divergent effects of antihypertensive therapy on cardiovascular responses and left ventricular...
TRANSCRIPT

Divergent Effects of Antihypertensive Therapy on Cardiovascular Responses and Left Ventricular Function During Upright Exercise
ROBERT A. BRUCE, MD, FACC REGINALD ELEADY-COLE, MB,
BChir, MRCP*t LOWELL J. BENNETT, MD* FUSAKO KUSUMI, MS
Seattle, Washington
From the Department of Medicine (Cardiolo- gy), University of Washington, Seattle, Wash. These studies were supported in part by Grants in Aid HE09773 and HE05281-13 from the National Heart and Lung Institute, RR37 from the National Institutes of Health, HSOOO92 from the National Center for Health Sciences Research, U.S. Public Health Ser- vice, and an award from Merck, Sharpe and Dohme Company. Manuscript received May 1, 1972: revised manuscript received Juty 1. 1972, accepted July 4, 1972.
*Recipients of the Poncin Scholarship for Medical Research, Seattle First National Bank.
*Recipient of Junior Research Award from World Health Organization.
Address for reprints: Robert A. Bruce, MD. Department of Medicine (Cardiology), Uni- versity Hospital, RG-20. University of Wash- ington, Seattle, Wash. 98195.
Maximal oxygen intake (defined by the highest value observed) dur- ing upright exercise increased (P qO.05) in 16 patients with essen- tial hypertension but not In 27 of 50 slightly younger, asymptomatic Negro male workers with high blood pressure. Antihypertensive ther- apy reduced resting blood pressure (P CO.001) in all and decreased pressure at maximal exercise in workers (P X0.001); but duration of multistage treadmill exercise increased significantly (P CO.001) only in patients. Hemodynamic studies at rest and at graded levels of submaximal exercise on a bicycle ergometer in 15 untreated volur~ teers (6 patients and 7 workers) revealed reduced cardiac output and asymptotic relation to oxygen intake In untreated patients. Dur- ing effective antihypertensive therapy, both systemic and pulmonary arterial mean pressure levels were slightly lower (P X0.001) at rest and during submaximal exercise. In patients, cardiac output at high er work loads increased as noncongestive left ventricular failure was corrected and left ventricular function Improved with treatment. In untreated workers, acute reduction of blood pressure with nitroglyc- erin increased maximal oxygen intake (P CO.001) but was lneffect- ual during antihypertensive therapy.
In conclusion, antihypertensive therapy reduces pressure and im- proves ventricular function, but only when hypertension is complicat- ed by clinical manifestations of disease and noncongestive heart fait- ure occurs with exertion. Lesser elevations of the level of blood pressure in asymptomatic persons can be modified by drug therapy, but exercise capacity is not improved.
Since administration of nitroglycerin improves work capacity and cardiovascular performance of patients with coronary disease,’ we considered evaluation of the effects of chemotherapy on hypertensive patients important. Patients with established hypertension, referred for treatment, and asymptomatic healthy workers with increased blood pressure were tested in the course of antihypertensive therapy for changes in maximal oxygen intake and hemodynamic responses to graded levels of upright exercise. Protection against congestive heart failure, as r’eported in clinical studies,* was noted. Since elec- trocardiographic manifestations of myocardial ischemia were more frequent, the possible relation to myocardial infarction as a compli- cation of otherwise successful treatment emerges.*,3
Material and Methods
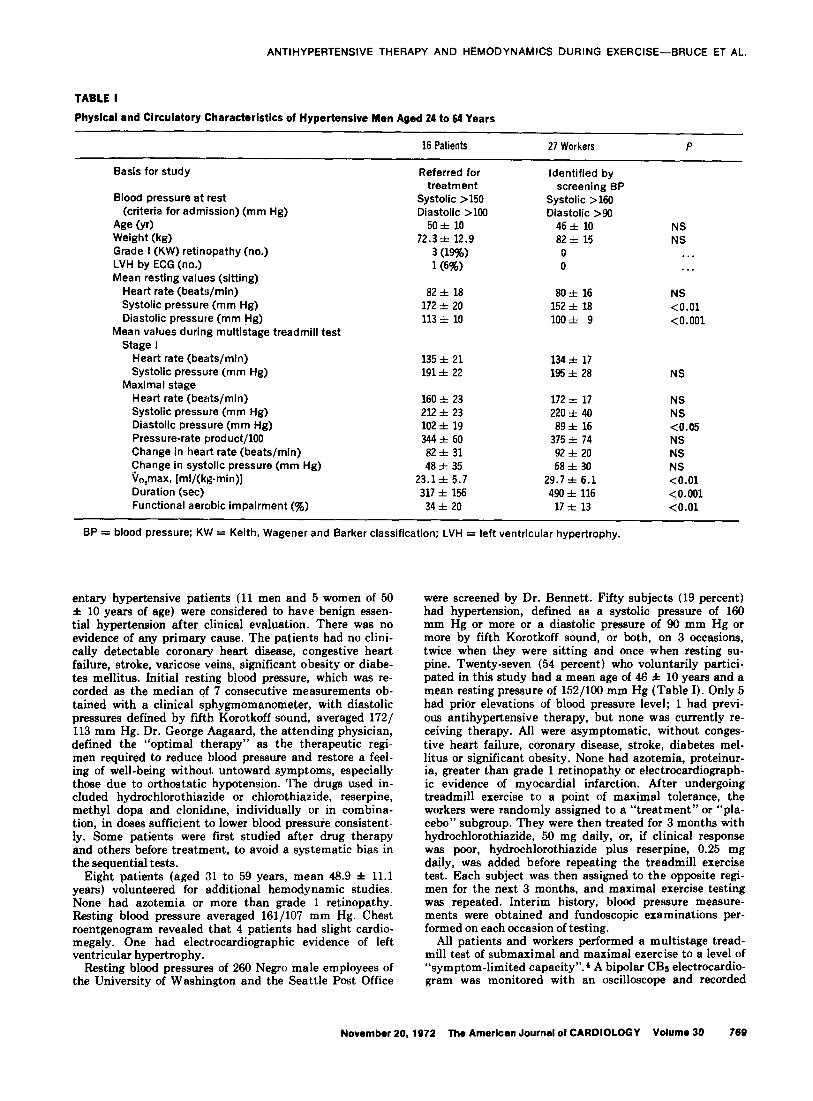
Table I shows the physical and circulatory characteristics of 16 clinical patients referred for treatment and studied by Dr. Eleady-Cole. These sed-
708 November 20,1972 The American Journal 01 CARDIOLOGY Volume 30
ANTIHYPERTENSIVE THERAPY AND HEMODYNAMICS DURING EXERCISE-BRUCE ET AL.
TABLE I
NS NS
NS
<O.Ol <O.OOl
NS
NS NS <0.05 NS NS NS <O.Ol <O.OOl <O.Ol
Physical and Circulatory Characteristics of Hypertensive Men Aged 24 to 64 Years
16 Patients 27 Workers P
Basis for study
Blood pressure at rest (criteria for admission) (mm Hg)
Age Or) Weight (kg) Grade I (KW) retinopathy (no.) LVH by ECG (no.) Mean resting values (sitting)
Heart rate (beats/min) Systolic pressure (mm Hg) Diastolic pressure (mm Hg)
Mean values during multistage treadmill test Stage I
Heart rate (beats/mln) Systolic pressure (mm Hg)
Maximal stage Heart rate (beats/min) Systolic pressure (mm Hg) Diastolic pressure (mm Hg) Pressure-rate product/100 Change in heart rate (beats/mm) Change in systolic pressure (mm Hg) Vo,max, [ml/(kg-min)] Duration (set) Functional aerobic impairment 6)
Referred for treatment
Systolic >150 Diastolic >lOO
50 f 10 72.3 f 12.9
3 (19%) 1(6%)
a2 f la 172 f 20 113 & 10
135 f 21 191* 22
160 f 23 2l2It 23 102 f 19 344+ 60 a2 + 31 48 f 35
23.1 f 5.7 317 f 156 34 * 20
Identified by screening BP
Systolic >160 Diastolic >90
46 f 10 a2 f 15 0 0
a0 z?z 16 152 f 18 loo* 9
134* 17 195k 28
172 +z 17 220 f 40 a9 f 16
375 z!z 74 92f 20 68& 30
29.7 f 6.1 490 f 116
17 f 13
BP = blood pressure; KW = Keith, Wagener and Barker classification; LVH = left ventricular hypertrophy.
entary hypertensive patients (11 men and 5 women of 50 f 10 years of age) were considered to have benign essen- tial hypertension after clinical evaluation. There was no evidence of any primary cause. The patients had no clini- cally detectable coronary heart disease, congestive heart failure, stroke, varicose veins, significant obesity or diabe- tes mellitus. Initial resting blood pressure, which was re- corded as the median of 7 consecutive measurements ob- tained with a clinical sphygmomanometer, with diastolic pressures defined by fiih Korotkoff sound, averaged 1721 113 mm Hg. Dr. George Aagaard, the attending physician, defined the “optimal therapy” as the therapeutic regi- men required to reduce blood pressure and restore a feel- ing of well-being without untoward symptoms, especially those due to orthostatic hypotension. The drugs used in- cluded hydrochlorothiazide or chlorothiazide, reserpine, methyl dopa and clonidine, individually or in combina- tion, in doses sufficient to lower blood pressure consistent- ly. Some patients were fiit studied after drug therapy and others before treatment, to avoid a systematic bias in the sequential tests.
Eight patients (aged 31 to 59 years, mean 46.9 * 11.1 years) volunteered for additional hemodynamic studies. None had azotemia or more than grade 1 retinopathy. Besting blood pressure averaged 161/107 mm Hp. Chest roentgenogram revealed that 4 patients had slight cardio- megaly. One had electrocardiographic evidence of left ventricular hypertrophy.
Besting blood pressures of 260 Negro male employees of the University of Washington and the Seattle Post Office
were screened by Dr. Bennett. Fifty subjects (19 percent) had hypertension, defined as a systolic pressure of 160 mm Hg or more or a diastolic pressure of 96 mm Hg or more by fifth Korotkoff sound, or both, on 3 occasions, twice when they were sitting and once when resting su- pine. Twenty-seven (54 percent) who voluntarily partici- pated in this study had a mean age of 46 f 10 years and a mean resting pressure of 152/100 mm Hg (Table I). Only 5 had prior elevations of blood pressure level; 1 had previ- ous antihypertensive therapy, but none was currently re- ceiving therapy. All were asymptomatic, without conges- tive heart failure, coronary disease, stroke, diabetes mel- litus or significant obesity. None had azotemia, proteinur- ia, greater than grade 1 retinopathy or electrocardiograph- ic evidence of myocardial infarction. After undergoing treadmill exercise to a point of maximal tolerance, the workers were randomly assigned to a “treatment” or “pla- cebo” subgroup. They were then treated for 3 months with hydrochlorothiazide, 50 mg daily, or, if clinical response was poor, hydrochlorothiazide plus reserpine, 0.25 mg daily, was added before repeating the treadmill exercise test. Each subject was then assigned to the opposite regi- men for the next 3 months, and maximal exercise testing was repeated. Interim history, blood pressure measure- ments were obtained and fundoscopic examinations per- formed on each occasion of testing.
All patients and workers performed a multistage tread- mill test of submaximal and maximal exercise to a level of “symptom-limited capacity”.’ A bipolar CBs electrocardio- gram was monitored with an oscilloscope and recorded
November 20.1972 The American Journal of CARDIOLOGY Volume 30 769
ANTIHYPERTEN~IVE THERAPY AND HEMODYNAMICS DURING EXERCISE-BRUCE ET AL.
TABLE II
Hemodynemic Characteristics Before and During Antihypertensive Therapy
Exercise
Before Antihypertensive Therapy (no. = 8)
Rest 1 2 3
During Antihypertensive Therapy (no. = 8)
- P Valuet Rest 1 2 3 P Valuet
A. Hypertensive Patients* -___
Work load (watts) 0 31+ 6 85 * 14 lO4z1~ 16 . . . 0 31+7 81 z!z 16 109 * 19 . . .
90, (ml/mm) 315 & 23 823 f 88 1443 i 107 1593 f 148 . . . 302 Z!I 36 854 & 67 1448 i 142 1548 f 247 NS ?TJ Vo, max 16 f 2 42 z!z 8 79 f 11 87 j, 11 . . . 15 * 3 42& 5 74 i 13 72~ 14 <O.Ol
Q (liters/min) 5.7zt 1.5 8.4ztz 1.2 11.9& 0.8 12.4zt 0.7 . . . 5.0 f 1.2 9.1+ 0.9 13.3zt 1.9 13.7 ziz 2.4 NS a-v 0, diff (ml/liter) 58 f 14 99 z!C 11 122 f 10 128 f 8 . . . 62zt 8 94zt-7 111 f 9 115 * 10 <O.OOl SV (ml) 64zt 11 78 f 10 86 f 7 84+8 . . . 59 f 11 81+ 11 97 f 13 95* 12 <0.02 HR (beats/min) 89 XIY 17 109 f 18 140 f 16 150 f. 16 . . . 84 f 12 114 f 14 138i21 144zt225 NS
S& P (mm Hg) 135 X!I 16 145 i 13 152 i 11 158 zk 10 . . . 121 IrI 9 131 i 15 144i 11 1401 13 <O.Ol E P (mm Hg) 15* 3 22* 3 31* 5 31*5 . . . 12* 2 18 f 3 27 z& 6 24 f 6 <O.OOl Est LVEDP (mm Hg) 10 f 2 14+ 2 21zt 3 21&3 . . . 8f2 11* 2 18 f 5 14 f 4 <O.OOl
SV/ti 4.6zrz 1.9 3.6zt 0.6 2.8& 0.3 2.7+ 0.4 . . . 5.1 f 1.1 4.5~tO.5 3.8ztl.O 4.0~1~0.5 <O.OOOl PR/lOO 118 z!z 26 155 f 25 2O6*31 234zt 30 . . . 99 zt 6 147 f 20 188 f 38 2O6z!z48 NS s R set (dyne cm-e) 1988 & 666 1375 f 341 988 f 83 938f 74 . . . 2554 zt 780 1425 zt 125 1103 f 132 1038 & 126 NS G R (dyne seccm+) 219 & 62 211 Z!G 41 205 i 28 199 * 30 ..* 197 * 40 160 + 28 165 f 50 147 * 33 .NS
STB&) lzt 58 -66 f 108 -122 f 141-124 z+z 138 . . . -14+ 30 -20 + 45 -41 C!Z 39 -61 f 53 NS
B. Hypertensive Workers*
Before Hypertensive Therapy (no. = 7) During Antihypertensive Therapy (no. = 7)
Work load (watts) 0 54 & 10 96 rt 19 125 f 31
00, (ml/min) 311 f 71 1088 f 168 1620 ZIX 283 1838 f 430 96 Vo, max 13* 3 45* 4 68z!z 8 76f 9 Q (liters/min) 5.1ztz 2.110.4& 2.0 13.2& 3.2 14.4& 3.6
(P<O.5) a-v OS diff (ml/liter) 63 f 11 105 f 9 123 zt 4 130 f 3 SV (ml) 61 Z!C 22 89 f 17 92 f 19 86 f 17 HR (beatsfmin) 89 i 18 118 i 18 145 i 16 165 f 23
S2 P (mm Hg) 127 f 18 145 z?z 28 158 z!z 19 fi P (mm Hg) llf 3 22 f 4 26zt 3
(P<O.o4) Est LVEDP (mm Hg) llf 2 20* 3 24+ 2
sv /PA 5.9zt 3.0 4.2f 1.1 3.6 ZII 1.0 (P<O .Ol)
PR/lOO 110 i 31 171 f 48 229 + 43 a R set cm (dyne -“) 2186 f 633 1147 f 337 1014 f 289 PA R set (dyne cm-‘) 193 f 74 169 f 37 165 f 47
166 z+z 13 31+ 6
27% 5
2.8 z!z 0.8 (P<O.O3) 272 f 42 964 + 231 176 f 41
(P<O.Ol)
STB (I1v) 46* 53 23& 43 -33zt 43 -59 f 59
. . . 0 55 f 11 95 f 21 125 + 31 . . .
. . . 292 * 48 1058 f 119 1497 zip 255 1748 f 357 <O.Ol . . . 12 f 2 44*7 62f 6 72+5 NS . . . 4.4+ 1.8 lO.lzt 1.9 12.4f 2.6 14.8+ 2.9 <O.Ol
. . . 57 f 7 104 ZIY 13 121 f 11 128 f 12 NS
. . . 69 f 27 94 f 17 94 f 18 91 YIZ 10 NS
. . . 79& 13 112 i 22 134 i 22 152 f 23 <O.OOl
. . . 127 f 17 149 zt 22 161 f 22 165 f 19 NS
. . . 14zt 3 25zt 3 26 f 4 28&t NS
. . . 13rt 2 22f 3 24f 3 25zt4 NS
. . . 5.1 f 2.1 3.7zt 0.5 3.6f 0.8 3.3+ 0.7 NS
. . . 99 f 22 165 f 32 212 f 26 247 ziz 25 <O.OOl
. . . 2658 f 1140 1214 f 365 1093 z& 359 lOO2 & 298 NS
. . . 223 & 69 MC29 173 f 46 170 +z 48 <0.02
. * . 60 f 56 54f 54 -22 f 53 -47 f 58 NS
C. Acute Effects of Nitroglycerin in Hypertensive Workers*
Work load (watts)
$0, (ml/min) % Vp, max
Q (liters/min)
a-v OI diff (ml/liter) SV (ml) HR (beats/min)
s P (mm Hg) PA P (mm Hg) Est LVEDP
Without Antihypertensive Therapy (no. = 6) With Antihypertensive Therapy (no. = 5)
. . . 60 f 14 1OO+20 131+ 32 . . . . . . 55 f 11 95 f 21 125 f 35 . . .
. . . 1112 +z 212 1614 i 346 1943 z!z 450 NS . . . 980 f 230 1545 f 310 1823 f 410 NS
. . . 46+6 66*7 79zt 5 NS . . . 38*4 60 zrz 7 71+5 NS
(P<O.O5) . . . 10.3+ 2.4 13.0+ 3.5 14.5+ 3.6 NS . . . 9.2zt 2.4 13.6 f 3.0 14.4 f 3.5 NS . . . 111 f 10 126 f 7 134 z?z 6 <O.Ol . . . 108 f 6 115 f 11 l28zr111 NS . . . 79* 19 87 f 19 84+ 16 <0.02 . . . 76 f 21 94 f 14 86 f 11 <0.05 . . . 137 f 13 150 f 17 174* 14 <O.Ol . . . 123 -I 21 142 f 18 160 f 21 <O.OOl
. . . 133 f 13 150 * 12 155 f 15 <O.Ol . . . l28zt 18 146+20 145 f 24 <O.OOl
. . . 16+ 5 21* 3 25 I!.Z 5 <O.OOl . . . 20* 4 24z?z 5 24z!z 4 <O.OOl
. . . 15 f 3 20* 2 22 f 4 <O.OOl . . . 18f 3 22rt 4 22+ 3 <O.OOl
(continued)
770 November 20,1972 The American Journal of CARDIOLOGY Volume 30
ANTlHYPERTENSIVE THERAPY AND HEMODYNAMICS DURING EXERCISE--BRUCE ET AL.
TABLE II (continued)
Hemodynamic Characteristics Before and During Antihypertensive Therapy
Exercice
Before Antihypertensive Therapy (no. = 8) During Antihypertensive Therapy (no. = 8) .--_ ~_._
Rest 1 2 3 PValuet Rest 1 2 3 P Valuet --. -. -.~ ---
SV/PA . . . 4.2f 1.0 3.6f 1.0 2.8& 0.7 <O.OOl . . . 3.9zt 1.3 4.0 f 0.8 3.7 + 0.6 NS
(PCO.05) PR/lOO . . . 17lk 48 224 f 34 268zk 23 NS . . . 155 +I 28 205 I 25 229 * 37 <O.Ol % R (dyne set cm -6) . . . 1090 f 280 985 k 274 898 + 258 NS . . . 1195 f 447 905 rt 291 844 f 260 NS l%R(dyneseccm-6) . . . 134f 49 139 t 44 141f 46 <O.OOl . . . 184~1176 138 z?z 44 141+ 47 <0.02
STB Gtv) . . . 3* 29 -9 f: 37 -33zk 87 NS . . . 20f 27 -15zk 25 -121k 84 NS
* Age range 35 to 55 years (mean 45.8).
i Pvalue in A and B refers to probability of difference between means for all periods of observation of treated patients with chronic
hypertension vs. untreated control subjects; in C, Pvalue refers to probability of difference between means for all periods of observa- tion with and without nitroglycerin.
a-v Ot diff = arterlovenous oxygen difference; HR = heart rate; LVEDP = left-ventricular end-diastolic pressure; NS = not significant. % P = pulmonary-arterial pressure; fi R = pulmonary-arterial resistance; PR = pressure-rate product (see text); 0 = cardiac out- put; $% P = mean systemic-arterial pressure; SA R = mean systemic-arterial resistance; STB = S-T segment at 50 to 69 msec after nadir of S; SV = stroke volume; 90, = oxygen consumption per minute.
directly on paper at 1 minute intervals for immediate qualitative assessment of electrocardiographic changes. Magnetic tape recordings were subsequently averaged by computer for 100 consecutive S-T segment responses at selected intervals. Methods are recorded elsewhere.s One minute samples of expiratory air were collected during the final 2 to 4 minutes of exercise; oxygen intake was calcu- lated from the volume of expired air and concentrations of oxygen, with and without absorption of carbon dioxide.* Blood pressure was recorded with a clinical sphygmoma- nometer while the subject sat at rest before exercise, 2 l/2 minutes later at the lowest work load of exercise (1.7 miles/hour, 10 percent gradient), and immediately after maximal exercise, while sitting. After resting.for 30 to 40 minutes, most hypertensive workers were given nitroglyc- erin, 0.4 mg sublingually, and retested for possible changes in cardiovascular performance.
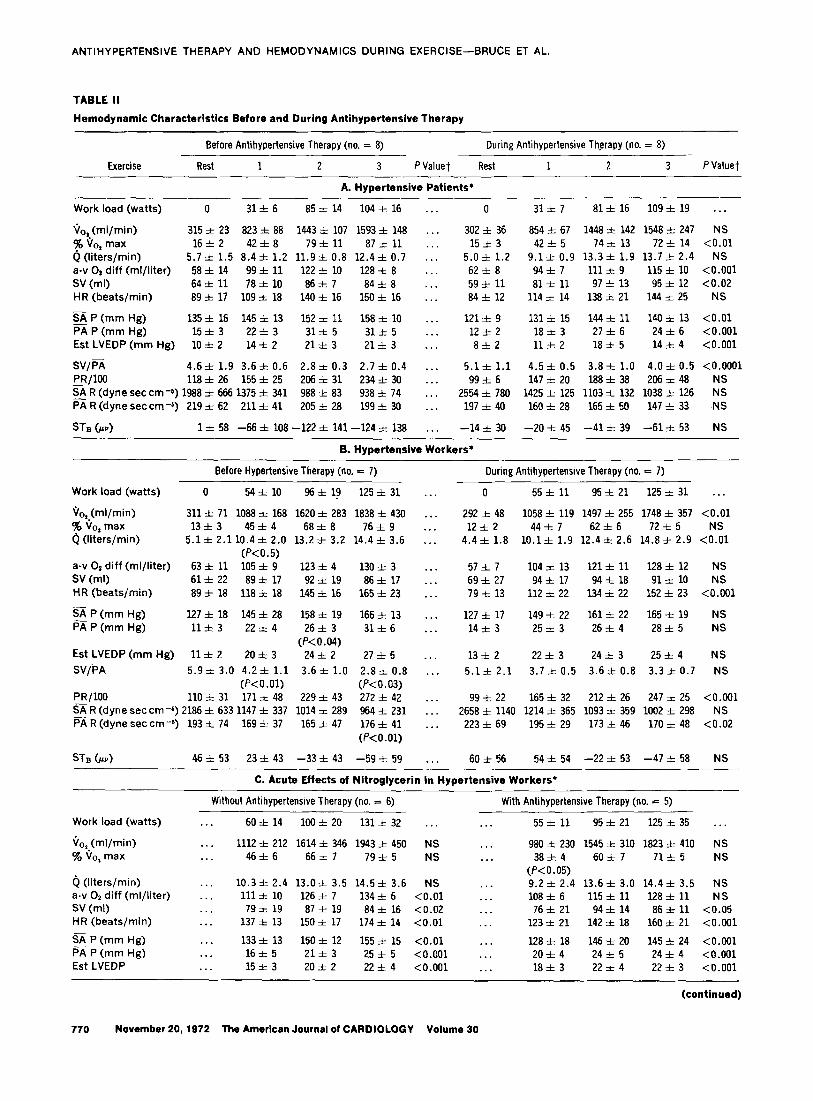
Eight patients and 7 workers participated in hemody- namic studies at rest and at graded levels of submaximal work loads on a bicycle ergometer. Right heart catheteri- zation was performed percutaneously with either a poly- vinyl catheter or a Swan-Ganz catheter inserted into an antecubital vein and advanced, with pressure monitoring, into the main pulmonary artery.6 Another catheter was introduced percutaneously into either the radial or the brachial artery. Zero pressure levels were adjusted to the fourth intercostal space at the mid-clavicular line ante- riorly. Pulmonary and systemic arterial pressures were re- corded with Statham pressure transducers, Honeywell carrier amplifiers and a direct-writer oscillograph. Mean arterial pressure was derived by a second-order low-pass filter with a 0.16 Hz cut-off frequency.
Pressures and direct Fick cardiac output determinations were obtained during the minute of rest and of upright exercise at 43 and 79 percent of individually measured maximal oxygen intake in patients, and at 45, 68 and 76 percent of maximal oxygen intake in workers, as described previously.7 Work loads 1 and 2 continued for 5 to 7 min- utes and work load 3 for 4 minutes. The subjects rested
for 20 minutes between the fit 2 work loads, and for 30 minutes before the last work load. After resting another hour, the hypertensive workers received nitroglycerin, 0.4 mg sublingually, and repeated the same exercise proce- dure.
Left ventricular end-diastolic pressure was estimated from mean pulmonary arterial pressure and stroke volume by regression equation (estimated left ventricular end- diastolic pressure = [mean pulmonary arterial pressure + 1.33 - 0.05 stroke volume)/1.34).s Hemodynamic after- load on myocardial metabolism was assessed by product of heart rate and mean systemic arterial pressure/lOO. Afterload was overestimated whenever peripheral vasodi- lation, induced by drug therapy, redistributed blood vol- ume into peripheral vessels. As a consequence, diastolic filling volume and pressure, as well as the systolic wall tension of the left ventricle, diminished in the upright posture. Ratio of stroke volume to mean pulmonary arte- rial pressure revealed changes in ventricular compliance in diastole and myocardial contractility in systole. (None of the subjects had pulmonary hypertension, mitral ste- nosis or pericardial constriction to affect pulmonary arterial pressure.)
Plotting the sequential relation of stroke volume to mean pulmonary arterial pressure and product of heart rate and mean systemic arterial pressure/100 at rest and graded levels of upright exercise showed a curve of left ventricular function; effects of drug therapy were mani- fested by a displacement of this function curve.
Differences in variables were evaluated by the unpaired t test; changes resulting from therapy were assessed by the paired t test.
Results
Major responses during the experimental condi- tions of selection and study are summarized in Table II, A to C, and Figures 1 to 5.
Changes in circulation and aerobic capacity at maximal exercise: Treatment of patients de-
November 2O,lg72 The American Journal oi CARDIOLOGY Volume 30 771
ANTIHYPERTENSIVE THERAPY AND HEMODYNAMICS DURING EXERCISE-BRUCE ET AL.
I Patlents (N=16-12) 1 Workers CN:27.18) 1
I” ; 200
r
2150 :
&
VlOO
E 5
2 50 In
0
t With Sphygmomanometer . Multistage TreadmIll
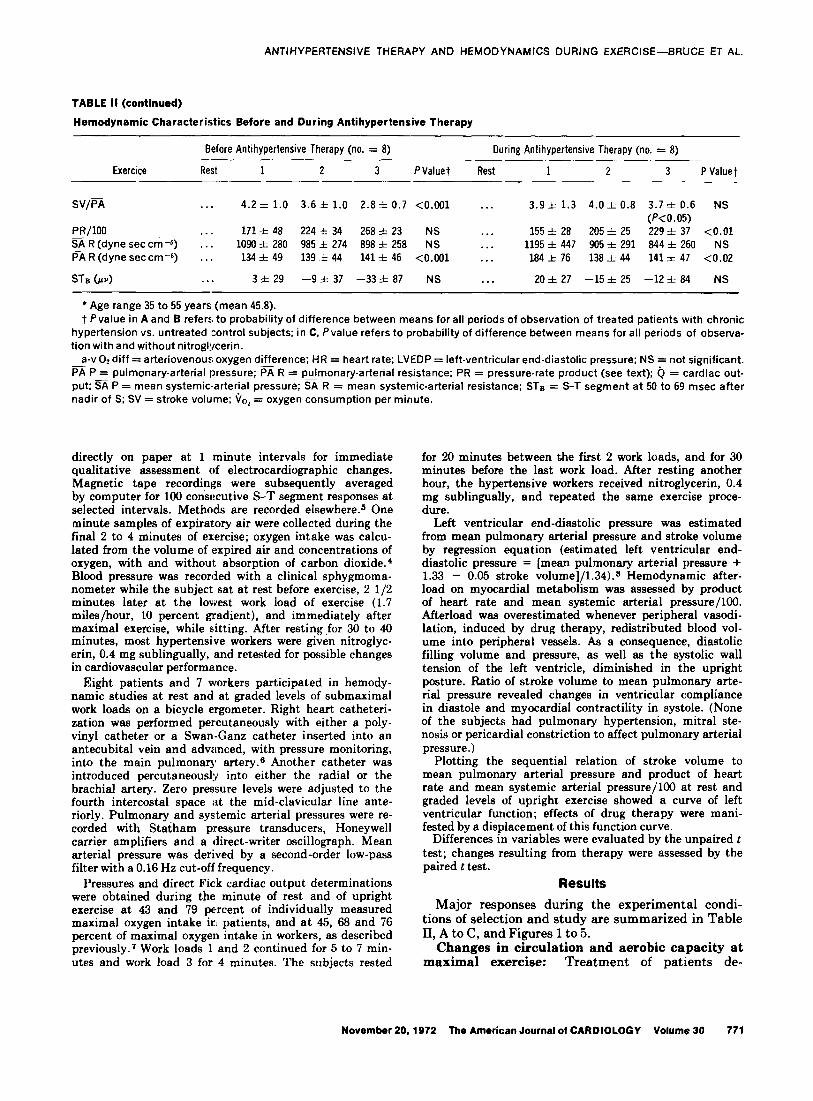
FIGURE 1. Effects of long-term antihypertensive therapy for 3 months on systolic (S) and diastolic (D) systemic arterial pres- sures at rest and during maximal exercise in patients and work- ers. Changes in mean talues indicated.
Patients
represented by -0, with probability
Workers
Dura tlon
- 0 .5 . 1.5 2.0 90, max L/mln
I 0 2 4 6 6 10
Minutes
0 .5 1.0 1.5 2.0 2.5 i/o2 max L/mln
FIGURE 2. Effects of chronic antihypertensive therapy on ex- ercise capacity. Graph shows duration of exercise and oxygen intake during maximal exercise in patients and workers.
! ‘f@ Antihypertensive 5,
(N=lB)
Rest Max Exe;
n-10
FIGURE 3. Effects of acute nitroglycerin therapy in workers with hypertension. Graph shows effects of nitroglycerin on sys- temic pressures, both systolic (S) and diastolic (D) at rest and during maximal exercise. The reductions in pressure are insig- nificant when workers are already receiving antihypertensive therapy.
creased systolic and diastolic blood pressures at rest (P <O.OOl) but not during maximal exercise (Fig. 1, Table I). Systolic and diastolic pressures in workers decreased with antihypertensive therapy both at rest and during maximal exercise (P CO.001).
Heart rates of patients were unchanged with ther- apy, whereas workers showed a slight reduction in resting heart rate with therapy (P cO.05). The pres- sure-rate product decreased significantly in both groups at rest and during submaximal and maximal exercise (Table II, A and B).
Mean duration of multistage treadmill exercise in- creased significantly (from 5.23 to 6.60 minutes) in patients (P <O.OOl) but insignificantly (from 8.17 to 8.65 minutes) in workers (Fig. 2). Maximal oxygen intake increased slightly in patients (P cO.05) with drug therapy, but remained at the same higher level in workers (Fig. 2).
Acute effects of nitroglycerin on responses to maximal exercise: Nitroglycerin given to workers reduced systolic and diastolic blood pressures (P <O.OOl) (Fig. 3) and increased maximal oxygen in- take from 29.7 to 31.5 ml/(kg-min) (P <O.OOl) (Table IIC).
Although heart rate was faster (P X0.001), pres- sure-rate product was unchanged at rest and de- creased with exercise. Duration of exercise increased slightly from 8.17 to 8.73 minutes (P <0.05), whereas functional aerobic impairment decreased from 17 to 11 percent (P <O.OOl). Nitroglycerin with chronic antihypertensive therapy decreased systolic pressures only (P <O.OOl), but neither resting nor maximal heart rate changed. Duration of exercise increased by only 12 seconds; functional aerobic impairment di- minished 2 percent.
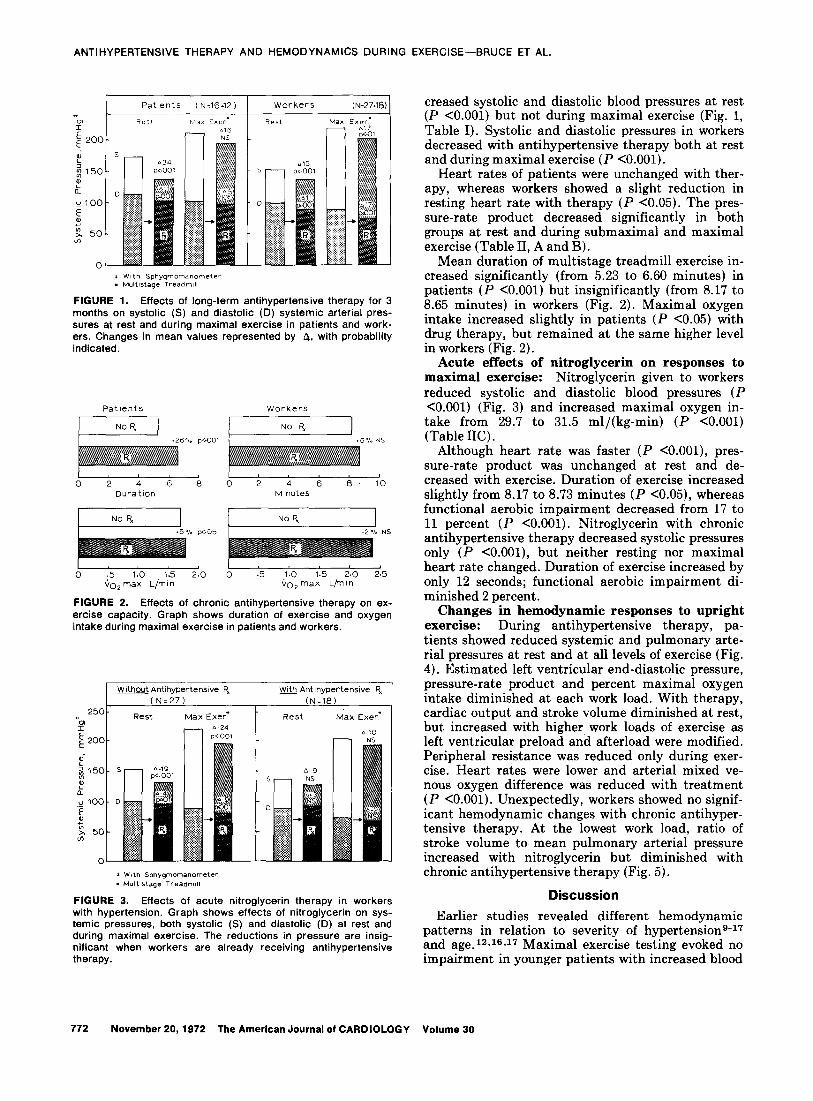
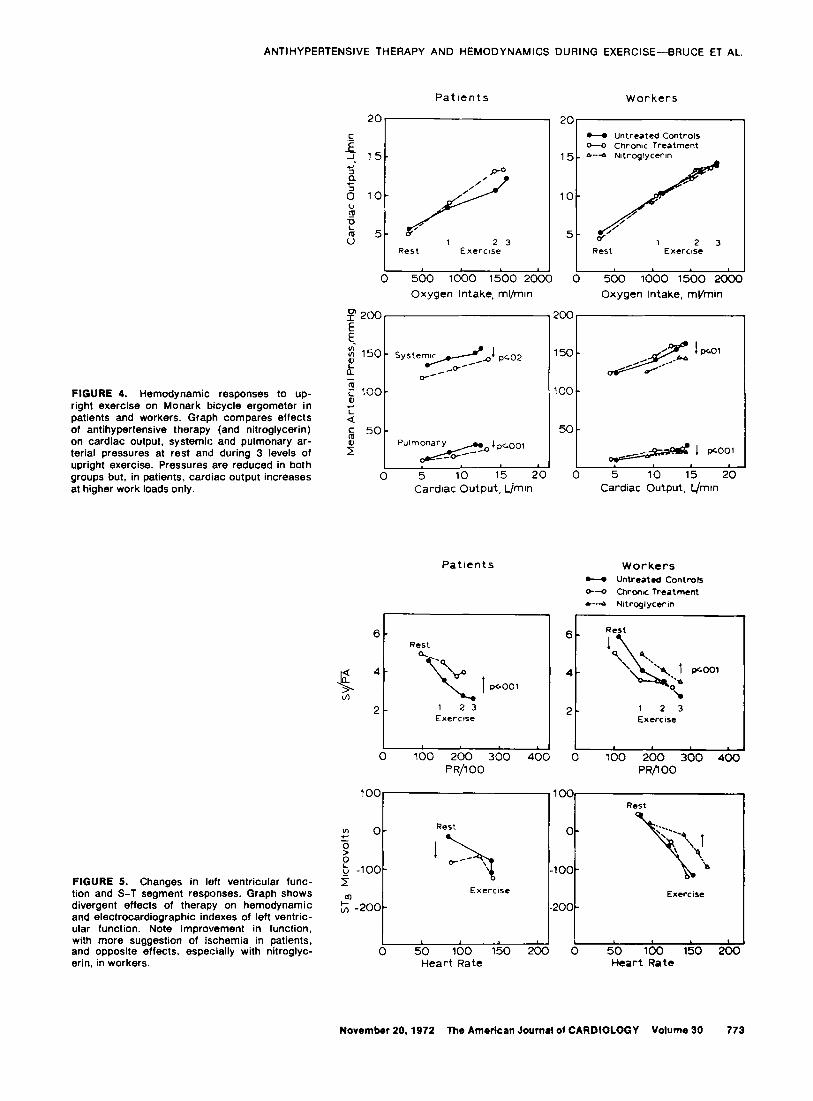
Changes in hemodynamic responses to upright exercise: During antihypertensive therapy, pa- tients showed reduced systemic and pulmonary arte- rial pressures at rest and at all levels of exercise (Fig. 4). Estimated left ventricular end-diastolic pressure, pressure-rate product and percent maximal oxygen intake diminished at each work load. With therapy, cardiac output and stroke volume diminished at rest, but increased with higher, work loads of exercise as left ventricular preload and afterload were modified. Peripheral resistance was reduced only during exer- cise. Heart rates were lower and arterial mixed ve- nous oxygen difference was reduced with treatment (P <O.OOl). Unexpectedly, workers showed no signif- icant hemodynamic changes with chronic antihyper- tensive therapy. At the lowest work load, ratio of stroke volume to mean pulmonary arterial pressure increased with nitroglycerin but diminished with chronic antihypertensive therapy (Fig. 5).
Discussion
Earlier studies revealed different hemodynamic patterns in relation to severity of hypertensions-17 and age.12J6,17 Maximal exercise testing evoked no impairment in younger patients with increased blood
772 November 20,1972 The American Journal of CARDIOLOGY Volume 30
ANTIHYPERTENSIVE THERAPY AND HEMODYNAMICS DURING EXERCISE-BRUCE ET AL.
FIGURE 4. Hemodynamic responses to up- right exercise on Monark bicycle ergometer in patients and Workers. Graph compares effects of antihypertensive therapy (and nitroglycerin) on cardiac output, systemic and pulmonary ar- terial pressures at rest and during 3 levels of upright exercise. Pressures are reduced in both groups but. in patients, cardiac output increases at higher work loads only.
FIGURE 5. Changes in left ventricular func- tion and S-T segment responses. Graph shows divergent 8ff8CtS Of therapy on hemodynamic and electrocardiographic ind8X8S of left ventric- ular function. Note improvement in function, with more suggestion of ischemia in patients, and opposite effects, especially with nitroglyc- erin. in workers.
Patrents Workers
- UntWJted CO”trOlS -0 Chrome TreJt”Wnt
I I I I 0 500 1000 1500 2CCC 0 5Dcl 1000 1500 2DCD
Oxygen Intake, ml/mm Oxygen Intake, mvmin
I”200 200
E
$ 150 - Systemic Pco2 150 - t /---9
,_/c- /&%I~’
m $ too- 100 -
r Q
$ 50- 5o 5 P”‘m~‘P~ool j 1 pcoo,
0 5 10 15 20 0 5 10 15 20
Cardiac Output, l_/mln Cardrac Output, L/mm
Patrents Workers v uP’,tI-tJtd Controls
W--o Chronr TreJtmcnt
6-d Nltroglycerln
6- 6- Rest
Rest 1
4- *oo’
2- 1 2 3 EXeKlSe Exercise
1 0 100 200 300 200 300 400
PR/lOO PR/lOO
100 100 Rest
n Rest
5 O-
b I b -lOO- 5
EXerClSc m Exercrse
L -2oo- -200 -
0 L
50 100 150 200 0 50 loo 150 200 Heart Rate Heart Rate
November 20.1972 The American Journal ot CARDIOLOGY Volume 30 773

ANTIHYPERTENSIVE THERAPY AND HEMODYNAMICS DURING EXERCISE-BRUCE ET AL.
pressures and showed progressively greater impair- ment in older patients with higher levels of hyper- tension, left ventricular hypertrophy, retinopathy and coronary heart disease.l? Sannerstedt16 found that hypertensive patients with retinopathy had a greater increase in arterial pressure and peripheral resistance and a smaller increase in cardiac output with exercise in the upright posture. In our study, ‘both workers and patients exhibited the divergent hemodynamic patterns noted in earlier reports. Ini- tially, the slightly younger, asymptomatic workers had lower systolic and diastolic pressures at rest and with maximal exercise, greater exercise capacity, longer exercise duration and greater maximal cardiac output. In workers, at a work load averaging 78 per- cent of maximal oxygen intake, values for arteriove- nous oxygen difference were 8 ml/liter lower and those for cardiac output and heart rate 2.5 liters/min and 25 beats, respectively, higher than values ob- served in patients. There was a greater difference in cardiac output ‘(21 percent) than in arteriovenous oxygen difference (6.5 percent), and a greater differ- ence in heart rate (18 percent) than in stroke volume (7 percent). In both groups, the greatest stroke vol- ume was observed at an intermediate work load level, and this volume diminished slightly as the lim- its of ventricular compliance and contractility were exceeded at the highest work load level.
In both groups, chronic antihypertensive therapy significantly reduced systemic and pulmonary arteri- al mean pressures. Although increased pulmonary arterial pressure in the supine position has been ob- served with exercise in older hypertensive patients,12 reduction of pulmonary arterial pressure with thera- py has not been reported to our knowledge. Estimat- ed end-diastolic pressure of the left ventricle showed
a statistically significant hemodynamic change with antihypertensive therapy, whereas the pressure-rate product at submaximal exercise diminished and the stroke volume to mean pulmonary arterial pressure ratio increased. Since only the cardiac output of treated patients increased at work loads of 70 to 80 percent of maximal oxygen intake, this response rep- resented improved cardiovascular efficiency. The finding suggests greater left ventricular diastolic compliance and greater contractile force during antihypertensive treatment. Functional aerobic im- pairment also diminished toward normal as duration of exercise lengthened.
Curiously, the workers showed little benefit from antihypertensive therapy. Oxygen intake, cardiac output and heart rate decreased slightly. The stroke volume to mean pulmonary arterial pressure ratio was slightly lower at rest and at moderate work. The condition of the workers was not refractory, because greater changes were observed acutely with nitroglyc- erin, except when the workers were already receiv- ing chronic antihypertensive therapy. Nevertheless, myocardial ischemia, especially when treatment was combined with nitroglycerin, increased as pressure decreased.
Since these studies document differences in hemo- dynamic responses to exercise between the earliest and intermediate phases of hypertensive cardiovas- cular disease, the reported protection of antihyper- tensive therapy in patients against congestive heart failure is more readily understood.2
Acknowledgment We acknowledge the clinical supervision and manage-
ment of the hypertensive patients by Dr. George Aagaard, and thank Alison Ross for editing and Jacqueline Eddy for typing the manuscript.
References
1. Detry JMR, Bruce RA: Effects of nitroglycerin on “maxi- mal” oxygen intake and exercise electrocardiogram in coro- nary heart disease. Circulation 43: 155-l 63, 1971
2. Veterans Administration Cooperative Study’Group on Antihy- pertensive Agents:
3. Smith WM, Datato AN, Galluzzi NJ, et al: The evaluation of
Effects of treatment on morbidity in hy-
antihypertensive therapy cooperative clinical trial method. I.
pertension. 2. Resu!ts in patients with diastolic. blood pres-
Double-blind control comparison of chlorothiazide, rauwolfia serpentina, and hydralazine. Ann Intern Med 61:829-846,
sure averaging 90 through 114 mmHg. JAMA 213:1143-
1964
1152.1970
4. Bruce, RA: Exercise testing of patients with coronary heart disease. Ann Clin Res 3:323-332. 1971
5. Bruce RA, Yarzarella JA, Jordan JW Jr, et al: Quantitation of QRS and ST segment responses to exercise. Amer Heart J 71:455-466.1966
measurement of effective renal blood flow and cardiac out- put in resting normal subjects and patients with essential hypertension. J Clin Invest 28:l O-l 7, 1949
10. Werko L, -Lageriof H:
11. Varnauskas E: Studies in hypertensive cardiovascular dis-
Studies on circulation in man;
ease with special reference to cardiac function. Stand J Clin Lab Invest 7:suppl 17:1-117, 1955
cardiac output and blood pressure in right auricle, right
12. Taylor SH, Donald KW, Bishop JM: Circulatory studies in hypertensive patients at rest and during exercise. Clin Sci
ventricle, and pulmonary artery in patients with hypertensive
16:351-376,1957
cardiovascular disease. Acta Med Stand 133:427- 436, 1949
6. Swan HJC, Ganz W, Forrester J, et al: Catheterization of the heart in man with use of a flow-directed balloon-tipped catheter. New Eng J Med 283:447-451, 1971
7. Detry JMR, Rousseau M, Vandenbroucke G, et al: In- creased arteriovenous oxygen difference after physical training in coronary heart disease. Circulation 44:109-l 18. 1971
8. Harvey RM, Enson Y: Pulmonary vascular resistance. Ad- vances Intern Med 15:73-93, 1969
9. Bolomey AA, Michie AJ, Michie C, et al: Simultaneous
13. Rowe GG, Castiiio CA, Maxwell GM, et al: A hemodynamic study of hypertension including observations on coronarv blood flow.Ann Intern Med 54:405-412, 1961
14. Finkielman S, Worcel M, Agrest A: Hemodynamic patterns in essential hypertension. Circulation 31:356-368, 1965
15. Beiio CT, Bevy RW, Harakal C: Varying hemodynamic pat- terns in essential hypertension. Amer J Med Sci 250:24-35. _ 1965
16. Sannerstedt R: Hemodynamic findings at rest and during exercise in mild arterial hypertension. Amer J Med Sci 258:70-79,1969
17. Wong HE, Kasser IS, Bruce RA: Impaired maximal exer- cise performance with hypertensive cardiovascular disease. Circulation 39:633-638, 1969
774 November 20,1972 The American Journal of CARDIOLOGY Volume 30