development and validation of a diabetes knowledge questionnaire
TRANSCRIPT
ORIGINAL ARTICLE
166 Pract Diab Int May 2011 Vol. 28 No. 4 Copyright © 2011 John Wiley & Sons
IntroductionImproving methods and strategiesfor evaluating diabetes patient education interventions has beenincreasingly advocated by bothprovider and consumer organisa-tions globally.1–3
Evaluation efforts have tradition-ally been hampered by lack of formalagreement about goals and systemati-cally derived benchmarks4–9 and lack of standardised and validatedevaluation measures.10–12 To addressthis problem, Diabetes Australiadeveloped an Australian NationalConsensus Position on Outcomesand Indicators for Diabetes PatientEducation (O&I).13,14 The O&I con-sensus identified four patient-centredkey outcome areas of knowledge andunderstanding, self-management,self-determination and psychologicaladjustment expressed in the order inwhich each area is most influenced bydiabetes education.
A subsequent study identifiedand evaluated available tools on theirability and suitability for measuringchanges in the four key outcomes.15
While three knowledge assessmenttools were identified, none met all ofthe systematically derived qualityappraisal criteria. The first of thethree tools, the diabetes knowledgetest (DKT), was developed and vali-dated in the mid-1980s by theMichigan Diabetes Research andTraining Centre to address the needfor a valid and reliable diabetes specific knowledge instrument thatcould be used by diabetes educatorsand researchers.16,17 Later scaleshave been adapted from the DKT to suit particular groups and
interventions.18–20 As some questionsdo not reflect current Australianguidelines (e.g. a free food is not defined as having less than 20 calories per serving), and uses terminology not used in theAustralian context (e.g. an insulinreaction), the DKT is not suitable foruse in Australia.
In 1984, a series of three diabetesknowledge assessment scales(DKNA, DKNB and DKNC, each of15 items) were developed and vali-dated for the Australian environ-ment.21 None of the DKN scales hassince been updated and they no
longer reflect current guidelinesand standards of care (e.g. they referto urine sugar testing which is nolonger recommended) and, like theDKT, they contain many questionsregarding insulin therapy which didnot fit our criteria for a generic toolthat is applicable to all people withtype 1 or 2 diabetes. The third iden-tified validated knowledge question-naire, the ADKnowl, was developedand tested in the UK.22 It consists of23-item sets with a total of 104 ques-tions/items which makes it a morecomprehensive, thus a more oner-ous and resource intensive tool for
Development and validation of a diabetesknowledge questionnaireCA Eigenmann*, T Skinner, R Colagiuri
ABSTRACTAn Australian National Consensus Position on Outcomes and Indicators for DiabetesEducation identified knowledge and understanding as the outcomes most directlyaffected by diabetes education. A subsequent literature review failed to identify avalidated, suitable questionnaire for measuring knowledge. Consequently, we aimed todevelop a minimum diabetes knowledge questionnaire (DKQ) suitable for people withboth type 1 and type 2 diabetes.
Content validity was established through literature review, Delphi survey of 52opinion leaders and a workshop of Australian Diabetes Educators (n ≥300). The resultinginstrument was tested for internal consistency on 129 and for reliability on 57 people withtype 1 and type 2 diabetes, respectively.
The final questionnaire contains: 12 multiple choice questions common to type 1 andtype 2 diabetes, e.g. normal blood glucose levels, complications, diet, exercise, self-monitoring of blood glucose, annual check-ups, support services, and sick-days; twoquestions for people on oral medication/insulin only; and one question (sick-days) forpeople with type 1 diabetes only.
For the first 12 questions, the internal consistency was good (Cronbach’s α=0.73);with the additional item for type 1 diabetes, the internal consistency was slightly better(α=0.79) as it was with the additional items for people on medication/insulin (α=0.76). Noparticular item seemed to adversely affect the overall consistency of the questionnaire.
Comparing test-retest pilots, total scores showed good reliability with no evidence ofchange over time (t=1.73; df=56; p<0.85), and a correlation of 0.62.
The DKQ is now ready to use for evaluating knowledge outcomes of diabeteseducation. Copyright © 2011 John Wiley & Sons.
Practical Diabetes Int 2011; 28(4): 166–170
KEY WORDSoutcome; measure; knowledge; questionnaire; diabetes education
Cecile A Eigenmann, RN, CDE, MPH,Australian Diabetes Council, Sydney, NewSouth Wales, AustraliaTimothy Skinner, BSc Hons, PhD, FlindersUniversity Rural Clinical School, MtGambier, South Australia, AustraliaRuth Colagiuri, RN, BEd, Grad Cert Health
Policy & Management, Sydney University –Health and Sustainability Unit – MenziesCentre for Health Policy, Sydney, NewSouth Wales, Australia
*Correspondence to: Cecile AEigenmann, Australian Diabetes Council,
26 Arundel St, Sydney, New South Wales2037, Australia; email:[email protected]
Received: 9 February 2011Accepted in revised form: 21 March 2011
OA Eigenmann_Layout 1 5/3/11 12:53 PM Page 1

application in a clinical setting, andhence did not meet our criteria for abrief tool.
Given the lack of an up-to-date,validated instrument, we aimed todevelop, pilot and validate a generic,brief DKQ capable of measuringknowledge change following a dia-betes education intervention andwhich would be suitable for peoplewith both type 1 and 2 diabetes.
MethodsEthical approval for the study wasobtained from the University ofSydney’s Human Ethics ResearchCommittee. Although the definitionof knowledge is a matter of on-goingdebate, for the purpose of this project the following definition wasadopted: ‘knowledge is the confi-dent understanding of a subject,potentially with the ability to use itfor a specific purpose’.
Design of the questionnaireDelphi survey. A purposive sampleof 52 nationally recognised diabeteseducators, dietitians, endocrin -ologists, podiatrists, psychologists,primary care physicians, andresearchers were invited to partici-pate in an email Delphi survey. TheDelphi method is widely used in thedevelopment of research scales andquestionnaires as a systematic, inter-active method where a panel ofexperts answers questionnaires intwo or more rounds.23 In the firstround, participants were asked toindicate, on a standard question-naire, their opinion on the mostimportant topics to be included inthe questionnaire. The secondround consisted of 20 questions withfive multiple choice options, devel-oped by the researcher (CAE) basedon the domains that were answeredas ‘very important’ by ≥60% of first-round survey respondents. Allquestions were based on currentAustralian clinical and/or educa-tional guidelines for the care of people with type 1 and 2 diabetes.Additional domains identified wereonly included if they were listed by≥15% of respondents. Commentswere incorporated into the second-round questionnaires.
Participants were asked to indi-cate their opinion of each question
as to whether it should be includedin the final questionnaire (fromstrongly agree to strongly disagree),whether the question should beincluded if the phrasing was modi-fied (from strongly agree to stronglydisagree) and, if they had to choosebetween two questions referring to the same domain, which one they would prefer to see included inthe questionnaire.
Diabetes educators’ consultationworkshop. To further test contentand face validity, the 20-item draftquestionnaire was presented at aconsultation workshop comprisingmembers of the Australian DiabetesEducators Association (ADEA) dur-ing a national diabetes conferencein 2007.24 Participants were asked todiscuss the questionnaire in smallgroups, and indicate on a standardsurvey, for each of the 20 questions,whether the questions should beincluded in the final questionnaire(yes or no response), and any com-ments they had with regard to thephrasing of the questions.
Responses from Delphi surveys andthe ADEA workshop were coded,analysed and collated into a pilotquestionnaire.
The readability of the question-naire was assessed by using theFlesch Reading Ease score.25 Thetest is based on the average numberof syllables per word and words per sentence with scores rangingfrom 0–100. The higher the score the easier a document is tocomprehend, with 60–70 consid-ered an acceptable score for lite rate adults.
Testing the questionnaireFor all pilot tests, a detailed studyinformation sheet was provided toprospective participants and writtenconsent was obtained.
People with type 1 and 2 diabeteswere recruited from: (a) three dia-betes centres attached to large metropolitan teaching hospitals inSydney; (b) attendees of group education programmes held atDiabetes Australia – New SouthWales (DANSW [since July 2010trading as Australian DiabetesCouncil]), a charitable, not for
profit organisation located in theSydney central business district; and(c) from one private diabetes educa-tor setting. Health professionals(primarily diabetes educators) wereasked to distribute the pilot ques-tionnaires to consecutive attendeesat regular clinic visits or educationprogrammes.
Reliability testing (test-retest)was carried out by random selectionof 300 people with type 1 or 2 dia-betes from the DANSW member-ship database. Letters of invitationwere mailed out and consentingrespondents were sent identicalquestionnaires on two differentoccasions with a two-week interval.Instructions accompanied the initialquestionnaire requesting partici-pants not to take part in diabeteseducation nor consult books, websites or colleagues, within thetwo-week interval.
Statistical analysisQuestionnaires were scored, witheach correct answer worth 1 point,each ‘unsure’ answer worth 0.5 andan incorrect answer received nopoints. This scoring system allowsfor all responses to be added in thetotal and is based on the premisethat it is preferable for the partici-pant to recognise that they are‘unsure’ of the answer, than forthem to ‘think’ they know the correct answer when in fact they are incorrect.
To determine internal consis-tency, item-to-total correlations andCronbach’s coefficient alpha (α)were used. For these reasons, it issuggested that Cronbach’s α shouldbe above 0.70 but not higher than0.90.26 Pearson’s r correlation co -efficient was used to examine therelationship between the totalknowledge score (calculated by summing the scores of all items) andage, type and duration of diabetes.Descriptive statistics were used todescribe the sample.
Stability (test-retest reliability)was assessed using Pearson’s product-moment correlation coefficient and paired t-tests to examine consis-tency and stability of responses.Commonly cited minimal standardsfor reliability coefficients are 0.70 forgroup data.26
ORIGINAL ARTICLE
Development and validation of a diabetes knowledge questionnaire
Pract Diab Int May 2011 Vol. 28 No. 4 Copyright © 2011 John Wiley & Sons 167
OA Eigenmann_Layout 1 5/3/11 12:53 PM Page 2

All responses were collated,coded and analysed by using theStatistical Package for the SocialSciences (SPSS 13.0, SPSS Inc,Chicago, IL, USA).
ResultsContent validityTwo rounds of the Delphi surveywere conducted for the develop-ment of questionnaire items. Theresponse rate for the first round was71% (37/52) and 62% for roundtwo (23/37).
In round one, 14 of 20 domainswere identified as ‘very important’by ≥60% of respondents (see Table1). A large number of key opinionleaders commented that only peopletreated on diabetes medicationand/or insulin needed to knowabout hypoglycaemia and medica-tion. Similarly, respondents indi-cated that sick-day managementshould include a separate questionfor people with type 1 diabetes to
emphasise the need for ketone test-ing as a self-care requirementunique to type 1 diabetes.
Two additional topics (i.e. familyadjustment/support and mentalhealth), indicated as very importantby ≥15% of respondents, were alsoincorporated into the round-twoquestionnaire.
Twenty questions with five multi-ple choice options, eliciting either‘one false answer’ or ‘one correctanswer’ response, were developed bythe researcher based on the 16agreed topics in round one.
Synthesis and analysis followinground-two surveys resulted in thedeletion of the items measuringmental health and family support asthese were difficult to phrase andreceived negative feedback from themajority of respondents.
A number of questions wererephrased to incorporate respon-dents’ constructive suggestions forsimplifying the language and short-ening the questions.
The ADEA workshop wasattended by over 300 people. A totalof 64 questionnaires were returned,each resulting from a group discus-sion of between three and seven participants. Results of summarisedconsensual comments are illustratedin Table 2.
The final questionnaire, incorpo-rating responses from the Delphisurvey and the ADEA workshop,contains 15 questions: nine ques-tions eliciting a ‘one answer’response to five multiple choiceoptions, and six questions elicitingan ‘as many as apply’ to six multiplechoice options. An ‘unsure’ optionwas included for each question.
Table 3 lists the question topics:12 topics common to people withtype 1 and 2 diabetes, two questionsfor people taking diabetes medica-tion/insulin, and one question forthose with type 1 only.
Seven demographic questionswere added including: age, gender,duration and type of diabetes, typeof medication (if any) and previousvisit to a diabetes educator and/or dietitian.
Flesch test readability score forthe total questionnaire was 66.5.
Pilot testingIn all, 129 people completed thepilot test of whom 47% were maleand 39% had type 1 diabetes; 10%had never seen a diabetes educatorand 13% had never seen a dietitian.
Internal consistency. Analysis of the129 pilots showed good internal con-sistency with a Cronbach’s α of 0.73
ORIGINAL ARTICLE
Development and validation of a diabetes knowledge questionnaire
168 Pract Diab Int May 2011 Vol. 28 No. 4 Copyright © 2011 John Wiley & Sons
Table 1. Results from the first roundof Delphi – domains to be includedin the knowledge questionnaire
Table 2. Consensual comments expressed by ADEA workshop participants
• Don’t use ‘false’ options; keep questions positive• Simplify language to accommodate for people with low literacy level• A question is needed with regard to carbohydrate food • Separate questionnaire or section for type 1 and type 2 diabetes in
particular with regard to sick-day management (including ketone testing), hypoglycaemia treatment and medications (i.e. insulin)
Table 3. Pilot diabetes knowledge questionnaire: question topics
Domains identified as ‘veryimportant’ by ≥60% of Delphirespondents1. Normal range of blood glucose
level2. Duration/chronic nature3. Consequences short- and
long-term4. Nutrition5. Physical activity6. Foot care7. Medication taking8. Sick-day management9. Self-monitoring of blood glucose10. Appropriate attendance for
medical care11. Support services
For people on insulin therapyand/or insulin stimulating tablets 12. Hypoglycaemia13. Medication14. Sick-day management
Additional domains identified as‘very important’ by ≥15% ofDelphi respondents15. Family adjustment/support 16. Effects on and management of
mental health
12 questions common to peoplewith type 1 and 2 diabetes:1. Ideal blood glucose levels2. HbA1c
3. Chronic nature (no cure)4. Dietary guidelines 5. Benefits of physical activity6. Frequency of physical activity 7. General diabetes long-term
complications8. Diabetes foot complications9. Self-monitoring of blood glucose 10. Sick-day management11. Annual check-ups
12. Support services – National Diabetes Services Scheme (NDSS – a government subsidised support scheme)
Two questions to be completed bypeople on oral medication and/orinsulin only:13. Diabetes medication 14. Hypoglycaemia
One question to be completed bypeople with type 1 diabetes only:15. Sick-day management
OA Eigenmann_Layout 1 5/3/11 12:53 PM Page 3

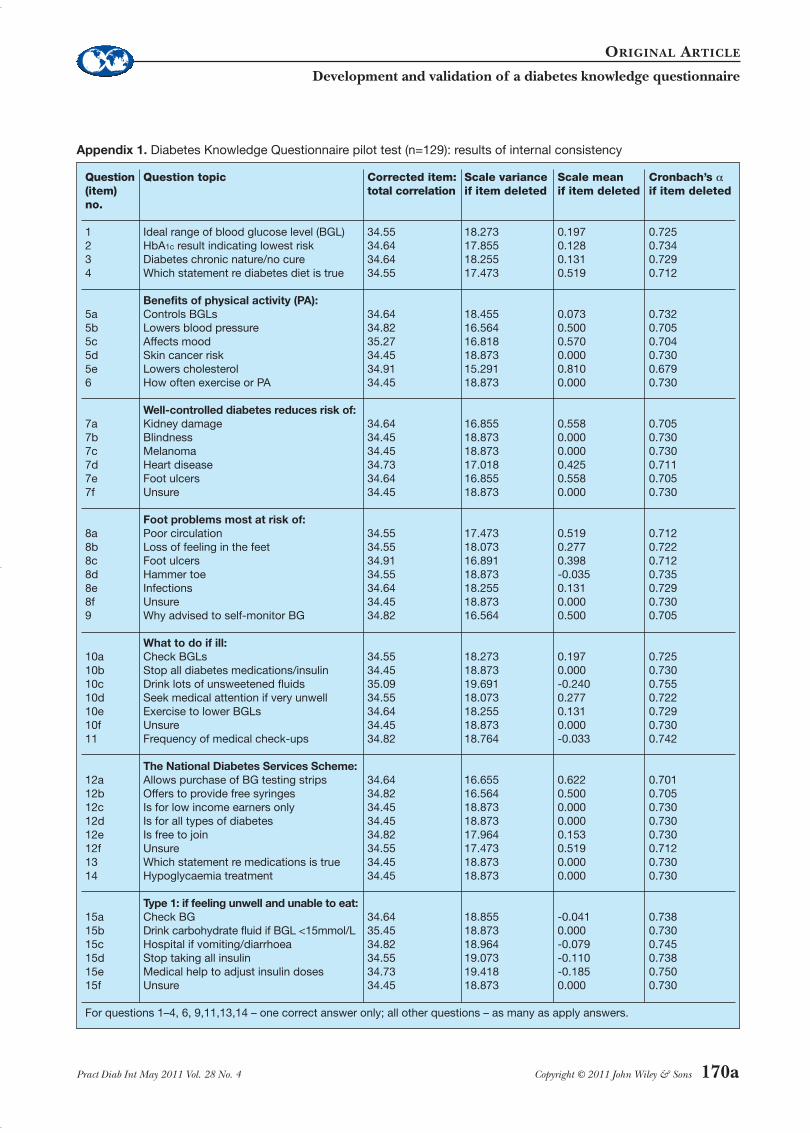
for the first 12 questions, commonto all individuals. Appendix 1 (avail-able online at www.practicaldiabetesinternational.com) lists for eachquestion the scale’s mean and variance if the item is deleted. Withthe additional question for type 1diabetes regarding sick-day manage-ment, the internal consistency wasslightly better (α=0.79). Similarly,Cronbach’s α was slightly better at0.76 with the two additional ques-tions regarding medication andhypoglycaemia.
No question seemed to particu-larly adversely affect the overall consistency of the questionnaire.Although seven items wouldimprove the consistency in respond-ing if removed, none would increasethe alpha by more than 0.01, and sodo not warrant removing.
Test-retest reliability. Comparing thefirst and second rounds of the 57completed pilots, total scoresshowed good reliability with no evi-dence of change over time (t=1.73;df=56; p<0.85), with a test-retest correlation of 0.62.
Construct validity. In support of thetool’s construct validity, there was nosignificant difference between malesand females (t=1.07; df=97; p>0.28)and no significant association withage (r=0.04) or duration of diabetes(r=0.12). However, as would beexpected, individuals with type 1 dia-betes scored slightly higher (mean29 [SD 3.7]) than individuals withtype 2 diabetes (mean 26 [SD 5.0];t=2.48; df=94; p<0.01).
DiscussionThe purpose of this study was todevelop a valid and reliable question-naire capable of assessing the effectof a diabetes education interventionon knowledge of diabetes and its self-management requirements in people with type 1 and 2 diabetes.
Although it is well acknowledgedthat knowledge acquisition does notreadily translate into behaviourchange, a myriad of studies discussthe need for assessing knowledge asan important measure of effective-ness of diabetes educational inter-ventions and as a prerequisite for informed health decision
making.27–31 Others advocate thatacquiring adequate knowledge ofthis chronic illness is the corner-stone for enabling people towardsdiabetes self-management andhence prevention of ill health.20 TheO&I Consensus Position13,14 identi-fied knowledge as the outcomemostly affected by diabetes educa-tion. Nonetheless, a further threekey outcomes, i.e. self-managementbehaviours, self-determination andpsychological adjustment, were iden-tified and recommended to formpart of the outcome assessments ofdiabetes education interventions –albeit with appropriate validatedinstruments.15
The DKQ is unique in the way inwhich it includes separate questionsfor people not taking diabetes med-ication (12 items), people takingdiabetes medication and/or insulin(two items) and an additional itemfor people with type 1 diabetes only(total 15 items), therefore making ita more widely applicable tool.
The DKQ is a brief, 15-itemknowledge questionnaire with sevenadditional demographic questionsadded if required, taking between5–15 minutes to complete – hencemaking it feasible to apply in a busyclinical setting.
The readability, using the ‘FleschReading Ease’ test, was considered
highly acceptable, hence making thetool applicable to people with a lowliteracy level.
The importance of consumerinput has been increasingly advo-cated by consumer and health careprovider organisations. Althoughthe Delphi survey did not specifi-cally obtain input from people withdiabetes, the draft questionnairewas pilot tested on a small sample ofpeople with diabetes, and their feed-back was sought and incorporatedbefore the large scale pilot test wasconducted. Further, a number ofDelphi and ADEA workshop partici-pants who responded in their professional capacity also have dia-betes themselves.
Valid outcome data can only beachieved if education providersassure adequate item to content cov-erage, i.e. all questions in the DKQneed to be covered during an educa-tion intervention.
Further testing for the scale’sresponsiveness/sensitivity to changethrough an education session is now needed. This is currentlyunderway at the Australian DiabetesCouncil where the DKQ is applied to assess the effect of anongoing diabetes group educationprogramme on type 2 diabetespatients’ knowledge before andafter the programme.
ORIGINAL ARTICLE
Development and validation of a diabetes knowledge questionnaire
Pract Diab Int May 2011 Vol. 28 No. 4 Copyright © 2011 John Wiley & Sons 169
Key points
• An Australian National Consensus Position on Outcomes and Indicators for Diabetes Patient Education identified knowledge and understanding as the key outcomes most directly influenced by diabetes education
• A subsequent literature review failed to identify a validated, suitable questionnaire for measuring diabetes knowledge
• We developed, piloted and validated a generic, brief diabetes knowledge questionnaire for application before and after education interventions and suitable for people with both type 1 and type 2 diabetes
• Methods to establish content validity included a literature review, a Delphi survey of national key opinion leaders and a workshop of Australian Diabetes Educator Association members
• The resulting 15-item diabetes knowledge questionnaire (DKQ), with an additional seven demographic questions, was pilot tested for internal consistency and for stability (test-retest) on 129 and 57 people with type 1 and type 2 diabetes, respectively
• Results showed good reliability and internal consistency and a highly acceptable ‘Flesch Reading Ease’ score, hence making the tool applicable to people with a low literacy level
• The DKQ can now be applied by health professionals as part of quality assurance and improvement for assessing their own diabetes education practice and as a research tool
OA Eigenmann_Layout 1 5/3/11 12:53 PM Page 4

LimitationsAlthough we do not claim that theDKQ will be applicable globally, it isimportant to note that the question-naire is based on international3
and Australian evidence-basedguidelines which have been derived from the international peerreviewed literature.6
In the face of ongoing changes indiabetes standards/guidelines ofcare and technologies, the DKQ willneed regular revision to assure con-tent accuracy and re-validation ifchanges are made.
ConclusionThe Diabetes Knowledge Question -naire has undergone rigorous valida-tion and has shown good reliabilityand internal consistency; it can nowbe applied by health professionals as part of quality assurance andimprovement for assessing their owndiabetes education practice and as aresearch tool.
Appendices 2 and 3 (available online atwww.practicaldiabetesinternational.com)show the text of the final DiabetesKnowledge Questionnaire and scoringinstructions, respectively.
A formatted version of the full ques-tionnaire is also available from http://www.australiandiabetescouncil.com/Resources/PDFs/Diabetes-Knowledge-Questionniare-DKQ-2009.pdf.
AcknowledgementsWe would like to thank the peoplewith diabetes who participated in thepilot testing, the members of theDelphi expert panel and the diabeteseducators who participated in theworkshop for their valuable input. Weare also very grateful for the assis-tance of diabetes educators from dia-betes centres and health professionalsat the Australian Diabetes Councilwho assisted with the pilot testing.
Declaration of interestsThis project was partially funded by a 2006 Australian DiabetesSociety–Servier National ActionPlan Grant.
References1. Corabian P, Harstall C. Patient dia-
betes education in the management ofadult type 2 diabetes. Alberta: Alberta
Heritage Foundation for MedicalResearch, 2001: IHTA 23 Series A.
2. Peeples M, et al. The ConceptualFramework of the National DiabetesEducation Outcomes System(NDEOS). Diabetes Educ 2001;27(4):547–62.
3. International Diabetes Federation.International Standards for DiabetesEducation, 3rd edn. Brussels: IDF, 2009.
4. Majumdar SR, et al. A CanadianConsensus for the StandardizedEvaluation of Quality ImprovementInterventions in Type 2 Diabetes.Can J Diabetes 2005;29(3):220–9.
5. Sigurdardottir AK, et al. Outcomes ofeducational interventions in type 2diabetes: WEKA data-mining analysis.Patient Educ Couns 2007;67(1–2):21–31.
6. Colagiuri R, et al. National EvidenceBased Guidelines for PatientEducation in Type 2 diabetes.Diabetes Australia and the NHMRC,Canberra 2009. Available from www.nhmrc.gov.au/_files_nhmrc/file/p u b l i c a t i o n s / s y n o p s e s / d i 1 6 -diabetes-patient-education.pdf [lastaccessed 12 Jan 2011].
7. Glasgow RE, Osteen VL. Evaluatingdiabetes education. Are we measur-ing the most important outcomes?Diabetes Care 1992;15(10):1423–32.
8. Home P, et al. Health OutcomeIndicators: Diabetes. Report of aworking group to the Department ofHealth. National Centre for HealthOutcomes, Oxford, 1999.
9. Naqib J. Patient education for effec-tive diabetes self-management:report, recommendations and exam-ples of good practice. London:Diabetes UK, 2002.
10.Scientific Advisory Committee of theMedical Outcomes Trust. Assessinghealth status and quality-of-life instru-ments: attributes and review criteria.Qual Life Res 2002;11:193–205.
11.Ellis SE, et al. Diabetes patient educa-tion: a meta-analysis and meta-regres-sion. Patient Educ Couns 2004;52(1):97–105.
12.Mokkink LB, et al. Protocol of theCOSMIN study: COnsensus-basedStandards for the selection of healthMeasurement INstruments. BMCMed Res Methodol 2006;6:2.
13.Eigenmann C, Colagiuri R. Outcomesand Indicators for Diabetes Education: ANational Consensus Position. Canberra:Diabetes Australia, 2007.
14.Colagiuri R, Eigenmann C. Anational consensus on outcomes andindicators for diabetes patient educa-tion. Diabet Med 2009;26:442–6.
15.Eigenmann C, et al. Are current psy-chometric tools suitable for measur-
ing outcomes of diabetes education?Diabet Med 2009;26:425–36.
16.Hess GE, Davis WK. The validation ofa diabetes patient knowledge test.Diabetes Care 1983;6(6):591–6.
17.Fitzgerald JT, et al. The reliability andvalidity of a brief diabetes knowledgetest. Diabetes Care 1998;21(5):706–10.
18. van den Arend IJM, et al. Educationintegrated into general practice carefor type 2 diabetic patients results insustained improvement of diseaseknowledge and self-care. Diabet Med2000;17:190–7.
19.Garcia AA, et al. The Starr CountyDiabetes Education Study – develop-ment of the Spanish-language dia-betes knowledge questionnaire.Diabetes Care 2001;24(1):16–21.
20.Persell SD, et al. Relationship of dia-betes-specific knowledge to self-man-agement activities, ambulatory pre-ventative care, and metabolic out-comes. Prev Med 2004;39:746–52.
21.Dunn SM, et al. Development of thediabetes knowledge (DKN) scales:forms DKNA, DKNB, and DKNC.Diabetes Care 1984;7(1):36–41.
22.Speight J, Bradley C. ADknowl: iden-tifying knowledge deficits in diabetescare. Diabet Med 2001;18:626–39.
23.Duffield C. The Delphi technique.Aust J Adv Nurs 1988;6:41–5.
24.Eigenmann C, et al. Measuring out-comes of diabetes education (MODE).A Consultation Work shop towards aNational Consensus. AustralianDiabetes Society/Australian DiabetesEducators Association AnnualScientific Meeting, Christchurch, NewZealand, Sept 2007.
25.Flesch RF. A new readability yard-stick. J Appl Psychol 1948;32:221–33.
26.Fitzpatrick R, et al. Evaluating patient-based outcome measures for use inclinical trials. Health Technol Assess1998;2(14):i–iv, 1–74.
27.Tomky D, et al. Diabetes educationoutcomes: what educators are doing.Diabetes Educ 2000;26(6):951–4.
28.Koopman DJEM, van der Bijl JJ. Theuse of self-efficacy enhancing meth-ods in diabetes education in theNetherlands. Sch Inq Nurs Pract 2001;15(3):249–57.
29.Mulcahy K, et al. Diabetes self-manage-ment education core outcomes meas-ures. Diabetes Educ 2003;29(5):768–70.
30.Mensing C, et al. National standardsfor diabetes self-management educa-tion. Diabetes Care 2003;26(Suppl1):S149–56.
31.Heisler M, et al. The relationshipbetween knowledge of recent HbA1c
values and diabetes care understand-ing and self-management. DiabetesCare 2005;28(4):816–22.
ORIGINAL ARTICLE
Development and validation of a diabetes knowledge questionnaire
170 Pract Diab Int May 2011 Vol. 28 No. 4 Copyright © 2011 John Wiley & Sons
OA Eigenmann_Layout 1 5/3/11 12:53 PM Page 5
ORIGINAL ARTICLE
Development and validation of a diabetes knowledge questionnaire
Pract Diab Int May 2011 Vol. 28 No. 4 Copyright © 2011 John Wiley & Sons 170a
Appendix 1. Diabetes Knowledge Questionnaire pilot test (n=129): results of internal consistency
Question Question topic Corrected item: Scale variance Scale mean Cronbach’s α(item) total correlation if item deleted if item deleted if item deleted
no.
1 Ideal range of blood glucose level (BGL) 34.55 18.273 0.197 0.7252 HbA1c result indicating lowest risk 34.64 17.855 0.128 0.7343 Diabetes chronic nature/no cure 34.64 18.255 0.131 0.7294 Which statement re diabetes diet is true 34.55 17.473 0.519 0.712
Benefits of physical activity (PA):5a Controls BGLs 34.64 18.455 0.073 0.7325b Lowers blood pressure 34.82 16.564 0.500 0.7055c Affects mood 35.27 16.818 0.570 0.7045d Skin cancer risk 34.45 18.873 0.000 0.7305e Lowers cholesterol 34.91 15.291 0.810 0.6796 How often exercise or PA 34.45 18.873 0.000 0.730
Well-controlled diabetes reduces risk of:7a Kidney damage 34.64 16.855 0.558 0.7057b Blindness 34.45 18.873 0.000 0.7307c Melanoma 34.45 18.873 0.000 0.7307d Heart disease 34.73 17.018 0.425 0.7117e Foot ulcers 34.64 16.855 0.558 0.7057f Unsure 34.45 18.873 0.000 0.730
Foot problems most at risk of:8a Poor circulation 34.55 17.473 0.519 0.7128b Loss of feeling in the feet 34.55 18.073 0.277 0.7228c Foot ulcers 34.91 16.891 0.398 0.7128d Hammer toe 34.55 18.873 -0.035 0.7358e Infections 34.64 18.255 0.131 0.7298f Unsure 34.45 18.873 0.000 0.7309 Why advised to self-monitor BG 34.82 16.564 0.500 0.705
What to do if ill:10a Check BGLs 34.55 18.273 0.197 0.72510b Stop all diabetes medications/insulin 34.45 18.873 0.000 0.73010c Drink lots of unsweetened fluids 35.09 19.691 -0.240 0.75510d Seek medical attention if very unwell 34.55 18.073 0.277 0.72210e Exercise to lower BGLs 34.64 18.255 0.131 0.72910f Unsure 34.45 18.873 0.000 0.73011 Frequency of medical check-ups 34.82 18.764 -0.033 0.742
The National Diabetes Services Scheme:12a Allows purchase of BG testing strips 34.64 16.655 0.622 0.70112b Offers to provide free syringes 34.82 16.564 0.500 0.70512c Is for low income earners only 34.45 18.873 0.000 0.73012d Is for all types of diabetes 34.45 18.873 0.000 0.73012e Is free to join 34.82 17.964 0.153 0.73012f Unsure 34.55 17.473 0.519 0.71213 Which statement re medications is true 34.45 18.873 0.000 0.73014 Hypoglycaemia treatment 34.45 18.873 0.000 0.730
Type 1: if feeling unwell and unable to eat:15a Check BG 34.64 18.855 -0.041 0.73815b Drink carbohydrate fluid if BGL <15mmol/L 35.45 18.873 0.000 0.73015c Hospital if vomiting/diarrhoea 34.82 18.964 -0.079 0.74515d Stop taking all insulin 34.55 19.073 -0.110 0.73815e Medical help to adjust insulin doses 34.73 19.418 -0.185 0.75015f Unsure 34.45 18.873 0.000 0.730
For questions 1–4, 6, 9,11,13,14 – one correct answer only; all other questions – as many as apply answers.
OA Eigenmann_Layout 1 5/3/11 12:53 PM Page 6

ORIGINAL ARTICLE
Development and validation of a diabetes knowledge questionnaire
170b Pract Diab Int May 2011 Vol. 28 No. 4 Copyright © 2011 John Wiley & Sons
Appendix 2. Text of the Diabetes Knowledge Questionnaire
1. What is the ideal range for blood glucose (sugar) levels a person with diabetes should aim for?Please circle ONE answer only a. 2 to 6mmol/Lb. 7 to 13mmol/Lc. 4 to 8mmol/Ld. 4.5 to 15mmol/Le. Unsure
2. A blood test called HbA1c (or A1c) measures the average blood glucose levels over the past 2 to 3 months. What is the HbA1c result that indicates a lowest risk of developing long-term diabetes complications?Please circle ONE answer only a. Less than or equal to 7%b. Less than 8%c. 9%d. Less than or equal to 10%e. Unsure
3. Diabetes is a condition that: Please circle ONE answer only a. Can be cured by adopting a healthy lifestyleb. Can be cured with tablets and/or insulinc. Is currently not curabled. Is always life threatening when first diagnosede. Unsure
4. Which of the following statements about diabetes and diet is true?Please circle ONE answer only a. People with diabetes should eat a sugar free dietb. It is OK to eat fried take away food three times a
week c. Red meat is a carbohydrate food d. A diet which is low in fat, high in fibre, low in added
sugar is recommended for everyone with diabetese. Unsure
5. Why is doing regular exercise or being physically active good for your health? Please circle AS MANY as apply, or circle ‘Unsure’a. It can help to control blood glucose levelsb. It can lower blood pressure
c. It can help to regulate a person’s moodd. It can reduce the risk of skin cancere. It can lower cholesterol levels f. Unsure
6. How often should people with diabetes exercise or be physically active?Please circle ONE answer onlya. Most days of the week for at least 30 minutes b. Once a week for at least 30 minutes c. Once a month for one hourd. At least every fortnight for two hourse. Unsure
7. Well-managed diabetes decreases the risk of:Please circle AS MANY as apply, or circle ‘Unsure’a. Kidney damageb. Blindnessc. Melanomad. Heart diseasee. Foot ulcersf. Unsure
8. What foot problems are people with diabetes most
at risk of?Please circle AS MANY as apply, or circle ‘Unsure’a. Poor circulationb. Loss of feeling in the feet c. Foot ulcersd. Hammer toee. Infectionsf. Unsure
9. Why are people with diabetes advised to test their own blood glucose (BG)?Please circle ONE option onlya. To alert them to changes in BG level patternsb. To help make decisions in relation to exercise,
treating ‘hypos’ (low BG) or sick-day managementc. It can make people more confident in looking after
their diabetes d. All of the abovee. Unsure
(continued on next page)
DIABETES KNOWLEDGE QUESTIONNAIRE
TEST YOUR KNOWLEDGE AND UNDERSTANDING OF DIABETES AND ITS MANAGEMENT
YOUR NAME: ..........................................
Dear participantPlease read the instruction for each question carefully as the required responses change from
‘circle ONE answer only’ to ‘circle AS MANY as apply’.Please assist us by answering ALL questions on EVERY page.
OA Eigenmann_Layout 1 5/3/11 12:53 PM Page 7

ORIGINAL ARTICLE
Development and validation of a diabetes knowledge questionnaire
Pract Diab Int May 2011 Vol. 28 No. 4 Copyright © 2011 John Wiley & Sons 170c
Appendix 2. Text of the Diabetes Knowledge Questionnaire (continued from previous page)
10. What should a person with diabetes do if s/he becomes ill (e.g. flu, gastric upset, infection)?Please circle AS MANY as apply, or circle ‘Unsure’a. Check blood glucose level more frequently (every
2 to 4 hours)b. Stop taking all diabetes tablets and/or insulinc. Drink lots of non-sweet fluid if blood glucose levels
are over 15mmol/Ld. Seek medical attention if very unwell and unable to
check blood glucose e. Try to do as much exercise as possible to lower
blood glucose levelsf. Unsure
11. People with diabetes need a medical check-up of their eyes, nerve and kidney function at least:Please circle ONE answer only a. Every monthb. Six monthlyc. Once a year d. Every two to three yearse. Unsure
12. The National Diabetes Services Scheme (NDSS): Please circle AS MANY as apply, or circle ‘Unsure’a. Allows members to purchase blood glucose testing
strips at reduced priceb. Offers members free syringes and insulin pen needlesc. Is only available to people on low incomesd. Is available to people with all types of diabetese. Is free to joinf. Unsure
The following questions (13 and 14) are to becompleted by people taking diabetes medication(i.e. blood glucose lowering tablets or insulin)If you are not taking any diabetes medication pleasego to question No 16
13. Which of the following statements about diabetes medication is true? Please circle ONE answer only a. If blood glucose levels are normal for two months,
diabetes medication can be stopped b. Tablets for diabetes work by increasing blood
glucose levelsc. Regular medical check-ups are necessary to assess
the need for adjustments to diabetes medicationd. People taking diabetes medication do not need to
worry about healthy eatinge. Unsure
14. If a person with diabetes has a hypo (low blood glucose level) reaction, s/he should:Please circle ONE answer onlya. Immediately take some insulin or diabetes tabletsb. Rest and wait until s/he feels better
c. Immediately have some sugary food or drink (e.g. jelly beans, soft drink)
d. Drink some diet soft drink e. Unsure
The next question (No 15) is to be completed bypeople with or carers of people with type 1diabetes only
15. A person with type 1 diabetes feeling unwell and
unable to eat should:Please circle AS MANY as apply, or circle ‘Unsure’a. Check blood glucose and ketone levels at least
every 2 hoursb. Drink carbohydrate containing (sugary) fluids if
blood glucose below 15mmol/Lc. Go to the hospital if persistent vomiting and/or
diarrhoead. Stop taking all insulin e. Seek medical advice for adjusting insulin dosesf. Unsure
16. Finally, we would like to ask you some questions about yourself. This questionnaire is strictly confidential. Please assist us by answering all questions.
Thank you very much for completing this questionnaire!
What is your age? ………… years
What is your gender? Female n Male n
How long have you had diabetes?….…. years or …..… months or …….. days
What type of diabetes do you have?Type 1 n Type 2 n Unsure nOther n please specify .....……….............................
Do you take diabetes medication? Yes n No nIf yes n glucose lowering tabletsand/or n insulin
If you ticked insulin how many injections per day?n 1 n 2 n 3 n 4n Other, please specify
………….........................
If you ticked glucose lowering tablets, how many different tablets?
n 1 n 2 n 3 n Other, please specify
……………………………
Have you ever seen a Diabetes Educator? Yes n No n
Have you ever seen a Dietitian? Yes n No n
OA Eigenmann_Layout 1 5/3/11 12:53 PM Page 8

ORIGINAL ARTICLE
Development and validation of a diabetes knowledge questionnaire
170d Pract Diab Int May 2011 Vol. 28 No. 4 Copyright © 2011 John Wiley & Sons
Appendix 3. Diabetes Knowledge Questionnaire scoring instructions
For all questions with ONE answer:
1 = correct 0 = incorrect 0.5 = unsure
For all questions with AS MANY asapply answers enterfor each option i.e. a. b. c. d. e.:
1 = correct 0 = incorrect
For Question 9: Enter 0.3 if option a. or b. or c. are circled individually or 1 = correct, i.e. option d.
For people with type 2 diabetesNOT taking diabetes medicationthe total possible score is 26.
For people with type 2 diabetestaking diabetes medication thetotal possible score is 28.
For people/carers of people withtype 1 diabetes the total possiblescore is 32.
Correct answers
Question Correct number answer(s)
1 c
2 a
3 c
4 d
5 a, b, c, e
6 a
7 a, b, d, e
8 a, b, c, e,
9 d
10 a, c, d
11 c
12 a, b, d, e
13 c
14 c
15 a, b, c, e
OA Eigenmann_Layout 1 5/3/11 12:53 PM Page 9