development of a locking femur nail for mice
TRANSCRIPT

ARTICLE IN PRESS
0021-9290/$ - se
doi:10.1016/j.jb
�CorrespondReconstructive
Saar, Germany
E-mail addr
Journal of Biomechanics 40 (2007) 215–219
www.elsevier.com/locate/jbiomech
Short communication
Development of a locking femur nail for mice
J.H. Holsteina,b,�, M.D. Mengerb, U. Culemanna, C. Meierc, T. Pohlemanna
aDepartment of Trauma, Hand and Reconstructive Surgery, University of Saarland, D-66421 Homburg/Saar, GermanybInstitute for Clinical & Experimental Surgery, University of Saarland, Homburg/Saar, Germany
cDivision of Trauma Surgery, University Hospital Zurich, Switzerland
Accepted 29 October 2005
www.JBiomech.com
Abstract
We herein report on a novel locking intramedullary nail system in a murine closed femur fracture model. The nail system consists
of a modified 24-gauge injection needle and a 0.1-mm-diameter tungsten guide wire. Rotation stability was accomplished by
flattening the proximal and distal end of the needle. Torsional mechanical testing of the implants in osteotomized cadaveric femora
revealed a superiority of the locking nail (3.971.01 rotation at a torque of 0.9Nmm, n ¼ 10) compared to the unmodified injection
needle (conventional nail; 52.473.21, n ¼ 10, po0:05). None of the implants, however, achieved the rotation stability of unfractured
femora (0.370.51, n ¼ 10). In a second step, we tested the feasibility of the in vivo application of the locking nail to stabilize a closed
femoral midshaft fracture in C57BL/6 mice. Of interest, none of the 10 animals showed a dislocation of the locking nail over a
5-week period, while 3 of 4 animals with conventional nail fracture stabilization showed a significant pin dislocation within the first 3
days (po0:05). Mechanical testing after 5-weeks stabilization with the locking nail revealed an appropriate bone healing with a
torque at failure of 71.673.4% and a peak rotation before failure of 68.475.3% relative to the unfractured contralateral femur.
With the advantage that closed fractures can be fixed with rotation stability, the herein introduced model may represent an ideal tool
to study bone healing in transgenic and knockout mice.
r 2005 Elsevier Ltd. All rights reserved.
Keywords: Closed fracture; Locking femur nail; Fracture healing; Torsional mechanical testing; Mice
1. Introduction
While former fracture studies have chosen largeanimal models, nowadays small animals, particularlyrats and mice are used. Due to the increasing availabilityof specific antibodies and gene-targeted animals, murinemodels became preferred tools in biomedical research(Jacenko and Olsen, 1995). Established fracture modelsin mice mostly use ribs, tibia or femur (Cho et al., 2002;Hiltunen et al., 1993; Nakase et al., 1994; Ohta et al.,1999; Yamagiwa et al., 1999). Although appropriate toexamine gene expression during fracture healing (Ito
e front matter r 2005 Elsevier Ltd. All rights reserved.
iomech.2005.10.034
ing author. Department of Trauma, Hand and
Surgery, University of Saarland, D-66421 Homburg/
. Tel.: +49 6841 16 31501; fax: +49 6841 16 31503.
ess: [email protected] (J.H. Holstein).
et al., 1999; Yamagiwa et al., 1999), the rib isinapplicable for mechanical testing procedures due toits anatomy (Cheung et al., 2003). The closed tibiafracture model described by Hiltunen et al. (1993) maybe considered the most established fracture model inmice. It is well reproducible and surgery causes minimalsoft tissue injury. However, the triangular distallydeclining caliber, the bended longitudinal axis and thedeficient soft tissue cover put the tibia at a disadvantagewith the femur for the use as a fracture model (Cheunget al., 2003).
Manigrasso and O’Connor (2004) developed a closedfemur fracture model in mice, but the intramedullary pindid not provide rotation stability after fracture. Incontrast, the application of an external fixator (Cheunget al., 2003) offers excellent rotation stability. However,this model is disadvantageous due to the high implant
ARTICLE IN PRESSJ.H. Holstein et al. / Journal of Biomechanics 40 (2007) 215–219216
weight and the large variation of the implant stiffness.Additionally, the surgery requires sophisticated skills,and, nonetheless, the open approach, which is necessaryto insert the pins, aggravates soft tissue trauma. Toovercome these disadvantages, we designed a lockingfemur nail for mice. This model bears the advantage thatclosed fractures can be fixed with rotation stability anddo not require pre-pinning of the bone before inductionof the fracture.
2. Material and methods
2.1. Animals and specimens
The initial torsional mechanical testing of theimplants was performed in osteotomized cadavericfemora of C57BL/6 mice (n ¼ 40). For in vivo studies,the right femur of additional animals was stabilized afterfracture with a locking (n ¼ 10) or a conventional nail(n ¼ 4), and torsional testing was performed after 5weeks comparing the fractured with the contralateral,non-fractured femur.
2.2. Locking nail system
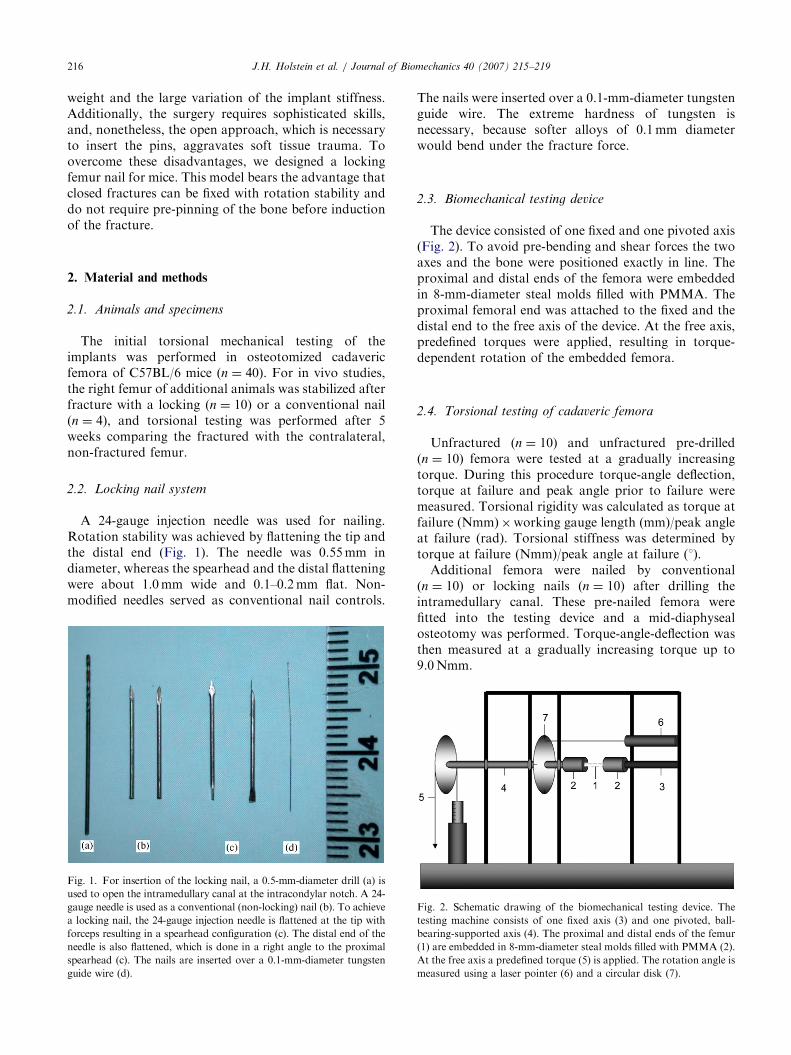
A 24-gauge injection needle was used for nailing.Rotation stability was achieved by flattening the tip andthe distal end (Fig. 1). The needle was 0.55mm indiameter, whereas the spearhead and the distal flatteningwere about 1.0mm wide and 0.1–0.2mm flat. Non-modified needles served as conventional nail controls.
Fig. 1. For insertion of the locking nail, a 0.5-mm-diameter drill (a) is
used to open the intramedullary canal at the intracondylar notch. A 24-
gauge needle is used as a conventional (non-locking) nail (b). To achieve
a locking nail, the 24-gauge injection needle is flattened at the tip with
forceps resulting in a spearhead configuration (c). The distal end of the
needle is also flattened, which is done in a right angle to the proximal
spearhead (c). The nails are inserted over a 0.1-mm-diameter tungsten
guide wire (d).
The nails were inserted over a 0.1-mm-diameter tungstenguide wire. The extreme hardness of tungsten isnecessary, because softer alloys of 0.1mm diameterwould bend under the fracture force.
2.3. Biomechanical testing device
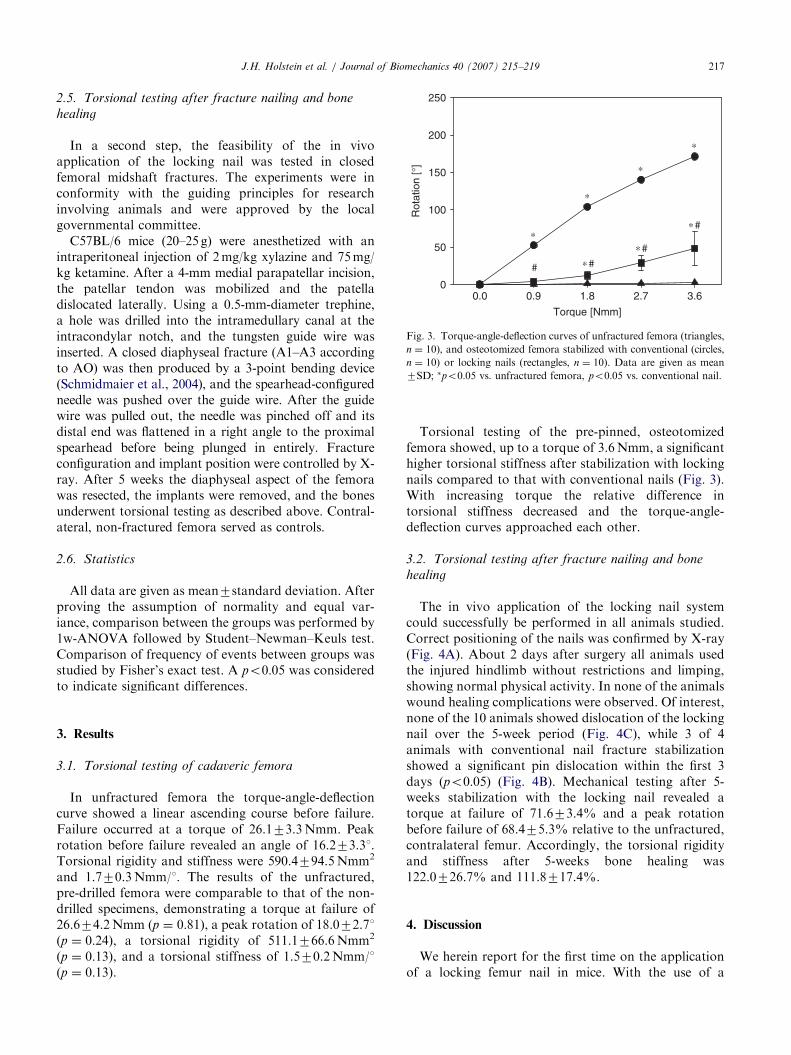
The device consisted of one fixed and one pivoted axis(Fig. 2). To avoid pre-bending and shear forces the twoaxes and the bone were positioned exactly in line. Theproximal and distal ends of the femora were embeddedin 8-mm-diameter steal molds filled with PMMA. Theproximal femoral end was attached to the fixed and thedistal end to the free axis of the device. At the free axis,predefined torques were applied, resulting in torque-dependent rotation of the embedded femora.
2.4. Torsional testing of cadaveric femora
Unfractured (n ¼ 10) and unfractured pre-drilled(n ¼ 10) femora were tested at a gradually increasingtorque. During this procedure torque-angle deflection,torque at failure and peak angle prior to failure weremeasured. Torsional rigidity was calculated as torque atfailure (Nmm)�working gauge length (mm)/peak angleat failure (rad). Torsional stiffness was determined bytorque at failure (Nmm)/peak angle at failure (1).
Additional femora were nailed by conventional(n ¼ 10) or locking nails (n ¼ 10) after drilling theintramedullary canal. These pre-nailed femora werefitted into the testing device and a mid-diaphysealosteotomy was performed. Torque-angle-deflection wasthen measured at a gradually increasing torque up to9.0Nmm.
Fig. 2. Schematic drawing of the biomechanical testing device. The
testing machine consists of one fixed axis (3) and one pivoted, ball-
bearing-supported axis (4). The proximal and distal ends of the femur
(1) are embedded in 8-mm-diameter steal molds filled with PMMA (2).
At the free axis a predefined torque (5) is applied. The rotation angle is
measured using a laser pointer (6) and a circular disk (7).
ARTICLE IN PRESS
Torque [Nmm]
0.0 0.9 1.8 2.7 3.6
Rot
atio
n [°
]
0
50
100
150
200
250
∗
∗
∗
∗
# ∗#∗#
∗#
Fig. 3. Torque-angle-deflection curves of unfractured femora (triangles,
n ¼ 10), and osteotomized femora stabilized with conventional (circles,
n ¼ 10) or locking nails (rectangles, n ¼ 10). Data are given as mean
7SD; �po0:05 vs. unfractured femora, po0:05 vs. conventional nail.
J.H. Holstein et al. / Journal of Biomechanics 40 (2007) 215–219 217
2.5. Torsional testing after fracture nailing and bone
healing
In a second step, the feasibility of the in vivoapplication of the locking nail was tested in closedfemoral midshaft fractures. The experiments were inconformity with the guiding principles for researchinvolving animals and were approved by the localgovernmental committee.
C57BL/6 mice (20–25 g) were anesthetized with anintraperitoneal injection of 2mg/kg xylazine and 75mg/kg ketamine. After a 4-mm medial parapatellar incision,the patellar tendon was mobilized and the patelladislocated laterally. Using a 0.5-mm-diameter trephine,a hole was drilled into the intramedullary canal at theintracondylar notch, and the tungsten guide wire wasinserted. A closed diaphyseal fracture (A1–A3 accordingto AO) was then produced by a 3-point bending device(Schmidmaier et al., 2004), and the spearhead-configuredneedle was pushed over the guide wire. After the guidewire was pulled out, the needle was pinched off and itsdistal end was flattened in a right angle to the proximalspearhead before being plunged in entirely. Fractureconfiguration and implant position were controlled by X-ray. After 5 weeks the diaphyseal aspect of the femorawas resected, the implants were removed, and the bonesunderwent torsional testing as described above. Contral-ateral, non-fractured femora served as controls.
2.6. Statistics
All data are given as mean7standard deviation. Afterproving the assumption of normality and equal var-iance, comparison between the groups was performed by1w-ANOVA followed by Student–Newman–Keuls test.Comparison of frequency of events between groups wasstudied by Fisher’s exact test. A po0:05 was consideredto indicate significant differences.
3. Results
3.1. Torsional testing of cadaveric femora
In unfractured femora the torque-angle-deflectioncurve showed a linear ascending course before failure.Failure occurred at a torque of 26.173.3Nmm. Peakrotation before failure revealed an angle of 16.273.31.Torsional rigidity and stiffness were 590.4794.5Nmm2
and 1.770.3Nmm/1. The results of the unfractured,pre-drilled femora were comparable to that of the non-drilled specimens, demonstrating a torque at failure of26.674.2Nmm (p ¼ 0:81), a peak rotation of 18.072.71(p ¼ 0:24), a torsional rigidity of 511.1766.6Nmm2
(p ¼ 0:13), and a torsional stiffness of 1.570.2Nmm/1(p ¼ 0:13).
Torsional testing of the pre-pinned, osteotomizedfemora showed, up to a torque of 3.6Nmm, a significanthigher torsional stiffness after stabilization with lockingnails compared to that with conventional nails (Fig. 3).With increasing torque the relative difference intorsional stiffness decreased and the torque-angle-deflection curves approached each other.
3.2. Torsional testing after fracture nailing and bone
healing
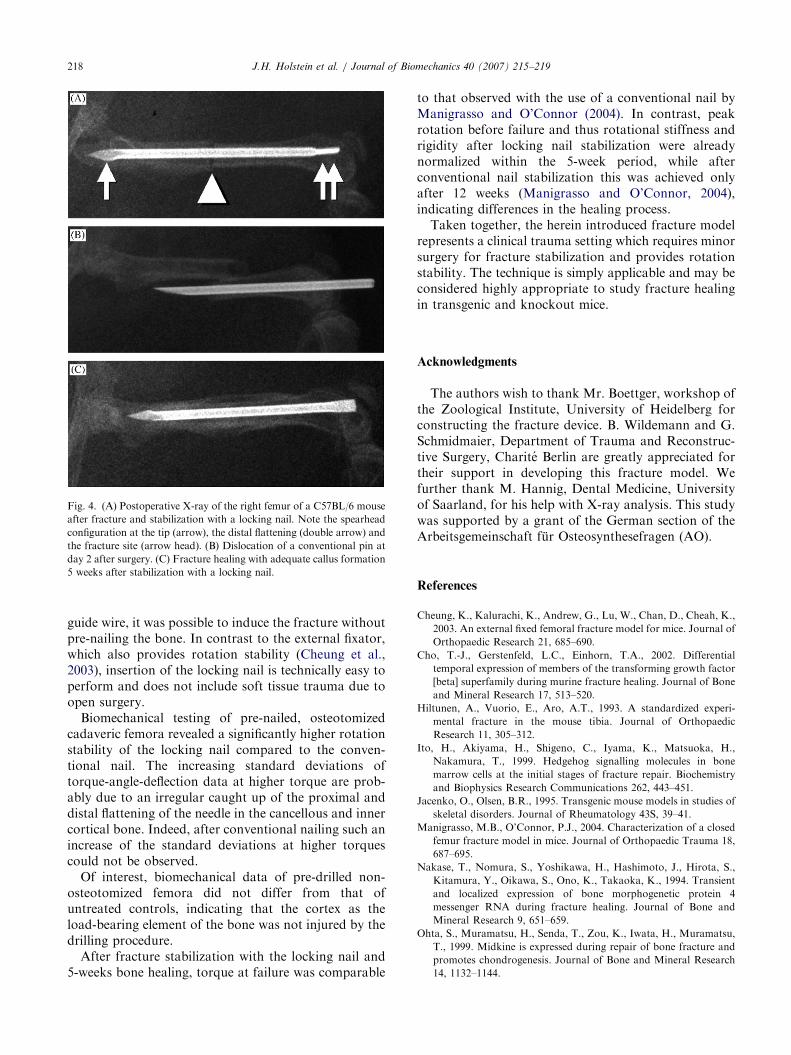
The in vivo application of the locking nail systemcould successfully be performed in all animals studied.Correct positioning of the nails was confirmed by X-ray(Fig. 4A). About 2 days after surgery all animals usedthe injured hindlimb without restrictions and limping,showing normal physical activity. In none of the animalswound healing complications were observed. Of interest,none of the 10 animals showed dislocation of the lockingnail over the 5-week period (Fig. 4C), while 3 of 4animals with conventional nail fracture stabilizationshowed a significant pin dislocation within the first 3days (po0:05) (Fig. 4B). Mechanical testing after 5-weeks stabilization with the locking nail revealed atorque at failure of 71.673.4% and a peak rotationbefore failure of 68.475.3% relative to the unfractured,contralateral femur. Accordingly, the torsional rigidityand stiffness after 5-weeks bone healing was122.0726.7% and 111.8717.4%.
4. Discussion
We herein report for the first time on the applicationof a locking femur nail in mice. With the use of a
ARTICLE IN PRESS
Fig. 4. (A) Postoperative X-ray of the right femur of a C57BL/6 mouse
after fracture and stabilization with a locking nail. Note the spearhead
configuration at the tip (arrow), the distal flattening (double arrow) and
the fracture site (arrow head). (B) Dislocation of a conventional pin at
day 2 after surgery. (C) Fracture healing with adequate callus formation
5 weeks after stabilization with a locking nail.
J.H. Holstein et al. / Journal of Biomechanics 40 (2007) 215–219218
guide wire, it was possible to induce the fracture withoutpre-nailing the bone. In contrast to the external fixator,which also provides rotation stability (Cheung et al.,2003), insertion of the locking nail is technically easy toperform and does not include soft tissue trauma due toopen surgery.
Biomechanical testing of pre-nailed, osteotomizedcadaveric femora revealed a significantly higher rotationstability of the locking nail compared to the conven-tional nail. The increasing standard deviations oftorque-angle-deflection data at higher torque are prob-ably due to an irregular caught up of the proximal anddistal flattening of the needle in the cancellous and innercortical bone. Indeed, after conventional nailing such anincrease of the standard deviations at higher torquescould not be observed.
Of interest, biomechanical data of pre-drilled non-osteotomized femora did not differ from that ofuntreated controls, indicating that the cortex as theload-bearing element of the bone was not injured by thedrilling procedure.
After fracture stabilization with the locking nail and5-weeks bone healing, torque at failure was comparable
to that observed with the use of a conventional nail byManigrasso and O’Connor (2004). In contrast, peakrotation before failure and thus rotational stiffness andrigidity after locking nail stabilization were alreadynormalized within the 5-week period, while afterconventional nail stabilization this was achieved onlyafter 12 weeks (Manigrasso and O’Connor, 2004),indicating differences in the healing process.
Taken together, the herein introduced fracture modelrepresents a clinical trauma setting which requires minorsurgery for fracture stabilization and provides rotationstability. The technique is simply applicable and may beconsidered highly appropriate to study fracture healingin transgenic and knockout mice.
Acknowledgments
The authors wish to thank Mr. Boettger, workshop ofthe Zoological Institute, University of Heidelberg forconstructing the fracture device. B. Wildemann and G.Schmidmaier, Department of Trauma and Reconstruc-tive Surgery, Charite Berlin are greatly appreciated fortheir support in developing this fracture model. Wefurther thank M. Hannig, Dental Medicine, Universityof Saarland, for his help with X-ray analysis. This studywas supported by a grant of the German section of theArbeitsgemeinschaft fur Osteosynthesefragen (AO).
References
Cheung, K., Kalurachi, K., Andrew, G., Lu, W., Chan, D., Cheah, K.,
2003. An external fixed femoral fracture model for mice. Journal of
Orthopaedic Research 21, 685–690.
Cho, T.-J., Gerstenfeld, L.C., Einhorn, T.A., 2002. Differential
temporal expression of members of the transforming growth factor
[beta] superfamily during murine fracture healing. Journal of Bone
and Mineral Research 17, 513–520.
Hiltunen, A., Vuorio, E., Aro, A.T., 1993. A standardized experi-
mental fracture in the mouse tibia. Journal of Orthopaedic
Research 11, 305–312.
Ito, H., Akiyama, H., Shigeno, C., Iyama, K., Matsuoka, H.,
Nakamura, T., 1999. Hedgehog signalling molecules in bone
marrow cells at the initial stages of fracture repair. Biochemistry
and Biophysics Research Communications 262, 443–451.
Jacenko, O., Olsen, B.R., 1995. Transgenic mouse models in studies of
skeletal disorders. Journal of Rheumatology 43S, 39–41.
Manigrasso, M.B., O’Connor, P.J., 2004. Characterization of a closed
femur fracture model in mice. Journal of Orthopaedic Trauma 18,
687–695.
Nakase, T., Nomura, S., Yoshikawa, H., Hashimoto, J., Hirota, S.,
Kitamura, Y., Oikawa, S., Ono, K., Takaoka, K., 1994. Transient
and localized expression of bone morphogenetic protein 4
messenger RNA during fracture healing. Journal of Bone and
Mineral Research 9, 651–659.
Ohta, S., Muramatsu, H., Senda, T., Zou, K., Iwata, H., Muramatsu,
T., 1999. Midkine is expressed during repair of bone fracture and
promotes chondrogenesis. Journal of Bone and Mineral Research
14, 1132–1144.

ARTICLE IN PRESSJ.H. Holstein et al. / Journal of Biomechanics 40 (2007) 215–219 219
Schmidmaier, G., Wildemann, B., Melis, B., Krummrey, G., Einhorn,
T.A., Haas, N.P., Raschke, M., 2004. Development and character-
ization of a standard closed tibial fracture model in the rat.
European Journal of Trauma 30, 35–42.
Yamagiwa, H., Tokunaga, K., Hayami, T., Hatano, H., Uchida, M.,
Endo, N., Takahashi, H.E., 1999. Expression of metalloproteinase-
13 (collagenase-3) is induced during fracture healing in mice. Bone
25, 197–203.