domestic violence against women/men in europe: prevalence ... · dove domestic violence against...
TRANSCRIPT
doVE
Domestic Violence against Women/Men in Europe:
Prevalence, determinants, effects and policies/practices
REPORT:
Validation of
Assessment Tool
(Piloting)
2
INDEX OF CONTENTS
Page
Introduction 4
1. Piloting the Main Instrument 9
2. Results 11
3. Conclusive Remarks 15
4. References 16
3
The present report corresponds to Deliverable 3 of DOVE Project.
4
INTRODUCTION
This Report contains a description of the results obtained from the Pilot process of DOVE’s
instrument in the participating countries.
The difficulties faced in every country are discussed, after summarizing individual reports
provided by each participating centre (conf. ANNEX 6, from Interim Report – Deliverable 4).
In the pilot study the instrument was translated and tested. The aims of the translation were
to translate the instrument in a linguistically and culturally appropriate way. The aims of the pilot
test were to investigate
- practicability of the compiled instrument in diverse cultural contexts;
- feasibility of the compiled instrument and the
- feasibility of the study organization in terms of input, data handling and cross-national
transfer of data.
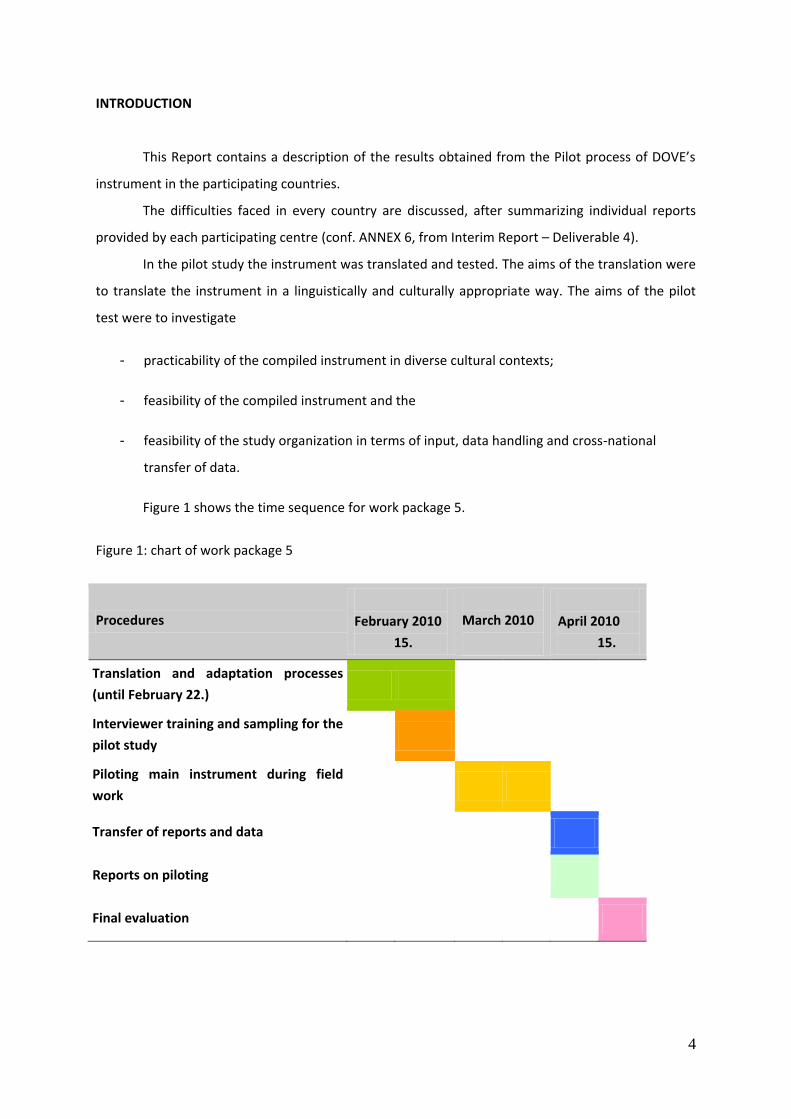
Figure 1 shows the time sequence for work package 5.
Figure 1: chart of work package 5
Procedures
February 2010
15.
March 2010
April 2010
15.
Translation and adaptation processes
(until February 22.)
Interviewer training and sampling for the
pilot study
Piloting main instrument during field
work
Transfer of reports and data
Reports on piloting
Final evaluation

5
The main underlying question of the pilot study was whether the assessment instrument is
appropriate for investigating the prevalence rates and the factors associated with domestic violence
in the 8 participating countries.
The main instrument was designed by the Swedish and the Portuguese partners and it was
circulated on February 2nd, 2010. The final draft version of this instrument was translated in the
specific languages of the partner countries (German, Portuguese, Hungarian, Spanish, Greek, Belgian
and Swedish). Appropriate translations implied:
- semantic equivalence,
- idiomatic equivalence,
- experiential equivalence and
- conceptual equivalence of the words, items, the parts and the whole instrument.
The translation and adaptation process itself includes 5 steps (WHO, 2010; Sperber, 1994;
Byrne & Campbell, 1999, Hilton and Skrutkowski, 2002), which are described in detail (see also figure
1).
Step 1: Forward translation
A health professional, who was familiar with domestic violence and respective instruments
in this area, translated the forward translation. He was aware of the concepts being examined in the
instrument to provide an equivalent and reliable translation in terms of specific constructs and
domestic violence related processes.
In case it was possible a second bilingual forward translator with a different background with
respect to the research area and the instrument under consideration additionally translated the
instrument (The second translator detected meanings of expressions and phrases from a perspective
unrelated to the scientific concepts of domestic violence Byrne & Campbell, 1999, Hilton and
Skrutkowski, 2002). He tried to find discrepancies looking to the wording and expressions that was
used in the general population. Both translators wrote a report with comments on difficult
expressions and phrases that had to be translated and suggestions of or comments on alternative
words and phrases.
Aims of the forward translation were(e.g. WHO, 2010):
6
- To perform a conceptual translation rather than a word-to-word translation;
- To provide simple and not complicated sentences;
- To target the translation for respondents from the general population;
- To avoid the use of jargon, technical terms or other specific expressions that are not
clearly to understand for respondents from the general population and
- to correspond the translation to the DOVE age-groups between 18 and 64 years.
Step 2: First expert panel
After the forward translation an expert panel of the country-specific DOVE group identified and
resolved inadequate translations. Some authors (e.g. Beaton et al., 2000) suggest this step during a
later final stage before pre-testing; however, it is preferable that the expert panel is involved during
all stages. Together with the two translators the expert panel synthesized the two versions of the
questionnaire that had to be translated or the main instrument, respectively. The expert panel used
the reports of the interpreters and discuss cultural appropriate versions of expressions and phrases.
It was important to reach consensus as far as possible if different expressions were suggested.
Previous translations of the questionnaires could be used for the discussion of specific issues.
Otherwise the concerns from one part of the expert panel had to be discussed again after the pre-
testing. This step resulted in a final version for back-translation and a report on how problems have
been resolved as well as on still existing concerns.
7
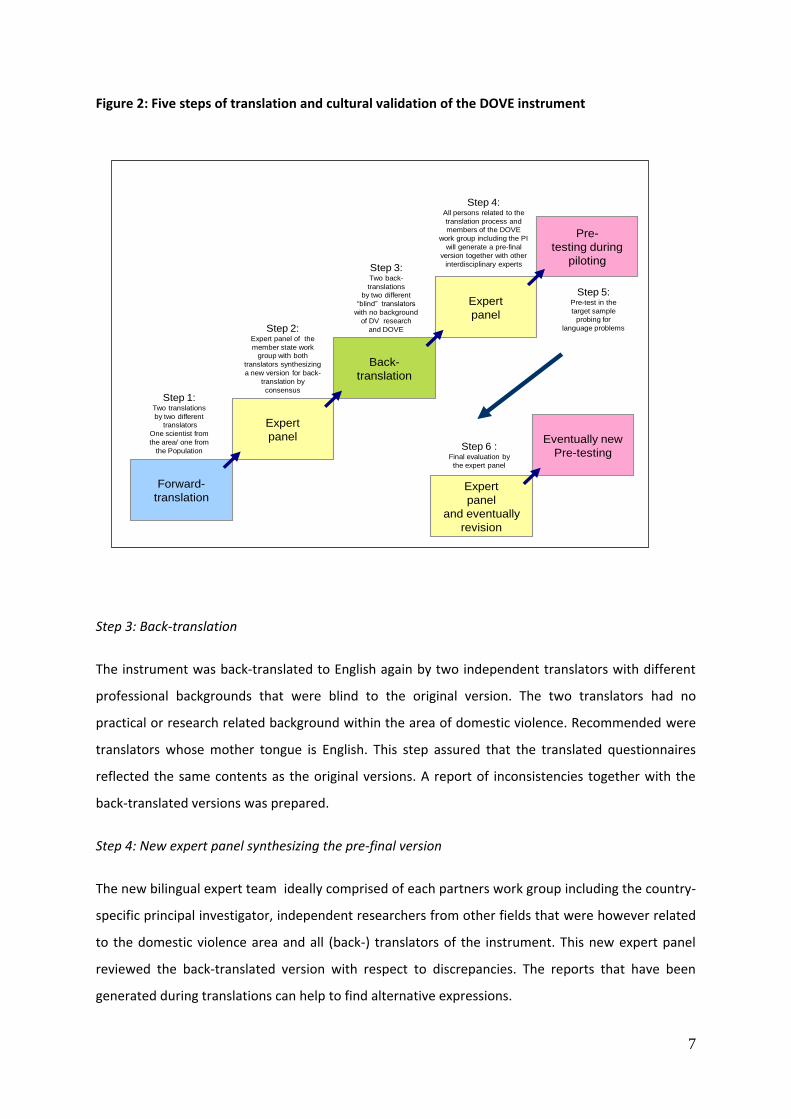
Figure 2: Five steps of translation and cultural validation of the DOVE instrument
Step 3: Back-translation
The instrument was back-translated to English again by two independent translators with different
professional backgrounds that were blind to the original version. The two translators had no
practical or research related background within the area of domestic violence. Recommended were
translators whose mother tongue is English. This step assured that the translated questionnaires
reflected the same contents as the original versions. A report of inconsistencies together with the
back-translated versions was prepared.
Step 4: New expert panel synthesizing the pre-final version
The new bilingual expert team ideally comprised of each partners work group including the country-
specific principal investigator, independent researchers from other fields that were however related
to the domestic violence area and all (back-) translators of the instrument. This new expert panel
reviewed the back-translated version with respect to discrepancies. The reports that have been
generated during translations can help to find alternative expressions.
Forward-
translation
Back-
translation
Expert
panel
Pre-
testing during
piloting
Expert
panel
Step 1:Two translations
by two different
translators
One scientist from
the area/ one from
the Population
Step 2:Expert panel of the
member state work
group with both
translators synthesizing
a new version for back-
translation by
consensus
Step 4:All persons related to the
translation process and
members of the DOVE
work group including the PI
will generate a pre-final
version together with other
interdisciplinary experts
Step 5:Pre-test in the
target sample
probing for
language problems
Eventually new
Pre-testing
Expert
panel
and eventually
revision
Step 6 :Final evaluation by
the expert panel
Step 3:Two back-
translations
by two different
“blind” translators
with no background
of DV research
and DOVE
8
In case of concerns about different interpretations and meanings of expressions it can be
also useful to present unclear items to children or adolescents. However, if no consensus is reached
on specific expressions interviewers had to be instructed to probe respondents for appropriate
understanding. The aim of this expert panel is to generate a pre-final version for pre-testing.
Equivalence of this version with the original version and cross cultural adaptation includes:
- Semantic equivalence (same meaning of the words with respect to the vocabulary and
grammar);
- Idiomatic equivalence (same meaning with respect to the intention of the word or
phrase)
- Experiential equivalence (same meaning with respect to corresponding experiences and
framework of violent situations)
- Conceptual equivalence (same meaning e.g. of behaviours with respect to the concept of
domestic violence in different cultures).
Step 5: Pre-testing the translated instrument
The pre-testing of the translated instrument was done during the pilot study. For this purpose it was
suggested to edit and print the complete instrument together with the instructions. Furthermore
forms to fill in with comments from the interviewers were prepared. Interviews were instructed to
control the application of the instrument with respect to its cultural adaptability. After the
assessment, the practicability and feasibility of the instrument was discussed in the expert panel
together with the interviewers.
9
1. PILOTING THE MAIN INSTRUMENT
Main question to be answered: Are the questionnaires appropriately adapted and feasible? Do the
respondents understand and accept all items of the main instrument?
In the Ludwigsburg meeting on December 3.-4., 2009 the partners agreed that the pilot study should
be conducted with 5 female and 5 male respondents aged 18-60 years in each participating country.
Snowball-sampling was suggested for recruitment. Snowball sampling means that persons in the
network of the researches are contacted and asked whether they agree in participating on the pilot
study (Patton, 1990).
INTERVIEWERS OF THE PILOT STUDY
At least 1 female and 1 male interviewee was recruited for the pilot study. Because gender might
play a role for the data assessment and the response behaviour the organizational staff allocated
both interviewers and interviewees according to the wishes of the interviewees.
FIELD WORK OF THE PILOT STUDY
The field work of the pilot study consisted of training of interviewers for the pilot study, assessment
of interviewees and of testing the organization of data management for the main study.
Interviewer training for the pilot study
Training of interviewers for the pilot study was done in 11 steps:
Step 1: General information about DOVE
Step 2: Functions and responsibilities of the interviewers
Step 3: Rights of the interviewees
Step 4: Data safety
Step 5: Handling of addresses
Step 6: First phone contact
Step 7: First personal contact
Step 8: Instructions for the administration of the instrument
Step 9: Instructions and practice of problematic situations during assessment
Step 10: Data management together with the study organization
10
Step 11: Recording of any problems in the matrix provided by the German team
Assessment of interviewees
Interviewees were assessed with the main instrument. Interviewers recorded length of the interview
and problems during interviewing. The following procedures were recommended with respect to the
cultural adaptation of the instrument:
(1) Interviewees were advised to note any unclear expression or phrase. These expressions and
phrases were recorded.
(2) Interviewees were debriefed after the assessment on further inadequate expressions and
phrases.
(3) Interviewers tried to find alternative words in the above cases together with the Interviewees.
(4) Results of this process of finding solutions for potential problems and any problems with the
instrument were recorded (e.g. appearance and layout of the instrument).
(5) Notes and suggestions for corrections were summarized in a report concerning the main
instrument also included additional information about the respondent.
11
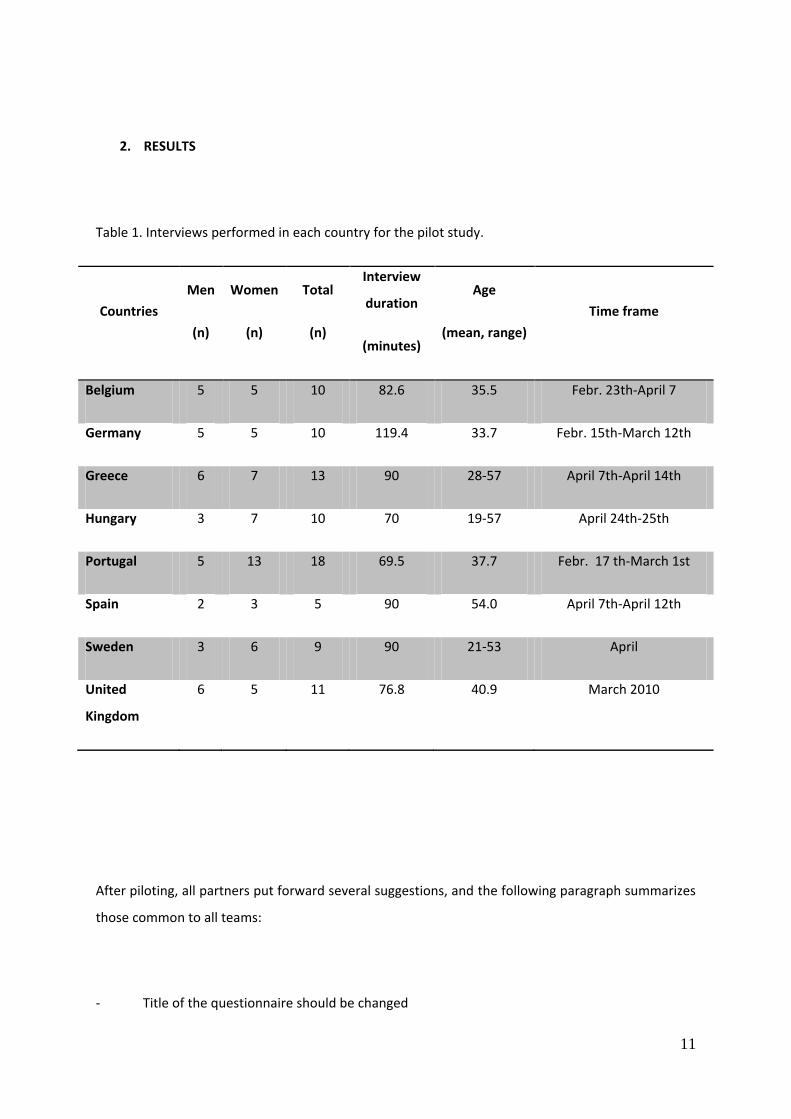
2. RESULTS
Table 1. Interviews performed in each country for the pilot study.
Countries
Men
(n)
Women
(n)
Total
(n)
Interview
duration
(minutes)
Age
(mean, range)
Time frame
Belgium 5 5 10 82.6 35.5 Febr. 23th-April 7
Germany 5 5 10 119.4 33.7 Febr. 15th-March 12th
Greece 6 7 13 90 28-57 April 7th-April 14th
Hungary 3 7 10 70 19-57 April 24th-25th
Portugal 5 13 18 69.5 37.7 Febr. 17 th-March 1st
Spain 2 3 5 90 54.0 April 7th-April 12th
Sweden 3 6 9 90 21-53 April
United
Kingdom
6 5 11 76.8 40.9 March 2010
After piloting, all partners put forward several suggestions, and the following paragraph summarizes
those common to all teams:
- Title of the questionnaire should be changed
12
- Lenght of the questionnaire (too long)
- Order of scales should be revised
- Transition between scales should be clear
- Introduction of systematic skips are needed
- Numbering of questions is absoluteley necessary
- Coding of missing data should be agreed upon
Additionally, some suggestions came only from one or two centres:
- Health care utilization scale should be simplified
- Smoking , Alcohol use scale needs revision
- Medication scales is too detailed
- Either questions of health or the SF-36
- Before asking for PTSD symptoms :
Type of event, period of life (use of original scale or use of the DSM-events
list)
- „Who did first“ and violence escalation should be omitted in case there was no violence
- „Who did it first“ should be skipped
- PTSD scale needs the full scale
13
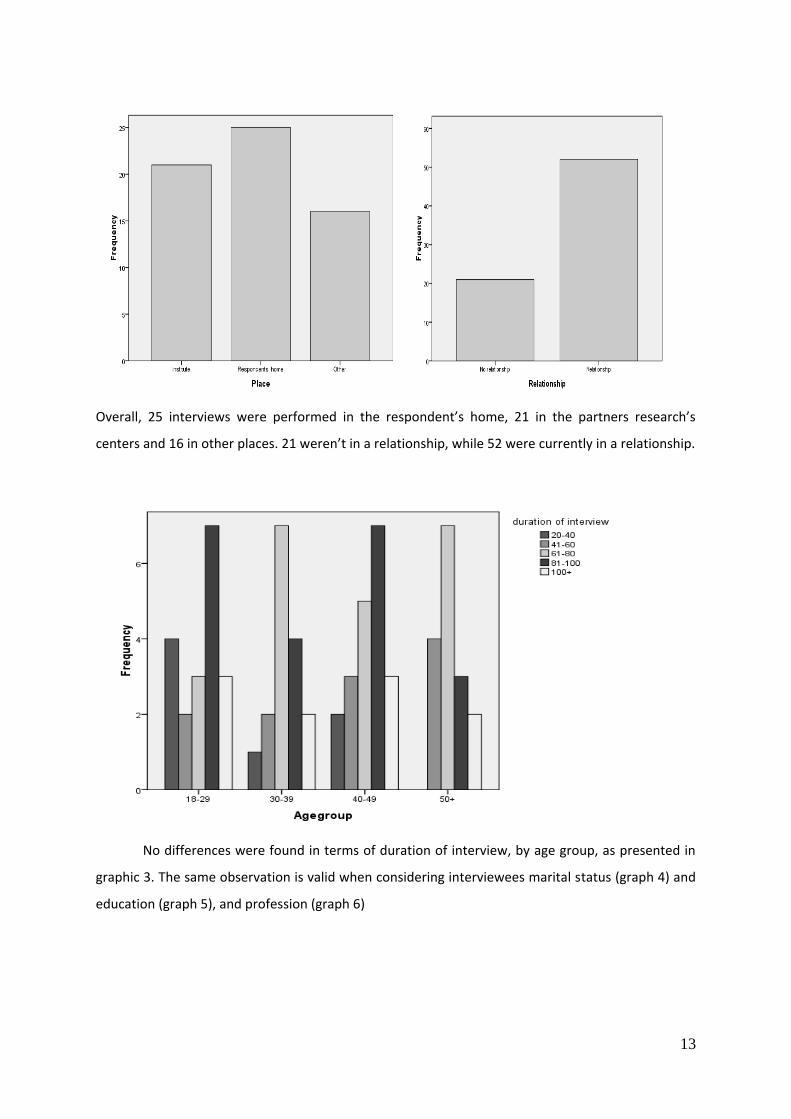
Overall, 25 interviews were performed in the respondent’s home, 21 in the partners research’s
centers and 16 in other places. 21 weren’t in a relationship, while 52 were currently in a relationship.
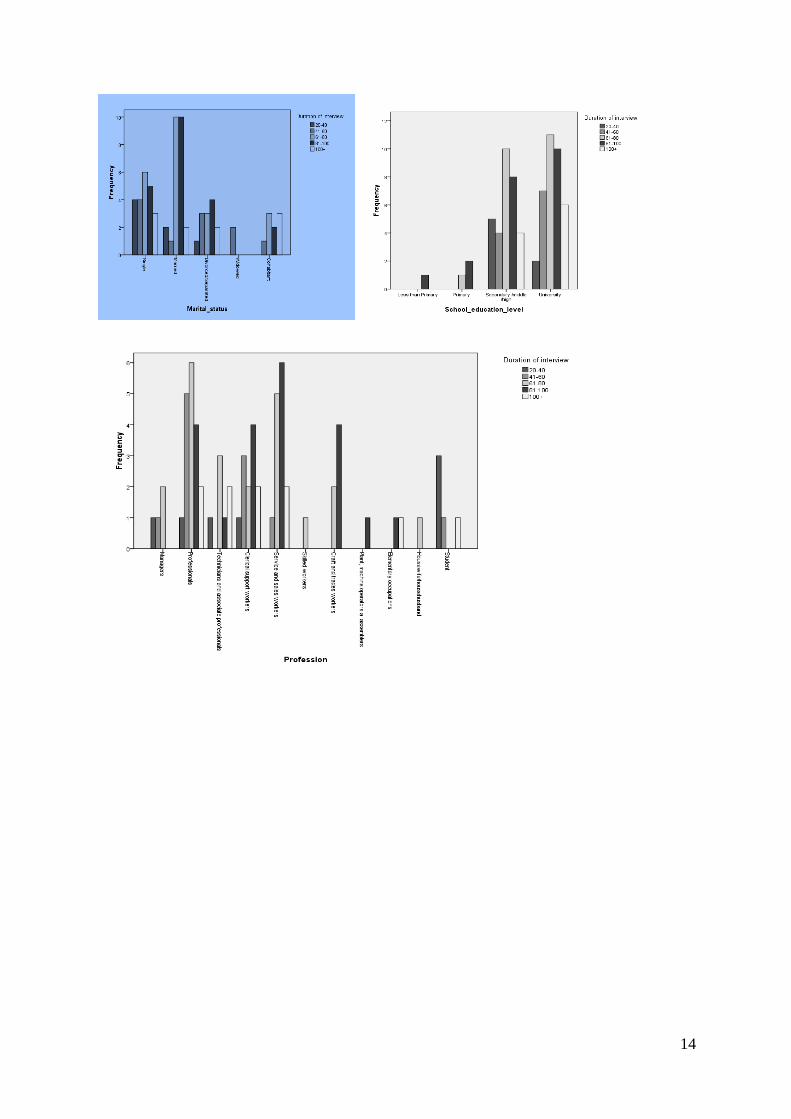
No differences were found in terms of duration of interview, by age group, as presented in
graphic 3. The same observation is valid when considering interviewees marital status (graph 4) and
education (graph 5), and profession (graph 6)
14
15
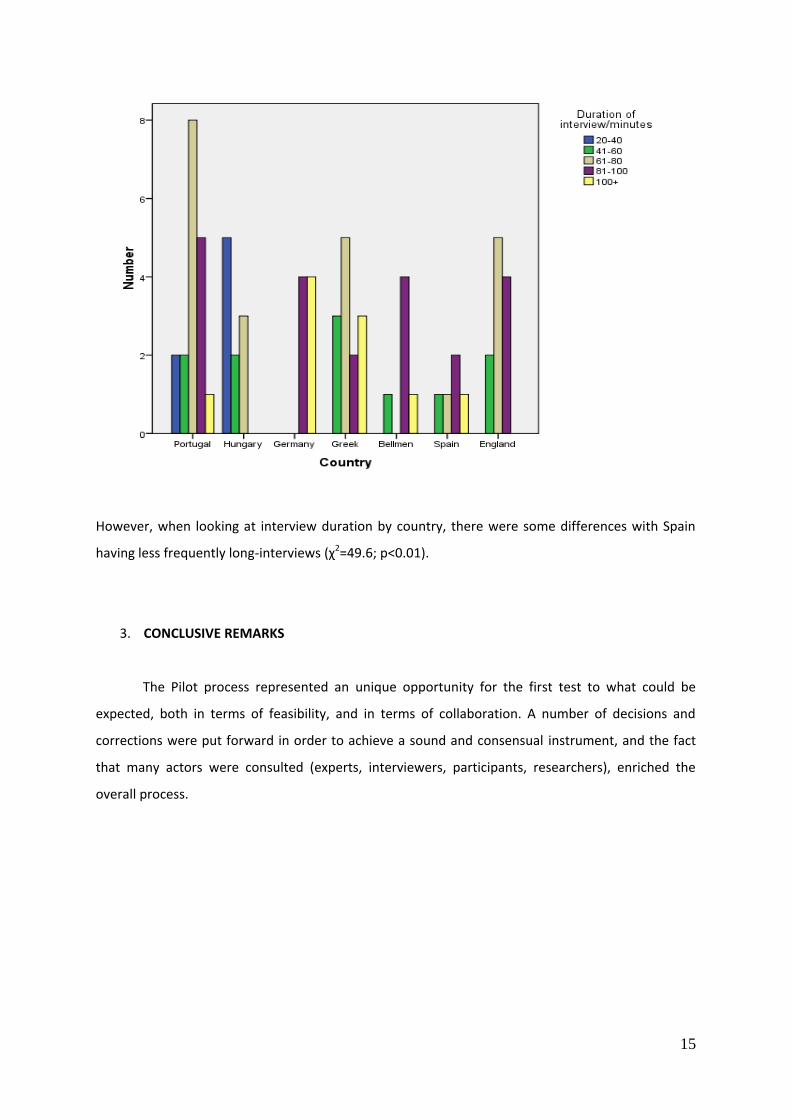
However, when looking at interview duration by country, there were some differences with Spain
having less frequently long-interviews (χ2=49.6; p<0.01).
3. CONCLUSIVE REMARKS
The Pilot process represented an unique opportunity for the first test to what could be
expected, both in terms of feasibility, and in terms of collaboration. A number of decisions and
corrections were put forward in order to achieve a sound and consensual instrument, and the fact
that many actors were consulted (experts, interviewers, participants, researchers), enriched the
overall process.
16
4. REFERENCES
1. Byrne BM, Campbell TL. (1999). Cross-cultural comparisons and the presumption of equivalent measurement and theoretical structure: A look beneath the surface. Journal of Cross-Cultural Psychology 30: 555-574.
2. Guillemin F, Bombardier C, Beaton D. (1993). Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guideline. J Clin Epidemiol. 46: 1417-1432.
3. Hilton A, Skrutkowski M. (2002). Translating instruments into other languages: Development and testing processes. Cancer Nursing 25 (1): 1-7.
4. Patton M. (1990). Qualitative evaluation and research methods. Sage:Nebury Park, Calif.
5. Sperber AD, Devellis RF, Boehlecke B. (1994). Cross-cultural translation. Journal of Cross-Cultural Psychology 25: 501-524.