd o
lder
N/A
War
ning
s and
pre
caut
ions:
1) T
wo tr
ials
in 2
58 p
edia
tric
patie
nts w
ith
depr
essio
n we
re c
ondu
cted
by
the
man
ufac
ture
r and
the
data
was
not
su
fficie
nt to
supp
ort a
clai
m fo
r use
. 2) D
o no
t tak
e if
an M
AO
I was
us
ed w
ithin
the
past
14 d
ays.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant w
omen
. T
here
wer
e no
tera
toge
nic
effe
cts s
een
in a
nim
al stu
dies
.La
ctatio
n: M
irtaz
apin
e m
ay b
e ex
cret
ed in
to h
uman
bre
ast m
ilk so
ca
utio
n sh
ould
be
exer
cised
whe
n ad
min
ister
ed to
nur
sing
wom
en.
(Con
tinue
d)
PB-Child & Adolescent Dosing.indd 57 05-02-2018 16:02:27
NOT FOR R
EPRINT
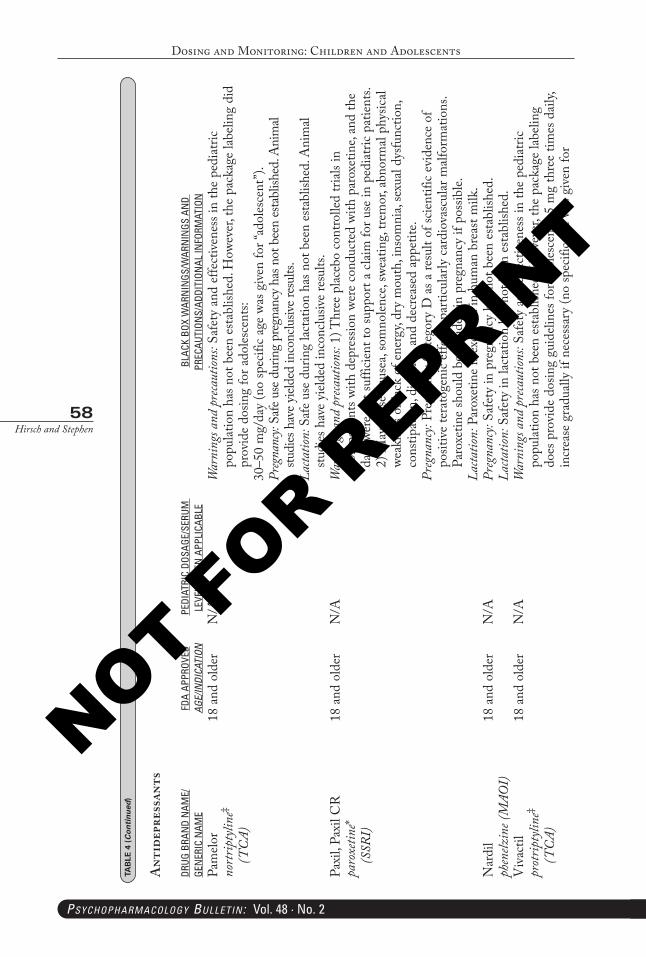
Dosing and Monitoring: Children and Adolescents
58Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Pam
elor
nort
ripty
line‡
(TC
A)
18 a
nd o
lder
N/A
War
ning
s and
pre
caut
ions:
Safe
ty a
nd e
ffect
iven
ess i
n th
e pe
diat
ric
popu
latio
n ha
s not
bee
n es
tabl
ished
. How
ever
, the
pac
kage
labe
ling
did
prov
ide
dosin
g fo
r ado
lesce
nts:
30–5
0 m
g/da
y (n
o sp
ecifi
c ag
e wa
s giv
en fo
r “ad
oles
cent
”).
Preg
nanc
y: Sa
fe u
se d
urin
g pr
egna
ncy h
as n
ot b
een
esta
blish
ed. A
nim
al stu
dies
hav
e yiel
ded
inco
nclu
sive r
esul
ts.La
ctatio
n: S
afe
use
durin
g lac
tatio
n ha
s not
bee
n es
tabl
ished
. Ani
mal
studi
es h
ave
yield
ed in
conc
lusiv
e re
sults
.Pa
xil,
Paxi
l CR
pa
roxe
tine*
(S
SRI)
18 a
nd o
lder
N/A
War
ning
s and
pre
caut
ions:
1) T
hree
plac
ebo
cont
rolle
d tri
als in
75
2 pa
tient
s with
dep
ress
ion
were
con
duct
ed w
ith p
arox
etin
e, an
d th
e da
ta w
ere
not s
uffic
ient
to su
ppor
t a c
laim
for u
se in
ped
iatri
c pa
tient
s. 2)
May
cau
se n
ause
a, so
mno
lence
, swe
atin
g, tre
mor
, abn
orm
al ph
ysica
l we
akne
ss o
r lac
k of
ene
rgy,
dry
mou
th, i
nsom
nia,
sexu
al dy
sfunc
tion,
co
nstip
atio
n, d
iarrh
ea, a
nd d
ecre
ased
app
etite
.Pr
egna
ncy:
Preg
nanc
y C
ateg
ory
D a
s a re
sult
of sc
ient
ific
evid
ence
of
posit
ive
tera
toge
nic
effe
cts,
parti
cular
ly c
ardi
ovas
cular
malf
orm
atio
ns.
Paro
xetin
e sh
ould
be
avoi
ded
in p
regn
ancy
if p
ossib
le.La
ctatio
n: P
arox
etin
e is
excr
eted
in h
uman
bre
ast m
ilk.
Nar
dil
phen
elzin
e (M
AOI)
18 a
nd o
lder
N/A
Preg
nanc
y: Sa
fety
in p
regn
ancy
has
not
bee
n es
tabl
ished
.La
ctatio
n: S
afet
y in
lact
atio
n ha
s not
bee
n es
tabl
ished
.V
ivac
til
prot
ripty
line‡
(TC
A)
18 a
nd o
lder
N/A
War
ning
s and
pre
caut
ions:
Safe
ty a
nd e
ffect
iven
ess i
n th
e pe
diat
ric
popu
latio
n ha
s not
bee
n es
tabl
ished
. How
ever
, the
pac
kage
labe
ling
does
pro
vide
dos
ing
guid
eline
s for
ado
lesce
nts:
5 m
g th
ree
times
dai
ly,
incr
ease
gra
duall
y if
nece
ssar
y (n
o sp
ecifi
c ag
e wa
s giv
en fo
r
TAB
LE 4
(Continued
)
Ant
idep
ress
ants
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM
LEVE
L W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 58 05-02-2018 16:02:28
NOT FOR R
EPRINT
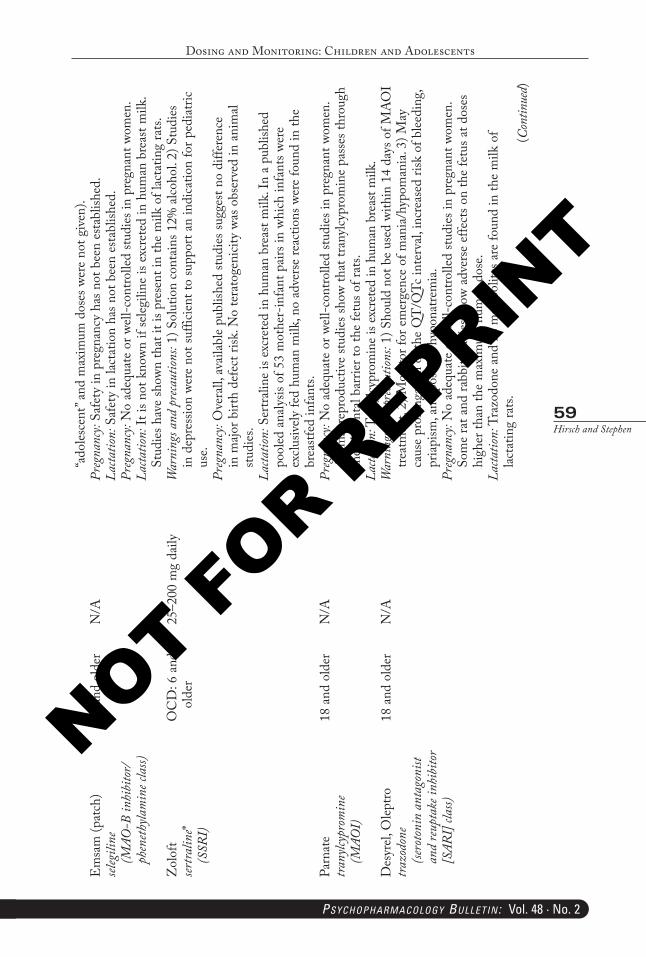
Dosing and Monitoring: Children and Adolescents
59Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
(Con
tinue
d)
“ado
lesce
nt” a
nd m
axim
um d
oses
wer
e no
t giv
en).
Em
sam
(pat
ch)
seleg
iline
(M
AO-B
inhi
bito
r/ph
eneth
ylam
ine c
lass)
18 a
nd o
lder
N/A
Preg
nanc
y: Sa
fety
in p
regn
ancy
has
not
bee
n es
tabl
ished
.La
ctatio
n: S
afet
y in
lact
atio
n ha
s not
bee
n es
tabl
ished
.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pre
gnan
t wom
en.
Lacta
tion:
It is
not
kno
wn if
seleg
iline
is e
xcre
ted
in h
uman
bre
ast m
ilk.
Stud
ies h
ave
show
n th
at it
is p
rese
nt in
the
milk
of l
acta
ting
rats.
Zol
oft
sertra
line*
(S
SRI)
OC
D: 6
and
ol
der
25–2
00 m
g da
ilyW
arni
ngs a
nd p
reca
ution
s: 1)
Sol
utio
n co
ntai
ns 1
2% a
lcoho
l. 2)
Stu
dies
in
dep
ress
ion
were
not
suffi
cient
to su
ppor
t an
indi
catio
n fo
r ped
iatri
c us
e.Pr
egna
ncy:
Ove
rall,
ava
ilabl
e pu
blish
ed st
udie
s sug
gest
no d
iffer
ence
in
majo
r birt
h de
fect
risk
. No
tera
toge
nicit
y wa
s obs
erve
d in
ani
mal
studi
es.
Lacta
tion:
Ser
tralin
e is
excr
eted
in h
uman
bre
ast m
ilk. I
n a
publ
ished
po
oled
ana
lysis
of 5
3 m
othe
r-in
fant
pai
rs in
whi
ch in
fant
s wer
e ex
clusiv
ely
fed
hum
an m
ilk, n
o ad
vers
e re
actio
ns w
ere
foun
d in
the
brea
stfed
infa
nts.
Parn
ate
trany
lcypr
omin
e (M
AOI)
18 a
nd o
lder
N/A
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant w
omen
. A
nim
al re
prod
uctiv
e stu
dies
show
that
tran
ylcy
prom
ine
pass
es th
roug
h th
e pl
acen
tal b
arrie
r to
the
fetu
s of r
ats.
Lacta
tion:
Tra
nylcy
prom
ine i
s exc
rete
d in
hum
an b
reas
t milk
.D
esyr
el, O
leptro
tra
zodo
ne
(sero
toni
n an
tago
nist
an
d re
upta
ke in
hibi
tor
[SAR
I] cla
ss)
18 a
nd o
lder
N/A
War
ning
s and
pre
caut
ions:
1) S
houl
d no
t be
used
with
in 1
4 da
ys o
f MA
OI
treat
men
t. 2)
Mon
itor f
or e
mer
genc
e of
man
ia/h
ypom
ania
. 3) M
ay
caus
e pr
olon
gatio
n of
the
QT
/QTc
inte
rval,
incr
ease
d ris
k of
blee
ding
, pr
iapi
sm, a
nd p
ossib
le hy
pona
trem
ia.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant w
omen
. So
me
rat a
nd ra
bbit
studi
es sh
ow a
dver
se e
ffect
s on
the
fetu
s at d
oses
hi
gher
than
the
max
imum
hum
an d
ose.
Lacta
tion:
Tra
zodo
ne a
nd it
s met
abol
ites a
re fo
und
in th
e m
ilk o
f lac
tatin
g ra
ts.
PB-Child & Adolescent Dosing.indd 59 05-02-2018 16:02:28
NOT FOR R
EPRINT
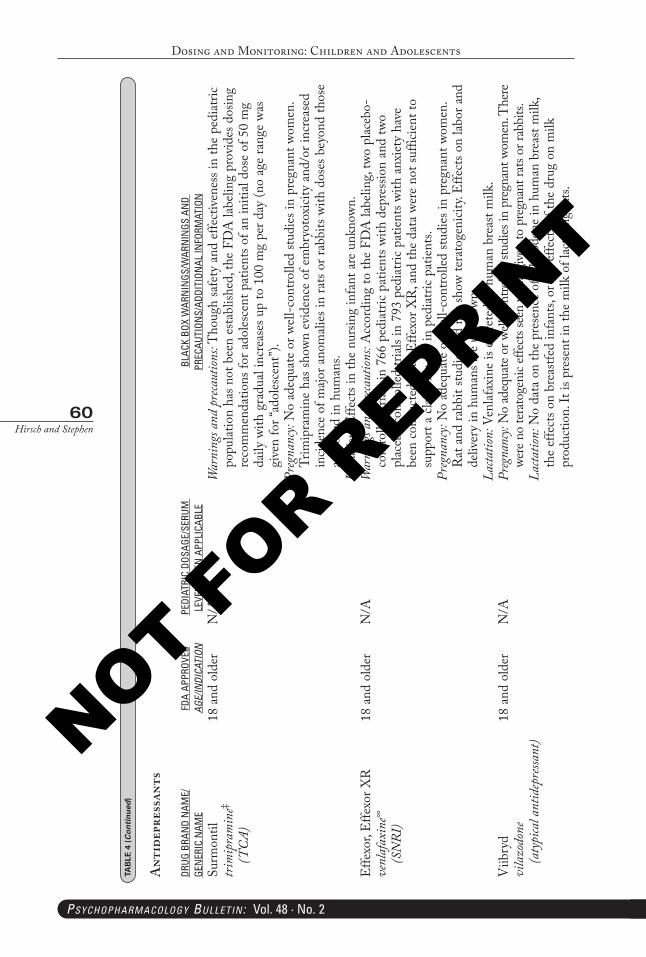
Dosing and Monitoring: Children and Adolescents
60Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Surm
ontil
tr
imip
ram
ine‡
(TC
A)
18 a
nd o
lder
N/A
War
ning
s and
pre
caut
ions:
Tho
ugh
safe
ty a
nd e
ffect
iven
ess i
n th
e pe
diat
ric
popu
latio
n ha
s not
bee
n es
tabl
ished
, the
FD
A la
belin
g pr
ovid
es d
osin
g re
com
men
datio
ns fo
r ado
lesce
nt p
atie
nts o
f an
initi
al do
se o
f 50
mg
daily
with
gra
dual
incr
ease
s up
to 1
00 m
g pe
r day
(no
age
rang
e wa
s gi
ven
for “
adol
esce
nt”)
.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pre
gnan
t wom
en.
Trim
ipra
min
e ha
s sho
wn e
vide
nce
of e
mbr
yoto
xicit
y an
d/or
incr
ease
d in
ciden
ce o
f majo
r ano
mali
es in
rats
or ra
bbits
with
dos
es b
eyon
d th
ose
appr
oved
in h
uman
s.La
ctatio
n: E
ffect
s in
the
nurs
ing
infa
nt a
re u
nkno
wn.
Effe
xor,
Effe
xor X
R
venl
afax
ine∞
(S
NRI
)
18 a
nd o
lder
N/A
War
ning
s and
pre
caut
ions:
Acc
ordi
ng to
the
FDA
labe
ling,
two
plac
ebo-
cont
rolle
d tri
als in
766
ped
iatri
c pa
tient
s with
dep
ress
ion
and
two
plac
ebo
cont
rolle
d tri
als in
793
ped
iatri
c pa
tient
s with
anx
iety
hav
e be
en c
ondu
cted
with
Effe
xor X
R, a
nd th
e da
ta w
ere
not s
uffic
ient
to
supp
ort a
clai
m fo
r use
in p
edia
tric
patie
nts.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant w
omen
. R
at a
nd ra
bbit
studi
es d
id n
ot sh
ow te
rato
geni
city.
Effe
cts o
n lab
or a
nd
deliv
ery
in h
uman
s are
unk
nown
.La
ctatio
n: V
enlaf
axin
e is
excr
eted
in h
uman
bre
ast m
ilk.
Viib
ryd
vila
zodo
ne
(aty
pica
l ant
idep
ressa
nt)
18 a
nd o
lder
N/A
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant w
omen
. The
re
were
no
tera
toge
nic e
ffect
s see
n wh
en g
iven
to p
regn
ant r
ats o
r rab
bits.
Lacta
tion:
No
data
on
the
pres
ence
of v
ilazo
done
in h
uman
bre
ast m
ilk,
the
effe
cts o
n br
eastf
ed in
fant
s, or
the
effe
cts o
f the
dru
g on
milk
pr
oduc
tion.
It is
pre
sent
in th
e m
ilk o
f lac
tatin
g ra
ts.
TAB
LE 4
(Continued
)
Ant
idep
ress
ants
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM
LEVE
L W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 60 05-02-2018 16:02:28
NOT FOR R
EPRINT
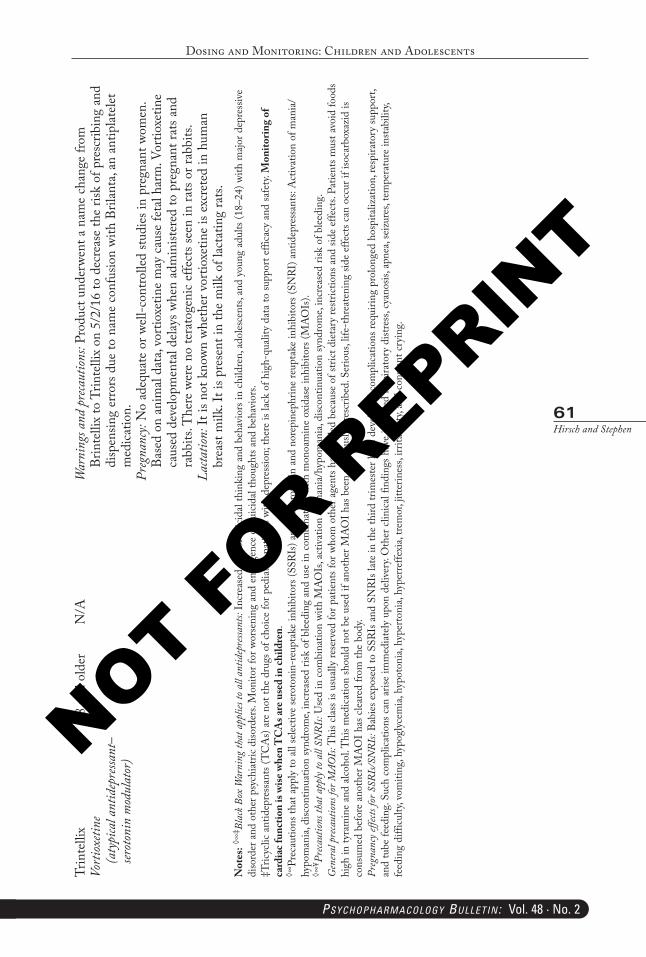
Dosing and Monitoring: Children and Adolescents
61Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Trin
telli
x Vo
rtiox
etine
(a
typi
cal a
ntid
epre
ssant
–ser
oton
in m
odul
ator
)
18 a
nd o
lder
N/A
War
ning
s and
pre
caut
ions:
Prod
uct u
nder
went
a n
ame
chan
ge fr
om
Brin
telli
x to
Trin
telli
x on
5/2
/16
to d
ecre
ase
the
risk
of p
resc
ribin
g an
d di
spen
sing
erro
rs d
ue to
nam
e co
nfus
ion
with
Bril
anta
, an
antip
latele
t m
edica
tion.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant w
omen
. Ba
sed
on a
nim
al da
ta, v
ortio
xetin
e m
ay c
ause
feta
l har
m. V
ortio
xetin
e ca
used
dev
elopm
enta
l dela
ys w
hen
adm
inist
ered
to p
regn
ant r
ats a
nd
rabb
its. T
here
wer
e no
tera
toge
nic
effe
cts s
een
in ra
ts or
rabb
its.
Lacta
tion:
It is
not
kno
wn w
heth
er v
ortio
xetin
e is
excr
eted
in h
uman
br
east
milk
. It i
s pre
sent
in th
e m
ilk o
f lac
tatin
g ra
ts.N
otes
: ◊∞‡ B
lack
Box
War
ning
that
app
lies t
o all
antid
epre
ssant
s: In
crea
sed
risk
of su
icida
l thi
nkin
g an
d be
havi
ors i
n ch
ildre
n, a
doles
cent
s, an
d yo
ung
adul
ts (1
8–24
) with
majo
r dep
ress
ive
diso
rder
and
oth
er p
sych
iatri
c di
sord
ers.
Mon
itor f
or w
orse
ning
and
em
erge
nce
of su
icida
l tho
ught
s and
beh
avio
rs.
‡Tric
yclic
ant
idep
ress
ants
(TC
As)
are
not t
he d
rugs
of c
hoice
for p
edia
tric
patie
nts w
ith d
epre
ssio
n; th
ere
is lac
k of
hig
h-qu
ality
dat
a to
supp
ort e
ffica
cy a
nd sa
fety.
Mon
itorin
g of
ca
rdia
c fun
ctio
n is
wise
whe
n T
CA
s are
use
d in
child
ren.
װPr
ecau
tions
that
app
ly to
all
selec
tive
sero
toni
n-re
upta
ke in
hibi
tors
(SSR
Is) a
nd a
ll se
roto
nin
and
nore
pine
phrin
e re
upta
ke in
hibi
tors
(SN
RI) a
ntid
epre
ssan
ts: A
ctiv
atio
n of
man
ia/
hypo
man
ia, d
iscon
tinua
tion
synd
rom
e, in
crea
sed
risk
of b
leedi
ng a
nd u
se in
com
bina
tion
with
mon
oam
ine
oxid
ase
inhi
bito
rs (M
AO
Is).
◊∞¥ P
reca
ution
s tha
t app
ly to
all
SNRI
s: U
sed
in c
ombi
natio
n wi
th M
AO
Is, a
ctiv
atio
n of
man
ia/h
ypom
ania
, disc
ontin
uatio
n sy
ndro
me,
incr
ease
d ris
k of
blee
ding
.G
ener
al p
reca
ution
s for
MAO
Is: T
his c
lass i
s usu
ally
rese
rved
for p
atie
nts f
or w
hom
oth
er a
gent
s hav
e fa
iled
beca
use
of st
rict d
ieta
ry re
strict
ions
and
side
effe
cts.
Patie
nts m
ust a
void
food
s hi
gh in
tyra
min
e an
d alc
ohol
. Thi
s med
icatio
n sh
ould
not
be
used
if a
noth
er M
AO
I has
bee
n pr
evio
usly
pre
scrib
ed. S
erio
us, l
ife-t
hrea
teni
ng si
de e
ffect
s can
occ
ur if
isoc
arbo
xazi
d is
cons
umed
bef
ore
anot
her M
AO
I has
clea
red
from
the
body
.Pr
egna
ncy e
ffects
for S
SRIs/
SNRI
s: Ba
bies
exp
osed
to S
SRIs
and
SN
RIs l
ate
in th
e th
ird tr
imes
ter h
ave
deve
lope
d co
mpl
icatio
ns re
quiri
ng p
rolo
nged
hos
pita
lizat
ion,
resp
irato
ry su
ppor
t, an
d tu
be fe
edin
g. Su
ch c
ompl
icatio
ns c
an a
rise
imm
edia
tely
upo
n de
liver
y. O
ther
clin
ical f
indi
ngs h
ave
inclu
ded
resp
irato
ry d
istre
ss, c
yano
sis, a
pnea
, sei
zure
s, te
mpe
ratu
re in
stabi
lity,
feed
ing
diffi
culty
, vom
iting
, hyp
ogly
cem
ia, h
ypot
onia
, hyp
erto
nia,
hype
rreffe
xia,
trem
or, j
itter
ines
s, irr
itabi
lity,
and
cons
tant
cry
ing.
PB-Child & Adolescent Dosing.indd 61 05-02-2018 16:02:28
NOT FOR R
EPRINT
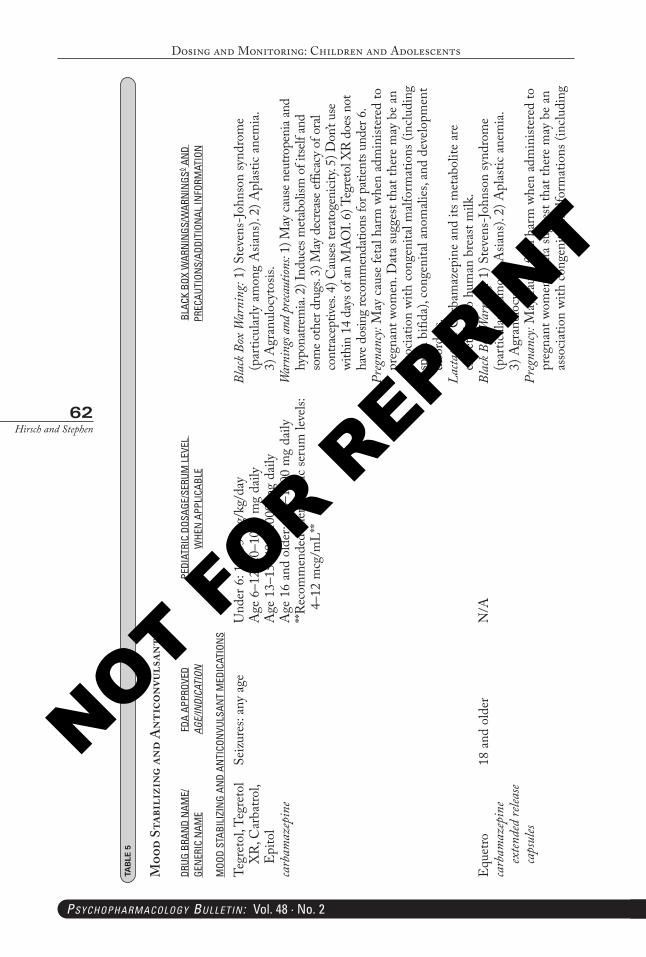
Dosing and Monitoring: Children and Adolescents
62Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
TAB
LE 5
Moo
d St
abil
izin
g an
d A
ntic
onvu
lsan
ts
DRUG
BRA
ND
NAM
E/GE
NER
IC N
AME
FDA
APPR
OVED
AGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS◊ A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
MOO
D ST
ABIL
IZIN
G AN
D AN
TICO
NVU
LSAN
T M
EDIC
ATIO
NS
Tegr
etol
, Teg
reto
l X
R, C
arba
trol,
Epi
tol
carb
amaz
epin
e
Seiz
ures
: any
age
Und
er 6
: 10–
35 m
g/kg
/day
Age
6–1
2: 2
0–10
00 m
g da
ilyA
ge 1
3–15
: 400
–100
0 m
g da
ilyA
ge 1
6 an
d ol
der:
400–
1200
mg
daily
**Rec
omm
ende
d th
erap
eutic
seru
m le
vels:
4–
12 m
cg/m
L**
Blac
k Box
War
ning
: 1) S
teve
ns-J
ohns
on sy
ndro
me
(par
ticul
arly
am
ong
Asia
ns).
2) A
plas
tic a
nem
ia.
3) A
gran
uloc
ytos
is.W
arni
ngs a
nd pr
ecaut
ions:
1) M
ay ca
use n
eutro
peni
a and
hy
pona
trem
ia. 2
) Ind
uces
met
abol
ism o
f itse
lf an
d so
me o
ther
dru
gs. 3
) May
dec
reas
e effi
cacy
of o
ral
cont
race
ptive
s. 4)
Cau
ses t
erat
ogen
icity.
5) D
on’t u
se
with
in 1
4 da
ys o
f an
MAO
I. 6)
Teg
reto
l XR
does
not
ha
ve d
osin
g re
com
men
datio
ns fo
r pat
ients
unde
r 6.
Preg
nanc
y: M
ay c
ause
feta
l har
m w
hen
adm
inist
ered
to
preg
nant
wom
en. D
ata
sugg
est t
hat t
here
may
be
an
asso
ciatio
n wi
th c
onge
nita
l malf
orm
atio
ns (i
nclu
ding
sp
ina
bifid
a), c
onge
nita
l ano
mali
es, a
nd d
evelo
pmen
t di
sord
ers.
Lacta
tion:
Car
bam
azep
ine
and
its m
etab
olite
are
ex
cret
ed in
to h
uman
bre
ast m
ilk.
Equ
etro
ca
rbam
azep
ine
exten
ded
relea
se ca
psul
es
18 a
nd o
lder
N/A
Blac
k Box
War
ning
: 1) S
teve
ns-J
ohns
on sy
ndro
me
(par
ticul
arly
am
ong
Asia
ns).
2) A
plas
tic a
nem
ia.
3) A
gran
uloc
ytos
is.Pr
egna
ncy:
May
cau
se fe
tal h
arm
whe
n ad
min
ister
ed to
pr
egna
nt w
omen
. Dat
a su
gges
t tha
t the
re m
ay b
e an
as
socia
tion
with
con
geni
tal m
alfor
mat
ions
(inc
ludi
ng
PB-Child & Adolescent Dosing.indd 62 05-02-2018 16:02:28
NOT FOR R
EPRINT
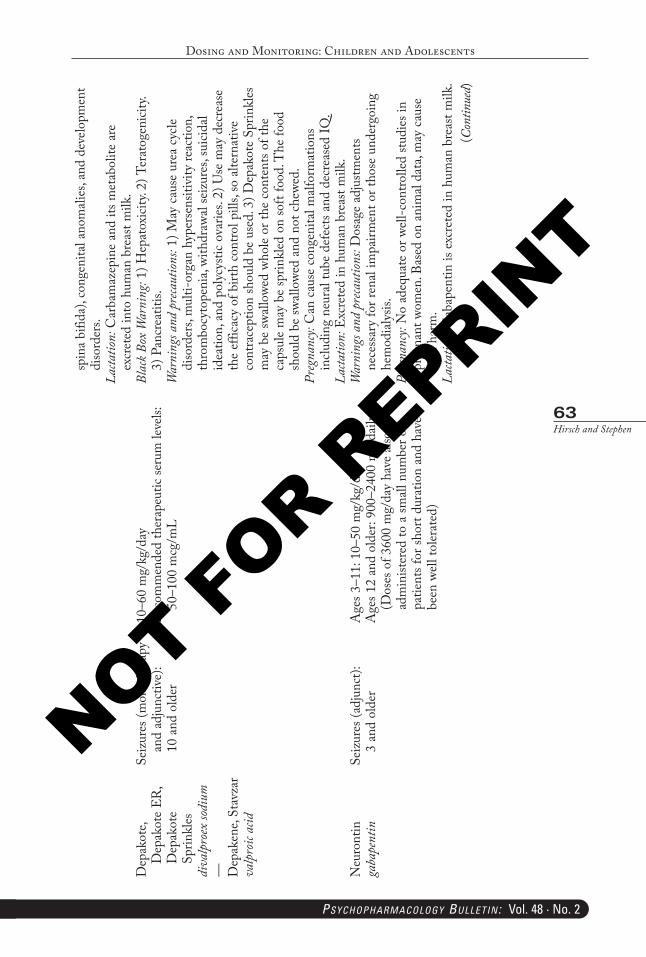
Dosing and Monitoring: Children and Adolescents
63Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
spin
a bi
fida)
, con
geni
tal a
nom
alies
, and
dev
elopm
ent
diso
rder
s.La
ctatio
n: C
arba
maz
epin
e an
d its
met
abol
ite a
re
excr
eted
into
hum
an b
reas
t milk
.D
epak
ote,
Dep
akot
e ER
, D
epak
ote
Sprin
kles
diva
lpro
ex so
dium
— Dep
aken
e, St
avza
r va
lpro
ic ac
id
Seiz
ures
(mon
othe
rapy
an
d ad
junc
tive)
: 10
and
old
er
10–6
0 m
g/kg
/day
Rec
omm
ende
d th
erap
eutic
seru
m le
vels:
50
–100
mcg
/mL
Blac
k Box
War
ning
: 1) H
epat
oxici
ty. 2
) Ter
atog
enici
ty.
3) P
ancr
eatit
is.W
arni
ngs a
nd p
reca
ution
s: 1)
May
cau
se u
rea
cycle
di
sord
ers,
mul
ti-or
gan
hype
rsen
sitiv
ity re
actio
n,
thro
mbo
cyto
peni
a, wi
thdr
awal
seiz
ures
, sui
cidal
idea
tion,
and
pol
ycys
tic o
varie
s. 2)
Use
may
dec
reas
e th
e ef
ficac
y of
birt
h co
ntro
l pill
s, so
alte
rnat
ive
cont
race
ptio
n sh
ould
be
used
. 3) D
epak
ote
Sprin
kles
m
ay b
e sw
allow
ed w
hole
or th
e co
nten
ts of
the
caps
ule
may
be
sprin
kled
on
soft
food
. The
food
sh
ould
be
swall
owed
and
not
che
wed.
Preg
nanc
y: C
an c
ause
con
geni
tal m
alfor
mat
ions
in
cludi
ng n
eura
l tub
e de
fect
s and
dec
reas
ed IQ
.La
ctatio
n: E
xcre
ted
in h
uman
bre
ast m
ilk.
Neu
ront
inga
bape
ntin
Seiz
ures
(adj
unct
): 3
and
olde
rA
ges 3
–11:
10–
50 m
g/kg
/day
Age
s 12
and
olde
r: 90
0–24
00 m
g da
ily
(Dos
es o
f 360
0 m
g/da
y ha
ve a
lso b
een
adm
inist
ered
to a
small
num
ber o
f pa
tient
s for
shor
t dur
atio
n an
d ha
ve
been
well
toler
ated
)
War
ning
s and
pre
caut
ions:
Dos
age
adju
stmen
ts ne
cess
ary
for r
enal
impa
irmen
t or t
hose
und
ergo
ing
hem
odia
lysis
.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pr
egna
nt w
omen
. Bas
ed o
n an
imal
data
, may
cau
se
feta
l har
m.
Lacta
tion:
Gab
apen
tin is
exc
rete
d in
hum
an b
reas
t milk
.(C
ontin
ued)
PB-Child & Adolescent Dosing.indd 63 05-02-2018 16:02:28
NOT FOR R
EPRINT
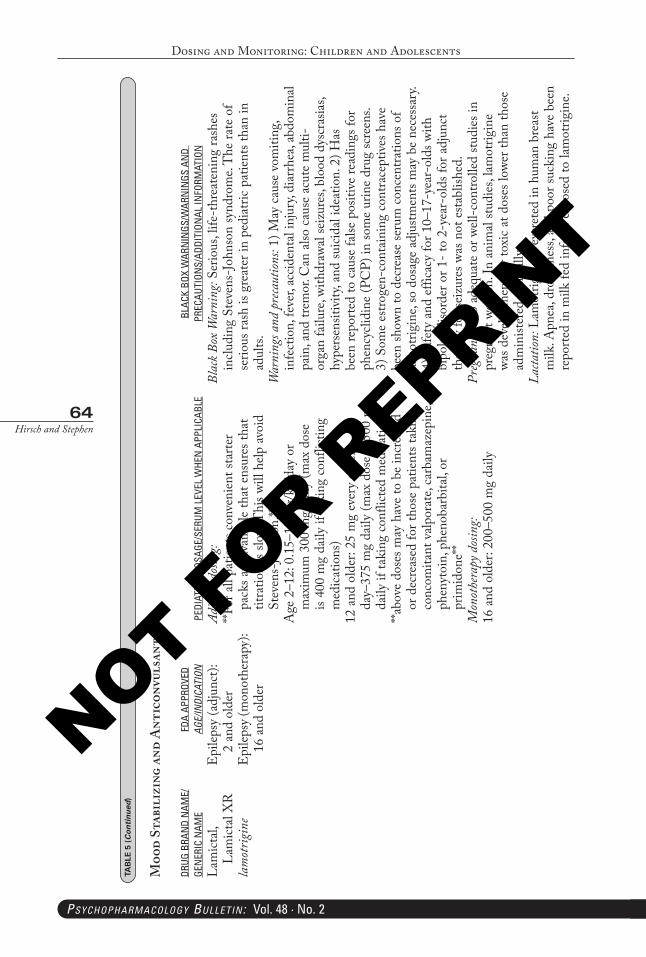
Dosing and Monitoring: Children and Adolescents
64Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Lam
ictal,
La
mict
al X
R
lam
otrig
ine
Epi
lepsy
(adj
unct
): 2
and
olde
rE
pilep
sy (m
onot
hera
py):
16 a
nd o
lder
Adju
nct d
osin
g:**F
or a
ll pa
tient
s con
veni
ent s
tarte
r pa
cks a
re a
vaila
ble
that
ens
ures
that
tit
ratio
n is
slow.
Thi
s will
help
avo
id
Stev
ens-
John
son.
**A
ge 2
–12:
0.1
5–15
mg/
kg/d
ay o
r m
axim
um 3
00 m
g da
ily (m
ax d
ose
is 40
0 m
g da
ily if
taki
ng c
onfli
ctin
g m
edica
tions
)12
and
old
er: 2
5 m
g ev
ery
othe
r da
y–37
5 m
g da
ily (m
ax d
ose
is 50
0 m
g da
ily if
taki
ng c
onfli
cted
med
icatio
ns)
**abo
ve d
oses
may
hav
e to
be
incr
ease
d or
dec
reas
ed fo
r tho
se p
atie
nts t
akin
g co
ncom
itant
valp
orat
e, ca
rbam
azep
ine,
phen
ytoi
n, p
heno
barb
ital,
or
prim
idon
e**
Mon
othe
rapy
dos
ing:
16 a
nd o
lder
: 200
–500
mg
daily
Blac
k Box
War
ning
: Ser
ious
, life
-thr
eate
ning
rash
es
inclu
ding
Ste
vens
-Joh
nson
synd
rom
e. T
he ra
te o
f se
rious
rash
is g
reat
er in
ped
iatri
c pa
tient
s tha
n in
ad
ults.
War
ning
s and
pre
caut
ions:
1) M
ay c
ause
vom
iting
, in
fect
ion,
feve
r, ac
ciden
tal i
njur
y, di
arrh
ea, a
bdom
inal
pain
, and
trem
or. C
an a
lso c
ause
acu
te m
ulti-
orga
n fa
ilure
, with
draw
al se
izur
es, b
lood
dys
cras
ias,
hype
rsen
sitiv
ity, a
nd su
icida
l ide
atio
n. 2
) Has
be
en re
porte
d to
cau
se fa
lse p
ositi
ve re
adin
gs fo
r ph
ency
clidi
ne (P
CP)
in so
me
urin
e dr
ug sc
reen
s. 3)
Som
e es
troge
n-co
ntai
ning
con
trace
ptiv
es h
ave
been
show
n to
dec
reas
e se
rum
con
cent
ratio
ns o
f lam
otrig
ine,
so d
osag
e ad
justm
ents
may
be
nece
ssar
y. 4)
Saf
ety
and
effic
acy
for 1
0–17
-yea
r-ol
ds w
ith
bipo
lar d
isord
er o
r 1- t
o 2-
year
-old
s for
adj
unct
th
erap
y fo
r sei
zure
s was
not
esta
blish
ed.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in
preg
nant
wom
en. I
n an
imal
studi
es, l
amot
rigin
e wa
s dev
elopm
enta
lly to
xic
at d
oses
lowe
r tha
n th
ose
adm
inist
ered
clin
ically
.La
ctatio
n: L
amot
rigin
e is
excr
eted
in h
uman
bre
ast
milk
. Apn
ea, d
rows
ines
s, an
d po
or su
ckin
g ha
ve b
een
repo
rted
in m
ilk fe
d in
fant
s exp
osed
to la
mot
rigin
e.
TAB
LE 5
(Continued
)
Moo
d St
abil
izin
g an
d A
ntic
onvu
lsan
ts
DRUG
BRA
ND
NAM
E/GE
NER
IC N
AME
FDA
APPR
OVED
AGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
WHE
N A
PPLI
CABL
EBL
ACK
BOX
WAR
NIN
GS/W
ARN
INGS
AN
D
PREC
AUTI
ONS/
ADDI
TION
AL IN
FORM
ATIO
N
PB-Child & Adolescent Dosing.indd 64 05-02-2018 16:02:28
NOT FOR R
EPRINT
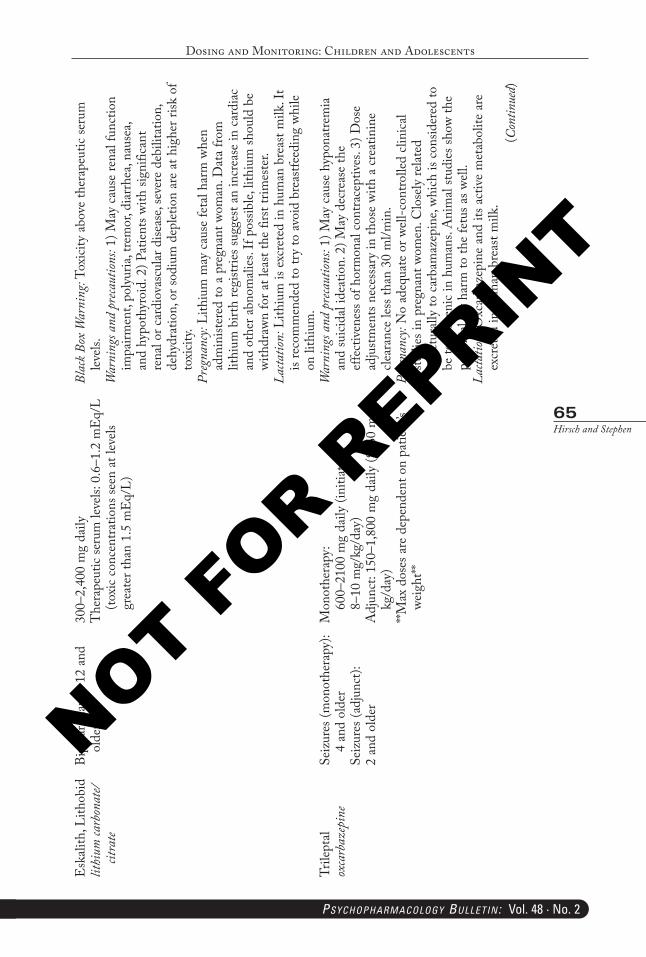
Dosing and Monitoring: Children and Adolescents
65Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
(Con
tinue
d)
Esk
alith
, Lith
obid
lithi
um ca
rbon
ate/
citra
te
Bipo
lar m
ania
: 12
and
olde
r30
0–2,
400
mg
daily
The
rape
utic
seru
m le
vels:
0.6
–1.2
mE
q/L
(toxi
c co
ncen
tratio
ns se
en a
t lev
els
grea
ter t
han
1.5
mE
q/L)
Blac
k Box
War
ning
: Tox
icity
abo
ve th
erap
eutic
seru
m
leve
ls.W
arni
ngs a
nd p
reca
ution
s: 1)
May
cau
se re
nal f
unct
ion
impa
irmen
t, po
lyur
ia, t
rem
or, d
iarrh
ea, n
ause
a, an
d hy
poth
yroi
d. 2
) Pat
ient
s with
sign
ifica
nt
rena
l or c
ardi
ovas
cular
dise
ase,
seve
re d
ebili
tatio
n,
dehy
drat
ion,
or s
odiu
m d
eplet
ion
are
at h
ighe
r risk
of
toxi
city.
Preg
nanc
y: Li
thiu
m m
ay c
ause
feta
l har
m w
hen
adm
inist
ered
to a
pre
gnan
t wom
an. D
ata
from
lit
hium
birt
h re
gistr
ies s
ugge
st an
incr
ease
in c
ardi
ac
and
othe
r abn
omali
es. I
f pos
sible,
lith
ium
shou
ld b
e wi
thdr
awn
for a
t lea
st th
e fir
st tri
mes
ter.
Lacta
tion:
Lith
ium
is e
xcre
ted
in h
uman
bre
ast m
ilk. I
t is
reco
mm
ende
d to
try
to a
void
bre
astfe
edin
g wh
ile
on li
thiu
m.
Trile
ptal
oxca
rbaz
epin
eSe
izur
es (m
onot
hera
py):
4 an
d ol
der
Seiz
ures
(adj
unct
):2
and
olde
r
Mon
othe
rapy
: 60
0–21
00 m
g da
ily (i
nitia
te a
t 8–
10 m
g/kg
/day
)A
djun
ct: 1
50–1
,800
mg
daily
(8–6
0 m
g/kg
/day
)**M
ax d
oses
are
dep
ende
nt o
n pa
tient
’s we
ight
**
War
ning
s and
pre
caut
ions:
1) M
ay c
ause
hyp
onat
rem
ia
and
suici
dal i
deat
ion.
2) M
ay d
ecre
ase
the
effe
ctiv
enes
s of h
orm
onal
cont
race
ptiv
es. 3
) Dos
e ad
justm
ents
nece
ssar
y in
thos
e wi
th a
cre
atin
ine
clear
ance
less
than
30
ml/m
in.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d cli
nica
l stu
dies
in p
regn
ant w
omen
. Clo
sely
relat
ed
struc
tura
lly to
car
bam
azep
ine,
which
is c
onsid
ered
to
be te
rato
geni
c in
hum
ans.
Ani
mal
studi
es sh
ow th
e po
tent
ial f
or h
arm
to th
e fe
tus a
s well
.La
ctatio
n: O
xcar
baze
pine
and
its a
ctiv
e m
etab
olite
are
ex
cret
ed in
hum
an b
reas
t milk
.
PB-Child & Adolescent Dosing.indd 65 05-02-2018 16:02:28
NOT FOR R
EPRINT
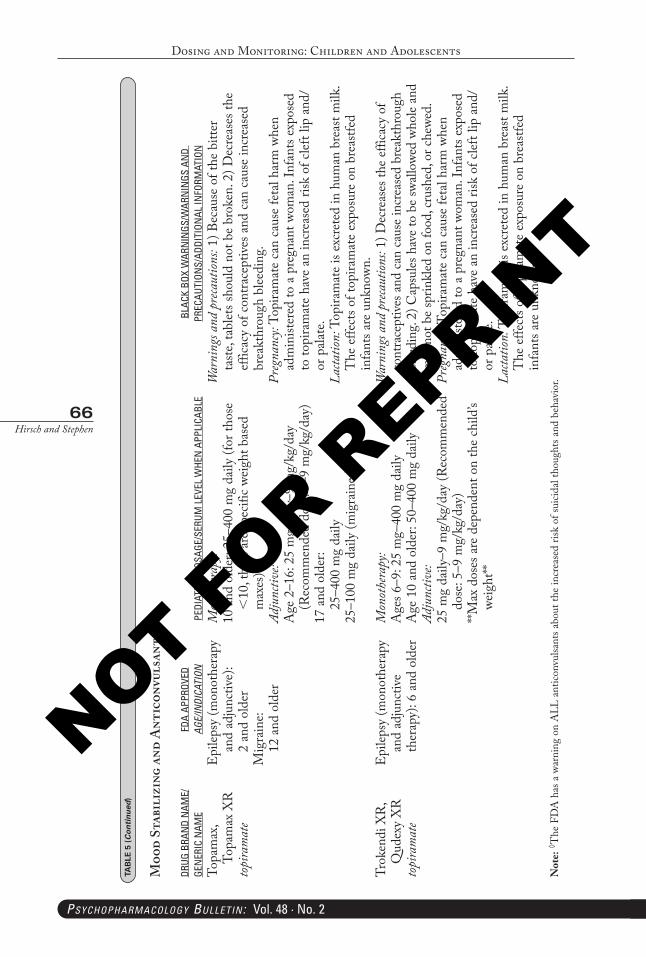
Dosing and Monitoring: Children and Adolescents
66Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Topa
max
, To
pam
ax X
R
topi
ram
ate
Epi
lepsy
(mon
othe
rapy
an
d ad
junc
tive)
: 2
and
olde
rM
igra
ine:
12
and
old
er
Mon
othe
rapy
:10
and
old
er: 2
5–40
0 m
g da
ily (f
or th
ose
<10
, the
re a
re sp
ecifi
c we
ight
bas
ed
max
es)
Adju
nctiv
e:A
ge 2
–16:
25
mg
daily
–9 m
g/kg
/day
(R
ecom
men
ded
dose
: 5–9
mg/
kg/d
ay)
17 a
nd o
lder
: 25
–400
mg
daily
25–1
00 m
g da
ily (m
igra
ines
)
War
ning
s and
pre
caut
ions:
1) B
ecau
se o
f the
bitt
er
taste
, tab
lets s
houl
d no
t be
brok
en. 2
) Dec
reas
es th
e ef
ficac
y of
con
trace
ptiv
es a
nd c
an c
ause
incr
ease
d br
eakt
hrou
gh b
leedi
ng.
Preg
nanc
y: To
pira
mat
e ca
n ca
use
feta
l har
m w
hen
adm
inist
ered
to a
pre
gnan
t wom
an. I
nfan
ts ex
pose
d to
topi
ram
ate
have
an
incr
ease
d ris
k of
clef
t lip
and
/or
pala
te.
Lacta
tion:
Top
iram
ate
is ex
cret
ed in
hum
an b
reas
t milk
. T
he e
ffect
s of t
opira
mat
e ex
posu
re o
n br
eastf
ed
infa
nts a
re u
nkno
wn.
Trok
endi
XR
, Q
udex
y X
Rto
pira
mat
e
Epi
lepsy
(mon
othe
rapy
an
d ad
junc
tive
ther
apy)
: 6 a
nd o
lder
Mon
othe
rapy
:A
ges 6
–9: 2
5 m
g–40
0 m
g da
ilyA
ge 1
0 an
d ol
der:
50–4
00 m
g da
ilyAd
junc
tive:
25 m
g da
ily–9
mg/
kg/d
ay (R
ecom
men
ded
dose
: 5–9
mg/
kg/d
ay)
**Max
dos
es a
re d
epen
dent
on
the
child
’s we
ight
**
War
ning
s and
pre
caut
ions:
1) D
ecre
ases
the
effic
acy
of
cont
race
ptive
s and
can
cau
se in
crea
sed
brea
kthr
ough
bl
eedi
ng. 2
) Cap
sules
hav
e to
be
swall
owed
who
le an
d m
ay n
ot b
e sp
rinkl
ed o
n fo
od, c
rush
ed, o
r che
wed.
Preg
nanc
y: To
pira
mat
e ca
n ca
use
feta
l har
m w
hen
adm
inist
ered
to a
pre
gnan
t wom
an. I
nfan
ts ex
pose
d to
topi
ram
ate
have
an
incr
ease
d ris
k of
clef
t lip
and
/or
pala
te.
Lacta
tion:
Top
iram
ate
is ex
cret
ed in
hum
an b
reas
t milk
. T
he e
ffect
s of t
opira
mat
e ex
posu
re o
n br
eastf
ed
infa
nts a
re u
nkno
wn.
Not
e: ◊ T
he F
DA
has
a w
arni
ng o
n A
LL a
ntico
nvul
sant
s abo
ut th
e in
crea
sed
risk
of su
icida
l tho
ught
s and
beh
avio
r.
TAB
LE 5
(Continued
)
Moo
d St
abil
izin
g an
d A
ntic
onvu
lsan
ts
DRUG
BRA
ND
NAM
E/GE
NER
IC N
AME
FDA
APPR
OVED
AGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
WHE
N A
PPLI
CABL
EBL
ACK
BOX
WAR
NIN
GS/W
ARN
INGS
AN
D
PREC
AUTI
ONS/
ADDI
TION
AL IN
FORM
ATIO
N
PB-Child & Adolescent Dosing.indd 66 05-02-2018 16:02:28
NOT FOR R
EPRINT
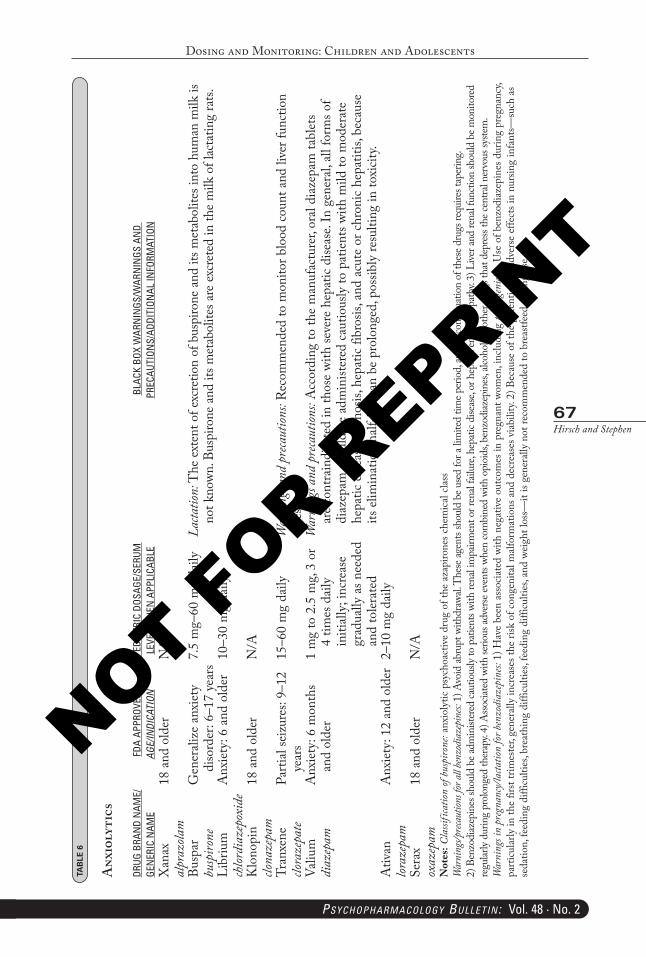
Dosing and Monitoring: Children and Adolescents
67Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
TAB
LE 6
Anx
ioly
tics
DRUG
BRA
ND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM
LEVE
L W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
Xan
ax
alpr
azola
m18
and
old
erN
/A
Busp
ar
busp
irone
Gen
erali
ze a
nxie
ty
diso
rder
: 6–1
7 ye
ars
7.5
mg–
60 m
g da
ilyLa
ctatio
n: T
he ex
tent
of e
xcre
tion
of b
uspi
rone
and
its m
etab
olite
s int
o hu
man
milk
is
not k
nown
. Bus
piro
ne a
nd it
s met
abol
ites a
re e
xcre
ted
in th
e m
ilk o
f lac
tatin
g ra
ts.Li
briu
m
chlor
diaz
epox
ide
Anx
iety
: 6 a
nd o
lder
10–3
0 m
g da
ily
Klo
nopi
n clo
naze
pam
18 a
nd o
lder
N/A
Tran
xene
clo
raze
pate
Parti
al se
izur
es: 9
–12
year
s15
–60
mg
daily
War
ning
s and
pre
caut
ions:
Rec
omm
ende
d to
mon
itor b
lood
coun
t and
live
r fun
ctio
n te
sts.
Valiu
m
diaz
epam
Anx
iety
: 6 m
onth
s an
d ol
der
1 m
g to
2.5
mg,
3 or
4
times
dai
ly
initi
ally;
incr
ease
gr
adua
lly a
s nee
ded
and
toler
ated
War
ning
s and
pre
caut
ions:
Acc
ordi
ng to
the
man
ufac
ture
r, or
al di
azep
am ta
blet
s ar
e co
ntra
indi
cate
d in
thos
e wi
th se
vere
hep
atic
dise
ase.
In g
ener
al, a
ll fo
rms o
f di
azep
am sh
ould
be
adm
inist
ered
cau
tious
ly to
pat
ient
s with
mild
to m
oder
ate
hepa
tic d
iseas
e, cir
rhos
is, h
epat
ic fib
rosis
, and
acu
te o
r chr
onic
hepa
titis,
bec
ause
its
elim
inat
ion
half-
life
can
be p
rolo
nged
, pos
sibly
resu
lting
in to
xicit
y.A
tivan
lor
azep
amA
nxie
ty: 1
2 an
d ol
der
2–10
mg
daily
Sera
x ox
azep
am18
and
old
erN
/A
Not
es: C
lassi
ficat
ion of
bus
piro
ne: a
nxio
lytic
psy
choa
ctiv
e dr
ug o
f the
aza
piro
nes c
hem
ical c
lass
War
ning
s/prec
autio
ns fo
r all b
enzo
diaz
epin
es: 1
) Avo
id ab
rupt
with
draw
al. T
hese
agen
ts sh
ould
be u
sed
for a
lim
ited
time p
erio
d, an
d di
scon
tinua
tion
of th
ese d
rugs
requ
ires t
aper
ing.
2)
Ben
zodi
azep
ines
shou
ld b
e adm
inist
ered
caut
ious
ly to
pat
ients
with
rena
l im
pairm
ent o
r ren
al fai
lure
, hep
atic
dise
ase,
or h
epat
ic en
ceph
alopa
thy.
3) L
iver a
nd re
nal f
uncti
on sh
ould
be m
onito
red
regu
larly
durin
g pr
olon
ged
ther
apy.
4) A
ssocia
ted
with
serio
us ad
verse
even
ts wh
en co
mbi
ned
with
opi
oids
, ben
zodi
azep
ines
, alco
hol, o
r oth
er d
rugs
that
dep
ress
the c
entra
l ner
vous
syste
m.
War
ning
s in
preg
nanc
y/la
ctatio
n for
benz
odia
zepi
nes:
1) H
ave
been
ass
ociat
ed w
ith n
egat
ive o
utco
mes
in p
regn
ant w
omen
, inc
ludi
ng te
rato
geni
city.
Use
of b
enzo
diaz
epin
es d
urin
g pr
egna
ncy,
parti
cular
ly in
the
first
trim
este
r, ge
nera
lly in
crea
ses t
he ri
sk o
f con
geni
tal m
alfor
mat
ions
and
dec
reas
es v
iabili
ty. 2
) Bec
ause
of t
he p
oten
tial f
or a
dver
se e
ffect
s in
nurs
ing
infa
nts—
such
as
seda
tion,
feed
ing
diffi
culti
es, b
reat
hing
diff
iculti
es, f
eedi
ng d
ifficu
lties
, and
weig
ht lo
ss—
it is
gene
rally
not
reco
mm
ende
d to
bre
astfe
ed d
urin
g us
e.
PB-Child & Adolescent Dosing.indd 67 05-02-2018 16:02:29
NOT FOR R
EPRINT
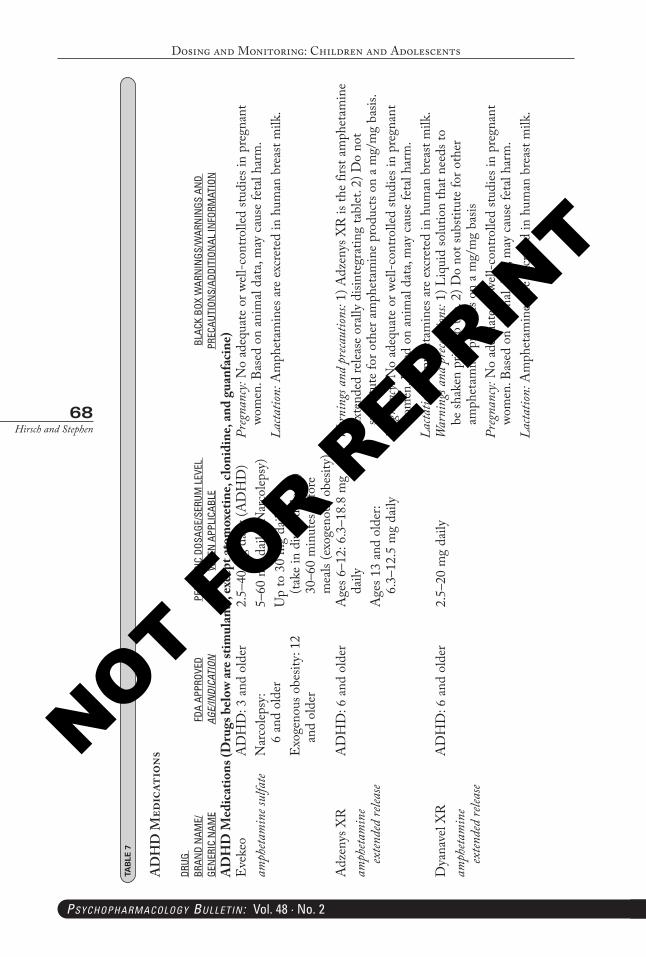
Dosing and Monitoring: Children and Adolescents
68Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
TAB
LE 7
AD
HD
Med
icat
ions
DRUG
BR
AND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
AD
HD
Med
icat
ions
(Dru
gs b
elow
are s
timul
ants
, exc
ept a
tom
oxet
ine,
clon
idin
e, an
d gu
anfa
cine
)E
veke
o am
pheta
min
e sul
fate
AD
HD
: 3 a
nd o
lder
Nar
colep
sy:
6 an
d ol
der
Exo
geno
us o
besit
y: 1
2 an
d ol
der
2.5–
40 m
g da
ily (A
DH
D)
5–60
mg
daily
(Nar
colep
sy)
Up
to 3
0 m
g da
ily
(take
in d
ivid
ed d
oses
) 30
–60
min
utes
bef
ore
mea
ls (e
xoge
nous
obe
sity)
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant
wom
en. B
ased
on
anim
al da
ta, m
ay c
ause
feta
l har
m.
Lacta
tion:
Am
phet
amin
es a
re e
xcre
ted
in h
uman
bre
ast m
ilk.
Adz
enys
XR
amph
etam
ine
exten
ded
relea
se
AD
HD
: 6 a
nd o
lder
Age
s 6–1
2: 6
.3–1
8.8
mg
daily
Age
s 13
and
olde
r: 6.
3–12
.5 m
g da
ily
War
ning
s and
pre
caut
ions:
1) A
dzen
ys X
R is
the
first
amph
etam
ine
exte
nded
relea
se o
rally
disi
nteg
ratin
g ta
blet
. 2) D
o no
t su
bstit
ute
for o
ther
am
phet
amin
e pr
oduc
ts on
a m
g/m
g ba
sis.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant
wom
en. B
ased
on
anim
al da
ta, m
ay c
ause
feta
l har
m.
Lacta
tion:
Am
phet
amin
es a
re e
xcre
ted
in h
uman
bre
ast m
ilk.
Dya
nave
l XR
am
pheta
min
e ex
tende
d re
lease
AD
HD
: 6 a
nd o
lder
2.5–
20 m
g da
ilyW
arni
ngs a
nd p
reca
ution
s: 1)
Liq
uid
solu
tion
that
nee
ds to
be
shak
en p
rior t
o us
e. 2)
Do
not s
ubsti
tute
for o
ther
am
phet
amin
e pr
oduc
ts on
a m
g/m
g ba
sisPr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pre
gnan
t wo
men
. Bas
ed o
n an
imal
data
, may
cau
se fe
tal h
arm
.La
ctatio
n: A
mph
etam
ines
are
exc
rete
d in
hum
an b
reas
t milk
.
PB-Child & Adolescent Dosing.indd 68 05-02-2018 16:02:29
NOT FOR R
EPRINT
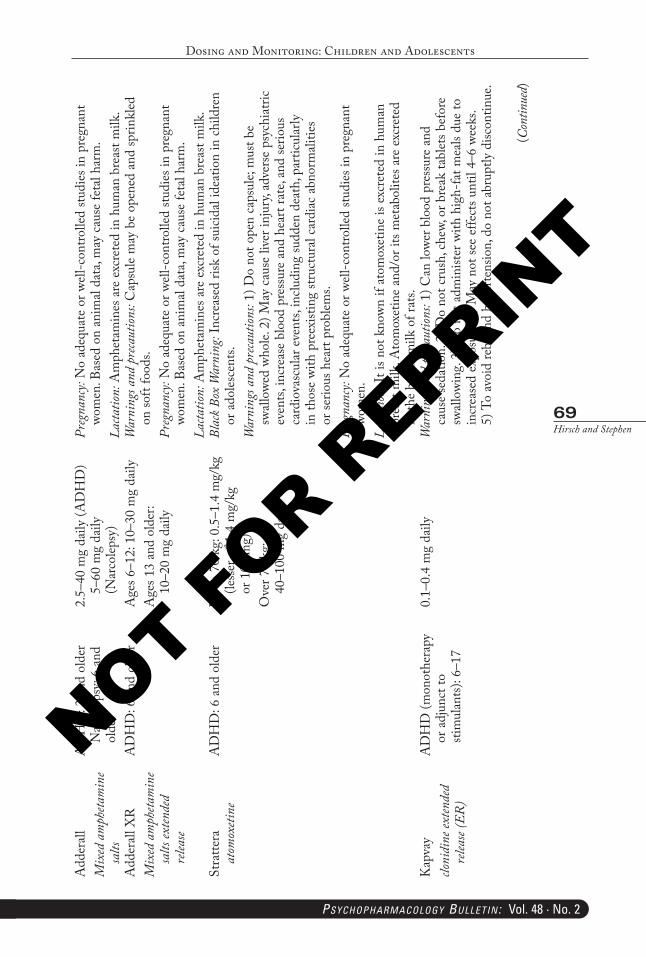
Dosing and Monitoring: Children and Adolescents
69Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
(Con
tinue
d)
Add
erall
M
ixed
am
pheta
min
e sa
lts
AD
HD
: 3 a
nd o
lder
N
arco
lepsy
: 6 a
nd
olde
r
2.5–
40 m
g da
ily (A
DH
D)
5–60
mg
daily
(N
arco
lepsy
)
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant
wom
en. B
ased
on
anim
al da
ta, m
ay c
ause
feta
l har
m.
Lacta
tion:
Am
phet
amin
es a
re e
xcre
ted
in h
uman
bre
ast m
ilk.
Add
erall
XR
M
ixed
am
pheta
min
e sa
lts ex
tende
d re
lease
AD
HD
: 6 a
nd o
lder
Age
s 6–1
2: 1
0–30
mg
daily
Age
s 13
and
olde
r:
10–2
0 m
g da
ily
War
ning
s and
pre
caut
ions:
Cap
sule
may
be
open
ed a
nd sp
rinkl
ed
on so
ft fo
ods.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant
wom
en. B
ased
on
anim
al da
ta, m
ay c
ause
feta
l har
m.
Lacta
tion:
Am
phet
amin
es a
re e
xcre
ted
in h
uman
bre
ast m
ilk.
Stra
ttera
at
omox
etine
AD
HD
: 6 a
nd o
lder
Up
to 7
0 kg
: 0.5
–1.4
mg/
kg
(less
er o
f 1.4
mg/
kg
or 1
00 m
g)O
ver 7
0 kg
: 40
–100
mg
daily
Blac
k Box
War
ning
: Inc
reas
ed ri
sk o
f sui
cidal
idea
tion
in c
hild
ren
or a
doles
cent
s.W
arni
ngs a
nd p
reca
ution
s: 1)
Do
not o
pen
caps
ule;
mus
t be
swall
owed
who
le. 2
) May
cau
se li
ver i
njur
y, ad
vers
e ps
ychi
atric
ev
ents,
incr
ease
blo
od p
ress
ure
and
hear
t rat
e, an
d se
rious
ca
rdio
vasc
ular
eve
nts,
inclu
ding
sudd
en d
eath
, par
ticul
arly
in
thos
e wi
th p
reex
istin
g str
uctu
ral c
ardi
ac a
bnor
mali
ties
or se
rious
hea
rt pr
oblem
s.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pre
gnan
t wo
men
.La
ctatio
n: It
is n
ot k
nown
if a
tom
oxet
ine
is ex
cret
ed in
hum
an
brea
st m
ilk. A
tom
oxet
ine
and/
or it
s met
abol
ites a
re e
xcre
ted
in th
e br
east
milk
of r
ats.
Kap
vay
cloni
dine
exten
ded
relea
se (E
R)
AD
HD
(mon
othe
rapy
or
adj
unct
to
stim
ulan
ts): 6
–17
0.1–
0.4
mg
daily
War
ning
s and
pre
caut
ions:
1) C
an lo
wer b
lood
pre
ssur
e an
d ca
use
seda
tion.
2) D
o no
t cru
sh, c
hew,
or b
reak
tabl
ets b
efor
e sw
allow
ing.
3) D
o no
t adm
inist
er w
ith h
igh-
fat m
eals
due
to
incr
ease
d ex
posu
re. 4
) May
not
see
effe
cts u
ntil
4–6
week
s. 5)
To
avoi
d re
boun
d hy
perte
nsio
n, d
o no
t abr
uptly
disc
ontin
ue.
PB-Child & Adolescent Dosing.indd 69 05-02-2018 16:02:29
NOT FOR R
EPRINT
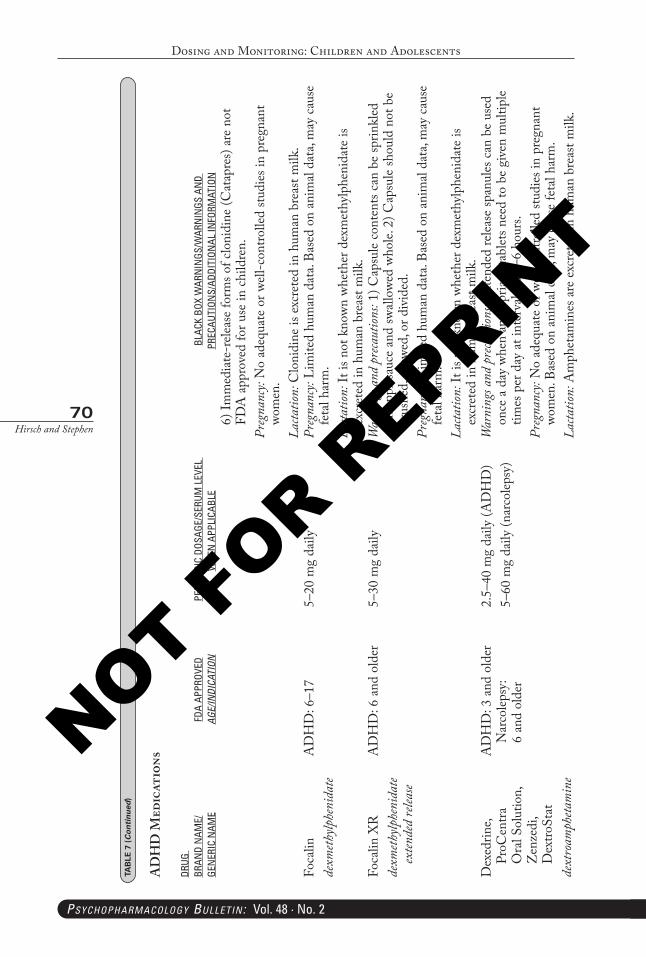
Dosing and Monitoring: Children and Adolescents
70Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
6) Im
med
iate
-rele
ase
form
s of c
loni
dine
(Cat
apre
s) ar
e no
t FD
A a
ppro
ved
for u
se in
chi
ldre
n.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pre
gnan
t wo
men
.La
ctatio
n: C
loni
dine
is e
xcre
ted
in h
uman
bre
ast m
ilk.
Foca
lin
dexm
ethylp
heni
date
AD
HD
: 6–1
75–
20 m
g da
ilyPr
egna
ncy:
Lim
ited
hum
an d
ata.
Base
d on
ani
mal
data
, may
cau
se
feta
l har
m.
Lacta
tion:
It is
not
kno
wn w
heth
er d
exm
ethy
lphe
nida
te is
ex
cret
ed in
hum
an b
reas
t milk
.Fo
calin
XR
de
xmeth
ylphe
nida
te ex
tende
d re
lease
AD
HD
: 6 a
nd o
lder
5–30
mg
daily
War
ning
s and
pre
caut
ions:
1) C
apsu
le co
nten
ts ca
n be
sprin
kled
on
app
lesau
ce a
nd sw
allow
ed w
hole.
2) C
apsu
le sh
ould
not
be
crus
hed,
che
wed,
or d
ivid
ed.
Preg
nanc
y: Li
mite
d hu
man
dat
a. Ba
sed
on a
nim
al da
ta, m
ay c
ause
fe
tal h
arm
.La
ctatio
n: It
is n
ot k
nown
whe
ther
dex
met
hylp
heni
date
is
excr
eted
in h
uman
bre
ast m
ilk.
Dex
edrin
e, Pr
oCen
tra
Ora
l Sol
utio
n,
Zen
zedi
, D
extro
Stat
de
xtro
amph
etam
ine
AD
HD
: 3 a
nd o
lder
N
arco
lepsy
: 6
and
olde
r
2.5–
40 m
g da
ily (A
DH
D)
5–60
mg
daily
(nar
colep
sy)
War
ning
s and
pre
caut
ions:
Ext
ende
d re
lease
span
ules
can
be
used
on
ce a
day
whe
n ap
prop
riate
, tab
lets n
eed
to b
e gi
ven
mul
tiple
times
per
day
at i
nter
vals
of 4
–6 h
ours
.Pr
egna
ncy:
No
adeq
uate
or w
ell c
ontro
lled
studi
es in
pre
gnan
t wo
men
. Bas
ed o
n an
imal
data
, may
cau
se fe
tal h
arm
.La
ctatio
n: A
mph
etam
ines
are
exc
rete
d in
hum
an b
reas
t milk
.
TAB
LE 7
(Continued
)
AD
HD
Med
icat
ions
DRUG
BR
AND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 70 05-02-2018 16:02:29
NOT FOR R
EPRINT
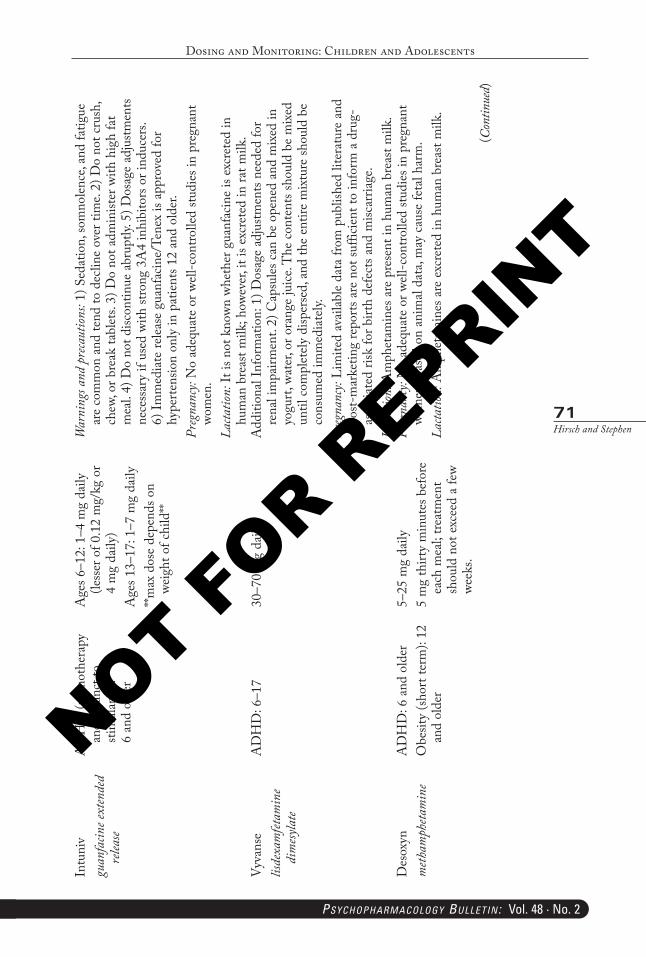
Dosing and Monitoring: Children and Adolescents
71Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Intu
niv
guan
facin
e ext
ende
d re
lease
AD
HD
(mon
othe
rapy
an
d ad
junc
t to
stim
ulan
ts):
6 an
d ol
der
Age
s 6–1
2: 1
–4 m
g da
ily
(less
er o
f 0.1
2 m
g/kg
or
4 m
g da
ily)
Age
s 13–
17: 1
–7 m
g da
ily**m
ax d
ose
depe
nds o
n we
ight
of c
hild
**
War
ning
s and
pre
caut
ions:
1) S
edat
ion,
som
nolen
ce, a
nd fa
tigue
ar
e co
mm
on a
nd te
nd to
dec
line
over
tim
e. 2)
Do
not c
rush
, ch
ew, o
r bre
ak ta
blet
s. 3)
Do
not a
dmin
ister
with
hig
h fa
t m
eal.
4) D
o no
t disc
ontin
ue a
brup
tly. 5
) Dos
age
adju
stmen
ts ne
cess
ary
if us
ed w
ith st
rong
3A
4 in
hibi
tors
or i
nduc
ers.
6) Im
med
iate
relea
se g
uanf
acin
e/Te
nex
is ap
prov
ed fo
r hy
perte
nsio
n on
ly in
pat
ient
s 12
and
olde
r.Pr
egna
ncy:
No
adeq
uate
or w
ell-c
ontro
lled
studi
es in
pre
gnan
t wo
men
.La
ctatio
n: It
is n
ot k
nown
whe
ther
gua
nfac
ine
is ex
cret
ed in
hu
man
bre
ast m
ilk; h
owev
er, i
t is e
xcre
ted
in ra
t milk
.Vy
vans
e lis
dexa
mfet
amin
e di
mesy
late
AD
HD
: 6–1
730
–70
mg
daily
Add
ition
al In
form
atio
n: 1
) Dos
age
adju
stmen
ts ne
eded
for
rena
l im
pairm
ent.
2) C
apsu
les c
an b
e op
ened
and
mix
ed in
yo
gurt,
wat
er, o
r ora
nge
juice
. The
con
tent
s sho
uld
be m
ixed
un
til c
ompl
etel
y di
sper
sed,
and
the
entir
e m
ixtu
re sh
ould
be
cons
umed
imm
edia
tely.
Preg
nanc
y: Li
mite
d av
ailab
le da
ta fr
om p
ublis
hed
liter
atur
e an
d po
st-m
arke
ting
repo
rts a
re n
ot su
fficie
nt to
info
rm a
dru
g-as
socia
ted
risk
for b
irth
defe
cts a
nd m
iscar
riage
.La
ctatio
n: A
mph
etam
ines
are
pre
sent
in h
uman
bre
ast m
ilk.
Des
oxyn
m
etham
pheta
min
eA
DH
D: 6
and
old
erO
besit
y (sh
ort t
erm
): 12
an
d ol
der
5–25
mg
daily
5 m
g th
irty
min
utes
bef
ore
each
mea
l; tre
atm
ent
shou
ld n
ot e
xcee
d a
few
week
s.
Preg
nanc
y: N
o ad
equa
te o
r well
-con
trolle
d stu
dies
in p
regn
ant
wom
en. B
ased
on
anim
al da
ta, m
ay c
ause
feta
l har
m.
Lacta
tion:
Am
phet
amin
es a
re e
xcre
ted
in h
uman
bre
ast m
ilk.
(Con
tinue
d)
PB-Child & Adolescent Dosing.indd 71 05-02-2018 16:02:29
NOT FOR R
EPRINT
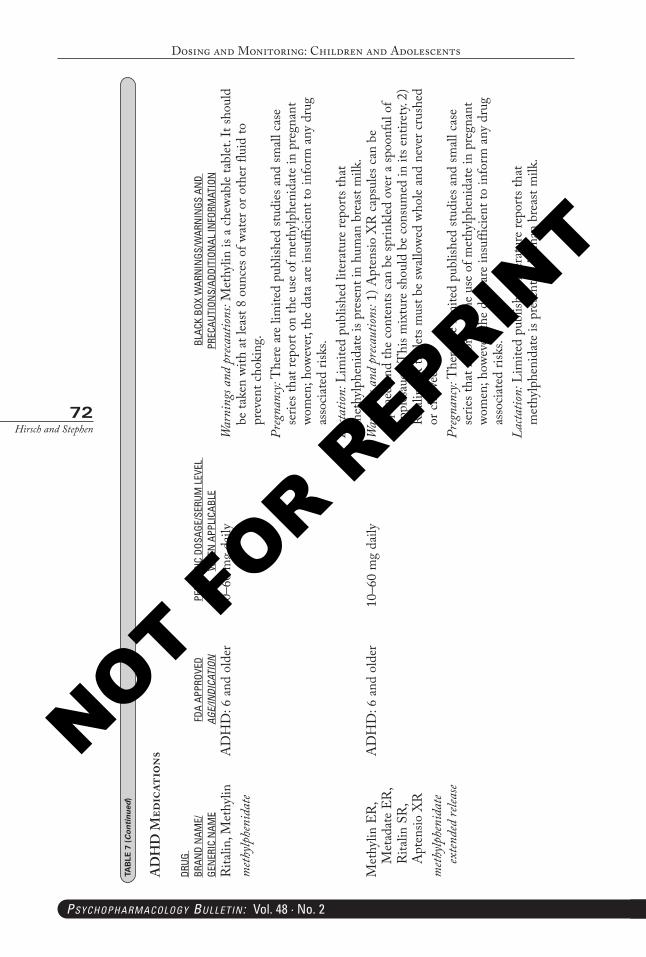
Dosing and Monitoring: Children and Adolescents
72Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Rita
lin, M
ethy
lin
meth
ylphe
nida
teA
DH
D: 6
and
old
er10
–60
mg
daily
War
ning
s and
pre
caut
ions:
Met
hylin
is a
che
wabl
e ta
blet
. It s
houl
d be
take
n wi
th a
t lea
st 8
ounc
es o
f wat
er o
r oth
er fl
uid
to
prev
ent c
hoki
ng.
Preg
nanc
y: T
here
are
lim
ited
publ
ished
stud
ies a
nd sm
all c
ase
serie
s tha
t rep
ort o
n th
e us
e of
met
hylp
heni
date
in p
regn
ant
wom
en; h
owev
er, t
he d
ata
are
insu
fficie
nt to
info
rm a
ny d
rug
asso
ciate
d ris
ks.
Lacta
tion:
Lim
ited
publ
ished
lite
ratu
re re
ports
that
m
ethy
lphe
nida
te is
pre
sent
in h
uman
bre
ast m
ilk.
Met
hylin
ER
, M
etad
ate
ER,
Rita
lin S
R,
Apt
ensio
XR
meth
ylphe
nida
te ex
tende
d re
lease
AD
HD
: 6 a
nd o
lder
10–6
0 m
g da
ilyW
arni
ngs a
nd p
reca
ution
s: 1)
Apt
ensio
XR
cap
sules
can
be
open
ed a
nd th
e co
nten
ts ca
n be
sprin
kled
ove
r a sp
oonf
ul o
f ap
ples
auce
. Thi
s mix
ture
shou
ld b
e co
nsum
ed in
its e
ntire
ty. 2
) R
italin
SR
tabl
ets m
ust b
e sw
allow
ed w
hole
and
neve
r cru
shed
or
che
wed.
Preg
nanc
y: T
here
are
lim
ited
publ
ished
stud
ies a
nd sm
all c
ase
serie
s tha
t rep
ort o
n th
e us
e of
met
hylp
heni
date
in p
regn
ant
wom
en; h
owev
er, t
he d
ata
are
insu
fficie
nt to
info
rm a
ny d
rug
asso
ciate
d ris
ks.
Lacta
tion:
Lim
ited
publ
ished
lite
ratu
re re
ports
that
m
ethy
lphe
nida
te is
pre
sent
in h
uman
bre
ast m
ilk.
TAB
LE 7
(Continued
)
AD
HD
Med
icat
ions
DRUG
BR
AND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 72 05-02-2018 16:02:29
NOT FOR R
EPRINT
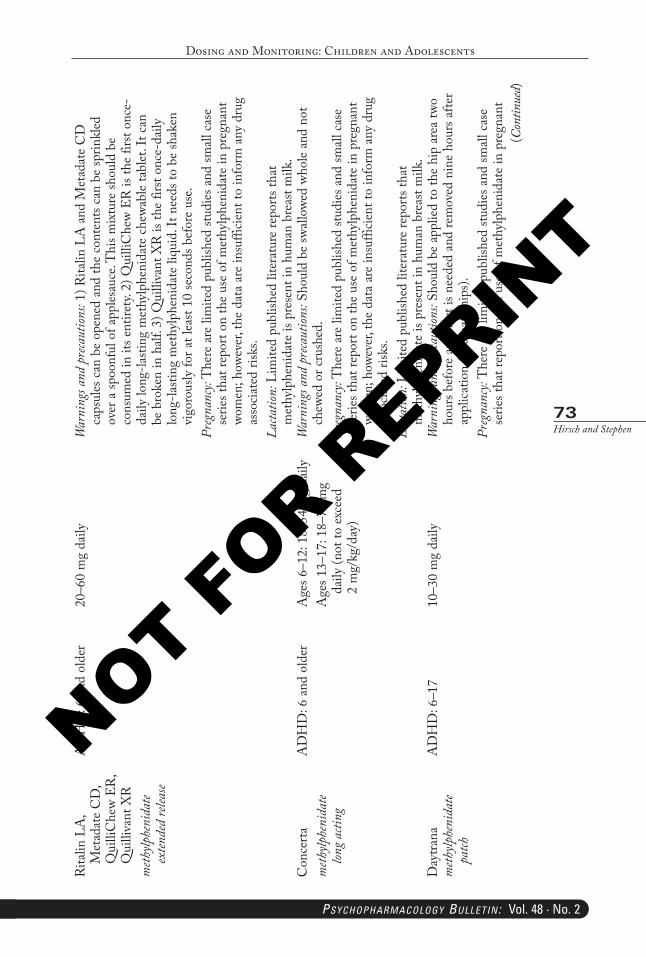
Dosing and Monitoring: Children and Adolescents
73Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Rita
lin L
A,
Met
adat
e C
D,
Qui
lliC
hew
ER,
Qui
lliva
nt X
Rm
ethylp
heni
date
exten
ded
relea
se
AD
HD
: 6 a
nd o
lder
20–6
0 m
g da
ilyW
arni
ngs a
nd p
reca
ution
s: 1)
Rita
lin L
A a
nd M
etad
ate
CD
ca
psul
es c
an b
e op
ened
and
the
cont
ents
can
be sp
rinkl
ed
over
a sp
oonf
ul o
f app
lesau
ce. T
his m
ixtu
re sh
ould
be
cons
umed
in it
s ent
irety.
2) Q
uilli
Che
w ER
is th
e fir
st on
ce-
daily
long
-lasti
ng m
ethy
lphe
nida
te c
hewa
ble
tabl
et. I
t can
be
bro
ken
in h
alf. 3
) Qui
lliva
nt X
R is
the
first
once
-dai
ly
long
-lasti
ng m
ethy
lphe
nida
te li
quid
. It n
eeds
to b
e sh
aken
vi
goro
usly
for a
t lea
st 10
seco
nds b
efor
e us
e.Pr
egna
ncy:
The
re a
re li
mite
d pu
blish
ed st
udie
s and
small
cas
e se
ries t
hat r
epor
t on
the
use
of m
ethy
lphe
nida
te in
pre
gnan
t wo
men
; how
ever
, the
dat
a ar
e in
suffi
cient
to in
form
any
dru
g as
socia
ted
risks
.La
ctatio
n: L
imite
d pu
blish
ed li
tera
ture
repo
rts th
at
met
hylp
heni
date
is p
rese
nt in
hum
an b
reas
t milk
.C
once
rta
meth
ylphe
nida
te lon
g acti
ng
AD
HD
: 6 a
nd o
lder
Age
s 6–1
2: 1
8–54
mg
daily
Age
s 13–
17: 1
8–72
mg
daily
(not
to e
xcee
d 2
mg/
kg/d
ay)
War
ning
s and
pre
caut
ions:
Shou
ld b
e sw
allow
ed w
hole
and
not
chew
ed o
r cru
shed
.Pr
egna
ncy:
The
re a
re li
mite
d pu
blish
ed st
udie
s and
small
cas
e se
ries t
hat r
epor
t on
the
use
of m
ethy
lphe
nida
te in
pre
gnan
t wo
men
; how
ever
, the
dat
a ar
e in
suffi
cient
to in
form
any
dru
g as
socia
ted
risks
.La
ctatio
n: L
imite
d pu
blish
ed li
tera
ture
repo
rts th
at
met
hylp
heni
date
is p
rese
nt in
hum
an b
reas
t milk
.D
aytra
nam
ethylp
heni
date
patch
AD
HD
: 6–1
710
–30
mg
daily
War
ning
s and
pre
caut
ions:
Shou
ld b
e ap
plie
d to
the
hip
area
two
hour
s bef
ore
an e
ffect
is n
eede
d an
d re
mov
ed n
ine
hour
s afte
r ap
plica
tion
(alte
rnat
e hi
ps).
Preg
nanc
y: T
here
are
lim
ited
publ
ished
stud
ies a
nd sm
all c
ase
serie
s tha
t rep
ort o
n th
e us
e of
met
hylp
heni
date
in p
regn
ant
(Con
tinue
d)
PB-Child & Adolescent Dosing.indd 73 05-02-2018 16:02:29
NOT FOR R
EPRINT
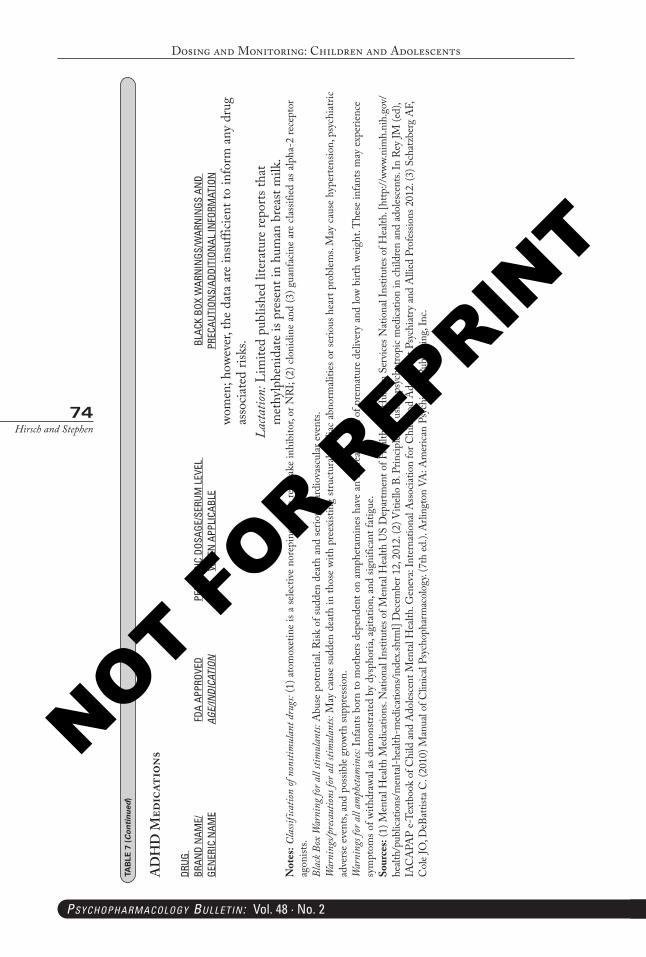
Dosing and Monitoring: Children and Adolescents
74Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
wom
en; h
owev
er, t
he d
ata
are
insu
fficie
nt to
info
rm a
ny d
rug
asso
ciate
d ris
ks.
Lacta
tion:
Lim
ited
publ
ished
lite
ratu
re re
ports
that
m
ethy
lphe
nida
te is
pre
sent
in h
uman
bre
ast m
ilk.
Not
es: C
lassi
ficat
ion of
non
stim
ulan
t dru
gs: (
1) a
tom
oxet
ine
is a
selec
tive
nore
pine
phrin
e re
upta
ke in
hibi
tor,
or N
RI; (
2) c
loni
dine
and
(3) g
uanf
acin
e ar
e cla
ssifi
ed a
s alp
ha-2
rece
ptor
ag
onist
s.Bl
ack B
ox W
arni
ng fo
r all
stim
ulan
ts: A
buse
pot
entia
l. R
isk o
f sud
den
deat
h an
d se
rious
car
diov
ascu
lar e
vent
s.W
arni
ngs/p
reca
ution
s for
all
stim
ulan
ts: M
ay c
ause
sudd
en d
eath
in th
ose
with
pre
exist
ing
struc
tura
l car
diac
abn
orm
alitie
s or s
erio
us h
eart
prob
lems.
May
cau
se h
yper
tens
ion,
psy
chia
tric
adve
rse
even
ts, a
nd p
ossib
le gr
owth
supp
ress
ion.
War
ning
s for
all
amph
etam
ines:
Infa
nts b
orn
to m
othe
rs d
epen
dent
on
amph
etam
ines
hav
e an
incr
ease
d ris
k of
pre
mat
ure
deliv
ery
and
low
birth
wei
ght.
The
se in
fant
s may
exp
erie
nce
sym
ptom
s of w
ithdr
awal
as d
emon
strat
ed b
y dy
spho
ria, a
gita
tion,
and
sign
ifica
nt fa
tigue
.So
urce
s: (1
) Men
tal H
ealth
Med
icatio
ns. N
atio
nal I
nstit
utes
of M
enta
l Hea
lth U
S D
epar
tmen
t of H
ealth
and
Hum
an S
ervic
es N
atio
nal I
nstit
utes
of H
ealth
. [ht
tp://
www.
nim
h.ni
h.go
v/he
alth/
publ
icatio
ns/m
enta
l-hea
lth-m
edica
tions
/inde
x.sht
ml]
Dec
embe
r 12,
2012
. (2)
Viti
ello
B. P
rincip
les in
usin
g ps
ycho
tropi
c med
icatio
n in
child
ren
and
adol
esce
nts.
In R
ey JM
(ed)
, IA
CA
PAP
e-Te
xtbo
ok o
f Chi
ld an
d A
doles
cent
Men
tal H
ealth
. Gen
eva:
Inte
rnat
iona
l Ass
ociat
ion
for C
hild
and
Ado
lesce
nt P
sych
iatry
and
Alli
ed P
rofe
ssio
ns 2
012.
(3) S
chat
zber
g A
F, C
ole J
O, D
eBat
tista
C. (
2010
) Man
ual o
f Clin
ical P
sych
opha
rmac
olog
y. (7
th ed
.). A
rling
ton
VA: A
mer
ican
Psyc
hiat
ric P
ublis
hing
, Inc
.
TAB
LE 7
(Continued
)
AD
HD
Med
icat
ions
DRUG
BR
AND
NAM
E/
GEN
ERIC
NAM
EFD
A AP
PROV
EDAGE/INDICATION
PEDI
ATRI
C DO
SAGE
/SER
UM L
EVEL
W
HEN
APP
LICA
BLE
BLAC
K BO
X W
ARN
INGS
/WAR
NIN
GS A
ND
PR
ECAU
TION
S/AD
DITI
ONAL
INFO
RMAT
ION
PB-Child & Adolescent Dosing.indd 74 05-02-2018 16:02:30
NOT FOR R
EPRINT
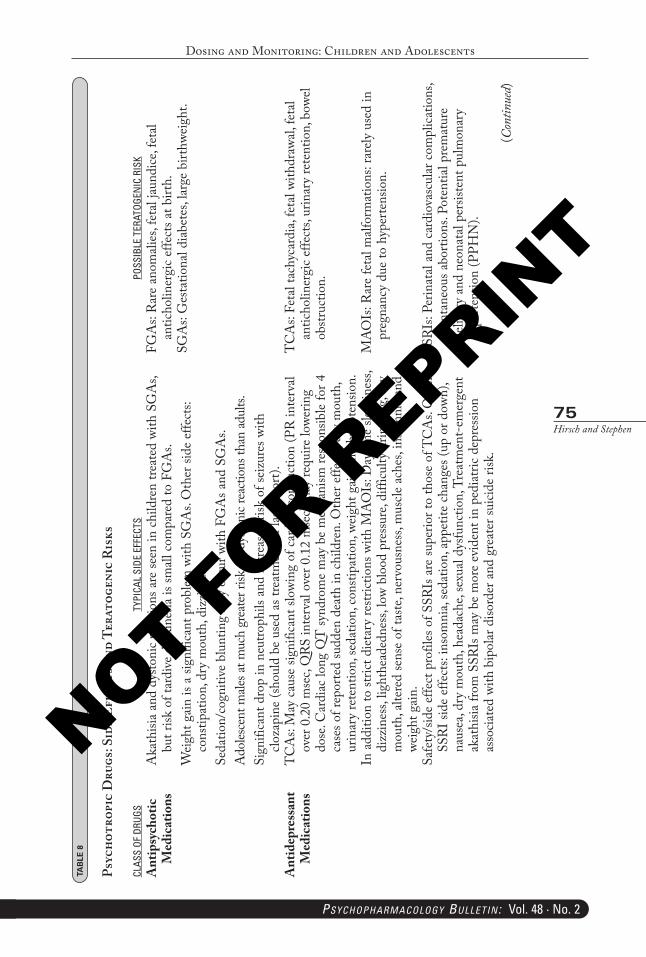
Dosing and Monitoring: Children and Adolescents
75Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
CLAS
S OF
DRU
GSTY
PICA
L SI
DE E
FFEC
TSPO
SSIB
LE T
ERAT
OGEN
IC R
ISK
Ant
ipsy
chot
ic
Med
icat
ions
Aka
thisi
a an
d dy
stoni
c re
actio
ns a
re se
en in
chi
ldre
n tre
ated
with
SG
As,
but r
isk o
f tar
dive
dys
kine
sia is
small
com
pare
d to
FG
As.
Wei
ght g
ain
is a
signi
fican
t pro
blem
with
SG
As.
Oth
er si
de e
ffect
s: co
nstip
atio
n, d
ry m
outh
, diz
zine
ss.
Seda
tion/
cogn
itive
blu
ntin
g m
ay o
ccur
with
FG
As a
nd S
GA
s.A
doles
cent
male
s at m
uch
grea
ter r
isk fo
r dys
toni
c rea
ctio
ns th
an ad
ults.
Sign
ifica
nt d
rop
in n
eutro
phils
and
incr
ease
d ris
k of
seiz
ures
with
clo
zapi
ne (s
houl
d be
use
d as
trea
tmen
t of l
ast r
esor
t).
FGA
s: R
are
anom
alies
, fet
al jau
ndice
, fet
al an
ticho
liner
gic
effe
cts a
t birt
h.SG
As:
Ges
tatio
nal d
iabe
tes,
large
birt
hwei
ght.
Ant
idep
ress
ant
Med
icat
ions
TC
As:
May
cau
se si
gnifi
cant
slow
ing
of c
ardi
ac c
ondu
ctio
n (P
R in
terv
al ov
er 0
.20
mse
c, Q
RS in
terv
al ov
er 0
.12
mse
c) m
ay re
quire
lowe
ring
dose
. Car
diac
long
QT
synd
rom
e m
ay b
e m
echa
nism
resp
onsib
le fo
r 4
case
s of r
epor
ted
sudd
en d
eath
in c
hild
ren.
Oth
er e
ffect
s: dr
y m
outh
, ur
inar
y re
tent
ion,
seda
tion,
con
stipa
tion,
wei
ght g
ain
and
hypo
tens
ion.
TC
As:
Feta
l tac
hyca
rdia
, fet
al wi
thdr
awal,
feta
l an
ticho
liner
gic
effe
cts,
urin
ary
rete
ntio
n, b
owel
obstr
uctio
n.
In a
dditi
on to
stric
t die
tary
restr
ictio
ns w
ith M
AO
Is: D
aytim
e sle
epin
ess,
dizz
ines
s, lig
hthe
aded
ness
, low
blo
od p
ress
ure,
diffi
culty
urin
atin
g, dr
y m
outh
, alte
red
sens
e of
taste
, ner
vous
ness
, mus
cle a
ches
, ins
omni
a an
d we
ight
gai
n.
MA
OIs
: Rar
e fe
tal m
alfor
mat
ions
: rar
ely
used
in
preg
nanc
y du
e to
hyp
erte
nsio
n.
Safe
ty/s
ide
effe
ct p
rofil
es o
f SSR
Is a
re su
perio
r to
thos
e of
TC
As.
Oth
er
SSRI
side
effe
cts:
inso
mni
a, se
datio
n, a
ppet
ite c
hang
es (u
p or
dow
n),
naus
ea, d
ry m
outh
, hea
dach
e, se
xual
dysfu
nctio
n, T
reat
men
t-em
erge
nt
akat
hisia
from
SSR
Is m
ay b
e m
ore
evid
ent i
n pe
diat
ric d
epre
ssio
n as
socia
ted
with
bip
olar
diso
rder
and
gre
ater
suici
de ri
sk.
SSRI
s: Pe
rinat
al an
d ca
rdio
vasc
ular
com
plica
tions
, sp
onta
neou
s abo
rtion
s. Po
tent
ial p
rem
atur
e de
liver
y an
d ne
onat
al pe
rsist
ent p
ulm
onar
y hy
perte
nsio
n (P
PHN
).
TAB
LE 8
Psyc
hotr
opic
Dru
gs: S
ide
Effe
cts a
nd T
erat
ogen
ic R
isks
(Con
tinue
d)
PB-Child & Adolescent Dosing.indd 75 05-02-2018 16:02:30
NOT FOR R
EPRINT
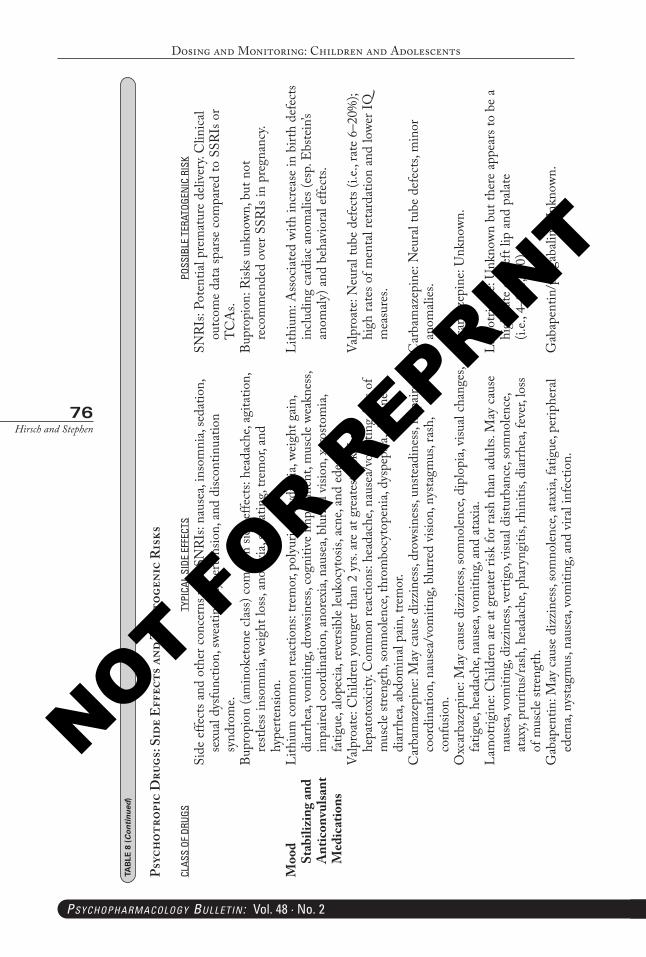
Dosing and Monitoring: Children and Adolescents
76Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
CLAS
S OF
DRU
GSTY
PICA
L SI
DE E
FFEC
TSPO
SSIB
LE T
ERAT
OGEN
IC R
ISK
Side
effe
cts a
nd o
ther
con
cern
s with
SN
RIs:
naus
ea, i
nsom
nia,
seda
tion,
se
xual
dysfu
nctio
n, sw
eatin
g, hy
perte
nsio
n, a
nd d
iscon
tinua
tion
synd
rom
e.
SNRI
s: Po
tent
ial p
rem
atur
e de
liver
y. C
linica
l ou
tcom
e da
ta sp
arse
com
pare
d to
SSR
Is o
r T
CA
s.Bu
prop
ion
(am
inok
eton
e cla
ss) c
omm
on si
de e
ffect
s: he
adac
he, a
gita
tion,
re
stles
s ins
omni
a, we
ight
loss
, ano
rexi
a, sw
eatin
g, tre
mor
, and
hy
perte
nsio
n.
Bupr
opio
n: R
isks u
nkno
wn, b
ut n
ot
reco
mm
ende
d ov
er S
SRIs
in p
regn
ancy
.
Moo
d St
abili
zing
and
Ant
icon
vulsa
nt
Med
icat
ions
Lith
ium
com
mon
reac
tions
: tre
mor
, pol
yuria
, pol
ydip
sia, w
eigh
t gai
n,
diar
rhea
, vom
iting
, dro
wsin
ess,
cogn
itive
impa
irmen
t, m
uscle
wea
knes
s, im
paire
d co
ordi
natio
n, a
nore
xia,
naus
ea, b
lurre
d vi
sion,
xer
osto
mia
, fa
tigue
, alo
pecia
, rev
ersib
le leu
kocy
tosis
, acn
e, an
d ed
ema.
Lith
ium
: Ass
ocia
ted
with
incr
ease
in b
irth
defe
cts
inclu
ding
car
diac
ano
mali
es (e
sp. E
bste
in’s
anom
aly)
and
beh
avio
ral e
ffect
s.
Valp
roat
e: C
hild
ren
youn
ger t
han
2 yr
s. ar
e at
gre
ates
t risk
for
hepa
toto
xicit
y. C
omm
on re
actio
ns: h
eada
che,
naus
ea/v
omiti
ng, l
oss o
f m
uscle
stre
ngth
, som
nolen
ce, t
hrom
bocy
tope
nia,
dysp
epsia
, diz
zine
ss,
diar
rhea
, abd
omin
al pa
in, t
rem
or.
Valp
roat
e: N
eura
l tub
e de
fect
s (i.e
., ra
te 6
–20%
); hi
gh ra
tes o
f men
tal r
etar
datio
n an
d lo
wer I
Q
mea
sure
s.
Car
bam
azep
ine:
May
cau
se d
izzi
ness
, dro
wsin
ess,
unste
adin
ess,
impa
ired
coor
dina
tion,
nau
sea/
vom
iting
, blu
rred
visio
n, n
ysta
gmus
, ras
h,
conf
usio
n.
Car
bam
azep
ine:
Neu
ral t
ube
defe
cts,
min
or
anom
alies
.
Oxc
arba
zepi
ne: M
ay c
ause
diz
zine
ss, s
omno
lence
, dip
lopi
a, vi
sual
chan
ges,
fatig
ue, h
eada
che,
naus
ea, v
omiti
ng, a
nd a
taxi
a.O
xcar
baze
pine
: Unk
nown
.
Lam
otrig
ine:
Chi
ldre
n ar
e at
gre
ater
risk
for r
ash
than
adu
lts. M
ay c
ause
na
usea
, vom
iting
, diz
zine
ss, v
ertig
o, vi
sual
distu
rban
ce, s
omno
lence
, at
axy,
prur
itus/
rash
, hea
dach
e, ph
aryn
gitis
, rhi
nitis
, dia
rrhea
, fev
er, l
oss
of m
uscle
stre
ngth
.
Lam
otrig
ine:
Unk
nown
but
ther
e ap
pear
s to
be a
hi
gh ra
te o
f clef
t lip
and
pala
te
(i.e.,
4–9
/1,0
00).
Gab
apen
tin: M
ay c
ause
diz
zine
ss, s
omno
lence
, ata
xia,
fatig
ue, p
erip
hera
l ed
ema,
nysta
gmus
, nau
sea,
vom
iting
, and
vira
l inf
ectio
n.G
abap
entin
/pre
gaba
lin: U
nkno
wn.
TAB
LE 8
(Continued
)
Psyc
hotr
opic
Dru
gs: S
ide
Effe
cts a
nd T
erat
ogen
ic R
isks
PB-Child & Adolescent Dosing.indd 76 05-02-2018 16:02:30
NOT FOR R
EPRINT
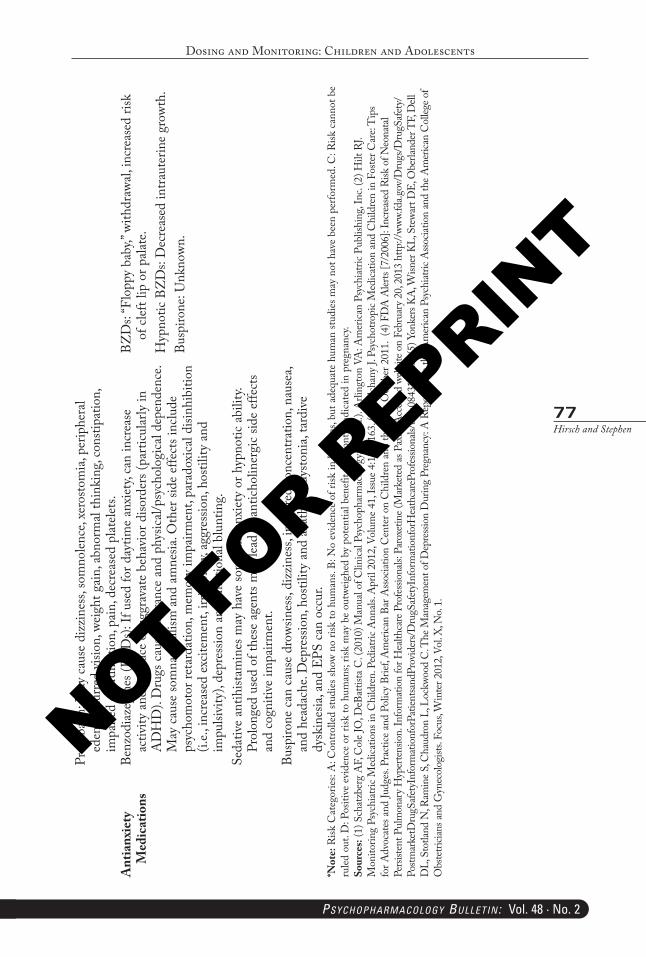
Dosing and Monitoring: Children and Adolescents
77Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Preg
abali
n: M
ay c
ause
diz
zine
ss, s
omno
lence
, xer
osto
mia
, per
iphe
ral
edem
a, bl
urre
d vi
sion,
wei
ght g
ain,
abn
orm
al th
inki
ng, c
onsti
patio
n,
impa
ired
coor
dina
tion,
pai
n, d
ecre
ased
plat
elets.
Ant
ianx
iety
M
edic
atio
nsBe
nzod
iaze
pine
s (BZ
Ds):
If u
sed
for d
aytim
e an
xiet
y, ca
n in
crea
se
activ
ity a
nd p
rodu
ce o
r agg
rava
te b
ehav
ior d
isord
ers (
parti
cular
ly in
A
DH
D).
Dru
gs c
ause
toler
ance
and
phy
sical/
psyc
holo
gica
l dep
ende
nce.
May
cau
se so
mna
mbu
lism
and
am
nesia
. Oth
er si
de e
ffect
s inc
lude
ps
ycho
mot
or re
tard
atio
n, m
emor
y im
pairm
ent,
para
doxi
cal d
isinh
ibiti
on
(i.e.,
incr
ease
d ex
citem
ent,
irrita
bilit
y, ag
gres
sion,
hos
tility
and
im
pulsi
vity
), de
pres
sion
and
emot
iona
l blu
ntin
g.Se
dativ
e an
tihist
amin
es m
ay h
ave
som
e an
tianx
iety
or h
ypno
tic a
bilit
y. Pr
olon
ged
used
of t
hese
age
nts m
ay le
ad to
ant
ichol
iner
gic
side
effe
cts
and
cogn
itive
impa
irmen
t.Bu
spiro
ne c
an c
ause
dro
wsin
ess,
dizz
ines
s, im
paire
d co
ncen
tratio
n, n
ause
a, an
d he
adac
he. D
epre
ssio
n, h
ostil
ity a
nd a
kath
isia,
dysto
nia,
tard
ive
dysk
ines
ia, a
nd E
PS c
an o
ccur
.
BZD
s: “F
lopp
y ba
by,”
with
draw
al, in
crea
sed
risk
of c
left l
ip o
r pala
te.
Hyp
notic
BZ
Ds:
Dec
reas
ed in
traut
erin
e gr
owth
.Bu
spiro
ne: U
nkno
wn.
*Not
e: R
isk C
ateg
orie
s: A
: Con
trolle
d stu
dies
show
no
risk
to h
uman
s. B:
No
evid
ence
of r
isk in
hum
ans,
but a
dequ
ate
hum
an st
udie
s may
not
hav
e be
en p
erfo
rmed
. C: R
isk c
anno
t be
ruled
out
. D: P
ositi
ve e
vide
nce
or ri
sk to
hum
ans;
risk
may
be
outw
eigh
ed b
y po
tent
ial b
enef
it. X
: Con
train
dica
ted
in p
regn
ancy
.So
urce
s: (1
) Sch
atzb
erg
AF,
Col
e JO
, DeB
attis
ta C
. (20
10) M
anua
l of C
linica
l Psy
chop
harm
acol
ogy.
(7th
ed.).
Arli
ngto
n VA
: Am
erica
n Ps
ychi
atric
Pub
lishi
ng, I
nc. (
2) H
ilt R
J. M
onito
ring
Psyc
hiat
ric M
edica
tions
in C
hild
ren.
Ped
iatric
Ann
als. A
pril
2012
, Vol
ume 4
1, Is
sue 4
:157
–163
. (3)
Sol
chan
y J.
Psyc
hotro
pic M
edica
tion
and
Chi
ldre
n in
Fos
ter C
are:
Tip
s fo
r Adv
ocat
es an
d Ju
dges
. Pra
ctice
and
Polic
y Br
ief, A
mer
ican
Bar A
ssoc
iatio
n C
ente
r on
Chi
ldre
n an
d th
e Law
. Oct
ober
201
1. (4
) FD
A A
lerts
[7/2
006]
: Inc
reas
ed R
isk o
f Neo
nata
l Pe
rsiste
nt P
ulm
onar
y Hyp
erte
nsio
n. In
form
atio
n fo
r Hea
lthca
re P
rofe
ssion
als: P
arox
etin
e (M
arke
ted
as P
axil)
. Acc
esse
d we
bsite
on
Febr
uary
20,
2013
http
://ww
w.fd
a.gov
/Dru
gs/D
rugS
afet
y/Po
stmar
ketD
rugS
afet
yInf
orm
atio
nfor
Patie
ntsa
ndPr
ovid
ers/D
rugS
afet
yInf
orm
atio
nfor
Hea
thca
rePr
ofes
siona
ls/uc
m08
4319
.htm
(5) Y
onke
rs KA
, Wisn
er K
L, S
tewa
rt D
E, O
berla
nder
TF,
Dell
D
L, S
totla
nd N
, Ram
ine S
, Cha
udro
n L,
Loc
kwoo
d C
. The
Man
agem
ent o
f Dep
ressi
on D
urin
g Pr
egna
ncy:
A R
epor
t fro
m th
e Am
erica
n Ps
ychi
atric
Asso
ciatio
n an
d th
e Am
erica
n C
olleg
e of
Obs
tetri
cians
and
Gyn
ecol
ogist
s. Fo
cus,
Win
ter 2
012,
Vol. X
, No.
1.
PB-Child & Adolescent Dosing.indd 77 05-02-2018 16:02:30
NOT FOR R
EPRINT
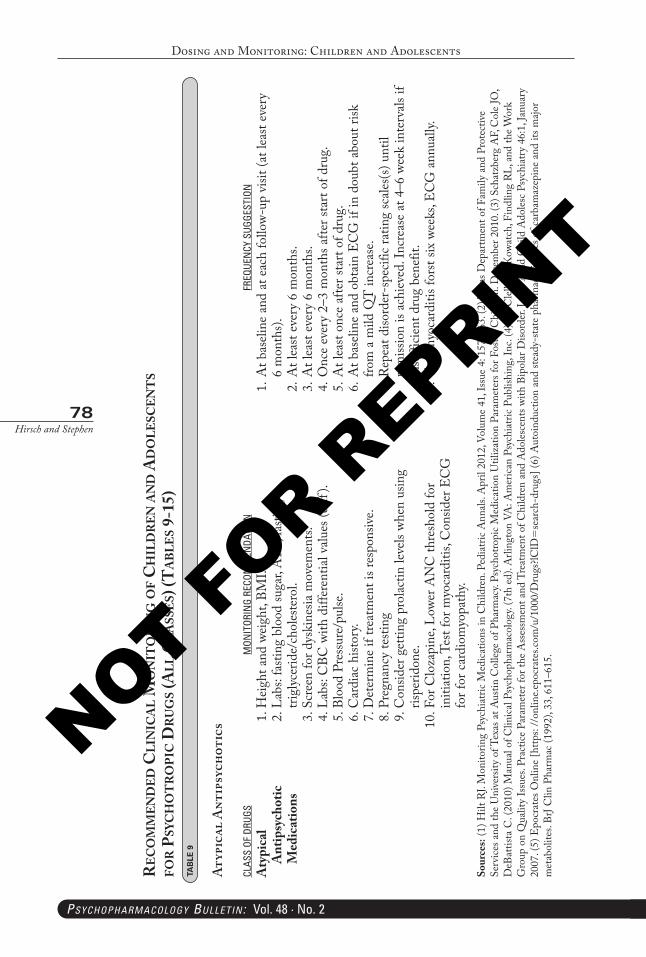
Dosing and Monitoring: Children and Adolescents
78Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
re
co
mm
end
ed c
lIn
Ica
l m
on
Ito
rIn
g o
f c
hIl
dr
en a
nd
ad
ole
scen
ts
for
Psy
ch
ot
ro
PIc
dr
ug
s (a
ll c
lass
es) (
ta
bles
9-1
5)TA
BLE
9
Atyp
ical
Ant
ipsy
chot
ics
CLAS
S OF
DRU
GSM
ONIT
ORIN
G RE
COM
MEN
DATI
ONFR
EQUE
NCY
SUG
GEST
ION
Aty
pica
l A
ntip
sych
otic
M
edic
atio
ns
1. H
eigh
t and
wei
ght,
BMI.
2. L
abs:
fasti
ng b
lood
suga
r, A
1C, f
astin
g tri
glyc
erid
e/ch
oles
tero
l. 3
. Scr
een
for d
yski
nesia
mov
emen
ts. 4
. Lab
s: C
BC w
ith d
iffer
entia
l valu
es (d
iff).
5. B
lood
Pre
ssur
e/pu
lse.
6. C
ardi
ac h
istor
y. 7
. Det
erm
ine
if tre
atm
ent i
s res
pons
ive.
8. P
regn
ancy
testi
ng 9
. Con
sider
get
ting
prol
actin
leve
ls wh
en u
sing
rispe
ridon
e.10
. For
Clo
zapi
ne, L
ower
AN
C th
resh
old
for
initi
atio
n, T
est f
or m
yoca
rditi
s, C
onsid
er E
CG
fo
r for
car
diom
yopa
thy.
1. A
t bas
eline
and
at e
ach
follo
w-up
visi
t (at
leas
t eve
ry
6 m
onth
s).2.
At l
east
ever
y 6
mon
ths.
3. A
t lea
st ev
ery
6 m
onth
s.4.
Onc
e ev
ery
2–3
mon
ths a
fter s
tart
of d
rug.
5. A
t lea
st on
ce a
fter s
tart
of d
rug.
6. A
t bas
eline
and
obt
ain
EC
G if
in d
oubt
abo
ut ri
sk
from
a m
ild Q
T in
crea
se.
7. R
epea
t diso
rder
-spe
cific
ratin
g sc
ales(s
) unt
il re
miss
ion
is ac
hiev
ed. I
ncre
ase
at 4
–6 w
eek
inte
rvals
if
insu
fficie
nt d
rug
bene
fit.
8. Te
st m
yoca
rditi
s for
st six
wee
ks, E
CG
ann
ually
.
Sour
ces:
(1) H
ilt R
J. M
onito
ring
Psyc
hiat
ric M
edica
tions
in C
hild
ren.
Ped
iatri
c A
nnals
. Apr
il 20
12, V
olum
e 41
, Iss
ue 4
: 157
–163
. (2)
Tex
as D
epar
tmen
t of F
amily
and
Pro
tect
ive
Serv
ices a
nd th
e U
nive
rsity
of T
exas
at A
ustin
Col
lege
of P
harm
acy.
Psyc
hotro
pic
Med
icatio
n U
tiliz
atio
n Pa
ram
eter
s for
Fos
ter C
hild
ren.
Dec
embe
r 201
0. (3
) Sch
atzb
erg
AF,
Col
e JO
, D
eBat
tista
C. (
2010
) Man
ual o
f Clin
ical P
sych
opha
rmac
olog
y. (7
th e
d). A
rling
ton
VA: A
mer
ican
Psyc
hiat
ric P
ublis
hing
, Inc
. (4)
McC
lellan
J, K
owat
ch, F
indl
ing
RL, a
nd th
e W
ork
Gro
up o
n Q
ualit
y Is
sues
. Pra
ctice
Par
amet
er fo
r the
Ass
essm
ent a
nd T
reat
men
t of C
hild
ren
and
Ado
lesce
nts w
ith B
ipol
ar D
isord
er. J
Am
Aca
d C
hild
Ado
lesc
Psyc
hiat
ry 4
6:1,
Janu
ary
2007
. (5)
Epo
crat
es O
nlin
e [h
ttps:
//on
line.e
pocr
ates
.com
/u/1
000/
Dru
gs?lC
lD=
sear
ch-d
rugs
] (6)
Aut
oind
uctio
n an
d ste
ady-
state
pha
rmac
okin
etics
of c
arba
maz
epin
e an
d its
majo
r m
etab
olite
s. Br
J Clin
Pha
rmac
(199
2), 3
3, 61
1–61
5.
PB-Child & Adolescent Dosing.indd 78 05-02-2018 16:02:30
NOT FOR R
EPRINT
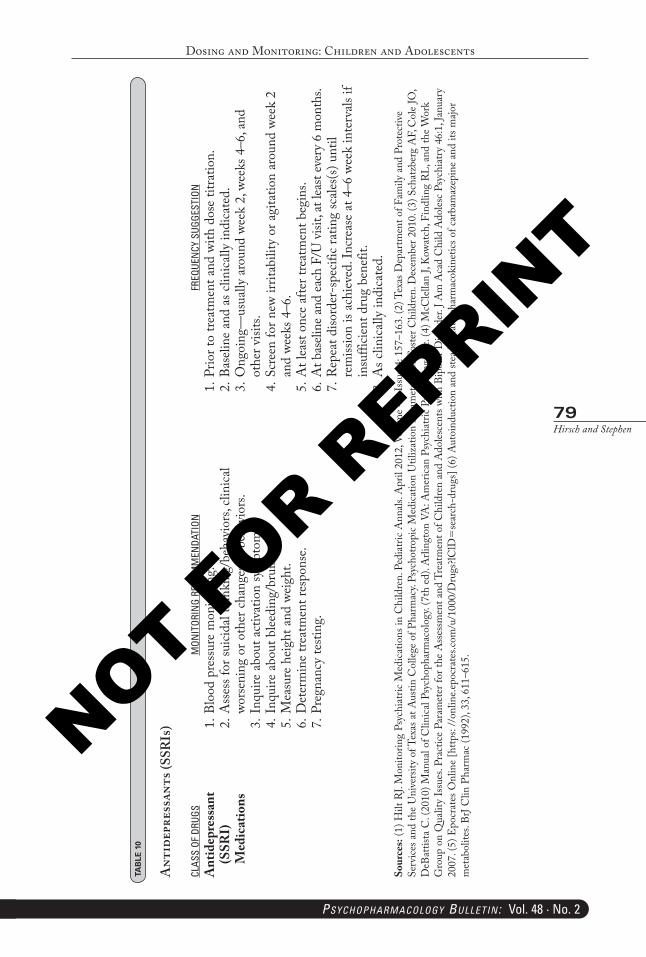
Dosing and Monitoring: Children and Adolescents
79Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
TAB
LE 1
0
Ant
idep
ress
ants
(SSR
Is)
CLAS
S OF
DRU
GSM
ONIT
ORIN
G RE
COM
MEN
DATI
ONFR
EQUE
NCY
SUG
GEST
ION
Ant
idep
ress
ant
(SSR
I)
Med
icat
ions
1. Bl
ood
pres
sure
mon
itorin
g.2.
Ass
ess f
or su
icida
l thi
nkin
g/be
havi
ors,
clini
cal
wors
enin
g or
oth
er c
hang
es in
beh
avio
rs.
3. In
quire
abo
ut a
ctiv
atio
n sy
mpt
oms.
4. In
quire
abo
ut b
leedi
ng/b
ruisi
ng.
5. M
easu
re h
eigh
t and
wei
ght.
6. D
eter
min
e tre
atm
ent r
espo
nse.
7. Pr
egna
ncy
testi
ng.
1. Pr
ior t
o tre
atm
ent a
nd w
ith d
ose
titra
tion.
2. Ba
selin
e an
d as
clin
ically
indi
cate
d.3.
Ong
oing
—us
ually
aro
und
week
2, w
eeks
4–6
, and
ot
her v
isits.
4. Sc
reen
for n
ew ir
ritab
ility
or a
gita
tion
arou
nd w
eek
2 an
d we
eks 4
–6.
5. A
t lea
st on
ce a
fter t
reat
men
t beg
ins.
6. A
t bas
eline
and
each
F/U
visi
t, at
leas
t eve
ry 6
mon
ths.
7. R
epea
t diso
rder
-spe
cific
ratin
g sc
ales(s
) unt
il re
miss
ion
is ac
hiev
ed. I
ncre
ase
at 4
–6 w
eek
inte
rvals
if
insu
fficie
nt d
rug
bene
fit.
8. A
s clin
ically
indi
cate
d.So
urce
s: (1
) Hilt
RJ.
Mon
itorin
g Ps
ychi
atric
Med
icatio
ns in
Chi
ldre
n. P
edia
tric
Ann
als. A
pril
2012
, Vol
ume
41, I
ssue
4: 1
57–1
63. (
2) T
exas
Dep
artm
ent o
f Fam
ily a
nd P
rote
ctiv
e Se
rvice
s and
the
Uni
vers
ity o
f Tex
as a
t Aus
tin C
olleg
e of
Pha
rmac
y. Ps
ycho
tropi
c M
edica
tion
Util
izat
ion
Para
met
ers f
or F
oste
r Chi
ldre
n. D
ecem
ber 2
010.
(3) S
chat
zber
g A
F, C
ole
JO,
DeB
attis
ta C
. (20
10) M
anua
l of C
linica
l Psy
chop
harm
acol
ogy.
(7th
ed)
. Arli
ngto
n VA
: Am
erica
n Ps
ychi
atric
Pub
lishi
ng, I
nc. (
4) M
cClel
lan J,
Kow
atch
, Fin
dlin
g RL
, and
the
Wor
k G
roup
on
Qua
lity
Issu
es. P
ract
ice P
aram
eter
for t
he A
sses
smen
t and
Tre
atm
ent o
f Chi
ldre
n an
d A
doles
cent
s with
Bip
olar
Diso
rder
. J A
m A
cad
Chi
ld A
doles
c Ps
ychi
atry
46:
1, Ja
nuar
y 20
07. (
5) E
pocr
ates
Onl
ine
[http
s: //
onlin
e.epo
crat
es.co
m/u
/100
0/D
rugs
?lClD
=se
arch
-dru
gs] (
6) A
utoi
nduc
tion
and
stead
y-sta
te p
harm
acok
inet
ics o
f car
bam
azep
ine
and
its m
ajor
met
abol
ites.
BrJ C
lin P
harm
ac (1
992)
, 33,
611–
615.
PB-Child & Adolescent Dosing.indd 79 05-02-2018 16:02:30
NOT FOR R
EPRINT
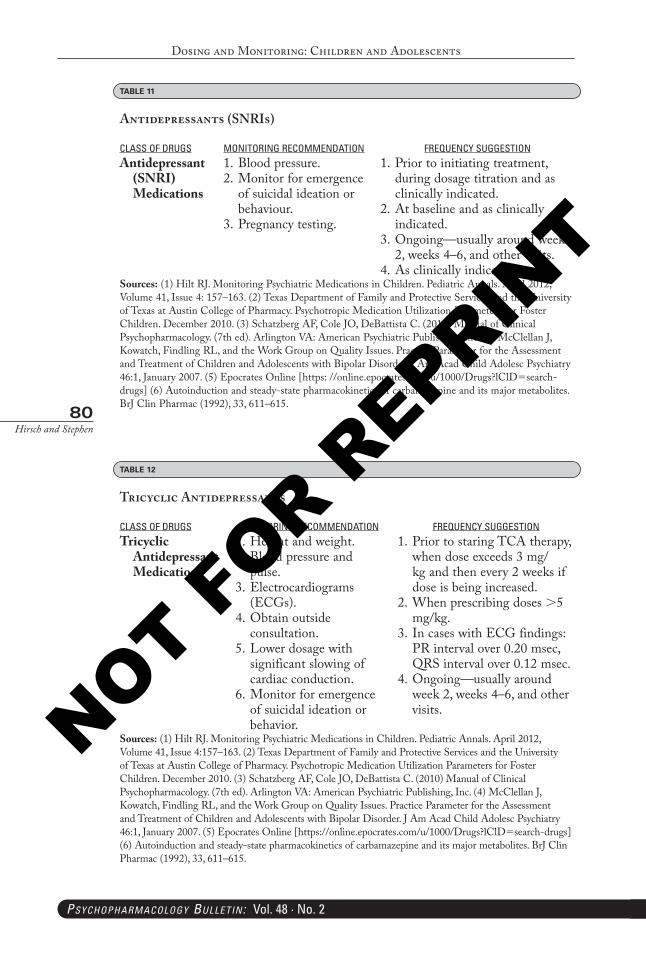
Dosing and Monitoring: Children and Adolescents
80Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
TABLE 12
Tricyclic Antidepressants
CLASS OF DRUGS MONITORING RECOMMENDATION FREQUENCY SUGGESTIONTricyclic
Antidepressant Medications
1. Height and weight.2. Blood pressure and
pulse.3. Electrocardiograms
(ECGs).4. Obtain outside
consultation.5. Lower dosage with
significant slowing of cardiac conduction.
6. Monitor for emergence of suicidal ideation or behavior.
1. Prior to staring TCA therapy, when dose exceeds 3 mg/kg and then every 2 weeks if dose is being increased.
2. When prescribing doses >5 mg/kg.
3. In cases with ECG findings: PR interval over 0.20 msec, QRS interval over 0.12 msec.
4. Ongoing—usually around week 2, weeks 4–6, and other visits.
Sources: (1) Hilt RJ. Monitoring Psychiatric Medications in Children. Pediatric Annals. April 2012, Volume 41, Issue 4:157–163. (2) Texas Department of Family and Protective Services and the University of Texas at Austin College of Pharmacy. Psychotropic Medication Utilization Parameters for Foster Children. December 2010. (3) Schatzberg AF, Cole JO, DeBattista C. (2010) Manual of Clinical Psychopharmacology. (7th ed). Arlington VA: American Psychiatric Publishing, Inc. (4) McClellan J, Kowatch, Findling RL, and the Work Group on Quality Issues. Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder. J Am Acad Child Adolesc Psychiatry 46:1, January 2007. (5) Epocrates Online [https://online.epocrates.com/u/1000/Drugs?lClD=search-drugs] (6) Autoinduction and steady-state pharmacokinetics of carbamazepine and its major metabolites. BrJ Clin Pharmac (1992), 33, 611–615.
TABLE 11
Antidepressants (SNRIs)
CLASS OF DRUGS MONITORING RECOMMENDATION FREQUENCY SUGGESTIONAntidepressant
(SNRI) Medications
1. Blood pressure.2. Monitor for emergence
of suicidal ideation or behaviour.
3. Pregnancy testing.
1. Prior to initiating treatment, during dosage titration and as clinically indicated.
2. At baseline and as clinically indicated.
3. Ongoing—usually around week 2, weeks 4–6, and other visits.
4. As clinically indicated.Sources: (1) Hilt RJ. Monitoring Psychiatric Medications in Children. Pediatric Annals. April 2012, Volume 41, Issue 4: 157–163. (2) Texas Department of Family and Protective Services and the University of Texas at Austin College of Pharmacy. Psychotropic Medication Utilization Parameters for Foster Children. December 2010. (3) Schatzberg AF, Cole JO, DeBattista C. (2010) Manual of Clinical Psychopharmacology. (7th ed). Arlington VA: American Psychiatric Publishing, Inc. (4) McClellan J, Kowatch, Findling RL, and the Work Group on Quality Issues. Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder. J Am Acad Child Adolesc Psychiatry 46:1, January 2007. (5) Epocrates Online [https: //online.epocrates.com/u/1000/Drugs?lClD=search-drugs] (6) Autoinduction and steady-state pharmacokinetics of carbamazepine and its major metabolites. BrJ Clin Pharmac (1992), 33, 611–615.
PB-Child & Adolescent Dosing.indd 80 05-02-2018 16:02:30
NOT FOR R
EPRINT
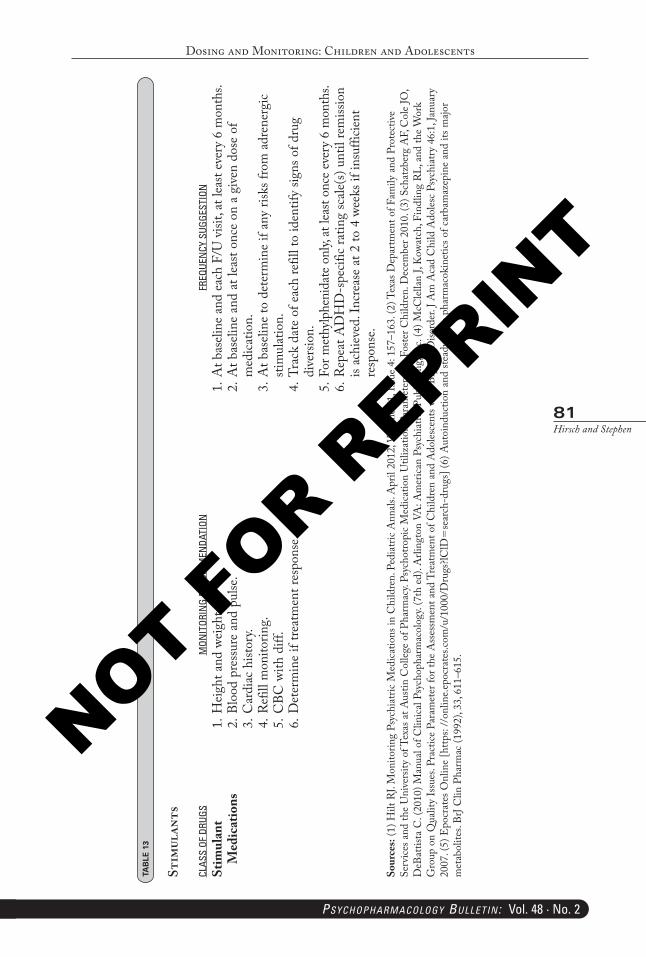
Dosing and Monitoring: Children and Adolescents
81Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
TAB
LE 1
3
Stim
ulan
ts
CLAS
S OF
DRU
GSM
ONIT
ORIN
G RE
COM
MEN
DATI
ONFR
EQUE
NCY
SUG
GEST
ION
Stim
ulan
t M
edic
atio
ns1.
Hei
ght a
nd w
eigh
t.2.
Bloo
d pr
essu
re a
nd p
ulse
.3.
Car
diac
hist
ory.
4. R
efill
mon
itorin
g.5.
CBC
with
diff
.6.
Det
erm
ine
if tre
atm
ent r
espo
nse.
1. A
t bas
eline
and
eac
h F/
U v
isit,
at le
ast e
very
6 m
onth
s.2.
At b
aseli
ne a
nd a
t lea
st on
ce o
n a
give
n do
se o
f m
edica
tion.
3. A
t bas
eline
to d
eter
min
e if
any
risks
from
adr
ener
gic
stim
ulat
ion.
4. Tr
ack
date
of e
ach
refil
l to
iden
tify
signs
of d
rug
dive
rsio
n.5.
For m
ethy
lphe
nida
te o
nly,
at le
ast o
nce e
very
6 m
onth
s.6.
Rep
eat A
DH
D-s
pecif
ic ra
ting
scale
(s) u
ntil
rem
issio
n is
achi
eved
. Inc
reas
e at
2 to
4 w
eeks
if in
suffi
cient
re
spon
se.
Sour
ces:
(1) H
ilt R
J. M
onito
ring
Psyc
hiat
ric M
edica
tions
in C
hild
ren.
Ped
iatri
c A
nnals
. Apr
il 20
12, V
olum
e 41
, Iss
ue 4
: 157
–163
. (2)
Tex
as D
epar
tmen
t of F
amily
and
Pro
tect
ive
Serv
ices a
nd th
e U
nive
rsity
of T
exas
at A
ustin
Col
lege
of P
harm
acy.
Psyc
hotro
pic
Med
icatio
n U
tiliz
atio
n Pa
ram
eter
s for
Fos
ter C
hild
ren.
Dec
embe
r 201
0. (3
) Sch
atzb
erg
AF,
Col
e JO
, D
eBat
tista
C. (
2010
) Man
ual o
f Clin
ical P
sych
opha
rmac
olog
y. (7
th e
d). A
rling
ton
VA: A
mer
ican
Psyc
hiat
ric P
ublis
hing
, Inc
. (4)
McC
lellan
J, K
owat
ch, F
indl
ing
RL, a
nd th
e W
ork
Gro
up o
n Q
ualit
y Is
sues
. Pra
ctice
Par
amet
er fo
r the
Ass
essm
ent a
nd T
reat
men
t of C
hild
ren
and
Ado
lesce
nts w
ith B
ipol
ar D
isord
er. J
Am
Aca
d C
hild
Ado
lesc
Psyc
hiat
ry 4
6:1,
Janu
ary
2007
. (5)
Epo
crat
es O
nlin
e [h
ttps:
//on
line.e
pocr
ates
.com
/u/1
000/
Dru
gs?lC
lD=
sear
ch-d
rugs
] (6)
Aut
oind
uctio
n an
d ste
ady-
state
pha
rmac
okin
etics
of c
arba
maz
epin
e an
d its
majo
r m
etab
olite
s. Br
J Clin
Pha
rmac
(199
2), 3
3, 61
1–61
5.
PB-Child & Adolescent Dosing.indd 81 05-02-2018 16:02:31
NOT FOR R
EPRINT
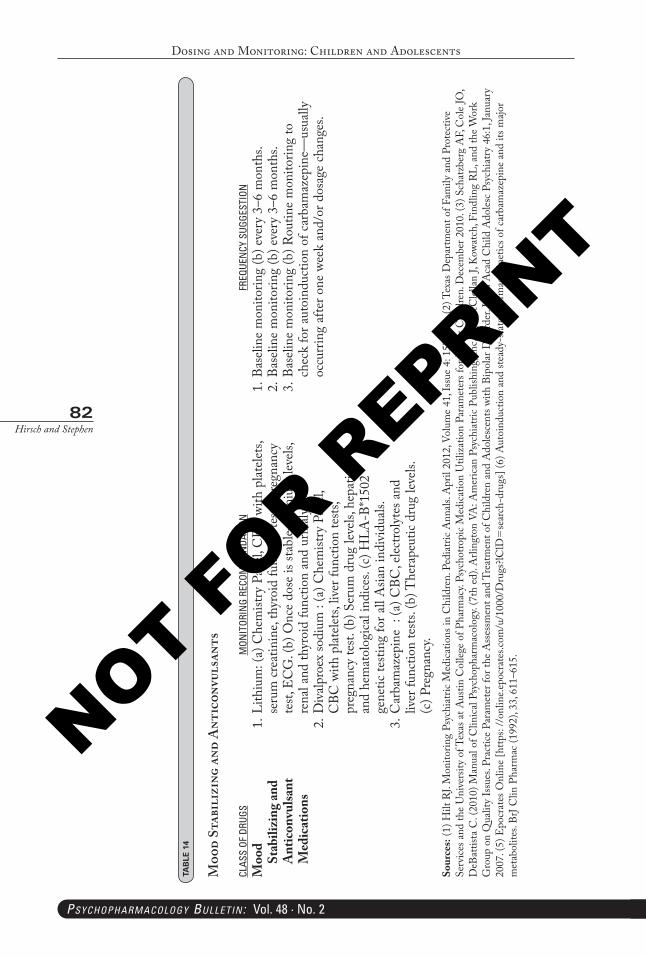
Dosing and Monitoring: Children and Adolescents
82Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
TAB
LE 1
4
Moo
d St
abil
izin
g an
d A
ntic
onvu
lsan
ts
CLAS
S OF
DRU
GSM
ONIT
ORIN
G RE
COM
MEN
DATI
ONFR
EQUE
NCY
SUG
GEST
ION
Moo
d St
abili
zing
and
Ant
icon
vulsa
nt
Med
icat
ions
1. Li
thiu
m: (
a) C
hem
istry
Pan
el, C
BC w
ith p
latele
ts,
seru
m c
reat
inin
e, th
yroi
d fu
nctio
n te
sts, p
regn
ancy
te
st, E
CG
. (b)
Onc
e do
se is
stab
le—lit
hium
leve
ls,
rena
l and
thyr
oid
func
tion
and
urin
alys
is.2.
Div
alpro
ex so
dium
: (a
) Che
mist
ry P
anel,
C
BC w
ith p
latele
ts, li
ver f
unct
ion
tests
, pr
egna
ncy
test.
(b) S
erum
dru
g le
vels,
hep
atic
and
hem
atol
ogica
l ind
ices.
(c) H
LA-B
*150
2 ge
netic
testi
ng fo
r all
Asia
n in
divi
duals
.3.
Car
bam
azep
ine
: (a
) CBC
, elec
troly
tes a
nd
liver
func
tion
tests
. (b)
The
rape
utic
drug
leve
ls.
(c) P
regn
ancy
.
1. Ba
selin
e m
onito
ring
(b) e
very
3–6
mon
ths.
2. Ba
selin
e m
onito
ring
(b) e
very
3–6
mon
ths.
3. Ba
selin
e m
onito
ring
(b) R
outin
e m
onito
ring
to
chec
k fo
r aut
oind
uctio
n of
car
bam
azep
ine—
usua
lly
occu
rrin
g af
ter o
ne w
eek
and/
or d
osag
e ch
ange
s.
Sour
ces:
(1) H
ilt R
J. M
onito
ring
Psyc
hiat
ric M
edica
tions
in C
hild
ren.
Ped
iatri
c A
nnals
. Apr
il 20
12, V
olum
e 41
, Iss
ue 4
: 157
–163
. (2)
Tex
as D
epar
tmen
t of F
amily
and
Pro
tect
ive
Serv
ices a
nd th
e U
nive
rsity
of T
exas
at A
ustin
Col
lege
of P
harm
acy.
Psyc
hotro
pic
Med
icatio
n U
tiliz
atio
n Pa
ram
eter
s for
Fos
ter C
hild
ren.
Dec
embe
r 201
0. (3
) Sch
atzb
erg
AF,
Col
e JO
, D
eBat
tista
C. (
2010
) Man
ual o
f Clin
ical P
sych
opha
rmac
olog
y. (7
th e
d). A
rling
ton
VA: A
mer
ican
Psyc
hiat
ric P
ublis
hing
, Inc
. (4)
McC
lellan
J, K
owat
ch, F
indl
ing
RL, a
nd th
e W
ork
Gro
up o
n Q
ualit
y Is
sues
. Pra
ctice
Par
amet
er fo
r the
Ass
essm
ent a
nd T
reat
men
t of C
hild
ren
and
Ado
lesce
nts w
ith B
ipol
ar D
isord
er. J
Am
Aca
d C
hild
Ado
lesc
Psyc
hiat
ry 4
6:1,
Janu
ary
2007
. (5)
Epo
crat
es O
nlin
e [h
ttps:
//on
line.e
pocr
ates
.com
/u/1
000/
Dru
gs?lC
lD=
sear
ch-d
rugs
] (6)
Aut
oind
uctio
n an
d ste
ady-
state
pha
rmac
okin
etics
of c
arba
maz
epin
e an
d its
majo
r m
etab
olite
s. Br
J Clin
Pha
rmac
(199
2), 3
3, 61
1–61
5.
PB-Child & Adolescent Dosing.indd 82 05-02-2018 16:02:31
NOT FOR R
EPRINT
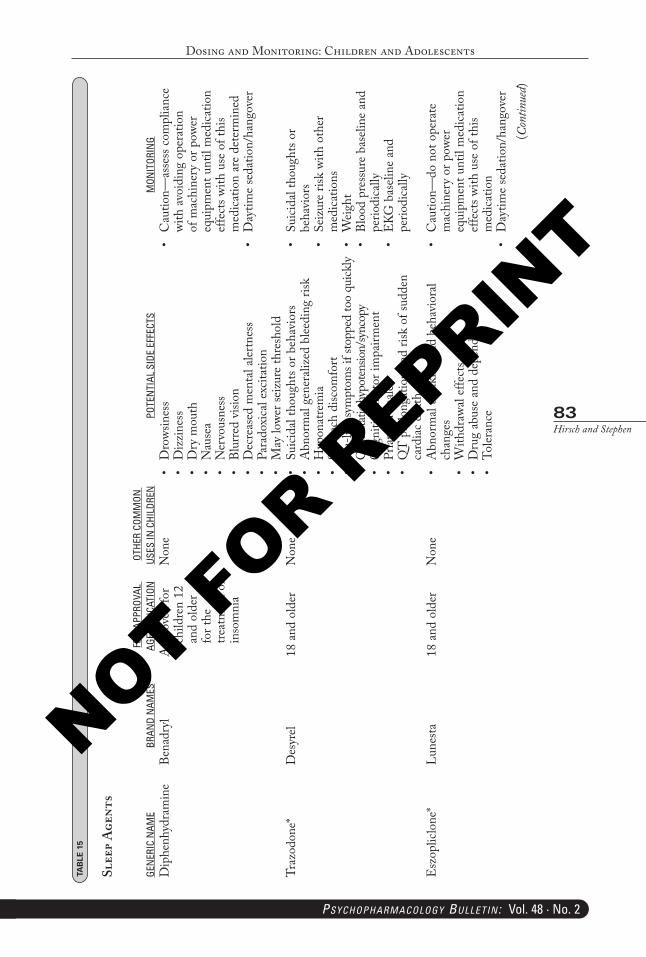
Dosing and Monitoring: Children and Adolescents
83Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
TAB
LE 1
5
Slee
p A
gent
s
GEN
ERIC
NAM
EBR
AND
NAM
ESFD
A AP
PROV
AL
AGE/
INDI
CATI
ONOT
HER
COM
MON
US
ES IN
CHI
LDRE
NPO
TEN
TIAL
SID
E EF
FECT
SM
ONIT
ORIN
GD
iphe
nhyd
ram
ine
Bena
dryl
App
rove
d fo
r ch
ildre
n 12
an
d ol
der
for t
he
treat
men
t of
inso
mni
a
Non
e•
Dro
wsin
ess
•D
izzi
ness
•D
rym
outh
•N
ause
a•
Ner
vous
ness
•Bl
urre
dvi
sion
•D
ecre
ased
men
tala
lertn
ess
•Pa
rado
xica
lexc
itatio
n•
May
lowe
rsei
zure
thre
shol
d
•C
autio
n—as
sess
com
plia
nce
with
avo
idin
g op
erat
ion
of m
achi
nery
or p
ower
eq
uipm
ent u
ntil
med
icatio
n ef
fect
s with
use
of t
his
med
icatio
n ar
e de
term
ined
•D
aytim
ese
datio
n/ha
ngov
er
Traz
odon
e*D
esyr
el18
and
old
erN
one
•Su
icida
ltho
ught
sorb
ehav
iors
•A
bnor
mal
gene
raliz
edb
leedi
ngri
sk•
Hyp
onat
rem
ia•
Stom
ach
disc
omfo
rt•
Flu-
likes
ympt
omsi
fsto
pped
too
quick
ly•
Orth
ostat
ichy
poten
sion/
sync
opy
•C
ogni
tive/
mot
orim
pairm
ent
•Pr
iapi
sm-m
ales
•Q
Tp
rolo
ngat
ion
and
risk
ofsu
dden
ca
rdiac
dea
th
•Su
icida
ltho
ught
sor
beha
vior
s•
Seiz
ure
risk
with
oth
er
med
icatio
ns•
Wei
ght
•Bl
ood
pres
sure
bas
eline
and
pe
riodi
cally
•EK
Gb
aseli
nea
nd
perio
dica
lly
Esz
oplic
lone
*Lu
nesta
18 a
nd o
lder
Non
e•
Abn
orm
alth
inki
nga
ndb
ehav
iora
lch
ange
s•
With
draw
alef
fect
s•
Dru
gab
use
and
depe
nden
ce•
Toler
ance
•C
autio
n—do
not
ope
rate
m
achi
nery
or p
ower
eq
uipm
ent u
ntil
med
icatio
n ef
fect
s with
use
of t
his
med
icatio
n•
Day
time
seda
tion/
hang
over
(Con
tinue
d)
PB-Child & Adolescent Dosing.indd 83 05-02-2018 16:02:31
NOT FOR R
EPRINT
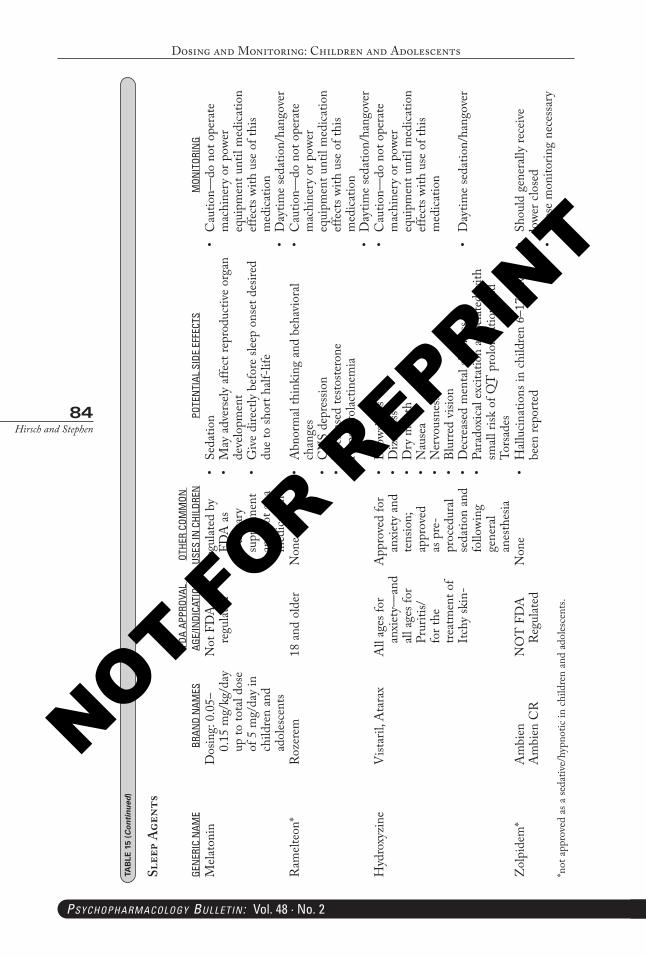
Dosing and Monitoring: Children and Adolescents
84Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Mela
toni
nD
osin
g: 0
.05–
0.15
mg/
kg/d
ay
up to
tota
l dos
e of
5 m
g/da
y in
ch
ildre
n an
d ad
oles
cent
s
Not
FD
A
regu
lated
Reg
ulat
ed b
y FD
A a
s a
diet
ary
supp
lemen
t an
d no
t as a
m
edica
tion
•Se
datio
n•
May
adv
erse
lya
ffect
repr
oduc
tive
orga
nde
velo
pmen
t•
Giv
edi
rect
lyb
efor
esle
epo
nset
des
ired
due
to sh
ort h
alf-li
fe
•C
autio
n—do
not
ope
rate
m
achi
nery
or p
ower
eq
uipm
ent u
ntil
med
icatio
n ef
fect
s with
use
of t
his
med
icatio
n•
Day
time
seda
tion/
hang
over
Ram
elteo
n*R
ozer
em18
and
old
erN
one
•A
bnor
mal
thin
king
and
beh
avio
ral
chan
ges
•C
NS
depr
essio
n•
Dec
reas
edte
stoste
rone
•H
yper
prol
actin
emia
•C
autio
n—do
not
ope
rate
m
achi
nery
or p
ower
eq
uipm
ent u
ntil
med
icatio
n ef
fect
s with
use
of t
his
med
icatio
n•
Day
time
seda
tion/
hang
over
Hyd
roxy
zine
Vist
aril,
Ata
rax
All
ages
for
anxi
ety—
and
all a
ges f
or
Prur
itis/
for t
he
treat
men
t of
Itch
y sk
in-
App
rove
d fo
r an
xiet
y an
d te
nsio
n;
appr
oved
as
pre
-pr
oced
ural
seda
tion
and
follo
wing
ge
nera
l an
esth
esia
•D
rows
ines
s•
Diz
zine
ss•
Dry
mou
th•
Nau
sea
•N
ervo
usne
ss•
Blur
red
visio
n•
Dec
reas
edm
enta
laler
tnes
s•
Para
doxi
cale
xcita
tion
asso
ciate
dwi
th
small
risk
of Q
T p
rolo
ngat
ion
and
Tors
ades
•C
autio
n—do
not
ope
rate
m
achi
nery
or p
ower
eq
uipm
ent u
ntil
med
icatio
n ef
fect
s with
use
of t
his
med
icatio
n
•D
aytim
ese
datio
n/ha
ngov
er
Zol
pide
m*
Am
bien
Am
bien
CR
NO
T F
DA
R
egul
ated
Non
e•
Hall
ucin
atio
nsin
chi
ldre
n6–
17h
ave
been
repo
rted
•Sh
ould
gen
erall
yre
ceiv
elo
wer c
lose
d•
Clo
sem
onito
ring
nece
ssar
y*n
ot a
ppro
ved
as a
seda
tive/
hypn
otic
in c
hild
ren
and
adol
esce
nts.
TAB
LE 1
5 (Continued
)
Slee
p A
gent
s
GEN
ERIC
NAM
EBR
AND
NAM
ESFD
A AP
PROV
AL
AGE/
INDI
CATI
ONOT
HER
COM
MON
US
ES IN
CHI
LDRE
NPO
TEN
TIAL
SID
E EF
FECT
SM
ONIT
ORIN
G
PB-Child & Adolescent Dosing.indd 84 05-02-2018 16:02:31
NOT FOR R
EPRINT
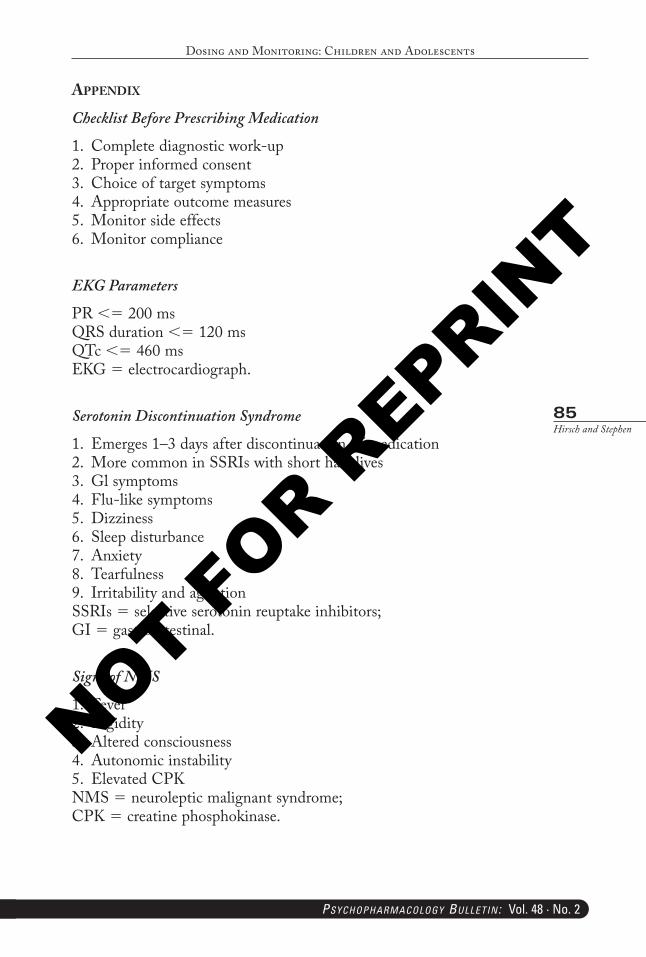
Dosing and Monitoring: Children and Adolescents
85Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
aPPendIx
Checklist Before Prescribing Medication
1. Complete diagnostic work-up2. Proper informed consent3. Choice of target symptoms4. Appropriate outcome measures5. Monitor side effects6. Monitor compliance
EKG Parameters
PR <= 200 msQRS duration <= 120 msQTc <= 460 msEKG = electrocardiograph.
Serotonin Discontinuation Syndrome
1. Emerges 1–3 days after discontinuation of medication2. More common in SSRIs with short half-lives3. Gl symptoms4. Flu-like symptoms5. Dizziness6. Sleep disturbance7. Anxiety8. Tearfulness9. Irritability and agitationSSRIs = selective serotonin reuptake inhibitors;GI = gastrointestinal.
Signs of NMS
1. Fever2. Rigidity3. Altered consciousness4. Autonomic instability5. Elevated CPKNMS = neuroleptic malignant syndrome;CPK = creatine phosphokinase.
PB-Child & Adolescent Dosing.indd 85 05-02-2018 16:02:31
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
86Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Signs Of Toxic [Central] Serotonin Syndrome
1. Gl symptoms2. Sweating3. Fever4. Tachycardia5. Hypertension6. Myoclonus7. Increased motor activity8. IrritabilityGI = gastrointestinal.
Internet Resources
• CytochromeP450Drug InteractionTablewww.drug-interactions.com
• HeightandWeightCharts—girlshttp://www.cdc.gov/nchs/about/major/nhanes/growthcharts/set1clinical/CJ41C022.pdf
• HeightandWeightCharts—boyshttp://www.cdc.gov/nchs/about/major/nhanes/growthcharts/set1clinical/CJ41C021.pdf
references
Agency for Health Care Administration: Florida Medicaid Drug Therapy Management Program for Behavioral Health. University of South Florida. 2016–17 Florida Best Practice Psychotherapeutic Medication Guidelines for Children and Adolescents. Accessed online on March 5, 2017 at http://www.medicaidmentalhealth.org/_assets/file/Guidelines/Web_2015-Psychotherapeutic%20Medication%20Guidelines%20for%20Adults_Final_Approved1.pdf
AIMS Center: Principles of Collaborative Care: Accessed online on March 15, 2017 at https://www.aacap.org/App_Themes/AACAP/docs/clinical_ practice_center/systems_of_care/AACAPPsychotropic_Medication_ Recommendations_2015_FINAL.pdf
Allen K, Jensen PS. CHCS Webinar: the Use of Psychotropic Medications for children Involved in Child Welfare. Presented on February 14, 2008. Accessed website on October 16, 2012 http://www.chcs.org/usr_doc/child_welfare_webinar_021408.pdf
American Academy of Child and Adolescent Psychiatry (AACAP) 2015: Recommendations about the use of psychotropic medications for children and adolescents involved in child-serving systems. Accessed online on March 5, 2017 at https://aims.uw.edu/collaborative-care/principles-collaborative-care
American Academy of Child and Adolescent Psychiatry (AACAP) 2017: Psychotherapy for chil-dren and adolescents: different types. Accesses online on March 15, 2017 at https://www.aacap.org/AACAP/Families_and_Youth/Facts_for_ Families/FFF-Guide/Psychotherapies-For-Children-And-Adolescents-086.aspx
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 2nd Edition. Washington, DC American Psychiatric Association, 1968
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 3rd Edition. Washington, DC, American Psychiatric Association, 1980
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 3rd Edition, Revised. Washington, DC, American Psychiatric Association, 1987
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 4th Edition. Washington, DC, American Psychiatric Association, 1994
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision. Washington, DC, American Psychiatric Association, 2000
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Arlington, VA, American Psychiatric Association, 2013
PB-Child & Adolescent Dosing.indd 86 05-02-2018 16:02:31
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
87Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
American Academy of Child and Adolescent Psychiatry: Bipolar Disorder Parents’ Medication Guide for Bipolar Disorder in Children and Adolescents. Accessed website on September 25, 2012 http://www.aacap.org/galleries/default-file/aacap_bipolar_medication_guide.pdf
American Academy of Pediatrics. ADHD: Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Pediatrics 128(5), November 2011
Andersen SL, Navalta CP. Altering the course of neurodevelopment: a framework for understanding the enduring effects of psychotropic drugs. Int J Devl Neuroscience 22:423–440, 2004
Andersen SL, Navalta CP. New frontiers in developmental neuropharmacology: Can long-term therapeu-tic effects of drugs be optimized through carefully timed early intervention? J Child Psychol Psychiatry 52(4):476–503, 2011
Anderson LE, Chen ML, Perrin JM, Cleave JC: Outpatient visits and medication prescribing for US chil-dren with mental health conditions. Pediatrics 136(5): e1178–e1185, 2015. Accessed online on March 5, 2017 at http://pediatrics. aappublications.org/content/pediatrics/early/2015/10/06/peds.2015-0807.full.pdf
APA Working Group on Psychoactive Medication for Children and Adolescents (2006): Report of the Working Group on Psychoactive Medications for Children and Adolescents. Psychopharmacological, psychosocial, and combined interventions for childhood disorder: Evidence base, contextual factors, and future directions. Washington, DC: American Psychological Association
Bauer MS, Dunner DL: Validity of seasonal pattern as a modifier for recurrent mood disorders for DSM-IV. Compr Psychiatry 34(3):159–170, 1993 8339533
Birmaher B, Brent D, and the AACAP Work Group on Quality Issues: Bernet W, Bukstein O, Walter H, Benson RS, Chrisman A, Farchione T, Greenhill L, Hamilton J, Keable H, Kinlan J, Schoettle U, Stock S. Practice Parameter for the Assessment and Treatment of Children and Adolescents with Depressive Disorders. J Am Acad Child Adolesc Psychiatry 46:11, November 2007
Blader JC, Schooler NR, Jensen PS, Pliszke SR, Karantaris V: Adjunctive Divalproex Versus Placebo for Children With ADHD and Aggression Refractory to Stimulant Monotherapy. Am J Psychiatry 166(12):1392–1401, December 2009
Bourdon KH, Boyd JH, Rae DS, et al: Gender differences in phobias: results of the ECA community survey. J Anxiety Disord 2:227–241, 1988
Boyd JH, Burke JD Jr, Gruenberg E, et al: Exclusion criteria of DSM-III: a study of co-occurrence of hierarchy-free syndromes. Arch Gen Psychiatry 41(10):983–989, 1984 6477056
Brasic JR, Pataki C: Autism Management and Treatment. Accessed website on June 18, 2012 http://emedi-cine.medscape.com/article/912781-treatment
Brent D, Emslie G, Fassler D, Kratochvil C, March J, Robb A, Shaffer D, Singh M: Membership of the Parents Medical Guide Workgroup. Parents Med Guide. The Use of Medication in the Treatment of Childhood and Adolescent Depression: Information for Patients and Families. Accessed website on September 25, 2012 http://www. parentsmedguide.org/parentsmedguide.htm#9
Cataife G, Weinberg DA: Racial and ethnic differences in antipsychotic medication use among children enrolled in Medicaid. Psychiatric Serv 66(9):946–951, 2015. Accessed online on March 5, 2017 at http://ps.psychiatryonline.org/doi/pdf/10.1176/appi.ps.201400045
Carrasco M, Volkmar FR, Bloch MH. Pharmacologic Treatment of Repetitive Behaviors in Autism Spectrum Disorders: Evidence of Publication Bias. Pediatrics 129(5), May 2012
Children’s Mental Health: Concerns Remain about Appropriate Services for Children in Medicaid and Foster Care. GAO-13-15. Washington, DC
Cincinnati Children’s Hospital Medical Center Best Evidence Statement (BESt): Treatment of children and Adolescents with Major Depressive Disorder (MDD) during the Acute Phase. January 2010
CMS 2017. A review of state Medicaid approaches on child antipsychotic monitoring programs. Accessed online on March 15, 2017 at https://www.medicaid.gov/medicaid-chip-program-information/by-topics/prescription-drugs/downloads/state-medicaid-dur-summaries.pdf
Cohen JA, and the Work Group on Quality Issues: Bukstein O, Walter H, Benson RS, Chrisman A, Farchione TR, Hamilton J, Keable H, Kinlan J, Schoettle, Siegal M, Stock S. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Posttraumatic Stress Disorder. J Am Acad Child Adolesc Psychiatry, 49(4), April 2010
Connelly SD, Bernstein GA, and the Work Group on Quality Issues: Bernet W, Bukstein O, Arnold V, Beitchman J, Benson S, Kinlan J, McClellan J, Schoettle U, Shaw J, Stock S, Walter H. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Anxiety Disorders. J Am Acad Child Adolesc Psychiatry. 46:2, February 2007
Cooper WO, Hickson GB, Fuch C, Arbogast PG, Ray W: New Users of Antipsychotic Medications Among Children Enrolled in TennCare. Arch Pediatr Adolesc Med/158, Aug. 2004
Correll CU, Dratochvil CJ, March JS: Developments in Pediatric Psychopharmacology: Focus on Stimulants, Antidepressants, and Antipsychotics. J Clin Psychiatry 72:5, May 2011
PB-Child & Adolescent Dosing.indd 87 05-02-2018 16:02:32
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
88Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Correll CU, Sheridan EM, DelBello MP: Antipsychotic and mood stabilizer efficacy and tolerability in pediatric and adult patients with bipolar I mania: a comparative analysis of acute, randomized, placebo-controlled trials. Bipolar disorder 12:116–141, 2010
Cos GR, Callahan P, Churchill R, Hunot V, Merry SN, Parker AG, Hetrick SE: Psychological therapies versus antidepressant medication, alone and in combination for depression in children and adolescents (Review). Cochrane Library, 2014. Accessed online on March 17, 2015 at http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD008324.pub3/pdf/abstract
Crystal S, Olfson M, Huang C, Pincus H: Gerhard. Broadened Use of Atypical Antipsychotics: Safety Effectiveness, and Policy Challenges: Expanded use of these medications, frequently off-label, has often outstripped the evidence base for the diverse range of patients who are treated with them. Health Aff (Millwood) 28(5), 2009
DeBattista C, Belanoff J, Glass S, et al: Mifepristone versus placebo in the treatment of psychosis in patients with psychotic major depression. Biol Psychiatry 60(12):1343–1349, 2006 16889757
Department of Health & Human Services: Collaborative efforts and technical assistance resources to strengthen the management of psychotropic medications for vulnerable populations. Accessed online at https://www.medicaid.gov/federal-policy-guidance/downloads/cib-08-24-12.pdf
Dobson ET, Strawn JR: Pharmacotherapy for pediatric generalized anxiety disorder: a systematic evaluation of efficacy, safety and tolerability. Paediatr drugs 18(1):45–53, 2016. Accessed online on March 5, 2017 at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4925147/pdf/nihms796969.pdf
dosReis S, Tai MH, Goffman D, Lynch SE, Reeves G, Shaw T: Age-related trends in psychotropic medica-tion use among very young children in foster care. Psychiatric Services 65(12):1452–1457, 2014
dosReis, S, Tai MH, Camelo WC, Reeves G: A national survey of state Medicaid psychotropic-monitoring programs targeting youths. Psychiatric Services 67(1):1146–1148, 2016
Eghaneyan BH, Sanchez, Mitschke DB: Implementation of a collaborative care model for the treat-ment of depression and anxiety in a community health center: results from a qualitative case study. J of Multidisciplinary Healthcare 503–513, 2014
Epstein RA, Bobo WV, Shelton RC, Arbogast PG, Morrow JA, Wang W, Chandrasekhar R, Cooper WO: Increasing use of atypical antipsychotics and anticonvulsants during pregnancy. Pharmacoepidemiology and Drug Safety (2012)
Evidence-Based Evaluation and Treatment of Youth with Maladaptive Aggression: American Academy of Child and Adolescent Psychiatry 57th Annual Meeting, New York, NY. Symposium 22. October 28, 2010
Fanton J, Gleason MM: Psychopharmacology and Preschoolers: A Critical Review of Current Conditions. Child Adolescent Psychiatric Clin N Am 18:753–771, 2009
Fava M, Rush AJ, Alpert JE, et al: Difference in treatment outcome in outpatients with anxious versus nonanxious depression: a STAR*D report. Am J Psychiatry 165(3):342–351, 2008 18172020
FDA Alerts [7/2006]: Increased Risk of Neonatal Persistent Pulmonary Hypertension. Information for Healthcare Professionals: Paroxetine (Marketed as Paxil). Accessed website on February 20, 2013 http://www.fda.gov/DrugsDrugSafetyPostmarketDrugSafetyInformationforPatientsandProviders/ DrugSafetyInformationforHeathcareProfessionals/ucm084319.htm
FDA Safety Communication: Antipsychotic drug labels updated on use during pregnancy and risk of abnormal muscle movements and withdrawal symptoms in newborns. (2-22-2011). Accessed website November 20, 2012 http://www.womensmentalhealth.org/posts/new-fda-warning-on-the-use-of-antipsychotic-medications-in-pregnancy/
Findling RL, Drury SS, Jensen PS, Rappoport JL and the AACAP Committee on Quality Issues: Bukstein OG, Walter HJ, Benson S, Chrisman A, Farchione TR, Hamilton J, Keable H, Kinlan J, Schoettle U, Siegel M, Stock S. Practice Parameter for the Use of Atypical Antipsychotic Medication in Children and Adolescents. J Am Acad Child Adolesc Psychiatry. 2011
Fink M: Catatonia in DSM-IV (editorial). Biol Psychiatry 36(7):431–433, 1994 7811838Flores BH, Kenna H, Keller J, et al: Clinical and biological effects of mifepristone treatment for psychotic
depression. Neuropsychopharmacology 31(3):628–636, 2006 16160710Franklin ME, Sapyta J, Freeman JB, Khanna M, Compton S, Almirall D, Moore P, Choate-Summers M,
Garcia A, Edson AL, Foa EB, March JS. Cognitive Behavior Therapy Augmentation of Pharmacotherapy in Pediatric Obsessive-Compulsive Disorder. JAMA 306(11), September 21, 2011
Frances A, Mack AH, First MB, et al: DMS-IV meets philosophy. J Med Philos 19(3):207–218, 1994 7964208
Garcia AM, Sapyta JJ, Moore PS, Freeman JB, Franklin ME, March JS, Foa EB: Predictor and Moderators for Treatment Outcome in Pediatric Obsessive Compulsive Treatment Study (POTS I). J Am Acad Child Adolesc Psychiatry 49(10):1024–1033, October 2010
Garfield LD, Brown DS, Allaire BT, Ross RE, Nicol GE, Raghavan R: Psychotropic drug use among preschool children in the Medicaid program from 36 states. American Journal of Public Health 105(3):524–529, 2015. Accessed online at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4330829/pdf/AJPH.2014.302258.pdf
PB-Child & Adolescent Dosing.indd 88 05-02-2018 16:02:32
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
89Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Geller DA, March J, and the AACAP Committee on Quality Issues: Walter HJ, Bukstein OG, Benson RS, Chrisman A, Farchione TR, Hamilton J, Keable H, Kinlan J, Schoettle U, Siegel M, Stock S. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Obsessive-Compulsive Disorder. J Am Acad Child Adolesc Psychiatry 51(1), January 2012
Gentile S: Antidepressant Use in Children and Adolescents Diagnosed with Major Depressive Disorder: What Can We Learn from the Published Data? Reviews on Recent Clinical Trials 5:63–75, 2010
Gentile S: Review: Neurodevelopmental Effects of Prenatal Exposure to Psychotropic Medications. Depression and Anxiety 27:675–686, 2010
Gibbons RD, Perraillon MC, Hur K, Conti RM, Valuck RJ, Brent DA: Antidepressant treatment sui-cide attempts and self-inflicted injury in children and adolescents. Pharmacoepidemiol Drug Saf 24(2):208–214, 2015. Accessed online on March 5, 2017 at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4312179/pdf/nihms628193.pdf
Gleason MM, Egger HL, Emslie GJ, Greenhill LL, Kowatch RA, Lieberman AF, Luby JL, Owens J, Scahill LD, Scheeringa MS, Stafford B, Wise B, Zeanah CH: Psychopharmacological Treatment for Very Young Children: Context and Guidelines. J Am Acad Child Adolesc Psychiatry 46:12, December 2007
Guo T, Xiang Y, Xiao L, et al: Measurement-based care versus standard care for major depression: a ran-domized controlled trial with blind raters. Am J Psychiatry 172:1004–1013, 2015
Gurnani T, Ivanov L, Newcorn JH: Pharmacotherapy of aggression in child and adolescent psychiatric disorders. J Child Adolesc Psychopharm 26(1): 65–73, 2016. Accessed online on March 5, 2017 at
Howie LD, Pastor PN, Lukacs SL: Use of medication prescribed for emotional or behavioral difficulties among children aged 6–17 years in the United States, 2011–2012
Insel TR: The NIMH Research Domain Criteria (RDoC) Project: precision medicine for psychiatry. Am J Psychiatry 171(4):395–397, 2014 17548842
Keller J, Schatzberg AF, Maj M: Current issues in the classification of psychotic major depression. Schizophr Bull 33(4):877–885, 2007 10865302
Kessler RC, McGonagle KA, Zhao S, et al: Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Arch Gen Psychiatry 51(1):8–19, 1994 8279933
Kieler H, Artama M, Engeland A, Ericsson O, Furu K, Gissler M, Nielsen RB, Norgaard M, Stephansson O, Valdimarsdottir U, Zoega H, Haglund B: Selective serotonin reuptake inhibitors during pregnancy and risk of persistent pulmonary hypertension in the newborn: population based cohort study from the five Nordic countries. BMJ 344:d8012, 2012
Kodish I, Rockhill C, Varley C: Pharmacotherapy for anxiety disorders in children and adolescents. Dialogues Clin Neurosci 13: 439–452, 2011
Kohlstadt I, Vitiello B: Use of Atypical Antipsychotics in Children: Balancing Safety and Effectiveness. American Family Physician 81(5):585–589, March 1, 2010
Liebowitz MR: Mixed anxiety and depression: should it be included in DSM-IV? J Clin Psychiatry 54:4–7 [discussion 17–20], 1993
Liu HY, Potter MP, Woodworth Y, Yorks D, Petty CR, Wozniak JR, Faroane SV, Biederman J: Pharmacologic Treatment for Pediatric Bipolar Disorder: A Review and Meta-Analysis. J Am Acad Child Adolesc Psychiatry 50(8), August 2011
MACPAC: Medicaid access in brief: children’s use of behavioral health services. Medicaid and CHIP Payment and Access Commission June 2016. Accessed online at https://www.macpac.gov/wp-content/uploads/2016/06/Childrens- access-to-behavioral-health-services.pdf
Madden JM, Lakoma MD, Lynch FL, Rusinak D, et al: Psychotropic medication use among insured children with autism spectrum disorder. J Autism Dev Disord 47:144–154, 2017
Magellan Health, Inc: Clinical Practice Guideline for Patients with Attention Deficit/Hyperactivity Disorder. Revised March 2014
Maj M, Pirozzi R, Magliano L, et al: Phenomenology and prognostic significance of delusions in major depressive disorder: a 10-year prospective follow-up study. J Clin Psychiatry 88:1411–1417, 2008 17915981
Marks I, Lader M: Anxiety states (anxiety neurosis): a review. J Nerv Ment Dis 156(1):3–18, 1973 4570384Mason BJ, Crean R, Goodell V, et al: A proof-of-concept randomized controlled study of gabapen-
tin: effects on cannabis use, withdrawal and executive function deficits in cannabis-dependent adults. Neuropsychophamacology 37(7):1689–1698, 2012 22373942
Mason BJ, Quello S, Goodell V, et al: Gabapentin treatment for alcohol dependence: a randomized clinical trial. JAMA Intern Med 174(l):70–77, 2014 24190578
McPheeters ML, Warren Z, Sathe N, Bruzek JL, Krishnaswami S, Jerome RN, Veenstra-VanderWeele J: A Systematic Review of Medical Treatment for Children With Autism Spectrum Disorders. Pediatrics 127(5), May 2011
Merikangas KR, Calkins ME, Burstein M, et al: Comorbidity of physical and mental disorders in the neu-rodevelopmental genomics cohort study. Pediatrics 135(4):e927–e938, 2015. Accessed online on March 5, 2017 at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4379458/pdf/peds.2014-1444.pdf
PB-Child & Adolescent Dosing.indd 89 05-02-2018 16:02:32
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
90Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Merikangas KR, He JP, Burstein ME et al: Service utilization for lifetime mental disorders in U.S. adoles-cents: results of the National Comorbidity Survey Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry 50(1):32–45, 2011. Accessed on March 5, 2017 at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4408275/
Meyers SM, Plauche Johnson C, and the Council on Children With Disabilities: Management of Children With Autism Spectrum Disorders. Pediatrics; 120(5):1162–1182, 2007. Reaffirmed September 2010
Michelson D, Wernicke J, Heiligenstein J, et al: LY 139603 (tomoxetine) a new, non-dopaminergic inter-vention for ADHD. Poster presented at the 41st annual meeting of the National Institute of Mental Health New Drug Clinical Drug Evaluation Unit, Phoenix, AZ, May 2001, Poster Session 11–55
Morris J, Stone G: Children and Psychotropic medication: A Cautionary Note. Journal of Marital and Family Therapy 37(3), 299–306, July 2011
Murphy GM, Kremer C, Rodrigues H, Schatzberg AF; Mitrazapine versus Paroxetine Study Group: The apolipoprotein E epsilon4 allele and antidepressant efficacy in cognitively intact elderly depressed patients. Biol Psychiatry 54(7):665–673, 2003a 14512205
Murphy GM Jr, Kremer C, Rodrigues HE, Schatzberg AF: Pharmacogenetics of antidepressant medication intolerance. Am J Psychiatry 160(10):1830–1835, 2003b 14514498
Murphy GM Jr, Hollander SB, Rodrigues HE, et al: Effects of the serotonin transporter gene promoter polymorphism on mirtazapine and paroxetine efficacy and adverse events in geriatric major depression. Arch Gen Psychiatry 61(11):1163–1169, 2004 15520364
Myers JK, Weissman MM, Tischler GL, et al: Six-month prevalence of psychiatric disorders in three com-munities 1980 to 1982. Arch Gen Psychiatry 41(10):959–967, 1984 6332591
Nathan PE: DSM-IV: empirical, accessible, not yet ideal (editorial). J Clin Psychol 50(1):103–110, 1994 8150989
National Institute of Mental Health. Any disorder among children. Accessed March 5, 2017 at https://www.nimh.nih.gov/health/statistics/prevalence/any-disorder-among-children.shtml.
Ohayon MM, Schatzberg AF: Prevalence of depressive episodes with psychotic features in the general population. Am J Psychiatry 159(11):1855–1861, 2002 12411219
Ohayon MM, Schatzberg AF: Using chronic pain to predict depressive morbidity in the general population. Arch Gen Psychiatry 60(1):39–47, 2003 12511171
Ohayon MM, Schatzberg AF: Chronic pain and major depressive disorder in the general population. J Psychiatr Res 44(7):454–461, 2010 20149391
Olfson M, Blanco C, Liu L, Moreno C, Laje G: National Trends in the Outpatient Treatment of Children and Adolescents With Antipsychotic Drugs. Arch Gen Psychiatry 63, June 2006
Olfson M, Druss BG, Marcus SC: Trends in mental health care among children and adolescents. N Engl J Med 372(21):2029–2038, 2015. Accessed online on March 5, 2017 at http://www.nejm.org/doi/pdf/10.1056/NEJMsa1413512.
Pagsberg AK, Tarp S, Glintborg D, et al: Acute antipsychotic treatment of children and adolescents with schizophrenia-spectrum disorders: a systematic review and network meta-analysis. J Amer Acad Child Adolesc Psychiatry 56(3):191–202, 2017
Paroxetine Pregnancy and Breastfeeding Warnings: Accessed website on February 20, 2013 http://www.drugs.com/pregnancy/paroxetine.html?printable=1
Pidano AE, Honigfeld L: Pediatric Psychopharmacology: Context, Model Programs, and Considerations for Care. Psychiatric Services 63(9):929–934, September 1, 2012.
Plauche Johnson C, Meyers SM and the Council on Children with Disabilities: Identification and Evaluation of Children with Autism Spectrum Disorders. Pediatrics 120(5):1183–1215, 2007. Reaffirmed September 2010
Policy Lab. Center to Bridge Research, Practice and Policy: Psychotropic Medication Use among Children in Foster Care: A National and State-Level Perspective. Research-At-A-Glance Fall 2012. Accessed on September 5, 2012 http://policylab.us/images/pdf/hsr_lpager_final.pdf
Pope HG Jr, Lipinski JF Jr: Diagnosis in schizophrenia and manic-depressive illness: a reassessment of the specificity of ‘schizophrenic’ symptoms in the light of current research. Arch Gen Psychiatry 35(7):811–828, 1978 354552
Primary Care Providers’ Role in Mental Health: A Healthcare Reform Issue Brief. Judge David L. Bazelon Center for Mental Health Law. Accessed website on September 5, 2012 http://www.bazelon.org/LinkClick.aspx?fileticket=CBTKUhx TIvw%3D&tabid=220
Raghavan R, Brown DS, Allaire B, Ross RE, Landsverk J: Associations between magnitude of child mal-treatment and Medicaid expenditures for psychotropic medications. Psychiatric Services 67(8):916–919, 2016
Raskind MA, Peterson K, Williams T, et al: A trial of prazosin for combat trauma PTSD with nightmares in active-duty soldiers returned from Iraq and Afghanistan. Am J Psychiatry 170(9):1003–1010, 2013 23846759
Regier DA, Boyd JH, Burke JD Jr, et al: One-month prevalence of mental disorders in the United States: based on five Epidemiologic Catchment Area sites. Arch Gen Psychiatry 45(11):977–986, 1988 3263101
PB-Child & Adolescent Dosing.indd 90 05-02-2018 16:02:32
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
91Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Regier DA, Narrow WE, Kuhl EA, Kupfer DJ: The conceptual development of DSM-V. Am J Psychiatry l66(6):645–650, 2009 19487400
Rosato NS, Correll CU, Pappadopulos E, Chait A, Crustal S, Jensen PS on behalf of the Treatment of Maladaptive Aggression in Youth Steering Committee. Pediatrics Volume 129, Number 6, June 2012
Robins LN, Helzer JE, Weissman MM, et al: Lifetime prevalence of specific psychiatric disorders in three sites. Arch Gen Psychiatry 41(10):949–958, 1984 6332590
Rush AJ, Weissenburger JE: Melancholic symptom features and DSM-IV. Am J Psychiatry 151(4):489–498, 1994 8147445
Sadler JZ, Hulgus YF, Agich GJ: On values in recent American psychiatric classification. J Med Philos 19(3):26l–277, 1994 7964211
Sakolsky D, Birmaher B. Developmentally Informed Pharmacotherapy for Child and Adolescent Depressive Disorders. Child Adolesc Psychiatric Clin N Am 21:313–325, 2012
SAMHSA 2013: Integrating behavioral health and primary care for children and youth: concepts and strat-egies. Accessed online at http://www.integration.samhsa.gov/integrated-care-models/13_June_CIHS_Integrated_Care_System_ for_Children_final.pdf
Schatzberg AF: Classification of affective disorders, in The Brain, Biochemistry, and Behavior (Proceedings of the Sixth Arnold O. Beckman Conference in Clinical Chemistry). Edited by Habig RL. Washington, DC, American Association for Clinical Chemistry 29–46, 1984
Schatzberg AF, Rothschild AJ: Psychotic (delusional) major depression: should it be included as a distinct syndrome in DSM-IV? (also see comments). Am J Psychiatry 149(6):733–745, 1992 1590491
Schatzberg AF, Kremer C, Rodrigues H, et al: Double-blind, randomized comparison of mirtazapine vs paroxetine in elderly depressed patients. Am J Geriatr Psychiatry 10(5):541–550, 2002 12213688
Schatzberg AF, Cole JO, DeBattista C: Manual of Clinical Psychopharmacology. (7th ed.). Arlington VA: American Psychiatric Publishing, Inc. 2010
Schmid I, Burcu M, Zito JM: Medicaid prior authorization policies for pediatric use of antipsychotic medi-cations. JAMA 313(9):966–967, 2015. Accessed online on March 5, 2017 at Medicaid prior authorization policies for pediatric use of antipsychotic medications
Scott K and Lewis C: Using measurement-based care to enhance any treatment. Cogn Behav Pract 49–59, 2015
Serretti A, Cusin C, Rausch JL, et al: Pooling pharmacogenetic studies on the serotonin transporter: a mega-analysis. Psychiatry Res l45(l):61–65, 2006 17069894
Sheehan DV, Sheehan KH: The classification of anxiety and hysterical states, Part I: historical review and empirical delineation. J Clin Psychopharmacol 2(4):235–244, 1982a 6749908
Sheehan DV, Sheehan KH: The classification of anxiety and hysterical states, Part II: toward a more heu-ristic classification. J Clin Psychopharmacol 2(6):386–393, 1982b 7174861
Seida JC, Schouten JR, Boylan K, Newton AS, Mousavi SS, Beaith A, Vandermeer B, Dryden DM, Carrey N: Antipsychotics for Children and Young Adults: A comparative Effectiveness Review. Pediatrics 129:e771, 2012
Sharma AN, Arango C, Coghill D, et al: BAP position statement: Off-label prescribing of psychotropic medication to children and adolescents. J of Psychopharm 30(5):416–421, 2016. Accessed online on March 5, 2017 at http://journals.sagepub.com/doi/pdf/10.1177/0269881116636107
Singh MK, Chang K: The neural effects of psychotropic medications in children and adolescents. Child Adolesc Psychiatr Clin N Am 21(4):753–771, 2012. Accessed online on March 5, 2017 at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3590023/pdf/nihms-398562.pdf
Smeraldi E, Zanardi R, Benedetti F, et al: Polymorphism within the promoter of the serotonin transporter gene and antidepressant efficacy of fluvoxamine. Mol Psychiatry 3(6):508–511, 1998 9857976
Solchany J: Psychotropic Medication and Children in Foster Care: Tips for Advocates and Judges. Practice and Policy Brief, American Bar Association Center on Children and the Law. October 2011
Stein BD, Leckman-Westin E, Okeke E, et al: The effects of prior authorization policies on Medicaid-enrolled children’s use of antipsychotic medications: evidence from two mid-Atlantic states. J Child Adolesc Psychopharm 374–381, 2014; Accessed online at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4162428/pdf/cap.2014.0008.pdf
Steiner H, Lemsing L and the Work Group on Quality Issues: Arnold V, Beitchman J, Benson S, Bernet W, Bukstein O, Kinlan J, Rue D, Shaw J, Schoettle U, Stock S, Walter H. Practice Parameter for the Assessment and Treatment of Children and Adolescents With Oppositional Defiant Disorders. J Am Acad Child Adolesc Psychiatry, 46:1, January 2007
Strawn JR, Dobson ET, Giles LL: Primary pediatric care psychopharmacology: focus on medication s for ADHD, depression, and anxiety. Curr Probl Pediatr Adolesc Health Care 1–12, 2016. Strawn JR, Keeshin BR, DelBello MP, Geracioti TD, Putnam FW. Psychopharmacological Treatment of Posttraumatic Stress Disorder in Children and Adolescents: A Review. J Clin Psychiatry 71:7, July 2010
Stein MB, Fyer AJ, Davidson JR, et al: Fluvoxamine treatment of social phobia (social anxiety disorder): a double-blind, placebo-controlled study. Am J Psychiatry 156(5):756–760, 1999 10327910
PB-Child & Adolescent Dosing.indd 91 05-02-2018 16:02:32
NOT FOR R
EPRINT
Dosing and Monitoring: Children and Adolescents
92Hirsch and Stephen
PsychoPharmacology Bulletin: Vol. 48 · No. 2
Texas Department of Family and Protective Services and the University of Texas at Austin College of Pharmacy: Psychotropic Medication Utilization Parameters for Foster Children. December 2010
Vanderwerker L, Akincigil A, Olfson M, Gerhard T, Neese-Todd S, Crystal S: Foster care, externalizing dis-orders, and antipsychotic use among Medicain-enrolled youths. Psychiatric Services 65(10):1281–1284, 2014. Accessed online on March 5, 2017 at Foster care, externalizing disorders, and antipsychotic use among Medicain-enrolled youths
Vega CP, Anderson P: SSRIs Not Recommended for Autism in Children or Adults Based on Current Evidence. Accessed website on February 14, 2012 http://www.medscape.org/viewarticle/726999_print
Walkup J and the Work Group on Quality Issues: Bernet W, Bukstein O, Walter H, Arnold V, Benson RS, Beitchman J, Chrisman A, Farchione TR, Hamilton J, Keable H, Kinlan J, McClellan J, Schoettle U, Shaw J, Siegel M, Stock S. Practice Parameter on the Use of Psychotropic Medication in Children and Adolescents. J Am Acad Child Adolesc Psychiatry, 48:9, September 2009
Warren Z, McPheeters ML, Sathe N, Foss-Feig JH, Glassner A, Veenstra-Vander-Weele J: A Systematic Review of Early Intensive Intervention for Autism Spectrum Disorders. Pediatrics 127( 5), May 2011
Williams K, Wheeler DM, Silove N, Hazell P: Selective serotonin reuptake inhibitors (SSRIs) for autism spectrum disorder (ASD) (Review). Cochrane Database Syst Rev 4(8), 2010
Woody G, Schuckit M, Weinrieb R, Yu E: A review of the substance use disorders section of the DSM-IV. Psychiatr Clin North Am 16(l):21–32, 1993 8456046
Zanarini MC, Schulz SC, Detke HC, et al: A dose comparison of olanzapine for the treatment of border-line personality disorder: a 12-week randomized, doubleblind, placebo-controlled study. J Clin Psychiatry 72(10):1353–1362, 2011 21535995
Zisook S, Corruble E, Duan N, et al: The bereavement exclusion and DSM-5. Depress Anxiety 29(5): 425–443, 2012 22495967
PB-Child & Adolescent Dosing.indd 92 05-02-2018 16:02:32
NOT FOR R
EPRINT