cytotoxicity of topical antimicrobial agents used in burn wounds in australasia
TRANSCRIPT
ANZ J. Surg.
2004;
74
: 139–142
ORIGINAL ARTICLE
ORIGINAL ARTICLE
CYTOTOXICITY OF TOPICAL ANTIMICROBIAL AGENTS USED IN BURN WOUNDS IN AUSTRALASIA
J
OHN
F. F
RASER
, L
EILA
C
UTTLE
, M
ARGIT
K
EMPF
AND
R
OY
M. K
IMBLE
Royal Children’s Hospital Burns Research Group, Department of Paediatrics and Child Health, University of Queensland, Royal Children’s Hospital, Brisbane, Queensland, Australia
Background:
Burn sepsis is a leading cause of mortality and morbidity in patients with major burns. The use of topical anti-microbial agents has helped improve the survival of these patients. Silvazine (Sigma Pharmaceuticals, Melbourne, Australia)(1% silver sulphadiazine and 0.2% chlorhexidine digluconate) is used exclusively in Australasia, and there is no published study onits cytotoxicity. This study compared the relative cytotoxicity of Silvazine with 1% silver sulphadiazine (Flamazine (Smith &Nephew Healthcare, Hull, UK)) and a silver-based dressing (Acticoat (Smith & Nephew Healthcare, Hull, UK)).
Methods:
Dressings were applied to the centre of culture plates that were then seeded with keratinocytes at an estimated 25%confluence. The plates were incubated for 72 h and culture medium and dressings then removed. Toluidine blue was added to stainthe remaining keratinocytes. Following removal of the dye, the plates were photographed under standard conditions and these digitalimages were analysed using image analysis software. Data was analysed using Student’s
t
-test.
Results:
In the present study, Silvazine is the most cytotoxic agent. Seventy-two hour exposure to Silvazine in the present studyresults in almost no keratinocyte survival at all and a highly statistically significant reduction in cell survival relative to control,Acticoat and Flamazine (
P
< 0.001,
P
< 0.01,
P
< 0.01, respectively). Flamazine is associated with a statistically significant reduc-tion in cell numbers relative to control (
P
< 0.05), but is much less cytotoxic than Silvazine (
P
< 0.005).
Conclusion:
In this
in-vitro
study comparing Acticoat, Silvazine and Flamazine, Silvazine shows an increased cytotoxic effect,relative to control, Flamazine and Acticoat. An
in-vivo
study is required to determine whether this effect is carried into the clinicalsetting.
Key words: antimicrobial, burn, cytotoxicity, sepsis, wound healing.
Abbreviations
: DMEM, Dulbecco’s Modified Eagle Medium; PBS, phosphate buffered saline; SSD, 1% silver sulphadiazine;TAA, topical antimicrobial agents.
INTRODUCTION
A cutaneous burn denudes the skin of the keratin layer and anumber of layers of essential skin cells, as well as inducing local-ized reduction of blood supply, thus resulting in tissue hypoxia.
1
Loss of this protective integuum results in bacterial penetrationinto the underlying tissue, which can result in fatal burn sepsis.Prevention of burn wound sepsis is dependant on optimal woundmanagement, including the use of topical antimicrobials andprompt closure of the wound defect. The advent of topical antimi-crobials in the 1960s reduced the mortality from burn woundsepsis from 60% to 28%.
2
However, burn wound sepsis remainsan important and potentially remediable cause of significant mor-tality and morbidity.
3
The advent of multiresistant bacteria has hastened the almostexclusive use of silver-based topical antimicrobial agents (TAA)for the prevention of burn wound sepsis.
4,5
The mainstay of burnwound topical antimicrobials in most countries is the preparationof 1% silver sulphadiazine (SSD or Flamazine (Smith & NephewHealthcare, Hull, UK) in the USA and UK). In Australasia, thiscompound has been combined with 0.2% chlorhexidine digluco-nate and marketed as Silvazine (USL Medical, Auckland, NewZealand). This product was the result of clinical trials conductedat the Royal Melbourne Hospital (Melbourne, Vic., Australia)in response to an outbreak of
Staphylococcus aureus
in the burnsunit that was resistant to standard SSD.
6
The transition fromstandard SSD to SSD with 0.2% chlorhexidine digluconateresulted in a 50% reduction of burn wound sepsis.
7,8
Prior to theintroduction of Acticoat (Smith & Nephew Healthcare, Hull,UK), Silvazine was the standard topical antimicrobial for burns,as well as for problematic infected venous ulcers.
3,8
A number of groups have compared the antimicrobial activityof Silvazine and other TAA, both clinically and
in vitro
, and abeneficial antimicrobial effect has consistently been found withthe addition of chlorhexidine digluconate.
9,10
However, therehave been no studies examining the relative cytotoxicity ofSilvazine with the same TAA, despite the obvious importance ofcytotoxicity profile to the development of nascent and adherentkeratinocytes and the deleterious effects a delay in wound closurecan cause. Agents that are highly effective at killing bacteria canalso be harmful to immature and nonadherent keratinocytes,hence, delaying wound closure and paradoxically increasing risk
Smith & Nephew provided all the dressings free of charge. They had noinvolvement in the study or manuscript. Smith & Nephew have assisted withDr Fraser’s travel costs associated with a conference where he presented someof the data described in this study.
J. F. Fraser
MBChB, MRCP, FRCA, FFARCSI, FJFICM;
L. Cuttle
BSc(Hons);
M. Kempf
DipMLSc;
R. M. Kimble
MBChB, FRCS, FRACS.
Correspondence: Dr J. F. Fraser, University of Queensland, Department ofPaediatrics and Child Health, Royal Children’s Hospital, Herston, Brisbane,QLD 4029, Australia.Email: [email protected]
Accepted for publication 3 August 2003.

140 FRASER
ET AL
.
of delayed burn infection. There are many potent antimicrobialagents which cannot be used long-term because of their extremecytotoxicity, such as povidine-iodine.
11–13
A balance must bemade between antimicrobial efficacy and cytotoxicity. If a TAAis a more potent toxin to the developing keratinocytes than to thebacteria, its use must be deleterious to the fragile environment ofthe healing wound.
The component parts as well as their carrier molecule determinethe toxicity of TAA. Silver is the main component of commonlyused TAA in burn injury, and in comparison to other heavy metals,such as lead and mercury, causes minimal clinically importantsequelae.
14
Argyria is a term used to describe silver toxicity, whichresults in grey/blue skin discolouration caused by both to directsilver deposition, and, indirectly by a silver-induced increase inmelanin complexes. Silver absorption can be significant in thetreatment of large (>60%) burns, such that urinary excretion ofsilver (a sensitive indicator of absorption) rises from <1
µ
g/24 h to>1100
µ
g/24 h.
15,16
Silver is rapidly absorbed through the burnwound. It has been reported in isolated incidences to inducehepatic, renal and central nervous system toxicity. Serum silverlevels do not correlate with hepatic and renal function.
16
Sulphadiazine is a sulphonamide molecule and is associatedwith allergic reactions including toxic epidermal necrolysis andrash formation, as well as nonallergic reactions, such as leuko-penia, which occurs in 3–60% of all patients treated.
17,18
In addi-tion to silver and sulphadiazine, Silvazine also contains chlor-hexidine gluconate, a biguanide. Chlorhexidine is active against awide range of Gram-positive and Gram-negative bacteria, yeast,and moulds.
19
Chlorhexidine disrupts cytoplasmic membranesand, importantly, remains active for at least 6 h after application.Its rapid uptake, with maximal absorption within 20 s, and pro-longed effect (>6 h) make chlorhexidine a very potent agent.
13
The cytotoxicity of chlorhexidine is well recognized in a numberof studies, but no study has examined the cytotoxicity of thecombination product Silvazine.
13,20,21
As a dressing used entirely in Australasia where the parentcompany has no research arm, there has been no publishedresearch conducted on the cytotoxicity of Silvazine. We designeda study to assess the relative cytotoxicity of Silvazine and anew nanocrystalline silver burn dressing, Acticoat, introducedrecently into Australasia. We also assessed the cytotoxic effect ofsilver sulphadiazine (Flamazine), to assess the difference in cyto-toxicity as a result of the addition of chlorhexidine digluconate.
MATERIALS AND METHODS
HaCaT cells (a strain of immortalized human keratinocytes)were grown in DMEM (Dulbecco’s Modified Eagle Medium)containing 10% fetal calf serum, 0.11 mg/mL sodium pyruvate,100
µ
g/mL streptomycin, 100 U/mL penicillin and 0.25
µ
g/mLamphotericin B. HaCaT cells are a robust cell line, which growmore easily than normal human keratinocytes in culture. Cellswere thawed and grown in our laboratory under standard condi-tions for 2 weeks prior to seeding.
All treatments were carried out in 100 mm diameter tissueculture plates. The treatments examined were: Silvazine,Flamazine, Acticoat, hystoacryl glue and a control plate with notreatment. All treatments were added to the plates inside a 10-mmsquare in the centre of each plate, to ensure equal surface area.For the Acticoat treatment, a 10-mm square of Acticoat (contain-ing 0.84–1.34 mg/cm
2
of silver) was glued to the centre of theplate. For the Silvazine and Flamazine treatments, 0.1 mL was
added to each plate, which contains an equivalent amount ofsilver w/w to the Acticoat. These were added with a syringe in asterile manner. Cells were seeded at a density of 0.75
×
10
6
cells(estimated 25% confluence) in 10 mL of media. All treatmentswere performed in triplicate. The plates were then incubated at37
°
C for 72 h. At the end of this time, the culture medium wasremoved along with the respective dressings. Ten drops of tolu-idine blue were added for 2 min, during which time the plateswere continuously agitated to ensure equal coverage. The plateswere then washed with PBS (phosphate buffered saline) and leftto dry. Each study was repeated three times, and the mean areaof each plate covered by cells was compared using the Stu-dent’s
t
-test. The cytotoxicity of chlorhexidine has been wellestablished in a multitude of previous studies, and is not used inisolation as a burn dressing.
20
Hence, the relevance of assayingchlorhexidine in a study assessing the relative cytotoxicity ofTAA was minimal.
Analysis
The stained cell culture dishes were allowed to dry and werephotographed under standard conditions using a Gel-Pro Imagersystem (Media Cybernetics, LR, USA). These digital imageswere analysed using Image Pro Plus image analysis software(Version 4.1, Media Cybernetics, LP, USA). The area coveredwith cells was analysed and calculated as a percentage of the totalarea of the culture dish. A central area, consistent with the posi-tion of the treatments, was excluded from the final analysis inall dishes, including controls. Results were compared using aStudent’s
t
-test to determine significant differences.
RESULTS
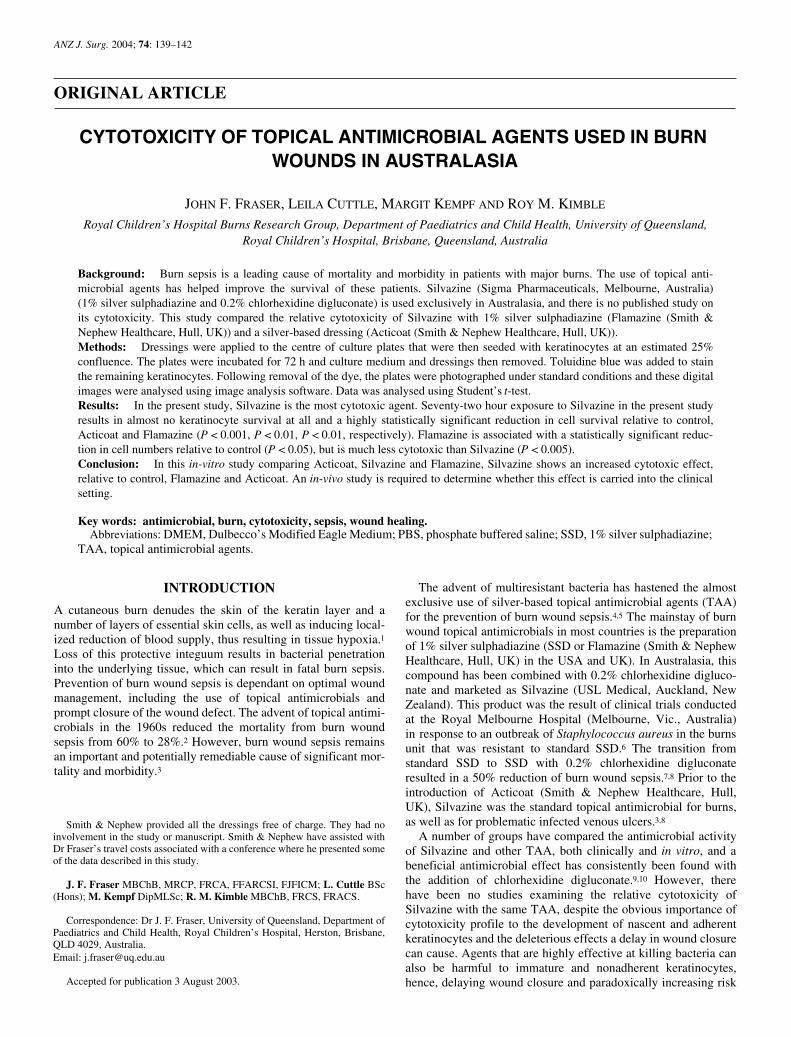
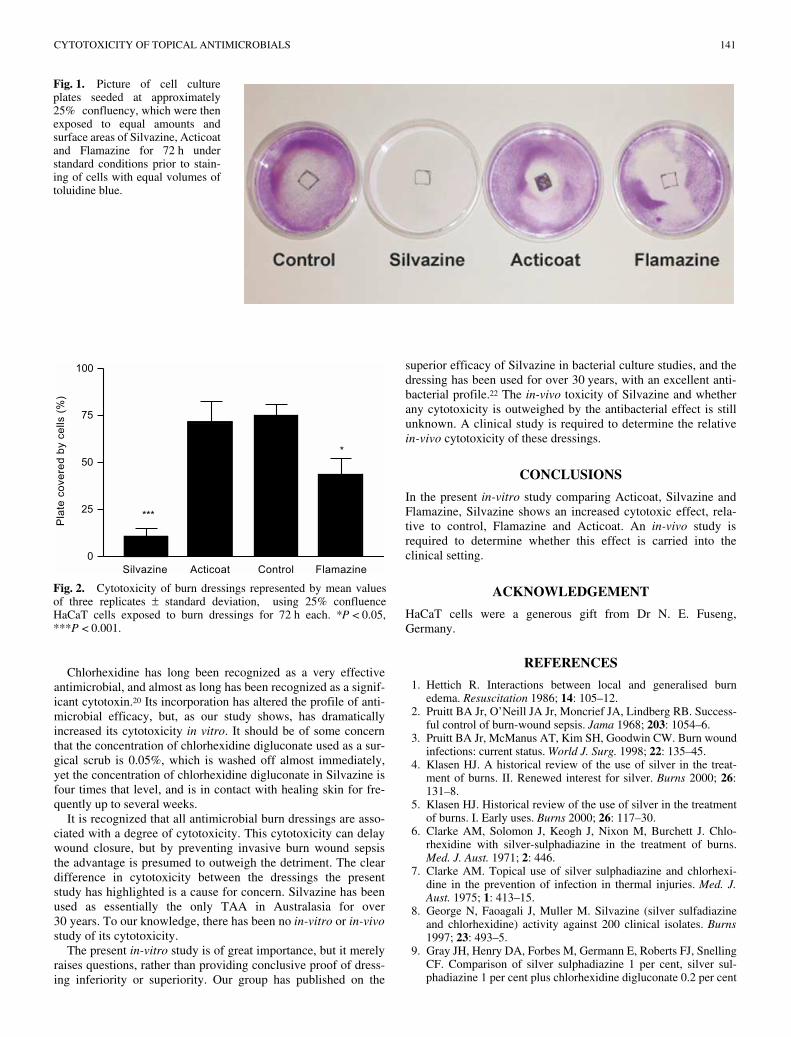
Macroscopically, it was evident that the Silvazine dishes hadalmost no keratinocytes after 72 h exposure to Silvazine (Fig. 1).This concurred with digital image analysis. Analysis of the digitalimages, using the Student’s
t
-test, shows a highly significantreduction in cell survival using Silvazine relative to control(
P
< 0.001) (Fig. 2). Flamazine is associated with a statisticallysignificant reduction in cell numbers relative to control(
P
< 0.05), as has been previously reported, but is much less cyto-toxic than Silvazine. In this assay, there was a consistent, butnon-significant cytotoxic effect seen with Acticoat (
P
> 0.05).The use of hystoacryl glue did not alter the cytotoxicity of Acti-coat significantly (data not shown).
DISCUSSION
The study design allowed for the dressings to be left untouchedfor 3 days, as the Acticoat dressing used is recommended for3 day use. Chlorhexidine, in contrast to SSD, is freely watersoluble, so a component of the widespread cytotoxicity couldbe related to the freely available chlorhexidine in solution,whereas the effects of the other dressings would be limitedto the area in which they are positioned. The present studydoes not exclude the possibility that chlorhexidine increasesthe solubility of SSD in the study, but this has never beforebeen reported. Silver is freely absorbed in significant quantitiesfrom SSD in burns patients, resulting in occasionally toxiclevels, so some of the silver from the SSD would be solubilizedin this study. We did not assess the amount of free silver in thegrowth medium.
CYTOTOXICITY OF TOPICAL ANTIMICROBIALS 141
Chlorhexidine has long been recognized as a very effectiveantimicrobial, and almost as long has been recognized as a signif-icant cytotoxin.
20
Its incorporation has altered the profile of anti-microbial efficacy, but, as our study shows, has dramaticallyincreased its cytotoxicity
in vitro
. It should be of some concernthat the concentration of chlorhexidine digluconate used as a sur-gical scrub is 0.05%, which is washed off almost immediately,yet the concentration of chlorhexidine digluconate in Silvazine isfour times that level, and is in contact with healing skin for fre-quently up to several weeks.
It is recognized that all antimicrobial burn dressings are asso-ciated with a degree of cytotoxicity. This cytotoxicity can delaywound closure, but by preventing invasive burn wound sepsisthe advantage is presumed to outweigh the detriment. The cleardifference in cytotoxicity between the dressings the presentstudy has highlighted is a cause for concern. Silvazine has beenused as essentially the only TAA in Australasia for over30 years. To our knowledge, there has been no
in-vitro
or
in-vivo
study of its cytotoxicity.The present
in-vitro
study is of great importance, but it merelyraises questions, rather than providing conclusive proof of dress-ing inferiority or superiority. Our group has published on the
superior efficacy of Silvazine in bacterial culture studies, and thedressing has been used for over 30 years, with an excellent anti-bacterial profile.
22
The
in-vivo
toxicity of Silvazine and whetherany cytotoxicity is outweighed by the antibacterial effect is stillunknown. A clinical study is required to determine the relative
in-vivo
cytotoxicity of these dressings.
CONCLUSIONS
In the present
in-vitro
study comparing Acticoat, Silvazine andFlamazine, Silvazine shows an increased cytotoxic effect, rela-tive to control, Flamazine and Acticoat. An
in-vivo
study isrequired to determine whether this effect is carried into theclinical setting.
ACKNOWLEDGEMENT
HaCaT cells were a generous gift from Dr N. E. Fuseng,Germany.
REFERENCES
1. Hettich R. Interactions between local and generalised burnedema.
Resuscitation
1986;
14
: 105–12.2. Pruitt BA Jr, O’Neill JA Jr, Moncrief JA, Lindberg RB. Success-
ful control of burn-wound sepsis.
Jama
1968;
203
: 1054–6.3. Pruitt BA Jr, McManus AT, Kim SH, Goodwin CW. Burn wound
infections: current status.
World J. Surg.
1998;
22
: 135–45.4. Klasen HJ. A historical review of the use of silver in the treat-
ment of burns. II. Renewed interest for silver.
Burns
2000;
26
:131–8.
5. Klasen HJ. Historical review of the use of silver in the treatmentof burns. I. Early uses.
Burns
2000;
26
: 117–30.6. Clarke AM, Solomon J, Keogh J, Nixon M, Burchett J. Chlo-
rhexidine with silver-sulphadiazine in the treatment of burns.
Med. J. Aust.
1971;
2
: 446.7. Clarke AM. Topical use of silver sulphadiazine and chlorhexi-
dine in the prevention of infection in thermal injuries.
Med. J.Aust.
1975;
1
: 413–15.8. George N, Faoagali J, Muller M. Silvazine (silver sulfadiazine
and chlorhexidine) activity against 200 clinical isolates.
Burns
1997;
23
: 493–5.9. Gray JH, Henry DA, Forbes M, Germann E, Roberts FJ, Snelling
CF. Comparison of silver sulphadiazine 1 per cent, silver sul-phadiazine 1 per cent plus chlorhexidine digluconate 0.2 per cent
Fig. 1.
Picture of cell cultureplates seeded at approximately25% confluency, which were thenexposed to equal amounts andsurface areas of Silvazine, Acticoatand Flamazine for 72 h understandard conditions prior to stain-ing of cells with equal volumes oftoluidine blue.
Fig. 2.
Cytotoxicity of burn dressings represented by mean valuesof three replicates
±
standard deviation, using 25% confluenceHaCaT cells exposed to burn dressings for 72 h each. *
P
< 0.05,***
P
< 0.001.

142 FRASER
ET AL
.
and mafenide acetate 8.5 per cent for topical antibacterial effectin infected full skin thickness rat burn wounds.
Burns
1991;
17
:37–40.
10. Inman RJ, Snelling CF, Roberts FJ, Shaw K, Boyle JC. Prospec-tive comparison of silver sulfadiazine 1 per cent plus chlorhexi-dine digluconate 0.2 per cent (Silvazine) and silver sulfadiazine1 per cent (Flamazine) as prophylaxis against burn wound infec-tion.
Burns Incl. Therm. Inj.
1984;
11
: 35–40.11. Steen M. Review of the use of povidone-iodine (PVP-I) in the
treatment of burns.
Postgrad Med. J.
1993;
69
: S84–92.12. al-Tannir MA, Goodman HS. A review of chlorhexidine and its
use in special populations.
Spec. Care Dentist
1994;
14
: 116–22.13. Hidalgo E, Dominguez C. Mechanisms underlying chlorhexi-
dine-induced cytotoxicity.
Toxicol. In Vitro
2001;
15
: 271–6.14. Hollinger MA. Toxicological aspects of topical silver pharma-
ceuticals.
Crit. Rev. Toxicol.
1996;
26
: 255–60.15. Lockhart SP, Rushworth A, Azmy AA, Raine PA. Topical silver
sulphadiazine: side effects and urinary excretion.
Burns Incl.Therm. Inj.
1983;
10
: 9–12.16. Maitre S, Jaber K, Perrot JL, Guy C, Cambazard F. Increased
serum and urinary levels of silver during treatment with topicalsilver sulfadiazine.
Ann. Dermatol. Venereol.
2002;
129
:217–19.
17. Ortiz JE, Horn MS, Peterson HD. Toxic epidermal necrolysis-case report and review of the literature.
Ann. Plast. Surg.
1982;
9
: 249–53.18. Sawada Y. Adverse reaction to sulphonamides in a burned
patient: a case report.
Burns Incl. Therm. Inj.
1985;
12
: 127–31.19. McDonnell G, Russell AD. Antiseptics and disinfectants: Activ-
ity, Action, Resistance.
Clin. Microbiol. Rev.
1999;
12
: 147–79.20. Gasset AR, Ishii Y. Cytotoxicity of chlorhexidine.
Can. J. Oph-thalmol.
1975; 10: 98–100.21. Wilken R, Botha SJ, Grobler A, Germishuys PJ. In vitro cyto-
toxicity of chlorhexidine gluconate, benzydamine-HCl andpovidone iodine mouth rinses on human gingival fibroblasts.Sadj 2001; 56: 455–60.
22. Fraser JF, Bodman J, Sturgess R, Faoagali J, Kimble RM. An invitro study of the antimicrobial efficacy of a 1% silver sulpha-diazine and 0.2% chlorhexidine digluconate cream and a silvercoated dressing. Burns 2004; 30: 35–41.