development of the chinese version of the dentine hypersensitivity experience questionnaire
TRANSCRIPT

Development of the Chinese versionof the Dentine HypersensitivityExperience Questionnaire
He SL, Wang JH, Wang MH. Development of the Chinese version of the DentineHypersensitivity Experience Questionnaire.Eur J Oral Sci 2012; 120: 218–223. © 2012 Eur J Oral Sci
The aim of this study was to evaluate the reliability and the validity of the Chineseversion of the Dentine Hypersensitivity Experience Questionnaire (DHEQ). Aftertranslation and cross-cultural adaptation following international guidelines, 110patients with dentine hypersensitivity were recruited to complete the questionnaire.The reliability of the Chinese version of the DHEQ was evaluated using internalconsistency and test–retest methods. Construct validity was determined based onfactor analysis, discriminative validity (by comparing the subscale scores differencein the degree of sensitivity being investigated), and convergent validity (by analyzingthe correlation between DHEQ subscale scores and the global rating of oral healthquestion). Cronbach’s alpha value (internal reliability) for the total DHEQ scorewas 0.95 and the intraclass correlation coefficient (ICC) value (test–retest reliability)was 0.85. Construct validity was determined by factor analysis, extracting eight fac-tors, accounting for 74% of the variance. All items had factor loadings of >0.40. Inaddition, the Chinese version of the DHEQ was found to be valid for distinguishingpatients with varying degrees of dentine hypersensitivity. In terms of convergentvalidity, the impact scale was significantly highly correlated to the global oral healthrating. The results suggest that the Chinese version of the DHEQ has satisfactorypsychometric properties and is applicable for patients with dentine hypersensitivityin China.
Song-lin He1,2, Jin-hua Wang1,2,Meng-hong Wang1,2
1Chongqing Research Center for OralDiseases and Biomedical Science,Chongqing; 2Department of Preventive andPediatric Dentistry, The Affiliated Hospital ofStomatology, Chongqing Medical University,Chongqing, China
Song-lin He, No. 7, Shang Qing Si Road,Department of Preventive and PediatricDentistry, The Affiliated Hospital ofStomatology, Chongqing Medical University,Chongqing, China 401147
Telefax: +86–023–89035800E-mail: [email protected]
Key words: dentine hypersensitivity;questionnaire; reliability; validity
Accepted for publication March 2012
Dentine hypersensitivity is a common oral complaintdefined as a ‘short, sharp pain arising from exposeddentin in response to stimuli typically thermal, evapora-tive, tactile, osmotic or chemical and which cannot beascribed to any other form of dental defect or pathol-ogy’ (1). It is a highly prevalent oral condition thataffects 25.5–34.1% of Chinese people (2,3). This oraldisorder not only affects patients’ physical health, butalso affects their social function and psychosocialwell-being (4). Therefore, there is a need for a compre-hensive assessment of the impact of dentine hypersensi-tivity on patients’ daily living and oral health-relatedquality of life (OHRQoL). Oral health-related qualityof life is a multidimensional construct quantifying theextent to which oral disorders affect functioning, psy-chosocial well-being, sense of self, expectations, andsatisfaction with care (5). It has important implicationsfor the clinical practice of dentistry and dental research(6,7).
Instruments commonly used to assess OHRQoLamong individuals include the Oral Health ImpactProfile (OHIP) (8–10) and the Oral Impacts on DailyPerformance (OIDP) (11,12). While these instrumentscan comprehensively assess the multidimensional impact
of oral disorders (13), they are inappropriate for assess-ing the burden of specific oral disorders [e.g. dentalesthetics (14), oral malodor (15), and impairment ofswallowing function (16)] on OHRQoL. These genericmeasures are too broad for accurate assessment of thelinks between specific oral conditions and OHRQoL (5).For dentine hypersensitivity, a recent investigation byBEKES et al. (17) found that the particular impacts ofdentine hypersensitivity were not fully obtained throughthe OHIP-49. Although the OHRQoL impact of dentinehypersensitivity has drawn significant attention formany years (17), for a long time no specific instrumentwith which to assess this problem was available.
However, BOIKO et al. (4) recently proposed a Den-tine Hypersensitivity Experience Questionnaire (DHEQ)that assessed aspects of OHRQoL related to dentinehypersensitivity. This condition-specific measure hasshown good psychometric properties. The data of theDHEQ can be used to evaluate negative emotions spe-cifically related to dentine hypersensitivity and aids inthe development of effective interventions and healthpolicies for dentine hypersensitivity (7, 18). Yet, thisquestionnaire cannot be directly used in non-English-speaking countries. A rigorous psychometric test stage
Eur J Oral Sci 2012; 120: 218–223DOI: 10.1111/j.1600-0722.2012.00962.xPrinted in Singapore. All rights reserved
� 2012 Eur J Oral Sci
European Journal ofOral Science

must be accomplished before it can be used in otherareas. Therefore, this study aimed to translate theDHEQ into Chinese, to evaluate its cross-culturaladaptation, and to test the reliability and validity ofthe DHEQ among the Chinese.
Material and methods
The DHEQ is a specific instrument for comprehensivelyassessing the physical, social, and psychosocial negativeimpacts of dentine hypersensitivity among adults. It is anEnglish-language OHRQoL instrument, developed by theUniversity of Sheffield in the UK (4). The DHEQ consistsof 50 items (two items were deleted from the revised Eng-lish version) grouped into five domains to describe pain(items 1–6), into three visual analog scales to measure pain(items 7–9), into impact subscales (items 10–45), into ascale to record effects on life overall (items 46–49), andinto a global oral health rating (item 50). The domain ofthe impact subscale has five subscales: ‘restrictions’, ‘adap-tation’, ‘social impact’, ‘emotional impact’, and ‘identity’.For items 1–6, each item is treated separately. For items 7–9, three visual analog scales are adopted, ranging from 0to 10 for each item. For items 10–45, responses are givenon a seven-point Likert scale, with responses ranging from‘strongly agree’ to ‘strongly disagree’ (equivalent to scoresof 1–7). For items 46–49, responses are given on a five-point Likert scale, with responses ranging from ‘not at all’to ‘very much’ (equivalent to scores of 1–5). For thelast item, a six-point Likert scale is used, ranging from‘excellent’ to ‘very poor’ (equivalent to scores of 1–6).
The DHEQ was translated into Chinese using the for-ward–backward process proposed by DEL GRECO et al.(19). The process included several major steps.
Two independent translators first translated the DHEQfrom English to Chinese. Both translators were fluent inEnglish and Chinese and had background knowledge ofdentistry. Then, the two independent versions were back-translated from Chinese to English by a professional Eng-lish teacher, and by two dental specialists. None were famil-iar with the original questionnaire, and all were fluent inboth English and Chinese. The translated and back-trans-lated versions were compared and discussed by an expertpanel. The expert panel consisted of two dental specialistswith extensive knowledge of OHRQoL assessment and whowere fluent in both English and Chinese. A preliminary Chi-nese version of the DHEQ was then produced. Finally, thepreliminary Chinese version of the DHEQ was pilot testedon a convenience sample of 20 patients. After the test,emerging problems were discussed. The Chinese version wasconsidered final when there were no substantial differences.
This study comprised a total of 110 patients with den-tine hypersensitivity who had been previously recruitedinto a randomized clinical trial to investigate the effect ofdesensitizing toothpaste at the West China College of Sto-matology, Sichuan University. The Schiff Cold Air Sensi-tivity Scale was used to assess patients’ response to air-blast hypersensitivity assessment (20). The scale was scoredas follows: 0, subject does not respond to air stimulus; 1,subject responds to air stimulus, but does not requestdiscontinuation of stimulus; 2, subject responds to airstimulus and requests discontinuation or moves from stim-ulus; and 3, subject responds to air stimulus, considersstimulus to be painful, and requests discontinuation of thestimulus.
Patients were included if they had at least one sensitivetooth with a response of � 1 on the Schiff scale. Teethwere evaluated for hypersensitivity by directing a 1-s blastof air onto the hypersensitive cervical area, from a dis-tance of 1 cm, using cold air from a dental unit at 60 ± 5psi and a temperature of 70 ± 3°F. The degree of hyper-sensitivity was recorded in accordance with the Schiff ColdAir Sensitivity Scale. Patients with any orthodontic appli-ances, or who were unable to understand the DHEQ ques-tions, were excluded from the study. Two patients wereexcluded because they were unable to understand theDHEQ questions.
The study was approved by the Ethics Committee of WestChina College of Stomatology, Sichuan University. Written,informed consent was obtained from patients. A detailedexplanation was provided before patients filled in the Chi-nese version of the DHEQ in the waiting room. If they hadany questions, they could consult research assistants at anytime. To evaluate the test–retest reliability, 30 patients wererandomly selected using a computer-generated randomisedtable to make a return visit after 2 weeks.
Statistical analysis
Reliability: Two types of reliability were adopted toassess the reliability of the DHEQ. Specifically, the inter-nal consistency reliability was evaluated by calculatingCronbach’s alpha for the multi-item subscales, and the test–retest reliability was determined by calculating intraclasscorrelation coefficients (ICCs) using data from the 30patients who filled in the DHEQ twice, with a 2-weekintervening interval. A Cronbach’s alpha of � 0.70 is con-sidered acceptable for between-group comparisons. TheICC is considered to indicate poor to fair agreement when<0.40, to indicate moderate agreement when 0.41–0.60, tosignify good agreement when 0.61–0.80, and to indicateexcellent agreement when >0.80 (21).
Validity: Validity was assessed in three ways: constructvalidity, discriminative validity, and convergent validity.Construct validity for the DHEQ was determined utilizingexploratory factor analysis. However, a Bartlett’s test ofsphericity coefficient and a Kaiser–Meyer–Olkin (KMO)test must first be conducted to determine whether therewere a sufficient number of significant correlations amongitems to carry out this analysis (22). Factor loadings of>0.40 were considered significant for this study.
Discriminative validity was tested by comparing thedifference in subscale scores in the degree of dentinehypersensitivity being investigated. The degree of hyper-sensitivity was recorded in accordance with the Schiff ColdAir Sensitivity Scale.
Finally, a standard global rating of oral health wasadded to examine convergent validity. Convergent validitywas tested through investigating the correlation betweenDHEQ subscale scores and the global rating of oral healthquestion. Statistical analyses were conducted using SPSS
20.0 (SPSS, Chicago, IL, USA).
Results
A total of 110 patients were recruited from a univer-sity-affiliated clinic for this study. All the DHEQ ques-tionnaires were completely filled out. The mean ± SD
Validation of the Chinese version of DHEQ 219

age of the patients was 47.2 ± 12.5 (range 20–67) yr,and the majority were women (73%). A total of 17patients (15%) were diagnosed with degree 1 hypersen-sitivity, 58 (53%) displayed degree 2 hypersensitivity,and 35 (32%) exhibited degree 3 hypersensitivity.Table 1 presents the mean score and SD for the painscale (items 1–6), for the effect on life overall scale(items 46–49), and for the global oral health rating(item 50). Table 3 shows that the items related to‘problems with eating ice-cream (90%)’, ‘avoidingcontact with certain teeth (87%)’, and ‘pleasure out ofeating (86%)’ were reported most frequently in DHEQ.
Table 2 shows the internal consistency of the multi-item scales. Cronbach’s alpha for the total impact scoreof DHEQ was 0.96. Cronbach’s alpha for the subscalesranged from 0.69 for ‘restrictions’ to 0.89 for ‘adapta-tion’. All subscales exceeded the minimum reliabilitystandard of 0.70, except for the functional restrictionssubscale, whose value of 0.69 almost reached thethreshold. The corrected item-total correlations for theDHEQ ranged from 0.129 (item 13) to 0.760 (item 11).Only the corrected item-total correlation of item 13(‘I am uncertain when I am going to have these sensa-tions in my teeth.’) failed to reach the recommendedminimum correlation of 0.20. In addition, when delet-ing item 13, the Cronbach’s alpha coefficient of the
DHEQ increased slightly. Test–retest reliability wascalculated for 30 patients who took the same test againafter a 2-week interval. Test–retest reliability was evalu-ated using ICCs, which were 0.73 and 0.90 for func-tional restrictions and adaptation, respectively. TheICC values for the DHEQ indicated good to excellentagreement.
Construct validity was assessed through factor analy-sis. The result of the KMO test was 0.75 and that ofBartlett’s test of sphericity was 3466.1 [degrees of free-dom (d.f.) = 630, P < 0.001]. This demonstrated thatthere were a sufficient number of significant correla-tions among items to perform factor analysis. Theresults of the factor analysis for the subscales are pre-sented in Table 3. All items had factor loadings of>0.40. Factor analysis extracted eight factors (a figureconsistent with the original English version), whichtogether accounted for 74% of the variance. Items inmost subscales loaded on only one factor for theDHEQ (i.e. ‘adaptation’, ‘social’, or ‘identity’), but theitems in the ‘emotions’ subscale were split into two dif-ferent factors, and the items in the ‘restrictions’ sub-scale were split into three factors. The results wereanalyzed using the Kruskal–Wallis test to determine thediscriminative validity. There were statistically signifi-cant differences in the median scores for total and sub-scale scores of the DHEQ, categorized by the SchiffCold Air Sensitivity Scale (Table 4). In order to testthe convergent validity of the DHEQ, the correlationsbetween DHEQ subscale scores and global oral healthstatus were examined. Total and subscale scores of theDHEQ had significantly negative correlations with glo-bal oral health status (rs ranged from �0.59 to �0.35),indicating good convergent validity (Table 5).
Discussion
To the best of our knowledge, this study provides thefirst introduction of the DHEQ in a non-English-speak-ing country and also constitutes the first evaluation ofthe psychometric properties of the DHEQ in a non-English-speaking country. In recent years, a large num-ber of studies (6, 10, 15, 23–25) assessing OHRQoLhave been conducted. Instruments must be adaptedbefore they can be used on speakers of different lan-guages in other cultures. Therefore, we performed across-cultural adaptation of the original DHEQ andevaluated the reliability and validity of the Chinese ver-sion of the DHEQ according to international studies(26). The results presented here demonstrate the feasi-bility of using the Chinese version of the DHEQ tomeasure the biopsychosocial impact of dentine hyper-sensitivity.
For internal consistency, Cronbach’s alpha (as a testof reliability) exceeded 0.70 for all measures, except forthe functional restrictions subscale. The corrected item-total correlations were all well above the recommendedlevel of 0.2 (27), except for item 13, ‘I am uncertainwhen I am going to have these sensations in my teeth’,which had a corrected item-total correlation of 0.129.
Table 1
Scores obtained for the pain scale, the effect on life overallscale, and the global oral health rating
Scale/ratingNo. ofitems Range
Meanscore (SD)
Pain scale (VAS)Intensity 1 1–10 6.25 (1.91)Bothersomeness 1 1–10 5.48 (2.05)Tolerability 1 1–10 4.82 (1.86)Effect on life overall 4 1–20 2.77 (0.97)Global oral health rating 1 1–6 4.45 (0.97)
VAS, visual analogue scale
Table 2
Internal consistency and test–retest reliability of the individualsubscales
SubscaleNo. ofitems
Internalconsistency(n = 110)
Test–retestreliability (n = 30)
Cronbach’salpha
Intraclass correlationcoefficient (95% CI)
Total score 36 0.955 0.85 (0.66–0.99)SubscalesRestrictions 5 0.69 0.73 (0.43–0.96)Adaptation 12 0.89 0.90 (0.77–0.99)Social impact 5 0.80 0.89 (0.75–0.99)Emotionalimpact
8 0.87 0.88 (0.69–0.99)
Identity 6 0.84 0.83 (0.62–0.99)
220 He et al.
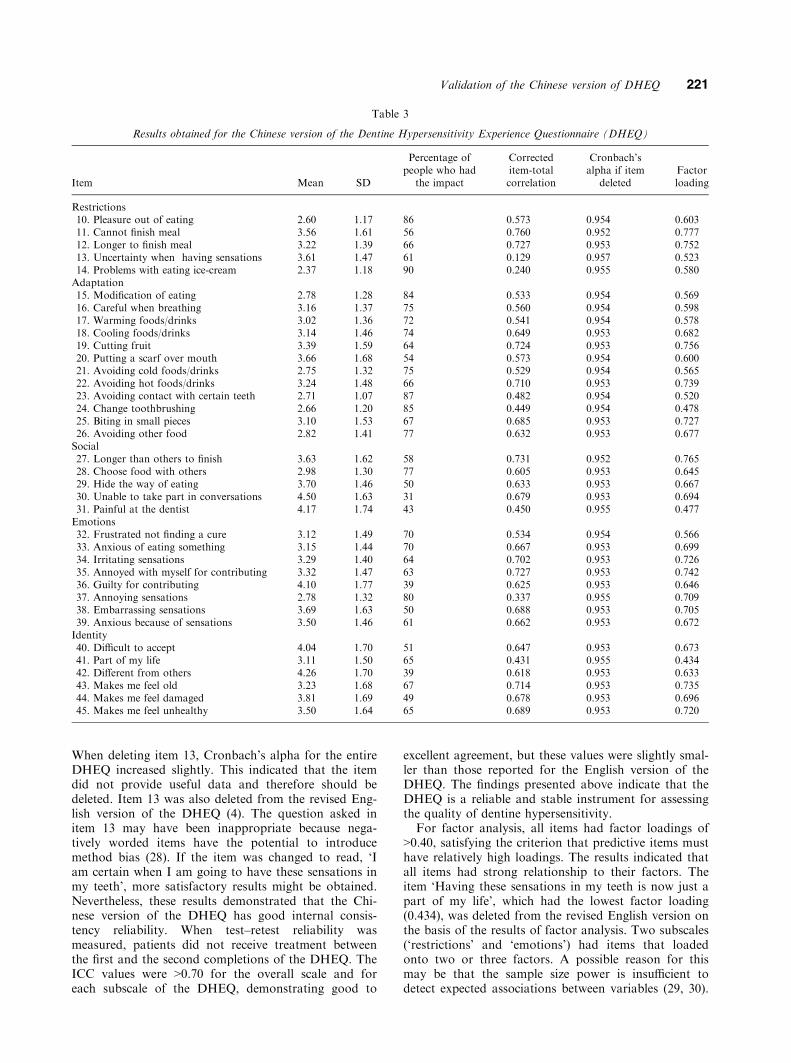
When deleting item 13, Cronbach’s alpha for the entireDHEQ increased slightly. This indicated that the itemdid not provide useful data and therefore should bedeleted. Item 13 was also deleted from the revised Eng-lish version of the DHEQ (4). The question asked initem 13 may have been inappropriate because nega-tively worded items have the potential to introducemethod bias (28). If the item was changed to read, ‘Iam certain when I am going to have these sensations inmy teeth’, more satisfactory results might be obtained.Nevertheless, these results demonstrated that the Chi-nese version of the DHEQ has good internal consis-tency reliability. When test–retest reliability wasmeasured, patients did not receive treatment betweenthe first and the second completions of the DHEQ. TheICC values were >0.70 for the overall scale and foreach subscale of the DHEQ, demonstrating good to
excellent agreement, but these values were slightly smal-ler than those reported for the English version of theDHEQ. The findings presented above indicate that theDHEQ is a reliable and stable instrument for assessingthe quality of dentine hypersensitivity.
For factor analysis, all items had factor loadings of>0.40, satisfying the criterion that predictive items musthave relatively high loadings. The results indicated thatall items had strong relationship to their factors. Theitem ‘Having these sensations in my teeth is now just apart of my life’, which had the lowest factor loading(0.434), was deleted from the revised English version onthe basis of the results of factor analysis. Two subscales(‘restrictions’ and ‘emotions’) had items that loadedonto two or three factors. A possible reason for thismay be that the sample size power is insufficient todetect expected associations between variables (29, 30).
Table 3
Results obtained for the Chinese version of the Dentine Hypersensitivity Experience Questionnaire (DHEQ)
Item Mean SD
Percentage ofpeople who had
the impact
Correcteditem-totalcorrelation
Cronbach’salpha if item
deletedFactorloading
Restrictions10. Pleasure out of eating 2.60 1.17 86 0.573 0.954 0.60311. Cannot finish meal 3.56 1.61 56 0.760 0.952 0.77712. Longer to finish meal 3.22 1.39 66 0.727 0.953 0.75213. Uncertainty when having sensations 3.61 1.47 61 0.129 0.957 0.52314. Problems with eating ice-cream 2.37 1.18 90 0.240 0.955 0.580Adaptation15. Modification of eating 2.78 1.28 84 0.533 0.954 0.56916. Careful when breathing 3.16 1.37 75 0.560 0.954 0.59817. Warming foods/drinks 3.02 1.36 72 0.541 0.954 0.57818. Cooling foods/drinks 3.14 1.46 74 0.649 0.953 0.68219. Cutting fruit 3.39 1.59 64 0.724 0.953 0.75620. Putting a scarf over mouth 3.66 1.68 54 0.573 0.954 0.60021. Avoiding cold foods/drinks 2.75 1.32 75 0.529 0.954 0.56522. Avoiding hot foods/drinks 3.24 1.48 66 0.710 0.953 0.73923. Avoiding contact with certain teeth 2.71 1.07 87 0.482 0.954 0.52024. Change toothbrushing 2.66 1.20 85 0.449 0.954 0.47825. Biting in small pieces 3.10 1.53 67 0.685 0.953 0.72726. Avoiding other food 2.82 1.41 77 0.632 0.953 0.677Social27. Longer than others to finish 3.63 1.62 58 0.731 0.952 0.76528. Choose food with others 2.98 1.30 77 0.605 0.953 0.64529. Hide the way of eating 3.70 1.46 50 0.633 0.953 0.66730. Unable to take part in conversations 4.50 1.63 31 0.679 0.953 0.69431. Painful at the dentist 4.17 1.74 43 0.450 0.955 0.477Emotions32. Frustrated not finding a cure 3.12 1.49 70 0.534 0.954 0.56633. Anxious of eating something 3.15 1.44 70 0.667 0.953 0.69934. Irritating sensations 3.29 1.40 64 0.702 0.953 0.72635. Annoyed with myself for contributing 3.32 1.47 63 0.727 0.953 0.74236. Guilty for contributing 4.10 1.77 39 0.625 0.953 0.64637. Annoying sensations 2.78 1.32 80 0.337 0.955 0.70938. Embarrassing sensations 3.69 1.63 50 0.688 0.953 0.70539. Anxious because of sensations 3.50 1.46 61 0.662 0.953 0.672Identity40. Difficult to accept 4.04 1.70 51 0.647 0.953 0.67341. Part of my life 3.11 1.50 65 0.431 0.955 0.43442. Different from others 4.26 1.70 39 0.618 0.953 0.63343. Makes me feel old 3.23 1.68 67 0.714 0.953 0.73544. Makes me feel damaged 3.81 1.69 49 0.678 0.953 0.69645. Makes me feel unhealthy 3.50 1.64 65 0.689 0.953 0.720
Validation of the Chinese version of DHEQ 221
Therefore, our results should be verified with a largersample.
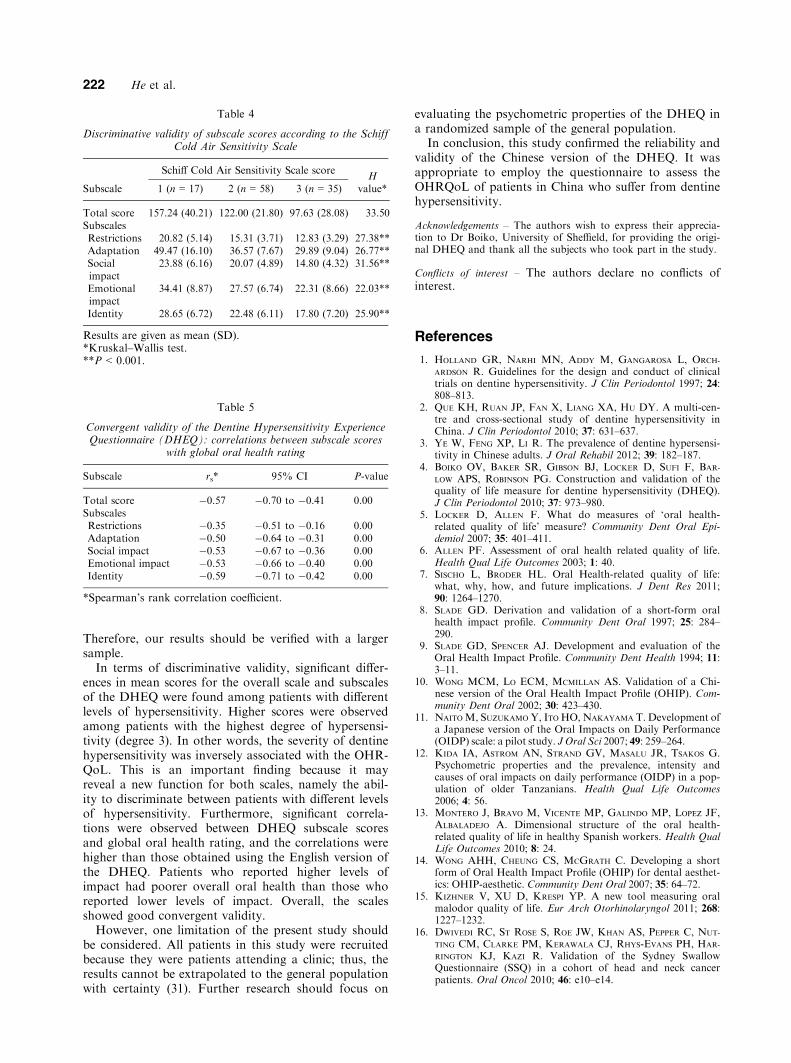
In terms of discriminative validity, significant differ-ences in mean scores for the overall scale and subscalesof the DHEQ were found among patients with differentlevels of hypersensitivity. Higher scores were observedamong patients with the highest degree of hypersensi-tivity (degree 3). In other words, the severity of dentinehypersensitivity was inversely associated with the OHR-QoL. This is an important finding because it mayreveal a new function for both scales, namely the abil-ity to discriminate between patients with different levelsof hypersensitivity. Furthermore, significant correla-tions were observed between DHEQ subscale scoresand global oral health rating, and the correlations werehigher than those obtained using the English version ofthe DHEQ. Patients who reported higher levels ofimpact had poorer overall oral health than those whoreported lower levels of impact. Overall, the scalesshowed good convergent validity.
However, one limitation of the present study shouldbe considered. All patients in this study were recruitedbecause they were patients attending a clinic; thus, theresults cannot be extrapolated to the general populationwith certainty (31). Further research should focus on
evaluating the psychometric properties of the DHEQ ina randomized sample of the general population.
In conclusion, this study confirmed the reliability andvalidity of the Chinese version of the DHEQ. It wasappropriate to employ the questionnaire to assess theOHRQoL of patients in China who suffer from dentinehypersensitivity.
Acknowledgements – The authors wish to express their apprecia-tion to Dr Boiko, University of Sheffield, for providing the origi-nal DHEQ and thank all the subjects who took part in the study.
Conflicts of interest – The authors declare no conflicts ofinterest.
References
1. HOLLAND GR, NARHI MN, ADDY M, GANGAROSA L, ORCH-
ARDSON R. Guidelines for the design and conduct of clinicaltrials on dentine hypersensitivity. J Clin Periodontol 1997; 24:808–813.
2. QUE KH, RUAN JP, FAN X, LIANG XA, HU DY. A multi-cen-tre and cross-sectional study of dentine hypersensitivity inChina. J Clin Periodontol 2010; 37: 631–637.
3. YE W, FENG XP, LI R. The prevalence of dentine hypersensi-tivity in Chinese adults. J Oral Rehabil 2012; 39: 182–187.
4. BOIKO OV, BAKER SR, GIBSON BJ, LOCKER D, SUFI F, BAR-
LOW APS, ROBINSON PG. Construction and validation of thequality of life measure for dentine hypersensitivity (DHEQ).J Clin Periodontol 2010; 37: 973–980.
5. LOCKER D, ALLEN F. What do measures of ‘oral health-related quality of life’ measure? Community Dent Oral Epi-demiol 2007; 35: 401–411.
6. ALLEN PF. Assessment of oral health related quality of life.Health Qual Life Outcomes 2003; 1: 40.
7. SISCHO L, BRODER HL. Oral Health-related quality of life:what, why, how, and future implications. J Dent Res 2011;90: 1264–1270.
8. SLADE GD. Derivation and validation of a short-form oralhealth impact profile. Community Dent Oral 1997; 25: 284–290.
9. SLADE GD, SPENCER AJ. Development and evaluation of theOral Health Impact Profile. Community Dent Health 1994; 11:3–11.
10. WONG MCM, LO ECM, MCMILLAN AS. Validation of a Chi-nese version of the Oral Health Impact Profile (OHIP). Com-munity Dent Oral 2002; 30: 423–430.
11. NAITO M, SUZUKAMO Y, ITO HO, NAKAYAMA T. Development ofa Japanese version of the Oral Impacts on Daily Performance(OIDP) scale: a pilot study. J Oral Sci 2007; 49: 259–264.
12. KIDA IA, ASTROM AN, STRAND GV, MASALU JR, TSAKOS G.Psychometric properties and the prevalence, intensity andcauses of oral impacts on daily performance (OIDP) in a pop-ulation of older Tanzanians. Health Qual Life Outcomes2006; 4: 56.
13. MONTERO J, BRAVO M, VICENTE MP, GALINDO MP, LOPEZ JF,ALBALADEJO A. Dimensional structure of the oral health-related quality of life in healthy Spanish workers. Health QualLife Outcomes 2010; 8: 24.
14. WONG AHH, CHEUNG CS, MCGRATH C. Developing a shortform of Oral Health Impact Profile (OHIP) for dental aesthet-ics: OHIP-aesthetic. Community Dent Oral 2007; 35: 64–72.
15. KIZHNER V, XU D, KRESPI YP. A new tool measuring oralmalodor quality of life. Eur Arch Otorhinolaryngol 2011; 268:1227–1232.
16. DWIVEDI RC, ST ROSE S, ROE JW, KHAN AS, PEPPER C, NUT-
TING CM, CLARKE PM, KERAWALA CJ, RHYS-EVANS PH, HAR-
RINGTON KJ, KAZI R. Validation of the Sydney SwallowQuestionnaire (SSQ) in a cohort of head and neck cancerpatients. Oral Oncol 2010; 46: e10–e14.
Table 5
Convergent validity of the Dentine Hypersensitivity ExperienceQuestionnaire (DHEQ): correlations between subscale scores
with global oral health rating
Subscale rs* 95% CI P-value
Total score �0.57 �0.70 to �0.41 0.00SubscalesRestrictions �0.35 �0.51 to �0.16 0.00Adaptation �0.50 �0.64 to �0.31 0.00Social impact �0.53 �0.67 to �0.36 0.00Emotional impact �0.53 �0.66 to �0.40 0.00Identity �0.59 �0.71 to �0.42 0.00
*Spearman’s rank correlation coefficient.
Table 4
Discriminative validity of subscale scores according to the SchiffCold Air Sensitivity Scale
Subscale
Schiff Cold Air Sensitivity Scale scoreH
value*1 (n = 17) 2 (n = 58) 3 (n = 35)
Total score 157.24 (40.21) 122.00 (21.80) 97.63 (28.08) 33.50SubscalesRestrictions 20.82 (5.14) 15.31 (3.71) 12.83 (3.29) 27.38**Adaptation 49.47 (16.10) 36.57 (7.67) 29.89 (9.04) 26.77**Socialimpact
23.88 (6.16) 20.07 (4.89) 14.80 (4.32) 31.56**
Emotionalimpact
34.41 (8.87) 27.57 (6.74) 22.31 (8.66) 22.03**
Identity 28.65 (6.72) 22.48 (6.11) 17.80 (7.20) 25.90**
Results are given as mean (SD).*Kruskal–Wallis test.**P < 0.001.
222 He et al.

17. BEKES K, JOHN MT, SCHALLER HG, HIRSCH C. Oral health-related quality of life in patients seeking care for dentinhypersensitivity. J Oral Rehabil 2009; 36: 45–51.
18. CARR AJ, GIBSON B, ROBINSON PG. Measuring quality of life:is quality of life determined by expectations or experience?BMJ 2001; 322: 1240–1243.
19. DEL GRECO L, WALOP W, EASTRIDGE L. Questionnaire devel-opment: 3. Translation. Can Med Assoc J 1987; 136: 817–818.
20. SCHIFF T, DOTSON M, COHEN S, DE VIZIO W, MCCOOL J, VOL-
PE A. Efficacy of a dentifrice containing potassium nitrate,soluble pyrophosphate, PVM/MA copolymer, and sodiumfluoride on dentinal hypersensitivity: a twelve-week clinicalstudy. J Clin Dent 1994; 5Spec No: 87–92.
21. BARTKO JJ. The intraclass correlation coefficient as a measureof reliability. Psychol Rep 1966; 19: 3–11.
22. BARTLETT MS. Tests of significance in factor analysis. Br JPsychol 1950; 3: 77–85.
23. AKARSLAN ZZ, ERTEN H. Reliability and validity of the Turk-ish version of the shorter form of the gagging problem assess-ment questionnaire. J Oral Rehabil 2010; 37: 21–25.
24. LARSSON P, JOHN MT, NILNER K, LIST T. Reliability andvalidity of the Orofacial Esthetic Scale in prosthodonticpatients. Int J Prosthodont 2010; 23: 257–262.
25. SOUZA FT, SANTOS TP, BERNARDES VF, TEIXEIRA AL, KUM-
MER AM, SILVA TA, ABREU MH. The impact of burningmouth syndrome on health-related quality of life. Health QualLife Outcomes 2011; 9: 57.
26. SPERBER AD. Translation and validation of study instrumentsfor cross-cultural research. Gastroenterology 2004; 126: S124–S128.
27. KLINE P. A hand book of psychological testing, 2nd edn. NewYork: Routledge, 1999.
28. DEVELLIS RF. Scale development: theory and applications.London: SAGE Publications, 2003.
29. YANG X, XIAO N, YAN J. The PedsQL in pediatric cerebralpalsy: reliability and validity of the Chinese version pediatricquality of life inventory 4.0 generic core scales and 3.0 cere-bral palsy module. Qual Life Res 2011; 20: 243–252.
30. TOUMA Z, GHANDOUR L, SIBAI A, PUZANTIAN H, HAMDAN A,HAMDAN O, MENASSA J, UTHMAN I, ARAYSSI T. Cross-culturaladaptation and validation of Behcet’s disease quality of lifequestionnaire. BMC Med Res Methodol 2011; 11: 52.
31. FOSTER PAGE LA, THOMSON WM, JOKOVIC A, LOCKER D. Val-idation of the Child Perceptions Questionnaire (CPQ 11–14).J Dent Res 2005; 84: 649–652.
Validation of the Chinese version of DHEQ 223