daniels - disaster preparedness for obstetric patients ...€¦ · disaster preparedness for ob...
TRANSCRIPT
1/15/2016
1
Disaster Preparedness for OB Units
Where babies come from
Kay Daniels, MDClinical ProfessorObstetrics and GynecologyStanford UniversitySchool of Medicine
Keeping mom and baby together…• In the days after Hurricane Katrina struck Louisiana, 125
critically ill newborn babies and 154 pregnant women were evacuated to Woman's Hospital in Baton Rouge
• It was at least 10 days before some of the infants and mothers were reunited
•
• Washington Post 2006
1/15/2016
2
If there is an OB Unit in your hospital..
The American College of Obstetricians and Gynecologists note:
“Providers of obstetric care and facilities that provide maternity services, offer services to a population that has many unique features warranting additional consideration”
Disaster Planning

1/15/2016
3
Northridge earthquake 1994
Earthquakes: Where art thou?• Alaska registers the most earthquakes in a given year
• California was second until 2014
• Oklahoma is now #2 with 585 quakes to California's 200• Of lower magnitude
• Earthquakes occur in other areas of the USA • ARIZONA (last night)• Missouri • South Carolina• Colorado• Montana• Virginia/Washington DC
http://earthquake.usgs.gov/
1/15/2016
4
The hospital as the “patient”Joplin Regional Medical Center, Joplin, MO 2011
Why Moms and their Babies are at Risk in Disasters?
• >97% of all births in the US occur in a hospital or clinical setting…which may not be accessible or may be severely damaged during a disaster event
• Mom and babies are physically more vulnerable to disaster-related toxins
1/15/2016
5
Why Moms and their Babies are at Risk in Disasters?
• Pregnant women are subject to the usual risks of injury at a disaster, but with more complicated care
Hospital disaster planning : OB is Unique
One size ≠ all in a disaster setting for OB
Within the same footprint of any OB unit there exists a large variety of patient acuity and needs
• Healthy postpartum patients with their newborns
• Laboring women
• Intra op and post operative patients
1/15/2016
6
Why is OB unique?
We always have 2 patients
• Ante partum = mom and fetus
• Postpartum = mom and newborn
We all need a plan…..
“In preparing for battle I have always found that plans are useless, but planning is indispensable”
~ Dwight D. Eisenhower

1/15/2016
7
Disaster Planning for OB: A Triage Algorithm
OB TRAIN* =
Triage by Resource Allocation for IN patient
*Based on the triage system created by Dr. Ron Cohen for the NICU at Lucile Packard Children’s Hospital
TRAIN
TRAIN '15 Mar R. S. Cohen, MD 14
1/15/2016
8
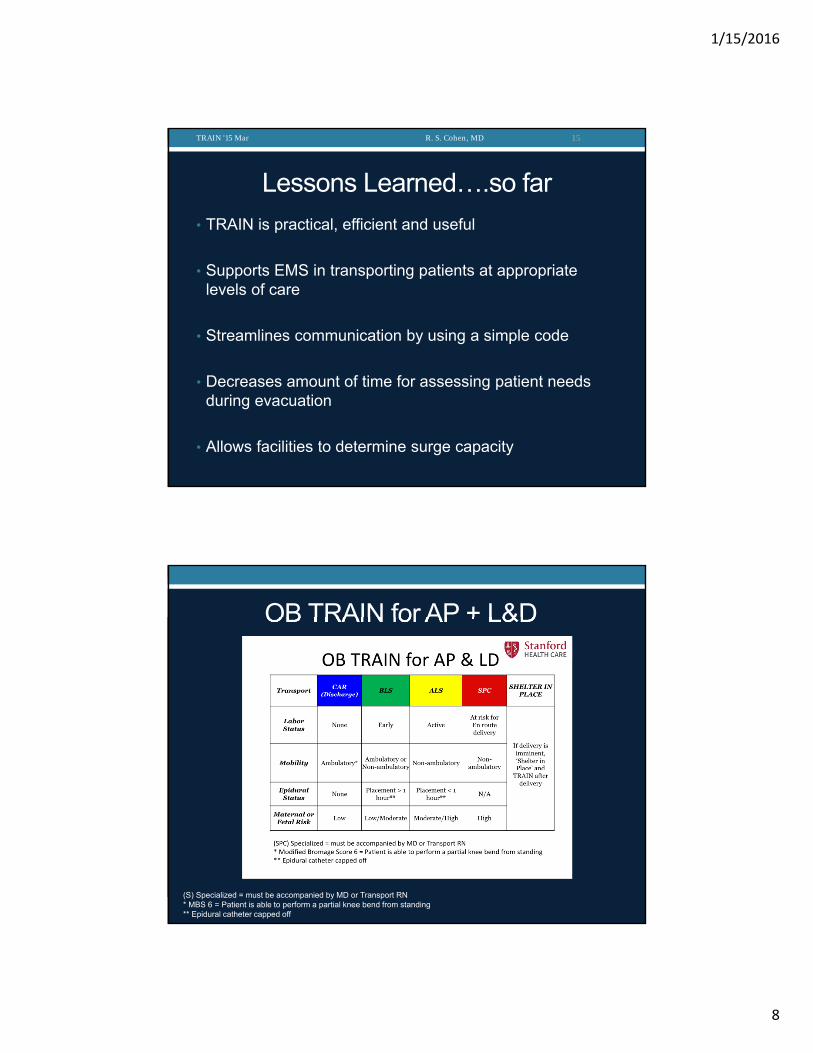
Lessons Learned….so far
TRAIN '15 Mar R. S. Cohen, MD 15
• TRAIN is practical, efficient and useful
• Supports EMS in transporting patients at appropriate levels of care
• Streamlines communication by using a simple code
• Decreases amount of time for assessing patient needs during evacuation
• Allows facilities to determine surge capacity
OB TRAIN for AP + L&D
(S) Specialized = must be accompanied by MD or Transport RN* MBS 6 = Patient is able to perform a partial knee bend from standing** Epidural catheter capped off
1/15/2016
9
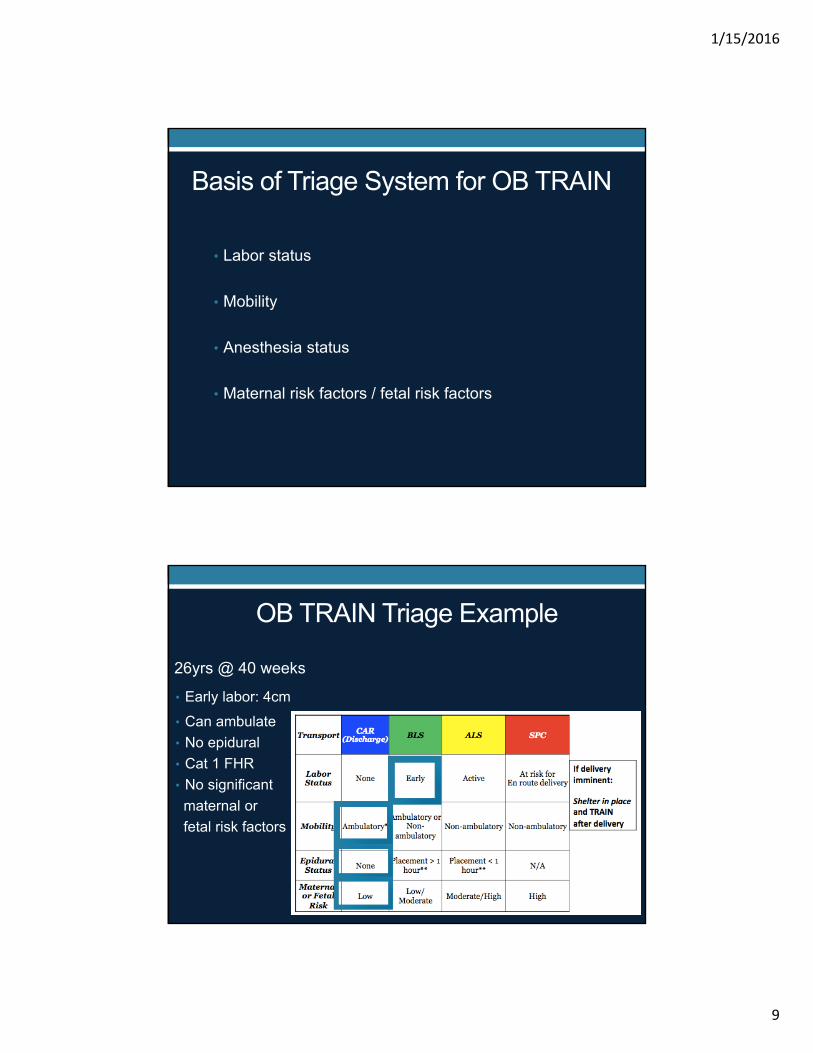
Basis of Triage System for OB TRAIN
• Labor status
• Mobility
• Anesthesia status
• Maternal risk factors / fetal risk factors
OB TRAIN Triage Example
26yrs @ 40 weeks
• Early labor: 4cm
• Can ambulate
• No epidural
• Cat 1 FHR
• No significant
maternal or
fetal risk factors
1/15/2016
10
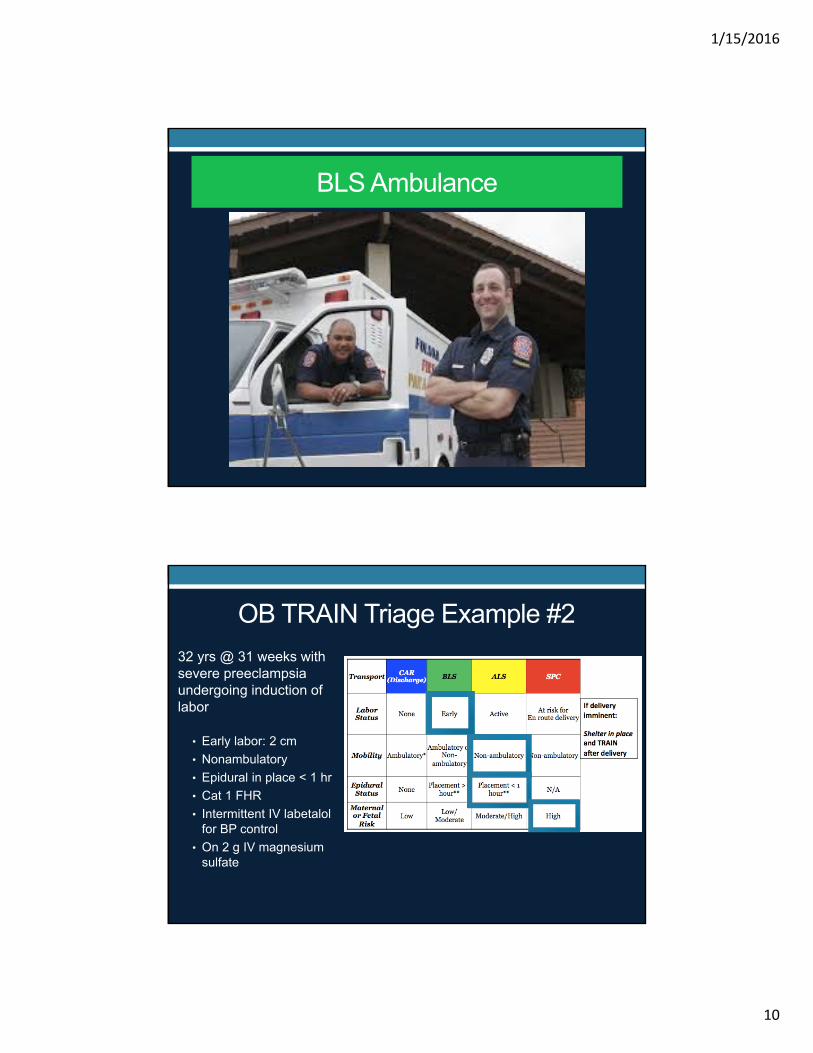
BLS Ambulance
OB TRAIN Triage Example #2
32 yrs @ 31 weeks with severe preeclampsia undergoing induction of labor
• Early labor: 2 cm
• Nonambulatory
• Epidural in place < 1 hr
• Cat 1 FHR
• Intermittent IV labetalol for BP control
• On 2 g IV magnesium sulfate
1/15/2016
11
Specialized
Levels of Maternity CareACOG Consensus Feb 2015
SENDING THE RIGHT PATIENT TO THERIGHT HOSPTIAL
1. Levels• Birthing Centers• Basic Care (Level l)• Specialty Care (Level ll)• Subspecialty Care (Level lll)• Regional Perinatal Health Care Centers (Level lV)
2. Capabilities
3. Types of providers
1/15/2016
12
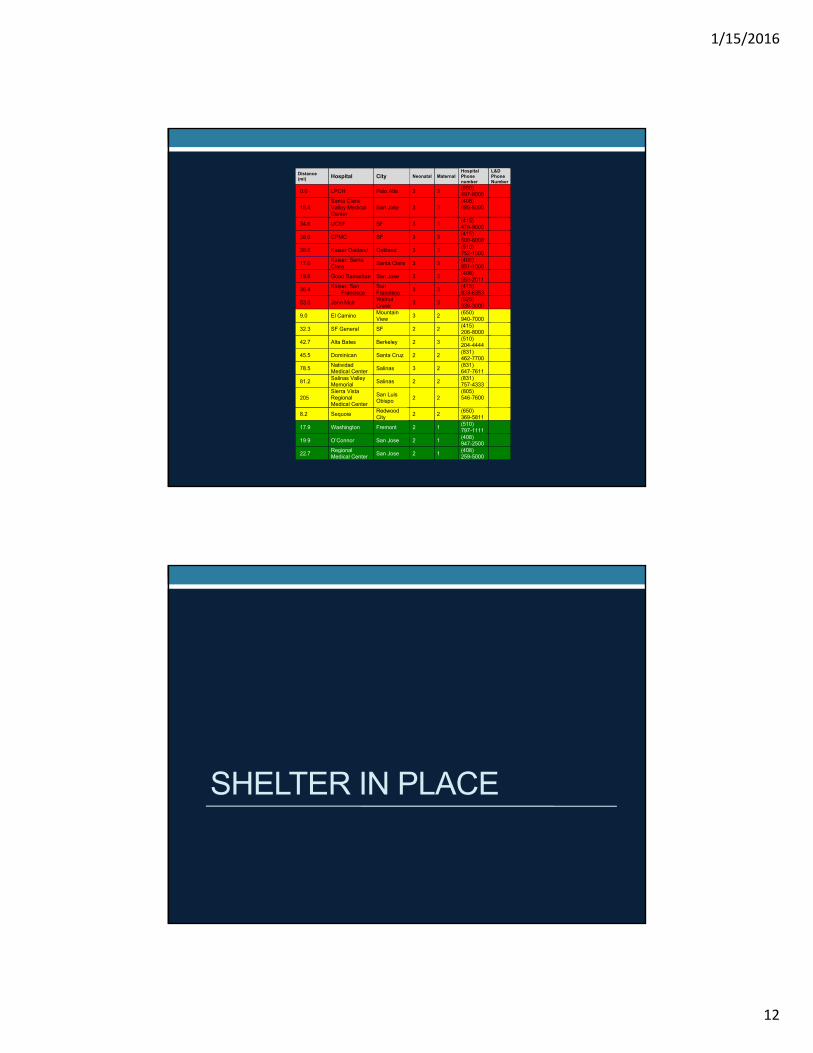
Distance (mi) Hospital City Neonatal Maternal
Hospital Phone number
L&D Phone Number
0.0 LPCH Palo Alto 3 3 (650) 497-8000
18.4 Santa Clara Valley Medical Center
San Jose 3 3 (408) 885-5000
34.6 UCSF SF 3 3 (415) 476-9000
36.0 CPMC SF 3 3 (415) 600-6000
38.6 Kaiser Oakland Oakland 3 3 (510) 752-1000
17.0 Kaiser: Santa Clara
Santa Clara 3 3 (408) 851-1000
19.8 Good Samaritan San Jose 3 3 (408) 559-2011
36.4 Kaiser: San
Francisco San Francisco
3 3 (415) 833-6353
53.0 John Muir Walnut Creek
3 3 (925) 939-3000
9.0 El Camino Mountain View
3 2 (650) 940-7000
32.3 SF General SF 2 2 (415) 206-8000
42.7 Alta Bates Berkeley 2 3 (510) 204-4444
45.5 Dominican Santa Cruz 2 2 (831) 462-7700
78.5 Natividad Medical Center Salinas 3 2
(831) 647-7611
81.2 Salinas Valley Memorial
Salinas 2 2 (831) 757-4333
205 Sierra Vista Regional Medical Center
San Luis Obispo 2 2
(805) 546-7600
8.2 Sequoia Redwood City
2 2 (650) 369-5811
17.9 Washington Fremont 2 1 (510) 797-1111
19.9 O’Connor San Jose 2 1 (408) 947-2500
22.7 Regional Medical Center San Jose 2 1
(408) 259-5000
SHELTER IN PLACE
1/15/2016
13
Being prepared to evacuate L&D
WE’VE GOT TO GO!!
1/15/2016
14
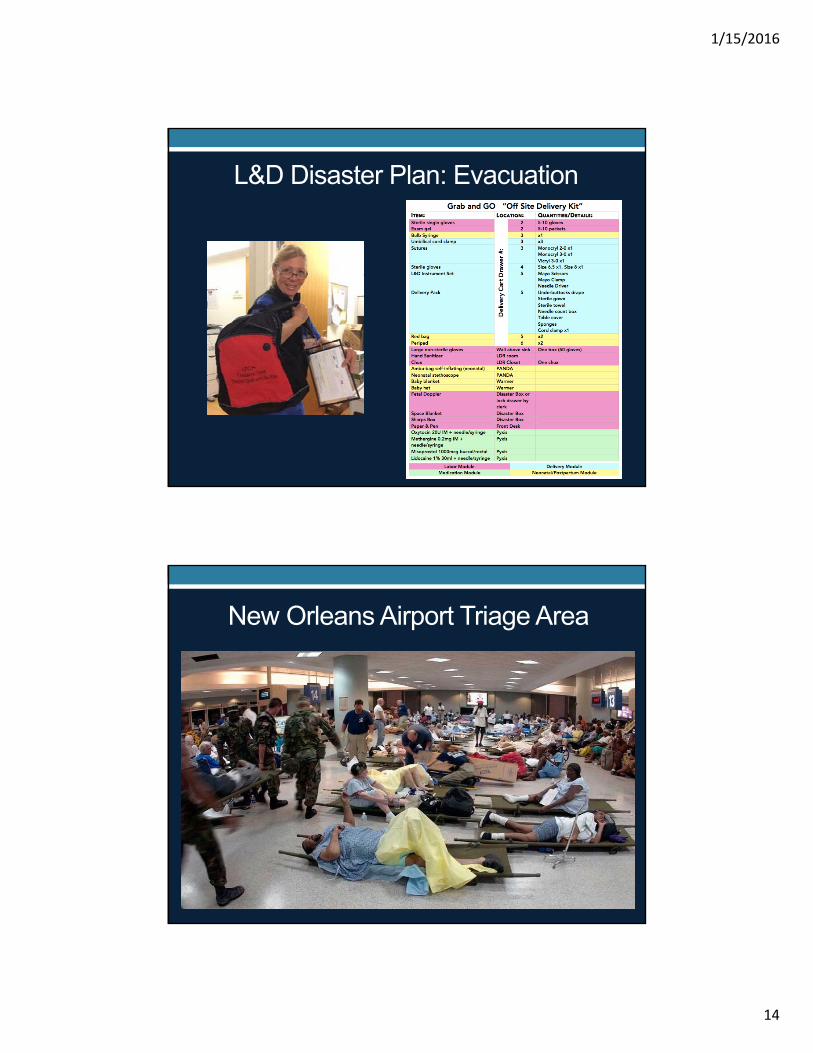
L&D Disaster Plan: Evacuation
New Orleans Airport Triage Area
1/15/2016
15
COMMUNICATION: Peds OB
How will peds know where OB is evacuating to?
• Is there a system in place for notification?
Who from peds has been designated to go with OB ?
• To care for ‘shelter in place’ in deliveries
Pediatric planning to assist OB units
Who is bringing neonatal equipment?
What is in your grab and go bag?
• Bulb syringe
• Self inflating bag
• Hard surface
• O2 and air tanks if possible
• Intubation equipment
• Other?
1/15/2016
16
POSTPARTUM EVACUATION
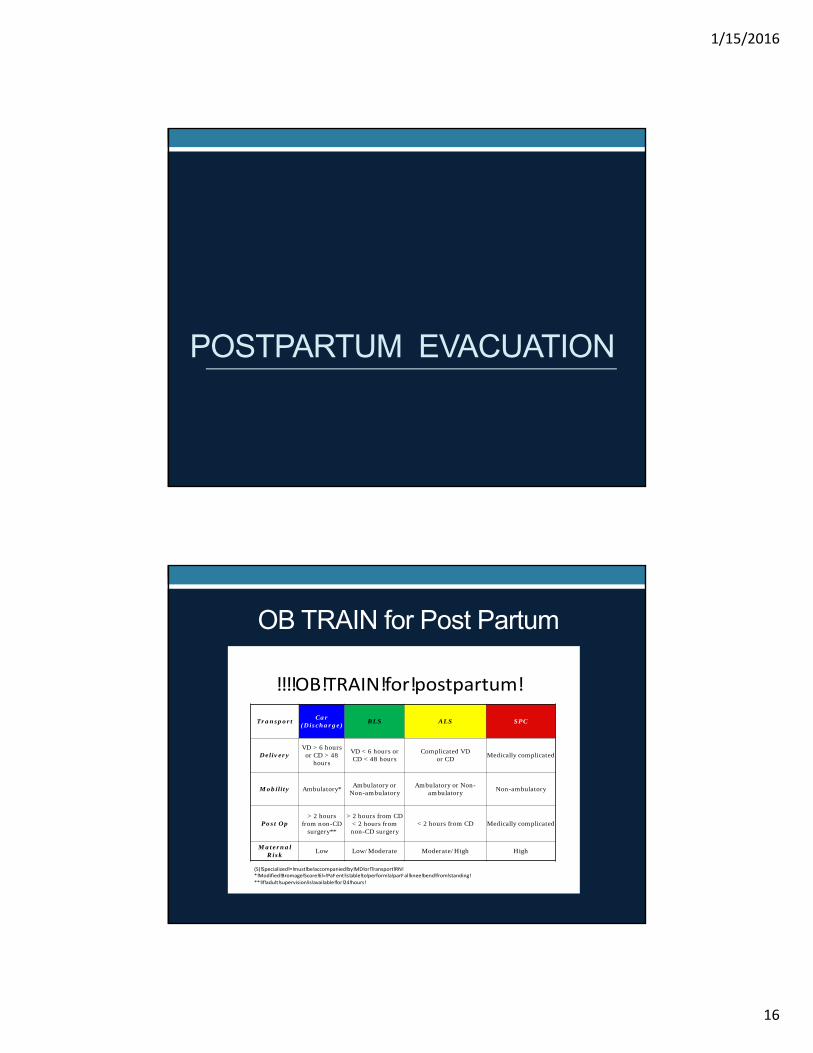
OB TRAIN for Post Partum
Transport Car
(Discharge) BLS ALS SPC
Delivery VD > 6 hours
or CD > 48 hours
VD < 6 hours or CD < 48 hours
Complicated VD or CD
Medically complicated
Mobility Ambulatory* Ambulatory or
Non-ambulatory Ambulatory or Non-
ambulatory Non-ambulatory
Post Op > 2 hours
from non-CD surgery**
> 2 hours from CD < 2 hours from non-CD surgery
< 2 hours from CD Medically complicated
Maternal Risk
Low Low/Moderate Moderate/High High
!!!!OB!TRAIN!for!postpartum!
(S)!Specialized!=!must!be!accompanied!by!MD!or!Transport!RN!*!Modified!Bromage!Score!6!=!PaFent!is!able!to!perform!a!parFal!knee!bend!from!standing!
**!If!adult!supervision!is!available!for!24!hours!
1/15/2016
17
Basis of Triage System for OB TRAIN Post partum
• Delivery - NSVD versus Cesarean delivery
- Time from delivery
• Mobility
• Anesthesia status
• Maternal risk factors
Evacuation: One pediatrician in the house, X # of babies
We’ve got to go!!
1/15/2016
18
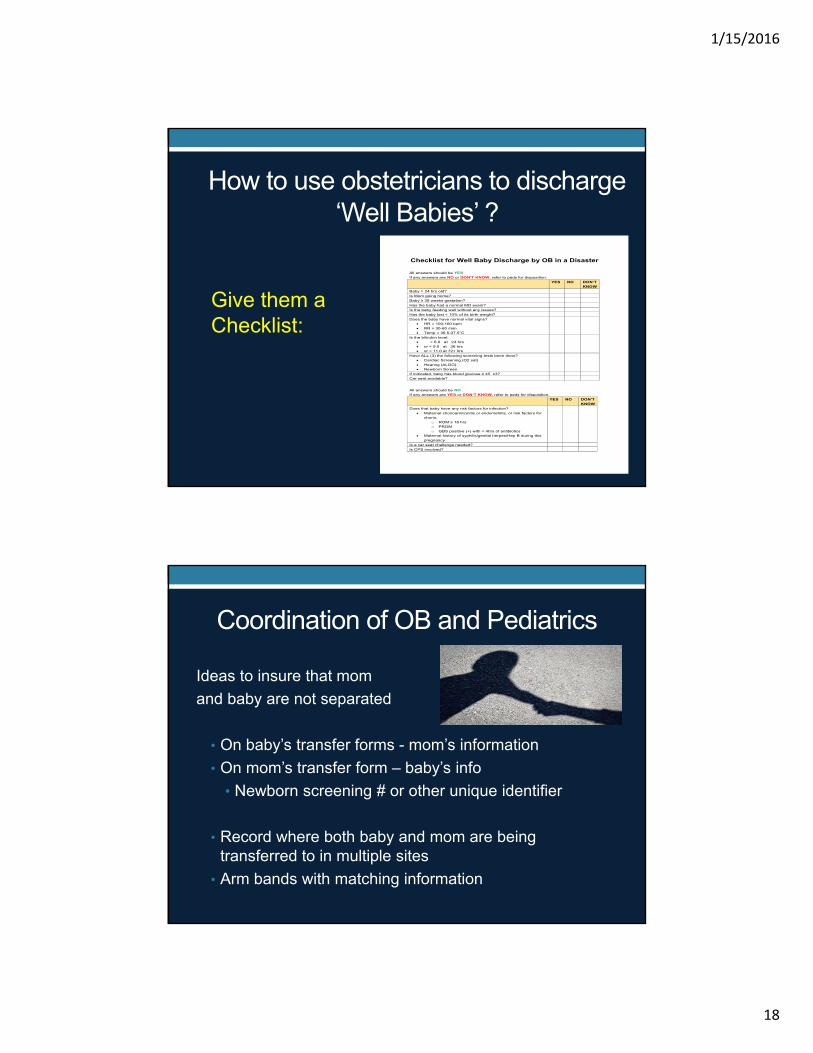
Checklist for Well Baby Discharge by OB in a Disaster All answers should be YES
If any answers are NO or DON'T KNOW, refer to peds for disposition.
YES NO DON’T
KNOW
Baby > 24 hrs old?
Is Mom going home?
Baby ≥ 38 weeks gestation?
Has the baby had a normal MD exam?
Is the baby feeding well without any issues?
Has the baby lost < 10% of its birth weight?
Does the baby have normal vital signs? HR = 100-160 bpm
RR = 30-60 /min Temp = 36.5-37.5°C
Is the bilirubin level: < 6.0 at 24 hrs
or < 9.0 at 36 hrs or < 11.0 at 72+ hrs
Have ALL (3) the following screening tests been done? Cardiac Screening (O2 sat)
Hearing (ALGO) Newborn Screen
If indicated, baby has blood glucose ≥ 45 x3?
Car seat available?
All answers should be NO
If any answers are YES or DON’T KNOW, refer to peds for disposition.
YES NO DON’T
KNOW
Does that baby have any risk factors for infection?
Maternal chorioamnionitis or endometritis, or risk factors for chorio:
o ROM ≥ 18 hrs o PROM
o GBS positive (+) with < 4hrs of antibiotics Maternal history of syphilis/genital herpes/Hep B during this
pregnancy
Is a car seat challenge needed?
Is CPS involved?
How to use obstetricians to discharge ‘Well Babies’ ?
Give them a Checklist:
Coordination of OB and Pediatrics
Ideas to insure that mom
and baby are not separated
• On baby’s transfer forms - mom’s information
• On mom’s transfer form – baby’s info
• Newborn screening # or other unique identifier
• Record where both baby and mom are being transferred to in multiple sites
• Arm bands with matching information
1/15/2016
19
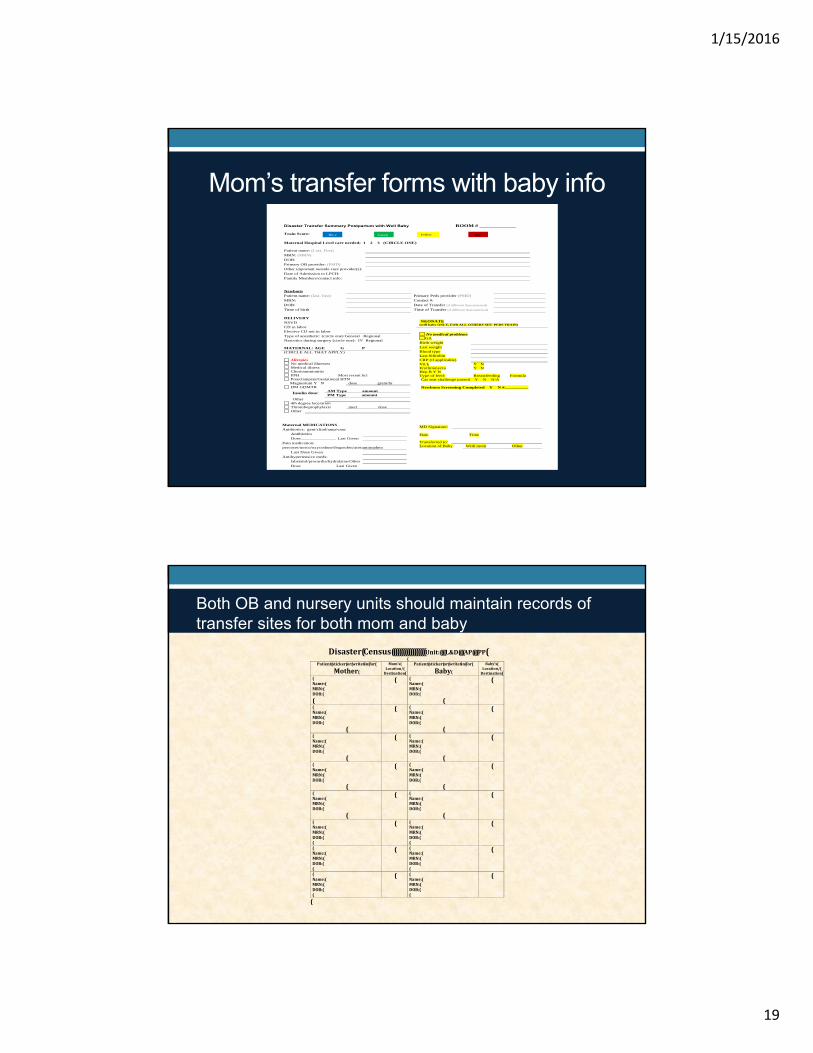
Mom’s transfer forms with baby infoDisaster Transfer Summary Postpartum with Well Baby ROOM # _____________ Train Score:
Maternal Hospital Level care needed; 1 2 3 (CIRCLE ONE) Patient name: (Last, First)
MRN: (MRN)
DOB:
Primary OB provider: (PMD) Other important outside care provider(s):
Date of Admission to LPCH: Family Members/contact info: Newborn Patient name: (last, first) Primary Peds provider (PMD)
MRN: Contact #:
DOB: Date of Transfer (if different than maternal)
Time of birth Time of Transfer (if different than maternal) DELIVERY NSVD CD in labor Elective CD not in labor
Type of anesthetic: (circle one) General Regional Narcotics during surgery (circle one): IV Regional
Car seat challenge passed Y N N/A
Newborn Screening Completed Y N #__________
MATERNAL: AGE G P (CIRCLE ALL THAT APPLY)
Allergies No medical illnesses Medical illness Chorioamnionitis PPH Most recent hct Preeclampsia/Gestational HTN
Magnesium Y N dose gram/hr DM GDM/IR
AM Type amount Insulin dose:
PM Type amount Other
4th degree laceration Thromboprophylaxis med dose Other
Maternal MEDICATIONS Antibiotics: gent/clind/amp/vanc
Antibiotics Dose_______________ Last Given
Pain medication: percocet/norco/oxycodone/ibuprofen/acetaminophen
Last Dose Given
Antihypertensive meds: labetalol/procardia/hydralzine/Other
Dose Last Given
NEONATE (well baby ONLY, FOR ALL OTHERS SEE PEDS TRAIN)
No medical problems GA
Birth weight Last weight Blood type Last bilirubin CRP (if applicable) Vit k Y N Erythromycin Y N Hep B Y N Type of feed: Breastfeeding Formula
MD Signature: Date Time
Transferred to:
Location of Baby With mom Other
Blue Green Yellow Red
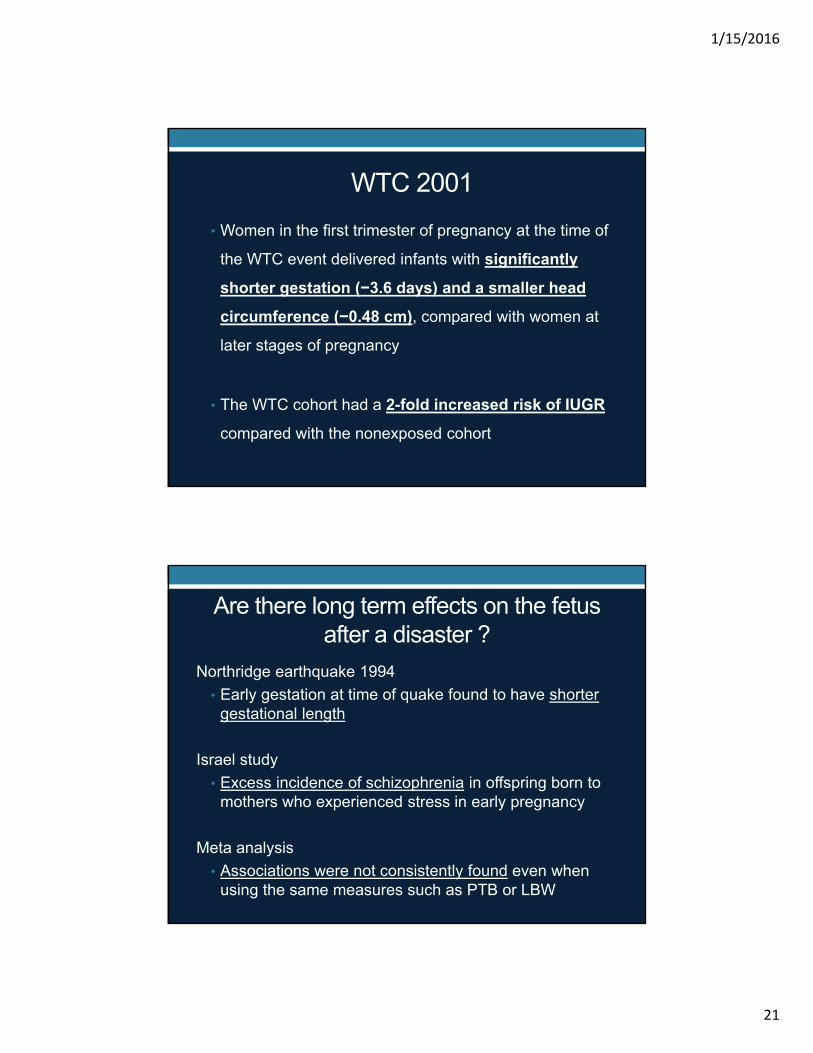
Both OB and nursery units should maintain records of transfer sites for both mom and baby
Disaster(Census((((((((((((((((((Unit:((((L&D((((AP((((PP((
Patient(sticker(or(write6in(for(
Mother(Mom’s(
Location/(Destination(
Patient(sticker(or(write6in(for(
Baby(Baby’s(
Location/(Destination(
(Name:(MRN:(DOB:(
(
( (Name:(MRN:(DOB:(
(
(
(Name:(MRN:(DOB:(
(
( (Name:(MRN:(DOB:(
(
(
(Name:(MRN:(DOB:(
(
( (Name:(MRN:(DOB:(
(
(
(Name:(MRN:(DOB:(
(
( (Name:(MRN:(DOB:(
(
(
(Name:(MRN:(DOB:(
(
( (Name:(MRN:(DOB:(
(
(
(Name:(MRN:(DOB:((
( (Name:(MRN:(DOB:((
(
(Name:(MRN:(DOB:((
( (Name:(MRN:(DOB:((
(
(Name:(MRN:(DOB:((
( (Name:(MRN:(DOB:((
(
(

1/15/2016
20
Food for thought
• Determine how to assure mom is able to continue to breast feed during a disaster
• How to monitor that babies are being adequately hydrated and fed during a disaster
Are there long term effects on the fetus after a disaster?
World Trade Center 2001 –
• Women who were pregnant on 11 September 2001 and
were living within a 2-mile radius of the WTC showed
significant decrements in term birth weight (−149 g)
and birth length (−0.82 cm), compared with infants
born to the other pregnant women
1/15/2016
21
WTC 2001
• Women in the first trimester of pregnancy at the time of
the WTC event delivered infants with significantly
shorter gestation (−3.6 days) and a smaller head
circumference (−0.48 cm), compared with women at
later stages of pregnancy
• The WTC cohort had a 2-fold increased risk of IUGR
compared with the nonexposed cohort
Are there long term effects on the fetus after a disaster ?
Northridge earthquake 1994
• Early gestation at time of quake found to have shorter gestational length
Israel study
• Excess incidence of schizophrenia in offspring born to mothers who experienced stress in early pregnancy
Meta analysis
• Associations were not consistently found even when using the same measures such as PTB or LBW
1/15/2016
22
Next steps: Collaborative network on a regional, statewide and national level
Lessons from Katrina
• Communications essential but are always a challenge
- Phone lines may be down
- Internet may be off
• All disaster response is local for the first 48–96 hours
• The ability to mobilize resources depends on a pre-existing local collaborative network
Mattox KL. Critical Care 2006, 10:205 (doi:10.1186/cc3942)
1/15/2016
23
In summary: To accomplish a comprehensive obstetric disaster plan
there needs to be:
1. Adoption of an obstetric-specific triage system like OB TRAIN to allow a universal language for evacuation and surge processes
2. A system in place to transfer OB patients to the appropriate hospital (the right patient to the right hospital)
In summary3. An comprehensive shelter in place plan for laboring
patients that includes:• Grab and go bags/equipment• Communication with peds
4. Postpartum plan that takes into consideration transport of mom and baby
• Avoid maternal-neonatal separation when possible• Accurately track location if separated
5. Create a regional and ultimately national collaborative network of maternity hospitals
1/15/2016
24
Online access to disaster tools
Stanford Disaster OB Planning “Tool kit”
http://obgyn.stanford.edu/community/disaster-planning.html
NICU TRAIN
http://cpqcc.org/quality_improvement/qi_toolkits/can_neonata
l_disaster_preparedness_toolkit.
Kay Daniels
THANK YOU FOR YOUR ATTENTION
Stanford University - Main Quad
1/15/2016
25
References1. Daniels K, Oakeson AM, Hilton G. Steps Toward a National Disaster
Plan for Obstetrics Obstet Gynecol July 2014;124:154–8
2. Jorgensen, A, Mendoza G, Henderson J. Emergency Preparedness and Disaster Response Core Competency Set for Perinatal and Neonatal Nurses. JOGNN 2010:39;450-467
3. Giarratano G, Sterling Y, Orlando S, Mathews P, Deeves G, Bernard ML, Danna D, Targeting Prenatal Emergency Preparedness Through Childbirth Education JOGNN, 39, 480-488; 2010
4. Orlando S, Danna D, Giarratano G, Prepas R, Barker Johnson C, Perinatal Considerations in the Hospital Disaster Management Process JOGNN, 39, 468-479; 2010
5. ACOG Hospital Disaster Preparedness for Obstetricians and Facilities Providing Maternity Care Committee Opinion Number 555 March 2013
6. ACOG Consensus : Levels of Maternal Care Obstet Gyecol Feb 2015:125 No 2
7. Glynn et al. When stress happens matters: Effects of earthquake timing on stress responsivity in pregnancy. Am J Obstet Gynecol March 2001
8. Lederman et al. The Effects of the World Trade Center Event on Birth Outcomes among Term Deliveries at Three Lower Manhattan Hospitals. Environ Health Perspect 2004 Dec:112(17)
9. Zotti et al. Post-Disaster Reproductive Health Outcomes
Matern Child Health J (2013) 17:783–796
10. Malaspina et al. Acute maternal stress in pregnancy and schizophrenia in offspring: A cohort prospective study
BMC Psychiatry. 2008;8:71.
11. Berkowitz et al. The World Trade Center Disaster and Intrauterine Growth Restriction Research letters JAMA, August 6, 2003 Vol 290, No. 5
12. Harville et al. Obstet Gynecol Surv. 2010 November;65:713–728