dental students’ attitude towards anti-smoking programmes: a study in flanders, belgium
TRANSCRIPT

Dental students’ attitude towards anti-smoking
programmes: a study in Flanders, Belgium
J. Vanobbergen, P. Nuytens, M. van Herk and L. De VisschereDe Pintelaan 185, Ghent, Belgium
Objective: The aim of the study was to assess the dentalstudents’ attitude towards tobacco cessation counselling in the
dental setting and to explore the influence of knowledge, belief ineffectiveness, smoking status, gender and curriculum.
Material and methods: The study group consisted of allundergraduate students from the 2002–2003 classes of the
Ghent University (n ¼ 96). A validated questionnaire was admin-istered to all students involving four different sections: demogra-
phic characteristics, attitude related to tobacco cessationprogrammes in the dental setting, belief in their effectiveness
and knowledge concerning tobacco health effects. Statisticalanalysis included simple univariate nonparametric tests for
evaluating differences in attitude towards tobacco cessation
programmes, belief in effectiveness of tobacco cessation pro-grammes in the dental setting and knowledge of students
concerning tobacco health effects by year of graduation, smokingstatus and gender. Multiple logistic regression was chosen to
calculate adjusted odds ratios and 95% confidence intervals.Results: Students view willingness to advise individual patients
to quit using tobacco. Yet only 51.3% are willing to co-operate inanti-tobacco programmes at the community level, and the
perception of students of the effectiveness of smoking cessationcounselling in the dental setting is low. The variance of attitude
towards tobacco cessation programmes was significantly affec-ted by knowledge and the belief in effectiveness of tobacco
cessation programmes in the dental setting. Better knowledgeand belief in effectiveness of tobacco cessation counselling was
associated with an increasing positive attitude towards tobaccocessation programmes expressed by an odds ratio of 3.12 (95%
CI 1.00–9.67) and 1.17 (95% CI 1.00–1.37) respectively.Conclusion: Belief in effectiveness and knowledge seem to
influence the attitude of students towards tobacco cessationcounselling.
Practice implications: Besides imparting knowledge, theattitude of newly graduated dentists could be improved by
stressing the effectiveness of smoking cessation activities during
lectures and integrated training modules in the undergraduateeducation.
Key words: tobacco control; dental students; attitudes; patientcounselling.
ª 2007 The Authors. Journal Compilation ª 2007 BlackwellMunksgaard
Accepted for publication, 3 January 2007
Introduction
S moking has an important negative effect on
health. According to the most recent estimate by
the World Health Organization (WHO), 4.9 million
people worldwide died in 2000 as a result of their
addiction to nicotine (1). Tobacco use also causes
serious oral health problems. It is firmly established
that tobacco use is a primary cause of many oral
diseases and adverse oral conditions (2). Tobacco is a
risk factor for oral cancer, oral cancer recurrence, adult
periodontal diseases and congenital defects such as
cleft lips and palate in children (3, 4).
The dental team can play an important role in
tobacco control programmes, both, directed towards
the community as a whole or towards the individual
patient. Through participation in community and
political action and in counselling their patients to
quit, the health professional, in particular the dentist
and his/her team, can contribute to a more tobacco-
free society. Besides the important impact of national
and international legislation, there is ample evidence
that general medical practitioner advice to quit
tobacco use is respected by the majority of patients,
and several recent studies show that the efforts of
dentists can be equally effective (5–7).
The problem is that, while the majority of dentists
believe that providing information about tobacco
cessation and offering smoking cessation support are
both part of their duty, fewer dentists actually do so.
The reasons for not providing it include time and
reimbursement issues, poor education and lack of
further postgraduate training and poor co-ordination
of dental and smoking cessation services (8–10).
Another matter of research is the attitude of dental
students, the future dentists, towards tobacco control
177
Eur J Dent Educ 2007; 11: 177–183All rights reserved
ª 2007 The Authors. Journal Compilation ª 2007 Blackwell Munksgaard
euro pean journal of
Dental Education

programmes. Even when some reservations are men-
tioned, USA dental students appear to be positive
regarding their responsibility to educate patients
about the risks of tobacco use. There was a general
agreement that their educational programme ade-
quately prepared them to help smokers quit (11–13).
The majority of Australian dental students planned to
advise patients about tobacco use, although their
perception of the effectiveness of smoking cessation
counselling seems to be low (14). The same trend was
observed in Europe where Greek students considered
tobacco cessation counselling a duty for every dentist,
although an important part (32%) believed it to be
ineffective. On the other hand, students showed
significant knowledge on tobacco health effects (15).
The high rate of smoking among healthcare profes-
sional students in Hungary, Eastern Europe (16),
compared with Western European, American and
Australian students, could be an explanation why
they are less proactive regarding tobacco intervention.
The effectiveness of training health professionals to
deliver smoking cessation interventions to their
patients has been reviewed recently and reported in
the Cochrane database. The authors concluded that
training health professionals to provide smoking
cessation interventions had a measurable effect on
professional performance but that there was no
strong evidence that it changed smoking behaviour
(17). At least there is an agreement that students’
attitude will be influenced by peers, teachers and
curriculum content. The educational system’s move-
ment towards prevention and holism is a trend that
deals with the relevant themes in our changing
society and that can contribute to the development
of students’ attitudes. The reformation of the dental
and medical curriculum at Ghent University
switched the traditional biomedical orientation into
a more biosocial oriented and integrated approach:
patient-centred; student-centred; community orien-
ted; problem and evidence based. Within this new
dental curriculum, attention is paid to oral health
promotion, including tobacco cessation counselling.
Yet tobacco cessation counselling is taught only in
theoretical terms during the second year of the
education. This reformation should be beneficial in
reorienting dental students’ attitudes towards a more
positive attitude regarding health promotional and
educational programmes (18).
The aim of the present study was to assess the
dental students’ attitude towards tobacco cessation
promotion in the dental setting and to explore the
influence of knowledge, belief in effectiveness,
smoking status, gender and curriculum.
Materials and methods
The study group for the present study comprised
the dental students from the 2002–2003 classes of the
Ghent University. Dental education programme at
the Ghent University consists of two first-cycle years
(bachelor) and three second-cycle years (master). All
undergraduate students (n ¼ 96) participated in the
study with 25 students in the first year, 25 in the
second, 13 in the third, 11 in the fourth and 22 in
the final year. The final year students went through
their undergraduate education in the old curriculum.
As, from this moment, the new curriculum was
entered progressively, comparison between curricula
is possible.
A questionnaire was administered to all students
(Fig. 1). This questionnaire was designed with four
different sections: demographic characteristics, atti-
tude related to tobacco cessation programmes in
the dental setting, belief in their effectiveness and
knowledge concerning tobacco health effects.
In the first section respondents were asked about
their age, sex, actual smoking status and undergradu-
ate level. Non-smokers and ex-smokers were classified
as non-current smokers, moderate/social and heavy
smokers as current smokers.
In the second section, a seven-item tool generated a
total score for attitude related to tobacco cessation
programmes in the dental setting, both on an individ-
ual and on community level. This score was calculated
by totalising the ‘yes’ responses and was further
standardised to a maximum of 10 [(number of positive
answers/number of questions) · 10], a higher score
indicating a more positive attitude. For use in the
logistic regression analyses this variable was dicho-
tomised with the median value as the cut-off.
The third section comprised items dealing with
students’ belief in effectiveness of tobacco cessation
programmes in the dental setting. Two ‘yes or no’ close-
ended questions and one rank ordering question were
used to assess this item. The rank ordering question
asked the respondents to rank, in order of importance in
the tobacco counselling process, a list including health-
care workers, family, friends and the media. All three
questions had the same weight (maximum 1—mini-
mum 0). The rank ordering question was scored from 0
(the dentist ranked in the last place) to 1 (the dentist
ranked in the first place). This variable was further
handled the same way as the variable attitude.
In the last section 19 questions were included
assessing students’ knowledge concerning tobacco
health effects, in particular oral health effects. This
variable was calculated as the sum of correct answers
Vanobbergen et al.
178

and standardised to a maximum of 10. The questions
in this section were checked for relevance and the
evidence of the answer was based on data directly
addressing the question (2,3, 19–25).
The questionnaires were administered anony-
mously during scheduled class times and/or clinical
courses.
The questionnaire was pilot-tested prior to the
study. The relevance of questions, response formats
and wording was tested. The process resulted in
some questions being deleted and others being
changed. A test–retest with 10 students, spread over
the graduations years, smoking status and gender,
was performed to assess the reliability of the ques-
tionnaire with an interval of 1 month. Test–retest
measures (intra-class correlation) were combined
with nonparametric tests for related samples and
were used for the sum scores of attitude, belief in
effectiveness and knowledge (Table 1). The Wilcoxon
signed rank test was used to measure systematic
differences between the two related measurements.
For knowledge a significant systematic increase was
Graduation year:……………………………………………………………………….. Age:……………………… Gender: o male o female Smoker: o never o in the past o moderate/ social smoker
o heavy smoker
1. Are you willing to show your patients the damage that smoking can cause upon oral health?2. Are you willing to show your patients the damage that smoking can cause upon general health? 3. Are you willing to forbid the patients to smoke in the waiting-room of your own practice? 4. Are you willing to advise patients to stop smoking? 5. Are you willing to cooperate actively in anti-tobacco programs on community level? 6. Are you willing to use anti-tobacco programs in your own practice? (e.g. flyers, advisement,…etc.) 7. Do you think that every dentist has the duty to cooperate in anti-tobacco programs? 8. Do you think that anti-tobacco programs in the dental practice can be effective? 9. Do you think that the patients will take notice of your advisement?
What/who has the greatest influence on smoking behaviour: (classify from 1 to 10, starting with 1 = of greatest influence and 10 = of smallest influence) School Commercials on the street Doctor Friends
Colleagues Dentist
Do you think that smoking: 1. -can cause a nose polyp? 2. -can cause lung cancer? 3. -can slow down oral wound healing? 4. -can slow down growing? 5. -can cause nefropathology? 6. -can increase an existing periodontal pathology? 7. -can cause cancer of the oesophagal tractus? 8. -can cause oral cancer? 9. -can cause liver-dysfunction?
10.11.12.13.14.
15.
16.17.18.19.
-combined with alcohol has an increased risk of oral cancer? -can cause oral implant failure? -on elder age influences saliva-constitution? -of selfmade-cigarettes is worse than filter-cigarettes? -occurs more in upper class of the society? -during the pregnancy can cause breathing problems on the newly born child? -influences oral candidiasis? -influences leukoplakia? -influences taste sensitivity?
-influences the amount of saliva?
Fig. 1. Questionnaire (translated from the original Dutch).
Belgian dental students’ attitude towards tobacco control
179
found at the retest compared to the first test
(P < 0.05).
The survey was analysed using the SPSS 12.0
software package. Descriptive statistics were gener-
ated for relevant items. Univariate analysis was
performed with nonparametric Kruskal–Wallis and
Mann–Whitney tests.
Multiple logistic regression analyses were carried
out to determine the factors that were independently
related to the attitude towards tobacco cessation
programmes, belief in their effectiveness and know-
ledge of students concerning tobacco health effects.
Data were analysed as dichotomous variables (except
for ‘age’ and ‘year of graduation’) and compared
using odds ratios. Point estimates and 95% confidence
intervals were calculated. Odds were calculated in one
group (e.g. males) by dividing the number of males
with e.g. high knowledge by the number of males with
low knowledge. This odds calculation was repeated
for girls. The odds ratio was obtained by dividing the
odds of having a high knowledge among males by the
odds of having a high knowledge among girls.
Statistical significance level was set at P < 0.05.
Results
Response rate was 81% (78/96). Respondents were
62% female and 38% male. The average age of the
sample was 21.79 (SD 4.16) years. Seventy-five per
cent of respondents reported to be non-smokers.
A narrow majority of the students (53.8%) had an
explicit positive attitude towards tobacco cessation
programmes, receiving an average rating of at least 7.5
out of 10 (a score of 10 is the best possible attitude) on
the responses related to this item. All respondents
agreed to show their individual patients the oral
health hazards of tobacco use and 96% of respondents
were willing to use anti-tobacco programmes in their
practice to advise patients to quit using tobacco.
However, only 40% of respondents agreed that it
is the responsibility and duty of every dentist to
co-operate in anti-tobacco programmes and only
51.3% are willing to co-operate actively in anti-tobacco
counselling programmes at the community level.
Based on the descriptive analyses of the responses
related to the effectiveness of tobacco cessation activ-
ities in the dental setting, one can observe that the
mean score of all respondents was clearly lower
compared with the mean scores of attitude and
knowledge (5.1 vs. 8.1 and 8.3 respectively). Only
32% of the respondents had a score equal to or higher
than 7 on the 1 to 10 scale.
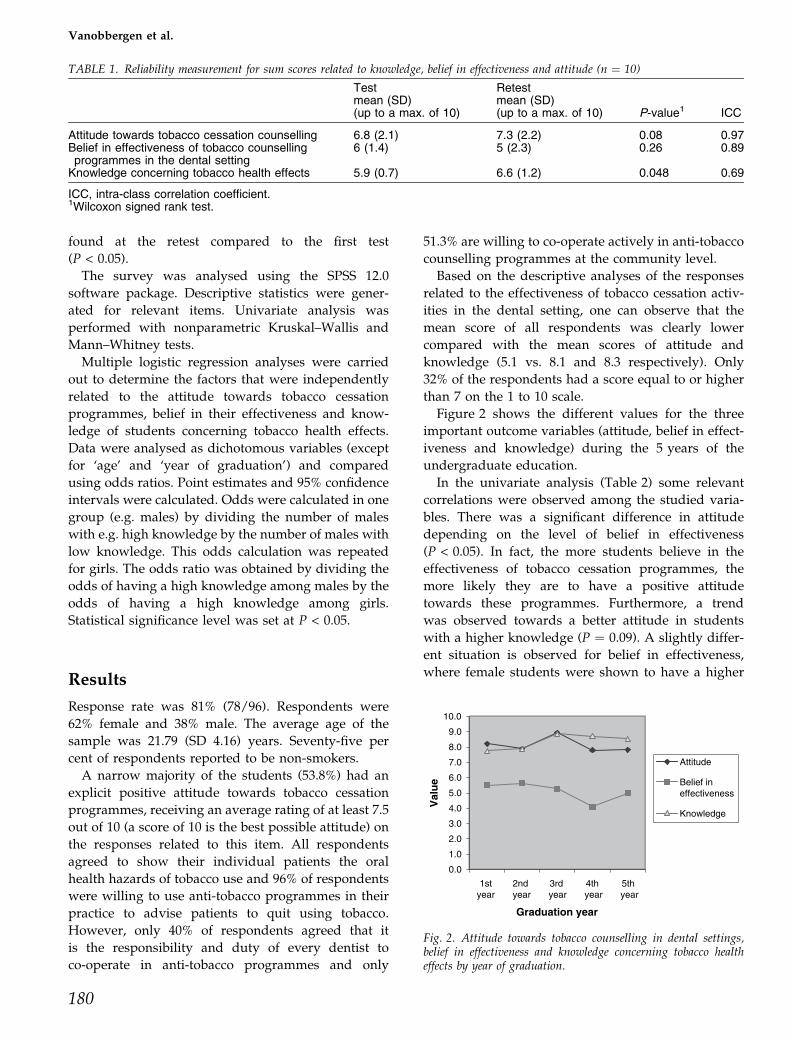
Figure 2 shows the different values for the three
important outcome variables (attitude, belief in effect-
iveness and knowledge) during the 5 years of the
undergraduate education.
In the univariate analysis (Table 2) some relevant
correlations were observed among the studied varia-
bles. There was a significant difference in attitude
depending on the level of belief in effectiveness
(P < 0.05). In fact, the more students believe in the
effectiveness of tobacco cessation programmes, the
more likely they are to have a positive attitude
towards these programmes. Furthermore, a trend
was observed towards a better attitude in students
with a higher knowledge (P ¼ 0.09). A slightly differ-
ent situation is observed for belief in effectiveness,
where female students were shown to have a higher
TABLE 1. Reliability measurement for sum scores related to knowledge, belief in effectiveness and attitude (n ¼ 10)
Testmean (SD)(up to a max. of 10)
Retestmean (SD)(up to a max. of 10) P-value1 ICC
Attitude towards tobacco cessation counselling 6.8 (2.1) 7.3 (2.2) 0.08 0.97Belief in effectiveness of tobacco counsellingprogrammes in the dental setting
6 (1.4) 5 (2.3) 0.26 0.89
Knowledge concerning tobacco health effects 5.9 (0.7) 6.6 (1.2) 0.048 0.69
ICC, intra-class correlation coefficient.1Wilcoxon signed rank test.
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
1styear
2nd year
3rd year
4th year
5th year
Graduation year
Val
ue
Attitude
Belief in effectiveness
Knowledge
Fig. 2. Attitude towards tobacco counselling in dental settings,belief in effectiveness and knowledge concerning tobacco healtheffects by year of graduation.
Vanobbergen et al.
180

belief in effectiveness of tobacco counselling than their
male counterparts (P < 0.05). For knowledge the only
significant correlation found in the data was the effect
of graduation level (P < 0.01). No differences were
found between final year students (old curriculum)
and the others (new curriculum).
Logistic regression models determined the inde-
pendent impact of demographic factors (gender,
smoking status, level of graduation and age) on
knowledge of students concerning tobacco health
effects, attitude towards tobacco cessation pro-
grammes and belief in effectiveness of tobacco cessa-
tion programmes in the dental setting. These models
explained about 18% of the variance of the outcome
variable (R2 ¼ 0.18, 0.18 and 0.17 respectively). They
indicated that knowledge increased with year of
graduation, but not necessarily with age (Table 3).
The odds ratio for increasing knowledge per year was
2.03 (95% CI 1.20–3.44), representing a significant
increasing knowledge during the undergraduate
education with a peak between the second and the
third year (first and second cycle). The variance of
attitude towards tobacco cessation programmes was
significantly affected by knowledge and the belief
in effectiveness of tobacco cessation programmes in
the dental setting. Better knowledge and belief in
effectiveness of tobacco cessation counselling was
associated with an increasing positive attitude
TABLE 2. Univariate analysis for differences in attitude towards tobacco cessation programmes, belief in effectiveness of tobacco cessationprogrammes in the dental setting and knowledge of students (n ¼ 78) concerning tobacco health effects by year of graduation, smoking statusand gender
Attitude Belief in effectiveness Knowledge
Mean P-value Mean P-value Mean P-value
Graduation year 0.361 0.741 <0.011
First year 82 5.5 7.8Second year 7.9 5.6 7.9Third year 8.9 5.3 8.9Fourth year 7.8 4.1 8.7Fifth year 7.8 5.0 8.5
Curriculum 0.342 0.662 0.192
New curriculum 8.2 5.2 8.2Old curriculum 7.8 5.0 8.5
Smoking status 0.242 0.642 0.442
Current smoker 7.7 4.8 8.4Current non-smoker 8.2 5.3 8.3
Gender 0.352 <0.052 0.972
Female 8.2 5.4 8.4Male 7.9 4.7 8.3
Belief in effectiveness <0.052
Less effective 7.7Effective 8.3
Knowledge 0.092 0.552
Low knowledge 7.7 5.5High knowledge 8.3 5.0
1Kruskal–Wallis test.2Mann–Whitney test.The P-values in bold are significant values at the 0.05 level.
TABLE 3. Logistic regression model with knowledge, attitude towards tobacco cessation programs and belief in effectiveness of tobaccocessation programs in the dental setting as dependent variables adjusting for gender, smoking status, year of graduation and age
Explanatory variable
Attitude Knowledge Effectiveness
P-value OR 95% CI P-value OR 95% CI P-value OR 95% CI
GenderMale vs. female 0.83 0.89 0.31–2.51 0.87 0.91 0.30–2.75 0.23 0.54 0.20–1.50
Smoking statusSmoker vs. non-smoker 0.51 0.68 0.22–2.16 0.91 0.88 0.25–3.10 0.62 0.75 0.31–2.34
Year of graduation 0.23 0.75 0.48–1.19 <0.01 2.03 1.20–3.44 0.44 0.84 0.54–1.30Age 0.96 1 0.84–1.18 <0.05 0.76 0.61–0.96 0.91 0.99 0.86–1.18Belief in effectiveness 0.05 1.17 1.00–1.37Attitude 0.09 2.22 0.89–5.97Knowledge 0.05 3.12 1.00–9.67 0.44 0.65 0.22–1.95Constant 0.84 0.72 0.02 96.80 0.82 1.44
Nagelkerke R 2 ¼ 0.18.
Belgian dental students’ attitude towards tobacco control
181

towards tobacco cessation programmes expressed
by an odds ratio of 3.12 (95% CI 1.00–9.67) and 1.17
(95% CI 1.00–1.37) respectively.
Discussion and conclusion
DiscussionWhen interpreting the results of this study one has to
take into consideration some limitations. First, not-
withstanding the high response rate, the 78 students
represent a rather small sample. The number of
incoming dental students in Flanders is actually very
low. During a national campaign a few years ago,
pursued by the dental association, young people were
dissuaded from attempting a dental career. This
resulted in a political debate followed by the restric-
tion of the intake of students to the programmes of
medicine and dentistry in Flanders through an
entrance examination. Second, the development and
implementation of the present study was conducted in
only one dental school (there are two dental schools in
Flanders). Thus, the findings reported in this study
may have a limited generalisability and the power of
the study may be limited. Non-response bias was
evaluated but no significant differences were found
between non-responders and responders in gender,
year of graduation and smoking status.
Nevertheless, the results may reveal important
information about Flemish dental students’ attitude,
beliefs and knowledge towards tobacco cessation
counselling in the dental setting.
Compared to the current literature, smoking pre-
valence of dental undergraduates in the University of
Gent remains high with 25% of the students being
current smokers. Unfortunately, smoking prevalence
increased progressively with the year of study from
12.5% in the first year to 38.1% in the final year, which
goes against the trend observed in several interna-
tional reports (12). In comparing current smokers with
non-smokers, no differences in attitudes, beliefs and
knowledge were observed, which is in agreement with
the literature.
Approximately two-thirds of the respondents were
female, reflecting the actual trend towards increasing
numbers of females in dental schools all over the
Western world. The only gender difference observed
in the univariate analysis was that females tended to
have more confidence in the effect of tobacco coun-
selling in the dental setting. Gender was one of the
confounders included in the logistic regression model,
but no gender differences were found in the multiple
analyses.
The fact that 96% of students were willing to advise
patients to quit using tobacco is consistent with the
results of previous studies mentioned in the Introduc-
tion, but it seems remarkable that a lower percentage
of them (40%) reported that it is their responsibility
and duty to co-operate in anti-tobacco programmes.
Knowledge seems to influence the attitude of dental
students, but the very wide confidence interval may
threaten the validity of this finding.
The low mean score observed for ‘belief in effect-
iveness’ indicates that respondents have low confid-
ence in the fact that tobacco counselling offered in the
dental office can have an impact on patients’ quitting.
This rather low perception of effectiveness follows the
general trend reported in the literature (13–15). These
responses suggest that many students may still be
sceptical about the extent to which tobacco cessation
counselling is effective in helping patients to quit.
Much remains to be done in the undergraduate
education to show the scientific evidence on both the
efficacy and cost-effectiveness of tobacco prevention.
Standardised and simple schemes, such as the ‘Four
As’, are widely used around the world, and advice on
how to use this scheme is available. Here too, there is
ample evidence proving that dentists’ advice to quit
tobacco use is respected by the majority of patients (26,
27). The present study shows that belief in effective-
ness of tobacco cessation counselling may also con-
tribute to the attitude of students towards tobacco
counselling. It is all the more reason why the effect-
iveness of tobacco programmes should be emphasised
in the dental curriculum.
So far, the effect of the new curriculum on students’
attitude, belief and knowledge has been minimal. As
suggested in the literature one may need more
alternate teaching methods such as problem-based
discussions, tutorials, small group discussion and
skills laboratories to improve the awareness, belief
and skills of dental students, especially in this matter,
in which attitudes play a significant role. Gradually
these alternate methods will be implemented in the
new curriculum, recently once again adapted to the
Bologna agreement. However, the follow-up period in
the present study was too short to reveal the longer
term effects of the new curriculum. Further research
will be carried out to evaluate this new Bachelor-
Master structure.
ConclusionDental students’ attitude towards tobacco cessation
counselling in the dental setting represents a promis-
ing baseline for future tobacco cessation programme
development. Students view willingness to advise
Vanobbergen et al.
182

individual patients to quit using tobacco. Yet only a
minority are willing to co-operate in anti-tobacco
programmes at the community level, and the percep-
tion of students of the effectiveness of smoking
cessation counselling in the dental setting is low.
Knowledge and belief in effectiveness seem to influ-
ence the attitude of students towards tobacco cessation
counselling.
Practice implicationsBesides imparting knowledge, the attitude of newly
graduated dentists could be improved by stressing the
effectiveness of smoking cessation activities during
lectures and integrated training modules in the
undergraduate education. Both aspects, the commu-
nity-based programmes and the individual communi-
cation skills, need to be emphasised.
References
1. Petersen PE. The World Oral Health Report 2003:continuous improvement of oral health in the 21stcentury – the approach of the WHO Global Oral HealthProgramme. Community Dent Oral Epidemiol 2003: 31(Suppl. 1): 3–23.
2. Petersen PE. Tobacco and oral health – the role of theWorld Health Organization. Oral Health Prev Dent 2003:1: 309–315.
3. Reibel J. Tobacco and oral diseases. Update on theevidence, with recommendations. Med Princ Pract 2003:12 (Suppl. 1): 22–32.
4. Little J, Cardy A, Munger RG. Tobacco smoking and oralclefts: a meta-analysis. Bull World Health Organ 2004: 82:213–218.
5. Warnakulasuriya S. Effectiveness of tobacco counsellingin the dental office. J Dent Educ 2002: 66: 1079–1087.
6. Johnson NW. The role of the dental team in tobaccocessation. Eur J Dent Educ 2004: 8 (Suppl. 4): 18–24.
7. Carr AB, Ebbert JO. Interventions for tobacco cessation inthe dental setting. Cochrane Database Syst Rev 2006: 1:CD005084.
8. Monaghan N. What is the role of dentists in smokingcessation? Br Dent J 2002: 193: 611–612.
9. Allard RH. Tobacco and oral health: attitudes andopinions of European dentists; a report of the EUworking group on tobacco and oral health. Int Dent J2000: 50: 99–102.
10. Allard RH. The role of health professionals in discour-aging tobacco use. Ned Tijdschr Tandheelkd 2004: 111:396–399.
11. Yip JK, Hay JL, Ostroff JS, Stewart RK, Cruz GD. Dentalstudents’ attitudes toward smoking cessation guidelines.J Dent Educ 2000: 64: 641–650.
12. Fried JL, Reid BC, DeVore LE. A comparison of healthprofessions student attitudes regarding tobacco curriculaand interventionist roles. J Dent Educ 2004: 68: 370–377.
13. Victoroff KZ, Dankulich-Huryn T, Haque S. Attitudes ofincoming dental students toward tobacco cessation pro-motion in the dental setting. J Dent Educ 2004: 68:563–568.
14. Rikard-Bell G, Groenlund C, Ward J. Australian dentalstudents’ views about smoking cessation counselling andtheir skills as counsellors. J Public Health Dent 2003: 63:200–206.
15. Polychonopoulou A, Gatou T, Athanassouli T. Greekdental students’ attitudes toward tobacco control pro-grammes. Int Dent J 2004: 54: 119–125.
16. Nagy K, Barabas K, Nyari T. Attitudes of Hungarianhealthcare professional students to tobacco and alcohol.Eur J Dent Educ 2004: 8 (Suppl. 4): 32–35.
17. Lancaster T, Silagy C, Fowler G. Training health profes-sionals in smoking cessation. Cochrane Database SystRev 2000: 3: CD000214.
18. Deveugele M, Derese A, DeMaesschalck S, Willems S,Van Driel M, De Maeseneer J. Teaching communicationskills to medical students, a challenge in the curriculum?Patient Educ Couns 2005: 58: 265–270.
19. Bergstrom J. Tobacco smoking and chronic destructiveperiodontal disease. Odontology 2004: 92: 1–8.
20. Whiteford L. Nicotine, CO and HCN: the detrimentaleffects of smoking on wound healing. Br J CommunityNurs 2003: 8: S22–S26.
21. Vehemente VA, Chuang SK, Daher S, Muftu A, DodsonTB. Risk factors affecting dental implant survival. J OralImplantol 2002: 28: 74–81.
22. Macgregor ID. Effects of smoking on oral ecology.A review of the literature. Clin Prev Dent 1989: 11:3–7.
23. Sudbo J, Samuelsson R, Risberg B, et al. Risk markers oforal cancer in clinically normal mucosa as an aid insmoking cessation counselling. J Clin Oncol 2005: 23:1927–1933.
24. Charalabopoulos K, Assimakopoulos D, Karkabounas S,Danielidis V, Kiortsis D, Evangelou A. Effects of cigarettesmoking on the antioxidant defence in young healthymale volunteers. Int J Clin Pract 2005: 59: 25–30.
25. Khan GJ, Mehmood R, Salah UD, Ihtesham UH. Effectsof long-term use of tobacco on taste receptors andsalivary secretion. J Ayub Med Coll Abbottabad 2003:15: 37–39.
26. Havlicek D, Stafne E, Pronk NP. Tobacco cessationinterventions in dental networks: a practice-based eval-uation of the impact of education on provider know-ledge, referrals, and pharmacotherapy use. Prev ChronicDis 2006: 3: A96.
27. Silagy C, Stead LF. Physician advice for smokingcessation. Cochrane Database Syst Rev 2001: 2:CD000165.
Address:
Prof Jacques Vanobbergen
De Pintelaan 185
Ghent
Belgium 9000
Tel: +32 9240 4025
Fax: +32 9240 3851
e-mail: [email protected]
Belgian dental students’ attitude towards tobacco control
183