cutaneous tuberculosis
TRANSCRIPT
Cutaneous Tuberculosis
PRESENTED BY,
JINU JANET VARGHESE
TBILISI STATE MEDICAL UNIVERSITY
Introduction
Cutaneous tuberculosis occurs rarely, despite a high and increasing
prevalence of tuberculosis worldwide. Mycobacterium tuberculosis,
Mycobacterrium bovis, and the Bacille Calmette-Guérin vaccine can
cause tuberculosis involving the skin.
Diagnosis of these lesions can be difficult, as they resemble many
other dermatological conditions that are often primarily considered.
Different Types of Cutaneous Tuberculosis

TB verrucosa cutis
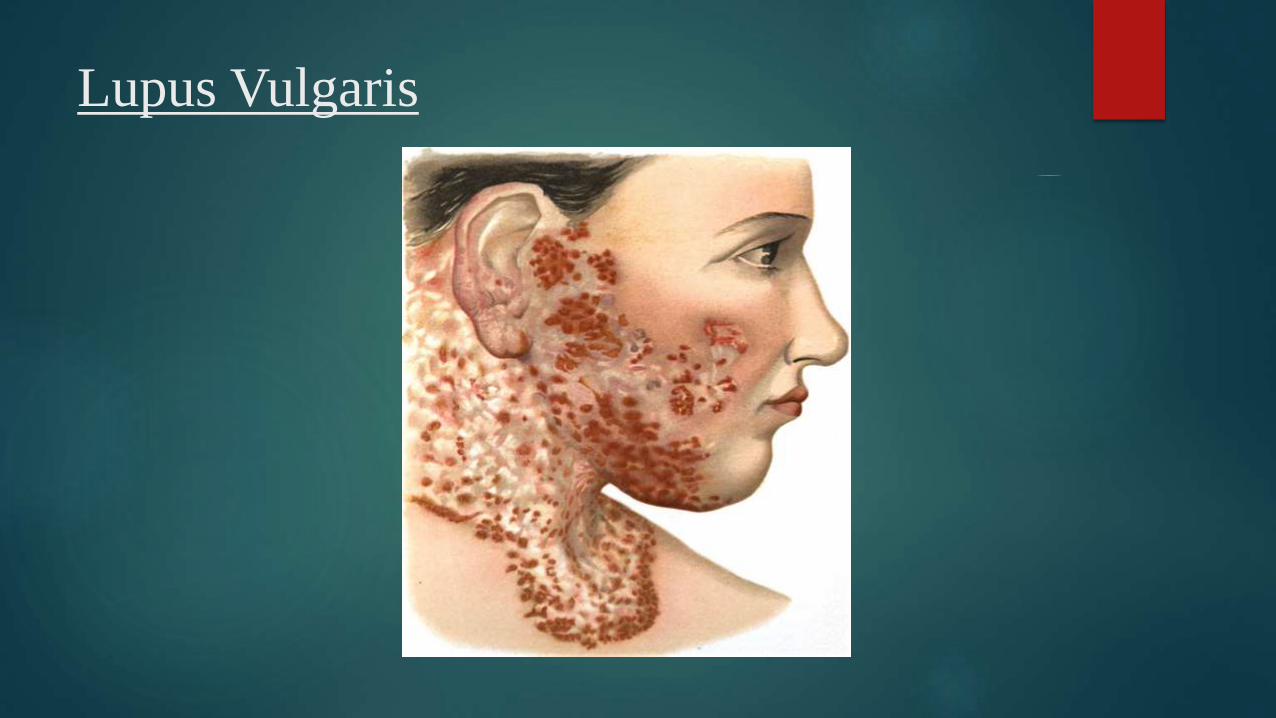
Lupus Vulgaris

Scrofuloderma

Miliary Tuberculosis

Tuberculid
Diagnostic Tests
The diagnosis is usually on skin biopsy. Typical tubercles are
caseating epithelioid granulomas that contain acid-fast bacilli. These
are detected by tissue staining, culture and polymerase chain
reaction (PCR).
Other tests that may be necessary include:
Tuberculin skin test (Mantoux)
Quantiferon-Gold blood test
Sputum culture (it may take a month or longer for results to be
reported)
Chest X-ray & other radiological tests for extrapulmonary infection.
Interferon gamma release assays (IGRA)
Tuberculin Skin Test
The Mantoux tuberculin skin test (TST) is the standard method of
determining whether a person is infected with Mycobacterium
tuberculosis.
The skin test reaction should be read between 48 and 72 hours after
administration.
The reaction should be measured in millimeters of the induration
(palpable, raised, hardened area or swelling) & erythema is not read.
Quantiferon-Gold blood test
TheQuantiFERON®‐TB Gold test (QFT‐G) is a whole‐blood test for use as an aid
in diagnosing Mycobacterium tuberculosis infection, including latent tuberculosis
infection (LBTI) and tuberculosis(TB) disease.
This test is the preferred method of testing for persons 5 years of age and older.
QFT‐G may be especially useful in patients suspected of having possible
false‐positive Tuberculin Skin Testing (TST) due to previous BCG vaccination or
environmental (non‐tuberculosis) mycobacterial infection.
A positive response to the QFT‐G does not mean the person has ACTIVE TB. It
simply means they have been exposed to the M.tuberculosis bacterium. They may
have latent infection, active infection, or treated infection.
Sputum Culture
Testing mucus from the lungs (sputum culture) is the best way to
diagnose active TB. But a sputum culture can take 1 to 8 weeks to
provide results.
Sputum smears and cultures should be done for acid-fast bacilli if
the patient is producing sputum. The preferred method for this is
fluorescence microscopy (auramine-rhodamine staining), which is
more sensitive than conventional Ziehl-Neelsen staining.
Chest X-ray & other radiological tests
Chest X-ray findings that can suggest active TB:
Infiltrate or consolidation
Any cavitary lesion
Nodule with poorly defined margins
Pleural effusion
Hilar or mediastinal lymphadenopathy (bihilar lymphadenopathy)
Linear, interstitial disease (in children only)
Interferon gamma release assays (IGRA)
Interferon-Gamma Release Assays (IGRAs) are whole-blood tests
that can aid in diagnosing Mycobacterium tuberculosis infection.
They do not help differentiate latent tuberculosis infection (LTBI)
from tuberculosis disease.
IGRAs measure a person’s immune reactivity to M. tuberculosis.
White blood cells from most persons that have been infected with
M. tuberculosis will release interferon-gamma (IFN-g) when mixed
with antigens (substances that can produce an immune response)
derived from M. tuberculosis.
Treatments
Currently, the treatment of all types of tuberculosis is by the directly observed treatment short course (DOTS) strategy, but chemotherapy is the treatment of choice for cutaneous tuberculosis. For the four-agent regimen, an initial combination of isoniazid, rifampin, pyrazinamide, and either ethambutol or streptomycin is given daily for 2 months.
DOTS has two phases - 2 months of intensive phase and 4 months of continuation phase, and, in severe cases, the treatment is extended to 8-12 months.
Most DOTS regimens have thrice-weekly schedules. For cutaneous tuberculosis, category III (2H 3 R 3 Z 3 + 4H 3 R 3 ) is recommended. In this category, Rifampicin (R-450 mg), Isoniazid (H-600 mg) and Pyrazinamide (Z-1500 mg) are administered for three days in a week for 2 months (intensive phase), followed by R-450 mg and H-600 mg given three days in a week as a continuation phase for 4 months.
In case of cutaneous tuberculosis with systemic infections, or when more than one group of lymph nodes are involved, category I with four drugs is advised. Depending on the clinical response, the duration of treatment can be extended under the guidance of the clinician. For children and adults who weigh less than 30 kg, these drugs are administered according to their weight.
References
http://dermnetnz.org/
http://www.ijdvl.com/article.asp?issn=0378-
6323;year=2011;volume=77;issue=3;spage=330;epage=332;aulast=Rama
http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.175.4340
&rep=rep1&type=pdf
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2923933/
http://www.cdc.gov/tb/publications/factsheets/testing/igra.htm
http://ftguonline.org/ftgu-232/index.php/ftgu/article/view/1983/3962