definition: epileptic seizure - cme · pdf fileassociated with long-term treatment ! ......
TRANSCRIPT
Definition: Epileptic Seizure n Dysfunction of the brain involving paroxysmal
and disorderly depolarization of neurons and spread of the resulting neuronal discharge through brain tissue
n Major categories for children – Febrile vs afebrile – Provoked vs unprovoked
Wilden JA, Cohen-Gadol AA. Am Fam Physician. 2012;86(4):334-340. Gilman S. N Engl J Med. 1992;326:1671-1676. Hirtz D, et al. Neurology. 2000;55(5):616-623.
Seizure Imitators n Tics n Attention deficits n Apneic attacks (breath-holding spells) n Headaches n Sleepwalking/night terrors n Fear/panic n Psychogenic seizures n Syncope
Prensky AL, Pshytycky A. In: Pellock JM, Bourgeois BFD, Dodson WE. Pediatric Epilepsy, 3rd ed. 2008.
Definition: “Epilepsy” n Variety of disorders characterized by chronic,
recurrent seizures of central nervous system origin
n ≥2 unprovoked epileptic seizuresàepilepsy
Wilden JA, Cohen-Gadol AA. Am Fam Physician. 2012;86(4):334-340. Gilman S. N Engl J Med. 1992;326:1671-1676. Hirtz D, et al. Neurology. 2000;55(5):616-623.
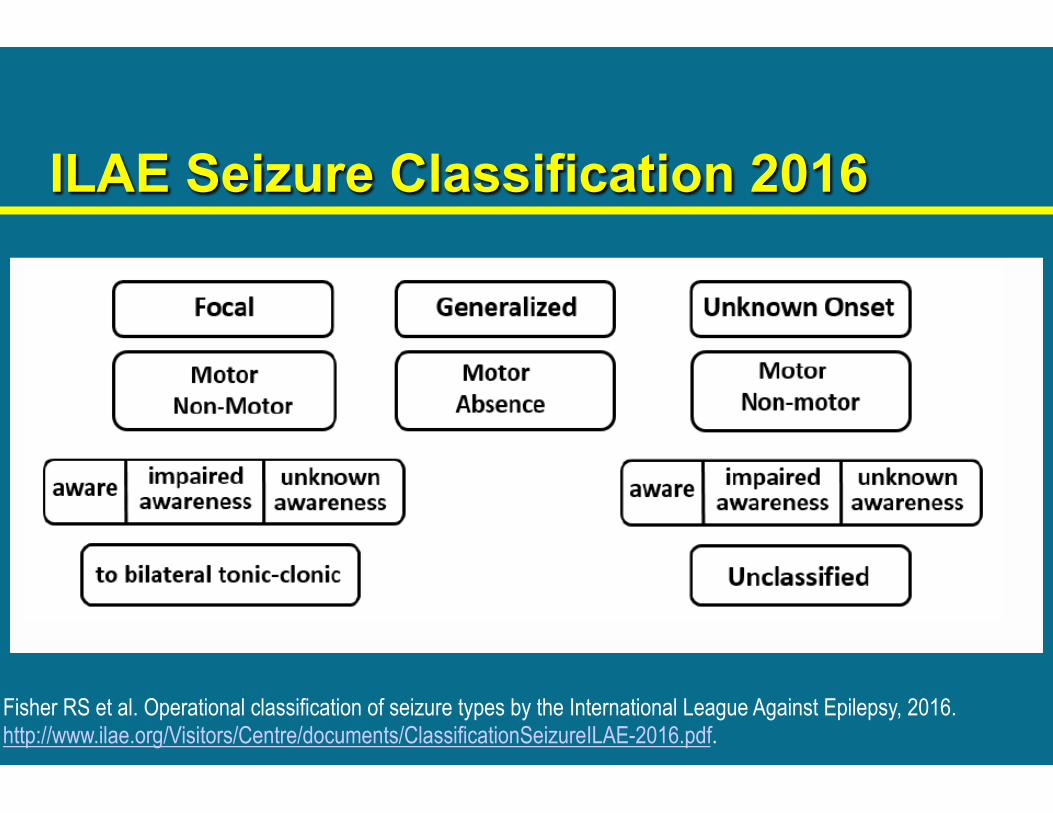
ILAE Seizure Classification 2016
Fisher RS et al. Operational classification of seizure types by the International League Against Epilepsy, 2016. http://www.ilae.org/Visitors/Centre/documents/ClassificationSeizureILAE-2016.pdf.
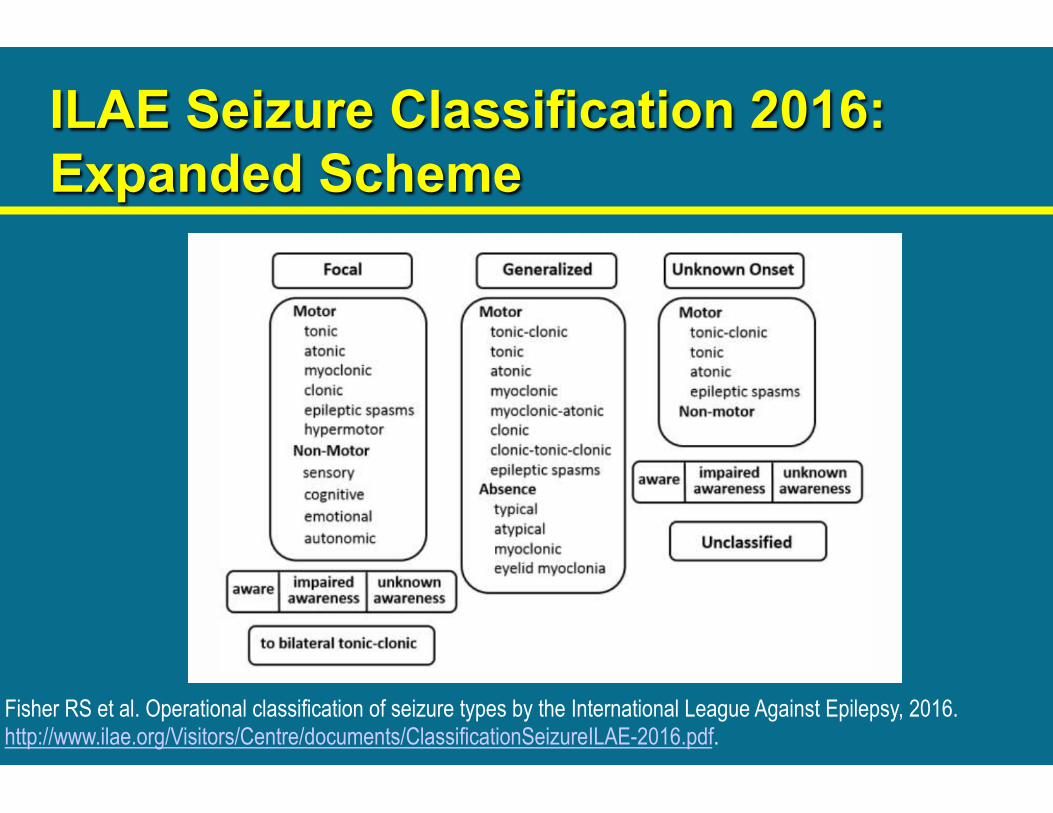
ILAE Seizure Classification 2016: Expanded Scheme
Fisher RS et al. Operational classification of seizure types by the International League Against Epilepsy, 2016. http://www.ilae.org/Visitors/Centre/documents/ClassificationSeizureILAE-2016.pdf.
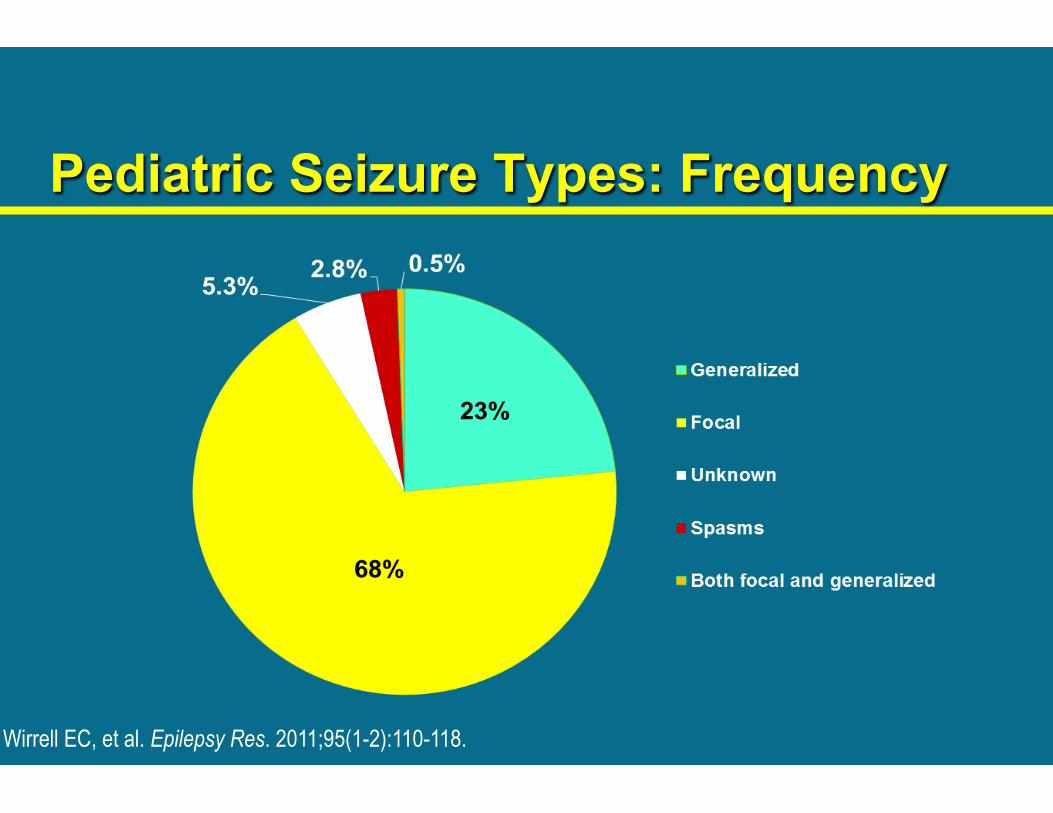
Pediatric Seizure Types: Frequency
Wirrell EC, et al. Epilepsy Res. 2011;95(1-2):110-118.

Etiology of Epilepsy
Idiopathic 65.5%
Degenerative 3.5%
Infection 2.5% Neoplastic
4.1%
Vascular 10.9%
Trauma 5.5%
Congenital 8.0%
Hauser WA. Epilepsia. 1992;33(suppl 4):S6-S14.
Epilepsy Syndromes 1. Benign familial neonatal convulsions 2. Severe myoclonic epilepsy of infancy 3. ADNFE – BECTS – BEOP 4. Childhood and juvenile absence epilepsy 5. Juvenile myoclonic epilepsy 6. Infantile spasms/West syndrome 7. Lennox-Gastaut syndrome 8. Progressive myoclonic epilepsies 9. Landau-Kleffner syndrome (LKS)
ADNFE = autosomal dominant nocturnal frontal lobe epilepsy; BECTS = benign rolandic epilepsy with centro-temporal spikes; BEOP = benign childhood epilepsy with occipital paroxysms. Epilepsy Foundation. Types of epilepsy syndromes. http://www.epilepsy.com/learn/types-epilepsy-syndromes.
Establishing Treatment Goals
n General goals with treatment – Eliminate seizures or reduce their frequency to
the maximum degree possible – Avoid adverse AED effects, particularly those
associated with long-term treatment n Monotherapy preferred
– Aid patients in maintaining or restoring usual psychosocial and vocational activities
Goldenberg MM. P T. 2010;35(7):392-415.
Medication Adherence
n Importance of medication adherence in epilepsy management
n Barriers to adherence n Ways to improve adherence in children
Modi AC, et al. Neurology. 2014;82(8):671-673.
Common, Pharmacology-related Side Effects of AEDs
n Predictable n Dose dependent
– Generally reversible with dose reduction or discontinuation
n Explained by known pharmacologic properties of AED
Crepeau AZ, et al. Drug Healthc Patient Saf. 2012;4:39-54.
Common Adverse Events of AEDs n Gastrointestinal: nausea, vomiting, increased
appetite, decreased appetite n Neurocognitive: sedation, ataxia/vertigo, tremor,
insomnia, irritability, hyperactivity n Headache n Electrolyte disturbances: hyponatremia,
metabolic acidosis n Reduced bone density
Crepeau AZ, et al. Drug Healthc Patient Saf. 2012;4:39-54.

Common Neurocognitive Comorbidities in Children with Epilepsy n Intellectual disabilities n Learning disorders n Attention deficit disorder (ADD) n Anxiety and depression/suicidal ideation n Important to identify and treat early n Avoid, if possible, AEDs that might exacerbate
– Phenobarbital, benzodiazepines, levetiracetam, valproic acid, vigabatrin, topiramate
n Start AEDs at lower dosages, titrate slowly
Crepeau AZ, et al. Drug Healthc Patient Saf. 2012;4:39-54.

Rare Serious Adverse Events of AEDs
n May be life-threatening n More commonly idiosyncratic, unpredictable n May not be reversible with AED discontinuation n Concerns heightened in…
– Specific age groups – Specific ethnic groups – With other associated conditions or medications
Crepeau AZ, et al. Drug Healthc Patient Saf. 2012;4:39-54.
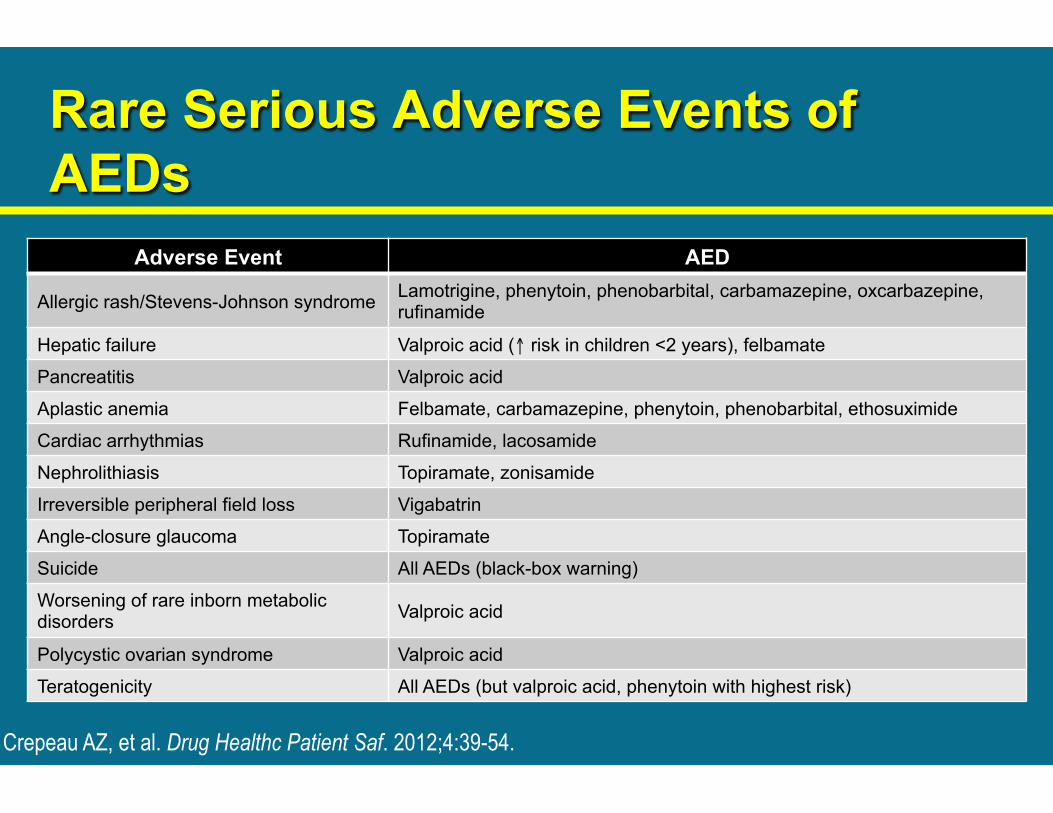
Rare Serious Adverse Events of AEDs
Adverse Event AED
Allergic rash/Stevens-Johnson syndrome Lamotrigine, phenytoin, phenobarbital, carbamazepine, oxcarbazepine, rufinamide
Hepatic failure Valproic acid (↑ risk in children <2 years), felbamate
Pancreatitis Valproic acid
Aplastic anemia Felbamate, carbamazepine, phenytoin, phenobarbital, ethosuximide
Cardiac arrhythmias Rufinamide, lacosamide
Nephrolithiasis Topiramate, zonisamide
Irreversible peripheral field loss Vigabatrin
Angle-closure glaucoma Topiramate
Suicide All AEDs (black-box warning)
Worsening of rare inborn metabolic disorders Valproic acid
Polycystic ovarian syndrome Valproic acid
Teratogenicity All AEDs (but valproic acid, phenytoin with highest risk)
Crepeau AZ, et al. Drug Healthc Patient Saf. 2012;4:39-54.
Monitoring for Adverse Effects n Before starting AED
– Educate parents and other family members about common and idiosyncratic reactions
– Obtain routine laboratory tests (CBC, LFTs) n While taking AED
– Periodic blood monitoring? n May lead to false security regarding idiosyncratic reactions n Minor WBC reductions or LFTs increasesà
possibly viral infection and not AED related
Crepeau AZ, et al. Drug Healthc Patient Saf. 2012;4:39-54.
Seizure Safety: Level of Intervention Depends on Nature of Seizure n Levels of responses
– Without changes in awareness—eg, focal aware seizure – With changes in awareness—eg, focal unaware or typical absence
seizure – With loss of consciousness—eg, generalized tonic-clonic seizure
n Responses generally focused on safety and protection from injury, not restraint – 911 if breathing difficulties, protracted seizures à concerns about status
epilepticus – Possible use of prescribed diazepam rectal gel by parents or other non-
medical persons for cluster or breakthrough seizures in people (>2 years) with refractory epilepsy
Epilepsy Foundation. Tailoring first aid plans http://www.epilepsy.com/get-help/seizure-first-aid/tailoring-first-aid-plans.
Convulsive Status Epilepticus n Prolonged generalized tonic-clonic seizure
– Active part of seizure lasts ≥5 minutes – Second seizure occurs without recovery of
consciousness from first seizure – Repeat seizures for ≥30 minutes
n Requires urgent treatment – Supportive (O2, IV fluids) and pharmacologic – In-hospital evaluation
Epilepsy Foundation. Status epilepticus. http://www.epilepsy.com/learn/impact/seizure-emergencies/status-epilepticus.
Nonconvulsive Status Epilepticus n Prolonged focal unaware or typical absence seizure n Prolonged confused or altered awareness, but patient
not “unconscious” n May be hard to recognize n Emergency intervention depends on how long a child’s
typical seizures are and how often they occur n Requires in-patient emergency medical treatment
– EEG may be needed to confirm diagnosis – Patients at risk for convulsive status epilepticus
Epilepsy Foundation. Status epilepticus. http://www.epilepsy.com/learn/impact/seizure-emergencies/status-epilepticus.
Sudden Unexpected Death in Epilepsy (SUDEP) n Sudden unexpected death of an otherwise-healthy
person with epilepsy1 – No other cause of death at autopsy
n >1/1000 people with epilepsy die of SUDEP1 – If seizures uncontrolled à risk of SUDEP increases to >1/150 – SUDEP rare in children, but leading cause of death in young
adults with uncontrolled seizures n Often not discussed with patients or caregivers, yet
parents want to know about it2
1. Epilepsy Foundation. SUDEP. http://www.epilepsy.com/learn/impact/mortality/sudep. 2. Institute of Medicine. Epilepsy Across the Spectrum: Promoting Health and Understanding. 2012.
SUDEP: When to Inform
n Growing consensus – Provide information around time of diagnosis, when
talking about epilepsy’s risks – Especially when SUDEP risk factors exist
n Persistent seizures n Refusal of treatment or suspected medication
nonadherence n When generalized tonic-clonic seizures occur
Institute of Medicine. Epilepsy Across the Spectrum: Promoting Health and Understanding. Washington (DC): National Academies Press (US); .