deferoxamine iron chelation increases δ-aminolevulinic acid induced protoporphyrin ix in xenograft...
TRANSCRIPT

Research Note
Deferoxamine Iron Chelation Increases d-Aminolevulinic Acid InducedProtoporphyrin IX in Xenograft Glioma Model
Pablo A. Valdes*1,2, Kimberley Samkoe2, Julia A. O’Hara2, David W. Roberts1,3, Keith D. Paulsen2
and Brian W. Pogue*2
1Dartmouth Medical School, Dartmouth College, Hanover, NH2Thayer School of Engineering, Dartmouth College, Hanover, NH3Section of Neurosurgery, Dartmouth-Hitchcock Medical Center, Lebanon, NH
Received 18 August 2009, accepted 5 October 2009, DOI: 10.1111/j.1751-1097.2009.00664.x
ABSTRACT
Exogenous administration of d-aminolevulinic acid (d-ALA)leads to selective accumulation of protoporphyrin IX (PpIX) in
brain tumors, and has shown promising results in increasing
extent of resection in fluorescence-guided resection (FGR) of
brain tumors. However, this approach still suffers from heter-
ogeneous staining and so some tumor margins may go undetected
because of this variation in PpIX production. The aim of this
study was to test the hypothesis that iron chelation therapy could
increase the level of fluorescence in malignant glioma tumors.
Mice implanted with xenograft U251-GFP glioma tumor cells
were given a 200 mg kg)1
dose of deferoxamine (DFO), once a
day for 3 days prior to d-ALA administration. The PpIX
fluorescence observed in the tumor regions was 1.9 times the
background in animal group without DFO, and 2.9 times the
background on average, in the DFO pre-treated group. A 50%increase in PpIX fluorescence contrast in the DFO group was
observed relative to the control group (t-test P-value == 0.0020).
These results indicate that iron chelation therapy could signif-
icantly increase d-ALA-induced PpIX fluorescence in malignant
gliomas, pointing to a potential role of iron chelation therapy for
more effective FGR of brain tumors.
INTRODUCTION
Malignant gliomas account for approximately 70% of primarybrain tumors in the United States (1). Surgical resection playsan important role in treatment and prognosis of patients with
brain tumors, with studies showing a correlation betweenextent of resection and patient survival (2–5). Current neuro-surgical resection of malignant gliomas includes intraoperative
3-D image guidance. A limitation of current image guidancetechnologies is the degree of intraoperative brain shift, causinga significant registration error between patient physical spaceand image space (6–8). In recent years, large clinical efforts,
mostly in Germany and Japan, have used fluorescence
characteristics of tumors after exogenous d-aminolevulinicacid (d-ALA) administration to guide neurosurgical resectionof brain tumors providing real-time neurosurgical guidance
(3,9–15). While this technique is promising, the fluorescencesignal from low-grade tumors and certain tumor types is stillbelow detectable levels, and so methods which might increase
the production of protoporphyrin IX (PpIX) generation arestill needed. Two major techniques have been used to increasePpIX fluorescence: iron chelation therapy and differentiationtherapy (e.g. methotrexate, vitamin D) (16–22). In this paper,
iron chelation to sequester away available iron in the body istested to see if this would increase the PpIX signal in gliomatumors.
Exogenous administration of d-ALA overloads the hemebiosynthetic pathway, causing accumulation of PpIX to levelswhich allow visual detection using commercial surgical micro-
scope systems. Studies have shown that PpIX accumulation isselective to high-grade brain tumor over normal tissue (12,23–26). The reasons for selective PpIX accumulation after d-ALAadministration are many and the causes likely vary with
different tumor types; however, in the brain, the breakdown ofthe blood–brain barrier is a major factor in increased deliveryof d-ALA (23).
The ALA-Glioma Study group used fluorescence-guidedresection (FGR) for treatment of glioblastoma multiforme,showing a highly statistically significant difference in extent of
resection between patients undergoing FGR compared withstandard white–light-guided resection (3,9,11). Although thesestudies showed an increase in extent of resection using FGR as
well as a correlation between extent of resection and patientsurvival, studies have also shed light on a major limitation ind-ALA-induced PpIX production for FGR: tumor marginscontaining diffuse tumor cells accumulate significant levels of
PpIX, nonetheless, these levels are not high enough to bedetected with commercial surgical systems (10,14,27,28). Thepotential for improved detection through enhancing the signal is
always present, however, this will likely not be in the area of thetotal light intensity, but rather in the area of enhanced filteringand fluorescence detection, relative to the excitation light.
Significantly increased PpIX levels at tumor margins mightlead to more effective FGR and greater extent of resection of
*Corresponding authors email: [email protected](Pablo A. Valdes); [email protected] (Brian W. Pogue)
� 2009TheAuthors. JournalCompilation.TheAmericanSociety ofPhotobiology 0031-8655/10
Photochemistry and Photobiology, 2010, 86: 471–475
471

previously undetected tumor tissue. Previous in vitro work withprostate cancer cells, brain tumor cells, adenocarcinoma celllines (20,29), bladder and pancreatic cancer cells (30), skin celllines (21,31,32), and in vivo work with bladder epithelium (22)
and skin tumors (31) used iron chelators to increase levels ofPpIX fluorescence. Iron chelation reduces the availability offree iron that would be used by the ferrochelatase enzyme for
insertion into the PpIX molecule, thereby increasing the netaccumulation of PpIX (29,33). In this study, we used deferox-amine (DFO), a well-known iron chelator in clinical use for
over 30 years (34,35). DFO is a hexadentate iron chelatororiginally isolated from the fungus Streptomyces pylosus,which forms feroxamine, a stable 1:1 chelator–iron complex,
with subsequent urinary and biliary excretion. DFO isadministered parenterally with reported doses from 20 to360 mg kg)1day)1, with a limit of 6 g day)1 (34,36–39). Somecommon adverse effects are: local skin reactions, urine
discoloration, neurotoxicity, ototoxicity and skeletal changes(35,36). In this report, the d-ALA-PpIX fluorescence systemwas studied in a xenograft glioma model with ex vivo analysis
of the enhancement ratio. Animals were treated with DFO, totest the hypothesis that iron chelation therapy leads tosignificant increases in PpIX fluorescence of gliomas.
MATERIALS AND METHODS
Cell culture. A GFP transfected U251 (U251-GFP) human glioma cellline was used in this study. Cells were cultured in Dulbecco’s modifiedeagle’s medium (Cellgro, Mediatech, Herndon, VA) with 10% fetalbovine serum (Atlanta Biologicals, Lawrenceville, GA) 1% (v ⁄ v)penicillin–streptomycin (P–S) prepared from a stock solution of10 000 IU penicillin and 10 000 g mL)1 streptomycin (Mediatech).Incubation was done in a humidified environment consisting of 95%air and 5% CO2 at 37�C.
Animal model. This study was approved by the Dartmouth CollegeAnimal Care and Use Committee (IACUC). Intracranial implantationof U251-GFP cells was performed on 6-week-old male athymic nudemice. Mice were anesthetized using a 90:10 mg kg)1 ratio mixture ofketamine ⁄ xylazine and body temperature was maintained using aheating pad during anesthesia. Skull landmarks were exposed via asmall scalp incision on the superior part of the cranium. A 1 mm holein the cranium located 2 mm anterior to the bregma and 2 mm left ofthe midline was made with a Dremel drill. A needle was subsequentlyinserted 2 mm deep into the brain via stereotactic frame guidance, and1 · 106 cells in 10 lL)1 of PBS were injected over a period of 5 minusing a Hamilton syringe. The needle was retracted and skull cleaned.The drilled hole was covered with bone wax and the scalp incisionclosed with Vetbond tissue adhesive (J.A. Webster, Inc., Sterling, MA).Mice were examined daily to ensure proper healing of the scalp.
Chelation therapy and PpIX fluorescence quantification. Mice wereseparated into two groups: the DFO treatment group and the controlgroup, with both receiving d-ALA. The DFO group received200 mg kg)1 of DFO mesylate (Sigma, St. Louis, MO) dissolved in200 lL)1 deionized water administered i.p. at 11, 12, and 13 days aftertumor implantation. An equal volume of deionized water wasadministered i.p. at 11, 12, and 13 days after tumor implantation tothe control group. At day 14 after tumor implantation 100 mg kg)1 d-ALA (Sigma) dissolved in PBS was administered to both groups i.p.Two hours after d-ALA administration mice were killed, their brainsresected whole under dim lighting, and sectioned into 1 mm thickcoronal slices. The sectioned faces were placed on a fluorescence platescanner (Typhoon 9410, GE Healthcare Life Sciences) facing thescanner imaging plane. Measurement of PpIX fluorescence was donewith a 633 nm excitation laser and 650 nm long pass emission filter,followed with measurements of tissue GFP fluorescence with a 488 nmlaser excitation and 526 nm short pass emission filter.
Image analysis. GFP and PpIX fluorescence contrast in braintumors was calculated:
FC ¼ SItumor � SIbkgSInl � SIbkg
ð1Þ
where FC refers to fluorescence contrast of tumor; SItumor refers to anaverage signal intensity of a region of known tumor tissue; SIbkg refersto an average signal intensity of background; SInl refers to an averagesignal intensity of normal brain in the contralateral hemisphere. Thecoefficient of variation for PpIX fluorescence was calculated:
CV ¼ SD
SItumorð2Þ
where CV refers to the coefficient of variation of tumor; SD refers tothe standard deviation of the signal intensity of a region of knowntumor tissue. Assessment of a significant difference of the mean GFPfluorescence contrast, mean PpIX fluorescence contrast and meancoefficient of variation in PpIX fluorescence between the control andDFO treatment groups was done using an unpaired Student’s t-test. Atotal of 10 mice were studied, five for each group. For each mouse,three different regions of tumor tissue were analyzed to determine theSItumor, for a total of 30 different tumor tissue regions analyzed. A P-value <0.05 was considered statistically significant. All statisticalanalyses were done with Stata 10.0 (Stata Corporation, College Sta-tion, TX).
RESULTS
Following the treatment with DFO and d-ALA, and extractionand fluorescence scanning of the samples, the regions to bequantified were identified by the GFP fluorescence, indicating
positive tumor regions. The PpIX-positive fluorescent tissuescolocalized to areas of GFP-positive fluorescent tissue in miceare shown for an example data set in Fig. 1. The GFP signal isonly visible in areas of tumor (right slices) and the PpIX is seen
in background normal brain, with highlighted areas in thetumor regions. Fluorescence intensities were quantified fromthe GFP-positive regions and are listed in the summary data of
Table 1.The values for mean GFP fluorescence contrast, mean PpIX
fluorescence contrast and mean coefficient of variation in PpIX
fluorescence contrast as well as their corresponding 95%confidence intervals for the DFO and control groups aresummarized in Table 1.
Figure 1. U251-GFP coronal brain sections. (upper) Representativecoronal brain section of control animal with PpIX-positive fluorescenttissue colocalized to a fraction of the GFP-positive fluorescent tumorarea. (lower) Representative coronal brain section of DFO-treatedanimal with PpIX-positive fluorescent tissue colocalized with themajority of GFP-positive fluorescent tissue.
472 Pablo A. Valdes et al.
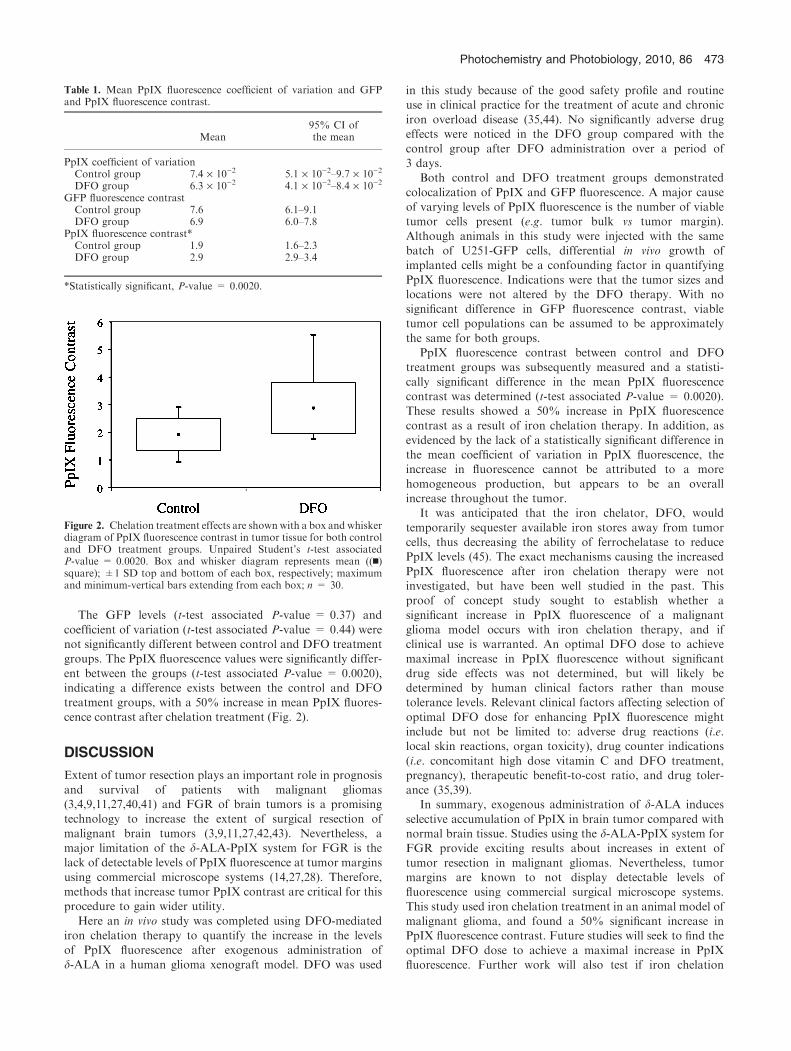
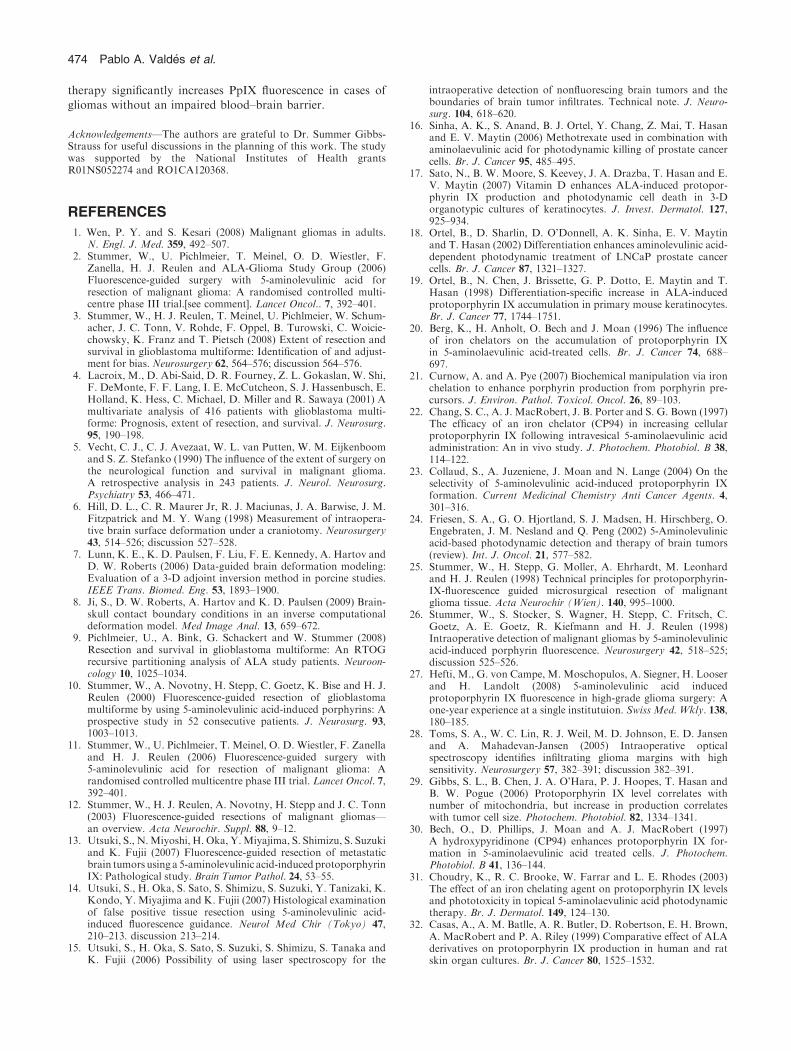
The GFP levels (t-test associated P-value = 0.37) and
coefficient of variation (t-test associated P-value = 0.44) werenot significantly different between control and DFO treatmentgroups. The PpIX fluorescence values were significantly differ-
ent between the groups (t-test associated P-value = 0.0020),indicating a difference exists between the control and DFOtreatment groups, with a 50% increase in mean PpIX fluores-cence contrast after chelation treatment (Fig. 2).
DISCUSSION
Extent of tumor resection plays an important role in prognosisand survival of patients with malignant gliomas(3,4,9,11,27,40,41) and FGR of brain tumors is a promisingtechnology to increase the extent of surgical resection of
malignant brain tumors (3,9,11,27,42,43). Nevertheless, amajor limitation of the d-ALA-PpIX system for FGR is thelack of detectable levels of PpIX fluorescence at tumor margins
using commercial microscope systems (14,27,28). Therefore,methods that increase tumor PpIX contrast are critical for thisprocedure to gain wider utility.
Here an in vivo study was completed using DFO-mediatediron chelation therapy to quantify the increase in the levelsof PpIX fluorescence after exogenous administration of
d-ALA in a human glioma xenograft model. DFO was used
in this study because of the good safety profile and routineuse in clinical practice for the treatment of acute and chroniciron overload disease (35,44). No significantly adverse drugeffects were noticed in the DFO group compared with the
control group after DFO administration over a period of3 days.
Both control and DFO treatment groups demonstrated
colocalization of PpIX and GFP fluorescence. A major causeof varying levels of PpIX fluorescence is the number of viabletumor cells present (e.g. tumor bulk vs tumor margin).
Although animals in this study were injected with the samebatch of U251-GFP cells, differential in vivo growth ofimplanted cells might be a confounding factor in quantifying
PpIX fluorescence. Indications were that the tumor sizes andlocations were not altered by the DFO therapy. With nosignificant difference in GFP fluorescence contrast, viabletumor cell populations can be assumed to be approximately
the same for both groups.PpIX fluorescence contrast between control and DFO
treatment groups was subsequently measured and a statisti-
cally significant difference in the mean PpIX fluorescencecontrast was determined (t-test associated P-value = 0.0020).These results showed a 50% increase in PpIX fluorescence
contrast as a result of iron chelation therapy. In addition, asevidenced by the lack of a statistically significant difference inthe mean coefficient of variation in PpIX fluorescence, theincrease in fluorescence cannot be attributed to a more
homogeneous production, but appears to be an overallincrease throughout the tumor.
It was anticipated that the iron chelator, DFO, would
temporarily sequester available iron stores away from tumorcells, thus decreasing the ability of ferrochelatase to reducePpIX levels (45). The exact mechanisms causing the increased
PpIX fluorescence after iron chelation therapy were notinvestigated, but have been well studied in the past. Thisproof of concept study sought to establish whether a
significant increase in PpIX fluorescence of a malignantglioma model occurs with iron chelation therapy, and ifclinical use is warranted. An optimal DFO dose to achievemaximal increase in PpIX fluorescence without significant
drug side effects was not determined, but will likely bedetermined by human clinical factors rather than mousetolerance levels. Relevant clinical factors affecting selection of
optimal DFO dose for enhancing PpIX fluorescence mightinclude but not be limited to: adverse drug reactions (i.e.local skin reactions, organ toxicity), drug counter indications
(i.e. concomitant high dose vitamin C and DFO treatment,pregnancy), therapeutic benefit-to-cost ratio, and drug toler-ance (35,39).
In summary, exogenous administration of d-ALA induces
selective accumulation of PpIX in brain tumor compared withnormal brain tissue. Studies using the d-ALA-PpIX system forFGR provide exciting results about increases in extent of
tumor resection in malignant gliomas. Nevertheless, tumormargins are known to not display detectable levels offluorescence using commercial surgical microscope systems.
This study used iron chelation treatment in an animal model ofmalignant glioma, and found a 50% significant increase inPpIX fluorescence contrast. Future studies will seek to find the
optimal DFO dose to achieve a maximal increase in PpIXfluorescence. Further work will also test if iron chelation
Table 1. Mean PpIX fluorescence coefficient of variation and GFPand PpIX fluorescence contrast.
Mean95% CI ofthe mean
PpIX coefficient of variationControl group 7.4 · 10)2 5.1 · 10)2–9.7 · 10)2
DFO group 6.3 · 10)2 4.1 · 10)2–8.4 · 10)2
GFP fluorescence contrastControl group 7.6 6.1–9.1DFO group 6.9 6.0–7.8
PpIX fluorescence contrast*Control group 1.9 1.6–2.3DFO group 2.9 2.9–3.4
*Statistically significant, P-value = 0.0020.
Figure 2. Chelation treatment effects are shownwith a box and whiskerdiagram of PpIX fluorescence contrast in tumor tissue for both controland DFO treatment groups. Unpaired Student’s t-test associatedP-value = 0.0020. Box and whisker diagram represents mean ((n)square); ±1 SD top and bottom of each box, respectively; maximumand minimum-vertical bars extending from each box; n = 30.
Photochemistry and Photobiology, 2010, 86 473
therapy significantly increases PpIX fluorescence in cases ofgliomas without an impaired blood–brain barrier.
Acknowledgements—The authors are grateful to Dr. Summer Gibbs-Strauss for useful discussions in the planning of this work. The studywas supported by the National Institutes of Health grantsR01NS052274 and RO1CA120368.
REFERENCES
1. Wen, P. Y. and S. Kesari (2008) Malignant gliomas in adults.N. Engl. J. Med. 359, 492–507.
2. Stummer, W., U. Pichlmeier, T. Meinel, O. D. Wiestler, F.Zanella, H. J. Reulen and ALA-Glioma Study Group (2006)Fluorescence-guided surgery with 5-aminolevulinic acid forresection of malignant glioma: A randomised controlled multi-centre phase III trial.[see comment]. Lancet Oncol.. 7, 392–401.
3. Stummer, W., H. J. Reulen, T. Meinel, U. Pichlmeier, W. Schum-acher, J. C. Tonn, V. Rohde, F. Oppel, B. Turowski, C. Woicie-chowsky, K. Franz and T. Pietsch (2008) Extent of resection andsurvival in glioblastoma multiforme: Identification of and adjust-ment for bias. Neurosurgery 62, 564–576; discussion 564–576.
4. Lacroix, M., D. Abi-Said, D. R. Fourney, Z. L. Gokaslan, W. Shi,F. DeMonte, F. F. Lang, I. E. McCutcheon, S. J. Hassenbusch, E.Holland, K. Hess, C. Michael, D. Miller and R. Sawaya (2001) Amultivariate analysis of 416 patients with glioblastoma multi-forme: Prognosis, extent of resection, and survival. J. Neurosurg.95, 190–198.
5. Vecht, C. J., C. J. Avezaat, W. L. van Putten, W. M. Eijkenboomand S. Z. Stefanko (1990) The influence of the extent of surgery onthe neurological function and survival in malignant glioma.A retrospective analysis in 243 patients. J. Neurol. Neurosurg.Psychiatry 53, 466–471.
6. Hill, D. L., C. R. Maurer Jr, R. J. Maciunas, J. A. Barwise, J. M.Fitzpatrick and M. Y. Wang (1998) Measurement of intraopera-tive brain surface deformation under a craniotomy. Neurosurgery43, 514–526; discussion 527–528.
7. Lunn, K. E., K. D. Paulsen, F. Liu, F. E. Kennedy, A. Hartov andD. W. Roberts (2006) Data-guided brain deformation modeling:Evaluation of a 3-D adjoint inversion method in porcine studies.IEEE Trans. Biomed. Eng. 53, 1893–1900.
8. Ji, S., D. W. Roberts, A. Hartov and K. D. Paulsen (2009) Brain-skull contact boundary conditions in an inverse computationaldeformation model. Med Image Anal. 13, 659–672.
9. Pichlmeier, U., A. Bink, G. Schackert and W. Stummer (2008)Resection and survival in glioblastoma multiforme: An RTOGrecursive partitioning analysis of ALA study patients. Neuroon-cology 10, 1025–1034.
10. Stummer, W., A. Novotny, H. Stepp, C. Goetz, K. Bise and H. J.Reulen (2000) Fluorescence-guided resection of glioblastomamultiforme by using 5-aminolevulinic acid-induced porphyrins: Aprospective study in 52 consecutive patients. J. Neurosurg. 93,1003–1013.
11. Stummer, W., U. Pichlmeier, T. Meinel, O. D. Wiestler, F. Zanellaand H. J. Reulen (2006) Fluorescence-guided surgery with5-aminolevulinic acid for resection of malignant glioma: Arandomised controlled multicentre phase III trial. Lancet Oncol. 7,392–401.
12. Stummer, W., H. J. Reulen, A. Novotny, H. Stepp and J. C. Tonn(2003) Fluorescence-guided resections of malignant gliomas—an overview. Acta Neurochir. Suppl. 88, 9–12.
13. Utsuki, S., N.Miyoshi, H. Oka, Y.Miyajima, S. Shimizu, S. Suzukiand K. Fujii (2007) Fluorescence-guided resection of metastaticbrain tumors using a 5-aminolevulinic acid-induced protoporphyrinIX: Pathological study. Brain Tumor Pathol. 24, 53–55.
14. Utsuki, S., H. Oka, S. Sato, S. Shimizu, S. Suzuki, Y. Tanizaki, K.Kondo, Y. Miyajima and K. Fujii (2007) Histological examinationof false positive tissue resection using 5-aminolevulinic acid-induced fluorescence guidance. Neurol Med Chir (Tokyo) 47,210–213. discussion 213–214.
15. Utsuki, S., H. Oka, S. Sato, S. Suzuki, S. Shimizu, S. Tanaka andK. Fujii (2006) Possibility of using laser spectroscopy for the
intraoperative detection of nonfluorescing brain tumors and theboundaries of brain tumor infiltrates. Technical note. J. Neuro-surg. 104, 618–620.
16. Sinha, A. K., S. Anand, B. J. Ortel, Y. Chang, Z. Mai, T. Hasanand E. V. Maytin (2006) Methotrexate used in combination withaminolaevulinic acid for photodynamic killing of prostate cancercells. Br. J. Cancer 95, 485–495.
17. Sato, N., B. W. Moore, S. Keevey, J. A. Drazba, T. Hasan and E.V. Maytin (2007) Vitamin D enhances ALA-induced protopor-phyrin IX production and photodynamic cell death in 3-Dorganotypic cultures of keratinocytes. J. Invest. Dermatol. 127,925–934.
18. Ortel, B., D. Sharlin, D. O’Donnell, A. K. Sinha, E. V. Maytinand T. Hasan (2002) Differentiation enhances aminolevulinic acid-dependent photodynamic treatment of LNCaP prostate cancercells. Br. J. Cancer 87, 1321–1327.
19. Ortel, B., N. Chen, J. Brissette, G. P. Dotto, E. Maytin and T.Hasan (1998) Differentiation-specific increase in ALA-inducedprotoporphyrin IX accumulation in primary mouse keratinocytes.Br. J. Cancer 77, 1744–1751.
20. Berg, K., H. Anholt, O. Bech and J. Moan (1996) The influenceof iron chelators on the accumulation of protoporphyrin IXin 5-aminolaevulinic acid-treated cells. Br. J. Cancer 74, 688–697.
21. Curnow, A. and A. Pye (2007) Biochemical manipulation via ironchelation to enhance porphyrin production from porphyrin pre-cursors. J. Environ. Pathol. Toxicol. Oncol. 26, 89–103.
22. Chang, S. C., A. J. MacRobert, J. B. Porter and S. G. Bown (1997)The efficacy of an iron chelator (CP94) in increasing cellularprotoporphyrin IX following intravesical 5-aminolaevulinic acidadministration: An in vivo study. J. Photochem. Photobiol. B 38,114–122.
23. Collaud, S., A. Juzeniene, J. Moan and N. Lange (2004) On theselectivity of 5-aminolevulinic acid-induced protoporphyrin IXformation. Current Medicinal Chemistry Anti Cancer Agents. 4,301–316.
24. Friesen, S. A., G. O. Hjortland, S. J. Madsen, H. Hirschberg, O.Engebraten, J. M. Nesland and Q. Peng (2002) 5-Aminolevulinicacid-based photodynamic detection and therapy of brain tumors(review). Int. J. Oncol. 21, 577–582.
25. Stummer, W., H. Stepp, G. Moller, A. Ehrhardt, M. Leonhardand H. J. Reulen (1998) Technical principles for protoporphyrin-IX-fluorescence guided microsurgical resection of malignantglioma tissue. Acta Neurochir (Wien). 140, 995–1000.
26. Stummer, W., S. Stocker, S. Wagner, H. Stepp, C. Fritsch, C.Goetz, A. E. Goetz, R. Kiefmann and H. J. Reulen (1998)Intraoperative detection of malignant gliomas by 5-aminolevulinicacid-induced porphyrin fluorescence. Neurosurgery 42, 518–525;discussion 525–526.
27. Hefti, M., G. von Campe, M. Moschopulos, A. Siegner, H. Looserand H. Landolt (2008) 5-aminolevulinic acid inducedprotoporphyrin IX fluorescence in high-grade glioma surgery: Aone-year experience at a single institutuion. Swiss Med. Wkly. 138,180–185.
28. Toms, S. A., W. C. Lin, R. J. Weil, M. D. Johnson, E. D. Jansenand A. Mahadevan-Jansen (2005) Intraoperative opticalspectroscopy identifies infiltrating glioma margins with highsensitivity. Neurosurgery 57, 382–391; discussion 382–391.
29. Gibbs, S. L., B. Chen, J. A. O’Hara, P. J. Hoopes, T. Hasan andB. W. Pogue (2006) Protoporphyrin IX level correlates withnumber of mitochondria, but increase in production correlateswith tumor cell size. Photochem. Photobiol. 82, 1334–1341.
30. Bech, O., D. Phillips, J. Moan and A. J. MacRobert (1997)A hydroxypyridinone (CP94) enhances protoporphyrin IX for-mation in 5-aminolaevulinic acid treated cells. J. Photochem.Photobiol. B 41, 136–144.
31. Choudry, K., R. C. Brooke, W. Farrar and L. E. Rhodes (2003)The effect of an iron chelating agent on protoporphyrin IX levelsand phototoxicity in topical 5-aminolaevulinic acid photodynamictherapy. Br. J. Dermatol. 149, 124–130.
32. Casas, A., A. M. Batlle, A. R. Butler, D. Robertson, E. H. Brown,A. MacRobert and P. A. Riley (1999) Comparative effect of ALAderivatives on protoporphyrin IX production in human and ratskin organ cultures. Br. J. Cancer 80, 1525–1532.
474 Pablo A. Valdes et al.

33. Ohgari, Y., Y. Nakayasu, S. Kitajima, M. Sawamoto, H. Mori, O.Shimokawa, H. Matsui and S. Taketani (2005) Mechanismsinvolved in delta-aminolevulinic acid (ALA)-induced photosensi-tivity of tumor cells: Relation of ferrochelatase and uptake ofALA to the accumulation of protoporphyrin. Biochem. Pharma-col. 71, 42–49.
34. Bernhardt, P. V. (2007) Coordination chemistry and biology ofchelators for the treatment of iron overload disorders. DaltonTrans. 30, 3214–3220.
35. Bring, P., N. Partovi, J. A. Ford and E. M. Yoshida (2008) Ironoverload disorders: Treatment options for patients refractory to orintolerant of phlebotomy. Pharmacotherapy 28, 331–342.
36. Maggio, A. (2007) Light and shadows in the iron chelation treat-ment of haematological diseases. Br. J. Haematol. 138, 407–421.
37. Hershko, C., A. Abrahamov, A. M. Konijn, W. Breuer, I. Z.Cabantchik, P. Pootrakul and G. Link (2003) Objectives andmethods of iron chelation therapy. Bioinorg. Chem. Appl. 1, 151–168.
38. Aldridge, M. D. (2007) Acute iron poisoning: What every pedi-atric intensive care unit nurse should know. Dimens Crit CareNurs. 26, 43–48. quiz 49–50.
39. Clinical Pharmacology [database online] (2009). Available at:http://cponline.hitchcock.org/. Accessed on 18 September 2009.
40. Albert, F. K., M. Forsting, K. Sartor, H. P. Adams and S. Kunze(1994) Early postoperative magnetic resonance imaging afterresection of malignant glioma: Objective evaluation of residualtumor and its influence on regrowth and prognosis. Neurosurgery34, 45–60; discussion 60–61.
41. Barker, F. G. II, M. D. Prados, S. M. Chang, P. H. Gutin, K. R.Lamborn, D. A. Larson, M. K. Malec, M. W. McDermott, P. K.Sneed, W. M. Wara and C. B. Wilson (1996) Radiation responseand survival time in patients with glioblastoma multiforme.J. Neurosurg. 84, 442–448.
42. Kremer, P., F. Mahmoudreza, R. Ding, M. Pritsch, S. Zoubaaand E. Frei (2009) Intraoperative fluorescence staining of malig-nant brain tumors using 5-aminofluorescein-labeled albumin.Neurosurgery 64, 53–60; discussion 60–61.
43. Shinoda, J., H. Yano, S. Yoshimura, A. Okumura, Y. Kaku,T. Iwama and N. Sakai (2003) Fluorescence-guided resection ofglioblastoma multiforme by using high-dose fluorescein sodium.Technical note. J. Neurosurg. 99, 597–603.
44. Cappellini, M. D. and P. Pattoneri (2009) Oral iron chelators.Annu. Rev. Med. 60, 25–38.
45. Iinuma, S., S. S. Farshi, B. Ortel and T. Hasan (1994) A mecha-nistic study of cellular photodestruction with 5-aminolaevulinicacid-induced porphyrin. Br. J. Cancer 70, 21–28.
Photochemistry and Photobiology, 2010, 86 475