dka in children
TRANSCRIPT

DKA Definition:A state of absolute or relative insuline defeciency resulting in hyperglycemia, dehydration and accumulation of ketone bodies in the blood with subsquent metabolic acidosis.
Causes of DKA: Causes of DKA: A. Initial presentation of type 1 diabetes A. Initial presentation of type 1 diabetes
mellitus mellitus B. Missed insulin injections B. Missed insulin injections C. Inadequate insulin dosage in a known C. Inadequate insulin dosage in a known
diabetic patient diabetic patient D. Emotional stress/ trauma/surgery D. Emotional stress/ trauma/surgery
without adequate insulin adjustment without adequate insulin adjustment E. Intercurrent illness/infection without E. Intercurrent illness/infection without
appropriate dose adjustment appropriate dose adjustment
PathophysiologyPathophysiology The combination of low serum insulin and high The combination of low serum insulin and high
counterregulatory hormone concentrations counterregulatory hormone concentrations results in:results in:
an accelerated catabolic state with increased an accelerated catabolic state with increased glucose production by the liver and kidney (via glucose production by the liver and kidney (via glycogenolysis And gluconeogenesis) glycogenolysis And gluconeogenesis)
impaired peripheral glucose utilization impaired peripheral glucose utilization resulting in hyperglycemia and resulting in hyperglycemia and hyperosmoLality , and increased lipolysis and hyperosmoLality , and increased lipolysis and ketogenesis ,causing Ketonemia and metabolic ketogenesis ,causing Ketonemia and metabolic acidosisacidosis
.Hyperglycemia that exceeds the renal threshold [180mg/dL]) and hyperketonemia cause osmotic diuresis, dehydration, and obligatory loss of electrolytes, which often is aggravated by vomiting.
These changes stimulate further stress hormone production ,which induces more severe insulin resistance and worsening hyperglycemia and hyperketonemia.
If this cycle is not interrupted with exogenous If this cycle is not interrupted with exogenous insulin, fluid and electrolyte therapy , fatal insulin, fluid and electrolyte therapy , fatal dehydration and metabolic acidosis will ensue.dehydration and metabolic acidosis will ensue.
Ketoacidosis may by aggravated by lactic Ketoacidosis may by aggravated by lactic acidosis from poor tissue perfusion or sepsis.acidosis from poor tissue perfusion or sepsis.
Clinical manifestations of Clinical manifestations of diabetic ketoacidosis diabetic ketoacidosis
• • DehydrationDehydration• • Rapid, deep, sighing (Kussmaul respiration)Rapid, deep, sighing (Kussmaul respiration)••Nausea, vomiting, and abdominal pain Nausea, vomiting, and abdominal pain
mimicking an acute abdomenmimicking an acute abdomen••Progressive obtundation and loss of Progressive obtundation and loss of
consciousnessconsciousness• • Increased leukocyte count with left shiftIncreased leukocyte count with left shift• • Non-specific elevation of serum amylaseNon-specific elevation of serum amylase• • Fever only when infection is presentFever only when infection is present
Biochemical criteria for the diagnosis of DKA
• Hyperglycemia (blood glucose > 11mmol/L [≈ 200 mg/dL])
• Venous pH <7.3 or bicarbonate <15mmol/L
• Ketonemia and ketonuria
The severity of DKA is categorized by the degree of acidosis :
• Mild: venous pH <7.3 or bicarbonate <15mmol/L
• Moderate: pH <7.2 , bicarbonate <10mmol/L
• Severe : pH <7.1, bicarbonate <5mmol/L
note
?
Partially treated children and children who Partially treated children and children who have consumed little or no carbohydrate have consumed little or no carbohydrate
may have, on rare occasion, only modestly may have, on rare occasion, only modestly increased blood glucose concentration increased blood glucose concentration
(‘‘euglycemic ketoacidosis’’)(‘‘euglycemic ketoacidosis’’)
managementmanagementA. History (key points) A. History (key points) 1.Classic triad = polydipsia, polyuria, and weight loss 1.Classic triad = polydipsia, polyuria, and weight loss
(polyphagia is unusual in children) (polyphagia is unusual in children) 2. Vomiting/abdominal pain 2. Vomiting/abdominal pain 3. Increased, difficult, or deep respirations 3. Increased, difficult, or deep respirations 4. Symptoms of infection/flu (may be similar to those of 4. Symptoms of infection/flu (may be similar to those of
DKA) DKA) 5. Illness in family members or close friends 5. Illness in family members or close friends 6. In a known diabetic: 6. In a known diabetic: *when and how much insulin was last taken? *when and how much insulin was last taken? *missed shots? *missed shots? *emotional stress as clues to missed shots? *emotional stress as clues to missed shots?
B. Physical exam :B. Physical exam : 1. Vital signs 1. Vital signs 2 Hydration status / peripheral perfusion / 2 Hydration status / peripheral perfusion /
hypovolemic shock? hypovolemic shock? 3. Acetone-fruity breath 3. Acetone-fruity breath 4. Kussmaul respirations 4. Kussmaul respirations 5. Neurologic status 5. Neurologic status 6. Signs of infection 6. Signs of infection
C. Initial labs-stat C. Initial labs-stat
1.For diagnosis: blood glucose and urine ketones. 1.For diagnosis: blood glucose and urine ketones. A simple urine dipstick and/or a meter glucose level in A simple urine dipstick and/or a meter glucose level in
an ED or office an ED or office
2.2. Serum glucose, electrolytes including Na+, K+, Serum glucose, electrolytes including Na+, K+, HCO3 and BUN, venous pH and PC02. HCO3 and BUN, venous pH and PC02.
[Arterial PC02 less than 20 mmHg may be an important [Arterial PC02 less than 20 mmHg may be an important predictor of cerebral edema in severe DKA. (pH <7.0)predictor of cerebral edema in severe DKA. (pH <7.0)
3-Calcium ,phosphorus, and magnesium concentrations (ifpossible), HbA1c, hemoglobin and hematocrit or completeBlood count .
Note, however, that an elevated white blood cell count in response to stress is characteristic of DKA an does not necessarily indicative of infection
4-4- Perform a urine analysis for ketones.Perform a urine analysis for ketones. 5- Measurement of blood ß-hydroxy butyrate 5- Measurement of blood ß-hydroxy butyrate
concentration, if available, is usefull to concentration, if available, is usefull to confirm ketoacidosis and may be used to confirm ketoacidosis and may be used to monitor the response to treatmentmonitor the response to treatment
6- Obtain appropriate specimens for culture 6- Obtain appropriate specimens for culture (blood, urine , throat), if there is evidence of (blood, urine , throat), if there is evidence of infection.infection.
7- If laboratory measurement of serum 7- If laboratory measurement of serum potassium is delayed, perform an (ECG) forpotassium is delayed, perform an (ECG) forbaseline evaluation of potassium statusbaseline evaluation of potassium status
Additional calculations that Additional calculations that may be informativemay be informative
Anion gap Anion gap = Na − (Cl + HCO3): normal is = Na − (Cl + HCO3): normal is 12 ± 2 12 ± 2 (m mol/L)(m mol/L)
In DKA the anion gap is typically In DKA the anion gap is typically 20–3020–30
m mol /L;m mol /L; An anion gap An anion gap >35 >35 m mol/L suggests m mol/L suggests
concomitant Lactic acidosisconcomitant Lactic acidosis
Pseudohyponatremia (hyperglycemia and hyperlipidemia result in falsely lowered plasma sodium
(Naactual = Nameasured + 1.6[(glucose – 100)/100]
••Corrected sodium Corrected sodium = measured Na + 2 = measured Na + 2 ([plasma glucose − 5.6] /5.6 ) (mmol/L)([plasma glucose − 5.6] /5.6 ) (mmol/L)
• • Effective osmolality Effective osmolality = (mOsm /kg) 2x(Na + = (mOsm /kg) 2x(Na + K) + glucose (mmol/L)K) + glucose (mmol/L)
Hyperosmolality as a result of progressive hyperglycemia contributes to cerebral obtundation in DKA
Serum osmolality:
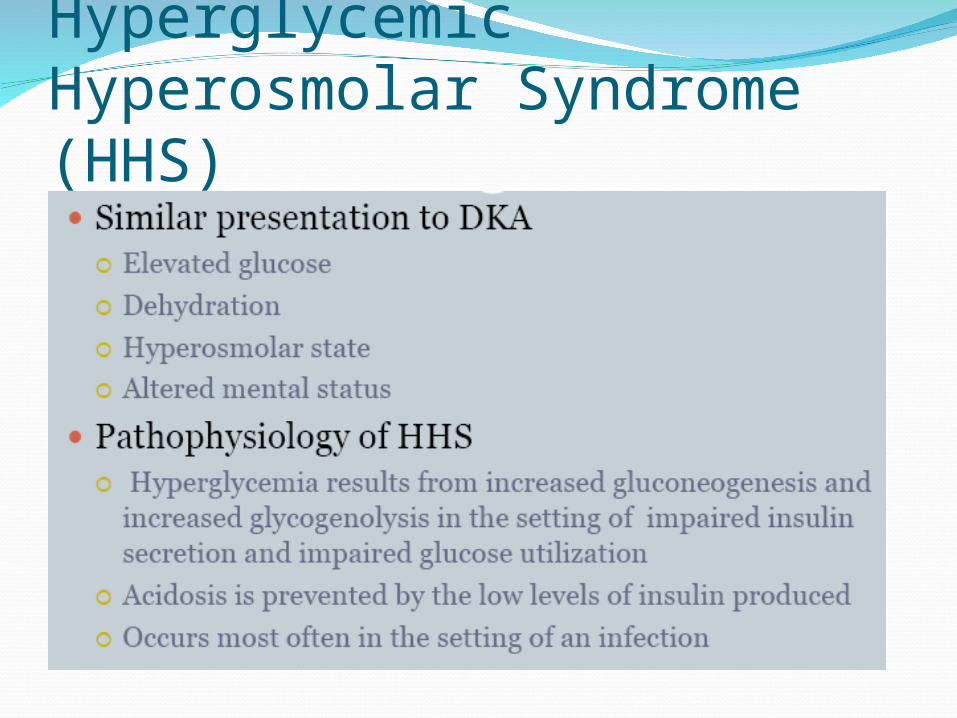
Hyperglycemic Hyperosmolar Syndrome (HHS)
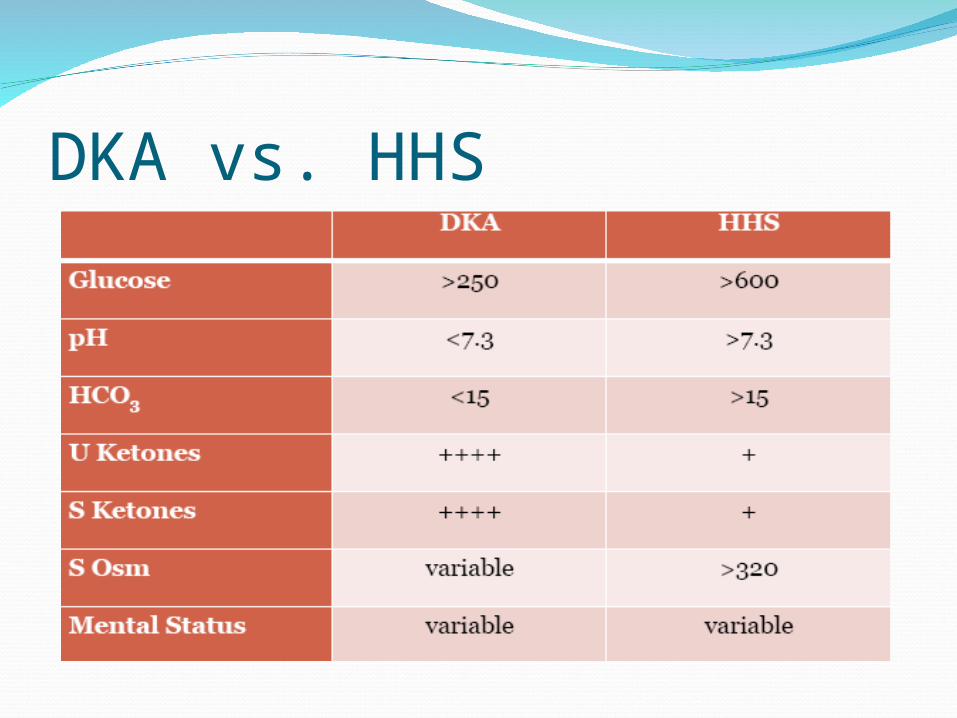
DKA vs. HHS
PathophysiologyWith progressive
dehydration, acidosis, hyperosmolality, and diminished cerebral oxygen utilization, consciousness becomes impaired, and the patient ultimately becomes comatose
treatmenttreatment
Goals of therapyGoals of therapy
Correct dehydrationCorrect dehydrationCorrect acidosis and reverse ketosisCorrect acidosis and reverse ketosisRestore blood glucose to near normalRestore blood glucose to near normalAvoid complications of therapyAvoid complications of therapyIdentify and treat any precipitating eventIdentify and treat any precipitating event
A. Mistakes and how to avoid them 1) Failure to recognize the problem (e.g., the diagnosis of
new onset diabetes, cerebral edema, hypokalemia, etc.).
2) Failure to react to the situation, whether the problem is due to the natural course of the disease, or secondary to therapy.
a. Keep a flow sheet for fluids, insulin, vital signs, lab values, etc. b. Record all intake and output meticulously. c. ECG monitor for K+ changes if severe acidosis or elevated K+.
d. Urinary catheter only if unconscious. If conscious, ask patient to void every hour. In the young child, weigh the diapers hourly.
e. Check pupils and sensorium hourly (for cerebral edema).
Fluids 1. Initial volume expansion =10 to20cc/kg (300-600cc/m2) of a physiologic solution (such as saline or lactated Ringers solution) over the first one to two hours.
This may need to be repeated if the patient is severely dehydrated and/or if urine output is massive. However, the initial bolus re-expansion should never exceed 40 cc/kg as a total fluid dose for the first four hours of treatment.
2. 24 hour fluid therapy a. Replacement: Use estimates of dehydration based on physical exam varying from 5 to 10% of body weight for mild to severe losses.
Deficits should be replaced evenly over 48 hours.
Remember to subtract the quantities given in the first hours of re-expansion from the 24 hour totals.
Follow urine output to be certain initial estimates are adequate. Replacement of urine output (“cc” for “cc”) is generally not required, since excessive urine output should resolve within the initial 2 to 4 hours of therapy as the hyperglycemia resolves. Total fluid replacement should not exceed 4 L per square meter per 24 hours. .
b. Maintenance
body weight (kg) 24 hour fluid maintenance
up to 10 100 ml/kg 10 to 20 1000 ml + 50 ml/kg over 10
kg >20 1500 ml + 20 ml/kg over 20
kg c. Special additional losses
Additional replacement may be required where there is severe vomiting, etc.
Insulin therapy
Although rehydration alone causes some decrease in blood glucose concentration, insulin therapy isessential to normalize blood glucose and suppresslipolysis and ketogenesis.
• Start insulin infusion 1–2hours after starting fluidReplacement therapy; i.e .after the patient hasReceived initial volume expansion
Correction of insulin deficiency
Dose: 0.1 unit/kg/hour (for example,one method is to dilute 50 units regular [soluble] insulin in 50 mL normal saline, 1unit = 1mL)
Route of administration IV
An IV bolus is unnecessary, may increase therisk of cerebral edema , and should not be used at the start of therapy
Goal is to slowly decrease serum glucose > 100 mg/dl/hr
The dose of insulin should usually remain at 0.1 unit/kg/hour at least until resolution of DKA (pH > 7.30 , bicarbonate > 15 mmol/L and/or closure of the anion gap), which invariably takes longer than normalization of blood glucose concentrations
To prevent an unduly rapid decrease in plasma glucose concentration and hypoglycemia , 5% glucose should be added to the IV fluid (e.g., 5% glucose in 0.45% saline) when the plasma glucose falls to approximately 14–17 mmol/L (250–300 mg/dL), or sooner if the rate of fall is precipitous.
It may be necessary to use 10% or even 12.5% dextrose to prevent hypoglycemia while continuing to infuse insulin to correct the metabolic acidosis.
Potassium
K+ is a special problem because high urinary losses occur in association with normal serum levels caused by the intracellular exodus of K+ in the presence of acidosis.
Vomiting may also contribute to hypokalemia. and as a consequence of osmotic diuresis.Volume depletion causes secondary hyperaldosteronism,which promotes urinary potassium excretion
Thus, total body depletion of potassium occurs, but at presentation serum potassium levels may be normal, increased or decreased. renal dysfunction, by enhancing hyperglycemia and reducing potassium excretion, contributes to hyperkalemia.
Total body potassium is usually depleted, but serum levels may be normal or high.
As acidosis is corrected, K+ is driven back into the cells and there is usually a fall in serum K+ in spite of large K+ replacements.
Low or high serum potassium levels can be a cause of cardiac arrhythmias, which can be fatal. a. Potassium must never be given until the serum potassium level is known. b. Once the serum potassium is known to be normal or low, and after voiding is observed, generally after the first hour of fluid resuscitation, all IV fluids should include 20-40 mEq/L of potassium. If the serum potassium is high, it is best to wait to add K+ to the IV until the K+ begins to decrease.
The potassium may be in the form of KCl, KAc, K2H PO4 or a combination of thes supplements.
Do not give K+ as a rapid IV bolus or cardiac arrest may result.
Severe hypokalemia may lead to respiratory arrest due to muscle dysfunction.
ECG strips (Lead II) may give the best indication of total body K+ deficit or change.
Potassium (give as Kphos, Kacetate, or KCl)If K > 6 = No K initiallyIf K 5 – 6 = consider adding K+If K < 5 = at least 40 mEq/LDon’t forget “hyperkalemia associated with
acidosis” and role of insulin
Acidosis
Severe acidosis is reversible by fluid and insulinreplacement; insulin stops further ketoacid production and allows ketoacids to be metabolized, which generates bicarbonate.
Treatment of hypovolemia improves tissue perfusion and renal function, thereby increasing the excretion of organic acids.
BICARBONATE IS ALMOST NEVER ADMINISTERED
bicarbonate administration can lead to paradoxical cerebral acidosis HCO3
- combines with H+ and dissociated to CO2 and H2O. Whereas bicarbonate passes the blood-brain barrier slowly, CO2 diffuses freely, thereby exacerbating cerebral acidosis and ischemia
Rapid correction of acidosis with bicarbonate causes hypokalemia and failure to account for the sodium being administered and appropriately reducing the NaCl concentration of the fluids can result in increasing osmolality
Nevertheless, there may be selected patients who may benefit from cautious alkali therapy. These include: Patients with severe acidemia (arterial pH <6.9) in whom decreased cardiac contractility and peripheral vasodilatation can further impair tissue perfusion, and patients with life-threatening hyperkalemia
Complications of therapy
• Inadequate rehydration• Hypoglycemia• Hypokalemia• Hyperchloremicacidosis• Cerebraledema
Case ScenarioA 4 y/o female in the PICU is undergoing
treatment for new onset IDDM and DKA. She is on an insulin infusion at 0.1 u/kg/hr, and fluids are running at 1.5 maintenance.
Over the last hour, she has been complaining about increasing headache. She is now found to be unresponsive with bilateral fixed and dilated pupils, HR is 50 with BP 150/100.
What is your next step in management?
Treatment pitfallsCerebral edema is the major life-threatening
complication seen in the treatment of children with DKAusually develops several hours after the
institution of therapyMost commonly presents in children between 5
–14 years
Treatment pitfallsCerebral edema is the major life-threatening
complication seen in the treatment of children with DKAusually develops several hours after the
institution of therapyMost commonly presents in children between 5
–14 years
Treatment pitfallsClinically evident
cerebral edema – about 1%. However, increasing evidence suggests that subclinical cerebral edema occurs in the majority of patients treated with fluids and insulin for DKA Glaser N J Pediatr. 2004
Treatment pitfallsCerebral edema
manifestations include headache, alteration in level of consciousness, bradycardia, emesis, diminished responsiveness to painful stimuli, and unequal or fixed, dilated pupils
Treatment pitfallsTherapy of cerebral
edema includes treatment aimed at lowering increased intracranial pressure (mannitol, hypertonic saline, hyperventilation, etc..)
Treatment pitfallsTraditional risk factors thought to be
excessive use of fluids, use of bicarbonate, and large doses of insulin (or just sicker patients?)
Treatment pitfallsMore recently
identified risk factors Increased BUN at
presentation (reflective of greater dehydration)
Profound neurologic depression at diagnosis of cerebral edema
Endotracheal intubation with hyperventilation (Marcin J Pediatr 2002)
But ….
Other pitfallsThrombosis associated with femoral venous
catheterization in children with DKA (Gutierrez JA. Critical Care Medicine 2001)
Hypoglycemic Reactions (Insulin Shock)symptoms and signs include pallor, sweating,
apprehension, trembling, tachycardia, hunger, drowsiness, mental confusion, seizures and coma
management includes administration (if conscious) of carbohydrate-containing snack or drink
glucagon 0.5 mg is administered to an unconscious or vomiting child
Cerebral edemaCerebral edema
incidence is 0.5–0.9% and the mortality rate isincidence is 0.5–0.9% and the mortality rate is21–24%.21–24%.
Pathogenesis is unclear and incompletely understood Pathogenesis is unclear and incompletely understood
Demographic risk factors include:Demographic risk factors include:• • Younger age Younger age • • New onset diabetesNew onset diabetes• • Longer duration of symptomsLonger duration of symptoms
Risk factors at diagnosis or during treatment Of DKA :
• Greater hypocapnia at presentation after adjustingFor degree of acidosis.
• Increased serum urea nitrogen at presentation.
• More severe acidosis at presentation.
• Bicarbonate treatment for correction of acidosis.
• An attenuated rise in measured serum sodiumConcentrations during therapy.
• Greater volumes of fluid given in the first 4 hours.
• Administration of insulin in the first hour of fluid treatment
Warning signs and symptoms of cerebral edema
• Headache & slowing of heart rate• Change in neurological status (restlessness,Irritability ,increased drowsiness,incontinence)• Specific neurological signs (e.g.,cranial nervepalsies)• Rising blood pressure• Decreased O2 saturation
Diagnostic criteria
• Abnormal motor or verbal response to pain
• Decorticate or decerebrate posture
• Cranial nerve palsy (especially III ,IV , and VI)
• Abnormal neurogenic respiratory pattern (e.g.,Grunting , tachypnea, Cheyne-Stokesrespiration, apneusis)
Major criteria• Altered mentation/fluctuating level of consciousness
• Sustained heart rate deceleration (decrease more than 20 beats per minute) not attributable to improvedIntravascular volume or sleep state
• Age-inappropriate incontinence
Minor criteria• Vomiting
• Headache
• Lethargy or not easily arousable
• Diastolic blood pressure >90 mmHg
• Age <5 years
One diagnostic criterion ,two major criteria, or one major and two minor criteria have a sensitivity of 92% and a false positive rate of only 4%.
Treatment of cerebral edema
• Initiate treatment as soon as the condition issuspected.• Reduce the rate of fluid administration by one-third.• Give mannitol 0.5–1 g /kg IV over 20 minutes andRepeat if there is no initial response in 30 minutes to2 hours .
• Hypertonic saline (3%), 5–10 mL/kg over30 Minutes ,may be an alternative to mannitol or a Second line of therapy if there is no initial response to mannitol .
O Mannitol or hypertonic saline should be availableat the bedside
Elevate the head of the bed
Intubation may be necessary for the patient with impending respiratory failure, but aggressive hyperventilation (to a pCO2 <2.9kPa [22mmHg]) has been associated with poor outcome and is not recommended

After treatment for cerebral edema has been started, a cranial CT scan should be obtained to rule out other possible intracerebral causes of neurologic deterioration ( ≈10%ofcases), especially thrombosis or hemorrhage, which may benefit from specific therapy.
Recommendations/ key points• DKA is caused by either relative or absolute insulin deficiency.
• Children and adolescents with DKA should be managed in centers experienced in its treatment andwhere vital signs, neurological status and laboratoryresults can be monitored frequently
• Begin with fluid replacement before starting insulintherapy.
• Volume expansion (resuscitation) is required only if needed to restore peripheral circulation.
Subsequent fluid administration (including oral fluids) should rehydrate evenly over 48 hours at a rate rarely in excess of 1.5–2 times the usual dailyMaintenance requirement.
Begin with 0.1U/kg/h. 1–2 hours AFTER startingfluid replacement therapy.
If the blood glucose concentration decreases tooQuickly or too low before DKA has resolved,Increase the amount of glucose administered. DoNOT decrease the insulin infusion
Even with normal or high levels of serum potassiumAt presentation, there is always a tota lbody deficit of potassium.
Begin with 40 mmol potassium/L in the infusate or20 mmol potassium/L in the patient receiving fluid At a rate >10 mL/kg/h.
• There is no evidence that bicarbonate is eitherNecessary or safe in DKA.
• Have mannitol or hypertonic saline at the bedsideAnd the dose to be given calculated before hand.
• In case of profound neurological symptoms, mannitol should be given immediately.• All cases of recurrent DKA are preventable
