development and validation of the gi-cognitions questionnaire
TRANSCRIPT

ORIGINAL ARTICLE
Development and Validation of the GI-Cognitions Questionnaire
Melissa G. Hunt • Elisabeth Ertel • Jordan A. Coello •
Lauren Rodriguez
� Springer Science+Business Media New York 2014
Abstract Patients with irritable bowel syndrome (IBS)
have been shown to have catastrophic cognitions regarding
the social and occupational consequences of GI symptoms.
Moreover, the efficacy of cognitive–behavioral therapy for
IBS may be partially mediated by reductions in such cog-
nitions. We aimed to develop and validate a short self-
report measure of GI specific catastrophic cognitions. The
GI-Cognitions Questionnaire (GI-Cog) was administered to
a total of 291 participants, including 65 IBS patients, 114
Crohn’s disease patients, 22 patients with co-morbid Cro-
hn’s and IBS and 90 healthy controls. The GI-Cog showed
high internal consistency (a = .92) and good test re-test
reliability (r = .87) as well as good factor structure. It
discriminated between IBS patients, Crohn’s disease
patients and normal controls, and explained unique vari-
ance in GI symptom severity. The GI-Cog is a short, easy-
to-administer self-report measure of GI specific cata-
strophic cognitions that appears to be both reliable and
valid and can be used in future research on vulnerability,
treatment outcome and mediators of treatment efficacy.
Keywords Catastrophizing � Cognitive–behavioral �Crohn’s disease � IBS � Irritable bowel syndrome
Introduction
Irritable bowel syndrome (IBS) is a functional gastroin-
testinal disorder characterized by recurrent abdominal
pain or discomfort associated with improvement with
defecation; a change in the frequency of stool; and/or a
change in the form or appearance of stool (Longstreth
et al. 2006). In addition to these formal diagnostic criteria
issued by the Rome III workgroup (the arm of the non-
profit Rome Foundation tasked with developing diagnostic
criteria for all functional gastrointestinal disorders)
(Drossman 2006), other symptoms associated with IBS
include bloating, urgency and straining during defecation.
These diagnostic criteria, however, do not fully capture
the burden of illness experienced by many IBS patients
(Lembo et al. 2005). IBS diarrhea is often associated with
burning, cramping abdominal pain and feelings of
urgency, which can significantly disrupt social, occupa-
tional and recreational activities. IBS patients experience
significant reductions in quality of life in a range of areas
including health, vitality, social and occupational func-
tioning, pain, diet, sexual function, and sleep (Luscombe
2000; Cho et al. 2011).
The level of disability, distress and dysfunction experi-
enced by IBS patients does not seem to be explained,
however, by the relatively benign physical symptoms and
is not correlated with actual intestinal motility disturbances
(Lackner and Quigley 2005). Moreover, numerous studies
have shown high levels of co-morbidity between IBS and
psychiatric disorders (Lydiard et al. 1993; Sykes et al.
2003; Gros et al. 2009), particularly Panic Disorder (e.g.
Maunder 1998; Kaplan et al. 1996). Indeed, several studies
have demonstrated that successful treatment of Panic Dis-
order often results in significant reductions in IBS symp-
toms (e.g. Noyes et al. 1990).
The development and validation of the GI-COG was presented in
poster format at the 2009 annual meeting of the Association of
Behavioral and Cognitive Therapies as the IBS Cognitions
Questionnaire.
M. G. Hunt (&) � E. Ertel � J. A. Coello � L. Rodriguez
Department of Psychology, University of Pennsylvania, 3720
Walnut Street, Philadelphia, PA 19104-6241, USA
e-mail: [email protected]
123
Cogn Ther Res
DOI 10.1007/s10608-014-9607-y
Cognitive models of Panic Disorder suggest that panic is
often precipitated by catastrophic misinterpretations of
bodily sensations (Clark 1986; Casey et al. 2004) along
with high levels of anxiety sensitivity and somatic hyper-
vigilance (Perez et al. 2009; Schmidt et al. 2003). There is
evidence that IBS patients are prone to similar cognitive
processes. IBS patients have been shown to be hypervigi-
lant to GI sensations (Posserud et al. 2009) and are high in
anxiety about visceral sensations (Hazlett-Stevens et al.
2003; Labus et al. 2004; Labus et al. 2007). Recent work
has suggested that IBS patients also show illness specific
catastrophic cognitions such as pain-catastrophizing (Gros
et al. 2009; Lackner et al. 2004b). IBS patients also hold a
number of catastrophic and dysfunctional beliefs about IBS
symptoms and about the social and occupational implica-
tions of those symptoms (Hunt et al. 2009a). Moreover,
reductions in IBS specific catastrophic thinking were
shown to partially mediate the efficacy of cognitive–
behavioral treatment for IBS in one recent clinical trial
(Hunt et al. 2009b).
Indeed, the beliefs of IBS patients look more like the
catastrophic beliefs of Panic patients, than they look like the
beliefs of most patients with Crohn’s Disease, an inflam-
matory bowel disease (Hunt et al. 2009a). Crohn’s patients
are a particularly relevant comparison group, as Crohn’s
shares many symptoms with IBS (especially abdominal
pain and diarrhea) and has many serious, potentially life
threatening complications. Nevertheless, Crohn’s patients
typically exhibit lower rates of psychiatric co-morbidity
than do IBS patients (Walker et al. 1990, North and Alpers
1994) and also show less propensity towards catastrophic,
distorted beliefs about their symptoms (Hunt et al. 2009a).
In a comprehensive review of cognitive and behavioral
therapies for IBS, Blanchard (2005) noted that the efficacy
of CBT for IBS seems due, at least in part, to changes in
the maladaptive cognitive processes that underlie IBS. He
notes that almost all CBT treatment protocols involve
psychoeducation about the GI system and the link between
IBS and stress, and that this undoubtedly marks the
beginning of cognitive change for patients. He also pointed
out that while most interventions include a relaxation
training component, relaxation-only conditions typically do
not do well. Two prior RCTs of CBT for IBS (Greene and
Blanchard 1994 and Payne and Blanchard 1995) attempted
to measure cognitive change with two standard (not IBS
specific) measures of maladaptive cognitions. These
included the Dysfunctional Attitude Scale (Weissman and
Beck 1978) and the Automatic Thoughts Questionnaire
(Hollon and Kendall 1980). Both studies found that mal-
adaptive cognitions declined significantly in the cognitive
therapy groups, but not in the symptom monitoring groups,
and that cognitive change was correlated with change in GI
symptoms.
Toner et al. (1998) developed a measure that is more
specific to the cognitions associated with IBS. The Cog-
nitive Scale for Functional Bowel Disorders (CS-FBD) was
designed to reflect a number of a priori themes, some of
which are directly related to GI symptoms like pain ca-
tastrophizing (e.g. ‘‘Bowel symptoms are agony’’), some of
which are related to social and occupational implications of
having IBS (e.g. ‘‘With frequent bathroom visits, others
think something is wrong’’) and a number of which are
related to more general themes of perfectionism and poor
self-care, but are not specific to GI symptoms (e.g. ‘‘Being
late upsets me’’ ‘‘Hate making a fool of myself’’ and
‘‘Feeling guilt if I nurture myself’’).
Toner’s scale, like the DAS and the ATQ, has proved
somewhat sensitive to treatment related changes during
CBT for IBS. Tkachuk et al. (2003) found that while the
CS-FBD changed significantly over the course of CBT, it
did not correlate well with IBS symptom change, which
was minimal in in their trial. Drossman et al. (2003) also
found that patients in the CBT condition changed signifi-
cantly on the CS-FBD. They also obtained significant
reductions in IBS symptoms, but changes on the CS-FBD
were related to some indices of change (like patient global
ratings of satisfaction) but not to others (like pain). Blan-
chard (2005, page 118) concluded that change on the CS-
FBD ‘‘does not seem related to symptomatic change.’’ This
is disappointing, but could be due to the inclusion of items
reflecting many maladaptive cognitions that might be
expected to change with good CBT, but are not actually
specific to GI symptoms.
There are good measures of IBS symptom severity
(Svedlund et al. 1988; Wiklund et al. 2003), quality of life
(Drossman et al. 2000) and visceral sensitivity (VSI, Labus
et al. 2007). The VSI captures an individual’s anxiety about
GI sensations (e.g. ‘‘When I feel discomfort in my belly, it
frightens me’’), hypervigilance and awareness of GI sen-
sations (e.g. ‘‘I am constantly aware of the feelings I have
in my belly’’), and fear and avoidance of food related sit-
uations (e.g. ‘‘I get anxious when I go to a new restau-
rant’’). It does not address why people are hypervigilant,
frightened and avoidant (i.e. because they have cata-
strophic beliefs about what might happen when they go to a
new restaurant). In some other studies of IBS specific
beliefs (Hunt et al. 2009a, b) catastrophic cognitions were
elicited as free responses to hypothetical scenarios, which
then needed to be coded by blind raters. Such methodology
is cumbersome and time consuming, and cannot be easily
disseminated for use in clinical trials. Thus, the goal of the
current study was to develop and provide initial validation
of a brief, easy-to-score, self-report measure of GI-specific
catastrophic cognitions. We hypothesize that this new
measure that captures GI-specific catastrophic cognitions
will discriminate between IBS, Crohn’s, and healthy
Cogn Ther Res
123
controls and will predict GI-symptom severity and quality
of life over and above existing measures of gastrointestinal
symptom-specific anxiety.
Method
Subjects
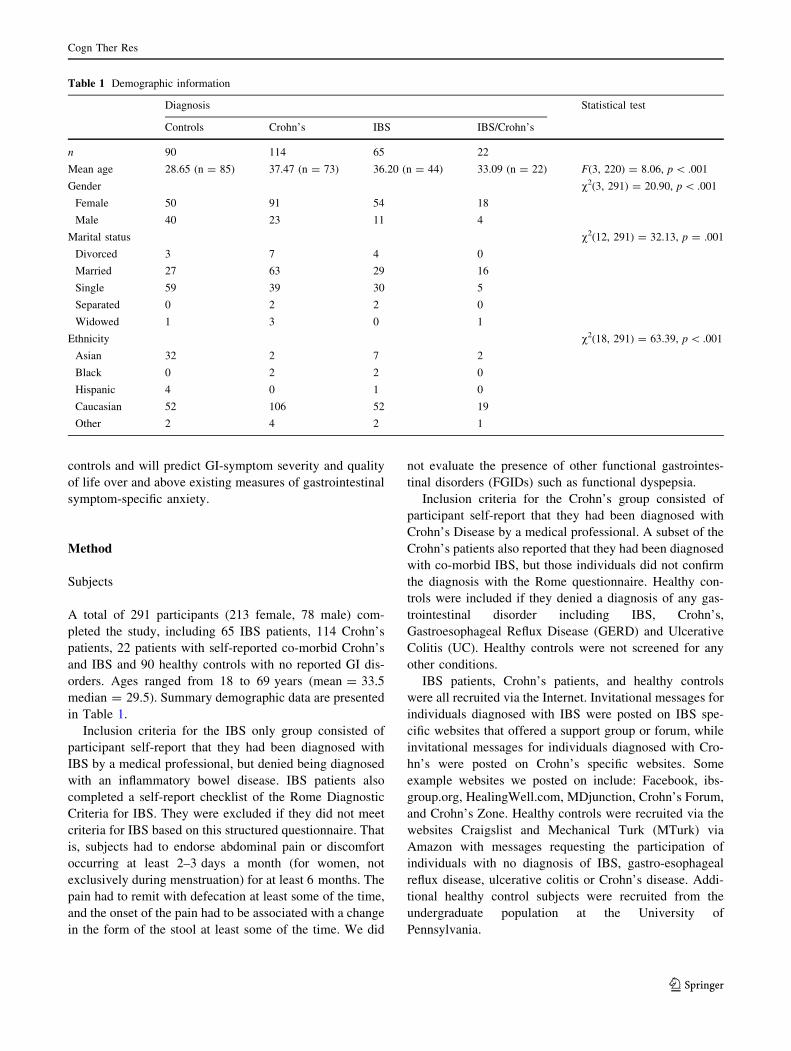
A total of 291 participants (213 female, 78 male) com-
pleted the study, including 65 IBS patients, 114 Crohn’s
patients, 22 patients with self-reported co-morbid Crohn’s
and IBS and 90 healthy controls with no reported GI dis-
orders. Ages ranged from 18 to 69 years (mean = 33.5
median = 29.5). Summary demographic data are presented
in Table 1.
Inclusion criteria for the IBS only group consisted of
participant self-report that they had been diagnosed with
IBS by a medical professional, but denied being diagnosed
with an inflammatory bowel disease. IBS patients also
completed a self-report checklist of the Rome Diagnostic
Criteria for IBS. They were excluded if they did not meet
criteria for IBS based on this structured questionnaire. That
is, subjects had to endorse abdominal pain or discomfort
occurring at least 2–3 days a month (for women, not
exclusively during menstruation) for at least 6 months. The
pain had to remit with defecation at least some of the time,
and the onset of the pain had to be associated with a change
in the form of the stool at least some of the time. We did
not evaluate the presence of other functional gastrointes-
tinal disorders (FGIDs) such as functional dyspepsia.
Inclusion criteria for the Crohn’s group consisted of
participant self-report that they had been diagnosed with
Crohn’s Disease by a medical professional. A subset of the
Crohn’s patients also reported that they had been diagnosed
with co-morbid IBS, but those individuals did not confirm
the diagnosis with the Rome questionnaire. Healthy con-
trols were included if they denied a diagnosis of any gas-
trointestinal disorder including IBS, Crohn’s,
Gastroesophageal Reflux Disease (GERD) and Ulcerative
Colitis (UC). Healthy controls were not screened for any
other conditions.
IBS patients, Crohn’s patients, and healthy controls
were all recruited via the Internet. Invitational messages for
individuals diagnosed with IBS were posted on IBS spe-
cific websites that offered a support group or forum, while
invitational messages for individuals diagnosed with Cro-
hn’s were posted on Crohn’s specific websites. Some
example websites we posted on include: Facebook, ibs-
group.org, HealingWell.com, MDjunction, Crohn’s Forum,
and Crohn’s Zone. Healthy controls were recruited via the
websites Craigslist and Mechanical Turk (MTurk) via
Amazon with messages requesting the participation of
individuals with no diagnosis of IBS, gastro-esophageal
reflux disease, ulcerative colitis or Crohn’s disease. Addi-
tional healthy control subjects were recruited from the
undergraduate population at the University of
Pennsylvania.
Table 1 Demographic information
Diagnosis Statistical test
Controls Crohn’s IBS IBS/Crohn’s
n 90 114 65 22
Mean age 28.65 (n = 85) 37.47 (n = 73) 36.20 (n = 44) 33.09 (n = 22) F(3, 220) = 8.06, p \ .001
Gender v2(3, 291) = 20.90, p \ .001
Female 50 91 54 18
Male 40 23 11 4
Marital status v2(12, 291) = 32.13, p = .001
Divorced 3 7 4 0
Married 27 63 29 16
Single 59 39 30 5
Separated 0 2 2 0
Widowed 1 3 0 1
Ethnicity v2(18, 291) = 63.39, p \ .001
Asian 32 2 7 2
Black 0 2 2 0
Hispanic 4 0 1 0
Caucasian 52 106 52 19
Other 2 4 2 1
Cogn Ther Res
123

The study was approved by the University of Pennsyl-
vania’s Internal Review Board.
Measures
Rome III Questionnaire
The Rome III IBS-specific Questionnaire is a widely used
10-item self-report scale that covers the diagnostic criteria
for IBS. It has been found to have acceptable sensitivity
and high specificity as well as good test–retest reliability
(Whitehead et al. 2006).
Visceral Sensitivity Index (VSI)
The VSI (Labus et al. 2004, 2007) is a unidimensional,
15-item scale that measures gastrointestinal symptom-
specific anxiety. It has high internal consistency, (a = .93)
and a mean inter-item correlation of .47 (Hazlett-Stevens
et al. 2003; Labus et al. 2004). It has good criterion, con-
struct and predictive validity (Labus et al. 2007).
Gastrointestinal Symptom Rating Scale-IBS (GSRS-IBS)
The GSRS (Wiklund et al. 2003) is a 13 item self-report
scale that measures GI symptom severity across five
domains (bloating, diarrhea, constipation, pain, and sati-
ety). Each domain has demonstrated high internal consis-
tency, with Cronbach’s alpha ranging from .74 (pain) to .85
(satiety). The scale also demonstrates high test–retest
reliability between the five factors (all r = .55–.70), and
good convergent validity (Wiklund et al. 2003).
Gastrointestinal Cognitions Questionnaire (GI-Cog)
The authors reviewed online IBS discussion forums to
determine common catastrophic thoughts and themes about
the implications of GI symptoms. Patient records from a
past cognitive–behavioral treatment study of IBS (Hunt
et al. 2009b) were also available for review. The initial
item pool for the GI-Cog was developed to reflect the types
of catastrophic fears that are often described clinically by
IBS patients undergoing cognitive–behavioral therapy. In
addition, items were developed to reflect the experiences
and fears IBS patients shared on a number of on-line for-
ums. The item pool was also chosen to reflect the areas that
prior cognitive theories of IBS have explored (Hunt et al.
2009a).
Items included thoughts about Social Embarrassment
(‘‘Having to deal with IBS is incredibly embarrassing’’),
Perceived Incompetence (‘‘If I have to interrupt a meeting
to go to the bathroom it will be awful and people will think
I’m incompetent or unreliable’’), Avoidance/Life
Interference (‘‘When my IBS acts up I have to cancel my
plans and miss out on important parts of my life’’), and
Urgency/Incontinence (‘‘If I feel the urge to defecate and
cannot find a bathroom right away I won’t be able to hold it
and I’ll be incontinent’’). A total of 18 items were included.
Subjects are asked to rate the degree to which they believe
the statements on a 5 point scale ranging from 0 (hardly at
all) to 4 (very much).
Although similar to the VSI in that it aims to identify
gastrointestinal related anxiety in sufferers of IBS, the GI-
Cog focuses more directly on the catastrophic cognitions
IBS sufferers experience that give rise to anxiety and
avoidance. That is, the cognitive–behavioral model of
psychopathology requires not only that we measure mal-
adaptive fear and avoidance, but that we elucidate the
underlying cognitions that presumably cause the anxiety to
occur.
Consistent with FDA guidelines on the development of a
patient-reported outcome measure (FDA PRO guidelines),
initial pilot testing of the draft instrument led to changes in
wording to ensure that we were targeting the intended
population. Because we wanted the questionnaire to be
equally appropriate for all individuals (not just those with
IBS) the term ‘‘IBS’’ was replaced with the term ‘‘gut’’ or
‘‘gut problems.’’ For example, the item ‘‘Having to deal
with IBS is incredibly embarrassing’’ became ‘‘Having to
deal with gut problems is incredibly embarrassing.’’
Irritable Bowel Syndrome Quality of Life (IBS-QoL)
The IBS-QoL is a 34 item self-report scale that measures
impairment in quality of life secondary to bowel problems
(Patrick et al. 1998). Items are rated on a Likert scale
ranging from 1 (not at all) to 5 (a great deal/extremely).
Summed, standardized scores range from 0 (not at all
impaired) to 100 (extremely impaired). The IBS-QoL has 8
subscales, including dysphoria, interference with activity,
body image, health worry, food avoidance, social reaction,
sexual, and relationship. The IBS-QoL has high internal
consistency (Cronbach’s a = .95), as well as high test–
retest reliability and good construct validity (Patrick et al.
1998). Items on the IBS-QoL refer to ‘‘bowel problems’’
and so are equally applicable to individuals with Crohn’s
and healthy controls. To avoid confusion among our sub-
jects, we referred to the measure as the ‘‘GI-QoL’’ but did
not change any item content or wording.
Procedure
Subjects viewed an invitational message on-line and fol-
lowed a link to the study’s home page where they read
about the study and provided consent. Individuals who
entered via an IBS support group forum completed a Rome
Cogn Ther Res
123

Criteria Questionnaire, while those that entered through a
Crohn’s Disease or normal control website did not. All
subjects completed a demographics questionnaire, the GI-
Cog, the VSI, the GSRS, and the IBS-QoL. Participants
were given the option of providing an email address in
order to be contacted for a follow up survey. Those par-
ticipants who provided their e-mail were asked to complete
the GI-Cog again approximately 1 week later, which pro-
vided us with test–retest data for the questionnaire from a
portion of the sample.
Statistical Analyses
To determine the comparability of our samples, we used Chi
square tests to examine diagnostic group differences on
demographic variables excluding age. Age differences
between groups were evaluated using a one-way analysis of
variance (ANOVA) and Tukey’s honestly significant dif-
ference (Tukey’s HSD) tests to correct for multiple com-
parisons. We then explored diagnostic group differences in
symptom severity, visceral sensitivity, and quality of life
separately using ANOVA and Tukey’s HSD tests. The pain,
diarrhea, and constipation symptom severity of our sample
was assessed using Wiklund et al. (2003) GSRS norms for
moderate and severe Rome-diagnosed IBS.
Each of the 18 items on the GI-Cog was tested individ-
ually for discriminative validity using independent t tests
comparing the IBS patients to the normal controls. Items
that did not discriminate were dropped. Dropped items were
then each analyzed using a one-way ANOVA to determine
if the item was able to discriminate between the diagnostic
groups to evaluate for possible re-inclusion in the GI-Cog.
Internal consistency and test–retest reliability were assessed
using Cronbach’s a and Pearson correlations.
Once the non-discriminating items were removed, we
examined the factorability of the remaining items. One
useful test of factorability is the Kaiser–Meyer–Olkin
(KMO) measure of sampling adequacy (Dziuban and
Shirkey 1974). The critical value for this test is .50, with
values above .7 being considered ‘‘middling’’, values above
.8 being considered ‘‘meritorious’’ and values above .9
being considered ‘‘marvelous.’’ After confirming that the
GI-Cog was appropriate for factor analysis, meeting the
assumptions of sampling adequacy and sphericity using the
KMO and Bartlett’s test of sphericity and verifying that the
selected items should be included in the factor analysis by
examining the anti-image matrix and communalities, we
analyzed the remaining items using principal component
analysis with Varimax (orthogonal) rotation and Kaiser
Normalization. Principal component analysis was used to
identify underlying constructs and compute composite
scores for factors. Items with Eigenvalues greater than 1
were extracted.
To assess the discriminative and predictive validity of
our measure, we tested whether the GI-Cog discriminated
by diagnosis and predicted GI symptom severity and
quality of life using a univariate general linear model with
diagnosis as a fixed factor and Tukey’s HSD. Pearson
correlations were used to examine if the GI-Cog converged
with the VSI. Finally, to determine whether the GI-Cog
explains unique variance in symptom severity above and
beyond visceral sensitivity, we conducted an ANCOVA
predicting symptom severity by diagnosis, with the VSI
and the GI-Cog entered as covariates. All analyses were
completed using SPSS for Windows, Version 20.0.
Results
Comparability of Samples
There were significant between group differences on sev-
eral demographic variables. The diagnostic groups differed
on gender, v2(3, 291) = 20.90, p \ .001, marital status,
v2(12, 291) = 32.13, p = .001, and race, v2(18,
291) = 63.39, p \ .001, but not education, v2(24,
291) = 28.08, p = .26. A one-way ANOVA was con-
ducted to determine group differences in age, F(3,
220) = 8.06, p \ .001. Tukey’s HSD revealed that the
control group (M = 28.65, SD = 12.38) was significantly
younger than the Crohn’s disease group (M = 37.47,
SD = 12.04) and the IBS group (M = 36.20,
SD = 12.12). Individuals in the control group were also
more likely to be single, male and/or Asian, reflecting the
age and race demographics of the University of Pennsyl-
vania. However, the Crohn’s and IBS groups did not differ
significantly on any of the demographic variables. To
correct for possible bias, all analyses were also re-run with
a restricted sample of white women only. See Table 1 for
summary demographic data.
Symptom Severity, Visceral Sensitivity and Quality
of Life
There were significant group differences in GI symptom
severity, visceral sensitivity, and quality of life. We con-
ducted separate ANOVAs predicting scores on the GSRS,
VSI, and IBS-QoL by diagnosis and all ANOVAs were
highly significant (all F [ 49.0, all p \ .001). For symp-
tom severity as measured by GSRS, Tukey’s HSD revealed
that all diagnostic groups were significantly different from
each other (p \ .01), except for IBS and IBS/Crohn’s
groups, which did not differ significantly (p = .42). Con-
trols had the lowest symptom severity, followed by Cro-
hn’s patients, with IBS and IBS/Crohn’s patients notably
having the highest severity scores. These results were the
Cogn Ther Res
123
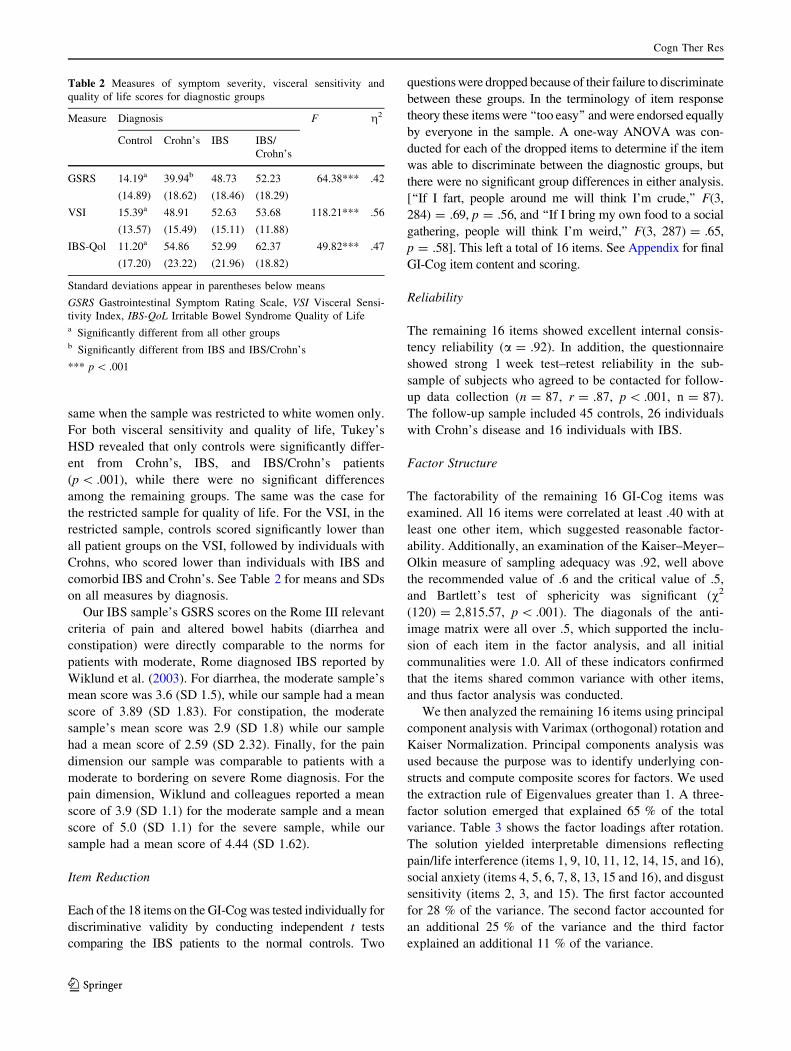
same when the sample was restricted to white women only.
For both visceral sensitivity and quality of life, Tukey’s
HSD revealed that only controls were significantly differ-
ent from Crohn’s, IBS, and IBS/Crohn’s patients
(p \ .001), while there were no significant differences
among the remaining groups. The same was the case for
the restricted sample for quality of life. For the VSI, in the
restricted sample, controls scored significantly lower than
all patient groups on the VSI, followed by individuals with
Crohns, who scored lower than individuals with IBS and
comorbid IBS and Crohn’s. See Table 2 for means and SDs
on all measures by diagnosis.
Our IBS sample’s GSRS scores on the Rome III relevant
criteria of pain and altered bowel habits (diarrhea and
constipation) were directly comparable to the norms for
patients with moderate, Rome diagnosed IBS reported by
Wiklund et al. (2003). For diarrhea, the moderate sample’s
mean score was 3.6 (SD 1.5), while our sample had a mean
score of 3.89 (SD 1.83). For constipation, the moderate
sample’s mean score was 2.9 (SD 1.8) while our sample
had a mean score of 2.59 (SD 2.32). Finally, for the pain
dimension our sample was comparable to patients with a
moderate to bordering on severe Rome diagnosis. For the
pain dimension, Wiklund and colleagues reported a mean
score of 3.9 (SD 1.1) for the moderate sample and a mean
score of 5.0 (SD 1.1) for the severe sample, while our
sample had a mean score of 4.44 (SD 1.62).
Item Reduction
Each of the 18 items on the GI-Cog was tested individually for
discriminative validity by conducting independent t tests
comparing the IBS patients to the normal controls. Two
questions were dropped because of their failure to discriminate
between these groups. In the terminology of item response
theory these items were ‘‘too easy’’ and were endorsed equally
by everyone in the sample. A one-way ANOVA was con-
ducted for each of the dropped items to determine if the item
was able to discriminate between the diagnostic groups, but
there were no significant group differences in either analysis.
[‘‘If I fart, people around me will think I’m crude,’’ F(3,
284) = .69, p = .56, and ‘‘If I bring my own food to a social
gathering, people will think I’m weird,’’ F(3, 287) = .65,
p = .58]. This left a total of 16 items. See Appendix for final
GI-Cog item content and scoring.
Reliability
The remaining 16 items showed excellent internal consis-
tency reliability (a = .92). In addition, the questionnaire
showed strong 1 week test–retest reliability in the sub-
sample of subjects who agreed to be contacted for follow-
up data collection (n = 87, r = .87, p \ .001, n = 87).
The follow-up sample included 45 controls, 26 individuals
with Crohn’s disease and 16 individuals with IBS.
Factor Structure
The factorability of the remaining 16 GI-Cog items was
examined. All 16 items were correlated at least .40 with at
least one other item, which suggested reasonable factor-
ability. Additionally, an examination of the Kaiser–Meyer–
Olkin measure of sampling adequacy was .92, well above
the recommended value of .6 and the critical value of .5,
and Bartlett’s test of sphericity was significant (v2
(120) = 2,815.57, p \ .001). The diagonals of the anti-
image matrix were all over .5, which supported the inclu-
sion of each item in the factor analysis, and all initial
communalities were 1.0. All of these indicators confirmed
that the items shared common variance with other items,
and thus factor analysis was conducted.
We then analyzed the remaining 16 items using principal
component analysis with Varimax (orthogonal) rotation and
Kaiser Normalization. Principal components analysis was
used because the purpose was to identify underlying con-
structs and compute composite scores for factors. We used
the extraction rule of Eigenvalues greater than 1. A three-
factor solution emerged that explained 65 % of the total
variance. Table 3 shows the factor loadings after rotation.
The solution yielded interpretable dimensions reflecting
pain/life interference (items 1, 9, 10, 11, 12, 14, 15, and 16),
social anxiety (items 4, 5, 6, 7, 8, 13, 15 and 16), and disgust
sensitivity (items 2, 3, and 15). The first factor accounted
for 28 % of the variance. The second factor accounted for
an additional 25 % of the variance and the third factor
explained an additional 11 % of the variance.
Table 2 Measures of symptom severity, visceral sensitivity and
quality of life scores for diagnostic groups
Measure Diagnosis F g2
Control Crohn’s IBS IBS/
Crohn’s
GSRS 14.19a
(14.89)
39.94b
(18.62)
48.73
(18.46)
52.23
(18.29)
64.38*** .42
VSI 15.39a
(13.57)
48.91
(15.49)
52.63
(15.11)
53.68
(11.88)
118.21*** .56
IBS-Qol 11.20a
(17.20)
54.86
(23.22)
52.99
(21.96)
62.37
(18.82)
49.82*** .47
Standard deviations appear in parentheses below means
GSRS Gastrointestinal Symptom Rating Scale, VSI Visceral Sensi-
tivity Index, IBS-QoL Irritable Bowel Syndrome Quality of Lifea Significantly different from all other groupsb Significantly different from IBS and IBS/Crohn’s
*** p \ .001
Cogn Ther Res
123
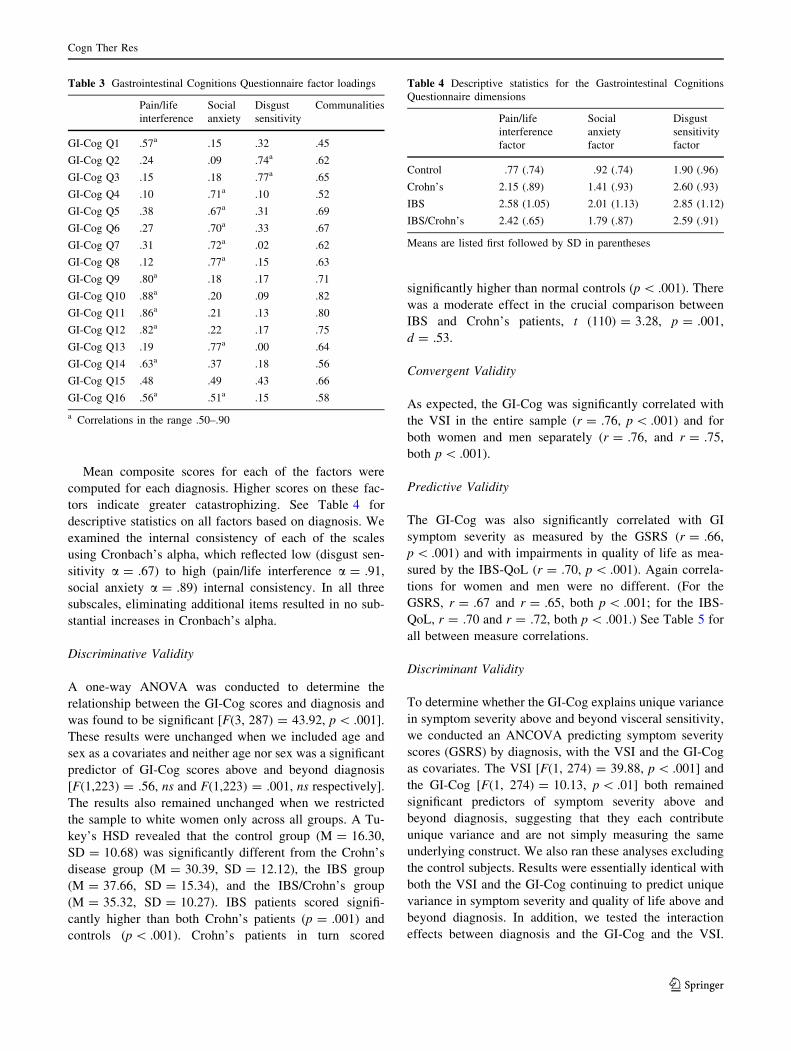
Mean composite scores for each of the factors were
computed for each diagnosis. Higher scores on these fac-
tors indicate greater catastrophizing. See Table 4 for
descriptive statistics on all factors based on diagnosis. We
examined the internal consistency of each of the scales
using Cronbach’s alpha, which reflected low (disgust sen-
sitivity a = .67) to high (pain/life interference a = .91,
social anxiety a = .89) internal consistency. In all three
subscales, eliminating additional items resulted in no sub-
stantial increases in Cronbach’s alpha.
Discriminative Validity
A one-way ANOVA was conducted to determine the
relationship between the GI-Cog scores and diagnosis and
was found to be significant [F(3, 287) = 43.92, p \ .001].
These results were unchanged when we included age and
sex as a covariates and neither age nor sex was a significant
predictor of GI-Cog scores above and beyond diagnosis
[F(1,223) = .56, ns and F(1,223) = .001, ns respectively].
The results also remained unchanged when we restricted
the sample to white women only across all groups. A Tu-
key’s HSD revealed that the control group (M = 16.30,
SD = 10.68) was significantly different from the Crohn’s
disease group (M = 30.39, SD = 12.12), the IBS group
(M = 37.66, SD = 15.34), and the IBS/Crohn’s group
(M = 35.32, SD = 10.27). IBS patients scored signifi-
cantly higher than both Crohn’s patients (p = .001) and
controls (p \ .001). Crohn’s patients in turn scored
significantly higher than normal controls (p \ .001). There
was a moderate effect in the crucial comparison between
IBS and Crohn’s patients, t (110) = 3.28, p = .001,
d = .53.
Convergent Validity
As expected, the GI-Cog was significantly correlated with
the VSI in the entire sample (r = .76, p \ .001) and for
both women and men separately (r = .76, and r = .75,
both p \ .001).
Predictive Validity
The GI-Cog was also significantly correlated with GI
symptom severity as measured by the GSRS (r = .66,
p \ .001) and with impairments in quality of life as mea-
sured by the IBS-QoL (r = .70, p \ .001). Again correla-
tions for women and men were no different. (For the
GSRS, r = .67 and r = .65, both p \ .001; for the IBS-
QoL, r = .70 and r = .72, both p \ .001.) See Table 5 for
all between measure correlations.
Discriminant Validity
To determine whether the GI-Cog explains unique variance
in symptom severity above and beyond visceral sensitivity,
we conducted an ANCOVA predicting symptom severity
scores (GSRS) by diagnosis, with the VSI and the GI-Cog
as covariates. The VSI [F(1, 274) = 39.88, p \ .001] and
the GI-Cog [F(1, 274) = 10.13, p \ .01] both remained
significant predictors of symptom severity above and
beyond diagnosis, suggesting that they each contribute
unique variance and are not simply measuring the same
underlying construct. We also ran these analyses excluding
the control subjects. Results were essentially identical with
both the VSI and the GI-Cog continuing to predict unique
variance in symptom severity and quality of life above and
beyond diagnosis. In addition, we tested the interaction
effects between diagnosis and the GI-Cog and the VSI.
Table 3 Gastrointestinal Cognitions Questionnaire factor loadings
Pain/life
interference
Social
anxiety
Disgust
sensitivity
Communalities
GI-Cog Q1 .57a .15 .32 .45
GI-Cog Q2 .24 .09 .74a .62
GI-Cog Q3 .15 .18 .77a .65
GI-Cog Q4 .10 .71a .10 .52
GI-Cog Q5 .38 .67a .31 .69
GI-Cog Q6 .27 .70a .33 .67
GI-Cog Q7 .31 .72a .02 .62
GI-Cog Q8 .12 .77a .15 .63
GI-Cog Q9 .80a .18 .17 .71
GI-Cog Q10 .88a .20 .09 .82
GI-Cog Q11 .86a .21 .13 .80
GI-Cog Q12 .82a .22 .17 .75
GI-Cog Q13 .19 .77a .00 .64
GI-Cog Q14 .63a .37 .18 .56
GI-Cog Q15 .48 .49 .43 .66
GI-Cog Q16 .56a .51a .15 .58
a Correlations in the range .50–.90
Table 4 Descriptive statistics for the Gastrointestinal Cognitions
Questionnaire dimensions
Pain/life
interference
factor
Social
anxiety
factor
Disgust
sensitivity
factor
Control .77 (.74) .92 (.74) 1.90 (.96)
Crohn’s 2.15 (.89) 1.41 (.93) 2.60 (.93)
IBS 2.58 (1.05) 2.01 (1.13) 2.85 (1.12)
IBS/Crohn’s 2.42 (.65) 1.79 (.87) 2.59 (.91)
Means are listed first followed by SD in parentheses
Cogn Ther Res
123

None of the interaction terms even approached signifi-
cance, and thus were dropped.
Discussion
The results of this study suggest that the GI-Cog is a
reliable and valid measure for assessing catastrophic cog-
nitions in patients with GI disorders. The measure has
excellent internal consistency and 1 week test–retest reli-
ability. It had good discriminative validity and was able to
differentiate between patients with IBS and normal con-
trols with no gastrointestinal disorder. It also was able to
discriminate between patients with IBS and Crohn’s Dis-
ease, with IBS patients scoring significantly higher even
though their symptom severity and visceral sensitivity were
comparable to the Crohn’s group. Perhaps even more
importantly, the GI-Cog was somewhat useful in identify-
ing a group of patients with co-morbid Crohn’s and IBS,
suggesting that catastrophic thinking may be a risk factor
for the development of secondary or co-morbid IBS in IBD
patients. The GI-Cog also showed good convergent valid-
ity, as it was strongly correlated with the VSI, as well as
predictive validity in that it correlated well with symptom
severity and quality of life.
The strength of the correlation between the VSI and the
GI-Cog raises the question of whether the GI-Cog has
sufficient discriminant validity. Indeed, visceral anxiety is
probably closely related to catastrophic cognitions. Inter-
estingly, however, the VSI did not discriminate between
IBS patients and Crohn’s patients. This is probably because
the content of the VSI covers fear of visceral sensations
and GI processes, some of which could be exaggerated (in
the case of IBS), but some of which could be realistic (in
the case of Crohn’s). For example, the VSI items ‘‘I often
worry about problems in my belly’’ and ‘‘I often feel dis-
comfort in my belly could be a sign of a serious illness’’ are
appropriate and realistic for Crohn’s patients, but not for
IBS patients. The GI-Cog goes beyond anxiety about vis-
ceral sensations per se and begins to delineate the cata-
strophic, distorted cognitions that may underlie that anxiety
in IBS. This may be why the GI-Cog both effectively
discriminates between IBS and Crohn’s patients and
explains unique variance in GI symptom severity above
and beyond both diagnosis and visceral sensitivity.
This is not to say, however, that Crohn’s patients never
catastrophize or develop distorted cognitions surrounding
their symptoms. On the contrary, Crohn’s patients still
worry about the impact of GI symptoms significantly more
than normal controls, indicating that this patient group
might also benefit from cognitive–behavioral interventions.
Furthermore, the subgroup of participants who indicated a
diagnosis of both IBS and Crohn’s suggests that catastro-
phizing may make Crohn’s patients vulnerable to the
development of secondary IBS, even when their Crohn’s
disease is under good control.
This study had a number of limitations, particularly with
respect to the sample. First, we did not require physician
confirmation of diagnosis for either IBS or Crohn’s Dis-
ease, but relied on patient self-report. It is unlikely that an
individual would claim a diagnosis of Crohn’s disease
without having received the diagnosis from a medical
professional after appropriate diagnostic testing. However,
it is possible that there were some patients with functional
GI disorders alone in the putative Crohn’s group. If any-
thing, this should have made it more difficult for us to
demonstrate discriminative validity. A ‘‘cleaner’’ sample
would presumably have reduced overlap between the two
groups and would have yielded lower mean scores on the
GI-Cog for the Crohn’s group. On the other hand, IBS is
relatively easy to ‘‘self-diagnose’’ and it may be that some
of the individuals within the IBS group would not actually
have met Rome criteria for IBS had more stringent diag-
nostic procedures been in place. Thus, some individuals in
our IBS sample may not actually have met severity or
duration criteria for IBS. Similarly, however, including
sub-syndromal individuals in the sample should bias the
results against us, making it more difficult to establish
discriminative validity between the IBS group and the
healthy controls. In addition, when comparing the IBS
samples’ symptom severity to existing norms, on average
our IBS sample was in the moderate range of severity.
Since our IBS group scored significantly higher on the GI-
Cog than both the Crohn’s group and the healthy controls
despite these limitations, we can assume that our findings
might have been stronger had we excluded individuals
based on failing to meet physician confirmed diagnostic
criteria for either IBS or Crohn’s.
With respect to the Crohn’s sample, we do not have
information pertaining to the disease state of individuals.
Some may have been experiencing active symptom flare
ups, while some might have been in remission. This makes
the symptom severity findings a bit hard to interpret. Are
IBS patients reporting greater GI symptom severity than
Table 5 Correlations between measures
GSRS VSI IBSQoL
GI-COG .76* .66* .70*
GSRS .75* .72*
VSI .83*
GI-COG Gastrointestinal Cognitions Questionnaire, GSRS Gastroin-
testinal Symptom Rating Scale, VSI Visceral Sensitivity Index, IBS-
QoL Irritable Bowel Syndrome Quality of Life
* p \ .001
Cogn Ther Res
123

Crohn’s patients who are in remission, or are they reporting
greater severity than Crohn’s patients with active disease?
We cannot be certain about this based on the current data
set. Nevertheless, the GI-Cog refers to stable beliefs about
the impact of GI symptoms when they are happening, and
does not assume that the individual is currently experi-
encing GI symptoms. Indeed, some of the items are
explicitly conditional, such as ‘‘If I’m experiencing a gut
attack and feeling sick, I can’t enjoy or pay attention to
anything else.’’ While it is possible that current disease
state would bias the responses of the Crohn’s patients, it is
also possible that the GI-Cog does indeed capture a stable
vulnerability to catastrophic cognitions that is independent
of current disease status. Future research is needed to
establish how the course of Crohn’s Disease interacts with
catastrophizing and visceral sensitivity.
The second major limitation of our sampling procedure
was that the healthy comparison group was not well mat-
ched demographically to the patient groups in a few
important respects. The control sample was recruited from
college students as well as older adults through online
forums. This sample tended to be single, had higher pro-
portions of Asian participants as well as males, and was
significantly younger on average than both the Crohn’s
disease and IBS patient samples. This limits the general-
izability of the findings with respect to the healthy controls,
and is especially problematic since both males and Asians
tend to have lower prevalence rates of anxiety related
disorders (McLean et al. 2011; Asnaani et al. 2010).
However, we did run several of the analyses controlling for
age and gender, which made no difference at all and we re-
ran a number of the crucial comparisons with a restricted
sample of white women only. Again, the findings were
essentially unchanged. Since the crucial comparisons were
really between the patient groups, which were well-mat-
ched demographically, we believe that this limitation is
less severe than it initially appears.
Another limitation is that other functional disorders
(such as functional dyspepsia) were not ruled out. We
recognize that other functional disorders may be related to
the severity of catastrophic thinking, visceral sensitivity,
symptoms and their impact on quality of life. However, the
GI-Cog focuses specifically on gut distress, not nausea,
heartburn, early satiety or other symptoms of dyspepsia.
Thus, it is unclear how screening such individuals in or out
of the study would have altered the results.
The final limitation of the study is that we were unaware
of the existence of the Cognitive Scale for Functional
Bowel Disorders (CS-FBD) developed by Toner et al.
(1998) which has some conceptual overlap with the GI-
Cog, when we developed our questionnaire. Had we known
about it, we would certainly have included it in the current
study. In one study, the CS-FBD proved to be somewhat
sensitive to therapeutic change during CBT for IBS
(Drossman et al. 2003), but in another study it was unre-
lated to symptom improvement (Tkachuk et al. 2003).
Blanchard (2005) concluded that the CS-FBD did not seem
to be related to symptomatic change, and it has not been
used in any further studies that we are aware of. An
advantage of the GI-COG over the CS-FBD is that the CS-
FBD includes many items that reflect general maladaptive
beliefs that are not GI specific. We hope that the GI-COG
will prove more sensitive to process and outcome changes
in successful CBT for IBS. Nevertheless, an important
future study might directly compare the CS-FBD and the
GI-COG to establish their relative convergent and dis-
criminant validity. We also might have included the Pain
Catastrophizing Scale (Sullivan et al. 1995), which shares
some conceptual overlap with both visceral anxiety and GI
symptom specific catastrophizing.
Despite these limitations, we believe that this study
provides compelling initial validation of a unique measure
of cognitive processes that may be highly relevant to the
development and maintenance of IBS. It has proved to
have good concurrent, predictive and discriminative or
known-groups validity, successfully distinguishing
between IBS patients and Crohn’s patients.
Future research endeavors could benefit from the use of the
GI-Cog not only in understanding IBS, but also in evaluating
the treatment of IBS, and in predicting vulnerability to the
development of secondary IBS in IBD patient populations.
Cognitive–behavioral therapy has been shown to be effective
in the treatment of IBS (e.g., Hunt et al. 2009b; Drossman et al.
2003; Craske et al. 2011; Lackner et al. 2004a; Ljotsson et al.
2011). Good CBT targets both behavioral avoidance and
distorted beliefs about GI symptoms and the implications of
those symptoms for social, occupational and recreational
functioning. The GI-Cog is a short, easy-to-administer self-
report measure that can be used to assess vulnerability, track
changes in catastrophic thinking during treatment and exam-
ine possible process variables underlying successful therapy.
Conflict of Interest Melissa G. Hunt, Elisabeth Ertel, Jordan A.
Coello and Lauren Rodriguez declare that they have no conflict of
interest. This research was unfunded.
Informed Consent All procedures followed were in accordance
with the ethical standards of the responsible committee on human
experimentation (institutional and national) and with the Helsinki
Declaration of 1975, as revised in 2000 (5). Informed consent was
obtained from all patients for being included in the study.
Animal Rights No animal studies were carried out by the authors
for this article.
Cogn Ther Res
123

Appendix
References
Asnaani, A., Richey, J. A., Dimaite, R., Hinton, D. E., & Hofmann, S.
G. (2010). A cross-ethnic comparison of lifetime prevalence
rates of anxiety disorders. Journal of Nervous and Mental
Disease, 198(8), 551–555.
Blanchard, E. B. (2005). A critical review of cognitive, behavioral,
and cognitive–behavioral therapies for irritable bowel syndrome.
Journal of Cognitive Psychotherapy: An International Quarterly,
19(2), 101–123.
Casey, L. M., Oei, T. P., Newcombe, P. A., & Kenardy, J. (2004). The
role of catastrophic misinterpretation of bodily sensations and
panic self-efficacy in predicting panic severity. Journal of
Anxiety Disorders, 18(3), 325–340.
Cho, H. S., Park, J. M., Lim, C. H., Cho, Y. K., Lee, I. S., Kim, S. W.,
et al. (2011). Anxiety, depression and quality of life in patients
with irritable bowel syndrome. Gut and Liver, 5(1), 29–36.
Clark, D. M. (1986). A cognitive approach to panic. Behaviour
Research and Therapy, 24, 461–470.
Craske, M. G., Wolitzky-Taylor, K. B., Labus, J., Wu, S., Frese, M.,
Mayer, E. A., et al. (2011). A cognitive–behavioral treatment for
irritable bowel syndrome using interoceptive exposure to visceral
sensations. Behaviour Research and Therapy, 49, 413–421.
Drossman, D. A. (2006). The functional gastrointestinal disorders and
the Rome III process. Gastroenterology, 130(5), 1377–1390.
Drossman, D. A., Patrick, D. L., Whitehead, W. E., Toner, B. B.,
Diamant, N. E., Hu, Y., et al. (2000). Further validation of the
IBS–QOL: A disease-specific quality-of-life questionnaire.
American Journal of Gastroenterology, 95(4), 999–1007.
Drossman, D. A., Toner, B. B., Whitehead, W. E., Diamant, N. E.,
Dalton, C. B., Duncan, S., et al. (2003). Cognitive–behavioral
therapy versus education and desipramine versus placebo for
moderate to severe functional bowel disorders. Gastroenterol-
ogy, 125, 19–31.
Dziuban, C. D., & Shirkey, E. C. (1974). When is a correlation matrix
appropriate for factor analysis? Some decision rules. Psycho-
logical Bulletin, 81(6), 358–361.
Greene, B., & Blanchard, E. B. (1994). Cognitive therapy for irritable
bowel syndrome. Journal of Consulting and Clinical Psychol-
ogy, 62, 576–582.
Gros, D. F., Antony, M. M., McCabe, R. E., & Swinson, R. P. (2009).
Frequency and severity of the symptoms of irritable bowel
syndrome across the anxiety disorders and depression. Journal of
Anxiety Disorders, 23(2), 290–296.
Hazlett-Stevens, H., Craske, M. G., Mayer, E. A., Chang, L., &
Naliboff, B. D. (2003). Prevalence of irritable bowel syndrome
among university students: The roles of worry, neuroticism,
GI Cognitions Questionnaires (GI-Cog)
Please rate the degree to which you believe each of the following statements Hardly
at all
A little
bit
Moderately A fair
bit
Very
much
1 If I feel the urge to defecate and cannot find a bathroom right away I won’t be able
to hold it and I’ll be incontinent
0 1 2 3 4
2 The thought of fecal incontinence is terrifying. If it happened, it would be awful 0 1 2 3 4
3 If I fart, people around me will be disgusted 0 1 2 3 4
4 If I don’t drink or eat with other people, they will think I’m antisocial and no fun 0 1 2 3 4
5 If I have to get up and leave an event, meeting or social gathering to go to the
bathroom people will think there’s something wrong with me
0 1 2 3 4
6 If I have to interrupt a meeting or presentation at work to go to the bathroom, it will
be awful, and people will think I’m incompetent or unreliable
0 1 2 3 4
7 If I have stop or leave to find a bathroom during an outing or trip my friends and
family will be frustrated and annoyed with me
0 1 2 3 4
8 If I told my coworkers or friends about my gut problems they wouldn’t understand
and would think I was weak or gross
0 1 2 3 4
9 When I feel my GI symptoms acting up, I’m afraid the pain will be excruciating and
intolerable
0 1 2 3 4
10 When my gut acts up, I have to cancel my plans and miss out on important parts of
life
0 1 2 3 4
11 If I’m experiencing a gut attack and feeling sick, I can’t enjoy or pay attention to
anything else
0 1 2 3 4
12 Having a gut attack during an outing or get together ruins the experience 0 1 2 3 4
13 If people knew about my gut problems, they would think about me negatively 0 1 2 3 4
14 If I leave the house without my emergency medicine(s) (e.g. Imodium, Lomotil,
Pepto-Bismol, Gas-Ex, Tums) it could lead to disaster
0 1 2 3 4
15 Having to deal with gut problems is incredibly embarrassing 0 1 2 3 4
16 If people knew what my life was really like they would think I was crazy 0 1 2 3 4
Subscale structure: Pain/life interference: items 1, 9, 10, 11, 12, 14, 15, and 16; Social anxiety: items 4, 5, 6, 7, 8, 13, 15 and 16; Disgust
sensitivity: items 2, 3, and 15
Cogn Ther Res
123

anxiety sensitivity and visceral anxiety. Journal of Psychoso-
matic Research, 55(6), 501–505.
Hollon, S. D., & Kendall, P. E. (1980). Cognitive self-statements in
depression: Development of an Automatic Thoughts Question-
naire. Cognitive Therapy and Research, 4, 383–396.
Hunt, M. G., Milonova, M., & Moshier, S. (2009a). Catastrophizing
the consequences of gastrointestinal symptoms in irritable bowel
syndrome. Journal of Cognitive Psychotherapy: An International
Quarterly, 23(2), 160–173.
Hunt, M. G., Moshier, S., & Milonova, M. (2009b). Brief cognitive–
behavioral internet therapy for irritable bowel syndrome.
Behavior Research and Therapy, 47, 797–802.
Kaplan, D. S., Masand, P. S., & Gupta, S. (1996). The relationship of
irritable bowel syndrome (IBS) and panic disorder. Annals of
Clinical Psychiatry, 8(2), 81–88.
Labus, J. S., Bolus, R., Chang, L., Wiklund, I., Naesdal, J., Mayer, E.
A., et al. (2004). The visceral sensitivity index: Development
and validation of a gastrointestinal symptom-specific anxiety
scale. Alimentary Pharmacology & Therapeutics, 20, 89–97.
Labus, J. S., Mayer, E. A., Chang, L., Bolus, R., & Naliboff, B. D.
(2007). The central role of gastrointestinal-specific anxiety in
irritable bowel syndrome: Further validation of the visceral
sensitivity index. Psychosomatic Medicine, 69, 89–98.
Lackner, J. M., Morley, S., Dowzer, C., Mesmer, C., & Hamilton, S.
(2004a). Psychological treatments for irritable bowel syndrome:
A systematic review and meta-analysis. Journal of Consulting
and Clinical Psychology, 72(6), 1100–1113.
Lackner, J. M., & Quigley, B. M. (2005). Pain catastrophizing
mediates the relationship between worry and pain suffering in
patients with irritable bowel syndrome. Behaviour Research and
Therapy, 43, 943–957.
Lackner, J. M., Quigley, B. M., & Blanchard, E. B. (2004b).
Depression and abdominal pain in IBS patients: The mediating
role of catastrophizing. Psychosomatic Medicine, 66, 435–441.
Lembo, A., Ameen, V. Z., & Drossman, D. A. (2005). Irritable bowel
syndrome: toward an understanding of severity. Clinical Gas-
troenterology & Hepatology, 3(8), 717–725.
Ljotsson, B., Hedman, E., Lindfors, P., Hursti, T., Lindefors, N.,
Andersson, G., et al. (2011). Long-term follow-up of internet-
delivered exposure and mindfulness based treatment for irritable
bowel syndrome. Behaviour Research and Therapy, 49(1), 58–61.
Longstreth, G. F., Thompson, W. G., Chey, W. D., Houghton, L. A.,
Mearin, F., & Spiller, R. C. (2006). Functional Bowel Disorders.
Gastroenterology, 130, 1480–1491.
Luscombe, F. A. (2000). Health-related quality of life and associated
psychosocial factors in irritable bowel syndrome: A review.
Quality of Life Research, 9(2), 161–176.
Lydiard, R. B., Fossey, M. D., Marsh, W., & Ballenger, J. C. (1993).
Prevalence of psychiatric disorder in patients with irritable
bowel syndrome. Psychosomatics, 34(3), 229–234.
Maunder, R. G. (1998). Panic disorder associated with gastrointestinal
disease: Review and hypotheses. Journal of Psychosomatic
Research, 44(1), 91–105.
McLean, C. P., Asnaani, A., Litz, B. T., & Hofmann, S. G. (2011).
Gender differences in anxiety disorders: Prevalence, course of
illness, comorbidity and burden of illness. Journal of Psychiatric
Research, 45(8), 1027–1035.
North, C. S., & Alpers, D. H. (1994). A review of studies of
psychiatric factors in Crohn’s disease: Etiologic implications.
Annals of Clinical Psychiatry, 6(2), 117–124.
Noyes, R., Cook, B., Garvey, M., & Summers, R. (1990). Reduction
of gastrointestinal symptoms following treatment for panic
disorder. Psychosomatics, 31, 75–79.
Patrick, D. L., Drossman, D. A., Frederick, I. O., DiCesare, J., &
Puder, K. L. (1998). Quality of life in persons with irritable
bowel syndrome: Development and validation of a new measure.
Digestive Diseases and Sciences, 43(2), 400–411.
Payne, A., & Blanchard, E. B. (1995). A controlled comparison of
cognitive therapy and self-help support groups in the treatment
of irritable bowel syndrome. Journal of Consulting and Clinical
Psychology, 63, 779–786.
Perez, B., Carlos, I., Shea, M. T., Raffa, S., Rende, R., Dyck, I. R.,et al. (2009). Anxiety sensitivity as a predictor of the clinical
course of panic disorder: A 1-year follow-up study. Depression
and Anxiety, 26(4), 335–342.
Posserud, I., Svedlund, J., Wallin, J., & Simren, M. (2009).
Hypervigilance in irritable bowel syndrome compared with
organic gastrointestinal disease. Journal of Psychosomatic
Research, 66, 399–405.
Schmidt, N. B., Joiner, T. E., Staab, J. P., & Williams, F. M. (2003).
Health perceptions and anxiety sensitivity in patients with panic
disorder. Journal of Psychopathology and Behavioral Assess-
ment, 25(3), 139–145.
Sullivan, M. J. L., Bishop, S., & Pivik, J. (1995). The pain
catastrophizing scale: Development and validation. Psycholog-
ical Assessment, 7, 524–532.
Svedlund, J., Sjodin, I., & Dotevall, G. (1988). GSRS—A clinical
rating scale for gastrointestinal symptoms in patients with
irritable bowel syndrome and peptic ulcer disease. Digestive
Diseases and Sciences, 33(2), 129–134.
Sykes, M. A., Blanchard, E. B., Lackner, J. M., Keefer, L., & Krasner,
S. (2003). Psychopathology in irritable bowel syndrome: Support
for a psychosomatic model. Journal of Behavioral Medicine, 26,
361–372.
Tkachuk, C. A., Graff, L. A., Martin, G. L., & Bernstein, C. N.
(2003). Randomized controlled trial of cognitive–behavioral
group therapy for irritable bowel syndrome in a medical setting.
Journal of Clinical Psychology in Medical Settings, 10, 57–69.
Toner, B. B., Stuckless, N., Ali, A., Downie, F., Emmott, S., & Akman,
D. (1998). The development of a cognitive scale for functional
bowel disorders. Psychosomatic Medicine, 60, 492–497.
Walker, E. A., Roy-Byrne, P. P., Katon, W. J., Li, L., Amos, D., &
Jiranek, G. (1990). Psychiatric illness and irritable bowel
syndrome: A comparison with inflammatory bowel disease.
American Journal of Psychiatry, 147(12), 1656–1661.
Weissman, A., & Beck, A. T. (November, 1978). Development and
validation of the Dysfunctional Attitude Scale: A preliminary
investigation. Presented at the annual meeting of the American
Educational Research Association, Toronto, Ontario, Canada.
Whitehead, W. E., Palsson, O. S., Thiwan, S., Talley, N. J., Chey, W.
D., Irvine, J., et al. (2006). Development and validation of the
Rome III diagnostic questionnaire. In D. A. Drossman, E.
Corazziari, R. C. Spiller, & W. G. Thompson (Eds.), Rome III:
The functional gastrointestinal disorders (3rd ed., pp. 835–853).
McLean, VA: Degnon Associates.
Wiklund, I. K., Fullerton, S., Hawkey, C. J., Jones, R. H., Longstreth,
G. F., Mayer, E. A., et al. (2003). An irritable bowel syndrome-
specific symptom questionnaire: Development and validation.
Scandinavian Journal of Gastroenterology, 38(9), 947–954.
Cogn Ther Res
123