cost effectiveness of once-daily oral chelation therapy with deferasirox versus infusional...
TRANSCRIPT
Pharmacoeconomics 2007; 25 (4): 329-342ORIGINAL RESEARCH ARTICLE 1170-7690/07/0004-0329/$44.95/0
© 2007 Adis Data Information BV. All rights reserved.
Cost Effectiveness of Once-Daily OralChelation Therapy with Deferasiroxversus Infusional Deferoxamine inTransfusion-DependentThalassaemia PatientsUS Healthcare System Perspective
Thomas E. Delea,1 Oleg Sofrygin,1 Simu K. Thomas,2 Jean-Francois Baladi,2Pradyumna D. Phatak3 and Thomas D. Coates4
1 Policy Analysis Inc. (PAI), Brookline, Massachusetts, USA2 Novartis Pharmaceuticals Corp., East Hanover, New Jersey, USA3 Hematology/Oncology Unit Rochester General Hospital, Rochester, New York, USA4 Center for Cancer and Blood Diseases, Childrens Hospital of Los Angeles, Los Angeles,
California, USA
Background: Deferasirox is a recently approved once-daily oral iron chelator thatAbstracthas been shown to reduce liver iron concentrations and serum ferritin levels to asimilar extent as infusional deferoxamine.Objective: To determine the cost effectiveness of deferasirox versus deferox-amine in patients with β-thalassaemia major from a US healthcare system per-spective.Methods: A Markov model was used to estimate the total additional lifetime costsand QALYs gained with deferasirox versus deferoxamine in patients with β-thalassaemia major and chronic iron overload from blood transfusions. Patientswere assumed to be 3 years of age at initiation of chelation therapy and to receiveprescribed dosages of deferasirox and deferoxamine that have been shown to besimilarly effective in such patients. Compliance with chelation therapy andprobabilities of iron overload-related cardiac disease and death by degree ofcompliance were estimated using data from published studies. Costs ($US, year2006 values) of deferoxamine administration and iron overload-related cardiacdisease were based on analyses of health insurance claims of transfusion-depen-dent thalassaemia patients. Utilities were based on a study of patient preferencesfor oral versus infusional chelation therapy, as well as published literature.Probabilistic and deterministic sensitivity analyses were employed to examine therobustness of the results to key assumptions.Results: Deferasirox resulted in a gain of 4.5 QALYs per patient at an additionalexpected lifetime cost of $US126 018 per patient; the cost per QALY gained was$US28 255. The cost effectiveness of deferasirox versus deferoxamine was sensi-tive to the estimated costs of deferoxamine administration and the quality-of-lifebenefit associated with oral versus infusional therapy. Cost effectiveness was also

330 Delea et al.
relatively sensitive to the equivalent daily dose of deferasirox, and the unit costs ofdeferasirox and deferoxamine, and was more favourable in younger patients.Conclusion: Results of this analysis of the cost effectiveness of oral deferasiroxversus infusional deferoxamine suggest that deferasirox is a cost effective ironchelator from a US healthcare perspective.
β-Thalassaemia is a rare recessively inherited agent. There is, therefore, a clear need in the US fordisorder of haemoglobin synthesis. Most infants an effective iron chelator that is less burdensome towho are homozygous for the β-thalassaemia gene administer than deferoxamine.develop β-thalassaemia major, a profound, transfu- Deferasirox (Exjade®, Novartis) is a member of asion-dependent anaemia, due to absent or ineffective new class of tridentate iron chelators, the N-substi-production of the haemoglobin β-chain. Without tuted bis-hydroxyphenyl-triazoles.[4] This drug istransfusions, most children with β-thalassaemia ma- orally bioavailable and its terminal elimination half-jor would die within a few years. Long-term transfu- life (t1/2) is between 8 and 16 hours, allowing forsion therapy prolongs life but, because humans can- once-daily administration.not actively eliminate iron from the body, results in A phase III trial was conducted to demonstratea toxic accumulation of iron in the liver, spleen, the efficacy of deferasirox versus deferoxamine inendocrine organs and myocardium. patients with β-thalassaemia aged ≥2 years who
Fortunately, iron overload may be controlled by received regular transfusions.[5] Patients wereusing a chelating agent capable of complexing with randomised to receive treatment with deferasiroxiron and promoting its excretion. Deferoxamine (n = 296) or deferoxamine (n = 290) with the dosage(Desferal®, Novartis)1 is the current standard for of each determined by baseline liver iron concentra-iron chelation therapy worldwide based on consis- tions (LIC) [i.e. for baseline LICs of 2–3, >3–7,tent evidence regarding its benefits in terms of both >7–14 and >14mg Fe/g dry weight (dw), respective-morbidity and mortality in patients with transfusion ly, dosages of 5, 10, 20 and 30 mg/kg once daily fordependent β-thalassaemia.[1] However, the poor deferasirox and 20–30, 25–35, 35–50 and ≥50 mg/bioavailability and short plasma elimination half- kg 5 days per week for deferoxamine]. The primarylife of deferoxamine require that it be administered endpoint was maintenance or reduction of LIC; sec-as a subcutaneous (SC) or intravenous (IV) infusion ondary endpoints included safety and tolerability,over an 8- to 12-hour period five to seven times per change in serum ferritin level and net body ironweek. Most patients in the US receive deferoxamine balance. Although the primary statistical endpoint ofvia SC infusions. IV administration may be necessa- noninferiority of deferasirox versus deferoxaminery for patients who cannot tolerate or adhere to SC was not met in the overall population, this was likelyinfusions, or those who need higher dose, 24-hour because of the disproportionally low doses of defer-continuous therapy (e.g. for treatment of complica- asirox administered to patients with baseline LICtions). This burdensome regimen can lead to poor <7mg Fe/g (dw) for whom doses of deferasirox andcompliance, reduced effectiveness and/or impaired deferoxamine were administered in a 1 : 4 ratio,quality of life (QOL).[2,3] compared with a 1 : 2 ratio for those with baseline
LIC >7mg Fe/g dw. Among patients with baselineUntil recently, deferoxamine was the only che->7mg Fe/g dw, deferasirox and deferoxamine result-lator commercially available in the US. Deferiproneed in significant and similar dose-dependent reduc-(Ferriprox®, Apotex), an iron chelator formulated astions in LIC and serum ferritin and improvements insolid tablets and administered three times a day, isnet body iron balance.available in the US only through the US FDA Treat-
ment Use Program, because of the increased risk of Policy decisions regarding appropriate use ofagranulocytosis and arthropathy associated with this new treatments such as deferasirox require consider-
1 The use of trade names is for product identification purposes only and does not imply endorsement.
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)

Cost Effectiveness of Deferasirox in Thalassaemia 331
ation of not only efficacy and safety, but also effec- Description of the Model and Assumptionstiveness and costs.[6] Although deferasirox and
We used a Markov model with annual transitionsdeferoxamine have been shown to be similarly effi-between the health states to project the lifetime costscacious in maintaining iron balance in controlledand survival in patients with β-thalassaemia who aretrials, their effectiveness in typical clinical practiceassumed to receive iron chelation therapy with ei-may differ because of differences in compliance andther deferasirox or deferoxamine (figure 1).QOL associated with oral versus infusional therapy.
Patients entering the model were assumed to be 3Also, the higher acquisition cost of deferasirox mayyears of age, not to have received prior chelationin part be offset by savings in the cost of infusionaltherapy, and to receive prescribed dosages of defer-therapy or treatment of complications of iron over-asirox or deferoxamine that have been shown to beload if patients receiving oral versus infusional ther-similarly effective in maintaining iron balance inapy are more compliant with iron chelation therapy.frequently-transfused thalassaemia patients (seeThe objective of this study, therefore, was toPrescribed Dosages).[5]
evaluate the cost effectiveness of deferasirox versusMortality was assumed to be dependent on agedeferoxamine in patients with β-thalassaemia major
and the presence of iron overload-related cardiacand chronic iron overload from blood transfusions,disease (cardiac arrhythmias and/or heart failure).from a US healthcare system perspective.Although other complications of iron overload mayaffect survival, cardiac disease has been shown toMethodsaccount for approximately 80% of deaths in patientswith transfusion-dependent thalassaemia.[9,10] The
Overview probability of cardiac disease (and therefore death)in each year was thus assumed to be dependent on
We used a Markov model[7] to evaluate the cost age and mean lifetime compliance with chelationeffectiveness of iron chelation therapy with defer- therapy, but to otherwise be the same for deferasiroxasirox versus deferoxamine in patients with β- and deferoxamine. This assumption is based on datathalassaemia major and chronic iron overload from showing that deferasirox and deferoxamine are sim-blood transfusions. We compared deferasirox with ilarly effective in maintaining LIC and serum ferri-deferoxamine, as the latter is the current standard of tin levels,[5] and that these factors are predictive ofcare for these patients in the US. We did not consid- complications of iron overload and survival iner deferiprone because it is not approved for wide- thalassemic patients (see also Probabilities of Ironspread use and is rarely prescribed in the US. Overload-Related Cardiac Disease and Death).[1]
For each strategy (deferasirox or deferoxamine), Compliance with chelation therapy was allowedwe used the model to calculate the expected lifetime to vary with the chelation therapy received, thuscosts of treatment of iron overload, life expectancy impacting on the risk of iron overload-related cardi-or life years (LYs) and QALYs. The incremental ac disease and death (see Compliance). Compliancecost effectiveness of deferasirox versus deferox- in any given year was defined as the ratio of theamine therapy was defined in terms of the ratio of number of doses of chelation therapy received to thethe difference in expected lifetime costs to the dif-ference in QALYs.
Our analysis was conducted from the perspectiveof the US healthcare system and therefore consid-ered only direct medical care costs. Consistent withrecommended good research practices for modellingstudies,[8] we considered only those costs related tothe disease of interest (iron overload), evaluatedoutcomes over a 50-year timeframe and discountedfuture costs and QALYs to their present value usingan annual discount rate of 3%.
Alive withoutcardiac disease
Alive with cardiac disease
Dead
Fig. 1. Schematic representation of the Markov model. Transitionsbetween health states occur annually.
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)

332 Delea et al.
Deferasiroxnumber of doses prescribed during the year. Life-Because data on compliance with deferasiroxtime compliance was calculated as the average of
were unavailable, we conservatively estimated theannual compliance values over all prior years ofimprovement in compliance that would result fromchelation therapy. For patients with many years ofusing a once-daily oral chelator versus an infusionalprior chelation therapy at suboptimal compliance,therapy based on data from a non-randomised pro-improvements in compliance were therefore as-spective study comparing the thrice-daily oral che-sumed to affect average lifetime compliance andlator, deferiprone, with deferoxamine.[12] In thatrisk of cardiac disease gradually over time.study, 54 patients with β-thalassaemia participatingin a programme of compassionate or experimental
Prescribed Dosages use of deferiprone (in some cases due to inability orunwillingness to comply with deferoxamine ther-
Prescribed dosages of deferasirox and deferox- apy) at a major thalassaemia research centre in Italyamine were estimated to be 24.6 mg/kg/day, 7 days were compared with 51 patients who continued toper week and 47.4 mg/kg/day, 5 days per week, receive SC deferoxamine. After approximately 24respectively. These estimates were based on the months, median compliance among patients receiv-mean prescribed dosages of deferasirox and defer- ing deferiprone improved by 11.4% from baselineoxamine among patients with an LIC >7mg Fe/g dw (from 88% to 98%) while compliance among pa-in the phase III deferasirox trial.[5]
tients receiving deferoxamine declined by 4.3%from baseline (from 94% to 90%).
We therefore estimated that once-daily oral che-Compliancelation with deferasirox would improve complianceby 16% (11.4% vs –4.3%) versus deferoxamine.
DeferoxamineCompliance with deferasirox was therefore estimat-
To estimate compliance with deferoxamine, we ed to be 74% (64% × 1.16), or 270 doses per yearidentified all published studies reporting compliance (5.2 per week).with deferoxamine in patients with thalassaemiamajor.[1,3,11-20] The study by Arboretti et al.[3] was by Probabilities of Iron Overload-Relatedfar the largest and represented the most diverse Cardiac Disease and Deathgroup of patients. In this study, which examined
Estimates of the annual probabilities of iron over-clinical outcomes and patient satisfaction with careload-related cardiac disease by age and degree ofin 857 thalassaemia patients seen in 16 thalassaemiacompliance, as well as the annual probabilities ofcentres in Italy, physician-assessed compliance wasdeath from iron overload-related cardiac disease andestimated to be <50% in 9% of patients, 50–80% inother causes were estimated as follows.27% of patients and >80% in 65% of patients. The
First, we assumed that the risk function for ironsecond largest study[1] reported that, among 257overload-related cardiac disease would be in theconsecutive patients seen at a centre in Italy over 30form of a shifted Weibull distribution.[22] Theyears, the compliance rate was >70% in 58% ofWeibull distribution represents a flexible risk func-patients.[1] Assuming that compliance would be uni-tion that allows for increasing or decreasing risk offormly distributed within the categories of compli-events over time. Changes in the values of indepen-ance reported in these studies, the mean compliancedent variables, such as compliance, are assumed torate in these studies can be estimated to be 77% andresult in proportional changes in annual risk. With64%, respectively. Results for other observationalthe addition of a third waiting-time parameter, thestudies were generally similar.[14,18-20] Because phy-‘shifted’ Weibull function allows for an initial peri-sicians may overestimate actual patient compli-od during which no events may occur.ance,[21] we used the lesser of these values, i.e. we
assumed that compliance with deferoxamine in typi- Second, we assumed that the mortality rate aftercal clinical practice would be 64% (166 infusions development of cardiac disease was approximatelyannually). 16% annually, based on data from a study of 52
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)
Cost Effectiveness of Deferasirox in Thalassaemia 333
Greek thalassaemia patients with recent-onset heart Costsfailure of whom 49% were alive after 4 years.[23]
Third, we assumed that patients without cardiac Base-case estimates of costs are described below.disease have a risk of non-cardiac death that is All costs are expressed as $US (year 2006 val-proportional to that of age-matched subjects in the ues).[25]
general population.[24] Finally, we assumed that pa-tients receiving 365 deferoxamine infusions annual- Drug Costsly would have no excess risk of cardiac disease- The unit costs of deferasirox ($US89.49 perrelated mortality compared with age-matched sub- gram) and deferoxamine ($US35.77 per gram) werejects in the general population. estimated based on the wholesale acquisition cost
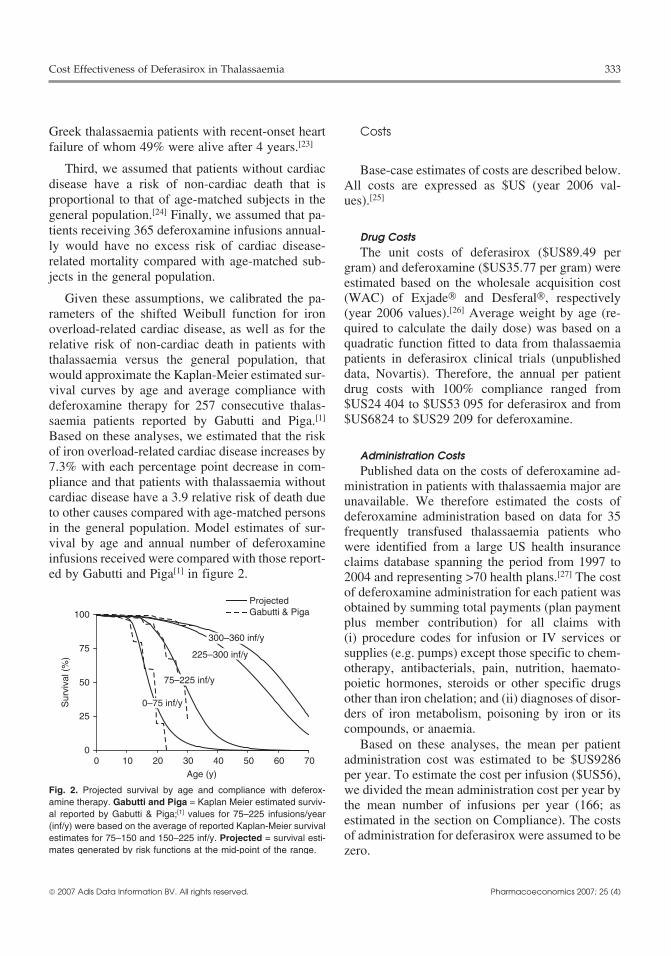
(WAC) of Exjade® and Desferal®, respectivelyGiven these assumptions, we calibrated the pa-(year 2006 values).[26] Average weight by age (re-rameters of the shifted Weibull function for ironquired to calculate the daily dose) was based on aoverload-related cardiac disease, as well as for thequadratic function fitted to data from thalassaemiarelative risk of non-cardiac death in patients withpatients in deferasirox clinical trials (unpublishedthalassaemia versus the general population, thatdata, Novartis). Therefore, the annual per patientwould approximate the Kaplan-Meier estimated sur-drug costs with 100% compliance ranged fromvival curves by age and average compliance with$US24 404 to $US53 095 for deferasirox and fromdeferoxamine therapy for 257 consecutive thalas-$US6824 to $US29 209 for deferoxamine.saemia patients reported by Gabutti and Piga.[1]
Based on these analyses, we estimated that the riskof iron overload-related cardiac disease increases by Administration Costs7.3% with each percentage point decrease in com- Published data on the costs of deferoxamine ad-pliance and that patients with thalassaemia without ministration in patients with thalassaemia major arecardiac disease have a 3.9 relative risk of death due unavailable. We therefore estimated the costs ofto other causes compared with age-matched persons deferoxamine administration based on data for 35in the general population. Model estimates of sur- frequently transfused thalassaemia patients whovival by age and annual number of deferoxamine were identified from a large US health insuranceinfusions received were compared with those report- claims database spanning the period from 1997 toed by Gabutti and Piga[1] in figure 2. 2004 and representing >70 health plans.[27] The cost
of deferoxamine administration for each patient wasobtained by summing total payments (plan paymentplus member contribution) for all claims with(i) procedure codes for infusion or IV services orsupplies (e.g. pumps) except those specific to chem-otherapy, antibacterials, pain, nutrition, haemato-poietic hormones, steroids or other specific drugsother than iron chelation; and (ii) diagnoses of disor-ders of iron metabolism, poisoning by iron or itscompounds, or anaemia.
Based on these analyses, the mean per patientadministration cost was estimated to be $US9286per year. To estimate the cost per infusion ($US56),we divided the mean administration cost per year bythe mean number of infusions per year (166; asestimated in the section on Compliance). The costsof administration for deferasirox were assumed to bezero.
0
25
50
75
100
0 10 20 30 40 50 60 70Age (y)
ProjectedGabutti & Piga
Sur
viva
l (%
)
300–360 inf/y
225–300 inf/y
75–225 inf/y
0–75 inf/y
Fig. 2. Projected survival by age and compliance with deferox-amine therapy. Gabutti and Piga = Kaplan Meier estimated surviv-al reported by Gabutti & Piga;[1] values for 75–225 infusions/year(inf/y) were based on the average of reported Kaplan-Meier survivalestimates for 75–150 and 150–225 inf/y. Projected = survival esti-mates generated by risk functions at the mid-point of the range.
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)

334 Delea et al.
Table I. Base-case values of the model parameters
Parameter Value
Prescribed dosages
deferasirox[5] 24.6 mg/kg/day every day of the week
deferoxamine[5] 47.4 mg/kg/day for 5 days of each week
Compliance (%)
deferoxamine[1] 64
deferasirox[12] 74
Annual mortality with cardiac disease (%) 16
Costs ($US, year 2006 values)
deferasirox, per gram[26] 89.49
deferoxamine, per gram[26] 35.77
deferasirox administration 0
deferoxamine administration, per infusion[1,27] 56.00
treatment of iron overload-related cardiac disease, per year[27] 14 770
Utility values (relative decrease, %)
no chelation vs perfect health[28] –15
deferasirox vs perfect health[28] –15
deferoxamine vs deferasirox[28] –28
iron overload-related cardiac disease vs no cardiac disease[29] –15
Cost of Iron Overload-Related Cardiac Disease infusion or once-daily oral iron chelation therapyWe estimated the mean annual cost of treatment that they would be willing to trade off for 10 years of
of iron overload-related cardiac disease based on the life with perfect health. Preliminary results based onanalysis of 35 frequently transfused thalassaemia the first 110 respondents showed an average utilitypatients (see Administration Costs).[27] Of these pa- value of 0.85 (95% CI 0.81, 0.89) for the once-dailytients, 16 had evidence of iron overload-related car-
oral iron chelator scenario versus 0.61 (95% CI 0.56,diac disease based on (i) medical claims with a0.66) for the SC infused iron chelator scenario.diagnosis of cardiomyopathy, conduction disorders,
We therefore assumed that patients receivingcardiac dysrhythmias or heart failure; or (ii) pharma-cy claims for β-adrenoceptor antagonists (β-block- deferasirox and deferoxamine would have 15% anders), ACE inhibitors, diuretics or antiarrhythmics. 39% reductions in utility compared with perfect
For these patients, the mean annual per patient health, respectively.payment for cardiac disease-related care was Although the use of deferasirox has been report-$US14 770.
ed to be associated with rash and gastrointestinaldisturbances, these adverse events are generally
Quality of Life transient.[5] Adverse effects associated with the useof deferasirox were therefore assumed to have no
Utilities for patients receiving deferasirox versus negative impact on QOL.deferoxamine were obtained from a study that used Patients with cardiac disease were assumed totime-trade-off (TTO) techniques to measure patient
have a 15% decrement in utility based on TTOpreferences for oral versus infusional chelation ther-
values for heart failure as reported in the Beaverapy.[28] In this study, a community sample of 120Dam Health Outcomes study,[29] a longitudinal co-adults in Australia participated in a TTO exercise tohort study of health status and health-related QOLelicit utility values, or preferences, for different(HR-QOL) for a random sample of 1356 US adultsmodes of administration of chelation therapy. Par-in a community population. Base-case values forticipants were queried to identify the number ofmodel parameters are summarised in table I.years of life with thalassaemia treated with either SC
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)
Cost Effectiveness of Deferasirox in Thalassaemia 335
Analyses therapy versus deferasirox (range 0–40%, base-casevalue 28%) in order to identify the relative contribu-tion of improvements in compliance versus QOL onBase-Case Analysesthe cost effectiveness of deferasirox.For each strategy, we calculated the expected
proportion of patients who would develop iron over-Probabilistic Sensitivity Analyses
load-related cardiac disease, the expected costs ofWe constructed 10 000 sets of probability andchelation therapy (drug and administration [deferox-
cost estimates by simultaneously sampling from es-amine only]), the expected costs of treatment of irontimated probability distributions of the key modeloverload-related cardiac disease, total costs (chela-parameters.[30] Probability estimates were assumedtion therapy plus cardiac disease), cardiac disease-to be distributed as beta random variables. Otherfree LYs, overall LYs, QALYs and cost effective-estimates were assumed to be distributed as Normalness.random variables. Estimates for which distributional
Deterministic Sensitivity Analyses information were unavailable were assumed to havelower bounds of 95% confidence intervals equal toOne-way sensitivity analyses were performed50% of base-case estimates.with model probabilities, and costs were varied over
their plausible ranges. Results were also generated For each simulation, we calculated expected life-by age at initiation of deferasirox therapy (assuming time costs and QALYs for each strategy, along withall patients initiated deferoxamine at 5 years of age) the differences between strategies in costs andand for alternative model timeframes ranging from 5 QALYs. The resulting estimates were then arrayedto 100 years. on a cost-effectiveness plane, and a cost-effective-
ness acceptability curve was constructed for defer-We calculated the break-even prices for defer-asirox versus deferoxamine to identify the propor-asirox (i.e. the prices at which total costs would betion of simulations for which deferasirox would bethe same as that for deferoxamine) under our base-preferred given various levels of decision-makers’case assumptions and assuming no improvement inwillingness to pay (WTP) for a QALY.compliance with deferasirox. We conducted a two-
way sensitivity analysis on the estimated improve- The model was programmed using Microsoft Ex-ment in compliance with deferasirox (range 0–25%, cel® and validated with a model developed withbase-case value 16%) versus deferoxamine and the TreeAge Data® Version 4.0 decision analysisestimated disutility associated with deferoxamine software (Williamstown, MA, USA).
Table II. Results from the base-case analyses
Outcome measure Deferasirox Deferoxamine Difference
Iron overload-related cardiac disease (% of patients) 90.9 95.0 –4.1
Cardiac disease-free life-years 29.3 24.0 5.4
Life-years
not discounted 34.4 29.6 4.8
discounted 21.0 19.3 1.8
QALYs
not discounted 28.6 20.1 8.5
discounted 17.6 13.2 4.5
Costs ($US, 2006 values)
Chelation therapy
drug 536 692 222 869 313 823
administration 0 179 331 –179 331
total 536 692 402 200 134 492
Iron overload-related cardiac disease 34 464 42 939 –8 474
Total 571 156 445 139 126 018
Cost per QALY gained ($US) 28 255
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)
336 Delea et al.
Sur
viva
l (%
)
Qua
lity-ad
justed
sur
viva
l (%
)
5 15 25 35 45 55
Age (y)
0
25
50
75
100
5 15 25 35 45 55
DeferasiroxDeferoxamine
a b
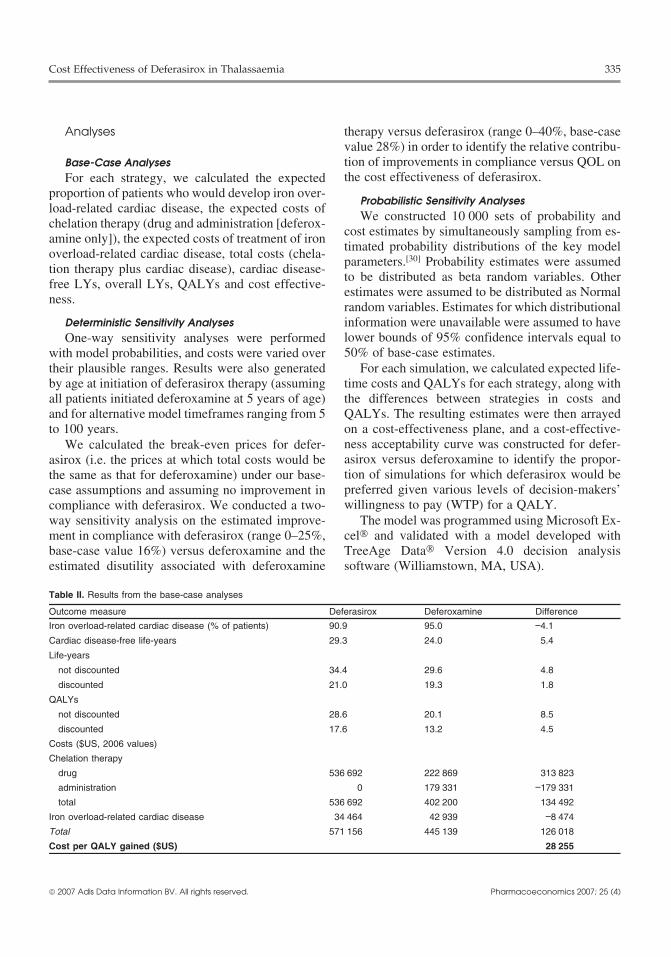
Fig. 3. Projected overall (a) and quality-adjusted survival (b) by age and chelation therapy received; areas between the survival curvesrepresent gains in life expectancy and quality-adjusted life expectancy, respectively, with deferasirox vs deferoxamine (not discounted).
Results therefore estimated to be $US28 255 per QALYgained.
Base-Case AnalysesDeterministic Sensitivity Analyses
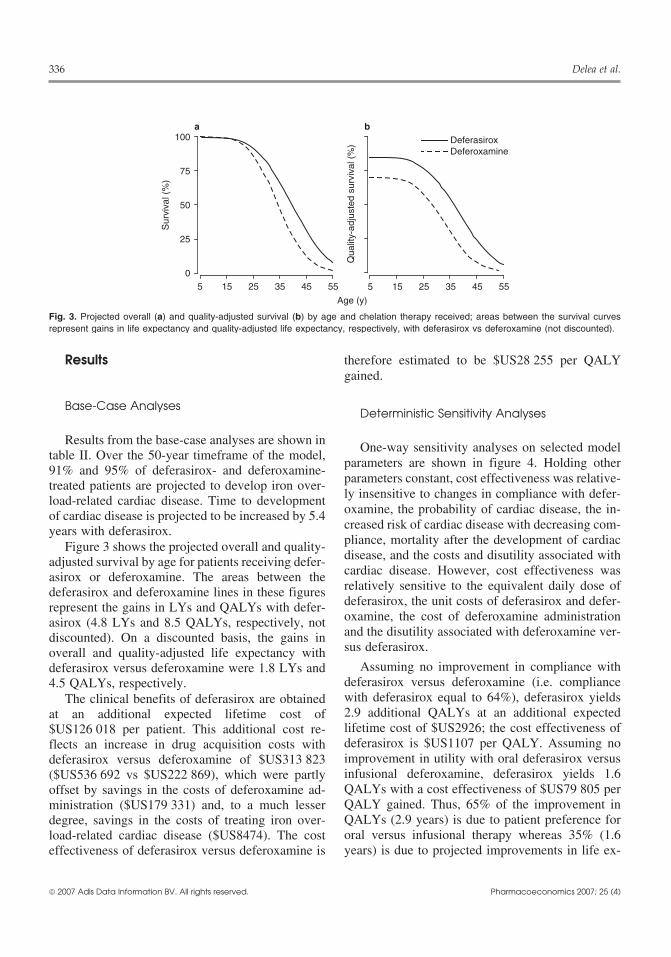
Results from the base-case analyses are shown in One-way sensitivity analyses on selected modeltable II. Over the 50-year timeframe of the model,
parameters are shown in figure 4. Holding other91% and 95% of deferasirox- and deferoxamine-
parameters constant, cost effectiveness was relative-treated patients are projected to develop iron over-ly insensitive to changes in compliance with defer-load-related cardiac disease. Time to developmentoxamine, the probability of cardiac disease, the in-of cardiac disease is projected to be increased by 5.4creased risk of cardiac disease with decreasing com-years with deferasirox.pliance, mortality after the development of cardiacFigure 3 shows the projected overall and quality-disease, and the costs and disutility associated withadjusted survival by age for patients receiving defer-cardiac disease. However, cost effectiveness wasasirox or deferoxamine. The areas between therelatively sensitive to the equivalent daily dose ofdeferasirox and deferoxamine lines in these figuresdeferasirox, the unit costs of deferasirox and defer-represent the gains in LYs and QALYs with defer-oxamine, the cost of deferoxamine administrationasirox (4.8 LYs and 8.5 QALYs, respectively, notand the disutility associated with deferoxamine ver-discounted). On a discounted basis, the gains insus deferasirox.overall and quality-adjusted life expectancy with
Assuming no improvement in compliance withdeferasirox versus deferoxamine were 1.8 LYs anddeferasirox versus deferoxamine (i.e. compliance4.5 QALYs, respectively.with deferasirox equal to 64%), deferasirox yieldsThe clinical benefits of deferasirox are obtained2.9 additional QALYs at an additional expectedat an additional expected lifetime cost oflifetime cost of $US2926; the cost effectiveness of$US126 018 per patient. This additional cost re-deferasirox is $US1107 per QALY. Assuming noflects an increase in drug acquisition costs withimprovement in utility with oral deferasirox versusdeferasirox versus deferoxamine of $US313 823infusional deferoxamine, deferasirox yields 1.6($US536 692 vs $US222 869), which were partlyQALYs with a cost effectiveness of $US79 805 peroffset by savings in the costs of deferoxamine ad-QALY gained. Thus, 65% of the improvement inministration ($US179 331) and, to a much lesserQALYs (2.9 years) is due to patient preference fordegree, savings in the costs of treating iron over-oral versus infusional therapy whereas 35% (1.6load-related cardiac disease ($US8474). The costyears) is due to projected improvements in life ex-effectiveness of deferasirox versus deferoxamine is
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)

Cost Effectiveness of Deferasirox in Thalassaemia 337
pectancy associated with reduced complications of tive) if the value of this parameter is set to half theiron overload. base-case value (12.3 mg/kg/day).
Under our base-case assumptions, the break-even The cost effectiveness of deferasirox versusprice for deferasirox is approximately $US69 per deferoxamine is most favourable in younger pa-gram. Assuming no improvement in compliance tients, increasing from $US28 255 per QALYversus deferoxamine, the break-even price is $US89 gained for patients aged 3 years at initiation ofper gram. therapy to $US76 459 per QALY gained for patients
aged 40 years at initiation of therapy. This findingThe cost effectiveness of deferasirox isreflects the shorter life expectancy of older patients,$US39 110 per QALY gained if the unit cost ofas well as increasing absolute difference in druggeneric deferoxamine is employed ($US28 percosts with increasing age and patient weight. Thegram),[26] and $US68 464 per QALY gained if thecost effectiveness of deferasirox increases with in-cost of deferoxamine administration is set to zero.creasing model timeframes, ranging from defer-Expected lifetime costs with deferasirox are lessasirox is dominant for a model timeframe of 10than those with deferoxamine if the cost of deferox-years to approximately $US29 000 per QALYamine administration is >$US69 per infusion. Costgained for model timeframes of ≥50 years. Thiseffectiveness is $US88 422 per QALY gained if thefinding is largely a consequence of less favourabledaily dose of deferasirox (24.6 mg/kg/day sevencost effectiveness with increasing patient age.times per week), which is equivalent to 47.4 mg/kg/
day deferoxamine five times per week, is set to Figure 5 presents a two-way sensitivity analysis1.5-fold its base-case value (36.9 mg/kg/day). on (i) the improvement in compliance with defer-Deferasirox is dominant (less costly and more effec- asirox versus deferoxamine and (ii) the disutility
50% 100%
64% 100%
2.0 xbase-case
0.25 xbase-case
14.68 0
10% 20%
12.3 36.9
35.77 0
35.77 89.49
84 0
$0 29 540
0% 30%
50% 0%
Compliance with deferoxamine (64%)
Compliance with deferasiox (74%)
Annual probabilities of cardiac disease (multiple values)
Annual mortality with cardiac disease (16%)
Daily dose: deferasirox (24.6 mg/kg/day)[equivalent to deferoxamine 47.4 mg/kg/day]
Cost of deferoxamine per g (35.77)
Cost of deferasirox per g (89.49)
Cost of deferoxamine administration per infusion (56)
Annual cost of cardiac disease (14 770)
Disutility for β-thalassemia and no chelation (15%)
Disutility for deferoxamine vs deferasirox (28%)
Disutility with cardiac disease (15%) 30% 0%
8
1
26
22
28
28
19
26
24
21
28
57
30
32
28
88
78
28
68
30
34
80
28
21
0 25 50 75 100
Cost per QALY gained ($US × 1000)
dominant
dominant
Increase in risk of cardiac disease per 1%increase in compliance (7.34)
Fig. 4. One-way sensitivity analyses on selected model parameters. The figure shows how the cost per QALY gained (year 2006 values)with deferasirox vs deferoxamine changes as individual model parameters are changed while holding all other parameters constant. Thebase-case value for each parameter (where applicable) is shown in parentheses. The values at the end of the bars represent the cost perQALY gained given the corresponding value of parameter. The base-case estimate of cost effectiveness is represented by the vertical line.
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)
338 Delea et al.
increases, the benefits of deferasirox versus deferox-amine are increasingly a consequence of improvedlife expectancy (due to better chelation) rather thanto improved QOL (due to the use of an oral versusinfusional chelator). The comparison of deferasiroxversus deferoxamine therefore increasingly be-comes one of deferasirox versus no chelation (be-cause patients who are not compliant receive nochelation).
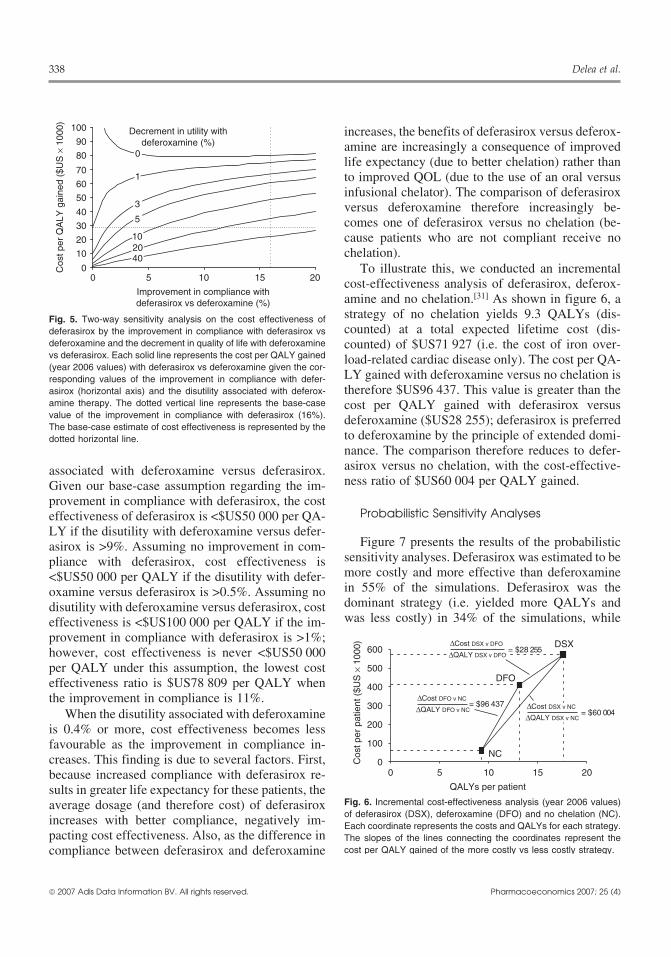
To illustrate this, we conducted an incrementalcost-effectiveness analysis of deferasirox, deferox-amine and no chelation.[31] As shown in figure 6, astrategy of no chelation yields 9.3 QALYs (dis-counted) at a total expected lifetime cost (dis-counted) of $US71 927 (i.e. the cost of iron over-load-related cardiac disease only). The cost per QA-LY gained with deferoxamine versus no chelation istherefore $US96 437. This value is greater than thecost per QALY gained with deferasirox versusdeferoxamine ($US28 255); deferasirox is preferredto deferoxamine by the principle of extended domi-
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20
Improvement in compliance withdeferasirox vs deferoxamine (%)
Cos
t per
QA
LY gai
ned
($U
S ×
100
0)
5
1020
3
40
Decrement in utility withdeferoxamine (%)
0
1
Fig. 5. Two-way sensitivity analysis on the cost effectiveness ofdeferasirox by the improvement in compliance with deferasirox vsdeferoxamine and the decrement in quality of life with deferoxaminevs deferasirox. Each solid line represents the cost per QALY gained(year 2006 values) with deferasirox vs deferoxamine given the cor-responding values of the improvement in compliance with defer-asirox (horizontal axis) and the disutility associated with deferox-amine therapy. The dotted vertical line represents the base-casevalue of the improvement in compliance with deferasirox (16%).The base-case estimate of cost effectiveness is represented by thedotted horizontal line.
nance. The comparison therefore reduces to defer-asirox versus no chelation, with the cost-effective-associated with deferoxamine versus deferasirox.ness ratio of $US60 004 per QALY gained.Given our base-case assumption regarding the im-
provement in compliance with deferasirox, the costProbabilistic Sensitivity Analyseseffectiveness of deferasirox is <$US50 000 per QA-
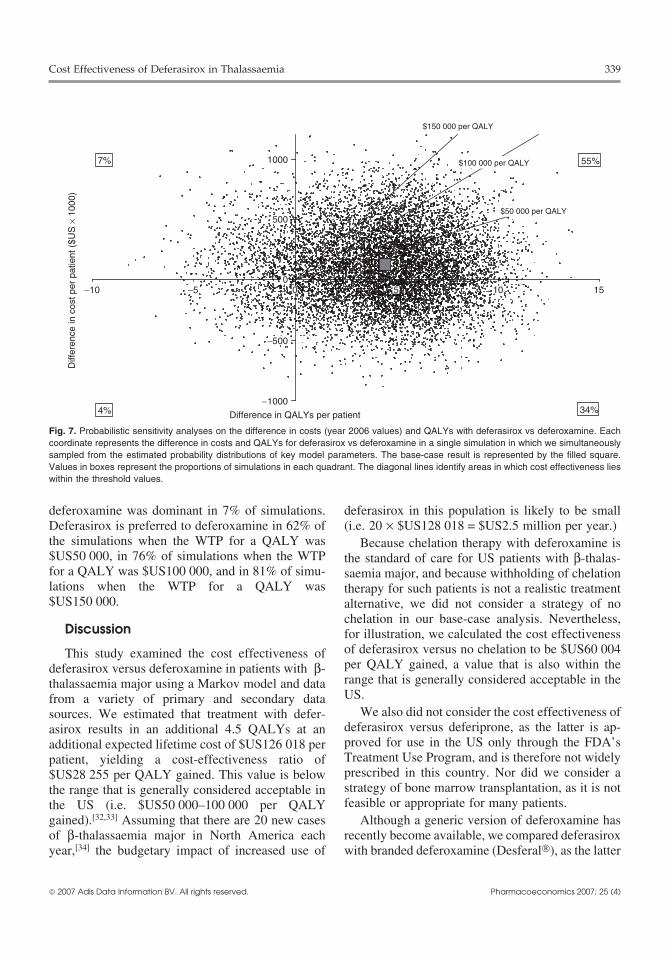
LY if the disutility with deferoxamine versus defer-Figure 7 presents the results of the probabilisticasirox is >9%. Assuming no improvement in com-
sensitivity analyses. Deferasirox was estimated to bepliance with deferasirox, cost effectiveness ismore costly and more effective than deferoxamine<$US50 000 per QALY if the disutility with defer-in 55% of the simulations. Deferasirox was theoxamine versus deferasirox is >0.5%. Assuming nodominant strategy (i.e. yielded more QALYs anddisutility with deferoxamine versus deferasirox, costwas less costly) in 34% of the simulations, whileeffectiveness is <$US100 000 per QALY if the im-
provement in compliance with deferasirox is >1%;however, cost effectiveness is never <$US50 000per QALY under this assumption, the lowest costeffectiveness ratio is $US78 809 per QALY whenthe improvement in compliance is 11%.
When the disutility associated with deferoxamineis 0.4% or more, cost effectiveness becomes lessfavourable as the improvement in compliance in-creases. This finding is due to several factors. First,because increased compliance with deferasirox re-sults in greater life expectancy for these patients, theaverage dosage (and therefore cost) of deferasiroxincreases with better compliance, negatively im-pacting cost effectiveness. Also, as the difference incompliance between deferasirox and deferoxamine
0
100
200
300
400
500
600
0 5 10 15 20
QALYs per patient
Cos
t per
pat
ient
($U
S ×
100
0)
DFO
DSX
NC
= $60 004Cost DSX v NC
∇
QALY DSX v NC
∇
= $28 255Cost DSX v DFO
∇
QALY DSX v DFO
∇
Cost DFO v NC
∇
QALY DFO v NC
∇ = $96 437
Fig. 6. Incremental cost-effectiveness analysis (year 2006 values)of deferasirox (DSX), deferoxamine (DFO) and no chelation (NC).Each coordinate represents the costs and QALYs for each strategy.The slopes of the lines connecting the coordinates represent thecost per QALY gained of the more costly vs less costly strategy.
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)
Cost Effectiveness of Deferasirox in Thalassaemia 339
Difference in QALYs per patient
Differen
ce in
cos
t per
patient
($U
S ×
100
0)
34%4%
55%7%
$150 000 per QALY
1000
500
−500
−10 −5 0 5 10 15
−1000
0
$100 000 per QALY
$50 000 per QALY
Fig. 7. Probabilistic sensitivity analyses on the difference in costs (year 2006 values) and QALYs with deferasirox vs deferoxamine. Eachcoordinate represents the difference in costs and QALYs for deferasirox vs deferoxamine in a single simulation in which we simultaneouslysampled from the estimated probability distributions of key model parameters. The base-case result is represented by the filled square.Values in boxes represent the proportions of simulations in each quadrant. The diagonal lines identify areas in which cost effectiveness lieswithin the threshold values.
deferoxamine was dominant in 7% of simulations. deferasirox in this population is likely to be smallDeferasirox is preferred to deferoxamine in 62% of (i.e. 20 × $US128 018 = $US2.5 million per year.)the simulations when the WTP for a QALY was Because chelation therapy with deferoxamine is$US50 000, in 76% of simulations when the WTP the standard of care for US patients with β-thalas-for a QALY was $US100 000, and in 81% of simu- saemia major, and because withholding of chelationlations when the WTP for a QALY was therapy for such patients is not a realistic treatment$US150 000. alternative, we did not consider a strategy of no
chelation in our base-case analysis. Nevertheless,Discussion for illustration, we calculated the cost effectiveness
of deferasirox versus no chelation to be $US60 004This study examined the cost effectiveness ofper QALY gained, a value that is also within thedeferasirox versus deferoxamine in patients with β-range that is generally considered acceptable in thethalassaemia major using a Markov model and dataUS.from a variety of primary and secondary data
We also did not consider the cost effectiveness ofsources. We estimated that treatment with defer-deferasirox versus deferiprone, as the latter is ap-asirox results in an additional 4.5 QALYs at anproved for use in the US only through the FDA’sadditional expected lifetime cost of $US126 018 perTreatment Use Program, and is therefore not widelypatient, yielding a cost-effectiveness ratio ofprescribed in this country. Nor did we consider a$US28 255 per QALY gained. This value is belowstrategy of bone marrow transplantation, as it is notthe range that is generally considered acceptable infeasible or appropriate for many patients.the US (i.e. $US50 000–100 000 per QALY
gained).[32,33] Assuming that there are 20 new cases Although a generic version of deferoxamine hasof β-thalassaemia major in North America each recently become available, we compared deferasiroxyear,[34] the budgetary impact of increased use of with branded deferoxamine (Desferal®), as the latter
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)

340 Delea et al.
is currently more widely used in the US. Sensitivity improvement in compliance with deferasirox versusanalyses suggest that the cost per QALY gained deferoxamine to be 16% based on published datawith deferasirox would be approximately comparing compliance with deferiprone with defer-$US39 110 if the unit cost of generic deferoxamine oxamine.[12] This estimate may be conservative, aswas employed ($US28 per gram). compliance with a once-daily oral agent (defer-
asirox) would be expected to be better than that withStudy Limitations a thrice-daily oral chelator (deferiprone).
This analysis did not consider the potential ad-Limitations of our study should be noted. First,verse effects of deferasirox. Although patients re-the cost effectiveness of deferasirox versus deferox-ceiving deferasirox in the pivotal study of this agentamine was sensitive to the estimated cost of deferox-had an increased incidence of rash and gastrointesti-amine administration. Our estimate of this costnal disturbances, these events were transient and($US56 per infusion) was based on an analysis of agenerally resolved without discontinuation of ther-relatively small sample (n = 35) of frequently trans-apy.[5] Consideration of these effects, therefore,fused thalassaemia patients in a variety of US man-would not have been likely to affect our conclusions.aged care plans.[27] Although we know of no otherNor did we consider the potential adverse effects ofpublished estimates of the cost of deferoxaminedeferoxamine, such as high-frequency hearing loss,administration in transfusion-dependent thalas-Yersinia infections, severe local reactions, or infec-saemia patients, our estimate of the monthly cost oftions resulting from central venous access devicesdeferoxamine administration with full compliance(CVADs). Although potentially life-threatening,($US1213) is less than contracted rates for homeYersinia infection is relatively rare (7.4/1000),[1] andinfusion services reported for five large health plansits severity can be limited by rapid diagnosis andin the Pacific Northwest Region ($US1400–3100treatment. In a study of 342 patients in the Registryper month).[35] Our estimate is also within the rangeof the National Institutes of Health-sponsoredof administration costs reported for multiply trans-Thalassaemia Clinical Research Network (TCRN),fused patients (predominantly with sickle cell dis-18% of patients receiving deferoxamine exper-ease or Diamond-Blackfan syndrome) receivingienced high-frequency hearing loss, and 9% hadchelation therapy at a California Children’s hospitalsevere local reactions, including 5% who required($US464–1324).[36] Our estimated annual adminis-CVADs as a consequence.[38] Overall, 22% of pa-tration cost with typical compliance ($US9286) istients in this study required CVADs, and 43% ofconsistent with administration costs reported in athese experienced infections related to the device.recent naturalistic cohort study of 49 patientsGiven the potentially serious clinical and economic(thalassaemia: n = 40; sickle cell disease: n = 9) re-consequences of these events, our estimates of theceiving deferoxamine at four US sites in whichcost effectiveness of deferasirox may be conserva-resource use was estimated based on patient inter-tive.views and charts.[37] In this latter study, the costs of
infusions in healthcare settings ($US1766), home We estimated the decrement in QOL associateddelivery ($US70) and equipment ($US3293) to- with the use of deferoxamine versus deferasiroxtalled $US5129 per year. Home healthcare costs, of based on results of a study of community-basedwhich some proportion was likely to be related to preferences for oral versus infusional chelation ther-chelation therapy, were an additional $US7232 an- apy among Australian adults.[28] Although thenually. generalisability of these estimates to US patients is
Our estimate of compliance with deferoxamine uncertain, the estimated decrement in QOL obtained(64% or 166 infusions per year) was based on results in this study (28% decline for SC vs oral chelation)of a single Italian cohort study.[1] Compliance in this was similar to that obtained in a US study comparingstudy may not be representative of that among patient preferences for infusional versus oralthalassaemia patients seen in typical US clinical ganciclovir for AIDS-related cytomegalovirus reti-practice. Also, because we lacked data on compli- nitis (30% for IV vs oral ganciclovir).[39] Also, theance with deferasirox, we estimated the expected sensitivity analyses suggested that the cost per QA-
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)

Cost Effectiveness of Deferasirox in Thalassaemia 341
7. Sonnenberg FA, Beck JR. Markov models in medical decisionLY gained with deferasirox is generallymaking: a practical guide. Med Decis Making 1993; 13 (4):
<$US50 000 when the estimated improvement in 322-388. Weinstein MC, O’Brien B, Hornberger J, et al. Principles ofQOL with deferasirox versus deferoxamine is
good practice for decision analytic modeling in health-care>19%. Such an improvement is reasonable given the evaluation: report of the ISPOR Task Force on Good ResearchPractices. Modeling studies. Value Health 2003; 6 (1): 9-17data showing greater patient satisfaction, conve-
9. Borgna-Pignatti C, Rugolotto S, De Stefano P, et al. Survivalnience ratings, preferences for continued treatmentand complications in patients with thalassemia major treated
and less negative impact on activities of daily living with transfusion and deferoxamine. Haematologica 2004; 89(10): 1187-93with deferasirox versus deferoxamine.[40]
10. Zurlo MG, De Stefano P, Borgna-Pignatti C, et al. Survival andcauses of death in thalassaemia major. Lancet 1989; 2 (8653):
Conclusion 27-3011. Pennell DJ, Berdoukas V, Karagiorga M, et al. Randomized
controlled trial of deferiprone or deferoxamine in beta-thalas-Deferasirox is a novel iron chelator that has beensemia major patients with asymptomatic myocardial siderosis.
shown to have efficacy and safety similar to that Blood 2006 May 1; 107 (Epub 2005 Dec 13): 3738-4412. Fischer R, Longo F, Nielsen P, et al. Monitoring long-termwith deferoxamine in patients with β-thalassaemia
efficacy of iron chelation therapy by deferiprone and desferri-major. Results of this analysis of the cost effective- oxamine in patients with beta-thalassaemia major: applicationof SQUID biomagnetic liver susceptometry. Br J Haematolness of oral deferasirox versus infusional deferox-2003; 121 (6): 938-48amine suggest that deferasirox is a cost effective
13. Piga A, Gagliotti C, Fogliacco E, et al. Comparative effects ofiron chelator from a US healthcare perspective, and deferiprone and deferoxamine on survival and cardiac disease
in patients with thalassemia major: a retrospective analysis.should be considered in patients who are appropriateHaematologica 2003; 88: 489-96candidates for such therapy. 14. Boturao-Neto E, Marcopito LF, Zago MA. Urinary iron excre-tion induced by intravenous infusion of deferoxamine in beta-thalassemia homozygous patients. Braz J Med Biol Res 2002;Acknowledgements35 (11): 1319-28
15. Maggio A, D’Amico G, Morabito A, et al. Deferiprone versusFunding for this study was provided by Novartis deferoxamine in patients with thalassemia major: a random-
Pharmaceuticals Corporation, East Hanover, NJ, USA. TE ized clinical trial. Blood Cells Mol Dis 2002; 28: 196-208Delea and O Sofrygin are employees of Policy Analysis Inc. 16. Ward A, Caro JJ, Green TC, et al. An international survey of
patients with thalassemia major and their views about sus-(PAI), an independent contract research organisation, whichtaining life-long desferrioxamine use. BMC Clin Pharmacolhas received research support and consulting fees from2002; 2: 3Novartis. TE Delea has also received speaker honorarium
17. Taher A, Sheikh-Taha M, Koussa S, et al. Comparison betweenfrom Novartis. SK Thomas and J-F Baladi are employees of deferoxamine and deferiprone (L1) in iron-loaded thalassemiaNovartis and own stock and/or stock options in Novartis. PD patients. Eur J Haematol 2001; 67 (1): 30-4Phatak has received consulting fees from PAI and honoraria 18. Richardson ME, Matthews RN, Alison JF, et al. Prevention offrom Novartis, and has served on advisory boards for Novar- heart disease by subcutaneous desferrioxamine in patients with
thalassaemia major. Aust N Z J Med 1993; 23: 656-61tis. TD Coates has received consulting fees, research funding19. Beratis S. Noncompliance with iron chelation therapy in pa-and honoraria from Novartis, has participated on advisory
tients with beta thalassaemia. J Psychosom Res 1989; 33:boards for Novartis, and is a member of the University739-45
Childrens Medical Group Speakers Bureau. 20. Wolfe L, Olivieri N, Sallan D, et al. Prevention of cardiacdisease by subcutaneous deferoxamine in patients with thalas-semia major. N Engl J Med 1985; 312 (25): 1600-3
References 21. Murri R, Antinori A, Ammassari A, et al. AdICoNA Study1. Gabutti V, Piga A. Results of long-term iron-chelating therapy. Group. Physician estimates of adherence and the patient-physi-
Acta Haematol 1996; 95: 26-36 cian relationship as a setting to improve adherence to antire-2. Cohen A. Management of iron overload in the pediatric patient. troviral therapy. J Acquir Immune Defic Syndr 2002 Dec 15;
Hematol Oncol Clin North Am 1987; 3: 521-44 31 Suppl. 3: S158-62.3. Arboretti R, Tognoni G, Alberti D. Pharmacosurveillance and 22. Kalbfleisch JD, Prentic RL. The statistical analysis of failure
quality of care of thalassaemic patients. Eur J Clin Pharmacol time data. New York: John Wiley & Sons, Inc., 19802001; 56: 915-22 23. Kremastinos DT, Tsetsos GA, Tsiapras DP, et al. Heart failure
4. Nick H-P, Acklin P, Lattmann R, et al. Development of triden- in beta thalassemia: a 5-year follow-up study. Am J Med 2001;tate iron chelators: from desferrithiocin to ICL670. Curr Med 111 (5): 349-54Chem 2003; 10: 1065-76 24. Anderson RN. United States life tables, 1998. National Vital
5. Cappellini MD, Cohen A, Piga A, et al. A phase III study of Statistics Reports 2001; 48 (18) [online]. Available from URL:deferasirox (ICL670), a once-daily oral iron chelator, in pa- http://www.cdc.gov [Accessed 2006 Jun 21]tients with . Blood 2006; 107 (9): 3455-62 25. Bureau of Labor Statistics. Consumer price index. Washington,
6. Weinstein MC, Toy EL, Sandberg EA, et al. Modeling for DC: US Department of Labor, 2006 [online]. Available fromhealth care and other policy decisions: uses, roles, and validity. URL: http://data.bls.gov/cgi-bin/surveymost [Accessed 2006Value Health 2001; 4 (5): 348-61 Mar 5]
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)

342 Delea et al.
26. Red Book Update December 2006. Montvale (NJ): Thomson line]. Available from URL: http://www.regencerx.com/learn/Healthcare Inc., 2005 physicianRx/index.html [Accessed 2006 Nov 12]
27. Delea TE, Sofrygin O, Baladi J-F, et al. Costs and consequences 36. DeSwarte-Wallace J, Groncy PK, Finkelstein JZ. Iron chelationof inadequate compliance with deferoxamine therapy in pa-
with deferoxamine: comparing the results of a critical pathwaytients with transfusion-dependent thalassemia: session typeto a national survey. J Pediatr Hematol Oncol 1999; 21 (2):[abstract 3134]. Blood 2005; 106 (11 Pt 1): 877a136-4128. De Abreu Lourenco R, Osborne R, Dalton A, et al. An oral iron
chelator and quality of life [abstract 5553]. Blood 2005, 106 37. Payne KA, Desrosiers MP, Proskorovsky I, et al. Total annual(11 Part 2) costs of infused iron chelation therapy in the United states
29. Fryback DG, Dasbach EJ, Klein R, et al. The Beaver Dam [abstract 3360]. Poster presented at the American Society ofHealth Outcomes Study: initial catalog of health-state quality
Hematology 2006 Annual Meeting; 2006 Dec 11; Orlandofactors. Med Decis Making 1993; 13 (2): 89-10238. Cunningham MJ, Macklin EA, Neufeld EJ, et al. Thalassemia30. Briggs AH. A bayesian approach to stochastic cost-effective-
ness analysis. Health Econ 1999; 8: 257-61 Clinical Research Network: complications of beta-thalassemiamajor in North America. Blood 2004; 104 (1): 34-931. Weinstein MC, Fineberg HV, Elstein AS, et al. Clinical decision
analysis. Philadelphia: W.B. Saunders, 1980: 260 39. Johnson ES, Sullivan SD, Mozaffari E, et al. A utility assess-32. Hirth RA, Chernew ME, Miller E, et al. Willingness to pay for a ment of oral and intravenous ganciclovir for the maintenance
quality-adjusted life year: in search of a standard. Med Decistreatment of AIDS-related cytomegalovirus retinitis. Pharma-Making 2000; 20 (3): 332-42coeconomics 1996; 10 (6): 623-933. Ubel PA, Hirth RA, Chernew ME, et al. What is the price of life
and why doesn’t it increase at the rate of inflation. Arch Intern 40. Cappellini MD, Bejaoui M, Agaoglu L, et al. Patient satisfactionMed 2003; 163: 1637-41 with deferasirox (exjade. Blood 2005; 106 (11 Pt 1): 759a
34. Pearson HA, Cohen AR, Giardina PJ, et al. The changing profileof homozygous beta-thalassemia: demography, ethnicity, andage distribution of current North American patients and Correspondence: Thomas E. Delea, Policy Analysis Inc.changes in two decades. Pediatrics 1996; 97 (3): 352-6
(PAI), Four Davis Court, Brookline, MA 02445, USA.35. RegenceRx Pharmacy Benefits Management. Therapeutic classreviewSM deferasirox (exjade®) [Novartis]. March 2006 [on- E-mail: [email protected]
© 2007 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2007; 25 (4)