dealing with difficult learners - uab learners- faculty... · labeling issue- once a difficult...
TRANSCRIPT
Dealing with Difficult Learners
Caroline Harada, MD Division of Gerontology, Geriatrics, and
Palliative Care
What is a “difficult learner?”
Cognitive vs. Non-cognitive issues
Labeling issue- once a difficult learner does not make a person forever difficult
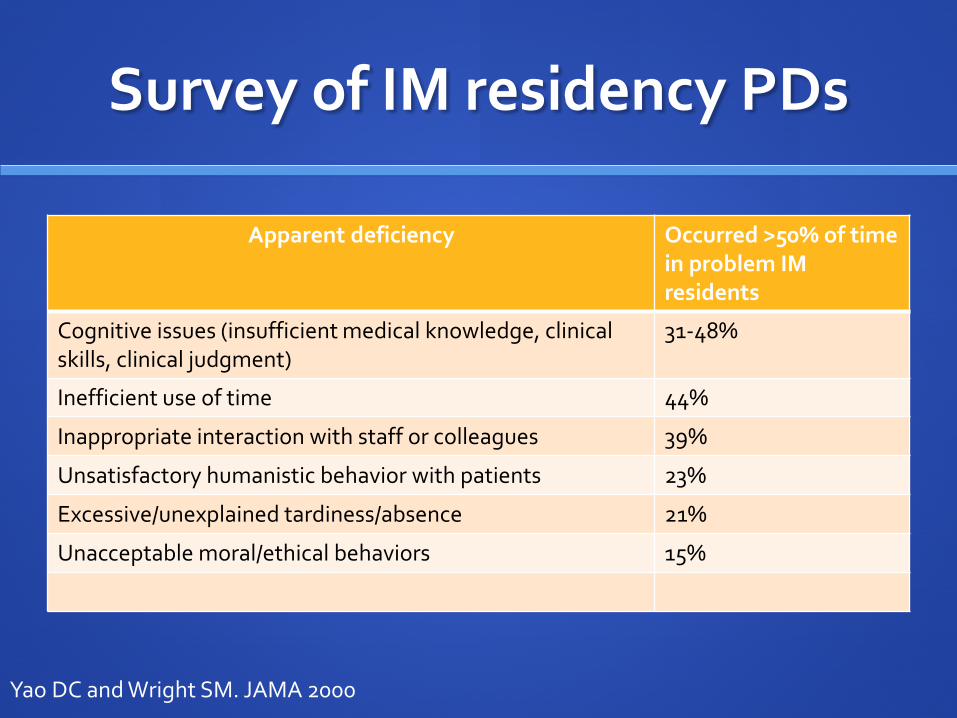
Survey of IM residency PDs
Apparent deficiency Occurred >50% of time in problem IM residents
Cognitive issues (insufficient medical knowledge, clinical skills, clinical judgment)
31-48%
Inefficient use of time 44%
Inappropriate interaction with staff or colleagues 39%
Unsatisfactory humanistic behavior with patients 23%
Excessive/unexplained tardiness/absence 21%
Unacceptable moral/ethical behaviors 15%
Yao DC and Wright SM. JAMA 2000
The plan
Description of problem
Approach: SOAP Differential diagnosis
3 Cases: Taylor Swift Tools to increase metacognition/insight
Starbucks Tools to increase motivation
Angry guy Tools for discussing concerns with the difficult learner
Why do we need to talk about this?
Learning to prevent this would save educators time and energy
Learner likely in need of help
Learner may go on to have difficulties in their professional life
Patients may get hurt
It’s not rare Up to 15% of medical students on an IM clerkship “struggling”
Frellsen SL et al. Acad Med. 2008
“Starbucks”
Trevor is an IM intern on a busy cardiology consult service. He often arrives late, frequently “disappears” during the day, when he reappears he’s always carrying a cup of coffee. He does not consistently return your pages.
His H &P’s and clinical reasoning seem fine for his level of training. Twice, he failed to write a progress note on a follow up patient after you asked him to do so.
“Angry Guy”
Jose is a PGY-2 resident in emergency medicine. He frequently gets in arguments with nurses and is openly hostile and disrespectful toward his attendings.
His knowledge and skills are on par with his peers, and his clinical judgment seems good. He seems to genuinely want to provide good care to his patients.
When confronted about his interpersonal communication and professionalism issues, he blames the nurses for being rude and disrespectful, and the attendings for being stupid and unreasonable.
“Taylor Swift”
Taylor is a third year medical student doing her pediatrics rotation. Her presentations are extremely long and focus on irrelevant details. She often misses key facts in the history and her physical exams are superficial. Her clinical reasoning is poor, she seems to get easily side-tracked by irrelevant details.
On her evaluation, you give her a pass (not high pass, not honors).
She comes to you when she receives the grade and is upset. She says she has never received lower than a high pass on the 4 rotations she has already completed. No one has ever told her there was a problem.
An Approach to Difficult Learners: SOAP
S- Name the problem, what do people say/think about it?
O- List the specific behaviors observed
A- Formulate a differential diagnosis
P- Partner with learner to Probe, Powwow, Plan
Adapted from Langlois JP, Thach S. Fam Med 2000
“A”: Differential Diagnosis
Cognitive Learning disability Poor fund of knowledge Poor procedural or clinical
reasoning skills Poor metacognitive skills
Mental health Depression, anxiety, other ADHD Personality disorders Autism spectrum disorders
Substance abuse Other medical problems Not handling stressors well Work-related stress External stressors
Behavioral/professionalism Mama didn’t teach him/her
right
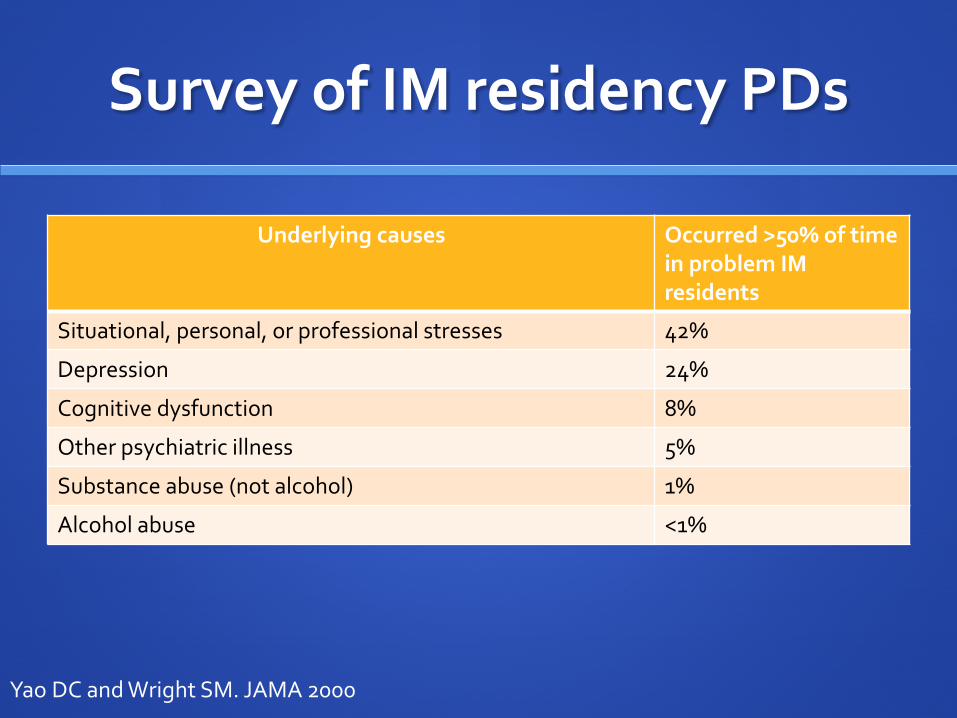
Survey of IM residency PDs
Underlying causes Occurred >50% of time in problem IM residents
Situational, personal, or professional stresses 42%
Depression 24%
Cognitive dysfunction 8%
Other psychiatric illness 5%
Substance abuse (not alcohol) 1%
Alcohol abuse <1%
Yao DC and Wright SM. JAMA 2000
“Taylor Swift”
Taylor is a third year medical student doing her pediatrics rotation. Her presentations are extremely long and focus on irrelevant details. She often misses key facts in the history and her physical exams are superficial. Her clinical reasoning is poor, she seems to get easily side-tracked by irrelevant details.
On her evaluation, you give her a pass (not high pass, not honors).
She comes to you when she receives the grade and is upset. She says she has never received lower than a high pass on the 4 rotations she has already completed. No one has ever told her there was a problem.
Apply SOAP
S- Describe Taylor Swift’s problem
O- list the specific behaviors
A- assessment
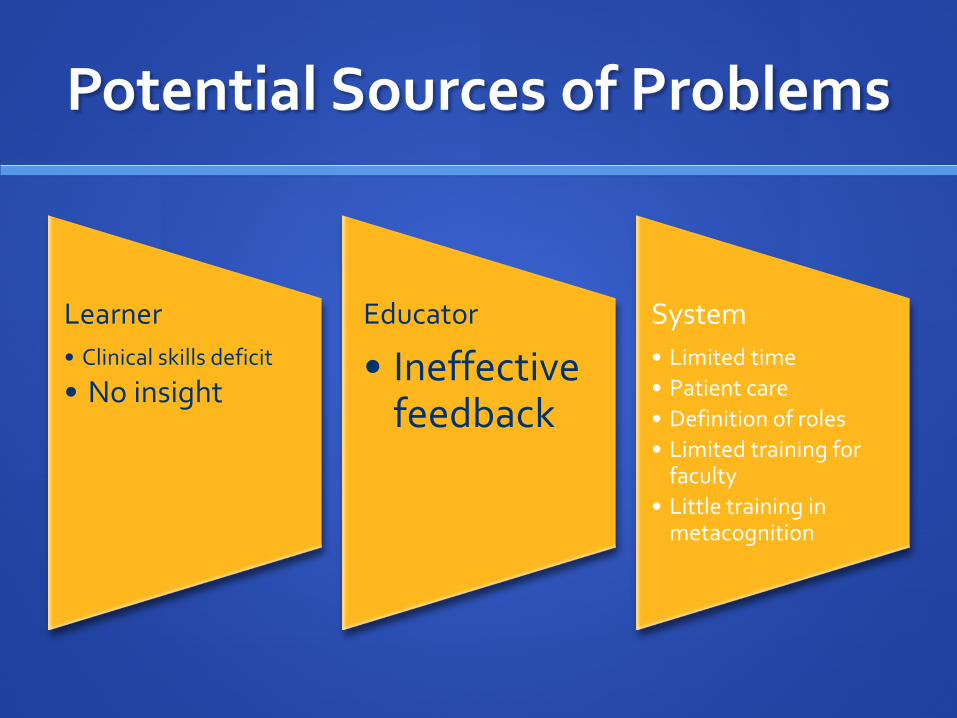
Potential Sources of Problems
Learner • Clinical skills deficit
•No insight
Educator
• Ineffective feedback
System • Limited time • Patient care • Definition of roles • Limited training for
faculty • Little training in
metacognition
How to improve insight?
Build metacognition
Metacognition
One’s knowledge concerning one's own
cognitive processes and products
“Thinking about thinking”
“Knowing about knowing”
How People Learn. National Research Council, 1999
Monitor Performance
Guided self-assessments Examples to help Taylor: Review of annotated H&P’s
Annotate own H&P (explain why you did/thought/wrote; how it could be better)
Watch video of herself performing a task, using a checklist, then compare to an video demonstration by an expert
Teach heuristics for self-correction (How to know if you’re off track?) Examples to help Taylor: How many items are reasonable in a differential diagnosis
Oral presentations no longer than 5 minutes Ambrose SA et al. How Learning Works, 2010
Reflect, Adjust as needed
Require reflection on performance What part of working up chest pain did you get better at? What part of working up chest pain to you want to
learn/practice now? How have your skills evolved over the last 3 rotations? How’s your current process for dealing with difficult learners
working for you?
Ambrose SA et al. How Learning Works, 2010
Potential Sources of Problems
Learner • Clinical skills deficit
• No insight
Educator
• Ineffective feedback
System • Limited time • Patient care • Definition of roles • Limited training for
faculty • Little training in
metacognition
Feedback Pearls
Same team! Common goal
Not a reflection of your personal worth
Invited feedback works better, should always be expected
Based on what YOU observed, descriptive, neutral, specific
Don’t interpret/assume intent of what you saw
Limit feedback to what’s fixable
Subjective data is ok if labeled as such
Ende, J JAMA 1983
Useful tools from Taylor
To enhance insight: Guided self assessments Heuristics for when self-correction is needed Require reflection on performance
Regular use of face-to-face feedback
“Starbucks”
Trevor is an IM intern on a busy cardiology consult service. He often arrives late, frequently “disappears” during the day, when he reappears he’s always carrying a cup of coffee. He does not consistently return your pages.
His H &P’s and clinical reasoning seem fine for his level of training. Twice, he failed to write a progress note on a follow up patient after you asked him to do so.
Apply SOAP
S- name the problem
O- list specific behaviors
A- assessment
Potential Sources of Problems
Learner • Mental health • Substance abuse • Learning disability • External stressor • Unmotivated • Unprofessional
Educator • Didn’t make
expectations clear • Didn’t provide
feedback
System • Fatigue • Isolation from
support network • High stakes work
What to do about motivation?
3 variables Environment: supportive or not? Learner self-efficacy: high or low? Learner values the work/goals set: yes or no?
Ambrose SA et al. How Learning Works, 2010
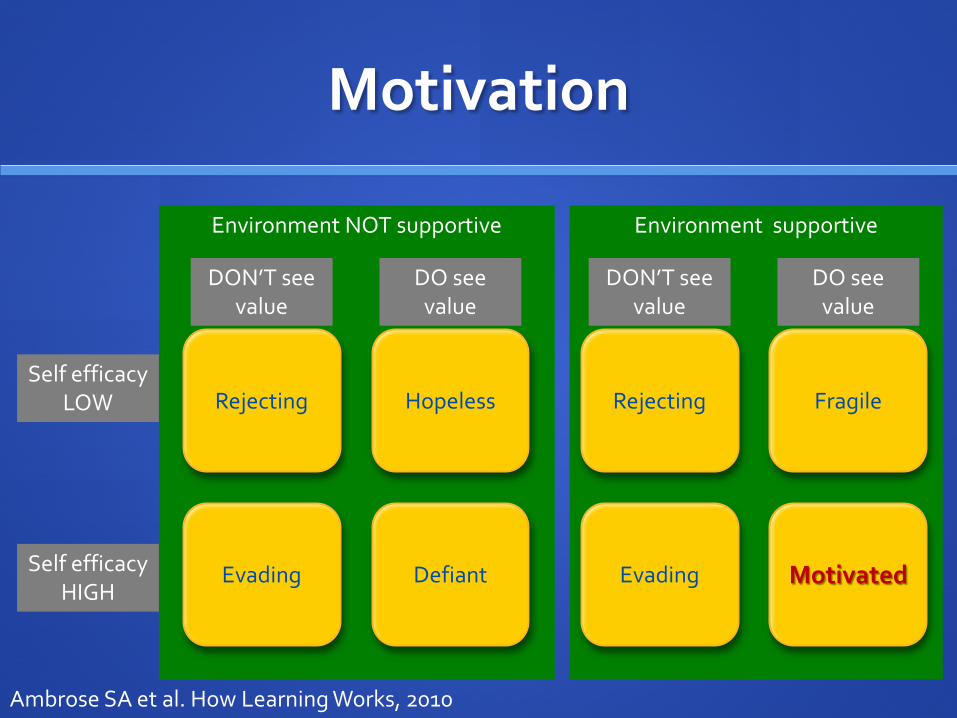
Environment supportive
Environment NOT supportive
Motivation
Rejecting
Evading Motivated
Fragile Rejecting
Evading Defiant
Hopeless Self efficacy
LOW
Self efficacy HIGH
DON’T see value
DO see value
DO see value
DON’T see value
Ambrose SA et al. How Learning Works, 2010
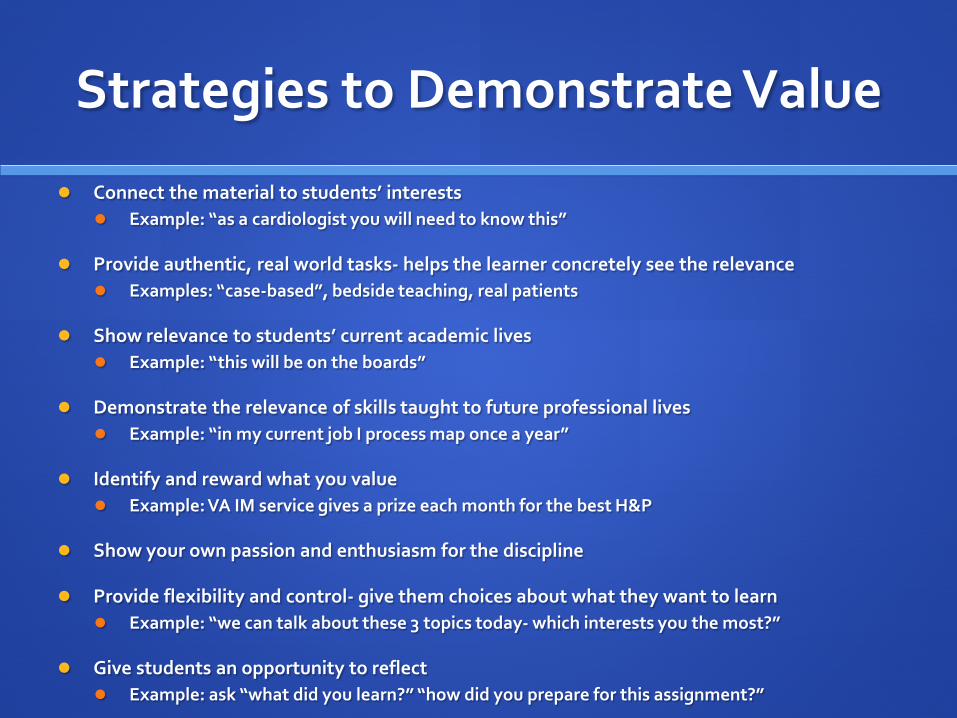
Strategies to Demonstrate Value
Connect the material to students’ interests Example: “as a cardiologist you will need to know this”
Provide authentic, real world tasks- helps the learner concretely see the relevance Examples: “case-based”, bedside teaching, real patients
Show relevance to students’ current academic lives Example: “this will be on the boards”
Demonstrate the relevance of skills taught to future professional lives Example: “in my current job I process map once a year”
Identify and reward what you value Example: VA IM service gives a prize each month for the best H&P
Show your own passion and enthusiasm for the discipline
Provide flexibility and control- give them choices about what they want to learn Example: “we can talk about these 3 topics today- which interests you the most?”
Give students an opportunity to reflect Example: ask “what did you learn?” “how did you prepare for this assignment?”
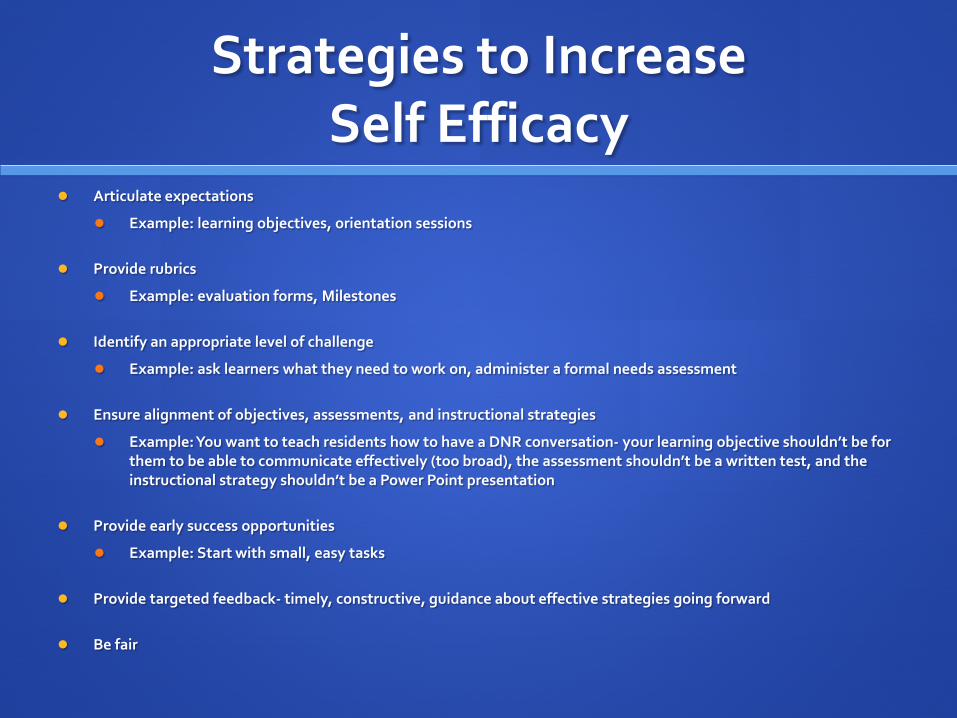
Strategies to Increase Self Efficacy
Articulate expectations
Example: learning objectives, orientation sessions
Provide rubrics
Example: evaluation forms, Milestones
Identify an appropriate level of challenge
Example: ask learners what they need to work on, administer a formal needs assessment
Ensure alignment of objectives, assessments, and instructional strategies
Example: You want to teach residents how to have a DNR conversation- your learning objective shouldn’t be for them to be able to communicate effectively (too broad), the assessment shouldn’t be a written test, and the instructional strategy shouldn’t be a Power Point presentation
Provide early success opportunities
Example: Start with small, easy tasks
Provide targeted feedback- timely, constructive, guidance about effective strategies going forward
Be fair
Educate students about the ways we make attributions about success and failure
Provide flexibility and control- give them choices about what they want to learn Example: “we can talk about these 3 topics today- which
interests you the most?”
Give students an opportunity to reflect Example: ask “what did you learn?” “how did you prepare for
this assignment?”
Useful tools from Starbucks
To enhance motivation: Demonstrate the value of the task (if needed) Build learner self efficacy (if needed) Maintain a supportive environment
“Angry Guy”
Jose is a PGY-2 resident in emergency medicine. He frequently gets in arguments with nurses and is openly hostile and disrespectful toward his attendings.
His knowledge and skills are on par with his peers, and his clinical judgment seems good. He seems to genuinely want to provide good care to his patients.
When confronted about this, he blames the nurses for being rude and disrespectful, and the attendings for being stupid and unreasonable.
Apply SOAP
S- name the problem
O- list specific behaviors
A- assessment
Potential Sources of Problems
Learner • Mental health • Substance abuse • External stressor • Unprofessional
Educator
System • Patient volume • Fatigue • Isolation from
support network • High stakes work
An Approach to Difficult Learners: SOAP
S- Name the problem, what do people say/think about it?
O- List the specific behaviors observed
A- Formulate a differential diagnosis
P- Partner with learner to Probe, Powwow, Plan SPIKES
Langlois JP, Thach S. Fam Med 2000
“P”-Partner with Learner
Probe to figure out the “why” that underlies the problem
Powwow- talk it through
Plan- what next?
How to Initiate this Conversation?
SPIKES protocol Setting: do all necessary background research, set up a good
time/place Probing: “how do you think it’s going?” Invitation: “would you like some feedback?” Knowledge: tell them what’s not working, explain potential
consequences of current trajectory. Let learner respond. Discuss. Emotion: learner may display some emotion, you display empathy Strategize/summarize: Create a plan together Set clear, specific, and doable tasks/goals with timetable Plan for what happens if goals not met
Baile WF et al. The Oncologist, 2000
Remediation Plan
Involve necessary experts when appropriate Clerkship/Program director, Chief residents, GME office, etc.
Provide appropriate treatment Addiction specialists Mental health specialists
Provide instruction with deliberate practice, feedback, reflection. Tutors for clinical knowledge/skills Tutors for interpersonal communication & professionalism
Reassessment and certification of competence
Document entire process in detail Ronan-Bentle SE et al. Int J Emerg Med, 2011
Metacognitive Summary
Description of problem
Approach: SOAP Differential diagnosis
3 Cases: Poor insight (Taylor Swift) Metacognition strategies to improve insight
Unmotivated (Starbucks) Motivation strategies
Angry (Angry guy) Probe, Powwow, Plan using SPIKES protocol
Toolbox for Dealing with Difficult Learners
To enhance insight: Guided self assessments Heuristics for when self-correction is needed Require reflection on performance Regular use of face-to-face feedback
To enhance motivation: Demonstrate the value of the task (if needed) Build learner self efficacy (if needed) Maintain a supportive environment
To approach a difficult learner issue: SOAP protocol
Subjective- get the full story Objective- document specific behaviors Assessment- come up with a differential diagnosis Partner with learner to probe, pow wow, and plan using SPIKES
To address concerns with the learner SPIKES protocol
Setting Probe Invitation Knowledge Empathy/emotion Strategize, summarize
Toolbox for Dealing with Difficult Learners
References
Baile, WF et al. SPIKES: A six-step protocol for delivering bad news. The Oncologist. 2000; 5:302-311.
Frellsen SL Medical school policies regarding struggling medical students during the internal medicine clerkships: results of a national survey. Academic Medicine. 2008;83(9):876-81.
Hauer KE et al. Remediation of the deficiencies of physicians across the continuum from medical school to practive: a thematic review of the literature. Academic Medicine. 2009; 84(12): 1822-32.
Hicks PJ et al. To the point: Medical education reviews- dealing with student difficulties in the clinical setting. Am J Obs Gynecol. 2005; 193:1915-22.
Langlois JP and Thach S. Managing the difficult learning situation. Fam Med. 2000; 32(5):307-9.
Langlois JP and Thach S. Preventing the difficult learning situation. Fam Med. 2000; 32(4):232-4.
Ronan-Bentle SE et al. Dealing with the difficult student in emergency medicine. Int J Emerg Med, 2011; 4:39.45.
Yao DC and Wright SM. National survey of internal medicine residency program directors regarding problem residents. JAMA. 2000; 284:1099-1104.