delayed hemorrhage after pancreaticoduodenectomy
TRANSCRIPT

DS
Tdp3
atabphhc
N
RFUCsI
©P
elayed Hemorrhage after Pancreaticoduodenectomyeong Ho Choi, MD, Hyoun Jong Moon, MD, Jin Seok Heo, MD, Jae Won Joh, MD, Yong Il Kim, MD
BACKGROUND: Postoperative hemorrhage, particularly delayed hemorrhage after pancreaticoduodenectomy, isa serious complication and one of the most common causes of mortality after pancreatico-duodenectomy.
STUDY DESIGN: The medical records of 500 patients who underwent pancreaticoduodenectomy between Oc-tober 1994 and December 2002 were analyzed with regard to postoperative hemorrhagiccomplications. Delayed hemorrhage was defined as bleeding at the operation site after 5 or morepostoperative days.
RESULTS: Delayed hemorrhage occurred in 22 patients (4.4%), with a median time of 13 days (range 7 to32 days) after pancreaticoduodenectomy, and developed more frequently (9/77 versus 13/423,p � 0.003) in patients with preceding intraabdominal complications such as pancreatic fistula,bile fistula, and intraabdominal abscess. In 17 of these 22 patients, angiography and laparotomyrevealed bleeding foci at 14 arterial and 3 anastomotic sites. In nine patients, hemorrhagedeveloped from pseudoaneurysms of the major arteries around the pancreaticojejunostomy.Hemostatis was attempted by transcatheter arterial embolization in 14 patients and with lapa-rotomy in 4 patients. Four of 14 patients who received transcatheter arterial embolizationeventually required laparotomy. Overall, 4 of the 22 delayed hemorrhage patients died (18.2%)of complications related to massive bleeding or transcatheter arterial embolization.
CONCLUSIONS: Delayed hemorrhage after pancreaticoduodenectomy is associated with a high mortality. Intra-abdominal complications after pancreaticoduodenectomy should be evaluated properly andguidelines for the diagnosis and treatment of delayed hemorrhage should be established inadvance. Clinicians must be alert to the possibility of pseudoaneurysm hemorrhage. ( J Am CollSurg 2004;199:186–191. © 2004 by the American College of Surgeons)
5mrm
MTdMsap18
tp(aa
he mortality rate after pancreaticoduodenectomy hasecreased markedly over the last several decades. Com-lication rates do persist at the unacceptably high level of0% to 40%.1-4
Hemorrhage is one of the leading causes of morbiditynd mortality after pancreaticoduodenectomy.5-9 In par-icular, delayed hemorrhage occurring 5 or more daysfter operation is associated with a high mortality rateecause diagnosis is difficult and the hemorrhage mayresent as abrupt massive bleeding.10-13 Several reportsave described experiences and the treatment of delayedemorrhage after pancreaticoduodenectomy but debateontinues as to its causes, diagnosis, and treatment.9,14-18
We encountered 22 delayed hemorrhages among
o competing interests declared.
eceived October 1, 2003; Revised April 6, 2004; Accepted April 7, 2004.rom the Department of Surgery, Samsung Medical Center, Sungkyunkwanniversity School of Medicine, Seoul, Korea.orrespondence address: Jin Seok Heo, MD, Department of Surgery, Sam-
ung Medical Center. Sungkyunkwan University School of Medicine, 50rwon-dong, Gangnam-gu, Seoul, Korea 135-710.
1862004 by the American College of Surgeons
ublished by Elsevier Inc.
00 pancreaticoduodenectomies over an approxi-ately 8-year period. Here, we provide a review of the
isk factors, clinical presentations, and treatmentodalities.
ETHODShe clinical and operative data of 500 patients who un-erwent pancreaticoduodenectomy at the Samsungedical Center, Seoul, Korea (Sungkyunkwan Univer-
ity) between October 1994 and December 2002 werenalyzed with regard to postoperative hemorrhagic com-lications. The patient group consisted of 303 men and97 women with a mean age of 57.3 years (range 16 to2 years).The classic Whipple procedure, involving gastric an-
rum removal, was performed in 310 patients (62%),ylorus-preserving pancreaticoduodenectomy in 13527%), total pancreatectomy in 40, and hepatopancre-ticoduodenectomy in 15. The pancreatic remnant wasnastomosed to the jejunum using the telescoping
ISSN 1072-7515/04/$30.00doi:10.1016/j.jamcollsurg.2004.04.005

mi
stqies
hwi
a�stwAwatFri
ROpcpetptcw
(dtclpccN
ttphtc4ppswAshtch
gotnfotihagcp
TdC
PDHWIBPNCOT
*g†
6
187Vol. 199, No. 2, August 2004 Choi et al Delayed Hemorrhage after Pancreaticoduodenectomy
ethod and a short silicone elastomer stent was insertednto the pancreatic duct without any external drainage.
We define delayed hemorrhage as bleeding from theurgical site 5 days or more after pancreaticoduodenec-omy, and this was further restricted to cases that re-uired a blood transfusion of � 2 U of packed RBCs,ntensive treatment such as laparotomy or transarterialmbolization (TAE), and surgical intensive care unitupervision.
Preceding intraabdominal complications that mayave affected the occurrence of delayed hemorrhageere specified as pancreatic fistula, biliary fistula, and
ntraabdominal abscess.Pancreatic fistula was defined as a condition with an
mylase level of five times the upper normal level, ie,100 U/L, as determined by the fluid taken from the
urgical drains after 3 postoperative days, without regardo the amount. Biliary fistula was defined as a conditionherein the bile was excreted through surgical drains.n intraabdominal abscess was defined as a conditionith clinical manifestations of fever and abdominal pain
nd complicated fluid collection by abdominal CT. Sta-istical analysis was performed using the chi-square test,isher’s exact test, t-test, Kruskal-Wallis test, and logisticegression as appropriate. Results were considered signif-cant when the p value was � 0.05.
ESULTSne or more significant complications occurred in 162
atients (32.4%) and 65 patients (13.0%) had 2 or moreomplications. The most frequent complication wasancreatic fistula (10.8%), followed by delayed gastricmptying (7.8%). A postoperative hemorrhage was thehird most common complication and occurred in 38atients (7.6%); delayed hemorrhage after 5 postopera-ive days developed in 22 patients. We experienced 6ases of postoperative mortality (1.2%), and 4 of theseere because of hemorrhage (Table 1).Sixteen men and 6 women, mean age 56.8 years
range 40 to 80 years), in whom delayed hemorrhageeveloped, experienced significant bleeding at a medianime of 13 days (range 7 to 32 days) after pancreati-oduodenectomy. Twenty-one patients experienced de-ayed bleeding during their first hospital stay and oneatient after discharge. Eleven patients were treated forommon bile duct cancer, five patients for pancreaticancer, and six patients for ampulla of Vater cancer.one of the patients underwent pancreaticoduodenec-
omy for benign disease. Surgical modalities includedhe classic Whipple procedure in 17 cases, pylorus-reserving pancreaticoduodenectomy in 3 cases, andepatopancreaticoduodenectomy in 2 cases. Nine ofhese 22 patients had definite preceding intraabdominalomplications. Mean length of hospital stay was1.6 days in patients with delayed bleeding, 36.1 days inatients with other complications, and 19.4 days inatients with no complications. By univariate analy-is, only preceding intraabdominal complicationsere statistically associated with delayed hemorrhage.ge, gender, type of disease, and type of operation
howed no significant statistical relation with delayedemorrhage development. Multivariate analysis of allhe risk factors showed that preceding intraabdominalomplications independently influenced delayedemorrhage development (p � 0.008, Table 2).The bleeding focus was verified surgically and angio-
raphically in 17 of the 22 patients with delayed hem-rrhage. Three of these patients showed hemorrhage inhe anastomotic area and included two pancreaticojeju-ostomies and one gastrojejunostomy. Hemorrhagerom the artery adjacent to the remnant pancreas devel-ped in 14 patients—including 5 cases of ligated gas-roduodenal artery, 3 common hepatic arteries, 3 prox-mal branches of the superior mesenteric artery, 1 properepatic artery, 1 right hepatic artery, and 1 short gastricrtery. Nine pseudoaneurysms occurred: five cases wereastroduodenal artery pseudoaneurysms, three wereommon hepatic artery pseudoaneurysms, and one wasroper hepatic artery pseudoaneurysm.
able 1. Postoperative Complications after Pancreaticoduo-enectomy (n � 500)omplication n %
ancreatic fistula 54 10.8elayed gastric emptying 39 7.8emorrhage 38* 7.6ound infection 38 7.6
ntraabdominal abscess 27 5.4iliary fistula 15 3.0ulmonary complication 12 2.4ewly developed diabetes mellitus 31 6.2hyle leakage 5 1.0thers 12 2.4otal 162† 32.4
Twenty-two patients (58%) developed delayed hemorrhage 5 days after sur-ery: 21 during hospital stay and 1 after discharge.Sixty-five patients developed 2 or more complications and death occurred incases.
ppdtapt
dsc(
cwatpbcseopttfordbmopioerrroaofst
TS
H
PAU
*
TH
C
A
G
P
M
L
P
T
P
*†
‡
tApNt
188 Choi et al Delayed Hemorrhage after Pancreaticoduodenectomy J Am Coll Surg
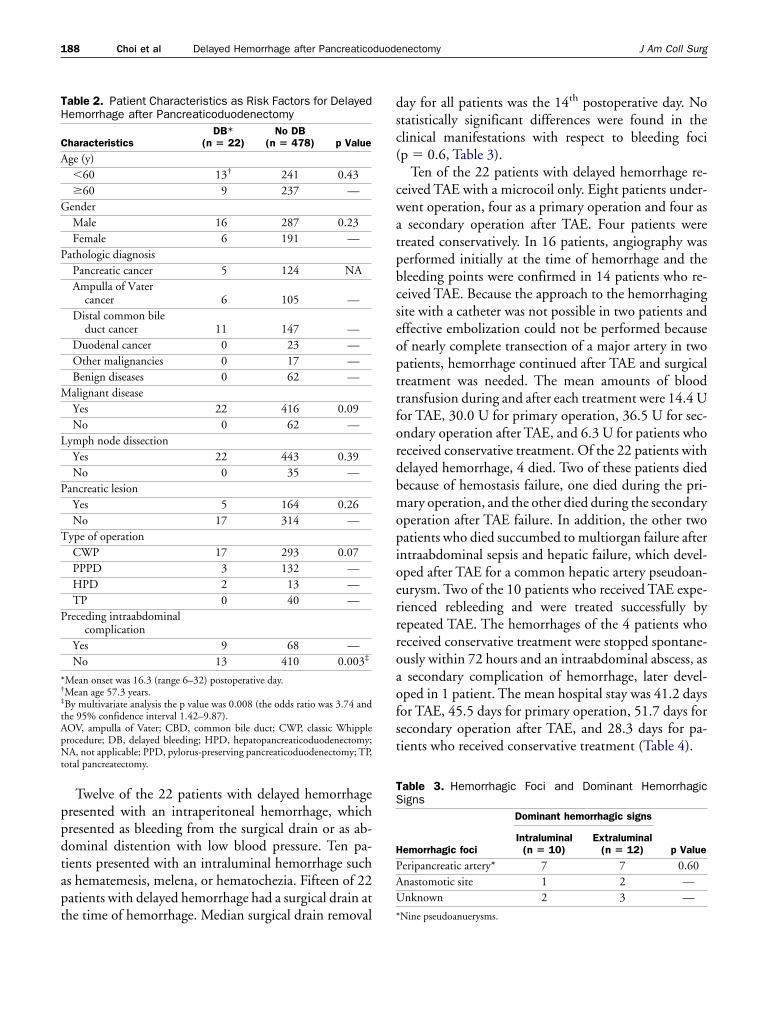
Twelve of the 22 patients with delayed hemorrhageresented with an intraperitoneal hemorrhage, whichresented as bleeding from the surgical drain or as ab-ominal distention with low blood pressure. Ten pa-ients presented with an intraluminal hemorrhage suchs hematemesis, melena, or hematochezia. Fifteen of 22atients with delayed hemorrhage had a surgical drain athe time of hemorrhage. Median surgical drain removal
able 2. Patient Characteristics as Risk Factors for Delayedemorrhage after Pancreaticoduodenectomy
haracteristicsDB*
(n � 22)No DB
(n � 478) p Value
ge (y)�60 13† 241 0.43�60 9 237 —
enderMale 16 287 0.23Female 6 191 —
athologic diagnosisPancreatic cancer 5 124 NAAmpulla of Vater
cancer 6 105 —Distal common bile
duct cancer 11 147 —Duodenal cancer 0 23 —Other malignancies 0 17 —Benign diseases 0 62 —alignant diseaseYes 22 416 0.09No 0 62 —
ymph node dissectionYes 22 443 0.39No 0 35 —
ancreatic lesionYes 5 164 0.26No 17 314 —
ype of operationCWP 17 293 0.07PPPD 3 132 —HPD 2 13 —TP 0 40 —
receding intraabdominalcomplication
Yes 9 68 —No 13 410 0.003‡
Mean onset was 16.3 (range 6–32) postoperative day.Mean age 57.3 years.By multivariate analysis the p value was 0.008 (the odds ratio was 3.74 andhe 95% confidence interval 1.42–9.87).OV, ampulla of Vater; CBD, common bile duct; CWP, classic Whipplerocedure; DB, delayed bleeding; HPD, hepatopancreaticoduodenectomy;A, not applicable; PPD, pylorus-preserving pancreaticoduodenectomy; TP,
otal pancreatectomy.
ay for all patients was the 14th postoperative day. Notatistically significant differences were found in thelinical manifestations with respect to bleeding focip � 0.6, Table 3).
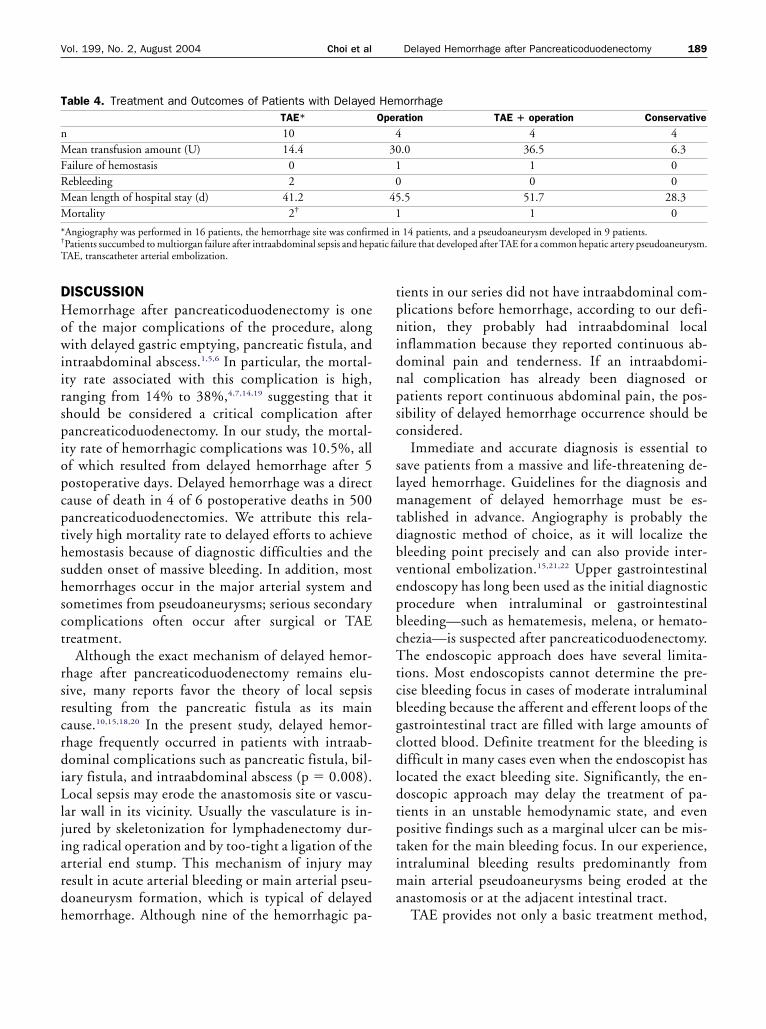
Ten of the 22 patients with delayed hemorrhage re-eived TAE with a microcoil only. Eight patients under-ent operation, four as a primary operation and four assecondary operation after TAE. Four patients were
reated conservatively. In 16 patients, angiography waserformed initially at the time of hemorrhage and theleeding points were confirmed in 14 patients who re-eived TAE. Because the approach to the hemorrhagingite with a catheter was not possible in two patients andffective embolization could not be performed becausef nearly complete transection of a major artery in twoatients, hemorrhage continued after TAE and surgicalreatment was needed. The mean amounts of bloodransfusion during and after each treatment were 14.4 Uor TAE, 30.0 U for primary operation, 36.5 U for sec-ndary operation after TAE, and 6.3 U for patients whoeceived conservative treatment. Of the 22 patients withelayed hemorrhage, 4 died. Two of these patients diedecause of hemostasis failure, one died during the pri-ary operation, and the other died during the secondary
peration after TAE failure. In addition, the other twoatients who died succumbed to multiorgan failure afterntraabdominal sepsis and hepatic failure, which devel-ped after TAE for a common hepatic artery pseudoan-urysm. Two of the 10 patients who received TAE expe-ienced rebleeding and were treated successfully byepeated TAE. The hemorrhages of the 4 patients whoeceived conservative treatment were stopped spontane-usly within 72 hours and an intraabdominal abscess, assecondary complication of hemorrhage, later devel-
ped in 1 patient. The mean hospital stay was 41.2 daysor TAE, 45.5 days for primary operation, 51.7 days forecondary operation after TAE, and 28.3 days for pa-ients who received conservative treatment (Table 4).
able 3. Hemorrhagic Foci and Dominant Hemorrhagicigns
emorrhagic foci
Dominant hemorrhagic signs
p ValueIntraluminal
(n � 10)Extraluminal
(n � 12)
eripancreatic artery* 7 7 0.60nastomotic site 1 2 —nknown 2 3 —
Nine pseudoanuerysms.
DHowiirspiopcpthshsct
rsrcrdiLljiardh
tpnidnpsc
slmtdbvepbcTtcbgcdldtptima
T
nMFRMM
*†
T
189Vol. 199, No. 2, August 2004 Choi et al Delayed Hemorrhage after Pancreaticoduodenectomy
ISCUSSIONemorrhage after pancreaticoduodenectomy is one
f the major complications of the procedure, alongith delayed gastric emptying, pancreatic fistula, and
ntraabdominal abscess.1,5,6 In particular, the mortal-ty rate associated with this complication is high,anging from 14% to 38%,4,7,14,19 suggesting that ithould be considered a critical complication afterancreaticoduodenectomy. In our study, the mortal-ty rate of hemorrhagic complications was 10.5%, allf which resulted from delayed hemorrhage after 5ostoperative days. Delayed hemorrhage was a directause of death in 4 of 6 postoperative deaths in 500ancreaticoduodenectomies. We attribute this rela-ively high mortality rate to delayed efforts to achieveemostasis because of diagnostic difficulties and theudden onset of massive bleeding. In addition, mostemorrhages occur in the major arterial system andometimes from pseudoaneurysms; serious secondaryomplications often occur after surgical or TAEreatment.
Although the exact mechanism of delayed hemor-hage after pancreaticoduodenectomy remains elu-ive, many reports favor the theory of local sepsisesulting from the pancreatic fistula as its mainause.10,15,18,20 In the present study, delayed hemor-hage frequently occurred in patients with intraab-ominal complications such as pancreatic fistula, bil-
ary fistula, and intraabdominal abscess (p � 0.008).ocal sepsis may erode the anastomosis site or vascu-
ar wall in its vicinity. Usually the vasculature is in-ured by skeletonization for lymphadenectomy dur-ng radical operation and by too-tight a ligation of therterial end stump. This mechanism of injury mayesult in acute arterial bleeding or main arterial pseu-oaneurysm formation, which is typical of delayedemorrhage. Although nine of the hemorrhagic pa-
able 4. Treatment and Outcomes of Patients with DelayedTAE*
10ean transfusion amount (U) 14.4
ailure of hemostasis 0ebleeding 2ean length of hospital stay (d) 41.2ortality 2†
Angiography was performed in 16 patients, the hemorrhage site was confirmPatients succumbed to multiorgan failure after intraabdominal sepsis and hepAE, transcatheter arterial embolization.
ients in our series did not have intraabdominal com-lications before hemorrhage, according to our defi-ition, they probably had intraabdominal local
nflammation because they reported continuous ab-ominal pain and tenderness. If an intraabdomi-al complication has already been diagnosed oratients report continuous abdominal pain, the pos-ibility of delayed hemorrhage occurrence should beonsidered.
Immediate and accurate diagnosis is essential toave patients from a massive and life-threatening de-ayed hemorrhage. Guidelines for the diagnosis and
anagement of delayed hemorrhage must be es-ablished in advance. Angiography is probably theiagnostic method of choice, as it will localize theleeding point precisely and can also provide inter-entional embolization.15,21,22 Upper gastrointestinalndoscopy has long been used as the initial diagnosticrocedure when intraluminal or gastrointestinalleeding—such as hematemesis, melena, or hemato-hezia—is suspected after pancreaticoduodenectomy.he endoscopic approach does have several limita-
ions. Most endoscopists cannot determine the pre-ise bleeding focus in cases of moderate intraluminalleeding because the afferent and efferent loops of theastrointestinal tract are filled with large amounts oflotted blood. Definite treatment for the bleeding isifficult in many cases even when the endoscopist has
ocated the exact bleeding site. Significantly, the en-oscopic approach may delay the treatment of pa-ients in an unstable hemodynamic state, and evenositive findings such as a marginal ulcer can be mis-aken for the main bleeding focus. In our experience,ntraluminal bleeding results predominantly from
ain arterial pseudoaneurysms being eroded at thenastomosis or at the adjacent intestinal tract.
TAE provides not only a basic treatment method,
orrhageation TAE � operation Conservative
4 4.0 36.5 6.3
1 00 0
.5 51.7 28.31 0
14 patients, and a pseudoaneurysm developed in 9 patients.ilure that developed after TAE for a common hepatic artery pseudoaneurysm.
HemOper
43010
451
ed inatic fa

beazomtgoIsoetfl
wecbagaeoodmawoepppsdetp
ASAADC
SOS
R
1
1
1
1
1
1
1
1
1
1
190 Choi et al Delayed Hemorrhage after Pancreaticoduodenectomy J Am Coll Surg
ut also a temporary hemostatic effect that makes itasy to operate if necessary. Recently, owing to theccumulation of experiences and advances in emboli-ation tools and materials, the management of hem-rrhage and minimization of adverse affects with TAEay be more possible in selective areas now than in
he past. TAE has also been used widely and hasained acceptance in the last decade for the treatmentf other forms of visceral bleeding or pseudoaneurysm.n cases where the distal part of an arteriogram is ob-cured, a nearly complete-cut vessel is observed, or hem-rrhage occurs in a technically unapproachable area, thefficiency of TAE may be markedly reduced and opera-ion should be undertaken without delay. In our series,atal hepatic failure occurred in one patient after embo-ization of the common hepatic artery.
Nine of our cases (40.9%) of delayed hemorrhageere the result of pseudoaneurysms. In our experi-
nce, pseudoaneurysmal bleeding after pancreati-oduodenectomy is not a rare complication and maye the most important cause of delayed hemorrhagefter pancreaticojejunostomy. Attention should beiven to hemorrhages from pseudoaneurysms becausecute massive bleeding may occur and treatment bymbolization and operation is more difficult than inther types of hemorrhage.23,24 In patients with risksf delayed hemorrhage, helical CT with three-imensional angiographic images that use a contrastedium to obtain overall information on the intra-
bdominal vascular state should be obtained evenhen there are no signs or symptoms. On observationf pseudoaneurysms by CT angiography, preventivembolization by conventional angiography should beerformed, even if small-sized. Delayed hemorrhageostpancreaticoduodenectomy remains a fatal com-lication. Patient’s risk factors and warning signshould be properly evaluated. Procedures for theiagnosis and treatment of hemorrhage must bestablished in advance; and it should be rememberedhat hemorrhage is likely in the event of aseudoaneurysm.
uthor Contributionstudy conception and design: Heocquisition of data: Moonnalysis and interpretation of data: Choirafting of manuscript: Moonritical revision: Heo
tatistical expertise: Choibtaining funding: Heo, Joh
upervision: Kim
EFERENCES
1. Crist DW, Sitzmann JV, Cameron JL. Improved hospital mor-bidity, mortality, and survival after the Whipple procedure. AnnSurg 1987;206:358–365.
2. Cameron JL, Pitt HA, Yeo CJ, et al. One hundred and forty-fiveconsecutive pancreaticoduodenectomies without mortality. AnnSurg 1993;217:430–435; discussion 435–438.
3. Trede M, Schwall G, Saeger HD. Survival after pancreatoduo-denectomy. 118 consecutive resections without an operativemortality. Ann Surg 1990;211:447–458.
4. Miedema BW, Sarr MG, van Heerden JA, et al. Complicationsfollowing pancreaticoduodenectomy. Current management.Arch Surg 1992;127:945–949; discussion 949–950.
5. Trede M, Schwall G. The complications of pancreatectomy. AnnSurg 1988;207:39–47.
6. Yeo CJ. Management of complications following pancreati-coduodenectomy. Surg Clin North Am 1995;75:913–924.
7. Chou FF, Sheen-Chen SM, Chen YS, et al. Postoperative mor-bidity and mortality of pancreaticoduodenectomy for periamp-ullary cancer. Eur J Surg 1996;162:477–481.
8. Farley DR, Schwall G, Trede M. Completion pancreatectomyfor surgical complications after pancreaticoduodenectomy. Br JSurg 1996;83:176–179.
9. Balladur P, Christophe M, Tiret E, Parc R. Bleeding of thepancreatic stump following pancreatoduodenectomy for cancer.Hepatogastroenterology 1996;43:268–270.
0. Sugimoto H, Kaneko T, Ishiguchi T, et al. Delayed rupture of apseudoaneurysm following pancreatoduodenectomy: report of acase. Surg Today 2001;31:932–935.
1. Papadimitriou J, Vassiliou J, Papadimitriou L, Prachalias A. De-layed haemorrhage after pancreatoduodenectomy. Int Surg2000;85:275.
2. Yoshida T, Matsumoto T, Morii Y, et al. Delayed massive intra-peritoneal hemorrhage after pancreatoduodenectomy. Int Surg1998;83:131–135.
3. Otah E, Cushin BJ, Rozenblit GN, et al. Visceral arterypseudoaneurysms following pancreatoduodenectomy. ArchSurg 2002;137:55–59.
4. Rumstadt B, Schwab M, Korth P, et al. Hemorrhage after pan-creatoduodenectomy. Ann Surg 1998;227:236–241.
5. Sato N, Yamaguchi K, Shimizu S, et al. Coil embolization ofbleeding visceral pseudoaneurysms following pancreatectomy:the importance of early angiography. Arch Surg 1998;133:1099–1102.
6. van Berge Henegouwen MI, Allema JH, van Gulik TM, et al.Delayed massive haemorrhage after pancreatic and biliary sur-gery. Br J Surg 1995;82:1527–1531.
7. Brodsky JT, Turnbull AD. Arterial hemorrhage after pancre-atoduodenectomy. The ‘sentinel bleed’. Arch Surg 1991;126:1037–1040.
8. Shankar S, Russell RC. Haemorrhage in pancreatic disease. Br JSurg 1989;76:863–866.
9. Bottger TC, Junginger T. Factors influencing morbidity andmortality after pancreaticoduodenectomy: critical analysis of

2
2
2
2
2
191Vol. 199, No. 2, August 2004 Choi et al Delayed Hemorrhage after Pancreaticoduodenectomy
221 resections. World J Surg 1999;23:164–171; discussion171–172.
0. Aranha GV, O’Neil S, Borge MA. Successful nonoperative man-agement of bleeding hepatic artery pseudoaneurysm followingpancreaticoduodenectomy. Dig Surg 1999;16:528–530.
1. Boudghene F, L’Hermine C, Bigot JM. Arterial complicationsof pancreatitis: diagnostic and therapeutic aspects in 104 cases. JVasc Interv Radiol 1993;4:551–558.
2. Reber PU, Baer HU, Patel AG, et al. Superselective microcoil
embolization: treatment of choice in high-risk patients with ex-trahepatic pseudoaneurysms of the hepatic arteries. J Am CollSurg 1998;186:325–330.
3. Yamakado K, Nakatsuka A, Tanaka N, et al. Transcatheter arte-rial embolization of ruptured pseudoaneurysms with coils andn-butyl cyanoacrylate. J Vasc Interv Radiol 2000;11:66–72.
4. Savastano S, Feltrin GP, Antonio T, et al. Arterial complicationsof pancreatitis: diagnostic and therapeutic role of radiology.
Pancreas 1993;8:687–692.