dorzolamide and corneal recovery from edema in patients with glaucoma or ocular hypertension
TRANSCRIPT

Dorzolamide and Corneal Recovery FromEdema in Patients With Glaucoma
or Ocular Hypertension
CLAUDE J. GIASSON, OD, PHD, TUAN QUYNH TRAM NGUYEN, MD,HELENE M. BOISJOLY, MD, MPH, MARK R. LESK, MSC, MD, MARCEL AMYOT, MD,
AND MANON CHAREST, RT
● PURPOSE: To investigate whether dorzolamide alterscorneal hydration control in patients with glaucoma orocular hypertension.● METHODS: Pachymetry, tonometry, and endothelialcell density were measured by a masked observer in 19subjects with bilateral glaucoma or ocular hypertension.They were treated with 2% dorzolamide in one eye, andwith saline in the other, before wearing contact lensesunder patched eyes. Corneal thickness, measured each30 minutes up to 4.5 hours after contact lens removal,enabled estimation of percentage recovery per hour andtime for 95% of corneal thickness recovery for both eyes.Seven patients repeated this test after 1 year of dorzol-amide use, and their results were compared with those ofthe preceding year.● RESULTS: After induction of hypoxic corneal edema,there was no significant difference between paired cor-neas in swelling levels (60.0 6 11.8 and 59.8 6 12.9mm) (P 5 .94), time to 95% recovery (440.6 6 255.8and 445.4 6 186.7 minutes) (P 5 .93), and percentagerecovery per hour (38.1% 6 10.9% and 36.1% 6 9.6%)(P 5 .40). Subjects followed up after 1 year of dorzol-amide use did not differ significantly in values of endo-thelial cell density, percentage recovery per hour, or timeto 95% recovery from those obtained a year before. Onesubject developed persistent corneal edema after hisstress test in the eye treated with dorzolamide.● CONCLUSION: There is no significant difference in therecovery from induced corneal edema after either ashort-term or 1-year use of dorzolamide in patients with
glaucoma or ocular hypertension with a normal cornealendothelium. One patient had persistent corneal edemaafter the stress test was performed on the dorzolamide-treated eye. (Am J Ophthalmol 2000;129:144–150.© 2000 by Elsevier Science Inc. All rights reserved.)
C ARBONIC ANHYDRASE (CA), THE ENZYME THAT
catalyzes the reversible hydration of carbon diox-ide, instantaneously converts carbon dioxide to
bicarbonate (HCO3). This anion is an important counte-rion to Na1 in secreting tissues,1 including ciliary epithe-lium and corneal endothelium.2–4 The human eye containsmany isoenzymes of carbonic anhydrase: cytosolic CAI andCAII are present in the corneal endothelium and CAII isobserved in nonpigmented ciliary epithelium.5 CAIV, themembrane-bound isoenzyme presumably involved in fluidtransport,1 is present in rat and mouse corneal endotheli-um,6,7 as well as in rabbit ciliary epithelium.8 CAIV isthought to be present in both of these tissues in the humaneye.9
Acetazolamide, a systemic carbonic anhydrase inhibitor,has been used since 1954 to reduce intraocular pressure inpatients with glaucoma.10 Carbonic anhydrase inhibitorsdiminish the secreted volume of aqueous humor presum-ably by decreasing the concentration of HCO32 ions. Invivo, oral administration of acetazolamide increases cor-neal thickness only in patients with abnormal cornealendothelium.11 However, the many undesirable systemiceffects associated with this route of administration areresponsible for sustained interest of a few pioneers indeveloping varieties of carbonic anhydrase inhibitors thatcould be used topically. Early attempts to deliver acetazol-amide topically or by subconjunctival injection resulted incorneal edema without any reduction in intraocular pres-sure12 because of poor penetration into the eye.1 Dorzol-amide, the first topical carbonic anhydrase inhibitorcommercially available, accumulates within the cornea,allowing a sustained delivery to the anterior uvea mainlythrough scleral and conjunctival routes.1,13,14 However,
Accepted for publication July 16, 1999.From the Guy-Bernier Research Center, Ophthalmology Research
Unit, Hopital Maisonneuve-Rosemont (Drs Giasson, Nguyen, Boisjoly,Lesk, and Amyot and Ms Charest), School of Optometry, Universite deMontreal (Dr Giasson), and Department of Ophthalmology, Faculty ofMedicine, Universite de Montreal (Drs Nguyen, Boisjoly, Lesk, andAmyot), Montreal, Quebec, Canada.
Reprint requests to Helene M. Boisjoly, MD, MPH, Maisonneuve-Rosemont Hospital, 5689 Boul Rosemont, Montreal, Quebec, CanadaH1T 2H1; Fax: (514)-252-3821; e-mail: [email protected]
© 2000 BY ELSEVIER SCIENCE INC. ALL RIGHTS RESERVED.144 0002-9394/00/$20.00PII S0002-9394(99)00274-3

increased tissue concentrations of carbonic anhydrase in-hibitors near corneal endothelium could inhibit itsHCO32-dependent fluid transport and reduce its capacityto maintain the cornea dehydrated. Previously, in vitroexperiments demonstrated a reduced rate of fluid trans-ported by bovine endothelial cells in culture and swellingof a mounted rabbit cornea when the endothelial superfu-sate of these preparations contained carbonic anhydraseinhibitors.15,16
In living humans, the effects of dorzolamide on cornealstructure and function are less clear. Corneal decompen-sation was reported in nine patients with compromisedcorneas using dorzolamide.17 Corneas of eyes treated withdorzolamide were reported to be thicker than those ofuntreated ones,18 to become slightly thicker,19 or to main-tain the same thickness after treatment with dorzol-amide.20 Finally, depending on the study, endothelial celldensity of patients treated with dorzolamide either did notchange or decreased after treatment.20,21
Nineteen normal subjects displayed similar kinetics ofcorneal deswelling whether their eyes had been exposed todorzolamide or to saline.22 However, compared with nor-mal patients, those with glaucoma have reduced endothe-lial cell density23 and, therefore, may be at a higher risk ofcorneal decompensation after prolonged use of this car-bonic anhydrase inhibitor. The aim of this study was to testif dorzolamide reduces rates of corneal deswelling inpatients with glaucoma or ocular hypertension.
PATIENTS AND METHODS
THIS RESEARCH PROJECT, APPROVED BY THE INSTITU-
tional experimentation committee on humans, adhered tothe tenets of the Declaration of Helsinki. Informed con-sent was obtained from each subject after the experimentswere fully explained. Nineteen eligible patients, referredfrom glaucoma specialists, participated in the initial stage.Seven of those patients consented to be seen on follow-up1 year later. All subjects were white, except for one blackwoman seen in the initial study; their other characteristicsand distribution by types of glaucoma or ocular hyperten-sion are summarized in Tables 1 and 2. Patients wereexcluded for the following reasons: uveitis, ocular surgery,trauma, or laser iridotomy within a year of their initialvisit; history of diabetes mellitus24; or mean endothelialcell density below 1,000 cells/mm2.
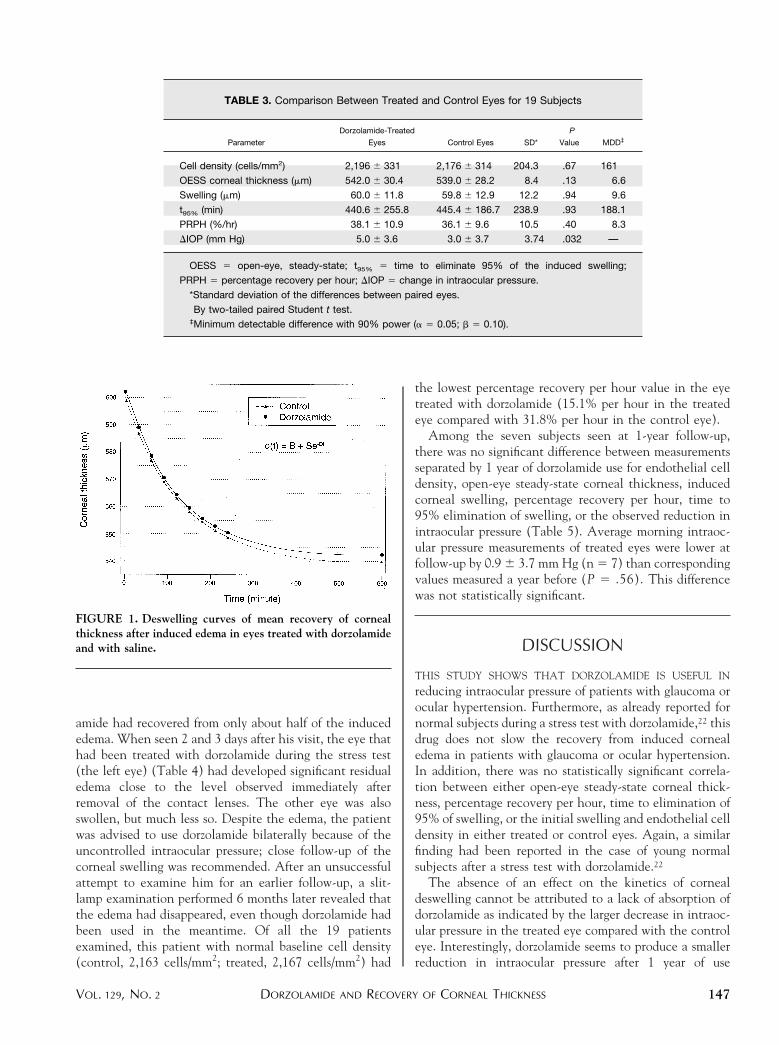
In both stages of the study, hypoxic corneal edema wasinduced in each subject by applying a thick contact lens(KF3M, 38% water; diameter, 14.0 mm; base curve, 8.40mm; 20.50 diopter; 0.22 mm thick; Blanchard, Sher-brooke, Quebec, Canada) over eyes treated 1 hour beforeon one side with dorzolamide and on the other with saline.The eyes were then patched for 2 hours, at the end ofwhich contact lenses were removed to perform pachymetryand tonometry. Corneal thickness and intraocular pressurewere then subsequently measured every 30 and 60 minutes,respectively, for 4.5 hours. The eyes were anesthetized withtopical proparacaine hydrochloride (Allergan, Markham,Ontario) when both intraocular pressure and cornealthickness were measured. Most often, 30 minutes afterboth procedures had been performed, corneal esthesia hadnot fully recovered, and further instillation of anestheticsbefore pachymetry was unnecessary. The observer takingmeasurements was masked as to which eye had receiveddorzolamide. The recovery in corneal thickness (q) overtime was modeled by means of a single exponential25,26:
q~t! 5 B 1 Se2Dt
where B is the open-eye steady-state corneal thickness; S,the initial corneal swelling at lens removal; and D, thedeswelling rate. Nonlinear regression of an individualdataset from each patient was obtained with a statisticalsoftware (Plotit 1.6; Scientific Enterprises Programming,Haslett, Michigan), considering that the cornea had re-covered its morning thickness 10 hours after removal ofthe contact lens. Fits were done both on a datasetimmediately after contact lens removal and on a truncatedset in which the initial 40 minutes after lens removal hadbeen eliminated. A larger proportion of the variance wasexplained by fits that contained all data points comparedwith the truncated datasets. Therefore, fits using all datapoints were used in this study.
Once D is obtained, it is possible to calculate thepercentage recovery per hour of corneal thickness (PRPH)and the time required by the cornea to eliminate 95% ofthe induced swelling (t95%)25,26:
PRPH 5 ~1 2 e260 D! 3 100
t95% 5 @ 2 ln ~0.05!#/D
Every subject was seen for slit-lamp examination 2 or 3days after the stress test. Except for one subject (seeResults), all corneas appeared normal then.
Patients were taking their usual medication, withoutdorzolamide. Those who had initiated therapy with dorzo-lamide had a washout period of 2 weeks. Subjects wereseen in the afternoon of the first day for measurement ofcentral corneal thickness by ultrasonic pachymetry (Al-
TABLE 1. Characteristics of the Subjects
Characteristic Initial Study Follow-up Study
Sample size (n) 19 7
Mean age (yrs) (range) 68 (47–83) 65 (48–84)
Gender (no. female/male) 9/10 2/5
DORZOLAMIDE AND RECOVERY OF CORNEAL THICKNESSVOL. 129, NO. 2 145

con, Fort Worth, Texas) and intraocular pressure byGoldmann applanation tonometry. The endothelium of acentral corneal area of each patient was photographed andanalyzed with a noncontact specular microscope (KonanNONCON-ROBO SP8000; Bio-Optics, Arlington, Mas-sachusetts) by indicating the center of about 100 adjacentcells within a field. Dorzolamide 2% (Trusopt; Merck andCo, Inc, West Point, Pennsylvania) was applied on oneeye, randomly chosen at patient dismissal, and on the sameeye on the following morning while saline was instilled onthe other eye. On the following morning, a stress test wasinitiated to monitor the resolution of corneal edema.Reduction in intraocular pressure was the difference be-tween the intraocular pressure measured at the first visitbefore any intake of dorzolamide and the one measured aday later at the same time in the afternoon. Patients wereexamined 2 or 3 days after this test and, when required,dorzolamide was added to their treatment.
Of the patients originally enrolled, only seven could beevaluated again a year later for reasons listed in Table 2.During that year, these patients had used dorzolamide inboth of their eyes. On the afternoon preceding their visit,patients were instructed to continue taking their usualmedication except for dorzolamide. After endothelial mor-phometry, tonometry, and pachymetry, one drop of dorzo-lamide and one drop of saline were instilled on the sameeyes as a year before. Again, a stress test was initiated 1hour after instillation of the drops. Coefficients describingthe kinetics of corneal recovery (B, S, PRPH, and t95%)obtained from each patient were compared with those ofthe previous year. The maximal reduction in intraocularpressure compared with the morning value was also calcu-lated for the initial and follow-up visits for the group ofpatients seen a year later.
Coefficients B, S, PRPH, and t95% and reductions inintraocular pressure of treated and control eyes from eachsubject were tested for statistical significance with paired
two-tailed t tests in the initial study. At follow-up, a similarmethod was used to compare corresponding results ob-tained a year apart in treated eyes. We used linearregression analysis (Systat 5.2.1; Systat Inc, Evanston,Illinois) to find if there was an association between any ofthese coefficients and endothelial cell count.
RESULTS
TABLE 3 SUMMARIZES THE RESULTS OBTAINED FOR 19 SUB-
jects in the initial study. Baseline endothelial cell densitiesof the eyes treated with dorzolamide and with saline werenot significantly different. Mean deswelling curves, that is,obtained by averaging coefficients of corneal thicknessrecovery, are shown in Figure 1 for control and treatedeyes. No significant difference was observed in the open-eye steady-state corneal thickness between treated andcontrol eyes, or in the swelling induced after instillation ofdorzolamide or of saline. The differences in time toeliminate 95% of swelling or in percentage recovery perhour between treated and control eyes were not signifi-cantly different. When percentage recovery per hour, timeto eliminate 95% of swelling, initial swelling, and their logwere plotted as a function of endothelial cell density, nodefinite pattern was observed for treated or control eyes(not shown). Linear regressions between these three vari-ables and endothelial cell density were not significantlydifferent. Intraocular pressure before initiation of treat-ment with dorzolamide was 22.4 6 5.4 mm Hg and 20.9 63.4 mm Hg (P 5 .28) in treated and control eyes,respectively. The reduction in intraocular pressure com-pared with the measurement done 24 hours before anyapplication of dorzolamide was significantly larger in thetreated eye compared with the control eye.
One patient still had some edema at the end of his stresstest; corneal thickness on the side treated with dorzol-
TABLE 2. Distribution of Subjects by Diagnosis
Diagnosis Initial Study Follow-up Study Lost to Follow-up
Ocular hypertension* 8 3 5†
Primary open-angle glaucoma 7 1 6‡
Angle-closure glaucoma 1 1 0
Pseudoexfoliative glaucoma 1 1 0
Pigmentary glaucoma 1 1 0
Pseudophakia 1 0 1
*Mean intraocular pressure between 24 and 30 mm Hg without any visual field defect or optic disk
cupping.†Three subjects had used dorzolamide only during the initial study, one discontinued it because of
an allergic reaction, and one declined the follow-up visit.‡Two subjects had serious unrelated health conditions that precluded testing (cancer and heart
attack), one had stopped taking dorzolamide because of suspected allergic reaction, one stopped for
an unspecified reason, and two could not be reached.
AMERICAN JOURNAL OF OPHTHALMOLOGY146 FEBRUARY 2000
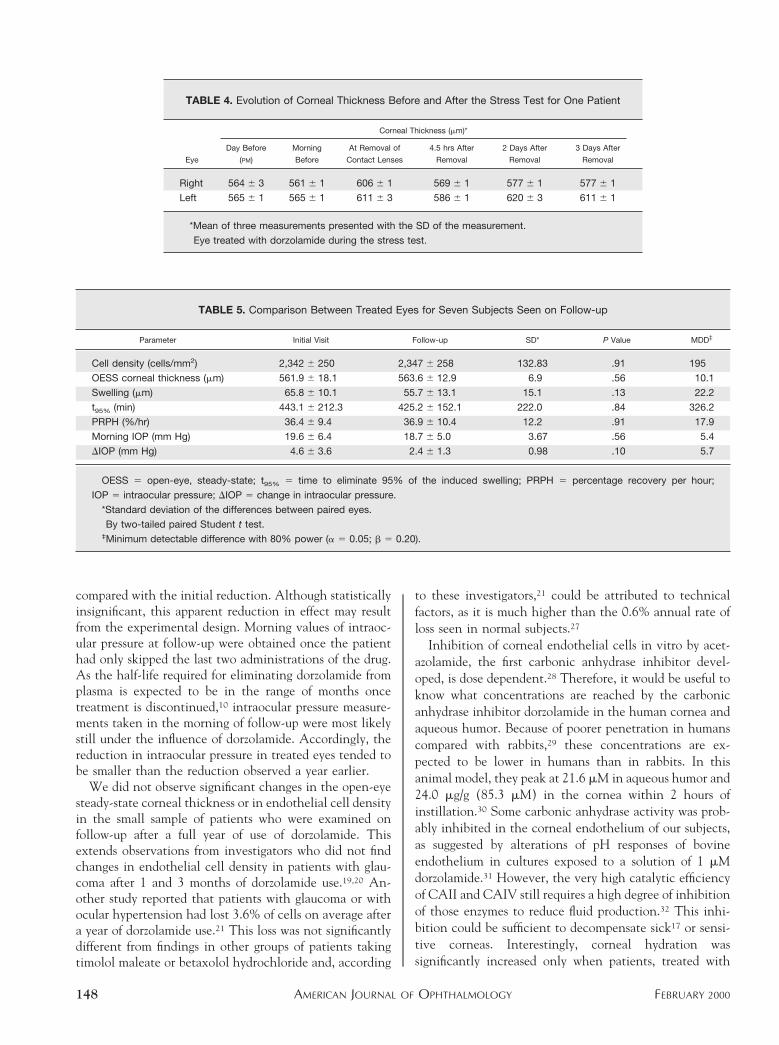
amide had recovered from only about half of the inducededema. When seen 2 and 3 days after his visit, the eye thathad been treated with dorzolamide during the stress test(the left eye) (Table 4) had developed significant residualedema close to the level observed immediately afterremoval of the contact lenses. The other eye was alsoswollen, but much less so. Despite the edema, the patientwas advised to use dorzolamide bilaterally because of theuncontrolled intraocular pressure; close follow-up of thecorneal swelling was recommended. After an unsuccessfulattempt to examine him for an earlier follow-up, a slit-lamp examination performed 6 months later revealed thatthe edema had disappeared, even though dorzolamide hadbeen used in the meantime. Of all the 19 patientsexamined, this patient with normal baseline cell density(control, 2,163 cells/mm2; treated, 2,167 cells/mm2) had
the lowest percentage recovery per hour value in the eyetreated with dorzolamide (15.1% per hour in the treatedeye compared with 31.8% per hour in the control eye).
Among the seven subjects seen at 1-year follow-up,there was no significant difference between measurementsseparated by 1 year of dorzolamide use for endothelial celldensity, open-eye steady-state corneal thickness, inducedcorneal swelling, percentage recovery per hour, time to95% elimination of swelling, or the observed reduction inintraocular pressure (Table 5). Average morning intraoc-ular pressure measurements of treated eyes were lower atfollow-up by 0.9 6 3.7 mm Hg (n 5 7) than correspondingvalues measured a year before (P 5 .56). This differencewas not statistically significant.
DISCUSSION
THIS STUDY SHOWS THAT DORZOLAMIDE IS USEFUL IN
reducing intraocular pressure of patients with glaucoma orocular hypertension. Furthermore, as already reported fornormal subjects during a stress test with dorzolamide,22 thisdrug does not slow the recovery from induced cornealedema in patients with glaucoma or ocular hypertension.In addition, there was no statistically significant correla-tion between either open-eye steady-state corneal thick-ness, percentage recovery per hour, time to elimination of95% of swelling, or the initial swelling and endothelial celldensity in either treated or control eyes. Again, a similarfinding had been reported in the case of young normalsubjects after a stress test with dorzolamide.22
The absence of an effect on the kinetics of cornealdeswelling cannot be attributed to a lack of absorption ofdorzolamide as indicated by the larger decrease in intraoc-ular pressure in the treated eye compared with the controleye. Interestingly, dorzolamide seems to produce a smallerreduction in intraocular pressure after 1 year of use
FIGURE 1. Deswelling curves of mean recovery of cornealthickness after induced edema in eyes treated with dorzolamideand with saline.
TABLE 3. Comparison Between Treated and Control Eyes for 19 Subjects
Parameter
Dorzolamide-Treated
Eyes Control Eyes SD*
P
Value† MDD‡
Cell density (cells/mm2) 2,196 6 331 2,176 6 314 204.3 .67 161
OESS corneal thickness (mm) 542.0 6 30.4 539.0 6 28.2 8.4 .13 6.6
Swelling (mm) 60.0 6 11.8 59.8 6 12.9 12.2 .94 9.6
t95% (min) 440.6 6 255.8 445.4 6 186.7 238.9 .93 188.1
PRPH (%/hr) 38.1 6 10.9 36.1 6 9.6 10.5 .40 8.3
DIOP (mm Hg) 5.0 6 3.6 3.0 6 3.7 3.74 .032 —
OESS 5 open-eye, steady-state; t95% 5 time to eliminate 95% of the induced swelling;
PRPH 5 percentage recovery per hour; DIOP 5 change in intraocular pressure.
*Standard deviation of the differences between paired eyes.†By two-tailed paired Student t test.‡Minimum detectable difference with 90% power (a 5 0.05; b 5 0.10).
DORZOLAMIDE AND RECOVERY OF CORNEAL THICKNESSVOL. 129, NO. 2 147
compared with the initial reduction. Although statisticallyinsignificant, this apparent reduction in effect may resultfrom the experimental design. Morning values of intraoc-ular pressure at follow-up were obtained once the patienthad only skipped the last two administrations of the drug.As the half-life required for eliminating dorzolamide fromplasma is expected to be in the range of months oncetreatment is discontinued,10 intraocular pressure measure-ments taken in the morning of follow-up were most likelystill under the influence of dorzolamide. Accordingly, thereduction in intraocular pressure in treated eyes tended tobe smaller than the reduction observed a year earlier.
We did not observe significant changes in the open-eyesteady-state corneal thickness or in endothelial cell densityin the small sample of patients who were examined onfollow-up after a full year of use of dorzolamide. Thisextends observations from investigators who did not findchanges in endothelial cell density in patients with glau-coma after 1 and 3 months of dorzolamide use.19,20 An-other study reported that patients with glaucoma or withocular hypertension had lost 3.6% of cells on average aftera year of dorzolamide use.21 This loss was not significantlydifferent from findings in other groups of patients takingtimolol maleate or betaxolol hydrochloride and, according
to these investigators,21 could be attributed to technicalfactors, as it is much higher than the 0.6% annual rate ofloss seen in normal subjects.27
Inhibition of corneal endothelial cells in vitro by acet-azolamide, the first carbonic anhydrase inhibitor devel-oped, is dose dependent.28 Therefore, it would be useful toknow what concentrations are reached by the carbonicanhydrase inhibitor dorzolamide in the human cornea andaqueous humor. Because of poorer penetration in humanscompared with rabbits,29 these concentrations are ex-pected to be lower in humans than in rabbits. In thisanimal model, they peak at 21.6 mM in aqueous humor and24.0 mg/g (85.3 mM) in the cornea within 2 hours ofinstillation.30 Some carbonic anhydrase activity was prob-ably inhibited in the corneal endothelium of our subjects,as suggested by alterations of pH responses of bovineendothelium in cultures exposed to a solution of 1 mMdorzolamide.31 However, the very high catalytic efficiencyof CAII and CAIV still requires a high degree of inhibitionof those enzymes to reduce fluid production.32 This inhi-bition could be sufficient to decompensate sick17 or sensi-tive corneas. Interestingly, corneal hydration wassignificantly increased only when patients, treated with
TABLE 4. Evolution of Corneal Thickness Before and After the Stress Test for One Patient
Eye
Corneal Thickness (mm)*
Day Before
(PM)
Morning
Before
At Removal of
Contact Lenses
4.5 hrs After
Removal
2 Days After
Removal
3 Days After
Removal
Right 564 6 3 561 6 1 606 6 1 569 6 1 577 6 1 577 6 1
Left† 565 6 1 565 6 1 611 6 3 586 6 1 620 6 3 611 6 1
*Mean of three measurements presented with the SD of the measurement.†Eye treated with dorzolamide during the stress test.
TABLE 5. Comparison Between Treated Eyes for Seven Subjects Seen on Follow-up
Parameter Initial Visit Follow-up SD* P Value† MDD‡
Cell density (cells/mm2) 2,342 6 250 2,347 6 258 132.83 .91 195
OESS corneal thickness (mm) 561.9 6 18.1 563.6 6 12.9 6.9 .56 10.1
Swelling (mm) 65.8 6 10.1 55.7 6 13.1 15.1 .13 22.2
t95% (min) 443.1 6 212.3 425.2 6 152.1 222.0 .84 326.2
PRPH (%/hr) 36.4 6 9.4 36.9 6 10.4 12.2 .91 17.9
Morning IOP (mm Hg) 19.6 6 6.4 18.7 6 5.0 3.67 .56 5.4
DIOP (mm Hg) 4.6 6 3.6 2.4 6 1.3 0.98 .10 5.7
OESS 5 open-eye, steady-state; t95% 5 time to eliminate 95% of the induced swelling; PRPH 5 percentage recovery per hour;
IOP 5 intraocular pressure; DIOP 5 change in intraocular pressure.
*Standard deviation of the differences between paired eyes.†By two-tailed paired Student t test.‡Minimum detectable difference with 80% power (a 5 0.05; b 5 0.20).
AMERICAN JOURNAL OF OPHTHALMOLOGY148 FEBRUARY 2000

systemic acetazolamide after their cataract surgery, hadendothelial guttae.11
A minimum value of percentage recovery per hour of17.1% per hour has been identified as the minimum valuebelow which the cornea could not regain its open-eyesteady-state corneal thickness.26 The patient who hadmarked swelling after his stress test had a percentagerecovery per hour value under that critical estimate on theside treated with dorzolamide. Not only did his cornea failto recover its pretest thickness on this side, but it alsodeveloped marked edema during the following days. Thisevent suggests that this stress test, combined with inhibi-tion of carbonic anhydrase activity by dorzolamide, wasalmost sufficient for this patient to develop corneal decom-pensation. However, his cornea had resumed a normalappearance after 6 months despite uninterrupted use ofdorzolamide, suggesting that the stress test was the maintriggering factor. Still, dorzolamide should be used withcaution in patients with corneal edema.
In patients with glaucoma or ocular hypertension withnormal endothelium, and without baseline corneal edema,inhibition of carbonic anhydrase with dorzolamide doesnot seem to affect corneal hydration control, as there areno apparent differences in the recovery from inducedcorneal edema, after either a short-term or 1-year use ofdorzolamide in patients with glaucoma or ocular hyperten-sion with a normal corneal endothelium.
ACKNOWLEDGMENTS
We are grateful to Laboratoires Blanchard, Sherbrook,Quebec, Canada, for generously supplying the contactlenses used in this research. Medication was supplied byMerck-Frosst Canada, Kirkland, Quebec, Canada.
REFERENCES
1. Maren TH. The development of topical carbonic anhydraseinhibitors. J Glaucoma 1995;4:49–62.
2. Maren TH. The development of ideas concerning the role ofcarbonic anhydrase in the secretion of aqueous humor:relation to the treatment of glaucoma. In: Drance SM,Neufeld AH, editors. Glaucoma: applied pharmacology inmedical treatment. New York: Grune and Stratton, 1984:325–355.
3. Hodson S, Miller F. The bicarbonate pump ion in theendothelium which regulates the hydration of rabbit cornea.J Physiol 1976;263:563–577.
4. Leibovitch L, Fischbarg J. Effects of inhibitors of passive Na1
and HCO32 fluxes on electrical potential and fluid transportacross the rabbit corneal endothelium. Curr Eye Res 1982/3;2:183–186.
5. Wistrand PJ, Schenholm M, Lonnerholm G. Carbonic isoen-zymes CAI and CaII in the human eye. Invest OphthalmolVis Sci 1986;27:419–428.
6. Terashima H, Suzuki K, Kato K, Sugai N. Membrane-boundcarbonic anhydrase activity in the rat corneal endotheliumand retina. Jpn J Ophthalmol 1996;40:142–153.
7. Ridderstrale Y, Wistrand PJ, Brechue WF. Membrane-asso-
ciated CA activity in the eye of the CAII-deficient mouse.Invest Ophthalmol Vis Sci 1994;35:2577–2584.
8. Schwam CF, Homnick CF, Michelson SR, et al. Identifica-tion and partial purification of a sodium dodecyl sulfateresistant carbonic anhydrase activity from the rabbit ciliaryprocess. ARVO abstracts. Invest Ophthalmol Vis Sci 1993;34(suppl 4):930.
9. Wistrand PJ. Distribution and function of carbonic anhy-drase (CA) isoenzymes in the human eye: relevance for thedesign of topical CA inhibitors. Exp Eye Res 1992;55(suppl1):S185.
10. Pfeiffer N. Dorzolamide: development and clinical applica-tion of a topical carbonic anhydrase inhibitor. Surv Oph-thalmol 1997;42:137–151.
11. Nielsen CB. The effect of carbonic anhydrase inhibition oncentral corneal thickness after cataract extraction. ActaOphtalmol 1980;58:985–990.
12. Becker B. The mechanism of the fall in intraocular pressureinduced by the carbonic anhydrase inhibitor Diamox. Am JOphtalmol 1954;39:177–184.
13. Brechue WF, Maren TH. A comparison between the effect oftopical and systemic carbonic anhydrase inhibitors on aque-ous humor secretion. Exp Eye Res 1993;57:67–78.
14. Schoenwald RD, Deshpande GS, Rethwisch DG, Bar-fknecht CF. Penetration into the anterior chamber via theconjunctival/scleral pathway. J Ocul Pharmacol Ther1997;13:41–59.
15. Kuang K, Xu M, Koniarek JP, Fischbarg J. Effects of ambientbicarbonate, phosphate and carbonic anhydrase inhibitors onfluid transport across rabbit corneal endothelium. Exp EyeRes 1990;50:487–493.
16. Fischbarg J, Lim JJ. Role of cations, anions and carbonicanhydrase in fluid transport across the rabbit corneal endo-thelium. J Physiol 1974;241:647–675.
17. Konowal A, Morrison JC, Brown SVL, et al. Irreversiblecorneal decompensation in patients treated with topicaldorzolamide. Am J Ophthalmol 1999;127:403–406.
18. Herndon LW, Choudhri SA, Cox T, et al. Central cornealthickness in normal glaucomatous and ocular hypertensiveeyes. Arch Ophthalmol 1997;115:1137–1141.
19. Wilkerson M, Cyrlin M, Lippa EA, et al. Four-week safetyand efficacy study of dorzolamide, a novel, active topicalcarbonic anhydrase inhibitor. Arch Ophthalmol 1993;111:1343–1350.
20. Kaminski S, Hommer A, Koyuncu D, Biowski R, Barisani T,Baumgartner I. Influence of dorzolamide on corneal thick-ness, endothelial cell count and corneal sensibility. ActaOphthalmol Scand 1998;76:78–79.
21. Lass JH, Khosrof SA, Laurence JK, Horwitz B, Ghosh K,Adamsons I. A double-masked, randomized, 1-year studycomparing the corneal effects of dorzolamide, timolol, andbetaxolol: Dorzolamide Corneal Effects Study Group. ArchOphthalmol 1998;116:1003–1010.
22. Egan CA, Hodge DO, McLaren JW, Bourne WM. Effect ofdorzolamide on corneal endothelial function in normalhuman eyes. Invest Ophthalmol Vis Sci 1998;39:23–29.
23. Gagnon MM, Boisjoly HM, Brunette I, Charest M, AmyotM. Corneal endothelial cell density in glaucoma. Cornea1997;16:314–318.
24. Weston BC, Bourne WM, Polse KA, Hodge DO. Cornealhydration control in diabetes mellitus. Invest OphthalmolVis Sci 1995;36:586–595.
25. Polse KA, Brand R, Mandell R, Vastine D, Demartini D,Flom R. Age differences in corneal hydration control. InvestOphthalmol Vis Sci 1989;30:392–399.
DORZOLAMIDE AND RECOVERY OF CORNEAL THICKNESSVOL. 129, NO. 2 149

26. Mandell R, Polse KA, Brand R, Vastine D, Demartini D,Flom R. Corneal hydration control in Fuch’s dystrophy.Invest Ophthalmol Vis Sci 1989;30:845–852.
27. Bourne WM, Nelson LR, Hodge DO. Central corneal endo-thelial cell changes over a ten-year period. Invest Ophthal-mol Vis Sci 1997;38:779–782.
28. Bonanno JA, Srinivas SP, Brown M. Effect of acetazol-amide on intracellular pH and bicarbonate transport inbovine corneal endothelium. Exp Eye Res 1995;60:425–434.
29. Edelhauser HF, Maren TH. Permeability of human cornea
and sclera to sulfonamides carbonic anhydrase inhibitors.Arch Ophthalmol 1988;106:1110–1115.
30. Sugrue MF. The preclinical pharmacology of dorzolamidehydrochloride, a topical carbonic anhydrase inhibitor. JOcular Pharmacol Ther 1996;12:363–376.
31. Ong AL, Srinivas SP, Bonanno JA. Influence of dorzolamide(Trusopt) on CO2/HCO32 transport in cultured cornealendothelial cells. ARVO abstracts. Invest Ophthalmol VisSci 1998;39(suppl 4):S930.
32. Conroy CW, Maren TH. The effect of temperature on thebinding of sulfonamides to carbonic anhydrase isoenzymes I,II, and IV. Mol Pharmacol 1995;48:486–491.
The full-text of AJO is now available online at www.ajo.com. AuthorsInteractivet, currently available in limited form, is undergoing an upgrade.
AMERICAN JOURNAL OF OPHTHALMOLOGY150 FEBRUARY 2000