diabetes voice online - may 2015
DESCRIPTION
In this first digital edition of Diabetes Voice, our contributors ask and provide meaningful points for fostering and nurturing healthy futures in a world that is combating the challenge of preventing and managing diabetes.TRANSCRIPT
Diabetes VoiceONLINE
GLOBAL PERSPECTIVES ON DIABETES May 2015
IN THIS ISSUE:Tackling childhood obesity in India
WDC15: improving outcomes in person-centred careShaping the future of diabetes prevention and education

Diabetes Voice Online - May 2015
2
30 November – 4 December
International Diabetes Federation Promoting diabetes care, prevention and a cure worldwide
Editor-in-Chief: Rhys WilliamsEditor: Elizabeth SnoufferEditorial Assistant: Lorenzo PiemonteAdvisory Group: Pablo Aschner (Colombia); Ruth Colagiuri (Australia); Maha Taysir Barakat (United Arab Emirates), Viswanathan Mohan (India); João Valente Nabais (Portugal); Kaushik Ramaiya (Tanzania); Carolyn Robertson (USA)
All correspondence should be addressed to:
International Diabetes Federation Chaussée de La Hulpe 166, 1170 Brussels, Belgium Tel: +32-2-538 55 11 | Fax: +32-2-538 51 [email protected]
Diabetes Voice is available online at www.diabetesvoice.org
Cover photo: © Bartosz Hardyniak, istockphoto.com
© International Diabetes Federation, 2015 - All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means without the written prior permission of the International Diabetes Federation (IDF). Requests to reproduce or translate IDF publications should be addressed to [email protected].
The information in this document is for information purposes only. IDF makes no representation or warrantires about the accuracy and reliability of any content in the document. Any opinions expressed are those of their authors, and do not necessarily represent the views of IDF. IDF shall not be liable for any loss or damage in connection with your use of this document. Through this document, you may link to third-party websites, which are not under IDF’s control. The inclusion of such links does not im-ply a recommendation or endorsement by IDF of any material, information, products and services advertised on third-party websites, and IDF disclaims any liability with regard to your access of such linked websites and use of any products or services advertised there. While some information in Diabetes Voice is about medical issues, it is not medical advice and should not be construed as such.
News in Brief 3
World Diabetes Congress 2015: Education and Integrated Care Stream 6 Defining roles and improving outcomes in person-centred careUnn-Britt Johansson
Shaping the future of diabetes prevention and education 9Linda Siminerio
Tackling childhood obesity: a novel school-based programme in India 11Shailesh R. Deshpande, Unnikrishnan A.G., Tushima A. Mashelkar

News in Brief
The European Association for the Study of Diabetes (EASD) and the American Diabetes Association (ADA) have called for a review of how insulin pumps are approved for use and monitored once on the market, citing serious safety gaps in the current pre- and post-market regulatory systems of both the United States and the EU. The groups published a position statement on 16 March 2015, setting out healthcare-wide recommendations for “stimulating the adoption of a more rigorous, standardised and transparent approach to safety.” They believe better measures for averting, recording and re-sponding to device failures and user errors would improve
medical technology development and access. The work by the ADA/EASD Diabetes Technology Working Group is the out-come of an 18 month study of current standards, regulatory regimes and research needs related to insulin pump therapy.
http://care.diabetesjournals.org/content/38/4/716.full.pdf
ADA, EASD call for insulin pump safety
New global diabetes research programme in IndiaEmory University has collaborated with the Public Health Foundation of India, Madras Diabetes Research Founda-tion, All India Institute of Medical Sciences, and Aga Khan University to win a grant to set up one of nine centres of excellence between the US and a developing country, fun-ded by the National Institutes of Health and United Health Group. K. M. Venkat Narayan, global health professor in the Rollins School of Public Health at Emory University led the
initiative for the global diabetes research programme. Emo-ry University is currently expanding the collaboration with the UK London School of Hygiene and Tropical Medicine, the Public Health Foundation of India, and All India Institute of Medical Sciences to create a global chronic disease centre headquartered in New Delhi. The launch of the Center for Control of Chronic Conditions (4C) in New Delhi occurred on April 8, 2015.
Highest proportion of type 2 diabetes in younger adultsSingapore has the highest proportion of young people with type 2 diabetes across nine Asian territories, ac-cording to a study by the Asian Diabetes Foundation. The two-year study polled people living with diabetes from Singapore, Thailand, China, the Philippines, Hong Kong, India, South Korea, Taiwan and Vietnam, and found that in Singapore three in 10 people had diabetes before the age of 40, the highest proportion with younger people. Ap-proximately 498,190 people in Singapore live with type 2 diabetes, and glycaemic control is considered a challenge for many. “Diabetes has no symptoms. So when you are young,
you don’t really think it’s a problem because there are no symptoms, you don’ t experience pain and you are not aware of its complications,” Dr. Ben Ng, consultant physician at Mount Elizabeth Novena Specialist Medical Centre told Channel NewsAsia.
3
Diabetes Voice Online - May 2015

SMART2D to help reduce hardest hitSMART2D (self-management and reciprocal learning for the prevention and management of type 2 diabetes) is a four-year collaborative research project between institutions in South Africa and Uganda, Belgium, Sweden and Finland to develop and test new approaches to substantially reduce type 2 dia-betes among populations in low-, middle- and high-income countries. The new initiative will conduct studies in three settings: a rural village setting in Uganda, an urban town-ship in South Africa and vulnerable urban immigrant popula-tions in Stockholm, Sweden. The overall aim is to strengthen capacity for the treatment and prevention of type 2 diabe-tes through proven strategies such as task-shifting and
expanding care networks. It is estimated that 41.5 million people have diabetes in sub-Saharan Africa. Globally, ap-proximately 387 million people have diabetes. This number is expected to jump to 592 million by 2035, and by 2030 it will become the seventh leading cause of death. According to those projections, sub-Saharan Africa is going to be hardest hit, said Professor Andre Kengne, director of the Non-Com-municable Diseases Research Unit at the South African Medical Research Council. “The global occurrence is marked by regional disparity. South Africa will be the driver of the epidemic in the region.”
Discovery: detecting type 1 diabetes earlierDoctors may be able to detect type 1 diabetes in children before they exhibit any symptoms of the disease, new re-search from Sweden shows. Scientists taking part in The En-vironmental Determinants of Diabetes in the Young (TEDDY) project have discovered four markers, or autoantibodies, in the blood of the study’s participants that make it possible to detect the disease earlier, meaning that treatment can also start earlier.
Type 1 diabetes occurs when beta cells in the pancreas are destroyed by autoantibodies. Once the beta cells are de-stroyed, the body can no longer produce insulin and cannot regulate blood glucose. Lead researcher, Ake Lernmark, from Sweden’s Lund University, says that measuring the levels of autoantibdodies in children’s blood indicates whether their immune system has started to attack beta cells. The TEDDY study, which is funded by the US National Institutes of Health
(NIH), involves 8,600 children - with an increased hereditary risk of type 1 diabetes - from Sweden, the United States, Germany and Finland. Lernmark’s work has revealed triggers of type 1 diabetes in children at a much earlier stage than was previously possible. The team now wants to test all four-year-old children in Sweden.The new discovery could lead to earlier treatment and lower doses of insulin used to treat the con-dition. It may even be possible for people with diabetes to postpone or avoid symptoms as the disease develops.
http://care.diabetes-journals.org/content/early/2015/02/03/dc14-2426.short
Most expensive place to live with type 2 diabetesThe US is the most expensive place to have type 2 diabetes, with an average lifetime price tag of US$283,000, according to a new study published in the journal PharmacoEconomics. Researchers at the UK University of East Anglia analysed 109 studies on the economic impact of type 2 diabetes and found
that costs are higher in the US, even compared with other countries with similar income levels.
http://link.springer.com/article/10.1007/s40273-015-0268-9
4
Diabetes Voice Online - May 2015
England launches programme to prevent type 2 diabetesAt the recent Diabetes UK Annual Professional Conference Simon Stevens, Chief Executive of NHS England, announced the launch of new evidence based type 2 diabetes preven-tion programme. At seven sites throughout the country, community-based initiatives will promote weight loss, encourage physical activity and cooking for better nutrition and will provide peer, telephone and online support. Several of the sites, for example Birmingham, Bradford and Salford,
have populations which are culturally and ethnically di-verse. The programme aims to replicate the results of the well known randomised controlled trials of intensive inter-ventions aimed at lifestyle changes and will serve as useful illustrations for the other parts of the UK – Scotland, Wales and Northern Ireland - of what can be achieved in community settings. Further information at: http://dx.doi.org/10.1136/bmj.h1400.
Delaying or preventing the onset of type 1 diabetesAt the same Diabetes UK (DUK) Annual Conference, four in-ter-related initiatives were announced funded jointly by DUK and JDRF. The first of these, led by Professor Mark Peak-man, based in London, will co-ordinate UK’s first trial of the use of a ‘vaccine’ aimed at modulating the immune response in children and young people living with or at a high risk of developing type 1 diabetes. Alongside this, Professor Colin Dayan, based in Cardiff, will develop a UK-wide network to enable more trials of immune-therapy to take place to wid-en the search for an effective intervention in this promising area. London-based Dr Tim Tree will head up a collaboration
of specialist laboratories tasked with determining exactly how these potential treatments influence the immune re-sponse while Professor Des Johnson, also based in London, will continue work to identify people newly diagnosed with type 1 diabetes who can be offered the opportunity to take part in clinical trials.
More information on these initiatives can be found at: http://www.diabetes.org.uk/About_us/News/Type-1-diabetes-vac-cine-possible-within-a-generation/
Ending childhood obesityThe World Health Organization’s Commission on Ending Childhood Obesity has released, for consultation, its Interim Report. The consultation period ends on 6 June. The Com-mission, co-chaired by Sir George Alleyne, Director Emeritus of PAHO and Dr Sania Nishtar, Founder of Heartfile, Pakistan, poses six questions to focus responses to its Report. These include: ‘Are there issues or strategies that have been over-looked?’ and ‘How can your sector/entity contribute to the proposed policy options to end childhood obesity?’ The text of the Interim Report and the comment form for responses
can be found at: www.who.int/end-childhood-obesity/inter-im-report-for-comment/en/.
5
Diabetes Voice Online - May 2015

The Education and Integrated Care Stream scheduled for the International Diabetes Federation (IDF) World Diabetes Con-gress Vancouver 2015 will consist of a group of sessions in different formats and will attempt to answer the question “How can people with diabetes effectively manage their own care and what is the role of healthcare professionals?”
Diabetes self-management education (DSME) is a critical part of care for all people with diabetes and those known to be at risk for developing the disease. The overall objectives included in DSME are to support informed decision-making, self-care behaviours, problem solving, and active collabora-tion with the health care team. In addition, it is important to improve clinical outcomes, general health status, and main-tain quality of life.1 At present, the majority of people with di-abetes and pre-diabetes have no access to structured DSME.
Today, person-centred care is recognised as an important as-pect of health care quality. The core of person-centred care is comprised of patient narratives and extended dialogue, to enable to the doctor and the person living with diabetes to build a successful and trusting partnership. Person-centred care recognises people with diabetes as equal partners in planning, developing and assessing ongoing care to assure the current therapy and DSME skills are most appropriate for needs. Findings from the DAWN study support a para-
digm shift from an acute care model to a person-centred integrated chronic care model, including self-management education and psychosocial support. In addition, a frequent-ly discussed topic is how to create more integrated care in order to ensure a personalised care organisation. The real challenge for all organisations is the movement from indi-vidual, person-centred moments to person-centred cultures.
During the Stream’s Open Forum, an interactive session will provide opportunities for participants to discuss what per-son-centred care looks like and how research findings can be translated to clinical practice highlighting personalised approaches to diabetes, shared decision-making, patient en-gagement and culturally relevant care. A symposium focus-ing on tackling the challenges of diabetes education in vul-nerable populations and for children and adolescents2 living with diabetes is included in the programme. There will also be opportunities for participants to interact in a workshop to share experiences and discuss how to integrate diabetes education into routine practice. Experts in the field of be-haviour change will focus on the topic of emotional and behavioural responses to the diagnosis of diabetes and prediabetes.
A field which continues to expand is e-Health. The number of
Defining roles and improving outcomes in person-centred care
Unn-Britt Johansson
WORLD DIABETES CONGRESS 2015: EDUCATION AND INTEGRATED CARE STREAM
6
Diabetes Voice Online - May 2015

publications evaluating web-based and mobile health inter-ventions is increasing rapidly. The term e-Health is described to characterise not only a technical development, but also a state-of-mind, a way of thinking, an attitude, a commit-ment for networked, global thinking, to improve health care locally, regionally, and worldwide by using information and communication technology. E-Health, supported by informa-tion and communication technology, is suggested to inspire patients to take an active part in their health care and the decision-making process, empower them, and support a person-centred approach.
A symposium on the current trends in this field will give the audience a hint of where it is going, how technology can be used, and will illustrate innovative health-care applications to prevent and treat diabetes. One of the symposia will pre-sent diverse research experiences from the field and how to use technology for online diabetes education.
Modern guideline development in diabetes care has fo-cused on supporting clinical practice recommendations with evidence. An example of one approach is to develop a full-process guideline which involves a full and systematic development of the clinical questions to be addressed, while also developing recommendations supported by complete and formal evidence searching and review, using primary sources.2 One symposium will present an overview of the various guidelines that have been developed in the field of diabetes and will demonstrate how to integrate the guide-lines into practice.
It is critically important that modern recommenda-tions for managing diabetes are closely aligned with individual characteristics such as functional status, presence of frailty and dependency, comorbidity profiles, and life expectancy. These characteristics influence treat-ment goals, the care/caring model and care/caring plan. The IDF global guideline for managing older people with type 2 diabetes is intended to support clinicians in order to provide a multidimensional integrated approach to the comprehensive management of diabetes in older
people.3 During one workshop, an interactive discussion will explore the key nursing and medical issues that occur in caring for older persons with diabetes.
Hypoglycaemia is a frequent adverse effect of diabetes treatment with insulin therapy and sulphonylureas. Effective education of patients and their relatives is fundamental in the treatment of diabetes mellitus. Fear of hypoglycaemia (FOH) can be a barrier to glycaemic control in type 1 diabe-tes. Findings from research highlight the complexity of FOH and a variety of factors need to be considered in order to un-derstand the psychological and clinical implications of FOH. A symposium about hypoglycaemia and tackling the issues is included in the programme.
Care for patients with diabetes requires a coordinated and collaborative team working in partnership with the patient. A multidisciplinary and interdisciplinary team is necessary to provide the long-term support needed by individuals with diabetes and their families. A symposium regarding team-based care and professional competencies is included in the programme. Examples for standards for professional educa-tion will be presented.
The key role that nutrition plays in supporting good health, prevention and effective diabetes treat-ment across the lifespan will be discussed in a
30 November – 4 December
7
Diabetes Voice Online - May 2015

symposium that begins with a fascinating presentation that explores epigenetics and the early prevention of obesity. Other topics in this symposium will focus on effective nu-trition strategies for prevention and treatment in children and adolescents, adults and older persons with, or at risk for diabetes.
The glycaemic index (GI) is utilised as a tool in diabetes nutrition management to greater or lesser degrees, de-pending on the area of the world and the nutrition guide-lines followed therein. The scientific evidence and practical application related to usefulness of the GI will be revisited in a spirited debate that will enable participants to re-ex-amine integration of GI into their clinical practices. Finally,
the Congress will have presentations from all IDF regions, and will highlight examples of innovative strategies from all over the world. The latest research and current trends in diabetes education and integrated care will be presented and discussed. Current IDF projects will be presented. There will also be patient narratives included in the programme, sharing stories and personal experiences of having diabe-tes and caring for diabetes. Moreover, the patient narratives are intended to address ideas, concerns and expectations regarding improving diabetes care.
About the Author
Unn-Britt Johansson is the lead for the Education and In-tegrated Care Stream for the World Diabetes Congress Vancouver 2015, and Professor at Sophiahemmet University and affiliated to Department of Clinical Sciences and Education, Södersjukhuset, Karolinska Institutet, Stockholm, Sweden.
References
1. The Global IDF/ISPAD Guideline for Diabetes in Childhood and Ado-
lescence. International Diabetes Federation 2013, http://www.idf.org/sites/default/files/attachments/ISPAD-LFAC-Pocketbook-final-2.pdf
2. A guide for clinical guideline development. International Diabetes Federation 2013, http://www.idf.org/webdata/docs/Guide-for-Guide-
lines.pdf
3. Managing older people with type 2 diabetes. International Diabetes Federation 2012.http://www.idf.org/sites/default/files/IDF-Guideline-for-older-people-T2D.pdf
8
Diabetes Voice Online - May 2015
Shaping the future of diabetes prevention and education
Linda Siminerio, RN, PhD
As the new chair of the National Diabetes Education Program (NDEP), a joint programme of the U.S. Department of Health & Human Services’ National Institutes of Health (NIH) and the Centers for Disease Control and Prevention (CDC), I am excited about the opportunity to work with NDEP in its mis-sion to improve diabetes treatment and outcomes, promote early diagnosis, and help people prevent or delay the onset of type 2 diabetes.
Progress in diabetes care and education
In recent decades, we have seen significant advances in diabetes medication therapies, insulin delivery options and glucose monitoring technology. Researchers and practitioners have moved the paradigm of nutrition therapy from strict dietary regimens to more flexible eating patterns. Research like the NIH-sponsored Diabetes Prevention Pro-gram (DPP) and Finnish Diabetes Prevention Study (DPS) demonstrated that type 2 diabetes can be prevented or de-layed. Major clinical trials have provided evidence about the effectiveness of glycaemic control for prevention of compli-cations such as retinopathy, nephropathy, neuropathy, and cardiovascular disease. Studies demonstrating the signifi-cant impact of self-management education and team-care on diabetes clinical and psychosocial outcomes are gaining widespread attention.
Challenges for health care providers
Despite progress, IDF reports that 387 million people have diabetes. That number is expected to rise to 592 million by 2035, when one in ten of the world’s population will have diabetes. Another 316 million are estimated to have impaired glucose tolerance or prediabetes which puts them at high risk for developing diabetes.1
Because diabetes is a disease that requires behaviour change and self-management, education and support are considered gold standards for prevention and care. In the US, the num-ber of people with prediabetes continues to escalate while disappointingly, the majority of adults already diagnosed never receives diabetes education. The NDEP realises that strategies must be developed to meet the needs of these growing populations.
Opportunities for prevention, education and care
Busy clinicians are faced with rising numbers of patients who are at risk for diabetes. Improved screening and tar-geted, ongoing diabetes prevention efforts are necessary if society is going to realise the benefits of therapies proven to delay or prevent the disease.
With respect to providing support for behaviour change, the
9
Diabetes Voice Online - May 2015
NDEP continues to draw attention to resources that address how to make and sustain important lifestyle changes, such as increasing activity, healthy eating, and coping with stress. The NDEP’s Diabetes HealthSense microsite is an online library of behaviour change resources for people at risk, people with dia-betes, community leaders and health care professionals alike.
The NDEP’s Practice Transformation resource serves as a guide to healthcare professionals as they work to trans-form the delivery of diabetes care most often delivered in primary care. One of the most promising components is the use of a team care approach. For example, profes-sionals such as diabetes educators, nurses, dieticians, pharmacists, peer leaders and community health work-ers, among others, are poised to coordinate care, shift provider workloads, and support patients in behaviour change.
The NDEP Strategic Plan advocates partner engagement in the broadest sense to meet the multifaceted needs of those living with diabetes. This means working with and through partners in the clinical setting, communi-
ty setting, at worksites, in schools – everywhere people with or at risk for diabetes live, work, play and worship.
Incorporating and applying team care and behaviour change support into a global approach to diabetes care and educa-tion are two essential steps to improving diabetes outcomes. It takes a village! As chair of the NDEP, I look forward to the opportunity to collaborate with our network of partners to create a better future for those affected by diabetes.
About the Author
Linda Siminerio, RN, PhD, former IDF Vice President is chair of the Na-
tional Diabetes Education Program (NDEP) in the US which is a part-
nership of the National Institutes of Health, the Centers for Disease
Control and Prevention, and more than 200 public and private organi-
sations. She is also the Director of the Adult Clinical Services Division
of the University of Pittsburgh Diabetes Institute.
References
1. IDF Diabetes Atlas Sixth Edition Update, International Diabetes
Federation 2014
10
Diabetes Voice Online - May 2015
Tackling childhood obesity: a novel school-based programme in India
Shailesh R. Deshpande, Unnikrishnan A.G., Tushima A. Mashelkar
Childhood obesity, which predisposes to type 2 diabetes and several other diseases, is an emerging health problem in India. Acknowledging that schools provide an effective plat-form to bring about behavioural change in children, Chel-laram Diabetes Institute has initiated a Childhood Obesity Prevention Programme in select schools of Pune city – the seventh largest city in India, 150 kilometres southeast of Mumbai. This interactive programme involves a set of topical slides on obesity, use of an audience response system and activities for secondary grade children, all providing a lively experience for learning. The promising results obtained so far offer scope for expansion of this programme on a wider scale.
Childhood obesity, which predisposes to type 2 diabetes and several other diseases, is an emerging health problem in In-dia. A recent multi-centric study of more than 38,000 chil-dren aged 8 to 18 years, found that 18.5% and 5.3% of the children were overweight and obese respectively.1
In another study in a city in South India, the overall preva-lence of overweight and obesity among adolescent school children was 9.9% and 4.8% respectively. The prevalence was higher among adolescents belonging to the high socioeconomic status group, those who had physical activity of less than one hour a day, watched television for more than
four hours a day and who ate chocolates daily.2 The risk fac-tors for childhood obesity, which include changing lifestyles, unhealthy diets and physical inactivity, are all on the rise in India.
Concerted action at the school level offers a lasting solu-tion to the problem of childhood obesity. Schools play a vital role in the upbringing of children and can therefore be an important setting for teaching healthy habits and helping children to better understand how to avoid health problems - including obesity - in their future lives.
This has been recognised by governments in countries with high rates of childhood obesity. For instance, the USA and the UK have been implementing countrywide campaigns like “Let’s Move” and “Change4life” which were developed to improve child nutrition and increase physical activity.3, 4 In India, however, there have only been sporadic efforts to address the issue of childhood obesity, especially at the school level.
In this context, Chellaram Diabetes Institute (CDI) has initi-ated a programme to address childhood obesity in the city of Pune in Western India.
CDI organised a conference on childhood obesity as part of a programme to mark World Diabetes Day 2013. The confe-
11
Diabetes Voice Online - May 2015
rence was well attended by principals, teachers, parents, students and healthcare providers in the city. The confer-ence group felt that obesity was certainly on the rise in chil-dren in Pune and the consensus was that schools can be an important medium for initiatives to address the problem of childhood obesity.
The Childhood Obesity Prevention Programme (COPP)
Subsequent to the discussions at the Pune Conference, CDI developed a programme called Childhood Obesity Preven-tion Programme (COPP) for implementation with secondary school students aged 12-16 years. Although still vulnerable to obesity, this age group was chosen because they are capa-ble of understanding the right messages to take appropriate action against obesity.
COPP involves an interactive PowerPoint presentation divided into five modules:
1. Definition and measurement of obesity2. Facts about obesity3. Causes, effects and contributory factors4. Nutritional management related to obesity5. Interventions to prevent and treat obesity
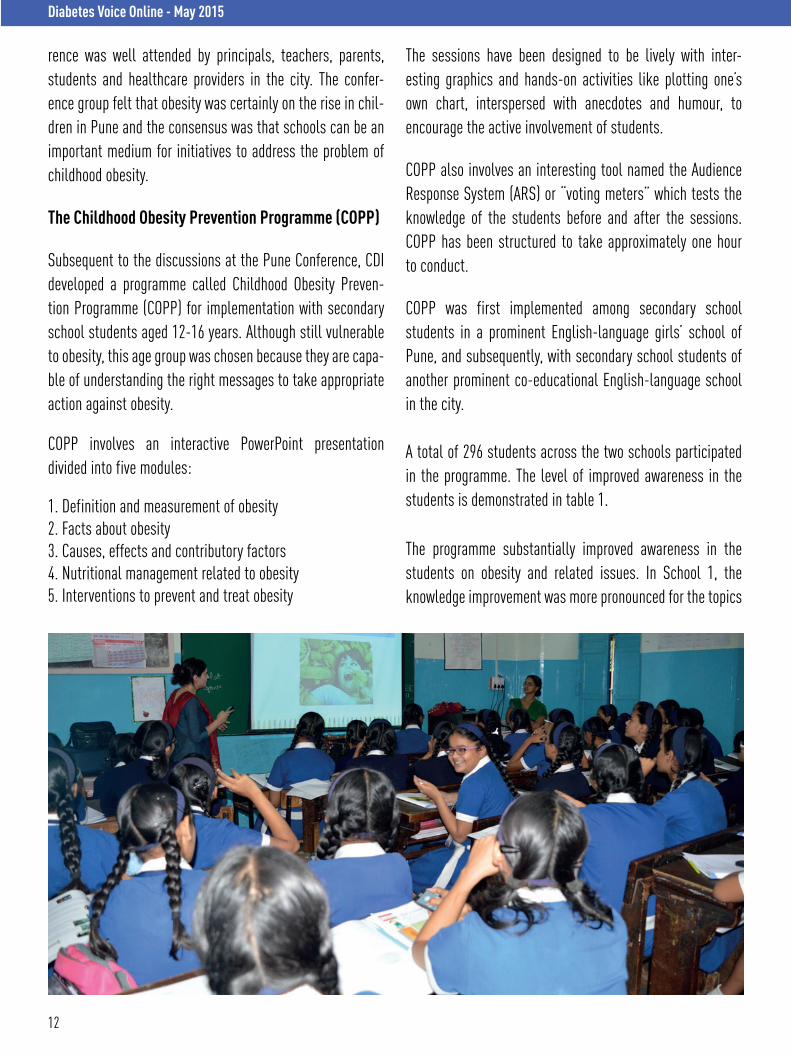
The sessions have been designed to be lively with inter-esting graphics and hands-on activities like plotting one’s own chart, interspersed with anecdotes and humour, to encourage the active involvement of students.
COPP also involves an interesting tool named the Audience Response System (ARS) or “voting meters” which tests the knowledge of the students before and after the sessions. COPP has been structured to take approximately one hour to conduct.
COPP was first implemented among secondary school students in a prominent English-language girls’ school of Pune, and subsequently, with secondary school students of another prominent co-educational English-language school in the city.
A total of 296 students across the two schools participated in the programme. The level of improved awareness in the students is demonstrated in table 1.
The programme substantially improved awareness in the students on obesity and related issues. In School 1, the knowledge improvement was more pronounced for the topics
12
Diabetes Voice Online - May 2015
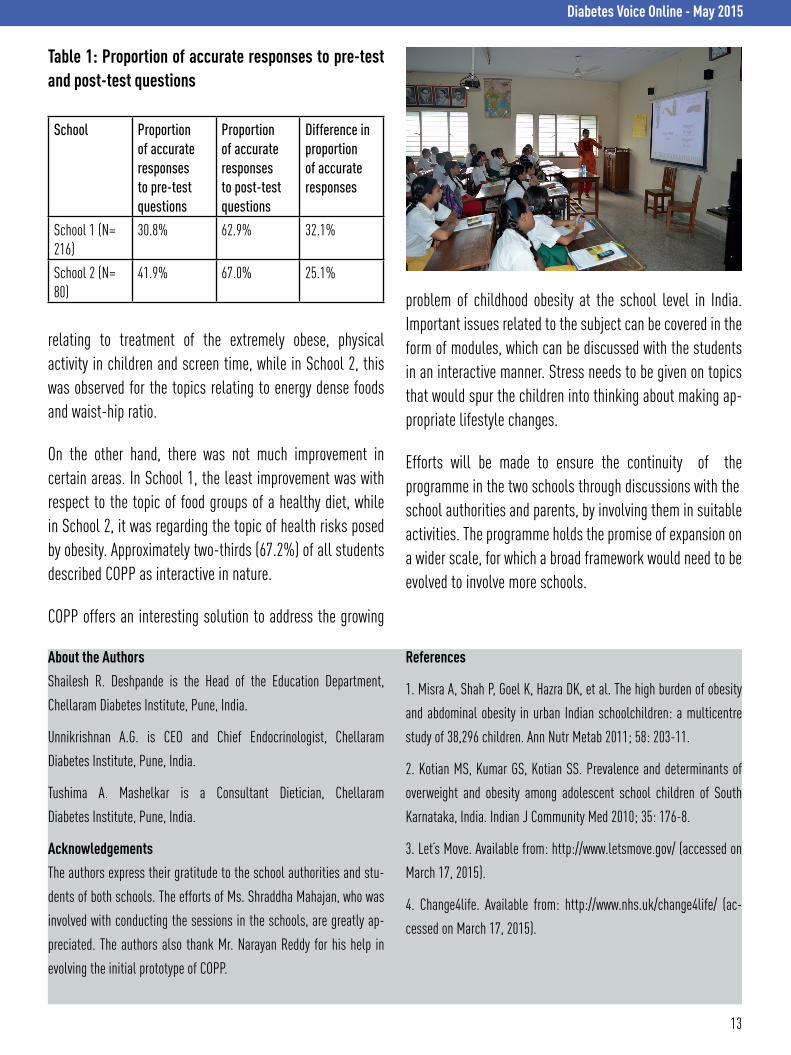
Table 1: Proportion of accurate responses to pre-test and post-test questions
School Proportion of accurate responses to pre-test questions
Proportion of accurate responses to post-test questions
Difference in proportion of accurate responses
School 1 (N= 216)
30.8% 62.9% 32.1%
School 2 (N= 80)
41.9% 67.0% 25.1%
relating to treatment of the extremely obese, physical activity in children and screen time, while in School 2, this was observed for the topics relating to energy dense foods and waist-hip ratio.
On the other hand, there was not much improvement in certain areas. In School 1, the least improvement was with respect to the topic of food groups of a healthy diet, while in School 2, it was regarding the topic of health risks posed by obesity. Approximately two-thirds (67.2%) of all students described COPP as interactive in nature.
COPP offers an interesting solution to address the growing
problem of childhood obesity at the school level in India. Important issues related to the subject can be covered in the form of modules, which can be discussed with the students in an interactive manner. Stress needs to be given on topics that would spur the children into thinking about making ap-propriate lifestyle changes.
Efforts will be made to ensure the continuity of the programme in the two schools through discussions with the school authorities and parents, by involving them in suitable activities. The programme holds the promise of expansion on a wider scale, for which a broad framework would need to be evolved to involve more schools.
About the Authors
Shailesh R. Deshpande is the Head of the Education Department,
Chellaram Diabetes Institute, Pune, India.
Unnikrishnan A.G. is CEO and Chief Endocrinologist, Chellaram
Diabetes Institute, Pune, India.
Tushima A. Mashelkar is a Consultant Dietician, Chellaram
Diabetes Institute, Pune, India.
Acknowledgements
The authors express their gratitude to the school authorities and stu-
dents of both schools. The efforts of Ms. Shraddha Mahajan, who was
involved with conducting the sessions in the schools, are greatly ap-
preciated. The authors also thank Mr. Narayan Reddy for his help in
evolving the initial prototype of COPP.
References
1. Misra A, Shah P, Goel K, Hazra DK, et al. The high burden of obesity
and abdominal obesity in urban Indian schoolchildren: a multicentre
study of 38,296 children. Ann Nutr Metab 2011; 58: 203-11.
2. Kotian MS, Kumar GS, Kotian SS. Prevalence and determinants of
overweight and obesity among adolescent school children of South
Karnataka, India. Indian J Community Med 2010; 35: 176-8.
3. Let’s Move. Available from: http://www.letsmove.gov/ (accessed on
March 17, 2015).
4. Change4life. Available from: http://www.nhs.uk/change4life/ (ac-
cessed on March 17, 2015).
13
Diabetes Voice Online - May 2015

Basic & Clinical Science
Diabetes in Indigenous Peoples Education & Integrated Care Global Challenges in Health
Living with Diabetes Public Health & Epidemiology
#WDC2015
SCIENTIFIC PROGRAMME
Learn.Discover. Connect.
JUNE 12Early registration deadlineSAVE UP TO 44%
www.wdc2015.org
Steven Kahn Malcolm King Unn-Britt Johansson Gojka Roglic Gordon Bunyan Edward Boyko
Chair: Bernard ZinmanDeputy Chair: Nam Cho
AUGUSTOnline ScientificProgramme
30 November – 4 December